Embed Size (px)
Citation preview

Role of proton therapy in thetreatment of cancer
RAD Magazine, 37, 434, 21-23
By Roger E TaylorProfessor of Clinical Oncology, School of
Medicine, Swansea University and South WestWales Cancer Centre, Singleton Hospital
Swansea
IntroductionHigh energy photons (x-rays) are employed as thestandard ionising radiation modality for mostpatients treated for cancer. However, for selectedgroups of patients, there is increasing interest inthe use of particle therapy, particularly protontherapy, as an alternative form of ionising radia-tion for clinical use. In the UK there is a highlysuccessful proton therapy programme for treat-ing ocular melanoma at the Douglas 62 MeVCyclotron at Clatterbridge, but there is no highenergy proton therapy facility (generally at least200 MeV) in the UK suitable for treating deep-seated tumours. Ensuring access to high energyproton therapy for suitable patients was incorpo-rated into the 2007 Cancer Reform Strategy and,since April 2008, appropriate UK patients arereferred abroad as an official NHS policy.
The concept of using protons for the treatment of canceris not new and the first clinical use of proton therapy was inthe 1950s, with clinical programmes in centres such as theMassachusetts General Hospital, Boston, and Uppsala,Sweden. However, there has been a dramatic increase ininterest in proton therapy over the last two decades. Severalradiotherapy equipment manufacturers have now taken aninterest in not only “marketing” equipment but in develop-ing new technology.
This article discusses the use of proton therapy in clini-cal practice. Other particles such as carbon ions may alsohave potential radiobiological advantages in addition to dosedistribution parameters similar to protons. However,whether these potential radiobiological advantages trans-late into clinical benefit is not clear and still the subject ofclinical investigation programmes in a very limited numberof centres worldwide. Production of protons for clinical useProtons for clinical use are produced by accelerating pro-tons (hydrogen nuclei) in a particle accelerator, usually acyclotron, or alternatively a synchrotron.
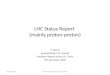
There is also increasing interest in the use of other particles, particularly carbon ions, which in addition to their dose distribution advantages (see below) may confer aradiobiological advantage form their high linear energytransfer (LET). Physical properties of proton beamsThe advantages of proton therapy arise from their physicaldose distribution with the sharp cut-off beyond the BraggPeak. Figure 1 compares the depth-dose characteristics ofproton and megavoltage photon beams. The important pointto note is that the proton beam deposits its energy withintissue along a defined track length as far as the Bragg Peak.Beyond the Bragg Peak there is very little dose deposited. Inother words a proton beam has considerable “stoppingpower” as compared with a photon beam. In order to con-
struct a clinically useful beam the Bragg Peak is “spreadout” (Spread Out Bragg Peak – SOBP). Although there is asignificant skin surface and entrance dose, there is virtu-ally no radiation dose beyond the SOBP.
Unlike many other particles which have been employedfor clinical use (eg neutrons, carbon ions) proton beams havelittle radiobiological advantage in terms of relative biologicaleffectiveness (RBE). The RBE for protons is generallyaccepted to be 1.1, although may be rather higher (approx-imately 1.4) at the very end of the Bragg Peak. Thus theclinical advantages of proton therapy refer to the physicalcharacteristics of the proton beam and the ability to achievea very high conformity index around the tumour. This fea-ture has been used for two main purposes:1, To enable the treatment with high dose (ie escalated
dose) irradiation for relatively radioresistant tumoursadjacent to radiosensitive critical organs, such as skullbase chordomas and chondrosarcomas adjacent to thebrainstem or spinal cord. The majority of patients withthese tumours are adults.
2, For the radiotherapeutic treatment of children the almostcomplete absence of dose delivery beyond the SOBP canbe used to reduce the radiation dose to normal tissuesand hopefully reduce the long-term side effects of radio-therapy (see below). In comparison Intensity Modulatedradiotherapy (IMRT) can also achieve high conformity,but the multiple fields employed will generally deliver alow to intermediate radiation dose to a wide area whichmay be significant for long-term effects (see below).
Proton dose definitionRadiation doses for proton therapy are expressed in terms ofthe dose of photons (x-rays) which would have the same bio-logical effect, taking into account the higher RBE of pro-tons. Proton doses are expressed as cobalt gray equivalent(CGE). Proton therapy centre designThe majority of proton therapy treatment centres have asingle particle accelerator producing a proton beam line,which is then directed electromagnetically as required toone of three to four treatment rooms. A typical design for aproton therapy facility would include a fixed horizontal beamline and several (usually three) gantry rooms (see figures2 and 3).
Largely because of their cost and complexity there arerelatively few facilities worldwide. The original establish-
FIGURE 1Depth dose characteristics of proton and photonbeams.

ment cost of setting up a proton facility is of the order of£70,000,000 and for each course of radical treatment theoverall cost is approximately three times the cost of the mostcomplex photon techniques.
There are operational high energy proton facilities inFrance, Switzerland, Germany, Italy, Japan and Austria,and approximately six centres in the USA.
Most proton therapy centres have the treatment of chil-dren as an important component of their programme. Thechildren most likely to benefit are young children, many ofwhom will require daily anaesthesia for immobilisation.Therefore proton therapy facilities require comprehensivesupport from a paediatric anaesthesia team. Role of proton therapy for adultsSkull base and spinal chordomas and chondrosarcomas Proton therapy is now well established as the most appro-priate radiotherapy modality for these uncommon tumours.
Chordomas are rare tumours which arise from the noto-chord (embryological component of the vertebral column).They generally arise in the sacrococcygeal region or skullbase. Chondrosarcomas are tumours which arise in carti-laginous tissue. They may arise at any site, but when theyarise in the skull base or spine complete surgical resectionis difficult. Both these tumours are also characterised bytheir relative radio-resistance and in order to achieve long-term tumour control it is necessary deliver a high radiationdose. Most are situated adjacent to the radiosensitive centralnervous system, and thus radiation dose escalation can be
problematic. In the case of skull base tumours the brain-stem lies immediately posterior to the resected tumour bed.However to overcome this, the “tight” dose distributionwhich can be achieved with protons can be used to escalatethe dose delivered to the target volume for a skull basetumour to doses in excess of 70 CGE. For these difficult totreat tumours of the skull base local tumour control rates atfive years of 73% for chordoma and 98% for chondrosarcomahave been achieved and reported in a series from theMassachusetts General Hospital/Boston.Proton therapy for melanoma of the irisAlthough the majority of melanomas arise in the skin, arare primary site is the iris of the eye. Radical proton ther-apy provides an excellent alternative to surgery. For manyyears there has been a highly successful ocular melanomaproton therapy programme at the Douglas Cyclotron atClatterbridge. A tumour control rate of 96.7% at four yearshas been reported for a series of 88 patients treated atClatterbridge.Role of proton therapy for childrenRadiotherapy is a highly effective treatment employed forapproximately one third of children with cancer. Howeverits use has been limited by a number of long-term effectswhich are generally more severe, the younger the age of thechild at treatment. These include the neuropsychologicalconsequences of brain radiotherapy, reproductive andendocrine sequelae and the effects of radiotherapy on bonedevelopment. Rationale of proton therapy for childrenAs in the treatment of adults, the physical properties of thedose distribution of the proton beam can be exploited inorder to achieve a radical dose in a target volume close toradiosensitive structures. However the dose distribution maybe used to reduce the volume of non-target tissue receivinga low to intermediate dose (the low dose ‘bath’ effect) andreduce the incidence and/or severity of long-term effects.Summary of late effects of radiotherapyThe long-term effects of radiotherapy for children are sum-marised in table 1. These generally have low threshold andthe severity is dose-related.
The long-term impairment of bone growth represents oneof the most problematic late effects of radiotherapy for chil-dren. The severity is worse for children irradiated at ayoung age, and also influenced by radiation dose, dose perfraction and other treatment factors such as the use ofchemotherapy or steroids. For late effects on bone there is athreshold dose of approximately 10 Gy with a dose/responseup to approximately 35 Gy.
The effects of radiotherapy on bone development are par-ticularly problematic following moderate to high dose radio-therapy to the head and neck region for tumours such asparameningeal rhabdomyosarcoma and retinoblastoma.
The long-term neuropsychological effects of radiotherapyto the brain became evident following the routine use of pro-phylactic cranial radiotherapy for acute lymphoblasticleukaemia (ALL) in the 1970s and 1980s, with an averagedecline in Full Scale IQ of approximately 12 points. For par-tial brain radiotherapy for brain tumours the situation ismore complex. IQ loss may range from no detectable loss atone extreme to a 40 point loss at the other, and is related toa number of factors including age, radiation dose and vol-ume, tumour extent of tumour, the effect of hydrocephalus,post-surgical complications, ‘catch-up’ education and pre-existing conditions such as neurofibromatosis.
Hormone production is also sensitive to the effects ofradiotherapy. Impaired growth hormone secretion is seen inapproximately 80% of children irradiated for brain tumours.Secretion of thyroid stimulating hormone (TSH), adrenocor-ticotrophic hormone (ACTH) and the gonadotrophins folli-cle stimulating hormone (FSH) and luteinising hormone(LH) but may be affected following a dose of greater than40 Gy.
Because of the relatively high probability of long-termsurvival following treatment of children, the risk of radia-tion-induced second malignancy is clinically far more sig-nificant than in the treatment of adults. The overall
FIGURE 2Proton gantry and treatment couch (photo courtesy ofFlorida Proton Centre, Jacksonville).
FIGURE 3Proton therapy centre design – the particle accelera-tor, in this case a synchrotron is on the right, with afixed beam room on the left and three gantry rooms(photo courtesy of MD Anderson Proton Centre,Houston).

cumulative risk of second malignancy following RT in child-hood has been reported as approximately 3-5%.Summary of evidence for proton therapy forchildrenFor the majority of children treated with proton therapy theaim is to reduce the severity of late effects of radiotherapy.These include children with rhabdomyosarcoma where theaim is to reduce the radiation dose to bones outside theradiotherapy target volume, and for several histologicaltypes of brain tumours, where the aim is to reduce the doseto the normal brain and reduce the severity of long-termneuropsychological effects.Base of skull chordoma and chondrosarcomaAs with adults, children with base of skull chordoma andchondrosarcoma have been treated with proton therapy. Theimproved dose distribution can be exploited in order to esca-late the dose and improve local control. However there arerare in children with only a handful of cases per annum inthe UK. RhabdomyosarcomaRhabdomyosarcomas may arise in muscle at any site, buthave a particular predilection for sites in the head and neck,including the nasopharynx and middle ear (where they arereferred to a “parameningeal”) and the orbit. They may alsoarise in the urogenital tract, eg bladder, prostate and uterus.Late effects of treating head and neck primary sites withradiotherapy, particularly in young children are problem-
atic because of the impairment of facial bone growth. Thesuperior dose distribution characteristics of proton comparedwith photon beams and their ability to reduce the dose tonon-target normal tissues have led many centres to employproton radiotherapy for the treatment of rhabdomyosarcomaarising in these areas, with the aim of reducing the severityof late effects.Low grade astrocytomaThe most frequent group of brain tumours arising in child-hood are the low-grade astrocytomas. Of these, the most fre-quent are the cerebellar pilocytic astrocytomas, which canusually be completely resected. However they may arisewithin the midline central structures of the brain, particu-larly associated with the optic nerves where they are gen-erally impossible to remove completely. Radiotherapy canachieve long-term tumour control, but neuropsycholgicalsequelae are of concern particularly for young children.Proton therapy can limit the radiation dose to the normalbrain and hopefully reduce the severity of these long-termeffects.CraniopharyngiomaCraniopharyngioma is a localised developmental tumourwhich arises in the suprasellar area (above the pituitarygland) generally in children or occasionally adults. Althoughbiologically “benign”, craniopharyngiomas are generallyattached to adjacent structures, such as the optic nervesand blood vessels. Complete surgical excision is difficult andcan frequently result in damage to these structures.Involvement of the hypothalamus by tumour, and damagefrom surgery can result in excessive weight gain and/or dis-turbances of temperature regulation. Because of the highprobability of long-term survival proton therapy is now beingused as a means of attempting to minimise some of the neu-ropsychological late effects resulting from radiotherapy.EpendymomaEpendymoma is glial tumour arising generally in childhood.Although primary tumours can arise anywhere in the cen-tral nervous system, the most frequent primary site is thecerebellum. Treatment policies are based on as complete asurgical excision as possible followed by post-operative radio-therapy. As with low grade astrocytomas, proton therapyhas the potential for improved dose distribution and reduc-tion in late effects.Primitive neuro-ectodermal tumour (PNET) includingmedulloblastomaPrimitive neuro-ectodermal tumours (PNETs) comprise animportant group of brain tumours arising mainly in chil-dren. The most frequent group of PNETs are medulloblas-tomas, which arise in the cerebellum. PNETs have thepropensity to metastasise via the cerebro-spinal fluid (CSF),and craniospinal radiotherapy (CSRT) is an essential com-
Organ/tissue Dose threshold Late toxicity
Centralnervoussystem
~ 18 Gy Neuropsychologicaldamage, reduced IQ,learning andbehaviour difficulties
Pituitary ~ 18 Gy forimpaired GHsecretion, higherthreshold (~ 40 Gy) forotherhormones
Multiple hormone defi-ciencies, particularlygrowth hormone (GH),also adreno-corticotrophic hormone(ACTH) and thyroidstimulating hormone(TSH)
Thyroid 20 Gy Reduced thyroidhormone secretion
Gonads 1-2 Gy (testes),6-10 Gy(ovaries)
Infertility if irradiation ofthe testes or ovariescannot be avoided
Bone Threshold ~ 10Gy fractionatedRTWorst in youngchildren treatedwith > 20 Gy
Impaired bone growth,and associated impair-ment of soft tissuedevelopment. This isparticularly severe inthe facial, head andneck regions
Kidney 12-15 Gy Hypertension, reducedrenal function
Dentition ~ 4-10 Gy Dental caries, impaireddental developmentand mal-developmentof jaw
Eye ~ 10 Gy(Cataract), ~ 25 Gy Dry eye
Cataract, dry eye
Second(radiationinduced)malignancy
Low threshold foradenocarcino-mas, eg breast,thyroid. Highthreshold forsarcomas
eg breast and thyroidcancers after RT forHodgkin’s Disease,Sarcomas after RT formany cancers, includ-ing brain tumours
TABLE 1Summary of late effect of radiotherapy for childrenwith cancer.
FIGURE 4Craniospinal radiotherapy dose distribution (figurecourtesy of Dr Nancy Tarbell, Massachusetts Hospital,Boston). Left: proton; and right: photon dose distrib-ution showing sharp fall-off in dose anterior to spinefor protons.

ponent of treatment. The spinal fields employed exit throughthe anterior structures, and as a consequence there is a riskof second malignancies in these organs. Proton spinal fieldscan be used to largely avoid this exit dose to the anteriorstructures (Figure 4). In the treatment of medulloblastomathe boost fields to the cerebellum involve irradiating themiddle and inner ear, which can give rise to long-term hear-ing problems, particularly when radiotherapy is combinedwith chemotherapy. The use of protons for the boost canreduce the radiation dose to the middle and inner ear.Current UK policy for referral abroadThe National Radiotherapy Advisory Group (NRAG) report(2007) included a proton therapy subgroup evidence review.Following this the 2007 Cancer Reform Strategy for Englandincluded a commitment that proton therapy should be avail-
able for selected patient groups. Because there is no suit-able high energy facility available in the UK it was agreedthat patients should be referred to centres abroad. Anational clinical referral panel was established and sinceApril 2008 has been reviewing cases for approval for pro-ton therapy in centres in Europe or North America. Furtherinformation on the function of the panel is available on theNHS Specialised Services website: (http://www.specialisedservices.nhs.uk/serv/proton-beam-therapy).
Criteria for referral abroad for adults are based on a welldefined diagnostic list which includes tumours for which theability to escalate the radiation dose improves tumour con-trol outcomes. These are base of skull and spinal chordoma,base of skull chondrosarcoma and spinal & paraspinal boneand soft tissue sarcomas (non-Ewing’s).
In the case of children the diagnostic list is wide, butcurrently also includes upper age limits even within the pae-diatric age group (see table 2). The capacity of proton ther-apy centres abroad to treat UK patients is finite and thepurpose of the age limits is to ensure that these young chil-dren who are likely to achieve clinically useful benefitreceive this therapy. The clinical referral panel operates onbehalf of the NHS in England, but also considers referralson behalf of Scotland, Wales and Northern Ireland.
Now that referral abroad for proton therapy is estab-lished as part of NHS policy it is important that proton ther-apy centres are developed in the UK. In October 2010, theHealth Secretary announced that three centres (UniversityCollege London Hospital, Christie Hospital, Manchester andUniversity Hospitals, Birmingham) would develop advancedbusiness cases for the development of proton treatment facil-ities. Plans for how these would function are at an earlystage, but the centres will share clinical protocols and exper-tise and provide multi-professional cross cover. The threecentres will need to develop effective networking with refer-ring oncology centres and neurosurgical units across the UK.
Further readingDeLaney T F, Kooy H M (Eds) Proton and Charged Particle Radiotherapy.
Lippincott, Williams & Wilkins 2008. This is a comprehensive textbook whichprovides a detailed review of all aspects of proton and charged particle ther-apy.
NHS Specialised Services website: (http://www.specialisedservices.nhs.uk/serv/proton-beam-therapy). The website includes the current indications forreferral abroad and also relevant practical information.
Merchant T E, Hua C H, Shukla H et al. St Jude Children’s ResearchHospital, Memphis, Tennessee, USA. Proton versus photon radiotherapy forcommon paediatric brain tumours: comparison of models of dose characteris-tics and their relationship to cognitive function. Pediatric Blood & Cancer2008;51:110-117. This paper reports the likely benefits of proton therapy forchildren with a variety of brain tumours based on mathematical modelling ofneuropsychological late effects.
Fitzek M M, Linggood R M, Adams J Munzenrider J E. Combined protonand photon irradiation for craniopharyngioma: long-term results of the earlycohort of patients treated at Harvard Cyclotron Laboratory and MassachusettsGeneral Hospital. International Journal of Radiation Oncology, Biology,Physics 2006;64:1348-1354. This paper reports outcomes for children treatedfor craniopharyngioma.
Munzenrider J E, Liebsch N J. Proton therapy for tumours of the skullbase. Strahlentherapie & Onkologie 1999;175:57-63. This is one of a series ofpublications from the pioneering proton centre at Massachusetts GeneralHospital which have played an important role in establishing proton therapyas the standard radiotherapy modality for skull base chordomas and chon-drosarcomas.
Damato B, Kacperek A, Chopra M et al. Proton therapy of choroidalmelanoma: The Liverpool-Clatterbridge experience. International Journal ofRadiation Oncology, Biology, Physics 2005;62:1405-1411. This paper reportsthe Liverpool-Clatterbridge (Douglas Cyclotron) extensive experience of treatingmelanoma of the iris.
Diagnostic list Age limits for referral
Skull base chordoma orchondrosarcoma
All ages
Retinoblastoma All ages
Spinal & paraspinal boneand soft tissue sarcomas
For “adult” histology casesandosteosarcoma, all ages
Rhabdomyosarcoma• Orbit• Parameningeal and head
& neck • Pelvis
Age up to but not including10th birthday
Ewing’s sarcoma Age up to but not including10th birthday
Pelvic sarcoma For “adult” histology cases andosteosarcoma, all ages. ForEwing’s sarcoma, up to but notincluding 10th birthday
Esthesioneuroblastoma All ages
Craniopharyngioma Age up to but not includingeighth birthday
Low grade glioma Age up to but not includingeighth birthday supratentorialtumours (including optic path-way glioma). Age up to thirdbirthday all cases
Ependymoma Age up to but not includingeighth birthday supratentorialtumours. Age up to third birth-day all cases
Pineal parenchymaltumours
Age up to but not includingeighth birthday
Children with NF1 (and anyother cancer predispositionsyndrome) requiring RT forany condition on the diag-nostic list
All ages
TABLE 2Current NHS specialised services paediatric referrallist.