Embed Size (px)
Citation preview
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Barb Bowsher MDLTC/MC/USA
Adolescent MedicineBAMC
Barb Bowsher, MD has no relevant financial relationships with commercial interests to disclose.
Objectives Knee Anatomy
Physical Exam of the knee
Radiologic studies
Identifying different conditions
Overuse injuries
Acute injury
Chronic knee pain
Management

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Anatomy of the knee
Anatomy of the knee

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
HistoryAcute Chronic
When did it occur
How did it happen
Able to walk after
Swelling, how quickly
Bruising
? Hear or feel a pop
Catching, locking, giving away, instability
How long has it hurt
Aggravating activities
Prolonged sitting
Stairs
Swelling
Catching, locking, giving away
Pain at rest
History Red flag symptoms – fevers, pain keeping up at night,
weight loss
What helps the pain (ice, heat, rest, NSAIDS)
Any other joint painful
Prior injuries or Physical therapy

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Physical exam Examine both sides for comparison
Exam joint above and joint below (hip pain can go to the knee – SCFE)
History can help with exam if they can show you where the pain is located
Use a systematic approach each time
Physical exam - Palpation
Effusion/swelling
Joint line tenderness
ROM
Tibial tuberosity
Retropatellar palpation
Crepitus
Patellofemoral grind test

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Physical exam – Meniscus test McMurrays
Apley’s test
Squatting causing deep posterior knee pain
Maximal flexion of knee – causing posterior knee pain often indicative of posterior horn tear
Physical exam – MCL/LCL 0 degrees 30 degrees
Physical exam – Patellar apprehension test

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Physical exam – Anterior Drawer
Physical exam – hamstring/quads
Physical exam – Posterior drawer

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Physical exam - Lachmans
Physical exam - Lachmans
Physical exam Assess gait
Limb length discrepancy
Valgus/varus deformity
Pes planus (flat foot) or cavus foot (rigid high arch)
Check ROM spine, hips, ankles
Graph

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Imaging studies
When to order?
What to order?
When do I need an MRI?
Normal Xray
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
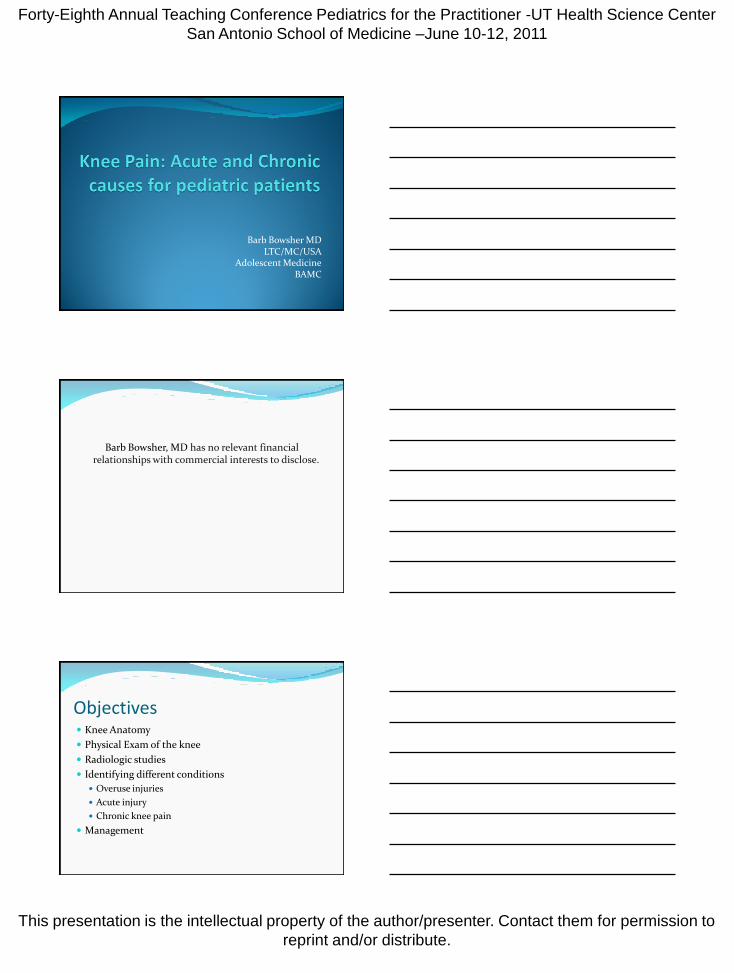
AP and Lateral view
Tunnel view
MRI - Meniscus

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Acute ACL injuries
Increasing frequency
Girls basketball and soccer
MOA injury similar in skeletally immature and adults
Noncontact stress with rapid directional change
Landing on rapidly flexed knee while jumping
1/3 hear a pop
Effusion is rapid
Unable to return to play
Refer to Ortho
MRI - ACL

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Acute – Meniscal tears Share weightbearing load, aid in synovial distribution,
and contributes to knee stability
Uncommon in < 10 yo if has normal meniscus
Usually see a longitudinal peripheral tear
Can be difficult to elicit MOA
Knee pain, joint line pain, effusion
Nonacute cases 0f locking, catching sensation
Xray – usually normal (except if have discoid menisci)
Refer to Ortho
Acute – MCL/LCL injuries Result from valgus or varus injuries
Can also result in medial menisal injuries and the “terrible triad” (MCL, ACL, medial menisuc)
Knee pain and medial swelling, minimal effusion
Exam –
MCL pain with ROM, valgus stress causes pain and or laxity
LCL – varus stress pain/laxity, pain over LCL, rarely exist alone (more effusion)
Acute – MCL/LCL injuries Graded
I - tenderness w/o laxity
II – tenderness with laxity and firm endpoint
III – laxity w/o endpoint (suggest complete tear)
Check meniscus and ACL
Xray – in skeletally immature may see epiphysealfracture
Usually do not need MRI to help diagnosis

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Overuse injuries – IT band Syndrome Lateral knee pain in runners or cyclist (swimmers)
Repetitive knee flexion– excessive friction at site where IT band crosses lateral femoral epicondyle
Lateral knee pain
Progressively worsens
Increased when running downhill, stairs
Exam – pain over ITB area, crepitus, + Ober’s test
No films needed usually
Overuse – IT Band Syndrome
Overuse – IT Band Syndrome Ober’s Test

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Overuse injuries – Osgood Schlatters Apophysitis Affects b/w 10-15 yo
M>F
Worse during rapid growth
½ Bilateral in boys
Pain with running and jumping
Acute pain with trauma consider fracture
Xrays generally not needed
Overuse – Osgood Schlatter
Overuse – Synding-Larsen-Johansson disease
Apophyisitis of inferior pole of patella
Ossicle formation and fragmentation
Assoc with growth velocity and loss of flexibility
M>F
Pain at inferior pole
Pain with knee flexed to 90 degrees

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Chronic pain/Overuse - PFS Pain underneath the knee cap
Increased pain with activity, walking up/down stairs, or after prolonged sitting
Generalized anterior knee pain
Subjective feeling of swelling
Knee gives away
Often history of recent change in activity
F>M
Mechanical features can place at increased risk for this Examine feet and hips in addition to knees
Chronic – Ostesochondritisdissecans Juvenile and adult types
30-40% youth with bilateral involvement
Lateral aspect of medial femoral condyle (80-85%)
Etiology unkown
Most with high activity level
Important to diagnose –high incidence of osteoarthritis if missed
Chronic - OCD Preceding hx of trauma in 40-60%
Knee pain worse with activity and improves at rest
Early can have vague knee pain symptoms +/- swelling
Grinding, locking, catching seen with late stages (loose detached FB)
Exam – tenderness of condyle with knee flexed, decreased ROM, effusion, +/- gait change
Wilson test
Need High index of suspicion

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Chronic – OCD plain films
Chronic – OCD plain films
Chronic OCD - MRI
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Referral
Features or exam c/w structural knee pain
Persistent or recurrent knee swelling
Locking, instability, or restricted joint motion
No improvement in 4 to 6 weeks of rehab
Treatment of acute Rest, ice, NSAID until pain free – may need to place on
crutches
Stretching and flexibility – quads, hamstrings, and calves
Strengthening – esp quadriceps
Consider sending to physical therapy
Bracing
Assess foot wear (pronation issues)

Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center
San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to
reprint and/or distribute.
Return to play Pain at rest can begin gradual return to play
Pain is not present net morning after activity
No limping with running or jumping (testing in office as guide to begin gradual return)
No ice or NSAID needed prior to activity
Comfortable in squatting stance (shows full ROM)