Embed Size (px)
Citation preview

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 1
Your Policy gives You important information about Your health care benefits. It includes information such as Pre-Authorization requirements. This “Schedule of Benefits – Dental” is issued to You with Your Policy. It summarizes Your dental services benefits. Please keep Your “Schedule of Benefits – Dental” with Your Policy. Phoenix Health Plans, Inc. will notify You if any changes are needed. We are partnering with DentaQuest of Arizona, LLC (DentaQuest) to provide the dental services that are covered under this plan. If You have any questions about the dental services covered under this plan, please call Our Customer Service Department at (855) 463-7275 or TTY: (855) 463-7279. Getting Dental Services DentaQuest contracts with dentists to provide dental services to Members. These contracted dentists are referred to as Participating Dentists in this “Schedule of Benefits – Dental”. Our provider directory has a list of Participating Dentists. To find a Participating Dentist, visit:
www.phxchoice.com/ProviderDirectory You may schedule appointments by calling a participating general dental office directly. Be sure to check that the dental office is participating with Us and DentaQuest before making each dental appointment and before receiving services. You must get Pre-Authorization before getting dental services. Call Our Customer Service Department or the Pre-Authorization Hotline at (855) 463-7275 or TTY: (855) 463-7279 to be sure the proposed service has received Pre-Authorization before getting the service. It is important to keep Your scheduled appointments. If You need to cancel, please call the dental office within 24 hours before Your scheduled visit. You are responsible for any fees for missed appointments. Specialist Services DentaQuest contracts with dental specialists in all fields: oral surgeons for extractions, periodontists for treatment of the gums, endodontists who specialize in root canals, and pedodontists and orthodontists for children. Please call Our Customer Service Department for more information if You need help finding a dental specialist. Emergency Services Members are covered for emergency dental services at participating dental offices. If You have a dental emergency, please call a participating dental office. If the office is not available immediately, call Us for assistance with obtaining an emergency appointment. In case of an acute emergency, seek immediate hospital care. Emergency office visits may be subject to additional charges. Members are also covered for emergency dental services while temporarily more than 50 miles from a Participating Dentist. Palliative treatment should be obtained from a licensed dentist and payment made for services rendered.

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 2
Members are reimbursed the usual and customary fees for covered dental services, subject to any applicable fees, not exceeding $100 per claim. To receive reimbursement, You must submit the following information within 90 days of the date of service:
Paid receipt
Member’s name
ID number
Address
Phone number
Policy Holder’s name and ID number
Any other supporting documentation necessary to process the reimbursement NOTE: Palliative (emergency) treatment of dental pain – minor Member Cost Sharing
Pediatric Members – Pediatric dental services are available to Members through the month of their 19th birthday. Class I services are covered in full with no Deductible. Class II, Class III and Class IV services are covered at 50% Coinsurance after a $100 Deductible. (The Deductible only applies to Classes II through IV.) Once the Member reaches the applicable integrated medical, drug and pediatric dental Annual Maximum Out-of-Pocket amount, the plan will cover 100% of costs for all Covered Services. (Please see Your Schedule of Benefits for the applicable Annual Maximum Out-of-Pocket.)
Adult Members – Adult dental services are available to Members age 19 and older. Class I services are covered in full with no Deductible. Class II services are covered at 50% Coinsurance after a $100 deductible. (The Deductible applies to Class II only.) The plan will cover up to $500 in Covered Services per Plan Year. NOTE: There is no coverage for Class III or Class IV services.
See Covered Services below for more information on what services are covered under this plan. There is no out of network coverage except in the case of emergencies (see Emergency Services above for more information). You are responsible for the entire cost of the service if You see a non-participating dentist. NOTE: Information on cost sharing and zero and limited cost share plan variants:
The adult dental Services covered under this plan are not Essential Health Benefits. The adult dental Services covered under this plan are subject to the cost sharing amounts outlined in this “Schedule of Benefits – Dental”. The pediatric dental Services covered under this plan are Essential Health Benefits. Cost sharing for pediatric dental Services are as follows:
For Members enrolled in a zero cost share plan variations: There is no cost sharing for covered pediatric dental Services received from an Indian Health Service dental provider or

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 3
Participating Dentist.
For Members enrolled in a limited cost share plan variations: There is no cost sharing for covered pediatric dental Services provided by an Indian Health Service dental provider. You must get a referral from Purchased/Referred Care (formerly Contract Health Services) to avoid cost sharing for covered pediatric dental Services with any other Participating Dentists.
Please see Your Policy for more information about zero and limited cost share plans. If You have any questions, please contact Our Customer Service Department.
Covered Services This “Schedule of Benefits – Dental” lists all of the dental services, procedures, treatment and supplies that are covered under this plan, the cost (if any) for each covered procedure and any Benefit Maximums (limitations) that apply to each Covered Service.
Services covered under this plan are identified by current dental terminology (CDT) code. Please see the following sections in this “Schedule of Benefits – Dental” for services by CDT codes covered under this plan:
Covered Services – Pediatric Dental Services:
(1) Class I Services: Diagnostic and Preventive Services
(2) Class II Services: Restorative and Other Basic Dental Services
(3) Class III Services: Complex and Major Restorative Dental Services
(4) Class IV Services: Orthodontic Services (Medically Necessary Orthodontic Treatment)
Covered Services – Adult Dental Services:
(1) Class I Services: Diagnostic and Preventive Services
(2) Class II Services: Restorative and Other Basic Dental Services CDT codes not listed are excluded from coverage under this plan. Covered Services are available only while You are covered under this plan. You are responsible for payment for any services not covered under this plan. Services are subject to Pre-Authorization or review by DentaQuest and/or Us. An alternate benefit may be paid. You have the right to benefits on a non-discriminatory basis for the Covered Services listed in this “Schedule of Benefits – Dental”. Please note that benefits and coverage may vary based on patient’s age at date of service. Pediatric Dental Services Pediatric dental benefits are available for Members through the month of their 19th birthday. This plan includes coverage of pediatric dental services as required under the PPACA.

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 4
(1) Class I Services: Diagnostic and Preventive Services
Benefits are available for the following dental services to diagnose or to prevent tooth decay and other forms of oral disease:
Class I Services: Diagnostic and Preventive Services
CDT Code Description Benefit Maximum Cost Share You Pay
D0120 Periodic oral evaluation – established patient
Once in 6 months $0
D0140 Limited oral evaluation – problem focused Once in 6 months
D0150 Comprehensive oral evaluation – new or established patient
Once in 6 months
D0180 Comprehensive periodontal evaluation – new or established patient
Once in 6 months
D0210 Intraoral – complete set of radiographic images
Once in 60 months, including bitewings
D0220 Intraoral – periapical first radiographic image
D0230 Intraoral – periapical each additional radiographic image
D0240 Intraoral – occlusal radiographic image
D0270 Bitewing – single radiographic image 1 set every 6 months
D0272 Bitewings – two radiographic images 1 set every 6 months
D0274 Bitewings – four radiographic images 1 set every 6 months
D0277 Vertical bitewings – 7 to 8 radiographic images
1 set every 6 months
D0330 Panoramic radiographic image Once in 60 months
D0470 Diagnostic casts
D1110 Prophylaxis – over age 14 Once in 6 months
D1120 Prophylaxis – ages 1-13 Once in 6 months
D1206 Topical application of fluoride varnish Twice in 12 months
D1208 Topical application of fluoride Once in 6 months
D1351 Sealant – per tooth Once per tooth per 36 months on occlusal surface of permanent molars
D1352 Preventive resin restoration in a moderate to high caries risk patient – permanent tooth
Once per tooth per 36 months on occlusal surface of permanent molars
D1510 Space maintainer – fixed – unilateral
D1515 Space maintainer – fixed – bilateral
D1520 Space maintainer – removable – unilateral
D1525 Space maintainer – removable – bilateral
D1550 Re-cementation of space maintainer
D9110 Palliative (emergency) treatment of dental pain – minor procedure

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 5
(2) Class II Services: Restorative and Other Basic Dental Services Benefits are available for the following dental services to treat oral disease:
Class II Services: Restorative and Other Basic Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D0391 Interpretation of diagnostic image by a practitioner not associated with capture of the image, including report
50% Coinsurance after $100 Deductible D2140 Amalgam – one surface, primary or
permanent
D2150 Amalgam – two surfaces, primary or permanent
D2160 Amalgam – three surfaces, primary or permanent
D2161 Amalgam – four or more surfaces, primary or permanent
D2330 Resin-based composite – one surface, anterior
D2331 Resin-based composite – two surfaces, anterior
D2332 Resin-based composite – three surfaces, anterior
D2335 Resin-based composite – four or more surfaces or involving incisal angle (anterior)
D2910 Recement inlay, onlay or partial coverage restoration
D2920 Recement crown
D2929 Prefabricated porcelain/ceramic crown – primary tooth
Once per tooth per 24 months on anterior primary teeth
D2930 Prefabricated stainless steel crown – primary tooth
Under age 15 – limited to once per tooth per 60 months
D2931 Prefabricated stainless steel crown – permanent tooth
Under age 15 – limited to once per tooth per 60 months
D2940 Protective restoration
D2951 Pin retention – per tooth, in addition to restoration

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 6
Class II Services: Restorative and Other Basic Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D3220 Therapeutic pulpotomy (excluding final restoration) – removal of pulp coronal to the dentinocemental junction and application of medicament
Limited to primary incisor teeth form members up to age 6 and for primary molars and cuspids up to age 11 and is limited to one per tooth per lifetime
50% Coinsurance after $100 Deductible
D3222 Partial pulpotomy for apexogenesis – permanent tooth with incomplete root development
Limited to primary incisor teeth form members up to age 6 and for primary molars and cuspids up to age 11 and is limited to one per tooth per lifetime
D3230 Pulpal therapy (resorbable filling) – anterior, primary tooth (excluding final restoration)
Limited to primary incisor teeth form members up to age 6 and for primary molars and cuspids up to age 11 and is limited to one per tooth per lifetime
D3240 Pulpal therapy (resorbable filling) – posterior, primary tooth (excluding final restoration)
Limited to primary incisor teeth form members up to age 6 and for primary molars and cuspids up to age 11 and is limited to one per tooth per lifetime
D4341 Periodontal scaling and root planing – four or more teeth per quadrant
Limited to 1 every 24 months
D4342 Periodontal scaling and root planing – one to three teeth per quadrant
Limited to 1 every 24 months
D4910 Periodontal maintenance 4 in 12 months combined with adult prophylaxis after the completion of active periodontal therapy
D5410 Adjust complete denture – maxillary
D5411 Adjust complete denture – mandibular
D5421 Adjust partial denture – maxillary
D5422 Adjust partial denture – mandibular
D5510 Repair broken complete denture base
D5520 Replace missing or broken teeth – complete denture (each tooth)
D5610 Repair resin denture base
D5620 Repair cast framework
D5630 Repair or replace broken clasp
D5640 Replace broken teeth – per tooth
D5650 Add tooth to existing partial denture

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 7
Class II Services: Restorative and Other Basic Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D5660 Add clasp to existing partial denture 50% Coinsurance after $100 Deductible
D5710 Rebase complete maxillary denture Once per arch per 36 months (after 6 months have elapsed since initial placement)
D5720 Rebase maxillary partial denture Once per arch per 36 months (after 6 months have elapsed since initial placement)
D5721 Rebase mandibular partial denture Once per arch per 36 months (after 6 months have elapsed since initial placement)
D5730 Reline complete maxillary denture (chairside)
Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)
D5731 Reline complete mandibular denture (chairside)
Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)
D5740 Reline maxillary partial denture (chairside) Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)
D5741 Reline mandibular partial denture (chairside)
Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)
D5750 Reline complete maxillary denture (laboratory)
Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 8
Class II Services: Restorative and Other Basic Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D5751 Reline complete mandibular denture (laboratory)
Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)
50% Coinsurance after $100 Deductible
D5760 Reline maxillary partial denture (laboratory)
Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)
D5761 Reline mandibular partial denture (laboratory)
Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)
D5850 Tissue conditioning, maxillary Not allowed within 6 months of initial placement
D5851 Tissue conditioning, mandibular Not allowed within 6 months of initial placement
D7140 Extraction, erupted tooth or exposed root (elevation and/or forceps removal)
D7210 Surgical removal of erupted tooth requiring removal of bone and/or sectioning of tooth, and including elevation of mucoperiosteal flap if indicated
D7220 Removal of impacted tooth – soft tissue
D7230 Removal of impacted tooth – partially bony
D7240 Removal of impacted tooth – completely bony
D7241 Removal of impacted tooth – completely bony, with unusual surgical complications
D7250 Surgical removal of residual tooth roots (cutting procedure)
D7251 Coronectomy – intentional partial tooth removal
D7270 Tooth reimplantation and/or stabilization of accidentally evulsed or displaced tooth

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 9
Class II Services: Restorative and Other Basic Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D7280 Surgical access of an unerupted tooth 50% Coinsurance after $100 Deductible
D7310 Alveoloplasty in conjunction with extractions – four or more teeth or tooth spaces, per quadrant
D7311 Alveoloplasty in conjunction with extractions – one to three teeth or tooth spaces, per quadrant
D7320 Alveoloplasty not in conjunction with extractions – four or more teeth or tooth spaces, per quadrant
D7321 Alveoloplasty not in conjunction with extractions – one to three teeth or tooth spaces, per quadrant
D7471 Removal of lateral exostosis (maxilla or mandible)
D7510 Incision and drainage of abscess – intraoral soft tissue
D7910 Suture of recent small wounds up to 5 cm Individual consideration
D7921 Collection and application of autologous blood concentrate product
D7971 Excision of pericoronal gingiva
D9220 Deep sedation/general synesthesia – first 30 minutes
D9221 Deep sedation/general anesthesia – each additional 15 minutes
D9241 Intravenous conscious sedation/analgesia – first 30 minutes
D9242 Intravenous conscious sedation/analgesia – each additional 15 minutes
D9310 Consultation – diagnostic service provided by dentist or physician other than requesting dentist or physician
D9610 Therapeutic parenteral drug, single administration
D9930 Treatment of complications (post-surgical) – unusual circumstances, by report
Individual consideration

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 10
(3) Class III: Complex and Major Restorative Dental Services Benefits are available for the following dental services and supplies to treat oral disease:
Class III Services: Complex and Major Restorative Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D0160 Detailed and extensive oral evaluation – problem focused, by report
50% coinsurance after $100 deductible
D2510 Inlay – metallic – one surface
D2520 Inlay – metallic – two surfaces
D2530 Inlay – metallic – three or more surfaces
D2542 Onlay – metallic – two surfaces Once per tooth per 60 months
D2543 Onlay – metallic – three surfaces Once per tooth per 60 months
D2544 Onlay – metallic – four or more surfaces Once per tooth per 60 months
D2740 Crown – porcelain/ceramic substrate Once per tooth per 60 months
D2750 Crown – porcelain fused to high noble metal
Once per tooth per 60 months
D2751 Crown – porcelain fused to predominantly base metal
Once per tooth per 60 months
D2752 Crown – porcelain fused to noble metal Once per tooth per 60 months
D2780 Crown – 3/4 cast high noble metal Once per tooth per 60 months
D2781 Crown – 3/4 cast predominantly base metal
Once per tooth per 60 months
D2783 Crown – 3/4 porcelain/ceramic Once per tooth per 60 months
D2790 Crown – full cast high noble metal Once per tooth per 60 months
D2791 Crown – full cast predominantly base metal
Once per tooth per 60 months
D2792 Crown – full cast noble metal Once per tooth per 60 months
D2794 Crown - titanium Once per tooth per 60 months
D2950 Core buildup, including any pins when required
Once per tooth per 60 months
D2954 Prefabricated post and core in addition to crown
Once per tooth per 60 months
D2980 Crown repair necessitated by restorative material failure

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 11
Class III Services: Complex and Major Restorative Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D2981 Inlay repair necessitated by restorative material failure
50% coinsurance after $100 deductible
D2982 Onlay repair necessitated by restorative material failure
Once per year per tooth after 24 months of crown insertion
D2983 Veneer repair necessitated by restorative material failure
D2990 Resin infiltration of incipient smooth surface lesions
D3310 Endodontic therapy, anterior tooth (excluding final restoration)
D3320 Endodontic therapy, bicuspid tooth (excluding final restoration)
D3330 Endodontic therapy, molar (excluding final restoration)
D3346 Retreatment of previous root canal therapy – anterior
D3347 Retreatment of previous root canal therapy – bicuspid
D3348 Retreatment of previous root canal therapy – molar
D3351 Apexification/recalcification – initial visit (apical closure/calcific repair of perforations, root resorption, pulp space disinfection, etc.)
D3352 Apexification/recalcification – interim medication replacement (apical closure/calcific repair of perforations, root resorption, pulp space disinfection, etc.)
D3353 Apexification/recalcification – final visit (includes completed root canal therapy – apical closure/calcific repair of perforations, root resorption, etc.)
D3410 Apicoectomy – anterior
D3421 Apicoectomy – bicuspid (first root)
D3425 Apicoectomy – molar (first root)
D3426 Apicoectomy (each additional root)
D3450 Root amputation – per root
D3920 Hemisection (including any root removal), not including root canal therapy
D4210 Gingivectomy or gingivoplasty – four or more contiguous teeth or tooth bounded spaces per quadrant
Once per quadrant per 36 months

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 12
Class III Services: Complex and Major Restorative Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D4211 Gingivectomy or gingivoplasty – one to three contiguous teeth or tooth bounded spaces per quadrant
50% coinsurance after $100 deductible D4212 Gingivectomy or gingivoplasty to allow
access for restorative procedure, per tooth
Once per quadrant per 36 months
D4240 Gingival flap procedure, including root planing, four or more contiguous teeth or tooth bounded spaces per quadrant
Once per quadrant per 36 months
D4249 Clinical crown lengthening – hard tissue
D4260 Osseous surgery (including flap entry and closure) – four or more contiguous teeth or tooth bounded spaces per quadrant
Once per quadrant per 36 months
D4270 Pedicle soft tissue graft procedure
D4273 Subepithelial connective tissue graft procedures, per tooth
D4277 Free soft tissue graft procedure (including donor site surgery), first tooth or edentulous tooth position in graft
Once per site/tooth per 36 months on the buccal surfaces of natural only. Not to exceed two sites/teeth per quadrant per 36 months
D4278 Free soft tissue graft procedure (including donor site surgery), each additional contiguous tooth or edentulous tooth position in same graft site
Two teeth per quadrant per 36 month on natural teeth only
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosis
Once per lifetime
D5110 Complete denture – maxillary Once per arch per 60 months
D5120 Complete denture – mandibular Once per arch per 60 months
D5130 Immediate denture – maxillary Once per arch per 60 months
D5140 Immediate denture – mandibular Once per arch per 60 months
D5211 Maxillary partial denture – resin base (including any conventional clasps, rests and teeth)
Once per arch per 60 months
D5212 Mandibular partial denture – resin base (including any conventional clasps, rests and teeth)
Once per arch per 60 months

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 13
Class III Services: Complex and Major Restorative Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D5213 Maxillary partial denture – cast metal framework with resin denture bases (including any conventional clasps, rests and teeth)
Once per arch per 60 months
50% coinsurance after $100 deductible
D5214 Mandibular partial denture – cast metal framework with resin denture bases (including any conventional clasps, rests and teeth)
Once per arch per 60 months
D5281 Removable unilateral partial denture – one piece cast metal
Once per arch per 60 months. Not to be combined with any other denture in the same arch
D6010 Surgical placement of implant body – endosteal implant
Once every 60 months
D6012 Surgical placement of interim implant body for transitional prosthesis – endosteal implant
Once every 60 months
D6040 Surgical placement – eposteal implant Once per tooth per 60 months
D6050 Surgical placement – transosteal implant Once per tooth per 60 months
D6053 Implant/abutment supported removable denture for completely endentulous arch
Once per 60 months per arch
D6054 Implant/abutment supported removable denture for partially edentulous arch
Once per 60 months per arch
D6055 Connecting bar – implant supported or abutment supported
Once per tooth per 60 months
D6056 Prefabricated abutment – includes modification and placement
Once per tooth per 60 months
D6058 Abutment supported porcelain/ceramic crown
Once per tooth per 60 months
D6059 Abutment supported porcelain fused to metal crown (high noble metal)
Once per tooth per 60 months
D6060 Abutment supported porcelain fused to metal crown (predominantly base metal)
Once per tooth per 60 months
D6061 Abutment supported porcelain fused to metal crown (noble metal)
Once per tooth per 60 months
D6062 Abutment supported cast metal crown (high noble metal)
Once per tooth per 60 months
D6063 Abutment supported cast metal crown (predominantly base metal)
Once per tooth per 60 months
D6064 Abutment supported cast metal crown (noble metal)
Once per tooth per 60 months
Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 14
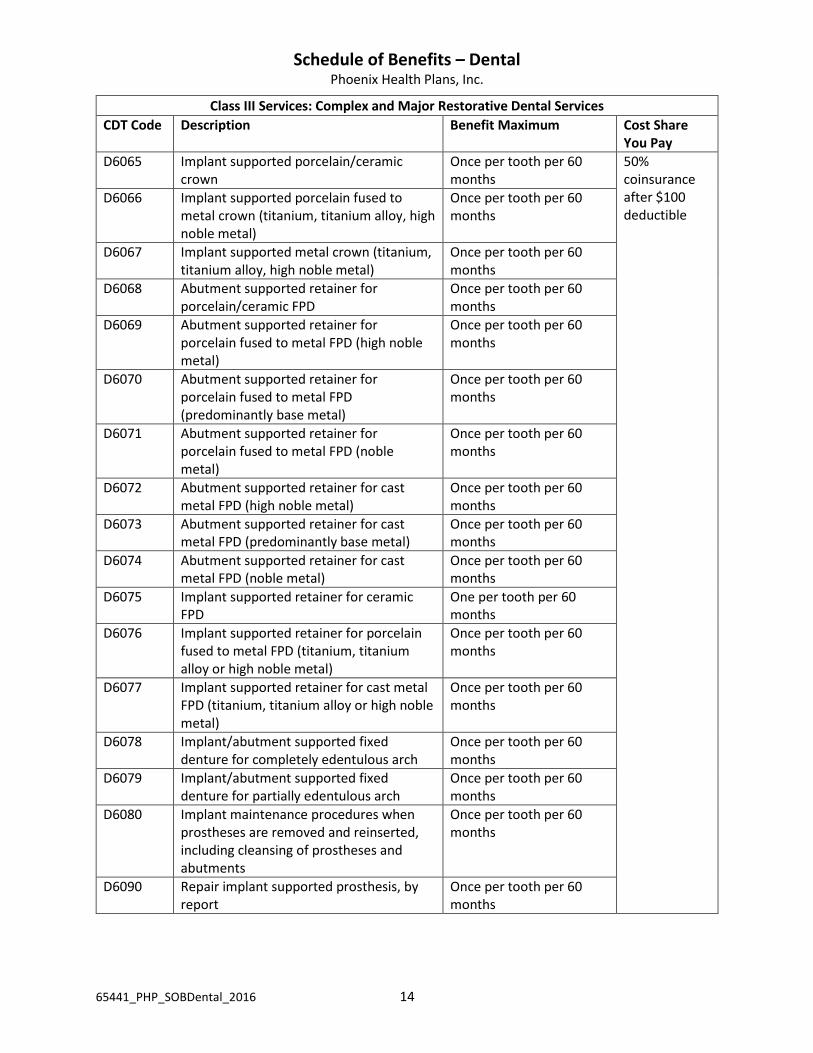
Class III Services: Complex and Major Restorative Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D6065 Implant supported porcelain/ceramic crown
Once per tooth per 60 months
50% coinsurance after $100 deductible
D6066 Implant supported porcelain fused to metal crown (titanium, titanium alloy, high noble metal)
Once per tooth per 60 months
D6067 Implant supported metal crown (titanium, titanium alloy, high noble metal)
Once per tooth per 60 months
D6068 Abutment supported retainer for porcelain/ceramic FPD
Once per tooth per 60 months
D6069 Abutment supported retainer for porcelain fused to metal FPD (high noble metal)
Once per tooth per 60 months
D6070 Abutment supported retainer for porcelain fused to metal FPD (predominantly base metal)
Once per tooth per 60 months
D6071 Abutment supported retainer for porcelain fused to metal FPD (noble metal)
Once per tooth per 60 months
D6072 Abutment supported retainer for cast metal FPD (high noble metal)
Once per tooth per 60 months
D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)
Once per tooth per 60 months
D6074 Abutment supported retainer for cast metal FPD (noble metal)
Once per tooth per 60 months
D6075 Implant supported retainer for ceramic FPD
One per tooth per 60 months
D6076 Implant supported retainer for porcelain fused to metal FPD (titanium, titanium alloy or high noble metal)
Once per tooth per 60 months
D6077 Implant supported retainer for cast metal FPD (titanium, titanium alloy or high noble metal)
Once per tooth per 60 months
D6078 Implant/abutment supported fixed denture for completely edentulous arch
Once per tooth per 60 months
D6079 Implant/abutment supported fixed denture for partially edentulous arch
Once per tooth per 60 months
D6080 Implant maintenance procedures when prostheses are removed and reinserted, including cleansing of prostheses and abutments
Once per tooth per 60 months
D6090 Repair implant supported prosthesis, by report
Once per tooth per 60 months

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 15
Class III Services: Complex and Major Restorative Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D6091 Replacement of semi-precision or precision attachment (male or female component) of implant/abutment supported prosthesis, per attachment
Once per tooth per 60 months
50% coinsurance after $100 deductible
D6095 Repair implant abutment, by report Once per tooth per 60 months
D6100 Implant removal, by report Once per tooth per 60 months
D6101 Debridement of a periimplant defect and surface cleaning of exposed implant surfaces, including flap entry and closure
D6102 Debridement and osseous contouring of a periimplant defect; includes surface cleaning of exposed implant surfaces and flap entry and closure
D6103 Bone graft for repair of perrimplant defect – not including flap entry and closure or, when indicated, placement of a barrier membrane or biologic materials to aid in osseous regeneration
D6104 Bone graft at time of implant placement
D6190 Radiographic/surgical implant index, by report
Once per tooth per 60 months
D6210 Pontic – cast high noble metal Once per tooth per 60 months
D6211 Pontic – cast predominantly base metal Once per tooth per 60 months
D6212 Pontic – cast noble metal Once per tooth per 60 months
D6214 Pontic – titanium Once per tooth per 60 months
D6240 Pontic – porcelain fused to high noble metal
Once per tooth per 60 months
D6241 Pontic – porcelain fused to predominantly base metal
Once per tooth per 60 months
D6242 Pontic – porcelain fused to noble metal Once per tooth per 60 months
D6245 Pontic – porcelain/ceramic Once per tooth per 60 months as an alternate benefit for porcelain fused to metal pontic (D6240)
D6545 Retainer – cast metal for resin bonded fixed prosthesis
Once per tooth per 60 months

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 16
Class III Services: Complex and Major Restorative Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D6548 Retainer – porcelain/ceramic for resin bonded fixed prosthesis
Once per tooth per 60 months
50% coinsurance after $100 deductible
D6740 Crown – porcelain/ceramic Once per tooth per 60 months
D6750 Crown – porcelain fused to high noble metal
Once per tooth per 60 months
D6751 Crown – porcelain fused to predominantly base metal
Once per tooth per 60 months
D6752 Crown – porcelain fused to noble metal Once per tooth per 60 months
D6780 Crown – 3/4 cast high noble metal Once per tooth per 60 months
D6781 Crown – 3/4 cast predominantly base metal
Once per tooth per 60 months
D6782 Crown – 3/4 cast noble metal Once per tooth per 60 months
D6783 Crown – 3/4 porcelain/ceramic Once per tooth per 60 months
D6790 Crown – full cast high noble metal Once per tooth per 60 months
D6791 Crown – full cast predominantly base metal
Once per tooth per 60 months
D6792 Crown – full cast noble metal Once per tooth per 60 months
D6930 Recement fixed partial denture
D6980 Fixed partial denture repair necessitated by restorative material failure
D9940 Occlusal guard, by report 1 in 12 months for members 13 years and older
(4) Class IV: Orthodontic Services (Medically Necessary Orthodontic Treatment)
This plan does not provide an orthodontic benefit except for Medically Necessary Orthodontic Treatment. Medically Necessary Orthodontic Treatment is defined as those circumstances where the Member’s condition creates a medical disability and impairment to their overall physical development. DentaQuest’s licensed dentists/specialists will review requests and make determinations. There is a waiting period of 24 months from the Effective Date of coverage for each Member under this Policy before that Member becomes eligible for Medically Necessary Orthodontic Treatment. The following is a list of Covered Services for Medically Necessary Orthodontic Treatment.

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 17
Class IV Services: Orthodontic Services (Medically Necessary Orthodontic Treatment)
CDT Code Description Benefit Maximum Cost Share You Pay
D0340 Cephalometric radiographic image 50% coinsurance after $100 deductible
D0350 Oral/facial photographic images obtained intraorally or extraorally
D8010 Limited orthodontic treatment of the primary dentition
D8020 Limited orthodontic treatment of the transitional dentition
D8030 Limited orthodontic treatment of the adolescent dentition
D8050 Interceptive orthodontic treatment of the primary dentition
D8060 Interceptive orthodontic treatment of the transitional dentition
D8070 Comprehensive orthodontic treatment of the transitional dentition
D8080 Comprehensive orthodontic treatment of the adolescent dentition
D8210 Removable appliance therapy
D8220 Fixed appliance therapy
D8660 Pre-orthodontic treatment visit
D8670 Periodic orthodontic treatment visit (as part of contract)
D8680 Orthodontic retention (removal of appliances, construction and placement of retainer(s))
Adult Dental Services Coverage for adult dental services are limited to the Class I and Class II Covered Services listed below. The plan will cover up to $500 in Covered Services per Plan Year. (1) Class I Services: Diagnostic and Preventive Services Benefits are available for the following dental services to diagnose or to prevent tooth decay and other forms of oral disease:
Class I Services: Diagnostic and Preventive Services
CDT Code Description Benefit Maximum Cost Share You Pay
D0120 Periodic oral evaluation – established patient
Once in 6 months $0
D0140 Limited oral evaluation – problem focused Once in 6 months
D0150 Comprehensive oral evaluation – new or established patient
Once in 6 months

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 18
Class I Services: Diagnostic and Preventive Services
CDT Code Description Benefit Maximum Cost Share You Pay
D0180 Comprehensive periodontal evaluation – new or established patient
Once in 6 months $0
D0210 Intraoral – complete set of radiographic images
Once in 60 months, including bitewings
D0220 Intraoral – periapical first radiographic image
D0230 Intraoral – periapical each additional radiographic image
D0240 Intraoral – occlusal radiographic image
D0270 Bitewing – single radiographic image 1 set every calendar year
D0272 Bitewings – two radiographic images 1 set every calendar year
D0274 Bitewings – four radiographic images 1 set every calendar year
D0277 Vertical bitewings – 7 to 8 radiographic images
1 set every calendar year
D0330 Panoramic radiographic image Once in 60 months
D0470 Diagnostic casts
D1206 Topical application of fluoride varnish Once in 12 months
D1208 Topical application of fluoride Once in 6 months
D9110 Palliative (emergency) treatment of dental pain – minor procedure
3 times per year with supporting documentation
(2) Class II Services: Restorative and Other Basic Dental Services Benefits are available for the following dental services to treat oral disease:
Class II Services: Restorative and Other Basic Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D0391 Interpretation of diagnostic image by a practitioner not associated with capture of the image, including report
50% coinsurance after $100 deductible D2140 Amalgam – one surface, primary or
permanent
D2150 Amalgam – two surfaces, primary or permanent
D2160 Amalgam – three surfaces, primary or permanent
D2161 Amalgam – four or more surfaces, primary or permanent
D2330 Resin-based composite – one surface, anterior
D2331 Resin-based composite – two surfaces, anterior

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 19
Class II Services: Restorative and Other Basic Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D2332 Resin-based composite – three surfaces, anterior
50% coinsurance after $100 deductible
D2335 Resin-based composite – four or more surfaces or involving incisal angle (anterior)
D2910 Recement inlay, onlay or partial coverage restoration
D2920 Recement crown
D2929 Prefabricated porcelain/ceramic crown – primary tooth
Once per tooth per 24 months on anterior primary teeth
D2940 Protective restoration
D2951 Pin retention – per tooth, in addition to restoration
D4341 Periodontal scaling and root planing – four or more teeth per quadrant
Limited to 1 every 24 months
D4342 Periodontal scaling and root planing – one to three teeth per quadrant
Limited to 1 every 24 months
D4910 Periodontal maintenance 4 in 12 months combined with adult prophylaxis after the completion of active periodontal therapy
D5410 Adjust complete denture – maxillary
D5411 Adjust complete denture – mandibular
D5421 Adjust partial denture – maxillary
D5422 Adjust partial denture – mandibular
D5510 Repair broken complete denture base
D5520 Replace missing or broken teeth – complete denture (each tooth)
D5610 Repair resin denture base
D5620 Repair cast framework
D5630 Repair or replace broken clasp
D5640 Replace broken teeth – per tooth
D5650 Add tooth to existing partial denture
D5660 Add clasp to existing partial denture
D5710 Rebase complete maxillary denture Once per arch per 36 months (after 6 months have elapsed since initial placement)
D5720 Rebase maxillary partial denture Once per arch per 36 months (after 6 months have elapsed since initial placement)

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 20
Class II Services: Restorative and Other Basic Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D5721 Rebase mandibular partial denture Once per arch per 36 months (after 6 months have elapsed since initial placement)
50% coinsurance after $100 deductible
D5730 Reline complete maxillary denture (chairside)
Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)
D5731 Reline complete mandibular denture (chairside)
Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)
D5740 Reline maxillary partial denture (chairside) Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)
D5741 Reline mandibular partial denture (chairside)
Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)
D5750 Reline complete maxillary denture (laboratory)
Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)
D5751 Reline complete mandibular denture (laboratory)
Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 21
Class II Services: Restorative and Other Basic Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D5760 Reline maxillary partial denture (laboratory)
Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)
50% coinsurance after $100 deductible
D5761 Reline mandibular partial denture (laboratory)
Once per arch per 36 months after 6 months from insertion date have elapsed. (3 months from insertion date of an immediate denture)
D5850 Tissue conditioning, maxillary Once per 60 months per arch
D5851 Tissue conditioning, mandibular Once per 60 months per arch
D7140 Extraction, erupted tooth or exposed root (elevation and/or forceps removal)
D7210 Surgical removal of erupted tooth requiring removal of bone and/or sectioning of tooth, and including elevation of mucoperiosteal flap if indicated
D7220 Removal of impacted tooth – soft tissue
D7230 Removal of impacted tooth – partially bony
D7240 Removal of impacted tooth – completely bony
D7241 Removal of impacted tooth – completely bony, with unusual surgical complications
D7250 Surgical removal of residual tooth roots (cutting procedure)
D7251 Coronectomy – intentional partial tooth removal
D7270 Tooth reimplantation and/or stabilization of accidentally evulsed or displaced tooth
D7280 Surgical access of an unerupted tooth
D7310 Alveoloplasty in conjunction with extractions – four or more teeth or tooth spaces, per quadrant
D7311 Alveoloplasty in conjunction with extractions – one to three teeth or tooth spaces, per quadrant

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 22
Class II Services: Restorative and Other Basic Dental Services
CDT Code Description Benefit Maximum Cost Share You Pay
D7320 Alveoloplasty not in conjunction with extractions – four or more teeth or tooth spaces, per quadrant
50% coinsurance after $100 deductible D7321 Alveoloplasty not in conjunction with
extractions – one to three teeth or tooth spaces, per quadrant
D7471 Removal of lateral exostosis (maxilla or mandible)
D7510 Incision and drainage of abscess – intraoral soft tissue
D7910 Suture of recent small wounds up to 5 cm Individual consideration
D7921 Collection and application of autologous blood concentrate product
D7971 Excision of pericoronal gingiva
D9220 Deep sedation/general synesthesia – first 30 minutes
D9221 Deep sedation/general anesthesia – each additional 15 minutes
D9241 Intravenous conscious sedation/analgesia – first 30 minutes
D9242 Intravenous conscious sedation/analgesia – each additional 15 minutes
D9610 Therapeutic parenteral drug, single administration
D9930 Treatment of complications (post-surgical) – unusual circumstances, by report
Individual consideration
Exclusions The exclusions in this section apply to all pediatric dental services and adult dental services benefits. Although We may list a specific service as a benefit, We will not cover it unless DentaQuest and/or We determine it necessary for the prevention, diagnosis, care or treatment of a covered condition. The following are not covered under this plan’s pediatric dental services or adult dental services benefit:
Services and treatment provided or commenced prior to the effective date of the Member’s coverage under the Policy or after the termination date of coverage unless otherwise indicated.
Services and treatment not described as a Covered Service in this “Schedule of Benefits – Dental”. (See the section “Covered Services” for a list of services and treatment that are covered under this plan.)
Dental procedures, services, treatment or supplies not prescribed or under the direct supervision of a dentist.
Experimental or investigational services and treatments.
Services and treatment which are for any Illness or Bodily Injury which occurs in the course of
Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 23
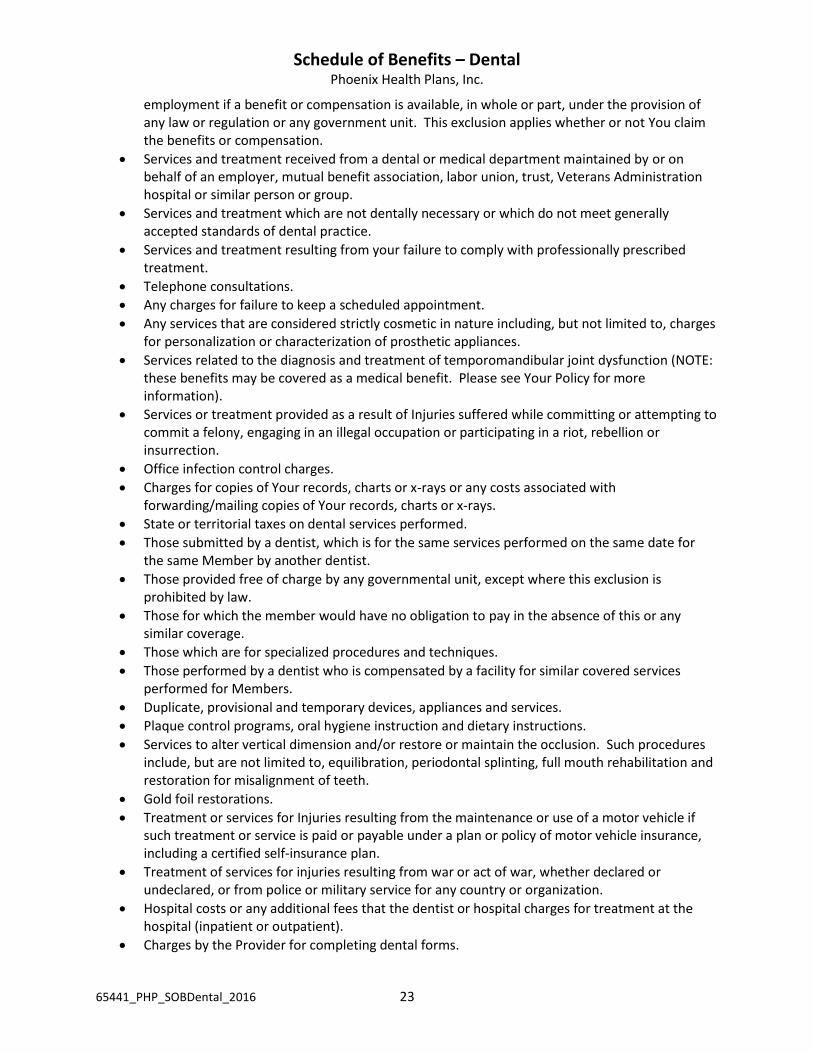
employment if a benefit or compensation is available, in whole or part, under the provision of any law or regulation or any government unit. This exclusion applies whether or not You claim the benefits or compensation.
Services and treatment received from a dental or medical department maintained by or on behalf of an employer, mutual benefit association, labor union, trust, Veterans Administration hospital or similar person or group.
Services and treatment which are not dentally necessary or which do not meet generally accepted standards of dental practice.
Services and treatment resulting from your failure to comply with professionally prescribed treatment.
Telephone consultations.
Any charges for failure to keep a scheduled appointment.
Any services that are considered strictly cosmetic in nature including, but not limited to, charges for personalization or characterization of prosthetic appliances.
Services related to the diagnosis and treatment of temporomandibular joint dysfunction (NOTE: these benefits may be covered as a medical benefit. Please see Your Policy for more information).
Services or treatment provided as a result of Injuries suffered while committing or attempting to commit a felony, engaging in an illegal occupation or participating in a riot, rebellion or insurrection.
Office infection control charges.
Charges for copies of Your records, charts or x-rays or any costs associated with forwarding/mailing copies of Your records, charts or x-rays.
State or territorial taxes on dental services performed.
Those submitted by a dentist, which is for the same services performed on the same date for the same Member by another dentist.
Those provided free of charge by any governmental unit, except where this exclusion is prohibited by law.
Those for which the member would have no obligation to pay in the absence of this or any similar coverage.
Those which are for specialized procedures and techniques.
Those performed by a dentist who is compensated by a facility for similar covered services performed for Members.
Duplicate, provisional and temporary devices, appliances and services.
Plaque control programs, oral hygiene instruction and dietary instructions.
Services to alter vertical dimension and/or restore or maintain the occlusion. Such procedures include, but are not limited to, equilibration, periodontal splinting, full mouth rehabilitation and restoration for misalignment of teeth.
Gold foil restorations.
Treatment or services for Injuries resulting from the maintenance or use of a motor vehicle if such treatment or service is paid or payable under a plan or policy of motor vehicle insurance, including a certified self-insurance plan.
Treatment of services for injuries resulting from war or act of war, whether declared or undeclared, or from police or military service for any country or organization.
Hospital costs or any additional fees that the dentist or hospital charges for treatment at the hospital (inpatient or outpatient).
Charges by the Provider for completing dental forms.

Schedule of Benefits – Dental Phoenix Health Plans, Inc.
65441_PHP_SOBDental_2016 24
Adjustment of a denture or bridgework which is made within six (6) months after installation by the same dentist who installed it.
Use of material or home health aids to prevent decay, such as toothpaste, fluoride gels, dental floss and teeth whiteners.
Sealants for teeth other than permanent molars.
Precision attachments, personalization, precious metal bases and other specialized techniques.
Replacement of dentures that have been lost, stolen or misplaced.
Orthodontic services provided to a Dependent of an enrolled Member show has not met the 24 month waiting period requirement.
Orthodontic care for Dependent Children age 19 and over.
Repair of damaged orthodontic appliances.
Replacement of lost or missing appliances.
Fabrication of athletic mouth guard.
Internal bleaching.
Nitrous oxide.
Oral sedation.
Topical medicament center.
Orthodontic care not covered under this Scheduled of Benefits – Dental and the Policy.
Bone grafts when done in connection with extractions, apicoetomies or non-covered/non-eligible implants.
When two (2) or more services are submitted and the services are considered part of the same service to one another We will pay the most comprehensive service (the service that includes the other non-benefited service) as determined by Us.
When two (2) or more services are submitted on the same day and the services are considered mutually exclusive (when one service contradicts the need for the other service), We will pay for the service that represents the final treatment as determined by Us.
All out-of-network services except as provided under this “Schedule of Benefits – Dental” and the Policy.





























