-
8/7/2019 Sautter1991 Capgras syndrome
1/12
Neuropsychology Copyright 1991 by the Educational Publishing
Foundation1991, Vol. 5, No. 3, 139-150 0894-4105/91/S3.00
A Neuropsychological Profileof Capgras Syndrome
SCOTT W. SAUTTERDivision of Behavioral MedicineWestern State
HospitalStaunton, VirginiaDepartment of Behavioral Medicine and
PsychiatryUniversity of Virginia School of MedicineLEONARD
BRISCOEKAY FARKASDepartm ent of Behavioral M edicine and
PsychiatryUniversity of Virginia School of Medicine
Abstract: The neuropsychological profile of a' woman with the
delusion ofmisidentification characteristic of Capgras syndrome is
presented. Capgras syn-drome can develop from both psychodynam ic a
nd neuropathological etiologies.The available empirical data in the
literature support a hypothesis ofbifrontaland temporal cerebral
dysfunction and a need fo r careful differential diagnosisto rule
out prosopagnosia and confusional states. The results of this
specific casesuggest greater impairment in anterior
right-hemisphere-mediated functions.These findings are discussed in
the context of clinical neuropsycho logical assess-ment and
treatment issues, and additional questions regarding use of the
termsyndrome are raised.Keywords: Capgras syndrome, neuropathology,
psychodynamic therapy, neu-ropsychology.
The delusion of misidentification has fascinated clin icians
since its original descrip-tion in the psychiatric literature
almost seven decades ago (Capgras & Reboul-Lachaux, 1923).
Psychodynam ic interpretations of this phen om enon were
richlydescribed in colorful terms; however, recent advances in the
clinical behavioralneurosciences have helped to elucidate a
possible neuropathological etiology. Inthis article, we present a
neuropsychological profile of Capgras syndrome. Bothpsychodynamic
and neuropathological interpretations are described in the
litera-ture review, and the results of this particular case support
evidence of anteriorright-hemisphere-mediated dysfunction. Further
questions are raised about com-peting explanations and use of the
term syndrome.Most of the literature we reviewed provided case
presentations with psycho-dynamic interpretations invo lving "ego
splitting an d projection in defense of
Address correspondence to Scott W. Sautter, Behavioral and
Neuropsychiatric Center,1745 Camelot Drive, Suite 200, Virginia
Beach, Virginia 23454.139
-
8/7/2019 Sautter1991 Capgras syndrome
2/12
14 0 Scott W . Sauter el al.overwhelming erotic or aggressive
impulses directed at a parental figure or intensiveambivalent
feelings directed toward a significant other, such as a spouse or
sibling"(Sullivan, Cavenor, M altbie, & Silverstein, 1978, p.
275). The delusion arises in analtered effective state toward
others with intolerable ambivalent feelings that areneutralized
through imaginal existence of doubles (O'Reilly & Malhatra,
1987).Berson (1983) reviewed 133 cases in the English-language
literature and reportedthat the syndrome is most commonly seen in
paranoid schizophrenics; although18 of these cases had
neuropathological involvement, he suggested that brainpathology
could no t account for the selectivity of the delusion. Berson
(1983)offered criteria for inclusion that required psychosis,
paranoia, pathological splittingof a significant other, and changes
in the crucial interpersonal relationship. Thereis a great deal of
heterogeneity in the literature, im plyin g a need to ex am ine
bothpsychopathological and neuropathological evidence in a careful
differential diag-nosis (Bienenfield & Brott, 1989).Others have
described Capgras syndrome as a disorder that occurs in womenonly
(Vogel, 1974), that involves family systems dynamics (Moskowitz,
1975), orthat is associated with reduced platelet monoamine oxidase
activity (Sullivan etal., 1978), drug toxicity (Daniel, Swallows,
& Wolff, 1987), hypothyroidism (Fish-bain, 1989; Madakasira
& Hall, 1981), or head traum a (Weston & Whitlock, 1971).In
a group comparison study, Joseph, O'Leary, an d Wheeler (1990)
examined 12Capgras syndrome patients with matched controls and
assessed computed tomo-graphies (CTs) in a single blind paradigm;
the results showed that Capgras syndrom epatients had significantly
greater bilateral frontal and temporal atrophy. A briefreview of
the literature that has been published since Berson's article is
presentedin Table 1.For the purpose of this article, Capgras
syndrome is defined as occurring in apsychotic state with paranoid
features, manifested by a delusion of misidentificationof a
significant other, an d having greater anterior than posterior
neuropsychologicaldysfunction in the absence of gross
visuoperceptual distortions, such as prosopag-nosia or acute
confusiona l states. The present case met the above criteria (as
wellas Berson's 198 3) but raised additional com peting hypotheses
that w ere not easilyruled out.
Case HistoryMs. C. is a 45-year-old, right-handed, divorced
White woman with 11 years ofeducation and an episodic work history
of unskilled jobs. She had a number ofpsychiatric hospitalizations
dating back to 1979 for psychotic symptomatology,including paranoid
delusions, depression, and noncompliance with medicationregimens.
She had been diagnosed with schizophrenia and treated with Xanax
andMellaril. W hen admitted to our facility on an involuntary, men
tally ill status, sheexhibited marked paranoid delusions and
reported that she felt someone had takenthe place of her real
father and that this person was out to kill her. Three weeksprior
to this hospitalization, M s. C. had been discharged from a
psychiatric facilityin New Orleans with the diagnosis of
undifferentiated schizophrenia. After dis-charge, she traveled to
Florida to meet her father for a return trip to Virginia,during
which they decided to take a vacation at a state park. Upon
returning froman evening walk in the park, the patient reportedly
found a man in her roomclaiming to be her father. She stated that
this man was not her real father, but an
-
8/7/2019 Sautter1991 Capgras syndrome
3/12
Capgras Syndrome 14 1imposter, and became very angry and
agitated. The park rangers were called tosubdue her and take her to
a local emergency room, where she complained oftactile
hallucinations and thought broadcasting. She also reported that she
felt shemay have done something to her real father and that this
imposter wanted to killher. Although Ms. C. has no history of
neuropathology in her medical records, herlong history of alcohol
abuse and numerous motor vehicle accidents suggestedotherwise. In
one accident, she lost consciousness and was hospitalized for 5
days.The duration of unconsciousness and probable posttraumatic
amnesia was notreported. Although she had been charged with driving
while under the influenceearlier in that year, Ms. C. denied using
alcohol or other drugs since that charge.At admission, Ms. C.'s
speech was quiet with decreased intonation and rate.Her thought
processes showed looseness of associations and tangentia lity.
Shedenied any suicidal or homicidal ideation. Her judgm ent w as
poor, and insight wasabsent. She was well dressed, groomed, and
appeared slightly younger than herchronological age of 45 years. At
admission, she scored 20/30 on the Mini-MentalState Examination
(MMSE; Folstein, Folstein, & McHugh, 1975), the next day,she
scored 27/30. She remained reserved and suspicious and was quite
guardedwhen talking about her "father." She complained of decreased
sleep and increasedfeelings of guilt but not of anhedonia, change
in energy, or decreased appetite. Ms.C. was given the diagnosis of
paranoid schizophrenia, chronic, with acute exacer-bation, and was
placed on a regimen of 100 mg of Thorazine twice a day
forattenuation of psychotic symptoms. After a brief hospital stay
of 3 weeks and acourse of neuroleptics, her psychotic symptoms
dissipated, and she was dischargedto her local community.
Neuropsychological ProfileMs. C. was referred for
neuropsychological evaluation for the purpose of providinga
differential diagnosis and documenting suspected brain-behavior
dysfunctionresulting from multiple motor vehicle accidents an d
alcohol abuse. During theevaluation, Ms. C. was initially
suspicious about being tested. However, after thetype of procedures
that would be given were explained to her, she relaxed. As aresult,
she was pleasant and cooperative but remained guarded. She denied
auditoryhallucinations but frequently smiled and laughed out loud
at inappropriate times.Ms. C. did not report that her father was an
imposter during the testing, althoughshe appeared perplexed when
confronted about this. An electroencephalographwas within normal
limits, and no further neuroradiological studies were
pursued.Neuropsychological impressions were consistent with greater
anterior right-hemisphere-mediated dysfunction of mild to moderate
cognitive impairment,particularly for tasksof memory and abstract
reasoning. Right- and left-hemisphere-mediated functions with
respect to normative data are presented as z scores inFigure 1 . A
breakdown of various neuropsychological functions (also z scores)
arepresented in Figure 2. Relatively greater impairmen t can be
seen in right-hemi-sphere-mediated functions (Figure 1 ) , as well
as more anterior functions (Figure2). Standard scores were computed
by subtracting the mean of each test from theraw score and dividing
the result by the test's standard deviation as found in
thenormative literature (Benton & Hamsher, 1976; Bornstein,
1984; Delis, Kramer,Kaplan, & Ober, 1987; Fromm-Auch &
Yeudall, 1983; Golden, 1978; Halstead &text continues on p.
148
-
8/7/2019 Sautter1991 Capgras syndrome
4/12
14 2 Scott W. Sauter el al .
r-o\< uocc w>.00O"o43I3t>OSc^Q JC O
ciscussio
Q
Method
c
Authors
< 2 < yTJ 3H "3c,'Mca oc "3|2 &itS 5J3 < u_, cc ^
*gt.i ISC J5 5W *" Mu
O" o ow.SPJ < - j h -vJ
Neuropathological:
neuropsychologic
visualfieldneglec
L ^sf-0\^
iWhitloc
ocoof)U
s> !C /D Ott-gS S?s1> !? gC i_'i152T3O Dc W Ca < n
-
8/7/2019 Sautter1991 Capgras syndrome
5/12
Capgras Syndrome 1 4 3
apgrassyndromewasresolved
withthyroidreplacement
O
europathological:rightcer-
ebraldysfunction;MMSE
andEEGwithhypothy-
roidism
Z
2 oo
jggestsbilateralimpairment,with
moreimpairmentinnondomi-
VIcSO
nanthemispherethanindomi-
a< ufu*-c
EGshowedslowwaveactivity;
tu
europathological:EEGwith
Z
3 3o
neurolepticsmaymaskinterme-
tamorphosissyndrome
historyofseizureandol-
factoryhallucinations
ilateralfrontalandtemporaldys-
function;focalhypothesisgiven
P Q
europathological:EEG,CT
abnormal,PETnormal
Z
38
eedbothanorganicandpsycho-
pathologicalconditionpriorto
diagnosingCapgrassyndrome
gnificantlymoreindexthancon-
Z
europathologicalandpsy-
chodynamic:CVA,EEGs,
Z
j >o
C /D
neuropsychologytests
europathological:13Fre-
ZcoCA ceooaot-cO
trolpatientshadfrontalandtem-
poralinvolvement;suggestsbilat-
golisyndromecases
matchedwithpsychiatric
eralanteriorcorticaldysfunction
c
( j
11O in
reaterright-hemisphereinvolve-
mentthanleft
O
europathological:assessed
asinitialdementia
Z
&53
1K
I
ooOs
13X "C'SX8
00O\
o fP^/l QQOOoo
' s
oooo
t
-
8/7/2019 Sautter1991 Capgras syndrome
6/12
14 4 Scott W . Sauter et al.
ia5K8 *!*
2H
Discussion
8x:4-*Os
^~
C/1s3* *
eedcarefuldifferentialdiagnosi:
ZT31J32'S a
SH
]gI|(L)Z1 >O
x-sOV 53!sSE
o
ofdelusionalmisidentification
i&o.o< L )1C fl
(j11 i
prosopagnosia
00V-J
so"o0
i
iggestsoccipital-temporalabno
o n
> ,< f taoi*c3'_ Wao< uZ
uo
_ ,oON
"o(S%03
t/3
13J.1ooo+-v >JS1 5 5> -, * - 'as
1o"oo
modelsofmisidentification
i 8S< L>O11-
iV),Q,rtU
aO1123uZcg caE0oQO
^j U js~jf"2,
i
generativeprocessaffectingant
-
8/7/2019 Sautter1991 Capgras syndrome
7/12
Capgras Syndrome 145
S3bO D S-Z
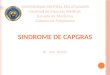
Figure 1. Ms. C's left-hemisphere- versus
right-hemisphere-mediated cognitive functioning,presented as z
scores (WAIS-R = Wechsler Adult Intelligence Scale-Revised; VIQ =
verbalIQ; PIQ = performance IQ; WMS = Wechsler Memory Scale; Hooper
= Hooper VisualOrganization Test).
-
8/7/2019 Sautter1991 Capgras syndrome
8/12
146 Scott W . Sauter et al.
S3HOOS-Z
Figure 2. Ms. C's individual test results, presented as z
scores, grouped by neuropsycholog-ical function (DH = dominant
hand; NDH = nondominant hand; REC = recognition;Hooper = Hooper
Visual Organization Test; WAIS-R = Wechsler Adult Intelligence
Scale-Revised; PIQ = performance IQ; VIQ = verbal IQ; CVLT =
California Verbal LearningTest; WMS = Wechsler Memory Scale; W =
word; C = color, C-W = color and word;WCST = Wisconsin Card Sort
Test; RESP = response).
-
8/7/2019 Sautter1991 Capgras syndrome
9/12
Capgras Syndrome 14 7
a s sS3HODS-1
Figure 3. Ms. C's Minnesota Multiphasic Inventory (MMPI) profile
(L = Lie scale; F =Frequency scale; K = Correction scale; 1 =
Hypochondriasis scale; 2 = Depression scale;3 = Hysteria scale; 4 =
Psychopathic Deviate scale; 5 = Masculinity-Femininity scale;6 =
Paranoia scale; 7 = Psychasthenia scale; 8 = Schizophrenia scale; 9
= Hypomania scale;0 = Social Introversion scale).
-
8/7/2019 Sautter1991 Capgras syndrome
10/12
14 8 Scott W . Sauter et al.Wepman, 1978; Heaton, 1981; Hooper,
1985; Loring, M artin, M eador, & Lee,1990; Wechsler, 1945,
1981; Yeudall, 1987).Ms. C's language skills were seen as a
relative strength, as were her attempts toincrease interpersonal
contact. Interestingly, the personality assessment depicted
aprofile uncharacteristic of paranoid schizophrenia; Ms. C.'s
profile may best bedescribed as a resolving episodic psychotic
depression (see Minnesota MultiphasicInventory profile in Figure
3). Ms. C.'s apparent need for nurturance and attemptsto increase
interpersonal contact were viewed as a positive prognostic sign
forfurther gains in adaptive competency, as long as she complies
with outpatientfollow-up (e.g., to the ex tent tha t she takes
medication as prescribed, abstains fromalcohol, and receives
supportive therapy). As her psychiatric symptomatologyclears, a
return to work will become important for continued recovery.
DiscussionThe results of this case presentation of Capgras
syndrome support the literature indescribing the neuropathological
aspects of this syndrome, as well as Berson's(1983) criteria for
Capgras syndrome. The use of the term syndrome may bemisleading
because of the heterogeneity of possible etiologies. Symptoms of
delu-sional misidentification may be a more accurate description
because it can occurin varied presentations. Some clinicians have
suggested that the use of multipleand colorful descriptions of
delusions of misidentification may not be as helpful asa thorough
and careful differential diagnosis based on neuropsychological
andpersonality testing, as well as neuroradiological evidence. Ms.
C. was psychoticwith paranoid features, had a delusion of
misidentification of a significant other,and had neuropsychological
impairment in the absence of prosopagnosia or anacute confusional
state.Treatm ent typically follows a therapeutic regimen of
antipsychotic medicationand supportive therapy in which areas of
cognitive-behavioral strength are used toovercome weak er areas of
functioning. Ms. C.'s case was useful for documentingthe many
competing explanations that clinicians are forced to rule out in
ahypothesis-testing model when m aking a differential diagnosis;
her history includedalcohol abuse and withdrawal, along with
neuropathological invo lvem ent, such ashead trauma, paranoid
delusions, and psychodynamic issues. With regard toassessment,
differential diagnosis, and subsequent treatment, the context of
thereferral and its specific question should dictate wh ether
neuroradiological, neuro-psychological, and psychodynamic
perspectives ought to be considered. It may bemore appropriate to
use the term symptoms of, rather than syndrome, whendescribing
delusions of misiden tification because of the heterogeneity of
etiologiesand varied clinical presentations.
ReferencesBenton, A., & Hamsher, K . deS. (1976).
Multilingual Aphasia Examination. Iowa C ity:
University of Iowa.Berson, R. (1983). Capgras syndrome. American
Journal of Psychiatry, 140, 969-978.Bick, P. (1984). The syndrome
of intermetamorphosis. A merican Journal of Psychiatry,
141,588-589.Bienenfield, D., & Brott, T. (1989). Drs.
Bienenfield and Brott reply. Journal of Clinical
-
8/7/2019 Sautter1991 Capgras syndrome
11/12
Capgras Syndrome 14 9Psychiatry, 5 0, 475.Bornstein, R. A.
(1984, August).Normative data on intermanual differences in
neuropsycho-logical performance. Paper presented at the 92nd Annual
Convention of the AmericanPsychological Association, Toronto,
Ontario, Canada.
Capgras, J., & Reboul-Lachaux, J. (1923). L'illusion des
sosies, dans un delire systematisechronique [Delusion of a double,
in systematic chronic delirium]. Bulletin de la SocieteClinique de
Medecine Mentale, 11,6-16.Christodoulou, G. N. (1977). The syndrome
of Capgras. British Journal of Psychiatry, 130,556-564.Daniel, D .
G., Swallows,A., & Wolff, F. (1987). Capgras delusion and
seizures in associationwith therapeutic dosages of D isulfiram.
Southern Medical Journal, 80, 1577-1579.Delis, D., Kramer, J.,
Kaplan, E., & Ober, B. (1987). California Verbal Learning
Test:Manual, adult version, research edition. Sa n Antonio, TX:
Psychological Corp.de Pauw, K., Szulecka, K., & Poltock, T.
(1987). Single case study: Fregoli syndrome aftercerebral
infarction. The Journal of Nervous and Mental Disease, 175,
433-438.Fishbain, D. A. (1989). Capgras syndrome and minor head
injury. Journal of ClinicalPsychiatry, 5 0, 474-475.Folstein, M.
F., Folstein, S. E. , & McHugh, P. R. (1975). Mini-Mental
State. Journal ofPsychiatric Research, 12, 189-198.Fromm-Auch, D.,
& Yeudall, L. (1983). Normative data for the Halstead-Reitan
neuropsy-chological tests. Journal of Clinical Neuropsychology, 5 ,
220-238.Golden, C. (1978). Stroop Color and Word Test: A manual fo
r clinical and experimentaluses. Chicago: Stocking.Halstead, W.,
& Wepman, J. (1978). The Halstead-Wepman Aphasia Screening
Test.Journal of Speech an d Hearing Disorders, 8, 135-141.Hayman,
M., & Abrams, R. (1977). Capgras syndrome and cerebral
dysfunction. British
Journal of Psychiatry, 130, 68-71.Heaton, R. (1981).
WisconsinCard Sorting Test manual. Odessa, FL: Psychological
Assess-ment Resources, Inc.Hooper, H. (1985). The Hooper Visual
Organization Test manual. Los Angeles: WesternPsychological
Services.Joseph, A. (1986). Cotard's syndrome in a patient with
coexistent Capgras' syndrome,syndrome of subjective doubles, and
palinopsia.Journal of Clinical Psychiatry, 47 , 605-606.Joseph, A.,
& O'Leary, D. (1987). Anterior cortical atrophy in Fregoli
syndrome. Journal ofClinical Psychiatry, 48 , 409-411.Joseph, A.
E., O'Leary, D. H., & Wheeler, H. G. (1990). Bilateral atrophy
of the frontal an dtemporal lobes in schizophrenic patients with
Capgras syndrome: A case-control studyusing computed tomography.
Journal of Clinical Psychiatry, 5 1, 322-325.Kiriakos, R., &
Ananth, J. (1980). Review of 13 cases of Capgras syndrome.
AmericanJournal of Psychiatry, 137, 1605-1606.Lipkin, B. (1988).
Capgras syndrome heralding the development of dementia. British
Journalof Psychiatry, 153, 117-118.Loring, D.', Martin, R., Meador,
K., & Lee, G. (1990). Psychometric construction of
theRey-Osterrieth complex figure. Methodological considerations and
interrater reliability.Archives of Clinical Neuropsychology, 5 ,
1-14.Madakasira, S., & Hall, T. B. (1981). Capgras syndrome in
a patient with myxedema.American Journal of Psychiatry, 138,
1506-1507.
Moskowitz, J. A. (1975). Capgras syndrome in male siblings
[letter to the editor]. AmericanJournal of Psychiatry, 131,
1.O'Reilly, R., & Malhatra, L. (1987). Capgras syndrome An
unusual case and discussion ofpsychodynamic factors. British
Journal of Psychiatry, 151, 262-265.Shaw, V. R., & Pool, K. D.
(1990, February). Orga nic factors in Capgras syndrome. Paper
-
8/7/2019 Sautter1991 Capgras syndrome
12/12
750 Scott W . Sauteretal.presented at the Annual Meeting of the
International Neuropsychological Society,Orlando, FL.Sullivan, J.
L., Cavenor, J. O., Maltbie, A. A., & Silverstein, E. (1978).
Capgras syndromeA biochemical marker? The Journal of Nervous an d
Mental Disease, 166 , 275-279.
Todd, J., Dewhurst, K., & Wallis, G. (1981). The syndrome of
Capgras. British Journ al ofPsychiatry, 139, 319-327.Vogel, B. F.
(1974). The Capgras syndrome and its psychopathology. Ame rican
Journa l ofPsychiatry, 131, 922-924.Wechsler, D. (1945). A
standardized memory scale for clinical use. Journal of
Psychology,19, 87-95.Wechsler, D. (1981). WAIS-R manual. New York:
Psychological Corp.Weston, M. J., & Whitlock, F. A. (1971). The
Capgras syndrom e following head injury.British Journal of
Psychiatry, 119, 25-31.Wilcox, J., & Waziri, R. (1983). The
Capgras syndrome and nond om inant cerebral dysfunc-tion. Journal
of Clinical Psychiatry, 44, 70-72.Yeudall, L. (1987). Normative
data for the Halstead-Reitan Neuropsychological Testsstratified by
age and sex. Journal of Clinical Psychology, 43, 346-366.