Embed Size (px)
Citation preview

School-Based Interventions
What is Depression?
episode of sadness or apathy that lasts at least two consecutive weeks
interrupts daily activities

Symptoms Emotional Symptoms
Sad mood Loss of interest in daily
activities Hopelessness Sulking Withdrawal Inability to concentrate Impulsiveness Feeling lonely Nervousness Extreme mood swings Recurring thoughts of
death or suicide.
Physical Symptoms Pain:
Headaches Back pain Tender muscles Fatigue Dizziness Sleeping too
much/little Appetite:
Unusual cravings Loss of appetite Persistent nausea Diarrhea or constipation

Red Flag Expressions
“Nobody cares about me”
“I’m bored and just want to sleep”
“I don’t care anymore”
suggestions that they want to end their life

Suicide Ideation
People who are depressed are more likely to attempt suicide.
Warning signs talking about death or suicide threatening to hurt people engaging in aggressive or risky behavior
Anyone who appears suicidal should be taken very
seriously.
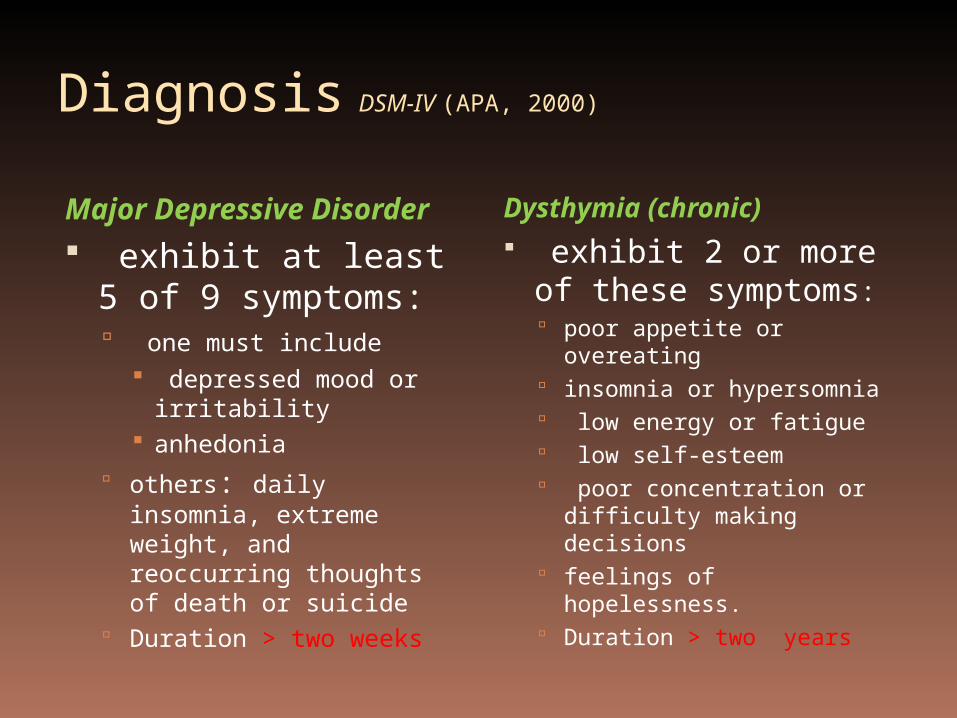
Diagnosis DSM-IV (APA, 2000)
Major Depressive Disorder
exhibit at least 5 of 9 symptoms: one must include
depressed mood or irritability
anhedonia others: daily insomnia,
extreme weight, and reoccurring thoughts of death or suicide
Duration > two weeks
Dysthymia (chronic) exhibit 2 or more
of these symptoms: poor appetite or
overeating insomnia or hypersomnia low energy or fatigue low self-esteem poor concentration or
difficulty making decisions
feelings of hopelessness. Duration > two years

Emergence & Prevalence
2% preteens and 5% adolescents (Battle, 2002)
Childhood rates: boys = girls Puberty rates: girls 2x boys (Bayridge Anxiety / Depression
Treatment Center, 2007)
In Saskatchewan: 9.8 % rate for urban, Caucasian youth 25% rate for First Nations youth on
reserves (Lemstra, A9).
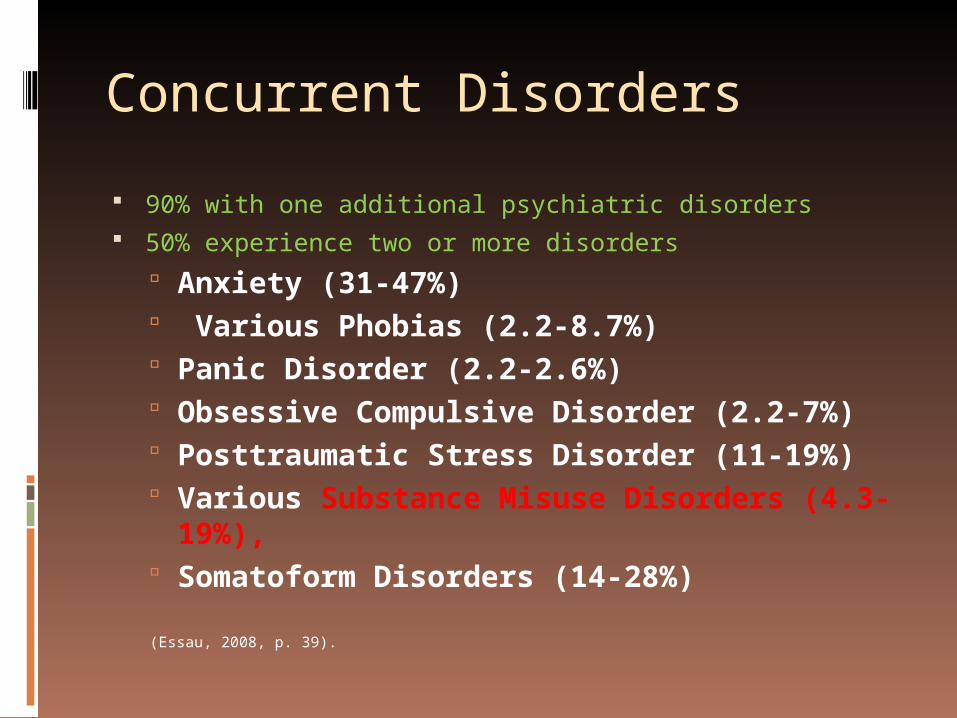
Concurrent Disorders
90% with one additional psychiatric disorders 50% experience two or more disorders
Anxiety (31-47%) Various Phobias (2.2-8.7%) Panic Disorder (2.2-2.6%) Obsessive Compulsive Disorder (2.2-7%) Posttraumatic Stress Disorder (11-19%) Various Substance Misuse Disorders (4.3-
19%), Somatoform Disorders (14-28%)
(Essau, 2008, p. 39).
Two Perspectives Medications for Depression
Antidepressants (SSRIs) change the levels of feel-good brain chemicals, serotonin. Prozac (fluoxetine) Zoloft (sertraline) Ludiomil (fluvoxamine) Paxil (paroxetine) Anafranil* (clomipramine)
selective serotonin reuptakeinhibitors (SSRIs) preferredover *tricyclic antidepressants(TCA)
Talk therapy (CBT) better cope with the
challenges of depression and life in general
help youth set realistic and positive personal goals
encourage participation in pleasant activities
learn to solve social problems
discourage negative thinking
foster assertiveness
Two Perspectives Treatment for Adolescent with Depression Study (NIMH, 2007)
Group 1 received medication only (Prozac) improvement : 60% (12 wks); 69% (18 wks)
Group 2 received medication combined with CBT (Prozac + CBT) improvement : 71% (12 wks); 85% (18 wks)
Group 3 received CBT only improvement : 44% (12 wks); 65% (18 wks) Suicidal thinking decreased in all active groups
Available at : https://trialweb.dcri.duke.edu/tads/tad/manuals/TADS_PT_Manual.pdf and
http://www.nimh.nih.gov/trials/practical/tads/questions-and-answers-about-the-nimh-treatment-for-adolescents-with-depression-study-tads.shtml
Alternative Strength-Based Perspective
Jonah Lehrer(2010), in Depression’s Upside
“capacity for intense focus” “reduced the possibility of becoming
distracted from the pressing problem” improve problem-solving “more aware and attentive” enhances “creative production” ie. Charles Darwin
Screening Measurements
Children's Depression Inventory (CDI) ages 7 to 17 ; 20-item self-report inventory
Beck Depression Inventory (BDI)adolescents; 21 m/c self-report inventory
Center for Epidemiologic Studies Depression (CES-DC) Scale www.brightfutures.org/mentalhealth/pdf/professionals/bridges/ces_dc.pdf
children & adolescents; 20-item self-report inventory(National Institute of Mental Health, n.d; Counselling Resource, 2002-11).

School-Based Interventions #1
Talk Therapy 1. Cognitive-Behavioral Therapy
focus on the ‘here and now’ focus on problem-solving strategies; goals Change maladaptive thinking patterns
2. Reality Therapy conversation-like ; open ended questions problem-solve and self-evaluate
School-Based Interventions #2 Group Counselling
teaching social skills in social and less threatening environment
openness food and drink availability relaxed, non-clinical environments part of the group

School-Based Interventions #3 Physical Activity
Walking, Running Yoga Kickboxing
More School-Based Interventions Mindfulness Meditation Breathing Exercises Gratitude Journal Light Therapy

Questions
Concerns
Worries
Beliefs

![Factors associated with health and work ability among long ... 5_1_2.pdfemotions, such as sadness, apathy and fear. In a study by Chen et al. [5], coping strategies based on self-blame](https://img.dokumen.tips/doc/110x75/5ecabd0b9e600e638c638c80/factors-associated-with-health-and-work-ability-among-long-512pdf-emotions.jpg)