Embed Size (px)
Citation preview

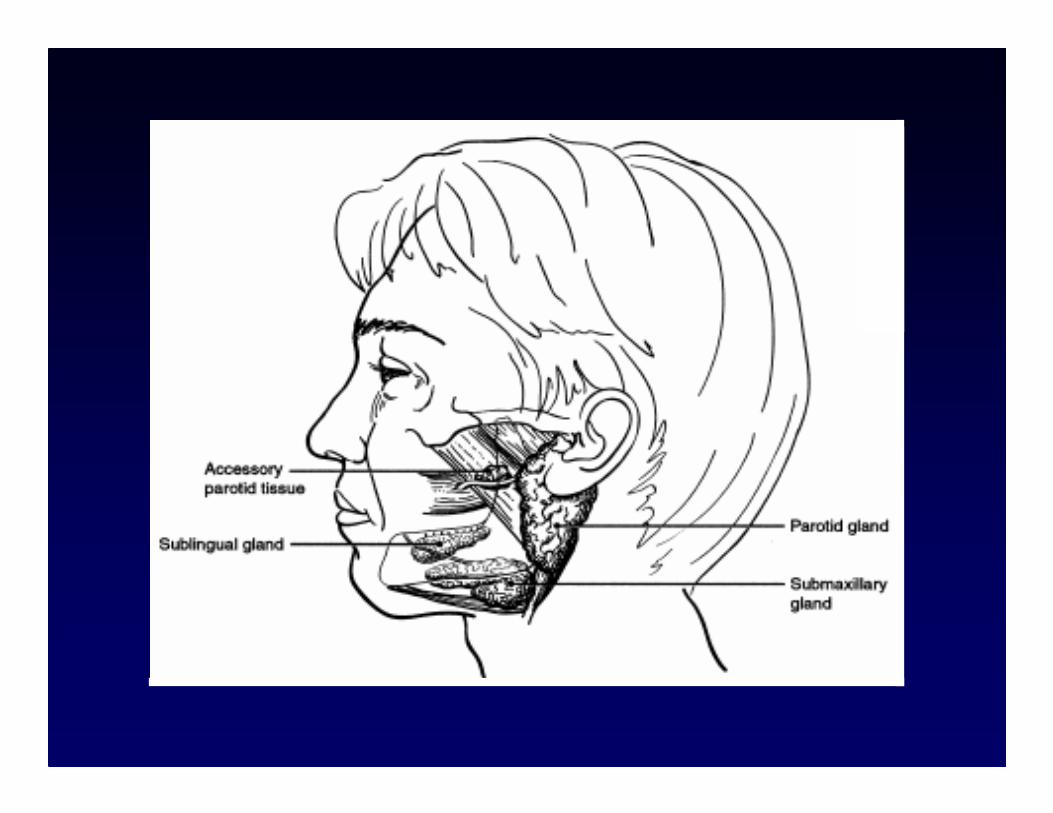
Salivary Gland Tumor
Major salivary glands
• Parotid
• Submandibular
• Sublingual glands
Minor salivary glands
• 500–700 in mucosa of upper aerodigestive tract
• Half are located on the hard palate

Parotid Gland
• The largest salivary gland
• Composed almost entirely of serous acinar
cells
• Accounts for the majority of salivary flow in
an active state but only provides 25 % of the
total volume of saliva
• Facial nerve divides the gland into superficial
lobes (80%) and deep lobes (20%).

Parotid Gland
• The most common site of salivary neoplasms
• Most tumors involve the superficial lobe.
• Successful surgery depends on identification,
dissection, and preservation of the facial nerve
and its branches (frontal, zygomatic, buccal,
marginal mandibular, and cervical)

Submandibular Gland
• The second largest salivary gland
• Composed of both mucous and serous secretory cells
• Supplying approximately 70 per cent of the total volume of saliva
• Wharton's duct drains the gland, eventually opening a few millimeters lateral to the midline lingual frenulum in the anterior floor of the mouth

Sublingual Gland
• The smallest of the major salivary glands
• Produces predominantly mucous secretions
• Lies just beneath the mucosa of the anterior
floor of the mouth

Salivary Gland Tumor
Parotid gland
Submandibular gland
Minor salivary glands
Site
25
50
81
67
8
27
% of
Malignant
% of all
Neoplasms
Shah JP, el al. 1990

Diagnostic Workup
• History: rapid growth, pain
• Physical examination:
- cranial nerve palsy
- neck node enlargement
- hard consistency and fixation
- distant metastasis
- submucosal swelling (minor salivary gland)

Diagnostic Workup
• Radiologic imaging: CT, MRI
- lesions fixed to adjacent bony structures
- lesion involves the parapharyngeal space
- minor salivary cancers arising in the
palate, nasal cavity, nasopharynx and
paranasal sinuses

Diagnostic Workup
• FNA cytology
- confirming the diagnosis of malignancy
- distinguish between salivary and
nonsalivary (lymph node) pathology
- diagnosis of tuberculosis and lymphoma
* A negative finding cannot rule out cancer

Benign Parotid Tumors
• Pleomorphic adenoma (mixed tumor): 80%
Carcinoma ex pleomorphic adenoma 1–7%
• Warthin’s tumor (papillary cystadenoma
lymphomatosum): 10-15%
• Monomorphic adenoma: adenolymphoma, oxyphil
adenoma, sebaceous adenoma, basal cell adenoma,
clear cell adenoma
• Benign lymphoepithelial lesions: AIDS

Pleomorphic Adenoma
• A benign tumor
composed of cells
exhibiting the ability to
differentiate to
epithelial (ductal, and
nonductal cells) and
mesenchymal
(chondroid, myxoid and
osseous) cells

Pleomorphic Adenoma
• Most common neoplasm of salivary glands (45-74%)
• Average age 40-45 years
• Slow growing and asymptomatic
• A single nodular, firm, mobile, slightly compressible mass.
• Recurrent lesions occur as multiple nodules and are less mobile than the original tumor

Warthin’s Tumor
• Occurs only in the parotid gland
• Second most common benign tumor of parotid gland
• Bilateral 10% and multiple lesions 10%
• More common in males (26:1) and smokers
• Occurs as a painless, fluctuant mass
• Retrograde infection
• Ear symptoms (tinnitus, deafness, earache)

Management of
Benign Parotid Tumors
• Superficial parotidectomy with preservation of the
facial nerve and its branches.
• Inadequate local excision or enucleation are prone
to local recurrence and nerve injury.
• Any tumor in the parotid area is considered a
parotid tumor until proved otherwise.
• For a very large deep-lobe parotid tumor, a lower-
lip split incision and mandibulotomy approach
may be required

TNM Staging for Cancers of
the Major Salivary GlandsPrimary tumor (T) Classification
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm in greatest dimension without extraparenchymal extension
T2 Tumor 2 cm but 4 cm in greatest dimension withoutextraparenchymal extension
T3 Tumor having extraparenchymal extension without seventh
nerve involvement and/or 4 cm but 6 cm in greatest
dimension
T4 Tumor invades base of skull, seventh nerve, and/or 6 cm in
greatest dimension

TNM Staging for Cancers of
the Major Salivary Glands

TNM Staging for Cancers of
the Major Salivary Glands
Stage I T1 N0 M0 T2 N0 M0
Stage II T3 N0 M0
Stage III T1 N1 M0 T2 N1 M0
Stage IV T4 N0 M0 T3 N1 M0 T4 N1 M0
Any T N2 M0
Any T N3 M0
Any T Any N M1


Complications of Parotidectomy
• Facial nerve injury
• Hematoma
• Infection
• Flap necrosis
• Salivary fistula
• Frey's syndrome

Malignant Salivary Gland Tumors
• Mucoepidermoid carcinoma is the most common cancer of the parotid gland and all salivary glands.
• Adenoid cystic carcinoma is the most common malignant tumor arising in the submandibular gland.
• In minor salivary sites, adenoid cystic carcinoma and adenocarcinoma are most prevalent.

Mucoepidermoid Carcinoma
• Occurs in major and minor salivary glands
• History of ionizing radiation
• Women to men = 1.5:1
• Occurs as a solitary nodule, pain and trismus
• Facial paralysis
• Numbness of teeth in tumors close to teeth
• Ulceration or hemorrhage from minor salivary gland tumors

Mucoepidermoid Carcinoma
• Low or high grade.
• A standard superficial parotidectomy is adequate treatment for low-grade mucoepidermoid carcinomas.
• High-grade tumors can invade the facial nerve, and the incidence of lymph node metastasis at presentation is approximately 50%.
Malignant Mixed Tumor
• Two types:
- carcinoma ex pleomorphic adenoma
a long-term history of a benign mixed tumor with
rapid growth and fixation to deeper structures and skin.
- true malignant mixed tumor or carcinosarcoma
• 15–20% present with regional lymph node metastases.

Adenoid Cystic Carcinoma
• More common in parotid gland
• Most common malignant tumor of intraoral salivary glands
• Female to male ratio, 3:2
• Local extension beyond the gross lesion
• Perineural involvement
• High incidence of local recurrence
• Distant metastases are common, mostly to the lung.

Factors Affecting Choice of
Treatment
• The extent of the lesion at diagnosis (the clinical
stage)
- small lesions: surgical resection
- large tumors invading adjacent structures:
extensive resection with adjuvant
radiotherapy
- unresectable disease
- disseminated disease

Factors Affecting Choice of
Treatment
• Location
- Borderline resectable lesions in inaccessible
locations, such as tumors involving the base of
skull, may be better suited for nonsurgical
therapy such as chemoradiotherapy or neutron
beam irradiation.
• Histology
- Adenoid cystic carcinoma
- High grade

Surgical Treatment for
Malignant Parotid Tumors
• Minimal operation for parotid lesion is a
superficial parotidectomy with preservation of
facial nerve.
• Deep-lobe parotid tumor can be removed without
injuring the facial nerve.
• A mandibulotomy approach may be necessary for
better exposure of the parapharyngeal area.


• If the facial nerve is not paralyzed preoperatively
and no direct extension into the nerve
- preserve the nerve.
• If the nerve is sacrificed
- immediate nerve grafting with interposition
grafts
- implantation of a Gold Weight in the upper
eyelid to improve eye function and eye closure.
Surgical Treatment for
Malignant Parotid Tumors


• Three important nerves in its vicinity:
- ramus mandibularis
- hypoglossal
- lingual
• Block dissection
- to remove entire contents of the submandibular triangle.
- marginal or segmental mandibulectomy if required.
- supraomohyoid neck dissection if indicated.
Surgical Treatment of Malignant
Submandibular Gland Tumors

• depending on the site of origin
- Lesions in the larynx: conservation laryngeal surgery
or total laryngectomy
- Tongue base: paramedian mandibulotomy
- Palate: partial or subtotal maxillectomy.
- Nasal cavity or paranasal sinuses: combined
craniofacial resection or orbital exenteration in
extensive disease
Surgical Treatment of Malignant
Minor Salivary Gland Tumors

Elective supraomohyoid neck dissection in
- High-grade mucoepidermoid and primary
squamous cell carcinoma.
- High-stage lesions.
Modified or radical neck dissection if
- suspicious lymph nodes are found at surgery.
- grossly palpable nodes at initial evaluation.
Cervical Lymph Nodes in
Malignant Salivary Tumors

• Advanced inoperable cancer
• High-grade, high-stage primary tumor
• Positive margins after surgery
• Deep-lobe malignant tumors
• Lymph node metastases
• Tumor spillage at surgery
Indications for Radiotherapy

• Prognostic factor
- tumor stage
- grade
- histologic type: acinic or low-grade muco-
epidermoid tumors have a better prognosis.
• Generally, tumors of the submandibular gland and minor salivary gland are more aggressive than are parotid tumors
Prognosis

Cure Rates in Patients with
Malignant Tumors