Embed Size (px)
Citation preview

Journal of Conservative Dentistry | Jul-Aug 2013 | Vol 16 | Issue 4284
Address for correspondence:Dr. M Jayadev, Department of Conservative Dentistry and Endodontics, Panineeya Dental College, Road No 5, Kamala Nagar, Dilsukhnagar, Hyderabad - 500 060, Andhra Pradesh, India. E-mail: [email protected]
Date of submission : 03.12.2012Review completed : 21.03.2013Date of acceptence : 22.04.2013
Role of Platelet rich fibrin in wound healing: A critical reviewBalaram Naik, P Karunakar1, M Jayadev1, V Rahul Marshal2
Department of Conservative Dentistry and Endodontics, Sri Dharmasthala Manjunatheshwara College of Dental Sciences, Dharwad, Karnataka, 1Department of Conservative Dentistry and Endodontics, Panineeya Dental College, Hyderabad, 2Department of Oral Medicine and Radiology, Panineeya Dental College, Hyderabad, Andhra Pradesh, India
A b s t r a c t
Aim: Aim: The aim is to review and discuss the strategies available for use of platelet rich fibrin as healing aid in dentistry.
BackgroundBackground: Platelet rich fibrin (PRF) is a fibrin matrix in which platelet cytokines, growth factors, and cells are trapped and may be released after a certain time and that can serve as a resorbable membrane. Choukroun and his associates were amongst the pioneers for using PRF protocol in oral and maxillofacial surgery to improve bone healing in implant dentistry. Autologous PRF is considered to be a healing biomaterial, and presently, studies have shown its application in various disciplines of dentistry.
Materials and Methods:Materials and Methods: By using specific keywords, electronic search of scientific papers was carried out on the entire PubMed database with custom range of 5 years. The electronic search yielded 302 papers; based on inclusion and exclusion criteria which were specifically predetermined, 72 papers were identified as suitable to the inclusion criteria and the remaining 230 papers were excluded. After adding three more selected papers through hand search, full text of all the articles retrieved and review was done. By pooling the extracted data from selected papers, the reviewed data was synthesized.
Conclusion:Conclusion: Recently by showing good promising results with use of the PRF, it has proved to have a good prospect for its use as healing aid in various aspects of the dentistry.
Keywords: Growth factors; platelet rich fibrin; platelet rich plasma; wound healing
INTRODUCTION
Development of the bioactive surgical additives is one of the great challenges of clinical research which has been used to regulate inflammation and increase the speed of healing process.[1] A wide range of intra- and extraarticular events and various signaling proteins mediate and regulate the healing process of both hard and soft tissues, respectively. But understanding this entire process is still incomplete; however, it is known that platelets play a crucial role not only in hemostasis, but also in the wound healing process.[2]
In 1974, platelets regenerative potentiality was introduced, and Ross et al.,[3] were first to describe a growth factor from platelets. After activation of the platelets which are trapped within fibrin matrix, growth factors released and stimulate the mitogenic response in the bone periosteum during normal wound healing for repair of the bone.[4] Better understanding of physiologic properties of platelets
in wound healing since last two decades led to increase its therapeutic applications in the various forms showing varying results.
MATERIALS AND METHODS
Structured electronic search of scientific papers published up to 15th March 2013 was carried out on the (http://www.ncbi.nlm.nih.gov/pubmed) entire PubMed database with a custom range of 5 years and hand search for term “platelet rich fibrin” (PRF); which was further filtered using Boolean operators (AND, OR, NOT) and combination of specific keywords as following: “Platelet rich fibrin Choukroun”, “platelet rich fibrin in dentistry”, “platelet rich fibrin dental”, “platelet rich fibrin in maxillofacial surgery”, “platelet rich fibrin implant”, “platelet rich fibrin periodontal”, “platelet rich fibrin extraction”, and “platelet rich fibrin oral”; abstracts of all relevant papers were thoroughly scrutinized and in the end and articles pertaining to the topic (PRF) were included. Relevant literature for “platelet
Review Article
Access this article online
Quick Response Code:Website: www.jcd.org.in
DOI: 10.4103/0972-0707.114344

Naik, et al.: Healing potential of PRF
285Journal of Conservative Dentistry | Jul-Aug 2013 | Vol 16 | Issue 4
rich fibrin” in common dental textbooks and for additional information bibliographies of papers and review articles together with appropriate peer reviewed journals were also scrutinized. The inclusion criteria set for this review were: All case reports, case series, original research papers, review papers, in vitro/in vivo studies, animal studies, and controlled clinical trials on PRF used in dentistry related studies. Exclusion criteria consisted of studies that did not meet the above inclusion criteria.
The electronic search yielded 302 papers, out of which 72 were identified as suitable papers to the inclusion criteria and the remaining 230 were excluded [Figure 1]. Only 75 papers selected, 72 from electronic search and three from other searches and full text of all articles retrieved and reviewed [Table 1], out of which 22 in vivo studies, 13 in vitro studies, 14 case reports, 11 animal studies, six controlled clinical trials, two combined in vivo and in vitro studies, and seven reviews [Figure 2].
PLATELET CONCENTRATE EVOLUTION
Platelets isolated from the peripheral blood acts as autologous source of growth factors. In general medical practice, platelet concentrate which is derived from blood can be used for the prevention and treatment of bleeding due to conditions like severe thrombocytopenia, severe oral hemorrhage associated with medullary aplasia, acute leukemia, etc.[5] The use of fibrin adhesives helps to initiate the development of platelet concentrate as a bioactive surgical additive. Several components in blood has been recognized since 1990, which are a part of the natural healing process and have the potential to accelerate wound healing when added to wounded tissues or surgical sites. In 1970, fibrin glue formed by polymerizing fibrinogen with thrombin and calcium was first described. Actually, it was prepared using donor plasma; but the stability and quality of fibrin glue was low because of low concentration
Table 1: Literature on platelet rich fibrinAuthor Year Type of
literature/studyConclusion/result
Gassling et al.[20] 2013 Mar In vitro Metabolic activity and proliferation of human osteoblast cells in vitro were supported to a significant higher extent by eluates from PRF membranes. Proliferation was significantly higher on PRF membranes and PRF clot than on Bio-Gide® membranes
Keyhan et al.[21] 2013 Mar A double-blinded prospective clinical trial
Combination of fat and PRF is more effective than the combination of fat and PRP in the context of facial lipostructure surgery
Gassling et al.[22] 2013 Jan In vivo Within the limits of study, coverage of lateral sinus window with two different absorbable membranes (PRF or a conventional collagen membrane), Bio-Gide® has been shown to result in a similar amount of vital bone formation and residual bone substitute
Pradeep et al.[23] 2012 Dec In vivo Within the limit of present study, there was similar PD (probing depth) reduction, CAL (clinical attachment level) gain, and bone fill at sites treated with PRF or PRP with conventional open flap debridement. Since PRF is less time consuming and less technique sensitive, it may seem a better treatment option than PRP
Vinaya Kumar et al.[24]
2012 Nov Review This second generation platelet concentrate called platelet rich fibrin (PRF), has been widely used to accelerate soft and hard tissue healing. Its advantages over better known PRP includes ease of preparation/application, minimal expense, and lack of biochemical modification (no bovine thrombin or anticoagulant is required)
Ozdemir et al.[25] 2012 Nov Animal study When used in conjunction with titanium barriers, PRF use can increase the quality of newly formed bone and enhance the rate of bone formation due to concentration of growth factors
Yang et al.[26] 2012 Nov Animal study This study demonstrated using autogenic cell transplantation in a porcine model, that dental bud cells (DBCs) seeded into fibrin glue-PRF could regenerate a complete tooth
Shivashankar et al.[27]
2012 Oct Case report On the basis of the results obtained in our case report we conclude that revitalization of necrotic-infected immature tooth is possible under conditions of total canal disinfection and PRF is an ideal biomaterial for pulp-dentin complex regeneration
Kocyigit et al.[28] 2012 Sep Case report This clinical report presents a successful reconstruction of a severe anterior mandibular alveolar bony defect using symphysis graft and PRF
Bambal et al.[29] 2012 Sep-Oct Case report This case report describes the successful use of PRF in treating periapical lesion showing better healing than the other site. This was confirmed with a 3-D X-ray
Bains et al.[30] 2012 Sep Case report Histological events and reaction of mineral trioxide aggregate (MTA) with PRF is not studied so far, however, the autologous and biocompatible nature of components used for present treatment modalities seems to be beneficial for long-term clinical results
Tunalı et al.[31] 2012 Aug Animal study (Titanium tubes) T-PRF could induce the formation of new bone with new connective tissue in a rabbit model of wound healing within 30 days of treatment
Lekovic et al.[32] 2012 Aug In vivo The results of this study indicate that PRF can improve clinical parameters associated with human intrabony periodontal defects and BPBM (bovine porous bone mineral) has the ability to augment effects of PRF in reducing pocket depth, improving clinical attachment levels, and promoting defect fill
Wu et al.[33] 2012 Jun In vitro PRF is capable of increasing osteoblast attachment, proliferation, and simultaneously upregulating collagen-related protein production. These actions in combination would effectively promote bone regeneration
Contd...

Naik, et al.: Healing potential of PRF
Journal of Conservative Dentistry | Jul-Aug 2013 | Vol 16 | Issue 4286
Table 1: Contd...Author Year Type of
literature/studyConclusion/result
Bielecki et al.[34] 2012 Jun Review In the four families of platelet concentrates, two families contain significant concentrations of leukocytes: Leukocyte PRP (L-PRP) and L-PRF. The presence of leukocytes has a great impact on biology of these products, not only because of their immune and antibacterial properties, but also because they are turntables of the wound healing process and the local factor regulation
Del Corso et al.[35] 2012 Jun Review The use of L-PRF also allowed defining new therapeutic principles: Natural tissue regeneration (NTR) for the treatment of periodontal intrabony lesions and natural bone regeneration (NBR) for the reconstruction of alveolar ridges
Simonpieri et al.[36]
2012 Jun Review PRPs failed to prove strong strategic advantages that could justify their use in daily practice and use of most PRP techniques will probably be limited to some very specific applications where satisfactory results have been reached. Only a few simple, inexpensive, and efficient techniques such as L-PRF will continue to develop in oral and maxillofacial surgery in the next years
Zhang et al.[37] 2012 Jun In vivo This preliminary study results demonstrated neither an advantage nor disadvantage of the application of PRF in combination with deproteinized bovine bone mineral in sinus augmentation after a healing period of 6 months
Douglas et al.[38] 2012 May In vitro Hydrogel biomaterials such as PRF can be mineralized through functionalization with alkaline phosphatase (ALP)
Kim et al.[39] 2012 May Animal study The PRF-mixed tricalcium phosphate (TCP) showed more rapid bone healing than the (recombinant human bone morphogenic protein 2) rhBMP-2-coated TCP or the TCP-only control
Jankovic et al.[40] 2012 Apr Randomized controlled clinical study
Use of a PRF membrane in gingival recession treatment provided acceptable clinical results, followed by enhanced wound healing and decreased subjective patient discomfort compared to connective tissue graft (CTG)-treated gingival recessions
Rudagi et al.[41] 2012 Apr Case report This case report presents the successful healing and apexification with combined use of MTA as an apical barrier and autologous PRF membrane as an internal matrix
Del Corso et al.[42] 2012 Apr Case report Successful use of leukocyte-PRF during immediate postextractive implantation and loading for esthetic replacement of a fractured maxillary central incisor with promising results
Lee et al.[43] 2012 Apr Animal study In the animal model, peri-implant defect sized 3.0×5.0 mm (width×length) was successfully repaired by the application of PRF alone
Mendonça-Caridad et al.[44]
2012 Mar In vivo The application of an autogenous platelet rich/fibrin rich composite matrix in tissue regeneration and wound healing has resulted in a favorable outcome, with no complications or sequelae, in a series of ten patients with advanced frontal sinus disease over a long period of time
Pradeep et al.[45] 2012 Mar Randomized control clinical trial
Porous hydroxyapatite (HA) when added to PRF increases the regenerative effects observed with PRF in treatment of human three wall intrabony defects
Anitua et al.[46] 2012 Mar In vivo Practically, plasma rich in growth factors (PRGF) may present a role in reducing tissue inflammation after surgery, increasing new bone formation, and promoting vascularization of bone tissue
Peck et al.[47] 2012 Mar Case report L-PRF is a newly developed platelet concentrate that has successfully been used in a number of surgical procedures to optimize wound healing and was used to stimulate bone formation to facilitate ideal placement of implants
Clipet et al.[48] 2012 Feb In vitro PRF conditioned medium induced gene expression in osteoblasts. Expression of osteopontin and osteocalcin and late osteogenic markers was observed and confirmed PRF is useful in stimulating tissue healing and bone regeneration
Jayalakshmi et al.[49]
2012 Case report Combined use of PRF and b-tricalcium phosphate (b-TCP) for bone augmentation in treatment of periapical defects is a potential treatment alternative for faster healing than using these biomaterials alone
Tatullo et al.[50] 2012 In vivo The use of PRF and piezosurgery reduced the healing time, compared to 150 days described in literature, favoring optimal bone regeneration. At 106 days, it is already possible to achieve good primary stability of endosseous implants, though lacking of functional loading
Vijayalakshmi et al.[51]
2012 Jan Case report Describes application of PRF along with bone graft and guided tissue regeneration (GTR) membrane in the treatment of fenestration defect around an implant
Chang et al.[52] 2011 Dec In vitro and in vivo
The enhancement of phosphorylated extracellular signal-regulated protein kinase (p-ERK), osteoprotegerin (OPG), and alkaline phosphatase (ALP) activity expression by PRF may provide benefits for periodontal regeneration. Clinical and radiologic analysis showed that use of PRF is an effective modality for periodontal infrabony defects
Taschieri et al.[53] 2011 Dec In vivo A modified osteotome sinus floor elevation technique with immediate postextraction implant placement and adjunct of a platelet-derived fibrin plug is a viable option for rehabilitation of fresh postextraction maxillary premolar sockets
Sammartino et al.[54]
2011 Dec In vivo Use of L-PRF as a safe filling and hemostatic material is a reliable therapeutic option to avoid significant bleeding after dental extractions without suspension of continuous oral anticoagulant therapy in heart surgery patients
Contd...
Naik, et al.: Healing potential of PRF
287Journal of Conservative Dentistry | Jul-Aug 2013 | Vol 16 | Issue 4
Table 1: Contd...Author Year Type of
literature/studyConclusion/result
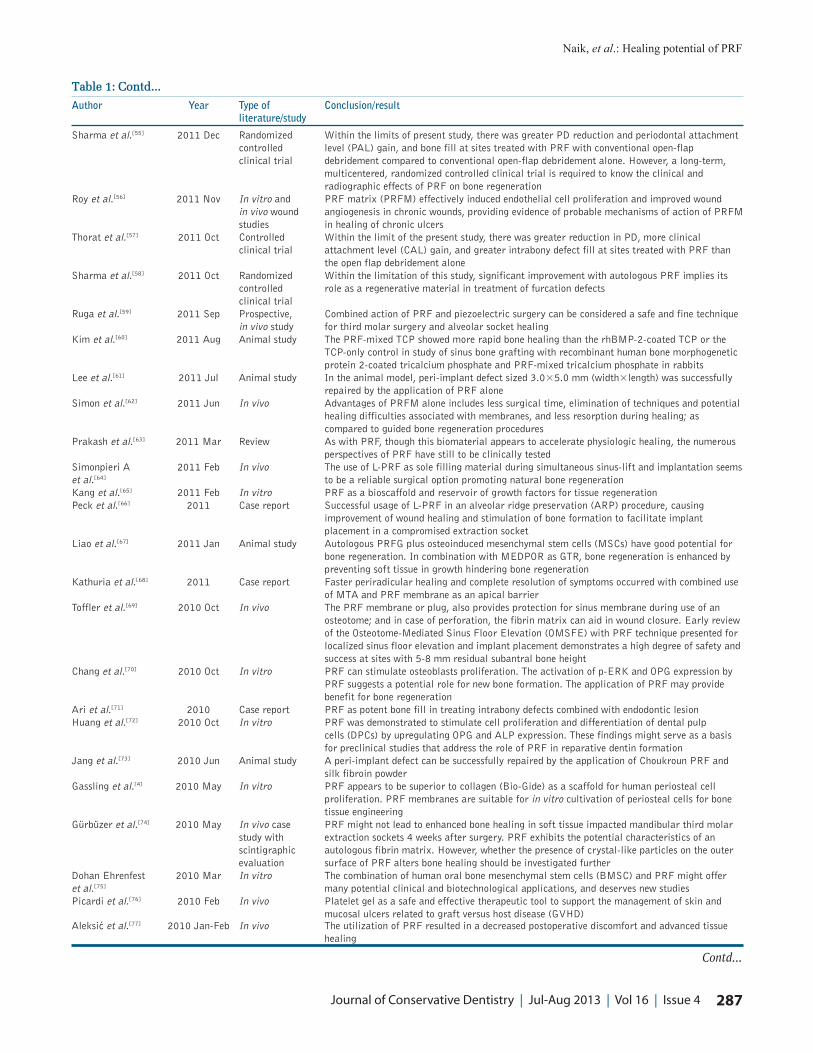
Sharma et al.[55] 2011 Dec Randomized controlled clinical trial
Within the limits of present study, there was greater PD reduction and periodontal attachment level (PAL) gain, and bone fill at sites treated with PRF with conventional open-flap debridement compared to conventional open-flap debridement alone. However, a long-term, multicentered, randomized controlled clinical trial is required to know the clinical and radiographic effects of PRF on bone regeneration
Roy et al.[56] 2011 Nov In vitro and in vivo wound studies
PRF matrix (PRFM) effectively induced endothelial cell proliferation and improved wound angiogenesis in chronic wounds, providing evidence of probable mechanisms of action of PRFM in healing of chronic ulcers
Thorat et al.[57] 2011 Oct Controlled clinical trial
Within the limit of the present study, there was greater reduction in PD, more clinical attachment level (CAL) gain, and greater intrabony defect fill at sites treated with PRF than the open flap debridement alone
Sharma et al.[58] 2011 Oct Randomized controlled clinical trial
Within the limitation of this study, significant improvement with autologous PRF implies its role as a regenerative material in treatment of furcation defects
Ruga et al.[59] 2011 Sep Prospective, in vivo study
Combined action of PRF and piezoelectric surgery can be considered a safe and fine technique for third molar surgery and alveolar socket healing
Kim et al.[60] 2011 Aug Animal study The PRF-mixed TCP showed more rapid bone healing than the rhBMP-2-coated TCP or the TCP-only control in study of sinus bone grafting with recombinant human bone morphogenetic protein 2-coated tricalcium phosphate and PRF-mixed tricalcium phosphate in rabbits
Lee et al.[61] 2011 Jul Animal study In the animal model, peri-implant defect sized 3.0×5.0 mm (width×length) was successfully repaired by the application of PRF alone
Simon et al.[62] 2011 Jun In vivo Advantages of PRFM alone includes less surgical time, elimination of techniques and potential healing difficulties associated with membranes, and less resorption during healing; as compared to guided bone regeneration procedures
Prakash et al.[63] 2011 Mar Review As with PRF, though this biomaterial appears to accelerate physiologic healing, the numerous perspectives of PRF have still to be clinically tested
Simonpieri A et al.[64]
2011 Feb In vivo The use of L-PRF as sole filling material during simultaneous sinus-lift and implantation seems to be a reliable surgical option promoting natural bone regeneration
Kang et al.[65] 2011 Feb In vitro PRF as a bioscaffold and reservoir of growth factors for tissue regenerationPeck et al.[66] 2011 Case report Successful usage of L-PRF in an alveolar ridge preservation (ARP) procedure, causing
improvement of wound healing and stimulation of bone formation to facilitate implant placement in a compromised extraction socket
Liao et al.[67] 2011 Jan Animal study Autologous PRFG plus osteoinduced mesenchymal stem cells (MSCs) have good potential for bone regeneration. In combination with MEDPOR as GTR, bone regeneration is enhanced by preventing soft tissue in growth hindering bone regeneration
Kathuria et al.[68] 2011 Case report Faster periradicular healing and complete resolution of symptoms occurred with combined use of MTA and PRF membrane as an apical barrier
Toffler et al.[69] 2010 Oct In vivo The PRF membrane or plug, also provides protection for sinus membrane during use of an osteotome; and in case of perforation, the fibrin matrix can aid in wound closure. Early review of the Osteotome-Mediated Sinus Floor Elevation (OMSFE) with PRF technique presented for localized sinus floor elevation and implant placement demonstrates a high degree of safety and success at sites with 5-8 mm residual subantral bone height
Chang et al.[70] 2010 Oct In vitro PRF can stimulate osteoblasts proliferation. The activation of p-ERK and OPG expression by PRF suggests a potential role for new bone formation. The application of PRF may provide benefit for bone regeneration
Ari et al.[71] 2010 Case report PRF as potent bone fill in treating intrabony defects combined with endodontic lesionHuang et al.[72] 2010 Oct In vitro PRF was demonstrated to stimulate cell proliferation and differentiation of dental pulp
cells (DPCs) by upregulating OPG and ALP expression. These findings might serve as a basis for preclinical studies that address the role of PRF in reparative dentin formation
Jang et al.[73] 2010 Jun Animal study A peri-implant defect can be successfully repaired by the application of Choukroun PRF and silk fibroin powder
Gassling et al.[4] 2010 May In vitro PRF appears to be superior to collagen (Bio-Gide) as a scaffold for human periosteal cell proliferation. PRF membranes are suitable for in vitro cultivation of periosteal cells for bone tissue engineering
Gürbüzer et al.[74] 2010 May In vivo case study with scintigraphic evaluation
PRF might not lead to enhanced bone healing in soft tissue impacted mandibular third molar extraction sockets 4 weeks after surgery. PRF exhibits the potential characteristics of an autologous fibrin matrix. However, whether the presence of crystal-like particles on the outer surface of PRF alters bone healing should be investigated further
Dohan Ehrenfest et al.[75]
2010 Mar In vitro The combination of human oral bone mesenchymal stem cells (BMSC) and PRF might offer many potential clinical and biotechnological applications, and deserves new studies
Picardi et al.[76] 2010 Feb In vivo Platelet gel as a safe and effective therapeutic tool to support the management of skin and mucosal ulcers related to graft versus host disease (GVHD)
Aleksić et al.[77] 2010 Jan-Feb In vivo The utilization of PRF resulted in a decreased postoperative discomfort and advanced tissue healing
Contd...

Naik, et al.: Healing potential of PRF
Journal of Conservative Dentistry | Jul-Aug 2013 | Vol 16 | Issue 4288
Table 1: Contd...Author Year Type of
literature/studyConclusion/result
Mazor et al.[12] 2009 Dec In vivo From a radiologic and histologic point of view at 6 months after surgery, the use of PRF as sole filling material during a simultaneous sinus lift and implantation stabilized a high volume of natural regenerated bone in subsinus cavity up to the tip of implants. Choukroun’s PRF is a simple and inexpensive biomaterial and its systematic use during a sinus lift seems a relevant option, particularly for the protection of the Schneiderian membrane
Sclafaniet al.[78] 2009 Nov Review A novel, simple method of preparing an autologous platelet derivative (Selphyl; Aesthetic Factors, Princeton, NJ) allows rapid and inexpensive generation of a PRFM that can be used to enhance healing after facial procedures as well as to rejuvenate the face without tissue manipulation
He et al.[79] 2009 Nov Animal study PRF released autologous growth factors gradually and expressed stronger and more durable effect on proliferation and differentiation of rat osteoblasts than PRP in vitro
Kfir et al.[80] 2009 Oct In vivo Successful application of minimally invasive antral membrane balloon elevation (MIAMBE) with injected PRF and bone substitutes under antral membrane as alternative to the currently employed methods of maxillary bone augmentation
Dohan Ehrenfest et al.[81]
2009 Sep In vitro Cultures with PRF are always cocultures with leukocytes. These “chaperone leukocytes” could be the source of differential geographic regulation within the culture and explain double contradictory effect proliferation/differentiation observed on osteoblasts
Gassling et al.[2] 2009 Jul In vitro PRP application in cell cultures leads to higher levels of growth factors than PRF applicationSu et al.[82] 2009 Jul In vitro The PRF membrane should be used immediately after formation to maximize release of GF to
surgical site. The remaining fluid can be recovered as an additional source of GF for graftingSimonpieri et al.[14]
2009 Jun In vivo PRF membranes are particularly helpful for periosteum healing and maturation. The thick peri-implant gingival is as a result of several healing phases on a PRF membrane layer
Simon et al.[83] 2009 May Animal study PRFM alone may be the best graft for ridge preservation proceduresSimonpieri et al.[13]
2009 Apr In vivo PRF membranes protects the surgical site, promotes soft tissue healing, and when its fragments mixed with graft material it functions as a “biological connector”
Magremanne et al.[84]
2009 Apr Case report PRF may induce healing of non-reossified cystic cavity by supplying local growth factors
Aroca et al.[19] 2009 Feb In vivo Modified coronally advanced flap (MCAF) is a predictable treatment for multiple adjacent Miller Class I or II recession-type defects. The addition of a PRF membrane positioned under the MCAF provided inferior root coverage, but an additional gain in gingival/mucosal thickness (GTH) at 6 months compared to conventional therapy
Anilkumar et al.[17]
2009 Jan Case report Described laterally displaced flap technique with PRF membrane technique as a navel root coverage approach for gingival recession of the mandibular anterior teeth
Diss et al.[85] 2008 May In vivo The bone-added osteotome sinus floor elevation (BAOSFE) procedure with PRF as grafting material can lead to an endosinus bone gain
Lundquist et al.[86] 2008 May Review PRF provides sustained release and protection against proteolytic degradation of endogenous fibrogenic factors important for wound healing
Choukroun et al.[87]
2006 In vitro PRF as healing biomaterial
PRF: Platelet rich fibrin
of fibrinogen in plasma. These fibrin adhesives can be derived autologously from the patient or can be obtained commercially, but with a small risk of disease transmission for the latter one.
PLATELET RICH PLASMA
It has been shown in several studies that bone regenerative procedures may be enhanced by the addition of specific growth factors.[6] platelet rich plasma (PRP) was used as a method of introducing concentrated growth factors platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-), and insulin-like growth factor 1 (IGF-1) to the surgical site, thereby enriching the natural blood clot in order to hasten wound healing and stimulate bone regeneration.[7] A natural human blood clot consists of 95% red blood cells (RBCs), 5% platelets, less than 1% white blood cells (WBCs), and numerous amounts of fibrin strands. A PRP blood clot, on the other hand, contains 4%
RBCs, 95% platelets, and 1% WBCs.[6] The PRP preparation protocol requires collection of blood with anticoagulant, centrifugation in two steps, and induced polymerization of the platelet concentrate using calcium chloride and bovine thrombin.[8] PRP has been used in conjunction with different grafting materials in bone augmentation procedures since the day of its introduction; the results from these studies are controversial and no conclusions can be drawn regarding the bone regenerative effect of PRP till date.
PRF
PRF represents a new revolutionary step in the platelet gel therapeutic concept.[1] Unlike other platelet concentrates, this technique does not require any gelifying agent, but not more than centrifugation of the natural blood without additives.[8] Choukroun et al.,[9] developed the PRF in 2001 at France and the production protocol of PRF attempts

Naik, et al.: Healing potential of PRF
289Journal of Conservative Dentistry | Jul-Aug 2013 | Vol 16 | Issue 4
to accumulate platelets and released cytokines in a fibrin clot. Actually the platelets and leukocyte cytokines are important part in role play of this biomaterial, but the fibrin matrix supporting them is very helpful in constituting the determining elements responsible for real therapeutic potential of PRF.[1] Cytokines are immediately used and destroyed in a healing wound. The harmony between cytokines and their supporting fibrin matrix has much more unique importance than any other constant. A fibrin glue, enriched with cytokines (such as PRP) with large uncontrollable and short-term effect is less better than a physiologic fibrin matrix (such as PRF) with good and better effects.
ADVANTAGES OF PRF OVER PRP
No biochemical handling of blood.[15]
Simplified and cost-effective process.[15]
Use of bovine thrombin and anticoagulants not required.[15]
Favorable healing due to slow polymerization.[15]
More efficient cell migration and proliferation.[15]
PRF has supportive effect on immune system.[15]
PRF helps in hemostasis.[15]
PREPARATION OF PRF
The protocol for PRF preparation is very simple and simulates that of PRP. It includes collection of whole venous blood (around 5 ml) in each of the two sterile vacutainer tubes (6 ml) without anticoagulant and the vacutainer tubes are then placed in a centrifugal machine [Figure 3] at 3,000 revolutions per minute (rpm) for 10 min, after which it settles into the following three layers: Upper straw-colored acellular plasma, red-colored lower fraction containing red blood cells (RBCs), and the middle fraction containing the fibrin clot [Figure 4]. The upper straw-colored layer is then removed and middle fraction is collected, 2 mm below to the lower dividing line, which is the PRF [Figure 5]. The mechanism involved in this is; the fibrinogen concentrated in upper part of the tube, combines with circulating thrombin due to centrifugation to form fibrin. A fibrin clot is then formed in the middle between the red corpuscles at bottom and acellular plasma at the top. The middle part is platelets trapped massively in fibrin meshes. The success of this technique entirely depends on time gap between the blood collection and its transfer to the centrifuge and it should be done in less time. The blood sample without anticoagulant, starts to coagulate almost immediately upon contact with the glass, and it decreases the time of centrifugation to concentrate fibrinogen. Following proper protocol and quick handling is the only way to obtain a clinically usable PRF clot charged with serum and platelets. Resistant autologous fibrin membranes may be available by driving out the fluids trapped in fibrin matrix.
Figure 3: Collection of blood, blood in vacutainer tube after centrifugation, and centrifuge machine
Figure 1: Search fl owchart on PubMed database
Total number of articlesfrom
Pubmed database755
302(After customized search with range
of five years)
72 Selected for review (All full text retreived)
230 excluded
Figure 2: Flowchart of total scrutinized articles
Total 75 articles reviewed(73 are pubmed indexed)
22In vivo studies
13In vitro studies
14Case reports
11Animal studies
6Controlled clinical trials
2Combined in vitro &
In vivo
7Reviews
CLINICAL APPLICATION
Choukroun et al.,[9] are well known for using autologous PRF protocol in oral and maxillofacial surgery to improve bone healing in implant dentistry.[9] The most common encountered problems are lack of adequate bone and proximity to anatomic structures at the implantation

Naik, et al.: Healing potential of PRF
Journal of Conservative Dentistry | Jul-Aug 2013 | Vol 16 | Issue 4290
site and recent advancements of PRF usage in surgical procedures can predictably combat such difficulties.
Choukroun et al.,[11] attempted to evaluate the potential of PRF in combination with freeze-dried bone allograft (FDBA) in sinus floor elevation to enhance bone regeneration and nine sinus floor augmentations were performed. Out of nine; in six sites, FDBA with PRF (test group), and in three sites FDBA without PRF (control group) was used. After 4 months, the test group and for the control group after 8 months; bone specimens from the augmented region during the implant insertion procedure were harvested and evaluated. After 4 months of healing time, histologic maturation of the test group appears to be identical to that of the control group which was for a period of 8 months with equivalent quantities for both protocols.[11]
In various bone reconstruction procedures Choukroun’s PRF could provide a possible new bone. Mazor et al.,[12] stated that use of PRF as the sole filling material during a simultaneous sinus lift and implantation procedure had stabilized a good amount of regenerated bone in the subsinus cavity up to the tip of implants in a case series through a radiological and histological evaluation at after 6 months from the surgery.[12] Also they advocated that Choukroun’s PRF, which is a simple and inexpensive biomaterial in systematic use during a sinus lift seems as an acceptable option.[12]
Simonpieri et al.,[13,14] reported and confirmed the validate usage of PRF membranes in reconstruction protocols along with FDBA, 0.5% metronidazole solution in about 20 patients who were treated using this new technique and followed-up during 1-5 years, and finally 184 dental implants were placed and they found no implant or graft loss in a case series.[13] PRF membranes protects the surgical site; promotes soft tissue healing; and when its fragments mixes with graft material, it functions as a “biological connector” between the different elements of graft and acts as a matrix which supports neoangiogenesis, capture of stem cells, and migration of osteoprogenitor cells to the center of graft.[14]
PRF plugs can also be used in treating the residual extraction sockets.[15] Use of autologous PRF in extracted socket filling after immediate bone augmentation using titanium membranes applied to the socket walls and primary closure was found to be feasible and safe with adequate bone filling after 8 weeks or above for implant fixation.[16]
Anilkumar et al.,[17] has reported PRF as a potential novel root coverage approach for treating gingival recession in mandibular anterior teeth using combined laterally positioned flap technique and PRF membrane.[17] Combined use of PRF and bone graft with good results has also been reported for combined periodontic-endodontic furcation defect.[18] Aroca et al.,[19] in the 6 month of their randomized clinical trial, concluded that addition of a PRF membrane positioned under the MCAF (modified coronally advanced flap) provided inferior root coverage, but an additional gain in gingival/mucosal thickness (GTH) at 6 months compared to conventional therapy [Table 1].[19]
DISCUSSION
PRF first described byChoukroun et al.,[9] is a new second generation of platelet concentrate. Simplified processing technique without any complex handling makes it superior to PRP. PRF can be used to promote wound healing, bone regeneration, graft stabilization, wound sealing, and hemostasis. Because the fibrin matrix is better organized, it is able to more efficiently direct stem cell migration and
Figure 4: Blood in the vacutainer tubes after centrifugation at 3,000 rpm for 10 min divided into three fractions; lower fraction of red blood cells, middle fraction containing fi brin clot, and upper acellular plasma fraction
Figure 5: Isolated platelet rich fi brin

Naik, et al.: Healing potential of PRF
291Journal of Conservative Dentistry | Jul-Aug 2013 | Vol 16 | Issue 4
the healing program. Release of growth factors from PRF through in vitro studies and good results from in vivo studies led to optimize the clinical application of PRF. It was shown that there are better results of PRF over PRP. Dohan et al.,[88] proved a slower release of growth factors from PRF than PRP and observed better healing properties with PRF. It was observed and shown that the cells are able to migrate from fibrin scaffold; while some authors demonstrated the PRF as a supportive matrix for bone morphogenetic protein as well.
CONCLUSION
Although PRF belongs to a new generation of platelet concentrates, the biologic activity of fibrin molecule is enough in itself to account for significant cicatricial capacity of the PRF. The slow polymerization mode confers to PRF membrane as a particularly favorable physiologic architecture to support the healing process.
However, it is now necessary to look further into platelet and inflammatory features of this biomaterial. Only a perfect understanding of its components and their significance will enable us to comprehend the clinical results obtained and subsequently extend the fields of therapeutic application of this protocol.
REFERENCES
1. Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJ, Mouhyi J, et al. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:e37-44.
2. Gassling VL, Açil Y, Springer IN, Hubert N, Wiltfang J. Platelet-rich plasma and platelet-rich fibrin in human cell culture. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:48-55.
3. Ross R, Glomset J, Kariya B, Harker L. A platelet-dependent serum factor that stimulates the proliferation of arterial smooth muscle cells in vitro. Proc Natl Acad Sci U S A 1974;71:1207-10.
4. Gassling V, Douglas T, Warnke PH, Açil Y, Wiltfang J, Becker ST. Platelet-rich fibrin membranes as scaffolds for periosteal tissue engineering. Clin Oral Implants Res 2010;21:543-9.
5. Sunitha Raja V, Munirathnam Naidu E. Platelet-rich fibrin: Evolution of a second-generation platelet concentrate. Indian J Dent Res 2008;19:42-6.
6. Nevins M, Giannobile WV, McGuire MK, Kao RT, Mellonig JT, Hinrichs JE, et al. Platelet-derived growth factor stimulates bone fill and rate of attachment level gain: Results of a large multicenter randomized controlled trial. J Periodontal 2005;76:2205-15.
7. Soffer E, Ouhayoun JP, Anagnostou F. Fibrin sealants and platelet preparations in bone and periodontal healing. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;95:521-8.
8. Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85:638-46.
9. Choukroun J, Adda F, Schoeffler C, Vervelle A. Une opportunité en paro-implantologie: Le PRF. Implantodontie 2001;42:55-62.
10. Saluja H, Dehane V, Mahindra U. Platelet-Rich fibrin: A second generation platelet concentrate and a new friend of oral and maxillofacial surgeons. Ann Maxillofac Surg 2011;1:53-7.
11. Choukroun J, Diss A, Simonpieri A, Girard MO, Schoeffler C, Dohan SL, et al. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part V: Histologic evaluations of PRF effects on bone allograft maturation in sinus lift. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:299-303.
12. Mazor Z, Horowitz RA, Del Corso M, Prasad HS, Rohrer MD, Dohan
Ehrenfest DM. Sinus floor augmentation with simultaneous implant placement using Choukroun’s platelet-rich fibrin as the sole grafting material: A radiologic and histologic study at 6 months. J Periodontol 2009;80:2056-64.
13. Simonpieri A, Del Corso M, Sammartino G, Dohan Ehrenfest DM. The relevance of Choukroun’s platelet-rich fibrin and metronidazole during complex maxillary rehabilitations using bone allograft. Part I: A new grafting protocol. Implant Dent 2009;18:102-11.
14. Simonpieri A, Del Corso M, Sammartino G, Dohan Ehrenfest DM. The relevance of Choukroun’s platelet-rich fibrin and metronidazole during complex maxillary rehabilitations using bone allograft. Part II: Implant surgery, prosthodontics, and survival. Implant Dent 2009;18:220-9.
15. Toffler M, Toscano N, Holtzclaw D, Corso MD, Dohan Ehrenfest DM. Introducing Choukroun’s platelet rich fibrin (PRF) to the reconstructive surgery milieu. J Implant Adv Clin Dent 2009;1:21-30.
16. Kfir E, Kfir V, Kaluski E. Immediate bone augmentation after infected tooth extraction using titanium membranes. J Oral Implantol 2007;33:133-8.
17. Anilkumar K, Geetha A, Umasudhakar, Ramakrishnan T, Vijayalakshmi R, Pameela E. Platelet-rich-fibrin: A novel root coverage approach. J Indian Soc Periodontol 2009;13:50-4.
18. Kanakamedala A, Ari G, Sudhakar U, Vijayalakshmi R, Ramakrishana T, Emmadi P. Treatment of a furcation defect with a combination of platelet rich fibrin and bone graft-A case report. ENDO (Lond Engl) 2009;3:127-35.
19. Aroca S, Keglevich T, Barbieri B, Gera I, Etienne D. Clinical evaluation of a modified coronally advanced flap alone or in combination with a platelet-rich fibrin membrane for the treatment of adjacent multiple gingival recessions: A 6-month study. J Periodontol 2009;80:244-52.
20. Gassling V, Hedderich J, Açil Y, Purcz N, Wiltfang J, Douglas T. Comparison of platelet rich fibrin and collagen as osteoblast-seeded scaffolds for bone tissue engineering applications. Clin Oral Implants Res 2013;24:320-8.
21. Keyhan SO, Hemmat S, Badri AA, Abdeshahzadeh A, Khiabani K. Use of platelet-rich fibrin and platelet-rich plasma in combination with fat graft: Which is more effective during facial lipostructure? J Oral Maxillofac Surg 2013;71:610-21.
22. Gassling V, Purcz N, Braesen JH, Will M, Gierloff M, Behrens E, et al. Comparison of two different absorbable membranes for the coverage of lateral osteotomy sites in maxillary sinus augmentation: A preliminary study. J Craniomaxillofac Surg 2013;41:76-82.
23. Pradeep AR, Rao NS, Agarwal E, Bajaj P, Kumari M, Naik SB. Comparative evaluation of autologous platelet-rich fibrin and platelet-rich plasma in the treatment of 3-wall intrabony defects in chronic periodontitis: A randomized controlled clinical trial. J Periodontol 2012;83:1499-507.
24. Vinaya Kumar R, Shubhashini N. Platelet rich fibrin: A new paradigm in periodontal regeneration. Cell Tissue Bank 2012.
25. Ozdemir H, Ezirganli S, Isa Kara M, Mihmanli A, Baris E. Effects of platelet rich fibrin alone used with rigid titanium barrier. Arch Oral Biol 2013;58:537-44.
26. Yang KC, Wang CH, Chang HH, Chan WP, Chi CH, Kuo TF. Fibrin glue mixed with platelet-rich fibrin as a scaffold seeded with dental bud cells for tooth regeneration. J Tissue Eng Regen Med 2012;6:777-85.
27. Shivashankar VY, Johns DA, Vidyanath S, Kumar MR. Platelet Rich Fibrin in the revitalization of tooth with necrotic pulp and open apex. J Conserv Dent 2012;15:395-8.
28. Kocyigit ID, Tuz HH, Alp YE, Atil F, Tekin U, Coskunses FM. Correction of postsurgical alveolar ridge defect with vertical alveolar distraction of the onlay block graft. J Craniofac Surg 2012;23:1550-2.
29. Bambal D, Manwar NU, Chandak M, Rudagi K. A comparative evaluation of the healing ability of bilateral periapical lesions treated with and without the use of platelet-rich fibrin. Todays FDA 2012;24:54-7.
30. Bains R, Bains VK, Loomba K, Verma K, Nasir A. Management of pulpal floor perforation and grade II Furcation involvement using mineral trioxide aggregate and platelet rich fibrin: A clinical report. Contemp Clin Dent 2012;3(Suppl 2):S223-7.
31. Tunalı M, Ozdemir H, Küçükodacı Z, Akman S, Fıratlı E. In vivo evaluation of titanium-prepared platelet-rich fibrin (T-PRF): A new platelet concentrate. Br J Oral Maxillofac Surg 2012.
32. Lekovic V, Milinkovic I, Aleksic Z, Jankovic S, Stankovic P, Kenney EB, et al. Platelet-rich fibrin and bovine porous bone mineral vs. platelet-rich fibrin in the treatment of intrabony periodontal defects. J Periodontal Res 2012;47:409-17.
33. Wu CL, Lee SS, Tsai CH, Lu KH, Zhao JH, Chang YC. Platelet-rich fibrin increases cell attachment, proliferation and collagen-related protein expression of human osteoblasts. Aust Dent J 2012;57:207-12.
34. Bielecki T, Dohan Ehrenfest DM, Everts PA, Wiczkowski A. The role of leukocytes from L-PRP/L-PRF in wound healing and immune defense:

Naik, et al.: Healing potential of PRF
Journal of Conservative Dentistry | Jul-Aug 2013 | Vol 16 | Issue 4292
New perspectives. Curr Pharm Biotechnol 2012;13:1153-62.35. Del Corso M, Vervelle A, Simonpieri A, Jimbo R, Inchingolo F,
Sammartino G, et al. Current knowledge and perspectives for the use of platelet-rich plasma (PRP) and platelet-rich fibrin (PRF) in oral and maxillofacial surgery part 1: Periodontal and dentoalveolar surgery. Curr Pharm Biotechnol 2012;13:1207-30.
36. Simonpieri A, Del Corso M, Vervelle A, Jimbo R, Inchingolo F, Sammartino G, et al. Current knowledge and perspectives for the use of platelet-rich plasma (PRP) and platelet-rich fibrin (PRF) in oral and maxillofacial surgery part 2: Bone graft, implant and reconstructive surgery. Curr Pharm Biotechnol 2012;13:1231-56.
37. Zhang Y, Tangl S, Huber CD, Lin Y, Qiu L, Rausch-Fan X. Effects of Choukroun’s platelet-rich fibrin on bone regeneration in combination with deproteinized bovine bone mineral in maxillary sinus augmentation: A histological and histomorphometric study. J Craniomaxillofac Surg 2012;40:321-8.
38. Douglas TE, Gassling V, Declercq HA, Purcz N, Pamula E, Haugen HJ, et al. Enzymatically induced mineralization of platelet-rich fibrin. J Biomed Mater Res A 2012;100:1335-46.
39. Kim BJ, Kwon TK, Baek HS, Hwang DS, Kim CH, Chung IK, et al. A comparative study of the effectiveness of sinus bone grafting with recombinant human bone morphogenetic protein 2-coated tricalcium phosphate and platelet-rich fibrin-mixed tricalcium phosphate in rabbits. Oral Surg Oral Med Oral Pathol Oral Radiol 2012;113:583-92.
40. Jankovic S, Aleksic Z, Klokkevold P, Lekovic V, Dimitrijevic B, Kenney EB, et al. Use of platelet-rich fibrin membrane following treatment of gingival recession: A randomized clinical trial. Int J Periodontics Restorative Dent 2012;32:e41-50.
41. Rudagi KB, Rudagi B. One-step apexification in immature tooth using grey mineral trioxide aggregate as an apical barrier and autologus platelet rich fibrin membrane as an internal matrix. J Conserv Dent 2012;15:196-9.
42. Del Corso M, Mazor Z, Rutkowski JL, Dohan Ehrenfest DM. The use of leukocyte- and platelet-rich fibrin during immediate postextractive implantation and loading for the esthetic replacement of a fractured maxillary central incisor. J Oral Implantol 2012;38:181-7.
43. Lee JW, Kim SG, Kim JY, Lee YC, Choi JY, Dragos R, et al. Restoration of a peri-implant defect by platelet-rich fibrin. Oral Surg Oral Med Oral Pathol Oral Radiol 2012;113:459-63.
44. Mendonça-Caridad J, Lopez PJ, Fayos FV, Miery G. A novel approach to human cranial tissue regeneration and frontal sinus obliteration with an autogenous platelet rich/fibrin-rich composite matrix: 10 patients with a 6-10 year follow-up. J Tissue Eng Regen Med 2012.
45. Pradeep AR, Bajaj P, Rao NS, Agarwal E, Naik SB. Platelet-Rich Fibrin combined with a porous hydroxyapatite graft for the treatment of three-wall intrabony defects in chronic periodontitis: A randomized controlled clinical trial. J Periodontol 2012.
46. Anitua E, Prado R, Orive G. Bilateral sinus elevation evaluating plasma rich in growth factors technology: A report of five cases. Clin Implant Dent Relat Res 2012;14:51-60.
47. Peck MT, Marnewick J, Stephen LX, Singh A, Patel N, Majeed A. The use of leukocyte- and platelet-rich fibrin (L-PRF) to facilitate implant placement in bone-deficient sites: A report of two cases. SADJ 2012;67:54-6:58-9.
48. Clipet F, Tricot S, Alno N, Massot M, Solhi H, Cathelineau G, et al. In vitro effects of Choukroun’s platelet-rich fibrin conditioned medium on 3 different cell lines implicated in dental implantology. Implant Dent 2012;21:51-6.
49. Jayalakshmi KB, Agarwal S, Singh MP, Vishwanath BT, Krishna A, Agrawal R. Platelet Rich Fibrin with -Tricalcium Phosphate-A noval approach for bone augmentation in chronic periapical lesion: A case report. Case Rep Dent 2012;2012:902858.
50. Tatullo M, Marrelli M, Cassetta M, Pacifici A, Stefanelli LV, Scacco S, et al. Platelet Rich Fibrin (PRF) in reconstructive surgery of atrophied maxillary bones: Clinical and histological evaluations. Int J Med Sci 2012;9:872-80.
51. Vijayalakshmi R, Rajmohan CS, Deepalakshmi D, Sivakami G. Use of platelet rich fibrin in a fenestration defect around an implant. J Indian Soc Periodontol 2012;16:108-12.
52. Chang YC, Zhao JH. Effects of platelet-rich fibrin on human periodontal ligament fibroblasts and application for periodontal infrabony defects. Aust Dent J 2011;56:365-71.
53. Taschieri S, Del Fabbro M. Postextraction osteotome sinus floor elevation technique using plasma-rich growth factors. Implant Dent 2011;20:418-24.
54. Sammartino G, Dohan Ehrenfest DM, Carile F, Tia M, Bucci P. Prevention of hemorrhagic complications after dental extractions into open heart surgery patients under anticoagulant therapy: The use of leukocyte- and platelet-rich fibrin. J Oral Implantol 2011;37:681-90.
55. Sharma A, Pradeep AR. Treatment of 3-wall intrabony defects in patients with chronic periodontitis with autologous platelet-rich fibrin: A randomized controlled clinical trial. J Periodontol 2011;82:1705-12.
56. Roy S, Driggs J, Elgharably H, Biswas S, Findley M, Khanna S, et al. Platelet-rich fibrin matrix improves wound angiogenesis via inducing endothelial cell proliferation. Wound Repair Regen 2011;19:753-66.
57. Thorat M, Pradeep AR, Pallavi B. Clinical effect of autologous platelet-rich fibrin in the treatment of intra-bony defects: A controlled clinical trial. J Clin Periodontol 2011;38:925-32.
58. Sharma A, Pradeep AR. Autologous platelet-rich fibrin in the treatment of mandibular degree II furcation defects: A randomized clinical trial. J Periodontol 2011;82:1396-403.
59. Ruga E, Gallesio C, Boffano P. Platelet-rich fibrin and piezoelectric surgery: A safe technique for the prevention of periodontal complications in third molar surgery. J Craniofac Surg 2011;22:1951-5.
60. Kim BJ, Kwon TK, Baek HS, Hwang DS, Kim CH, Chung IK, et al. A comparative study of the effectiveness of sinus bone grafting with recombinant human bone morphogenetic protein 2-coated tricalcium phosphate and platelet-rich fibrin-mixed tricalcium phosphate in rabbits. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011.
61. Lee JW, Kim SG, Kim JY, Lee YC, Choi JY, Dragos R, et al. Restoration of a peri-implant defect by platelet-rich fibrin. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011.
62. Simon BI, Gupta P, Tajbakhsh S. Quantitative evaluation of extraction socket healing following the use of autologous platelet-rich fibrin matrix in humans. Int J Periodontics Restorative Dent 2011;31:285-95.
63. Prakash S, Thakur A. Platelet concentrates: Past, present and future. J Maxillofac Oral Surg 2011;10:45-9.
64. Simonpieri A, Choukroun J, Del Corso M, Sammartino G, Dohan Ehrenfest DM. Simultaneous sinus-lift and implantation using microthreaded implants and leukocyte- and platelet-rich fibrin as sole grafting material: A six-year experience. Implant Dent 2011;20:2-12.
65. Kang YH, Jeon SH, Park JY, Chung JH, Choung YH, Choung HW, et al. Platelet-rich fibrin is a Bioscaffold and reservoir of growth factors for tissue regeneration. Tissue Eng Part A 2011;17:349-59.
66. Peck MT, Marnewick J, Stephen L. Alveolar ridge preservation using leukocyte and platelet-rich fibrin: A report of a case. Case Rep Dent 2011;2011:345048.
67. Liao HT, Chen CT, Chen CH, Chen JP, Tsai JC. Combination of guided osteogenesis with autologous platelet-rich fibrin glue and mesenchymal stem cell for mandibular reconstruction. J Trauma 2011;70:228-37.
68. Kathuria A, Chaudary S, Talwar S, Verma M. Endodontic management of single rooted immature mandibular second molar with single canal using MTA and platelet-rich fibrin membrane: A case report. J Clin Exp Dent 2011;3:e487-90.
69. Toffler M, Toscano N, Holtzclaw D. Osteotome-mediated sinus floor elevation using only platelet-rich fibrin: An early report on 110 patients. Implant Dent 2010;19:447-56.
70. Chang IC, Tsai CH, Chang YC. Platelet-rich fibrin modulates the expression of extracellular signal-regulated protein kinase and osteoprotegerin in human osteoblasts. J Biomed Mater Res A 2010;95:327-32.
71. Ari G, Anil Kumar K, Ramakrishnan T. Treatment of an intrabony defect combined with an endodontic lesion: A case report. Endo (lond Engl) 2010;4:215-22.
72. Huang FM, Yang SF, Zhao JH, Chang YC. Platelet-rich fibrin increases proliferation and differentiation of human dental pulp cells. J Endod 2010;36:1628-32.
73. Jang ES, Park JW, Kweon H, Lee KG, Kang SW, Baek DH, et al. Restoration of peri-implant defects in immediate implant installations by Choukroun platelet-rich fibrin and silk fibroin powder combination graft. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109:831-6.
74. Gürbüzer B, Pikdöken L, Tunali M, Urhan M, Küçükodaci Z, Ercan F. Scintigraphic evaluation of osteoblastic activity in extraction sockets treated with platelet-rich fibrin. J Oral Maxillofac Surg 2010;68:980-9.
75. Dohan Ehrenfest DM, Doglioli P, de Peppo GM, Del Corso M, Charrier JB. Choukroun’s platelet-rich fibrin (PRF) stimulates in vitro proliferation and differentiation of human oral bone mesenchymal stem cell in a dose-dependent way. Arch Oral Biol 2010;55:185-94.
76. Picardi A, Lanti A, Cudillo L, Cerretti R, Dentamaro T, De Angelis G, et al. Rome Transplant Network. Platelet gel for treatment of mucocutaneous lesions related to graft-versus-host disease after allogeneic hematopoietic stem cell transplant. Transfusion 2010;50:501-6.
77. Aleksić Z, Janković S, Dimitrijević B, Divnić-Resnik T, Milinković I, Leković V. The use of platelet-rich fibrin membrane in gingival recession treatment. Srp Arh Celok Lek 2010;138:11-8.
78. Sclafani AP. Applications of platelet-rich fibrin matrix in facial plastic surgery. Facial Plast Surg 2009;25:270-6.
79. He L, Lin Y, Hu X, Zhang Y, Wu H. A comparative study of platelet-rich

Naik, et al.: Healing potential of PRF
293Journal of Conservative Dentistry | Jul-Aug 2013 | Vol 16 | Issue 4
fibrin (PRF) and platelet-rich plasma (PRP) on the effect of proliferation and differentiation of rat osteoblasts in vitro. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:707-13.
80. Kfir E, Goldstein M, Yerushalmi I, Rafaelov R, Mazor Z, Kfir V, et al. Minimally invasive antral membrane balloon elevation-Results of a multicenter registry. Clin Implant Dent Relat Res 2009;11 Suppl 1:e83-91.
81. Dohan Ehrenfest DM, Diss A, Odin G, Doglioli P, Hippolyte MP, Charrier JB. In vitro effects of Choukroun’s PRF (platelet-rich fibrin) on human gingival fibroblasts, dermal prekeratinocytes, preadipocytes, and maxillofacial osteoblasts in primary cultures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:341-52.
82. Su CY, Kuo YP, Tseng YH, Su CH, Burnouf T. In vitro release of growth factors from platelet-rich fibrin (PRF): A proposal to optimize the clinical applications of PRF. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:56-61.
83. Simon BI, Zatcoff AL, Kong JJ, O’Connell SM. Clinical and histological comparison of extraction socket healing following the use of autologous platelet-rich fibrin matrix (PRFM) to ridge preservation procedures employing demineralized freeze dried bone allograft material and membrane. Open Dent J 2009;3:92-9.
84. Magremanne M, Baeyens W, Awada S, Vervaet C. Solitary bone cyst of the mandible and platelet rich fibrin (PRF). Rev Stomatol Chir Maxillofac 2009;110:105-8.
85. Diss A, Dohan DM, Mouhyi J, Mahler P. Osteotome sinus floor elevation using Choukroun’s platelet-rich fibrin as grafting material: A 1-year prospective pilot study with microthreaded implants. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:572-9.
86. Lundquist R, Dziegiel MH, Agren MS. Bioactivity and stability of endogenous fibrogenic factors in platelet-rich fibrin. Wound Repair Regen 2008;16:356-63.
87. Choukroun J, Diss A, Simonpieri A, Girard MO, Schoeffler C, Dohan SL, et al. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part IV: Clinical effects on tissue healing. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:e56-60.
88. Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJ, Mouhyi J, et al. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part II: Platelet-related biologic features. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:e45-50.
How to cite this article: Naik B, Karunakar P, Jayadev M, Marshal VR. Role of Platelet rich fi brin in wound healing: A critical review. J Conserv Dent 2013;16:284-93.Source of Support: Nil, Confl ict of Interest: None declared.
Author Help: Online submission of the manuscripts
Articles can be submitted online from http://www.journalonweb.com. For online submission, the articles should be prepared in two files (first page file and article file). Images should be submitted separately.1) First Page File: Prepare the title page, covering letter, acknowledgement etc. using a word processor program. All information related to your identity
should be included here. Use text/rtf/doc/pdf files. Do not zip the files.2) Article File: The main text of the article, beginning with the Abstract to References (including tables) should be in this file. Do not include any information
(such as acknowledgement, your names in page headers etc.) in this file. Use text/rtf/doc/pdf files. Do not zip the files. Limit the file size to 1024 kb. Do not incorporate images in the file. If file size is large, graphs can be submitted separately as images, without their being incorporated in the article file. This will reduce the size of the file.
3) Images: Submit good quality color images. Each image should be less than 4096 kb (4 MB) in size. The size of the image can be reduced by
decreasing the actual height and width of the images (keep up to about 6 inches and up to about 1800 x 1200 pixels). JPEG is the most suitable file format. The image quality should be good enough to judge the scientific value of the image. For the purpose of printing, always retain a good quality, high resolution image. This high resolution image should be sent to the editorial office at the time of sending a revised article.
4) Legends: Legends for the figures/images should be included at the end of the article file.





























