Embed Size (px)
Citation preview

Role of the Venous System in
Baroreceptor-Mediated Reflexes in Man
STEPHENE. EPSTEIN, G. DAVID BEISER, MORRIS STAMPFER, and EucGN BRAUNWALDFrom the Cardiology Branch, National Heart Institute, Bethesda, Maryland
A B S T R A C T Although baroreceptor stimulationproduced by marked alterations in arterial pres-sure has been shown to produce reflex changesin venous tone in animals, the effects on venoustone in man of altering arterial pressure within thephysiologic range have not been clear. In six sub-jects, venous tone did not change when mean ar-terial pressure was raised by 25-40 mmHg, al-though heart rate fell reflexly by 40%o. Venoustone remained constant in 10 subjects when ar-terial pressure was lowered. This contrasted tothe sustained rise in forearm vascular resistance andthe persistent tachycardia that occurred. However,12 subjects continued to respond to these interven-tions by transient venoconstriction. To eliminatepossible emotional influences on venous tone dueto the experimental intervention, venous responseswere studied before and during general anesthesiain five of these subjects. In contrast to the responsebefore anesthesia, an equivalent fall in arterialpressure during anesthesia no longer evoked avenoconstrictor response. Venous reactivity andthe baroreceptor reflex arc remained intact duringanesthesia, since venous tone always rose after adeep inspiration, and tachycardia always accom-panied the fall in arterial pressure. It is concludedthat changes in arterial pressure in the physiologicrange in man do not induce measurable reflexalterations in venous tone, and that the increasessometimes seen with decreases in arterial pressureappear to be due to extraneous psychic factors.
Address requests for reprints to Dr. Eugene Braunwald,Cardiology Branch, National Heart Institute, Bethesda,Md. 20014.
Received for publication 29 May 1967 and in revisedform 21 August 1967.
INTRODUCTION
It has long been recognized that the veins containa large proportion of the total blood volume andhence function as a capacitance system (1-6).Since small alterations in the size of these capaci-tance vessels might p)lay an important homeostaticrole in the control of cardiac outl)plt and(l arteriallressure, much interest has centered upon. themechanisms resl)onsil)le for the regulation of thevenous bed. One mneans by which such regulationcan be achieved is through l)arorecel)tor-mediatedreflexes, and substantial evidence is available tosul)port the contention that this system plays animportant role in the regulation of the degree ofNrenocoinstriction. Thus, a number of investigationshav-e (lemolnstrated that a reduction in carotid sinuspressure produces venoconstriction in the dog(7-12), and that carotid sinus hypertension pro-dluces venodilation (7, 9, 10). As a result of suchstudies, in their moiiograph Heymans and Neilwrote that "the most important change (luring re-flex systemic hypertension of sino-aortic origin isJrobably that of venoconstriction" (13).
On the other hand, Browse, Donald, and Shep-herd (14) have recently shown that venous tonein dogs is not significantly altered l)y changes inbaroreceptor activity if the range of pressure changeinduced in the carotid sinus is kept within physio-logic limits; alterations in venous tone occurredonly with large variations in carotid sinus pressure.The role of the baroreceptor system in regulatingvenous tone in man is also disputed. Thus, uprighttilt, lower-body negative pressure, and drug-in-(luced hypotension have all been shown to befollowed by venoconstriction ( 1 5-20); on the
The Journal of Clinical Investigation Volume 47 1968 139

other hand, several recent studies have shown thatthe venoconstriction after upright tilt and lower-body negative pressure occurs irregularly and isgenerally slight and transient (21-23). It has beenour experience in studies on conscious man that itis often extremely difficult to determine whetheran increase in venous tone after an interventionwhich decreases baroreceptor activity is trulymediated by the baroreceptor system, or is theresult of the well-known responsiveness of thevenous system to many sensory and emotionalstimuli. This consideration suggested the possibil-ity that the variable results of the earlier studiesin man might -have been caused by the reaction ofthe capacitance vessels to stimuli other than thosesensed by the baroreceptor system.
In the present investigation an attempt wasmade to determine whether or not the capacitancesystem participates in reflexes mediated by thebaroreceptor system. Accordingly, venous tonewas measured before and during arterial hyper-tension induced pharmacologically, and arterialhypotension induced pharmacologically and bysubatmospheric pressure applied to the body belowthe iliac crests (lower-body negative pressure).In order to eliminate as completely as possible allextraneous stimuli that might affect venous toneand thereby lead to erroneous interpretations, thefollowing steps were taken.
(a) Each subject was thoroughly familiarizedwith the experimental procedure and was studiedseveral times until reproducible reactions wereelicited.
(b) The response of the veins to arterial hypo-tension was studied before and during general an-esthesia. While the depth of anesthesia used wassufficient to abolish responses to painful and othernoxious stimuli, it did not abolish reflex changesin heart rate in response to induced hypotension,or venoconstriction in response to chest wall move-ment.
METHODS21 male and 3 female subjects whose ages ranged from19 to 54 yr were studied. 11 of the subjects were normalvolunteers and 13 were patients with various forms ofheart disease in functional classes I-III (New YorkHeart Association). 4 of the patients had had a Starr-Edwards mitral valve prosthesis inserted 6-15 monthspreviously. Before any of the patients were included inthe study, it was first determined that each had the usualincrease in venous tone in response to such standard
stimuli as a deep inspiration, mental arithmetic, or appli-cation of ice to the skin (15, 21, 24-29). Venous tone wasmeasured in each subject by the occluded limb techniquerecently described in detail by Samueloff, BevegArd, andShepherd (28). In several subjects forearm venous tonewas also measured simultaneously by either the equili-bration technique (18) or the acute occlusion method(17, 18, 29).
A. OCCLUDEDLIMB TECHNIQUEVenous pressure was measured through a 19 or 21
gauge scalp vein needle or a small polyethylene catheterintroduced percutaneously into a superficial vein of theforearm or hand. The tip of the needle or catheter wasused as the zero reference level for venous pressure. Asphygmomanometric cuff was placed at the wrist when a
-hand vein was used and both above the elbow and at thewrist when a forearm vein was used. The hand or fore-arm was then isolated from the circulation by the rapidinflation of the cuff to 270-300 mmHg. In order to achievevenous pressures less than 20-25 mmHg after -occlusion,it was often necesary to empty the veins by elevating thelimb above the level of the heart before the cuff wasinflated.
B. EQUILIBRATION TECHNIQUE
This technique has been described in detail (18) andwas performed by placing a sphygmomanometric cuffabove the elbow and a Whitney mercury-in-rubber straingauge plethysmograph at the mid-forearm. Venous pres-sure was recorded proximal to the strain gauge througha 21 gauge scalp vein needle. The forearm was elevatedso that the forearm venous pressure was near zero andfailed to decrease with further elevation of the arm.Before any measurements were made, the hand was ex-cluded from the system by inflation of a wrist cuff tosuprasystolic levels. The cuff above the elbow was theninflated to 30 mmHg, and forearm circumference, asmeasured by the plethysmograph, and the venous pressurewere allowed to equilibrate. Since forearm venous pres-sure remains stable at 30 mmHg after equilibration,acute alterations in forearm volume, as assessed bychanges in circumference, reflect a change in venoustone.
C. ACUTEOCCLUSIONTECHNIQUE
With the forearm prepared in the same manner as de-scribed for the equilibration technique, the brachial cuffwas rapidly inflated to 30 mmHg, and forearm bloodflow, expressed in ml/100 g of tissue per minute, was cal-culated from the rate of change in forearm circumferenceduring venous occlusion (18, 29). Venous tone was cal-culated as the ratio of increase in venous pressure to theincrease in forearm volume that occurred during venousocclusion and was expressed in mmHg/ml (17, 18, 29).Forearm vascular resistance (FVR) was calculated asthe ratio of mean arterial pressure to forearm blood flow,expressed as mmHg/ml/100 g per minute.
Baroreceptor activity was modified by the followingmethods.
140 S. E. Epstein, G. D. Beiser, M. Stampfer, and E. Braunwald

(a) With the subjects in the 800 head-up positionphenylephrine (0.3-0.8 mg/minute) was infused at a con-stant rate with an infusion pump to raise mean systemicarterial pressure by 25-30 mmHg.
(b) With the subjects ill the supine positioni, 25-200 j)gof synthetic bradykinin (Sandoz Pharmaceuticals, Han-over, N. J.) was injected intravenously over 5-10 sec tolower mean arterial pressure by 10-30 mmHg.
(c) Nitroglycerin was administered sublingually in adose of 0.4-0.8 mg with the subjects in the 800 head-upposition.
(d) Lower body negative pressure was produced withthe subjects supine by placing the lower part of the bodyfrom the level of the iliac crests into an airtight box(22, 23, 30) and decreasing pressure within it to 60 mmHg below ambient barometric pressure. This level ofnegative pressure was achieved in 60-90 sec and main-tained for 5-15 min.
(e) Subjects were tilted in less than 5 sec from the
aD Y. '67
RESPIRATIONS
E 40VENOUS TONE E
Occiuded lInrib
technique a. 20
>0 '- .' ';'..
E.
VENOUS TONE E 10Equilibrotion Z 14
technique 1-Dn
.......... ....... _.._
-:' --------- .--......._- _|fmin A
Menal ICEArithmetic Deep Inspiration
0rIEE
LADZ)0,zI1-
Qujz0
co
0LU
LUz0
D0zLU
supine to the 800 head-up position on a standard tilt table.The recording of venous tone, measured by the occludedlimb technique, began 1-2 min before the tilt, and wascontinued until the subjects were returned to the supineposition. The subjects remained in the head-up positionfor a period of time ranging from 5 to 15 min. The armin which venous tone was measured was placed on an armboard at right angles to the body in order to maintain arelatively constant relationship to the level of the heartthroughout the tilt. The pressure transducer was mountedon the arm board and was thus always approximately atthe same level as the tip of the needle from which pres-sure was measured. Any deviation from zero referencethat occurred during the tilt was determined by with-drawing the venous needle at the end of the procedure,repositioning it over the vein from which it had beenwithdrawn, and repeating the tilt; venous pressure changesmeasured during the tilt were subsequently corrected forany change from the zero reference point.
b
JM -30
-o p So 20
I _ 0 <
rn
RM 0.1-A- 0o°
-0 M
/~~ ~ ~~~~[ CIads2~~~~~~~~M 30
3>22
10
--C Occluded LImb&---- Equw/brotllon 7echnlque
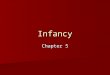
FIGURE 1 The effects on venous tone of ice water placed on the abdomen, mental arithmetic, and deep inspira-tion, as measured simultaneously by the occluded limb and equilibration techniques (see text). a, Recordingshows from above downwards: respirations (as recorded by a pneumograph); venous tone (occluded limbtechnique); venous tone (equilibration technique). b, Venous tone responses obtained from 4 normal subjects.
Venous System in Baroreceptor-Mediated Reflexes in Man 141

VENOUS J.M.I-13-67PRESSURE, 40OCCLUDED
LIMB 20mmHg OL
VENOUS TONE 40FACUTE
OCCLUSION 20-mmHg/ml 0Lm- -
HEART 100
RATEbeats /min
i~~7i~~ute~~~" ~~4L0WER BO0DY NEGATI VE PREUR'/m/nuleDeep
Inspiration
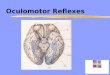
FIGURE 2 The effects on venous tone of deep inspiration and lower body negative pressure, as measuredsimultaneously by the occluded limb and acute occlusion techniques. Lower body negative pressure causesno change in venous tone as recorded either by the occluded limb or acute occlusion techniques. Reactivityof the veins is shown by the venoconstriztion after a deep breath. The increased heart rate that occurs dur-ing lower body negative pressure demonstrates that the intervention initiates baroreceptor reflexes.
The studies were performed at a room temperature of23'C. All subjects had received a light breakfast beforethe study, and were thoroughly familiarized with thelaboratory and methodology of the study. After placementof the catheters, a deep inspiration was performed to en-sure that the venous system was responsive. Dependingoln the particular experimental protocol, the response ofvenous tone to several of the following interventions wasmeasured: mental arithmetic; cold stimulation (by im-mersing the opl)osite hand in ice water or placing severalpieces of ice oln the abdomen) ; 800 head-up tilt; infusionof phenylephrine; injection of bradykinin; sublingualadministration of nitroglycerin; or lower body negativepressure.
In five l)atients with. atrial fibrillation who were sched-uled for elective electrical conversion, the response ofvenous tone to changes in arterial pressure was studiedbefore and (during general anesthesia produced by theintravenous injection of sodium thiopental. These l)a-tients ranged in age from 37 to 68 yr. Three had had amitral valve prosthesis inserted at least 6 months previ-ously. One had mitral stenosis, and one had arterioscler-otic heart disease. Arterial pressure was lovered in fourof the subjects by injecting bradykinin and in one by lowerbody negative pressure. The study (luring anesthesia wasperformed before electrical conversion, and venous tonewas measured by the occluded limb technique. With thismethod it was possible to arrest the circulation to the limbunder investigation before injection of sodium thiopentaland thus obviate any direct effects this agent might haveoln the reactivity of the veins. In order to ensure that thelevel of anesthesia did not abolish the ability of the veinsto respond reflexly, the venous pressure response of theoccluded limib to chest wall movements was tested im-mediately after the intervention used to* lower arterial
pressure by producing a moderately deep, forced in-spiration.
RESULTS
I. Comparison of occluded limb with equilibra-tion and acute occlusion techniques for de-termination of venous tone
The effects of ice placed on the abdomen, mentalarithmetic, and deep inspiration were measuredsimultaneously by the occluded limb and equilibra-tion techniques in four subjects. In all of themeach stimulus increased venous tone as measuredl)y both methods (Figs. 1 a and b).
The effects of a deep inspiration and lowerbody negative pressure were measured simulta-nieously by the occluded limb and acute occlusiontechniques in eight subjects. Similar changes invenous tone were recorded by the two methods ineach subject. At no time was a change in venoustone recorded with one method when such achange was not recorded with the other method(Figs. 2 and 3).
II. Effects of extraneous environmental stimulion venous tone
Many examples of venoconstriction were ob-served in response to extraneous stimuli such asmanipulations of the intravenous tubing, injectionsof saline, sudden noises, the turning on or off of
142 S. E. Epstein, G. D. Beiser, M. Stampfer, and E. Braunwald

VENOUS TONE
Jw
4r~~~-)_F --0 V
RM
CE
_~~~~~~~- - -o')~~~~~~~~~~~~~ - MC-
_---0 @ --
RvA
-o~~~~o
Control LBNP Control DeepInspiration
_- --- Acute Occlusion Me/hod*-O Occluded Limb Technique
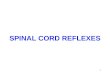
FIGURE 3 The effects on venous tone of lower bodynegative pressure (LBNP) and deep inspiration as mea-sured simultaneously by the occluded limb and acute oc-clusion techniques in six subjects. No change in venoustone during LBNP was recorded by either technique.Venous reactivity is demonstrated by the venoconstrictorresponse to a deep inspiration.
equipment, the presence of a full bladder, the de-velopment of a severe headache, or an investigatortalking or walking in front of the subject. Fig. 4shows the effects of a variety of such stimuli on a
normal subject.
III. Response of venous tone to elevating sys-temic arterial pressure
In six subjects at rest in the 800 head-upposition, elevations in mean arterial pressure uni-formly resulted in decreases in heart rate; an aver-
age increase of 29% in mean arterial pressurecaused an average decrease in rate of 40%o. Al-though this pressure elevation was sufficient tocause pronounced reflex bradycardia, no reflexchanges in venotus tone were observed in any ofthe subjects. All the subjects demonstrated velno-constriction with deep inspiration (Figs. 5 and 6).
IV. Response of venous tone to decreasingsystemic arterial pressure
A. CONSCIOUSSUBJECTS
1. Bradykinin. The effects on venous tone ofthe intravenous injection of bradykinini were stud-ied in 12 subjects. In eight of them, venoconstric-tion occurred consistently. However, in several ofthese studies the increase in venous tone actuallypreceded any fall in arterial pressure (Fig. 7), andan injection of saline often produced as much veno-constriction as occurred during the administrationof bradykinini. It was thus impossible to determinewhether the venoconstriction in these subjects wasinitiated by a baroreceptor-mediated reflex in re-sponse to arterial hypotension, or from the discom-fort (local pain, flushing, palpitations, etc.) pro-duced by bradykinin, or whether it resulted frompsychic stimuli precipitated by the anticipation ofthese effects.
In the other four subjects venous tone wasunchanged during the hypotension produced bybradykinin (Fig. 8). That the baroreceptor reflexarc was intact in these individuals is attested to bythe fact that the fall in arterial pressure was alwaysassociated with a marked increase in heart rate; inthese four subjects a decrease in mean arterialpressure averaging 19%o was accompanied by areciprocal increase in heart rate averaging 26%o.Reactivity of the venous system was demonstratedin each instance by the increase in venous tonethat followed a deep inspiration. While three ofthese four subjects initially responded to brady-kinin by venoconstriction, after one or more ex-periences with the drug venous tone no longerchanged, despite the fact that bradykinin continuedto cause comparable decreases in arterial pressureand elevations of heart rate. All these findings sug-gest that any venoconstriction occurring afterbradykinin was due to its side effects rather thanto a baroreceptor-mediated. reflex resulting fromhypotension.
Venous System in Baroreceptor-Mediated Reflexes in Man
:7020
0
0
30
20
10
0
302010
0
30
2010
0
30
20
0
0
30
20
0
0
a'...1
-i
'-J
L JI)
'3ID0en
LI
zw
143

200X- - -
100ARTERIALPRESSURE
mmHg
MEANARTERIALPRESSURE
mmHg
VENOUSPRESSURE(occluded limb)
mmHg
RESPI RATIONS
HEART RATEbeats/ min
POSITIONED
FIGURE 4 The effects on venous tone of various extraneous stimuli.
2. Nitroglycerin. In an attempt to obviate theinfluence on venous tone of psychic stimuli whichmight be activated by a sudden reduction in ar-
terial pressure, arterial pressure was lowered grad-ually in two subjects by the sublingual adminis-tration of nitroglycerin. Although the systolicarterial pressure decreased by an average of 17%oand pulse pressure by 30%, no increase in venous
tone occurred. That the baroreceptor reflex arc
was intact was again demonstrated by the findingof a reciprocal increase in heart rate, averaging21%o. In both subjects venous tone increased inresponse to a deep inspiration.
3. Lower body negative pressure. Lower bodynegative pressure produced venoconstriction in 4of 10 subjects studied and no change in venous
tone in 6 as measured simultaneously by the oc-
cluded limb and acute occlusion techniques (Figs.2 and 3). Of the subjects who responded withvenoconstriction, in several instances venoconstric-tion occurred immediately after turning on the
vacuum pump and clearly preceded the onset of
negative pressure. In these individuals venocon-
striction could be produced when the pump was
turned on even when it was not attached to the
pressure box. In four of the six subjects whodemonstrated no venoconstriction in response to
lower body negative pressure, the initial exposureproduced a marked rise in venous tone; subsequentexposures, however, consistently produced no
changes in venous tone despite the persistence ofreflex tachycardia (Fig. 9). Although these sixsubjects did not respond to lower body negativepressure with venoconstriction, heart rate in-crease(l in all subjects, and venous responsivenesswas demonstrated by the venoconstriction that oc-
curred after a deep breath. In addition, forearmvascular resistance was measured in five of thesubjects and rose from an average of 29 mmHg/ml per 100 g per min to 40 mmHg/ml per 100 g
per min.4. 800 head-up tilt. In each of five subjects
144 S. E. Epstein, G. D. Beiser, M. Stampfer, and E. Braunwald
MAXIMALEXPI RATION
O1

who were tilted, an increase in venous tone mea-
sured by the occluded limb technique commencedwithin 5-10 sec of the start of the tilt, but returnedto base-line values within 3 min. After this initialtransient increase, no further elevations in venous
tone occurred during the duration of the tilt unlesssyncopal symptoms developed. In 2 such individ-uals venous tone began to increase as arterialpressure and heart rate fell precipitously. Thesechanges occurred well after the 12th min ofhead-up tilt and were preceded by a period ofat least 10 min during which venous pressure inthe occluded limb was equal to that which existedin the supine position.
B. ANESTHETIZED SUBJECTS
In order to eliminate completely the influenceof extraneous psychic stimuli on venous tone, we
studied the response of the venous system to ar-
terial hypotension in five patients before and dur-ing sodium thiopental anesthesia. Each patient hadpreviously demonstrated a venoconstrictor re-
sponse to bradykinin (four patients) or lowerbody negative pressure (one patient) in the un-
anesthetized state. During anesthesia, however,similar decreases in arterial pressure no longerresulted in venoconstriction. In contrast, anes-
thesia did not diminish the reflex tachycardia after
ARTERI ALPRESSURE
mmHg
MEANARTERIALPRESSURE
mmHg
VENOUS PRESSURE( occluded limb)
mmHg
RESPIRATIONS
HEART RATEbeats/min
10~ ~ ~ 1T
200 I-4 ZL7~~~~~~~~~~~~~
100 - -
L ..J ._.
A-:4 ~ ~ ~ ~ ~ -
'40 _7-:.
J ~ ~ ~ Z I
20
; - ---...
...... ... - -.- .. _ _ ..._..
[:,...II' IS 1 '~ ~w___1- 7g--a j---. Li. ..
........iii._.;...._loCo
O.n,--;-iT; tee. m-*.-+.-; Is..] 4 i~~~~~~~~l--3-~iof.ATILT DEEP
INSPIRATION
PHENYLEPHRINE
FIGURE 5 Recording obtained from one subject showingthe effects of intravenous infusion of phenylephrine. Al-
though arterial pressure rises sufficiently to produce a
reflex fall in heart rate, no change in venous tone oc-
curs. A transient increase in venous tone is recorded aftertilt from the supine to the 80° head-up position, and aftera deep inspiration.
HEART RATE
, / min
Control Phenylephrine
mmHg
Control
VENOUS PRESSURE, occluded limb
mmHg
Phenylephrine Control DeepInspiration
FIGURE 6 The effects of arterial hypertension produced by the intravenous infu-
sion of phenylephrine. No decrease in venous tone occurred despite baroreceptor-induced reflex bradycardia. Venous reactivity is demonstrated by the venocon-
strictor response to a deep inspiration.
Veowu System in B3aroreceptor-Mediated Reflexes in Man
40-
30
20 - o
e0
40-
30 -&
20 l
10-.e
14x5

ARTERIALPRESSURE
mmHg
MEANARTERIALPRESSURE
mmHg
VENOUSPRESSURE(occluded limb)
mmHg
RESPI RATIONS
HEARTRATEbeats /min
:-r l ..:... --. .. .I ....j... ;_ -
> A f~l t__ -...--..... --i.. ...i.......:.: ....0.p.+.:. .!:_.....:.... ,.. -- -- ---1: t , , , ~~~~~~~~~~~~.. ,..... .. .... .. .....
i
:.
200 'Ii i- i'' i------- ......------. - .-, ,~~~~~~~~~~~. ...... ... ................,,.--,*---to'
::........
...d..:...
100 Itj~~~~~~~~~~~~~...°i,] _,,..., 1; -- :.:.. ........
min fBRADYKININ BRADYKININ
INSPIRATION
FIGURE 7 The effects on arterial pressure, venous tone, andheart rate of the intravenous administration of bradykinin. Al-though an increase in venous tone occurred after bradykinin,the increase began before any discernible fall in arterial pressure.
hypotension, or venoconstriction in response toforced inspiration (Figs. 10 and 11).
DISCUSSION
The results of this study demonstrate a dissocia-tion between the response to baroreceptor-mediatedreflexes of the capacitance vessels on the one hand,and the heart and resistance vessels on the other;when arterial pressure was changed to a degreesufficient to produce reflex alterations in sym-pathetic discharge to the resistance vessels and tothe heart, as manifest by consistent changes inforearm vascular resistance and heart rate, no
alterations in venous tone occurred when extra-neous psychic stimuli were eliminated. Thus, al-though it has been generally believed that the veinsnormally play an important role in baroreceptor-mediated reflexes, it now appears that the ca-pacitance vessels of the limb do not participate inthese reflexes in man when physiologic alterationsof baroreceptor stimulation are induced.
Although use of the occluded limb technique asa qualitative measure of changes in venous toneis theoretically acceptable, is technically simple,has been used successfully by several investigators(20, 21, 28, 31), and has been found to show
146 S. E. Epstein? G. D. Beiser, M. Stampfer, and E. Braunwald

HEART RATE
beats / min
120F
I0OF
80F-
VENOUS PRESSURE, occluded limb
Control Bradykinin Control Bradykinin Control Inspiration
FIGURE 8 The effects of arterial hypotension produced by the intravenous ad-ministration of bradykinin in four subjects. No increase in venous tone occurreddespite baroreceptor-induced reflex tachycardia. Venous reactivity is demonstratedby the venoconstrictor response to a deep inspiration.
RESPI RATIONS
VENOUSPRESSURE(occluded limb)
mmHg
ARTERIALPRESSURE
rmmHg
MEAN ARTERIALPRESSURE
mmHg
HEART RATEbeats/min
_ _.Th~~~N
40
20-
0
...200
100
0
200 . .....- ...
00
KI0..OF.
F -H1min
INEGATIVE PRESSURE
DEEP'INSP
RB.B, 12/15 /66
~&--t41 I j}.{t~, .~44n4P4d
.A-iQmm"rn-nfllT
.....
....l
NEGATIVE...R..... L.J.E
.........DEE.lN.
FIGURE 9 The effects on venous tone of two sequential exposures to lower body negative pressure in one subj ect.The left panel demonstrates the increase in venous tone that occurred after the subject's first exposure. No venocon-striction occurred several minutes later during the second exposure, as demonstrated in the recording at the right.The degree of reflex tachycardia is unchanged during the second exposure, and venous reactivity is shown by thevenoconstriction after a deep inspiration.
Venous System in Baroreceptor-Mediated Reflexes in Man 147
r%
601 -&
2C

40
_NOUS PRESSURE .loccluded limb) 20 .:.:.:
mmHq
2007. ...
1ENARTERIAL
.0 L4. ',U.:.W
PRESSURE 40
mm , :.: N... D.
RESPIRATIONS *.. 7 I RATION
AWAKE
J. K. 9/22/66.. ...mi!--
HR'=6 -4 !; ;; ;INSPIATIO!A:NE:STHETIZED
FIGURE 10 The effects of anesthesia in one subject on the venous tone response
to a reduction in arterial pressure produced by bradykinin. The left panelshows that while conscious, venoconstriction occurred after bradykinin adminis-tration. The right panel demonstrates that after anesthesia no venoconstrictionoccurred despite a similar decrease in arterial pressure. Anesthesia did not im-pair the heart rate response to hypotension or the increase in venous tone inresponse to a forced deep inspiration.
changes in venous tone similar to those found byother methods (20, 21), a critical comparison ofthis technique with more frequently used methodshas not heretofore been reported. This is of im-portance since it is conceivable that changes in thepressure in a superficial vein of an occluded limbmay not accurately reflect directional changes oc-
curring in other superficial and/or deep veins.However, when venous tone was measured simul-taneously by the occluded limb technique andeither the acute occlusion or the equilibration meth-ods, the directional changes in venous tone occur-
ring in response to any of several stimuli were
identical, regardless of the method used (Figs.1-3).
The present investigation also emphasizes theimportance in the interpretation of data obtainedon the venous bed of recognizing the exquisitesensitivity displayed by the veins to subtle emo-
tional and physical stimuli. For example, the veno-
constriction seen in many of the subjects in re-
sponse to bradykinin, lower body negative pres-
sure, or upright tilt could have been interpreted as
demonstrating that the venous system does in factrespond reflexly to changes in arterial pressure.
That this was not the case was suggested by thetransient nature of the response of the veins to lowerbody negative pressure and tilting at a time whenthe increases in heart rate and forearm vascularresistance persisted. Similar findings relating tothe transient response of the veins to upright tiltwere obtained by Gauer and Thron (21), to lowerbody negative pressure by Plassaras, Brown, Goei,and Greenfield (22), and to upright tilt and lowerbody negative pressure by Samueloff, Browse, andShepherd (23). These latter investigators con-
trasted the transient response of the capacitancevessels of the limb to the sustained response of theresistance vessels throughout the duration of thestimulation (23, 32), a finding confirmed by thisinvestigation. They also observed that if tilting isproduced slowly or if lower body negative pressure
is gradually increased, the magnitude of the in-crease in venous tone is diminished.
Although it has been proposed that the response
of the veins to baroreceptor stimuli may be delayed
148 S. E. Epstein, G. D. Beiser, M, Stampfer, and E. Braunwald
VE
p

oeats / min
120k
lo00
801e
HEART PATE
,0
/i -e-/
601
Control Bradyki ni nLBNP
mmHgVENOUS PRESSURE occluded limb
mm1l9
40( 401
30-
201
301
20
10
Control BradykininLBNP
Control
ANESTHESIA
HEART RATE
-ommHg
401
301
20p
10
VENOUS PRESSURE, occludedmmHg
40k
301
20K
ControlControl Bradykinin Control BradykininLBNP LBNP
FIGURE 11 The effects of anesthesia on the venous tone response to a reduction inarterial pressure. Upper panels demonstrate that venoconstriction occurred in eachsubject, while conscious, after a decrease in arterial pressure produced either bybradykinin (solid lines) or lower body negative pressure (LBNP) (broken lines).Lower panels demonstrate that when noxious and psychic stimuli are eliminated byanesthesia, a similar reduction in arterial pressure no longer results in venoconstric-tion. The reflex tachycardia that occurred during anesthesia suggests that anesthesiadid not significantly diminish baroreceptor reflexes, and the venoconstrictor responseto a forced deep inspiration demonstrates the unimpaired capacity of the veins toreact reflexly.
and require up to 30 min to appear (16), it is ap-
parent that such a delayed response would play no
role in the type of rapid compensatory adjustmentsthat are necessary to buffer the effects of therelatively acute alterations in arterial pressure
that so often occur during everyday life. It wouldalso be difficult to interpret the cause of the
changes in venous tone that take place after so
long a period of time, since the duration of the ex-
perimental intervention might in itself producepotent psychic stimuli capable of changing venous
tone independently of any reflexes mediated by thebaroreceptor system.
In addition to the transient nature of the venous
Venous System in Baroreceptor-Mediated Reflexes in Man
beats / min
DeepInspiration
limb
201
00k
80a
60k
Deepnspiration
-e-
0- --.-
Itp-e- -&
0 -W
0 -0
149

tone responses to upright tilt and lower bodynegative pressure, several other observations pro-vide strong evidence against the hypothesis thatthe increase in venous tone that often occurredafter interventions that lowered arterial pressurewas due to a baroreceptor-mediated reflex. First, itwas observed that the venoconstrictor responsedisappeared in several subjects after bradykininhad been injected or lower body negative pressureapplied several times (Fig. 9). This lack of venousresponse was seen despite changes in arterial pres-sure comparable to those initially present whenvenoconstriction. did occur, and contrasted with thechanges in heart rate and forearm vascular re-sistance which were unaltered with repeated in-terventions. Second, in several subjects in whomvenous tone increased during either pharmacolog-ically or mechanically induced reductions in arterialpressure, the increase in venous tone began beforeany effect oln arterial pressure occurred (Fig. 7).Indeed , in many of these subjects anl injection ofsaline or simply turning oln the vacuum pumpwithout connecting it to the negative pressure boxwas sufficient to evoke a venoconstrictor response.
However, although repeated exposure of 10subjects to the experimental intervention resultedin the elimination of the venoconstrictor responseinitially observed during bradykinin administra-tion and lower body negative pressure, 12 subjectscontinued to respond in such a manner despiterepeated exposure. In order to determine whetherthis venoconstrictor response after either brady-kinin injection or lower body negative pressureresulted from psychic stimulation, venous tone re-sponses were studied before and during generalanesthesia in a group of patients in whom, whileconscious, the intervention leading to arterial hy-poten1sioln consistently l)rodlltced an increase invenctis tone. In this way, noxious and psychicstimnitli could be eliminated alnd the response ofthe cal)acitallce vessels to simple arterial hypoten-sion could be evaluated. When the subjects wereanesthetized, in contrast to the response beforeanesthesia, an equivalent fall in arterial pressureno longer evoked an increase in venous tone (Figs.10 and '11). Although it could be argued thatanesthesia per se was responsible for abolishingreflex responses to arterial hypotension, this seemsunlikely in view of the fact that the reflex tachy-
cardia occurring with hypotension was undimin-ished, and the capacity of the veins to react toreflexes that usually evoke venoconstriction wasunimpaired.
The hypothesis that the capacitance vessels ofthe arm do not normally participate in barorecep-tor-mediated reflexes is also supported by the workof Bevega'rd and Shepherd (33) who showed thatincreasing the transmural pressure across thecarotid arteries did not result in a decrease invenous tone. However, since the aortic arch baro-receptors were not exposed to this stimulus, itcould be argued that they effectively buffered anyreflex changes in venous tone evoked by selectivestimulation of the baroreceptors located in theneck. That this was not the case is shown in thepresent study by the observation that no decreasein venous tone occurred when both the carotid andaortic arch baroreceptors were stimulated simul-taneously by the generalized elevation of systemicarterial presure. The effects of systemic hyper-tension were studied with the subjects in the800 head-up position, since it previously hasbeen shown that a significant degree of sympa-thetic activity is present in this position (34).Hence if alteration of sympathetic activity to theveins were an integral part of the baroreceptor-mediated reflex, it would be expected that withthe subjects in the 80° head-up position veno-dilation would have been observed in response toan increase in arterial pressure.
While this study indicates that the veins do notordinarily participate in baroreceptor reflexes inman it should be emphasized that this conclusioncan be applied only to the veins of the limbs, sinceonly these have been studied thus far. In addition,it appears possible that extreme changes in baro-receptor activity, as would occur in cardiogenicshock, massive hemorrhage, syncope, or in individ-uals subjected to large gravitational stresses suchas those induced during centrifugal studies, mightlead to changes in venous tone. Indeed, this wouldappear to be likely if observations on such- ex-treme interventions in the dog are relevant to man.
In conclusion, the results of this investigationsuggest that while the venous bed of the humanforearm is extremely reactive to a number of stim-uli, physiologic alterations in arterial pressure donot in fact produce reflex changes in venous tone.
150 S. E. Epstein, G. D. Beiser, M. Stampfer, and E. Braunwald

It would thus appear that in the face of posturalchanges, or moderate changes in central bloodvolume, arterial pressure is maintained relativelyconstant by alterations in sympathetic outflow tothe heart and to the resistance vessels, rather thanto the venous bed.
ACKNOWLEDGMENTS
The authors wish to express their appreciation to Mr.Allen Nimetz and Dr. Barry Silverman for their valuableassistance during many phases of this investigation, and toDr. John T. Shepherd, who kindly provided plans forconstruction of the negative pressure box.
REFERENCES
1. Alexander, R. S. 1963. The peripheral venous system.In Handbook of Physiology. W. F. Hamilton and P.Dow, editors. American Physiological Society, Wash-ington, D. C. 2: 1075.
2. Green, H. D. 1944. Circulation: Physical principles.In Medical Physics. 0. Glasser, editor. Year BookPublishers, Chicago. 1: 208.
3. Landis, E. M., and J. C. Hortenstine. 1950. Functionalsignificance of venous blood pressure. Physiol. Rev.30: 1.
4. Greenfield, A. D. M., and G. C. Patterson. 1956. Onthe capacity and distensibility of the blood vessels ofthe human forearm. J. Physiol. (London). 131: 290.
5. Wiedeman, M. P. 1963. Dimensions of blood vesselsfrom distributing artery to collecting vein. CirculationRes. 12: 375.
6. Folkow, B., and S. Mellander. 1964. Veins andvenous tone. Am. Heart J. 68: 397.
7. Alexander, R. S. 1954. The participation of the veno-motor system in pressor reflexes. Circulation Res. 2:405.
8. Salzman, E. W. 1957. Reflex peripheral venoconstric-tion induced by carotid occlusion. Circulation Res. 5:149.
9. Bartelstone, H. J. 1960. Role of the veins in venousreturn. Circulation Res. 8: 1059.
10. Ross, J., Jr., C. J. Frahm, and E. Braunwald. 1961.Influence of carotid baroreceptors and vasoactive drugson systemic vascular volume and venous distensibility.Circulation Res. 9: 75.
11. Gaffney, T. E., W. M. Bryant, and E. Braunwald.1962. Effects of reserpine and guanethidine on venousreflexes. Circulation Res. 11: 889.
12. Zingher, D., and F. S. Grodins. 1964. Ex ffect of carotidbaroceptor stimulation upon the forelimb vascular bedof the dog. Circulation Res. 14: 392.
13. Heymans, C., and E. Neil. 1958. Reflexogenic Areasof the Cardiovascular System. Little, Brown and Co.,Boston.
14. Browse, N. L., D. E. Donald, and J. T. Shepherd.1966. Role of the veins in the carotid sinus reflex..Amn. J. Physiol. 210: 1424.
15. Page, E. B., J. B. Hickam, H. 0. Sicker, H. D. Mc-Intosh, and W. W. Pryor. 1955. Reflex venomotor ac-tivity in normal persons and in patients with posturalhypotension. Circulation. 11: 262.
16. Wood, J. E., and J. W. Eckstein. 1958. A tandemforearm plethysmograph for study of acute responsesof the peripheral veins of man: The effect of environ-mental and local temperature change, and the effect ofp)ooling blood in the extremities. J. Clin. Invest. 37: 41.
17. Sharpey-Schafer, E. P. 1961. Venous tone. Brit. Med.J. 2: 1589.
18. Mason, D. T., and E. Braunwald. 1965. The effects ofnitroglycerin and amyl nitrite on arteriolar and venoustone in the human forearm. Circulation. 32: 755.
19. Mason, D. T., and K. L. Melmon. 1965. Effects ofbradykinin on forearm venous tone and vascular re-sistance in man. Circulation Res. 17: 106.
20. Gilbert, C. A., and P. M. Stevens. 1966. Forearmvascular responses to lower body negative pressureand orthostasis. J. Appl. Physiol. 21: 1265.
21. Gauer, 0. H., and H. L. Thron. 1962. Properties ofveins in vivo: Integrated effects of their smooth mus-cle. Physiol. Rev. 42 (Suppl. 5): 283.
22. Plassaras, G. C., E. Brown, J. S. Goei, and A. D. M.Greenfield. 1963. Effects of simulated postural bloodshifts on the capacity function of the limb vessels.Physiologist. 6: 255.
23. Samueloff, S. L., N. L. Browse, and J. T. Shepherd.1966. Response of capacity vessels in human limbs tohead-up tilt and suction on lower body. J. Appl.Physiol. 21: 47.
24. Duggan, J. J., V. L. Love, an(l R. H. Lyons. 1953. Astudy of reflex venomotor reactions in man. Circula-tion. 7: 869.
25. Burch, G. E., and M. Murtadha. 1956. A study ofthe venomotor tone in a short intact venous segment ofthe forearm of man. Am. Heart J. 51: 807.
26. Eckstein, J. W., W. K. Hamilton, and J. M. McCam-mond. 1958. Pressure-volume changes in the forearmveins of man during hyperventilation. J. Clin. Invest.37: 956.
27. Merritt, F. L., and A. M. Weissler. 1959. Reflexvenomotor alterations during exercise and hyperven-tilation. Am. Heart J. 58: 382.
28. Samueloff, S. L., B. S. Bevegard, and J. T. Shepherd.1966. Temporary arrest of circulation to a limb forthe study of venomotor reactions in man. J. Appl.Phv-siol. 21: 341.
29. Mason, D. T., and E. Braunwald. 1964. Effects ofguanethidine, reserpine, and methyldopa on reflexvenous and arterial constriction in man. J. Clin. Invest.43: 1449.
30. Stevens, P. M., and L. E. Lamb. 1965. Effects oflower body negative pressure on the cardiovascularsystem. Am. J. Cardiol. 16: 506.
Venous System in Baroreceptor-Mediated Reflexes in Man 151

31. Wallace, J. M. 1956. Pressure relationships amongarteries and large and small veins. Circulation. 14:1013.
32. Shepherd, J. T. 1966. Role of the veinis in the circula-tion. Circulation. 33: 484.
33. BevegArd, B. S., and J. T. Shepherd. 1966. Circulatoryeffects of stimulating the carotid arterial stretch re-
ceptors in man at rest and during exercise. J. (Clin.Invest. 45: 132.
34. Robinson, B. F., S. E. Epstein, G. D. Beiser, all(l E.Brautnwald. 1966. Coitrol of heart rate by the auto-nomic nervous system: Studies in man on the initer-relation between baroreceptor mechanisms and exer-cise. Circulationi Res. 19: 400.
152 S. E. Epstein, G. D. Beiser, M. Stampfer, and E. Braunwald