Embed Size (px)
Citation preview
Running title: Preliminary findings from the EVASYON study 1
2
Address for correspondence: 3
4
Ascension Marcos, PhD. 5
Immunonutrition Research Group, Department of Metabolism and Nutrition, Institute of Food 6
Science, Technology and Nutrition (ICTAN), Spanish National Research Council (CSIC) 7
C/José Antonio Novais, 10 8
28040 Madrid, Spain 9
Phone: +34 915445607 10
Fax. + 34 91 5493627 11
E-mail: [email protected] 12
13
14
15
16
17
18
19
20
21
22

Changes in cardiometabolic risk factors, appetite-controlling 23
hormones and cytokines after a treatment programme in overweight 24
adolescents: preliminary findings from the EVASYON study 25
26
Javier Romeo1, David Martinez-Gomez
1,2, L. Esperanza Diaz
1, Sonia Gómez-Martinez
1, 27
Amelia Marti3, Miguel Martin-Matillas
4, M. Angeles Puertollano
5, Oscar L. Veiga
2, J. 28
Alfredo Martinez3, Julia Wärnberg
6, Belen Zapatera
1, Jesus M. Garagorri
7, Gonzalo 29
Morandé8, Cristina Campoy
9, Luis A Moreno
10, Ascension Marcos
1; EVASYON Study 30
Group* 31
32
1Immunonutrition Research Group, Department of Metabolism and Nutrition, Institute of 33
Food Science, Technology and Nutrition (ICTAN), Spanish National Research Council 34
(CSIC), Madrid, Spain. 2Department of Physical Education, Sport and Human Movement, 35
Facultad de Formación del Profesorado y Educación, Universidad Autonoma de Madrid, 36
Madrid, Spain. 3Department of Physiology and Nutrition. University of Navarra. Pamplona. 37
Spain. 4Department of Physical Education and Sport, School of Physical Activity and Sport 38
Sciences, University of Granada, Granada, Spain. 5Department of Health Sciences. Faculty of 39
Experimental Sciences. University of Jaén. Jaén. Spain. 6Department of Preventive Medicine 40
and Public Health, School of Medicine, University of Navarra, Pamplona, Spain. 7Department 41
of Pediatric, Radiology and Physical Medicine, University of Zaragoza, Spain. 8Servicio de 42
Psiquiatría, Hospital Infantil Universitario Niño Jesús, Madrid, Spain. 9 Faculty of Medicine. 43
University of Granada. Granada. Spain. 10GENUD “Growth; Exercise, Nutrition and 44
Development” research group. University School of Health Sciences, University of Zaragoza, 45
Zaragoza, Spain. 46
47

EVASYON Study Group* 48
49
Coordinator: Marcos A. 50
Local clinical treatment teams and researchers (Principal Investigators are italics); Granada: 51
Campoy C., López-Belmonte G., Delgado M., Martín-Matillas M., Aparicio V., Carbonell A., 52
Agil A., Silva D.R., Molina Font J.A., Pérez-Ballesteros C., Piqueras M.J., Chillón P., 53
Tercedor P., Martín-Lagos J.A., Martín-Bautista E., Pérez-Expósito M., Garófano M., Aguilar 54
M.J., Fernández-Mayorga A., Sánchez P.; Madrid: Marcos A., Gómez-Martínez S., Zapatera 55
B., Nova E., Romeo J., Díaz L.E., Pozo T., Wärnberg J., Puertollano M.A., Morandé G., 56
Villaseñor A., Madruga D., Muñoz R., Veiga O.L., Villagra A., Martínez-Gómez D., Garcia 57
R.M., Vaquero M.P., Pérez-Granados A.M., Navas-Carretero S.; Pamplona: Martí A., Azcona 58
C., Moleres A., Rendo T., Marqués M., Martínez J.A.; Santander: Redondo-Figuero C., 59
García-Fuentes M., DeRufino P., González-Lamuño D., Amigo T., Lanza R., Noriega M.J.; 60
Zaragoza: Garagorri J.M., Moreno L.A., Romero P., De Miguel P., Rodríguez G., Bueno G., 61
Mesana Ma.I., Vicente G., Fernández J., Rey-López P., Muro C., Tomás C.; Data 62
management and statistical analysis: Wärnberg J., Calle M.E., Barrios L. 63
64
65
66
Word count for the manuscript: 2822 67
68
69
ABSTRACT 70
71

Objective: We investigated the effects of the EVASYON programme on body fatness, 72
cardiometabolic risk factors, gut appetite-controlling hormones and serum levels of cytokines 73
in adolescents with overweight or obesity (OW/OB). Methods: The study comprised 13 boys 74
(10 obese) and 12 girls (8 obese), aged 13 to 16 years, from a Madrid Hospital. The 75
EVASYON programme was based on a calorie-restricted diet (10-40%), increased physical 76
activity (at least 60 min/day 5 days a week), psychological therapy and nutritional education 77
for 13-month. Anthropometric and blood pressure measurements were measured before and 78
after intervention. Serum glucose, total cholesterol, high-density lipoprotein cholesterol, 79
triglycerides, leptin, total peptide YY and insulin levels were determined before and after 80
intervention. Serum levels of cytokines IL-1β, IL-2, IL-4, IL-5, IL-6, IL-8, IL-10 and TNF- 81
were also assessed before and after intervention. Results: A decrease in body mass index 82
(BMI), BMI z-score, skinfolds (triceps, biceps, subscapular, thigh, and calf), sum of 6 83
skinfolds and body circumferences (arm relaxed and flexed, waist, hip and proximal thigh) 84
values were observed after the intervention programme (all P<0.05). In addition, diastolic 85
blood pressure also decreased (P<0.05). A decrease in serum leptin levels (–48.4%, P<0.001) 86
was observed after intervention without changes in total peptide PYY and insulin levels. 87
Levels of IL-8, IL-10 and TNF- also decreased (all P<0.05) after the intervention 88
programme. Conclusions: These preliminary results evidence that the EVASYON 89
programme may improve body fat, leptin, and some pro-inflammatory cytokines in 90
adolescents with OW/OB. 91
92
Key words: adolescents; obesity; metabolic syndrome; gut hormones; cytokines. 93
94
INTRODUCTION 95

Obesity is the most prevalent metabolic disease in adult humans, which has been 96
associated with cardiometabolic risk factors, such as low-grade inflammation, insulin 97
resistance, hypertension and dislipidemia (1,2). Since some of these cardiometabolic risks 98
have been already identified in obese children and adolescents, early obesity underlies the 99
metabolic groundwork for adult cardiovascular diseases (3-6). 100
In this context, adipose tissue is a rich source of many immune-related mediators (e.g. 101
cytokines such as tumour-necrosis factor-alpha [TNF-] and interleukin-6 [IL-6]) that are 102
involved in the inflammatory response (4-6), mediating cardiometabolic disorders (7). 103
Furthermore, adipose tissue is currently regarded as an active endocrine organ that, since in 104
addition to regulating fat mass and energy homeostasis, it releases a large number of bioactive 105
mediators modulating appetite and metabolism (8). Some of these bioactive mediators are 106
hormones called adipokines and include leptin, adiponectin, peptide YY (PYY), among others 107
(9,10). Recent data also suggest that these hormones have immunomodulating effects 108
involving inflammatory processes (8-10). 109
In this sense, the EVASYON (Development, implementation and evaluation of the 110
efficacy of a therapeutic programme for adolescents with overweight and obesity: integral 111
education on nutrition and physical activity) programme comprised a long-term intervention 112
with calorie-restricted diet, physical activity, psychological therapy and nutritional education 113
in adolescents with overweight or obesity (OW/OB) in hospital settings from Spain. Since 114
inflammation associated with obesity declines after weight loss in adults (4), we hypothesized 115
that a programme aimed to lose fat mass might modify specific obesity-associated markers of 116
inflammation in adolescents. Therefore, this preliminary study was performed to characterize 117
the effects of the EVASYON treatment programme on body fat, cardiometabolic risk factors, 118
gut appetite-controlling hormones and cytokines levels in adolescents with OW/OB. 119
METHODS AND PROCEDURES 120

Study design and participants 121
The EVASYON study is a multidisciplinary treatment programme study conducted in 122
5 hospitals from 5 Spanish cities (Granada, Madrid, Pamplona, Santander and Zaragoza) in 123
OW/OB adolescents. The complete and detailed methodology of the EVASYON Study has 124
been described elsewhere (11). Briefly, the EVASYON treatment programme was conducted 125
in small groups (8-10 participants) during 13-month including twenty visits within two 126
specific stages: 1) Intensive intervention (9 visits): participants visited the hospitals weekly 127
for 2 months and one-week objectives were defined; 2) Extensive intervention (11 visits): 128
participants visited the hospital monthly during 11 months. In this stage, objectives for the 129
adolescents were to be accomplished in one month's time. 130
The EVASYON intervention included calorie-restricted diet (10 to 40%), increased 131
physical activity (at least 60 min/day 5 days a week), psychological therapy and nutritional 132
education for these 13 months. Paediatricians explained the patients several motivational 133
strategies, life and time management strategies including physical activity and sedentary 134
behaviour recommendations, adequate sleep time, nutritional advice, family involvement, 135
among others. 136
Adolescents included in the EVASYON treatment met the inclusion criteria for 137
participating: i) To be aged 13 to 16 years; ii) To be OW/OB in agreement with the 138
International Obesity Task Force age- and sex-specific body mass index (kg/m2, BMI) values 139
(12); iii) To be Spanish or to have been educated in Spain; iv) To be free of other diagnosed 140
disease. Moreover, adolescents in pharmacological treatment or diagnosed with anorexia, 141
bulimia or other eating disorder, except binge eating disorder, were excluded. 142
In order to evaluate the long-term effect of the programme, we analyzed preliminary 143
results corresponding to basal point (before the intervention) and after intensive and extensive 144
phases of interventions (2+11 months) in OW/OB adolescents from the Madrid Hospital 145
(Figure 1). A total of 31 adolescents (13 girls) finished the EVASYON programme in this 146
Hospital. This study encompassed 13 boys and 12 girls (n=25) with valid data on 147
anthropometry and blood samples before intervention and the end of the EVASYON 148
treatment. These adolescents maintained an apparently good health status and did not 149
consume any medications during the study. 150
The study was conducted in accordance with the ethical rules of the Helsinki 151
Declaration (Hong Kong revision, September 1989, in Edinburgh in 2000 and in Korea in 152
2008), following the EEC Good Clinical Practice guidelines (document 111/3976/88 of July 153
1990) and current Spanish law, which regulates clinical research in humans (Royal Decree 154
561/1993 regarding clinical trials). Informed consent was obtained from all adolescents and 155
their parents, and the study was approved by the local ethics committees. 156
157
Anthropometry measurements 158
Body weight was measured without shoes and with light clothing to the nearest 0.05 159
kg by using a standard beam balance. Body height was measured using a stadiometer SECA 160
714 (range, 60-200 cm). BMI z-scores were calculated as a function of the subject’s obesity 161
degree when compared with BMI local reference standards (13). Skinfold thicknesses were 162
measured on the left side of the body (14) to the nearest 0.1 mm with a skinfold caliper 163
(Caliper Holtain; Holtain Ltd., Walles, UK) at triceps, biceps, subscapular, suprailiac, thigh, 164
and calf. The five circumferences (arm relaxed, arm flexed, waist, hip and proximal waist) 165
were measured in centimetres with an inelastic tape to the nearest millimetre. All the 166
anthropometric variables were measured in order, three times and averaged. For all the 167
anthropometric measurements, intraobserver reliability was >95% and interobserver 168
reliability was >90%. In the present study, the sum of 6 skinfolds and waist circumference 169
were used as indicators of total and central body fat, respectively. 170

171
Resting blood pressure 172
Blood pressure was measured using a validated digital automatic blood pressure 173
monitor (Omron M6, Omron Health Care Co., Ltd., Kyoto, Japan) according to the 174
International Protocol of the European Society of Hypertension (15). 175
176
Blood sampling 177
Blood samples were taken twice for each subject before and after the intervention (13-178
month). After an overnight fast (12-hour fast), subjects went to the hospital for blood 179
sampling at 8:00 a.m. Blood samples were collected by puncture of the cubital vein. For 180
biochemical analyses, the blood was collected in SST-Vacutainer (BD) and serum was 181
separated by centrifugation at 3000 rpm for 15 min at 22-24ºC, divided into aliquots, and 182
frozen and stored at –80ºC until withdrawn for analysis. 183
Biochemical parameters. Total cholesterol, HDL-cholesterol, triglycerides, and 184
glucose were analysed by a biochemical autoanalyser (Olympus model AU2700). All serum 185
analysis were performed at the end of the study, in order to have the three samples from each 186
subject analysed in the same run, to avoid systematic errors. Coefficients of variance of lipid 187
variables were 2% for total cholesterol, 2% for HDL-cholesterol and 3% for triacylglycerols. 188
VLDL-cholesterol and LDL-cholesterol were calculated from existing cholesterol, HDL-189
cholesterol, and triglycerides values (16). 190
Appetite-controlling hormones. Serum levels of leptin, total peptide YY, insulin and 191
adiponectin were measured by Luminex-100 IS (Integrated System: Luminex Corporation, 192
Austin, TX, USA) using the human gut hormone multiplex immunoassay kit (HGT-68K) and 193
Human CVD1 kit (HCVD1-67AK). The intra- and inter-assay precision coefficients of 194

variation were: 7% and 9% respectively for leptin; 5% and 10% respectively for total peptide 195
YY; 4% and 6% respectively for insulin; and 9% and 16% respectively for adiponectin. 196
Serum cytokines. Determination of serum cytokines IL-1β, IL-2, IL-4, IL-5, IL-6, IL-197
8, IL-10 and TNF- was performed on the Luminex-100 IS (Integrated System: Luminex 198
Corporation, Austin, TX, USA) using the multiplex assay kit Linco High Sensitivity Human 199
Cytokine Panel Lincoplex, 96 Well Plate Assay (HSCYTO-60SK), manufactured by Linco 200
Research, Inc., MO, USA. Multianalyte profiling calibration microspheres for classification 201
and reporter readings, as well as sheath fluid were also purchased from Luminex Corporation. 202
Acquired fluorescence data were analyzed by the Luminex-100 IS v.2.3. All analyses were 203
performed according to the manufacturer's protocols. The intra- and inter-assay precision 204
coefficients of variation were: 3% and 2%, respectively for IL-1β; 4% and 8%, respectively 205
for IL-2; 4% and 9%, respectively for IL-4; 5% and 14%, respectively for IL-5; 4% and 5%, 206
respectively for IL-6; respectively for IL-8; 3% and 12%, respectively for IL-10; and 4%, 207
respectively for TNF-. 208
209
Statistical analyses 210
Data were assessed for normality and homogeneity of variance, and are expressed as 211
mean ± standard deviation (SD). Student’s t test was used to compare means between before 212
and after intervention (13-month). Due to non-normal distribution, the Wilcoxon test was 213
applied to appetite-controlling hormones and cytokine values to compare means between 214
before and after intervention. Effect sizes (ES) were also calculated using Cohen's d as a 215
measure of ES that reflects the magnitude of the difference between groups in SD units. 216
Cohen's d is computed by subtracting the average score for the control group (before the 217
intervention) from the average score for the treatment group (after the EVASYON treatment 218
programme), and then dividing the difference by the SD on the outcome measure for the 219

sample (17). We used the standard criteria for ES of small (d=0.20), medium (d=0.50), and 220
large effects (d=0.80). We employed these criteria along with the results of the statistical tests 221
in evaluating the impact of the previous results of EVASYON programme presented in the 222
present work. Analysis was performed using SPSS software v.17. Statistical significance was 223
set at P<0.05. 224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
RESULTS 243

Adolescents included in the final analysis were 14.1 ± 1.1 years old, and the 244
prevalence of obesity at baseline was 72% (10 boys and 8 girls). These subjects showed 245
marked differences in body fat characteristics after the intervention programme (Table 1). 246
Thus, significant decreases in BMI mean values (–6.8%) and BMI z-score (–28.0%) were 247
found after the intervention (all P<0.05). Levels of body fat measured by anthropometry at 248
triceps, biceps, subscapular, thigh, and calf also decreased after the intervention (all P<0.05). 249
The main indicators of total and central body fat, that is, the sum of 6 skinfolds (–17.8%) and 250
waist circumference (–3.8%), also significantly decreased after the intervention (both 251
P<0.05). 252
Regarding cardiometabolic risk factors included in the metabolic syndrome definition 253
(Table 2), a more favourable profile was found in all of them, but only diastolic blood 254
pressure (–7.6%) significantly decreased after the intervention programme (P=0.018). No 255
significant changes on adiponectin, total peptide YY and insulin levels were observed after 256
the intervention (Table 3). In contrast, a decrease (P<0.001) on serum leptin levels (–48.4%) 257
was found after the intervention (Table 3). Levels of IL-8 (–34.4%), IL-10 (–39.8%) and 258
TNF- (–21.5%) also significantly decreased (all P<0.05) after the intervention programme 259
(Table 4). 260
261
262
263
264
265
266
267
DISCUSSION 268
These preliminary results of the EVASYON treatment programme indicate a clinically 269
relevant body fat reduction after the intervention programme in adolescents with OW/OB. 270
This outcome has been observed mainly in the sum of 6 skinfolds (large ES) as an indicator of 271
total body fat. Adolescence is characterised by an intense growth and development and in this 272
sense, it is important to stress the fact that although body weight did not decrease after 273
intervention, the decrease in BMI values observed is attributable to the increase in the body 274
height observed. These results also point out that in adolescents with OW/OB, the 275
improvement of body composition induced by the EVASYON intervention programme was 276
concomitant with decreased serum concentrations of leptin, IL-8, IL-10 and TNF-. 277
High serum leptin levels have been positively correlated with the components of the 278
metabolic syndrome in obesity during adolescence (18,19). The reduction of leptin levels 279
observed in the present study after body composition improvement is in agreement with other 280
trials (20,21). Although these studies did not evaluate the ES, the leptin decrease observed 281
after the EVASYON treatment programme showed a medium to large ES. Elloumi and co-282
workers (20) evaluated the effect of 2-month weight-loss programme (based on energy 283
restriction and training at the point of maximum lipid oxidation) on plasma levels of 284
adiponectin and leptin, in 21 obese adolescent boys. The authors found that the adolescents 285
who improved their body composition showed an increase in plasma adiponectin 286
concentrations (+74%) and a decrease in plasma leptin levels (–39%). In addition, a decrease 287
in plasma leptin levels (–70%) together with an increase in plasma adiponectin concentrations 288
(+27%) have been found after a 9-month multidisciplinary weight-reduction programme with 289
lifestyle education, moderate energy restriction and regular physical activity (21). Likewise, 290
our results have not reflected the increase in adiponectin levels previously reported by these 291
two studies and others (20-23), and seem to be in disagreement with the favourable body 292
composition changes observed after the intervention programme. 293
On the other hand, high means of BMI and waist circumference values have been 294
highly associated with elevated circulating levels of IL-6 and IL-8 (24). Since elevated levels 295
of pro-inflammatory cytokines correlate with obesity in adolescents confirming the presence 296
of early phases of atherosclerosis risk (25), the decrease in serum IL-8 and TNF- 297
concentrations (medium to large ES) observed in the current study after the intervention, 298
might suggest an attenuation of inflammation related risk factors. 299
To our knowledge, only a small number of studies concerning changes on serum 300
cytokine levels after intervention obesity programmes in adolescents are available. Thus, a 301
significant decrease in circulating IL-6 levels (–48%), associated with weight loss and 302
reduction of fat mass, have been reported (26) after short-term (3 weeks) under energy 303
restriction and exercise programme, in 49 obese adolescents. On the contrary, our results have 304
not reflected a significant decrease in IL-6 levels (–36%) after the intervention programme. 305
This conflicting outcome might be due to, for example, the differences in (i) the duration of 306
the interventions (3-week vs 13-month); (ii) IL-6 levels at baseline (3.9±4.7 vs 3.3±3.0 307
pg/mL); (iii) laboratory methods (ELISA vs Luminex); (iv) and sample sizes (49 vs 25 308
adolescents). 309
Although several authors have found no changes in TNF- in obese adolescents or 310
adults after weight loss (27-29), other studies in adults are in agreement with our results 311
showing decreased TNF- levels after weight loss (30-34). The release of pro-inflammatory 312
biomarkers might be one mechanism through which obesity is linked to increased leptin 313
values (7,10), and the current study concur with this hypothesis since leptin decreases were 314
concurrent with IL-8 and TNF- decreases after intervention. 315
Another conflicting finding in the present study is the decreased IL-10 levels observed 316
after our intervention programme. On the contrary, increased serum IL-10 levels have been 317
found after weight loss in obese adults (35). Since activated adipose tissue increases the 318

synthesis of pro-inflammatory cytokines while regulatory cytokines, such as IL-10 are 319
decreased (36); the decrease in IL-10 values observed after intervention seems to be 320
contradictory. In any case, no studies evaluating IL-10 cytokine after a weight loss 321
programme are available in adolescents. 322
Our results have shown relevant results. Obese subjects go on to display a 323
characteristic profile of hypertension, reduced HDL-cholesterol, and increased levels of LDL-324
cholesterol, triglycerides, and insulin resistance (metabolic syndrome), even during childhood 325
(37-39). In another study, after two-months of a physical-endurance and diet-restriction 326
programme in 24 obese adolescent boys, reductions in BMI and waist circumference (–13%) 327
were associated with decreased plasma triglycerides, LDL-cholesterol and total cholesterol 328
levels (40). Although a decrease in diastolic blood pressure was observed, the present study 329
has not reflected changes on cardiometabolic risk factors such as systolic blood pressure and 330
lipid profile after body composition reduction. The different findings found among studies 331
might be partially explained by the specific characteristics of each study (e.g. study duration, 332
sample size) as commented above. For example, other authors have detected an improvement 333
on lipid profile after decreasing BMI in 37 obese children who participated in a 12-month 334
intervention programme called "Obeldicks" (41). Although the duration of this programme 335
was one year, in this case, the age differences of the subjects involved in each study (mean 336
age 11 vs 14 years) could support the differences between their lipid profile results and our 337
current findings. 338
The novelty of the current study is that it is the first long-term study (13-month) 339
concerning the relationships between serum gut appetite-controlling hormones, serum 340
cytokines and changes in body composition in OW/OB adolescents. One limitation of the 341
present study includes the relative small sample size which could reduce the significance of 342
the detected changes and the ES. In addition, body fat was obtained by anthropometric 343

measurements and other methods (e.g. dual energy X-ray absorptiometry, air displacement 344
plethysmography, bioelectric impedance) may be more accurate for assessing body 345
composition changes. In any case, these preliminary results point out to a prominent body fat 346
reduction after the intervention programme, suggesting the potential usefulness of 347
implementing the EVASYON intervention programme for weight management in adolescents 348
with OW/OB. Future studies including the whole sample recruited in the EVASYON study 349
must analyse the role of important determinants (e.g. sexual maturation, socioeconomic 350
status, gene-environmental interactions) on the changes in body fat and cardiometabolic risks 351
during the EVASYON treatment programme. 352
In conclusion, our preliminary results indicate that the EVASYON programme may 353
produce moderate to large treatment effects for body fat reduction in adolescents with 354
OW/OB. Although the body composition improvement did not improve all the classic 355
metabolic syndrome components, these preliminary results suggest that the EVASYON 356
programme may reduce earlier cardiometabolic risk factors such as leptin, IL-8 and TNF- 357
levels, contributing to prevent future cardiovascular events. Nevertheless, further research is 358
required to examine whether this improvement in the inhibition of cardiometabolic risk 359
factors (mainly by an earlier decline in low-grade systemic inflammation) will eventually lead 360
to a clinical benefit associated with an improvement on body composition in children and 361
adolescents. 362
363
364
365
ACKNOWLEDGEMENTS 366
The authors would like to thank the Spanish Ministry of Health and Consumption 367
(Carlos III Institute of Health. FIS. Grant PI 051579). D. Martínez-Gómez receives a 368

predoctoral fellowship from the Spanish Ministry of Education and Science (AP2006-02464). 369
M.A. Puertollano owned a research contract ("Juan de la Cierva") from the Spanish Ministry 370
of Education and Science. The EVASYON study has received the award from AESAN 371
(Spanish Agency for Food Security and Nutrition) from the Spanish Ministry of Health and 372
Consumption to the best applied research project in 2009. 373
374
DISCLOSURE 375
The authors declare that they have no competing interests. 376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
REFERENCES 391
1. Isomaa B, Almgren P, Tuomi T, et al. Cardiovascular morbidity and mortality associated 392
with the metabolic syndrome. Diabetes Care 2001;24:683-689. 393

2. Hotamisligil GS. Inflammation and metabolic disorders. Nature 2006;444:860-867. 394
3. Must A, Strauss RS. Risks and consequences of childhood and adolescent obesity. Int J 395
Obes Relat Metab Disord 1999; 23(Suppl 2):s2-s11. 396
4. Schwarzenberg SJ, Sinaiko AR. Obesity and inflammation in children. Paediatr Respir 397
Rev 2006;7:239-46. 398
5. Wärnberg J, Nova E, Moreno LA, et al. Inflammatory proteins are related to total and 399
abdominal adiposity in a healthy adolescent population: the AVENA Study. Am J Clin 400
Nutr 2006;84:505-512. 401
6. Wärnberg J, Nova E, Romeo J, Moreno LA, Sjöström M, Marcos A. Lifestyle-related 402
determinants of inflammation in adolescence. Br J Nutr 2007;98(Suppl 1):s116-s120. 403
7. Bastard JP, Maachi M, Lagathu C, et al. Recent advances in the relationship between 404
obesity, inflammation, and insulin resistance. Eur Cytokine Netw 2006;17:4-12. 405
8. Rabe K, Lehrke M, Parhofer KG, Broedl UC. Adipokines and insulin resistance. Mol 406
Med 2008;14:741-751. 407
9. Sledzińska M, Liberek A, Kamińska B. Adipokines and obesity in children and 408
adolescents. Med Wieku Rozwoj 2009;13:244-251. 409
10. Antuna-Puente B, Feve B, Fellahi S, Bastard JP. Adipokines: the missing link between 410
insulin resistance and obesity. Diabetes Metab 2008;34:2-11. 411
11. Martinez-Gomez D, Gomez-Martinez S, Puertollano MA, et al. Design and evaluation of 412
a treatment programme for Spanish adolescents with overweight and obesity. The 413
EVASYON Study. BMC Public Health 2009;9:414. 414
12. Cole TJ, Belizzy MC, Flegal KM, Dietz WH. Establishing a standard definition for child 415
overweight and obesity worldwide: international survey. BMJ 2000;320:1-6. 416

13. Moreno LA, Mesana MI, González-Gross M, et al. Anthropometric body fat composition 417
reference values in Spanish adolescents. The AVENA Study. Eur J Clin Nutr 418
2006;60:191-196. 419
14. Moreno LA, Rodríguez G, Guillén J, Rabanaque MJ, León JF, Ariño A. Anthropometric 420
measurements in both sides of the body in the assessment of nutritional status in 421
prepubertal children. Eur J Clin Nutr 2002;56:1208-1215. 422
15. Topouchian JA, El Assaad MA, Orobinskaia LV, El Feghali RN, Asmar RG. Validation 423
of two automatic devices for self-measurement of blood pressure according to the 424
International Protocol of the European Society of Hypertension: the Omron M6 (HEM-425
7001-E) and the Omron R7 (HEM 637-IT). Blood Press Monit 2006;11:165-171. 426
16. Wallach J. Interpretation of diagnostic tests. 8th ed. Lippincott Williams & Wilkins: 427
Philadelphia, 2003. 428
17. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Lawrence 429
Erlbaum Associates: Hillsdale, 1988. 430
18. Sudi KM, Gallistl S, Weinhandl G, Muntean W, Borkenstein MH. Relationship between 431
plasminogen activitor inhibitor-1 antigen, leptin, and fat mass in obese children and 432
adolescents. Metabolism 2000;49:890-895. 433
19. Chu NF, Wang DJ, Shieh SM, Rimm EB. Plasma leptin concentrations and obesity in 434
relation to insulin resistance syndrome components among school children in Taiwan-435
The Taipei Children Heart Study. Int J Obes (Lond) 2000;24:1265-1271. 436
20. Elloumi M, Ben Ounis O, Makni E, Van Praagh E, Tabka Z, Lac G. Effect of 437
individualized weight-loss programmes on adiponectin, leptin and resistin levels in obese 438
adolescent boys. Acta Paediatr 2009;98:1487-1493. 439

21. Lazzer S, Vermorel M, Montaurier C, Meyer M, Boirie Y. Changes in adipocyte 440
hormones and lipid oxidation associated with weight loss and regain in severely obese 441
adolescents. Int J Obes (Lond) 2005;29:1184-1191. 442
22. Asayama K, Hayashibe H, Dobashi K, et al. Decrease in serum adiponectin level due to 443
obesity and visceral fat accumulation in children. Obes Res 2003;11:1072-1079. 444
23. Reinehr T, Roth C, Menke T, Andler W. Adiponectin before and after weight loss in 445
obese children. J Clin Endocrinol Metab 2004;89:3790-3794. 446
24. Herder C, Schneitler S, Rathmann W, et al. Low-grade inflammation, obesity, and insulin 447
resistance in adolescents. J Clin Endocrinol Metab 2007;92:4569-4574. 448
25. Głowińska B, Urban M. Selected cytokines (Il-6, Il-8, Il-10, MCP-1, TNF-alpha) in 449
children and adolescents with atherosclerosis risk factors: obesity, hypertension, diabetes. 450
Wiad Lek 2003;56:109-116. 451
26. Gallistl S, Sudi KM, Aigner R, Borkenstein M. Changes in serum interleukin-6 452
concentrations in obese children and adolescents during a weight reduction program. Int J 453
Obes Relat Metab Disord 2001;25:1640-1643. 454
27. Bastard JP, Jardel C, Bruckert E, et al. Elevated levels of interleukin-6 are reduced in 455
serum and subcutaneous adipose tissue of obese women after weight loss. J Clin 456
Endocrinol Metab 2000;85:3338-3342. 457
28. Xydakis AM, Case CC, Jones PH, et al. Adiponectin, inflammation, and the expression 458
of the metabolic syndrome in obese individuals: the impact of rapid weight loss through 459
caloric restriction. J Clin Endocrinol Metab 2004;89:2697-2703. 460
29. Reinehr T, Stoffel-Wagner B, Roth CL, Andler W. High-sensitive C-reactive protein, 461
tumor necrosis factor alpha, and cardiovascular risk factors before and after weight loss 462
in obese children. Metabolism 2005;54:1155-1161. 463

30. Xenachis C, Samojlik E, Raghuwanshi MP, Kirschner MA. Leptin, insulin and TNF-464
alpha in weight loss. J Endocrinol Invest 2001;24:865-870. 465
31. Nicoletti G, Giugliano G, Pontillo A, et al. Effect of a multidisciplinaryprogram of 466
weight reduction on endothelial functions in obese women. J Endocrinol Invest 467
2003;26:rc5-8. 468
32. Bruun JM, Verdich C, Toubro S, Astrup A, Richelsen B. Association between measures 469
of insulin sensitivity and circulating levels of interleukin-8, interleukin-6 and tumor 470
necrosis factor–alpha. Effect of weight loss in obese men. Eur J Endocrinol 471
2003;148:535-542. 472
33. Monzillo LU, Hamdy O, Horton ES, et al. Effect of lifestyle modification on adipokine 473
levels in obese subjects with insulin resistance. Obes Res 2003;11:1048-1054. 474
34. Samuelsson L, Gottsater A, Lindgarde F. Decreasing levels of tumour necrosis factor 475
alpha and interleukin 6 during lowering of body mass index with orlistat or placebo in 476
obese subjects with cardiovascular risk factors. Diabetes Obes Metab 2003;5:195-201. 477
35. Jung SH, Park HS, Kim KS, et al. Effect of weight loss on some serum cytokines in 478
human obesity: increase in IL-10 after weight loss. J Nutr Biochem 2008;19:371-375. 479
36. Iannone F, Lapadula G. Obesity and inflammation--targets for OA therapy. Curr Drug 480
Targets 2010;11:586-598. 481
37. Jiang X, Srinivasan SR, Webber LS, et al. Association of fasting insulin level with serum 482
lipid and lipoprotein levels in children, adolescents, and young adults: the Bogalosa Heart 483
Study. Arch Intern Med 1995;23:190-196. 484
38. Facchini FS, Hua N, Abbasi F, et al. Insulin resistance as a predictor of age-related 485
diseases. J Clin Endocrinol Metab 2001;86:3574-3578. 486
39. Kiess W, Reich A, Muller G, et al. Clinical aspects of obesity in childhood and 487
adolescence—diagnosis, treatment and prevention. Int J Obes Relat Metab Disord 488
2001;(25 Suppl 1):s75-s79. 489
40. Ben Ounis O, Elloumi M, Ben Chiekh I, et al. Effects of two-month physical-endurance 490
and diet-restriction programmes on lipid profiles and insulin resistance in obese 491
adolescent boys. Diabetes Metab 2008;34:595-600. 492
41. Reinehr T, Andler W. Changes in the atherogenic risk factor profile according to degree 493
of weight loss. Arch Dis Child 2004;89:419-422. 494

EXTENSIVE INTERVENTION
(10th-20th visit) 1 visit monthly
(11 months)
INTENSIVE INTERVENTION
(1st-9th visit) 1 visit weekly
(2 months)
RECRUITMENT IN A HOSPITAL FROM MADRID HEALTH
CARE SERVICE
GROUP I n=6
(3 girls)
GROUP II n=7
(2 girls)
GROUP III n=9
(5 girls)
GROUP IV n=9
(3 girls)
EVASYON treatment programme n=35
(15 girls)
EVASYON Inclusion/Exclusion criteria
Adolescents in Madrid with overweight or obesity
Screening N=42
(16 girls)
GROUP I n=6
(3 girls)
GROUP II n=9
(2 girls)
GROUP III n=10
(6 girls)
GROUP IV n=10
(4 girls)
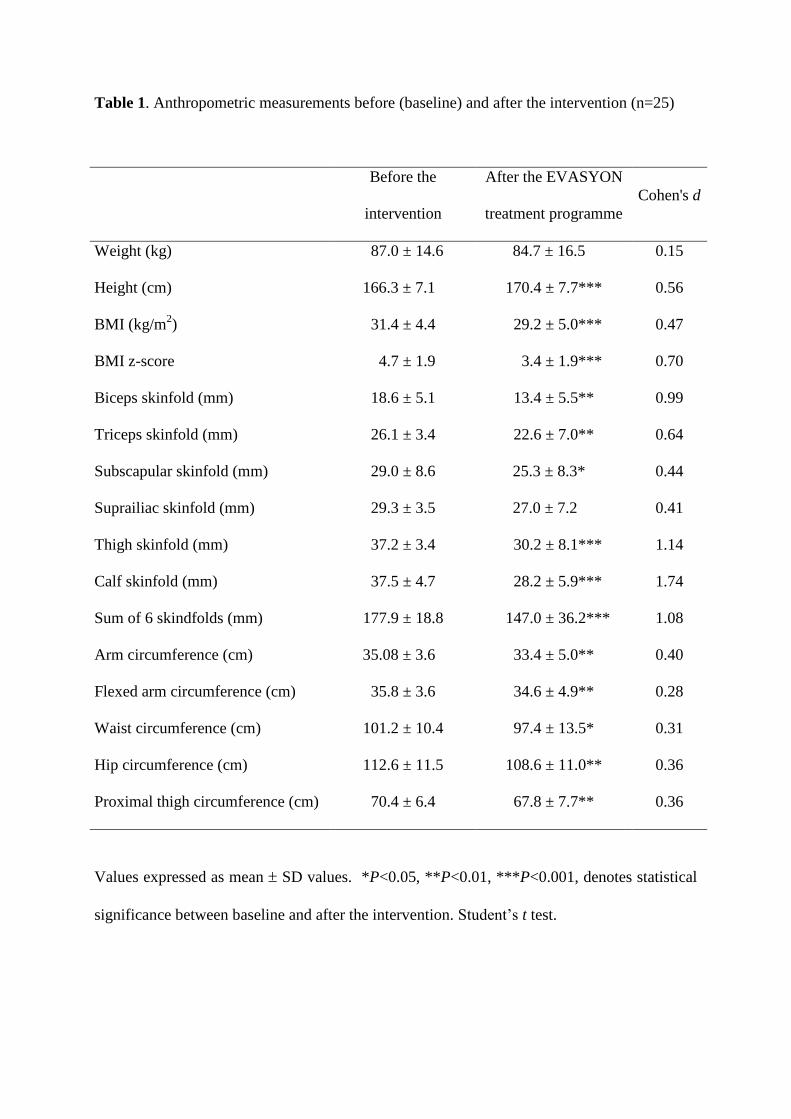
Table 1. Anthropometric measurements before (baseline) and after the intervention (n=25)
Before the
intervention
After the EVASYON
treatment programme
Cohen's d
Weight (kg) 87.0 ± 14.6 84.7 ± 16.5 0.15
Height (cm) 166.3 ± 7.1 170.4 ± 7.7*** 0.56
BMI (kg/m2)
31.4 ± 4.4 29.2 ± 5.0*** 0.47
BMI z-score
4.7 ± 1.9 3.4 ± 1.9*** 0.70
Biceps skinfold (mm) 18.6 ± 5.1 13.4 ± 5.5** 0.99
Triceps skinfold (mm) 26.1 ± 3.4 22.6 ± 7.0** 0.64
Subscapular skinfold (mm) 29.0 ± 8.6 25.3 ± 8.3* 0.44
Suprailiac skinfold (mm) 29.3 ± 3.5 27.0 ± 7.2 0.41
Thigh skinfold (mm) 37.2 ± 3.4 30.2 ± 8.1*** 1.14
Calf skinfold (mm) 37.5 ± 4.7 28.2 ± 5.9*** 1.74
Sum of 6 skindfolds (mm) 177.9 ± 18.8 147.0 ± 36.2*** 1.08
Arm circumference (cm) 35.08 ± 3.6 33.4 ± 5.0** 0.40
Flexed arm circumference (cm) 35.8 ± 3.6 34.6 ± 4.9** 0.28
Waist circumference (cm) 101.2 ± 10.4 97.4 ± 13.5* 0.31
Hip circumference (cm) 112.6 ± 11.5 108.6 ± 11.0** 0.36
Proximal thigh circumference (cm) 70.4 ± 6.4 67.8 ± 7.7** 0.36
Values expressed as mean SD values. *P<0.05, **P<0.01, ***P<0.001, denotes statistical
significance between baseline and after the intervention. Student’s t test.

Table 2. Cardiometabolic risk factors before (baseline) and after the intervention (n=25)
Before the
intervention
After the EVASYON
treatment programme
Cohen's d
Fasting glucose (mg/dL) 98.4 ± 8.1 95.9 ± 5.8 0.35
Total cholesterol (mg/dL) 146.2 ± 23.2 143.8 ± 24.6 0.10
Triglycerides (mg/dL) 56.7 ± 22.6 53.3 ± 31.1 0.13
HDL-Cholesterol (mg/dL) 45.1 ± 10.1 45.8 ± 10.4 0.07
LDL- Cholesterol (mg/dL) 89.8 ± 18.4 87.3 ± 17.5 0.14
Systolic blood pressure (mm Hg) 130.4 ± 17.6 127.4 ± 3.8 0.24
Diastolic blood pressure (mm Hg) 70.2 ± 8.8 65.4 ± 5.4* 0.67
Values expressed as mean SD values. *P<0.05, denotes statistical significance between
baseline and after the intervention. Student’s t test.

Table 3. Serum appetite-controlling hormones before (baseline) and after the intervention
(n=25)
Before the
intervention
After the EVASYON
treatment programme
Cohen's d
Leptin (ng/mL) 22.0 ± 12.0 14.1 ± 10.1 * 0.71
Insulin (pg/mL) 488.6 ± 366.7 490.7 ± 444.2 0.01
Total peptide YY (pg/mL) 89.6 ± 47.0 87.6 ± 58.1 0.04
Adiponectin (ng/mL) 5.5 ± 8.7 5.4 ± 8.4 0.01
Values expressed as mean SD values. *P<0.05, denotes statistical significance between
baseline and after the intervention. Wilcoxon test.

Table 4. Serum cytokines before (baseline) and after the intervention (n=25)
Before the
intervention
After the EVASYON
treatment programme
Cohen's d
IL-1β (pg/mL) 1.1 ± 2.8 0.6 ± 1.2 0.21
IL-2 (pg/mL) 3.0 ± 5.3 2.2 ± 4.6 0.17
IL-6 (pg/mL) 3.3 ± 3.0 2.1 ± 1.4 0.50
IL-4 (pg/mL) 5.2 ± 4.7 4.8 ± 3.9 0.10
IL-8 (pg/mL) 10.0 ± 6.2 6.5 ± 3.8 * 0.66
IL-10 (pg/mL) 17.6 ± 9.0 13.4 ± 6.7 * 0.52
TNF-α (pg/mL) 10.2 ± 4.4 8.0 ± 2.7 * 0.60
Values expressed as mean SD values. TNF-α: tumour necrosis factor-α. *P<0.05, denotes
statistical significance between baseline and after the intervention. Wilcoxon test.





























