Embed Size (px)
Citation preview

Safety and efficacy of the prostaglandin D2 receptorantagonist AMG 853 in asthmatic patients
William W. Busse, MD,a Sally E. Wenzel, MD,b Eli O. Meltzer, MD,c Edward M. Kerwin, MD,d Mark C. Liu, MD,e
Nan Zhang, PhD,f Yun Chon, PhD,f Alison L. Budelsky, PhD,f Joseph Lin, MD,f and Shao-Lee Lin, MD, PhDf
Madison, Wis, Pittsburgh, Pa, San Diego and Thousand Oaks, Calif, Medford, Ore, and Baltimore, Md
Background: The D-prostanoid receptor and thechemoattractant receptor homologous molecule expressed onTH2 cells (CRTH2) are implicated in asthma pathogenesis.AMG 853 is a potent, selective, orally bioavailable, small-molecule dual antagonist of human D-prostanoid and CRTH2.Objective: We sought to determine the efficacy and safety ofAMG 853 compared with placebo in patients with inadequatelycontrolled asthma.Methods: Adults with moderate-to-severe asthma wererandomized to placebo; 5, 25, or 100 mg of oral AMG 853 twicedaily; or 200 mg of AMG 853 once daily for 12 weeks. Allpatients continued their inhaled corticosteroids. Long-actingb-agonists were not allowed during the treatment period.Allowed concomitant medications included short-actingb-agonists and a systemic corticosteroid burst for asthmaexacerbation. The primary end point was change in totalAsthma Control Questionnaire score from baseline to week 12.Secondary and exploratory end points included FEV1, symptomscores, rescue short-acting b-agonist use, and exacerbations.
From atheDepartment ofMedicine, University ofWisconsin,Madison; btheUniversity of
PittsburghMedical Center; cAllergy and AsthmaMedical Group and Research Center,
San Diego; dthe Clinical Research Institute of Southern Oregon, Medford; ethe Johns
Hopkins Asthma and Allergy Center, Baltimore; and fAmgen, Thousand Oaks, Calif.
Supported by Amgen.
Disclosure of potential conflict of interest: W.W. Busse has served on the advisory board
for Merck; has consultant arrangements with Amgen, AstraZeneca, Novartis,
GlaxoSmithKline, MedImmune, and Genentech; has received research support from
the National Institutes of Health (NIH)/National Institute of Allergy and Infectious
Diseases and the NIH/National Heart, Lung, and Blood Institute. S. E. Wenzel has re-
ceived research support from Amgen. E. M. Kerwin has received research support
from Amgen; has served on advisory boards or speakers’ panels for Astra Zeneca
(MAP Pharma), Dey Laboratories, Ironwood Pharmaceuticals, Pfizer, Sanofi Aventis,
Sunovion (Sepracor), and Targacept; has received travel reimbursement from Merck
(Schering-Plough), Forest Labs, and Novartis; has conducted clinical research trials
for Abbott, Actelion, Adams, Alcon, ALK-Abell�o, Allergy Therapeutics, Almirall,
Amgen, Amphastar, Astellas, Astra Zeneca (MAP Pharma), Asubio, Biota, Boeh-
ringer Ingelheim, Cephalon (Centocor, Ception), Chiesi, Critical Therapeutics, Daii-
chi Sankyo, Dey Labs, Elevation Pharma, Elixir, Exelixis, Forest, Genentech,
GlaxoSmithKline, Incyte, Inflazyme, Johnson & Johnson, Lilly, Meda, Medicinova,
MedImmune, Med Pointe, Merck (Schering-Plough), Mpex, Novartis, Novo Nordisk,
Otsuka, Pearl, Pfizer (Wyeth), Phenomix, Replidyne, Roche, Sanofi-Aventis, Skye
Pharma, Stallergenes, Sunovion (Altana, Sepracor), TAP, Takeda, Targacept, Teva
(Ivax), UCB Pharma, and Wellstat. M. C. Liu has received research support from
GlaxoSmithKline, MedImmune, Sanofi-Aventis, and Amgen and has served on the
Data Safety Monitoring Board for Cephalon. N. Zhang, A. L. Budelsky, J. Lin, and
S.-L. Lin are employed by Amgen. Y. Chon is employed by and holds stock in Amgen.
The rest of the authors declare that they have no relevant conflicts of interest.
Received for publication April 10, 2012; revised October 2, 2012; accepted for publica-
tion October 12, 2012.
Available online November 20, 2012.
Corresponding author: William W. Busse, MD, Allergy, Pulmonary and Critical Care
Medicine, University of Wisconsin School of Medicine and Public Health, K4/910
CSC, MC 9988, 600 Highland Ave, Madison, WI 53792. E-mail: Wwb@medicine.
wisc.edu.
0091-6749/$36.00
� 2012 American Academy of Allergy, Asthma & Immunology
http://dx.doi.org/10.1016/j.jaci.2012.10.013
Results: Among treated patients, no effect over placebo (n 5 79)was observed in mean changes in Asthma ControlQuestionnaire scores at 12 weeks (placebo, 20.492; range forAMG 853 groups [n 5 317], 20.444 to 20.555). No significantdifferences between the active and placebo groups wereobserved for secondary end points. The most commonlyreported adverse events were asthma, upper respiratory tractinfection, and headache; 9 patients experienced serious adverseevents, all of which were deemed unrelated to study treatmentby the investigator.Conclusion: AMG 853 as an add-on to inhaled corticosteroidtherapy demonstrated no associated risks but was not effectiveat improving asthma symptoms or lung function in patients withinadequately controlled moderate-to-severe asthma. (J AllergyClin Immunol 2013;131:339-45.)
Key words: Asthma, chemoattractant receptor homologousmolecule expressed on TH2 cells, D-prostanoid, Asthma ControlQuestionnaire, prostaglandin D2
Allergic asthma is characterized by an abnormal shift towardthe TH2 lymphocyte immune response, increasing the release ofcytokines that promote airway inflammation.1 Prostaglandin D2
(PGD2), a major COX product formed in activated mast cells,has been reported to mediate asthmatic responses.2-4 The activityof PGD2 is exerted through 2 different G protein–coupled recep-tors, D-prostanoid (DP) and chemoattractant receptor homolo-gous molecule expressed on TH2 cells (CRTH2), which appearto play a central role in the development of asthma.5 Preclinicalstudies in DP-deficient mice2 and with an oral DP antagonist6,7
have shown that DP mediates asthma-related inflammation.CRTH2 antagonism has been shown to reduce inflammation inanimal models of asthma8,9 and in patients with moderate persis-tent asthma.10 Taken together, this suggests that inhibition of DPand CRTH2 could be a potential therapeutic approach to asthma.AMG 853 is a potent, selective, and orally bioavailable small-
molecule dual antagonist of human DP and CRTH2.11-13 In vitroradioligand-binding studies indicate that AMG 853 inhibits bind-ing of PGD2 to humanCRTH2 and humanDP.12 In phase 1 studiesadministration of AMG853 has been shown to have no associatedsafety risks, has approximately dose-proportional pharmacoki-netics, and effectively antagonizes ex vivo PGD2 responses medi-ated by DP and CRTH2.11,13 The current study examined thesafety and efficacy of AMG 853 compared with placebo in pa-tients with inadequately controlled asthma.
METHODS
PatientsEligible patients were aged 18 to 65 years, had moderate-to-severe asthma,
and were receiving stable inhaled corticosteroids (ICSs; >_200 and <_1000mg/d
339

J ALLERGY CLIN IMMUNOL
FEBRUARY 2013
340 BUSSE ET AL
Abbreviations used
ACQ: A
sthma Control QuestionnaireAQLQ: A
sthma Quality of Life QuestionnaireBID: T
wice dailyCRTH2: C
hemoattractant receptor homologous molecule expressedon TH2 cells
DP: D
-prostanoidFENO: F
raction of exhaled nitric oxideICS: In
haled corticosteroidLABA: L
ong-acting b-agonistPEFR: P
eak expiratory flow ratePGD2: P
rostaglandin D2QD: O
nce dailySABA: S
hort-acting b-agonistfluticasone or equivalent) for 30 or more days, with consecutive use for at least
the prior 3 months before screening. Patients were recruited from each clinical
site’s pool of patients or from referral and selected based on key inclusion
criteria, which included ongoing asthma symptoms with Asthma Control
Questionnaire (ACQ) scores of 1.5 or greater at screening and baseline, 50%or
greater and 80% or less FEV1 at screening, and at least 12% reversibility over
baseline FEV1 with a short-acting b-agonist (SABA; <_8 puffs) or nebulized
equivalent (<_2 treatments with 2.5 mg of albuterol). Key exclusion criteria in-
cluded asthma exacerbation requiring emergency department treatment or
hospitalization within 2 months of screening, history of any chronic non-
asthma pulmonary condition, or systemic corticosteroid use within 6 weeks
of screening. Full inclusion and exclusion criteria are available in the protocol
synopsis in the Methods section in this article’s Online Repository at
www.jacionline.org. Atopy status was assessed for all patients by using either
skin prick tests or RASTs, but data regarding allergen exposure on study were
not collected.
All patients providedwritten informed consent, and the studywas approved
by the institutional review board of each participating site. Subject compen-
sation for study involvement varied by site and region as directed by national
and local guidelines for each region andAmgen (ThousandOaks, Calif) policy.
Study designThis phase 2, randomized, double-blind, placebo-controlled study was
conducted in 73 centers located in the United States, Canada, and Europe.
Eligible patients completed a 4-week run-in period and a washout of excluded
asthma medication before the run-in period. Patients were randomized in a
1:1:1:1:1 ratio to receive oral placebo; 5, 25, or 100 mg of AMG 853 twice
daily (BID); or 200 mg of AMG 853 once daily (QD). All patients continued
on ICSs at the screening dose or equivalent, with no adjustments permitted.
Rescue therapy allowed during the study included as-needed SABAs and
1 course of systemic corticosteroids for an asthma exacerbation. If a subject
required a prolonged or second course of systemic corticosteroids, cessation of
blinded investigational product was mandated.
The primary endpointwas the change inACQsymptomscores frombaseline
to week 12. Secondary end points included change from baseline to week 12 in
prebronchodilator and postbronchodilator FEV1 (percentage change), morning
and evening peak expiratory flow rate (PEFR), frequency of rescue SABA use,
daily asthma symptoms, AsthmaQuality of Life Questionnaire (AQLQ) scores,
and the proportion of symptom-free days over the treatment period. The inci-
dence of asthma exacerbations (defined as asthma deteriorations requiring
administration of systemic corticosteroids) was evaluated as an exploratory
end point. Other exploratory end points included fraction of exhaled nitric oxide
(FENO) and induced sputum eosinophil numbers (substudy). Blood eosinophil
numbers and serum IgE levels were also assessed. PGD2 is chemically unstable
and rapidly metabolized in the presence of albumin, and thus serum measure-
ments of PGD2 can be difficult to interpret.14,15
Safety evaluations included incidence and severity of adverse events and
changes in electrocardiographic results, laboratory profiles, and vital signs.
AssessmentsThe ACQ results in a validated composite symptom score that assesses
disease control, which includes symptoms and FEV1.16,17 The ACQ was ad-
ministered at every scheduled study visit, which occurred every other week
during the treatment period.
For FEV1 evaluations, patients were instructed towithhold use of SABAs at
least 6 hours before each scheduled test; the highest value from 3 separate eval-
uations was recorded for each test. Prebronchodilator spirometric evaluations
were performed in themorningbefore anyuseof bronchodilators. Postbroncho-
dilator measurements were recorded 15 to 45minutes after bronchodilator use.
A peak flowmeter was dispensed, and patients were instructed to measure
PEFR twice daily at approximately the same times each day (eg, within 1 hour
of waking and immediately before bedtime) at least 6 hours after the last use of
a SABA. The best of 3 PEFR efforts was recorded.
FENO values were assessed by using the NioxMino (Niox,Morrisville, NC)
at day 1 and weeks 4, 12, and 14 (end of study visit) according to American
Thoracic Society/European Respiratory Society guidelines.18 Induced sputum
samples were obtained at the baseline visit (day 1) and at the week 12 visit in a
subset of patients who consented to the procedure. Sites participating in the
induced sputum substudy used their institution’s standard procedure for col-
lection and processing for cell counts. All samples were sent to a central lab-
oratory for analysis.
Patients received an electronic diary (e-diary, AM3 device; ERT, Phila-
delphia, Pa) to record their rescue SABA use, PEFR, and asthma symptoms
twice a day. Symptoms were assessed on a 21-point scale (each of 7 items on a
0- to 3-point Likert scale) and included nighttime awakenings/symptoms,
wheezing, shortness of breath, cough, chest tightness, and activity limitation.
Site staff trained patients on the proper use of the e-diary at run-in and
downloaded the e-diary at each visit to ensure adherence.
The AQLQ, a 32-item, validated quality-of-life instrument,19 was adminis-
tered during visits at screening, run-in, baseline, week 12, and week 14.
Statistical analysisA patient population of 375 (75 per treatment arm) was estimated to
provide greater than 80% power to detect a linear trend for drug effect in the
primary end point of ACQ score change from baseline at week 12 with a
significance level of .05. This calculation assumed a mean difference of 0.05,
0.3, and 0.5 for the 5-, 25-, and 100-mg AMG 853 BID dose groups,
respectively, compared with placebowith an SD of 1.0. A dropout rate of 15%
was assumed. The primary end point was analyzed by using an analysis of
covariance with the treatment group as the main factor, adjusting for baseline
ACQ scores and the stratification factor. Similar analyses of covariance were
performed for the continuous secondary end points, and the stratifiedCochran-
Mantel-Haenszel test was used to analyze categorical end points. Means and
SEs were reported for the differences between each arm of the AMG 853 and
placebo groups. Linear trend tests of the AMG 853 BID treatment arms were
performed to test for a drug effect. The last observation carried forward
method was used to impute missing data, except for safety and patient-
reported outcomes, for which data were reported as observed. Efficacy and
safety analyses were performed for the intent-to-treat population, who were
randomized and received at least 1 dose of AMG 853 or placebo.
RESULTS
DispositionA total of 397 patients were randomized (placebo, n5 79; 5mg
of AMG 853 BID, n5 80; 25 mg of AMG 853 BID, n5 79; 100mg of AMG 853 BID, n5 79; and 200 mg of AMG 853 QD, n580), and 396 received investigational product. One patientenrolled into the 5-mg AMG 853 BID group but did not meeteligibility requirements and therefore did not receive investiga-tional product. Of all patients randomized, 351 (88.4%) com-pleted the study. Forty-six patients prematurely discontinued thestudy, with 7 (8.9%), 14 (17.5%), 4 (5.1%), 9 (11.4%), and 12

J ALLERGY CLIN IMMUNOL
VOLUME 131, NUMBER 2
BUSSE ET AL 341
(15.0%) patients discontinuing in the placebo, 5 mg of AMG 853BID, 25 mg of AMG 853 BID, 100mg of AMG 853 BID, and 200mg of AMG 853QD groups, respectively. Patients withdrewmostcommonly because of adverse events (n5 13 [3.3%]), withdrawnconsent (n 5 10 [2.5%]), or protocol deviations (n 5 6 [1.5%]).
Baseline demographics and disease characteristicsBaseline demographics and disease characteristics are pre-
sented in Table I. Overall, patients had a mean age of approxi-mately 45 years, and the majority were white (76.0%) andfemale (59.8%). Mean duration of asthma ranged from 24.8 to28.9 years between study groups. Mean ACQ scores, percentpredicted FEV1, and rescue medication use (Table I) were consis-tent with a population of patients with moderate-to-severe asthmawhose symptoms were not well controlled per National AsthmaEducation and Prevention Program guidelines.20 There were nonotable differences in baseline characteristics among the treat-ment groups. See Tables E1 and E2 in this article’s OnlineRepository at www.jacionline.org regarding comorbidities andconcomitant medications not related to asthma.
EfficacyACQ. At week 12, the placebo group had a mean ACQ score
change from baseline of20.492, and the 5 mg of AMG 853 BID,25 mg of AMG 853 BID, 100 mg of AMG 853 BID, and 200 mgof AMG 853 QD groups demonstrated mean changes of20.541,20.555, 20.444, and 20.498, respectively (Fig 1 and Table II).No statistically significant differences were observed in the over-all linear trend test or any pairwise comparison between the activeversus placebo groups.Lung function. At week 12, the placebo group had a mean
prebronchodilator FEV1 volume change from baseline of 0.019 L,and the 5mgofAMG853BID, 25mgofAMG853BID, 100mg ofAMG853 BID, and 200mg of AMG 853QDgroups demonstratedchanges of 0.045, 0.039,20.021, and 0.050 L, respectively, repre-senting changes in percent predicted prebronchodilator FEV1 of0.896, 1.462, 1.019,20.518, and 1.288 (Fig 2 and Table II). Valuesformorning and eveningPEFRchange frombaseline atweek12 areavailable in Table II. For FEV1 and PEFR, no statistically signifi-cant differences were observed in the overall linear trend test orany pairwise comparison between the active versus placebo groups.Symptoms. The daily diary symptom score mean change
from baseline at week 12 for the placebo, 5 mg of AMG 853 BID,25 mg of AMG 853 BID, 100 mg of AMG 853 BID, and 200 mgof AMG 853 QD groups were21.370,21.478,21.225,21.110,and21.273, respectively (Table II). The proportion of symptom-free days during the 12-week double-blind period were 0.220,0.214, 0.238, 0.187, and 0.189, respectively (Table II). Themean change from baseline in number of puffs of SABA usedper day at week 12 were 20.497, 0.357, 20.144, 20.329, and20.204, respectively (Table II). No statistically significant differ-ences were observed in the overall linear trend test or any pairwisecomparison between the active versus placebo groups.Exacerbations. The incidences of exacerbation during the
12-week double-blind treatment period for the placebo, 5 mg ofAMG 853 BID, 25 mg of AMG 853 BID, 100 mg of AMG 853BID, and 200 mg of AMG 853 QD groups were 7.6%, 10.1%,5.1%, 10.1%, and 7.5%, respectively. No statistically significantdifferences were observed between the active versus placebo
groups; however, this study was not powered to detect statisticallysignificant differences in exacerbations.Quality of Life. Themean change from baseline at week 12 in
the AQLQ total score for the placebo, 5 mg of AMG 853 BID,25 mg of AMG 853 BID, 100 mg of AMG 853 BID, and 200 mgof AMG 853 QD groups were 0.530, 0.705, 0.518, 0.575, and0.565, respectively (Table II). No statistically significant differ-ences were observed in the overall linear trend test or any pairwisecomparison between the active versus placebo groups.Subgroups analyses. Prespecified subgroups defined by
surrogates of disease severity (baseline ACQ score tertile, FEV1,bronchodilator response, ICS dose, and long-acting b-agonist[LABA] use at screening) or markers of inflammation (atopic sta-tus, baseline FENO value, and blood eosinophilia) were analyzedto investigate whether there was a subpopulation that had differ-ential efficacy. For the ICS dose, patients were segregated into2 groups: those receiving 500 mg/d or greater of fluticasone pow-der equivalent and those receiving less than 500mg/d. No increasein efficacy over placebo was observed for all subgroups analyzed.
BiomarkersThe baseline serum IgE level did not change at week 12 for the
placebo, 5mg of AMG853BID, 25mg of AMG853BID, 100mgof AMG 853 BID, and 200 mg of AMG 853 QD groups (meanchange from baseline: 0.62%, 6.45%, 1.43%, 1.57%, and 3.23%,respectively; all P > .05 vs placebo). The FENO value also did notchange from baseline to week 12 (mean change from baseline:0.221, 2.368, 20.080, 1.333, and 27.000 ppb, respectively; allP >.05 vs placebo). A substudy, which included 59 patients, eval-uated induced sputum cell counts at the baseline and week 12visits. There was variability in sputum eosinophil and neutrophildata (see Table E3 in this article’s Online Repository at www.jacionline.org), and no patterns regarding efficacy relative to spu-tum cell counts could be identified.
SafetyThe incidence of treatment-emergent and treatment-related
adverse events was similar between study groups (Table III). Themost commonly reported adverse events among all patients wereasthma, upper respiratory tract infection, and headache (Table III).Nine patients reported serious adverse events (Table III), includ-
ing 1 death (autopsy finding of dilated cardiomyopathy) in the 200mg ofAMG853QDgroup. The death and all other serious adverseevents were assessed by the investigators to be unrelated to studytreatment, and there was no dose-related trend. Patient discontinu-ation of study treatment because of adverse events was 3.8% (n53) for the placebo group and 4.1% (n 5 13) for the AMG 853groups overall. Therewere no clinically significant changes invitalsign measurements and no clinically significant treatment-relatedtrends in laboratory results (data not shown). The observed adverseevents did not affect the benefit/risk assessment for AMG 853.
DISCUSSIONThis study provides the first clinical data to date examining the
effects of a CRTH2 and DP dual antagonist as add-on treatment toICS therapy in asthma. The findings from this study suggest thatAMG 853, when evaluated as add-on treatment to ICSs in patientswithmoderate-to-severe persistent asthmawhose symptoms are not

TABLE I. Baseline demographics and disease characteristics
Characteristic Placebo (n 5 79)
AMG 853
5 mg BID
(n 5 79)
25 mg BID
(n 5 79)
100 mg BID
(n 5 79)
200 mg QD
(n 5 80)
Mean (SD) age (y) 46.3 (11.4) 44.7 (11.5) 45.0 (11.3) 44.6 (11.4) 43.7 (11.4)
Female sex, no. (%) 52 (65.8) 52 (65.8) 46 (58.2) 55 (69.8) 32 (40.0)
Race, no. (%)
White 62 (78.5) 59 (74.7) 59 (74.7) 60 (75.9) 61 (76.3)
Black 8 (10.1) 9 (11.4) 12 (15.2) 11 (13.9) 11 (13.8)
Hispanic/Latino 6 (7.6) 7 (8.9) 5 (6.3) 4 (5.1) 5 (6.3)
Asian 2 (2.5) 3 (3.8) 1 (1.3) 1 (1.3) 3 (3.8)
Other 1 (1.3) 1 (1.3) 2 (2.5) 3 (3.8) 0 (0)
Mean (SD) BMI (kg/m2) 31.0 (7.2) 29.6 (6.4) 32.0 (6.5) 31.9 (8.0) 31.4 (7.2)
Mean (SD) ACQ score 2.5 (0.6) 2.5 (0.6) 2.4 (0.5) 2.5 (0.6) 2.5 (0.6)
Mean (SD) AQLQ score 4.7 (1.1) 4.6 (1.2) 4.7 (1.0) 4.5 (1.1) 4.6 (1.1)
Mean (SD) prebronchodilator FEV1 (L/s) 2.106 (0.476) 2.259 (0.580) 2.266 (0.540) 2.151 (0.545) 2.305 (0.528)
Mean (SD) percent predicted prebronchodilator FEV1 66.3 (7.8) 68.2 (7.9) 67.1 (7.9) 66.7 (8.5) 66.1 (8.9)
Mean (SD) reversibility of prebronchodilator FEV1 (%) 17.1 (11.2) 20.9 (13.6) 17.9 (11.7) 15.8 (9.7) 17.9 (13.8)
Mean (SD) postbronchodilator FEV1 (L/s) 2.460 (0.568) 2.717 (0.693) 2.658 (0.650) 2.484 (0.660) 2.712 (0.675)
Mean (SD) predicted postbronchodilator FEV1 (%) 77.6 (10.9) 82.1 (10.2) 78.6 (10.2) 76.8 (9.3) 77.8 (12.2)
Mean (SD) duration of asthma (y) 28.2 (14.1) 28.0 (14.1) 24.8 (13.2) 28.9 (14.5) 27.3 (12.8)
Prior LABA use (%) 74.7 75.9 65.8 73.4 76.3
Mean (SD) baseline ICS dose* (mg/d) 409.5 (241.4) 442.3 (244.0) 423.7 (234.5) 431.0 (239.7) 483.8 (259.4)
Mean (SD) rescue b-agonist use (puffs/d) 3.6 (6.6) 2.7 (2.2) 2.7 (3.1) 3.3 (3.8) 2.9 (2.5)
Mean (SD) morning peak flow (L/min) 339.3 (98.5) 347.2 (101.5) 366.5 (115.1) 347.6 (106.7) 386.9 (96.5)
Mean (SD) daily asthma symptom score 5.1 (3.1) 4.9 (3.2) 4.9 (3.1) 4.8 (2.8) 5.2 (3.3)
Mean (SD) overall daily asthma control score 6.4 (3.7) 6.2 (3.7) 6.1 (3.8) 6.2 (3.4) 6.6 (3.8)
Atopic,� no. (%) 73 (92.4) 74 (93.7) 72 (91.1) 72 (91.1) 76 (95.0)
Mean (SD) FENO (ppb) 28.1 (22.0) 31.9 (21.4) 30.9 (30.5) 28.3 (23.2) 33.5 (31.6)
Mean (SD) total serum IgE (IU/mL) 321.4 (518.2) 487.0 (633.2) 488.2 (1030.8) 344.9 (594.3) 276.0 (307.1)
BMI, Body mass index.
*Fluticasone or equivalent.
�Atopy was defined on study as a positive skin prick test response (>_3 mm wheal) or a positive RAST result.
FIG 1. Change from baseline in total ACQ score for patients receiving placebo, 5 mg of AMG 853 BID, 25 mg
of AMG 853 BID, 100 mg of AMG 853 BID, and 200 mg of AMG 853 QD. BL, Baseline.
J ALLERGY CLIN IMMUNOL
FEBRUARY 2013
342 BUSSE ET AL
fully controlledwith ICSs, demonstratedno improvement in controlof asthma or modifying biomarkers. The adverse events observedafter AMG 853 treatment would not preclude further clinicaldevelopment if AMG 853 had demonstrated a clinical benefit.Doses of AMG 853 used in this study were chosen based on
phase 1 data, which applied assays of ex vivo PGD2 responses inwhole blood mediated by CRTH2 and DP receptors to generateinhibitory thresholds for both targets (IC90).
11 In whole bloodAMG 853 has a CRTH2 receptor potency value of 0.12 ng/mL
(reported as 0.2 nmol/L) and a DP receptor potency value of2.87 ng/mL (4.7 nmol/L).12 The ex vivo assays of cyclic AMPrelease downstream of DP1, CRTH2 internalization, and eosino-phil shape change are live cell assays. These pharmacodynamicassays are more commonly used to bridge phase 1 data to guidedose selection in phase 2 studies. The 100 mg of AMG 853BID and 200 mg of AMG 853 QD doses in this phase 2 studywere modeled to yield plasma drug levels near or greater thanthe IC90. Exposure data from this study showed that plasma
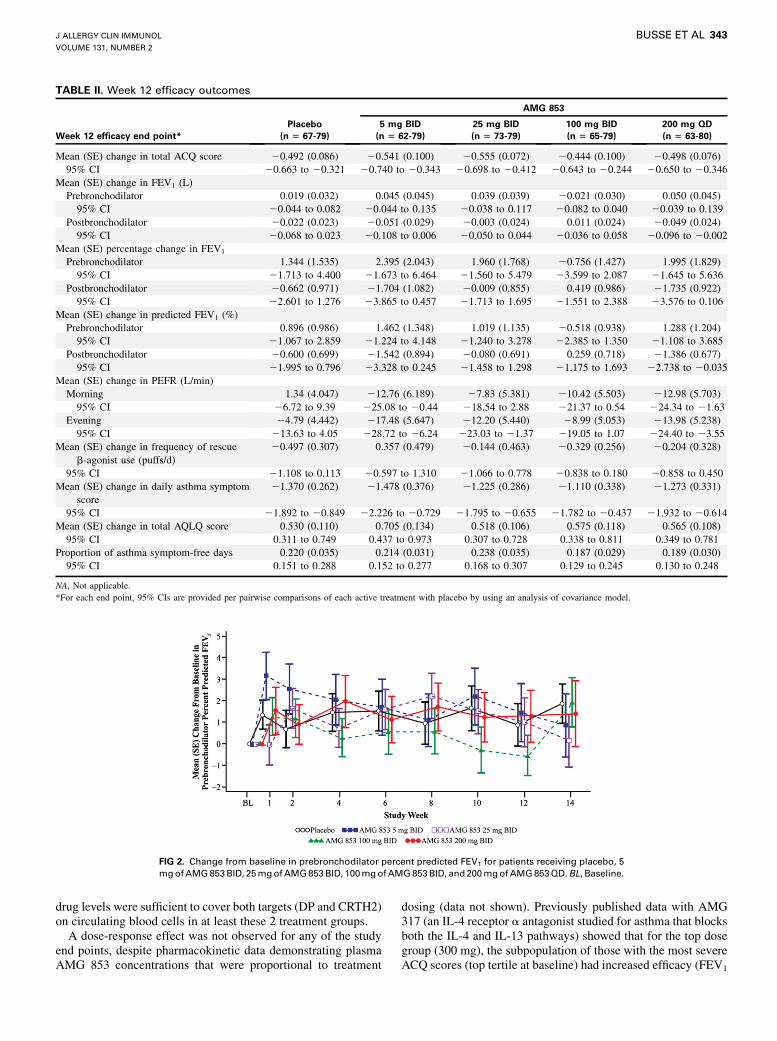
TABLE II. Week 12 efficacy outcomes
Week 12 efficacy end point*
Placebo
(n 5 67-79)
AMG 853
5 mg BID
(n 5 62-79)
25 mg BID
(n 5 73-79)
100 mg BID
(n 5 65-79)
200 mg QD
(n 5 63-80)
Mean (SE) change in total ACQ score 20.492 (0.086) 20.541 (0.100) 20.555 (0.072) 20.444 (0.100) 20.498 (0.076)
95% CI 20.663 to 20.321 20.740 to 20.343 20.698 to 20.412 20.643 to 20.244 20.650 to 20.346
Mean (SE) change in FEV1 (L)
Prebronchodilator 0.019 (0.032) 0.045 (0.045) 0.039 (0.039) 20.021 (0.030) 0.050 (0.045)
95% CI 20.044 to 0.082 20.044 to 0.135 20.038 to 0.117 20.082 to 0.040 20.039 to 0.139
Postbronchodilator 20.022 (0.023) 20.051 (0.029) 20.003 (0.024) 0.011 (0.024) 20.049 (0.024)
95% CI 20.068 to 0.023 20.108 to 0.006 20.050 to 0.044 20.036 to 0.058 20.096 to 20.002
Mean (SE) percentage change in FEV1
Prebronchodilator 1.344 (1.535) 2.395 (2.043) 1.960 (1.768) 20.756 (1.427) 1.995 (1.829)
95% CI 21.713 to 4.400 21.673 to 6.464 21.560 to 5.479 23.599 to 2.087 21.645 to 5.636
Postbronchodilator 20.662 (0.971) 21.704 (1.082) 20.009 (0.855) 0.419 (0.986) 21.735 (0.922)
95% CI 22.601 to 1.276 23.865 to 0.457 21.713 to 1.695 21.551 to 2.388 23.576 to 0.106
Mean (SE) change in predicted FEV1 (%)
Prebronchodilator 0.896 (0.986) 1.462 (1.348) 1.019 (1.135) 20.518 (0.938) 1.288 (1.204)
95% CI 21.067 to 2.859 21.224 to 4.148 21.240 to 3.278 22.385 to 1.350 21.108 to 3.685
Postbronchodilator 20.600 (0.699) 21.542 (0.894) 20.080 (0.691) 0.259 (0.718) 21.386 (0.677)
95% CI 21.995 to 0.796 23.328 to 0.245 21.458 to 1.298 21.175 to 1.693 22.738 to 20.035
Mean (SE) change in PEFR (L/min)
Morning 1.34 (4.047) 212.76 (6.189) 27.83 (5.381) 210.42 (5.503) 212.98 (5.703)
95% CI 26.72 to 9.39 225.08 to 20.44 218.54 to 2.88 221.37 to 0.54 224.34 to 21.63
Evening 24.79 (4.442) 217.48 (5.647) 212.20 (5.440) 28.99 (5.053) 213.98 (5.238)
95% CI 213.63 to 4.05 228.72 to 26.24 223.03 to 21.37 219.05 to 1.07 224.40 to 23.55
Mean (SE) change in frequency of rescue
b-agonist use (puffs/d)
20.497 (0.307) 0.357 (0.479) 20.144 (0.463) 20.329 (0.256) 20.204 (0.328)
95% CI 21.108 to 0.113 20.597 to 1.310 21.066 to 0.778 20.838 to 0.180 20.858 to 0.450
Mean (SE) change in daily asthma symptom
score
21.370 (0.262) 21.478 (0.376) 21.225 (0.286) 21.110 (0.338) 21.273 (0.331)
95% CI 21.892 to 20.849 22.226 to 20.729 21.795 to 20.655 21.782 to 20.437 21.932 to 20.614
Mean (SE) change in total AQLQ score 0.530 (0.110) 0.705 (0.134) 0.518 (0.106) 0.575 (0.118) 0.565 (0.108)
95% CI 0.311 to 0.749 0.437 to 0.973 0.307 to 0.728 0.338 to 0.811 0.349 to 0.781
Proportion of asthma symptom-free days 0.220 (0.035) 0.214 (0.031) 0.238 (0.035) 0.187 (0.029) 0.189 (0.030)
95% CI 0.151 to 0.288 0.152 to 0.277 0.168 to 0.307 0.129 to 0.245 0.130 to 0.248
NA, Not applicable.
*For each end point, 95% CIs are provided per pairwise comparisons of each active treatment with placebo by using an analysis of covariance model.
FIG 2. Change from baseline in prebronchodilator percent predicted FEV1 for patients receiving placebo, 5
mgofAMG853BID, 25mgofAMG853BID, 100mgofAMG853BID, and200mgofAMG853QD.BL, Baseline.
J ALLERGY CLIN IMMUNOL
VOLUME 131, NUMBER 2
BUSSE ET AL 343
drug levels were sufficient to cover both targets (DP and CRTH2)on circulating blood cells in at least these 2 treatment groups.A dose-response effect was not observed for any of the study
end points, despite pharmacokinetic data demonstrating plasmaAMG 853 concentrations that were proportional to treatment
dosing (data not shown). Previously published data with AMG317 (an IL-4 receptor a antagonist studied for asthma that blocksboth the IL-4 and IL-13 pathways) showed that for the top dosegroup (300 mg), the subpopulation of those with the most severeACQ scores (top tertile at baseline) had increased efficacy (FEV1

TABLE III. Summary of adverse events
Adverse events, no. (%) Placebo (n 5 79)
AMG 853
5 mg BID (n 5 79) 25 mg BID (n 5 79) 100 mg BID (n 5 79) 200 mg QD (n 5 80)
All 36 (45.6) 43 (54.4) 52 (65.8) 42 (53.2) 41 (51.3)
Treatment related 6 (7.6) 11 (13.9) 11 (13.9) 7 (8.9) 8 (10.0)
SAE 2 (2.5) 1 (1.3) 0 (0) 3 (3.8) 3 (3.8)
SAE, treatment related 0 (0) 0 (0) 0 (0) 0 (0) 0 (0)
Occurring in >_5% of patients
Asthma 12 (15.2) 12 (15.2) 13 (16.5) 12 (15.2) 11 (13.8)
Upper respiratory tract infection 6 (7.6) 9 (11.4) 9 (11.4) 5 (6.3) 4 (5.0)
Headache 0 (0) 4 (5.1) 5 (6.3) 1 (1.3) 5 (6.3)
Nasopharyngitis 3 (3.8) 2 (2.5) 3 (3.8) 5 (6.3) 1 (1.3)
Sinusitis 1 (1.3) 3 (3.8) 4 (5.1) 1 (1.3) 0 (0)
Viral gastroenteritis 0 (0) 4 (5.1) 2 (2.5) 0 (0) 1 (1.3)
Back pain 4 (5.1) 0 (0) 2 (2.5) 1 (1.3) 0 (0)
SAE, Serious adverse event.
J ALLERGY CLIN IMMUNOL
FEBRUARY 2013
344 BUSSE ET AL
and ACQ score improvement) relative to the overall population.21
A similar pattern in efficacy was observed in 2 other subpopula-tions: one with peripheral blood eosinophilia of 6% or greaterand the other with bronchodilator response of 20% or greater atbaseline (Amgen, data on file). Recently published data with leb-rikizumab showed increased efficacy (FEV1 and exacerbations) insubpopulations with high FENO or high periostin values at base-line.22 However, in this study with AMG 853, despite comparablenumbers of patients for evaluation, similar prespecified subgroupanalyses (subpopulations segregated by LABA use at screening,baseline FEV1, ACQ score, ICS dose, bronchodilator response,FENO value, and blood eosinophilia) did not identify a subpopula-tion with improved efficacy over placebo.There are published data for a DP-selective agent23 and a
CRTH2-selective agent.10The studywith aDP-selective agent (lar-opiprant) used a double-blind crossover designwith a 5-week treat-ment period in patientswithmild-to-severe asthma, about one thirdof whomwere receiving ICS therapy.23 No improvements in FEV1
or asthma symptomswere noted.23OC000459, a CRTH2-selectiveantagonist, hadmixed results in the setting of inhaled allergen chal-lenge24: one crossover group had a positive result, but the other didnot.A trial ofOC000459 (at dose levels comparablewithAMG853doses in this study) in patients with moderate-to-severe persistentasthma who were not receiving ICSs showed a 22% improvementin nighttime symptom scores over placebo and a statistically signif-icant but not clinically meaningful change in FEV1 of 2.8% overplacebo in the overall population.10 The CRTH2 receptor potencyvalue of AMG 853 of 0.12 ng/mL12 is higher when compared withthat ofOC000459 (35ng/mL).10Comparisonof potencies are com-plicated by reports from different groups with assays using differ-ent methods. The key difference between the study reported hereand the OC000459 study is that AMG 853 was tested as an add-on to ICS controller therapy, whereas OC000459 was studied asmonotherapy (in ICS-naive subjects). Therefore it is uncertainwhether OC000459 or other CRTH2-selective antagonists can im-prove asthma-related end points as add-on therapy to ICSs inpatients with inadequately controlled moderate-to-severe disease.Other CRTH2 antagonists are currently being tested.There are inherent limitations to the target population, study
design, and mechanism of action. Patients with asthma whosesymptoms are not controlled despite ICS therapy (with or withoutadditional LABAs) have a high threshold for demonstratingefficacy with additional therapies. The study design (limitedsample size and treatment period) focused on demonstrating
improvement inACQ scores and lung function but limited analysisof other end points, such as exacerbations, to an exploratorymanner. Moreover, the inhibition of one inflammatory pathwaymight not be sufficient to improve clinical outcomes in patientswith moderate-to-severe inadequately controlled asthma. Thesample size of this study, 397 total patients with approximately79 patients per arm, was of adequate power (based on theminimally important difference) to detect meaningful changes inACQ scores and FEV1. The population studied had characteristicsconsistent with moderate-to-severe asthma, and a low dropout rateand a high compliance rate (investigational product administrationand study assessments) were observed. The exposure data com-bined with previous pharmacodynamic data indicated that thedoses used effectively inhibited the DP and CRTH2 receptors inthe blood.11,13 The data showed a consistent lack of response ob-served for all the efficacy end points in the overall populationand subpopulations that were evaluated. The placebo response ob-served in this study is comparable with that of recently publishedstudieswithmAbs.21,22 Improvements frombaseline in patients re-ceiving AMG 853 as add-on therapy to ICSs were not statisticallysuperior to those achieved with ICS monotherapy (ie, placebo) inall predefined primary and secondary efficacy end points.Althoughthe PGD2 pathway has been implicated in the pathogenesis andmaintenance of asthma, on the basis of these results, with theknown properties of AMG 853, it does not appear that blockadeof PGD2 receptors (DP and CRTH2) provides clinically relevantimprovements in asthma-related outcomes as add-on therapy toICSs in patients with inadequately controlled moderate-to-severeasthma. Given our findings, it will be of interest to learn of experi-ences with other CRTH2 dual antagonists in clinical studies.
We thank Chris A. Kirk and Rick Davis of Complete Healthcare Commu-
nications (Chadds Ford, Pa), whoseworkwas funded byAmgen, for providing
assistance in the drafting of this manuscript.
Clinical implications: AMG 853 did not improve asthma symp-tom management as add-on therapy to ICSs in patients withinadequately controlled moderate-to-severe asthma.
REFERENCES
1. Kaiko GE, Foster PS. New insights into the generation of Th2 immunity and
potential therapeutic targets for the treatment of asthma. Curr Opin Allergy Clin
Immunol 2011;11:39-45.

J ALLERGY CLIN IMMUNOL
VOLUME 131, NUMBER 2
BUSSE ET AL 345
2. Matsuoka T, Hirata M, Tanaka H, Takahashi Y, Murata T, Kabashima K, et al.
Prostaglandin D2 as a mediator of allergic asthma. Science 2000;287:2013-7.
3. Hirai H, Tanaka K, Yoshie O, Ogawa K, Kenmotsu K, Takamori Y, et al. Prostaglan-
din D2 selectively induces chemotaxis in T helper type 2 cells, eosinophils, and
basophils via seven-transmembrane receptor CRTH2. J Exp Med 2001;193:255-61.
4. Lewis RA, Soter NA, Diamond PT, Austen KF, Oates JA, Roberts LJ 2nd. Prosta-
glandin D2 generation after activation of rat and human mast cells with anti-IgE.
J Immunol 1982;129:1627-31.
5. Chen JJ, Budelsky AL. Prostaglandin D(2) Receptor CRTH2 Antagonists for the
Treatment of Inflammatory Diseases. Prog Med Chem 2011;50:49-107.
6. Arimura A, Yasui K, Kishino J, Asanuma F, Hasegawa H, Kakudo S, et al. Preven-
tion of allergic inflammation by a novel prostaglandin receptor antagonist, S-5751.
J Pharmacol Exp Ther 2001;298:411-9.
7. Shichijo M, Arimura A, Hirano Y, Yasui K, Suzuki N, Deguchi M, et al. A pros-
taglandin D2 receptor antagonist modifies experimental asthma in sheep. Clin Exp
Allergy 2009;39:1404-14.
8. Lukacs NW, Berlin AA, Franz-Bacon K, Sasik R, Sprague LJ, Ly TW, et al.
CRTH2 antagonism significantly ameliorates airway hyperreactivity and downre-
gulates inflammation-induced genes in a mouse model of airway inflammation.
Am J Physiol Lung Cell Mol Physiol 2008;295:L767-79.
9. Gervais FG, Sawyer N, Stocco R, Hamel M, Krawczyk C, Sillaots S, et al. Phar-
macological characterization of MK-7246, a potent and selective CRTH2 (chemo-
attractant receptor-homologous molecule expressed on T-helper type 2 cells)
antagonist. Mol Pharmacol 2011;79:69-76.
10. Barnes N, Pavord I, Chuchalin A, Bell J, Hunter M, Lewis T, et al. A randomized,
double-blind, placebo-controlled study of the CRTH2 antagonist OC000459 in
moderate persistent asthma. Clin Exp Allergy 2012;42:38-48.
11. Banfield C, Parnes J, Emery M, Ni L, Zhang N, Hodsman P. Single-dose, first-in-
human study of AMG 853: Pharmacokinetics, pharmacodynamics, and safety in
healthy adults [abstract]. J Allergy Clin Immunol 2010;125:AB66.
12. Liu J, Li A-R, Wang Y, Johnson MG, Su Y, Shen W, et al. Discovery of AMG 853,
a CRTH2 and DP dual antagonist. ACS Med Chem Lett 2011;2:326-30.
13. Parnes J, Banfield C, Chow V, Zhang N, Hodsman P. Multiple-dose study of
AMG 853 in healthy adults: safety and pharmacokinetics [P1165]. Paper presented
at: European Respiratory Society Annual Congress; September 18-22, 2010;
Barcelona, Spain.
14. Fitzpatrick FA, Wynalda MA. Albumin-catalyzed metabolism of prostaglandin D2.
Identification of products formed in vitro. J Biol Chem 1983;258:11713-8.
15. Roberts LJ 2nd, Sweetman BJ. Metabolic fate of endogenously synthesized pros-
taglandin D2 in a human female with mastocytosis. Prostaglandins 1985;30:
383-400.
16. Juniper EF, Bousquet J, Abetz L, Bateman ED, Committee G. Identifying ‘‘well-
controlled’’ and ‘‘not well-controlled’’ asthma using the Asthma Control Question-
naire. Respir Med 2006;100:616-21.
17. Juniper EF, O’Byrne PM, Guyatt GH, Ferrie PJ, King DR. Development and val-
idation of a questionnaire to measure asthma control. Eur Respir J 1999;14:902-7.
18. Reddel HK, Taylor DR, Bateman ED, Boulet LP, Boushey HA, Busse WW, et al.
An official American Thoracic Society/European Respiratory Society statement:
asthma control and exacerbations: standardizing endpoints for clinical asthma trials
and clinical practice. Am J Respir Crit Care Med 2009;180:59-99.
19. Juniper EF, Buist AS, Cox FM, Ferrie PJ, King DR. Validation of a standardized
version of the Asthma Quality of Life Questionnaire. Chest 1999;115:1265-70.
20. National Asthma Education and Prevention Program. Expert panel report 3: guide-
lines for the diagnosis and management of asthma. National Heart Lung and Blood
Institute. Available at: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm.
Accessed November 21, 2011.
21. Corren J, Busse W, Meltzer EO, Mansfield L, Bensch G, Fahrenholz J, et al. A ran-
domized, controlled, phase 2 study of AMG 317, an IL-4Ralpha antagonist, in pa-
tients with asthma. Am J Respir Crit Care Med 2010;181:788-96.
22. Corren J, Lemanske RF, Hanania NA, Korenblat PE, Parsey MV, Arron JR, et al.
Lebrikizumab treatment in adults with asthma. N Engl J Med 2011;365:1088-98.
23. Philip G, van Adelsberg J, Loeys T, Liu N, Wong P, Lai E, et al. Clinical studies of
the DP1 antagonist laropiprant in asthma and allergic rhinitis. J Allergy Clin Im-
munol 2009;124:942-8, e1-9.
24. Singh D, Hunter M, Collins L, Perkins M, Pettipher R, Townsend E, et al. Inhibi-
tion of the inhaled allergen challenge response by the CRTH2 antagonist OC00459
in patients with asthma [abstract no. 371]. Paper presented at: European Respira-
tory Society Annual Congress; September 18-22, 2010; Barcelona, Spain.

![RoleofPGE inAsthmaandNonasthmatic EosinophilicBronchitis2) by COXs, and metabolism of prostaglandin H 2 to prostaglandin E 2 via prostaglandin E synthase [12]. There are three enzymes](https://img.dokumen.tips/doc/110x75/60d522031e41432a8f254505/roleofpge-inasthmaandnonasthmatic-eosinophilicbronchitis-2-by-coxs-and-metabolism.jpg)
![OBE022, an Oral and Selective Prostaglandin F Receptor Antagonist · specific prostaglandin synthases], and metabolism via pros-taglandin dehydrogenase enzymes. Prostaglandin E 2](https://img.dokumen.tips/doc/110x75/612431e6b1d2d8488c3d852e/obe022-an-oral-and-selective-prostaglandin-f-receptor-antagonist-specific-prostaglandin.jpg)


























