Embed Size (px)
Citation preview

SAMPLE FORMS – EQUINE
The attached documents are intended as samples which provide an equine veterinarian with forms that he/she may choose to consider or adapt as part of their practice. In addition to forms that apply to equine practice, documents with forms specific to companion animals, food producing animals and poultry are available as well as forms that may be used by all practices.
Sample Form Page
Equine Client Information Sheet 2
Equine Continuing Care Summary Sheet 3
Equine Medical Record 4-5
Equine Stable Visit Form 6
Herd Health Reproduction Record (Equine) 7
Herd Health Vaccination Record (Equine) 8
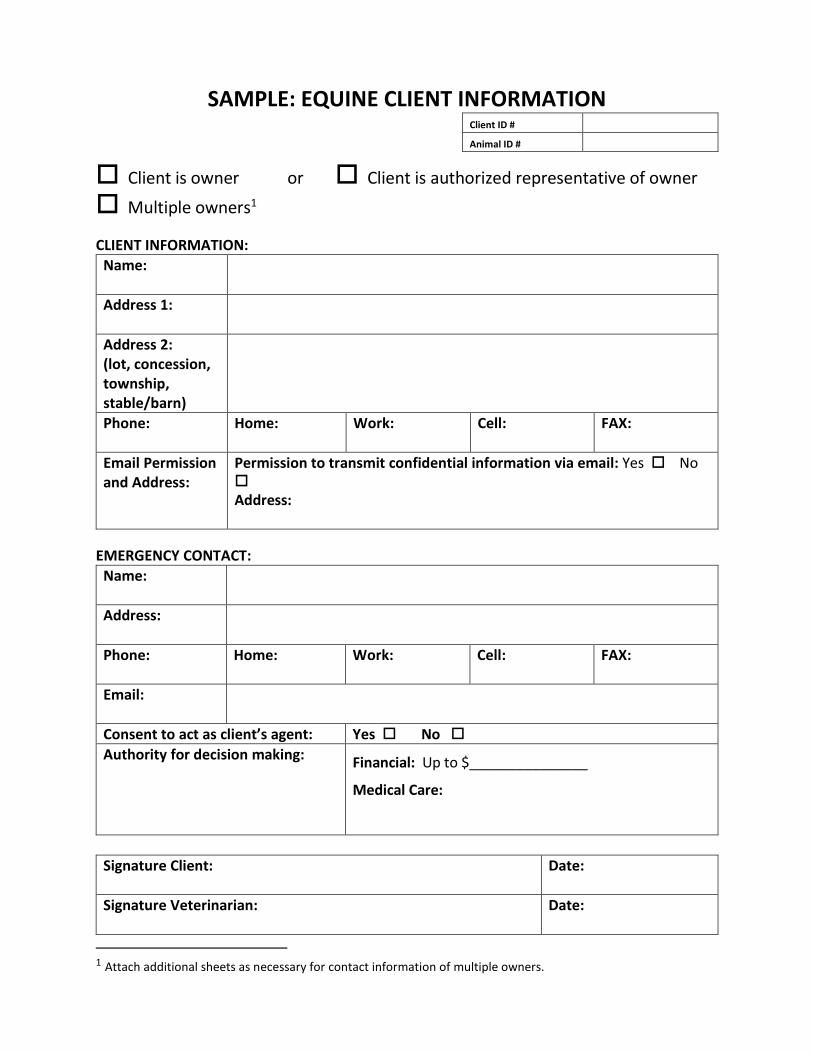
SAMPLE: EQUINE CLIENT INFORMATION Client ID #
Animal ID #
Client is owner or Client is authorized representative of owner
Multiple owners1
CLIENT INFORMATION:
Name:
Address 1:
Address 2: (lot, concession, township, stable/barn)
Phone: Home: Work: Cell: FAX:
Email Permission and Address:
Permission to transmit confidential information via email: Yes No
Address:
EMERGENCY CONTACT:
Name:
Address:
Phone: Home: Work: Cell: FAX:
Email:
Consent to act as client’s agent: Yes No
Authority for decision making: Financial: Up to $_______________
Medical Care:
Signature Client: Date:
Signature Veterinarian: Date:
1 Attach additional sheets as necessary for contact information of multiple owners.

SAMPLE: EQUINE CONTINUING CARE SUMMARY SHEET
Client ID: Animal ID:
Diagnosis:
Treatment / Tests:
Medications:
Exercise:
Withdrawal Times:
Dietary Directions:
Recheck Date:
Additional Instructions:
Veterinarian Signature: Date:
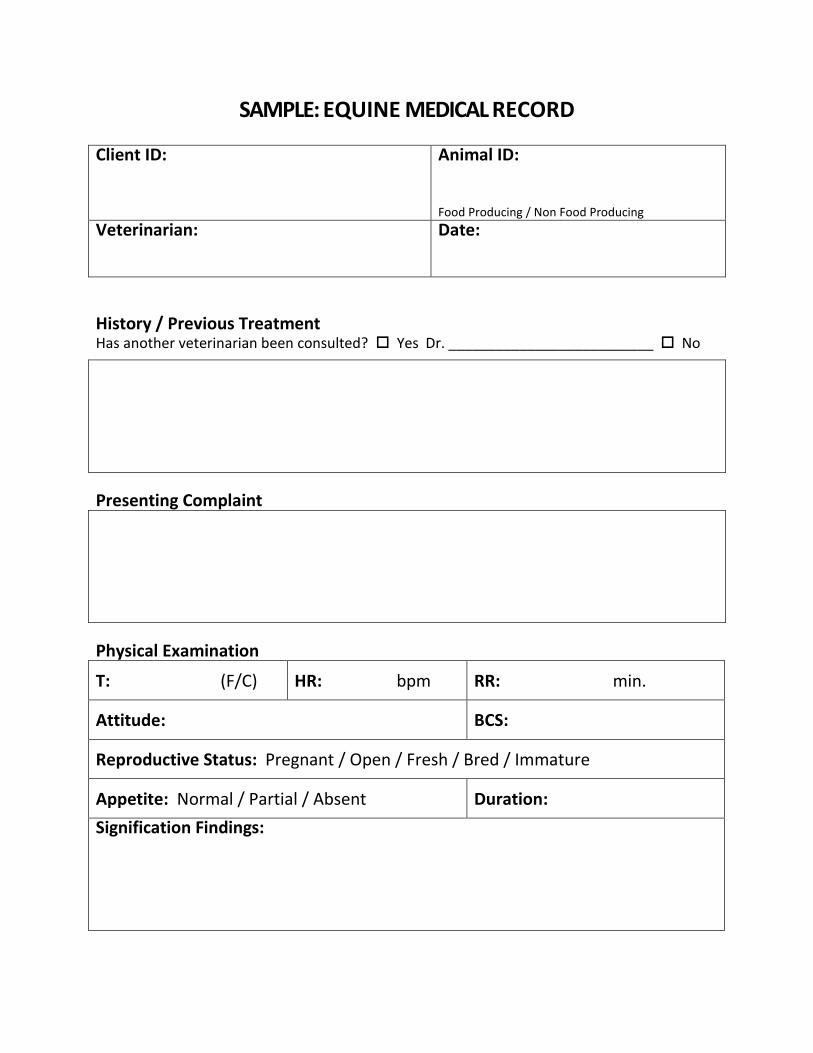
SAMPLE: EQUINE MEDICAL RECORD
Client ID: Animal ID:
Food Producing / Non Food Producing
Veterinarian: Date:
History / Previous Treatment Has another veterinarian been consulted? Yes Dr. __________________________ No
Presenting Complaint
Physical Examination
T: (F/C) HR: bpm RR: min.
Attitude: BCS:
Reproductive Status: Pregnant / Open / Fresh / Bred / Immature
Appetite: Normal / Partial / Absent Duration:
Signification Findings:
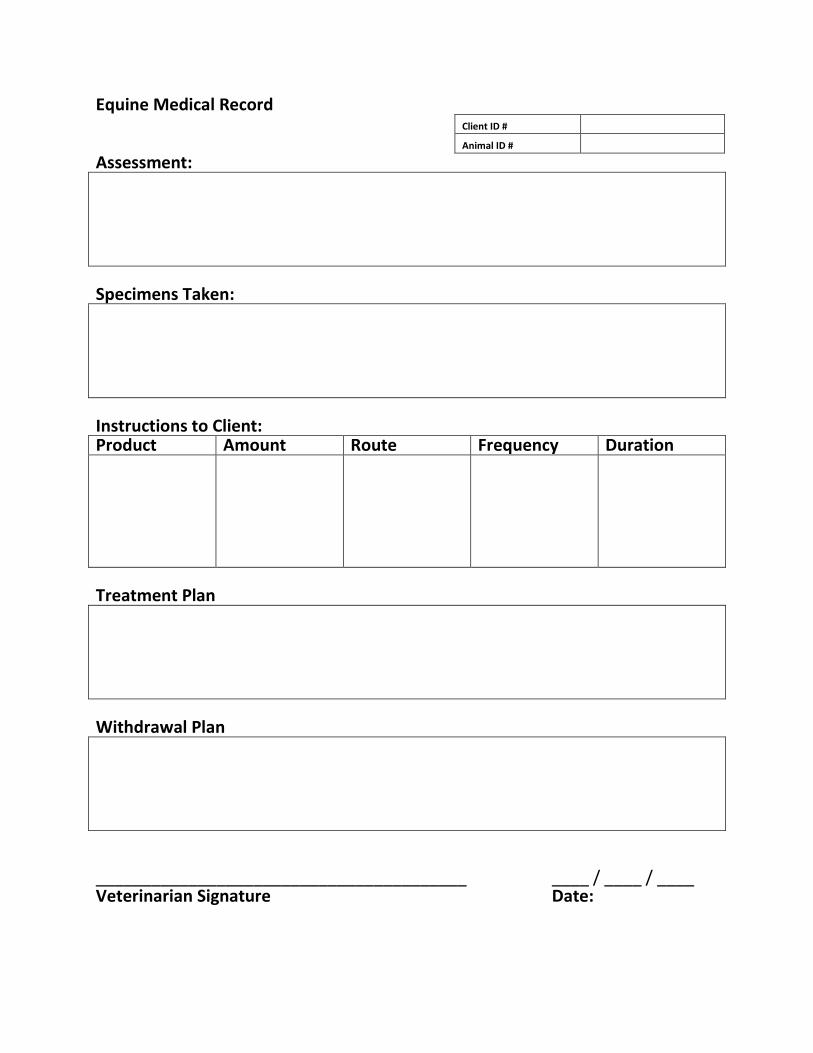
Equine Medical Record Client ID #
Animal ID #
Assessment:
Specimens Taken:
Instructions to Client: Product Amount Route Frequency Duration
Treatment Plan
Withdrawal Plan
________________________________________ Veterinarian Signature
____ / ____ / ____ Date:
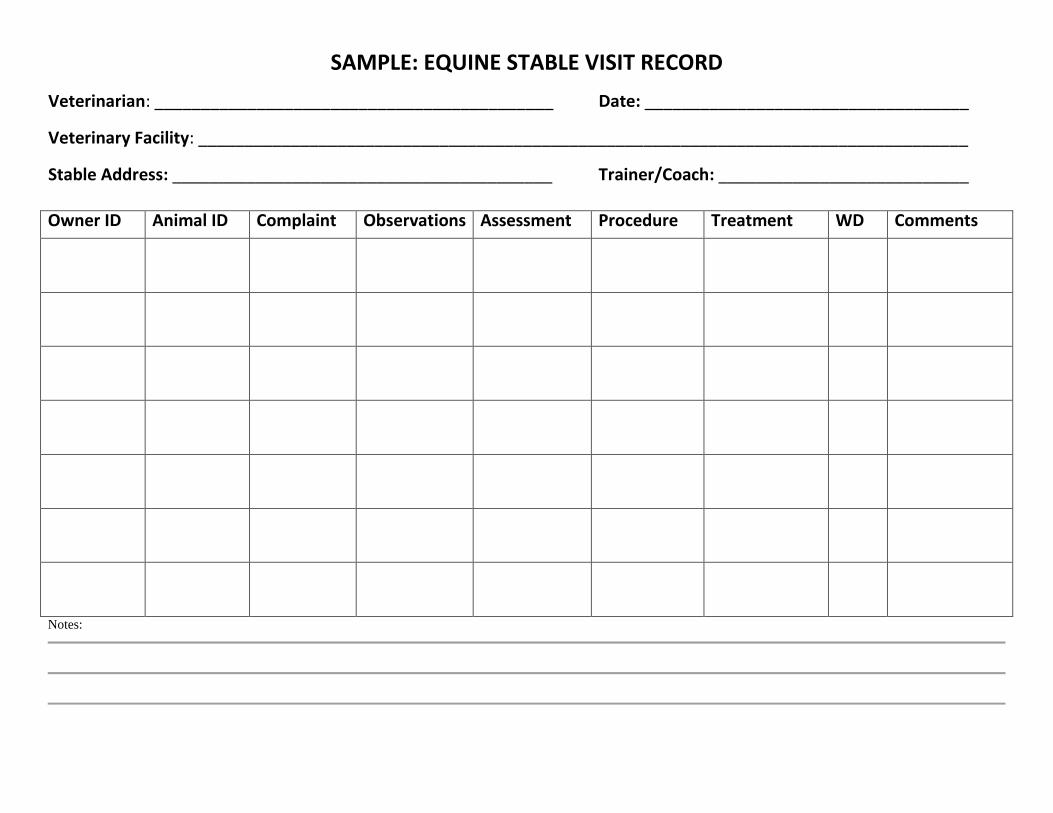
SAMPLE: EQUINE STABLE VISIT RECORD
Veterinarian: ___________________________________________ Date: ___________________________________
Veterinary Facility: ___________________________________________________________________________________
Stable Address: _________________________________________ Trainer/Coach: ___________________________
Owner ID Animal ID Complaint Observations Assessment Procedure Treatment WD Comments
Notes:

SAMPLE: HERD HEALTH REPRODUCTION RECORD (EQUINE)
Year
Client ID #
Herd ID #
Veterinarian Signature: Date:
Date Herd ID # Services Date
Conceived Date Fresh
# Days Open
Remarks Initials
Total # of Services: Total # of Days Open:
Avg. # of Services / Conception: Avg. # of Days Open:
First Service Conception Rate:

SAMPLE: HERD HEALTH VACCINATION RECORD (EQUINE) (where no protocol exists)
Client ID: Animal/Herd ID:
Veterinarian: Date:
Disease to be vaccinated for: IBR, BVD, PI-3, BRSV / Leptospirosis
Age group to be vaccinated:
Vaccine Type:
Primary Dose:
Site of Administration:
Dosage and needle size:
Slaughter or milk withdrawal:
Disease to be vaccinated for: Neonatal Scours
Age group to be vaccinated:
Vaccine Type:
Primary Dose:
Site of Administration:
Dosage and needle size:
Slaughter or milk withdrawal:
Disease to be vaccinated for:
Age group to be vaccinated:
Vaccine Type:
Primary Dose:
Site of Administration:
Dosage and needle size:
Slaughter or milk withdrawal:





























