Embed Size (px)
Citation preview

KNEE
Rotatory knee laxity tests and the pivot shift as toolsfor ACL treatment algorithm
Volker Musahl • Sebastian Kopf • Stephen Rabuck •
Roland Becker • Willem van der Merwe • Stefano Zaffagnini •
Freddie H. Fu • Jon Karlsson
Received: 29 November 2011 / Accepted: 19 December 2011 / Published online: 30 December 2011
� Springer-Verlag 2011
Abstract The goal of anterior cruciate ligament (ACL)
reconstruction surgery is to eliminate the pivot shift phe-
nomenon. Different injury mechanisms and injury patterns
may lead to specific knee laxity patterns. Computer navi-
gation is helpful for the surgeon during examination under
anesthesia. Surgical treatment may have to be altered if
high-grade laxity is detected preoperatively for example by
utilizing a computer navigation that is a helpful adjunct for
surgeons during examination under anesthesia. A typical
case for revision ACL reconstruction is presented. This
article describes several techniques of laxity assessments.
Based on the type and degree of pathologic laxity, a
treatment algorithm has been developed.
Level of evidence V.
Keywords Anterior cruciate ligament � Treatment �Pivot shift � Clinical examination
Introduction
During the past decade, a large body of research has focused
on the function of the two functional bundles of the anterior
cruciate ligament (ACL). The posterolateral (PL) bundle is
taut and locks the knee in full extension by inhibiting anterior
tibial translation [2, 38, 42, 43]. During knee flexion, the PL
bundle relaxes and allows the tibia to internally rotate while
the quadriceps muscle contracts. This supports function of
knee weight bearing in extension and allowing movement
during knee flexion [38]. This physiologic movement pattern
is disrupted during knee injuries involving rupture of the
ACL leading to rotatory knee laxity [28, 38, 43].
The resultant pivot shift phenomenon is a shift of the knee
pivot from the medial tibial spine centrally (intact knee) to
produce an anterior and medial subluxation (ACL-deficient
knee). Therefore, the anterior tibial translation in the lateral
compartment is exaggerated, but it is still anterior tibial
translation, and not rotation [11, 24]. The cause of the pivot
shift phenomenon is not only injury of the ACL, but also
injury to secondary restraints, such as collateral ligaments,
especially the lateral collateral ligament, capsule, meniscus
roots, meniscotibial ligaments, and shape of the bones
(compression fractures of posterolateral tibial plateau and/or
anterolateral femur) [11, 18, 31, 33, 35, 36, 54]. Any
meaningful treatment algorithm would have to address these
factors to achieve a successful clinical outcome.
V. Musahl (&) � S. Rabuck � F. H. Fu
Department of Orthopaedic Surgery, Center for Sports Medicine,
University of Pittsburgh, 3200 S Water Street,
Pittsburgh, PA 15203, USA
e-mail: [email protected]
S. Kopf
Center for Musculoskeletal Surgery, Charite,
University Medicine, Berlin, Germany
R. Becker
Department of Orthopaedic and Traumatology,
City Hospital Brandenburg, Brandenburg, Germany
W. van der Merwe
The Sports Science Orthopaedic Clinic,
Cape Town, South Africa
S. Zaffagnini
Sports Traumatology Department and Biomechanics
Laboratory, Instituti Ortopedici Rizzoli,
Bologna University, Bologna, Italy
J. Karlsson
Department of Orthopaedics, Sahlgrenska University Hospital,
Goteborg, Sweden
123
Knee Surg Sports Traumatol Arthrosc (2012) 20:793–800
DOI 10.1007/s00167-011-1857-6

The elimination of the pivot shift is one of the goals in
ACL reconstruction surgery (B. Clancy, August 25, 2011,
What have we learnt over the last 30 years of ACL
reconstruction, Personal Communication) [19]! Studies of
simulated pivot shift or simulated combined rotatory
loading conditions have shown variable magnitudes of
increased tibial rotation following ACL deficiency [29, 37].
However, in vivo, and in numerous clinical outcome
studies, the pivot shift has been shown to persist in a
considerable number of patients, even following anatomic
ACL reconstruction [32]. The question is, what exactly are
the factors contributing to this persistent rotational insta-
bility, and how can this be avoided?
The success of ACL reconstruction should be considered
in short term but also in a long-term aspect. The short-term
goal of ACL reconstruction is to return the athlete to sport as
quickly and safely as possible [15, 46, 47]. While the long-
term goal is to avoid further injury or re-injury as well as
avoid chronic pain and the development of osteoarthritis
(OA) [7]. Therefore, ACL healing and recovery of muscle
function would be predictors of short-term outcome, while
meniscal injury and chondral damage are the most accurate
predictors of long-term knee function [1, 8, 41].
Clinical scenario
A typical scenario may be a patient presenting with a
history of an acute non-contact knee injury and a ‘‘pop’’. A
clinical examination may or may not have been obtained,
but the MRI reveals a bone bruise pattern and torn ACL.
The patient is indicated for surgery. Autograft ACL
reconstruction is performed, and a concomitantly present
medial meniscus tear is treated with partial resection [36].
The outcome of this patient is good, but mild rotatory
instability persists over the years. We all know the fate of
this patients’ ACL reconstructed knee in the medium-term,
i.e., OA [8, 12].
An alternate, and preferred, diagnostic procedure for the
same patient would include a specifically history of pre-
vious or contralateral knee injury, generalized ligamentous
laxity, and injury mechanism. The evaluation of each
patient should focus on identifying the unique character-
istics of that patient’s injury pattern. Anatomic ACL
reconstruction has demonstrated significant variability in
the anatomy of the ACL and a resultant variability in ACL
injuries. As a result, when anatomically reconstructing the
ACL, the goal should be to individualize the surgical
procedure to the unique characteristics of that patient
[20–22, 40, 45, 48]. Clinical examination should consist of
several tests for rotatory knee laxity, e.g., pivot shift test,
varus–valgus (VV) laxity test, internal–external (IE) rota-
tion dial tests, and exclusion of further ligamentous knee
injuries such as PCL rupture. It is preferred that clinical
examination is performed on at least two different occa-
sions. At the time of surgery, a useful preoperative plan-
ning tool is examination under anesthesia (EUA) [35, 49].
Case example
An 18-year-old division I football player underwent ACL
reconstruction at the end of his junior year in high school.
Following surgery, he played his senior year denying pain or
any symptoms of instability. His college pre-season physical
examination 18 months later revealed near-symmetric
quadriceps strength, no loss of motion, but a moderate
effusion. Laxity examination demonstrated a 2B Lachman
test, a 2? opening on varus stress with a strong end point. The
pivot shift test was a 2? with a ‘‘clunk’’ and at least 10 mm of
noticeable translation in the lateral compartment.
MRI revealed a vertical and slightly anterior femoral
tunnel of the ACL reconstruction. The tibial tunnel is
posteriorly located within the native footprint. The ACL
graft is absent (Figs. 1, 2). The medial meniscus is status
post partial posterior horn resection. A vertical split is
present in the vascular zone at the junction of meniscus and
posteromedial capsule (Fig. 3). The lateral meniscus is
intact. The lateral collateral ligament and posterolateral
corner complex are intact.
The assessment following EUA was a chronic, recur-
rent, high-grade ACL insufficiency with associated medial
meniscus capsule separation. Existing tunnels are non-
Fig. 1 Sagittal fat suppressed MRI of failed ACL reconstruction.
ACL graft is deficient/absent
794 Knee Surg Sports Traumatol Arthrosc (2012) 20:793–800
123
anatomic (femur) and partially anatomic (tibia; Fig. 2). The
pathologic opening of the knee on varus stress testing in
extension was felt to be secondary to medial meniscus
insufficiency. The lack of subjective instability of the
patient was judged to be secondary to the well-functioning
quadriceps muscle.
Based on the high-grade positive pivot shift test, the
surgical plan was for (1) revision ACL reconstruction,
utilizing autologous BTB graft, (2) anatomic single-bundle
technique (Fig. 4), and (3) medial meniscus repair. If the
meniscus is found to be irreparable (4), staged medial
meniscus reconstruction with allograft or collagen menis-
cus implant would be recommended.
The resolution for this case was revision ACL recon-
struction as planned and medial meniscus repair. The
medial meniscus capsule separation was repaired utilizing
an accessory posteromedial portal and all-inside suture
repair with two braided sutures using a 70�-curved suture
passer (Fig. 5). The medial meniscus vertical split of mid
body to posterior horn junction was repaired utilizing an
all-inside suture-passing device.
Information gained from pivot shift test
The pivot shift test is the most important and most specific
test during EUA [4]. Clinical grading is complicated.
However, from controlled laboratory studies, it is known
that lateral compartment translation predicts the grade of
the pivot shift [3]. The surgeon should therefore attempt to
focus on the movement of the lateral compartment and try
Fig. 2 Flexion posteroanterior weight bearing and lateral radiograph
of the left knee demonstrating preserved joint spaces and vertical
tunnel architecture. The angle of the femoral tunnel in the coronal
plane is \15�
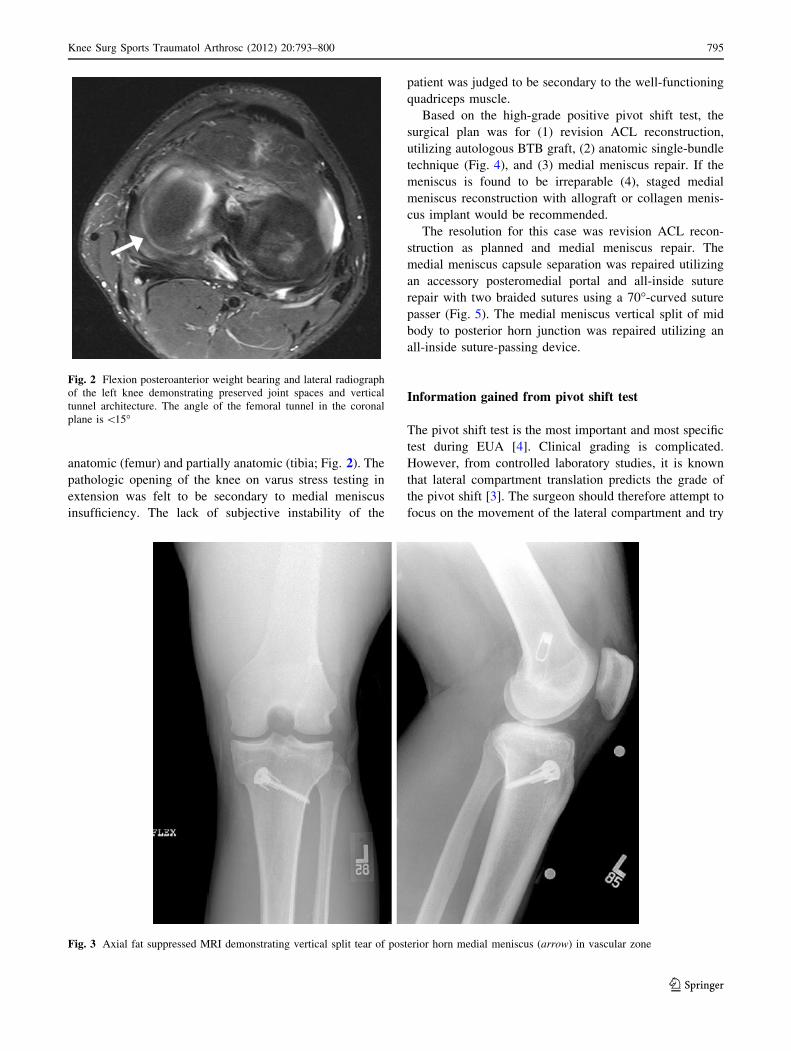
Fig. 3 Axial fat suppressed MRI demonstrating vertical split tear of posterior horn medial meniscus (arrow) in vascular zone
Knee Surg Sports Traumatol Arthrosc (2012) 20:793–800 795
123

to understand if there is more or less than *10 mm of
translation present. For example, a grade I pivot shift
(*6 mm of lateral compartment translation) usually rep-
resents an isolated ACL injury. A grade II pivot shift or
higher ([12 mm of lateral compartment translation) usu-
ally indicates concomitant injury to secondary restraints,
most commonly the medial meniscus [35]. Therefore, a
grade II? pivot shift on EUA should leave the surgeon
suspicious for concomitant injuries. A medial meniscus
tear in this case scenario should be repaired, because its
integrity will contribute to the elimination of excess rota-
tory knee laxity [36].
What if a grade II pivot shift is present and no con-
comitant meniscus or collateral ligament injury can be
found? Here, it may be an injury or permanent strain of the
capsule, generalized ligamentous laxity, or underlying
morphologic abnormalities. Zaffagnini et al. [53] have
shown that in those cases, a concomitant lateral tenodesis
may be indicated. The goal of this review paper is to
present methods to assess and treat different injury
patterns.
Anterior–posterior laxity
When intra-operative laxity data were analyzed pre- and
postoperatively, a significant reduction in all knee laxities
was shown after ACL reconstruction [49]. The navigation
system was also validated for the use of anterior–posterior
laxity tests, by direct comparison with commercial
arthrometer testing systems [25, 34]. These systems have
been proven for evaluating and detecting different laxity
patterns following anatomic double-bundle ACL recon-
struction [10, 16, 44, 51].
Kinematic analysis of the knee
Navigation technology allows for a complete kinematic
analysis of the limb. These systems have been used to
evaluate not only the AP translation during Lachman and
anterior drawer testing, but also IE and VV rotations of the
tibia under different stress tests at fixed flexion angles.
Several studies quantitatively report the effect of ACL
reconstruction on controlling global knee laxity. Intra-
observer reliability was \1 mm/1.5� and an inter-observer
repeatability \1.2 mm/2.3� [30].
Combined ACL and extraarticular tenodesis
A very useful application of navigation systems is the
evaluation of laxity patterns following different surgical
reconstruction procedures. Isolated single-bundle and sin-
gle-bundle reconstruction with lateral plasty were com-
pared [6, 49]. The extra-articular procedure controlled
lateral tibial compartment during the Lachman testing,
reducing translation by 1.6 mm, whereas during drawer
Fig. 4 Arthroscopic image of
the notch demonstrating a
malplaced and high original
femoral tunnel (a) and anatomic
center of the ACL for planned
tunnel in revision surgery (b)
Fig. 5 Arthroscopic image of
the posterior compartment (with
70� arthroscope through
Gillquist portal) demonstrating
a vertical split of posterior horn
to posteromedial capsule
junction (a). Image b is taken
after all-inside repair with 2 no.
2 braided sutures
796 Knee Surg Sports Traumatol Arthrosc (2012) 20:793–800
123

testing, the control was about 1 mm in both compartments.
Additional lateral tenodesis was shown to result in
improved static laxity reduction in VV stress test at full
extension and in IE rotation at 90� of flexion [53].
Combined ACL and MCL injury
Computer navigation was shown to be able to detect the
presence of additional ligamentous lesions. Combined
ACL/MCL lesions result in greater AP laxity and greater
VV laxity. It has been shown that residual laxity remains
when ACL reconstruction is performed in patients with
combined ACL and MCL lesions [50].
Dynamic laxity testing
While AP laxity testing of the knee has been demonstrated
to be effective, rotational laxity testing is less consistent.
Variability in rotational laxity measurements may be
related to the fact that other structures of the knee joint can
be involved, while the constitutional laxity of the patient
must be considered.
Recent studies have focused on the analysis of the pivot
shift test. However, it has been difficult to describe and
quantify dynamic laxity of the knee joint utilizing the pivot
shift. Preliminary results demonstrate good intra-tester
reliability of pivot shift test performed before and after
ACL reconstruction [17, 26].
Clinical grading, which has been historically inconsis-
tent, can be correlated with different parameters by means
of navigation [3, 24]. The clinical grade correlated well
with the dynamic behavior (AP translation and IE rotation)
of the joint, specifically the lateral compartment [5, 26].
Additional tenodesis may improve static laxity as reported
above; however, anatomic double-bundle reconstruction
presented better results in controlling the dynamic laxity of
the knee joint, especially when the acceleration during
reduction is considered [53].
Preoperative high laxity
Preoperative laxity measurements have been taken recently
in a study in order to define the threshold for pathological
knee condition. For this study, laxity data from 115 patients
who underwent ACL reconstruction were analyzed.
Patients were divided into 4 groups (A, B, C, and D)
according to their preoperative laxity, determined with a
surgical navigation system. Patients with higher preopera-
tive laxity (group C and D) maintained higher values for all
laxity tests also following ACL reconstruction (Fig. 6). The
findings from this study can be used to further analyze and
stratify the presence of peripheral soft-tissue injuries, such
as MCL and meniscal lesions. In the future, treatment
algorithms may be modified to be more injury-specific
(Zaffagnini et al., personal communication).
Treatment algorithm
The main focus of the treatment algorithm is the amount of
laxity that dictates treatment. A low-grade pivot shift and
negative findings of additional laxity tests would indicate
ACL augmentation or primary ACL reconstruction. How-
ever, in cases where the pivot shift is 2? and greater on
preoperative EUA ([12 mm lateral compartment transla-
tion), additional surgical repair or reconstruction may be
necessary (Fig. 7). In this scenario, meniscus deficiency
would mandate surgical repair. Low-grade opening with a
good end point on VV stress testing can sometimes indicate
chronic meniscus deficiency. Treatment could consist of
meniscus reconstruction and/or biplanar osteotomy [9, 13].
High-grade medial laxity should be treated with MCL
surgery, lateral laxity with posterolateral corner surgery.
Some data exist to support extra-articular tenodesis
[39, 53].
The unique presentation of each patient’s injury and
anatomy requires an individualized approach. Suboptimal
outcomes following ACL reconstruction may be a result of
a surgical plan that incompletely addresses the patient’s
injury or anatomy. By improving the ability to detect the
Fig. 6 Pre- and Postoperative
knee laxities according to
defined preoperative laxity
groups (A, B, C, and D).
*P \ 0.05 for one-way
ANOVA analysis with all pair
wise contrast, from Zaffagnini
et al. [53]
Knee Surg Sports Traumatol Arthrosc (2012) 20:793–800 797
123

subtleties of each injury, the patient’s anatomy may be
better restored. However, the anatomy of the ACL is var-
iable. An individualized approach, whereby the graft and
surgical technique are chosen based on the patient’s unique
anatomy, may be necessary to restore the native kinematics
of the knee. Ultimately, the goal of anatomic ACL recon-
struction is to achieve improved clinical outcomes and
avoidance of the development of OA [20–22, 40, 45, 48].
Conclusion
Navigation systems have demonstrated feasibility in cus-
tomizing the surgical strategy to be patient-specific. The
focus is on evaluation and comparison of laxity parameters
between injured and healthy knee. The philosophy of
computer navigation as an intra-operative tool for treat-
ment algorithm is changing. Surgeons are ready to accept
the quantitative information on static and, above all,
dynamic behavior of the joint, as provided by computer
navigation. This approach may be able to aid in improving
ligament reconstruction surgery. In the future, the intro-
duction of hard- and soft-tissue modeling into navigation
may also improve the knowledge of patient-specific
parameters, leading toward a predictive planning of the
surgery itself based both on anatomy and joint function.
Recently, noninvasive methodologies based on electro-
magnetic or acceleration sensors have been shown to
quantitatively evaluate the pivot shift test [14, 23, 27, 52].
In the future, quantitative dynamic laxity testing can be
performed in the office. Together with imaging modalities
and patient-specific parameters of joint laxity and mor-
phology, quantitative pivot shift testing will enable sur-
geons to modify their treatment plans based on the
requirements of each individual patient.
References
1. Ait Si Selmi T, Fithian D, Neyret P (2006) The evolution of
osteoarthritis in 103 patients with ACL reconstruction at 17 years
follow-up. Knee 13(5):353–358
2. Amis AA, Dawkins GP (1991) Functional anatomy of the anterior
cruciate ligament. Fibre bundle actions related to ligament
replacements and injuries. J Bone Joint Surg Br 73(2):260–267
3. Bedi A, Musahl V, Lane C, Citak M, Warren RF, Pearle AD
(2010) Lateral compartment translation predicts the grade of
pivot shift: a cadaveric and clinical analysis. Knee Surg Sports
Traumatol Arthrosc 18(9):1269–1276
4. Benjaminse A, Gokeler A, van der Schans CP (2006) Clinical
diagnosis of an anterior cruciate ligament rupture: a meta-anal-
ysis. J Orthop Sports Phys Ther 36(5):267–288
5. Bignozzi S, Zaffagnini S, Lopomo N, Fu FH, Irrgang JJ, Marc-
acci M (2010) Clinical relevance of static and dynamic tests after
anatomical double-bundle ACL reconstruction. Knee Surg Sports
Traumatol Arthrosc 18(1):37–42
6. Bignozzi S, Zaffagnini S, Lopomo N, Martelli S, Iacono F,
Marcacci M (2009) Does a lateral plasty control coupled trans-
lation during antero-posterior stress in single-bundle ACL
reconstruction? An in vivo study. Knee Surg Sports Traumatol
Arthrosc 17(1):65–70
Fig. 7 Treatment algorithm for
acute and chronic ACL
deficiency
798 Knee Surg Sports Traumatol Arthrosc (2012) 20:793–800
123

7. Chu CR, Beynnon BD, Buckwalter JA, Garrett WE Jr, Katz JN,
Rodeo SA, Spindler KP, Stanton RA (2011) Closing the gap
between bench and bedside research for early arthritis therapies
(EARTH): report from the AOSSM/NIH U-13 Post-Joint Injury
Osteoarthritis Conference II. Am J Sports Med 39(7):1569–1578
8. Daniel DM, Stone ML, Dobson BE, Fithian DC, Rossman DJ,
Kaufman KR (1994) Fate of the ACL-injured patient. A pro-
spective outcome study. Am J Sports Med 22(5):632–644
9. Dejour H, Neyret P, Boileau P, Donell ST (1994) Anterior cru-
ciate reconstruction combined with valgus tibial osteotomy. Clin
Orthop Relat Res 299:220–228
10. Ferretti A, Monaco E, Labianca L, Conteduca F, De Carli A
(2008) Double-bundle anterior cruciate ligament reconstruction: a
computer-assisted orthopaedic surgery study. Am J Sports Med
36(4):760–766
11. Fetto JF, Marshall JL (1979) Injury to the anterior cruciate lig-
ament producing the pivot-shift sign. J Bone Joint Surg Am
61(5):710–714
12. Fithian DC, Paxton LW, Goltz DH (2002) Fate of the anterior
cruciate ligament-injured knee. Orthop Clin North Am
33(4):621–636
13. Giffin JR, Vogrin TM, Zantop T, Woo SL, Harner CD (2004)
Effects of increasing tibial slope on the biomechanics of the knee.
Am J Sports Med 32(2):376–382
14. Hoshino Y, Kuroda R, Nagamune K, Yagi M, Mizuno K, Yam-
aguchi M, Muratsu H, Yoshiya S, Kurosaka M (2007) In vivo
measurement of the pivot-shift test in the anterior cruciate liga-
ment-deficient knee using an electromagnetic device. Am J
Sports Med 35(7):1098–1104
15. Irrgang JJ, Delitto A, Hagen B, Huber F, Pezzullo D (1995)
Rehabilitation of the injured athlete. Orthop Clin North Am
26(3):561–577
16. Ishibashi Y, Tsuda E, Tazawa K, Sato H, Toh S (2005) Intra-
operative evaluation of the anatomical double-bundle anterior
cruciate ligament reconstruction with the OrthoPilot navigation
system. Orthopedics 28(10 Suppl):1277–1282
17. Ishibashi Y, Tsuda E, Yamamoto Y, Tsukada H, Toh S (2009)
Navigation evaluation of the pivot-shift phenomenon during dou-
ble-bundle anterior cruciate ligament reconstruction: is the pos-
terolateral bundle more important? Arthroscopy 25(5):488–495
18. Johnson DL, Urban WP Jr, Caborn DN, Vanarthos WJ, Carlson
CS (1998) Articular cartilage changes seen with magnetic reso-
nance imaging-detected bone bruises associated with acute
anterior cruciate ligament rupture. Am J Sports Med
26(3):409–414
19. Kocher MS, Steadman JR, Briggs KK, Sterett WI, Hawkins RJ
(2004) Relationships between objective assessment of ligament
stability and subjective assessment of symptoms and function
after anterior cruciate ligament reconstruction. Am J Sports Med
32(3):629–634
20. Kopf S, Musahl V, Tashman S, Szczodry M, Shen W, Fu FH
(2009) A systematic review of the femoral origin and tibial
insertion morphology of the ACL. Knee Surg Sports Traumatol
Arthrosc 17(3):213–219
21. Kopf S, Pombo MW, Shen W, Irrgang JJ, Fu FH (2011) The
ability of 3 different approaches to restore the anatomic antero-
medial bundle femoral insertion site during anatomic anterior
cruciate ligament reconstruction. Arthroscopy 27(2):200–206
22. Kopf S, Pombo MW, Szczodry M, Irrgang JJ, Fu FH (2011) Size
variability of the human anterior cruciate ligament insertion sites.
Am J Sports Med 39(1):108–113
23. Labbe DR, de Guise JA, Mezghani N, Godbout V, Grimard G,
Baillargeon D, Lavigne P, Fernandes J, Ranger P, Hagemeister N
(2010) Feature selection using a principal component analysis of
the kinematics of the pivot shift phenomenon. J Biomech
43(16):3080–3084
24. Lane CG, Warren RF, Stanford FC, Kendoff D, Pearle AD (2008)
In vivo analysis of the pivot shift phenomenon during computer
navigated ACL reconstruction. Knee Surg Sports Traumatol
Arthrosc 16(5):487–492
25. Lopomo N, Bignozzi S, Martelli S, Zaffagnini S, Iacono F, Visani
A, Marcacci M (2009) Reliability of a navigation system for
intra-operative evaluation of antero-posterior knee joint laxity.
Comput Biol Med 39(3):280–285
26. Lopomo N, Zaffagnini S, Bignozzi S, Visani A, Marcacci M
(2010) Pivot-shift test: analysis and quantification of knee laxity
parameters using a navigation system. J Orthop Res
28(2):164–169
27. Lopomo N, Zaffagnini S, Signorelli C, Bignozzi S, Giordano G,
Marcheggiani Muccioli GM, Visani A (2011) An original clinical
methodology for non-invasive assessment of pivot-shift test.
Comput Methods Biomech Biomed Eng. doi:10.1080/10255842.
2011.591788
28. Losee RE (1983) Concepts of the pivot shift. Clin Orthop Relat
Res 172:45–51
29. Markolf KL, Park S, Jackson SR, McAllister DR (2008) Simu-
lated pivot-shift testing with single and double-bundle anterior
cruciate ligament reconstructions. J Bone Joint Surg Am
90(8):1681–1689
30. Martelli S, Zaffagnini S, Bignozzi S, Lopomo N, Marcacci M
(2007) Description and validation of a navigation system for
intra-operative evaluation of knee laxity. Comput Aided Surg
12(3):181–188
31. McLean SG, Oh YK, Palmer ML, Lucey SM, Lucarelli DG,
Ashton-Miller JA, Wojtys EM (2011) The relationship between
anterior tibial acceleration, tibial slope, and ACL strain during a
simulated jump landing task. J Bone Joint Surg Am
93(14):1310–1317
32. Meredick RB, Vance KJ, Appleby D, Lubowitz JH (2008) Out-
come of single-bundle versus double-bundle reconstruction of the
anterior cruciate ligament: a meta-analysis. Am J Sports Med
36(7):1414–1421
33. Monaco E, Labianca L, Conteduca F, De Carli A, Ferretti A
(2007) Double bundle or single bundle plus extraarticular teno-
desis in ACL reconstruction? A CAOS study. Knee Surg Sports
Traumatol Arthrosc 15(10):1168–1174
34. Monaco E, Labianca L, Maestri B, De Carli A, Conteduca F,
Ferretti A (2009) Instrumented measurements of knee laxity: KT-
1000 versus navigation. Knee Surg Sports Traumatol Arthrosc
17(6):617–621
35. Musahl V, Ayeni OR, Citak M, Irrgang JJ, Pearle AD, Wick-
iewicz TL (2010) The influence of bony morphology on the
magnitude of the pivot shift. Knee Surg Sports Traumatol Arth-
rosc 18(9):1232–1238
36. Musahl V, Citak M, O’Loughlin PF, Choi D, Bedi A, Pearle AD
(2010) The effect of medial versus lateral meniscectomy on the
stability of the anterior cruciate ligament-deficient knee. Am J
Sports Med 38(8):1591–1597
37. Oh YK, Kreinbrink JL, Ashton-Miller JA, Wojtys EM (2011)
Effect of ACL transection on internal tibial rotation in an in vitro
simulated pivot landing. J Bone Joint Surg Am 93(4):372–380
38. Palmer I (2007) On the injuries to the ligaments of the knee joint:
a clinical study. 1938. Clin Orthop Relat Res 454:17–22
39. Pernin J, Verdonk P, Si Selmi TA, Massin P, Neyret P (2010)
Long-term follow-up of 24.5 years after intra-articular anterior
cruciate ligament reconstruction with lateral extra-articular aug-
mentation. Am J Sports Med 38(6):1094–1102
40. Pombo MW, Shen W, Fu FH (2008) Anatomic double-bundle
anterior cruciate ligament reconstruction: where are we today?
Arthroscopy 24(10):1168–1177
41. Rotterud JH, Risberg MA, Engebretsen L, Aroen A (2011)
Patients with focal full-thickness cartilage lesions benefit less
Knee Surg Sports Traumatol Arthrosc (2012) 20:793–800 799
123

from ACL reconstruction at 2–5 years follow-up. Knee Surg
Sports Traumatol Arthrosc. doi:10.1007/s00167-011-1739-y
42. Sakane M, Livesay GA, Fox RJ, Rudy TW, Runco TJ, Woo SL
(1999) Relative contribution of the ACL, MCL, and bony contact
to the anterior stability of the knee. Knee Surg Sports Traumatol
Arthrosc 7(2):93–97
43. Slocum DB, Larson RL (1968) Rotatory instability of the knee.
Its pathogenesis and a clinical test to demonstrate its presence.
J Bone Joint Surg Am 50(2):211–225
44. Steckel H, Murtha PE, Costic RS, Moody JE, Jaramaz B, Fu FH
(2007) Computer evaluation of kinematics of anterior cruciate
ligament reconstructions. Clin Orthop Relat Res 463:37–42
45. Tashman S, Kopf S, Fu FH (2008) The kinematic basis of ACL
reconstruction. Oper Tech Sports Med 16(3):116–118
46. Thomee R, Kaplan Y, Kvist J, Myklebust G, Risberg MA,
Theisen D, Tsepis E, Werner S, Wondrasch B, Witvrouw E
(2011) Muscle strength and hop performance criteria prior to
return to sports after ACL reconstruction. Knee Surg Sports
Traumatol Arthrosc 19(11):1798–1805
47. Thomee R, Werner S (2011) Return to sport. Knee Surg Sports
Traumatol Arthrosc 19(11):1795–1797
48. van Eck CF, Kopf S, van Dijk CN, Fu FH, Tashman S (2011)
Comparison of 3-dimensional notch volume between subjects
with and subjects without anterior cruciate ligament rupture.
Arthroscopy 27(9):1235–1241
49. Zaffagnini S, Bignozzi S, Martelli S, Imakiire N, Lopomo N,
Marcacci M (2006) New intraoperative protocol for kinematic
evaluation of ACL reconstruction: preliminary results. Knee Surg
Sports Traumatol Arthrosc 14(9):811–816
50. Zaffagnini S, Bignozzi S, Martelli S, Lopomo N, Marcacci M
(2007) Does ACL reconstruction restore knee stability in com-
bined lesions?: an in vivo study. Clin Orthop Relat Res
454:95–99
51. Zaffagnini S, Bruni D, Martelli S, Imakiire N, Marcacci M, Russo
A (2008) Double-bundle ACL reconstruction: influence of fem-
oral tunnel orientation in knee laxity analysed with a navigation
system—an in vitro biomechanical study. BMC Musculoskelet
Disord 9:25
52. Zaffagnini S, Klos TV, Bignozzi S (2010) Computer-assisted
anterior cruciate ligament reconstruction: an evidence-based
approach of the first 15 years. Arthroscopy 26(4):546–554
53. Zaffagnini S, Signorelli C, Lopomo N, Bonanzinga T, March-
eggiani Muccioli GM, Bignozzi S, Visani A, Marcacci M (2011)
Anatomic double-bundle and over-the-top single-bundle with
additional extra-articular tenodesis: an in vivo quantitative
assessment of knee laxity in two different ACL reconstructions.
Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-
011-1589-7
54. Zantop T, Schumacher T, Diermann N, Schanz S, Raschke MJ,
Petersen W (2007) Anterolateral rotational knee instability: role
of posterolateral structures. Winner of the AGA-DonJoy award
2006. Arch Orthop Trauma Surg 127(9):743–752
800 Knee Surg Sports Traumatol Arthrosc (2012) 20:793–800
123





























