Embed Size (px)
Citation preview

605 Vol 314 No 10 PHYSICAL ACTIVI1Y MORTALITY AND LONGEVITY PAFFENBARGER ET AL
PHYSICAL ACTIVITY ALL-CAUSE MORTALITY AND WNGEVITY OF COLLEGE ALUMNI
RALPH S PAFFENBARGER JR MD DRPH ROBERT T HYDE MA ALVIN L WING MBA
AND CHUNG-CHENG HSIEH ScD
Abstract We examined the physical activity and other life-style characteristics of 16936 Harvard alumni aged 35 to 74 for relations to rates of mortality from all causes and for influences on length of life A total of 1413 alumni died during 12 to 16 years of follow-up (1962 to 1978) Exercise reported as walking stair climbing and sports play related inversely to total mortality primarily to death due to cardiovascular or respiratory causes Death rates declined steadily as energy expended on such activity inshycreased from less than 500 to 3500 kcal per week beyond which rates increased slightly Rates were one quarter to one third lower among alumni expending 2000 or more
I MPROVED nutrition reduced mortality from inshyfectious diseases and modification of some adshy
verse personal characteristics such as the cigarette habit are accepted as having extended human longevshyity The importance of adequate physical exercise to cardiovascular health is becoming appreciated yet there is a longstanding debate about whether exercise also extends longevityI-6 To assess influences on length of life we examined the relations of life-style elements to mortality from all causes among 16936 Harvard alumni aged 35 to 74 who were initially free of clinically recognized coronary heart disease Earshylier studies in this population l1ad shown that the risk of coronary heart disease was affected signifishycantly by histories of hypertension cigarette smokshying overweight for height and habitual physical inshyactivity18 We then studied whether exercise could be shown to delay all-cause mortality in this populashytion The thesis that exercise does in fact add extra years to life is examined in this continuing study of ways of living and health among Harvard Colshylege alumni
METHODS
Men who entered college in the period 1916 to 1950 were studied Their personal and life-style characteristics (including exercise habits) during their college and post-college days were recorded with follow-up data on influences on mortality and estimated length of life Over three quarters of the known surviving alumni respondshyed to mailed questionnaires that asked about specific physicianshydiagnosed diseases physical activities cigarette smoking habits and parental diseases and death Weekly updating of death lists by the Harvard Alumni Office provided the means to obtain death certificates and identify underlying causes of death Fewer than I percent of alumni were lost to follow-up without death notishyfica tion 78
From the Department of Family Community and Preventive Medicine Stanmiddot ford University School of Medicine Stanford and the Department of Epidemiol ogy Harvard University School of Public Health Boston Address reprint reo quests to Dr Paffenbarger at the Stanford University School of Medicine Department of Family Community and Preventive Medicine Health Research and Policy Bldg Stanford CA 94305
Supported by a grant (HL 24133) from the National Heart Lung and Blood Institute and by the Marathon Oil Foundation the G Unger Vetlesen Foundation and the El du Pont de Nemours Company
kcal during exercise per week than among less active men With or without consideration of hypertension cigashyrette smoking extremes or gains in body weight or early parental death alumni mortality rates were significantly lower among the physically active Relative risks of death for individuals were highest among cigarette smokers and men with hypertension and attributable risks in the comshymunity were highest among smokers and sedentary men By the age of 80 the amount of additional life attributable to adequate exercise as compared with sedentariness was one to more than two years (N Engl J Med 1986 314 605-13)
Records of college physical examinations performed early in the freshman year and records of participation in intercollegiate (varsishyty) sports during years of undergraduate attendance provided measures of students blood pressure levels body weight and height and athleticism These records were examined in conjuncshytion with data on post-college physical activities other patterns of living and histories of personal health and parental death obtained by return-mail questionnaires in 1962 and 1966 Data on physical energy expenditure and personal characteristics so gathered were related to time and cause of death as reported on official death certificates between 1962 and 1978 Man-years of observation for level of energy expenditure and other characteristics under study were recorded according to single years of age for the follow-up interval of 12 to 16 years
A total of 782 alumni who had initially reported physician-diagshynosed coronary heart disease were excluded from he starting popushylation to reduce any selective bias toward low-level activity as a result of their disease A separate analysis (not reported here) showed little difference between the exercise habits of this group and the other alumni but mortality rates were highrr among the patients with coronary heart disease despite a saving effect of modshyerate exerCise9 On the whole the results of the present study would not be altered appreciably if the group with coronary heart disease had been retained A smaller group of men with a diagnosis of cancer stroke or other ailments was not excluded from the starting population Any influences of disease on their physical activity patshyterns or vice versa are inherent in the all-cause mortality findings reported here
Alumni aged 35 to 74 years had reported by questionnaire how many city blocks they walked how many stairs they climbed and the types of sports they participated in and time they spent on them each week 10 After adjustment for seasonal variation and estimates of overreporting and underreporting the energy used for these acshytivities was expressed in kilocalories per week Walking seven city blocks (094 km or 7t2 mil was rated as 56 kcal and climbing 70 stairs was rated as 28 kcal sports were classified as light (5 kcal per minute) vigorous (10 kcal per minute) or mixed (75 kcal per minute) A physical-activity index was computed as an estimate of energy expended in walking climbing stairs playing sports yard work and so forth 11 When divided into ranges of less than 500 500 to 1999 and 2000 or more kcal per week index increments represhysented 15 percent 46 percent and 39 percent of the man-years of observation respectively These measures were regarded as indicashytors rather than absolute totals of energy expenditure largely in leisure time
In studying the influence of other personal characteristics as conshytinuous variables (eg cigarette smoking body weight in relation to height and weight change since college) break points were chosen to provide three levels or categories that might reveal any gradient risk of death Mortality rates were computed for the follow-up intershyval by the indirect method using 213716 man-years of observation for the total population as standard with adjustment for age differshy
606 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
ences by five-yeargroups Interrelations of paired characteristics (eg physical-activity index and cigarette smoking habit) were then examined by cross-tabulation of their three-level categories in which all-cause mortality rates were computed In analyses of trends of mortality using these cross-tabulations the influence of one characteristic was assessed with the influence of age and the other characteristic held constant The Mantel extension of the Mantel-Haenszel test was used in determining the significance of linear trends 12
Three groups were established for blood-pressure status normoshytensive alumni whose systolic blood pressure level during college was less than 130 mm Hg (69 percent of man-years) normotensive alumni whose systolic level during college was 130 or more mm Hg (22 percent) and alumni with physician-diagnosed hypertension (9 percent)
The three categories for cigarette smoking were nonsmokers (62 percent of man-years) men who smoked less than one pack a day (II percent) and men who smoked one or more packs a day (27 percent)
Body weight for height was expressed as body-mass index comshyputed from English units (1000 X weight in pounds divided by height in inches squared) Alumni were classified into three levels those with an index of 36 or more - who were 20 percent or more above their ideal weight according to 1959 Metropolitan Life Insurance Company standards (37 percent of man-years) those with an index of 34 to 35 - men who were 10 to 19 percent overshyweight (25 percent of man-years) and those with a body-mass index of less than 34 - men less than 10 percent overweight (38 percent of man-years) Net weight change (almost always a gain) after the college physical examination was middotcomputedmiddot in units of body-mass index an increase of 5 or more units represented a gain of 115 or more kg or 25 or more Ib (40 percent of man-years) an increase of 3 to 4 units a gain of 7 to 114 kg or 15 to 24 Ib (25 percent) and an increase of less than 3 units a gain of less than 7 kg or less than 15 Ib (35 percent)
The three categories for history of parental death before the age of 65 contained alumni without such a history (67 percent of manshyyears) those reporting that one parent was dead (29 percent) and those reporting that both parents were dead (4 percent)
Student participation in college athletics was established in three levels varsity sports play (21 percent of man-years) intramural sports play for five or more hours per week (37 percent) and intra~ mural play for less than five hours per week or not at all (42 percent)
Mortality rates per 10000 man-years of observation were used to compute relative risks of death the base representing men whose characteristic or level carried the highest risk (Tables I and 2 and the figures) or the lower risk (Table 3) Attributable risks (percentages) were computed as clinical estimates (I - IIrelative risk) x 100 and as community estimates
(prevalence of characteristic) X (rdative risk - I) X 100
I + (prevalence of characteristic) X (relative risk I)
Multivariate analyses for estimating the relative risks of death associated with the three levels of physical-activity index (less than 500500 to 1999 and 2000 or more kcal per week) were based on Coxs proportional-hazards models 13 Estimated adjusted probabilshyities of survival (Table 5) were based on a fitted proportionalshyhazards model If All probability values cited were determined with two-tailed tests
RESULTS
Of the 16936 alumni aged 35 to 74 who returned questionnaires in 1962 or 1966 reporting their health status exercise habits and other personal and lifeshystyle characteristics 1413 (8 percent) died from some cause between the ages of 35 and 80 in the 213716 man-years of follow-up ending in 1978 Underlying causes of death were cardiovascular disease in 45 pershy
cent cancer in 32 percent other natural causes in 13 percent and trauma in 10 percent
Table 1 shows age-adjusted rates of death from all causes during the 16-year follow-up period (1962 through 1978) according to physical activity (walkshying stair climbing and sports play) and the combinashytionphysical-activity index Relative risks of death are also shown
A small gradient effect of walking led to a 21 pershycent lower risk of death as distance was increased from less than 3 miles to 9 or more miles per week The pattern of benefit from stair climbing was less consisshytent possibly because of misclassifications due to ershyroneous reporting at the higher levels of stair countshying since some respondents (as requested) reported flights of stairs climbed and others (mistakenly) gave number of stairs Light sports did not influence the incidence of coronary heart disease78 but all-cause mortality rates were lowered by increased hours of play somewhat more than by walking For vigorous sports which tended to avert coronary heart disease there was also a significant inverse relation to all-cause mortality but with a reversing trend at three or more hours of play much as in the stair-climbing data This shift may also have been due to exaggerations in reshyporting or perhaps to actual increased hazards associshyated with vigorous activities Likewise such influences may account for the upswing at the highest level of physical activity (3500 or more kcal per week) Aside from that tendency the risk of death became progresshysively lower as the physical-activity level increased from below 500 to about 3500 kcal per week - the level at which the relative risk was less than half that associated with the least activity At an index of 3500 or more kcal per week the all-cause death rates beshycame relatively stable
Men with an index of less than 2000 kcal per week had a 38 percent greater risk of death in the 12- to 16shyyear follow-up period than men with a higher index Or in a positive sense men whose weekly energy outshyput in walking climbing stairs and playing sports totaled 2000 or more kcal per week had a 28 percent lower aU-cause death rate than less active men When the mortality data were analyzed for successive intershyvals of two five and another five years of follow-up during 1962 to 1974 or 1966 to 1978 the same trends were observed in each interval as over the total period The corresponding higher death rates for sedentary as compared with active men were 68 54 and 12 pershycent This finding supports the view that the inverse relation of physical activity to mortality was derived from a beneficial influence of exercise on survival and not merely from a selective effect of alumni who were or became physically inactive because they were chronically ill or had premonitory symptoms of disease
In all age groups there was a consistent trend toshyward a lower death rate as physical activity increased from less than 500 to 2000 or more kcal per week
Vol 314 No 10 PHYSICAL ACTIVITY MORTALITY AND LONGEVITY -PAFFENBARGER ET AL 607
Table 1 Age-Adjusted Rates and Relative Risks of Death (frorTl All Causes) among but was strongest and most signifishy16936 Harvard Alumni 1962 to 1978 According to Measures of Physical Activity cant in relation to cardiovascular
and respiratory diseases 7 PHYSICAL DEATHS PER RELATIVE
ACT1VITY PREVALENCE No OF 10000 RISK OF P OF In Table 2 age-adjusted all-cause (WEEKLY) (MANYEAlltS ) DEATHS MANYEARS DEATH TREND death rates are tabulated according Miles walked to alumni characteristics commonly
lt3 260 408 781 100 associated with an increased risk 3--8 442 573 667 085 00009 9 298 392 618 079 hypertension cigarette smoking
Stairs climbed extremes of weight in relation to lt350 344 545 740 100 height patterns of weight change 350-1049 500 627 627 085 00646 and early parental death Hypershy1050 156 200 680 092
tensive men had nearly twice theLight sports played (hr) risk of normotensive men whereas
None 770 837 812 100 the mortality rates among normoshy1-2 62 61 614 076 lt00001
tensive men differed only slightly 3 168 145 567 070 according to whether their systolic Vigorous sports
played (hr)t blood pressure during college was None 614 1046 754 100 below 130 mm Hg or 130 mm Hg1-2 184 166 491 065 lt00001 3 202 187 559 074 or higher Relative risks of death
Physicalmiddot activity among cigarette smokers were twice index (kcal)l those among nonsmokers
lt500 154 308 937 1m Alumni with a body-mass index
500-999 209 322 Qn 1000-1499 152 202 ~~~ 752 Qn 1m below 32 and those with an index of 1500-1999 104 121 593 Q~ lt00001 38 or higher contributed 17 and 18 2000-2499 lU 89
577 o~ percent of the man-years of obsershy2500-2999 69 62 485 O~544 Q on3000-3499 50 42 427 vation respectively Although the
3500 181 203 584 Q~ overall trend of association beshy-Exels subjecls who played vigorous sports tWilh or without light sportS play tween body-mass index and total tSummation of above measures equated to kilocalories + mortali ty was not significan t the
two thirds of alumni with indexes beiween the two extremes had a
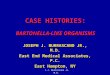
(Fig I) The older alumni at the highest activity level lower risk The higher rates for their classmates with had half the risk of those at the low end the relative extremes of physique suggest that overlyfat men may risks were 051 for active men aged 70 to 84 and 053 succurpb to cardiovascular disease and the very unshyfor those aged 60 to 69 Younger alumni at the highest derweight possibly to wasting diseases such as cancer activity level had 25 percent less risk than those at the Of further interest the association of mortality with lowest level the relative risk was 064 for men aged 50 a low net gain in body-mass inqex was considerable to 59 and 079 for men aged 35 to 49 As would be Alumni with the lowest net gain since college had a 29 expected death rates were comparatively low in the percent higher risk of death than their classmates who younger age groups at all levels of physical activity In gained the most This trend represents departure from addition the onset of cancer or other terminal disease findings for coronary heart disease 78 The high risk of among the older men could have led some to shift into the group with the lowest net gain may reflect the low-activity life styles introducing an element of seshy wasting effects of disease the influence of cigarette lection manifested by the steeper slope in the lowshy smoking or some inherited insufficiency activity segments of the two upper curves in Figure 1 Hereditary or familial influences may help to exshyAside from this the general trend toward a lower plain why alumni whose parents had both died before death rate with increased physical activity was uriishy the age of 65 had a 29 percent higher risk of death form and significant than alumni whose parents had both lived to age
To allow for self-selection affecting exercise choice 65 or older (ie by alumni choosing a sedentary life because of ill The data in Table 2 do not consider physical activshyhealth) a11-cause and caQse-specific death rates from ity which has been shown to counteract the risks of cardiovascular or respiratory diseases cancer other coronary heart disease that are associated with most natural causes and trauma were examined along this of the characteristics listed therein 78 To refine and same gradient of physical activity Rates were adjustshy extend the above observations and assess the conshyed for differences in age cigarette smoking hypertenshy founding influences of any of those characteristics sion a low net body weight gain since college and and physical exercise the series of stereograms in Figshyearly parental death - personal characteristics affectshy ure 2 show relative risks of death from any cause ing all-cause mortality (see below) A decline in death according to levels of physicalactivity and selected rates with increasing activity was seen for each cause characteristics
608 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
All-Cause Oeath Rates per 10000 Man-Years
Observation 500rl----------------------------~
400
300
200
100
80
60
40
20
bull Relative Risk s above PIOI Po
100
~72 Inls
100 bull ~1Age
63 bull 70-84
bull~360-69
100 86
-------- 64
----50-59
100 97---shylt500 500-1999 2000+
Physical Activity in Kilocalories per Week
Figure 1 Age-Specific Mortality from All Causes among 16936 Harvard Alumni in 1962 to 1978 According to Physical-Activity
LevelS
In each stereogram mortality trends become evishydent as the influence of each characteristic is assessed with the influences of age and the paired characteristic held constant Relative-risk estimates were derived from the death rate in the presumed highest risk category represented by the back corner block which was assigned a relative risk of l00 Respective relative risks are shown by the heights of the other blocks Death rates per 10000 man-years are shown at the tops of the blocks and the numbers of decedents in the nine categories are tabulated in an accompanying diamond
Figure 2A assesses the influences of the physical activity of alumni and the blood pressure of students or alumni on the risk of death from all causes Throughout the stereoshygram death risks are reduced as physical activity is increased (from lt500 to 500-1999 to ~2000 kcal per week) and the drop in risk is proportionately greater with inshycreased exercise among the hypershytensive alumni Alumni with physishycian-diagnosed hypertension had about twice the risk of death of
normotensive alumni with the difshyference declining as exercise inshycreased Mortality rates were someshy
what lower among the normotensive alumni whose systolic bloqd pressure during college was below 130 mm Hg than for those with higher readings as stushydents The initial data on hypertension and exercise were collected in 1962 or 1966 before modern stepwise methods of blood-pressure management came into use Hence there is no good reason to suppose that the apparent benefit of exercise among the men with hyshypertension was due instead to differences in diagnosis of hypertension or to drug or dietary therapy for blood-pressure controL 15 The hypertensive alumni who exercised lowered their risk of death even though they remained hypertensive~
Figure 2B shows a steady reduction in the risk of death as exercise increased and cigarette smoking deshycreased The risk among sedentary heavy smokers was reduced by two thirds among the most active nonshysmokers At each level of exercise a reduction in smoking from one or more packs down to none cut the risk of death in half Cigaxette smoking and exercise had strong opposite influences on the risk of death from all causes and the figure has dual implications for behavior modification
In Figure 2C the highest mortality is seen among the alumni who were least active and had the lowest body-mass index At ariy level of body-mass index the risk of death decreased as physical activity increased from less than 500 to 2000 or more kcal per week However the relation of body mass to the risk of
Table 2 Age-Adjusted Rates and Relative Risks ofDeath (from All Causes) among 16936 HarVard Alumni 1962 to 1978 According to Selected Characteristics
of Alumni
DEATHS PER RELATIVE
ALUMNUS PREVALENCE No OF 10000 RISK OF P OF
CHAMCfERISTle (MANmiddot YEARS ) DEATHS MAN-YEARS DEATH TREND
Blood-pressure status Hypertension Normotension 130 Normotension lt 130t
Cigarette smoking (packsday)
1 ltI None
BOdy-mass indexl 31 32-33 34-35 36-37 38
Gain in body-mass index since college
lt3 3 4 5 6
Parents dead before age 65 Both One Neither
94 283 1173 100 214 275 680 058 lt00001 692 714 594 051
272 480 1104 100 110 129 644 058 lt00001 618 648 547 050
165 259 798 100 210 259 629 079 253 331 653 082 06308 190 236 608 076 182 286 761 095
350 432 8Ll 100 123 140 677 084 126 122 572 071 lt00001 ILl 132 623 077 290 401 626 077
41 87 808 100 292 491 773 096 lt00001 667 835 626 077
Nonnotensicin with student systolic blood pressure ~ 130 mm Hg
tNonnotension with student systolic blood pressure lt130 mm Hg
~Weight in potnds divided by the square of height in inches times 1000
609
-0$00_
- ~~-1~O
Vol 314- No IO PHYSICAL ACTIVITY MORTALITY AND LONGEVITY - PAFFENBARGER ET AL
Figure 2 Relative Risks (RR) of Death from All Causes among 16936 Harvard Alumni in 1962 to 1978 According to Post-College Physical-Activity Levels and (A) Alumnus and Student Blood-Pressure Status (B) Alumnus Cigarette Smoking (C) Alumnus Body Weight for Height (D) Net Change in Body Weight since College (E) History of Early Parental Death and (F) Participation in
College Sports Blocks designate the relative risk based on age-adjusted death rates (numbers at top of blocks) per 10000 man-years of observation Death rates in the back corner blocks establish the relative risk of 100 Numbers of deaths are given in a corresponding key below each stereogram P values are based on trends of rates for one characteristic adjusted for differences in age and the paired characteristic
death was uneven and the trend was not significant when age and physical activity index were held conshystant There is perhaps some hint that the risk among the most active alumni tended to increase at both the high and low extremes of body-mass index Again as noted in the discussion of Table 2 the high risk for sedentary men with a low body-mass index may inshyvolve a wasting disease such as cancer whereas men with a high body-mass index may invite death from cardiovascular disease
Table 2 also shows that men with the least net gain in body-mass index after their physical examination in college had a greater risk of death than those who gained more This is also evident in Figure 2D where mortality can be seen to decline with an increasing net gain in body mass-index and also with increasing curshyrent physical activity Inactive status with a low weight gain may signify illness whereas the gain in body-mass index among the more active men may reflect healthy muscularity - ie body leanness rathshyer than body fat
As shown in Figure 2E the death of one or both parents before the age of 65 was related to an inshycreased risk of death among the alumni but the risk was lower among the physically active Early loss of parents may suggest a hereditary risk but it does not appear to influence the risk of death as strongly as
does lack of exercise Whether or not the two factors are interrelated both have significant effects on morshytality and adequate contemporary exercise may virtushyally offset the influence of early parental death
The pattern of relative risks in Figure 2F shows that the rate of death from any cause was reduced with increased physical activity by alumni but that the sports-activity level in their student days did not have a similar effect on subsequent mortality Former varsishyty athletes who exercised at less than 500 or at 2000 or more kcal per week in their post-college years had higher death rates (93 and 73 per 10000 man-years of observation respectively) than those who reported continuing moderate exercise at 500 to 1999 kcal per week (61 per 10000 man-years) The most active group of former varsity players with a higher mortalshyity includes those who died from cancer or cardiovasshycularcauses Although in this pattern former varsity athletes seem to have had a higher risk than their less athletic classmates the chart overall shows a consisshytent pattern of benefit from habitual exercise by alumshyni Evidently inheritance of a sturdy constitution (as implied by varsity athletic status) is less important to longevity than continuation of adequate life-time exerCIse
Each stereogram in Figure 2 shows that the physical activity of alumni had an independent and significant
A B
~ 00 ~
075 shy 01gt shy
0$0 cSO shy
015 --
Alumrul Physlcol etlyU
ftld tKcIWbullbulltt ~~I~ -0001 fI 0001
D E
ARA~
100 100
07S shy075
aso 00
~oaI Oili
000 000 shy
SCtdy fn 11IwJI Physical ActivUy -- Gain Sinc Collaga PhyiealAcUvHy
thdu KeIWutt IweighOHighI2 nd KuilWbullbullk) 0001 ~ 0001 p 0001
AlutlUHJ
c
100 --- shy 015
oso -
025
Alumnut Cigarttbullbull Per Oy
p OOOt
F
AR
100
05
OliO gt
01$ ~
Au Phyak1 Activity
Indbullbull KcaUWbullbullle1 0001
610 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
inverse relation to mortality Moreover adequate exshyercise enhanced the mortality reduction associated with favorable levels of the other post-college characshyteristics studied
Table 3 shows relative and attributable risks of death from any cause which were derived from a multivariate analysis and computed for the presence versus the absence of each adverse characteristic with adjustment for the differences in age and each of the other characteristics listed 13 The relative risk of 131 associated with a sedentary life style signifies that men expending fewer than 2000 kcal per week had a 31 percent higher risk of death than more active men Likewise men with physician-diagnosed hypertension had a 73 percent higher risk than normotensive men and cigarette smokers had a 76 percent higher risk than nonsmokers Men who had a net weight gain of less than 7 kg (IS Ib) after college were at a 33 percent greater risk than men who gained more The alumni who had lost one or both patients before the age of 65 had a 15 percent higher risk of death than their classshymates whose parents had survived to age 65 or older The five characteristics assessed in the table or the basic mechanisms of causation they represent conshytribute independently to the risk of death from all causes
The clinical attributable risks listed in Table 3 are estimates of potential percentage reductions in the risk of death for persons who exchange the adverse characteristic for a more healthful characteristic Sedshyentary men who become more active might reduce their risk of d~ath by 24 percent If hypertensive men could obtain normal blood pressure they would have 42 percent less risk reformed cigarette smokers 43 percent less Men whose net weight gain since college was below 7 kg might have had a 25 percent lower risk of death if they had gained more If men who lost one or both parents early had had parents living to age 65 or older their own risk of death might have been 13 percent less The clinical percentage estimates in Tashyble 3 are not additive
The community attributable risks in Table 3 are
estimates that take prevalence into account They inshydicate what percentage of risk might be spared in a community or population if the adverse characterisshytics listed were converted to more favorable characshyteristics The risk of death might be reduced by 16 percent in the alumni population if every man had exercised at 2000 or more kcal per week Abolition of hypertension might cut the community death rate anshyother 6 percent total abstinence from cigarettes anshyother 23 percent a greater net weight gain 10 percent more and survival of both parents to age 65 or older another 5 percent These estimates though hypothetishycal are additive so thlttt if all five adverse characterisshytics were eliminated the total risk of death in the community of alumni might be cut by more than half - ie there might have been 60 percent fewer deaths during the study period (1962 to 1978) or a loss of only 551 alumni instead of 1413
Relative and attributable risks of death from carshydiovascular disease in association with similar adverse characteristics (sedentariness hypertension smoking overweight and parental coronary heart disease) among the alumni were of the same general order of magnishytude as risks of all-cause mortality After allowance for age and each other adverse characteristic sedentary alumni had a 31 percent higher risk of cardiovascular mortality than more physically active men hypertensive men had a 118 percent greater risk than normotensive men cigarette smokers had an 84 percen greater risk than nonsmokers heavier men had an 18 percent higher risk than leaner men and alumni with a parenshytal history of coronary heart disease had a 33 percent higher risk of dying from cardiovascular disease than classmates whose parents were free of coronary heart disease The attributable-risk estimates (community) corresponding to these same characteristics were 16 9 25 6 and II percent respectively In combination they indicated that there might have been 67 percent fewer deaths from cardiovascular disease during the study period in the absence of all five characteristics or a loss of only 196 alumni instead of the 640 who died from underlying cardiovascular disease
As shown in Table 4 the mortalshyity and survival experience of the
Table 3 Relative and Attributable Risks of Death (from All Causes) among 16936 Harvard alumni during the 16-year Harvard Alumni 1962 to 1978 According to Selected Adverse Characteristics follow-up period were used to deshy
velop estimates of years of added CLINICAL COMMUNITY
life gained (up to age 80) from anALUMNUS PREVALENCE RELATIVE RISK AlTRIBJTABLE A lTlUBUTABLE
CHARACTERISTIC (MAN-YEAlIS ) OF DEATHt P VALUE ~K( ~K() active life style rather than an inacshySedentary life stylet 620 131 (115-149) 00001 236 161 tive life style The results are tabushyHypertensionsect 94 1 73 (14S-201) lt00001 421 64 lated for five-year age groups at the Cigarette smoking~ 382 176 (156-199) lt00001 432 225 start of follow-up and selected measshyLow net weight gainll 351 133 (117-151) 00001 246 103 ures of physical activity The data Early parental death 333 U5 (102-130) 00248 131 48 are shown with and without adshybullAdjusted for differences in age and each of the other characteristics listed
tFigures in parentheses are 95 percent confidence intervals
Energy expenditure of lt2000 kcal per week in walking climbing stairs and playing sports
sectPhysician-dignosed
Any amount
IINet gain in body-mass index of lt3 units since college ie bull nO more than 7 leg (15 Ib)
bull One or both parents dead before he age of 65
justment for differences in bloodshypressure status cigarette use net gain in body-mass index and pashyrental death The first two columns under physical-activity show the crude and adjusted estimated years
611 VoL 314 NoO PHYSICAL ACTIVITY MORTALITY AND LONGEVITY PAFFENBARGER ET AL
Table 4 Added life from an Active life Style in Men Jp to the Age of 80 Estimated from Harvard Alumni Mortality 1962 to 1978
PHYSICAL-ACTIVITY INDEXmiddot VIGOItOUS SPOIlTS ILAY
AGE AT 2000 VS 2000 VS 2000 VS PusENT vs ENTIlY lt500 lt2000 500-1999 ABSENT
(n) CltUDE AllJUSTEot CRUDE AllJUSTEOt CRUDE ADJUSTEOt CRUOE ADJUSTEot
esrimaJed no of years gained
35-39 264 251 166 150 126 107 166 155 4)-44 248 234 146 139 104 099 154 145 45-49 232 20 24 110 080 067 138 123 50-54 237 211 135 120 093 081 140 132 55-59 225 202 127 113 087 075 125 121 60-64 198 175 104 093 065 057 100 095 65-69 164 135 082 067 048 036 070 055 70-74 094 072 057 044 042 middot031 011 -011 75-79 035 042 029 030 026 024 001
35-79i 233 215 138 125 099 086 137 128
Kilocalories experuled per week in walking climbing stairs and plying sports
t Adjusted for differences in blood-pIeS stalUs cigarette smoking net gain in body-mass index since college and age of parental death
lWeighted vgbull
of survival gained by men expending 2000 or more kcal per week on exercise as compared with those expending less than 500 kcal per week The latter group might be considered likely to include most men who had selectively reduced their exercise levels beshycause of disease or premonitory symptoms As would be expected the survival difference (or number of years gained) was greatest between the extremes for levels of activity The third and fourth columns show the estimated results when all ~lumni are inshycluded with a single break point at 2000 kcal per week and the differences are still consistent though smaller In the fifth and sixth columns the group with the lowest activity (less than 500 kcal per week) is omitted yet the benefit of exercise is still evident
The data in the seventh and eighth columns showshying the survival advantages associated with vigorous sports parallel those in the third and fourth columns except in the age groups 65 and older in which indulshygence in vigorous sports is less likely In addition parshyticipation in vigorous sports would be expected to be most common among alumni expending 2000 or more kcal per week and this likely possibility may well acshycount for some of the contrast noted earlier regarding the first two columns in Table 4 if participating in vigorous sports is considered to enhance survival more than a high activity level In addition the influence of vigorous sports would probably be split in the fifth and sixth columns and so dampen the differences listed there as can be seen In view of these consistent patshyterns the data in Table 4 support the hypothesis that survival and hence longevity among the Harvard alumni has been influenced to an appreciable degree by both the total amount and the intensity of habitual physical activity engaged in throughout adult life The bottom line of Table 4 presents weighted avershy~ges for years gained up to the age of 80 as a result of Increased physical activity between the ages of 35 and
79 The survival estimates given in the table or othershywise calculated would vary depending on the definishytions or standards of physical activity employed in the analysis
Another assessment of the influence of physical acshytivity on longevity is shown in Table 5 in which the survival of active and sedentary alumni up to the age of 80 is estimated for five-year age groups after adshyjustment for differences in hypertension smoking low weight gain and early parental death Weigllted avershyages for the total age range are also shown For both active and sedentary men the percentage predicted to reach age 80 increases somewhat with age perhaps becausethe younger groups have yet to escape hazshyards of mortality that the older men have already avoided whereas the latter need to survive for fewer years to reach the age of 80 Nevertheless the physshyically active men had a continuing 10 percent advan-
Table 5 Proportions of Active and Sedentary Men Surviving to the Age of 80 Estimated from Harvard Alumni Mortality
1962 to 1978
AGE ATENny PHYSICALmiddotACTIVITY INOEX
(YR) 2000 lt2000
survivingt
35-39 682 578 40-44 685 582 45-49 690 592 50-54 699 598 55-59 711 610 60-64 730 634 65-69 764 676 70-74 824 746
75-79 918 850
35-791 697 598
Kilocalories expended per week in walking climbing tairs and playing sports
t Adjusted for differences in blood-pressure stalUs cigarette smoking net gain in body-mass mdex since college and age of parental death
jWeighted average
612 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
tage over the sedentary men until they reached the 65-to-69-year age bracket thereafter a tapering effect occurred because all the survivors from those groups had to reach the age of 80 within the follow-up period and hence their comparison was based on fewer years of mortality data It is possible too that contrasts between an active and sedentary life style were less marked in the older groups than in the younger groups Overall the table suggests a considerable gain in man-years of life for the habitually energetic alumshyni especially if any avoidable adverse characteristics such as cigarette smoking and obesity have been minimized
DISCUSSION
Survival is the result of a number of interacting influences (many hazardous in character or degree some beneficial in the same way) including physical activity and other life-style elements susceptible to opshytional adjustment Their combined effect determines whether increases in longevity are feasible or even deshysirable The findings reported here represent only a small part of the total picture but they suggest a proshytective effect of exercise against all-cause mortality in all age groups studied and therefore an indieationof additional years of life expectancy
The Harvard alumni may not be typical of the genshyeral population Their age-specific death rates from each major cause except suicide were roughly half the 1980 rates for white males in the United States (In contrast rates of self-destruction among the alumshyni 16- 18 were 50 percent higher than suicide rates in the general population) Yet the large alumni experience with delayed mortality for active men should imply increased life expectancy over that for sedentary men as the data demonstrate It is likely that some alumni increased their exercise reduced their smoking and received treatment for hypertension since the early 1960s when these characteristics were assessed Such changes would minimize the importance of these characteristics in the present findings The true force of the beneficial effects from physical activity nonshysmoking and control of hypertension would be even larger than that observed
Table 4 presents survival data in terms of definishytions of exercise that were necessarily limited by the design of the study to increases in kilocalories per week or to intensity as expressed by participation in vigorous sports The estimates of years gained reflect the experience of college alumni already recognized as long-lived whose economic status and behavior patterns differ from other populations in habitual physical exercise and other life-style elements Direct extrapolation to a general population should take these considerations into account
Since the data in Tables 4 and 5 represent only a portion of the total life experience of the study populashytion over time they may be viewed as a segment seen as through a window implying extensions that might
be estimated from the actual experience observed The differences in survival to the age of 80 between active and sedentary alumni may reflect a stage of optimal benefit from physical activity by the age of 65 and a rectangularization or converging trend may be estabshylished as the total life experience of the population of alumni approaches completion 19
Improvements in epidemiologic surveillance and medical management of such chronic disorders as hyshypertension abnormal blood lipid profiles and osteoshyporosis may defer mortality and extend survival However the effect of adequate physical exercise is partly independent of such influences and it countershyacts many adverse characteristics through metabolic and other processes20-25 Even when other procedures for health maintenance and disease prevention are deshyveloped to increase longevity the relevance of exercise is likely to remain
In studies of longevity the question arises whether the aging process is capable of modification but there is much uncertainty about the definitions of aging and of chronic disease Approaches to fend off disease or postpone aging are suggested or aging is regarded as an inexorable degenerative process that cannot be alshytered although perhaps chronic diseases may be avoided or deferred 2627 The present study considers chronic diseases but not the aging process itself
Extended follow-up of the Harvard alumni may reshyveal trends of aging or at least show at what stage of life the roles of exercise and10ther natural therapies become diminished The data in Tables 4 and 5 do offer some implications as a brief preliminary analysis of survival in various age and exercise groups In view of the data base and the consistency represented in the study it seems likely that the observed patterns are predictive
There is a widespread and longstanding popular belief that adequate physical exercise is necessary to preserve life and its desirable qualities into old age Discussions of this thesis date back to antiquity and have intensified in recent times 28
-40 The present study
adds new evidence to support this view
REFERENCES
1 Keys A Seven countries a multivariate analysis of death and coronary heart disease Cambridge Mass Harvard University Press 1980196-217276middot 8
2 Leon AS Blackburn H Physical inactivity In Kaplan NM Stamler I eds Prevention of coronary heart disease practical management of the risk factors Philadelphia WB Saunders 198386-97
3 Karvonen MJ Physical activity in work and leisure time in relation to cardiovascular diseases Ann Clin Res 1983 14SuppJ 34118-23
4 Morris IN Uses of epidemiology 3rd ed Edinburgh Churchill Livingshystone 1975163-5
5 Morris IN Kagan A Pattison DC Gardner MJlncidence and prediction of ischaemic heart-disease in London busmen Lancet 1966 2552-9
6 Paffenbarger RS Ir Brand RI Sholtz RI Jung DL Energy expenditure cigarette smoking and blood pressure level as related to death from specific diseases Am I Epidemiol 1978 10812-8
7 Paffenbarger RS Jr Hyde RT Wing AL Steinmetz CH A natural history of athleticism and cardiovascular health lAMA 1984 252491-5
8 Paffenbarger RS Ir Wing AL Hyde RT Physical activity as an index of heart attack risk in college alumni Am I Epidemiol 1978 108161shy75
613 Vol 314 No 10 PHYSICAL ACTIVITY MORTALITY AND LONGEVITY - PAFFENBARGER ET AL
9 Thomas GS Lee PR Franks P Paffenbarger RS Jr Exercise and health the evidence and the implications Cambridge Mass Oelgeschlager Gunn amp Hain 1981
10 Paffenbarger RS Jr Notkin J Krueger DE et al Chronic disease in former college students II Methods of study and observations on mortality from coronary heart disease Am J Public Health 1966 56962middot71
11 Passmore R Durnin JVGA Human energy expenditure Physiol Rev 1955 35801-40
12 Mantel N Chimiddotsquare tests with one degree of freedom extensions of the Mantel-Haenszel procedure J Am Stat Assoc 1963 58690middot700
13 Cox DR Regression models and life-tables J R Soc Biostat 1972 34187middot 220
14 Chang ImiddotM Gelman R Pagano M Corrected group prognostic curves and summary statistics J Chronic Dis 1982 35669-74
15 Paffenbarget RS Jr Wing AL Hyde RT Jung DL Physical activity and incidence of hypertension in college alumni Am J Epidemiol 1983 117245middot57
16 Paffenbarger RS Jr Asnes DP Chronic disease in former college students III Precursors of suicide in early and middle life Am J Public Health 1966 561026-36
17 Paffenbarger RS Jr Chronic disease in former college students VI Implicamiddot tiOlls for college health programs J Am College Health Assoc 1967 1651middot 5
IS Paffenbarger RS Jr King SH Wing AL Chronic disease in former college students IX Characteristics in youth that predispose to suicide and accidenshytal death in later life Am J Public Health 1969 5990()S
19 Fries IF Crapo LM Vitality and aging implications of the rectangular curve San Francisco WH Freeman 1981
20 Paffenbarger RS Jr Hyde RT Exercise as protection against heart attack N Engl J Med 1980 3021026-7
21 Wood PO Haskell WL BlairSN etal1ncreased exercise level and plasma lipoprotein concentrations a one-year randomized controlled study in sedmiddot entary middle-aged men Metabolism 1983 3231middot9
22 Morris IN Smith A eds Exercise health and medicine proceedings of the Lilleshall Conference London The Sports Council 1984
23 Leon AS ed Forum Exercise and healthPrev Med 1984 131middot99
24 Powell KE ed Workshop on epidemiologic and public health aspects of physical activity and exercise Public Health Rep 1985 100113-224
25 Hyde RT Paffenbarger RS Jr Epidemiologic uses of genera population assessments of physical activity patterns National Center for Health Statisshytics (in press)
26 Schneider EL Reed JD Jr Life extension N Engl J Med 1985 3121159shy68
27 Olshansky SJ Pursuing longevity delay vs elimination of degenerative diseases Am J Public Health 1985 75754-6
28 Ramazzini B Diseases of workers New York Hafner 1964 29 Guy WA Contributions to a knowledge of the influence of employments
upon health J R Stat Soc 1843 6197-21l 30 Smith E Report on the sanitary circumstances of tailors in London (Report
of the Medical Officer Privy Council) London Her Majestys Stationery Office 1864416-30
31 Morgan JE University oars being a critical enquiry into the after health of the men who rowed in the Oxford Ifld Cambridge hoat-race from the year 1829 to 1869 London Macmillan 1873
32 Hedley OF Analysis of 5116 deaths reported as due to acute coronary occlusion in Philadelphia 1933-1936 US WeekJyPublic Health Rep 1939 54972
33 Morris IN Heady JA Raffle PAB Roberts CG Parks JW Coronary heart disease and physical activity of work Lancet 1953 21053-7 1111-20
34 Montoye ill Van Huss WD Olson HW et al Longevity and morbidity of college athletes Lansing Mich Michigan State University 1957
35 Pomeroy WC White PD Coronary heart disease in former football players JAMA 1958 167711-4
36 Prout C Life expectancy of college oarsmen JAMA 1972 220 1709middot1 L 37 Belloc NB Relationship of health practices and mortality Prev Med 1973
267-81 38 Wiley JA Camacho TC Life-style and future health evidence from the
Alameda County study Prev Med 1980 91middot21 39 Breslow L Enstrom J Persistence of health habits and their relationship to
mortality Prev Med 1980 9469-83 40 Wingard DL Berkman LF Brand RJ A multivariate analysis of healthshy
related practices Am J Epidemiol 1982 116765-75
LARRY VELTMAN MD

606 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
ences by five-yeargroups Interrelations of paired characteristics (eg physical-activity index and cigarette smoking habit) were then examined by cross-tabulation of their three-level categories in which all-cause mortality rates were computed In analyses of trends of mortality using these cross-tabulations the influence of one characteristic was assessed with the influence of age and the other characteristic held constant The Mantel extension of the Mantel-Haenszel test was used in determining the significance of linear trends 12
Three groups were established for blood-pressure status normoshytensive alumni whose systolic blood pressure level during college was less than 130 mm Hg (69 percent of man-years) normotensive alumni whose systolic level during college was 130 or more mm Hg (22 percent) and alumni with physician-diagnosed hypertension (9 percent)
The three categories for cigarette smoking were nonsmokers (62 percent of man-years) men who smoked less than one pack a day (II percent) and men who smoked one or more packs a day (27 percent)
Body weight for height was expressed as body-mass index comshyputed from English units (1000 X weight in pounds divided by height in inches squared) Alumni were classified into three levels those with an index of 36 or more - who were 20 percent or more above their ideal weight according to 1959 Metropolitan Life Insurance Company standards (37 percent of man-years) those with an index of 34 to 35 - men who were 10 to 19 percent overshyweight (25 percent of man-years) and those with a body-mass index of less than 34 - men less than 10 percent overweight (38 percent of man-years) Net weight change (almost always a gain) after the college physical examination was middotcomputedmiddot in units of body-mass index an increase of 5 or more units represented a gain of 115 or more kg or 25 or more Ib (40 percent of man-years) an increase of 3 to 4 units a gain of 7 to 114 kg or 15 to 24 Ib (25 percent) and an increase of less than 3 units a gain of less than 7 kg or less than 15 Ib (35 percent)
The three categories for history of parental death before the age of 65 contained alumni without such a history (67 percent of manshyyears) those reporting that one parent was dead (29 percent) and those reporting that both parents were dead (4 percent)
Student participation in college athletics was established in three levels varsity sports play (21 percent of man-years) intramural sports play for five or more hours per week (37 percent) and intra~ mural play for less than five hours per week or not at all (42 percent)
Mortality rates per 10000 man-years of observation were used to compute relative risks of death the base representing men whose characteristic or level carried the highest risk (Tables I and 2 and the figures) or the lower risk (Table 3) Attributable risks (percentages) were computed as clinical estimates (I - IIrelative risk) x 100 and as community estimates
(prevalence of characteristic) X (rdative risk - I) X 100
I + (prevalence of characteristic) X (relative risk I)
Multivariate analyses for estimating the relative risks of death associated with the three levels of physical-activity index (less than 500500 to 1999 and 2000 or more kcal per week) were based on Coxs proportional-hazards models 13 Estimated adjusted probabilshyities of survival (Table 5) were based on a fitted proportionalshyhazards model If All probability values cited were determined with two-tailed tests
RESULTS
Of the 16936 alumni aged 35 to 74 who returned questionnaires in 1962 or 1966 reporting their health status exercise habits and other personal and lifeshystyle characteristics 1413 (8 percent) died from some cause between the ages of 35 and 80 in the 213716 man-years of follow-up ending in 1978 Underlying causes of death were cardiovascular disease in 45 pershy
cent cancer in 32 percent other natural causes in 13 percent and trauma in 10 percent
Table 1 shows age-adjusted rates of death from all causes during the 16-year follow-up period (1962 through 1978) according to physical activity (walkshying stair climbing and sports play) and the combinashytionphysical-activity index Relative risks of death are also shown
A small gradient effect of walking led to a 21 pershycent lower risk of death as distance was increased from less than 3 miles to 9 or more miles per week The pattern of benefit from stair climbing was less consisshytent possibly because of misclassifications due to ershyroneous reporting at the higher levels of stair countshying since some respondents (as requested) reported flights of stairs climbed and others (mistakenly) gave number of stairs Light sports did not influence the incidence of coronary heart disease78 but all-cause mortality rates were lowered by increased hours of play somewhat more than by walking For vigorous sports which tended to avert coronary heart disease there was also a significant inverse relation to all-cause mortality but with a reversing trend at three or more hours of play much as in the stair-climbing data This shift may also have been due to exaggerations in reshyporting or perhaps to actual increased hazards associshyated with vigorous activities Likewise such influences may account for the upswing at the highest level of physical activity (3500 or more kcal per week) Aside from that tendency the risk of death became progresshysively lower as the physical-activity level increased from below 500 to about 3500 kcal per week - the level at which the relative risk was less than half that associated with the least activity At an index of 3500 or more kcal per week the all-cause death rates beshycame relatively stable
Men with an index of less than 2000 kcal per week had a 38 percent greater risk of death in the 12- to 16shyyear follow-up period than men with a higher index Or in a positive sense men whose weekly energy outshyput in walking climbing stairs and playing sports totaled 2000 or more kcal per week had a 28 percent lower aU-cause death rate than less active men When the mortality data were analyzed for successive intershyvals of two five and another five years of follow-up during 1962 to 1974 or 1966 to 1978 the same trends were observed in each interval as over the total period The corresponding higher death rates for sedentary as compared with active men were 68 54 and 12 pershycent This finding supports the view that the inverse relation of physical activity to mortality was derived from a beneficial influence of exercise on survival and not merely from a selective effect of alumni who were or became physically inactive because they were chronically ill or had premonitory symptoms of disease
In all age groups there was a consistent trend toshyward a lower death rate as physical activity increased from less than 500 to 2000 or more kcal per week
Vol 314 No 10 PHYSICAL ACTIVITY MORTALITY AND LONGEVITY -PAFFENBARGER ET AL 607
Table 1 Age-Adjusted Rates and Relative Risks of Death (frorTl All Causes) among but was strongest and most signifishy16936 Harvard Alumni 1962 to 1978 According to Measures of Physical Activity cant in relation to cardiovascular
and respiratory diseases 7 PHYSICAL DEATHS PER RELATIVE
ACT1VITY PREVALENCE No OF 10000 RISK OF P OF In Table 2 age-adjusted all-cause (WEEKLY) (MANYEAlltS ) DEATHS MANYEARS DEATH TREND death rates are tabulated according Miles walked to alumni characteristics commonly
lt3 260 408 781 100 associated with an increased risk 3--8 442 573 667 085 00009 9 298 392 618 079 hypertension cigarette smoking
Stairs climbed extremes of weight in relation to lt350 344 545 740 100 height patterns of weight change 350-1049 500 627 627 085 00646 and early parental death Hypershy1050 156 200 680 092
tensive men had nearly twice theLight sports played (hr) risk of normotensive men whereas
None 770 837 812 100 the mortality rates among normoshy1-2 62 61 614 076 lt00001
tensive men differed only slightly 3 168 145 567 070 according to whether their systolic Vigorous sports
played (hr)t blood pressure during college was None 614 1046 754 100 below 130 mm Hg or 130 mm Hg1-2 184 166 491 065 lt00001 3 202 187 559 074 or higher Relative risks of death
Physicalmiddot activity among cigarette smokers were twice index (kcal)l those among nonsmokers
lt500 154 308 937 1m Alumni with a body-mass index
500-999 209 322 Qn 1000-1499 152 202 ~~~ 752 Qn 1m below 32 and those with an index of 1500-1999 104 121 593 Q~ lt00001 38 or higher contributed 17 and 18 2000-2499 lU 89
577 o~ percent of the man-years of obsershy2500-2999 69 62 485 O~544 Q on3000-3499 50 42 427 vation respectively Although the
3500 181 203 584 Q~ overall trend of association beshy-Exels subjecls who played vigorous sports tWilh or without light sportS play tween body-mass index and total tSummation of above measures equated to kilocalories + mortali ty was not significan t the
two thirds of alumni with indexes beiween the two extremes had a
(Fig I) The older alumni at the highest activity level lower risk The higher rates for their classmates with had half the risk of those at the low end the relative extremes of physique suggest that overlyfat men may risks were 051 for active men aged 70 to 84 and 053 succurpb to cardiovascular disease and the very unshyfor those aged 60 to 69 Younger alumni at the highest derweight possibly to wasting diseases such as cancer activity level had 25 percent less risk than those at the Of further interest the association of mortality with lowest level the relative risk was 064 for men aged 50 a low net gain in body-mass inqex was considerable to 59 and 079 for men aged 35 to 49 As would be Alumni with the lowest net gain since college had a 29 expected death rates were comparatively low in the percent higher risk of death than their classmates who younger age groups at all levels of physical activity In gained the most This trend represents departure from addition the onset of cancer or other terminal disease findings for coronary heart disease 78 The high risk of among the older men could have led some to shift into the group with the lowest net gain may reflect the low-activity life styles introducing an element of seshy wasting effects of disease the influence of cigarette lection manifested by the steeper slope in the lowshy smoking or some inherited insufficiency activity segments of the two upper curves in Figure 1 Hereditary or familial influences may help to exshyAside from this the general trend toward a lower plain why alumni whose parents had both died before death rate with increased physical activity was uriishy the age of 65 had a 29 percent higher risk of death form and significant than alumni whose parents had both lived to age
To allow for self-selection affecting exercise choice 65 or older (ie by alumni choosing a sedentary life because of ill The data in Table 2 do not consider physical activshyhealth) a11-cause and caQse-specific death rates from ity which has been shown to counteract the risks of cardiovascular or respiratory diseases cancer other coronary heart disease that are associated with most natural causes and trauma were examined along this of the characteristics listed therein 78 To refine and same gradient of physical activity Rates were adjustshy extend the above observations and assess the conshyed for differences in age cigarette smoking hypertenshy founding influences of any of those characteristics sion a low net body weight gain since college and and physical exercise the series of stereograms in Figshyearly parental death - personal characteristics affectshy ure 2 show relative risks of death from any cause ing all-cause mortality (see below) A decline in death according to levels of physicalactivity and selected rates with increasing activity was seen for each cause characteristics
608 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
All-Cause Oeath Rates per 10000 Man-Years
Observation 500rl----------------------------~
400
300
200
100
80
60
40
20
bull Relative Risk s above PIOI Po
100
~72 Inls
100 bull ~1Age
63 bull 70-84
bull~360-69
100 86
-------- 64
----50-59
100 97---shylt500 500-1999 2000+
Physical Activity in Kilocalories per Week
Figure 1 Age-Specific Mortality from All Causes among 16936 Harvard Alumni in 1962 to 1978 According to Physical-Activity
LevelS
In each stereogram mortality trends become evishydent as the influence of each characteristic is assessed with the influences of age and the paired characteristic held constant Relative-risk estimates were derived from the death rate in the presumed highest risk category represented by the back corner block which was assigned a relative risk of l00 Respective relative risks are shown by the heights of the other blocks Death rates per 10000 man-years are shown at the tops of the blocks and the numbers of decedents in the nine categories are tabulated in an accompanying diamond
Figure 2A assesses the influences of the physical activity of alumni and the blood pressure of students or alumni on the risk of death from all causes Throughout the stereoshygram death risks are reduced as physical activity is increased (from lt500 to 500-1999 to ~2000 kcal per week) and the drop in risk is proportionately greater with inshycreased exercise among the hypershytensive alumni Alumni with physishycian-diagnosed hypertension had about twice the risk of death of
normotensive alumni with the difshyference declining as exercise inshycreased Mortality rates were someshy
what lower among the normotensive alumni whose systolic bloqd pressure during college was below 130 mm Hg than for those with higher readings as stushydents The initial data on hypertension and exercise were collected in 1962 or 1966 before modern stepwise methods of blood-pressure management came into use Hence there is no good reason to suppose that the apparent benefit of exercise among the men with hyshypertension was due instead to differences in diagnosis of hypertension or to drug or dietary therapy for blood-pressure controL 15 The hypertensive alumni who exercised lowered their risk of death even though they remained hypertensive~
Figure 2B shows a steady reduction in the risk of death as exercise increased and cigarette smoking deshycreased The risk among sedentary heavy smokers was reduced by two thirds among the most active nonshysmokers At each level of exercise a reduction in smoking from one or more packs down to none cut the risk of death in half Cigaxette smoking and exercise had strong opposite influences on the risk of death from all causes and the figure has dual implications for behavior modification
In Figure 2C the highest mortality is seen among the alumni who were least active and had the lowest body-mass index At ariy level of body-mass index the risk of death decreased as physical activity increased from less than 500 to 2000 or more kcal per week However the relation of body mass to the risk of
Table 2 Age-Adjusted Rates and Relative Risks ofDeath (from All Causes) among 16936 HarVard Alumni 1962 to 1978 According to Selected Characteristics
of Alumni
DEATHS PER RELATIVE
ALUMNUS PREVALENCE No OF 10000 RISK OF P OF
CHAMCfERISTle (MANmiddot YEARS ) DEATHS MAN-YEARS DEATH TREND
Blood-pressure status Hypertension Normotension 130 Normotension lt 130t
Cigarette smoking (packsday)
1 ltI None
BOdy-mass indexl 31 32-33 34-35 36-37 38
Gain in body-mass index since college
lt3 3 4 5 6
Parents dead before age 65 Both One Neither
94 283 1173 100 214 275 680 058 lt00001 692 714 594 051
272 480 1104 100 110 129 644 058 lt00001 618 648 547 050
165 259 798 100 210 259 629 079 253 331 653 082 06308 190 236 608 076 182 286 761 095
350 432 8Ll 100 123 140 677 084 126 122 572 071 lt00001 ILl 132 623 077 290 401 626 077
41 87 808 100 292 491 773 096 lt00001 667 835 626 077
Nonnotensicin with student systolic blood pressure ~ 130 mm Hg
tNonnotension with student systolic blood pressure lt130 mm Hg
~Weight in potnds divided by the square of height in inches times 1000
609
-0$00_
- ~~-1~O
Vol 314- No IO PHYSICAL ACTIVITY MORTALITY AND LONGEVITY - PAFFENBARGER ET AL
Figure 2 Relative Risks (RR) of Death from All Causes among 16936 Harvard Alumni in 1962 to 1978 According to Post-College Physical-Activity Levels and (A) Alumnus and Student Blood-Pressure Status (B) Alumnus Cigarette Smoking (C) Alumnus Body Weight for Height (D) Net Change in Body Weight since College (E) History of Early Parental Death and (F) Participation in
College Sports Blocks designate the relative risk based on age-adjusted death rates (numbers at top of blocks) per 10000 man-years of observation Death rates in the back corner blocks establish the relative risk of 100 Numbers of deaths are given in a corresponding key below each stereogram P values are based on trends of rates for one characteristic adjusted for differences in age and the paired characteristic
death was uneven and the trend was not significant when age and physical activity index were held conshystant There is perhaps some hint that the risk among the most active alumni tended to increase at both the high and low extremes of body-mass index Again as noted in the discussion of Table 2 the high risk for sedentary men with a low body-mass index may inshyvolve a wasting disease such as cancer whereas men with a high body-mass index may invite death from cardiovascular disease
Table 2 also shows that men with the least net gain in body-mass index after their physical examination in college had a greater risk of death than those who gained more This is also evident in Figure 2D where mortality can be seen to decline with an increasing net gain in body mass-index and also with increasing curshyrent physical activity Inactive status with a low weight gain may signify illness whereas the gain in body-mass index among the more active men may reflect healthy muscularity - ie body leanness rathshyer than body fat
As shown in Figure 2E the death of one or both parents before the age of 65 was related to an inshycreased risk of death among the alumni but the risk was lower among the physically active Early loss of parents may suggest a hereditary risk but it does not appear to influence the risk of death as strongly as
does lack of exercise Whether or not the two factors are interrelated both have significant effects on morshytality and adequate contemporary exercise may virtushyally offset the influence of early parental death
The pattern of relative risks in Figure 2F shows that the rate of death from any cause was reduced with increased physical activity by alumni but that the sports-activity level in their student days did not have a similar effect on subsequent mortality Former varsishyty athletes who exercised at less than 500 or at 2000 or more kcal per week in their post-college years had higher death rates (93 and 73 per 10000 man-years of observation respectively) than those who reported continuing moderate exercise at 500 to 1999 kcal per week (61 per 10000 man-years) The most active group of former varsity players with a higher mortalshyity includes those who died from cancer or cardiovasshycularcauses Although in this pattern former varsity athletes seem to have had a higher risk than their less athletic classmates the chart overall shows a consisshytent pattern of benefit from habitual exercise by alumshyni Evidently inheritance of a sturdy constitution (as implied by varsity athletic status) is less important to longevity than continuation of adequate life-time exerCIse
Each stereogram in Figure 2 shows that the physical activity of alumni had an independent and significant
A B
~ 00 ~
075 shy 01gt shy
0$0 cSO shy
015 --
Alumrul Physlcol etlyU
ftld tKcIWbullbulltt ~~I~ -0001 fI 0001
D E
ARA~
100 100
07S shy075
aso 00
~oaI Oili
000 000 shy
SCtdy fn 11IwJI Physical ActivUy -- Gain Sinc Collaga PhyiealAcUvHy
thdu KeIWutt IweighOHighI2 nd KuilWbullbullk) 0001 ~ 0001 p 0001
AlutlUHJ
c
100 --- shy 015
oso -
025
Alumnut Cigarttbullbull Per Oy
p OOOt
F
AR
100
05
OliO gt
01$ ~
Au Phyak1 Activity
Indbullbull KcaUWbullbullle1 0001
610 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
inverse relation to mortality Moreover adequate exshyercise enhanced the mortality reduction associated with favorable levels of the other post-college characshyteristics studied
Table 3 shows relative and attributable risks of death from any cause which were derived from a multivariate analysis and computed for the presence versus the absence of each adverse characteristic with adjustment for the differences in age and each of the other characteristics listed 13 The relative risk of 131 associated with a sedentary life style signifies that men expending fewer than 2000 kcal per week had a 31 percent higher risk of death than more active men Likewise men with physician-diagnosed hypertension had a 73 percent higher risk than normotensive men and cigarette smokers had a 76 percent higher risk than nonsmokers Men who had a net weight gain of less than 7 kg (IS Ib) after college were at a 33 percent greater risk than men who gained more The alumni who had lost one or both patients before the age of 65 had a 15 percent higher risk of death than their classshymates whose parents had survived to age 65 or older The five characteristics assessed in the table or the basic mechanisms of causation they represent conshytribute independently to the risk of death from all causes
The clinical attributable risks listed in Table 3 are estimates of potential percentage reductions in the risk of death for persons who exchange the adverse characteristic for a more healthful characteristic Sedshyentary men who become more active might reduce their risk of d~ath by 24 percent If hypertensive men could obtain normal blood pressure they would have 42 percent less risk reformed cigarette smokers 43 percent less Men whose net weight gain since college was below 7 kg might have had a 25 percent lower risk of death if they had gained more If men who lost one or both parents early had had parents living to age 65 or older their own risk of death might have been 13 percent less The clinical percentage estimates in Tashyble 3 are not additive
The community attributable risks in Table 3 are
estimates that take prevalence into account They inshydicate what percentage of risk might be spared in a community or population if the adverse characterisshytics listed were converted to more favorable characshyteristics The risk of death might be reduced by 16 percent in the alumni population if every man had exercised at 2000 or more kcal per week Abolition of hypertension might cut the community death rate anshyother 6 percent total abstinence from cigarettes anshyother 23 percent a greater net weight gain 10 percent more and survival of both parents to age 65 or older another 5 percent These estimates though hypothetishycal are additive so thlttt if all five adverse characterisshytics were eliminated the total risk of death in the community of alumni might be cut by more than half - ie there might have been 60 percent fewer deaths during the study period (1962 to 1978) or a loss of only 551 alumni instead of 1413
Relative and attributable risks of death from carshydiovascular disease in association with similar adverse characteristics (sedentariness hypertension smoking overweight and parental coronary heart disease) among the alumni were of the same general order of magnishytude as risks of all-cause mortality After allowance for age and each other adverse characteristic sedentary alumni had a 31 percent higher risk of cardiovascular mortality than more physically active men hypertensive men had a 118 percent greater risk than normotensive men cigarette smokers had an 84 percen greater risk than nonsmokers heavier men had an 18 percent higher risk than leaner men and alumni with a parenshytal history of coronary heart disease had a 33 percent higher risk of dying from cardiovascular disease than classmates whose parents were free of coronary heart disease The attributable-risk estimates (community) corresponding to these same characteristics were 16 9 25 6 and II percent respectively In combination they indicated that there might have been 67 percent fewer deaths from cardiovascular disease during the study period in the absence of all five characteristics or a loss of only 196 alumni instead of the 640 who died from underlying cardiovascular disease
As shown in Table 4 the mortalshyity and survival experience of the
Table 3 Relative and Attributable Risks of Death (from All Causes) among 16936 Harvard alumni during the 16-year Harvard Alumni 1962 to 1978 According to Selected Adverse Characteristics follow-up period were used to deshy
velop estimates of years of added CLINICAL COMMUNITY
life gained (up to age 80) from anALUMNUS PREVALENCE RELATIVE RISK AlTRIBJTABLE A lTlUBUTABLE
CHARACTERISTIC (MAN-YEAlIS ) OF DEATHt P VALUE ~K( ~K() active life style rather than an inacshySedentary life stylet 620 131 (115-149) 00001 236 161 tive life style The results are tabushyHypertensionsect 94 1 73 (14S-201) lt00001 421 64 lated for five-year age groups at the Cigarette smoking~ 382 176 (156-199) lt00001 432 225 start of follow-up and selected measshyLow net weight gainll 351 133 (117-151) 00001 246 103 ures of physical activity The data Early parental death 333 U5 (102-130) 00248 131 48 are shown with and without adshybullAdjusted for differences in age and each of the other characteristics listed
tFigures in parentheses are 95 percent confidence intervals
Energy expenditure of lt2000 kcal per week in walking climbing stairs and playing sports
sectPhysician-dignosed
Any amount
IINet gain in body-mass index of lt3 units since college ie bull nO more than 7 leg (15 Ib)
bull One or both parents dead before he age of 65
justment for differences in bloodshypressure status cigarette use net gain in body-mass index and pashyrental death The first two columns under physical-activity show the crude and adjusted estimated years
611 VoL 314 NoO PHYSICAL ACTIVITY MORTALITY AND LONGEVITY PAFFENBARGER ET AL
Table 4 Added life from an Active life Style in Men Jp to the Age of 80 Estimated from Harvard Alumni Mortality 1962 to 1978
PHYSICAL-ACTIVITY INDEXmiddot VIGOItOUS SPOIlTS ILAY
AGE AT 2000 VS 2000 VS 2000 VS PusENT vs ENTIlY lt500 lt2000 500-1999 ABSENT
(n) CltUDE AllJUSTEot CRUDE AllJUSTEOt CRUDE ADJUSTEOt CRUOE ADJUSTEot
esrimaJed no of years gained
35-39 264 251 166 150 126 107 166 155 4)-44 248 234 146 139 104 099 154 145 45-49 232 20 24 110 080 067 138 123 50-54 237 211 135 120 093 081 140 132 55-59 225 202 127 113 087 075 125 121 60-64 198 175 104 093 065 057 100 095 65-69 164 135 082 067 048 036 070 055 70-74 094 072 057 044 042 middot031 011 -011 75-79 035 042 029 030 026 024 001
35-79i 233 215 138 125 099 086 137 128
Kilocalories experuled per week in walking climbing stairs and plying sports
t Adjusted for differences in blood-pIeS stalUs cigarette smoking net gain in body-mass index since college and age of parental death
lWeighted vgbull
of survival gained by men expending 2000 or more kcal per week on exercise as compared with those expending less than 500 kcal per week The latter group might be considered likely to include most men who had selectively reduced their exercise levels beshycause of disease or premonitory symptoms As would be expected the survival difference (or number of years gained) was greatest between the extremes for levels of activity The third and fourth columns show the estimated results when all ~lumni are inshycluded with a single break point at 2000 kcal per week and the differences are still consistent though smaller In the fifth and sixth columns the group with the lowest activity (less than 500 kcal per week) is omitted yet the benefit of exercise is still evident
The data in the seventh and eighth columns showshying the survival advantages associated with vigorous sports parallel those in the third and fourth columns except in the age groups 65 and older in which indulshygence in vigorous sports is less likely In addition parshyticipation in vigorous sports would be expected to be most common among alumni expending 2000 or more kcal per week and this likely possibility may well acshycount for some of the contrast noted earlier regarding the first two columns in Table 4 if participating in vigorous sports is considered to enhance survival more than a high activity level In addition the influence of vigorous sports would probably be split in the fifth and sixth columns and so dampen the differences listed there as can be seen In view of these consistent patshyterns the data in Table 4 support the hypothesis that survival and hence longevity among the Harvard alumni has been influenced to an appreciable degree by both the total amount and the intensity of habitual physical activity engaged in throughout adult life The bottom line of Table 4 presents weighted avershy~ges for years gained up to the age of 80 as a result of Increased physical activity between the ages of 35 and
79 The survival estimates given in the table or othershywise calculated would vary depending on the definishytions or standards of physical activity employed in the analysis
Another assessment of the influence of physical acshytivity on longevity is shown in Table 5 in which the survival of active and sedentary alumni up to the age of 80 is estimated for five-year age groups after adshyjustment for differences in hypertension smoking low weight gain and early parental death Weigllted avershyages for the total age range are also shown For both active and sedentary men the percentage predicted to reach age 80 increases somewhat with age perhaps becausethe younger groups have yet to escape hazshyards of mortality that the older men have already avoided whereas the latter need to survive for fewer years to reach the age of 80 Nevertheless the physshyically active men had a continuing 10 percent advan-
Table 5 Proportions of Active and Sedentary Men Surviving to the Age of 80 Estimated from Harvard Alumni Mortality
1962 to 1978
AGE ATENny PHYSICALmiddotACTIVITY INOEX
(YR) 2000 lt2000
survivingt
35-39 682 578 40-44 685 582 45-49 690 592 50-54 699 598 55-59 711 610 60-64 730 634 65-69 764 676 70-74 824 746
75-79 918 850
35-791 697 598
Kilocalories expended per week in walking climbing tairs and playing sports
t Adjusted for differences in blood-pressure stalUs cigarette smoking net gain in body-mass mdex since college and age of parental death
jWeighted average
612 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
tage over the sedentary men until they reached the 65-to-69-year age bracket thereafter a tapering effect occurred because all the survivors from those groups had to reach the age of 80 within the follow-up period and hence their comparison was based on fewer years of mortality data It is possible too that contrasts between an active and sedentary life style were less marked in the older groups than in the younger groups Overall the table suggests a considerable gain in man-years of life for the habitually energetic alumshyni especially if any avoidable adverse characteristics such as cigarette smoking and obesity have been minimized
DISCUSSION
Survival is the result of a number of interacting influences (many hazardous in character or degree some beneficial in the same way) including physical activity and other life-style elements susceptible to opshytional adjustment Their combined effect determines whether increases in longevity are feasible or even deshysirable The findings reported here represent only a small part of the total picture but they suggest a proshytective effect of exercise against all-cause mortality in all age groups studied and therefore an indieationof additional years of life expectancy
The Harvard alumni may not be typical of the genshyeral population Their age-specific death rates from each major cause except suicide were roughly half the 1980 rates for white males in the United States (In contrast rates of self-destruction among the alumshyni 16- 18 were 50 percent higher than suicide rates in the general population) Yet the large alumni experience with delayed mortality for active men should imply increased life expectancy over that for sedentary men as the data demonstrate It is likely that some alumni increased their exercise reduced their smoking and received treatment for hypertension since the early 1960s when these characteristics were assessed Such changes would minimize the importance of these characteristics in the present findings The true force of the beneficial effects from physical activity nonshysmoking and control of hypertension would be even larger than that observed
Table 4 presents survival data in terms of definishytions of exercise that were necessarily limited by the design of the study to increases in kilocalories per week or to intensity as expressed by participation in vigorous sports The estimates of years gained reflect the experience of college alumni already recognized as long-lived whose economic status and behavior patterns differ from other populations in habitual physical exercise and other life-style elements Direct extrapolation to a general population should take these considerations into account
Since the data in Tables 4 and 5 represent only a portion of the total life experience of the study populashytion over time they may be viewed as a segment seen as through a window implying extensions that might
be estimated from the actual experience observed The differences in survival to the age of 80 between active and sedentary alumni may reflect a stage of optimal benefit from physical activity by the age of 65 and a rectangularization or converging trend may be estabshylished as the total life experience of the population of alumni approaches completion 19
Improvements in epidemiologic surveillance and medical management of such chronic disorders as hyshypertension abnormal blood lipid profiles and osteoshyporosis may defer mortality and extend survival However the effect of adequate physical exercise is partly independent of such influences and it countershyacts many adverse characteristics through metabolic and other processes20-25 Even when other procedures for health maintenance and disease prevention are deshyveloped to increase longevity the relevance of exercise is likely to remain
In studies of longevity the question arises whether the aging process is capable of modification but there is much uncertainty about the definitions of aging and of chronic disease Approaches to fend off disease or postpone aging are suggested or aging is regarded as an inexorable degenerative process that cannot be alshytered although perhaps chronic diseases may be avoided or deferred 2627 The present study considers chronic diseases but not the aging process itself
Extended follow-up of the Harvard alumni may reshyveal trends of aging or at least show at what stage of life the roles of exercise and10ther natural therapies become diminished The data in Tables 4 and 5 do offer some implications as a brief preliminary analysis of survival in various age and exercise groups In view of the data base and the consistency represented in the study it seems likely that the observed patterns are predictive
There is a widespread and longstanding popular belief that adequate physical exercise is necessary to preserve life and its desirable qualities into old age Discussions of this thesis date back to antiquity and have intensified in recent times 28
-40 The present study
adds new evidence to support this view
REFERENCES
1 Keys A Seven countries a multivariate analysis of death and coronary heart disease Cambridge Mass Harvard University Press 1980196-217276middot 8
2 Leon AS Blackburn H Physical inactivity In Kaplan NM Stamler I eds Prevention of coronary heart disease practical management of the risk factors Philadelphia WB Saunders 198386-97
3 Karvonen MJ Physical activity in work and leisure time in relation to cardiovascular diseases Ann Clin Res 1983 14SuppJ 34118-23
4 Morris IN Uses of epidemiology 3rd ed Edinburgh Churchill Livingshystone 1975163-5
5 Morris IN Kagan A Pattison DC Gardner MJlncidence and prediction of ischaemic heart-disease in London busmen Lancet 1966 2552-9
6 Paffenbarger RS Ir Brand RI Sholtz RI Jung DL Energy expenditure cigarette smoking and blood pressure level as related to death from specific diseases Am I Epidemiol 1978 10812-8
7 Paffenbarger RS Jr Hyde RT Wing AL Steinmetz CH A natural history of athleticism and cardiovascular health lAMA 1984 252491-5
8 Paffenbarger RS Ir Wing AL Hyde RT Physical activity as an index of heart attack risk in college alumni Am I Epidemiol 1978 108161shy75
613 Vol 314 No 10 PHYSICAL ACTIVITY MORTALITY AND LONGEVITY - PAFFENBARGER ET AL
9 Thomas GS Lee PR Franks P Paffenbarger RS Jr Exercise and health the evidence and the implications Cambridge Mass Oelgeschlager Gunn amp Hain 1981
10 Paffenbarger RS Jr Notkin J Krueger DE et al Chronic disease in former college students II Methods of study and observations on mortality from coronary heart disease Am J Public Health 1966 56962middot71
11 Passmore R Durnin JVGA Human energy expenditure Physiol Rev 1955 35801-40
12 Mantel N Chimiddotsquare tests with one degree of freedom extensions of the Mantel-Haenszel procedure J Am Stat Assoc 1963 58690middot700
13 Cox DR Regression models and life-tables J R Soc Biostat 1972 34187middot 220
14 Chang ImiddotM Gelman R Pagano M Corrected group prognostic curves and summary statistics J Chronic Dis 1982 35669-74
15 Paffenbarget RS Jr Wing AL Hyde RT Jung DL Physical activity and incidence of hypertension in college alumni Am J Epidemiol 1983 117245middot57
16 Paffenbarger RS Jr Asnes DP Chronic disease in former college students III Precursors of suicide in early and middle life Am J Public Health 1966 561026-36
17 Paffenbarger RS Jr Chronic disease in former college students VI Implicamiddot tiOlls for college health programs J Am College Health Assoc 1967 1651middot 5
IS Paffenbarger RS Jr King SH Wing AL Chronic disease in former college students IX Characteristics in youth that predispose to suicide and accidenshytal death in later life Am J Public Health 1969 5990()S
19 Fries IF Crapo LM Vitality and aging implications of the rectangular curve San Francisco WH Freeman 1981
20 Paffenbarger RS Jr Hyde RT Exercise as protection against heart attack N Engl J Med 1980 3021026-7
21 Wood PO Haskell WL BlairSN etal1ncreased exercise level and plasma lipoprotein concentrations a one-year randomized controlled study in sedmiddot entary middle-aged men Metabolism 1983 3231middot9
22 Morris IN Smith A eds Exercise health and medicine proceedings of the Lilleshall Conference London The Sports Council 1984
23 Leon AS ed Forum Exercise and healthPrev Med 1984 131middot99
24 Powell KE ed Workshop on epidemiologic and public health aspects of physical activity and exercise Public Health Rep 1985 100113-224
25 Hyde RT Paffenbarger RS Jr Epidemiologic uses of genera population assessments of physical activity patterns National Center for Health Statisshytics (in press)
26 Schneider EL Reed JD Jr Life extension N Engl J Med 1985 3121159shy68
27 Olshansky SJ Pursuing longevity delay vs elimination of degenerative diseases Am J Public Health 1985 75754-6
28 Ramazzini B Diseases of workers New York Hafner 1964 29 Guy WA Contributions to a knowledge of the influence of employments
upon health J R Stat Soc 1843 6197-21l 30 Smith E Report on the sanitary circumstances of tailors in London (Report
of the Medical Officer Privy Council) London Her Majestys Stationery Office 1864416-30
31 Morgan JE University oars being a critical enquiry into the after health of the men who rowed in the Oxford Ifld Cambridge hoat-race from the year 1829 to 1869 London Macmillan 1873
32 Hedley OF Analysis of 5116 deaths reported as due to acute coronary occlusion in Philadelphia 1933-1936 US WeekJyPublic Health Rep 1939 54972
33 Morris IN Heady JA Raffle PAB Roberts CG Parks JW Coronary heart disease and physical activity of work Lancet 1953 21053-7 1111-20
34 Montoye ill Van Huss WD Olson HW et al Longevity and morbidity of college athletes Lansing Mich Michigan State University 1957
35 Pomeroy WC White PD Coronary heart disease in former football players JAMA 1958 167711-4
36 Prout C Life expectancy of college oarsmen JAMA 1972 220 1709middot1 L 37 Belloc NB Relationship of health practices and mortality Prev Med 1973
267-81 38 Wiley JA Camacho TC Life-style and future health evidence from the
Alameda County study Prev Med 1980 91middot21 39 Breslow L Enstrom J Persistence of health habits and their relationship to
mortality Prev Med 1980 9469-83 40 Wingard DL Berkman LF Brand RJ A multivariate analysis of healthshy
related practices Am J Epidemiol 1982 116765-75
LARRY VELTMAN MD

Vol 314 No 10 PHYSICAL ACTIVITY MORTALITY AND LONGEVITY -PAFFENBARGER ET AL 607
Table 1 Age-Adjusted Rates and Relative Risks of Death (frorTl All Causes) among but was strongest and most signifishy16936 Harvard Alumni 1962 to 1978 According to Measures of Physical Activity cant in relation to cardiovascular
and respiratory diseases 7 PHYSICAL DEATHS PER RELATIVE
ACT1VITY PREVALENCE No OF 10000 RISK OF P OF In Table 2 age-adjusted all-cause (WEEKLY) (MANYEAlltS ) DEATHS MANYEARS DEATH TREND death rates are tabulated according Miles walked to alumni characteristics commonly
lt3 260 408 781 100 associated with an increased risk 3--8 442 573 667 085 00009 9 298 392 618 079 hypertension cigarette smoking
Stairs climbed extremes of weight in relation to lt350 344 545 740 100 height patterns of weight change 350-1049 500 627 627 085 00646 and early parental death Hypershy1050 156 200 680 092
tensive men had nearly twice theLight sports played (hr) risk of normotensive men whereas
None 770 837 812 100 the mortality rates among normoshy1-2 62 61 614 076 lt00001
tensive men differed only slightly 3 168 145 567 070 according to whether their systolic Vigorous sports
played (hr)t blood pressure during college was None 614 1046 754 100 below 130 mm Hg or 130 mm Hg1-2 184 166 491 065 lt00001 3 202 187 559 074 or higher Relative risks of death
Physicalmiddot activity among cigarette smokers were twice index (kcal)l those among nonsmokers
lt500 154 308 937 1m Alumni with a body-mass index
500-999 209 322 Qn 1000-1499 152 202 ~~~ 752 Qn 1m below 32 and those with an index of 1500-1999 104 121 593 Q~ lt00001 38 or higher contributed 17 and 18 2000-2499 lU 89
577 o~ percent of the man-years of obsershy2500-2999 69 62 485 O~544 Q on3000-3499 50 42 427 vation respectively Although the
3500 181 203 584 Q~ overall trend of association beshy-Exels subjecls who played vigorous sports tWilh or without light sportS play tween body-mass index and total tSummation of above measures equated to kilocalories + mortali ty was not significan t the
two thirds of alumni with indexes beiween the two extremes had a
(Fig I) The older alumni at the highest activity level lower risk The higher rates for their classmates with had half the risk of those at the low end the relative extremes of physique suggest that overlyfat men may risks were 051 for active men aged 70 to 84 and 053 succurpb to cardiovascular disease and the very unshyfor those aged 60 to 69 Younger alumni at the highest derweight possibly to wasting diseases such as cancer activity level had 25 percent less risk than those at the Of further interest the association of mortality with lowest level the relative risk was 064 for men aged 50 a low net gain in body-mass inqex was considerable to 59 and 079 for men aged 35 to 49 As would be Alumni with the lowest net gain since college had a 29 expected death rates were comparatively low in the percent higher risk of death than their classmates who younger age groups at all levels of physical activity In gained the most This trend represents departure from addition the onset of cancer or other terminal disease findings for coronary heart disease 78 The high risk of among the older men could have led some to shift into the group with the lowest net gain may reflect the low-activity life styles introducing an element of seshy wasting effects of disease the influence of cigarette lection manifested by the steeper slope in the lowshy smoking or some inherited insufficiency activity segments of the two upper curves in Figure 1 Hereditary or familial influences may help to exshyAside from this the general trend toward a lower plain why alumni whose parents had both died before death rate with increased physical activity was uriishy the age of 65 had a 29 percent higher risk of death form and significant than alumni whose parents had both lived to age
To allow for self-selection affecting exercise choice 65 or older (ie by alumni choosing a sedentary life because of ill The data in Table 2 do not consider physical activshyhealth) a11-cause and caQse-specific death rates from ity which has been shown to counteract the risks of cardiovascular or respiratory diseases cancer other coronary heart disease that are associated with most natural causes and trauma were examined along this of the characteristics listed therein 78 To refine and same gradient of physical activity Rates were adjustshy extend the above observations and assess the conshyed for differences in age cigarette smoking hypertenshy founding influences of any of those characteristics sion a low net body weight gain since college and and physical exercise the series of stereograms in Figshyearly parental death - personal characteristics affectshy ure 2 show relative risks of death from any cause ing all-cause mortality (see below) A decline in death according to levels of physicalactivity and selected rates with increasing activity was seen for each cause characteristics
608 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
All-Cause Oeath Rates per 10000 Man-Years
Observation 500rl----------------------------~
400
300
200
100
80
60
40
20
bull Relative Risk s above PIOI Po
100
~72 Inls
100 bull ~1Age
63 bull 70-84
bull~360-69
100 86
-------- 64
----50-59
100 97---shylt500 500-1999 2000+
Physical Activity in Kilocalories per Week
Figure 1 Age-Specific Mortality from All Causes among 16936 Harvard Alumni in 1962 to 1978 According to Physical-Activity
LevelS
In each stereogram mortality trends become evishydent as the influence of each characteristic is assessed with the influences of age and the paired characteristic held constant Relative-risk estimates were derived from the death rate in the presumed highest risk category represented by the back corner block which was assigned a relative risk of l00 Respective relative risks are shown by the heights of the other blocks Death rates per 10000 man-years are shown at the tops of the blocks and the numbers of decedents in the nine categories are tabulated in an accompanying diamond
Figure 2A assesses the influences of the physical activity of alumni and the blood pressure of students or alumni on the risk of death from all causes Throughout the stereoshygram death risks are reduced as physical activity is increased (from lt500 to 500-1999 to ~2000 kcal per week) and the drop in risk is proportionately greater with inshycreased exercise among the hypershytensive alumni Alumni with physishycian-diagnosed hypertension had about twice the risk of death of
normotensive alumni with the difshyference declining as exercise inshycreased Mortality rates were someshy
what lower among the normotensive alumni whose systolic bloqd pressure during college was below 130 mm Hg than for those with higher readings as stushydents The initial data on hypertension and exercise were collected in 1962 or 1966 before modern stepwise methods of blood-pressure management came into use Hence there is no good reason to suppose that the apparent benefit of exercise among the men with hyshypertension was due instead to differences in diagnosis of hypertension or to drug or dietary therapy for blood-pressure controL 15 The hypertensive alumni who exercised lowered their risk of death even though they remained hypertensive~
Figure 2B shows a steady reduction in the risk of death as exercise increased and cigarette smoking deshycreased The risk among sedentary heavy smokers was reduced by two thirds among the most active nonshysmokers At each level of exercise a reduction in smoking from one or more packs down to none cut the risk of death in half Cigaxette smoking and exercise had strong opposite influences on the risk of death from all causes and the figure has dual implications for behavior modification
In Figure 2C the highest mortality is seen among the alumni who were least active and had the lowest body-mass index At ariy level of body-mass index the risk of death decreased as physical activity increased from less than 500 to 2000 or more kcal per week However the relation of body mass to the risk of
Table 2 Age-Adjusted Rates and Relative Risks ofDeath (from All Causes) among 16936 HarVard Alumni 1962 to 1978 According to Selected Characteristics
of Alumni
DEATHS PER RELATIVE
ALUMNUS PREVALENCE No OF 10000 RISK OF P OF
CHAMCfERISTle (MANmiddot YEARS ) DEATHS MAN-YEARS DEATH TREND
Blood-pressure status Hypertension Normotension 130 Normotension lt 130t
Cigarette smoking (packsday)
1 ltI None
BOdy-mass indexl 31 32-33 34-35 36-37 38
Gain in body-mass index since college
lt3 3 4 5 6
Parents dead before age 65 Both One Neither
94 283 1173 100 214 275 680 058 lt00001 692 714 594 051
272 480 1104 100 110 129 644 058 lt00001 618 648 547 050
165 259 798 100 210 259 629 079 253 331 653 082 06308 190 236 608 076 182 286 761 095
350 432 8Ll 100 123 140 677 084 126 122 572 071 lt00001 ILl 132 623 077 290 401 626 077
41 87 808 100 292 491 773 096 lt00001 667 835 626 077
Nonnotensicin with student systolic blood pressure ~ 130 mm Hg
tNonnotension with student systolic blood pressure lt130 mm Hg
~Weight in potnds divided by the square of height in inches times 1000
609
-0$00_
- ~~-1~O
Vol 314- No IO PHYSICAL ACTIVITY MORTALITY AND LONGEVITY - PAFFENBARGER ET AL
Figure 2 Relative Risks (RR) of Death from All Causes among 16936 Harvard Alumni in 1962 to 1978 According to Post-College Physical-Activity Levels and (A) Alumnus and Student Blood-Pressure Status (B) Alumnus Cigarette Smoking (C) Alumnus Body Weight for Height (D) Net Change in Body Weight since College (E) History of Early Parental Death and (F) Participation in
College Sports Blocks designate the relative risk based on age-adjusted death rates (numbers at top of blocks) per 10000 man-years of observation Death rates in the back corner blocks establish the relative risk of 100 Numbers of deaths are given in a corresponding key below each stereogram P values are based on trends of rates for one characteristic adjusted for differences in age and the paired characteristic
death was uneven and the trend was not significant when age and physical activity index were held conshystant There is perhaps some hint that the risk among the most active alumni tended to increase at both the high and low extremes of body-mass index Again as noted in the discussion of Table 2 the high risk for sedentary men with a low body-mass index may inshyvolve a wasting disease such as cancer whereas men with a high body-mass index may invite death from cardiovascular disease
Table 2 also shows that men with the least net gain in body-mass index after their physical examination in college had a greater risk of death than those who gained more This is also evident in Figure 2D where mortality can be seen to decline with an increasing net gain in body mass-index and also with increasing curshyrent physical activity Inactive status with a low weight gain may signify illness whereas the gain in body-mass index among the more active men may reflect healthy muscularity - ie body leanness rathshyer than body fat
As shown in Figure 2E the death of one or both parents before the age of 65 was related to an inshycreased risk of death among the alumni but the risk was lower among the physically active Early loss of parents may suggest a hereditary risk but it does not appear to influence the risk of death as strongly as
does lack of exercise Whether or not the two factors are interrelated both have significant effects on morshytality and adequate contemporary exercise may virtushyally offset the influence of early parental death
The pattern of relative risks in Figure 2F shows that the rate of death from any cause was reduced with increased physical activity by alumni but that the sports-activity level in their student days did not have a similar effect on subsequent mortality Former varsishyty athletes who exercised at less than 500 or at 2000 or more kcal per week in their post-college years had higher death rates (93 and 73 per 10000 man-years of observation respectively) than those who reported continuing moderate exercise at 500 to 1999 kcal per week (61 per 10000 man-years) The most active group of former varsity players with a higher mortalshyity includes those who died from cancer or cardiovasshycularcauses Although in this pattern former varsity athletes seem to have had a higher risk than their less athletic classmates the chart overall shows a consisshytent pattern of benefit from habitual exercise by alumshyni Evidently inheritance of a sturdy constitution (as implied by varsity athletic status) is less important to longevity than continuation of adequate life-time exerCIse
Each stereogram in Figure 2 shows that the physical activity of alumni had an independent and significant
A B
~ 00 ~
075 shy 01gt shy
0$0 cSO shy
015 --
Alumrul Physlcol etlyU
ftld tKcIWbullbulltt ~~I~ -0001 fI 0001
D E
ARA~
100 100
07S shy075
aso 00
~oaI Oili
000 000 shy
SCtdy fn 11IwJI Physical ActivUy -- Gain Sinc Collaga PhyiealAcUvHy
thdu KeIWutt IweighOHighI2 nd KuilWbullbullk) 0001 ~ 0001 p 0001
AlutlUHJ
c
100 --- shy 015
oso -
025
Alumnut Cigarttbullbull Per Oy
p OOOt
F
AR
100
05
OliO gt
01$ ~
Au Phyak1 Activity
Indbullbull KcaUWbullbullle1 0001
610 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
inverse relation to mortality Moreover adequate exshyercise enhanced the mortality reduction associated with favorable levels of the other post-college characshyteristics studied
Table 3 shows relative and attributable risks of death from any cause which were derived from a multivariate analysis and computed for the presence versus the absence of each adverse characteristic with adjustment for the differences in age and each of the other characteristics listed 13 The relative risk of 131 associated with a sedentary life style signifies that men expending fewer than 2000 kcal per week had a 31 percent higher risk of death than more active men Likewise men with physician-diagnosed hypertension had a 73 percent higher risk than normotensive men and cigarette smokers had a 76 percent higher risk than nonsmokers Men who had a net weight gain of less than 7 kg (IS Ib) after college were at a 33 percent greater risk than men who gained more The alumni who had lost one or both patients before the age of 65 had a 15 percent higher risk of death than their classshymates whose parents had survived to age 65 or older The five characteristics assessed in the table or the basic mechanisms of causation they represent conshytribute independently to the risk of death from all causes
The clinical attributable risks listed in Table 3 are estimates of potential percentage reductions in the risk of death for persons who exchange the adverse characteristic for a more healthful characteristic Sedshyentary men who become more active might reduce their risk of d~ath by 24 percent If hypertensive men could obtain normal blood pressure they would have 42 percent less risk reformed cigarette smokers 43 percent less Men whose net weight gain since college was below 7 kg might have had a 25 percent lower risk of death if they had gained more If men who lost one or both parents early had had parents living to age 65 or older their own risk of death might have been 13 percent less The clinical percentage estimates in Tashyble 3 are not additive
The community attributable risks in Table 3 are
estimates that take prevalence into account They inshydicate what percentage of risk might be spared in a community or population if the adverse characterisshytics listed were converted to more favorable characshyteristics The risk of death might be reduced by 16 percent in the alumni population if every man had exercised at 2000 or more kcal per week Abolition of hypertension might cut the community death rate anshyother 6 percent total abstinence from cigarettes anshyother 23 percent a greater net weight gain 10 percent more and survival of both parents to age 65 or older another 5 percent These estimates though hypothetishycal are additive so thlttt if all five adverse characterisshytics were eliminated the total risk of death in the community of alumni might be cut by more than half - ie there might have been 60 percent fewer deaths during the study period (1962 to 1978) or a loss of only 551 alumni instead of 1413
Relative and attributable risks of death from carshydiovascular disease in association with similar adverse characteristics (sedentariness hypertension smoking overweight and parental coronary heart disease) among the alumni were of the same general order of magnishytude as risks of all-cause mortality After allowance for age and each other adverse characteristic sedentary alumni had a 31 percent higher risk of cardiovascular mortality than more physically active men hypertensive men had a 118 percent greater risk than normotensive men cigarette smokers had an 84 percen greater risk than nonsmokers heavier men had an 18 percent higher risk than leaner men and alumni with a parenshytal history of coronary heart disease had a 33 percent higher risk of dying from cardiovascular disease than classmates whose parents were free of coronary heart disease The attributable-risk estimates (community) corresponding to these same characteristics were 16 9 25 6 and II percent respectively In combination they indicated that there might have been 67 percent fewer deaths from cardiovascular disease during the study period in the absence of all five characteristics or a loss of only 196 alumni instead of the 640 who died from underlying cardiovascular disease
As shown in Table 4 the mortalshyity and survival experience of the
Table 3 Relative and Attributable Risks of Death (from All Causes) among 16936 Harvard alumni during the 16-year Harvard Alumni 1962 to 1978 According to Selected Adverse Characteristics follow-up period were used to deshy
velop estimates of years of added CLINICAL COMMUNITY
life gained (up to age 80) from anALUMNUS PREVALENCE RELATIVE RISK AlTRIBJTABLE A lTlUBUTABLE
CHARACTERISTIC (MAN-YEAlIS ) OF DEATHt P VALUE ~K( ~K() active life style rather than an inacshySedentary life stylet 620 131 (115-149) 00001 236 161 tive life style The results are tabushyHypertensionsect 94 1 73 (14S-201) lt00001 421 64 lated for five-year age groups at the Cigarette smoking~ 382 176 (156-199) lt00001 432 225 start of follow-up and selected measshyLow net weight gainll 351 133 (117-151) 00001 246 103 ures of physical activity The data Early parental death 333 U5 (102-130) 00248 131 48 are shown with and without adshybullAdjusted for differences in age and each of the other characteristics listed
tFigures in parentheses are 95 percent confidence intervals
Energy expenditure of lt2000 kcal per week in walking climbing stairs and playing sports
sectPhysician-dignosed
Any amount
IINet gain in body-mass index of lt3 units since college ie bull nO more than 7 leg (15 Ib)
bull One or both parents dead before he age of 65
justment for differences in bloodshypressure status cigarette use net gain in body-mass index and pashyrental death The first two columns under physical-activity show the crude and adjusted estimated years
611 VoL 314 NoO PHYSICAL ACTIVITY MORTALITY AND LONGEVITY PAFFENBARGER ET AL
Table 4 Added life from an Active life Style in Men Jp to the Age of 80 Estimated from Harvard Alumni Mortality 1962 to 1978
PHYSICAL-ACTIVITY INDEXmiddot VIGOItOUS SPOIlTS ILAY
AGE AT 2000 VS 2000 VS 2000 VS PusENT vs ENTIlY lt500 lt2000 500-1999 ABSENT
(n) CltUDE AllJUSTEot CRUDE AllJUSTEOt CRUDE ADJUSTEOt CRUOE ADJUSTEot
esrimaJed no of years gained
35-39 264 251 166 150 126 107 166 155 4)-44 248 234 146 139 104 099 154 145 45-49 232 20 24 110 080 067 138 123 50-54 237 211 135 120 093 081 140 132 55-59 225 202 127 113 087 075 125 121 60-64 198 175 104 093 065 057 100 095 65-69 164 135 082 067 048 036 070 055 70-74 094 072 057 044 042 middot031 011 -011 75-79 035 042 029 030 026 024 001
35-79i 233 215 138 125 099 086 137 128
Kilocalories experuled per week in walking climbing stairs and plying sports
t Adjusted for differences in blood-pIeS stalUs cigarette smoking net gain in body-mass index since college and age of parental death
lWeighted vgbull
of survival gained by men expending 2000 or more kcal per week on exercise as compared with those expending less than 500 kcal per week The latter group might be considered likely to include most men who had selectively reduced their exercise levels beshycause of disease or premonitory symptoms As would be expected the survival difference (or number of years gained) was greatest between the extremes for levels of activity The third and fourth columns show the estimated results when all ~lumni are inshycluded with a single break point at 2000 kcal per week and the differences are still consistent though smaller In the fifth and sixth columns the group with the lowest activity (less than 500 kcal per week) is omitted yet the benefit of exercise is still evident
The data in the seventh and eighth columns showshying the survival advantages associated with vigorous sports parallel those in the third and fourth columns except in the age groups 65 and older in which indulshygence in vigorous sports is less likely In addition parshyticipation in vigorous sports would be expected to be most common among alumni expending 2000 or more kcal per week and this likely possibility may well acshycount for some of the contrast noted earlier regarding the first two columns in Table 4 if participating in vigorous sports is considered to enhance survival more than a high activity level In addition the influence of vigorous sports would probably be split in the fifth and sixth columns and so dampen the differences listed there as can be seen In view of these consistent patshyterns the data in Table 4 support the hypothesis that survival and hence longevity among the Harvard alumni has been influenced to an appreciable degree by both the total amount and the intensity of habitual physical activity engaged in throughout adult life The bottom line of Table 4 presents weighted avershy~ges for years gained up to the age of 80 as a result of Increased physical activity between the ages of 35 and
79 The survival estimates given in the table or othershywise calculated would vary depending on the definishytions or standards of physical activity employed in the analysis
Another assessment of the influence of physical acshytivity on longevity is shown in Table 5 in which the survival of active and sedentary alumni up to the age of 80 is estimated for five-year age groups after adshyjustment for differences in hypertension smoking low weight gain and early parental death Weigllted avershyages for the total age range are also shown For both active and sedentary men the percentage predicted to reach age 80 increases somewhat with age perhaps becausethe younger groups have yet to escape hazshyards of mortality that the older men have already avoided whereas the latter need to survive for fewer years to reach the age of 80 Nevertheless the physshyically active men had a continuing 10 percent advan-
Table 5 Proportions of Active and Sedentary Men Surviving to the Age of 80 Estimated from Harvard Alumni Mortality
1962 to 1978
AGE ATENny PHYSICALmiddotACTIVITY INOEX
(YR) 2000 lt2000
survivingt
35-39 682 578 40-44 685 582 45-49 690 592 50-54 699 598 55-59 711 610 60-64 730 634 65-69 764 676 70-74 824 746
75-79 918 850
35-791 697 598
Kilocalories expended per week in walking climbing tairs and playing sports
t Adjusted for differences in blood-pressure stalUs cigarette smoking net gain in body-mass mdex since college and age of parental death
jWeighted average
612 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
tage over the sedentary men until they reached the 65-to-69-year age bracket thereafter a tapering effect occurred because all the survivors from those groups had to reach the age of 80 within the follow-up period and hence their comparison was based on fewer years of mortality data It is possible too that contrasts between an active and sedentary life style were less marked in the older groups than in the younger groups Overall the table suggests a considerable gain in man-years of life for the habitually energetic alumshyni especially if any avoidable adverse characteristics such as cigarette smoking and obesity have been minimized
DISCUSSION
Survival is the result of a number of interacting influences (many hazardous in character or degree some beneficial in the same way) including physical activity and other life-style elements susceptible to opshytional adjustment Their combined effect determines whether increases in longevity are feasible or even deshysirable The findings reported here represent only a small part of the total picture but they suggest a proshytective effect of exercise against all-cause mortality in all age groups studied and therefore an indieationof additional years of life expectancy
The Harvard alumni may not be typical of the genshyeral population Their age-specific death rates from each major cause except suicide were roughly half the 1980 rates for white males in the United States (In contrast rates of self-destruction among the alumshyni 16- 18 were 50 percent higher than suicide rates in the general population) Yet the large alumni experience with delayed mortality for active men should imply increased life expectancy over that for sedentary men as the data demonstrate It is likely that some alumni increased their exercise reduced their smoking and received treatment for hypertension since the early 1960s when these characteristics were assessed Such changes would minimize the importance of these characteristics in the present findings The true force of the beneficial effects from physical activity nonshysmoking and control of hypertension would be even larger than that observed
Table 4 presents survival data in terms of definishytions of exercise that were necessarily limited by the design of the study to increases in kilocalories per week or to intensity as expressed by participation in vigorous sports The estimates of years gained reflect the experience of college alumni already recognized as long-lived whose economic status and behavior patterns differ from other populations in habitual physical exercise and other life-style elements Direct extrapolation to a general population should take these considerations into account
Since the data in Tables 4 and 5 represent only a portion of the total life experience of the study populashytion over time they may be viewed as a segment seen as through a window implying extensions that might
be estimated from the actual experience observed The differences in survival to the age of 80 between active and sedentary alumni may reflect a stage of optimal benefit from physical activity by the age of 65 and a rectangularization or converging trend may be estabshylished as the total life experience of the population of alumni approaches completion 19
Improvements in epidemiologic surveillance and medical management of such chronic disorders as hyshypertension abnormal blood lipid profiles and osteoshyporosis may defer mortality and extend survival However the effect of adequate physical exercise is partly independent of such influences and it countershyacts many adverse characteristics through metabolic and other processes20-25 Even when other procedures for health maintenance and disease prevention are deshyveloped to increase longevity the relevance of exercise is likely to remain
In studies of longevity the question arises whether the aging process is capable of modification but there is much uncertainty about the definitions of aging and of chronic disease Approaches to fend off disease or postpone aging are suggested or aging is regarded as an inexorable degenerative process that cannot be alshytered although perhaps chronic diseases may be avoided or deferred 2627 The present study considers chronic diseases but not the aging process itself
Extended follow-up of the Harvard alumni may reshyveal trends of aging or at least show at what stage of life the roles of exercise and10ther natural therapies become diminished The data in Tables 4 and 5 do offer some implications as a brief preliminary analysis of survival in various age and exercise groups In view of the data base and the consistency represented in the study it seems likely that the observed patterns are predictive
There is a widespread and longstanding popular belief that adequate physical exercise is necessary to preserve life and its desirable qualities into old age Discussions of this thesis date back to antiquity and have intensified in recent times 28
-40 The present study
adds new evidence to support this view
REFERENCES
1 Keys A Seven countries a multivariate analysis of death and coronary heart disease Cambridge Mass Harvard University Press 1980196-217276middot 8
2 Leon AS Blackburn H Physical inactivity In Kaplan NM Stamler I eds Prevention of coronary heart disease practical management of the risk factors Philadelphia WB Saunders 198386-97
3 Karvonen MJ Physical activity in work and leisure time in relation to cardiovascular diseases Ann Clin Res 1983 14SuppJ 34118-23
4 Morris IN Uses of epidemiology 3rd ed Edinburgh Churchill Livingshystone 1975163-5
5 Morris IN Kagan A Pattison DC Gardner MJlncidence and prediction of ischaemic heart-disease in London busmen Lancet 1966 2552-9
6 Paffenbarger RS Ir Brand RI Sholtz RI Jung DL Energy expenditure cigarette smoking and blood pressure level as related to death from specific diseases Am I Epidemiol 1978 10812-8
7 Paffenbarger RS Jr Hyde RT Wing AL Steinmetz CH A natural history of athleticism and cardiovascular health lAMA 1984 252491-5
8 Paffenbarger RS Ir Wing AL Hyde RT Physical activity as an index of heart attack risk in college alumni Am I Epidemiol 1978 108161shy75
613 Vol 314 No 10 PHYSICAL ACTIVITY MORTALITY AND LONGEVITY - PAFFENBARGER ET AL
9 Thomas GS Lee PR Franks P Paffenbarger RS Jr Exercise and health the evidence and the implications Cambridge Mass Oelgeschlager Gunn amp Hain 1981
10 Paffenbarger RS Jr Notkin J Krueger DE et al Chronic disease in former college students II Methods of study and observations on mortality from coronary heart disease Am J Public Health 1966 56962middot71
11 Passmore R Durnin JVGA Human energy expenditure Physiol Rev 1955 35801-40
12 Mantel N Chimiddotsquare tests with one degree of freedom extensions of the Mantel-Haenszel procedure J Am Stat Assoc 1963 58690middot700
13 Cox DR Regression models and life-tables J R Soc Biostat 1972 34187middot 220
14 Chang ImiddotM Gelman R Pagano M Corrected group prognostic curves and summary statistics J Chronic Dis 1982 35669-74
15 Paffenbarget RS Jr Wing AL Hyde RT Jung DL Physical activity and incidence of hypertension in college alumni Am J Epidemiol 1983 117245middot57
16 Paffenbarger RS Jr Asnes DP Chronic disease in former college students III Precursors of suicide in early and middle life Am J Public Health 1966 561026-36
17 Paffenbarger RS Jr Chronic disease in former college students VI Implicamiddot tiOlls for college health programs J Am College Health Assoc 1967 1651middot 5
IS Paffenbarger RS Jr King SH Wing AL Chronic disease in former college students IX Characteristics in youth that predispose to suicide and accidenshytal death in later life Am J Public Health 1969 5990()S
19 Fries IF Crapo LM Vitality and aging implications of the rectangular curve San Francisco WH Freeman 1981
20 Paffenbarger RS Jr Hyde RT Exercise as protection against heart attack N Engl J Med 1980 3021026-7
21 Wood PO Haskell WL BlairSN etal1ncreased exercise level and plasma lipoprotein concentrations a one-year randomized controlled study in sedmiddot entary middle-aged men Metabolism 1983 3231middot9
22 Morris IN Smith A eds Exercise health and medicine proceedings of the Lilleshall Conference London The Sports Council 1984
23 Leon AS ed Forum Exercise and healthPrev Med 1984 131middot99
24 Powell KE ed Workshop on epidemiologic and public health aspects of physical activity and exercise Public Health Rep 1985 100113-224
25 Hyde RT Paffenbarger RS Jr Epidemiologic uses of genera population assessments of physical activity patterns National Center for Health Statisshytics (in press)
26 Schneider EL Reed JD Jr Life extension N Engl J Med 1985 3121159shy68
27 Olshansky SJ Pursuing longevity delay vs elimination of degenerative diseases Am J Public Health 1985 75754-6
28 Ramazzini B Diseases of workers New York Hafner 1964 29 Guy WA Contributions to a knowledge of the influence of employments
upon health J R Stat Soc 1843 6197-21l 30 Smith E Report on the sanitary circumstances of tailors in London (Report
of the Medical Officer Privy Council) London Her Majestys Stationery Office 1864416-30
31 Morgan JE University oars being a critical enquiry into the after health of the men who rowed in the Oxford Ifld Cambridge hoat-race from the year 1829 to 1869 London Macmillan 1873
32 Hedley OF Analysis of 5116 deaths reported as due to acute coronary occlusion in Philadelphia 1933-1936 US WeekJyPublic Health Rep 1939 54972
33 Morris IN Heady JA Raffle PAB Roberts CG Parks JW Coronary heart disease and physical activity of work Lancet 1953 21053-7 1111-20
34 Montoye ill Van Huss WD Olson HW et al Longevity and morbidity of college athletes Lansing Mich Michigan State University 1957
35 Pomeroy WC White PD Coronary heart disease in former football players JAMA 1958 167711-4
36 Prout C Life expectancy of college oarsmen JAMA 1972 220 1709middot1 L 37 Belloc NB Relationship of health practices and mortality Prev Med 1973
267-81 38 Wiley JA Camacho TC Life-style and future health evidence from the
Alameda County study Prev Med 1980 91middot21 39 Breslow L Enstrom J Persistence of health habits and their relationship to
mortality Prev Med 1980 9469-83 40 Wingard DL Berkman LF Brand RJ A multivariate analysis of healthshy
related practices Am J Epidemiol 1982 116765-75
LARRY VELTMAN MD
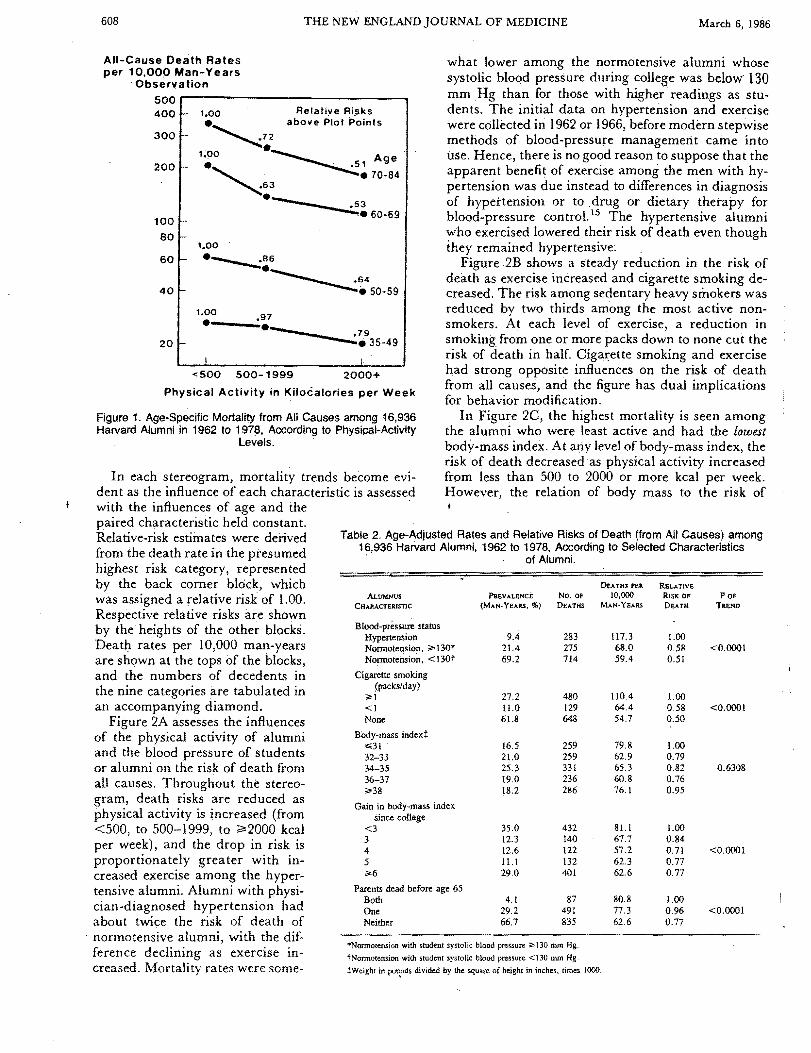
608 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
All-Cause Oeath Rates per 10000 Man-Years
Observation 500rl----------------------------~
400
300
200
100
80
60
40
20
bull Relative Risk s above PIOI Po
100
~72 Inls
100 bull ~1Age
63 bull 70-84
bull~360-69
100 86
-------- 64
----50-59
100 97---shylt500 500-1999 2000+
Physical Activity in Kilocalories per Week
Figure 1 Age-Specific Mortality from All Causes among 16936 Harvard Alumni in 1962 to 1978 According to Physical-Activity
LevelS
In each stereogram mortality trends become evishydent as the influence of each characteristic is assessed with the influences of age and the paired characteristic held constant Relative-risk estimates were derived from the death rate in the presumed highest risk category represented by the back corner block which was assigned a relative risk of l00 Respective relative risks are shown by the heights of the other blocks Death rates per 10000 man-years are shown at the tops of the blocks and the numbers of decedents in the nine categories are tabulated in an accompanying diamond
Figure 2A assesses the influences of the physical activity of alumni and the blood pressure of students or alumni on the risk of death from all causes Throughout the stereoshygram death risks are reduced as physical activity is increased (from lt500 to 500-1999 to ~2000 kcal per week) and the drop in risk is proportionately greater with inshycreased exercise among the hypershytensive alumni Alumni with physishycian-diagnosed hypertension had about twice the risk of death of
normotensive alumni with the difshyference declining as exercise inshycreased Mortality rates were someshy
what lower among the normotensive alumni whose systolic bloqd pressure during college was below 130 mm Hg than for those with higher readings as stushydents The initial data on hypertension and exercise were collected in 1962 or 1966 before modern stepwise methods of blood-pressure management came into use Hence there is no good reason to suppose that the apparent benefit of exercise among the men with hyshypertension was due instead to differences in diagnosis of hypertension or to drug or dietary therapy for blood-pressure controL 15 The hypertensive alumni who exercised lowered their risk of death even though they remained hypertensive~
Figure 2B shows a steady reduction in the risk of death as exercise increased and cigarette smoking deshycreased The risk among sedentary heavy smokers was reduced by two thirds among the most active nonshysmokers At each level of exercise a reduction in smoking from one or more packs down to none cut the risk of death in half Cigaxette smoking and exercise had strong opposite influences on the risk of death from all causes and the figure has dual implications for behavior modification
In Figure 2C the highest mortality is seen among the alumni who were least active and had the lowest body-mass index At ariy level of body-mass index the risk of death decreased as physical activity increased from less than 500 to 2000 or more kcal per week However the relation of body mass to the risk of
Table 2 Age-Adjusted Rates and Relative Risks ofDeath (from All Causes) among 16936 HarVard Alumni 1962 to 1978 According to Selected Characteristics
of Alumni
DEATHS PER RELATIVE
ALUMNUS PREVALENCE No OF 10000 RISK OF P OF
CHAMCfERISTle (MANmiddot YEARS ) DEATHS MAN-YEARS DEATH TREND
Blood-pressure status Hypertension Normotension 130 Normotension lt 130t
Cigarette smoking (packsday)
1 ltI None
BOdy-mass indexl 31 32-33 34-35 36-37 38
Gain in body-mass index since college
lt3 3 4 5 6
Parents dead before age 65 Both One Neither
94 283 1173 100 214 275 680 058 lt00001 692 714 594 051
272 480 1104 100 110 129 644 058 lt00001 618 648 547 050
165 259 798 100 210 259 629 079 253 331 653 082 06308 190 236 608 076 182 286 761 095
350 432 8Ll 100 123 140 677 084 126 122 572 071 lt00001 ILl 132 623 077 290 401 626 077
41 87 808 100 292 491 773 096 lt00001 667 835 626 077
Nonnotensicin with student systolic blood pressure ~ 130 mm Hg
tNonnotension with student systolic blood pressure lt130 mm Hg
~Weight in potnds divided by the square of height in inches times 1000
609
-0$00_
- ~~-1~O
Vol 314- No IO PHYSICAL ACTIVITY MORTALITY AND LONGEVITY - PAFFENBARGER ET AL
Figure 2 Relative Risks (RR) of Death from All Causes among 16936 Harvard Alumni in 1962 to 1978 According to Post-College Physical-Activity Levels and (A) Alumnus and Student Blood-Pressure Status (B) Alumnus Cigarette Smoking (C) Alumnus Body Weight for Height (D) Net Change in Body Weight since College (E) History of Early Parental Death and (F) Participation in
College Sports Blocks designate the relative risk based on age-adjusted death rates (numbers at top of blocks) per 10000 man-years of observation Death rates in the back corner blocks establish the relative risk of 100 Numbers of deaths are given in a corresponding key below each stereogram P values are based on trends of rates for one characteristic adjusted for differences in age and the paired characteristic
death was uneven and the trend was not significant when age and physical activity index were held conshystant There is perhaps some hint that the risk among the most active alumni tended to increase at both the high and low extremes of body-mass index Again as noted in the discussion of Table 2 the high risk for sedentary men with a low body-mass index may inshyvolve a wasting disease such as cancer whereas men with a high body-mass index may invite death from cardiovascular disease
Table 2 also shows that men with the least net gain in body-mass index after their physical examination in college had a greater risk of death than those who gained more This is also evident in Figure 2D where mortality can be seen to decline with an increasing net gain in body mass-index and also with increasing curshyrent physical activity Inactive status with a low weight gain may signify illness whereas the gain in body-mass index among the more active men may reflect healthy muscularity - ie body leanness rathshyer than body fat
As shown in Figure 2E the death of one or both parents before the age of 65 was related to an inshycreased risk of death among the alumni but the risk was lower among the physically active Early loss of parents may suggest a hereditary risk but it does not appear to influence the risk of death as strongly as
does lack of exercise Whether or not the two factors are interrelated both have significant effects on morshytality and adequate contemporary exercise may virtushyally offset the influence of early parental death
The pattern of relative risks in Figure 2F shows that the rate of death from any cause was reduced with increased physical activity by alumni but that the sports-activity level in their student days did not have a similar effect on subsequent mortality Former varsishyty athletes who exercised at less than 500 or at 2000 or more kcal per week in their post-college years had higher death rates (93 and 73 per 10000 man-years of observation respectively) than those who reported continuing moderate exercise at 500 to 1999 kcal per week (61 per 10000 man-years) The most active group of former varsity players with a higher mortalshyity includes those who died from cancer or cardiovasshycularcauses Although in this pattern former varsity athletes seem to have had a higher risk than their less athletic classmates the chart overall shows a consisshytent pattern of benefit from habitual exercise by alumshyni Evidently inheritance of a sturdy constitution (as implied by varsity athletic status) is less important to longevity than continuation of adequate life-time exerCIse
Each stereogram in Figure 2 shows that the physical activity of alumni had an independent and significant
A B
~ 00 ~
075 shy 01gt shy
0$0 cSO shy
015 --
Alumrul Physlcol etlyU
ftld tKcIWbullbulltt ~~I~ -0001 fI 0001
D E
ARA~
100 100
07S shy075
aso 00
~oaI Oili
000 000 shy
SCtdy fn 11IwJI Physical ActivUy -- Gain Sinc Collaga PhyiealAcUvHy
thdu KeIWutt IweighOHighI2 nd KuilWbullbullk) 0001 ~ 0001 p 0001
AlutlUHJ
c
100 --- shy 015
oso -
025
Alumnut Cigarttbullbull Per Oy
p OOOt
F
AR
100
05
OliO gt
01$ ~
Au Phyak1 Activity
Indbullbull KcaUWbullbullle1 0001
610 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
inverse relation to mortality Moreover adequate exshyercise enhanced the mortality reduction associated with favorable levels of the other post-college characshyteristics studied
Table 3 shows relative and attributable risks of death from any cause which were derived from a multivariate analysis and computed for the presence versus the absence of each adverse characteristic with adjustment for the differences in age and each of the other characteristics listed 13 The relative risk of 131 associated with a sedentary life style signifies that men expending fewer than 2000 kcal per week had a 31 percent higher risk of death than more active men Likewise men with physician-diagnosed hypertension had a 73 percent higher risk than normotensive men and cigarette smokers had a 76 percent higher risk than nonsmokers Men who had a net weight gain of less than 7 kg (IS Ib) after college were at a 33 percent greater risk than men who gained more The alumni who had lost one or both patients before the age of 65 had a 15 percent higher risk of death than their classshymates whose parents had survived to age 65 or older The five characteristics assessed in the table or the basic mechanisms of causation they represent conshytribute independently to the risk of death from all causes
The clinical attributable risks listed in Table 3 are estimates of potential percentage reductions in the risk of death for persons who exchange the adverse characteristic for a more healthful characteristic Sedshyentary men who become more active might reduce their risk of d~ath by 24 percent If hypertensive men could obtain normal blood pressure they would have 42 percent less risk reformed cigarette smokers 43 percent less Men whose net weight gain since college was below 7 kg might have had a 25 percent lower risk of death if they had gained more If men who lost one or both parents early had had parents living to age 65 or older their own risk of death might have been 13 percent less The clinical percentage estimates in Tashyble 3 are not additive
The community attributable risks in Table 3 are
estimates that take prevalence into account They inshydicate what percentage of risk might be spared in a community or population if the adverse characterisshytics listed were converted to more favorable characshyteristics The risk of death might be reduced by 16 percent in the alumni population if every man had exercised at 2000 or more kcal per week Abolition of hypertension might cut the community death rate anshyother 6 percent total abstinence from cigarettes anshyother 23 percent a greater net weight gain 10 percent more and survival of both parents to age 65 or older another 5 percent These estimates though hypothetishycal are additive so thlttt if all five adverse characterisshytics were eliminated the total risk of death in the community of alumni might be cut by more than half - ie there might have been 60 percent fewer deaths during the study period (1962 to 1978) or a loss of only 551 alumni instead of 1413
Relative and attributable risks of death from carshydiovascular disease in association with similar adverse characteristics (sedentariness hypertension smoking overweight and parental coronary heart disease) among the alumni were of the same general order of magnishytude as risks of all-cause mortality After allowance for age and each other adverse characteristic sedentary alumni had a 31 percent higher risk of cardiovascular mortality than more physically active men hypertensive men had a 118 percent greater risk than normotensive men cigarette smokers had an 84 percen greater risk than nonsmokers heavier men had an 18 percent higher risk than leaner men and alumni with a parenshytal history of coronary heart disease had a 33 percent higher risk of dying from cardiovascular disease than classmates whose parents were free of coronary heart disease The attributable-risk estimates (community) corresponding to these same characteristics were 16 9 25 6 and II percent respectively In combination they indicated that there might have been 67 percent fewer deaths from cardiovascular disease during the study period in the absence of all five characteristics or a loss of only 196 alumni instead of the 640 who died from underlying cardiovascular disease
As shown in Table 4 the mortalshyity and survival experience of the
Table 3 Relative and Attributable Risks of Death (from All Causes) among 16936 Harvard alumni during the 16-year Harvard Alumni 1962 to 1978 According to Selected Adverse Characteristics follow-up period were used to deshy
velop estimates of years of added CLINICAL COMMUNITY
life gained (up to age 80) from anALUMNUS PREVALENCE RELATIVE RISK AlTRIBJTABLE A lTlUBUTABLE
CHARACTERISTIC (MAN-YEAlIS ) OF DEATHt P VALUE ~K( ~K() active life style rather than an inacshySedentary life stylet 620 131 (115-149) 00001 236 161 tive life style The results are tabushyHypertensionsect 94 1 73 (14S-201) lt00001 421 64 lated for five-year age groups at the Cigarette smoking~ 382 176 (156-199) lt00001 432 225 start of follow-up and selected measshyLow net weight gainll 351 133 (117-151) 00001 246 103 ures of physical activity The data Early parental death 333 U5 (102-130) 00248 131 48 are shown with and without adshybullAdjusted for differences in age and each of the other characteristics listed
tFigures in parentheses are 95 percent confidence intervals
Energy expenditure of lt2000 kcal per week in walking climbing stairs and playing sports
sectPhysician-dignosed
Any amount
IINet gain in body-mass index of lt3 units since college ie bull nO more than 7 leg (15 Ib)
bull One or both parents dead before he age of 65
justment for differences in bloodshypressure status cigarette use net gain in body-mass index and pashyrental death The first two columns under physical-activity show the crude and adjusted estimated years
611 VoL 314 NoO PHYSICAL ACTIVITY MORTALITY AND LONGEVITY PAFFENBARGER ET AL
Table 4 Added life from an Active life Style in Men Jp to the Age of 80 Estimated from Harvard Alumni Mortality 1962 to 1978
PHYSICAL-ACTIVITY INDEXmiddot VIGOItOUS SPOIlTS ILAY
AGE AT 2000 VS 2000 VS 2000 VS PusENT vs ENTIlY lt500 lt2000 500-1999 ABSENT
(n) CltUDE AllJUSTEot CRUDE AllJUSTEOt CRUDE ADJUSTEOt CRUOE ADJUSTEot
esrimaJed no of years gained
35-39 264 251 166 150 126 107 166 155 4)-44 248 234 146 139 104 099 154 145 45-49 232 20 24 110 080 067 138 123 50-54 237 211 135 120 093 081 140 132 55-59 225 202 127 113 087 075 125 121 60-64 198 175 104 093 065 057 100 095 65-69 164 135 082 067 048 036 070 055 70-74 094 072 057 044 042 middot031 011 -011 75-79 035 042 029 030 026 024 001
35-79i 233 215 138 125 099 086 137 128
Kilocalories experuled per week in walking climbing stairs and plying sports
t Adjusted for differences in blood-pIeS stalUs cigarette smoking net gain in body-mass index since college and age of parental death
lWeighted vgbull
of survival gained by men expending 2000 or more kcal per week on exercise as compared with those expending less than 500 kcal per week The latter group might be considered likely to include most men who had selectively reduced their exercise levels beshycause of disease or premonitory symptoms As would be expected the survival difference (or number of years gained) was greatest between the extremes for levels of activity The third and fourth columns show the estimated results when all ~lumni are inshycluded with a single break point at 2000 kcal per week and the differences are still consistent though smaller In the fifth and sixth columns the group with the lowest activity (less than 500 kcal per week) is omitted yet the benefit of exercise is still evident
The data in the seventh and eighth columns showshying the survival advantages associated with vigorous sports parallel those in the third and fourth columns except in the age groups 65 and older in which indulshygence in vigorous sports is less likely In addition parshyticipation in vigorous sports would be expected to be most common among alumni expending 2000 or more kcal per week and this likely possibility may well acshycount for some of the contrast noted earlier regarding the first two columns in Table 4 if participating in vigorous sports is considered to enhance survival more than a high activity level In addition the influence of vigorous sports would probably be split in the fifth and sixth columns and so dampen the differences listed there as can be seen In view of these consistent patshyterns the data in Table 4 support the hypothesis that survival and hence longevity among the Harvard alumni has been influenced to an appreciable degree by both the total amount and the intensity of habitual physical activity engaged in throughout adult life The bottom line of Table 4 presents weighted avershy~ges for years gained up to the age of 80 as a result of Increased physical activity between the ages of 35 and
79 The survival estimates given in the table or othershywise calculated would vary depending on the definishytions or standards of physical activity employed in the analysis
Another assessment of the influence of physical acshytivity on longevity is shown in Table 5 in which the survival of active and sedentary alumni up to the age of 80 is estimated for five-year age groups after adshyjustment for differences in hypertension smoking low weight gain and early parental death Weigllted avershyages for the total age range are also shown For both active and sedentary men the percentage predicted to reach age 80 increases somewhat with age perhaps becausethe younger groups have yet to escape hazshyards of mortality that the older men have already avoided whereas the latter need to survive for fewer years to reach the age of 80 Nevertheless the physshyically active men had a continuing 10 percent advan-
Table 5 Proportions of Active and Sedentary Men Surviving to the Age of 80 Estimated from Harvard Alumni Mortality
1962 to 1978
AGE ATENny PHYSICALmiddotACTIVITY INOEX
(YR) 2000 lt2000
survivingt
35-39 682 578 40-44 685 582 45-49 690 592 50-54 699 598 55-59 711 610 60-64 730 634 65-69 764 676 70-74 824 746
75-79 918 850
35-791 697 598
Kilocalories expended per week in walking climbing tairs and playing sports
t Adjusted for differences in blood-pressure stalUs cigarette smoking net gain in body-mass mdex since college and age of parental death
jWeighted average
612 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
tage over the sedentary men until they reached the 65-to-69-year age bracket thereafter a tapering effect occurred because all the survivors from those groups had to reach the age of 80 within the follow-up period and hence their comparison was based on fewer years of mortality data It is possible too that contrasts between an active and sedentary life style were less marked in the older groups than in the younger groups Overall the table suggests a considerable gain in man-years of life for the habitually energetic alumshyni especially if any avoidable adverse characteristics such as cigarette smoking and obesity have been minimized
DISCUSSION
Survival is the result of a number of interacting influences (many hazardous in character or degree some beneficial in the same way) including physical activity and other life-style elements susceptible to opshytional adjustment Their combined effect determines whether increases in longevity are feasible or even deshysirable The findings reported here represent only a small part of the total picture but they suggest a proshytective effect of exercise against all-cause mortality in all age groups studied and therefore an indieationof additional years of life expectancy
The Harvard alumni may not be typical of the genshyeral population Their age-specific death rates from each major cause except suicide were roughly half the 1980 rates for white males in the United States (In contrast rates of self-destruction among the alumshyni 16- 18 were 50 percent higher than suicide rates in the general population) Yet the large alumni experience with delayed mortality for active men should imply increased life expectancy over that for sedentary men as the data demonstrate It is likely that some alumni increased their exercise reduced their smoking and received treatment for hypertension since the early 1960s when these characteristics were assessed Such changes would minimize the importance of these characteristics in the present findings The true force of the beneficial effects from physical activity nonshysmoking and control of hypertension would be even larger than that observed
Table 4 presents survival data in terms of definishytions of exercise that were necessarily limited by the design of the study to increases in kilocalories per week or to intensity as expressed by participation in vigorous sports The estimates of years gained reflect the experience of college alumni already recognized as long-lived whose economic status and behavior patterns differ from other populations in habitual physical exercise and other life-style elements Direct extrapolation to a general population should take these considerations into account
Since the data in Tables 4 and 5 represent only a portion of the total life experience of the study populashytion over time they may be viewed as a segment seen as through a window implying extensions that might
be estimated from the actual experience observed The differences in survival to the age of 80 between active and sedentary alumni may reflect a stage of optimal benefit from physical activity by the age of 65 and a rectangularization or converging trend may be estabshylished as the total life experience of the population of alumni approaches completion 19
Improvements in epidemiologic surveillance and medical management of such chronic disorders as hyshypertension abnormal blood lipid profiles and osteoshyporosis may defer mortality and extend survival However the effect of adequate physical exercise is partly independent of such influences and it countershyacts many adverse characteristics through metabolic and other processes20-25 Even when other procedures for health maintenance and disease prevention are deshyveloped to increase longevity the relevance of exercise is likely to remain
In studies of longevity the question arises whether the aging process is capable of modification but there is much uncertainty about the definitions of aging and of chronic disease Approaches to fend off disease or postpone aging are suggested or aging is regarded as an inexorable degenerative process that cannot be alshytered although perhaps chronic diseases may be avoided or deferred 2627 The present study considers chronic diseases but not the aging process itself
Extended follow-up of the Harvard alumni may reshyveal trends of aging or at least show at what stage of life the roles of exercise and10ther natural therapies become diminished The data in Tables 4 and 5 do offer some implications as a brief preliminary analysis of survival in various age and exercise groups In view of the data base and the consistency represented in the study it seems likely that the observed patterns are predictive
There is a widespread and longstanding popular belief that adequate physical exercise is necessary to preserve life and its desirable qualities into old age Discussions of this thesis date back to antiquity and have intensified in recent times 28
-40 The present study
adds new evidence to support this view
REFERENCES
1 Keys A Seven countries a multivariate analysis of death and coronary heart disease Cambridge Mass Harvard University Press 1980196-217276middot 8
2 Leon AS Blackburn H Physical inactivity In Kaplan NM Stamler I eds Prevention of coronary heart disease practical management of the risk factors Philadelphia WB Saunders 198386-97
3 Karvonen MJ Physical activity in work and leisure time in relation to cardiovascular diseases Ann Clin Res 1983 14SuppJ 34118-23
4 Morris IN Uses of epidemiology 3rd ed Edinburgh Churchill Livingshystone 1975163-5
5 Morris IN Kagan A Pattison DC Gardner MJlncidence and prediction of ischaemic heart-disease in London busmen Lancet 1966 2552-9
6 Paffenbarger RS Ir Brand RI Sholtz RI Jung DL Energy expenditure cigarette smoking and blood pressure level as related to death from specific diseases Am I Epidemiol 1978 10812-8
7 Paffenbarger RS Jr Hyde RT Wing AL Steinmetz CH A natural history of athleticism and cardiovascular health lAMA 1984 252491-5
8 Paffenbarger RS Ir Wing AL Hyde RT Physical activity as an index of heart attack risk in college alumni Am I Epidemiol 1978 108161shy75
613 Vol 314 No 10 PHYSICAL ACTIVITY MORTALITY AND LONGEVITY - PAFFENBARGER ET AL
9 Thomas GS Lee PR Franks P Paffenbarger RS Jr Exercise and health the evidence and the implications Cambridge Mass Oelgeschlager Gunn amp Hain 1981
10 Paffenbarger RS Jr Notkin J Krueger DE et al Chronic disease in former college students II Methods of study and observations on mortality from coronary heart disease Am J Public Health 1966 56962middot71
11 Passmore R Durnin JVGA Human energy expenditure Physiol Rev 1955 35801-40
12 Mantel N Chimiddotsquare tests with one degree of freedom extensions of the Mantel-Haenszel procedure J Am Stat Assoc 1963 58690middot700
13 Cox DR Regression models and life-tables J R Soc Biostat 1972 34187middot 220
14 Chang ImiddotM Gelman R Pagano M Corrected group prognostic curves and summary statistics J Chronic Dis 1982 35669-74
15 Paffenbarget RS Jr Wing AL Hyde RT Jung DL Physical activity and incidence of hypertension in college alumni Am J Epidemiol 1983 117245middot57
16 Paffenbarger RS Jr Asnes DP Chronic disease in former college students III Precursors of suicide in early and middle life Am J Public Health 1966 561026-36
17 Paffenbarger RS Jr Chronic disease in former college students VI Implicamiddot tiOlls for college health programs J Am College Health Assoc 1967 1651middot 5
IS Paffenbarger RS Jr King SH Wing AL Chronic disease in former college students IX Characteristics in youth that predispose to suicide and accidenshytal death in later life Am J Public Health 1969 5990()S
19 Fries IF Crapo LM Vitality and aging implications of the rectangular curve San Francisco WH Freeman 1981
20 Paffenbarger RS Jr Hyde RT Exercise as protection against heart attack N Engl J Med 1980 3021026-7
21 Wood PO Haskell WL BlairSN etal1ncreased exercise level and plasma lipoprotein concentrations a one-year randomized controlled study in sedmiddot entary middle-aged men Metabolism 1983 3231middot9
22 Morris IN Smith A eds Exercise health and medicine proceedings of the Lilleshall Conference London The Sports Council 1984
23 Leon AS ed Forum Exercise and healthPrev Med 1984 131middot99
24 Powell KE ed Workshop on epidemiologic and public health aspects of physical activity and exercise Public Health Rep 1985 100113-224
25 Hyde RT Paffenbarger RS Jr Epidemiologic uses of genera population assessments of physical activity patterns National Center for Health Statisshytics (in press)
26 Schneider EL Reed JD Jr Life extension N Engl J Med 1985 3121159shy68
27 Olshansky SJ Pursuing longevity delay vs elimination of degenerative diseases Am J Public Health 1985 75754-6
28 Ramazzini B Diseases of workers New York Hafner 1964 29 Guy WA Contributions to a knowledge of the influence of employments
upon health J R Stat Soc 1843 6197-21l 30 Smith E Report on the sanitary circumstances of tailors in London (Report
of the Medical Officer Privy Council) London Her Majestys Stationery Office 1864416-30
31 Morgan JE University oars being a critical enquiry into the after health of the men who rowed in the Oxford Ifld Cambridge hoat-race from the year 1829 to 1869 London Macmillan 1873
32 Hedley OF Analysis of 5116 deaths reported as due to acute coronary occlusion in Philadelphia 1933-1936 US WeekJyPublic Health Rep 1939 54972
33 Morris IN Heady JA Raffle PAB Roberts CG Parks JW Coronary heart disease and physical activity of work Lancet 1953 21053-7 1111-20
34 Montoye ill Van Huss WD Olson HW et al Longevity and morbidity of college athletes Lansing Mich Michigan State University 1957
35 Pomeroy WC White PD Coronary heart disease in former football players JAMA 1958 167711-4
36 Prout C Life expectancy of college oarsmen JAMA 1972 220 1709middot1 L 37 Belloc NB Relationship of health practices and mortality Prev Med 1973
267-81 38 Wiley JA Camacho TC Life-style and future health evidence from the
Alameda County study Prev Med 1980 91middot21 39 Breslow L Enstrom J Persistence of health habits and their relationship to
mortality Prev Med 1980 9469-83 40 Wingard DL Berkman LF Brand RJ A multivariate analysis of healthshy
related practices Am J Epidemiol 1982 116765-75
LARRY VELTMAN MD

609
-0$00_
- ~~-1~O
Vol 314- No IO PHYSICAL ACTIVITY MORTALITY AND LONGEVITY - PAFFENBARGER ET AL
Figure 2 Relative Risks (RR) of Death from All Causes among 16936 Harvard Alumni in 1962 to 1978 According to Post-College Physical-Activity Levels and (A) Alumnus and Student Blood-Pressure Status (B) Alumnus Cigarette Smoking (C) Alumnus Body Weight for Height (D) Net Change in Body Weight since College (E) History of Early Parental Death and (F) Participation in
College Sports Blocks designate the relative risk based on age-adjusted death rates (numbers at top of blocks) per 10000 man-years of observation Death rates in the back corner blocks establish the relative risk of 100 Numbers of deaths are given in a corresponding key below each stereogram P values are based on trends of rates for one characteristic adjusted for differences in age and the paired characteristic
death was uneven and the trend was not significant when age and physical activity index were held conshystant There is perhaps some hint that the risk among the most active alumni tended to increase at both the high and low extremes of body-mass index Again as noted in the discussion of Table 2 the high risk for sedentary men with a low body-mass index may inshyvolve a wasting disease such as cancer whereas men with a high body-mass index may invite death from cardiovascular disease
Table 2 also shows that men with the least net gain in body-mass index after their physical examination in college had a greater risk of death than those who gained more This is also evident in Figure 2D where mortality can be seen to decline with an increasing net gain in body mass-index and also with increasing curshyrent physical activity Inactive status with a low weight gain may signify illness whereas the gain in body-mass index among the more active men may reflect healthy muscularity - ie body leanness rathshyer than body fat
As shown in Figure 2E the death of one or both parents before the age of 65 was related to an inshycreased risk of death among the alumni but the risk was lower among the physically active Early loss of parents may suggest a hereditary risk but it does not appear to influence the risk of death as strongly as
does lack of exercise Whether or not the two factors are interrelated both have significant effects on morshytality and adequate contemporary exercise may virtushyally offset the influence of early parental death
The pattern of relative risks in Figure 2F shows that the rate of death from any cause was reduced with increased physical activity by alumni but that the sports-activity level in their student days did not have a similar effect on subsequent mortality Former varsishyty athletes who exercised at less than 500 or at 2000 or more kcal per week in their post-college years had higher death rates (93 and 73 per 10000 man-years of observation respectively) than those who reported continuing moderate exercise at 500 to 1999 kcal per week (61 per 10000 man-years) The most active group of former varsity players with a higher mortalshyity includes those who died from cancer or cardiovasshycularcauses Although in this pattern former varsity athletes seem to have had a higher risk than their less athletic classmates the chart overall shows a consisshytent pattern of benefit from habitual exercise by alumshyni Evidently inheritance of a sturdy constitution (as implied by varsity athletic status) is less important to longevity than continuation of adequate life-time exerCIse
Each stereogram in Figure 2 shows that the physical activity of alumni had an independent and significant
A B
~ 00 ~
075 shy 01gt shy
0$0 cSO shy
015 --
Alumrul Physlcol etlyU
ftld tKcIWbullbulltt ~~I~ -0001 fI 0001
D E
ARA~
100 100
07S shy075
aso 00
~oaI Oili
000 000 shy
SCtdy fn 11IwJI Physical ActivUy -- Gain Sinc Collaga PhyiealAcUvHy
thdu KeIWutt IweighOHighI2 nd KuilWbullbullk) 0001 ~ 0001 p 0001
AlutlUHJ
c
100 --- shy 015
oso -
025
Alumnut Cigarttbullbull Per Oy
p OOOt
F
AR
100
05
OliO gt
01$ ~
Au Phyak1 Activity
Indbullbull KcaUWbullbullle1 0001
610 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
inverse relation to mortality Moreover adequate exshyercise enhanced the mortality reduction associated with favorable levels of the other post-college characshyteristics studied
Table 3 shows relative and attributable risks of death from any cause which were derived from a multivariate analysis and computed for the presence versus the absence of each adverse characteristic with adjustment for the differences in age and each of the other characteristics listed 13 The relative risk of 131 associated with a sedentary life style signifies that men expending fewer than 2000 kcal per week had a 31 percent higher risk of death than more active men Likewise men with physician-diagnosed hypertension had a 73 percent higher risk than normotensive men and cigarette smokers had a 76 percent higher risk than nonsmokers Men who had a net weight gain of less than 7 kg (IS Ib) after college were at a 33 percent greater risk than men who gained more The alumni who had lost one or both patients before the age of 65 had a 15 percent higher risk of death than their classshymates whose parents had survived to age 65 or older The five characteristics assessed in the table or the basic mechanisms of causation they represent conshytribute independently to the risk of death from all causes
The clinical attributable risks listed in Table 3 are estimates of potential percentage reductions in the risk of death for persons who exchange the adverse characteristic for a more healthful characteristic Sedshyentary men who become more active might reduce their risk of d~ath by 24 percent If hypertensive men could obtain normal blood pressure they would have 42 percent less risk reformed cigarette smokers 43 percent less Men whose net weight gain since college was below 7 kg might have had a 25 percent lower risk of death if they had gained more If men who lost one or both parents early had had parents living to age 65 or older their own risk of death might have been 13 percent less The clinical percentage estimates in Tashyble 3 are not additive
The community attributable risks in Table 3 are
estimates that take prevalence into account They inshydicate what percentage of risk might be spared in a community or population if the adverse characterisshytics listed were converted to more favorable characshyteristics The risk of death might be reduced by 16 percent in the alumni population if every man had exercised at 2000 or more kcal per week Abolition of hypertension might cut the community death rate anshyother 6 percent total abstinence from cigarettes anshyother 23 percent a greater net weight gain 10 percent more and survival of both parents to age 65 or older another 5 percent These estimates though hypothetishycal are additive so thlttt if all five adverse characterisshytics were eliminated the total risk of death in the community of alumni might be cut by more than half - ie there might have been 60 percent fewer deaths during the study period (1962 to 1978) or a loss of only 551 alumni instead of 1413
Relative and attributable risks of death from carshydiovascular disease in association with similar adverse characteristics (sedentariness hypertension smoking overweight and parental coronary heart disease) among the alumni were of the same general order of magnishytude as risks of all-cause mortality After allowance for age and each other adverse characteristic sedentary alumni had a 31 percent higher risk of cardiovascular mortality than more physically active men hypertensive men had a 118 percent greater risk than normotensive men cigarette smokers had an 84 percen greater risk than nonsmokers heavier men had an 18 percent higher risk than leaner men and alumni with a parenshytal history of coronary heart disease had a 33 percent higher risk of dying from cardiovascular disease than classmates whose parents were free of coronary heart disease The attributable-risk estimates (community) corresponding to these same characteristics were 16 9 25 6 and II percent respectively In combination they indicated that there might have been 67 percent fewer deaths from cardiovascular disease during the study period in the absence of all five characteristics or a loss of only 196 alumni instead of the 640 who died from underlying cardiovascular disease
As shown in Table 4 the mortalshyity and survival experience of the
Table 3 Relative and Attributable Risks of Death (from All Causes) among 16936 Harvard alumni during the 16-year Harvard Alumni 1962 to 1978 According to Selected Adverse Characteristics follow-up period were used to deshy
velop estimates of years of added CLINICAL COMMUNITY
life gained (up to age 80) from anALUMNUS PREVALENCE RELATIVE RISK AlTRIBJTABLE A lTlUBUTABLE
CHARACTERISTIC (MAN-YEAlIS ) OF DEATHt P VALUE ~K( ~K() active life style rather than an inacshySedentary life stylet 620 131 (115-149) 00001 236 161 tive life style The results are tabushyHypertensionsect 94 1 73 (14S-201) lt00001 421 64 lated for five-year age groups at the Cigarette smoking~ 382 176 (156-199) lt00001 432 225 start of follow-up and selected measshyLow net weight gainll 351 133 (117-151) 00001 246 103 ures of physical activity The data Early parental death 333 U5 (102-130) 00248 131 48 are shown with and without adshybullAdjusted for differences in age and each of the other characteristics listed
tFigures in parentheses are 95 percent confidence intervals
Energy expenditure of lt2000 kcal per week in walking climbing stairs and playing sports
sectPhysician-dignosed
Any amount
IINet gain in body-mass index of lt3 units since college ie bull nO more than 7 leg (15 Ib)
bull One or both parents dead before he age of 65
justment for differences in bloodshypressure status cigarette use net gain in body-mass index and pashyrental death The first two columns under physical-activity show the crude and adjusted estimated years
611 VoL 314 NoO PHYSICAL ACTIVITY MORTALITY AND LONGEVITY PAFFENBARGER ET AL
Table 4 Added life from an Active life Style in Men Jp to the Age of 80 Estimated from Harvard Alumni Mortality 1962 to 1978
PHYSICAL-ACTIVITY INDEXmiddot VIGOItOUS SPOIlTS ILAY
AGE AT 2000 VS 2000 VS 2000 VS PusENT vs ENTIlY lt500 lt2000 500-1999 ABSENT
(n) CltUDE AllJUSTEot CRUDE AllJUSTEOt CRUDE ADJUSTEOt CRUOE ADJUSTEot
esrimaJed no of years gained
35-39 264 251 166 150 126 107 166 155 4)-44 248 234 146 139 104 099 154 145 45-49 232 20 24 110 080 067 138 123 50-54 237 211 135 120 093 081 140 132 55-59 225 202 127 113 087 075 125 121 60-64 198 175 104 093 065 057 100 095 65-69 164 135 082 067 048 036 070 055 70-74 094 072 057 044 042 middot031 011 -011 75-79 035 042 029 030 026 024 001
35-79i 233 215 138 125 099 086 137 128
Kilocalories experuled per week in walking climbing stairs and plying sports
t Adjusted for differences in blood-pIeS stalUs cigarette smoking net gain in body-mass index since college and age of parental death
lWeighted vgbull
of survival gained by men expending 2000 or more kcal per week on exercise as compared with those expending less than 500 kcal per week The latter group might be considered likely to include most men who had selectively reduced their exercise levels beshycause of disease or premonitory symptoms As would be expected the survival difference (or number of years gained) was greatest between the extremes for levels of activity The third and fourth columns show the estimated results when all ~lumni are inshycluded with a single break point at 2000 kcal per week and the differences are still consistent though smaller In the fifth and sixth columns the group with the lowest activity (less than 500 kcal per week) is omitted yet the benefit of exercise is still evident
The data in the seventh and eighth columns showshying the survival advantages associated with vigorous sports parallel those in the third and fourth columns except in the age groups 65 and older in which indulshygence in vigorous sports is less likely In addition parshyticipation in vigorous sports would be expected to be most common among alumni expending 2000 or more kcal per week and this likely possibility may well acshycount for some of the contrast noted earlier regarding the first two columns in Table 4 if participating in vigorous sports is considered to enhance survival more than a high activity level In addition the influence of vigorous sports would probably be split in the fifth and sixth columns and so dampen the differences listed there as can be seen In view of these consistent patshyterns the data in Table 4 support the hypothesis that survival and hence longevity among the Harvard alumni has been influenced to an appreciable degree by both the total amount and the intensity of habitual physical activity engaged in throughout adult life The bottom line of Table 4 presents weighted avershy~ges for years gained up to the age of 80 as a result of Increased physical activity between the ages of 35 and
79 The survival estimates given in the table or othershywise calculated would vary depending on the definishytions or standards of physical activity employed in the analysis
Another assessment of the influence of physical acshytivity on longevity is shown in Table 5 in which the survival of active and sedentary alumni up to the age of 80 is estimated for five-year age groups after adshyjustment for differences in hypertension smoking low weight gain and early parental death Weigllted avershyages for the total age range are also shown For both active and sedentary men the percentage predicted to reach age 80 increases somewhat with age perhaps becausethe younger groups have yet to escape hazshyards of mortality that the older men have already avoided whereas the latter need to survive for fewer years to reach the age of 80 Nevertheless the physshyically active men had a continuing 10 percent advan-
Table 5 Proportions of Active and Sedentary Men Surviving to the Age of 80 Estimated from Harvard Alumni Mortality
1962 to 1978
AGE ATENny PHYSICALmiddotACTIVITY INOEX
(YR) 2000 lt2000
survivingt
35-39 682 578 40-44 685 582 45-49 690 592 50-54 699 598 55-59 711 610 60-64 730 634 65-69 764 676 70-74 824 746
75-79 918 850
35-791 697 598
Kilocalories expended per week in walking climbing tairs and playing sports
t Adjusted for differences in blood-pressure stalUs cigarette smoking net gain in body-mass mdex since college and age of parental death
jWeighted average
612 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
tage over the sedentary men until they reached the 65-to-69-year age bracket thereafter a tapering effect occurred because all the survivors from those groups had to reach the age of 80 within the follow-up period and hence their comparison was based on fewer years of mortality data It is possible too that contrasts between an active and sedentary life style were less marked in the older groups than in the younger groups Overall the table suggests a considerable gain in man-years of life for the habitually energetic alumshyni especially if any avoidable adverse characteristics such as cigarette smoking and obesity have been minimized
DISCUSSION
Survival is the result of a number of interacting influences (many hazardous in character or degree some beneficial in the same way) including physical activity and other life-style elements susceptible to opshytional adjustment Their combined effect determines whether increases in longevity are feasible or even deshysirable The findings reported here represent only a small part of the total picture but they suggest a proshytective effect of exercise against all-cause mortality in all age groups studied and therefore an indieationof additional years of life expectancy
The Harvard alumni may not be typical of the genshyeral population Their age-specific death rates from each major cause except suicide were roughly half the 1980 rates for white males in the United States (In contrast rates of self-destruction among the alumshyni 16- 18 were 50 percent higher than suicide rates in the general population) Yet the large alumni experience with delayed mortality for active men should imply increased life expectancy over that for sedentary men as the data demonstrate It is likely that some alumni increased their exercise reduced their smoking and received treatment for hypertension since the early 1960s when these characteristics were assessed Such changes would minimize the importance of these characteristics in the present findings The true force of the beneficial effects from physical activity nonshysmoking and control of hypertension would be even larger than that observed
Table 4 presents survival data in terms of definishytions of exercise that were necessarily limited by the design of the study to increases in kilocalories per week or to intensity as expressed by participation in vigorous sports The estimates of years gained reflect the experience of college alumni already recognized as long-lived whose economic status and behavior patterns differ from other populations in habitual physical exercise and other life-style elements Direct extrapolation to a general population should take these considerations into account
Since the data in Tables 4 and 5 represent only a portion of the total life experience of the study populashytion over time they may be viewed as a segment seen as through a window implying extensions that might
be estimated from the actual experience observed The differences in survival to the age of 80 between active and sedentary alumni may reflect a stage of optimal benefit from physical activity by the age of 65 and a rectangularization or converging trend may be estabshylished as the total life experience of the population of alumni approaches completion 19
Improvements in epidemiologic surveillance and medical management of such chronic disorders as hyshypertension abnormal blood lipid profiles and osteoshyporosis may defer mortality and extend survival However the effect of adequate physical exercise is partly independent of such influences and it countershyacts many adverse characteristics through metabolic and other processes20-25 Even when other procedures for health maintenance and disease prevention are deshyveloped to increase longevity the relevance of exercise is likely to remain
In studies of longevity the question arises whether the aging process is capable of modification but there is much uncertainty about the definitions of aging and of chronic disease Approaches to fend off disease or postpone aging are suggested or aging is regarded as an inexorable degenerative process that cannot be alshytered although perhaps chronic diseases may be avoided or deferred 2627 The present study considers chronic diseases but not the aging process itself
Extended follow-up of the Harvard alumni may reshyveal trends of aging or at least show at what stage of life the roles of exercise and10ther natural therapies become diminished The data in Tables 4 and 5 do offer some implications as a brief preliminary analysis of survival in various age and exercise groups In view of the data base and the consistency represented in the study it seems likely that the observed patterns are predictive
There is a widespread and longstanding popular belief that adequate physical exercise is necessary to preserve life and its desirable qualities into old age Discussions of this thesis date back to antiquity and have intensified in recent times 28
-40 The present study
adds new evidence to support this view
REFERENCES
1 Keys A Seven countries a multivariate analysis of death and coronary heart disease Cambridge Mass Harvard University Press 1980196-217276middot 8
2 Leon AS Blackburn H Physical inactivity In Kaplan NM Stamler I eds Prevention of coronary heart disease practical management of the risk factors Philadelphia WB Saunders 198386-97
3 Karvonen MJ Physical activity in work and leisure time in relation to cardiovascular diseases Ann Clin Res 1983 14SuppJ 34118-23
4 Morris IN Uses of epidemiology 3rd ed Edinburgh Churchill Livingshystone 1975163-5
5 Morris IN Kagan A Pattison DC Gardner MJlncidence and prediction of ischaemic heart-disease in London busmen Lancet 1966 2552-9
6 Paffenbarger RS Ir Brand RI Sholtz RI Jung DL Energy expenditure cigarette smoking and blood pressure level as related to death from specific diseases Am I Epidemiol 1978 10812-8
7 Paffenbarger RS Jr Hyde RT Wing AL Steinmetz CH A natural history of athleticism and cardiovascular health lAMA 1984 252491-5
8 Paffenbarger RS Ir Wing AL Hyde RT Physical activity as an index of heart attack risk in college alumni Am I Epidemiol 1978 108161shy75
613 Vol 314 No 10 PHYSICAL ACTIVITY MORTALITY AND LONGEVITY - PAFFENBARGER ET AL
9 Thomas GS Lee PR Franks P Paffenbarger RS Jr Exercise and health the evidence and the implications Cambridge Mass Oelgeschlager Gunn amp Hain 1981
10 Paffenbarger RS Jr Notkin J Krueger DE et al Chronic disease in former college students II Methods of study and observations on mortality from coronary heart disease Am J Public Health 1966 56962middot71
11 Passmore R Durnin JVGA Human energy expenditure Physiol Rev 1955 35801-40
12 Mantel N Chimiddotsquare tests with one degree of freedom extensions of the Mantel-Haenszel procedure J Am Stat Assoc 1963 58690middot700
13 Cox DR Regression models and life-tables J R Soc Biostat 1972 34187middot 220
14 Chang ImiddotM Gelman R Pagano M Corrected group prognostic curves and summary statistics J Chronic Dis 1982 35669-74
15 Paffenbarget RS Jr Wing AL Hyde RT Jung DL Physical activity and incidence of hypertension in college alumni Am J Epidemiol 1983 117245middot57
16 Paffenbarger RS Jr Asnes DP Chronic disease in former college students III Precursors of suicide in early and middle life Am J Public Health 1966 561026-36
17 Paffenbarger RS Jr Chronic disease in former college students VI Implicamiddot tiOlls for college health programs J Am College Health Assoc 1967 1651middot 5
IS Paffenbarger RS Jr King SH Wing AL Chronic disease in former college students IX Characteristics in youth that predispose to suicide and accidenshytal death in later life Am J Public Health 1969 5990()S
19 Fries IF Crapo LM Vitality and aging implications of the rectangular curve San Francisco WH Freeman 1981
20 Paffenbarger RS Jr Hyde RT Exercise as protection against heart attack N Engl J Med 1980 3021026-7
21 Wood PO Haskell WL BlairSN etal1ncreased exercise level and plasma lipoprotein concentrations a one-year randomized controlled study in sedmiddot entary middle-aged men Metabolism 1983 3231middot9
22 Morris IN Smith A eds Exercise health and medicine proceedings of the Lilleshall Conference London The Sports Council 1984
23 Leon AS ed Forum Exercise and healthPrev Med 1984 131middot99
24 Powell KE ed Workshop on epidemiologic and public health aspects of physical activity and exercise Public Health Rep 1985 100113-224
25 Hyde RT Paffenbarger RS Jr Epidemiologic uses of genera population assessments of physical activity patterns National Center for Health Statisshytics (in press)
26 Schneider EL Reed JD Jr Life extension N Engl J Med 1985 3121159shy68
27 Olshansky SJ Pursuing longevity delay vs elimination of degenerative diseases Am J Public Health 1985 75754-6
28 Ramazzini B Diseases of workers New York Hafner 1964 29 Guy WA Contributions to a knowledge of the influence of employments
upon health J R Stat Soc 1843 6197-21l 30 Smith E Report on the sanitary circumstances of tailors in London (Report
of the Medical Officer Privy Council) London Her Majestys Stationery Office 1864416-30
31 Morgan JE University oars being a critical enquiry into the after health of the men who rowed in the Oxford Ifld Cambridge hoat-race from the year 1829 to 1869 London Macmillan 1873
32 Hedley OF Analysis of 5116 deaths reported as due to acute coronary occlusion in Philadelphia 1933-1936 US WeekJyPublic Health Rep 1939 54972
33 Morris IN Heady JA Raffle PAB Roberts CG Parks JW Coronary heart disease and physical activity of work Lancet 1953 21053-7 1111-20
34 Montoye ill Van Huss WD Olson HW et al Longevity and morbidity of college athletes Lansing Mich Michigan State University 1957
35 Pomeroy WC White PD Coronary heart disease in former football players JAMA 1958 167711-4
36 Prout C Life expectancy of college oarsmen JAMA 1972 220 1709middot1 L 37 Belloc NB Relationship of health practices and mortality Prev Med 1973
267-81 38 Wiley JA Camacho TC Life-style and future health evidence from the
Alameda County study Prev Med 1980 91middot21 39 Breslow L Enstrom J Persistence of health habits and their relationship to
mortality Prev Med 1980 9469-83 40 Wingard DL Berkman LF Brand RJ A multivariate analysis of healthshy
related practices Am J Epidemiol 1982 116765-75
LARRY VELTMAN MD

610 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
inverse relation to mortality Moreover adequate exshyercise enhanced the mortality reduction associated with favorable levels of the other post-college characshyteristics studied
Table 3 shows relative and attributable risks of death from any cause which were derived from a multivariate analysis and computed for the presence versus the absence of each adverse characteristic with adjustment for the differences in age and each of the other characteristics listed 13 The relative risk of 131 associated with a sedentary life style signifies that men expending fewer than 2000 kcal per week had a 31 percent higher risk of death than more active men Likewise men with physician-diagnosed hypertension had a 73 percent higher risk than normotensive men and cigarette smokers had a 76 percent higher risk than nonsmokers Men who had a net weight gain of less than 7 kg (IS Ib) after college were at a 33 percent greater risk than men who gained more The alumni who had lost one or both patients before the age of 65 had a 15 percent higher risk of death than their classshymates whose parents had survived to age 65 or older The five characteristics assessed in the table or the basic mechanisms of causation they represent conshytribute independently to the risk of death from all causes
The clinical attributable risks listed in Table 3 are estimates of potential percentage reductions in the risk of death for persons who exchange the adverse characteristic for a more healthful characteristic Sedshyentary men who become more active might reduce their risk of d~ath by 24 percent If hypertensive men could obtain normal blood pressure they would have 42 percent less risk reformed cigarette smokers 43 percent less Men whose net weight gain since college was below 7 kg might have had a 25 percent lower risk of death if they had gained more If men who lost one or both parents early had had parents living to age 65 or older their own risk of death might have been 13 percent less The clinical percentage estimates in Tashyble 3 are not additive
The community attributable risks in Table 3 are
estimates that take prevalence into account They inshydicate what percentage of risk might be spared in a community or population if the adverse characterisshytics listed were converted to more favorable characshyteristics The risk of death might be reduced by 16 percent in the alumni population if every man had exercised at 2000 or more kcal per week Abolition of hypertension might cut the community death rate anshyother 6 percent total abstinence from cigarettes anshyother 23 percent a greater net weight gain 10 percent more and survival of both parents to age 65 or older another 5 percent These estimates though hypothetishycal are additive so thlttt if all five adverse characterisshytics were eliminated the total risk of death in the community of alumni might be cut by more than half - ie there might have been 60 percent fewer deaths during the study period (1962 to 1978) or a loss of only 551 alumni instead of 1413
Relative and attributable risks of death from carshydiovascular disease in association with similar adverse characteristics (sedentariness hypertension smoking overweight and parental coronary heart disease) among the alumni were of the same general order of magnishytude as risks of all-cause mortality After allowance for age and each other adverse characteristic sedentary alumni had a 31 percent higher risk of cardiovascular mortality than more physically active men hypertensive men had a 118 percent greater risk than normotensive men cigarette smokers had an 84 percen greater risk than nonsmokers heavier men had an 18 percent higher risk than leaner men and alumni with a parenshytal history of coronary heart disease had a 33 percent higher risk of dying from cardiovascular disease than classmates whose parents were free of coronary heart disease The attributable-risk estimates (community) corresponding to these same characteristics were 16 9 25 6 and II percent respectively In combination they indicated that there might have been 67 percent fewer deaths from cardiovascular disease during the study period in the absence of all five characteristics or a loss of only 196 alumni instead of the 640 who died from underlying cardiovascular disease
As shown in Table 4 the mortalshyity and survival experience of the
Table 3 Relative and Attributable Risks of Death (from All Causes) among 16936 Harvard alumni during the 16-year Harvard Alumni 1962 to 1978 According to Selected Adverse Characteristics follow-up period were used to deshy
velop estimates of years of added CLINICAL COMMUNITY
life gained (up to age 80) from anALUMNUS PREVALENCE RELATIVE RISK AlTRIBJTABLE A lTlUBUTABLE
CHARACTERISTIC (MAN-YEAlIS ) OF DEATHt P VALUE ~K( ~K() active life style rather than an inacshySedentary life stylet 620 131 (115-149) 00001 236 161 tive life style The results are tabushyHypertensionsect 94 1 73 (14S-201) lt00001 421 64 lated for five-year age groups at the Cigarette smoking~ 382 176 (156-199) lt00001 432 225 start of follow-up and selected measshyLow net weight gainll 351 133 (117-151) 00001 246 103 ures of physical activity The data Early parental death 333 U5 (102-130) 00248 131 48 are shown with and without adshybullAdjusted for differences in age and each of the other characteristics listed
tFigures in parentheses are 95 percent confidence intervals
Energy expenditure of lt2000 kcal per week in walking climbing stairs and playing sports
sectPhysician-dignosed
Any amount
IINet gain in body-mass index of lt3 units since college ie bull nO more than 7 leg (15 Ib)
bull One or both parents dead before he age of 65
justment for differences in bloodshypressure status cigarette use net gain in body-mass index and pashyrental death The first two columns under physical-activity show the crude and adjusted estimated years
611 VoL 314 NoO PHYSICAL ACTIVITY MORTALITY AND LONGEVITY PAFFENBARGER ET AL
Table 4 Added life from an Active life Style in Men Jp to the Age of 80 Estimated from Harvard Alumni Mortality 1962 to 1978
PHYSICAL-ACTIVITY INDEXmiddot VIGOItOUS SPOIlTS ILAY
AGE AT 2000 VS 2000 VS 2000 VS PusENT vs ENTIlY lt500 lt2000 500-1999 ABSENT
(n) CltUDE AllJUSTEot CRUDE AllJUSTEOt CRUDE ADJUSTEOt CRUOE ADJUSTEot
esrimaJed no of years gained
35-39 264 251 166 150 126 107 166 155 4)-44 248 234 146 139 104 099 154 145 45-49 232 20 24 110 080 067 138 123 50-54 237 211 135 120 093 081 140 132 55-59 225 202 127 113 087 075 125 121 60-64 198 175 104 093 065 057 100 095 65-69 164 135 082 067 048 036 070 055 70-74 094 072 057 044 042 middot031 011 -011 75-79 035 042 029 030 026 024 001
35-79i 233 215 138 125 099 086 137 128
Kilocalories experuled per week in walking climbing stairs and plying sports
t Adjusted for differences in blood-pIeS stalUs cigarette smoking net gain in body-mass index since college and age of parental death
lWeighted vgbull
of survival gained by men expending 2000 or more kcal per week on exercise as compared with those expending less than 500 kcal per week The latter group might be considered likely to include most men who had selectively reduced their exercise levels beshycause of disease or premonitory symptoms As would be expected the survival difference (or number of years gained) was greatest between the extremes for levels of activity The third and fourth columns show the estimated results when all ~lumni are inshycluded with a single break point at 2000 kcal per week and the differences are still consistent though smaller In the fifth and sixth columns the group with the lowest activity (less than 500 kcal per week) is omitted yet the benefit of exercise is still evident
The data in the seventh and eighth columns showshying the survival advantages associated with vigorous sports parallel those in the third and fourth columns except in the age groups 65 and older in which indulshygence in vigorous sports is less likely In addition parshyticipation in vigorous sports would be expected to be most common among alumni expending 2000 or more kcal per week and this likely possibility may well acshycount for some of the contrast noted earlier regarding the first two columns in Table 4 if participating in vigorous sports is considered to enhance survival more than a high activity level In addition the influence of vigorous sports would probably be split in the fifth and sixth columns and so dampen the differences listed there as can be seen In view of these consistent patshyterns the data in Table 4 support the hypothesis that survival and hence longevity among the Harvard alumni has been influenced to an appreciable degree by both the total amount and the intensity of habitual physical activity engaged in throughout adult life The bottom line of Table 4 presents weighted avershy~ges for years gained up to the age of 80 as a result of Increased physical activity between the ages of 35 and
79 The survival estimates given in the table or othershywise calculated would vary depending on the definishytions or standards of physical activity employed in the analysis
Another assessment of the influence of physical acshytivity on longevity is shown in Table 5 in which the survival of active and sedentary alumni up to the age of 80 is estimated for five-year age groups after adshyjustment for differences in hypertension smoking low weight gain and early parental death Weigllted avershyages for the total age range are also shown For both active and sedentary men the percentage predicted to reach age 80 increases somewhat with age perhaps becausethe younger groups have yet to escape hazshyards of mortality that the older men have already avoided whereas the latter need to survive for fewer years to reach the age of 80 Nevertheless the physshyically active men had a continuing 10 percent advan-
Table 5 Proportions of Active and Sedentary Men Surviving to the Age of 80 Estimated from Harvard Alumni Mortality
1962 to 1978
AGE ATENny PHYSICALmiddotACTIVITY INOEX
(YR) 2000 lt2000
survivingt
35-39 682 578 40-44 685 582 45-49 690 592 50-54 699 598 55-59 711 610 60-64 730 634 65-69 764 676 70-74 824 746
75-79 918 850
35-791 697 598
Kilocalories expended per week in walking climbing tairs and playing sports
t Adjusted for differences in blood-pressure stalUs cigarette smoking net gain in body-mass mdex since college and age of parental death
jWeighted average
612 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
tage over the sedentary men until they reached the 65-to-69-year age bracket thereafter a tapering effect occurred because all the survivors from those groups had to reach the age of 80 within the follow-up period and hence their comparison was based on fewer years of mortality data It is possible too that contrasts between an active and sedentary life style were less marked in the older groups than in the younger groups Overall the table suggests a considerable gain in man-years of life for the habitually energetic alumshyni especially if any avoidable adverse characteristics such as cigarette smoking and obesity have been minimized
DISCUSSION
Survival is the result of a number of interacting influences (many hazardous in character or degree some beneficial in the same way) including physical activity and other life-style elements susceptible to opshytional adjustment Their combined effect determines whether increases in longevity are feasible or even deshysirable The findings reported here represent only a small part of the total picture but they suggest a proshytective effect of exercise against all-cause mortality in all age groups studied and therefore an indieationof additional years of life expectancy
The Harvard alumni may not be typical of the genshyeral population Their age-specific death rates from each major cause except suicide were roughly half the 1980 rates for white males in the United States (In contrast rates of self-destruction among the alumshyni 16- 18 were 50 percent higher than suicide rates in the general population) Yet the large alumni experience with delayed mortality for active men should imply increased life expectancy over that for sedentary men as the data demonstrate It is likely that some alumni increased their exercise reduced their smoking and received treatment for hypertension since the early 1960s when these characteristics were assessed Such changes would minimize the importance of these characteristics in the present findings The true force of the beneficial effects from physical activity nonshysmoking and control of hypertension would be even larger than that observed
Table 4 presents survival data in terms of definishytions of exercise that were necessarily limited by the design of the study to increases in kilocalories per week or to intensity as expressed by participation in vigorous sports The estimates of years gained reflect the experience of college alumni already recognized as long-lived whose economic status and behavior patterns differ from other populations in habitual physical exercise and other life-style elements Direct extrapolation to a general population should take these considerations into account
Since the data in Tables 4 and 5 represent only a portion of the total life experience of the study populashytion over time they may be viewed as a segment seen as through a window implying extensions that might
be estimated from the actual experience observed The differences in survival to the age of 80 between active and sedentary alumni may reflect a stage of optimal benefit from physical activity by the age of 65 and a rectangularization or converging trend may be estabshylished as the total life experience of the population of alumni approaches completion 19
Improvements in epidemiologic surveillance and medical management of such chronic disorders as hyshypertension abnormal blood lipid profiles and osteoshyporosis may defer mortality and extend survival However the effect of adequate physical exercise is partly independent of such influences and it countershyacts many adverse characteristics through metabolic and other processes20-25 Even when other procedures for health maintenance and disease prevention are deshyveloped to increase longevity the relevance of exercise is likely to remain
In studies of longevity the question arises whether the aging process is capable of modification but there is much uncertainty about the definitions of aging and of chronic disease Approaches to fend off disease or postpone aging are suggested or aging is regarded as an inexorable degenerative process that cannot be alshytered although perhaps chronic diseases may be avoided or deferred 2627 The present study considers chronic diseases but not the aging process itself
Extended follow-up of the Harvard alumni may reshyveal trends of aging or at least show at what stage of life the roles of exercise and10ther natural therapies become diminished The data in Tables 4 and 5 do offer some implications as a brief preliminary analysis of survival in various age and exercise groups In view of the data base and the consistency represented in the study it seems likely that the observed patterns are predictive
There is a widespread and longstanding popular belief that adequate physical exercise is necessary to preserve life and its desirable qualities into old age Discussions of this thesis date back to antiquity and have intensified in recent times 28
-40 The present study
adds new evidence to support this view
REFERENCES
1 Keys A Seven countries a multivariate analysis of death and coronary heart disease Cambridge Mass Harvard University Press 1980196-217276middot 8
2 Leon AS Blackburn H Physical inactivity In Kaplan NM Stamler I eds Prevention of coronary heart disease practical management of the risk factors Philadelphia WB Saunders 198386-97
3 Karvonen MJ Physical activity in work and leisure time in relation to cardiovascular diseases Ann Clin Res 1983 14SuppJ 34118-23
4 Morris IN Uses of epidemiology 3rd ed Edinburgh Churchill Livingshystone 1975163-5
5 Morris IN Kagan A Pattison DC Gardner MJlncidence and prediction of ischaemic heart-disease in London busmen Lancet 1966 2552-9
6 Paffenbarger RS Ir Brand RI Sholtz RI Jung DL Energy expenditure cigarette smoking and blood pressure level as related to death from specific diseases Am I Epidemiol 1978 10812-8
7 Paffenbarger RS Jr Hyde RT Wing AL Steinmetz CH A natural history of athleticism and cardiovascular health lAMA 1984 252491-5
8 Paffenbarger RS Ir Wing AL Hyde RT Physical activity as an index of heart attack risk in college alumni Am I Epidemiol 1978 108161shy75
613 Vol 314 No 10 PHYSICAL ACTIVITY MORTALITY AND LONGEVITY - PAFFENBARGER ET AL
9 Thomas GS Lee PR Franks P Paffenbarger RS Jr Exercise and health the evidence and the implications Cambridge Mass Oelgeschlager Gunn amp Hain 1981
10 Paffenbarger RS Jr Notkin J Krueger DE et al Chronic disease in former college students II Methods of study and observations on mortality from coronary heart disease Am J Public Health 1966 56962middot71
11 Passmore R Durnin JVGA Human energy expenditure Physiol Rev 1955 35801-40
12 Mantel N Chimiddotsquare tests with one degree of freedom extensions of the Mantel-Haenszel procedure J Am Stat Assoc 1963 58690middot700
13 Cox DR Regression models and life-tables J R Soc Biostat 1972 34187middot 220
14 Chang ImiddotM Gelman R Pagano M Corrected group prognostic curves and summary statistics J Chronic Dis 1982 35669-74
15 Paffenbarget RS Jr Wing AL Hyde RT Jung DL Physical activity and incidence of hypertension in college alumni Am J Epidemiol 1983 117245middot57
16 Paffenbarger RS Jr Asnes DP Chronic disease in former college students III Precursors of suicide in early and middle life Am J Public Health 1966 561026-36
17 Paffenbarger RS Jr Chronic disease in former college students VI Implicamiddot tiOlls for college health programs J Am College Health Assoc 1967 1651middot 5
IS Paffenbarger RS Jr King SH Wing AL Chronic disease in former college students IX Characteristics in youth that predispose to suicide and accidenshytal death in later life Am J Public Health 1969 5990()S
19 Fries IF Crapo LM Vitality and aging implications of the rectangular curve San Francisco WH Freeman 1981
20 Paffenbarger RS Jr Hyde RT Exercise as protection against heart attack N Engl J Med 1980 3021026-7
21 Wood PO Haskell WL BlairSN etal1ncreased exercise level and plasma lipoprotein concentrations a one-year randomized controlled study in sedmiddot entary middle-aged men Metabolism 1983 3231middot9
22 Morris IN Smith A eds Exercise health and medicine proceedings of the Lilleshall Conference London The Sports Council 1984
23 Leon AS ed Forum Exercise and healthPrev Med 1984 131middot99
24 Powell KE ed Workshop on epidemiologic and public health aspects of physical activity and exercise Public Health Rep 1985 100113-224
25 Hyde RT Paffenbarger RS Jr Epidemiologic uses of genera population assessments of physical activity patterns National Center for Health Statisshytics (in press)
26 Schneider EL Reed JD Jr Life extension N Engl J Med 1985 3121159shy68
27 Olshansky SJ Pursuing longevity delay vs elimination of degenerative diseases Am J Public Health 1985 75754-6
28 Ramazzini B Diseases of workers New York Hafner 1964 29 Guy WA Contributions to a knowledge of the influence of employments
upon health J R Stat Soc 1843 6197-21l 30 Smith E Report on the sanitary circumstances of tailors in London (Report
of the Medical Officer Privy Council) London Her Majestys Stationery Office 1864416-30
31 Morgan JE University oars being a critical enquiry into the after health of the men who rowed in the Oxford Ifld Cambridge hoat-race from the year 1829 to 1869 London Macmillan 1873
32 Hedley OF Analysis of 5116 deaths reported as due to acute coronary occlusion in Philadelphia 1933-1936 US WeekJyPublic Health Rep 1939 54972
33 Morris IN Heady JA Raffle PAB Roberts CG Parks JW Coronary heart disease and physical activity of work Lancet 1953 21053-7 1111-20
34 Montoye ill Van Huss WD Olson HW et al Longevity and morbidity of college athletes Lansing Mich Michigan State University 1957
35 Pomeroy WC White PD Coronary heart disease in former football players JAMA 1958 167711-4
36 Prout C Life expectancy of college oarsmen JAMA 1972 220 1709middot1 L 37 Belloc NB Relationship of health practices and mortality Prev Med 1973
267-81 38 Wiley JA Camacho TC Life-style and future health evidence from the
Alameda County study Prev Med 1980 91middot21 39 Breslow L Enstrom J Persistence of health habits and their relationship to
mortality Prev Med 1980 9469-83 40 Wingard DL Berkman LF Brand RJ A multivariate analysis of healthshy
related practices Am J Epidemiol 1982 116765-75
LARRY VELTMAN MD

611 VoL 314 NoO PHYSICAL ACTIVITY MORTALITY AND LONGEVITY PAFFENBARGER ET AL
Table 4 Added life from an Active life Style in Men Jp to the Age of 80 Estimated from Harvard Alumni Mortality 1962 to 1978
PHYSICAL-ACTIVITY INDEXmiddot VIGOItOUS SPOIlTS ILAY
AGE AT 2000 VS 2000 VS 2000 VS PusENT vs ENTIlY lt500 lt2000 500-1999 ABSENT
(n) CltUDE AllJUSTEot CRUDE AllJUSTEOt CRUDE ADJUSTEOt CRUOE ADJUSTEot
esrimaJed no of years gained
35-39 264 251 166 150 126 107 166 155 4)-44 248 234 146 139 104 099 154 145 45-49 232 20 24 110 080 067 138 123 50-54 237 211 135 120 093 081 140 132 55-59 225 202 127 113 087 075 125 121 60-64 198 175 104 093 065 057 100 095 65-69 164 135 082 067 048 036 070 055 70-74 094 072 057 044 042 middot031 011 -011 75-79 035 042 029 030 026 024 001
35-79i 233 215 138 125 099 086 137 128
Kilocalories experuled per week in walking climbing stairs and plying sports
t Adjusted for differences in blood-pIeS stalUs cigarette smoking net gain in body-mass index since college and age of parental death
lWeighted vgbull
of survival gained by men expending 2000 or more kcal per week on exercise as compared with those expending less than 500 kcal per week The latter group might be considered likely to include most men who had selectively reduced their exercise levels beshycause of disease or premonitory symptoms As would be expected the survival difference (or number of years gained) was greatest between the extremes for levels of activity The third and fourth columns show the estimated results when all ~lumni are inshycluded with a single break point at 2000 kcal per week and the differences are still consistent though smaller In the fifth and sixth columns the group with the lowest activity (less than 500 kcal per week) is omitted yet the benefit of exercise is still evident
The data in the seventh and eighth columns showshying the survival advantages associated with vigorous sports parallel those in the third and fourth columns except in the age groups 65 and older in which indulshygence in vigorous sports is less likely In addition parshyticipation in vigorous sports would be expected to be most common among alumni expending 2000 or more kcal per week and this likely possibility may well acshycount for some of the contrast noted earlier regarding the first two columns in Table 4 if participating in vigorous sports is considered to enhance survival more than a high activity level In addition the influence of vigorous sports would probably be split in the fifth and sixth columns and so dampen the differences listed there as can be seen In view of these consistent patshyterns the data in Table 4 support the hypothesis that survival and hence longevity among the Harvard alumni has been influenced to an appreciable degree by both the total amount and the intensity of habitual physical activity engaged in throughout adult life The bottom line of Table 4 presents weighted avershy~ges for years gained up to the age of 80 as a result of Increased physical activity between the ages of 35 and
79 The survival estimates given in the table or othershywise calculated would vary depending on the definishytions or standards of physical activity employed in the analysis
Another assessment of the influence of physical acshytivity on longevity is shown in Table 5 in which the survival of active and sedentary alumni up to the age of 80 is estimated for five-year age groups after adshyjustment for differences in hypertension smoking low weight gain and early parental death Weigllted avershyages for the total age range are also shown For both active and sedentary men the percentage predicted to reach age 80 increases somewhat with age perhaps becausethe younger groups have yet to escape hazshyards of mortality that the older men have already avoided whereas the latter need to survive for fewer years to reach the age of 80 Nevertheless the physshyically active men had a continuing 10 percent advan-
Table 5 Proportions of Active and Sedentary Men Surviving to the Age of 80 Estimated from Harvard Alumni Mortality
1962 to 1978
AGE ATENny PHYSICALmiddotACTIVITY INOEX
(YR) 2000 lt2000
survivingt
35-39 682 578 40-44 685 582 45-49 690 592 50-54 699 598 55-59 711 610 60-64 730 634 65-69 764 676 70-74 824 746
75-79 918 850
35-791 697 598
Kilocalories expended per week in walking climbing tairs and playing sports
t Adjusted for differences in blood-pressure stalUs cigarette smoking net gain in body-mass mdex since college and age of parental death
jWeighted average
612 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
tage over the sedentary men until they reached the 65-to-69-year age bracket thereafter a tapering effect occurred because all the survivors from those groups had to reach the age of 80 within the follow-up period and hence their comparison was based on fewer years of mortality data It is possible too that contrasts between an active and sedentary life style were less marked in the older groups than in the younger groups Overall the table suggests a considerable gain in man-years of life for the habitually energetic alumshyni especially if any avoidable adverse characteristics such as cigarette smoking and obesity have been minimized
DISCUSSION
Survival is the result of a number of interacting influences (many hazardous in character or degree some beneficial in the same way) including physical activity and other life-style elements susceptible to opshytional adjustment Their combined effect determines whether increases in longevity are feasible or even deshysirable The findings reported here represent only a small part of the total picture but they suggest a proshytective effect of exercise against all-cause mortality in all age groups studied and therefore an indieationof additional years of life expectancy
The Harvard alumni may not be typical of the genshyeral population Their age-specific death rates from each major cause except suicide were roughly half the 1980 rates for white males in the United States (In contrast rates of self-destruction among the alumshyni 16- 18 were 50 percent higher than suicide rates in the general population) Yet the large alumni experience with delayed mortality for active men should imply increased life expectancy over that for sedentary men as the data demonstrate It is likely that some alumni increased their exercise reduced their smoking and received treatment for hypertension since the early 1960s when these characteristics were assessed Such changes would minimize the importance of these characteristics in the present findings The true force of the beneficial effects from physical activity nonshysmoking and control of hypertension would be even larger than that observed
Table 4 presents survival data in terms of definishytions of exercise that were necessarily limited by the design of the study to increases in kilocalories per week or to intensity as expressed by participation in vigorous sports The estimates of years gained reflect the experience of college alumni already recognized as long-lived whose economic status and behavior patterns differ from other populations in habitual physical exercise and other life-style elements Direct extrapolation to a general population should take these considerations into account
Since the data in Tables 4 and 5 represent only a portion of the total life experience of the study populashytion over time they may be viewed as a segment seen as through a window implying extensions that might
be estimated from the actual experience observed The differences in survival to the age of 80 between active and sedentary alumni may reflect a stage of optimal benefit from physical activity by the age of 65 and a rectangularization or converging trend may be estabshylished as the total life experience of the population of alumni approaches completion 19
Improvements in epidemiologic surveillance and medical management of such chronic disorders as hyshypertension abnormal blood lipid profiles and osteoshyporosis may defer mortality and extend survival However the effect of adequate physical exercise is partly independent of such influences and it countershyacts many adverse characteristics through metabolic and other processes20-25 Even when other procedures for health maintenance and disease prevention are deshyveloped to increase longevity the relevance of exercise is likely to remain
In studies of longevity the question arises whether the aging process is capable of modification but there is much uncertainty about the definitions of aging and of chronic disease Approaches to fend off disease or postpone aging are suggested or aging is regarded as an inexorable degenerative process that cannot be alshytered although perhaps chronic diseases may be avoided or deferred 2627 The present study considers chronic diseases but not the aging process itself
Extended follow-up of the Harvard alumni may reshyveal trends of aging or at least show at what stage of life the roles of exercise and10ther natural therapies become diminished The data in Tables 4 and 5 do offer some implications as a brief preliminary analysis of survival in various age and exercise groups In view of the data base and the consistency represented in the study it seems likely that the observed patterns are predictive
There is a widespread and longstanding popular belief that adequate physical exercise is necessary to preserve life and its desirable qualities into old age Discussions of this thesis date back to antiquity and have intensified in recent times 28
-40 The present study
adds new evidence to support this view
REFERENCES
1 Keys A Seven countries a multivariate analysis of death and coronary heart disease Cambridge Mass Harvard University Press 1980196-217276middot 8
2 Leon AS Blackburn H Physical inactivity In Kaplan NM Stamler I eds Prevention of coronary heart disease practical management of the risk factors Philadelphia WB Saunders 198386-97
3 Karvonen MJ Physical activity in work and leisure time in relation to cardiovascular diseases Ann Clin Res 1983 14SuppJ 34118-23
4 Morris IN Uses of epidemiology 3rd ed Edinburgh Churchill Livingshystone 1975163-5
5 Morris IN Kagan A Pattison DC Gardner MJlncidence and prediction of ischaemic heart-disease in London busmen Lancet 1966 2552-9
6 Paffenbarger RS Ir Brand RI Sholtz RI Jung DL Energy expenditure cigarette smoking and blood pressure level as related to death from specific diseases Am I Epidemiol 1978 10812-8
7 Paffenbarger RS Jr Hyde RT Wing AL Steinmetz CH A natural history of athleticism and cardiovascular health lAMA 1984 252491-5
8 Paffenbarger RS Ir Wing AL Hyde RT Physical activity as an index of heart attack risk in college alumni Am I Epidemiol 1978 108161shy75
613 Vol 314 No 10 PHYSICAL ACTIVITY MORTALITY AND LONGEVITY - PAFFENBARGER ET AL
9 Thomas GS Lee PR Franks P Paffenbarger RS Jr Exercise and health the evidence and the implications Cambridge Mass Oelgeschlager Gunn amp Hain 1981
10 Paffenbarger RS Jr Notkin J Krueger DE et al Chronic disease in former college students II Methods of study and observations on mortality from coronary heart disease Am J Public Health 1966 56962middot71
11 Passmore R Durnin JVGA Human energy expenditure Physiol Rev 1955 35801-40
12 Mantel N Chimiddotsquare tests with one degree of freedom extensions of the Mantel-Haenszel procedure J Am Stat Assoc 1963 58690middot700
13 Cox DR Regression models and life-tables J R Soc Biostat 1972 34187middot 220
14 Chang ImiddotM Gelman R Pagano M Corrected group prognostic curves and summary statistics J Chronic Dis 1982 35669-74
15 Paffenbarget RS Jr Wing AL Hyde RT Jung DL Physical activity and incidence of hypertension in college alumni Am J Epidemiol 1983 117245middot57
16 Paffenbarger RS Jr Asnes DP Chronic disease in former college students III Precursors of suicide in early and middle life Am J Public Health 1966 561026-36
17 Paffenbarger RS Jr Chronic disease in former college students VI Implicamiddot tiOlls for college health programs J Am College Health Assoc 1967 1651middot 5
IS Paffenbarger RS Jr King SH Wing AL Chronic disease in former college students IX Characteristics in youth that predispose to suicide and accidenshytal death in later life Am J Public Health 1969 5990()S
19 Fries IF Crapo LM Vitality and aging implications of the rectangular curve San Francisco WH Freeman 1981
20 Paffenbarger RS Jr Hyde RT Exercise as protection against heart attack N Engl J Med 1980 3021026-7
21 Wood PO Haskell WL BlairSN etal1ncreased exercise level and plasma lipoprotein concentrations a one-year randomized controlled study in sedmiddot entary middle-aged men Metabolism 1983 3231middot9
22 Morris IN Smith A eds Exercise health and medicine proceedings of the Lilleshall Conference London The Sports Council 1984
23 Leon AS ed Forum Exercise and healthPrev Med 1984 131middot99
24 Powell KE ed Workshop on epidemiologic and public health aspects of physical activity and exercise Public Health Rep 1985 100113-224
25 Hyde RT Paffenbarger RS Jr Epidemiologic uses of genera population assessments of physical activity patterns National Center for Health Statisshytics (in press)
26 Schneider EL Reed JD Jr Life extension N Engl J Med 1985 3121159shy68
27 Olshansky SJ Pursuing longevity delay vs elimination of degenerative diseases Am J Public Health 1985 75754-6
28 Ramazzini B Diseases of workers New York Hafner 1964 29 Guy WA Contributions to a knowledge of the influence of employments
upon health J R Stat Soc 1843 6197-21l 30 Smith E Report on the sanitary circumstances of tailors in London (Report
of the Medical Officer Privy Council) London Her Majestys Stationery Office 1864416-30
31 Morgan JE University oars being a critical enquiry into the after health of the men who rowed in the Oxford Ifld Cambridge hoat-race from the year 1829 to 1869 London Macmillan 1873
32 Hedley OF Analysis of 5116 deaths reported as due to acute coronary occlusion in Philadelphia 1933-1936 US WeekJyPublic Health Rep 1939 54972
33 Morris IN Heady JA Raffle PAB Roberts CG Parks JW Coronary heart disease and physical activity of work Lancet 1953 21053-7 1111-20
34 Montoye ill Van Huss WD Olson HW et al Longevity and morbidity of college athletes Lansing Mich Michigan State University 1957
35 Pomeroy WC White PD Coronary heart disease in former football players JAMA 1958 167711-4
36 Prout C Life expectancy of college oarsmen JAMA 1972 220 1709middot1 L 37 Belloc NB Relationship of health practices and mortality Prev Med 1973
267-81 38 Wiley JA Camacho TC Life-style and future health evidence from the
Alameda County study Prev Med 1980 91middot21 39 Breslow L Enstrom J Persistence of health habits and their relationship to
mortality Prev Med 1980 9469-83 40 Wingard DL Berkman LF Brand RJ A multivariate analysis of healthshy
related practices Am J Epidemiol 1982 116765-75
LARRY VELTMAN MD

612 THE NEW ENGLAND JOURNAL OF MEDICINE March 6 1986
tage over the sedentary men until they reached the 65-to-69-year age bracket thereafter a tapering effect occurred because all the survivors from those groups had to reach the age of 80 within the follow-up period and hence their comparison was based on fewer years of mortality data It is possible too that contrasts between an active and sedentary life style were less marked in the older groups than in the younger groups Overall the table suggests a considerable gain in man-years of life for the habitually energetic alumshyni especially if any avoidable adverse characteristics such as cigarette smoking and obesity have been minimized
DISCUSSION
Survival is the result of a number of interacting influences (many hazardous in character or degree some beneficial in the same way) including physical activity and other life-style elements susceptible to opshytional adjustment Their combined effect determines whether increases in longevity are feasible or even deshysirable The findings reported here represent only a small part of the total picture but they suggest a proshytective effect of exercise against all-cause mortality in all age groups studied and therefore an indieationof additional years of life expectancy
The Harvard alumni may not be typical of the genshyeral population Their age-specific death rates from each major cause except suicide were roughly half the 1980 rates for white males in the United States (In contrast rates of self-destruction among the alumshyni 16- 18 were 50 percent higher than suicide rates in the general population) Yet the large alumni experience with delayed mortality for active men should imply increased life expectancy over that for sedentary men as the data demonstrate It is likely that some alumni increased their exercise reduced their smoking and received treatment for hypertension since the early 1960s when these characteristics were assessed Such changes would minimize the importance of these characteristics in the present findings The true force of the beneficial effects from physical activity nonshysmoking and control of hypertension would be even larger than that observed
Table 4 presents survival data in terms of definishytions of exercise that were necessarily limited by the design of the study to increases in kilocalories per week or to intensity as expressed by participation in vigorous sports The estimates of years gained reflect the experience of college alumni already recognized as long-lived whose economic status and behavior patterns differ from other populations in habitual physical exercise and other life-style elements Direct extrapolation to a general population should take these considerations into account
Since the data in Tables 4 and 5 represent only a portion of the total life experience of the study populashytion over time they may be viewed as a segment seen as through a window implying extensions that might
be estimated from the actual experience observed The differences in survival to the age of 80 between active and sedentary alumni may reflect a stage of optimal benefit from physical activity by the age of 65 and a rectangularization or converging trend may be estabshylished as the total life experience of the population of alumni approaches completion 19
Improvements in epidemiologic surveillance and medical management of such chronic disorders as hyshypertension abnormal blood lipid profiles and osteoshyporosis may defer mortality and extend survival However the effect of adequate physical exercise is partly independent of such influences and it countershyacts many adverse characteristics through metabolic and other processes20-25 Even when other procedures for health maintenance and disease prevention are deshyveloped to increase longevity the relevance of exercise is likely to remain
In studies of longevity the question arises whether the aging process is capable of modification but there is much uncertainty about the definitions of aging and of chronic disease Approaches to fend off disease or postpone aging are suggested or aging is regarded as an inexorable degenerative process that cannot be alshytered although perhaps chronic diseases may be avoided or deferred 2627 The present study considers chronic diseases but not the aging process itself
Extended follow-up of the Harvard alumni may reshyveal trends of aging or at least show at what stage of life the roles of exercise and10ther natural therapies become diminished The data in Tables 4 and 5 do offer some implications as a brief preliminary analysis of survival in various age and exercise groups In view of the data base and the consistency represented in the study it seems likely that the observed patterns are predictive
There is a widespread and longstanding popular belief that adequate physical exercise is necessary to preserve life and its desirable qualities into old age Discussions of this thesis date back to antiquity and have intensified in recent times 28
-40 The present study
adds new evidence to support this view
REFERENCES
1 Keys A Seven countries a multivariate analysis of death and coronary heart disease Cambridge Mass Harvard University Press 1980196-217276middot 8
2 Leon AS Blackburn H Physical inactivity In Kaplan NM Stamler I eds Prevention of coronary heart disease practical management of the risk factors Philadelphia WB Saunders 198386-97
3 Karvonen MJ Physical activity in work and leisure time in relation to cardiovascular diseases Ann Clin Res 1983 14SuppJ 34118-23
4 Morris IN Uses of epidemiology 3rd ed Edinburgh Churchill Livingshystone 1975163-5
5 Morris IN Kagan A Pattison DC Gardner MJlncidence and prediction of ischaemic heart-disease in London busmen Lancet 1966 2552-9
6 Paffenbarger RS Ir Brand RI Sholtz RI Jung DL Energy expenditure cigarette smoking and blood pressure level as related to death from specific diseases Am I Epidemiol 1978 10812-8
7 Paffenbarger RS Jr Hyde RT Wing AL Steinmetz CH A natural history of athleticism and cardiovascular health lAMA 1984 252491-5
8 Paffenbarger RS Ir Wing AL Hyde RT Physical activity as an index of heart attack risk in college alumni Am I Epidemiol 1978 108161shy75
613 Vol 314 No 10 PHYSICAL ACTIVITY MORTALITY AND LONGEVITY - PAFFENBARGER ET AL
9 Thomas GS Lee PR Franks P Paffenbarger RS Jr Exercise and health the evidence and the implications Cambridge Mass Oelgeschlager Gunn amp Hain 1981
10 Paffenbarger RS Jr Notkin J Krueger DE et al Chronic disease in former college students II Methods of study and observations on mortality from coronary heart disease Am J Public Health 1966 56962middot71
11 Passmore R Durnin JVGA Human energy expenditure Physiol Rev 1955 35801-40
12 Mantel N Chimiddotsquare tests with one degree of freedom extensions of the Mantel-Haenszel procedure J Am Stat Assoc 1963 58690middot700
13 Cox DR Regression models and life-tables J R Soc Biostat 1972 34187middot 220
14 Chang ImiddotM Gelman R Pagano M Corrected group prognostic curves and summary statistics J Chronic Dis 1982 35669-74
15 Paffenbarget RS Jr Wing AL Hyde RT Jung DL Physical activity and incidence of hypertension in college alumni Am J Epidemiol 1983 117245middot57
16 Paffenbarger RS Jr Asnes DP Chronic disease in former college students III Precursors of suicide in early and middle life Am J Public Health 1966 561026-36
17 Paffenbarger RS Jr Chronic disease in former college students VI Implicamiddot tiOlls for college health programs J Am College Health Assoc 1967 1651middot 5
IS Paffenbarger RS Jr King SH Wing AL Chronic disease in former college students IX Characteristics in youth that predispose to suicide and accidenshytal death in later life Am J Public Health 1969 5990()S
19 Fries IF Crapo LM Vitality and aging implications of the rectangular curve San Francisco WH Freeman 1981
20 Paffenbarger RS Jr Hyde RT Exercise as protection against heart attack N Engl J Med 1980 3021026-7
21 Wood PO Haskell WL BlairSN etal1ncreased exercise level and plasma lipoprotein concentrations a one-year randomized controlled study in sedmiddot entary middle-aged men Metabolism 1983 3231middot9
22 Morris IN Smith A eds Exercise health and medicine proceedings of the Lilleshall Conference London The Sports Council 1984
23 Leon AS ed Forum Exercise and healthPrev Med 1984 131middot99
24 Powell KE ed Workshop on epidemiologic and public health aspects of physical activity and exercise Public Health Rep 1985 100113-224
25 Hyde RT Paffenbarger RS Jr Epidemiologic uses of genera population assessments of physical activity patterns National Center for Health Statisshytics (in press)
26 Schneider EL Reed JD Jr Life extension N Engl J Med 1985 3121159shy68
27 Olshansky SJ Pursuing longevity delay vs elimination of degenerative diseases Am J Public Health 1985 75754-6
28 Ramazzini B Diseases of workers New York Hafner 1964 29 Guy WA Contributions to a knowledge of the influence of employments
upon health J R Stat Soc 1843 6197-21l 30 Smith E Report on the sanitary circumstances of tailors in London (Report
of the Medical Officer Privy Council) London Her Majestys Stationery Office 1864416-30
31 Morgan JE University oars being a critical enquiry into the after health of the men who rowed in the Oxford Ifld Cambridge hoat-race from the year 1829 to 1869 London Macmillan 1873
32 Hedley OF Analysis of 5116 deaths reported as due to acute coronary occlusion in Philadelphia 1933-1936 US WeekJyPublic Health Rep 1939 54972
33 Morris IN Heady JA Raffle PAB Roberts CG Parks JW Coronary heart disease and physical activity of work Lancet 1953 21053-7 1111-20
34 Montoye ill Van Huss WD Olson HW et al Longevity and morbidity of college athletes Lansing Mich Michigan State University 1957
35 Pomeroy WC White PD Coronary heart disease in former football players JAMA 1958 167711-4
36 Prout C Life expectancy of college oarsmen JAMA 1972 220 1709middot1 L 37 Belloc NB Relationship of health practices and mortality Prev Med 1973
267-81 38 Wiley JA Camacho TC Life-style and future health evidence from the
Alameda County study Prev Med 1980 91middot21 39 Breslow L Enstrom J Persistence of health habits and their relationship to
mortality Prev Med 1980 9469-83 40 Wingard DL Berkman LF Brand RJ A multivariate analysis of healthshy
related practices Am J Epidemiol 1982 116765-75
LARRY VELTMAN MD

613 Vol 314 No 10 PHYSICAL ACTIVITY MORTALITY AND LONGEVITY - PAFFENBARGER ET AL
9 Thomas GS Lee PR Franks P Paffenbarger RS Jr Exercise and health the evidence and the implications Cambridge Mass Oelgeschlager Gunn amp Hain 1981
10 Paffenbarger RS Jr Notkin J Krueger DE et al Chronic disease in former college students II Methods of study and observations on mortality from coronary heart disease Am J Public Health 1966 56962middot71
11 Passmore R Durnin JVGA Human energy expenditure Physiol Rev 1955 35801-40
12 Mantel N Chimiddotsquare tests with one degree of freedom extensions of the Mantel-Haenszel procedure J Am Stat Assoc 1963 58690middot700
13 Cox DR Regression models and life-tables J R Soc Biostat 1972 34187middot 220
14 Chang ImiddotM Gelman R Pagano M Corrected group prognostic curves and summary statistics J Chronic Dis 1982 35669-74
15 Paffenbarget RS Jr Wing AL Hyde RT Jung DL Physical activity and incidence of hypertension in college alumni Am J Epidemiol 1983 117245middot57
16 Paffenbarger RS Jr Asnes DP Chronic disease in former college students III Precursors of suicide in early and middle life Am J Public Health 1966 561026-36
17 Paffenbarger RS Jr Chronic disease in former college students VI Implicamiddot tiOlls for college health programs J Am College Health Assoc 1967 1651middot 5
IS Paffenbarger RS Jr King SH Wing AL Chronic disease in former college students IX Characteristics in youth that predispose to suicide and accidenshytal death in later life Am J Public Health 1969 5990()S
19 Fries IF Crapo LM Vitality and aging implications of the rectangular curve San Francisco WH Freeman 1981
20 Paffenbarger RS Jr Hyde RT Exercise as protection against heart attack N Engl J Med 1980 3021026-7
21 Wood PO Haskell WL BlairSN etal1ncreased exercise level and plasma lipoprotein concentrations a one-year randomized controlled study in sedmiddot entary middle-aged men Metabolism 1983 3231middot9
22 Morris IN Smith A eds Exercise health and medicine proceedings of the Lilleshall Conference London The Sports Council 1984
23 Leon AS ed Forum Exercise and healthPrev Med 1984 131middot99
24 Powell KE ed Workshop on epidemiologic and public health aspects of physical activity and exercise Public Health Rep 1985 100113-224
25 Hyde RT Paffenbarger RS Jr Epidemiologic uses of genera population assessments of physical activity patterns National Center for Health Statisshytics (in press)
26 Schneider EL Reed JD Jr Life extension N Engl J Med 1985 3121159shy68
27 Olshansky SJ Pursuing longevity delay vs elimination of degenerative diseases Am J Public Health 1985 75754-6
28 Ramazzini B Diseases of workers New York Hafner 1964 29 Guy WA Contributions to a knowledge of the influence of employments
upon health J R Stat Soc 1843 6197-21l 30 Smith E Report on the sanitary circumstances of tailors in London (Report
of the Medical Officer Privy Council) London Her Majestys Stationery Office 1864416-30
31 Morgan JE University oars being a critical enquiry into the after health of the men who rowed in the Oxford Ifld Cambridge hoat-race from the year 1829 to 1869 London Macmillan 1873
32 Hedley OF Analysis of 5116 deaths reported as due to acute coronary occlusion in Philadelphia 1933-1936 US WeekJyPublic Health Rep 1939 54972
33 Morris IN Heady JA Raffle PAB Roberts CG Parks JW Coronary heart disease and physical activity of work Lancet 1953 21053-7 1111-20
34 Montoye ill Van Huss WD Olson HW et al Longevity and morbidity of college athletes Lansing Mich Michigan State University 1957
35 Pomeroy WC White PD Coronary heart disease in former football players JAMA 1958 167711-4
36 Prout C Life expectancy of college oarsmen JAMA 1972 220 1709middot1 L 37 Belloc NB Relationship of health practices and mortality Prev Med 1973
267-81 38 Wiley JA Camacho TC Life-style and future health evidence from the
Alameda County study Prev Med 1980 91middot21 39 Breslow L Enstrom J Persistence of health habits and their relationship to
mortality Prev Med 1980 9469-83 40 Wingard DL Berkman LF Brand RJ A multivariate analysis of healthshy
related practices Am J Epidemiol 1982 116765-75
LARRY VELTMAN MD