Embed Size (px)
Citation preview


Saverio Cinieri
Disclosures
Direct and indirect with Oncology Companies:
Honoraria, Institutional grants/research support, Advisory Boards, Scientific
National and International Meeting Support.
Lilly, Pfizer, Roche, AstraZeneca, Amgen, Novartis, Pierre Fabre, Italfarmaco, Astellas, Takeda, Eisai, Bayer, Teva, Boehringer Ingelheim, Servier, Sanofi Genzyme, MSD, MerkSerono, Celgene, BMS, Ipsen, Puma, Incyte.


St. Gallen 2017

Equivocal results
Equivocal by IHC
score 2+ (FDA, ASCO/CAP 2007 & 2013)
Equivocal by ISH:
By single color ISH: mean GCN 4-<6
By dual color ISH:
ratio 1.8-2.2 (ASCO/CAP 2007)
ratio<2, GCN: 4-<6 (ASCO/CAP 2013)

Be prepared: New ASCO/CAP coming!
2017 FOCUSED UPDATE OF AMERICAN SOCIETY OF CLINICAL ONCOLOGY/COLLEGE OF AMERICAN PATHOLOGISTS BREAST CANCER CLINICAL PRACTICE GUIDELINE ON HER2 TESTING Authors: Antonio C. Wolff, Pamela B. Mangu, Brittany E. Harvey, Kimberly H. Allison, John M.S. Bartlett, Michael Bilous, Mitchell Dowsett, Ian O. Ellis, Patrick Fitzgibbons, Wedad Hanna, Robert B. Jenkins, Lisa M. McShane, Michael F. Press, Patricia A. Spears, Gail H. Vance, Giuseppe Viale, M. Elizabeth Hale Hammond
CLINICAL QUESTION 3: Should invasive cancers with a HER2/CEP17 ratio ≥2.0 but an average HER2 copy number <4.0 signals/cell be considered ISH Positive?
CLINICAL QUESTION 5: What is the appropriate diagnostic work-up for invasive cancers with an average HER2 copy number ≥4.0 but <6.0 signals/cell and a HER2/CEP17 ratio <2.0 and initially deemed to have an equivocal HER2 ISH test result?
Il sugo di tutta la storia… (Viale dixit o Manzoni dixit?)
Patients with equivocal HER2 status have not been enrolled in RCTs with anti-HER2 agents
There is no evidence of Trastuzumab benefit for these patients
The results of the NSABP B-47 are still awaited
ASCO/CAP will update the current guideline recommendations
Equivocal means Negative!

ISSUES WITH TREATMENT OF ERB2/+ ADVANCED
BREAST CANCER
High response rates and numerous treatments but the
majority of patients progress anddevelop resistance:
- can we improve therapy?
- can we understand the mechanisms of
resistance?
- can we personalized treatment to specific erb2/+
disease?
CNS disease
Long term survivors
Treat forever? Psychological issues of being
diagnosed with a fatal disease but experiencing
a long survival

Number of Lines and Median Duration of Chemotherapy by Subtype (n=199)

Multi-target Strategies in HER2 Therapy

Milestones in the Management of HER2-positive ABC

Trastuzumab and Pertuzumab Bind to Different Regions on HER2 and Have Synergistic Activity

Cleopatra Study Design

Cleopatra PFS<br />Investigator-Assessed

Cleopatra Final OS Analysis<br />Median follow-up 50 months (range 0–70 months)

CLEOPATRA: <br />Toxicity and PFS in Patients with Prior Trastuzumab <br />

Pertuzumab has become standard 1st line HER2+ metastatic treatment

Continued HER2 Blockade After Progression on Trastuzumab Improves Outcome

T-DM1 structure

EMILIA Study Design

EMILIA Progression-Free Survival by Independent Review

EMILIA : Overall Survival: Confirmatory Analysis

TH3RESA: A Phase III Trial of T-DM1 vs TPC

TH3RESA – Final OS

T-DM1 and Pertuzumab Mechanisms of Action

MARIANNE Study Design

MARIANNE: Final Analysis <br />of Overall Survival

MARIANNE: Summary of Findings From Primary Analysis

HER2–ER Cross-talk

Single Agent HER2 targeted therapy adds modestly to endocrine therapy
Presented By Karen Gelmon at 2017 ASCO Annual Meeting

ALTERNATIVE: Study Design –Gradishar Abstract 1004

ALTERNATIVE: Baseline Characteristics

ALTERNATIVE: Primary Endpoint<br />PFS with LAP+TRAS+AI versus TRAS+AI

ALTERNATIVE: Secondary Endpoint<br />PFS in all treatment arms

ALTERNATIVE: Secondary Endpoint<br />OS in all treatment arms








P+H+AI (n=54)
H+AI (n=56)
Events, n (%) 29 (53.7) 43 (76.8)
Median PFS, months 21.72 12.45
(95% CI) (12.42, 32.95) (6.21, 18.53)
∆, months 9.27
HR (95% CI) 0.55 (0.34, 0.88)
p-value 0.0111


Summary HT and HER2 directed therapy
Presented By Karen Gelmon at 2017 ASCO Annual Meeting

CNS Disease

Lapatinib + Capecitabine for HER2+ CNS Metastases

EMILIA<br />OS in Patients with CNS Mets at Baseline

Phase II trial of Neratinib and Capecitabine for Patients with Human Epidermal Growth Factor Receptor 2 (HER2+) Breast Cancer Brain Metastases : TBCRC 022 Study Cohorts
(Freedman et al, Abstract #1005)

Slide 42

Neratinib non CNS HER2+ ABC

Tucatinib Response in Patients With and Without Brain Metastases in the Triplet Cohort

Slide 46

Margetuximab-Fc-optimized anti-HER2 Monoclonal Ab
Slide 51

Immune System as a Target
Presented By Karen Gelmon at 2017 ASCO Annual Meeting

PANACEA trial: NCT02129556
Presented By Karen Gelmon at 2017 ASCO Annual Meeting

Impact of Long Term Survivorship
Presented By Karen Gelmon at 2017 ASCO Annual Meeting

Two (+) Clinical Scenarios in HER2+ ABC
Presented By Karen Gelmon at 2017 ASCO Annual Meeting
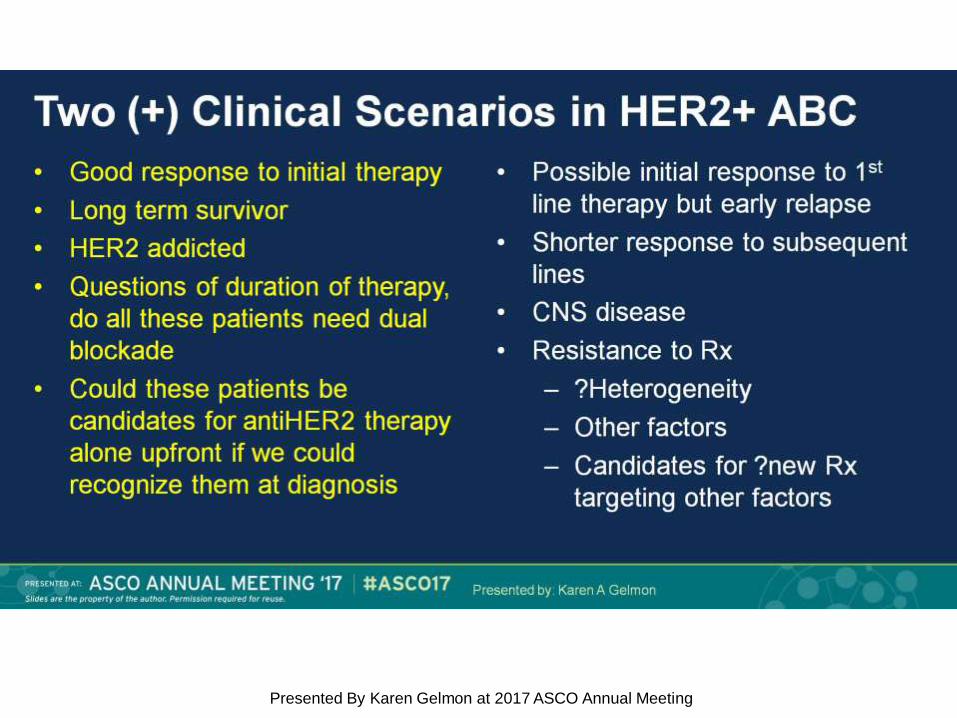
Two (+) Clinical Scenarios in HER2+ ABC
Presented By Karen Gelmon at 2017 ASCO Annual Meeting

Treatment Algorithm For Patients With HER2+ ABC

Considerazioni Personali
1. Dubitate quando vi trovate di fronte a dati discordanti
2. L’impatto clinico ed economico delle vostre scelte è
rilevante
3. I biosimilari risolveranno alcune problematiche alle
nostre aziende ma ne creeranno innumerevoli ai clinici:

I BIOSIMILARI RISOLVERANNO ALCUNE
PROBLEMATICHE ALLE NOSTRE AZIENDE
MA NE CREERANNO INNUMEREVOLI AI CLINICI:
1. Poca conoscenza su cosa succede in pazienti che
abbiano fatto terapia adiuvante o neoadiuvante con i
farmaci originator e diventino metastatici.
2. Assenza di informazioni sul doppio blocco (biosimilare
+ pertuzumab)
3. Assenza di informazioni sul passaggio da sc (
originator) a ev ( biosimilars).