Embed Size (px)
Citation preview

ANNA Advanced Practice Special Interest Group ProjectANNA Advanced Practice Special Interest Group ProjectANNA Advanced Practice Special Interest Group ProjectANNA Advanced Practice Special Interest Group Project
Description: This program focuses on the importance of vein preservation in chronic kidney disease (CKD) patients. At the heart of this project is a silicone wristband that reads “SAVE VEINS – NO IV/LAB DRAWS.” This webinar will provide nurses working with patients with CKD stages 3-5 the knowledge, tools, skills, and infrastructure to care for and educate patients about vein preservation and the importance of self-care access management. By encouraging patients to assume an active role in their own care related to vein preservation, we hope the goal of a 66% AV fistula rate set by the Center for Medicare & Medicaid Services (CMS) can be met.
Objectives: Upon completion of this presentation, the learner will be able to:
1. Identify CKD patients who need education related to vein preservation. 2. Analyze the tools and skills nephrology nurses must exhibit to adequately prepare
patients for preserving their veins for an AV fistula. 3. Design a plan to educate patients about the importance of being actively involved in
their care in anticipation of the eventual need for hemodialysis. 4. Summarize the importance of vein preservation for patients with CKD stages 3-5.

ANNA Advanced Practice Special Interest Group ProjectANNA Advanced Practice Special Interest Group ProjectANNA Advanced Practice Special Interest Group ProjectANNA Advanced Practice Special Interest Group Project
AAAAAAAABBBBBBBBOOOOOOOOUUUUUUUUTTTTTTTT TTTTTTTTHHHHHHHHEEEEEEEE PPPPPPPPRRRRRRRREEEEEEEESSSSSSSSEEEEEEEENNNNNNNNTTTTTTTTEEEEEEEERRRRRRRR……………………
Timothy Ray, DNP, CNP, CNN-NP, is a nephrology nurse practitioner and ANNA’s director for the Save the Vein project. He has been a nephrology nurse practitioner for 11 years, working in private practice with three nephrologists in the Cleveland, OH area. His clinical focus is ESRD, acute care, CKD, and general nephrology. Mr. Ray is also on clinical faculty at Case Western Reserve University, Kent State University, and Ursuline College. He is currently a member of ANNA’s Advanced Practice Special Interest Group, recently presented at ANNA’s Fall Meeting about CKD clinics, and has a special interest in CKD management and vein preservation.
Disclosures to Activity Participants
Requirements for Successful Completion: Attend 90% of the program, complete an evaluation and CNE certificate. Conflict of Interest Disclosure: No speaker has a financial relationship to declare relevant to the information provided in their presentation. No planning committee member, or ANNA staff have a financial relationship with any relevant commercial entity to declare. Commercial Support Disclosure: This activity is supported by a grant provided by AMAG. Non-Endorsement of Products: Accreditation of activities for contact hours does not imply approval or endorsement of any product, advertising, or education content by the American Nephrology Nurses’ Association or the American Nurses Credentialing Center’s Commission on Accreditation. Off-Label Discussion Disclosures: No speakers will discuss unlabeled uses of pharmaceutical or medical devices during their presentation.
11111111........2222222255555555 CCCCCCCCOOOOOOOONNNNNNNNTTTTTTTTAAAAAAAACCCCCCCCTTTTTTTT HHHHHHHHOOOOOOOOUUUUUUUURRRRRRRRSSSSSSSS
CONTINUING EDUCATION CREDIT - This educational activity has been provided by the American Nephrology Nurses' Association (ANNA). ANNA is a Provider approved by the California Board of Registered Nursing, provider number CEP 00910. ANNA is accredited as a provider of continuing nursing education (CNE) by the American Nurses Credentialing Center-Commission on Accreditation (ANCC-COA).
The ANCC-COA requires that all CNE and participant records be kept on file at the ANNA National Office for a period of five years. Licensees in the states of CA must retain this certificate for four years after the CE activity is completed. Other mandatory CNE states may have different record keeping requirements. Please be aware of your state's procedure.

Timothy Ray, DNP, CNP, CNN-NP
ANNA Project Director: Save the Vein
Save the Vein:What Nurses Need to Know
Objectives1. Identify CKD patients with a need for
education related to vein preservation.2. Analyze the tools and skills nephrology
nurses must exhibit in order to adequately prepare patients for preserving their veins for an AV fistula.
3. Design a plan to educate patients about the importance of being actively involved in their care in anticipation of the eventual need for hemodialysis.
4. Summarize the importance of vein preservation for patients with CKD stages 3-5.
Why Focus on Vein Preservation?
• There is still a high incidence of catheter use and vascular problems caused by peripheral IV’s, blood draws, and PICC lines in our CKD patients.
• Limited emphasis in presentations and research articles about vein preservation.
• We need to teach people to understand why we want them to preserve their veins.
• Long-term cost savings
Importance of Vein Preservation
• Vascular access is one of the most challenging areas of care confronting the nephrology team.
• A functional access is known as the “lifeline” of the hemodialysis patient.
• Protecting veins early on will lessen problems later when the patient needs an AVF placed.
What Do Nurses Need to Know about Vascular Access?
• Review vascular A&P and CKD staging
• Discuss hemodialysis access options and cost
• When to refer for access placement
• Benefits and barriers to vein preservation
• Options for blood draws and IV therapy lines
• Resources for nurses and patients
• Promoting vein preservation to others
• Use of the Save the Vein wristbands and brochure
Chronic Kidney DiseaseWhat is Chronic Kidney Disease (CKD)?
• Kidney damage for >3 months, as defined by structural or functional abnormalities of the kidney with or without decreased GFR.
• GFR <60 mL/min for >3 months, with or without kidney damage.
K/DOQI management guidelines
• Are based on recommendations from the National Kidney Foundation’s K/DOQI clinical practice guidelines, an evidence based approach to CKD care.

KDOQI
• Early identification of patients who have progressive kidney disease
• Protection of potential fistula construction sites
• Multidisciplinary supportwith use of a vascularaccess team approach
The 2006 vascular access
guidelines emphasize:
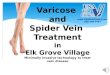
Progression and Prevalenceof CKD by Stage of Disease
GFR = glomerular filtration rate
300<15 (or dialysis)5 (kidney failure)
40015-294 (severe decrease in kidney function)
760030-593 (moderate decrease in kidney function)
530060-892 (kidney damage with mild decrease in kidney function)
5900≥901 (kidney damage with normal or increased kidney function)
Number of Patients
(thousands)2,3GFR Range
(mL/min/1.73 m2)CKD Stage1
1. National Kidney Foundation. K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease Am J Kidney Dis. 2003;42(suppl 3):S1-S201.
2. Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS. Prevalence of chronic kidney disease and decreased kidney function in the adult US population: Third National Health and Nutrition Examination Survey. Am J Kidney Dis. 2003;41:1-12.
3. U.S. Renal Data System, USRDS 1998 Annual Data Report. National Institutes of Health, Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 1998. Cited by: National Kidney Foundation. K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification—Quick Reference Clinical Handbook. New York, NY: National Kidney Foundation; 2002.
Projected Growth inCKD Stage 5 Prevalence
Gilbertson D et al. Presented at the 2003 ASN annual meeting.
Nu
mb
er o
f p
atie
nts
(m
illio
ns)
Year
2.2 million (60% diabetic)
2000 2010 2020 20301978
3.0
2.0
1.0
0
1.3 million
0.7 million
Causesof ESRD
in the USA:
Incident counts & adjusted rates,
by primary diagnosis
2009 USRDS
Vascular Anatomy& Physiology
Artery: � Carries blood away from the heart
� High pressure
Vein:� Carries blood towards the heart
� Low pressure, with valves
Arterio-Venous fistula� Surgical connection between an artery & vein
� Rush of blood flow from high to low pressure causes thrill/bruit
� Vein enlarges over time due to higher pressure creating enough space for large hemodialysis needles
Vascular Anatomy& Physiology
• Each time an IV is started or blood is taken there is a small amount of scar tissue created that over time can have a negative impact on a future AV fistula.
• Effect of aging on the vascular system:� Anatomic and hemodynamic changes
� Degeneration of collagen
� Loss of elastin
� Increased intima-media arterial wall thickness
� Reduced vascular compliance
• Vein mapping evaluates size of vessel and problem areas to avoid.

Vascular Access Atlas
www.fistulafirst.org- Listed under “What’s New”
HemodialysisAccess Options
• Arterio-venous fistula (AVF)� Surgical connection of an artery and vein� Nothing artificial� Needs 6-12+ weeks to “mature” before use� “Gold standard” for access
• Arterio-venous graft (AVG)� Artificial soft plastic tube (PTFE) connects an artery
to a vein� Can often be used within 2-4 weeks
• Tunneled cuffed catheter� Greater risk for infection, vein thrombosis� Can be used immediately after placement
Benefits of an AVF(vs. other)
• Less likely to develop clots
• Tend to last longer
• More cost effective
• Less infection
• Improved blood flow leading to better toxin clearance during dialysis
• Less hospitalizations
• Less potential inflammatory response
Barriers to Vein Preservation
• CKD not identified and/or eGFR not calculated by lab
• Late referral to nephrology• Prior vascular trauma• Upper extremity vascular contraindication,
e.g. mastectomy, previous access• Lack of education or understanding about
why vein preservation is important• Cultural issues
Percentage of Patients with an Arteriovenous Fistula
USRDS Data 2009
Per Person Per Year Access Event Costs
USRDS Data 2009

Access Cost Comparison
• U.S. 2008 ESRD population 547,982 with total cost of $39.5 billion/year.
• Cost for all CKD patients is 23% of total Medicare budget.
• Cost for vascular access: (per year)
� AVF: $3,480
� AVG: $8,683
� Catheter: $6,402
USRDS, 2010
Preparing the Patientfor Vascular Access
• Education about options and what to expect early on
• Evaluate to make sure patient is well prepared physically and psychologically for access surgery
• Forward planning ensures that sufficient time is available for the preservation of the access site, its creation and maturation
• Early referral to vascular surgeon for vein mapping and discussion of AVF placement
Vascular Surgery Intervention
• Referral when eGFR <30 with sufficient lead time for AVF maturation
• Vein mapping done early• Surgeon selection based on best outcomes
and willingness, and ability to provide access services
• Full range of appropriate surgical approaches
• AVF evaluation on patients with catheters/AVG’s
• Communication with nephrology/dialysis staff
Fistula First Change Package (2010)
Vascular Surgery ReferralVascular Surgery Referral Form
Date: __________________Surgeon: __________________________ Phone: ______________ Fax: ________________Patient: _________________________________________________ DOB: _______________Nephrologist: _______________________Phone: ______________ Fax: _______________PCP: ______________________________ Phone: _______________
This patient is being referred to you for access placement. The desired access is an AV Fistula. In the event you are not planning to place an AV Fistula in this patient, please call the nephrologist prior to placing any other access.
Patient’s non-dominant are is: ���� Right ���� LeftPatient has been saving the following arm: ���� Right ���� LeftComments (i.e: arm injury/mastectomy/pacemaker/previous access):Vein Mapping done pre-referral: ���� No ���� Yes – Date/Location: ______________________
Patient is currently on dialysis:Days: ____________________________________________________________________Location/Phone: ____________________________________________________________Patient is not on dialysis at this time:Anticipated hemodialysis start date: _______________________ monthsMost recent serum creatinine: ________ mg/dL & Creatinine Clearance/GFR: ________ ml/minPatient is on Anti-Coagulant Therapy: ���� No ���� Yes ___________________________________Allergies: ���� NKDA ���� Yes _______________________________________________________
The following patient information is also enclosed:���� Face Sheet ���� Vein Mapping Report���� H & P ���� Recent Lab work���� Medication List
Renal Physician’s Association (RPA)
Pre-Initiation Nephrologist Care
USRDS 2009
Vascular Access Use at Initiation
USRDS, 2010

Fistula First
• (2003) National Vascular Access Improvement Initiative (NVAII) developed by CMS, ESRD Networks, and providers
• (2005) Fistula First Breakthrough Initiative (FFBI)
• AVF’s Nationally
Aug ‘09: 53.5%
Aug ‘10: 56.5%
www.fistulafirst.org
Goal: 66%
Fistula First
Change Concept 10 promotes routine education for all renal caregivers specifically about vascular access and vein preservation.
FFBI Change Concepts: 13 clinical and organizational recommendations based on best practices for increasing AVF use/outcomes.
Vascular Access Initiative (VAI)
• Developed in 2010 by national nephrology/dialysis organizations, Fistula First, the ESRD Networks, and CMS/QIO’s.
• Collaborative goals:� Lower the rate of central venous catheter
(CVC) use� Ensure that all patients have a plan for a
permanent access within 90 days of initiating dialysis
� Achieve 66% AVF rate
Vascular Access Initiative (VAI)
Recommendations:
• Identify a vascular access coordinator
• ESRD patients shouldn’t be discharged from hospital without a AVF or plan for a AVF.
• Improved time-frame for outpatient access work: vein mapping, declots, placement of AVF’s
• Report eGFR with each serum creatinine order
• Hospital policy to minimize PICC lines with eGFR <45
• CKD patients to wear wristbands to protect veins
• Support CKD education and nephrology referral
• Follow the 30-20-10 rule
• Dialysis providers to continue active support even for ESRD patients
30-20-10 RuleWhen eGFR is:≤ 30, the patient should be evaluated by a
nephrologist.
≤ 20, the patient should be given information about renal replacement options and if the choice is hemodialysis then referral for AVF is made.
≤ 10, (or ≤≤≤≤ 15 in DM) the patient should have a mature access and be ready for initiation of chronic renal replacement.
Vascular Need Assessment
• Is there an oral therapy alternative?
• How long is venous access needed?
• How frequent are blood draws?
• Type of medication needed to be given
• Vascular history
• How difficult is peripheral venous access?
• Use of a Vascular AccessService Team (VAST)

Alternative IVAccess Options
• Use of dorsum of both hands
• Central venous catheter� Via internal jugular site
� Triple lumen catheter (short term)
� Tunneled cuffed catheter (long term) (Hohn, Pro-line, Groshong, Broviac)
� Avoid subclavian site due to high risk of stenosis
• PICC line may be appropriate for critically ill or terminal patients for whom hemodialysis is not an option.
• PICC Avoidance Tool Kit: The Renal Network 4, 9, 10 www.therenalnetwork.org/home/form1.php
Damage Causedby PICC Lines
• Endothelial denudation• Vein wall thickening• Increased number of smooth muscle
cells• Focal catheter attachments to the vein
wall with thrombus and collagen formation
• Higher risk of central venous stenosis, when compared to a tunneled cuffed central catheter.
Forauer & Theoharis, 2003. J Vasc Interv Radiol 14:1: 1163-1168.
Nursing Input• Comprehensive and multidisciplinary vascular
access plan should be implemented once patient is identified as having CKD.
• Education
� Patient, family, healthcare staff
• Minimize vascular damage
� No IV’s, BP’s, phlebotomy in protected arm once eGFR <60 or Scr >2.0
� Use dorsum of hands instead
� Any surgical procedures to avoid access arm damage
� Restrict PICC lines or subclavian catheter placement
Nursing Input• Identifying CKD patients early on
� Automatic calculation of eGFR with labs
� Use of EMR to identify and stage patients
• Vascular preservation tools
� Use of “Save the Vein” wristbands
� Post signs in prominent patient specific places
Arm veins suitable for placement of vascular access should be preserved regardless of arm dominance. - KDOQI
UNC Model for CKD• Need for a multidisciplinary approach to
effectively care for today’s CKD patient.
• Timely placement of vascular access is a consistent problem.
• Education of patients and other healthcare staff is essential.
• Collaborative communication between all points of care has lead to improvement in CKD outcomes.
Neyhart, C.D. et al. (2010). A New Nursing Model for the Care of Patients with ChronicKidney Disease: The UNC Kidney Center Nephrology Nursing Initiative. Nephrology Nursing Journal; March-April; Vol 37 (2), 121-130.
UNC Model for CKD
Reprinted from Nephrology Nursing Journal , 2010, Volume 37, Number 2, pp 121-130. Reprinted with
permission of the publisher, the American Nephrology Nurses' Association (ANNA), East Holly Avenue, Box 56, Pitman, NJ 08071-0056; 856-256-2320; FAX 856-589-7463; E-mail: [email protected] ; Web site: www.annanurse.org

Educating the Patient
Information to be presented:� CKD stages
� At what point would they get an AVF placed
� Options for when they need to have blood drawn or an IV
� Brief overview of vascular anatomy
� Benefits of vein preservation and AVF
� Use of the Save the Vein (STV) wristband
Encouraging Self Care• FFBI (Change Concept 13) promotes patient
self-management throughout CKD stages, including vascular access.
• Improvement in survival and quality of life for patients that actively participate� Take responsibility
� Active participation
� Dedicate the time and effort required
� Vigilantly follow the procedures and guidelines
� Work collaboratively with their healthcare team
Self care - practice of activities that an individual initiates and performs on their own behalf in maintaining life, health, and well being.
- Dorothea Orem’s Self-Care Theory
Getting the Word Out about Save the Vein
Educating and discussing with:� Nephrologists
� Nephrology nurses
� APN/PAs
� Primary care practitioners
� Vascular Surgeons
� Interventional radiologist/nephrologist
� Hospital staff: ER, phlebotomy, nurses, MD
� Community phlebotomy labs
ANNA Support• Vascular Access Position Statement:
� Vein preservation should be incorporated into patient teaching and care.
� Use dorsum of hands for all blood work/IV’s.
� Avoid use of subclavian catheters or PICC lines.
• Enthusiastic support from Board of Directors for the Save the Vein project.
• APN SIG group support and work on moving this project forward.
• ANNA website: www.annanurse.orgResources ����Fact sheets����Vascular access
Resources����Save the Vein
Save the VeinWristbands
• Many nephrology/vascular organizations emphasize use of a “medic alert bracelet”or wristband to identify CKD patient and need to preserve arm veins, including Fistula First (Change Concept 2) and VAI.
• Our Save the Vein (STV) wristbands were developed and successfully used in Tennessee by a CMS organization.
• STV wristbands are at the heart of our project; to be given out by nephrology nurses to CKD patients that have been educated about vein preservation.
Ordering WristbandsNote - wristbands are not produced by ANNA.
To order online:1. Go to: www.annanurse.org/savethevein
Click “wristband order form”
2. List in box #8: "Layout #3816”
3. Special instructions box:
State "Individually wrapped”
4. Leave all other boxes blank/unchanged
To order by phone:1. Call 1-800-778-1580
2. Provide Layout #3816

Save the VeinBrochure
• Patient handout• Explains use of wristband• Discusses benefits of vein
preservation• Provides resource info about
fistulas and vein preservation
PDF version available for download and printing by going to:
www.annanurse.org/savethevein
References
For the most current information and resources on vein preservation
management go to:
www.annanurse.org/savethevein
Take Home Message• Vein preservation should be followed not
only in CKD but continued in ESRD patients
• Review options to minimize vascular trauma
• Educate patients, family, healthcare staff about preventative measures
• Multi-disciplinary approach
• Early referral to vascular surgerywill give the patient the bestchance of starting dialysis with a functional AVF
• Use of STV wristbands early on will minimize vascular trauma

Vein PreservationVein PreservationVein PreservationVein Preservation On On On On----line Resourcesline Resourcesline Resourcesline Resources American Nephrology Nurses Association (ANNA). (2009). Position Statement: Vascular Access for
Hemodialysis. Retrieved from
http://www.annanurse.org/download/reference/health/position/vascAccess.pdf
Chan, K.E., Hakim, R.M., & Pulliam, J. (2010). The ’30-20-10’ Rule for Renal Care. Retrieved from
http://wwwrenalandurologynews.com/the-30-20-10-rule-for-renal-care/printarticle/162113/
Fistula First (2009). Fistula First Breakthrough Initiative Strategic Plan. Retrieved from
http://www.fistulafirst.org/
Geigle, R. (2009). Clinical Labs Report Additional Data to Aid in Detecting Kidney Disease.
Retrieved from http://www.medicalnewstoday.com/articles/163768.php
Hakim, R.M. & Himmelfarb, J. (2009). Hemodialysis access failure: a call to action – revisited.
Retrieved from http://www.nature.com/ki/journal/v76/n10/abs/ki2009318a.html
National Guideline Clearinghouse. (2008). Preservation of peripheral veins in patients with chronic
kidney disease. Retrieved from
http://www.guideline.gov/summary/summary.aspx?doc_id=12497&nbr=6428&ss=6&xl=999
National Kidney Foundation (NKF). (2006). 2006 Updates: Clinical Practice Guidelines and
Recommendations. Retrieved from
http://www.kidney.org/professionals/kdoqi/guideline_uphd_pd_va/index.htm
Renal Business. (2010). ESRD Population Reaches Record High. Retrieved from
http://www.renalbusiness.com/news/2010/09/esrd-population-reaches-record-high.aspx
The Renal Network, Inc. (2010). PICC Line Resource Toolkit. Retrieved from
http://www.therenalnetwork.org/home/form1.php
Vachharajani, T.J. (2010). Atlas of Dialysis Vascular Access. Retrieved from
http://www.fistulafirst.org/portals/0/atlas/index.html
Vachharajani, T.J. (2009). Medic Alert Bracelet to Preserve Veins for Future Dialysis Vascular Access.
Retreived from http://medscape.com/viewarticle/585510_print
Vachharajani, T. (2011). The Atlas of Dialysis Vascular Access. Retrieved from http://www.fistulafirst.org/

Vein Preservation ResourcesVein Preservation ResourcesVein Preservation ResourcesVein Preservation Resources
Allon, M. (2011). Fistula First: Recent Progress and Ongoing Challenges. American Journal of Kidney Disease, 57(1), 3-6.
Banerjee, S. (2009). Beyond Needle Placement: The Role of the Nephrology Nurse in Arteriovenous
Fistula Management. Nephrology Nursing Journal, 36(6), 657-659.
Ferring, M. et al. (2010). Routine Preoperative Vascular Ultrasound Improves Patency and Use of
Arteriovenous Fistulas for Hemodialysis: A Randomized Trial. Clinical Journal of American
Society of Nephrology, 5, 2236-2244.
Forauer, A.R. & Theoharis, C. (2003). Histologic changes in the human vein wall adjacent
to indwelling central venous catheters. Journal of Vascular Interventional Radiology,
14(9),1163-1168.
Futterman, L.G. & Lemberg, L. (2003). The Effects of Aging on Arteries. American Journal of
Critical Care, 12, 472-475.
Hoggard, J. et al. (2008). Guidelines for Venous Access in Patients with Chronic Kidney Disease.
Seminars in Dialysis, 21(2), 186-191.
Maya, I.D. & Allon, M. (2008). Core Curriculum in Nephrology: Vascular Access. American Journal
of Kidney Diseases, 51(4), 702-708.
McCann, M. et al. (2008). Vascular Access Management 1: An Overview. Journal of Renal Care,
34(2), 77-84.
Neyhart, C.D. et al. (2010). A New Nursing Model for the Care of Patients with Chronic Kidney
Disease: The UNC Kidney Center Nephrology Nursing Initiative. Nephrology Nursing
Journal, 37(2), 121-130.
Saad, T.F. & Vesely, T.M. (2004). Venous Access for Patients with Chronic Kidney Disease. Journal
of Vascular Interventional Radiology, 15, 1041-1045.
Trerotola et al. (2000). Tunneled Infusion Catheters: Increased Incidence of Symptomatic
Venous Thrombosis after Subclavian versus Internal Jugular Venous Access. Radiology, 217,
89-93.
Vachharajani, T.J. & Vachharajani, V. (2010). Obstacles for Clinical Monitoring in Hemodialysis
Patients Because of Multiple Vascular Accesses. Seminars in Dialysis, 23(1), 114-116.