-
NEUROSURGICAL FOCUS Neurosurg Focus 47 (1):E8, 2019
Physiological changes that occur during a woman’s lifetime may
predispose her to different levels of risk for cerebral aneurysm
formation, growth, and rup-ture. Female sex has been studied as a
significant indepen-dent risk factor for intracranial aneurysm
formation and
growth,10 and the International Study of Unruptured
Intra-cranial Aneurysms evaluated 4060 patients and found that 75%
were women.32 Two instances during which women are believed to have
a unique risk for the development or rupture of cerebral aneurysms
due to hormonal and hemo-
ABBREVIATIONS aSAH = aneurysmal SAH; AVM = arteriovenous
malformation; CCA = common carotid artery; CI = confidence
interval; C-section = caesarean section; GDC = Guglielmi detachable
coil; HBMEC = human brain microvascular endothelial cell; HRT =
hormone replacement therapy; OR = odds ratio; SAH = subarachnoid
hem-orrhage.SUBMITTED March 1, 2019. ACCEPTED April 12,
2019.INCLUDE WHEN CITING DOI: 10.3171/2019.4.FOCUS19228.
Role of pregnancy and female sex steroids on aneurysm formation,
growth, and rupture: a systematic review of the literatureMilli
Desai, MHS,1 Arvin R. Wali, MD, MAS,2 Harjus S. Birk, MD,2 David R.
Santiago-Dieppa, MD,2 and Alexander A. Khalessi, MD, MS2
1School of Medicine and 2Department of Neurological Surgery,
University of California, San Diego, California
OBJECTIVE Women have been shown to have a higher risk of
cerebral aneurysm formation, growth, and rupture than men. The
authors present a review of the recently published neurosurgical
literature that studies the role of pregnancy and female sex
steroids, to provide a conceptual framework with which to
understand the various risk factors associated with cerebral
aneurysms in women at different stages in their lives.METHODS The
PubMed database was searched for “(“intracranial” OR “cerebral”)
AND “aneurysm” AND (“pregnancy” OR “estrogen” OR “progesterone”)”
between January 1980 and February 2019. A total of 392 articles
were initially identi-fied, and after applying inclusion and
exclusion criteria, 20 papers were selected for review and
analysis. These papers were then divided into two categories: 1)
epidemiological studies about the formation, growth, rupture, and
management of cerebral aneurysms in pregnancy; and 2)
investigations on female sex steroids and cerebral aneurysms
(animal stud-ies and epidemiological studies).RESULTS The 20
articles presented in this study include 7 epidemiological articles
on pregnancy and cerebral an-eurysms, 3 articles reporting case
series of cerebral aneurysms treated by endovascular therapies in
pregnancy, 3 epidemiological articles reporting the relationship
between female sex steroids and cerebral aneurysms through
retro-spective case-control studies, and 7 experimental studies
using animal and/or cell models to understand the relationship
between female sex steroids and cerebral aneurysms. The studies in
this review report similar risk of aneurysm rupture in pregnant
women compared to the general population. Most ruptured aneurysms
in pregnancy occur during the 3rd trimester, and most pregnant
women who present with cerebral aneurysm have caesarean section
deliveries. Endovas-cular treatment of cerebral aneurysms in
pregnancy is shown to provide a new and safe form of therapy for
these cases. Epidemiological studies of postmenopausal women show
that estrogen hormone therapy and later age at menopause are
associated with a lower risk of cerebral aneurysm than in matched
controls. Experimental studies in animal models corroborate this
epidemiological finding; estrogen deficiency causes endothelial
dysfunction and inflammation, which may predispose to the formation
and rupture of cerebral aneurysms, while exogenous estrogen
treatment in this popula-tion may lower this risk.CONCLUSIONS The
aim of this work is to equip the neurosurgical and
obstetrical/gynecological readership with the tools to better
understand, critique, and apply findings from research on sex
differences in cerebral
aneurysms.https://thejns.org/doi/abs/10.3171/2019.4.FOCUS19228KEYWORDS
cerebral aneurysm; pregnancy; female sex steroids; estrogen
Neurosurg Focus Volume 47 • July 2019 1©AANS 2019, except where
prohibited by US copyright law
Unauthenticated | Downloaded 06/15/21 12:39 PM UTC
-
Desai et al.
Neurosurg Focus Volume 47 • July 20192
dynamic changes are during pregnancy and menopause. For example,
cardiac output increases by 30%–50% during pregnancy and peaks by
the 3rd trimester,16 and estrogen, which is increased in pregnancy,
appears to enhance cere-bral blood flow.19 In contrast to pregnancy
during which fe-male sex steroids are increased, hormones such as
estrogen are decreased in peri- and postmenopause. Studies suggest
that this estrogen deficiency leads to endothelial dysfunc-tion and
inflammation and explains the increased risk for aneurysmal rupture
in women through menopause, but the exact mechanisms remain
unspecified.25
Cerebral aneurysms in pregnancy represent a rare but important
cause of subarachnoid hemorrhage (SAH), as management and treatment
are complicated by consider-ations of both the mother and the
fetus. The incidence of unruptured aneurysms in pregnancy is not
well established in the literature, and the rate of ruptured
aneurysms ranges from 3 to 11 per 100,000 pregnancies.12 Fifty
percent of all aneurysm ruptures in women younger than 40 years are
reported to be pregnancy related.2 Aneurysm rupture has been shown
to have greater mortality risk in pregnant patients than in
nonpregnant patients.18 There are limited studies on the
relationship of pregnancy and cerebral aneu-rysms: the incidence is
rare, and additionally it is not fea-sible to study cohorts of
pregnant women through random-ized controlled trials. The risk of
aneurysm rupture during pregnancy and subsequent options for
treatment and de-livery are controversial. Previous studies have
reported an increased risk of aneurysm rupture and subsequent SAH
during pregnancy and delivery, with as many as 77% of 154 cases of
verified intracranial hemorrhage during preg-nancy caused by
aneurysm rupture.5 However, the afore-mentioned study did not
include a control group and is therefore limited in interpretation,
and more recent studies indicate the risk of aneurysm rupture
during pregnancy is similar to that of the general population.11
Treatment mo-dalities for aneurysms have changed since early case
re-ports in 1965 showed the options for a ruptured aneurysm in
pregnancy were intracranial surgery versus bed rest with imminent
death.22 Current treatment modalities in-clude endovascular
treatment with a focus on minimizing morbidity from intracranial
surgery, as well as minimizing fetal exposure to angiography.17 We
rely on epidemiologi-cal data and reviews of cases to identify
which trimester of pregnancy patients present with aneurysm
rupture, how aneurysms grow during pregnancy, treatment options,
and whether vaginal versus caesarean section (C-section)
de-liveries are indicated to minimize the risk of aneurysmal SAH
(aSAH) during pregnancy.
Women are at highest risk for aneurysm rupture in the
perimenopausal and postmenopausal state.4 The relation-ship between
postmenopausal estrogen deficiency and aSAH has been studied and
described more extensively through experimental studies using
animal models.25 Un-derstanding the current literature about
experimental mod-els to explain the pathophysiology of cerebral
aneurysms in estrogen-deficient states and epidemiological data to
understand population health components will shed light on the
overall role of female sex steroids and hormones on the development
of cerebral aneurysms. These findings can be applied to multiple
scenarios of aneurysm formation,
growth, and rupture. Furthermore, these findings point to the
development of hormone therapy and targeted therapy to prevent the
formation of aneurysms, halt growth, and prevent aneurysm rupture.
Understanding the role of fe-male sex steroids such as estrogen
will also contribute to an understanding of the underlying sex
disparities that ex-ist in presentation of cerebral aneurysms.
Here, we review the literature on the role of pregnancy and sex
steroids on cerebral aneurysms and summarize salient findings from
epidemiological and experimental studies.
MethodsA systematic review to analyze the role of pregnancy
and
sex steroids in cerebral aneurysms was performed through the
PubMed registry with articles dating from January 1, 1980, to
February 1, 2019. Search terms were “(“intracrani-al” OR
“cerebral”) AND “aneurysm” AND (“pregnancy” OR “estrogen” OR
“progesterone”).” This search yielded a total of 392 results from
the PubMed database. Articles were included within this review if
they presented primary human or animal data or investigated the
epidemiology of pregnancy, sex steroids (i.e., estrogen and/or
progesterone), and cerebral aneurysms. Case-series analyses were
includ-ed. Articles were excluded if aneurysms were not
differen-tiated from other intracranial vascular abnormalities
(i.e., arteriovenous malformations [AVMs]). Single case reports
were excluded from our review because multiple articles have
already synthesized the published single case reports as case
series.
The extracted articles were then divided into two cat-egories:
1) epidemiological studies about the formation, growth, rupture,
and management of cerebral aneurysms in pregnancy; and 2)
investigations on female sex steroids and cerebral aneurysms
(animal studies and epidemio-logical studies). Epidemiological
studies were reviewed for study design, sample size of population
studied, age and gestational age if applicable, and outcomes of
cerebral an-eurysm formation, growth, rupture, treatment, and
man-agement. Animal studies were evaluated for study design (in
vivo vs in vitro), subject type, injury model, number of animals
included in experimental and control groups, and outcomes of
cerebral aneurysm formation, growth, rup-ture, treatment, and
management.
ResultsThree hundred ninety-two articles were initially
identi-
fied from the PubMed database. After applying inclusion and
exclusion criteria, 20 papers were selected for review and
analysis. Using the search criteria, no prospective or randomized
controlled trials in pregnancy were identified. The 20 articles
presented here include 7 epidemiological articles on pregnancy and
cerebral aneurysms, 3 articles reporting case series of cerebral
aneurysms treated by en-dovascular therapies in pregnancy, 3
epidemiological arti-cles reporting the relationship between female
sex steroids and cerebral aneurysms through retrospective
case-control studies, and 7 experimental studies using animal
and/or cell models to understand the relationship between female
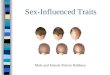
sex steroids and cerebral aneurysms. Figure 1 is a flow-chart
describing the paper selection process.
Unauthenticated | Downloaded 06/15/21 12:39 PM UTC
-
Desai et al.
Neurosurg Focus Volume 47 • July 2019 3
Epidemiological Studies of Cerebral Aneurysms in Pregnancy
Seven epidemiological articles reporting cerebral aneu-rysms in
pregnancy were included. A full description of results from these
investigations can be found in Table 1. Within the 7 articles, we
include 1 case crossover study, 1 retrospective cohort study, 2
retrospective reviews, 1 ret-rospective review and literature
review of cases, 1 case-series report, and 1 literature review of
cases. Among 89 cases from single case reports that have been
summarized in 2 studies, 72 (approximately 80%) represented cases
of ruptured aneurysms in the 3rd trimester of pregnancy.1,23 This
finding is consistent with previous studies and case-series reports
that have found that aneurysms are most likely to rupture in the
3rd trimester of pregnancy and up to 6 weeks postpartum.12,24
Studies that summarized case reports also indicated aneurysm
occlusion through surgi-cal clipping in 53.8% of cases and with an
endovascular procedure in 36.5% of cases,23 and coil embolization
being associated with a lower complication rate than clipping in
patients with ruptured aneurysms (9.5% vs 23.1%).1 One study in our
analysis reported that 19.8% (22 of 111 cases) of hemorrhagic
stroke in pregnancy was due to aneurysm rupture.33 In 2
longitudinal studies in our analysis with a combined sample size of
1130 patients, the relative risk of rupture during pregnancy and
deliveries was compa-rable to the annual rupture risk in the
general population (1.4%, 95% confidence interval [CI] 1.35%–1.57%)
during pregnancy and 0.05% (95% CI 0.0468%–0.0634%) during
delivery; and in the second study, 0.4% (95% CI 0.2%–0.9%) during
pregnancy, delivery, or the puerperium.11,30 In
a study of 5 aneurysms in pregnancy with monitoring of aneurysm
growth, the aneurysms in 4 pregnancies did not change in size,
remaining 2–5 mm, while in 1 pregnancy, the aneurysm increased from
6 to 7 mm during the 3rd trimester, but returned to its original
size in the postpar-tum period.28 Of the 5 studies we include that
compared C-section and vaginal delivery rates in pregnant women
with cerebral aneurysms, all reported increased rates of C-sections
as the method of delivery, regardless of aneurysm rupture or
nonrupture.1,11,23,24,28 A C-section followed by an-eurysm
treatment was reported in 1 study as the accepted delivery method
for ruptured aneurysms,24 whereas in 2 other studies the widespread
use of C-sections in unrup-tured aneurysms was reported to be
unnecessary.11,30
Endovascular Treatment of Cerebral Aneurysms in Pregnancy
Three articles reporting case series of cerebral aneu-rysms
treated by endovascular therapies in pregnancy were identified. A
full description of results from these investi-gations can be found
in Table 2. Summaries of case reports that we have included report
that in 89 cases of cerebral aneurysms in pregnancy, occlusion of
the aneurysm was achieved through surgical clip placement in 53.8%
of cas-es.23 Surgical clipping of aneurysms is still used and
re-ported in the literature, but the most recent neurosurgical
literature has discussed endovascular coil embolization of
aneurysms as a treatment option. In the combined 8 cases of
aneurysms treated endovascularly in pregnancy that we include in
this review, all were treated successfully with Guglielmi
detachable coils (GDCs) and without the need
FIG. 1. Flow diagram demonstrating the search algorithm to
identify literature from the PubMed database. A total of 392
articles were initially identified using our search criteria, of
which 20 met the inclusion and exclusion criteria and were included
within this review.
Unauthenticated | Downloaded 06/15/21 12:39 PM UTC
-
Desai et al.
Neurosurg Focus Volume 47 • July 20194
TABL
E 1.
Seve
n ep
idem
iolo
gica
l stu
dies
on
preg
nanc
y and
cere
bral
aneu
rysm
s
Auth
ors &
Ye
arSt
udy T
ype
Title
Yrs
Samp
le Si
zeM
atern
al Ag
e &
Gesta
tiona
l Age
Relat
ive R
iskVa
ginal
Birth
vs C
-Sec
tion
Conc
lusion
s
Tiel
Groe
ne-
stege
et
al., 2
009
Case
cros
s-ov
er st
udy
The r
isk of
aneu
rys-
mal s
ubar
achn
oid
hemo
rrhag
e du
ring p
regn
ancy
, de
liver
y, an
d the
pu
erpe
rium
in th
e Ut
rech
t pop
ulatio
n
1987
–200
624
418
–42 y
rsRe
lative
risk
of aS
AH du
ring
preg
, deli
v, or
puer
pe-
rium
was 0
.4% (9
5% C
I 0.
2–0.9
%); b
ased
on no
. of
wome
n age
d 18–
42 yr
s w/
in ca
tchme
nt ar
ea &
no. o
f pr
egs w
/in st
udy p
eriod
, ex
pecte
d no.
of pts
w/ a
SAH
durin
g pre
g, de
liv, o
r pue
r-pe
rium
was 1
2, re
sultin
g in
stand
ardiz
ed in
ciden
ce ra
tio
of 0.6
% (9
5% C
I 0.2
–1.1%
)
NAaS
AH ri
sk is
not in
cr du
ring
preg
, labo
r, or p
uerp
e-riu
m; no
need
to ad
vise
again
st pr
eg in
wom
en
w/ an
incr
risk o
f SAH
&
no ev
idenc
e to a
dvise
ag
ainst
vagin
al de
liv in
su
ch w
omen
Kim
et al.
, 20
13Re
tro co
hort
study
Ce
rebr
al an
eury
sms
in pr
egna
ncy a
nd
deliv
ery:
preg
nanc
y an
d deli
very
do no
t inc
reas
e the
risk
of
aneu
rysm
ruptu
re
1988
–200
971
4 RAs
in pr
eg,
172 R
As in
de
liv
NARu
pture
risk
s dur
ing pr
eg &
de
livs w
ere 1
.4% (9
5%
CI 1.
35–1
.57%
) & 0.
05%
(9
5% C
I 0.0
468–
0.063
4%),
resp
ectiv
ely
Of 21
8 deli
vs pe
rform
ed w
/ UA
, 153
wer
e C-s
ectio
n de
livs (
70.18
%, 9
5% C
I 64
.06–
76.3
0%),
sugg
est-
ing th
e rate
of C
-sec
tion
deliv
s in p
ts w/
UAs
is
signifi
cantl
y high
er th
an
in ge
nera
l pop
ulatio
n (p
5
mm
but w
/o ble
bs,
irreg
ular s
hape
, high
-risk
loc
ation
, or in
cr as
pect
ratio
are a
lso at
low
risk
of ru
pture
& ar
e not
likely
to
chan
ge du
ring p
reg
CONT
INUE
D ON
PAG
E 5
»
Unauthenticated | Downloaded 06/15/21 12:39 PM UTC
-
Desai et al.
Neurosurg Focus Volume 47 • July 2019 5
TABL
E 1.
Seve
n ep
idem
iolo
gica
l stu
dies
on
preg
nanc
y and
cere
bral
aneu
rysm
s
Auth
ors &
Ye
arSt
udy T
ype
Title
Yrs
Samp
le Si
zeM
atern
al Ag
e &
Gesta
tiona
l Age
Relat
ive R
iskVa
ginal
Birth
vs C
-Sec
tion
Conc
lusion
s
Yosh
ida et
al.
, 201
7Re
tro re
view
Stro
kes a
ssoc
iated
wi
th pr
egna
ncy
and p
uerp
erium
: a
natio
nwide
stud
y by
the J
apan
Stro
ke
Socie
ty
2012
–201
315
1 pre
g-as
soci-
ated s
troke
sNA
Caus
es &
freq
uenc
ies of
111
hemo
rrhag
ic str
okes
wer
e an
eury
sm, 2
2 (19
.8%);
AVM,
19 (1
7.1%)
; PIH
, 13
(11.7%
); HE
LLP
synd
rome
, 9
(8.1%
); ca
vern
ous a
ngiom
a, 8 (
7.2%)
; RCV
S, 5
(4.5%
); mo
yamo
ya di
seas
e, 2
(1.8%
), oth
er C
VDs,
8 (7.
2%);
other
obste
tric
comp
licati
ons,
7 (6.
3%);
& un
deter
mine
d, 18
(16.
2%)
NAM
ay be
diffe
renc
es in
pro-
porti
on of
hemo
rrhag
ic str
oke a
mong
preg
nant
Japa
nese
wom
en vs
wo
men i
n Wes
tern
coun
tries
Robb
a et a
l., 20
16Re
tro re
view
& lit
revie
w of
case
s
Aneu
rysm
al su
bara
ch-
noid
hemo
rrhag
e in
preg
nanc
y—ca
se
serie
s, re
view,
an
d poo
led da
ta
analy
sis
1995
–200
552
(7 fr
om re
tro
analy
sis of
int
erna
l dat
a &
45 fr
om lit
da
ta ex
trac-
tion)
31.5
± 5.
8 yrs
(ra
nge 2
0–42
; me
dian 3
1);
73.1%
(n =
38)
in
3rd t
rimes
ter,
19.2
% (n
=
10) in
2nd
seme
ster, &
7.7
% (n
= 4)
in
1st tr
imes
ter;
mean
gest
was
29.0
± 8.1
0 wks
(ra
nge 9
–39
wks,
media
n 32
wks)
Mea
n H&H
scor
e (8 c
ases
NA
) 2.7
± 0.9
(ran
ge 2–
5; me
dian 2
); Fis
her s
core
was
de
scrib
ed fo
r 67.3
% (n
= 3
5)
pts; o
f thes
e, 65
.7% (n
= 23
) ha
d Fish
er sc
ore I
V &
34.3%
(n
= 12
) had
Fish
er sc
ore
btwn
I & II
I; dist
ribut
ion of
an
eury
sms w
as in
76.9
%
of pts
in an
terior
circ
ulatio
n (n
= 15
ICA,
n =
9 MCA
, n =
6 AC
omA,
n =
2 ACA
, n =
7 PC
omA)
& 23
.0% in
ps
t circ
ulatio
n (n =
8 VA
, BA
, or P
ICA,
& n
= 4 P
CA);
aneu
rysm
occlu
sion w
as
achie
ved b
y sur
gical
clipp
ing
in 53
.8% of
case
s (n =
28) &
w/
endo
proc
edur
e in 3
6.5%
(n
= 19
)
Data
on m
ode o
f deli
v we
re av
ailab
le fo
r 49/
52
wome
n; 3 (
6.4%)
did n
ot de
liver
at al
l (1 ab
ortio
n &
2 dea
ths i
n uter
o); of
re
maini
ng 4
6 pts,
72.3%
(n
= 3
4) ha
d C-s
ectio
n, of
which
mor
e tha
n 70%
we
re em
erge
ncy p
roce
-du
res;
rema
ining
25.5%
(n
= 12
) had
vagin
al de
liv
RAs i
n pre
gnan
t pts
w/
aSAH
may
be sa
fely
se-
cure
d in t
imely
man
ner;
diagn
ostic
& Tx
stra
tegy
fo
r eac
h of th
ese p
ts sh
ould
cons
ider p
eculi
ar
mater
nal &
obste
tric
factor
s & re
quire
s mu
ltidisc
iplina
ry as
sess
-me
nt inv
olving
obste
t-ric
s, ne
uros
urge
ons,
& int
ensiv
ists
» CON
TINU
ED F
ROM
PAGE
4
CONT
INUE
D ON
PAG
E 6
»
Unauthenticated | Downloaded 06/15/21 12:39 PM UTC
-
Desai et al.
Neurosurg Focus Volume 47 • July 20196
TABL
E 1.
Seve
n ep
idem
iolo
gica
l stu
dies
on
preg
nanc
y and
cere
bral
aneu
rysm
s
Auth
ors &
Ye
arSt
udy T
ype
Title
Yrs
Samp
le Si
zeM
atern
al Ag
e &
Gesta
tiona
l Age
Relat
ive R
iskVa
ginal
Birth
vs C
-Sec
tion
Conc
lusion
s
Roma
n et
al., 2
004
Case
serie
sSu
bara
chno
id he
morrh
age d
ue to
ce
rebr
al an
eury
s-ma
l rup
ture d
uring
pr
egna
ncy
1992
–200
08
31.5
± 4.
8 yrs;
6 p
ts we
re in
3r
d ges
tatio
nal
trime
ster, 1
in
2nd t
rimes
ter,
& 1 i
n 1st
trime
ster
Aneu
rysm
was
resp
onsib
le fo
r SAH
in 6
case
s & fo
r cr
anial
nerv
e pals
y by
aneu
rysm
al co
mpre
ssion
in
2 cas
es; s
urgic
al cli
pping
wa
s per
form
ed in
4 ca
ses;
2 pts
admi
tted w
/ gra
de II
I &
IV st
atus,
resp
ectiv
ely,
were
trea
ted 3
days
after
C-
secti
on w
hen s
tatus
had
impr
oved
; 1 pt
had s
urgic
al cli
pping
at 12
wks
’ ges
t; 1
pt ha
d ane
urys
mal s
urge
ry
befo
re de
liv, a
t 34 w
ks’ g
est,
but a
few
hrs l
ater C
-sec
tion
was p
erfo
rmed
; IVE
was
pe
rform
ed on
2 pts
Emer
genc
y C-s
ectio
n was
pe
rform
ed on
5 pts
w/
3rd t
rimes
ter ge
st &
it pr
eced
ed an
eury
sm Tx
in
4 cas
es; v
agina
l deli
v wa
s per
form
ed on
1 pt
who h
ad co
mplet
e an-
eury
smal
clipp
ing du
ring
1st tr
imes
ter &
in 1
pt w/
2n
d trim
ester
unde
tected
SA
H; th
ere w
as no
deliv
fo
r pt 7
due t
o dea
th of
fetus
, follo
wed a
few
hrs
later
by de
ath of
pt
If ges
tatio
nal a
ge al
lows i
t, im
media
te de
liv sh
ould
be pe
rform
ed w
hene
ver
poss
ible;
other
wise
, feta
l mo
nitor
ing sh
ould
be
perfo
rmed
syste
matic
al-ly;
C-s
ectio
n foll
owed
by
aneu
rysm
al Tx
appe
ars
to be
a wi
dely
acce
pted
strate
gy; o
utcom
e of p
ts w/
good
clini
cal s
tatus
is
as fa
vora
ble as
that
of no
npre
gnan
t ser
ies
Barb
arite
et
al., 2
016
Lit re
view
of ca
ses
The m
anag
emen
t of
intra
cran
ial
aneu
rysm
s dur
ing
preg
nanc
y: a s
ys-
temati
c rev
iew
1991
–201
544
NARu
pture
was
confi
rmed
on
imag
ing in
36 a
neur
ysms
(7
2%),
& mo
st an
eury
sms
ruptu
red d
uring
3rd
trim
ester
(7
7.8%)
; coil
embo
lizati
on
was a
ssoc
iated
w/ lo
wer
comp
licati
on ra
te th
an cl
ip-pin
g in p
ts w/
RAs
(9.5%
vs
23.1%
); fo
r pts
w/ U
As,
surg
ical m
anag
emen
t was
as
socia
ted w
/ 31.9
% fe
wer
comp
licati
ons v
s no T
x
Mos
t pts
unde
rwen
t C-
secti
on de
liv (8
4%),
& a
comb
ined n
euro
surg
ical
obste
trica
l pro
cedu
re
was u
sed f
or 8
pts w
/ RA
s nea
r ter
m
Tx of
intra
cran
ial an
eury
sms
durin
g pre
g is s
afe &
ef
fectiv
e; fu
rther
more
, en
do co
iling w
as su
g-ge
sted a
s 1st-
line T
x ove
r su
rgica
l clip
ping
ACA
= an
terio
r cer
ebra
l arte
ry; A
Com
A =
ante
rior c
ommu
nicat
ing ar
tery
; BA
= ba
silar
arte
ry; C
VD =
card
iovas
cular
dise
ase;
deliv
= de
liver
y; en
do =
endo
vasc
ular;
gest
= ge
statio
n; HE
LLP
= he
moly
sis, e
levate
d live
r en-
zyme
s, low
plat
elet c
ount;
H&H
= H
unt a
nd H
ess;
ICA
= int
erna
l car
otid
arte
ry; in
cr =
incr
ease
(d);
IVE
= int
rava
scula
r emb
oliza
tion;
lit =
litera
ture
; MCA
= m
iddle
cere
bral
arte
ry; N
A =
not a
vaila
ble; P
CA =
pos
terio
r cer
ebra
l ar
tery
; PCo
mA
= po
sterio
r com
munic
ating
arte
ry; P
ICA
= po
sterio
r infe
rior c
ereb
ellar
arte
ry; P
IH =
preg
nanc
y-ind
uced
hype
rtens
ion; p
reg =
preg
nanc
y; ps
t = p
oste
rior;
pt =
patie
nt; R
A =
rupt
ured
aneu
rysm
; RCV
S =
reve
rs-
ible c
ereb
ral v
asoc
onstr
iction
synd
rome
; ret
ro =
retro
spec
tive;
Tx =
trea
tmen
t; UA
= un
rupt
ured
aneu
rysm
; VA
= ve
rtebr
al ar
tery.
» CON
TINU
ED F
ROM
PAGE
5
Unauthenticated | Downloaded 06/15/21 12:39 PM UTC
-
Desai et al.
Neurosurg Focus Volume 47 • July 2019 7
TABL
E 2.
Thr
ee ca
se se
ries o
n ce
rebr
al an
eury
sm ru
ptur
e and
trea
tmen
t/man
agem
ent i
n pr
egna
ncy
Auth
ors &
Ye
arTy
pe of
St
udy
Title
No. o
f Ca
ses
Mate
rnal
Age &
Ge
statio
nal A
geCl
inica
l Pre
sent
ation
& Tx
Vagin
al De
liv vs
C-S
ectio
nCo
nclus
ions
Kizil
kilic
et al.
, 200
3Ca
se se
ries
Endo
vasc
ular t
reatm
ent
of ru
pture
d intr
acra
-nia
l ane
urys
ms du
ring
preg
nanc
y: re
port
of th
ree c
ases
325
, 26,
& 39
yrs
at 10
, 18,
& 28
wk
s’ ge
st
Aneu
rysm
s tre
ated i
n pre
g w/ G
DCs:
1) H&
H gr
ade 2
PCo
mA,
10 ×
7 mm
; 2)
H&H
grad
e 2 lt
ICA,
20 ×
12 m
m; 3)
H&
H gr
ade 1
ACo
mA,
2 ×
3 mm
1 pt’s
aneu
rysm
aros
e dur
ing
fetal
perio
d (8t
h wk o
f pr
eg);
electi
ve ab
ortio
n was
pe
rform
ed du
e to p
roba
ble
injur
y to f
etus f
rom
radia
tion
expo
sure
Preg
nant
wome
n can
be su
cces
sfully
tre
ated f
or ru
pture
d intr
acra
nial
aneu
rysm
s w/ e
ndo a
ppro
ach
Pioti
n et a
l., 20
01Ca
se se
ries
Endo
vasc
ular t
reatm
ent
of ac
utely
ruptu
red i
n-tra
cran
ial an
eury
sms
in pr
egna
ncy
228
yrs a
t 32 w
ks’
gest,
31 yr
s at
22 w
ks’ g
est
Aneu
rysm
s tre
ated i
n pre
g w/ G
DCs:
1) 4-
mm an
eury
sm at
bifu
rcati
on of
rt
ICA;
embo
lizati
on pr
oced
ure p
er-
form
ed w
/ sup
erse
lectiv
e cath
eteriz
a-tio
n of a
neur
ysm
unde
r fluo
rosc
opic
contr
ol; 2)
8-m
m an
eury
sm of
rt
supr
aclin
oid ca
rotid
arter
y; w/
pt un
-de
r gen
eral
anes
thes
ia &
w/ sh
ieldin
g of
fetus
, sup
erse
lectiv
e cath
eteriz
a-tio
n of a
neur
ysm
allow
ed an
eury
sm
occlu
sion w
/ plat
inum
GDCs
1) C-
secti
on be
fore
endo
Tx of
an
eury
sm; 2
) vag
inal d
eliv
after
endo
Tx of
aneu
rysm
Succ
essfu
l mate
rnal
& fet
al ou
tcome
s we
re ac
hieve
d in b
oth ca
ses w
/o cr
aniot
omy &
aneu
rysm
al su
rgica
l ex
posu
re
Mey
ers e
t al.
, 200
0Ca
se se
ries
Endo
vasc
ular t
reatm
ent
of ce
rebr
al ar
tery
aneu
rysm
s dur
ing
preg
nanc
y: re
port
of th
ree c
ases
334
yrs a
t 33 w
ks’
gest;
36 y
rs,
mid-
3rd t
rimes
-ter
; 36 y
rs, la
te 3r
d trim
ester
(in
labor
)
1) pte
riona
l cra
niotom
y rev
ealed
fusi-
form
aneu
rysm
, whic
h cou
ld no
t be
direc
tly cl
ipped
durin
g 11th
wk,
then
co
iling i
n 33r
d wk f
usifo
rm an
eury
sm
of pr
oxim
al rt
PCA;
2) 7-
mm ba
silar
ter
minu
s ane
urys
m &
1.4-m
m lt
supe
rior c
ereb
ellar
aneu
rysm
, 4
GDC-
10 co
ils de
ploye
d, re
sultin
g in
comp
lete o
cclus
ion of
basil
ar te
rmi-
nus a
neur
ysm;
3) 7-
mm an
eury
sm in
rt
PCom
A, 4
GDC-
10 co
ils, p
rodu
cing
comp
lete o
cclus
ion af
ter C
-sec
tion
deliv
1) va
ginal
deliv
; 2) u
nkno
wn;
3) C
-sec
tion o
f twi
ns be
fore
en
do Tx
of an
eury
sm
Limite
d alte
ratio
ns in
mate
rnal-
fetal
phys
iolog
y, low
relat
ive ri
sk of
sig-
nifica
nt ra
diatio
n exp
osur
e to f
etus
when
appr
opria
te tec
hniqu
es ar
e ob
serv
ed, &
succ
essfu
l outc
omes
su
gges
t end
o app
roac
h to a
neu-
rysm
s dur
ing pr
eg is
war
rante
d &
may b
e les
s inv
asive
to bo
th mo
ther
& fe
tus th
an co
nven
tiona
l ne
uros
urge
ry
Unauthenticated | Downloaded 06/15/21 12:39 PM UTC
-
Desai et al.
Neurosurg Focus Volume 47 • July 20198
for open craniotomy.13,17,21 Endovascular treatment occurred
before vaginal deliveries, as well as after C-section
deliver-ies.13,17,21 Time of endovascular treatment ranged from
1st, 2nd, and 3rd trimester of gestation; the only adverse
preg-nancy outcome reported was an elective abortion after
suc-cessful endovascular treatment of an aneurysm during the 8th
week of gestation due to concern for fetal injury from radiation
exposure.13
Epidemiological Studies of Female Sex Steroids and Cerebral
Aneurysms
Three epidemiological articles reporting the relation-ship
between female sex steroids and cerebral aneurysms through
retrospective case-control studies were included. A full
description of results from these investigations can be found in
Table 3. In 76 postmenopausal women with ce-rebral aneurysms
compared to matched controls, both later menopause age (odds ratio
[OR] 0.79, 95% CI 0.63–0.996, p = 0.046) and ever use of hormone
replacement thera-py (HRT; OR 0.23, 95% CI 0.13–0.42, p <
0.0001) were significantly associated with a lower risk of aneurysm
in women in the case group.6 Conversely, and showing the same
results, in 60 postmenopausal women with intradu-ral aneurysms
compared to matched controls, there was a significant association
between a lower rate of oral contra-ceptive (OR 2.1, 95% CI
1.17–3.81, p = 0.01) and HRT (OR 3.09, 95% CI 1.54–6.22, p = 0.002)
use and the presence of a cerebral aneurysm.3 In a study of 233
women in which 43 had hysterectomies, the women with a history of
hyster-ectomy had fewer large aneurysms (8% vs 24%, p = 0.03), and
fewer presented with a ruptured aneurysm (28%) than the
nonhysterectomy group (51%, p = 0.004).20
Experimental (animal and cell model) Studies Investigating
Female Sex Steroids and Cerebral Aneurysms
Seven experimental studies using animal and/or cell models to
understand the relationship between female sex steroids and
cerebral aneurysms were included. A full de-scription of results
from these experimental investigations can be found in Table 4. All
7 studies used in vivo experi-ments, with 1 study using both in
vivo and in vitro (human brain microvascular endothelial cell
[HBMEC]) experi-ments. Four studies used rat models, 2 studies used
mice models, and 1 study used a rabbit model, for a total of 264
animals in the experimental groups, and a total of 98 ani-mals in
the control groups. Mechanisms to create cerebral aneurysms in
animal models were ligation of a common carotid artery (CCA) and
bilateral posterior renal arter-ies,7–9,27 hypertensive diet, and
angiotensin II,7 and injec-tion of elastase into the CSF with
deoxycorticosterone ac-etate salt hypertension.26 Estrogen
deficiency was induced through bilateral oophorectomy7–9,15,26,27
and estrogen E2 receptor blockade.7 Ovariectomized female mice had
a sig-nificantly higher incidence of aneurysms than male mice with
sham ovariectomy,26 and 3 times higher incidence of cerebral
aneurysm formation than females without bilat-eral oophorectomy.8
Estrogen deficiency has been shown to cause endothelial
dysfunction, which may lead to changes in vascular wall integrity
and contribute to aneurysm for-mation. Aneurysm changes in animal
models with oopho-
rectomy and HRT were limited to stage I or II, whereas most
changes in animal models with oophorectomy but no HRT were
identified as saccular dilation (stage III).9 Estrogen deficiency
induced endothelial dysfunction and reactive oxygen species
generation in animal models and HBMECs, which triggered endothelial
damage that led to cerebral aneurysms.27 Estrogen deficiency may
lead to in-flammatory changes that contribute to aneurysm rupture.
Estrogen-deficient mice had more aneurysm ruptures than control
mice, and were found to upregulate IL-17A, which downregulates
E-cadherin, encouraging macrophage in-filtration in the aneurysm
vessel wall.7 Hypertension is an additional risk factor for
aneurysm development in animal models with estrogen deficiency.9,31
Animal models with estrogen deficiency and induced hypertension had
signifi-cantly higher vascular damage scores in multiple regions of
the circle of Willis, signifying that hypertension and estro-gen
deficiency make the circle of Willis more vulnerable to
flow-induced aneurysmal remodeling and tortuosity.31 While estrogen
deficiency itself has been reported by the previously mentioned
studies to increase risk for cerebral aneurysm complications,
exogenous estrogen treatment in an estrogen-deficient state has
been shown to be protective from cerebral aneurysm complications in
the following 3 studies. Treatment with estradiol,7 a selective
estrogen re-ceptor modulator such as bazedoxifene,15 and estrogen26
was shown to decrease the amount of aneurysm ruptures in animal
models of estrogen deficiency.
DiscussionSex differences in the care of patients with
cerebral
aneurysms provide a unique opportunity for collabora-tion among
multiple physician specialties: neurosurgeons,
obstetricians/gynecologists, perinatologists, anesthesiolo-gists,
radiologists, intensivists, and primary care provid-ers. This
systematic review describes the spectrum of risk for women in
pregnancy and in estrogen-deficient states (i.e., menopause,
surgical oophorectomy, etc.) and provides readers with the
information that female sex steroids may impact women and their
cerebrovascular anatomy differ-ently at different stages of their
life.
Studies included in this review suggest that the rate of
aneurysm rupture in pregnancy is not increased compared to the
general population. Neurosurgeons can be prepared to manage
pregnant women with aneurysms similarly to the general population.
As our review indicated, it may not be necessary to advise pregnant
women with cerebral an-eurysms against vaginal deliveries, and
obstetricians can use these data to collaborate with neurosurgeon
colleagues and provide risk stratification to their patients
according-ly.11,30 An older study from 1990 reports a fetal case
fatality rate of approximately 17% as a result of ruptured
intracra-nial aneurysms in pregnancy.5 A more recent retrospective
review of case reports describes a fetal case fatality rate of
approximately 6.5%.23 In reviewing published papers, stud-ies have
not commented extensively on adverse pregnancy outcomes through the
natural history of a patient with a ruptured aneurysm or through
treatment, perhaps because study design is limited to retrospective
and case-series for-mats. We hypothesize that fetal case fatality
rates have de-
Unauthenticated | Downloaded 06/15/21 12:39 PM UTC
-
Desai et al.
Neurosurg Focus Volume 47 • July 2019 9
TABL
E 3.
Thre
e epi
dem
iolo
gica
l stu
dies
on
fem
ale s
ex st
eroi
ds an
d ce
rebr
al an
eury
sms i
n wo
men
Auth
ors &
Ye
arTy
pe of
St
udy
Title
Yrs
Samp
le Si
zeAg
eRe
lative
Risk
Conc
lusion
s
Niss
on et
al.
, 201
8Re
tro ca
se-
contr
olCe
rebr
al an
eury
sms
differ
in pa
tients
wi
th hy
stere
cto-
mies
2010
–201
323
3: his
tory p
ositiv
e for
hy
stere
ctomy
was
pres
-en
t in 18
.5% (4
3/23
3) of
stu
dy po
pulat
ion, n
one
had o
opho
recto
mies
re
cord
ed; o
nly fe
male
pts &
pts e
qual
or ol
der
in ag
e to y
oung
est p
t in
hyste
recto
my gr
oup w
ere
includ
ed in
contr
ol gr
oup
NAPt
s in h
yster
ectom
y gro
up m
ore o
ften
pres
ented
in go
od ne
urolo
gical
cond
ition b
efore
surg
ery (
88%
vs
74%
, p =
0.04
) & ha
d few
er la
rge
aneu
rysm
s (8%
vs 24
%, p
= 0.
03);
fewer
pres
ented
w/ R
A (2
8%) t
han
nonh
yster
ectom
y gro
up (5
1%, p
=
0.004
); 7.7
% (3
/39)
of hy
stere
c-tom
y pts
had l
arge
aneu
rysm
s vs
23.7%
(40/1
69) in
nonh
yster
ec-
tomy g
roup
Fema
le pts
w/ s
urgic
al his
tory o
f hy
stere
ctomy
have
lowe
r rate
s of
large
aneu
rysm
s, pr
esen
t in be
tter
neur
ologic
al co
nditio
n, &
are
less l
ikely
to pr
esen
t w/ R
A th
an
female
s w/o
hyste
recto
my
Ding
et al
., 20
13Re
tro ca
se-
contr
olYo
unge
r age
of
meno
paus
e in
wome
n with
cere
-br
al an
eury
sms
2007
– 201
176
postm
enop
ausa
l wom
en
w/ ce
rebr
al an
eury
sms
(und
er ca
re of
sing
le ph
y-sic
ian);
case
grou
p dat
a we
re m
atche
d w/ th
ose o
f co
ntrol
grou
p for
age (
in ca
tego
ries o
f <45
, 45–
54,
& >5
4 yrs)
& ed
ucati
on
level
(≤12
th gr
ade,
>12t
h gr
ade)
Age a
t men
opau
se w
as
subd
ivide
d into
prem
a-tur
e men
opau
se (<
40
yrs),
early
men
opau
se
(41–4
4 yrs)
, nor
mal
meno
paus
e (45
–55
yrs),
& la
te me
nopa
use
(>56
yrs)
Both
later
men
opau
se ag
e (OR
0.79
, 95
% C
I 0.6
3–0.9
96, p
= 0.
046)
&
ever
use o
f HRT
(OR
0.23
, 95%
CI
0.13
–0.42
, p <
0.000
1) we
re si
g-nifi
cantl
y ass
ociat
ed w
/ lowe
r risk
of
aneu
rysm
in w
omen
in th
e cas
e gr
oup;
for e
ach c
atego
rical
incr in
me
nopa
use a
ge, r
isk of
cere
bral
aneu
rysm
decr
by 21
%
Tren
d sho
wing
that
earlie
r age
at
meno
paus
e is a
ssoc
iated
w/
pres
ence
of ce
rebr
al an
eury
sm;
this
sugg
ests
that
loss o
f estr
ogen
ea
rlier in
a wo
man’s
life m
ay co
n-tri
bute
to pa
thog
enes
is of
cere
bral
aneu
rysm
; thes
e dat
a may
iden
tify
a risk
facto
r for
cere
bral
aneu
rysm
pa
thog
enes
is &
also a
poten
tial
targ
et fo
r futu
re th
erap
iesCh
en et
al.,
2011
Retro
case
-co
ntrol
Oral
contr
acep
tive
and h
ormo
ne
repla
ceme
nt th
erap
y in w
omen
wi
th ce
rebr
al an
eury
sms
2008
–201
060
wom
en w
/ intra
dura
l ce
rebr
al an
eury
sms
NAM
ultiva
riate
logist
ic re
gres
sion
show
ed si
gnific
ant a
ssoc
iation
bt
wn lo
wer r
ate of
oral
contr
a-ce
ptive
use (
OR 2.
1, 95
% C
I 1.1
7–3.
81, p
= 0.
01) &
HRT
(OR
3.09
, 95%
CI 1
.54–
6.22
, p =
0.0
02) &
pres
ence
of ce
rebr
al an
eury
sm
Thes
e dat
a sug
gest
that
expo
sure
to
exog
enou
s estr
ogen
agen
ts in
wome
n is a
ssoc
iated
w/ lo
wer
frequ
ency
of ce
rebr
al an
eury
sms
decr
= de
crea
se(d
).
Unauthenticated | Downloaded 06/15/21 12:39 PM UTC
-
Desai et al.
Neurosurg Focus Volume 47 • July 201910
TABL
E 4.
Seve
n ex
perim
enta
l stu
dies
usin
g an
imal
and/
or ce
ll mod
els t
o un
ders
tand
the r
elat
ions
hip
betw
een
fem
ale s
ex st
eroi
ds an
d ce
rebr
al an
eury
sms
Auth
ors &
Ye
arTi
tleSt
udy
Desig
nSu
bject
Type
Injur
y Mod
elEx
perim
enta
l Gro
upCo
ntrol
Grou
pFin
dings
Conc
lusion
s
Hoh e
t al.,
2018
Estro
gen d
eficie
ncy
prom
otes c
ereb
ral
aneu
rysm
ruptu
re
by up
regu
lation
of
Th17
cells
and
inter
leukin
-17A
which
down
regu
-lat
es E
-cad
herin
In viv
oMi
ceCe
rebr
al an
eury
sm
(lt CC
A &
rt re
nal
arter
y wer
e liga
t-ed
, hyp
erten
sive
diet, a
ngiot
ensin
II)
; estr
ogen
de
ficien
cy (O
VE
or by
estro
gen
E2 re
cepto
r blo
ckad
e)
1819
Estro
gen d
eficie
ncy u
preg
ulates
Th1
7 ce
lls &
IL-17
A &
prom
otes a
neu-
rysm
ruptu
re; e
strog
en-d
eficie
nt mi
ce ha
d mor
e rup
tures
than
co
ntrols
(47%
vs 7%
, p =
0.04
); es
tradio
l sup
pleme
ntati
on or
IL-17
A inh
ibitio
n dec
r the
no. o
f rup
tures
in
estro
gen-
defic
ient m
ice (e
strad
iol
6% vs
37%
, p =
0.04
; IL-1
7A in
hibi-
tion 1
8% vs
47%
, p =
0.01
8)
Estro
gen d
eficie
ncy p
ro-
motes
cere
bral
aneu
rysm
ru
pture
by up
regu
lating
IL-
17A,
whic
h dow
nreg
ulates
E-
cadh
erin,
enco
urag
ing
macr
opha
ge in
filtra
tion i
n an
eury
sm ve
ssel
wall
Mae
kawa
et
al., 2
017
Baze
doxif
ene,
a se
lectiv
e estr
ogen
re
cepto
r mod
ulator
, re
duce
s cer
ebra
l an
eury
sm ru
pture
in
ovar
iectom
ized
rats
In viv
oRa
tCe
rebr
al an
eury
sm
& es
troge
n de
ficien
cy (O
VE,
hemo
dyna
mic
chan
ges,
& HT
N)
n = 8
4; 28
vehic
le,
28 0.
3 mg/
kg/da
y BZ
A, 28
1.0 m
g/kg
/day B
ZA
28Du
ring 1
2-wk
obse
rvati
on, in
ciden
ce
of an
eury
sm ru
pture
was
52%
in
ovar
iectom
ized r
ats; w
/ no e
ffect
on bl
ood p
ress
ure,
Tx w
/ 0.3
or 1.
0 mg
/kg/da
y BZA
lowe
red t
his ra
te to
11%
& 17
%, a
lmos
t the s
ame a
s in
HTN
rats
(17%)
BZA
decr
the i
ncide
nce
of an
eury
sm ru
pture
in
ovar
iectom
ized r
ats
Tutin
o et a
l., 20
15Hy
perte
nsion
and
estro
gen d
eficie
ncy
augm
ent a
neur
ys-
mal re
mode
ling i
n th
e rab
bit ci
rcle
of W
illis i
n res
pons
e to
caro
tid lig
ation
In viv
oRa
bbit
Intra
cran
ial an
eu-
rysm
& es
troge
n de
ficien
cy (H
TN
& es
troge
n defi
-cie
ncy,
then
bilat
CC
A lig
ation
)
83,
ligati
on on
ly Co
mpar
ed to
ligati
on-o
nly ra
b-bit
s, lig
ation
+ H
TN &
estro
gen
defic
iency
grou
p had
sign
ifican
tly
highe
r vas
cular
dama
ge sc
ore i
n 3 r
egion
s: BA
(16.
8 ± 2.
9 vs 7
.8 ±
1.8
, p =
0.02
5), S
CA or
igin (
10.6
± 1.6
vs 5.
6 ± 1.
2, p =
0.02
5), &
PC
omA
origi
n (11
.1 ±
1.5 vs
6.6 ±
1.2
, p =
0.03
1)
HTN
& es
troge
n defi
cienc
y ma
ke ci
rcle
of W
illis m
ore
vulne
rable
to flo
w-ind
uced
an
eury
smal
remo
delin
g &
tortu
osity
; we p
ropo
se
they
do so
by lo
werin
g to
leran
ce of
vasc
ular
tissu
e to h
emod
ynam
ic fo
rces
caus
ed by
CCA
lig
ation
, thus
lowe
ring t
he
thre
shold
nece
ssar
y to
incite
vasc
ular d
amag
eTa
da et
al.,
2014
Roles
of es
troge
n in
the f
orma
tion
of int
racr
anial
aneu
-ry
sms i
n ova
riecto
-mi
zed f
emale
mice
In viv
oMi
ceInt
racr
anial
aneu
-ry
sms (
single
inj
ectio
n of e
las-
tase
into
CSF
w/
deox
ycor
ticos
te-
rone
acet
ate sa
lt HT
N)
3 fem
ale m
ice w
/ bil
at OV
E (su
rgica
l me
nopa
use),
4 ov
ariec
tomize
d fem
ale m
ice w
/ es
troge
n Tx (
surg
i-ca
l men
opau
se +
es
troge
n rep
lace-
ment)
1 male
mou
se
w/ sh
am O
VE
(lapa
rotom
y),
2 fem
ale m
ice
w/ sh
am O
VE
Ovar
iectom
ized f
emale
mice
had
signifi
cantl
y high
er in
ciden
ce of
an-
eury
sms t
han m
ale m
ice w
/ sha
m OV
E (5
9% vs
15%
, p <
0.01);
ther
e wa
s also
a tre
nd fo
r estr
ogen
Tx to
re
duce
incid
ence
of an
eury
sms i
n ov
ariec
tomize
d fem
ale m
ice (3
8%
vs 59
%, p
= 0.
06)
Resu
lts ar
e con
sisten
t w/
epide
miolo
gical
studie
s th
at sh
owed
fema
le pr
e-po
nder
ance
of an
eury
sms
after
perim
enop
ausa
l age
CONT
INUE
D ON
PAG
E 11
»
Unauthenticated | Downloaded 06/15/21 12:39 PM UTC
-
Desai et al.
Neurosurg Focus Volume 47 • July 2019 11
TABL
E 4.
Seve
n ex
perim
enta
l stu
dies
usin
g an
imal
and/
or ce
ll mod
els t
o un
ders
tand
the r
elat
ions
hip
betw
een
fem
ale s
ex st
eroi
ds an
d ce
rebr
al an
eury
sms
Auth
ors &
Ye
arTi
tleSt
udy
Desig
nSu
bject
Type
Injur
y Mod
elEx
perim
enta
l Gro
upCo
ntrol
Grou
pFin
dings
Conc
lusion
s
Jamo
us et
al.
, 200
59Ro
le of
estro
gen
defic
iency
in th
e fo
rmati
on an
d pro
-gr
essio
n of c
ereb
ral
aneu
rysm
s. Pa
rt I: e
xper
imen
tal
study
of th
e effe
ct of
ooph
orec
tomy
in ra
ts
In viv
oRa
tCe
rebr
al an
eury
sm
(ligati
on of
rt C
CA
& bil
at ps
t ren
al ar
teries
, OVX
)
30 ra
ts in
grou
ps II
& III
unde
rwen
t lig
ation
of rt
CCA
&
bilat
pst r
enal
ar-
teries
; 1 m
o afte
r lig
ation
proc
edur
e, gr
oup I
I rats
un
derw
ent O
VX
15; g
roup
I con
-sis
ted of
inta
ct fem
ales
Incid
ence
of ce
rebr
al an
eury
sm
form
ation
in gr
oup I
I (60
%) w
as 3×
hig
her t
han t
hat in
grou
p III (
20%)
, &
mean
aneu
rysm
size
in gr
oup I
I (m
ean 7
6 ± 27
μm) w
as la
rger
than
th
at in
grou
p III (
28 ±
4.6 μ
m; p
-
Desai et al.
Neurosurg Focus Volume 47 • July 201912
TABL
E 4.
Seve
n ex
perim
enta
l stu
dies
usin
g an
imal
and/
or ce
ll mod
els t
o un
ders
tand
the r
elat
ions
hip
betw
een
fem
ale s
ex st
eroi
ds an
d ce
rebr
al an
eury
sms
Auth
ors &
Ye
arTi
tleSt
udy
Desig
nSu
bject
Type
Injur
y Mod
elEx
perim
enta
l Gro
upCo
ntrol
Grou
pFin
dings
Conc
lusion
sTa
mura
et
al., 2
009
Endo
theli
al da
mage
du
e to i
mpair
ed
nitric
oxide
bioa
vail-
abilit
y trig
gers
ce
rebr
al an
eury
sm
form
ation
in fe
male
rats
In viv
o &
in vit
ro
Rat, HB
MEC
sCe
rebr
al an
eury
sm
(ligati
on of
rt C
CA
& bil
at ps
t ren
al ar
teries
, OVX
)
Hype
rtens
ive ra
ts (n
= 20
), OV
X (n
=
18),
ooph
orec
-tom
ized h
yper
-ten
sive (
n = 18
), oo
phor
ectom
ized
hype
rtens
ive w
/ HR
T (n
= 15
), oo
phor
ectom
ized
hype
rtens
ive ra
ts w/
ARB
(n =
16)
15 sh
amIn
ciden
ce of
aneu
rysm
al ch
ange
s (h
igher
than
stag
e I) w
as hi
gher
in
OVX
& oo
phor
ectom
ized h
yper
-ten
sive t
han i
n hyp
erten
sive r
ats
(p <
0.05 v
s HTN
), su
gges
ting t
hat
OVX
marke
dly ex
acer
bated
endo
-th
elial
dama
ge; 1
/2 of
ooph
orec
to-
mize
d hyp
erten
sive r
ats de
velop
ed
sacc
ular a
neur
ysms
(sta
ge II
I); th
is wa
s tru
e for
10%
of hy
perte
nsive
ra
ts &
17%
of O
VX ra
ts (p
<0.0
5);
signifi
cantl
y few
er oo
phor
ectom
ized
hype
rtens
ive ra
ts re
ceivi
ng H
RT
than
untre
ated o
opho
recto
mize
d hy
perte
nsive
rats
exhib
ited c
ereb
ral
aneu
rysm
al ch
ange
s (p <
0.05)
; th
ere w
as no
stati
stica
l diffe
renc
e bt
wn un
treate
d & A
RB-tr
eated
oo
phor
ectom
ized h
yper
tensiv
e rats
; inc
idenc
e of s
accu
lar an
eury
sms
was s
ignific
antly
lowe
r in oo
phor
ec-
tomize
d hyp
erten
sive r
ats re
ceivi
ng
HRT
or A
RB th
an in
ooph
orec
to-
mize
d hyp
erten
sive r
ats re
ceivi
ng
no Tx
(p <
0.05)
Resu
lts su
gges
t that
estro
-ge
n defi
cienc
y ind
uces
en
doth
elial
dysfu
nctio
n &
reac
tive O
2 spe
cies
gene
ratio
n, tri
gger
ing
endo
theli
al da
mage
that
leads
to ce
rebr
al an
eu-
rysm
s, &
that
HTN
is ad
-dit
ional
risk f
actor
; ther
apy
targ
eted a
t end
otheli
um
& ma
nage
ment
of HT
N ma
y help
prev
ent c
ereb
ral
aneu
rysm
s
ARB
= an
giote
nsin
II rec
epto
r bloc
ker;
BZA
= ba
zedo
xifen
e; HT
N =
hype
rtens
ion; O
VE =
ovar
iecto
my; O
VX =
bilat
eral
ooph
orec
tomy
; SCA
= su
perio
r cer
ebell
ar ar
tery.
» CON
TINU
ED F
ROM
PAGE
11
Unauthenticated | Downloaded 06/15/21 12:39 PM UTC
-
Desai et al.
Neurosurg Focus Volume 47 • July 2019 13
creased due to advancements in obstetric care, but further
research is needed to evaluate this topic.
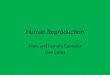
Based on the data that we present, we have created a
diagrammatic algorithm of how to approach a patient who presents
with an incidental aneurysm diagnosed during pregnancy (Fig. 2). We
conclude that if unruptured intra-cranial aneurysms in pregnancy
are stable and asymptom-atic, they may be observed. Symptomatic
and/or enlarging unruptured aneurysms may be treated on an
individual basis. Ruptured intracranial aneurysms in pregnancy are
treated as they would be in nonpregnant patients. Neuro-surgical
considerations generally take precedence over obstetric
considerations for ruptured, symptomatic, and/or growing
intracranial aneurysms. Surgical clipping has historically been
accepted as the treatment for ruptured in-tracranial aneurysms
during pregnancy, but endovascular coiling is now believed to be a
safe treatment and may be preferred to clipping. Because there are
no prospective or randomized controlled trials investigating this
subject, we rely on retrospective and case report data to inform
our clinical decision-making. We have included 2 studies that
address this topic. In a retrospective cohort analysis,
en-dovascular coiling had lower mortality rates in pregnant women
with ruptured aneurysms compared to clipping.11 In a previous
literature review, endovascular coiling was found to have lower
complication rates than surgical clip-ping in pregnant women with
ruptured aneurysms.1 In both studies, surgical management of
ruptured intracranial an-eurysms during pregnancy was found to be
superior to no treatment. Considerations for endovascular coiling
of in-tracranial aneurysms during pregnancy include concern for
harmful effects of radiation to the fetus and potential
harmful effects of anticoagulation. Given that the probabil-ity
of radiation damage increases with increasing absorbed dose, the
radiation dose and stage of fetal development at the time of
exposure should be evaluated for endovascu-lar coiling procedures
during pregnancy. An International Commission on Radiation
Protection report recommended that with optimized abdominal lead
shielding, coiling-re-lated fetal radiation can be neglected.29 In
the studies we include that used coiling for ruptured aneurysms,
radiation exposure was limited through abdominal lead shielding,
limited fluoroscopy in proximity to the uterus, and precau-tions to
limit radiation exposure to the patient as well as adequate fetal
monitoring.11,14,17 Regarding anticoagulation during the
endovascular procedure, heparin is not terato-genic and has
previously been used for coiling of ruptured intracranial aneurysms
during pregnancy, but would need to be discontinued before a
C-section.14 Further research is needed to evaluate additional
endovascular treatment op-tions such as stent-assisted coiling
during pregnancy, and whether aspirin and/or clopidogrel are safe
to use in this setting.
This review elucidates the potential with which neuro-surgeons
and gynecologists can determine how estrogen deficiency contributes
to endothelial dysfunction and in-flammation, which may lead to
cerebral aneurysm forma-tion, growth, and rupture as reported by
multiple studies in this review. Estrogen HRT is commonly used
among postmenopausal women, and this review presents animal data
that suggest improvement in aneurysmal outcomes with HRT.3,6
Hormonal therapies and the effect of targeted drugs on cerebral
aneurysms should be further studied in human clinical trials.
FIG. 2. Diagrammatic algorithm of how to clinically approach a
patient who presents with an incidental aneurysm diagnosed during
pregnancy. *Can use MRI to evaluate aneurysm growth during
pregnancy. Further research is necessary to elucidate size cutoffs
that are clinically meaningful in this population. **Coiling
thought to be a safe treatment and may be preferred to clipping in
pregnancy. Consider abdominal lead shielding and radiation
exposure. ***There is no evidence to suggest that maternal or fetal
outcome is improved by C-section delivery in comparison with
closely supervised vaginal delivery.
Unauthenticated | Downloaded 06/15/21 12:39 PM UTC
-
Desai et al.
Neurosurg Focus Volume 47 • July 201914
Our review suggests that estrogen deficiency in ani-mal models
contributes to aneurysm formation and rup-ture.7,8,26,27,31
Pregnancy is a high-estrogen state, which might suggest less
aneurysm formation and rupture during this time through the
findings of estrogen as a protective cerebrovascular factor in
animal studies. However, our review of epidemiological data in
pregnant women with cerebral aneurysms shows a similar rate of
rupture as the general population. In addition to hormonal and
hemody-namic factors, there may be additional factors inherent to
pregnancy that raise the risk of aneurysm rupture com-pared to that
of the general population, despite a high es-trogen state during
pregnancy. We hope this review article encourages additional
longitudinal research in prospective cohorts to further
characterize the underlying causes of pregnancy and sex steroid
effects on cerebral aneurysms.
ConclusionsThe mechanisms of cerebral aneurysm formation,
growth, and rupture during pregnancy and in estrogen-de-ficient
states are complex. This review article summarizes the current
literature of hormonal- and pregnancy-related risks for cerebral
aneurysms, and can help guide clinical decision-making for both
neurosurgeons and obstetricians and multiple members of the
healthcare team about treat-ment and management options for
pregnant women with cerebral aneurysms. This article helps readers
understand the current research on estrogen deficiency contributing
to vascular abnormalities, and the future research of targeted
drugs and therapies to prevent aneurysmal growth and rup-ture.
Given the sex differences in cerebral aneurysms, this review
article allows readers to understand risk prediction for individual
patients and populations of women with ce-rebral aneurysms at
various stages of their life, from preg-nancy to menopause.
References 1. Barbarite E, Hussain S, Dellarole A, Elhammady MS,
Pe-
terson E: The management of intracranial aneurysms during
pregnancy: a systematic review. Turk Neurosurg 26:465–474, 2016
2. Barrett JM, Van Hooydonk JE, Boehm FH: Pregnancy-related
rupture of arterial aneurysms. Obstet Gynecol Surv 37:557–566,
1982
3. Chen M, Ouyang B, Goldstein-Smith L, Feldman L: Oral
contraceptive and hormone replacement therapy in women with
cerebral aneurysms. J Neurointerv Surg 3:163–166, 2011
4. de Rooij NK, Linn FH, van der Plas JA, Algra A, Rinkel GJ:
Incidence of subarachnoid haemorrhage: a systematic review with
emphasis on region, age, gender and time trends. J Neu-rol
Neurosurg Psychiatry 78:1365–1372, 2007
5. Dias MS, Sekhar LN: Intracranial hemorrhage from aneu-rysms
and arteriovenous malformations during pregnancy and the
puerperium. Neurosurgery 27:855–866, 1990
6. Ding C, Toll V, Ouyang B, Chen M: Younger age of meno-pause
in women with cerebral aneurysms. J Neurointerv Surg 5:327–331,
2013
7. Hoh BL, Rojas K, Lin L, Fazal HZ, Hourani S, Nowicki KW, et
al: Estrogen deficiency promotes cerebral aneurysm rupture by
upregulation of Th17 cells and interleukin-17A which downregulates
E-cadherin. J Am Heart Assoc 7:7, 2018
8. Jamous MA, Nagahiro S, Kitazato KT, Satomi J, Satoh K: Role
of estrogen deficiency in the formation and progression of cerebral
aneurysms. Part I: experimental study of the ef-fect of
oophorectomy in rats. J Neurosurg 103:1046–1051, 2005
9. Jamous MA, Nagahiro S, Kitazato KT, Tamura T, Kuwaya-ma K,
Satoh K: Role of estrogen deficiency in the formation and
progression of cerebral aneurysms. Part II: experimental study of
the effects of hormone replacement therapy in rats. J Neurosurg
103:1052–1057, 2005
10. Juvela S, Poussa K, Porras M: Factors affecting formation
and growth of intracranial aneurysms: a long-term follow-up study.
Stroke 32:485–491, 2001
11. Kim YW, Neal D, Hoh BL: Cerebral aneurysms in pregnan-cy and
delivery: pregnancy and delivery do not increase the risk of
aneurysm rupture. Neurosurgery 72:143–150, 2013
12. Kittner SJ, Stern BJ, Feeser BR, Hebel R, Nagey DA,
Buch-holz DW, et al: Pregnancy and the risk of stroke. N Engl J Med
335:768–774, 1996
13. Kizilkilic O, Albayram S, Adaletli I, Kantarci F, Uzma O,
Islak C, et al: Endovascular treatment of ruptured intracrani-al
aneurysms during pregnancy: report of three cases. Arch Gynecol
Obstet 268:325–328, 2003
14. Liu P, Lv X, Li Y, Lv M. Endovascular management of
intra-cranial aneurysms during pregnancy in three cases and re-view
of the literature. Interv Neuroradiol 21:654–658, 2015
15. Maekawa H, Tada Y, Yagi K, Miyamoto T, Kitazato KT, Korai M,
et al: Bazedoxifene, a selective estrogen receptor modulator,
reduces cerebral aneurysm rupture in ovariecto-mized rats. J
Neuroinflammation 14:197, 2017
16. Meah VL, Cockcroft JR, Backx K, Shave R, Stöhr EJ: Car-diac
output and related haemodynamics during pregnancy: a series of
meta-analyses. Heart 102:518–526, 2016
17. Meyers PM, Halbach VV, Malek AM, Phatouros CC, Dowd CF,
Lawton MT, et al: Endovascular treatment of cerebral artery
aneurysms during pregnancy: report of three cases. AJNR Am J
Neuroradiol 21:1306–1311, 2000
18. Miller HJ, Hinkley CM: Berry aneurysms in pregnancy: a 10
year report. South Med J 63:279, 1970
19. Nevo O, Soustiel JF, Thaler I: Cerebral blood flow is
in-creased during controlled ovarian stimulation. Am J Physiol
Heart Circ Physiol 293:H3265–H3269, 2007
20. Nisson PL, Meybodi AT, Brasiliense L, Berger GK, Golisch K,
Benet A, et al: Cerebral aneurysms differ in patients with
hysterectomies. World Neurosurg 120:e400–e407, 2018
21. Piotin M, de Souza Filho CB, Kothimbakam R, Moret J:
En-dovascular treatment of acutely ruptured intracranial aneu-rysms
in pregnancy. Am J Obstet Gynecol 185:1261–1262, 2001
22. Pool JL: Treatment of intracranial aneurysms during
preg-nancy. JAMA 192:209–214, 1965
23. Robba C, Bacigaluppi S, Bragazzi NL, Bilotta F, Sekhon MS,
Bertuetti R, et al: Aneurysmal subarachnoid hemor-rhage in
pregnancy—case series, review, and pooled data analysis. World
Neurosurg 88:383–398, 2016
24. Roman H, Descargues G, Lopes M, Emery E, Clavier E, Diguet
A, et al: Subarachnoid hemorrhage due to cerebral aneurysmal
rupture during pregnancy. Acta Obstet Gynecol Scand 83:330–334,
2004
25. Tabuchi S: Relationship between postmenopausal estrogen
deficiency and aneurysmal subarachnoid hemorrhage. Behav Neurol
2015:720141, 2015
26. Tada Y, Makino H, Furukawa H, Shimada K, Wada K, Li-ang EI,
et al: Roles of estrogen in the formation of intracrani-al
aneurysms in ovariectomized female mice. Neurosurgery 75:690–695,
2014
27. Tamura T, Jamous MA, Kitazato KT, Yagi K, Tada Y, Uno M, et
al: Endothelial damage due to impaired nitric oxide bioavailability
triggers cerebral aneurysm formation in fe-male rats. J Hypertens
27:1284–1292, 2009
Unauthenticated | Downloaded 06/15/21 12:39 PM UTC
-
Desai et al.
Neurosurg Focus Volume 47 • July 2019 15
28. Tanaka H, Katsuragi S, Tanaka K, Iwanaga N, Yoshimatsu J,
Takahashi JC, et al: Impact of pregnancy on the size of small
cerebral aneurysm. J Matern Fetal Neonatal Med 30:2759–2762,
2017
29. Task Group on Control of Radiation Dose in Computed
To-mography: Managing patient dose in computed tomography. A report
of the International Commission on Radiological Protection. Ann
ICRP 30:7–45, 2000
30. Tiel Groenestege AT, Rinkel GJ, van der Bom JG, Algra A,
Klijn CJ: The risk of aneurysmal subarachnoid hemor-rhage during
pregnancy, delivery, and the puerperium in the Utrecht population:
case-crossover study and standardized incidence ratio estimation.
Stroke 40:1148–1151, 2009
31. Tutino VM, Mandelbaum M, Takahashi A, Pope LC, Sid-diqui A,
Kolega J, et al: Hypertension and estrogen defi-ciency augment
aneurysmal remodeling in the rabbit circle of Willis in response to
carotid ligation. Anat Rec (Hoboken) 298:1903–1910, 2015
32. Wiebers DO, Whisnant JP, Huston J III, Meissner I, Brown RD
Jr, Piepgras DG, et al: Unruptured intracranial aneu-rysms: natural
history, clinical outcome, and risks of surgical and endovascular
treatment. Lancet 362:103–110, 2003
33. Yoshida K, Takahashi JC, Takenobu Y, Suzuki N, Ogawa A,
Miyamoto S: Strokes associated with pregnancy and puerpe-rium: a
nationwide study by the Japan Stroke Society. Stroke 48:276–282,
2017
DisclosuresThe authors report no conflict of interest concerning
the materi-als or methods used in this study or the findings
specified in this paper.
Author ContributionsConception and design: Khalessi, Desai,
Wali, Santiago-Dieppa. Acquisition of data: Desai, Wali. Analysis
and interpretation of data: Desai, Wali, Santiago-Dieppa. Drafting
the article: all authors. Critically revising the article:
Khalessi, Desai, Wali, Santiago-Dieppa. Reviewed submitted version
of manuscript: all authors. Approved the final version of the
manuscript on behalf of all authors: Khalessi. Statistical
analysis: Desai, Wali. Administrative/technical/material support:
Khalessi, Desai, Wali. Study supervision: Khalessi, Desai,
Wali.
CorrespondenceAlexander A. Khalessi: University of California,
San Diego, CA. [email protected].
Unauthenticated | Downloaded 06/15/21 12:39 PM UTC