Embed Size (px)
Citation preview

ROBOTIC-ASSISTED MINIMALLY INVASIVE SURGERY:
COMMUNICATION IN A COMPLEX SOCIO-TECHNICAL SYSTEM
A thesis
submitted by
Stacey A. Cunningham
In partial fulfillment of the requirements
for the degree of
Master of Science
in
Human Factors
TUFTS UNIVERSITY
May 2012
Adviser: Caroline G. L. Cao

ii
Abstract
Surgical robots are controlled from a remote console, inhibiting face-to-
face communication between the surgeon and the rest of the team. This research
viewed the robotic operating room as a socio-technical system where team mem-
bers adapt to technology by modifying their communication. The goal of this re-
search was to understand the nature of communication in robotic surgery. A field
study was conducted to examine communication as a function of workplace cul-
ture and experience level with the robot. Surgical teams in the US and France had
different workflows, roles, and communication patterns. The study revealed the
difficulty of communicating spatial information during surgery. Controlled ex-
periments were conducted to examine spatial communication in a simulated ro-
botic surgical task. Results indicate that using a spatial communication aid may
positively impact task time and communication, regardless of natural spatial abil-
ity. The research contributes to robotic surgery requirements analysis, training
protocol design, and future telesurgery applications.

iii
Acknowledgements
There are countless people who deserve gratitude for their part in enabling me
to complete this thesis. I hope that all of them will accept my deepest thanks.
First, I would like to thank my husband Drew for supporting me in my deci-
sion to return to graduate school. Your appreciation for the importance of a life-
long pursuit of knowledge is just one of the many reasons that I love you. To my
family, thank you for raising me in a loving and supportive environment in which
I learned the value of hard work and perseverance.
I owe gratitude to Caroline Cao, my thesis advisor, for believing in me and
mentoring me over the course of this research. You have provided me with a
wealth of opportunity and imparted valuable knowledge of human factors that
will shape my career for years to come. I would especially like to thank Dr. Jean-
Marc Classe and his surgical team for welcoming me into their operating room in
order to conduct my research. Thank you also to Holly Taylor and Jason Rife for
taking the time to read and evaluate my thesis. Your input has helped to increase
the breadth and depth of my research.
I owe a special thank you to Jay Banez for helping me in numerous ways, in-
cluding using a couteau and for generally keeping me sane. Finally, I would like
to thank all of my fellow graduate students for their support. Your willingness to
participate, provide input, and especially your friendship has made this work pos-
sible.

iv
Table of Contents
1. Introduction ................................................................................................. 2
2. Background ................................................................................................. 3
2.1. Minimally Invasive Surgery ..................................................................... 3
2.2. Robotic-Assisted Minimally Invasive Surgery ........................................ 5
2.3. Safety in the Operating Room ................................................................ 10
3. Survey of Literature .................................................................................. 12
3.1. Socio-Technical Systems ....................................................................... 12
3.2. Effects of New Technology.................................................................... 14
3.3. Teams ..................................................................................................... 18
3.3.1. Team Performance Model............................................................... 20
3.3.2. Temporary Teams ........................................................................... 20
3.4. Communication ...................................................................................... 22
3.4.1. Communication Failures in Robotic Surgery ................................. 24
3.4.2. Common Ground ............................................................................ 27
3.4.3. Shared Mental Models .................................................................... 28
3.4.4. Spatial Communication ................................................................... 29
3.4.5. Improving Communication ............................................................. 31
4. Field Study of Robotic Surgery as a Socio-Technical System ................. 33
4.1. Synopsis ................................................................................................. 33
4.2. Background ............................................................................................ 33
4.3. Method ................................................................................................... 37
4.3.1. Research Setting.............................................................................. 37
4.3.2. Data Analysis .................................................................................. 40
4.4. Results .................................................................................................... 42
4.4.1. Workflow Analysis ......................................................................... 43

v
4.4.2. Timeline Analysis ........................................................................... 46
4.4.3. Differences in Roles ........................................................................ 47
4.4.4. Communication Analysis of Select Phases ..................................... 50
4.4.5. Communication Pattern Analysis ................................................... 52
4.4.6. Communication and Viewing Perspective Differences .................. 52
4.5. Discussion .............................................................................................. 54
4.5.1. Workflow Analysis ......................................................................... 54
4.5.2. Timeline Analysis ........................................................................... 55
4.5.3. Differences in Roles ........................................................................ 56
4.5.4. Communication Analysis of Select Phases ..................................... 57
4.5.5. Communication Pattern Analysis ................................................... 58
4.5.6. Communication and Viewing Perspective Differences .................. 60
4.6. Limitations ............................................................................................. 61
4.7. Summary ................................................................................................ 62
5. Design of a Spatial Aid for Communication in Robotic Surgery ............. 63
5.1. Problem Statement ................................................................................. 63
5.2. Experimental Task.................................................................................. 64
5.3. Experiment 1 .......................................................................................... 65
5.3.1. Synopsis .......................................................................................... 65
5.3.2. Hypotheses ...................................................................................... 65
5.3.3. Method ............................................................................................ 66
5.3.4. Results ............................................................................................. 72
5.3.5. Discussion ....................................................................................... 77
5.3.6. Limitations ...................................................................................... 82
5.4. Experiment 2 .......................................................................................... 83
5.4.1. Synopsis .......................................................................................... 83
5.4.2. Spatial Ability Literature ................................................................ 84

vi
5.4.3. Hypotheses ...................................................................................... 86
5.4.4. Method ............................................................................................ 86
5.4.5. Results ............................................................................................. 91
5.4.6. Discussion ....................................................................................... 97
5.4.7. Limitations .................................................................................... 109
5.5. Summary .............................................................................................. 110
5.6. Suggestions for Future Work ............................................................... 111
6. Conclusion .............................................................................................. 112
APPENDIX A: US SURGERY TRANSCRIPTIONS ....................................... 114
APPENDIX B: FRENCH SURGERY TRANSCRIPTIONS ............................. 117
APPENDIX C: NOTES FROM SURGEON INTERVIEW ............................... 152
APPENDIX D: STATISTICAL ANALYSIS FOR EXPERIMENT 1............... 154
APPENDIX E: STATISTICAL ANALYSIS FOR EXPERIMENT 2 ............... 155
References ........................................................................................................... 156

vii
List of Tables
Table 1. Verbal exchange taxonomy for coding surgical transcriptions .............. 41
Table 2. Definitions of the phases of robotic surgery ........................................... 44
Table 3. Comparison of verbal exchange percentage between US and France teams for all surgical phases except Console ............................................ 51
Table 4. Pattern analysis comparison of single statement communication data for the two observed French team robotic surgeries....................................... 52
Table 5. Spatial communication examples ........................................................... 53
Table 6. Communication volume and ratio results ............................................... 74
Table 7. Frame of reference analysis results ......................................................... 75
Table 8. Communication excerpts from Experiment 1 ......................................... 77
Table 9. Taxonomy used to code experimental spatial communication data ....... 90
Table 10. Spatial ability average test scores, standard deviation in parentheses .. 92
Table 11. Average time, volume of communication and ratio of communication data. Standard deviations are shown in parentheses. ................................ 93
Table 12. Correlation results for Experiment 2 .................................................... 94
Table 13. Content distribution analysis of verbal data ......................................... 96
Table 14. Frame of reference analysis of verbal data ........................................... 96

viii
List of Figures
Figure 1. An example of a robotic surgery operating room .................................... 6
Figure 2. Top: Minimally invasive surgery (Strauss, 2011) Bottom: Minimally invasive surgery with surgical robot ........................................................... 8
Figure 3. Surgeon’s view at the robotic console ................................................... 15
Figure 4. Shannon and Weaver’s Communication Model. This figure depicts a general communication system (Adapted from Shannon & Weaver, 1949)................................................................................................................... 22
Figure 5. The da Vinci surgical system, showing (from left to right) the patient cart, console, and tower ............................................................................ 38
Figure 6. Placement of digital video cameras shown in physical layout of operating room (a) Robotic patient cart (b) Robotic tower (c) Sterile instruments table (d) Operating table (e) Camera (f) Camera (g) Anesthesiology equipment (h) Robotic console ....................................... 39
Figure 7. Workflow diagram depicting each of the robotic surgery phases for this analysis. Each phase is shown along with the steps performed during that phase, listed in a typical working order. Boxes highlighted in gray are robotic specific tasks ................................................................................. 45
Figure 8. Robot in French operating room during console phase ......................... 46
Figure 9. Phase times in minutes for each of the five robotic phases, shown across observed US and French procedures......................................................... 47
Figure 10. Allocation of the most frequent topic and percentage of verbal exchange with surgeon in US team based on verbal exchange codes (from Table 1). (A) Anesthesiologist, (SN) Scrub Nurse, (PA) Physician’s Assistant, (MS) Medical Student, (S-T) Surgeon Trainee, (S) Surgeon, (CN) Circulating Nurse ............................................................................. 48
Figure 11. Allocation of the most frequent topic and percentage of verbal exchange with surgeon in French team based on verbal exchange codes. (A) Anesthesiologist, (N) Nurses, (R) da Vinci Surgical Representative, (S) Surgeon, (S-T) Surgeon Trainee ......................................................... 49
Figure 12. Subjects performing experiment.......................................................... 66
Figure 13. Task space for “surgeon” role in experiment ...................................... 68
Figure 14. “Assistant” role performing task in grid spatial aid condition ............ 68
Figure 15. Visual-motor congruency diagram for the two camera conditions ..... 69

2
Figure 16. Foam liver and target outline displayed on “surgeon” role’s screen ... 70
Figure 17. Results of the time analysis for all experimental conditions ............... 73
Figure 18. Task completion time vs. communication volume for novices for spatial aid conditions (averaged across camera rotations) ........................ 73
Figure 19. Ratio of “surgeon” to “assistant” communication (averaged across camera rotations) ....................................................................................... 75
Figure 20. Laparoscopic trainer box ..................................................................... 88
Figure 21. View of the “assistant” task monitor in the grid aid condition ............ 89
Figure 22. “Surgeon” role task monitor in cardinal directions aid condition ....... 89
Figure 23. Average performance time (seconds) for dyads in of the three spatial interface aid conditions ............................................................................. 92
Figure 24. Two strategies for reaching the target. Left: Long range move of liver to target area. Right: Fine-grained rotation and orientation into final position .................................................................................................... 107

1
ROBOTIC-ASSISTED MINIMALLY INVASIVE SURGERY:
COMMUNICATION IN A COMPLEX SOCIO-TECHNICAL SYSTEM

2
1. Introduction
Technology advancement over the past several decades has greatly in-
creased the range of available medical care. Smarter devices, computerized imag-
ing and the ability to share data over high speeds are all shaping the practice of
modern medicine. All of these advances have the capability to impact the quality
and distribution of medical care to people around the world. However, technology
brings new challenges in the form of user acceptance, re-training and changes to
process and personnel roles within the medical system. The surgical field has re-
cently seen the rise of technology in the operating room along with some of these
challenges to the system. Robots are now used in minimally invasive surgical
procedures, providing increased precision in surgical manipulation and ergonomic
benefits to the surgeon over traditional open and laparoscopic surgery. Adding a
robotic system to an operating room introduces a new layer of complexity to the
traditional workflow. The operating room can be considered a socio-technical en-
vironment with a semi-autonomous team at its core. The team relies upon knowl-
edge brought from individual roles in pursuit of common goals. They make use of
tools and technologies and are externally supported by the organizational culture
of the hospital. The introduction of robotics, however, has altered the traditional
team structure and communication patterns found within the operating room
(Healey & Benn, 2009). The team depends on communication as a cornerstone of
successful robotic surgical procedures (Nyssen & Blavier, 2010). In open or
minimally invasive surgery, team member roles are established and set working
procedures are relied upon throughout the delivery of surgical care to a patient.

3
The robot changes that established dynamic; team members must adjust to it. One
way of doing so is by modifying the way in which they communicate and share
information. Along with change comes the possibility for uncertainty and mis-
communication, which may cause error. For this research, a human factors ap-
proach was taken to examine the nature of communication and information flow
in the robotic operating room. The robotic operating room was examined as a
socio-technical system, with the ultimate goal of understanding the role that a ro-
botic system plays within the surgical team and how it changes communication
patterns and team structure in this environment. This research consisted of two
parts: the first was a field study of robotic surgery and the second was a series of
controlled experiments. The goal of the field study was to characterize the envi-
ronment of robotic surgery and introduce a layered approach to analyzing the
socio-technical system including the communication patterns found in an operat-
ing room. The second part of the research consisted of two controlled experiments
designed to further investigate specific communication challenges uncovered by
the field analysis. The overall goal of the experiments was to contribute to the de-
sign of tools and training that can promote better communication and effective
teamwork.
2. Background
2.1. Minimally Invasive Surgery
Over the past thirty years, minimally invasive surgery has been widely
adopted as a preferred alternative to open surgery. Also known as laparoscopic

4
surgery, in this type of procedure several small incisions are made in the abdomen
to allow access into the abdominal cavity, creating access ports, or trocars. A fiber
optic camera called a laparoscope is inserted, usually at the umbilicus, and long
thin surgical instruments with scissor-like handles are inserted into the other ports
to triangulate around the operative site. The abdominal cavity is insufflated with
carbon dioxide to provide room for the surgeon to work. The surgeons operate by
watching a monitor in the operating room which shows a video image on a two-
dimensional screen of the inside of the body. Minimally invasive techniques are
used in a variety of procedures that have only grown over the years, with the most
common procedure being the laparoscopic cholecystectomy, or gallbladder re-
moval.
The benefits to the patient in a minimally invasive procedure are numer-
ous (NIH, 1992). Smaller incisions yield smaller scars and less disruption of
healthy tissue, reduced hospital stays and faster recovery time. However, these
advantages are not without increased burden to the surgeon, who must learn to use
a new set of tools and develop visual motor skills due to the separation of visual
and physical operative site (Tendick, Jennings, Tharp, & Stark, 1993). Addition-
ally, in minimally invasive surgery the surgeon’s view is reduced to a two-
dimensional workspace with fewer degrees of freedom of movement for the tools
(Gallagher & Smith, 2003). This complex arrangement presents challenges to the
surgeon in terms of sensory coordination and tool manipulation (Tendick et al.,
1993). Surgeons are also faced with reduced haptic feedback, which may lead to
excess force being applied in tissue handling, resulting in tearing or stretching. It

5
may also contribute to longer procedure times as well as increased cognitive load
(Schostek, Schurr, & Buess, 2009).
2.2. Robotic-Assisted Minimally Invasive Surgery
The emergence of robotic-assisted minimally invasive surgery has helped
address some of the aforementioned challenges facing surgeons (Ballantyne,
2002). The operative site is still accessed through tiny incisions, and the overall
procedural flow is similar. However, robotic arms replace the surgeon at the oper-
ating table in order to hold the camera and instruments. The robot is capable of
executing precise maneuvers on the patient under full control of the surgeon. This
configuration is known as a master-slave setup; the surgeon works at an ergo-
nomic console, the master, and controls the robotic arms, the slave (Lirici, Papas-
pyropoulos, & Angelini, 1997). An assistant surgeon is present at the patient side
and is tasked with manipulating organs and tissue to give the surgeon better ac-
cess to the operative site. The assistant is also responsible for irrigating and intro-
ducing procedure-related tools such as sutures, mesh, and the organ collection
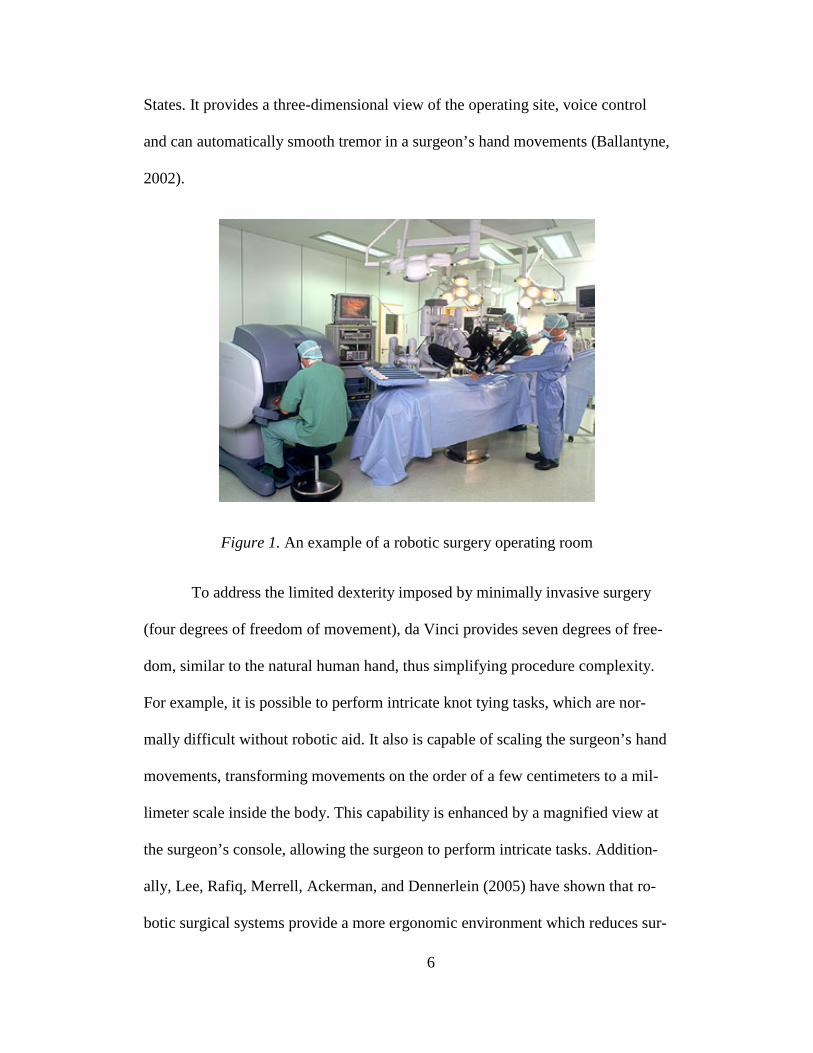
bag. Figure 1 depicts a typical robotic surgery environment. In robotic surgery,
the surgical team must still set up ports through which to access the operative site
with a camera and surgical tools. However, the robot itself, positioned above the
operating table, performs movement of the tools and camera while guided by the
surgeon.
The da Vinci Surgical System produced by Intuitive Surgical is currently
the only FDA approved robotic-assisted surgical system being used in the United
6
States. It provides a three-dimensional view of the operating site, voice control
and can automatically smooth tremor in a surgeon’s hand movements (Ballantyne,
2002).
Figure 1. An example of a robotic surgery operating room
To address the limited dexterity imposed by minimally invasive surgery
(four degrees of freedom of movement), da Vinci provides seven degrees of free-
dom, similar to the natural human hand, thus simplifying procedure complexity.
For example, it is possible to perform intricate knot tying tasks, which are nor-
mally difficult without robotic aid. It also is capable of scaling the surgeon’s hand
movements, transforming movements on the order of a few centimeters to a mil-
limeter scale inside the body. This capability is enhanced by a magnified view at
the surgeon’s console, allowing the surgeon to perform intricate tasks. Addition-
ally, Lee, Rafiq, Merrell, Ackerman, and Dennerlein (2005) have shown that ro-
botic surgical systems provide a more ergonomic environment which reduces sur-

7
geon fatigue and stress. However, the same study has shown robotic surgery to
take longer than its traditional minimally invasive counterpart (Lee et al., 2005).
Many hospitals now have a robotic surgical system, and surgeons in sub-
disciplines such as neurology, urology and gynecology have embraced the robotic
system as a beneficial tool in their field as it has made difficult operations possi-
ble.
Surgeons using a robotic system rely on both visual and audio feedback as
important sensory inputs while using the system. Visual feedback provides a view
of the surgical area and helps to guide the surgeon while executing the procedure.
A special three-dimensional laparoscopic camera is used with the robotic system
to give the surgeon an enhanced view. Audio feedback allows for the surgeon to
communicate with the team while working at the console, which is necessary to
maintain status on the state of the procedure, condition of the patient and proper
functioning of the equipment. Compared to the reduced haptic feedback found in
minimally invasive surgery, robotic surgical systems generally lack haptic feed-
back altogether.
The large physical footprint of the robot is another differentiator from
minimally invasive surgery. The robotic system includes a console where the sur-
geon sits, a set of three or four large robotic arms on a stand that is docked to the
access ports called trocars that have been in the patient, and a number of monitors
mounted or placed around the room. In comparison, the largest piece of equip-
ment for a minimally invasive procedure is a cart that holds the laparoscopic cam-
era device; it is wheeled to the operating table for the procedure. The robotic arms

8
and monitors generally envelop the operating table. This prevents easy and fast
access to the patient on the table, and the arms may collide with each other or the
surgical lights suspended from the ceiling of the operating room that illuminate
the operating table.
Figure 2. Top: Minimally invasive surgery (Strauss, 2011) Bottom: Minimally
invasive surgery with surgical robot
As is often the case, the operating room may not have been designed spe-
cifically to house a robot. Therefore, there may not be adequate space for the ro-
botic equipment in a room already crowded with surgical equipment. Hospitals
may also lack the ability to provide an operating room dedicated solely to robotic
9
procedures. Some hospitals choose to keep the robot outside the operating room
and move it in only when needed. Figure 2 shows both a standard operating room
used for minimally invasive surgery as well as an operating room containing the
da Vinci surgical robot. In the photo on the bottom, the robot’s physical footprint
has crowded the space and it is difficult to see the team members working along-
side the operating table.
A promising future capability of the robotic surgical system is telesurgery,
in which the surgeon and patient are not co-located, and the surgeon controls the
robot from a remote location. This technological advance presents challenges in
the form of delay in transmission (Sheridan, 2002; Ottensmeyer, Hu, Thompson,
Ren, & Sheridan, 2000), as well as team coordination at the remote sites. As pre-
viously discussed, use of the robot necessitates extra steps related to preparation
of the robot and specialized instruments along with instrument changes during
surgery. The team must do this on top of maintaining patient status and ensuring a
smooth flow of the procedure. Telesurgery requires operating team members to be
physically separated between remote locations, yet they must still accomplish the
same surgical tasks as if they were co-located. Once telesurgery becomes more
practicable, it is expected that teams from different countries will collaborate on
medical procedures on a routine basis. Thus, understanding the differences in op-
erating standards between hospitals in different locations may be an important
part in the implementation of a telesurgery program.

10
2.3. Safety in the Operating Room
In 1999, a landmark study by the Institute of Medicine revealed there are
between 44,000 and 98,000 American deaths and more than 1 million injuries per
year due to medical error (Kohn, Corrigan, & Donaldson, 1999). The study
prompted a call for more focus on patient safety in medicine. Yet in a follow-up
study, researchers found that in the 10 years since the original study was pub-
lished, medical errors in North Carolina hospitals did not decrease significantly
despite the appeals for a stronger focus on patient safety (Landrigan, Parry,
Bones, Hackbarth, Goldman, & Sharek, 2010). The same study also divided harm
counts into specific subspecialties; it revealed that surgical patients were prone to
a higher risk of harm. An analysis of 15,000 records from Colorado and Utah
found that 54% of adverse surgical events were preventable (Gawande, Thomas,
Zinner, & Brennan, 1999). Another study at a university teaching hospital simi-
larly found that approximately 49% of both major and minor surgical complica-
tions were avoidable (Healey, Shackford, Osler, Rogers, & Burns, 2002).
In order to understand the root cause of these errors, it is important to first
define errors within the scope of medicine. According to noted expert Reason
(1990), errors depend on two kinds of failures: either the correct action does not
proceed as intended (an error of execution) or the original intended action is not
correct (an error of planning). This definition is supported by Helmreich (2000)
who discussed error within the team oriented fields of aviation and medicine; in

11
he defined team error as “action or inaction leading to deviation from team or or-
ganizational intentions” (pg. 781). In medicine, not all errors are preventable, de-
pending on the patient’s underlying condition. However, errors, if not caught, can
inflict harm or even death to the patient. Examples of types of medical error in-
clude physical injury, misdiagnosis and delayed treatment (Leape, 1994). In the
medical culture, it is thought that training is sufficient to prevent errors, yet when
they inevitably occur physicians and nurses are subjected to social punishment by
their peers, creating an environment in which it is difficult to disclose errors, even
if for the common good (Leape, 1994).
Effort has been made to address the needs in medical error prevention and
cultivate an awareness of patient safety. For example, the World Health Organiza-
tion began a patient safety campaign through which it developed a surgical safety
checklist that was shown through pilot studies to reduce the rates of surgery re-
lated deaths and complications by one third (WHO, 2011). Since then over 3,900
hospitals in more than 122 countries have signed on to use the surgical safety
checklist (WHO, 2011).
Research into ways to minimize the risk of preventable errors in surgery is
ongoing; there is still work to be done. It may be safe to say that adding yet a new
layer in the form of robotic systems to surgery only complicates the efforts to re-
duce medical errors. As discussed previously, however, the robotic system brings
many advantages to both the patient and the surgeon in terms of recovery, ergo-
nomics, and the ability to execute complex procedures. Therefore, it is likely that
robotics will remain, if not grow, in the field of surgery. Patient safety is a top

12
goal in healthcare and lessons from existing human factors research must be con-
sidered when using robotics in a clinical setting. Thus, an important goal of this
research is to consider patient safety within the scope of robotic surgery.
While the advent of robotic surgical systems has capitalized on techno-
logical advancements and opened the door for future surgical possibilities, it is
important to remember that this is a relatively new field in the much studied world
of surgery. Given the dynamic nature and critical environment of the operating
room, a goal of this research is to further examine the impact of the robot in sur-
gery from a human factors perspective. Doing so will allow for incorporation of
lessons learned from minimally invasive surgery to combine with new realizations
brought to light by robotic systems and promote safety and efficacy in the operat-
ing environment.
3. Survey of Literature
3.1. Socio-Technical Systems
This research considers the robotic operating room as a socio-technical
system in which people interact with tools and techniques/technology in a com-
plex work environment. The subject of socio-technical systems was originally
proposed in a seminal study by Trist and Bamforth (1951), in which highly col-
laborative and self-regulating work teams were observed in the coal industry. The
workers formed groups that were modeled after the type of small group interac-
tion that existed prior to mechanization in the coal industry, in which pairs or
small teams existed. These teams carried their work through the entire cycle of

13
operations, and workers became skilled in multiple tasks and job roles. This type
of work structure not only brought a sense of pride and accomplishment to the
workers, but it allowed leadership and self-regulation to emerge in the groups,
which Trist and Bamforth (1951) called responsible autonomy. The workers
formed closely bonded units that provided social support for one another and
helped them to adapt quickly to the changing and often dangerous working condi-
tions in the mines.
The introduction of mechanization to the mines dissolved the small group
structure and changed the work organization into that of a small factory hierarchy.
Despite this, the miners were able to self-form into new working groups as an ad-
aptation strategy to the changes brought about by the new mining technology.
This working group phenomenon was observed in contrast to some of the typical
side effects of increased automation: jobs were broken down into one-man-one-
task roles with little chance for interpersonal interaction, and coordination was
handled by external, higher level supervisors (Trist, 1981).
Socio-technical systems theory places the team at the core of the system;
specialization of team members and effective personal interactions yield autono-
mous working groups, as opposed to individual or high level control (Trist, 1981).
Socio-technical systems promote meaningful work; in the operating room this jus-
tifies the need for well-defined roles and responsibilities, each person contributing
in a different way. Team members feel a sense of personal commitment to their
tasks and cooperate together to achieve the ultimate goals of the system. Addi-
tionally, socio-technical systems view the machine as complementary rather than

14
an extension of the human (Jordan, 1963). The surgical robot compliments human
skills in planning and decision making throughout the surgery by providing sup-
port in areas more limited to humans, such as precise, small scale manipulation.
The principles of socio-technical theory translate well to the robotic oper-
ating environment. According to Orasanu and Connolly (1993), ill-structured
problems, time stress and high stakes characterize the socio-technical system. The
surgical environment is shaped by all of these factors. There are a number of dif-
ferent medical devices and equipment to operate, including the robot itself. There
are team members from different healthcare professions such as surgery, anesthe-
siology and nursing. The team members must work within the constraints of not
only the type of procedure and equipment, but the process and organization of the
hospital. All of these factors contribute to a complex, layered system. To mediate
this complexity, the team members engage in meaningful tasks that contribute to
the success of the surgery; for example, ensuring all equipment is prepared in ad-
vance, assisting the surgeon with patient side activities, and providing feedback
regarding the status of tool changes (Nyssen & Blavier, 2010; Webster & Cao,
2006). They do so by collaborating and communicating throughout the procedure.
3.2. Effects of New Technology
In socio-technical systems, workers form teams and develop adaptive
strategies as a mechanism for adjusting to new technology. Robotic surgical sys-
tems introduce challenges to their users who may react in a similar way. Technol-
ogy developers see exciting possibilities for robotics in diverse domains such as

15
military, mining and medicine. This is captured in the Law of Stretched Systems,
which notes that new technologies will be exploited in pursuit of new levels of
performance and efficiency (Hollnagel & Woods, 2005). However, the thrust of
advanced robotics onto practitioners in established fields such as surgery warrants
examination of the technology from another angle.
Figure 3. Surgeon’s view at the robotic console
Robotic surgical systems are inherently complex devices. There are multi-
ple layers of hardware, software, control, displays, and countless ways to interact
with the device. Davies (2000) defined the surgical robot as “powered computer-
controlled manipulator with artificial sensing that can be reprogrammed to move
and position tools to carry out a range of surgical tasks” (p. 129). Ultimately, the
robot is not meant to replace the surgeon, but to enhance the capability of the sur-
geon. Figure 3 shows a view of the surgical site from the surgeon’s console with a
robotic tool in view. The console and robotic arms consist of highly complex
software and electro-mechanical components.
Any new technology introduced into an established system will face ob-
stacles in terms of re-training, adoption, and adjustments to procedure. In addi-

16
tion, changes to established medical protocols and teams can have a direct effect
on the safety of the patient and outcome of procedures. Thus, hospital manage-
ment may be slower to adopt new technology despite encouragement from
thought leaders in the medical arena.
The shift from traditional minimally invasive techniques to robotic surgery
is a large step due to the introduction of new forms of automation. In the former,
humans are separated from the patient by simple tools. Conversely, in the latter a
complex computer driven electro-mechanical robot is inserted between the human
and the patient. This is an example of increasing system automation. In automa-
tion, technology is used to replace human functions in manual control, planning or
problem solving. One of the ironies of automation is that in the attempt to reduce
complexity through automation, the system actually becomes more complex
(Bainbridge, 1983). This is because new types of errors are introduced, new use
cases evolve and in turn the role of the human operator is redefined. A mismatch
between the designer’s mental model and the user’s view of the system may also
exist (Lee, 2006). This is especially of concern when the technology is adapted
from another application where it was originally designed for a different use. In
this case, the way in which the user expects to interact or use the technology may
not follow suit in the actual operation and function of the technology. This can
lead to errors and even mistrust of the system (Lee, 2006).
Hollnagel and Woods (2005) also discussed the complexities found in
human encounters with technology, and how users adopt different coping strate-
gies in order to maintain control and stability while interacting with a complex

17
system. In medicine, one common example of a coping strategy is when auto-
mated alerts or alarms are disabled on devices because they are activated fre-
quently and not always at the most appropriate moments; this situation is known
as alarm fatigue. When a cause for real concern does arise, there is no alarm to
alert the staff, which could lead to patient harm or even death. In addition, users
may exhibit tailoring behavior, in which they alter the system to meet their needs
or they change their procedure or task in order to adapt to the system (Hollnagel
& Woods, 2005).
Oftentimes when new technology is introduced into an environment, team
members bend or adapt to constraints of poorly designed systems. The surgical
environment is not an exception. Cook and Woods (1996) studied how anesthesi-
ologists adapted to a new computer-based physiological monitoring system and
found it introduced changes to the typical workflow. For example, the mismatch
of data on the display to the anesthesiologists’ mental representation of the data
created cognitive burdens. They also found that the anesthesiologists had diffi-
culty interacting with an automated window management system imposed by the
software. As a result, the anesthesiologists tweaked the way they accessed the
data on the screen in order to more effectively use the technology to perform their
jobs.
New technology can also change the way in which information is dissemi-
nated in the operating room. Webster and Cao (2006) compared traditional mini-
mally invasive with robotic minimally invasive cholecystectomy procedures and
found a large difference in the amount and type of information between the two

18
surgical methods; for example, tasks such as instrument changes required more
steps and information exchange in the robotic case. Additionally, the amount of
communication between team members increased in the robotic case, yielding
greater chances for miscommunication and error.
Use of a new technology can also affect the communication patterns nor-
mally used by the surgical team members. Nyssen and Blavier (2010) studied the
effects of a new robotic surgical system on the operating room team and found
that robotic procedures took longer, and not only did the amount of communica-
tion increase, but it took on new forms. For example, because of the distance be-
tween surgeon and assistant, a division of work is required, led by the surgeon
who gives orders to the assistant. This creates a new type of communication pat-
tern in surgery and also changes the role of the assistant to more of a technician.
3.3. Teams
The team is at the core of a socio-technical system. This research uses the
definition of a team provided by Salas, Dickinson, Converse, and Tannenbaum
(1992): “a distinguishable set of two or more people who interact, dynamically,
interdependently, and adaptively toward a common and valued
goal/objective/mission, who have each been assigned specific roles or functions to
perform, and who each have a limited life-span of membership” (p. 4). There are
many causes for teamwork within the operating room. Lingard, Reznick, Espin,
Regehr, and DeVito (2002) found that dominant needs in the operating room are
safety, timeliness, sterility, resources, roles and situation. In order to satisfy these

19
needs, operating room team members must possess the knowledge of both proce-
dure and available resources in terms of both equipment and personnel. They
must work to maintain a safe and sterile environment and move the procedure
along in a timely manner. The overall time for a case additionally affects the
throughput at a hospital and billing. To accomplish all of these things in the oper-
ating room, staff must communicate and work together as a team.
Considering the model of robotic surgery as a socio-technical system, in
robotic surgery the medical staff unites to form teams with the common goal of
providing medical care to a patient. The teams are diverse, and professionals bring
knowledge from different health care professions such as anesthesiology, surgery,
nursing, and sometimes radiology and pathology. The environment is dynamic, as
patient status and the path of the operation can change at any time. Each member
of the operating team has specific roles. The surgeon executes the surgery with
robotic aid and acts as the overall leader. The assistant and scrub nurse work at
the operating table to interchange instruments at the robot, and the assistant fur-
ther performs duties such as irrigation and suction, along with manipulation of the
organs and tissues to aid the surgeon. The circulating nurse acts as a liaison be-
tween sterile and non-sterile fields. Each person contributes in a different way,
and an efficient and safe operation depends on the ability of the staff to work to-
gether effectively.

20
3.3.1. Team Performance Model
A well accepted model for team performance is based on the systems
model of input-throughput-output. This is a linear model of teamwork; the input
factors are those present in the environment prior to the start of the team activity,
the throughput phase uses group processes to transform the inputs into meaningful
and quality output (Salas, Dickinson, Converse, & Tannenbaum, 1992). This
model was further adapted for the operating room by Helmreich and Schaefer
(1994), who studied factors influencing team performance. In their model, inputs
consist of factors such as the hospital culture and working norms, training, roles
of medical staff, variations within the team itself and the physical environment. In
the surgical setting, the outcome factors are safety and quality of patient care.
There are many group process factors (throughput stage) that influence the output.
Planning and preparation for anticipated complications in surgery, distribution of
the workload throughout the surgical team, leadership and group interactions all
play a role. Knowledge sharing via consultation, debriefs and information systems
influence group process effects in a positive way. Furthermore, communication
skills were noted as a contributor to success in the group process stage (Helmreich
& Schaefer, 1994).
3.3.2. Temporary Teams
Surgical teams can also be considered a type of temporary team. Unlike
permanent teams, which are established for long periods of time with persistent
members, temporary teams come together for short durations to accomplish com-

21
plex task(s), and then dissolve after completion. There may be different team
members involved each time a temporary team convenes. Temporary teams are
characterized by people with knowledge in diverse areas and rely on a high de-
gree of interdependence in order to accomplish the tasks (Goodman & Goodman,
1976). In this light, temporary teams follow suit with viewing the robotic operat-
ing room as a socio-technical system. While the operating room staff members are
permanent employees of the hospital, in the context of surgery, they come to-
gether only for the period required for delivering surgical care to the patient. The
same teams do not always work together on every surgery, and there are often
new and unfamiliar team members in the operating room, especially in teaching
hospitals with residents and medical students.
In Trist and Bamforth’s (1951) observation of socio-technical teams in the
coal mines, workers often chose their workmates, and the teams were in part suc-
cessful due to the close social bonds and trust developed over time. In contrast,
temporary team members have less of a chance to build rapport and trust with one
another, yet they need to rely on communication and personal interaction in order
to complete the task at hand within the given timeframe. Thus, the surgical envi-
ronment requires swift trust, a concept in which team members move forward in
their actions as if trust were already established in order to accomplish task goals
(Meyerson, Weick, & Kramer, 1996). Establishment of team member roles con-
tributes to swift trust in temporary teams, whereas blurring of roles and responsi-
bilities leads to a slower building of trust. Additionally, the time pressure found in
temporary systems causes team members to follow a speed-accuracy tradeoff in

22
their interpersonal communications; devoting time to developing relationships is
traded for time spent on the task (Meyerson et al., 1996). This can be counterac-
tive by negatively affecting team performance, and as a result, outcomes of the
task. Furthermore, the robotic operating room also creates a distributed team, due
to the separation of the surgeon from the rest of the team and the operating table.
This reduces face-to-face interaction. For example, in electronic teams, the lack of
face-to-face communication creates a barrier to interpersonal interaction by re-
moving the use of nonverbal communication cues (Meyerson et al., 1996).
3.4. Communication
Communication is a means through which workers in a socio-technical
system share information and accomplish work tasks. Communication is also a
group process strategy used by the operating team in the pursuit of common goals
such as patient safety, delivery of care and efficiency of procedure.
Figure 4. Shannon and Weaver’s Communication Model. This figure depicts a
general communication system (Adapted from Shannon & Weaver, 1949)

23
The Oxford English Dictionary offers one definition of communication as
the “transmission or exchange of information, knowledge, or ideas, by means of
speech, writing, mechanical or electronic media” (2011). Thus, communication is
an act of conveying information. It also implies there must be both a sender and a
receiver. This research focuses on verbal communication, as it is the most observ-
able way that team members share information with each other in the robotic op-
erating room.
Shannon and Weaver’s (1949) influential model of communication is pre-
sented in Figure 4. The model identifies a linear path along which a message is
transmitted from source to destination. The message is encoded and transmitted
along a channel, received, and then decoded at the destination. During transmis-
sion, the message is subject to interference from noise. This model can be adapted
to human verbal communication. The sender (person A) forms a message either
from knowledge in the mind, or knowledge in the environment and translates it to
verbal form. The message is transmitted via spoken word, where it is susceptible
to interference such as environmental noise, and received by person B, who must
then make sense of the received message. The sender and receiver are also both
susceptible to distractions which can interfere with the encoding or decoding of
the message.
In the operating room, transmission of information is accomplished via
spoken word, written files and whiteboard information, electronic patient files and
test results available on the computer, and digital radiology images. It can also be
conveyed via visual cues or facial expressions between team members. With the

24
robotic surgical system, a microphone and speakers facilitate communication be-
tween the surgeon and other team members. Noise can occur in the form of device
alarms, pagers beeping, attention distractions due to patient status changes or
team members talking. A difference in mental model or skill/knowledge level be-
tween sender and receiver can distort the encoding or decoding of the message.
Additionally, humans have limits on their ability to correctly process information
at an efficient rate, known as the channel capacity (Miller, 1956). Beyond this,
humans have storage limits in working memory that impede their ability to proc-
ess large amounts of information at once (Miller, 1956). This suggests that while
of course the content of the message is important, the amount of information and
also the timing of the transmission play a role in successful communication. For
all these reasons, there are many possible points of failure along the communica-
tion pathway.
3.4.1. Communication Failures in Robotic Surgery
Communication and teamwork are important for many reasons. While the
surgical team’s competency in technical skills is required for achieving the ulti-
mate needs in the operating room, it is not the sole contributor. Catchpole,
Mishra, Handa, and McCulloch (2008) have shown errors outside the operative
field (for example: sterile break, forgetting to fully connect equipment, admini-
stration of wrong medication) are two- to three-times more common than errors in
surgical technique. In recent years, non-technical skills have been shown to be
contributors to positive surgical outcomes and patient safety. Non-technical skills
are cognitive or interpersonal related skills; such as communication, teamwork,

25
decision making, situation awareness and leadership. In order to maintain a safe
and productive environment, surgical teams need to possess the ability to engage
in effective communication and teamwork throughout the entire continuum of
care.
Because communication is a vital component of the surgical process, it is
a much studied subject in both open and minimally invasive surgery. Christian et
al. (2006) performed prospective observations of general surgical procedures and
post-operation classification and analysis of the data. They found that breakdowns
in communication and information flow negatively impacted both team perform-
ance and patient safety in the ten cases involved. A review of over 100 studies on
communication in surgery through the continuum of care was performed by Nag-
pal et al. (2010), and found researchers uncovering communication failures in di-
verse areas such as critical care, nursing, staff changes and the perioperative envi-
ronment.
Other researchers conducted structured focus groups with residents, nurses
and surgeons in order to investigate the contribution of breakdowns in the sharing
of information and communication to medical errors (Williams et al., 2007). They
found that blurred boundaries of responsibility, diversion of attention and dis-
torted or inhibited communication were all reported as contributors to events such
as delay in patient care as well as adverse events. They defined one form of com-
munication failure as distorted or inhibited communication between care provid-
ers. Contributing factors were assumption of provider skill, variations in provider
skill, knowledge, experience, and motivation. Other factors were the absence of

26
feedback to originator orders and absence or presence of face-to-face communica-
tion. For example, they found different standards for communication between day
and night; residents were hesitant to call surgeons at night, resulting in suboptimal
care for a patient who is admitted at night. They observed a patient develop a
bowel complication in the ICU because, in the transfer of care, the resident on
duty was assumed to know specific actions to take in case of a blood pressure de-
crease, when in fact he did not. They also found that face-to-face communication
results in more complete transfer of information than alternate methods such as
electronic page.
Lingard et al. (2004) attempted to isolate communication relevant to a
procedure (not social) and identified four types of communication they then clas-
sified as failures. They defined communication failure as an event flawed in a di-
mension of content (insufficiency or inaccuracy in the information), audience
(gaps in the group involved in the communication), purpose (unclear, inappropri-
ate, or not achieved), and occasion (situation or context). The researchers found
communication failures in a third of the communication events due to poor tim-
ing, misinformation, unresolved issues, and excluded individuals in the informa-
tion exchange. A third of the failures further affected the outcome and progress of
the procedure. Several effects of the failures that negatively affected performance
were increased cognitive load, interruption of routines, rise in tension, and com-
promising patient safety. For example, they observed a failure of occasion when
the surgeon inquired about antibiotics over an hour into a procedure, when in fact
antibiotics need to be administered within 30 minutes of incision. In another case

27
they observed audience failures such as discussions about patient positioning on
the bed without the relevant surgical representative present.
3.4.2. Common Ground
In order to mitigate communication failures, surgical team members may
work to establish common ground in communication. Common ground is
achieved by coordinating the content and process by two people who are working
together in order to achieve mutual knowledge, mutual beliefs, and mutual expec-
tations (Clark & Marshall, 1981). A speaker and a listener engage in a series of
back and forth communication until a mutual understanding is reached and ac-
cepted (Clark & Gibbs, 1986). Strategies such as responses/acknowledgements,
posing questions, and seeking evidence of paying attention all contribute to the
grounding process; however constraints such as those found in the robotic operat-
ing room detract from it. These include lack of co-presence, visibility, and audi-
bility (Clark & Brennan, 1991). Cramton discussed failures surrounding the estab-
lishment of common ground among dispersed teams, including the failure to
communicate and retain contextual information, and problems interpreting the
meaning of silence (2001).
In a robotic surgical environment, where face-to-face communication is
limited, yet the surgical team relies upon communication in order to progress the
surgery and ensure safety of the patient, finding common ground is especially im-
portant. Common ground can be established during preparation of equipment, by
engaging in discourse related to the proper positioning of the robotic arms. When

28
the team members understand the reasons for proper arm placement (to avoid in-
ternal tool collisions and external arm collisions during surgery), and share a vo-
cabulary describing the robotic components, joint angles, and procedure types,
they have started to establish common ground. This research considers the con-
cept of common ground as a key contributor to successful communication in ro-
botic surgery.
3.4.3. Shared Mental Models
Mental models concerning the equipment and procedure in robotic surgery
may also affect or detract from or contribute to effective communication. Team
members attempt to share mental models in order to achieve common goals by
synchronizing their actions and promoting team performance (Mathieu, Heffner,
Goodwin, Salas, & Cannon-Bowers, 2000). Furthermore, they help people to de-
scribe, explain and predict events in the environment (Mathieu et al., 2000). In
robotic surgery, when a new robotic surgeon is trained, the experienced surgeon
encounters difficulty describing and explaining to the trainee how to localize and
approach organs and tissues, and how to orient the tools and perform tasks such as
suturing and cutting. This may be because of a difference in mental models be-
tween the experienced and novice surgeons. Because the tools and technology are
different from traditional minimally invasive surgery, the novice may need time to
come up to speed with equipment operation as well as the fundamental differ-
ences between a robotic-assisted and a traditional procedure. Conversely, the ex-
perienced surgeon, who has performed the robotic surgery many times, has al-
ready developed a new mental model of the process which is different than non

29
robotic-assisted procedure. In another case, team members can use shared mental
models to help predict the environment. This can be seen with the assistant, who
may be able to anticipate the needs and next moves of the surgeon if their mental
models converge.
In the robotic operating room, there are different parallel tasks, such as
preparing equipment, performing surgical steps, or managing the next case. In or-
der for the team to execute these tasks concurrently, it is likely that they possess
different mental models depending on their role within the team. In fact, Cannon-
Bowers, Salas, and Converse (1993) noted that teams working on complex tasks
need to have multiple shared mental models in order to encompass all of the tasks
at hand. Furthermore, the understanding of each other’s mental models, leading to
a sharing of mental models, helps team members to converge upon common ob-
jectives and be able to synchronize their actions (Mathieu et al., 2000). Commu-
nication is an important factor to linking shared mental models in pursuit of good
performance (Fleishman & Zaccaro, 1992).
3.4.4. Spatial Communication
Robotic surgery relies heavily on the communication of spatial related in-
formation, especially during the operative portion of the surgery during which
team members discuss where to work inside of the body. In order to more effec-
tively communicate spatial related information, the surgical team members must
achieve some degree of common ground. Varying communication strategies may
enhance or detract from the establishment of common ground. For example, in the

30
communication of spatial information, different frames of reference (egocentric,
exocentric, or allocentric) may be taken, influencing the effort required to achieve
common ground (Gugerty & Brooks, 2004). Additionally, the method in which
spatial information is conveyed, such as through route lists that provide spatial
information in a step-by-step format, eliminate spatial cognitive loading because
each piece of information is congruent with an action (Wickens & Carswell,
1998). In surgery, one surgeon may be providing procedural cues to another sur-
geon in order to assist with the steps of the surgery. In aviation, electronic dis-
plays can also be used to highlight current position, and provide a common frame
of reference for communication. These all facilitate transmission of spatial infor-
mation by providing a basis for common ground and shared mental models.
Other studies have looked at remote collaboration in a visual task. The
role of multiple camera views in a remote office collaboration task has been in-
vestigated, and it was found that it was difficult to present a complete picture of
the environment, difficult to establish reference, and difficult to establish a mutual
orientation to relevant objects due to the lack of co-presence (Gaver, Sellen,
Heath, & Luff, 1993). Another group studied the use of similar or different refer-
ence frames in a distributed but collaborative virtual task, and found that egocen-
tric pairs performed the slowest but reported the most understanding of the envi-
ronment, whereas exocentric pairs performed the fastest but reported more diffi-
culty (Schafer & Bowman, 2004). An egocentric and exocentric subject mixture
married efficiency and user awareness.

31
A third study explored the role of co-presence in a collaborative bicycle
repair task, and found that video collaboration is not sufficient to enhance col-
laboration compared to that of physical co-presence, but was better than audio-
only communication (Kraut, Fussell, & Siegel, 2003). The same study also found
that subjects adapted their language based on the degree of co-presence. Investi-
gation into a virtual, 3D figure reconstruction task showed that contextual clues
present in the virtual environment positively benefits collaboration (Chellali,
Milleville-Pennel, & Dumas, 2008). These studies suggest that visual cues and
choice of frame of reference are important contributors to successful communica-
tion of spatial related information during surgery.
3.4.5. Improving Communication
Researchers have attempted to understand how different modes of com-
munication affect performance in the operating room. Standardized communica-
tion is one mode of mitigating error occurring in high risk environments, and is
used frequently in aviation. Applied to medicine, it has been shown to decrease
communication breakdowns during critical points of cardiovascular surgery (Hen-
rickson, Wadhera, Weigmann & Sundt, 2009). Researchers studying the concept
of telementoring, in which a surgeon remotely mentors a medical or surgical pro-
cedure, have suggested standard military guidelines as a basis for communication
between mentor and student surgeon to eliminate communication discrepancies
(Rosser, Young, & Klonsky, 2007). These include using call signs as well as
wearing personal headsets. Another study used pre-operative checklists as a
means to encourage teams to communicate prior to beginning surgery (Lingard et

32
al., 2005). Techniques of ‘callbacks,’ ‘readouts,’ and the use of names in the op-
erating room have been shown to significantly improved surgeons’ preoperative
briefings as well as positively influenced team perceptions on communication,
teamwork and potential error reduction (Guerlain, Turrentine, Bauer, Calland, &
Adams, 2008). All of these strategies work because they form a basis for promot-
ing common ground, or allowing for convergence of team member mental models
related to surgical tasks.
There have been limited studies examining communication in the robotic
operating room. Webster and Cao (2006) examined open communication, scripted
communication, and automated communication in a controlled study simulating
robotic surgery and found that simulated surgeon-nurse teams performed faster in
the scripted and automated conditions, but the automated conditions had the high-
est error rates due to lack of familiarity with the new information format. This
suggests that pointed, procedure-related communication has a positive effect on
performance. Another study attributed the new and higher communication occur-
rences in robotic surgery, compared to a similar minimally invasive procedure, as
an adaptation to insufficient feedback in the robotic environment (Nyssen & Bla-
vier, 2010). This same study found that inexperienced teams communicate more
than experienced teams – and if even one member of the team is inexperienced,
the amount of communication was higher. Robotic surgery can further benefit
from studies in communication, as the surgical team is distributed throughout the
operating room, posing new challenges in how information is transmitted, which
ultimately affects performance.

33
4. Field Study of Robotic Surgery as a Socio-Technical System
4.1. Synopsis
This field study aimed to build on previous research by further examining
the nature of communication in robotic surgery. Teams in the US and in France
were observed while using a surgical robot. A layered approach was taken to ex-
amine the data collected during the surgeries, including the analysis of workflow,
time, and communication content and pattern. The surgical teams varied in their
experience level with the robot in addition to working in different hospital settings
in two countries. Therefore, the results of the analysis seemed to suggest that
variations found in each teams’ workflow, time, and their topics of communica-
tion could be due to both experience level as well as workplace culture differ-
ences. A more detailed pattern analysis conducted on the French teams’ commu-
nication data helped to shed light on the team’s interaction during use of the ro-
bot.
4.2. Background
Due to the complex nature of socio-technical systems including the pres-
ence of multiple team members, a complicated workflow and a high-stress envi-
ronment, it is difficult to study human behavior and technology interaction in this
type of setting. Not surprisingly, researchers who wish to study surgery often en-
counter the problem of gaining access to an operating room and subsequently col-
lecting data in order to analyze the environment. Traditional human factors analy-
sis techniques may include observations, interviews, timeline analysis, and task

34
analysis (Chapanis, 1996). In this study, the approach taken was to combine sev-
eral traditional methods along with the analysis of communication data. In doing
so, a complex environment can be analyzed layer by layer to capture many of the
elements present in a socio-technical system such as roles, time stress elements
and interactions.
Communication analysis, as a general methodology to study teamwork ef-
fectiveness and workflow coordination, has been used in various contexts such as
aviation and medicine. However, as the environment in each of these contexts is
characterized by its own set of constraints, the methodology must necessarily be
modified to adapt to the specific environment being studied.
In general, real-time verbal utterances by team members are recorded
along with observable events, either using hand-written notes or videotapes.
These verbal and non-verbal events are then analyzed for content and/or pattern,
based on the research questions. A coding scheme can be generated according to
the themes that emerge, allowing for subsequent detailed analysis. Typically, ver-
bal data can be processed and categorized as single-statements in which each ver-
bal utterance is considered a separate communication entry, or contextual summa-
ries with content, participants, and timing of events. In the medical environment,
verbal and non-verbal data have been collected in real-time during surgeries, tran-
scribed, and subsequently categorized into themes (e.g., equipment, planning, and
non-task related) (Nyssen & Blavier, 2010). Another approach is to group com-
munication data into types of communication failure caused by flaws in content,
audience, or purpose (Lingard et al., 2004). In aviation, single-statement verbal

35
events have been recorded, transcribed, and then analyzed for patterns such as
questions/directives followed by responses/one-bit acknowledgements (Bowers,
Jentsch, Salas, & Braun, 1998). Transcribed verbal events have also been ana-
lyzed to look for themes related to the usage of first person plural (we, us, and
ours) or verbal events related to a successful outcome or sense of achievement
(Sexton & Helmreich, 1999).
A goal of this research was to characterize and understand the behavior of
robotic surgery as a socio-technical system. As previously discussed, robotic sur-
gery has the potential to allow for remote control of the robot across distances,
necessitating collaboration between teams in different facilities. Additionally, the
implementation of a technological system in different hospitals may yield differ-
ent outcomes related to technology acceptance and team coordination within each
individual facility. This research also aimed to examine the differences in use of a
surgical robot in two very different locations: the US and France, and to examine
workplace cultural factors that may produce differences in workflow, roles, or
communication between the teams.
Professional, organizational, and ethnic or regional cultures often combine
to shape human behavioral patterns and beliefs. Differences in cultural norms can
result in different views on safety, procedures, use of technology, and interper-
sonal relationships within the work environment (Helmreich, Wilhelm, Klinect, &
Merritt, 2001). Moray has studied cultural ergonomics related to technology use,
and cites anthropometric issues, stereotypes related to a culture’s response to
stimuli, and language/iconic differences as the primary causes for cultural diffi-

36
culties in the use of technology (Moray, 2004). Ethnic and language cultural dif-
ferences add a layer to expectations of behavior and working standards in the
medical field. In the OR, there are certain standard views about team hierarchy,
decision-making power, and levels of trust and respect between medical person-
nel. Organizational factors as basic as shift scheduling, and those affecting task
outcomes such as job priorities, may also affect coordination between disparate
cultural groups. In surgery, ignoring such ethnic cultural factors may negatively
impact OR dynamics (Helmreich & Merritt, 2001). As cultural norms dictate the
behavior of individuals and teams in social settings, it is important to understand
these differences to be able to facilitate the cross-cultural team communication for
telesurgery.
Because breakdowns in teamwork and communication can jeopardize pa-
tient safety, being able to analyze team communication for points of uncertainty
or difficulty was an additional facet of this field study. In this research, an ap-
proach combining communication content and pattern analysis was used in order
to assess verbal data. This hybrid style of analysis was chosen, as it provides sev-
eral different ways of looking at communication data. Content analysis, in which
verbal events are categorized according to a pre-defined taxonomy, can be tai-
lored to look for specific topics of verbal exchanges in surgery, or can be devel-
oped over time based on the themes that emerge in preliminary observations.
On the other hand, pattern analysis provides a more generalized approach
to measuring characteristics of team interaction and performance. Pattern analysis
allows interactions between two or more team members to be examined to reveal

37
instances of uncertainty, confusion, or confidence. In addition, pattern analysis
may help to show how a team gains experience over time (e.g. from an initial sur-
gical case to a later one). It allows for comparison across surgical domains (i.e.
robotic, laparoscopic, and open surgery) and can serve as a contrast to aviation, a
similar, complex domain in which much more research into teamwork and com-
munication has been conducted. Studying only topics of conversation may not
reveal cultural or experience differences, and studying only patterns of communi-
cation may not reveal the specific workflow points at which teams collaborate to a
higher degree.
4.3. Method
4.3.1. Research Setting
A field study was conducted in the hospital OR to examine the communi-
cation patterns of surgical teams while they performed a surgical procedure using
a robotic system. Only gynecologic procedures were observed in this study, al-
lowing comparison of different teams’ communication independent of the surgical
procedure. However, given the complex nature of surgery and the constraints of
scheduling and space within the OR, data collection for this observational study
was purely opportunistic based on availability and access to robotic surgery cases.
Two cases each of two different surgical teams were observed during the spring
of 2011; one team at a teaching hospital in Boston, US, while the other team was
at a teaching hospital in Nantes, France for a total of four observed cases. The
surgical team in the US contained a mix of novice members and experienced

members of robotic surgery. In contrast, the French team members were all new
to robotic surgery (having performed less than 5 cases). Both hospitals used the da
Vinci robotic surgery syst
nents in the da Vinci system
arms, and a vision system (
monitors, placed near the operating table)
Figure 5. The da Vinci surgical system, showing (from left to right) the patient
4.3.1.1. US Data Collection
Two regularly scheduled gynecology robotic surgery cases were observed
in the US OR. During observation, hand
procedure. The notes consist
ment, the team composition, and progress of the operation with time
events such as intubation,
undocking, closure, extubation, transfer
38
members of robotic surgery. In contrast, the French team members were all new
to robotic surgery (having performed less than 5 cases). Both hospitals used the da
Vinci robotic surgery system from Intuitive Surgical, Inc. There are three
system (Figure 5): a console, a patient cart with four robotic
a vision system (referred to as the tower, consisting of speaker and
near the operating table).
The da Vinci surgical system, showing (from left to right) the patient
cart, console, and tower
US Data Collection
Two regularly scheduled gynecology robotic surgery cases were observed
he US OR. During observation, hand-written notes were taken throughout the
notes consisted of general descriptions of the physical enviro
composition, and progress of the operation with time-stamped
intubation, anesthesia administration, incision, robotic docking and
undocking, closure, extubation, transfer of patient out of room, etc. In addition,
members of robotic surgery. In contrast, the French team members were all new
to robotic surgery (having performed less than 5 cases). Both hospitals used the da
three compo-
: a console, a patient cart with four robotic
consisting of speaker and
The da Vinci surgical system, showing (from left to right) the patient
Two regularly scheduled gynecology robotic surgery cases were observed
written notes were taken throughout the
environ-
stamped
, incision, robotic docking and
, etc. In addition,

the researcher recorded, as much as possible, the verbalized communication
events that occurred in the OR.
video and audio recordings in the US operating room
completed by hand.
4.3.1.2. France Data Collection
A parallel approach was used in the robotic OR in France. Hand
notes were taken during observation of two regularly scheduled gynecology su
gical procedures. In addition, two digital video cameras, as well as a directional
microphone, were used to record all surgical events and verbal communication
between the surgical team members.
Figure 6. Placement of digital video cameras shown in physical layout of opera
ing room (a) Robotic patient cart (b) Robotic tower (c) Sterile instruments table
39
the researcher recorded, as much as possible, the verbalized communication
events that occurred in the OR. It was not possible to obtain permission to create
video and audio recordings in the US operating room; all data collection was
France Data Collection
A parallel approach was used in the robotic OR in France. Hand-written
observation of two regularly scheduled gynecology su
gical procedures. In addition, two digital video cameras, as well as a directional
used to record all surgical events and verbal communication
between the surgical team members.
Placement of digital video cameras shown in physical layout of opera
ing room (a) Robotic patient cart (b) Robotic tower (c) Sterile instruments table
the researcher recorded, as much as possible, the verbalized communication
t possible to obtain permission to create
all data collection was
written
observation of two regularly scheduled gynecology sur-
gical procedures. In addition, two digital video cameras, as well as a directional
used to record all surgical events and verbal communication
Placement of digital video cameras shown in physical layout of operat-
ing room (a) Robotic patient cart (b) Robotic tower (c) Sterile instruments table

40
(d) Operating table (e) Camera (f) Camera (g) Anesthesiology equipment
(h) Robotic console
Figure 6 depicts the placement of the video cameras as setup in the robotic
operating room. It was possible to create a more detailed timeline of observable
surgical events (such as intubation robotic docking, etc.) from subsequent tran-
scription of the video and audio recordings. In contrast to the US operating room,
the French surgical team granted permission to obtain video and audio recordings
of the surgery.
Finally, semi-structured interviews with several of the French surgical
team members were conducted in order to obtain more information as to their
training background, hospital process, opinions of teamwork, and to provide in-
sight into the strategies and difficulties encountered by novice users of the robotic
system. An interview summary is presented in Appendix C.
4.3.2. Data Analysis
Data were analyzed by first examining the hand-written notes and avail-
able video recordings of the surgeries. A high-level workflow analysis was con-
ducted to characterize the different phases of robotic surgery; each phase was
based on common surgical events found in all four cases that were used to create
a typical/canonical surgical workflow diagram. These events included tasks such
as preparing the patient, preparing the equipment, and use of the robot during sur-
gery. The events were grouped together to form phases. These events are also
readily identifiable when directly observing or viewing the videos of a surgery.

41
Next, a timeline analysis was performed to map the observed surgical events to
each of the robotic surgical phases, and to calculate performance time for all of
the phases in each of the four robotic cases.
Recorded verbal exchanges between the French surgical team members
were transcribed and translated from French to English. All verbal data (tran-
scribed and hand-written) were then coded according to a communication content
taxonomy (Table 1) adapted from Nyssen and Blavier (2010) but also based on
observed communication in this field study. The taxonomy defines three different
verbal exchange topics: equipment-related, procedure-related, and all other topics.
Table 1. Verbal exchange taxonomy for coding surgical transcriptions
Verbal Exchange Taxonomy
Equipment
E1 - Instrument change or request, clean camera
E2 - Equipment adjustment - monitor, table, lights, camera
E3 = Equipment not working / not set up
E4 - Uncertainty in equipment use / teaching use
E5 - Equipment preparation
Procedure
P1 - Task related action irrigation/cutting/suturing etc
P2 - Manipulation or removal of organs/tissue
P3 - Discuss/clarify strategy/plans/procedure/technique
P4 - Localization of organs/anatomy/where to work
P5 - Medication/anesthesia related
P6 - Status related - request patient status or info from chart
Other
WF - Non-verbal/verbal workflow related
O - Unrelated conversation, discuss other cases etc.

42
Because the robotic surgeries in France were recorded on video, a more
detailed analysis of the verbal data was performed on the French data only. This
analysis used a secondary coding scheme, adapted from previous work on team
performance and communication in the aviation industry (Bowers et al., 1998).
The purpose was to analyze communication patterns of the team in order to fur-
ther understand how experience level or workplace culture may factor into the
team’s use of the robot. Single statement verbal data were coded according to six
different categories:
1) uncertainty statements or questions
2) action statements requiring team member to perform a task
3) one-bit acknowledgement statements following (a) or (b)
4) responses, more than one-bit of info following (a) or (b)
5) planning statements
6) factual statements.
Once the data were coded and organized into a tabular format, patterns of
team interaction during various phases of the robotic surgery were extracted by
coding each single-statement verbalization according to one of the six pattern
codes listed above.
4.4. Results
Two US and two French gynecologic robotic surgery cases were observed
and analyzed, totaling 14.5 hours of observation data. The two US cases were
both robot-assisted hysterectomies. The first US case lasted 3 hours and 40 min-
utes from the time the patient was brought into the room until the time the patient

43
left the room. The second US case lasted 3 hours and 10 minutes from the time
the patient was brought into the room until the time the patient left the room.
Both cases had a similar makeup of team members: an attending robotic
surgeon, physician’s assistant, scrub nurse, and circulating nurse, all of whom
were experienced at robotic surgery. They also all had an assistant surgeon and a
medical student who were less experienced with robotic surgery. Both cases had
an anesthesiologist and a representative from Intuitive Surgical, the manufacturer
of the da Vinci system. The first French surgery lasted 4 hours and 20 minutes
from the time the patient was wheeled into the operating room, and the second
observed surgery lasted 4 hours and 10 minutes from the time the patient was
brought into the room. The French team had a similar composition for both cases;
there was an attending surgeon, assistant surgeon, three nurses, and an anesthesi-
ologist who were all new to robotic surgery. A representative from Intuitive Sur-
gical was present at both cases. The first observed French procedure was to re-
move the right ovary and the second procedure was removal of the para-aortic
lymph nodes.
4.4.1. Workflow Analysis
A robotic surgery procedure can be divided into five phases hat are largely
centered on the preparation and use of the robot (Table 2). Each phase is marked
by readily identifiable start and end points and is composed of one or more tasks.
Figure 7 shows the result of the workflow analysis.

44
In the preparation phase, both nurses and surgeons performed activities
divided into five tasks such as preparing the robot and positioning the patient on
the operating table. During the port placement phase, the surgeon, aided by an as-
sistant, installed the trocars into the patient’s abdomen and insufflated the ab-
dominal cavity to create a work volume.
The docking phase was divided into three steps (Figure 7): (1) moving the
patient cart from the corner of the room to the operating table, (2) positioning the
robotic arms and locking them into the trocars in the patient, and (3) inserting in-
struments and the camera into the robotic arms.
Table 2. Definitions of the phases of robotic surgery
Definitions of robotic surgery phases
Phase Definition
Preparation Begins after anesthesia is administered and ends just before the first skin incision. Includes preparation of robotic equipment, other surgical equipment, and patient.
Port placement Begins with the first skin incision and ends when all of the trocars have been installed and the team is ready to dock the robot.
Docking Begins when a team member first begins to move the robot to the operating table. Ends when the camera or last instrument is properly installed on the robotic arm and attached to a trocar in the patient.
Console The surgeon works a the console to complete the technical part of the surgery. The surgeon is assisted by a nurse with instrument changing, camera cleaning, and irrigation/suction. Begins when the surgeon first sits at the console and ends when the surgeon announces he or she is finished and leaves the console.
Undocking Begins when the first instrument or camera is unattached from its trocar, and ends when the robot has been moved away from the operating table.

After adjusting placement of
sions as well as internal tool collisions, the surgeon moved to the robotic console,
stationed in the corner of the OR (
procedure. An image of the robot in the French OR is shown in
eral, the surgeon worked independently, requesting instrument changes or irrig
tion/suctioning to be performed
Figure 7. Workflow diagram depicting each of the robotic surgery phases for this
analysis. Each phase is shown along with the steps performed during that phase,
listed in a typical wo
45
After adjusting placement of the robotic arms to avoid both external coll
sions as well as internal tool collisions, the surgeon moved to the robotic console,
stationed in the corner of the OR (Figure 6), and began the operative phase of the
procedure. An image of the robot in the French OR is shown in Figure 8. In ge
eral, the surgeon worked independently, requesting instrument changes or irrig
tion/suctioning to be performed from the assistant or scrub nurse as needed.
Workflow diagram depicting each of the robotic surgery phases for this
analysis. Each phase is shown along with the steps performed during that phase,
listed in a typical working order. Boxes highlighted in gray are
robotic specific tasks
the robotic arms to avoid both external colli-
sions as well as internal tool collisions, the surgeon moved to the robotic console,
), and began the operative phase of the
. In gen-
eral, the surgeon worked independently, requesting instrument changes or irriga-
from the assistant or scrub nurse as needed.
Workflow diagram depicting each of the robotic surgery phases for this
analysis. Each phase is shown along with the steps performed during that phase,
rking order. Boxes highlighted in gray are

46
At the completion of the robotic portion of the surgery, the robotic arms
were withdrawn and the robot was moved into the corner of the OR. The closure
phase was not included in this analysis because it occurred after the robotic por-
tion was complete and was variable from one case to another due to other factors
(i.e. patient condition, type of procedure or scheduling of the next procedure).
Figure 8. Robot in French operating room during console phase
4.4.2. Timeline Analysis
Figure 9 shows the results of the timeline analysis for the five phases of
robotic surgery for all four cases (two US cases and two French cases). Timing of
each phase was based on wall clock and/or video timestamp of each surgery. The
results show that the French team had longer phase times for preparation, port
placement, and docking, whereas the US team had longer console and undocking
phase times. For example, the US preparation times were 42 minutes and 32 min-

47
utes for the two observed cases. The French preparation times were 75 minutes
and 76 minutes for each of the two surgeries.
Figure 9. Phase times in minutes for each of the five robotic phases, shown across
observed US and French procedures
4.4.3. Differences in Roles
In the US, there were at least five team members working in the OR dur-
ing a robotic procedure: the surgeon, a second assistant surgeon who was experi-
enced in non-robotic surgery but who was new to robotic surgery (referred to as
surgeon trainee), a physician’s assistant (responsible for assisting the surgeon
with preparation and planning tasks, and providing surgical assistance at the op-
erative site through an “assistant port” in the patient), and two nurses (one
scrubbed in and one circulating), and a medical student. The dominant topics in
the US OR were 36% equipment-related and 53% procedure-related. Topic per-
centage was computed by dividing the number of recorded verbalizations for each

category in the content taxonomy
transcript of the data, please refer to Appendix A.
Figure 10 depicts each of the US team members physically distributed
around the operating space. Each team member’s dominant topic of verbal e
change with the surgeon is shown. These values were comp
number of verbal exchanges between two team members for each of the verbal
exchange categories and dividing that tally by the total verbal exchanges for the
pair.
Figure 10. Allocation of the most frequent t
change with surgeon in US team based on verbal exchange codes (from Table 1).
(A) Anesthesiologist, (SN) Scrub Nurse, (PA) Physician’s Assistant, (MS) Med
cal Student, (S-T) Surgeon Trainee, (S) Surgeon, (CN) Circulating Nur
48
category in the content taxonomy by the total number of verbalizations. For the
transcript of the data, please refer to Appendix A.
depicts each of the US team members physically distributed
around the operating space. Each team member’s dominant topic of verbal e
change with the surgeon is shown. These values were computed by counting the
number of verbal exchanges between two team members for each of the verbal
exchange categories and dividing that tally by the total verbal exchanges for the
Allocation of the most frequent topic and percentage of verbal e
change with surgeon in US team based on verbal exchange codes (from Table 1).
(A) Anesthesiologist, (SN) Scrub Nurse, (PA) Physician’s Assistant, (MS) Med
T) Surgeon Trainee, (S) Surgeon, (CN) Circulating Nur
For the
depicts each of the US team members physically distributed
around the operating space. Each team member’s dominant topic of verbal ex-
uted by counting the
number of verbal exchanges between two team members for each of the verbal
exchange categories and dividing that tally by the total verbal exchanges for the
opic and percentage of verbal ex-
change with surgeon in US team based on verbal exchange codes (from Table 1).
(A) Anesthesiologist, (SN) Scrub Nurse, (PA) Physician’s Assistant, (MS) Medi-
T) Surgeon Trainee, (S) Surgeon, (CN) Circulating Nurse

The topics of discussion varied depending on the roles of the team me
bers involved in each exchange. O
geon and surgeon trainee, 85.1% of them related to strategy, technique, and wor
ing site localization. The surgeon’s verbal exchanges with the nurses involved
equipment preparation and use (55.6% and 40.0% for the scrub nurse and the ci
culating nurse, respectively).
Figure 11. Allocation of the most frequent topic and percentage o
change with surgeon in
(A) Anesthesiologist, (N)
(S) Surgeon
49
The topics of discussion varied depending on the roles of the team me
each exchange. Out of all of the verbal exchanges between su
geon and surgeon trainee, 85.1% of them related to strategy, technique, and wor
e surgeon’s verbal exchanges with the nurses involved
equipment preparation and use (55.6% and 40.0% for the scrub nurse and the ci
culating nurse, respectively).
Allocation of the most frequent topic and percentage of verbal e
change with surgeon in French team based on verbal exchange codes
(A) Anesthesiologist, (N) Nurses, (R) da Vinci Surgical Representative
(S) Surgeon, (S-T) Surgeon Trainee
The topics of discussion varied depending on the roles of the team mem-
of all of the verbal exchanges between sur-
geon and surgeon trainee, 85.1% of them related to strategy, technique, and work-
e surgeon’s verbal exchanges with the nurses involved
equipment preparation and use (55.6% and 40.0% for the scrub nurse and the cir-
f verbal ex-
team based on verbal exchange codes.
R) da Vinci Surgical Representative,

50
Figure 11 depicts each of the French team members physically distributed
around the robotic operating space. There were two surgeons, both new to robotic
surgery (one surgeon had completed several robotic surgery cases while the other
surgeon had completed none), and two nurses being trained together in the roles
of scrub nurse and circulating nurse for robotic surgery. Because the nurses alter-
nated the roles of circulating and scrub nurse between each case, assisting each
other in all duties so as to learn the required tasks, they were merged into a single
role of “nurse” for this analysis. A third nurse was present in the surgeries and
also assisted the other nurses with surgical duties. There was also a representative
from Intuitive Surgical present, as well as an anesthesiologist.
The French surgeon and surgeon trainee primarily discussed strategy,
technique, and working site localization (65.5%), and the interaction with the
nurses centered on preparing and learning how to use/prepare the robotic equip-
ment (33.9%). The nurses primarily discussed usage and preparation of the
equipment (53.8%). The representative from Intuitive Surgical was involved in
verbal exchanges related to both equipment use and procedural technique for port
placement (75.9%). A full transcript of French surgery data is presented in Ap-
pendix B.
4.4.4. Communication Analysis of Select Phases
Table 3 shows a comparison of verbal exchanges between the US and
French teams for all phases of robotic surgery except undocking, which varies
based on other underlying factors such as whether there is another procedure

51
scheduled. All verbal events were categorized according to the taxonomy inde-
pendent of role or who was talking to whom. Percentages of verbal events in each
content category were calculated based on the tallies of each category divided by
the total verbal events in the surgery.
Table 3. Comparison of verbal exchange percentage between US and France
teams for all surgical phases except Console
The average value was taken between the two observed cases. In the
phases leading up to use of the console, the US team had a total of 36% equip-
ment related verbal exchanges and 53.5% procedure related exchanges. The
French team’s verbal exchanges were 56.5% equipment related and 39.1% related
to procedure. In the category of uncertainty in use of equipment, the French team
Prep, Port Placement, Docking, Console Phases
Verbal Exchange Topics
Description of Code US % France %
Equipment Related
E1: Instrument change or request 10.0 7.7
E2: Adjust equipment 11.0 9.5
E3: Not working/not set up 3.0 2.5
E4: Uncertainty in use/teaching use 4.5 25.4
E5: Equipment Preparation 7.5 11.4
Procedure Related
P1: Task related (irrigation, sutures) 7.5 4.4
P2: Manuipulation of organs/tissue 13.5 0.9
P3: Strategy/clarify plans/procedure/technique 17.5 19.3
P4: Localization of organs or workspace 8.0 13.2
P5: Anesthesia or medication 5.0 0.3
P6: Patient status/underlying patient condition 2.0 1.0
Other : Other cases, other conversation 10.5 4.5

52
had 25.4% exchanges as compared to 4.5% in the US. Conversely, the US team
had 13.5% verbal exchanges related to manipulating organs and tissues vs. the
French team, who had only 0.9% similar exchanges.
4.4.5. Communication Pattern Analysis
Table 4 shows the results of the communication pattern analysis for the
French team. The percent usage of each type of pattern (listed in left hand column
of the table) was calculated by tallying the number of verbalizations coded for
each pattern type within each phase and dividing by the total number of verbaliza-
tions for that phase.
Table 4. Pattern analysis comparison of single statement communication data for
the two observed French team robotic surgeries
4.4.6. Communication and Viewing Perspective Differences
Analysis of the communication data uncovered scenarios where team
members were collaborating on surgical tasks during the console phase, yet had
different viewing perspectives of the operative site. This situation occurred in two
Prep, Port Placement, Docking, Console Phases
Pattern Analysis
Description of Code Case 1 Case 2 Case 1 Case 2 Case 1 Case 2 Case 1 Case 2 Total %
Uncertainty statements or questions 35.3 22.5 26.7 21.7 22.9 28.1 21.8 24.4 25.3
Action statements or requests 7.5 5.5 13.3 16.1 23.2 22.9 28.9 8.6 15.2
One-bit acks to uncertainty/action 11.4 5.5 3.6 8.6 7.1 4.8 6.7 8.0 7.4
Responses to uncertainty/action 29.7 20.3 21.0 19.0 28.6 23.3 18.8 18.9 22.4
Planning statements 9.8 39.6 22.6 21.1 12.8 17.6 17.2 35.5 22.1
Observable fact statements 2.9 1.6 12.8 8.9 4.2 4.3 6.7 2.3 5.1
Other 3.3 6.6 0.0 4.5 1.2 1.0 0.0 2.7 2.4
Console %Docking %Port Placement %Prep %

53
different contexts: (1) between a more experienced surgeon and a surgeon trainee,
when the trainee was working at the console, and (2) between the surgeon work-
ing at the console and a nurse or assistant at the patient side. In all cases, the team
members were discussing where to work in the body or how to insert or move a
tool. Team members appeared to exhibit confusion and frustration while doing so.
In all cases, the surgeon was separated from the team at the console.
Table 5. Spatial communication examples
In the US cases, the surgeon often had a difficult time articulating what the
assistants should do (i.e. verbalizing the arm on which to change a tool, explain-
ing a particular location within the body that a tool should be moved to, or de-
scribing the location or anatomy where a surgeon trainee should work). Appendix
A captures general spatial communication events in the US cases. Because word-
Role: Verbalization:Surgeon 1: Where are you?Nurse: HereSurgeon 1: Push a little bit dow nNurse: Here?Surgeon 1: More dow n and tow ards the medianSurgeon 1: Yeah but here you w ill be in conflict w ith my armSurgeon 1: More dow nNurse: Here?Surgeon 1: YeahNurse: So I'll put it here?Surgeon 1: Wait, w ait. I w ill check w here you are
Role: Verbalization:Surgeon 1: I think this is the aorta because there is this thing Surgeon 2: It must be verticalSurgeon 1: You can totally see it hereSurgeon 2: No no, you should go the opposite w aySurgeon 1: Oh, you mean like upw ardSurgeon 2: No the opposite, dow nw ard
Spatial Communication Examples
Example 1: Surgeon-Nurse
Example 2: Surgeon-Surgeon

54
for-word communication transcripts and video logs were not created for the US
surgeries, it was difficult to analyze further details of these situations.
In one observed French case (Table 5, Example 1), the surgeon and the
nurse became disoriented within the patient cavity and had difficulty communicat-
ing where to move the tool. Another example from the French team (Table 5, Ex-
ample 2) involved two surgeons discussing the patient’s anatomy and surgical
plan while viewing the same site from different perspectives. In this particular
scenario, one of the surgeons was working at the robotic console while the other
was viewing the procedure via a screen in the operating room.
4.5. Discussion
4.5.1. Workflow Analysis
The tasks in the workflow diagram that are highlighted in gray are either
completely new to robotic surgery, or changed from a similar task in a non-
robotic surgery. This lends support to the idea that robotic surgery creates new
types of information as well as changing roles and responsibilities for the team
members.
Surgical teams work to achieve goals related to safety, timeliness, sterility,
resources, roles, and situation (Lingard et al., 2002). However, differences can
exist in the order or emphasis of these goals based on the local culture found in an
OR. While the workflow diagram shows a typical order of tasks, derived from the
overall observational data, there were slight variations in task order between the
US and French teams. For example, the US team completed most of the robot

55
preparation prior to the patient entering the room, whereas during the French team
cases, the robot was prepared concurrent to the port planning by the surgeons. The
difference in task order may be influenced by patient throughput and time priori-
ties at the hospital. Similarly, there were recorded instances in the US data where
the team discussed the next case or a later case, yet similar observations were not
made in France, further suggesting differences in priority based on organizational
and work cultures at the hospitals. Task order differences could also be a result of
experience level with the robot, since the novice French team had not yet opti-
mized their preparation activities in robotic surgery.
4.5.2. Timeline Analysis
An analysis of the time needed to complete each phase of the surgery pro-
vided an indication of the performance of the US and French teams. The initial
data (Figure 9) showed that the French team took longer in the phases leading up
to use of the robot, but the US team spent more time executing at the console.
Even though the console phase was the longest, it is procedure dependent, and
may not provide a good indication of experience or workplace culture differences
when compared across different cases. Preparation, port placement, and docking
times, however, are independent of the surgical procedure, and the workflow
analysis showed that all of these phases required multiple tasks. It took more time
and careful planning to ensure proper setup of the equipment and installation of
the ports and tools. While some of the time difference between the US and French
preparation may be attributed to the experience levels of the teams, during inter-
views the French team stressed an emphasis on preparation. Taking more time

56
during preparation of the robotic environment may be a result of workplace cul-
tural differences vs. the efficiency observed in the US hospital. The longer times
of the French team may also be indicative of interaction challenges when using
the robot as a new technology.
The differences in time, combined with the different order in which
equipment was prepared between the US and France suggest implications for pa-
tient safety, as the French team’s patient was under anesthesia during more of the
preparation tasks than the US team. Time is an important consideration for a pa-
tient under anesthesia, as longer times may contribute to post-operative complica-
tions and increased hospital stays (Boruk, Chernobilsky, Rosenfeld, & Har-El,
2005).
4.5.3. Differences in Roles
The results also shed light on the interpersonal structure from which roles
emerge in the OR. As shown in Figure 10 and Figure 11, the team composition
was different in France than in the US in both size and roles. For example, there
was no physician’s assistant in the French OR as there was in the US. The same
duties were performed by the nurses and surgeons together. . In France, the sur-
geon was more involved in each step of preparation whereas the US surgeon
seemed to take on more of an overseer and approver role, delegating many tasks
to the rest of the team. The roles found in each of the operating teams also suggest
that different workplace cultures exist between the French US hospitals. Previous
research has shown that blurred lines of responsibility and assumptions about
57
provider skills and knowledge may contribute to delays in patient care and ad-
verse events (Landrigan et al., 2010). For future telesurgery environments, it is
important to consider how duties will be divided between the remote teams and
that each team member is provided with a clear definition of expectations to sup-
port his or her role.
The results also show that the French and US teams share similar topics of
discussion; the surgeon and surgeon trainee discussed strategy, technique, and
working site localization, whereas communication with nurses was largely cen-
tered on equipment. Even for an experienced team such as the in the US, the team
members had to discuss and clarify how to interact with the robot. These results
indicate that even an experienced team will encounter challenges using new tech-
nology such as the surgical robot.
4.5.4. Communication Analysis of Select Phases
Communication analysis suggested differences in style and experience
level. As indicated in Table 3, the US team spent a larger percentage of communi-
cation discussing the procedure. However, the French team’s high percentage of
equipment related exchanges suggest uncertainty in use of the equipment that is
indicative of a novice team. For example, while the US team was discussing
equipment adjustment in order to optimize the robotic setup, the French team was
discussing the use and function of the equipment. At the same time, both teams
still had to devote a large percentage of communication to discuss equipment.
This supports the idea that the introduction of a robot to the operating room ne-

58
cessitates continued discussion related to the new robotic equipment, even for an
experienced team such as in the US.
During the procedure, the US surgeons directed verbalization towards ma-
nipulating organs and tissues while working in the body. In contrast, the novice
French team spent little time in this category, as they were more focused on locat-
ing where to work and understanding usage of the equipment. As teams devote a
larger percentage of communication to uncertainty in equipment use and uncer-
tainty in procedural steps, there is potentially a higher chance for communication
breakdowns and miscommunication, which may jeopardize patient safety. There-
fore, the results of this analysis shed light on possible causal factors that could
lead to patient harm.
The verbal exchange topics of the US team were also more widely distrib-
uted throughout all the topics of exchange, also suggesting a difference in experi-
ence level. It may also be indicative of a cultural or hospital organizational differ-
ence, where in the US management of the case is different than in French surgery.
4.5.5. Communication Pattern Analysis
The pattern analysis of the French data suggests several things related to
this novice team. Overall, there were more uncertainty/question statements than
action/command statements. This suggests that the inexperience of the team ne-
cessitated more clarification related to the robotic surgery activities. There were
also more detailed responses than one-bit responses (i.e., “yes” or “okay”). This
result suggests both a lack of experience (which in turn requires more information

59
feedback), but also could indicate team culture. Throughout the entire preparation
phase, the surgical team members in France were constantly communicating,
clarifying next steps or cross-checking with each other. While at first glance this
could be a result of a novice team who is uncertain of their actions, this style of
communication did not change from the first observed case to the second, despite
the gain in experience. Therefore, it could also indicate workplace cultural values
that emphasize open communication and information sharing.
Finally, the number of planning statements increased from case 1 to case
2. This result suggests that the novice team was learning and gaining confidence,
allowing them to discuss plans and strategy, as opposed to focusing more on
equipment issues.
In certain phases of robotic surgery, there were lower percentages of ver-
bal responses (e.g., docking, port placement, and console). This is not necessarily
indicative of poor team communication. Analysis of the video logs revealed that
in these phases, many responses were issued non-verbally. Examples of these oc-
curred when the surgeon asked for a tool and the nurse handed the surgeon the
tool immediately, or when the surgeons discussed port placement and indicated
with their hands or instruments instead of providing verbal confirmations.
The difference in response type between port placement and docking also
suggests something about the team’s interaction with the robot. The higher per-
centage of action statements/commands during the docking phase is indicative of
how the surgeon and rep must issue commands on how to set up the robot at the

60
operating table. For docking, non-verbal responses (in the form of moving the ro-
bot) were sufficient to close the loop on positioning directions offered by the
team, helping to explain the lower percentage of response statements. However
for port planning, the team closed the loop with verbal communication, as indi-
cated by a higher percentage of response statements. This is because the port
planning process is complex and therefore is knowledge in the head versus
knowledge in the world (Norman, 1998); the surgeon’s willingness to talk aloud
not only solidified his understanding of the process, but allowed other team mem-
bers to experience the same understanding and learning.
4.5.6. Communication and Viewing Perspective Differences
In the field study, it was observed that the surgical teams seemed to ex-
perience difficulty communicating while performing certain tasks in the console
phase, as evidenced by the communication excerpts shown in Table 5. It is plau-
sible that the lack of face-to-face communication exacerbated the difficulty of
communicating spatial information for both the US and the French teams. It is
also possible that the communication challenge was a result of the different view-
ing perspectives held by members of the operating room team. The robotic con-
sole provides the surgeon with a three-dimensional view of the operating space
that is also perfectly aligned to his or her hand movements. In contrast, anyone
else in the operating room can only view the operating site on a two-dimensional
monitor, and the view is relative to his or her stance relative to the patient on the
operating table. In addition, the US team was more experienced with the robot,

61
but still encountered the communication difficulty, perhaps because there was a
less experienced robotic surgeon working at the console.
One of the robotic surgeons in France was interviewed to gather further
insight into this problem. In the interview, spatial communication was discussed
in the context of instrument changes during the console phase of surgery. The
surgeon revealed that there is a problem with common language in robotic sur-
gery, and spatial descriptors such as “left” can mean many things, making it diffi-
cult for the surgeon and nurse to collaborate. (See Appendix C for interview
notes). As such, this field study provided the opportunity to further analyze situa-
tions such as these, where collaboration was difficult as a result of the technology.
Moving forward, further investigations into spatial communication in robotic sur-
gery could be based on the results of this initial investigation, and could propel
subsequent designs or training protocols.
4.6. Limitations
This research was a preliminary analysis of robotic surgery as a socio-
technical system. While concrete conclusions cannot be drawn, many hypotheses
can be formulated such as the influence of workplace culture on workflow and
communication, and that experience level has an effect on the topic and pattern of
communication in robotic surgery. In addition, the data set was small. Data col-
lection in a dynamic environment such as surgery generally proves to be challeng-
ing; uncertainty in the environment can cause cancelled surgeries and delays,
making it a time consuming field study. Capturing all concurrent tasks through

62
video and audio analysis must be carefully planned. The additional step of trans-
lating and understanding the context of a foreign operating team adds an addi-
tional layer to data analysis. The original two US surgeries were not videotaped;
therefore it was not possible to complete a direct comparison of single statement
data with the French team.
4.7. Summary
It is difficult to analyze a socio-technical system, especially in a complex
and dynamic environment such as the OR. In this study, workflow, time, roles,
and communication were examined in a layered methodology in an effort to un-
derstand the nature of communication in robotic surgery. Beginning with high-
level observations that formed a picture of the overall process and workflow,
teams in two different countries were observed to share the same end goal of de-
livering surgical care to a patient. These common goals align with the end goals
shared by team members in a socio-technical system. By analyzing the verbal ex-
changes for communication content, frequent topics of discussion about equip-
ment and use of the robot were observed, suggesting that the adoption of such a
new technology may be challenging, even for a more experienced team. The re-
sults shed light on how differences in experience level with the robot as well as
workplace culture differences can lead to disparities in workflow and time to ac-
complish surgical tasks. They also potentially contribute to different topics and
patterns of communication. Finally, the results helped to uncover possible con-
tributors to reduced patient safety, such as increasing the length of time under an-
63
esthesia, or potential communication breakdowns due to uncertainty in spatial dia-
logue.
If cultural ergonomic considerations are commonly applied to the design
of medical devices, then team interaction and training methods need to be studied
as well in order to facilitate successful telemedicine applications. Use of a surgi-
cal robot requires many changes to planning and use of equipment as compared to
minimally invasive surgery. Roles, tasks and workflow need to be well-defined
using a common language agreed upon and understood by all members of the lo-
cal and remote teams. This preliminary research provides an important first step
to understanding robotic surgery as a socio-technical system and in understanding
the effects of workplace culture and experience between different teams.
5. Design of a Spatial Aid for Communication in Robotic Surgery
5.1. Problem Statement
The results of the field study revealed that an especially challenging sce-
nario in robotic surgery is the communication of spatial information during the
console phase of a surgery (Table 5). As previously discussed, the surgeon is
physically separated from an assistant in order to control the robot at a console in
the corner of the room. The nurse provides intra-operative assistance with surgical
tools at the patient side. The dyad must discuss where to work, irrigate, suture,
and how to manipulate tissues and organs. However they have different viewing
perspectives associated with the single camera inside of the patient and their par-

64
ticular angle of approach to the body. Such a situation has potential for communi-
cation breakdowns, which may lead to errors.
5.2. Experimental Task
In order to investigate the way in which spatial information is communi-
cated during robotic surgery, two controlled experiments were conducted. In both
experiments, pairs of subjects worked together to move a foam liver to a target
location inside of a laparoscopic surgery training box. A camera was used to pro-
vide a view of the inside of the training box, simulating the body cavity of a pa-
tient, and the camera view was projected onto two display monitors, one for each
subject. The first subject acted as the “surgeon” at a robotic console, providing
verbal guidance to the second subject (the “assistant”), who used a laparoscopic
grasper to manipulate the foam liver. Only the “surgeon” knew the location to
which the liver would be moved. The subjects were separated by a barrier to limit
face-to-face communication, as in robotic surgery.
Subjects were given different types of spatial communication aids that
provided a shared language and could be used to support collaboration during the
task; the spatial communication aids were overlaid on each participant’s display
monitor. The first type of spatial communication aid was the cardinal directions
north, east, south, and west. The second spatial communication aid was a naviga-
tion grid. Subjects in the control condition were not given a spatial communica-
tion aid.

65
5.3. Experiment 1
5.3.1. Synopsis
Experiment 1 was an initial investigation into whether spatial communica-
tion aids may promote common ground in communication despite different view-
ing perspectives. Subjects were either given no aid at all, or were provided with a
cardinal directions aid or a grid aid. In addition, subjects performed the experi-
ment with both an aligned (0 degree) and misaligned (90 degree) perspective of
the task. There was a significant difference in performance time between the 0
and 90 degree camera rotation conditions. The results also showed that expert
surgeons, who may benefit from experience and better developed spatial abilities,
performed the experimental task two to three times faster than novices. No statis-
tically significant difference in performance time or volume of communication
when using the aids was found, potentially due to the small sample size or the in-
fluence of novice subjects’ innate spatial abilities. However, trends in the data
suggest that those who received the spatial communication aids performed faster
than subjects who received no aid.
5.3.2. Hypotheses
It was hypothesized that providing a spatial communication aid would im-
prove performance time, reduce the volume of communication, and improve the
efficiency of communication for novices.

66
5.3.3. Method
5.3.3.1. Subjects
Sixteen pairs of novice subjects who were students or staff at Ecole des
Mines in Nantes, France, aged 18-35, with no previous laparoscopic or surgical
exposure participated in the experiment. Four pairs were excluded from this
analysis for failing to follow instructions for a final total of twelve dyads. Addi-
tionally, three pairs of expert surgeons from the Institut de Cancérologie de
l’Ouest in Nantes, France participated in the experiment. Due to time and staffing
limitations when working with medical personnel, one surgeon participated in the
experiment twice, first as the person performing the task, and then as the instruc-
tor in the dyad. Figure 12 depicts a pair of subjects performing the experiment.
Figure 12. Subjects performing experiment
5.3.3.2. Apparatus
Task space: A laparoscopic training box was used to simulate the abdomi-
nal cavity of a patient. The task was set up inside the training box. The task space
consisted of a liver-shaped piece of foam placed at the bottom of the box.

67
Web Camera: A web camera was used to obtain a view of the task space
in the box. The web camera view was duplicated on two video monitors, one for
each participant.
Laparoscopic tool: A laparoscopic grasping tool was inserted through the
top of the trainer box, used for manipulating the foam organ during the task.
Video Monitor: Two video monitors were used to provide a view of the
task space, one to each of the participants. One was a 17” LCD monitor and the
other was a 17” laptop display.
Video Camera: A digital video camera with an external directional micro-
phone was used to record all subjects in the experiment.
5.3.3.3. Design
A split-plot design with three spatial interface aid conditions as the be-
tween-subjects factor and two camera rotations as the within-subjects factor was
used. In the control spatial aid condition, subjects were given no aid, and therefore
the display interface simply consisted of a video output of the task space. In the
two experimental spatial aid conditions, the video display was overlaid with a
sheet of plastic that had a spatial aid drawn on it. In one, the cardinal directions
north, south, east, and west were overlaid on the sides of the video display to pro-
vide an exocentric frame of reference and a common spatial vocabulary (Figure
13).

68
Figure 13. Task space for “surgeon” role in experiment
In the other, a navigation grid consisting of equal sized squares labeled
A,B,C,D,E and 1,2,3,4,5 was overlaid on the video display (Figure 14). Subjects
could use the grid, such as in map-reading (A2, E3, etc.) to describe the start and
end positions for the liver-shaped piece of foam, allowing for a shared under-
standing of the end goal to be quickly developed.
Figure 14. “Assistant” role performing task in grid spatial aid condition

The web camera inside
or rotated 90 degrees clockwise to provide a rotated view of the task space, as
shown in Figure 15. As depicted in the figure
cal space in which the hand
on the display monitor. Therefore, in the 0 degree condition, a parti
movement of the grasping tool
(right would appear to move to the right, left would appear to move to the left)
the 90 degree condition, there is a discrepancy between the hand movement and
the display monitor. Moving the laparoscopic
box (away from oneself) would appear as a left movement on the screen.
Figure 15. Visual-motor congruency diagram for the two camera conditions
A single trial consisted of moving the liver from a
position. Each dyad performed three trials in both camera conditions. The order of
camera rotation was counterbalanced between pairs and the end location of the
target was randomized each trial. Subjects were not told the degree o
tation (only that the camera was rotated), nor details about the spatial interface
69
inside of the trainer box was either aligned at 0 degrees,
or rotated 90 degrees clockwise to provide a rotated view of the task space, as
As depicted in the figure, the white ovals represent the p
cal space in which the hand tool moves, and the gray ovals represent what is seen
Therefore, in the 0 degree condition, a participant’s
movement of the grasping tool would be exactly mimicked on the display screen
(right would appear to move to the right, left would appear to move to the left)
the 90 degree condition, there is a discrepancy between the hand movement and
Moving the laparoscopic grasping tool forward in the task
box (away from oneself) would appear as a left movement on the screen.
motor congruency diagram for the two camera conditions
A single trial consisted of moving the liver from a start position to an end
position. Each dyad performed three trials in both camera conditions. The order of
camera rotation was counterbalanced between pairs and the end location of the
target was randomized each trial. Subjects were not told the degree of camera r
tation (only that the camera was rotated), nor details about the spatial interface
the trainer box was either aligned at 0 degrees,
or rotated 90 degrees clockwise to provide a rotated view of the task space, as
, the white ovals represent the physi-
tool moves, and the gray ovals represent what is seen
pant’s
would be exactly mimicked on the display screen
(right would appear to move to the right, left would appear to move to the left). In
the 90 degree condition, there is a discrepancy between the hand movement and
grasping tool forward in the task
box (away from oneself) would appear as a left movement on the screen.
motor congruency diagram for the two camera conditions
start position to an end
position. Each dyad performed three trials in both camera conditions. The order of
camera rotation was counterbalanced between pairs and the end location of the
f camera ro-
tation (only that the camera was rotated), nor details about the spatial interface

70
aids presented on their screens. They also were not told whether the other partici-
pant had the same spatial interface aids, but they were allowed to ask each other
about it during the experiment.
5.3.3.4. Procedure
The training box was set up on a table, and subjects were separated at the
table by a divider so that they could not see each other. One participant in the pair
was randomly assigned the role of “surgeon” and the other “assistant”. The “sur-
geon’s” goal was to reposition the foam liver to a location prescribed by a line
drawing of the liver, displayed only on the “surgeon’s” screen, as shown in Figure
16.
The “surgeon” was instructed to verbally guide the “assistant” in complet-
ing the task, and the pair was encouraged to talk freely in order to collaborate dur-
ing the exercise. The trainer box was placed in front of the “assistant”, who was
provided with a laparoscopic grasper. The “assistant” was given a brief orienta-
tion on how to operate the grasper and allowed to practice for one minute.
Figure 16. Foam liver and target outline displayed on “surgeon” role’s screen

71
Subjects were also told to complete the task as quickly and as accurately
as possible. Once both participants were ready, timing began when the “surgeon”
uttered the first instruction. Timing ended for each trial when the experimenter
verified that the organ was correctly aligned within the target outline.
5.3.3.5. Analysis
Participants performed the task in either English or French, depending on
which language they were more comfortable with. All experimental trials were
videotaped. French communication data were transcribed and translated into Eng-
lish for analysis, and English communication data were transcribed for analysis.
In the transcription of communication data, each complete utterance or logical
train of thought was coded as a single unit, up until the point at which a subject
paused during communication, or when the end of a verbal utterance was clear.
Recorded communications therefore consisted of whole sentences, questions,
fragments or chains of fragments, and one word commands or responses.
One pair performed only 5 trials due to a technical difficulty with the
equipment (as compared to the 6 total trials if all went well). Participants were
stopped after 8 minutes if they had not yet completed the trial in order to avoid
fatigue, in which case the time data was recorded at a cap of 480 seconds.
The video and audio logs were analyzed to calculate trial completion
times. From this, overall mean times were calculated for each camera condition
and for each spatial interface aid condition.

72
Quantitative communication data consisted of the total number of com-
munications per trial (communication volume) and communication ratio (# “sur-
geon” communications/ # “assistant” communications). Overall mean communi-
cation values were calculated for each camera condition and spatial interface aid
condition for each pair.
Split-plot ANOVAs were performed on the time and communication vol-
ume data using SAS at an alpha level of 0.05. Residual data were first tested for
normality in SAS using the Shapiro-Wilk statistic.
Transcribed communication data were also examined to determine which
frame of reference was utilized. Data were categorized according to exocentric,
allocentric, or egocentric frames of reference. References made to the grid and the
cardinal directions, or directions relative to the sides of the video monitor were
categorized as exocentric. References made to the liver were categorized as allo-
centric, and directions given relative to the “assistant” performing the task were
categorized as egocentric. Additionally, the average number of reference frame
switches per trial was tabulated.
5.3.4. Results
The results of the time analysis are presented in Figure 17. For the novices
(N=24), subjects in the grid condition performed the fastest, with a mean time of
178.3 + 31.3 seconds, followed by the cardinal directions condition, 191.5 + 38.2
seconds, and those in the no aid condition performed the slowest at 256.3 + 68.3
seconds. Expert surgeons (N=6) performed two times faster than novices in the 0

73
degree camera condition, and three times faster than the novices in the 90 degree
camera condition. Expert surgeons also performed five times faster than novices
in the no aid condition, twice as fast as novices in the cardinal directions condi-
tion, and three times faster in the grid aid condition.
Figure 17. Results of the time analysis for all experimental conditions
Figure 18. Task completion time vs. communication volume for novices for
spatial aid conditions (averaged across camera rotations)
0
50
100
150
200
250
300
350
400
450
500
No Aid Cardinal Directions Aid Grid Aid
Tim
e (s
ec)
Novice - 0 Deg.
Novice - 90 Deg.
Expert - 0 Deg.
Expert - 90 Deg.
0
50
100
150
200
250
300
350
No Aid Cardinal Directions Aid
Grid Aid
Avg. # Comms.
Avg. Time (sec)

74
The two-way ANOVA analysis on the novice subjects’ data (which was
first tested for normality using the Shapiro-Wilk statistic) showed a significant
difference in time performance between the rotated and non-rotated camera angles
(p < 0.0001), but no significant effect as a function of spatial interfaces (p =
0.104) nor an interaction effect between the two factors (p = 0.183). Because only
one pair of expert surgeons performed in each spatial aid condition, expert data
could not be included in the statistical analysis.
The volume of communication that occurred within dyads remained rela-
tively constant over each of the spatial aid conditions, as shown in Figure 18. Ta-
ble 6 shows the number of verbalizations for each of the experimental conditions.
Table 6. Communication volume and ratio results
No Aid Volume Ratio Volume Ratio
0 Degrees 34 10 12 3790 Degrees 77 3 17 7
Mean 55 6 15 22
Cardinal Directions Aid
0 Degrees 30 4 17 2490 Degrees 71 2 40 6
Mean 51 3 28 15
Grid Aid
0 Degrees 36 2 17 5
90 Degrees 62 2 22 3
Mean 49 2 20 4
Communication Volume and Ratio Results
Novices Experts

75
Figure 19. Ratio of “surgeon” to “assistant” communication
(averaged across camera rotations)
Table 7. Frame of reference analysis results
Two-way ANOVA on the volume of communication (which was first
tested for normality using the Shapiro-Wilk statistic) showed a significant effect
due to the camera angle (p < 0.0001) but not due to the spatial interface aid condi-
0
5
10
15
20
25
No Aid Cardinal Directions Aid
Grid Aid
Rat
io o
f C
om
mu
nic
atio
n Novices
Experts
No Aid 0 Degrees 90 Degrees 0 Degrees 90 Degrees
Allocentric 79.75 57.5 13 67Exocentric 3.75 12 87 33Egocenric 16 27.5 0 0# Sw itches 2 6 6 2
Cardinal Directions AidAllocentric 39.8 52.3 36.0 45.0Exocentric 47.8 38.8 62.0 50.0Egocenric 12.5 9.0 2.0 4.0# Sw itches 2 10 6 6
Grid AidAllocentric 68.0 54.4 46.0 55.0Exocentric 25.0 30.9 54.0 45.0Egocenric 6.8 13.9 0.0 0.0# Sw itches 3 5 4 6
Frame of Reference Analysis Results
Novices Experts

76
tion (p = 0.851). No interaction between the two factors was found (p = 0.419).
Once again, expert surgeon data could not be included in the statistical analysis
because only one pair participated in each spatial aid condition.
The communication ratio, which is a measure of how balanced the ver-
balizations were between “surgeon” and “assistant” roles, was calculated by di-
viding the number of “surgeon” communications by the number of “assistant”
communications. A 1.0 ratio suggests that the subjects each had an equal number
of communications in the task. In both non-rotated and rotated camera conditions,
a ratio of 6.37 was obtained for the no aid condition, while a ratio of 3.2 was ob-
tained for the cardinal directions condition, and 1.88 for the grid condition. Table
6 and Figure 19 show the average ratio of communication for each of the experi-
mental conditions between novices and expert dyads.
Table 7 presents the results of the frame of reference analysis. Novices in
the cardinal directions and grid conditions utilized an exocentric frame of refer-
ence more than novices in the no aid condition. The no aid condition (21.75%)
participants employed an egocentric reference frame more often than in the cardi-
nal directions (10.8%), and grid conditions (10.3%). Subjects also utilized a vari-
ety of communication strategies, as shown in Table 8.

77
Table 8. Communication excerpts from Experiment 1
5.3.5. Discussion
These results suggest the benefit of an interface aid to improve spatial
communication during robotic surgery. It was hypothesized that task time and
communication would improve in the cardinal directions and grid aid conditions
Grid Condition
"Surgeon" Ok so the top part of the liver has to be in c3, bottom part, very very very bottom part it slightly touches it
"Assistant" The bottom part is in c3?"Surgeon" Top part"Assistant" Ok"Surgeon" So just a smaller one"Surgeon" And then the bottom part, the big bump, is in d5 and the top upper left
square"Surgeon" So you have to bring it dow n a little bit"Surgeon" You understand w hat I am saying, or...?"Assistant" Yeah"Surgeon" Yeah ok
Cardinal Directions Condition"Surgeon" And now rotate it 90 degrees "Assistant" Which direction? East or w est?"Surgeon" East"Assistant" East 90 degrees"Surgeon" Exactly"Assistant" That w as 45"Surgeon" That looked like 90. ok you w ant it to be on the opposite side so 180
degrees"Assistant" Ok"Surgeon" Ok that’s perfect"Surgeon" Now just move it up"Assistant" Up?"Surgeon" Well just push it a little bit to the north
No Aid Condition"Surgeon" Alright, you have to rotate it, like counterclockw ise, 90 degrees"Surgeon" But w ithouth moving it just rotate it"Surgeon" Ok that position is perfect but you have to move it dow n like 3 cm"Assistant" Ok"Surgeon" Try not to like change the inclination or the angle"Surgeon" Ok"Assistant" Ok f ine, or more?"Surgeon" To the right now"Assistant" To my right?"Surgeon" Yes"Surgeon" Yeah now rotate it a little bit fom the low er part"Assistant" Which direction?"Surgeon" From the low er part, a little bit to the left
Communication Excerpts from Spatial Interface Aid Conditions

78
because these spatial communication aids provided a common language that sub-
jects could use while collaborating.
5.3.5.1. Time
While there was not a significant difference in time amongst the spatial in-
terface conditions, the trends in the data in Figure 17 suggest that participants us-
ing the cardinal directions performed faster, and even more so when using the
grid, versus no aid at all. This result was even more pronounced when the task
camera was rotated by 90 degrees, at which point the task became increasingly
difficult for novices and the surgical experts alike. Past studies have shown that a
90 degree rotation is especially difficult (Macedo, Kaber, Endsley, Powanusorn,
& Myung, 1998; Cao, 2004; Smith & Smith, 1962). The lack of significance
among spatial aid conditions could potentially be explained by a large variation in
subjects’ innate spatial abilities, a metric not collected in Experiment 1. In fact,
novices may rely more on their natural spatial abilities in laparoscopic surgery,
while experts rely more on their experience and training (Keehner, Tendick, &
Meng, 2004). It was expected that the task would be difficult for novices, who
would improve their visual-motor skills over time. The large variance in perform-
ance data could also be explained by the small data set. Furthermore, participant
trials were stopped at 480 seconds (8 minutes) in order to prevent fatigue. There
were several novice groups who reached the 480 second maximum, the majority
of whom were in the no aid condition. This suggests that there could have been a
larger separation in performance time between the control and experimental spa-
tial interface aid conditions. In surgery, time is an important consideration when a

79
patient is under anesthesia. At the same time, however, time is not necessarily the
best indicator of performance; accuracy may be more critical than speed in some
surgical situations, and small reductions in time of a few seconds have less of an
impact in hours-long surgical procedures.
5.3.5.2. Communication Volume
It was expected that the volume of communication would decrease in the
cardinal directions and grid aid conditions when compared to the no aid condition.
The results did not support this hypothesis. However, a significant difference in
the volume of communication occurred between the 0 degree and 90 degree cam-
era conditions, again suggesting the increase in difficulty in the task. Therefore, it
is possible that the decrease in communication among spatial interface aid condi-
tions was not seen because the task was difficult and necessitated more communi-
cation regardless of spatial aid. There was also a limitation in the original instruc-
tions provided to subjects in the experiment. Subjects were not told that both the
“assistant” and “surgeon” had the same spatial aid, and instructions were not pro-
vided to the participants about how the spatial aid could be used. Therefore, sub-
jects may have had to engage in more communication than originally expected in
order to perform the task.
5.3.5.3. Communication Ratio
There was a shift in the ratio of communication from the no aid condition,
in which a higher ratio could indicate a one-sided dialogue in the task, to a lower
ratio in the cardinal directions and grid conditions. As the ratio moves towards
1.0, it suggests a more collaborative environment in which the subjects are work-

80
ing together in order to achieve common ground. The ratio in the grid condition
was the lowest, as expected, because it is designed to not only provide a shared
language and common visual aid, but allows both people to share a vision of the
end position. While the cardinal directions spatial aid provided a shared language
and common visual aid, it did not provide a way to visualize the end position as
the grid did (“the end position is in C2”). Therefore, while the ratio in the cardinal
directions condition was lower than the no aid condition, it was not as low as the
grid condition. This result is important as it suggests collaboration; the pairs are
working to achieve common ground while completing the task. The same trend
can be seen with the surgeon data, suggesting that even experts may benefit from
the spatial communication aids.
The ratio effect is especially revealing because of the importance of col-
laboration and communication between surgical team members. The traditional
hierarchy found in surgery may have, in the past, inhibited nurses or junior sur-
geons from speaking up. However, surgery is beginning to adopt the more open
environment found in aviation in order to promote effective communication and
team skills. The spatial interface aids promote collaboration in the surgical task
despite the lack of face-to-face communication, moving it towards a truly team-
oriented environment.
5.3.5.4. Frame of Reference
Novices and experts varied in their choice of frame of reference to de-
scribe the task, shown in Table 7. Experts tended to utilize an exocentric frame of
reference in all conditions regardless of spatial aid, perhaps due to their experi-

81
ence level in this type of visual-motor task. Novice subjects, in contrast to experts,
attempted to work from an egocentric frame of reference, centered on the “assis-
tant” who was performing the task. This may have been due to the difficulty of
the “assistant” adjusting to the 90 degree camera rotation, and the “surgeon” role
attempting to assist by adopting the “assistant” view (subjects were both aware
that the camera was rotated, but not which direction or the degrees of rotation).
Past studies have shown that people either try to take the other person’s egocen-
tric frame of reference, or use language that makes sense from either person’s per-
spective (allocentric, in this case) (Schober, 1995). However, for the novices,
adopting an egocentric viewpoint in spatial descriptions proved to be less success-
ful than the surgeons, who clearly performed faster and did not utilize a person-
centered reference frame.
5.3.5.5. Communication Strategies
Subjects adopted strategies related to both manipulation and task plan
(Table 8). Regarding movement, the “surgeon” either first had the “assistant” ro-
tate the organ to reach the correct orientation, and then translate it to the correct
target position, or conversely, the “surgeon” would direct the “assistant” to move
the organ to the general target area first, and then work on fine-grained rotation.
In the former, “assistants” often struggled to keep the original rotation in
place while performing longer lateral movements, and had to make adjustments
once in place. Dyads usually adopted the option that seemed easiest for the “assis-
tant” performing the manipulations, sometimes settling on a strategy in the first
trial and sometimes not until the last trial. The grid aid condition seemed to be

82
especially conducive to this goal-based strategy, and it appeared to promote
common ground in communication by allowing the “assistant” to share in the vi-
sion of where the target was located. Subjects’ overall success related to the
strategies appeared to be related to consistency developed over the course of the
six trials. Dyads that established a consistent plan and consistent spatial descrip-
tions seemed to perform the best.
5.3.6. Limitations
Many of the novice subjects were students at an international school who
performed the task in English, which was not their native language. Therefore,
possible effects due to language barriers may exist. Subjects also had varying
natural spatial abilities that were neither measured nor accounted for, which may
have had an effect on the results, especially of either poorer or better performing
teams.
Four of the original dyads did not make use of the spatial interface aids
that were provided during the experiment and were therefore excluded from this
analysis. Those subjects cited lack of awareness of the spatial aid or not feeling
they needed to use it as reasons for ignoring the aid. This complication is an inter-
esting finding, given the fact that technology designers often add functionality
that is never engaged by the end users. Finally, this was a limited data set, and
more data should be collected from both novices and the expert surgeon group in
order to see the true effects of the spatial aids on the end user group.

83
5.4. Experiment 2
5.4.1. Synopsis
The results of Experiment 1 suggested that spatial communication aids
may be beneficial to collaboration in a complex, visual-motor task such as robotic
surgery, where face-to-face communication is limited. However, the experiment
lacked evidence of the influence of innate spatial ability on performance in the
task. It was unclear whether subjects in the grid aid or cardinal aid conditions per-
formed faster because of the spatial aid alone, or because subjects in those condi-
tions had a higher natural spatial ability. There were also potentially some effects
due to language barriers present in the data and issues with subjects ignoring the
provided spatial aids. To address these concerns, a follow-up experiment was
conducted. Specifically, the second experiment aimed to examine the influence of
spatial ability in the absence or presence of a spatial communication aid by testing
subjects’ spatial abilities. Modifications were made to the language requirements
and the experimental instructions in order to address the other shortcomings of
Experiment 1. The performance times and communication volumes among the
three spatial aid conditions were not found to be statistically different. However,
trends in the data suggested that subjects who were given a spatial aid performed
faster and communicated less than those who had no aid at all. Furthermore, sig-
nificant correlations were found between spatial ability, performance time, and
communication volume, suggesting that using a spatial aid reduces some reliance
on natural spatial ability. Analysis of communication for content, frame of refer-
ence, and strategy provided examples of subjects who performed well and used

84
the spatial interface aids, as well as poor performers who were not given a spatial
aid.
5.4.2. Spatial Ability Literature
Previous research has uncovered correlations between spatial ability and
surgical performance, most prominently in novices. One such study investigating
the influence of external factors on laparoscopic skills found that variables such as
age, experience, and visual spatial perceptual ability affect the speed at which
surgeons can perform fundamental laparoscopic drills (Risucci, Geiss, Gellman,
Pinard & Rosser, 2001). A second study measured spatial ability, videoscopic
experience, and operative skills across novice and experienced laparoscopic sur-
geons and found the novice subjects to have a significant positive correlation be-
tween spatial ability and operative skills, a correlation not present for the experi-
enced subjects (Keenher et al., 2004). Thus, spatial ability certainly influences
one’s ability to perform well in a complex visual-motor task. In a collaborative
environment, spatial abilities of each team member come into play when govern-
ing the overall performance in the task.
Over time, as novices move toward more of an expert level, spatial ability
improves through practice. For example, in a study of repeated 3D mental rotation
problems, Lohman and Nichols (1990) found that subjects gained in speed and
accuracy by up to one standard deviation over the course of several blocks of tri-
als, an effect attributed to practice. When another group of subjects performed the
test with no practice, the large gains in accuracy were absent (Lohman & Nichols,

85
1990). Stransky, Wilcox, and Dubrowski (2010) studied the impact of mental ro-
tation training on performance in laparoscopic surgical training tasks, and found
that participants performed significantly better on surgical training tasks that re-
quired a higher degree of mental rotation after completing mental rotation training
exercises. Thus, practice also plays a role in performance during a complex task,
and Experiment 2 included the addition of a practice trial in order to offset some
of the visual-motor difficulty encountered by novices in the task.
Many tests have been developed to isolate and measure spatial ability.
These include figural rotation tests (Shepard & Metzler, 1971), card rotation tests
(Ekstrom, French, Harman & Dermen, 1976) and form board tests (Likert &
Quasha, 1970). Such tests are simple to administer and can quickly be analyzed
and incorporated into a larger dataset for examination. Obtaining a measure of
spatial ability provides further insight into the behavior observed in a motor skill.
In Experiment 2, the spatial ability test of Ekstrom et al. (1976) was incorporated
in order to examine the interaction between spatial interface aid design and innate
spatial ability.
Heagerty, Montello, Richardson, Ishikawa and Lovelace (2006) investi-
gated how transferrable figural-scale paper and pencil spatial ability tests are to
larger-scale object manipulation or navigation tasks and found some degree of
difference between factors contributing to small-scale and those to large-scale
abilities. In this study, a paper and pencil spatial ability test was utilized; however,
such smaller-scale exercises may translate more readily to similarly small-scale
laparoscopic tasks visualized in 2D format.

86
5.4.3. Hypotheses
Akin to Experiment 1, it was hypothesized that spatial interface aids
would promote common ground in a collaborative spatial task by improving per-
formance time and lowering the volume of communication. It was further hy-
pothesized that subjects with a higher spatial ability (measured via a spatial ability
test) would perform faster and communicate less than subjects with a lower spa-
tial ability. It was also hypothesized that the spatial interface aids would help sub-
jects perform faster and with less communication than subjects who did not re-
ceive a spatial aid, regardless of spatial ability score. Finally, because surgery is a
local task (i.e., versus global), it was hypothesized that the grid aid would provide
a greater benefit over a global oriented aid such as the cardinal directions.
5.4.4. Method
5.4.4.1. Subjects
Fifteen dyads of novice subjects who were students at Tufts University or
local Boston residents, aged 18-42, with no previous laparoscopic or surgical ex-
perience, participated in the experiment. An effort was made to balance the num-
ber of males and females assigned to each of the roles for the task. In order to re-
move any effects due to language barriers encountered during Experiment 1, only
native English speakers were recruited for the study.
5.4.4.2. Apparatus
Several improvements were made to the experimental space, including (1)
improvement of the task by using a digital spatial aid overlay instead of a plastic

87
overlay in order to present the spatial aid in a more professional manner, and (2)
reconstructing the liver-shaped piece of foam to be sturdier (it was easily flipped
over in Experiment 1). Otherwise, the apparatus used in Experiment 2 were the
same as in Experiment 1, except both participants used the a 17” LCD monitor to
view the task space (i.e., as opposed to a laptop and a monitor in the first experi-
ment). Figure 20, Figure 21 and Figure 22 depict the new task space.
5.4.4.3. Design
The design of the experiment was the same as Experiment 1, except that
the non-rotated camera condition was removed, yielding a between-subjects de-
sign with three spatial interface aid conditions at a fixed 90 degree camera rota-
tion for all participants. The 90 degree visual-motor diagram is shown on the left-
hand side of Figure 15.
5.4.4.4. Procedure
The procedure for Experiment 2 was the same as that of Experiment 1, ex-
cept for the following changes:
First, both participants were administered a standardized spatial ability
written test pre-experiment in order to gather data on subjects’ innate spatial abili-
ties. The test was part of the Educational Testing Services (ETS) Cognitive Test
Kit, and consisted of a two-dimensional (2D) card rotation test as well as a three-
dimensional (3D) cube rotation test. Both parts were listed as components of the
Spatial Ability cognitive factor in the Cognitive Test Kit.

88
Figure 20. Laparoscopic trainer box
Second, both participants were made aware of the entire experimental
setup; i.e., they were both shown the “assistant” and “surgeon” task space, with
trainer box and monitor, and told that both subjects had the exact same monitor
with the same spatial interface aid (where applicable). Examples of both the “as-
sistant” and “surgeon” workspaces are shown in Figure 21 and Figure 22, respec-
tively. Subjects were given a short introduction to the spatial interface aid. Those
receiving the grid aid were told they could use the grid to explain the final posi-
tion of the organ or how to orient it.
Likewise, those receiving the cardinal directions aid were told they could
use the directions to describe how to move or rotate the organ, or use it to de-
scribe the approximate final position. Subjects were told that the aids were there
to help them, but there were no rules imposed on how they could communicate.
All participants were told that the purpose of the experiment was to study their

89
collaboration in the task. Third, subjects performed one untimed practice trial be-
fore completing the three official timed trials of the experiment.
Figure 21. View of the “assistant” task monitor in the grid aid condition
Figure 22. “Surgeon” role task monitor in cardinal directions aid condition

90
5.4.4.5. Analysis
Data were analyzed in a manner similar to Experiment 1. Time data were
extracted from the video logs, and all verbal events were transcribed for analysis.
From the transcription, communication volumes for each individual subject and
the total per each dyad were tabulated, and the ratio metric was computed for each
dyad as well.
Table 9. Taxonomy used to code experimental spatial communication data
A one-way ANOVA was performed in SAS on the time data, and non-
parametric Kruskal-Wallis tests were performed on the communication and ratio
data. The spatial abilities tests were scored to produce an overall score for each of
Communication Content Taxonomy
Code: Description:
CD
LRUD
GRID
ROT
DIS
ANT
GEN General spatial utterances (“move it more”, “keep going”)
NS Non-spatial utterances (“this is difficult”)
Verbal references to the anatomy of the liver (liver had a large side and a small side, a convex side, and a concave side)
Verbal references to the cardinal directions “north”, “south”, “east”, "west"
Verbal references to the directions “left”, “right”, “up”, or “down”
Verbal references to the navigation grid interface
Verbal references to rotating or flipping the liver (including clockwise/counterclockwise, number of degrees to rotate, or specific discourse instructing to rotate or turn the liver)
Verbal references to exact distances to move (inches, cm)

91
the 2D and 3D components. Individual scores for each role were recorded along
with the overall average per dyad. A correlation analysis was conducted in Excel
using the spatial ability scores, time, and communication data.
Transcribed communication data were also examined for frame of refer-
ence using the same taxonomy as Experiment 1. The data were also coded accord-
ing to one of eight categories, developed based on observational analysis of the
data. The categories are shown in Table 9.
5.4.5. Results
Table 10 presents the average spatial ability scores for each of the experi-
mental conditions, as determined via the pre-experiment paper test. Paired t-tests
were conducted to assess homogeneity of spatial abilities among groups. The spa-
tial data were first tested for normality and equality of variance. The t-tests re-
vealed that subjects had the same spatial ability in all conditions except for a dif-
ference in 2D score between the grid aid and the no aid conditions (P(T<=t) two-
tail = 0.026). Subjects in all three experimental conditions had the same 3D spa-
tial ability.
The results of the time analysis are presented in Figure 23 and Table 11.
Subjects in the spatial aid condition performed the fastest, with a mean time of
210.5 + 114.7 seconds, followed by the grid aid condition, 244.9 + 70.0 seconds,
and those in the no aid condition performed the slowest at 303.1 + 73.1 seconds.
Time data were tested for normality using the Shapiro-Wilk statistic. A one-way
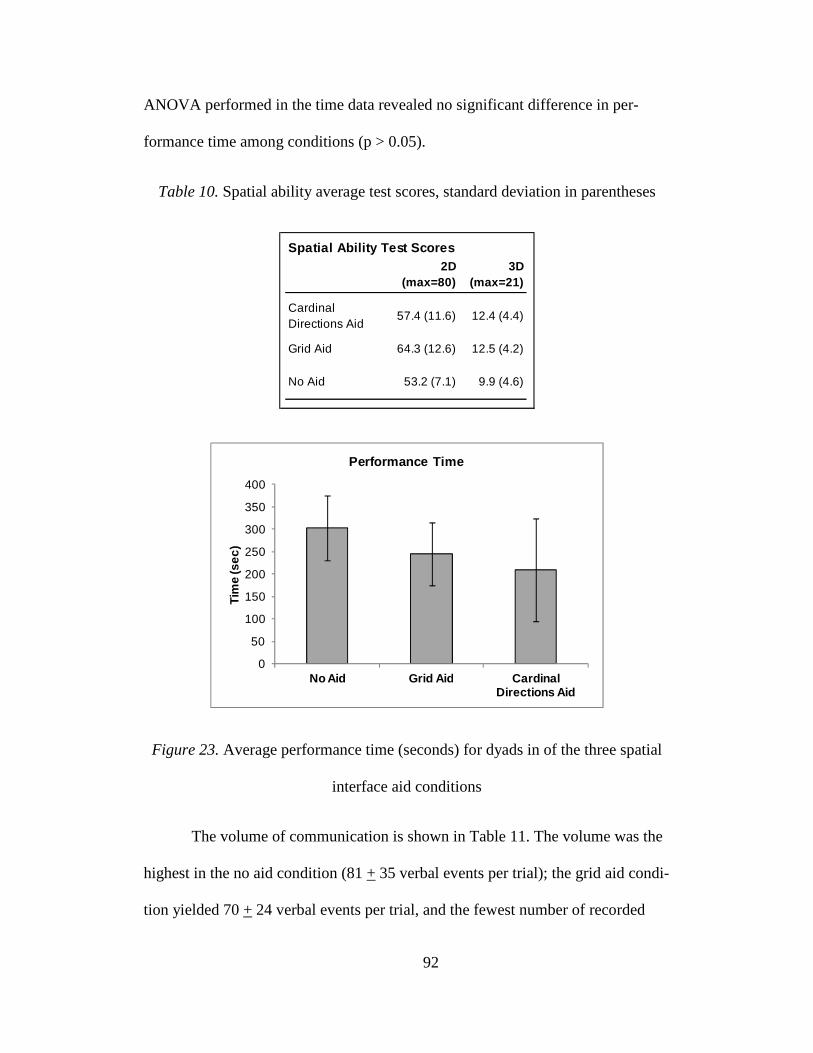
92
ANOVA performed in the time data revealed no significant difference in per-
formance time among conditions (p > 0.05).
Table 10. Spatial ability average test scores, standard deviation in parentheses
Figure 23. Average performance time (seconds) for dyads in of the three spatial
interface aid conditions
The volume of communication is shown in Table 11. The volume was the
highest in the no aid condition (81 + 35 verbal events per trial); the grid aid condi-
tion yielded 70 + 24 verbal events per trial, and the fewest number of recorded
2D (max=80)
3D (max=21)
Cardinal Directions Aid
57.4 (11.6) 12.4 (4.4)
Grid Aid 64.3 (12.6) 12.5 (4.2)
No Aid 53.2 (7.1) 9.9 (4.6)
Spatial Ability Test Scores
0
50
100
150
200
250
300
350
400
No Aid Grid Aid Cardinal Directions Aid
Tim
e (s
ec)
Performance Time

93
verbal events occurred in the cardinal directions condition at 56 + 25 verbal
events per trial. Non-parametric Kruskal-Wallis analysis did not reveal any sig-
nificant difference in volume across conditions. The communication ratio, also
shown in Table 11, did not vary significantly among conditions according to a
Kruskal-Wallis non-parametric analysis.
Table 11. Average time, volume of communication, and ratio of communication.
Standard deviations are shown in parentheses.
The results of the correlation analysis (Table 12) show trends in correla-
tion between spatial ability, time, and communication volume for each of the ex-
perimental conditions. There is a significantly strong negative correlation between
the dyad 2D spatial score and performance time when no spatial interface aid was
provided (-0.88*). The correlation between the individual spatial ability of the
“surgeon” role compared to the dyad’s performance time increases negatively
from the no aid condition (-0.25) to the grid aid condition (-0.46). Conversely, the
correlation between the “assistant” role’s spatial score and time increases posi-
tively from the no aid condition (-0.75) to the grid condition (-0.22).
Time (s) # Comm Ratio
Cardinal Directions Aid
210.5 (114.7) 56 (25) 4.0 (2.1)
Grid Aid 244.8 (70.0) 70 (24) 2.9 (1.2)
No Aid 303.1 (73.1) 81 (35) 3.7 (2.9)
Performance Metrics

94
Table 12. Correlation results for Experiment 2
There is a significantly strong negative correlation between the spatial
ability of the “surgeon” role and the amount he or she communicates in the grid
aid condition (-0.91*). Finally, the trend in the “assistant” role’s communication
volume correlated with his or her spatial score changes from a stronger negative
correlation in the no aid condition (-0.65) to a strong positive correlation in the
grid aid condition (0.83).
Upon examining the correlation between a pair’s average 3D spatial score
and time, there is little correlation in the grid aid (-0.06) and cardinal directions (-
0.14) condition, but an increasingly negative correlation in the no aid condition (-
0.51). The data also show an increasingly strong negative correlation between the
“surgeon” role’s 3D spatial ability and the pair’s performance time (-
Correlations Between Spatial Abilities, Performance Times
and Communication Volume
Dyad Score vs.
Time
Surgeon Score vs.
Time
Assistant Score vs.
Time
Dyad Score vs. # Comm
Surgeon Score vs. Surgeon Comm
Assistant Score vs. Assistant
Comm
2D Spatial Score Correlations
Grid Aid -0.62 -0.46 -0.22 -0.38 -0.91* 0.83
Cardinal Directions Aid -0.66 -0.38 -0.44 -0.49 0.16 -0.36
No Aid -0.88* -0.25 -0.75 -0.48 0.15 -0.65
3D Spatial Score Correlations
Grid Aid -0.06 -0.02 -0.09 -0.08 -0.19 0.56
Cardinal Directions Aid -0.14 -0.39 -0.14 -0.38 -0.06 -0.06
No Aid -0.51 -0.80 0.41 -0.96* -0.67 0.12
Correlation Between Dyad Communication and Time
Grid Aid 0.44
Cardinal Directions Aid 0.95*
No Aid 0.34
Note. *p<.05

95
0.80).Examining the average dyad score vs. the volume of communication, the
data show little correlation in the spatial aid conditions, but a significantly strong
negative correlation for the no aid condition (-0.96*).
The data also show a higher negative correlation between the “surgeon”
role’s 3D spatial score and the “surgeon” role’s volume of communication for the
no aid condition. Additionally, while there was little correlation between the “as-
sistant’s” spatial score and “assistant’s” communication in the no aid and cardinal
directions condition, there was a positive correlation in the grid aid condition
(0.56).
Finally, the data show that there is a significantly strong positive correla-
tion between performance time and volume of communication in the cardinal di-
rections condition (0.96*).
The verbal content distribution is shown in Table 13. Subjects in the car-
dinal directions interface aid condition referenced the cardinal directions the most,
where as only subjects in the grid aid condition referenced the grid. Subjects in
the grid aid condition also utilized the spatial descriptors “left”, “right”, “up”, and
“down” the most (17.2%) compared to the no aid condition (14.6%) and the car-
dinal direction interface aid condition (5.4%). Subjects in the no aid condition
spent a higher percentage of their discourse using general communication descrip-
tors (e.g., “move it more” as opposed to “move it more to the left” or “move it
clockwise”) at 39.6%, whereas subjects in the cardinal directions (33.2%) and
grid aid condition (32.0%) used less overall generic spatial descriptors.
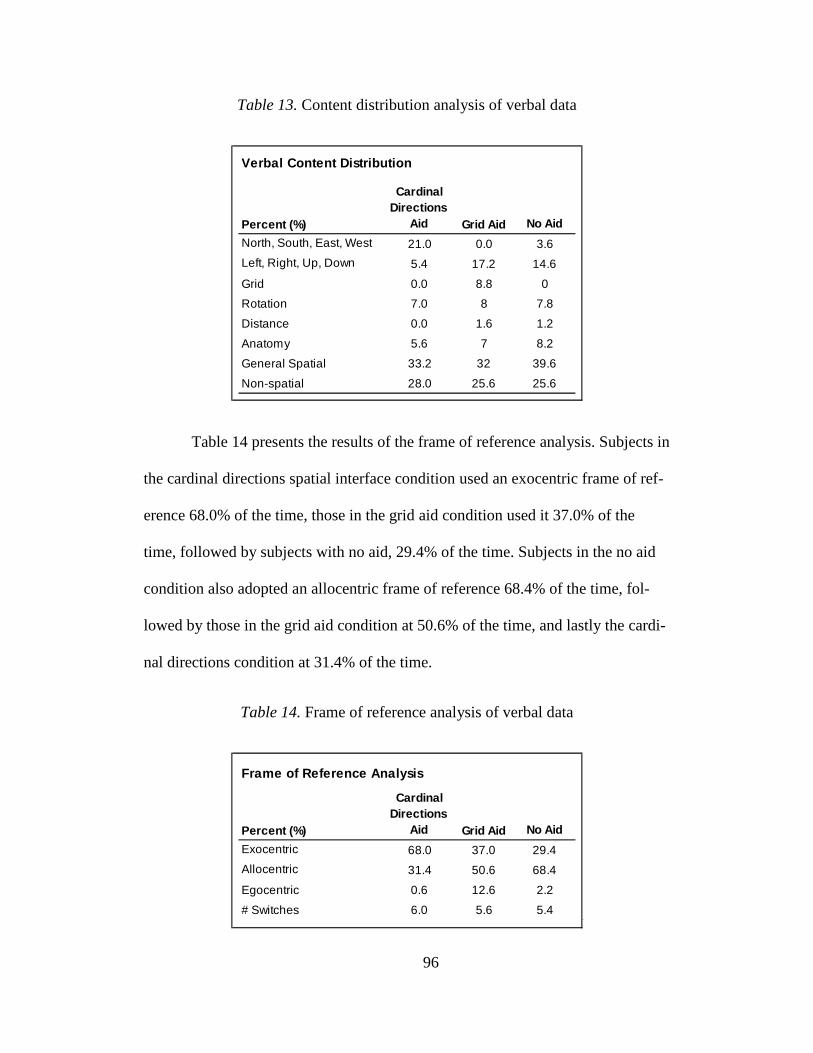
96
Table 13. Content distribution analysis of verbal data
Table 14 presents the results of the frame of reference analysis. Subjects in
the cardinal directions spatial interface condition used an exocentric frame of ref-
erence 68.0% of the time, those in the grid aid condition used it 37.0% of the
time, followed by subjects with no aid, 29.4% of the time. Subjects in the no aid
condition also adopted an allocentric frame of reference 68.4% of the time, fol-
lowed by those in the grid aid condition at 50.6% of the time, and lastly the cardi-
nal directions condition at 31.4% of the time.
Table 14. Frame of reference analysis of verbal data
Verbal Content Distribution
Percent (%)
Cardinal Directions
Aid Grid Aid No Aid
North, South, East, West 21.0 0.0 3.6
Left, Right, Up, Down 5.4 17.2 14.6
Grid 0.0 8.8 0
Rotation 7.0 8 7.8
Distance 0.0 1.6 1.2
Anatomy 5.6 7 8.2
General Spatial 33.2 32 39.6
Non-spatial 28.0 25.6 25.6
Frame of Reference Analysis
Percent (%)
Cardinal Directions
Aid Grid Aid No Aid
Exocentric 68.0 37.0 29.4
Allocentric 31.4 50.6 68.4
Egocentric 0.6 12.6 2.2
# Switches 6.0 5.6 5.4

97
5.4.6. Discussion
The results of Experiment 2 support the hypotheses that spatial interface
aids may improve task performance time and reduce the amount of communica-
tion necessary for the task. The results also support the hypothesis that subjects
with a higher spatial ability would perform better than those with a lower spatial
ability, while at the same time, the spatial interface aids have the potential to help
subjects with a lower spatial ability perform better than those with no aid at all.
The results also support the hypothesis that adopting an exocentric frame of refer-
ence yields better task performance; however, the data from Experiment 2 suggest
that perhaps the cardinal directions aid was more beneficial than the grid aid.
5.4.6.1. Spatial Abilities
One advantage of the second experiment was the collection of 2D and 3D
spatial ability scores prior to the task. By chance, subjects in the grid condition
happened to have a higher 2D spatial ability than the no aid condition. While this
may not provide any additional support for the experimental results presented in
this discussion, there was no difference between the cardinal directions and no aid
condition, leaving the ability to compare at least one of the spatial interface aid
conditions more closely without the influence of spatial skills. Having the ability
to examine performance in the context of both dimensions of spatial skills is an
interesting facet of the research, because while the task itself is a 3D task, it is
viewed within the confines of a 2D space, leaving room for influence from both
levels of spatial ability, especially depending on the role of the participant (i.e.,
“surgeon” vs. “assistant”).

98
5.4.6.2. Time
The performance time results followed the same general trend as seen in
the 90 degree camera condition of Experiment 1. In Experiment 2, however, the
fastest average performance appeared in the cardinal directions condition (Figure
23), as opposed to the grid aid condition in Experiment 1. This may have been
due to the addition of instructions provided to participants, in which subjects were
given a short overview of how the spatial aids could be utilized. Subjects in both
experimental conditions were told they could use the grid or cardinal directions to
describe the target position of the organ on the screen (i.e., “it’s in cell D2” or
“it’s in the northeast quadrant”). Subjects in the cardinal directions condition were
also given the added ability to use “north,” “south,” “east,” and “west” to describe
the direction to move the organ. Perhaps the additional functionality provided by
the cardinal directions on the screen influenced the faster time. Since spatial abili-
ties were the same, this suggests some contribution of the spatial cues that helped
improve time in this task.
There may be some explanation as to why there was no statistically sig-
nificant difference in performance time among conditions. A power analysis re-
vealed these results to have a low power, a probable cause being the small sample
size. In this type of experiment, where the task is largely dependent on novice
subject’s innate spatial and motor skills ability, it is not surprising that there was a
large variance in the data, coupled with a small sample size (due to recruiting and
time limitations) that produced non-significant results. Yet the fact that subjects
who were given a spatial aid performed faster than the control condition in two

99
independent experiments is promising for the benefits of spatial communication
aids.
5.4.6.3. Communication Volume
Subjects in the no aid condition had an average of 25 more verbal events
than those using the cardinal directions (Table 11). Knowing there was no differ-
ence in spatial ability between the no aid and cardinal directions (2D) and no dif-
ference among all three conditions (3D) suggests that the cues provided in the in-
terface had an influence on the amount of communication required to complete
the task. This result may be due to an increase in common ground between par-
ticipants. There is little common ground to be found when no spatial aid is pro-
vided, but the intent of the cardinal directions was to provide a set spatial dis-
course used for collaboration. In contrast to Experiment 1, where little change in
communication volume was seen among spatial interface aid conditions, the addi-
tion of instructions at the start of the experiment may have helped participants to
capitalize on the benefits of the spatial interface aids in pursuit of common
ground. Furthermore, the difference in communication volume between experi-
ments could be seen as a cultural factor, since non-native English performed Ex-
periment 1, whereas native English speakers who were comfortable with the lan-
guage participated in Experiment 2.
5.4.6.4. Communication Ratio
Cultural differences between subjects in the two experiments (i.e., Ex-
periment 1 conducted in France with international students and Experiment 2
conducted in the US with native English speakers) could potentially explain the

100
different communication ratio results between experiments. Or the influence of
instructions provided at the start of the experiment could have had an impact on
the ratio of communication. Additionally, the difficulty of the task may have pre-
vented more of a one-on-one collaboration, since subjects performing the task of-
ten had to concentrate more fully on the manipulation of the organ instead of fully
engaging in collaboration with the “surgeon” role.
5.4.6.5. Correlations
Perhaps the most striking results of Experiment 2 lie in the correlations
found between spatial ability and performance metrics. The correlation between
spatial ability and performance time (Table 12) suggests that subjects had to rely
more on their natural spatial ability in order to perform faster when they were not
given a communication aid. This result is similar to performance of the expert
surgeons in Experiment 1, who, through experience, have highly developed spa-
tial skills and also performed the task two to three times faster than novices. Inter-
estingly, there is more of a correlation between 2D spatial ability and time than
3D ability and time, perhaps due to the fact that the task becomes 2D when
viewed on a monitor.
These results also show the influence of the average spatial ability of a
dyad; a stronger spatial ability of one subject might not necessarily be enough to
carry the pair to high performance. Upon breaking down the correlation between
individual spatial abilities and dyad performance time, there is a stronger negative
correlation of the “surgeon” role’s 3D ability (-0.80) in the no aid condition,
whereas the strongest “assistant” correlation, also in the no aid condition, is with

101
2D ability (-0.75). These results suggest that, in the absence of any spatial inter-
face aids, “surgeons” with a higher spatial ability are better able to conceptualize
the 3D task in order to more effectively communicate with the “assistants,” and
conversely, “assistants” need to rely on their higher spatial abilities in order to
translate a 3D physical task into a 2D visual task. In both the cardinal directions
and grid conditions, these correlations are less apparent because the navigation
tools provided in the interface may remove some of the reliance on innate spatial
ability.
The results also show interesting correlations between spatial ability and
the volume of communication. The significantly strong negative correlation be-
tween 3D ability and the volume of communication in the no aid condition sug-
gests that one’s 3D ability has an influence on the way in which the task is verbal-
ized. In medicine, where miscommunication can lead to patient harm, it is possi-
ble that a higher volume of communication may translate accordingly to an in-
creased risk of miscommunication. Furthermore, because the effect was seen in
the 3D condition, there is increased support for the requirement for a concise spa-
tial language that can be expressed in three dimensions yet applied to two dimen-
sions, as in the case of minimally invasive surgery.
The relationships between individual spatial ability and individual com-
munication volume suggest a possible benefit of the grid aid to subjects with a
higher natural spatial ability. Here, subjects in the “surgeon” role had a signifi-
cantly strong negative correlation (-0.91*), potentially suggesting the role played
by the grid aid in positively affecting the quality of communication for those with

102
a natural ability. Conversely, those with a low spatial skill set need more verbali-
zation in order to explain the 2D rendering of the object in space within the con-
fines of the grid. Additionally, subjects in the “assistant” role had a larger positive
correlation between both 2D (0.83) and 3D (0.56) spatial ability and communica-
tion volume, suggesting that the grid could possibly move the “assistant” into
more of a collaborative position. Alternatively, it could be explained by the “as-
sistant” needing to supplement the reduced communication with the surgeon in an
effort to establish rapport.
The significantly strong positive correlation between time and communi-
cation in the cardinal directions condition supports the idea that the cardinal direc-
tions are capable of both improving performance in a collaborative task as well as
promoting common ground. Subjects in this condition are able to accomplish the
task faster yet with fewer verbal exchanges. Not surprisingly, the cardinal direc-
tions condition yielded both the fastest average time performance as well as the
lowest volume of communication. Considering that subjects in the cardinal direc-
tions condition had the same spatial abilities as those in both the grid and the no
aid conditions, this correlation presents a compelling argument for the use of the
cardinal directions. Furthermore, because this particular correlation result is inde-
pendent of spatial ability, it suggests that the cardinal directions may be more uni-
versal as a spatial navigation aid (i.e., as opposed to the grid, which as just dis-
cussed may be more beneficial to those with a higher spatial ability).

103
5.4.6.6. Content Distribution
The behavior of subjects in the no aid condition, who had the highest per-
centage of general spatial discourse, could potentially be explained by the smaller
toolset they had to work with necessitating more generic dialogue, such as
“more” or “turn it” instead of “turn it to face northeast” or “more into cell C1.”
Interestingly, one dyad in the no aid condition self-established use of “north,”
“south,” “east,” and “west” in order to describe movement of the object as they
felt that “left,” “right,” “up,” and “down” were confusing due to the visual-motor
misalignment. Accordingly, because this dyad made an effort to establish com-
mon ground in their spatial discourse, they performed the fastest out of all sub-
jects in the no aid condition and, further, had one of the fastest times out of the
whole subject population. Conversely, another group in the no aid condition who
happened to perform the slowest also engaged in the largest volume of non-spatial
related discourse during the task and utilized the spatial descriptors “left,” “right,”
“up,” and “down” the least. The combination of these two factors, coupled with a
lower spatial ability of the dyad, suggests that it could be difficult to establish
common ground.
As to be expected, subjects in the cardinal directions condition made use
of the cardinal directions more than subjects in the other two conditions, and
likewise with the grid aid. In the cardinal condition, the slowest performing group
also happened to have the highest volume of communication as well as the largest
percentage of non-spatial discourse. Dyads in the grid interface condition actually
used the terms “left,” “right,” “up,” and “down” the most in the experiment
104
(17.2%). A similar trend was observed in Experiment 1, where subjects who used
the grid also used “left…” in order to supplement their descriptions of moving the
object. Upon examining individual dyads in the grid condition, the pair that made
reference to the grid the most often also happened to perform the fastest in the
grid condition, and the pair that made reference to the grid the least often also
happened to perform the slowest in the grid condition. This result provides sup-
port for the grid as a useful tool in positively affecting spatial communication in a
collaboration task.
5.4.6.7. Frame of Reference
Two people who are collaborating must often adopt a common frame of
reference in order to establish common ground in their collaboration, and an exo-
centric view point helps to eliminate inconsistencies in their individual views of
the task. Therefore it is not surprising that both the cardinal directions and grid
conditions utilized an exocentric frame of reference the most (Table 14), and
similarly had the fastest times and lowest volumes of communication.
In fact, the dyad that used an exocentric reference frame the most in the
entire experiment also happened to perform the fastest in the entire experiment.
These subjects were given the cardinal directions aid, and interestingly, the sub-
ject in the “surgeon” role had a much lower spatial ability than the subject per-
forming the task. While it might normally have been difficult for the “surgeon”
role to plan and explain how to manipulate the organ due to the lower spatial abil-
ity, adopting an exocentric reference may have provided the key to establishing
common ground, allowing for the “assistant” to successfully perform the task.

105
Several dyads in the no aid condition attempted to convey an exocentric,
local frame of reference by using the descriptors “left on the screen,” “up on the
screen,” etc., a strategy that seemed to immediately eliminate confusion in deter-
mining if left meant a left movement by the “assistant” role or left in the camera
view. Therefore, these further results suggest that an exocentric frame of refer-
ence can help establish common ground.
Subjects in the grid aid and no aid conditions utilized an allocentric refer-
ence frame the most. In the absence of other common cues, providing spatial de-
scriptors in terms of the current position of the liver may have helped to establish
common ground because both subjects had the same view of the object as shown
on the monitors. In the grid condition, it was previously discussed that references
to the grid itself are supplemented with “left”, “right…” descriptors to aid in final
positioning and orientation of the object, helping to explain a potential cause of
the higher usage of allocentric in the grid condition.
In the grid condition, one dyad partially adopted an egocentric frame of
reference, and that dyad also referenced the grid the least, had the highest volume
of communication, and the slowest task time. The performance of this group,
then, does not appear to provide support for an egocentric reference frame as a
promoter of common ground in communication. On the other hand, the group that
both adopted the most exocentric references out of the grid condition, and refer-
enced the grid the most, also happened to perform the fastest in that condition.

106
Subjects in all conditions switched between reference frames throughout
the experiment. There did not seem to be any large differences in the number of
switches. However, the choice of reference frame depending on the type of
movement or progress of the task is an interesting subject. For example, subjects
may use an exocentric reference frame to better convey larger scale movements
but an allocentric reference frame to describe finer grained movements related to
final position and orientation of the organ. While some of the transcribed and
coded communication data seem to suggest this idea, better instrumentation and
timeline analysis would need to be conducted to examine this relationship more
closely.
5.4.6.8. Communication Strategies
As in Experiment 1, dyads in Experiment 2 adopted a wide variety of
communication strategies that proved both successful and unsuccessful. In Ex-
periment 2, however, subjects were allowed to perform one practice trial before
commencing the three official timed trials. During the practice trial, many dyads
were able to establish strategies that they seemed to carry through the rest of the
experiment. Reviewing the video logs and transcriptions also revealed that sub-
jects in the “surgeon” role became truly engaged in the success of the “assistant”
subject. The surgeons wanted the “assistant” to perform well and frequently modi-
fied the style of instructions if the “assistant” was struggling or not progressing at
an acceptable rate.
Strategies included providing an initial overview of the final target loca-
tion before giving more fine-grained instructions, for example: “The final location

is in the southwest quadrant,” or simply dictatin
ment instructions: “It needs to go up and to the right.” While progressive instru
tions are beneficial in reducing mental load on a person performing a complex
task, using only progressives could potentially reduce the amount
ground related to the overall task goal.
Figure 24. Two strategies for reaching the target. Left: Long range move of liver
to target area. Right: Fine
Subjects also differed by the order in which they chose to orient/rotate the
liver and position it. For example, some dyads chose to orient the liver first (into
the correct rotation) and then move it to the target while correctly oriented: “A
right, let’s start by spinning it 180 degrees”
with the dyad performing the
box task. This type of strategy did not always prove successful, because ofte
times the liver moved out of p
However, the “assistant” generally remembered the initial rotation, and was ther
fore able to rotate it with less assistance
target.
107
is in the southwest quadrant,” or simply dictating a series of progressive mov
ment instructions: “It needs to go up and to the right.” While progressive instru
tions are beneficial in reducing mental load on a person performing a complex
task, using only progressives could potentially reduce the amount of common
ground related to the overall task goal.
Two strategies for reaching the target. Left: Long range move of liver
to target area. Right: Fine-grained rotation and orientation into final position
differed by the order in which they chose to orient/rotate the
For example, some dyads chose to orient the liver first (into
the correct rotation) and then move it to the target while correctly oriented: “A
nning it 180 degrees”. This strategy is shown in Figure
with the dyad performing the right-hand box task first, followed by the left
type of strategy did not always prove successful, because ofte
moved out of place while performing the longer range movements
However, the “assistant” generally remembered the initial rotation, and was ther
fore able to rotate it with less assistance from the “surgeon” once near the final
g a series of progressive move-
ment instructions: “It needs to go up and to the right.” While progressive instruc-
tions are beneficial in reducing mental load on a person performing a complex
of common
Two strategies for reaching the target. Left: Long range move of liver
grained rotation and orientation into final position
differed by the order in which they chose to orient/rotate the
For example, some dyads chose to orient the liver first (into
the correct rotation) and then move it to the target while correctly oriented: “Al-
Figure 24,
left-hand
type of strategy did not always prove successful, because often-
lace while performing the longer range movements.
However, the “assistant” generally remembered the initial rotation, and was there-
once near the final

108
An opposing strategy was to complete the long range movements first and
then tackle more fine-grained movements such as obtaining the correct rotation:
“So basically we’re going to move it towards the northeast region, not all the way
to the corner but towards that region.” In Figure 24, subjects adopting this strat-
egy executed the left hand box action first, followed by the right hand box. Such a
strategy seemed to prove successful because both subjects had common knowl-
edge of where the target was from the start of the trial and were able to save de-
tailed positioning movements for last, eliminating the scenario where the liver
would fall from the initial rotation/orientation during long range movements.
The initial strategy was often established by the subject in the “surgeon”
role. However, it seemed that the spatial abilities of both subjects influenced
which strategy dominated over the course of the experiment. Some pairs were
more evenly matched, while other pairs had a greater difference in spatial ability
that either favored the “surgeon” role or the “assistant”. When the spatial ability
of the “surgeon” role was higher, his or her strategy seemed to emerge early on as
the dominant strategy. The “surgeon’s” ability was 30 points higher than the “as-
sistant” in one grid aid dyad. However, the pair had one of the fastest performance
times, perhaps due to both the benefit of the grid aid and the keen spatial aware-
ness of the “surgeon”, which could have allowed for a clear and understandable
strategy.
On the other hand, in another dyad in the grid condition the “assistant’s”
2D ability was almost 20 points higher. The “surgeon” delivered a series of small
progressive instructions from an egocentric reference frame, and did not appear to

109
give an overview of the final target position/ orientation. The dyad had some of
the slowest trial times for the entire experiment, until the third trial, when the “as-
sistant” (with the higher spatial ability) began leading the collaboration by asking
pointed, relevant spatial questions to draw the correct information from the “sur-
geon” role. With the new strategy, they were able to complete the third trial in
half the time than the average of the other two trials.
5.4.7. Limitations
There were several limitations present in Experiment 2. Originally, it was
thought that Experiment 2 would remove enough potentially confounding factors
(e.g., language barriers) to provide significant outcomes; however, the power
analysis revealed that larger samples size was needed. Nevertheless, it was still
possible to examine individual dyads that performed on the higher and lower end
of the spectrum in order to draw preliminary suggestions about the benefits of the
spatial aids.
Because of limiting factors in experiment time and recruiting of partici-
pants who were not paid, it was difficult to administer the spatial test in advance
in order to create well-balanced groups. By chance, the grid aid and no aid groups
did not have the same 2D spatial ability, but because the cardinal directions group
performed the best overall and had the same ability as both grid and no aid, it was
still possible to examine the benefit of the spatial aids without spatial ability as a
factor. Additionally, the task itself proved to be very difficult, especially for nov-
ices and even despite increased training via a practice trial.

110
5.5. Summary
Overall, Experiments 1 and 2 examined spatial aids for communication in
a collaborative task has suggested the benefit of either a cardinal directions or grid
aid as opposed to that of no aid at all. Experiment 1 revealed a significant differ-
ence in performance time between the 0 and 90 degree camera rotation condi-
tions. It also showed that experts, who may benefit from experience and better
developed spatial abilities, performed the experimental task two to three times
faster than novices, depending on camera rotation. In Experiment 1, subjects who
did not have a spatial aid performed the slowest, while subjects with a cardinal
directions aid or grid aid performed the fastest. The benefit of spatial aids was es-
pecially seen when there was a misalignment of the camera and the task space, as
in the 90 degree camera condition. No statistically significant difference in per-
formance time or volume of communication when using the aids was found; how-
ever, that may be due to the low power from a small sample size as well as a large
variance in novice subjects’ innate spatial abilities.
Building upon the results from Experiment 1, Experiment 2 sought to ex-
amine the role that natural spatial ability plays in the task by administering a spa-
tial skills test to subjects. Despite having no difference in spatial ability between
subjects in each of the experimental conditions (except for grid aid versus no aid
in the 2D spatial ability), subjects who were given the grid aid and cardinal direc-
tions aid performed faster and communicated less than those with no aid at all.
The trends that suggest faster performance time with the spatial aids and changes
in communication patterns are present in both experiments, which were run inde-

111
pendently in different countries. Furthermore, the presence of statistically signifi-
cant correlations between spatial ability, time, and communication in Experiment
2 help to suggest the benefit of spatial communication aids on collaboration. Both
the cardinal directions and the grid aid may act as promoters of common ground
in the task by providing subjects with a shared language. Additionally, providing
instructions on use of the spatial aids in Experiment 2 led to a 100% adoption rate
of the aids as compared to Experiment 1, where several groups of subjects ignored
the aids.
There are several potential applications of the results of this controlled
study. In terms of requirements analysis, the results have made a preliminary case
for the need for a shared language in surgery. That could transfer into the design
of the technology itself, where the lessons learned about spatial communication
aids could be used to design similar spatial aids that are integrated seamlessly into
the robotic system. In order to encourage use of the spatial aid and promote
awareness, training protocols would need to be redesigned such that team mem-
bers learn how to use the aids from their initial encounter with the technology,
and emphasized as a best practice.
5.6. Suggestions for Future Work
A future study could further compare the cardinal directions aid to the grid
aid, or even investigate other types of spatial aids. Increasing the sample size, in-
cluding the expert surgeon population, could potentially lead to more concrete
results. Making use of any automated data capture systems or creating a program

112
to facilitate coding of the data would certainly make a larger sample size more
feasible. In the future, pre-screening participants for spatial ability would be bene-
ficial, and could provide for some interesting experimental conditions. A future
study may also consider reducing the difficulty of the task, while still maintaining
the incongruence between participant task spaces, to allow for full benefit of the
spatial aids. Alternatively, perhaps providing several practice rounds instead of
just one would allow for a better adjustment to the camera misalignment and for
dyads to better establish a consistent communication strategy.
6. Conclusion
The results of this research have provided an opportunity to analyze a
complex medical environment from a human factors context. Robotic surgery can
be considered a socio-technical system, where surgeons and nurses come together
with common goals of caring for a patient, making use of technology along the
way, and relying on teamwork and communication to accomplish their tasks.
In part one (Field Study), observations of robotic surgeries in the US and
in France and subsequent communication analysis suggested a layered approach
to analyzing a socio-technical system. The results suggested that inexperience can
affect teams in terms of time spent learning how to use a technology, and also af-
fect their communication patterns. There may also be organizational and cultural
factors that affect the adoption of robotic surgery in different hospitals as well as
countries. Designers need to examine the data and take these factors into account
when building the technology and establishing training programs.

113
Part two (Experiments 1 and 2) examined the problem of communicating
spatial information during robotic surgery due to viewing perspective differences,
a scenario uncovered as part of the field analysis. The results suggest that spatial
interface aids can possibly be beneficial to communication in a collaborative task
related to robotic surgery. In such an environment, where face-to-face communi-
cation is limited, yet the surgical team relies upon communication in order to pro-
gress the surgery and ensure safety of the patient, finding common ground is es-
pecially important. The results suggest that utilizing a common, exocentric set of
spatial language descriptors such as the cardinal directions north, south, east, and
west can improve task time and promote a balance in communication between dy-
ads. Using a navigation grid has the potential to be more effective because it not
only provided shared language, but could be used to jointly establish a vision of
where to work. Overlaying these aids on the robotic surgical system monitors
provides a seamless reminder of communication while performing the task.
As technology integration into many facets of healthcare gains momen-
tum, there will inevitably be challenges in terms of adoption and training. By
studying the nature of these changes, healthcare providers can reap the benefits
provided by technology while still maintaining a primary focus on patient care.

114
APPENDIX A: US SURGERY TRANSCRIPTIONS
Case 1:
TIME EVENT ORIGIN-ATOR
RECIP- IENT
CODE
8:08 S DISCUSSING STRATEGY S RST P3 8:11 A ASKS S ABOUT ANTIBIODICS A S P5 8:11 A ASKS TEAM TO GET ANTIBIODICS, DOESN’T HAVE ACCESS A S P5 8:11 S VOLUNTEERS TO WATCH PATIENT WHILE A GETS MEDS S A P5 8:13 S ASKS CN HER OPINION OF AIR MATTRESS, INTERESTED IN
TRYING IT S CN O
8:15 CN READS MEDS AND EXPIRATION DATE CN A P5 8:28 DURING INSUFFLATION, CONFIRM CO2 SETTINGS W CN S CN E5 8:29 S CHECK PT STATUS WITH A S A P6 8:33 S TEACHING RST S RST P3 8:33 S NOTES PROBLEM WITH LAP. CAMERA LENS - CLEANING
LENS S SN E1
8:36 S ASKS IF TEAM HAVE ALL MET EACH OTHER S O O 8:41 S TEACHING PORT PLACEMENT STRATEGY S RST P3 8:41 S CALLS FOR TOOL PREP, READY TO DOCK ROBOT S SN E5 8:43 CN DRIVING ROBOT TO TABLE, ASK GUIDANCE FROM PA CN PA E5 8:43 YELL TO STOP WHEN ALMOST AT PT LEGS PA CN E5 8:44 CN ASKS S IF NEED CONSOLE PEDAL ADJUSTMENT CN S E2 8:44 PA DIRECTING PLACEMENT OF PATIENT CART PA CN E5 8:46 INTUITIVE REP DIRECTING ARM PLACEMENT O SN E2 8:48 S DISCUSSING ROBOTIC STRATEGY WITH RST S RST P3 8:55 S DIRECTING CAMERA POSITIONING S SN E2 8:56 S ASKS SN TO ADJUST A TOOL S SN E2 8:58 INTUITIVE REP TEACHING/DISCUSSING W/ S O S P3 9:02 S GRUFFLY ASKS MS TO MANIPULATE OVARY S MS P2 9:03 S COMMUNICATING TO PA REGARDING PLACEMENT OF
ARMS S PA E2
9:03 S CUTTING, STATES HAVING A SCISSOR PROBLEM, STAFF READJUSTED ARM
S PA E2
9:04 S SEEMS TO THINK TEAM IS SLOW S O O 9:06 S GUIDING RST AT CONSOLE S RST P4 9:09 PA TRAINING SNT, WORKING THROUGH PROCEDURE PA ST P3 9:10 PA YELLS SHE CAN HOLD ORGAN TO S PA S P2 9:10 S, INTUITIVE REP TALKING NEAR CONSOL S O O 9:11 PA ASKS FOR MORE VOLUME ON SPEAKER PA RST E2 9:12 PA YELLING STATUS ACROSS ROOM PA RST P6 9:18 S GIVES RST TECHNIQUE SUGGESTION S RST P3 9:20 PA STILL CANNOT HEAR CLEARLY, FIXING MICROPHONE PA RST E3 9:23 S REQUESTING BETTER HOLD OF UTERUS SO BLADDER CAN
BE VISUALIZED S MS P2
9:28 CONFUSION BETWEEN ALL ABOUT TASK S PA P3 9:29 S ASKS RST IF OK TO LEAVE ROOM S RST O 9:35 CN ASKED FOR NON-ESSENTIAL CONVERSATION TO STOP,
HARD TO HEAR CN O O
9:35 CN TALKING TO S ABOUT ANOTHER CASE CN S O 9:35 PA HELPS MS ADJUST UTERUS, S YELLING S PA P2 9:36 PA STATES SOMETHING ABOUT ABDOMEN MOVING TO A PA A P5 9:40 CN CHECKING WITH RST ABOUT WHICH OVARY WILL BE RE-
MOVED CN RST P4
9:40 RST ASKS FOR UTERUS REMOVAL RST PA P2 9:41 PA TEACHING ON UTERUS REMOVAL PA MS P2 9:45 COORDINATING LIGHTS OVER TABLE - LIGHTS COLLIDING PA CN E2 9:45 S CONFIRMS PLAN WITH RST S RST P3 9:46 PA CONFIRMS SPECIMEN WITH CN PA CN P6 9:48 S ASKS FOR TUBE HELD, SHE IS BUSY, ASKS A FEW TIMES S PA P2 9:50 S NEEDS SCREEN WRITING REMOVED S CN E2 9:50 S ASKS FOR TUBE HELD AGAIN S PA P2

115
9:50 S USING TELESTRATOR TO MARK WHERE TO CAUTERIZE OVERY WITH CYST
S RST P4
9:53 S ASKS PA TO REMOVE CYST S PA P2 9:54 PA STATES S NOT LISTENING PA S O 9:54 S ASKING FOR TOOL CHANGE FOR RST S SN E1 9:55 PA ASKING WHICH TOOL TO SWITCH PA S E1 9:55 S TEACHING RST S RST P3 9:56 SN NOT SURE WHERE TO PUT TOOL BACK IN SN S E1 9:58 S INSTRUCTING INTERNAL SUTURING TO RST S RST P3
10:04 S DRAWING ON SCREEN AT SPLEEN, YELLING TO RST S RST P4 10:06 S INSTRUCTING TO RST S RST P4 10:07 S SUGGESTS PLAN, COORDINATES WITH PA S PA P3 10:07 S TELLING RST TO TAKE HIS TIME S RST P3 10:12 CN GOES TO HELP PA IN TOOL CHANGE PROBLEM CN PA E4 10:12 S DISCUSSING ANOTHER CASE WITH CN S CN O 10:12 S AT CONSOLE HELPING RST S RST P3 10:14 S ASKS FOR GORTEX S CN E1 10:15 PA CONFIRMS STEPS WITH S PA S P3 10:17 S GUIDING FINAL CLOSURE S RST P3 10:19 S CONFIRMS NEXT PATIENT WITH CN S CN O 10:19 S CONFIRMS TOOL CHANGE WITH SN S SN E1 10:20 S CORRECTS RST - USING WRONG HAND IN SUTURING S RST P3 10:28 S ASKS FOR TOOL CHANGE S PA E1 10:28 S UNCLEAR HOW TO MOVE INSTRUMENT TO BASE POSITION
- TOOL NOT WORKING VERY WELL, BUT DOES NOT NEED REPLACEMENT AT THIS TIME
S PA E4
10:40 S STATES DONE WITH ROBOT S PA P3 10:43 S ASKS RST TO SCRUB IN AND HELP CLOSE PATIENT S RST P3 10:49 CN ASKS S ABOUT DOING ANOTHER CASE NEXT WEEK CN S O 10:50 CN COORDINATING WITH S ABOUT SCHEDULING CN S O 10:53 PA ASKS FOR ROOM LIGHTS PA CN E2 10:57 RST SHOWING MS HOW TO DO SUTURES RST MS P3 11:03 RST ASKS A ABOUT PT FLUIDS RST A P5
Case 2:
TIME EVENT ORIGIN-ATOR
RECIP-IENT
CODE
8:08 S DISCUSSING STRATEGY S RST P3 8:11 A ASKS S ABOUT ANTIBIODICS A S P5 8:11 A ASKS TEAM TO GET ANTIBIODICS, DOESN’T HAVE ACCESS A S P5 8:11 S VOLUNTEERS TO WATCH PATIENT WHILE A GETS MEDS S A P5 8:13 S ASKS CN HER OPINION OF AIR MATTRESS, INTERESTED IN
TRYING IT S CN O
8:15 CN READS MEDS AND EXPIRATION DATE CN A P5 8:28 DURING INSUFFLATION, CONFIRM CO2 SETTINGS W CN S CN E5 8:29 S CHECK PT STATUS WITH A S A P6 8:33 S TEACHING RST S RST P3 8:33 S NOTES PROBLEM WITH LAP. CAMERA LENS - CLEANING
LENS S SN E1
8:36 S ASKS IF TEAM HAVE ALL MET EACH OTHER S O O 8:41 S TEACHING PORT PLACEMENT STRATEGY S RST P3 8:41 S CALLS FOR TOOL PREP, READY TO DOCK ROBOT S SN E5 8:43 CN DRIVING ROBOT TO TABLE, ASK GUIDANCE FROM PA CN PA E5 8:43 YELL TO STOP WHEN ALMOST AT PT LEGS PA CN E5 8:44 CN ASKS S IF NEED CONSOLE PEDAL ADJUSTMENT CN S E2 8:44 PA DIRECTING PLACEMENT OF PATIENT CART PA CN E5 8:46 INTUITIVE REP DIRECTING ARM PLACEMENT O SN E2 8:48 S DISCUSSING ROBOTIC STRATEGY WITH RST S RST P3 8:55 S DIRECTING CAMERA POSITIONING S SN E2 8:56 S ASKS SN TO ADJUST A TOOL S SN E2

116
8:58 INTUITIVE REP TEACHING/DISCUSSING W/ S O S P3 9:02 S GRUFFLY ASKS MS TO MANIPULATE OVARY S MS P2 9:03 S COMMUNICATING TO PA REGARDING PLACEMENT OF ARMS S PA E2 9:03 S CUTTING, STATES HAVING A SCISSOR PROBLEM, STAFF
READJUSTED ARM S PA E2
9:04 S SEEMS TO THINK TEAM IS SLOW S O O 9:06 S GUIDING RST AT CONSOLE S RST P4 9:09 PA TRAINING SNT, WORKING THROUGH PROCEDURE PA ST P3 9:10 PA YELLS SHE CAN HOLD ORGAN TO S PA S P2 9:10 S, INTUITIVE REP TALKING NEAR CONSOL S O O 9:11 PA ASKS FOR MORE VOLUME ON SPEAKER PA RST E2 9:12 PA YELLING STATUS ACROSS ROOM PA RST P6 9:18 S GIVES RST TECHNIQUE SUGGESTION S RST P3 9:20 PA STILL CANNOT HEAR CLEARLY, FIXING MICROPHONE PA RST E3 9:23 S REQUESTING BETTER HOLD OF UTERUS SO BLADDER CAN
BE VISUALIZED S MS P2
9:28 CONFUSION BETWEEN ALL ABOUT TASK S PA P3 9:29 S ASKS RST IF OK TO LEAVE ROOM S RST O 9:35 CN ASKED FOR NON-ESSENTIAL CONVERSATION TO STOP,
HARD TO HEAR CN O O
9:35 CN TALKING TO S ABOUT ANOTHER CASE CN S O 9:35 PA HELPS MS ADJUST UTERUS, S YELLING S PA P2 9:36 PA STATES SOMETHING ABOUT ABDOMEN MOVING TO A PA A P5 9:40 CN CHECKING WITH RST ABOUT WHICH OVARY WILL BE RE-
MOVED CN RST P4
9:40 RST ASKS FOR UTERUS REMOVAL RST PA P2 9:41 PA TEACHING ON UTERUS REMOVAL PA MS P2 9:45 COORDINATING LIGHTS OVER TABLE - LIGHTS COLLIDING PA CN E2 9:45 S CONFIRMS PLAN WITH RST S RST P3 9:46 PA CONFIRMS SPECIMEN WITH CN PA CN P6 9:48 S ASKS FOR TUBE HELD, SHE IS BUSY, ASKS A FEW TIMES S PA P2 9:50 S NEEDS SCREEN WRITING REMOVED S CN E2 9:50 S ASKS FOR TUBE HELD AGAIN S PA P2 9:50 S USING TELESTRATOR TO MARK WHERE TO CAUTERIZE OV-
ERY WITH CYST S RST P4
9:53 S ASKS PA TO REMOVE CYST S PA P2 9:54 PA STATES S NOT LISTENING PA S O 9:54 S ASKING FOR TOOL CHANGE FOR RST S SN E1 9:55 PA ASKING WHICH TOOL TO SWITCH PA S E1 9:55 S TEACHING RST S RST P3 9:56 SN NOT SURE WHERE TO PUT TOOL BACK IN SN S E1 9:58 S INSTRUCTING INTERNAL SUTURING TO RST S RST P3
10:04 S DRAWING ON SCREEN AT SPLEEN, YELLING TO RST S RST P4 10:06 S INSTRUCTING TO RST S RST P4 10:07 S SUGGESTS PLAN, COORDINATES WITH PA S PA P3 10:07 S TELLING RST TO TAKE HIS TIME S RST P3 10:12 CN GOES TO HELP PA IN TOOL CHANGE PROBLEM CN PA E4 10:12 S DISCUSSING ANOTHER CASE WITH CN S CN O 10:12 S AT CONSOLE HELPING RST S RST P3 10:14 S ASKS FOR GORTEX S CN E1 10:15 PA CONFIRMS STEPS WITH S PA S P3 10:17 S GUIDING FINAL CLOSURE S RST P3 10:19 S CONFIRMS NEXT PATIENT WITH CN S CN O 10:19 S CONFIRMS TOOL CHANGE WITH SN S SN E1 10:20 S CORRECTS RST - USING WRONG HAND IN SUTURING S RST P3 10:28 S ASKS FOR TOOL CHANGE S PA E1 10:28 S UNCLEAR HOW TO MOVE INSTRUMENT TO BASE POSITION -
TOOL NOT WORKING VERY WELL, BUT DOES NOT NEED RE-PLACEMENT AT THIS TIME
S PA E4
10:40 S STATES DONE WITH ROBOT S PA P3 10:43 S ASKS RST TO SCRUB IN AND HELP CLOSE PATIENT S RST P3 10:49 CN ASKS S ABOUT DOING ANOTHER CASE NEXT WEEK CN S O 10:50 CN COORDINATING WITH S ABOUT SCHEDULING CN S O 10:53 PA ASKS FOR ROOM LIGHTS PA CN E2 10:57 RST SHOWING MS HOW TO DO SUTURES RST MS P3 11:03 RST ASKS A ABOUT PT FLUIDS RST A P5

117
APPENDIX B: FRENCH SURGERY TRANSCRIPTIONS
Case 1, Prep:
Time Who To Who Text VE
Code
Bow-ers Code
0:39 surg1 All surgeon informs team about EMN researchers in OR O g 1:07 surg1 rep surgeon explains to rep O g
2:20 surg1 rep surgeon explains robotic setup and planned approach to table (from left) P3 e
2:40 surg1 Other surg explains anatomy of case to amine O g 4:24 surg1 nurse surgeon jokes be careful not to break $2m davinci! O g 4:51 nurse surg1 laughing about surgeon's joke O g 4:52 surg1 rep greets rep, glad he is there O g
5:09 surg1 rep surg explains anatomy of case and plan to rep: right external illiac - must locate it now so rep can help with the placement
P4 e
5:21 surg1 rep
surg points to abdomen, says normally its here, will enter from this spot to clean out - comparing to another case rep may be familiar with. Showing the angle of approach, asking if it is a good angle. Wants to use all four arms. Because we need to centralize the tools in one area, even if we are not sure, and surg states he is trying to think about all four arms
P3 e
5:49 surg1 rep explains he will place camera on the median, maybe higher because P4 a
5:55 rep surg1 maybe higher, yes, confirms higher P4 d 6:05 rep surg1 ideally, we have to be between 15-20cm <something> P4 d
6:16 surg2 surg1 surg2 mentions the patient was already opened - with other operations, and need to avoid the last operative area, need to be careful, she was "undermined"
P6 e
6:16 All All team laughing about undermining O g 6:24 surg1 surg2 mentions it’s a very difficult case, and the patient knows it too P6 f
6:30 rep surg1 explain to surg need 15-20cm between instruments, joking a little P3 d
6:53 surg1 surg2 explains to surg2, they cant make a mistake, want to be in a certain spot in the body
P4 e
6:55 surg1 rep asks rep if they need t be so high P4 a 7:02 rep surg1 states they can go from 20-25cm inside the body P4 d 7:05 surg1 rep says ok, asks if can place the camera here <points to body> P4 a 7:06 rep surg1 yes P4 c 7:11 surg2 surg1 points to another area, prefers to place camera there P4 a 7:11 surg1 rep but the tools are long, and the woman is not so fat P4 d
7:18 surg1 rep talking about the pressure in the abdomen, will not put a lot (insufflation) P3 g
7:24 surg1 rep talking about trocar P3 g 7:31 surg1 anesth asks anesth if placed the <something> for the patient P5 a 7:41 surg1 rep asks to place 2 trocars on 1 side and 1 on the other P4 a 7:42 rep surg1 says absolutely P4 c 7:53 surg1 rep not sure, we will see if we need an assistant port P3 a 7:58 surg2 surg1 said something <?>, related to assistant port P3 d 8:02 rep surg1 responded that there are already 3 there P3 d 8:02 nurse nurse shit! E3 a 8:03 nurse nurse I will go get another one E3 d 8:05 nurse nurse yes, go get another one for the camera arm E3 b
8:32 surg1 surg2,rep says, lets come back to our case O g
8:39 surg1 rep this is where port 1 will go, because here <in this other spot> we will place 2 P4 a
8:40 rep surg1 yes, its ok P4 c 8:40 surg1 rep should they be separated by at least 5-6cm? P4 a
rep surg1 yes, remember it will change when we insufflate P3 d 8:56 surg1 rep we will put one here and here, not along the same line? P4 a
rep surg1 yes, exactly P4 c
surg1 rep we will put one here laterally, and then place another one P4 a

118
here? 9:09 rep surg1 yes P4 c
9:12 surg1 rep asks if is should be like this <indicates on body>, because if I put it there, it will be along the same line P4 a
9:15 rep surg1 yes P4 c 9:16 surg1 rep <pointing> there? P4 a 9:20 rep surg1 yes, there is not so bad P4 d 9:28 surg1 rep now the ports are shifted so not along the same line P4 a 9:32 rep surg1 they are shifted, asks if instruments will be constrained P4 a
9:36 surg1 rep Doesn’t answer, then says where he will put the last port (on other side), equivalent to the other on, but on the other side P4 a
9:41 surg1 rep the other thing we can do because we are there far, we can put this one there <indicates> and the other one there <indi-cates> and because
P4 a
9:50 rep surg1 you will be better if you put it shifted like this <indicates>, the trocar for the 3rd arm be lateral, the third one must always be more lateral than the first one
P4 d
10:08 surg1 rep ok, so we will put the other one here <indicates>, here we are at 5cm, and we can put the third one here <indicates> P4 a
10:34 rep surg1 angle of arm 3 is more horizontal, so make it more lateral P4 d 10:38 surg1 rep better to get it at the external part P4 d
11:00 surg1 rep,nu
rse
and then we can put it…so what we will do: we prepared the patient for the first step, and for the second step we place the trocars, the third step is to verify with the camera that there is not a lot of adhesion (to nurse and b., telling the plan and waiting for confirmation). so if we do that, we will place the davinci trocars using the cutting tool
P3 e
nurse surg1 ok,<something> discussing what surg said, asks question P3 a
surg1 nurse on the first time, yes P3 d
nurse surg1 ok P3 c 11:37 surg1 nurse once the port placement is done, we will dock the robot P3 a
nurse surg1 ok P3 c 11:48 nurse surg1 asking which arm will you put in this port, the third one? P3 a
11:49 surg1 surg1 no, we'll put the trocar there, and using the camera, we'll check the position of all the davinci trocars P3 d
11:51 surg1 nurse before docking, we will check adhesions, and then if there is adhesiolyse, and if we have an adhesiolyse to make with the scissors, and once it is done, we dock
P3 a
12:00 nurse surg1
do we need the trocar for what were talking about before, no, if we take out the gonglion (tumor tissue). Asking about add-ing another hole for removing the mass later on. Oh yeah, an assistant port. Asked the assistant,
P3 a
12:14 surg1 nurse he said, yes, we will put it there P3 d 12:17 nurse surg1 she said yes, we were talking about that this morning P3 d
surg1 nurse when we will finish P3 a 12:40 nurse nurse asking about tape for plastic over the robot E5 a
nurse nurse asking about how to position the patient P3 a
13:30 nurse nurse we will put the table down first E2 d
nurse nurse give me two minutes O d
nurse nurse tell me when you are ready O b
13:40 nurse nurse asks if the patient should be moved down, will we move the patient down using the sheet, or only the patient P3 a
nurse nurse we will move only the patient b/c everything else is already
set up P3 d
nurse nurse asks about tape on robot arms E5 a
13:51 nurse nurse yes E5 c 14:04 nurse nurse ready to move the patient down using the sheet P3 b 14:13 nurse nurse give me two minutes to install the leg boards E5 d 14:16 nurse nurse asks why don’t you put a warming cover on E5 a 14:20 nurse nurse no E5 c
nurse nurse trying to explain why (can’t understand) E5 e
14:30 nurse nurse talking about the legs and shoulder P4 e 14:54 nurse nurrse leaves, asks for 2 minutes O a 15:00 anesth nurse asks if we need to tilt the table or not E2 a
nurse nurse yes, but we need to put the legs on first (stirrups) E5 d
15:20 nurse nurse before moving the table, we need to move the patient down on the table P3 e

119
15:40 nurse nurse talking about warming covers P5 e 15:46 team all making a joke about the covers and the robot O g 15:59 surg1 all talking about obama and binladen, killing O g 16:20 surg1 nurse asks nurse, do you need me to do something? O a
nurse surg1 no, the cover and the <?>, (what goes under the patients head) E5 d
nurse nurse sorry O c 16:30 anesth nurse do you need it to go down P3 a
anesth nurse all at the same time P3 d
surg1 nurse what do you want me to do, up or down P3 a
16:29 nurse surg1 20 cm down P3 d 16:35 nurse nurse including the cover/sheet, 1,2,3 then move the patient P3 b 16:50 nurse nurse now, move only the paient P3 b
16:55 anesth nurse here we have to deal with this <equipment> (always talk about it (this hole), so they should know what it is/how to deal with it)
E5 e
17:00 nurse anesth we normally put something over the hole to cover it E5 e 17:15 nurse nurse nurses talking to each other about moving pt P3 e
surg1 anesth talking about moving pt to each other P3 e 17:15 nurse nurse ready to move the patient P3 e 17:29 nurse nurse 1,2,3, move the patient P3 a 17:30 nurse nurse need to get something to put under the patient P3 d
nurse nurse is it okay now P3 a 17:32 surg1 nurse its okay, no more uterus P3 d 17:36 nurse anesth asks anesth if she needs to put the board at the patient E5 a 17:36 anesth nurse yeah, maybe E5 c 17:57 surg1 patient don’t worry everything is okay (to the patient P6 g 19:09 nurse surg1 asks if he wants to put the second arm down P3 a 19:12 nurse nurse no, keep it as is P3 d 19:12 nurse nurse ok P3 c 19:27 nurse other here is where to plug in the power supply for a.’s camera O g 20:02 nurse nurse I will put the leg down, and the other leg also? P3 a
nurse nurse yes P3 c 20:09 nurse nurse then we need to pull the leg a little P3 b 20:11 nurse nurse down or up? P3 a 20:11 nurse nurse down P3 c 20:42 nurse nurse asks another nurse what trouble she is having P3 a 20:26 nurse nurse she thinks the leg should be positioned further down P3 d 20:51 nurse nurse both? P3 a
nurse nurse no this one is good P3 d 20:56 nurse nurse do you need help? P3 a
nurse nurse thus on is causing me problems (the leg) P3 d 21:07 nurse nurse is it okay now? P3 a 21:17 nurse nurse it will be easier now to place the arms P3 d
21:20 surg1 nurse she doesn’t have <> anymore, so we don’t have to go into this position
P3 e
21:22 nurse surg1 we also have something here P3 e 21:30 nurse surg1 we need to <tilt>, don’t think the arms are positioned correctly P3 b 21:31 nurse nurse I will put the legs down more? P3 a 21:37 nurse nurse we cannot P3 d 21:37 nurse nurse I will do it here P3 b 21:54 surg1 nurse more? Is it okay now? P3 a 21:58 nurse surg1 ok, its perfect now P3 d 22:07 nurse nurse do you need anything v.? E5 a 22:10 nurse nurse no, but maybe we can get the table for the camera E5 d 22:16 nurse nurse do you want to do it now? E5 a
nurse nurse in this case, we need to make some space on the other side E5 d
22:40 surg1 nurse do you remember how the other surgeon set up/positioned the patient in the first robotic surgery? P3 a
22:40 nurse nurse asks v. - I set up the table for you near the column ?(video cart)
E5 a
nurse nurse yes, ok, this table (indicates to table) E5 d 22:52 nurse nurse ok, I will make some space E5 d
nurse surg1 is it okay? (the patient position) P3 a
surg1 nurse yes, its good now P3 d
nurse surg1 for the legs it will be okay P3 d

120
nurse surg1 and then when we move the robot over, it will be like this
<indicates> E5 d
23:10 nurse nurse where is <other team member>? P3 a
nurse nurse I am here…<walks over to table> P3 d
nurse nurse I want you to help me, we need to put the arms near the body P3 b
23:20 surg1 all joking about his pink phone <all laughing> O g
23:52 surg1 all using the phone for an app that tells angle of the table, asks if anyone remembers what the table angle was last time
E2 a
nurse surg1 32? E2 c
nurse surg1 no, 24 (v.) degrees E2 c
24:27 nurse all talking more about the phone, laughing O g 24:40 nurse nurse says to another nurse, don’t hesitate to ask about anything O f 25:10 other nurse someone in hallway saying hello to the nurses O g
26:08 nurse nurse discussing something about the patient’s arm, we need a support to maintain it (hold it up) …using tape to hold the arm in place
P3 e
26:34 nurse nurse asks another nurse, do you want me to put this <indicates> around the arm? P3 a
nurse nurse yes P3 c
nurse nurse like this, is this okay? P3 a
nurse nurse can I start? <something> O a 26:40 nurse nurse no, I will do it O d 26:47 nurse nurse oh, ok O c
nurse nurse well, if you want to do it you can O d
nurse nurse no, no, its ok O d
nurse nurse I don’t want to (make trouble?) O d 26:58 nurse nurse we will deal with the camera E5 e 27:00 surg1 nurse asking for the camera to take photos of the patient E5 a
nurse nurse there is not enough space for the camera table E5 f
nurse nurse the <column> is very disturbing (in the way, taking up space) E5 f
nurse nurse discussing how to set up the camera table in the limited
space E5 e
28:00 nurse nurse I'll move the table toward you? E2 a
nurse nurse yes, okay E2 c
nurse nurse not so much E2 b
nurse nurse I will move it up now E2 b
surg1 nurse okay E2 c 29:00 nurse nurse need water for cleaning the camera E5 a
nurse nurse I forgot to get this >takes something> - a solution for cleaning the camera E5 d
30:40 nurse nurse you can also take <indicates to table of instruments> E5 a
nurse nurse all the materials for the cytoscopy are on thie table E5 d
31:00 nurse nurse is there is a problem, we need to ask for more space, we'll have to push the table back? E5 a
nurse nurse yes, to the right, but there is not very much space E5 d
36:00 nurse nurse we will put… E5 a
nurse nurse yes this one (cable for video cart) v.) E5 d
nurse nurse I will maybe connect it there (plugging in cables) - the small something to the camera E4 e
nurse nurse and there? E4 a
nurse nurse yes, that’s it E4 c
nurse nurse you need to put <something> on it E4 b
nurse nurse and then I will turn it E4 e
nurse nurse yes E4 c
nurse nurse you need to get it in your hands and you need to put the ca-bles down and then grab it very tightly. You need a lot of force
E4 b
36:40 nurse nurse ok, will you be the one to turn it/use the equipment? E4 a
nurse nurse no, its you E4 d
37:00 nurse nurse stop, she is not sure who needs to turn and who needs to grab
E4 b
nurse nurse yes, its v., or we can do it the other way also. The rep told me we can do it both ways. E4 d
nurse nurse but its so complicated E4 f
nurse nurse if we do it, you are doing it this way E4 e 0:01 nurse nurse asked the other nurse to takeaway the plastic E4 b 0:13 nurse nurse need to put it on the right, otherwise you won’t have anything E4 b

121
to hold on to on it 0:14 nurse nurse asking: do I need to put my hand inside? E4 a
0:23 nurse rep (to b.) asks if she needs to put her hand inside? Because I need to grab the camera here E4 a
0:28 rep nurse you need to get only the cable E4 d 0:28 nurse nurse the camera is not connected yet E4 e 0:31 nurse nurse I won’t be able to… E4 a 0:31 nurse nurse ok, and now I will…..we will put it E4 d 0:57 nurse nurse I think it’s ok here E4 a
nurse rep I didn’t hear a click E4 d
1:04 rep nurse no, we didn’t hear the click E4 d 1:08 nurse nurse because, what I understand is <reading text on monitor> E4 a 1:10 nurse rep is it connected the right way? E4 a 1:12 rep nurse yes, it is connected in the right direction E4 d 1:17 nurse nurse it does not seem like this way is correct E4 a 1:30 nurse nurse but now it doesn’t move E4 d 1:36 nurse rep yeah, still not convinced it is set up correctly E4 a 1:42 rep nurse from your position, it is easier to… E4 d
nurse nurse I will unroll it E4 b 1:47 nurse nurse wait E4 b 1:54 nurse nurse wait. Wait! E4 b 2:18 nurse rep asking if she has to close the end of the plastic cover now? E4 a
rep nurse no E4 c
2:38 nurse rep I cannot do anything else here E5 f 2:46 rep nurse It’s not connected yet E3 f
nurse rep asks: it’s not plugged in yet? E3 a
nurse nurse wait, I will finish (doing something else) then help O d
nurse rep still not okay? E3 a
3:00 rep nurse no E3 c 3:30 nurse nurse we need to calibrate the white color (on the light). E5 e 3:57 nurse nurse asking if everything is connected now E3 a
nurse nurse do you have the light now? E4 a 4:07 nurse nurse wait, wait! Do you see the light on at the end or not E4 d
nurse nurse no, I don’t E4 d
nurse nurse ok I will turn it on for you E4 d 4:12 nurse nurse now the light is on, you can calibrate E4 b
4:17 nurse nurse Do I have to switch into calibration mode (on the touchscreen menu)? Do we need to start with the calibration? E4 a
4:22 nurse nurse no, no, no, you have to click the other button, the other arrow E4 d 4:30 nurse nurse move down? (on the screen) E4 a
nurse nurse and then if you go up, what happens? E4 a 4:45 nurse nurse we have to do calibration? E4 a
4:55 nurse nurse in fact, its for making the calibration to get it well centered, because it isn’t really centered E4 d
5:00 nurse nurse we have to switch from 2D to 3D E4 d 5:06 nurse nurse then from black and white E4 d 5:13 nurse nurse do you always press the same button>? E4 a
nurse nurse yes E4 c
nurse nurse ok then, this is ok also E4 d
nurse nurse now we need to calibrate the other one E4 b
5:33 nurse nurse oops, I made a mistake, I will redo it, and you do … E4 d 5:40 nurse nurse I have to press quit E4 b
6:00 nurse nurse even with <your ability/skill?> you wont be successful with the calibration E4 d
nurse nurse no, it’s the other which is blue E4 d 6:06 nurse nurse the camera itself… E4 a 6:12 nurse nurse thirty E4 c
nurse nurse its not so easy E4 d
6:25 nurse nurse no its okay, we are correct now, points to something on screen E4 d
nurse nurse then select validate E4 b
nurse nurse calibration (reading from screen) E4 f
nurse nurse <beep> whats this? E4 a 6:30 nurse nurse you arent on the correct position of the camera E4 d 6:40 nurse nurse its thirty, and you have up and down E4 d

122
Case 1, Port Planning:
Time Who To Who Text VE Code
Bow-ers Code
5:09 surg1 rep surg explains anatomy of case and plan to rep: right external illiac - must locate it now so rep can help with the placement P4 e
5:21 surg1 rep
surg points to abdomen, says normally its here, will enter from this spot to clean out - comparing to another case rep may be familiar with. Showing the angle of approach, asking if it is a good angle. Wants to use all four arms. Because we need to centralize the tools in one area, even if we are not sure, and surg states he is trying to think about all four arms
P3 e
5:49 surg1 rep explains he will place camera on the median, maybe higher because
P4 a
5:55 rep surg1 maybe higher, yes, confirms higher P4 d 6:05 rep surg1 ideally, we have to be between 15-20cm <something> P4 d
6:16 surg2 surg1 surg2 mentions the patient was already opened - with other operations, and need to avoid the last operative area, need to be careful, she was "undermined"
P6 e
6:24 surg1 surg2 mentions it’s a very difficult case, and the patient knows it too P6 f
6:30 rep surg1 explain to surg need 15-20cm between instruments, joking a little
P3 d
6:53 surg1 surg2 explains to surg2, they can’t make a mistake, want to be in a certain spot in the body P4 e
6:55 surg1 rep asks rep if they need t be so high P4 a 7:02 rep surg1 states they can go from 20-25cm inside the body P4 d 7:05 surg1 rep says ok, asks if can place the camera here <points to body> P4 a 7:06 rep surg1 yes P4 c 7:11 surg2 surg1 points to another area, prefers to place camera there P4 a 7:11 surg1 rep but the tools are long, and the woman is not so fat P4 d
7:18 surg1 rep talking about the pressure in the abdomen, will not put a lot (insufflation)
P3 g
7:24 surg1 rep talking about trocar P3 g 7:41 surg1 rep asks to place 2 trocars on 1 side and 1 on the other P4 a 7:42 rep surg1 says absolutely P4 c 7:53 surg1 rep not sure, we will see if we need an assistant port P3 a 7:58 surg2 surg1 said something <?>, related to assistant port P3 d 8:02 rep surg1 responded that there are already 3 there P3 d
8:32 surg1 surg2,rep says, lets come back to our case O g
8:39 surg1 rep this is where port 1 will go, because here <in this other spot> we will place 2
P4 a
8:40 rep surg1 yes, it’s ok P4 c 8:40 surg1 rep should they be separated by at least 5-6cm? P4 a
rep surg1 yes, remember it will change when we insufflate P3 d 8:56 surg1 rep we will put one here and here, not along the same line? P4 a
rep surg1 yes, exactly P4 c
surg1 rep we will put one here laterally, and then place another one here? P4 a
9:09 rep surg1 yes P4 c
9:12 surg1 rep asks if is should be like this <indicates on body>, because if I put it there, it will be along the same line P4 a
9:15 rep surg1 yes P4 c 9:16 surg1 rep <pointing> there? P4 a 9:20 rep surg1 yes, there is not so bad P4 d 9:28 surg1 rep now the ports are shifted so not along the same line P4 a 9:32 rep surg1 they are shifted, asks if instruments will be constrained P4 a
9:36 surg1 rep doesn’t answer, then says where he will put the last port (on other side), equivalent to the other on, but on the other side P4 a
9:41 surg1 rep the other thing we can do because we are there far, we can put this one there <indicates> and the other one there <indi-cates> and because
P4 a
9:50 rep surg1 you will be better if you put it shifted like this <indicates>, the trocar for the 3rd arm be lateral, the third one must always be more lateral than the first one
P4 d
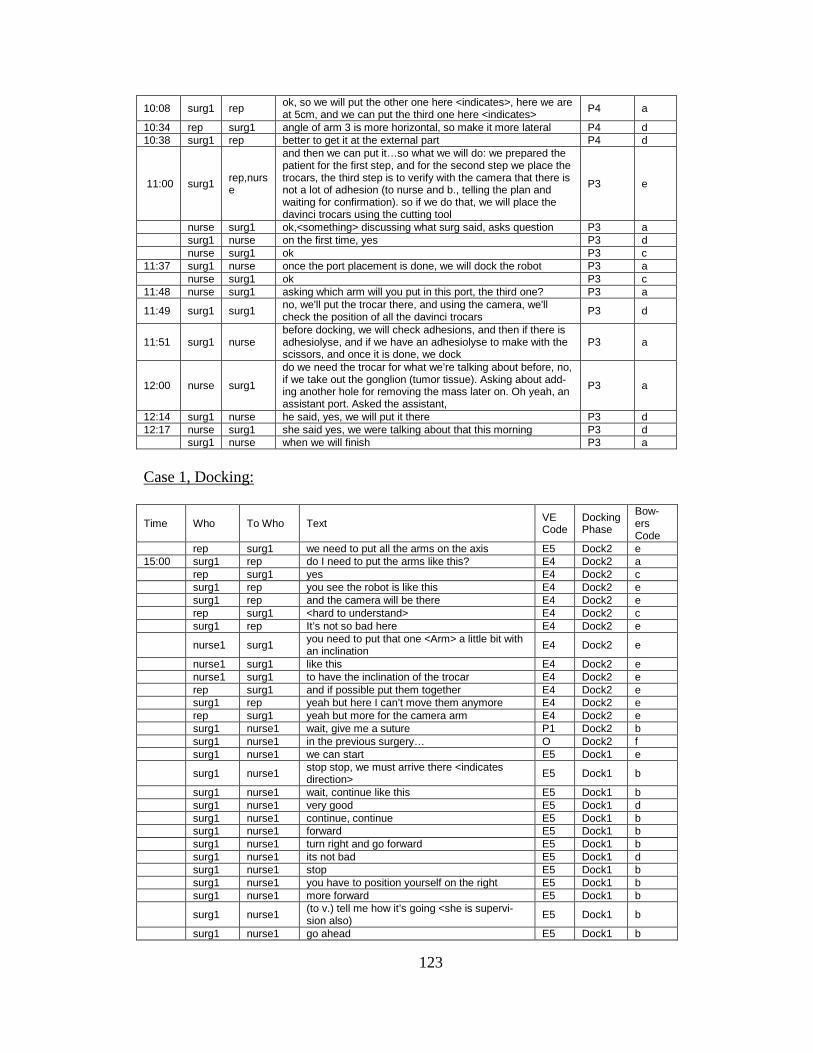
123
10:08 surg1 rep ok, so we will put the other one here <indicates>, here we are at 5cm, and we can put the third one here <indicates>
P4 a
10:34 rep surg1 angle of arm 3 is more horizontal, so make it more lateral P4 d 10:38 surg1 rep better to get it at the external part P4 d
11:00 surg1 rep,nurse
and then we can put it…so what we will do: we prepared the patient for the first step, and for the second step we place the trocars, the third step is to verify with the camera that there is not a lot of adhesion (to nurse and b., telling the plan and waiting for confirmation). so if we do that, we will place the davinci trocars using the cutting tool
P3 e
nurse surg1 ok,<something> discussing what surg said, asks question P3 a
surg1 nurse on the first time, yes P3 d
nurse surg1 ok P3 c 11:37 surg1 nurse once the port placement is done, we will dock the robot P3 a
nurse surg1 ok P3 c 11:48 nurse surg1 asking which arm will you put in this port, the third one? P3 a
11:49 surg1 surg1 no, we'll put the trocar there, and using the camera, we'll check the position of all the davinci trocars P3 d
11:51 surg1 nurse before docking, we will check adhesions, and then if there is adhesiolyse, and if we have an adhesiolyse to make with the scissors, and once it is done, we dock
P3 a
12:00 nurse surg1
do we need the trocar for what we’re talking about before, no, if we take out the gonglion (tumor tissue). Asking about add-ing another hole for removing the mass later on. Oh yeah, an assistant port. Asked the assistant,
P3 a
12:14 surg1 nurse he said, yes, we will put it there P3 d 12:17 nurse surg1 she said yes, we were talking about that this morning P3 d
surg1 nurse when we will finish P3 a
Case 1, Docking:
Time Who To Who Text VE Code
Docking Phase
Bow-ers Code
rep surg1 we need to put all the arms on the axis E5 Dock2 e 15:00 surg1 rep do I need to put the arms like this? E4 Dock2 a
rep surg1 yes E4 Dock2 c
surg1 rep you see the robot is like this E4 Dock2 e
surg1 rep and the camera will be there E4 Dock2 e
rep surg1 <hard to understand> E4 Dock2 c
surg1 rep It’s not so bad here E4 Dock2 e
nurse1 surg1 you need to put that one <Arm> a little bit with an inclination E4 Dock2 e
nurse1 surg1 like this E4 Dock2 e
nurse1 surg1 to have the inclination of the trocar E4 Dock2 e
rep surg1 and if possible put them together E4 Dock2 e
surg1 rep yeah but here I can’t move them anymore E4 Dock2 e
rep surg1 yeah but more for the camera arm E4 Dock2 e
surg1 nurse1 wait, give me a suture P1 Dock2 b
surg1 nurse1 in the previous surgery… O Dock2 f
surg1 nurse1 we can start E5 Dock1 e
surg1 nurse1 stop stop, we must arrive there <indicates direction> E5 Dock1 b
surg1 nurse1 wait, continue like this E5 Dock1 b
surg1 nurse1 very good E5 Dock1 d
surg1 nurse1 continue, continue E5 Dock1 b
surg1 nurse1 forward E5 Dock1 b
surg1 nurse1 turn right and go forward E5 Dock1 b
surg1 nurse1 its not bad E5 Dock1 d
surg1 nurse1 stop E5 Dock1 b
surg1 nurse1 you have to position yourself on the right E5 Dock1 b
surg1 nurse1 more forward E5 Dock1 b
surg1 nurse1 (to v.) tell me how it’s going <she is supervi-sion also) E5 Dock1 b
surg1 nurse1 go ahead E5 Dock1 b

124
surg1 nurse1 stop E5 Dock1 b
nurse1 nurse1 v. to nurse: no E5 Dock1 b
surg1 nurse1 no it was the other side E5 Dock1 b
surg1 nurse1 no, position yourself to the left E5 Dock1 b 17:41 nurse1 nurse1 a little bit more E5 Dock1 b
surg1 nurse1 a little bit more E5 Dock1 b
surg1 nurse1 along the left E5 Dock1 b
surg1 nurse1 stop E5 Dock1 b
surg1 nurse1 now move forward E5 Dock1 b
surg1 nurse1 stop E5 Dock1 b
surg1 nurse1 I will try to move the arm out of the way (so not to hit table) E5 Dock1 e
surg1 nurse1 move forward E5 Dock1 b
surg1 nurse1 its not bad E5 Dock1 d
surg1 nurse1 stop E5 Dock1 b
surg1 nurse1 asks: can I have a suture <air is leaking from trocar> E1 Dock1 a
nurse1 surg1 no, you must have it E1 Dock1 d
surg1 nurse1 no, I gave it back to you, I put it on the table E1 Dock1 a
nurse1 surg1 here it is E1 Dock1 d
surg1 nurse1 don’t move E1 Dock1 b
surg1 nurse1 we have a robot but we don’t have needles?! (joking) O Dock1 g
surg1 rep we have a 2m euro robot, and we need to use a pink iphone to calculate the angles! O Dock1 g
surg1 nurse1 ok, its good, we need to continue to move forward E5 Dock1 b
surg1 nurse1 again, again, again E5 Dock1 b
surg1 nurse1 there is no contact here, that’s ok E5 Dock1 f
surg1 nurse1 move forward E5 Dock1 b
nurse1 nurse1 you are hitting the table E5 Dock1 f
surg1 nurse1 what are you colliding with E5 Dock1 a
nurse1 surg1 the table E5 Dock1 c
nurse1 nurse1 it wasn’t bad E5 Dock1 c
surg1 nurse1 ok, don’t move E5 Dock1 b
nurse1 surg1 now we can move the arms E5 Dock2 a
surg1 nurse1 yes, we can try E5 Dock2 c
rep surg1 it will be better if you move the patient cart a
little bit more E5 Dock1 e
surg1 nurse1 move it backward E5 Dock1 b
surg1 nurse1 stop E5 Dock1 b
surg1 nurse1 turn the handles to the right E5 Dock1 b
surg1 nurse1 yes E5 Dock1 c
surg1 nurse1 stop E5 Dock1 b 20:00 surg1 nurse1 move forward E5 Dock1 b
surg1 nurse1 not so bad E5 Dock1 d
surg1 nurse1 stop E5 Dock1 b
surg1 nurse1 position the handles on the left E5 Dock1 b
surg1 nurse1 move forward until you touch the table E5 Dock1 b
surg1 nurse1 move again E5 Dock1 b
surg1 nurse1 stop E5 Dock1 b
surg1 nurse1 not so bad E5 Dock1 d
rep nurse1 a little bit more E5 Dock1 b
surg1 nurse1 stop E5 Dock1 b
surg1 nurse1 move forward if you can E5 Dock1 b
surg1 nurse1 stop, its touching the table, its good E5 Dock1 f
nurse1 surg1 can I lock it down? E5 Dock1 a
surg1 nurse1 yes yes, wait E5 Dock1 d
21:20 rep nurse1 we will lock it once one of the trocars is con-nected
E5 Dock1 d
surg1 nurse1 joking about the cable, because the anesth. Tripped before O Dock1 g
nurse1 surg1 asks: is it clipped in? E5 Dock2 a
surg1 nurse1 if it doesn’t click, it’s not good E5 Dock2 d
nurse1 surg1 no, its not good then. We need to pull the tro-car out a little bit. We need to be on the white E2 Dock2 e

125
line
surg1 nurse1 all needs to be white E2 Dock2 a
nurse1 surg1 I think so E4 Dock2 d
surg1 rep asking if it all needs to be white when con-nected E4 Dock2 a
22:25 rep surg1 its down on the gray surface E4 Dock2 d
surg1 nurse1 I'm not surprised it didn’t work E4 Dock2 f
surg1 nurse1 and then after, which one will we connect next? E4 Dock2 a
rep surg1 we need to do number 2 now E4 Dock2 d
nurse1 surg1 no, we'll set up all the others, and then do the
camera last E4 Dock2 d
surg1 rep do we need to put the #2 there <indicating> E4 Dock2 a
rep surg1 yes E4 Dock2 c
rep surg1 no, no, it’s number 3 E4 Dock2 d
rep surg1 its number 3? E4 Dock2 a
nurse1 rep number 3 is over there <pointing> E4 Dock2 d
rep nurse1 yeah, that’s it, number 3 on the top and num-ber 2 down E4 Dock2 d
surg1 nurse1 this one is not green E4 Dock2 a
surg1 rep ok, and now chief, can you tell me how to put
#3 in E4 Dock2 a
rep surg1 (hesitating) you have to position number 1 first E4 Dock2 d
surg1 rep no, but number 3 E4 Dock2 a
rep surg1
because we have to position it on the other side. We will have some more space. the joint with the blue arrow, it needs to be near the number 1
E4 Dock2 d
surg1 rep this one? E4 Dock2 a
rep surg1 yes, we need to put it on the other side E4 Dock2 d
surg1 rep do we need to unlock this one? E4 Dock2 a
rep surg1 no, just push the button on the other side E4 Dock2 d
nurse1 rep here? E4 Dock2 a
24:07 rep nurse1 yes E4 Dock2 c
rep nurse1 no we can, invert/swivel it E4 Dock2 d
surg1 nurse1 that’s it, here we get some more space E4 Dock2 f
surg1 nurse1 and now we can insert arm number 3 down E4 Dock2 e
surg1 nurse1 we will put it very horizontal, with the port clutch E4 Dock2 e
surg1 nurse1 go down (guiding v.) E4 Dock2 b
surg1 nurse1 I'm not very convinced by that E4 Dock2 a
surg1 nurse1 no, it’s badly installed again E4 Dock2 d
nurse1 surg1 yes, yes, yes E4 Dock2 c
surg1 rep Take a look. E4 Dock2 b
rep surg1 no, because we will be able to move this one
onto this side by pushing this button E4 Dock2 d
surg1 rep which one, number 2? E4 Dock2 a
rep surg1 number 2 E4 Dock2 c
surg1 rep we can push it E4 Dock2 b
surg1 rep so the clutch of number 2? E4 Dock2 a
rep surg1 yes, we need to push the clutch of number 2
inside E4 Dock2 d
rep surg1 now, we have enough space for number 3, to dock it E4 Dock2 e
surg1 rep where is the camera trocar? E4 Dock2 a
rep surg1 It’s not open there E4 Dock2 d
surg1 rep It’s not so simple after all E4 Dock2 a
27:11 surg1 nurse1 grasp it like that E4 Dock2 d
surg1 nurse1 is it really open there? E4 Dock2 a
nurse1 surg1 It’s completely open, yes E4 Dock2 d
nurse1 surg1 no, it won’t connect there E4 Dock2 a
surg1 nurse1 no, but I cannot bring it any closer E4 Dock2 a
nurse1 surg1 try to E4 Dock2 b
surg1 nurse1 we must be at least there <indicating>, it won’t be so bad there E4 Dock2 d
surg1 nurse1 that’s it. E4 Dock2 d
surg1 nurse1 take a look at the skin E4 Dock2 b

126
surg1 nurse1 the trocar is not in enough E4 Dock2 d
rep surg1 they are not on the same axis, you have to put
the arm down on both sides E4 Dock2 b
surg1 rep what? E4 Dock2 d
rep surg1 more laterally on the right E4 Dock2 b
surg1 rep what do you mean? E4 Dock2 d
rep surg1 toward yourself E4 Dock2 b
surg1 rep I cannot E4 Dock2 d
rep surg1 not that one, E4 Dock2 b
surg1 rep move it down toward the patient E4 Dock2 b
rep surg1 trocar is like this <showing>, and the arm is like this E4 Dock2 e
surg1 rep
yeah I know that, but it doesn’t move down more than that, and doesn’t move up more than that
E4 Dock2 a
rep surg1 the trocar must be in a reasonable position E4 Dock2 d
rep surg1 yeah, like this here. E4 Dock2 d
surg1 rep so, like this? And here? E4 Dock2 a
rep surg1 yeah that’s it, if you can move down a little more, you need to put the trocar more horizon-tally,
E4 Dock2 d
nurse1 rep yes like this? E4 Dock2 a
rep nurse1 yes, exactly. Because its position must be horizontal E4 Dock2 d
rep nurse1 the number 3 must always be on the horizontal
position E4 Dock2 d
29:20 surg1 nurse1 are both positioned now? E4 Dock2 a
nurse1 surg1 yes E4 Dock2 c
surg1 nurse1 ok, and we still have to do yours <last arm
near nurse> E2 Dock2 e
rep surg1 the number 1 E2 Dock2 e
rep surg1 here, you need to move the clutch, because it is not really maintaining the trocar. Yes ex-actly, like this.
E2 Dock2 b
surg1 nurse1 now we have to position the camera to verify all this E2 Dock2 b
rep surg1 what I would also do is to orient the camera,
and position it on the axis E2 Dock3 d
surg1 nurse1 can I have the camera E2 Dock3 b
nurse1 surg1 yes E2 Dock3 c
surg1 rep this one? <the arm/ button for installing cam-
era on arm> E2 Dock3 a
rep surg1 no, with the other button E2 Dock3 d
rep surg1 the light gray area, which is on the top, posi-tion it on the axis of the patient’s head E2 Dock3 d
rep surg1 no, on the axis of the patients head <correct-
ing surgeon> E2 Dock3 b
nurse1 surg1 this way E2 Dock3 a
rep surg1 that’s it E2 Dock3 c
rep surg1 a little bit more if possible E2 Dock3 b
surg1 nurse1 ok, let’s see, so this is number zero E2 Dock3 e
surg1 rep is there a certain direction? E4 Dock3 a
rep surg1 yes, the buttons inside E4 Dock3 d
surg1 rep which buttons? E4 Dock3 a
rep surg1 the button with + (plus) inside E4 Dock3 d
surg1 rep inside, what do you mean? E4 Dock3 a
rep surg1 no, yes, like this E4 Dock3 d
surg1 rep this, we will attach it E2 Dock3 e
surg1 rep and then can we move the camera down E2 Dock3 e
rep surg1 yes, you need to push the port clutch on the top E2 Dock3 b
rep surg1 yes, and now you can move it all directions E2 Dock3 b
surg1 rep and now to adjust the focus of the camera? E4 Dock3 a
rep surg1 adjust the focus, you need to go on it, you have the buttons, I don’t remember exactly, E4 Dock3 d
surg1 rep yes, just check E4 Dock3 b
surg1 nurse1 so here is number 2 E4 Dock3 e
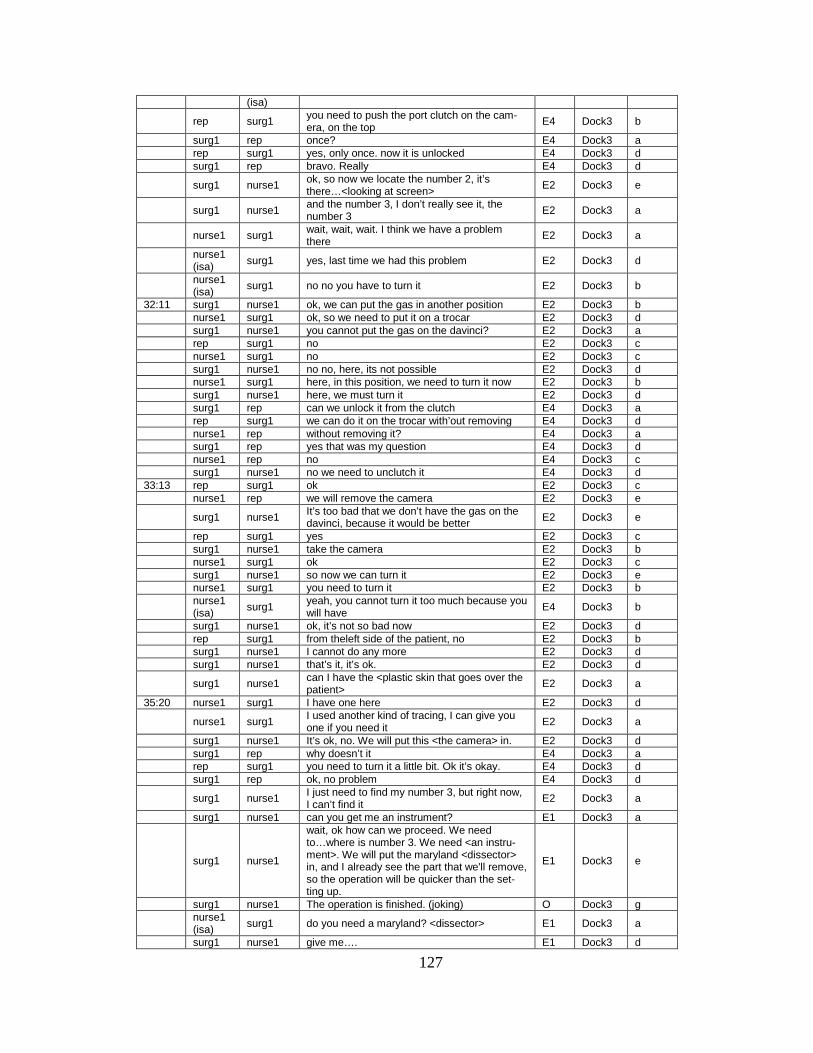
127
(isa)
rep surg1 you need to push the port clutch on the cam-
era, on the top E4 Dock3 b
surg1 rep once? E4 Dock3 a
rep surg1 yes, only once. now it is unlocked E4 Dock3 d
surg1 rep bravo. Really E4 Dock3 d
surg1 nurse1 ok, so now we locate the number 2, it’s
there…<looking at screen> E2 Dock3 e
surg1 nurse1 and the number 3, I don’t really see it, the number 3 E2 Dock3 a
nurse1 surg1 wait, wait, wait. I think we have a problem
there E2 Dock3 a
nurse1 (isa) surg1 yes, last time we had this problem E2 Dock3 d
nurse1 (isa)
surg1 no no you have to turn it E2 Dock3 b
32:11 surg1 nurse1 ok, we can put the gas in another position E2 Dock3 b
nurse1 surg1 ok, so we need to put it on a trocar E2 Dock3 d
surg1 nurse1 you cannot put the gas on the davinci? E2 Dock3 a
rep surg1 no E2 Dock3 c
nurse1 surg1 no E2 Dock3 c
surg1 nurse1 no no, here, its not possible E2 Dock3 d
nurse1 surg1 here, in this position, we need to turn it now E2 Dock3 b
surg1 nurse1 here, we must turn it E2 Dock3 d
surg1 rep can we unlock it from the clutch E4 Dock3 a
rep surg1 we can do it on the trocar with’out removing E4 Dock3 d
nurse1 rep without removing it? E4 Dock3 a
surg1 rep yes that was my question E4 Dock3 d
nurse1 rep no E4 Dock3 c
surg1 nurse1 no we need to unclutch it E4 Dock3 d 33:13 rep surg1 ok E2 Dock3 c
nurse1 rep we will remove the camera E2 Dock3 e
surg1 nurse1 It’s too bad that we don’t have the gas on the davinci, because it would be better E2 Dock3 e
rep surg1 yes E2 Dock3 c
surg1 nurse1 take the camera E2 Dock3 b
nurse1 surg1 ok E2 Dock3 c
surg1 nurse1 so now we can turn it E2 Dock3 e
nurse1 surg1 you need to turn it E2 Dock3 b
nurse1 (isa) surg1
yeah, you cannot turn it too much because you will have E4 Dock3 b
surg1 nurse1 ok, it’s not so bad now E2 Dock3 d
rep surg1 from theleft side of the patient, no E2 Dock3 b
surg1 nurse1 I cannot do any more E2 Dock3 d
surg1 nurse1 that’s it, it’s ok. E2 Dock3 d
surg1 nurse1 can I have the <plastic skin that goes over the
patient> E2 Dock3 a
35:20 nurse1 surg1 I have one here E2 Dock3 d
nurse1 surg1 I used another kind of tracing, I can give you one if you need it E2 Dock3 a
surg1 nurse1 It’s ok, no. We will put this <the camera> in. E2 Dock3 d
surg1 rep why doesn’t it E4 Dock3 a
rep surg1 you need to turn it a little bit. Ok it’s okay. E4 Dock3 d
surg1 rep ok, no problem E4 Dock3 d
surg1 nurse1 I just need to find my number 3, but right now,
I can’t find it E2 Dock3 a
surg1 nurse1 can you get me an instrument? E1 Dock3 a
surg1 nurse1
wait, ok how can we proceed. We need to…where is number 3. We need <an instru-ment>. We will put the maryland <dissector> in, and I already see the part that we'll remove, so the operation will be quicker than the set-ting up.
E1 Dock3 e
surg1 nurse1 The operation is finished. (joking) O Dock3 g
nurse1 (isa) surg1 do you need a maryland? <dissector> E1 Dock3 a
surg1 nurse1 give me…. E1 Dock3 d

128
(isa)
surg1 nurse1 what I want is to see my instrument on the screen. By installing the instrument, we can see it
E1 Dock3 e
surg1 nurse1 give me a <instrument> E1 Dock3 b
video ends surg1 rep
once you connect an instrument, if you remove it and put it on another position, does it use up one life?
E4 Dock3 a
0:30 rep surg1
no, the instrument is recognized once by the system, after that you can put it where you want. Since the robot is not turned off, it keeps its life.
E4 Dock3 d
surg1 rep do I need to install the <reducer - tool> E4 Dock3 a
rep surg1 no, the reducer is for the specimen bag E4 Dock3 d
surg1 nurse1 where is it <still trying to find #3>. E4 Dock3 a
surg1 nurse1 its surprising. Ah, here it is. E4 Dock3 d
nurse1 surg1 oh yeah E4 Dock3 d
surg1 nurse1 ok E4 Dock3 d
surg1 nurse1
can you give me….here we have….if we co-agulate, we'll grasp with this, it will not be so bad. Yes we will coagulate there, yes, give me the maryland
E1 Dock3 b
1:04 rep nurse1 you need to move forward #1, imagine that it will work down, so that the #1 cannot move outside.
E2 Dock3 b
nurse1 rep here? E2 Dock3 a
rep nurse1
by pushing this button, so, no not in that direc-tion, the number 1 more on the outside. More there…yes. <responding to movements>
E2 Dock3 d
surg1 nurse1 be careful with the trocar E2 Dock3 b
rep nurse1 maybe put your whole hand on #1 E2 Dock3 b
surg1 nurse1 here its not so bad E2 Dock3 d
surg1 nurse1 can you give me the maryland E1 Dock3 a
surg1 nurse1 What’s wrong with the tool? E4 Dock3 a 1:40 nurse1 surg1 tool is not compatible with the cannula E4 Dock3 d
surg1 nurse1 it isn't happy E4 Dock3 f
nurse1 surg1 why E4 Dock3 a
surg1 nurse1 it's not happy E4 Dock3 d
nurse1 surg1 ah, because there are two bipolars E4 Dock3 f
2:15 surg1 nurse1 why are there two bipolars E4 Dock3 a
nurse12 surg1 no, there arent two bipolars E4 Dock3 d
nurse1 surg1 I don’t know E4 Dock3 a
rep surg1 maybe it doesn't recognize the tool E4 Dock3 d 2:40 nurse1 surg1 no E4 Dock3 c
rep nurse1 I cannot see the screen, can you read me the error message E4 Dock3 b
nurse1 rep instrument not compatible with the cannula E4 Dock3 d
nurse1 surg1 I don’t know why it is not compatible E4 Dock3 a
nurse12 nurse1 what is the cannula? E4 Dock3 a
3:30 nurse1 nurse12 the cannula is the trocar E4 Dock3 d
rep nurse1 maybe we can try docking it on arm 1, not
completely but just to see if its compatible E4 Dock3 e
surg1 nurse1 can someone check the patient's skin (around the trocar) E4 Dock3 b
nurse1 surg1 if you want I can do it (dock instrument in arm
1)? E4 Dock3 a
4:00 surg1 nurse1 yes E4 Dock3 c
nurse1 surg1 it’s the same error E4 Dock3 d
rep nurse1 the instrument is not compatible with the can-nula. I think there is a problem with the instru-ment
E4 Dock3 d
surg1 rep do you mean we need another maryland? E4 Dock3 a
surg1 nurse1 do you have anything else we can use to co-
agulate? E4 Dock3 a
nurse12 surg1 I have a bipolar micro grasper E4 Dock3 d
surg1 rep in that case, what can we do? Practically speaking E4 Dock3 a

129
rep surg1 we will change the maryland, and then we can run a procedure to determine the number of lives on the tool
E4 Dock3 d
4:50 nurse12 surg1 do you need the maryland and then.. E4 Dock3 a
surg1 nurse12 yes, why not E4 Dock3 d
rep surg1 today we tried the instrument twice on 2 arms and it didn’t work, so I think the problem is with the instrument
E4 Dock3 e
surg1 rep the light blue color code compared to the white, what does it mean? It is waiting for an instrument?
E4 Dock3 a
rep surg1
yes, its waiting for an instrument, exactly. See how on number three, it has an instrument and the color is dark blue. And when its waiting for an instrument its light blue.
E4 Dock3 d
surg1 rep is there a trocar for the davinci that we can use
the gas with? E4 Dock3 a
rep surg1 yeah, I think there is one E4 Dock3 d
surg1 nurse12 next Thursday I don’t know what we'll do if we have the same problem because we have <names type of operation>.
E4 Dock3 e
surg1 nurse12 I don’t know what instrument we need to choose, this one, this one , or this one. E1 Dock3 a
nurse13 surg1 I have a pro grasp E1 Dock3 d
surg1 nurse12 bipolar? E1 Dock3 a
nurse13 surg1 yes, bipolar E1 Dock3 d
surg1 rep ok, that will be interesting E1 Dock3 e
rep surg1 there is no other maryland? E1 Dock3 a
nurse12 surg1 no, there is not E1 Dock3 d
surg1 nurse1 lets go, lets go E1 Dock3 e
rep nurse12
<talking, unable to understand fully b/c in cor-ner of room, but opening instruments and explaining that she didn’t find another mary-land, etc>
E1 Dock3 e
8:00 surg1 nurse1 why are you warming the tip of the instrument? E1 Dock3 a
nurse1 surg1 to avoid getting another instrument that doesn’t work E1 Dock3 d
surg1 nurse1 oh, it likes this one E1 Dock3 f
nurse1 surg1
<watching instrument in patient, moving around> yes <when surgeon reaches correct position>
E1 Dock3 f
surg1 nurse1 now we will put the grasper E1 Dock3 e
nurse1 surg1 scissors also? E1 Dock3 a
surg1 nurse1 ah yes, give me the scissors also E1 Dock3 d
nurse1 nurse12 can you give me the scissors please E1 Dock3 b
nurse12 nurse1 for the scissors we have that kind and that kind <pointing> E1 Dock3 f
nurse12 surg1 I think we need to reduce the pressure? E2 Dock3 a
surg1 nurse12 yes, you can do it E2 Dock3 d 10:05 surg1 nurse1 these are the scissors? E1 Dock3 a
nurse1 surg1 yes E1 Dock3 c
surg1 nurse1 can you put the cap on E2 Dock3 b
surg1 nurse1 <get same error message when docking> oh, this one doesn’t work either E4 Dock3 f
11:00 nurse1 surg1 there is no instrument E4 Dock3 d
surg1 nurse1 I think I know why E4 Dock3 d
nurse1 surg1 can you explain why? E4 Dock3 a
surg1 nurse1 I don’t think we can move it down E4 Dock3 d
rep surg1
there is no cannula detected. That means it doesn’t recognize the trocar. Maybe there is a problem with the connection between trocar and instrument
E4 Dock3 d
11:50 nurse1 surg1 it works now, its okay now E4 Dock3 f
surg1 nurse1 the trocar is sticking out of the skin E4 Dock3 f
surg1 nurse1 so wait, now we have a problem. During the manipulations the trocar came out. We need to unlock the arm, remove it, and fix the trocar by
E2 Dock3 e

130
pushing it back in. 12:30 surg1 nurse1 so wait, now the instrument comes out E2 Dock3 a 13:00 nurse1 surg1 that’s it E2 Dock3 c
rep surg1 can you push the arm on the other side E2 Dock3 b
surg1 nurse1 that doesn’t work, can you explain why E4 Dock3 d
surg1 nurse1 ok <fiddling with arm/instrument> E4 Dock3 e
surg1 nurse1 come on baby <to instrument/arm> E4 Dock3 e
surg1 nurse1 is it okay here? E4 Dock3 a
nurse1 surg1 I think so E4 Dock3 d
surg1 nurse1 clutch E4 Dock3 b
surg1 nurse1 ok, yes E4 Dock3 c
nurse1 surg1 the scissors <hands to surgeon> E1 Dock3 e
surg1 nurse1 ok, so, let’s go WF Dock3 e
nurse1 surg1 we arent putting an inversed trocar? P3 Dock3 a
surg1 nurse1
do you want to put it in now? We need to remove the piece. We will put at 10mm trocar in place when we finish (after the robot)
P3 Dock3 d
nurse1 surg1 ok, I will plug in the cable E5 Dock3 e
surg1 nurse1 do you remember when we started? WF a
Case 1, Console: Time Who To Who Text VE
Code Bowers Code
13:00 nurse1 surg1 its on the number 2 <tool for surgeon> E5 f
surg1 nurse1 can you check whether thre is a conflict with the patient
body E5 b
14:00 nurse surg1 its ok E5 d
rep nurse2 explaining how to change video on mon from l eye to r eye E4 e
surg1 nurse1 is it mono or bi(polar)? E5 a
nurse1 surg1 it is bi (bipolar> E5 d
nurse1 surg1 if you want I can put a mono (polar)? E5 a
surg nurse1 no its okay E5 d
surg1 nurse1 there is no scissors? E5 a
nurse1 nurse2 no this is the bipolar E5 d
nurse2 nurse1 the screen doesn’t display anything E3 a
nurse2 nurse1 wait, the wire, its not this one E3 d
nurse2 nurse1 its this one, let me put the bipolar E5 e
nurse3 nurse2 this is a monopolar wire E3 a
nurse2 nurse3 yes that’s it E3 d
nurse2 nurse1 it will display something normally, but nothing is displayed E3 e
surg nurse2 is there a conflict there? Because I cannot go further with
number 3 E3 a
nurse2 surg1 yes there is a conflict E3 d
surg1 nurse2 is number 3 the one that is lowest? E3 a
rep surg1 you can avoid the conflict by..number 3 is like this <show> number 2 is like this <show> so we need to shift the arm this way. This permits sometimes to limit the conflict
E4 d
17:00 nurse2 nurse3 talking how to organize each tool E4 e
surg1 nurse1 can I try now? E4 a
nurse1 surg1 yes, the bipolar is connected now E4 d
6:00 surg1 rep it will be cool because here we can open the peritum and we can see what there is behind P3 e
nurse1 surg1 does it work? E5 a
surg1 nurse1 yes it works E5 d 17:30 nurse1 surg1 do you want me to plug the monopolar on the scissors now E1 a
surg1 nurse1 yes E1 c
surg1 nurse1 do you want me to stop moving the arms E2 a
nurse1 surg1 yes because I need to move the scissors arm to reach E5 d
surg1 nurse1 what are you doing here E5 a
nurse1 surg1 wait im trying to E5 d
surg1 nurse1 are you performing the operation in my place O a
nurse1 surg1 no, can you move the arm because I need to plug the E2 d
surg1 nurse1 ok here you can go E5 b
nurse1 surg1 I think its ok now E5 d

131
surg1 nurse1 ok thank you E5 d
surg1 surg3 explaining case to another surgeon in the room O e
surg1 nurse1 are you used to the procedure to undocking the robot quickly and to convert laparo P3 a
nurse1 surg1 why, because you think that P3 d
surg1 nurse1 because ths here <showing arm on screen> this is the ar-
tery <implying difficulty> P3 e
0:00 surg1 nurse1 where is the rep? <rep not in room> E4 a
surg1 nurse1 the scissors, can we move them up? Because its becoming more difficult E2 b
nurse1 surg1 move them up that’s it? E2 d
surg1 nurse1 yes, does it work? E2 a
surg1 nurse1 ok, move it up E2 b
surg1 nurse1 move it up E2 b
surg1 nurse1 stop E2 b
surg1 nurse1 ok, very well E2 f
surg1 nurse1 is there a conflict there? E3 a
nurse1 surg1 yes, between number 2 and number 3 E3 d
surg1 nurse1 this one is number 3? E3 a
nurse1 surg1 yes E3 c
nurse2 surg1 can we move number 3 to the other side to save some space? E2 a
surg1 nurse1 is the bipolar on the left? E2 a 8:00 nurse1 surg1 the bipolar is on arm number 2 E2 d
surg1 nurse1 yeah that’s it E2 f
surg1 nurse1 because its not working well. Can you check if the wire is still connected E3 b
nurse1 surg1 maybe its unplugged, let me check E3 d
nurse1 surg1 here try it E3 b
surg1 nurse1 no E3 c
surg1 nurse1 don’t worry E3 b
nurse1 surg1 no I'll try to unplug it and replug it again E3 e
surg1 nurse1 is there a conflict there E3 a
nurse1 surg1 yes, there is a conflict between number 2 and number 3 again. E3 d
nurse1 surg1 What do you want me to do? E3 a
surg1 nurse1 as you can see, the setting up is very important E3 d
surg1 nurse1 because here the tumor is mostly removed but I cannot go farther E3 f
surg1 nurse2 can you look for the rep? E3 a
surg1 other you see, the guy told us that everything is set up well, and now we are having problems. So this is the objective for our project.
E3 f
surg1 rep chief, our excellent installation is causing some troubles E4 a
rep surg1 it moves to the other side E4 d
surg1 rep yeah but now I don’t have access to this area E4 e
surg1 rep the tumor is almost removed, but I cannot move forward because I have this one here and this one is blocked E4 e
rep surg1 because number 3 is blocking it E4 e
rep nurse1 what we need to do is to remove arm 3 and move it to the
other side E4 e
rep surg1 we need to remove arm 3 and move it to the other side E4 e
nurse1 surg1 can I remove the instrucmt from number 3? E4 a
surg1 nurse1 yeah you can go because I stopped E4 d
rep nurse1 remove the instrucment and move the arm to the other side E4 b
rep nurse1 so we need to push the button on the arm and move it backward E4 b
rep nurse1 that’s it E4 f
surg1 nurse1 maybe you can move it completely on the other side E4 e
surg1 nurse1 more to the robot center E4 e
nurse1 surg1 this arm? E4 a
surg1 nurse1 yes because the collison is higher than we expect E4 d
surg1 nurse1 yeah its not bad now E4 f
rep nurse1 after, if it blocks here, we can use this space, we can change the arm's orientation E4 e
nurse1 rep move this backward? E4 a
rep nurse1 that’s it E4 d

132
surg1 nurse1 wait, I will look on the screen to see the tool moving E4 b
surg1 nurse1 ok you can go im seeing it E4 b
surg1 nurse1 no move it down E2 b
surg1 nurse1 try to move the tool tip towards the pelvis E2 b
surg1 nurse1 pelvis, down E2 b
surg1 nurse1 and now move it to the right E2 b
nurse1 surg1 no I cannot move now, im blocked by the other arm E2 d
nurse1 surg1 or maybe I can move it down E2 b
rep nurse1 we need to move this one here, push the button, move the arm to this area E4 e
surg1 nurse1 ok move forward now E2 b
surg1 nurse1 move the instrument inside E2 b
surg1 nurse1 stop, I think the trocar is outside the skin now E2 f
surg1 nurse1 yeah its completely out E2 f
rep nurse1 you need to remove the instrument and try to move the trocar inside E2 b
surg1 nurse1 do you want me to scrub out <to help her, she is having
trouble inserting the instrument back in the new port> E4 a
nurse2 nurse1 you are not so far now E2 f
surg1 nurse1 you arent so far now E2 f
surg1 nurse1 now you need to move it completely on the other side E2 b
surg1 nurse1 yes like this E2 b
surg1 nurse1 ok I can try now E2 e
nurse1 surg1 no wait I need to close it E2 e
nurse1 surg1 now its closed E2 f
surg1 nurse1 now can you put the instrument in? E2 b
nurse1 surg1 ok E2 c
surg1 nurse1 and now I move forward E2 e
surg1 nurse1 no you need to dive the tool. For you it will be toward the vulva of the patient and toward her right P4 b
surg1 nurse1 that’s it P4 b
surg1 nurse1 continue P4 b
nurse1 surg1 here? P4 a
surg1 nurse1 yes P4 c
surg1 nurse1 yeah not so bad P4 b
surg1 nurse1 move down a little bit more P4 b
surg1 nurse1 no I meant driving P4 b
surg1 nurse1 no come back to the middle line P4 b
surg1 nurse1 very well stop P4 b
nurse1 surg1 ok I leave it here P4 a
surg1 nurse1 ok P4 c
surg1 nurse1 can I now? P4 a
nurse1 surg1 yeah you can. P4 d
nurse1 surg1 I think there is a conflict E3 a
nurse1 surg1 it seems to be better than before E3 e
surg1 nurse1 yes thank you E3 d
surg1 nurse2 needs the supplementary trocar to insert the specimen bag E1 b
nurse2 surg1 yes I will ask the scrub nurse to do it E1 d
nurse2 surg1 do you want a massage <joking to surgeon at console> O
37:00 surg1 nurse1 now its your time, because here we have finished O e
nurse1 surg1 as k surgeon to make the new port (for specimen bag) E1 a
nurse1 surg1 or I can do it if you want E1 a
surg1 nurse1 yes yes E1 c
nurse1 surg1 do we put it here? P3 a
surg1 nurse1 lets think about it P3 d
14:00 surg1 nurse1 I will move the camera so that we can see inside when we arrive
E2 e
surg1 nurse1 where are you? P4 a
nurse1 surg1 here P4 c
surg1 nurse1 push a little bit down P4 b
nurse1 surg1 here? P4 c
surg1 nurse1 more down and towards the median P4 b
surg1 nurse1 yeah but here you will be in conflict with my arm P4 e
surg nurse1 more down P4 b
nurse1 surg1 here? P4 c
surg1 nurse1 yeah P4 c

133
nurse1 surg1 so I'll put it here? P4 a
surg1 nurse1 wait wait I will check where you are P4 d
surg1 nurse1 try it more here and more here P4 b
surg1 nurse1 yeah we can see yo uhere, you are almost inside P4 f
surg1 nurse1
push more and then push back to ser where you are, then push again with all your strength unti lyou see the blue on the screen<hard to translate rest of sentence, but way of pushing>
P4 b
nurse1 surg1 can you move the camera so that we can see it arriving? E2 a
surg1 nurse1 where are you now? P4 a
surg1 nurse1 ok so keep going P4 b
surg1 nurse1 ok so now remove your trocar P4 b
surg1 nurse1 go towards the pubic P4 b
surg1 nurse1 put your bag inside P1 b
surg1 nurse1 ok, now open the bag P1 b
nurse1 surg1 how does it work? P1 d
nurse1 surg1 like this? P1 a
surg1 nurse1 ok now, leave the trocar in its position remove the string to deploy the bag P1 b
surg1 nurse1 ok now push it up P1 b
nurse surg1 do I need to remove the shaft? P1 a
surg1 nurse1 no, no we'll stop P1 d
nurse1 surg1 ok P1 c
surg1 nurse1 now push it up so that we can see what is going on down P1 b
nurse1 surg1 like this? P1 a
surg1 nurse1 yeah perfect P1 d
nurse1 surg1 do you want me to irrigate the cavity? P1 a
surg1 nurse1 this is what I was thinking about P1 d
surg1 nurse1 can we use the davinci for washing? P1 a
nurse1 surg1 no we need to use another trocar P1 d
surg1 nurse1 otherwise I will put the instruments here so that we can see them correctly P1 e
surg1 nurse1 I am going to scrub in P1 e
surg1 nurse1 it will be interesting to have a washing system with the dav-inci O e
nurse1 surg1 its stupid to use another trocar to do it O e
nurse1 surg1 I will put the stand P1 e
nurse1 surg1 I will open it P1 e
nurse1 surg1 it works now P1 e
surg1 nurse1 oh, we don’t have a second screen E3 f
nurse1 surg1 no, we didn’t set up the second screen today E3 f
surg1 nurse1 can we have more light E2 b
surg1 nurse1 here we have a problem of the mass (ibgger than the hole) P2 e
surg1 nurse1 give me the scissors with the teeth E1 b
surg1 nurse1 we will put in the trocar again P3 e
surg1 nurse1 you can stop insufflating for a moment P1 b
nurse1 surg1 ok P1 c
surg1 nurse we can start again the insufflation P1 b
other surg1 why did you make a new hole? P3 a
surg1 other
the diameter is different, the tool for the davinci is smaller than the specimen bag tool, and not done with the davinci yet so cannot use these holes
P3 d
30:00 surg1 nurse1 is this our trocar? (back at console) P4 a
surg1 nurse1 orient it toward the vulva P4 b
nurse1 surg1 ok P4 c
surg1 nurse1 then put in side P1 b
nurse1 surg1 the washer? P1 a
surg1 nurse1 yes P1 c
nurse1 surg1 can I put the water inside P1 a
surg1 nurse1 wait im just checking what this is P1 d
surg1 nurse1 yes now you can put the water in P1 b
surg1 nurse1 ok go go go P1 b
surg1 nurse1 stop P1 b
surg1 nurse1 now wait P1 b
surg1 nurse1 ok you can go to wash this area P1 b
surg1 nurse1 good P1 b

134
surg1 nurse1 now move it down P4 b
nurse1 surg1 more water? P1 d
surg1 nurse1 no wait I am disturbed by the arm E3 b
surg1 nurse1 ok you can go P4 b
surg1 nurse1 move it backward a little bit P4 b
surg1 nurse1 wait wait P4 b
surg1 nurse1 yes here you can go P4 b
surg1 nurse1 so wait we will see on the other side P3 e
surg1 nurse1 ok I think it works for me P3 e
surg1 nurse1 oh P3 e
nurse1 surg1 yeah there is a conflict there always E3 e
nurse1 surg1 can I remove it E2 a
surg1 nurse1 yes I think you can because we are leaving now E2 d
surg1 nurse1 remove the tools first E2 b
nurse1 surg1 yes, we need to remove the instrument first because if I remove that we will not have insufflation E2 d
surg1 nurse1 now I position the tools E2 b
surg1 nurse1 did you remove the scissors? E2 a
nurse1 surg1 yes E2 c
surg1 nurse1 can you give me the scissors E1 a
nurse1 surg1 there is the camera E1 d
nurse1 surg1 do you need to see? P3 a
surg1 nurse1 do I don’t need to see anything P3 d
surg1 nurse1 you can stop insufflation we will remove the camera E2 b
surg1 nurse1 its ok I got it E2 e
surg1 nurse1 can you move the robot backward E2 b
surg1 anesth if you want we can move the table horizontally E2 e
anesth surg1 that’s ok E2 d
7:29 surg1 nurse1 we will clean up E2 e
surg1 nurse talking about next case O e
nurse2 nurse3 oh it stopped working E3 f
nurse2 nurse3 turn on the power (accidentally turned off davinci and could-n't move arms to take off davinci cover) E2 b
Case 2, Prep: Time From To Verbal Data Verbal
Code Bowers Code
0:00 surg1 surg2 I want the arm to approach from this way, because if the robot is too close we'll have to approach from a different <this> way, and we can't reach the <operative site>
E5 e
surg1 surg2 so if the arms are right here, we can go there <indicates> E5 e
surg1 surg2
something about arm 3, it should end up here <indicat-ing>, and once its inside, we'll orient it this way <indicat-ing>
E5 e
surg1 surg2 we don’t want to approach this way, or else we'll see this
way, so we need to enter from this point <indicating> E5 e
nurse2 surg2 I am leaving the robot there for now, i., and we're going to catch it this way E5 e
nurse2 surg2 we're done E5 f
surg2 nurse2 wait, because we will need to test something E5 e
nurse2 surg2 ok, I'll push it a bit more E2 e
14:55 anesth1 nurse1 can I have the table controller? E1 a
nurse1 anesth1 yes, its on your left E1 d
15:25 anesth2 anesth1 is it okay? E2 a
anesth1
anesth2 yes, a bit more E2 d
surg2 nurse1 what is this tool used for? E4 a
nurse1 surg2 this one is going on this arm <a tool> E4 d
18:45 surg2 nurse2 we are going to leave it this way because… E4 e
nurse2 surg2 yes we need to move it in this way E2 e
nurse2 surg2 can you put the arm with the camera above? E2 a
nurse3 nurse2 you're not getting it closer right now <the robot>? E2 a

135
nurse2 nurse3 not right now, it depends on the <arm positions> E2 d
nurse2 surg1 the robot is ready, and we are just waiting for you to start
before we'd move it closer E5 e
nurse2 nurse3 no you don’t really need them but we can keep it anyway E4 d
nurse2 surg2 no, its not in the right direction <sterile sleeve for robot> E4 e
nurse2 surg2 you have to put it the other way E4 b
surg2 nurse2 oh im sorry E4 d
nurse2 surg2 no, no problem E4 d
nurse2 surg2 can you lift up the arm? E2 a 23:00 surg2 nurse2 I will try to put it back E2 d
nurse2 nurse3 yeah it was <eh> EE5 g
nurse3 nurse2 yeah it definitely took longer than before E5 g
nurse2 nurse3 he was constrained by a problem with the trocar between
arm 2 and a 3 O g
nurse3 nurse2 so actually it was on the side O g
nurse2 nurse3 yes, and there were 2 others on the other side, and there were a lot of conflicts O g
surg2 nurse2 ’'m going to put this one on <sterile sleeve on robot arm> E5 e
surg2 nurse2
I will need to look exactly where the robot is placed, be-cause ’'m trying to make a report on it in the medical jour-nal
O e
surg2 nurse2 yeah its always in this medical journal, I will just take <this> and remove the name of the patient O g
nurse1 surg2 later we will be able to pick up <something> in the other room E5 e
surg2 nurse1 yeah right now, nobody's using it E5 e 24:30 nurse1 nurse2 can you put it on the top? E5 b
nurse1 nurse2 can you put the arm a bit more this way? <wants to drape it> E2 b
25:50 nurse1 nurse2 thanks E2 g
surg2 anesth2 be careful with this, because we need to be able to go through here <or something will need to pass this way> E5 b
nurse1 surg1 <asked question> E5 a
surg1 nurse1 no we are just going to set up around there, and we'll just
wait for them E5 d
surg1 nurse2 do you have a pen? E1 a
surg1 nurse2 who operated on the patient before? P6 a
surg1 anesth2 do you still have stuff to do here? P5 a
anesth2
surg1 yes P5 c
anesth1 surg1 no, but we can leave now P5 d
surg1 anesth1 no, you do whatever you need to do P5 b 42:36 anesth nurse1 we will inflate the mattress E5 e nurse1 anesth then it will be ok E5 e nurse2 nurse1 you need first to deflate it before you inflate it again E5 b nurse1 nurse2 now its ok, its deflated E5 d nurse1 nurse2 I don’t know how ths one works E4 a nurse2 nurse1 whats wrong E4 a nurse1 nurse2 I am not able to move it up E4 d nurse2 nurse1 there is a clip on the other side E4 d nurse1 nurse2 here? E4 a nurse2 nurse1 no, down E4 d nurse1 nurse2 yes, here E4 a nurse2 nurse1 then you need to move it up E4 d
anesth1 anesth2 the patient is tall P6 f
nurse1 nurse2 we need to move her down P6 e nurse2 nurse1 ok P6 e nurse2 anesth2 only the sheet E2 e nurse2 nurse1 1,2,3 move E2 b
nurse1 anesth1 I need to get your aspy (ventilator?/suction?/ for insuffla-tion) E1 a
anesth1
nurse1 its on the other side E1 d
screen cam nurse2 anesth2 do you need more? E1 a

136
2 anesth2
nurse1 yes more E1 d
nurse2 anesth1 no I don’t think its enough E1 e nurse2 anesth1 no it doesn’t work? E4 a
anesth1 nurse1 yeah its ok E4 d
anesth1 nurse1 yeah it works E4 d
nurse1 anesth2 no it think it will be ok? E4 a
anesth2
nurse1 yes E4 c
surg1 anesth2 the robot will be positioned near the shoulder E5 e surg1 anesth2 do you need some help? E5 a
nurse2 anesth1 we also need to get more space here because this arm needs to be on that side E5 d
nurse2 anesth1 we will move the robot on that side E5 e surg1 nurse2 is everything ok now? E5 e
nurse2 surg1 we need to call <nurse1> and we need to move it on that side <the robot> E5 e
surg1 surg2 discuss another surgery O g
surg1 surg3 this problem with the robot is also present in classical celioscopy O g
surg3 surg1 yes sure, when we are in the same axis O g
surg1 surg3 here is more linked to the size of the instruments. When you are like this its ok, <showing> but here you have conflicts
O g
nurse1 anesth1 I will start to move her down, but just a little bit P6 e
nurse2 nurse1 we need to leave her horizontally to correctly position the trocars
P6 e
nurse1 nurse2 yeah I know, it’s just to avoid the fact that her feet hit the ground P6 e
nurse1 nurse2 I forgot <something> to attach E5 e surg1 anesth2 what did she forget? E5 a
anesth2 surg2 she forgot the <something to attach> E5 d
surg1 nurse2 position it correctly on the pubis E5 b
17:00 surg1 surg3
before that we work only on the pelvis, for the robot, you have the base, the arms move forward and the work is done towards the inside, and the arms came back to the base <showing>. In this case we will work in this direc-tion, that’s why we will position the base here, the arms will be positioned in this direction, and we will work to this direction. that's why its more cumbersome than usual
P3 e
surg1 surg3 explaining why they choose to work from this side and not the other side, some constraint in the anatomy P3 e
nurse2 anesth1 can we move the table down please E2 b
nurse1 nurse2 <connecting the camera> do I need to turn it or do yo have to?
E4 a
nurse1 nurse2 I feel its not well connected E4 d
nurse1 rep you can take it because I didn’t succeed in connecting it, because I don’t understand how it works E4 b
nurse2 rep no there is a problem E4 d rep nurse2 I will remove it to see if E4 e rep nurse2 we can try to turn it to see if… E4 e rep nurse2 because it was in closed position E4 e nurse2 rep we need to position it this way E4 e rep nurse2 I will check something else E4 e
nurse2 rep and if I try to position it, because maybe if we don’t have both at the same time its hard to connect them E4 e
rep nurse2 we'll try it on the other way E4 e surg1 nurse2 do you have a problem? E4 a nurse2 surg1 yes E4 c
rep surg1 as the last time, we aren’t succeeding in closing the con-nectors E4 e
surg1 rep last time we had some troubles also E4 e
nurse2 rep there is a little thing to do but I don’t remember what, last time I succeeded to make it
E4 e

137
rep nurse2 we can try E4 e rep nurse2 how can we proceed E4 a 24:00 surg2 nurse2 you are waiting for something? WF a
nurse2 surg2 yeah we are waiting for the rep who left to get some documentation WF d
surg1 nurse2 What’s the problem exactly? E4 a
nurse2 surg1 we had the problem with the camera like last time do you remember
E4 d
surg1 nurse2 yes yes with the camera E4 d
nurse2 surg1 we think there is a problem because we don’t succeed to connect it. Last time it was badly positioned, and this time w cannot connect it at all
E4 e
surg1 nurse2 at all? E4 a nurse2 surg1 yes E4 c
nurse2 surg1 we can do it like last week but it’s not a solution. It must work
E4 e
25:00 surg1 nurse2 we have that and we also have <something else>that doesn’t work E4 e
nurse2 surg1 but I found the solution for that E4 e
nurse2 surg1 because if you remember well we tried the other grasper and we got the same message, and we found that there was a triangle that was closed on the other side
E4 e
surg1 nurse2 ah ok E4 e
Case 2, Port Planning: Time From To Verbal Data Verbal
Code Bowers Code
30:39 surg2 surg1 Are you starting from the top P3 a
surg1 surg2 yes, but we can see it together P3 d
31:26 surg1 surg2
what ’'m proposing to save time is once we place the camera, we'll see what inside. The patient was operated on before, need to remove the scar tissue. Use the cam-era to see the scar tissues before placing ports. If there is scar tissue, we can put a bipolar hand tool inside
P3 e
32:09 surg1 surg2
After we place the camera, as the woman is only 56 kg, we will use the camera to see the upper side of her cav-ity. When you place the ports along the same line, there will be an instrument conflict/collision. (indicating) after we place here, we can place what we want
P3 e
32:19 surg1 surg2 talking about the 3rd port, where the robot arm will go - we will calculate where to put the …
P3 e
32:29 surg1 rep is this one number three? Or number two? <indicating> P4 a
rep surg1 number three P4 d
surg1 rep we will put number 2 here, which will be useful to work here P3 e
32:40 surg1 rep and then, port 3 will be useful for grabbing <anatomy> P4 e
32:47 surg1 rep and there will be no conflicts also, because last Tuesday we had a big conflict (with the tools colliding) P3 e
32:54 surg1 rep we won’t be so far and not on the same line for port 3 P3 e
surg2 surg1 and the tension ? (for the tissue) P4 a
33:01 surg1 surg2 because g. was there, and he had some difficulties, so this is bad P3 f
33:07 surg2 surg1 yes, because we are working on this area (indicating>, so we may <indicating to a certain area>
P4 d
surg1 surg2 this whole area - <limiting the work area> P4 e 33:17 surg1 surg2 ok, we will let the anesth finish their work O g
34:43 surg1 surg2 I hope there will be no problems, because we have a limited workspace P4 e
surg2 surg1 yeah P4 c
34:46 surg1 surg2 its not impossible to convert from robotic to laparoscopic (planning to convert if necessary) P3 e
surg1 surg2 yesterday, I was talking with the patient, and discussing
the object is to clean out the tumors P6 e
34:54 surg1 surg2 we will try to perform it robotically, but if not possible, we will convert P3 e

138
surg2 surg1 so the goal is cleaning out P3 a
surg1 surg2 yes, completely P3 d
35:03 surg1 surg2 so if we see that we are working slowly, and we progress normally, we will continue, but if we see that its not ac-cessible because of the scar tissue, we will stop it
P3 e
35:11 surg2 surg1 will you put the camera there? <indicates> P4 a
35:24 surg1 surg2
since we have bigger robotic arms, I will put it in between them, which is our working axis, with an arm on each side <indicating with hand motions>, because the problem of the camera is that we can only put one type of trocar, we cannot move it
P3 d
35:39 rep surg1 gives port placement guide, explaining it P3 e 35:50 surg1 rep discussing port placement sheet P3 e 35:53 surg1 surg2 we will put the ports more down P3 e 35:57 rep surg2 this is the standard? P3 a 36:00 surg2 rep yes that’s it P3 c
surg1 rep this is theory P3 a
36:05 rep surg1 this is just to show that you need triangulation P3 d
36:09 rep surg1
it shows the working area around the robot, so if we put it this way, we put the camera here <indicates>, both side arms will be in triangulation that permits work on this space there <pointing>
P4 d
36:27 surg1 surg2 must not put the second one there? So we can move it forward. What do you think about that?
P4 a
36:36 surg2 surg1 asks something <?> P3 a
surg1 surg2 yes, in fact, but we will see it when we are there P3 d
36:42 surg1 surg2 I don’t know, it will be <?> these instruments are so long, if the <indicating on body> junction is there, this will be like this <indicates>
P4 a
37:00 surg2 surg1 <something> <pointing on body> P4 a
surg1 surg2 yes, so we must not higher than that P4 d 37:03 surg1 surg2 do you see it lower? P4 a
37:08 surg2 surg1 no, but if we want to work in this area, this is 9cm <using ruler>, so if we focus on the interest zone, the interest zone is there <pointing>
P4 d
37:34 surg1 surg2 if the junction is there, then you have the nerve, you have all this stuff there, so if you want to clean it out P4 e
37:39 surg1 surg2 yes, yes P4 d
37:40 surg1 surg2 after that, we are there <second port>, the two that will serve to we have to put them on the sides, at least 6cm, but 6 is the minimum, so it can be 9cm
P3 e
38:06 rep surg1 consider the insufflation P3 e 38:15 surg1 surg2 and then we will put the assistant port here… P4 e
surg1 surg2 and then here we have <something>, we must not make
a mistake P4 e
38:27 surg1 surg2 she is tall so, we can put 9cm here, so we are there <points> P4 e
38:40 surg2 rep and last time we were blocked because the ports were on the same axis?
P3 a
rep surg2 yes P3 c
38:56 surg1 surg2 so where do you think we can put the last one? More forward? P4 a
39:09 surg2 surg1 shows where P4 c
surg1 surg2 yes P4 c
39:40 surg1 surg2 so this is number 3, this is number 2, we have 9 cm be-tween each one. And here we'll put another one <indi-cates>
P4 e
surg1 surg2 do you think this is helpful to do that? Or should we go ahead with the first solution? P3 a
surg2 surg1 yes, yes P3 c 39:50 surg1 surg2 actually, because we can have some surprises there P3 e
Case 2, Docking: Time Who To Who Text VE
Code Bowers Code

139
2:09 nurse2 nurse4 get closer E5 b 2:10 n3 n4 talking about how to move arms E5 e 32:00 surg1 nurse2 so, WF e rep nurse2 now you need to move it the other direction E4 b nurse2 I need to bend the arm E4 d rep nurse2 you can move it up if necessary E4 b nurse1 nurse2 you need to bend the arm E4 b surg2 nurse2 be careful while moving it <surg light in the way> E4 b surg2 rep can you move the light because it will constrain me E4 a nurse2 rep move the arm from the left, to turn it inside? E4 a rep nurse2 you need to place the elbow of the arm on the axis E4 d surg1 nurse2 let’s go P3 e 34:42 nurse2 rep completely folded in? E4 a rep nurse2 yes, but this one needs to be on the other side <indicat-
ing>, because arm 3 is there E4 d
surg1 surg2 this is very important, i.. On the side where there is only one arm,
E4 e
surg2 surg2 this one, ah ok. the one with the blue (tape) on the knee joint.
E4 e
surg2 surg1 after that, will you turn it on once you've docked? E4 a surg1 surg2 yes E4 c rep nurse2 as high as possible E4 d nurse1 surg1 we will try to come like this? <indicates> E4 a surg1 nurse1 yes, because we need to put the camera here on this
trocar E4 d
nurse1 surg1 so I need to go this way <showing> E4 a surg1 nurse1 yes, this way will be okay <showing>. Exactly the same
thing we did in previous surgery E4 d
surg2 surg1 like this? E4 a surg1 surg2 yes, but not too much on this side. Here on the axis E4 d surg1 nurse1 go backward. Wait. Position yourself on your left. E5 b sueg1 nurse1 move forward. E5 b surg1 nurse1 move backward, and watch the cables E5 b surg1 nurse1 stop, and now.. E5 b position yourself completely on your left E5 b stop E5 b very good E5 e nurse1 surg1 wait, I think I will do it by myself. I will come back forward E5 e surg1 nurse1 you aren’t so bad, so move forward E5 b nurse1 surg1 do you think it’s ok like this? E5 a surg1 nurse1 move forward, move forward E5 d nurse1 surg1 more this way? E5 a surg1 nurse1 don’t worry, we will maneuver again E5 d surg1 nurse1 move forward E5 b 36:36 surg1 nurse1 stop E5 b surg1 nurse1 now move backward. E5 b surg1 nurse1 you need to move forward by going to your right. E5 b surg1 nurse1 now to your right, this is your left E5 b surg1 nurse1 good, move backward E5 b surg1 nurse1 to your left now E5 b surg1 nurse1 your left, your left E5 b surg1 nurse1 it’s ok, keep going E5 b surg1 nurse1 stop E5 b surg1 nurse1 and now, you need to E5 b surg1 nurse1 stop E5 b surg1 nurse1 now position yourself on your right and move forward
toward us E5 b
surg1 nurse1 stop E5 b surg1 nurse1 it’s not so bad E5 e nurse1 surg1 and now, move forward? E5 a surg1 nurse1 I think so, move forward, yes. E5 d surg1 nurse1 stop E5 b surg1 nurse1 I think it’s better to be there (points) E5 a surg2 surg1 yes I think so E5 d surg2 nurse1 you need to <indicates> E5 b nurse1 surg2 do you want me to move backward this way E5 a

140
surg1 surg2 yes, but in my opinion, she need to be more horizontal, don’t you think so? B.?
E4 a
surg1 rep if we make her move backward, we need to position this arm here.
E4 d
rep surg1 we need to move this way <indicating> E4 b nurse1 surg1 is it okay now? E4 a surg1 surg2 joking O g surg1 rep why can’t I move the arm down? E4 a surg1 rep ah, I know why E4 d 38:00:00
surg1 nurse2 asks about the "ailettes" connection piece for arms/trocars E4 a
nurse2 surg1 yes they are open E4 d surg1 surg2 ok, I'll go E5 e surg1 surg2 here, you have to be careful about that E5 e nurse1 surg1 don’t you want to position it more like this? <indicates> E4 a surg1 nurse1 yes if you want, why E4 d rep surg1 to make it come like this <indicating> E4 e surg1 rep and for what reason? E4 a 38:44 rep surg1 so that arm 1 "arrives" like this <showing> E4 d surg1 rep yeah, ok ok. E4 c rep surg1 the problem is that we are concentrating too many arms in
one area E4 e
surg1 nurse1 this case you need to move backward E4 b 40:09 surg1 nurse1 no in the other direction E4 d rep nurse1 like this, you need to enter in this corridor E4 b surg1 nurse1 that’s good, now turn the other direction E5 b rep nurse1 now keep straight backward E5 b surg1 rep ok stop E4 b nurse1 surg1 and now I need to turn this way? E4 a surg1 nurse1 yes that’s it E5 d surg1 nurse1 move forward E5 b surg1 nurse1 stop E5 b surg1 surg2 is it okay, did you close it <refeffing to locking the arm to
trocar> E5 a
surg1 rep so, dear B… E5 e surg2 surg1 here, typically between number 2 and number 3 E5 e surg1 rep so will we put number 3 on the other side? E5 a rep surg1 yes E5 c surg1 rep and we will put number 1 here E5 a rep surg1 yes E5 c surg1 rep yeah I think we will improve E5 f rep surg1 you should put it more horizontally E5 b surg2 surg1 should we put the camera in now, no? E5 a surg1 surg2 now immediately? E5 a surg1 surg2 yeah, we can put it in for you if you want E5 d surg1 surg3 explains how to install arms. Yes like this very good. Now
close the latch. E4 b
nurse2 surg2 you see that’s the one for the camera and you need to put it on this side <pointing> because right now its on the other side
E4 e
nurse2 surg2 this arm, I. <showing> E4 b nurse2 surg2 there will be a conflict between number 1 and number 3 E4 e surg2 nurse2 can anyone start the insufflation P1 b 45:45 nurse1 surg2 yes, ah yes P1 c nurse1 surg2 its ok like this, right? E4 a surg2 nurse1 yes E4 c surg1 rep there is something new, because we cannot close the
latches E4 f
rep surg1 you need to push the arm to the right E4 b surg1 rep no, this is not the solution E4 d surg1 rep I am frustrated E4 g surg1 rep wait, now it’s ok, I think E4 f surg1 ok that’s it E4 d rep surg1 ok now you need to position it on the working axis be-
cause the camera will be oriented like this E4 e
surg1 rep we will put in our instruments first? E4 a

141
rep surg1 no, you need to position the arms first to be in a good position
E4 d
surg1 rep the problem is that we don’t know where the instrument will be inside, you put your instrument in first, no?
P4 a
rep surg1 but the configuration of the arms E4 d surg1 rep this one? E4 a rep surg1 no, this one, you need to be on the working axis E4 d rep surg1 it needs to be oriented like this, because we will work
towards the head of the patient P4 d
surg1 rep now it’s not the case because its good, no? E4 a rep surg1 this arm needs to be like this <indicates> E4 d surg1 rep which arm? E4 a rep surg1 this one E4 d surg1 rep this joint? E4 a rep surg1 yes this joint needs to be on the axis. It needs to be ori-
ented toward the direction we want to go (work) P4 d
surg1 rep do we need to move it backward E4 a rep surg1 no we just need to push it by pushing the button to that it
is positioned on the working axis E4 d
surg1 rep like this? E4 a rep surg1 exactly c surg1 surg2 maybe we need to … I think for the setup, we need to
move the screen up E2 a
surg2 surg1 yes, we'll move the screen up E2 d surg1 surg3 this one is not good E2 f nurse1 surg1 I put it on "13" (level) E2 f surg1 nurse1 actually we need a trocar. V.? E1 a 48:50 surg1 nurse1 do you have trocars for next time? 5 12 without blades
"ailettes" E1 a
nurse1 surg1 ah yes, wait E1 d rep surg1 or we can put an "8" (size) trocar on an arm and then put
the insufflation E1 d
surg1 surg2 ok E5 c surg1 surg2 that’s it E5 f surg1 surg2 so we know that we need to go this way (moving camera),
after that, the instruments… P3 e
surg1 surg2 we need to finish the setup with more instruments <some-thing> on <something>, but we don’t have any instru-ments here
E1 e
surg1 nurse1 can I have an instrument E1 a surg1 surg2 so what can we put here? E1 a nurse1 surg1 I have pro-graspers and scissors E1 d 1:35 surg1 nurse1 we will need a bipolar at any moment E1 e 1:44 nurse1 surg1 do you want it now? E1 a surg1 surg2 yes, why not, because we will grasp it now and we need
to coagulate, so we should put the scissors in now? E1 d
surg2 surg1 yes E1 c surg1 surg2 we will start here (at this position), and then we will move
up? P4 a
surg2 surg1 yes P4 c surg1 surg2 so this is the arm P4 a nurse1 surg1 this is the maryland P4 d surg2 surg1 do you want me to look for the other arms? P4 a 3:00 surg1 surg2 and for the instrument, what will we put here? P3 a surg2 surg1 maybe the scissors P3 d surg1 surg2 yes, maybe the scissors P3 e surg2 surg1 I don’t know if I am pushing it inside E4 a 4:15 surg2 nurse2 can I have a scalpel? E1 a surg2 surg1 its okay here P3 d 5:42 surg1 surg2 you are ok at the skin level P3 d surg2 surg1 am I inside here? P4 a surg1 surg2 yes you are inside, you are too deep <moves trocar out a
little> P4 d
surg1 surg2 ok its better now P4 e 6:08 surg1 surg2 here you are able to see the landmarks <anatomy>.
When she is insufflated. Here is <anatomy>, and here you are above, you are between, you are looking at the back-
P4 e

142
side of the illiac artery surg2 surg1 yes I recognize it P4 e surg1 surg2 because here you have the external one P4 e surg2 surg1 yes, yes P4 e surg1 surg2 so if we really want to do something with the lower side… P4 e 8:30 surg1 surg2 ok, did you put the scissors inside here? E1 a rep surg1 you need to remove the cover E2 b surg2 surg1 it’s in this direction? P4 a surg1 surg2 no, but we will start here, as far as possible or maybe at
the middle P4 d
surg2 surg2 is it ok now? P4 a surg1 surg2 yes, because after we can progress P4 d surg1 nurse1 I am missing an instrument to put here, give me a grasper E1 b surg1 nurse1 wait, I will try to see where the trocar is first P4 e surg1 rep I have reached the max insertion of the tool here (horizon-
tal positioning)? E4 a
rep surg1 to go down? E4 d 9:30 surg1 rep no to make it more horizontal. I mean, you don’t touch
anything of this, but making it more horizontal. E4 e
surg1 rep you see? E4 a rep surg1 if you continue you can reach it E4 d surg1 rep yes but here we will brush the patient inside E4 a rep surg1 so you need to remove the tool, move the arm, and put in
the instrument again E4 d
surg1 surg2 oh, its not so bad here E4 e surg2 surg1 do you have a bipolar here? E4 a surg2 surg1 which one is the bipolar? E4 a surg2 surg2 and which one is the grasper? E4 a surg2 surg1 and one is sharper E4 f surg1 surg2 the one that is the closest to us E4 d nurse2 surg2 the maryland is a little bit sharp E4 f rep surg1 this is perfect. The only change is that this one needs to
be on the axis P3 e
surg1 rep ok, we can try now P3 e 10:10 rep surg1 the idea will be to get this joint on the axis, because oth-
erwise we risk having a conflict with arm 2 E4 e
rep surg1 if we look at <showing the paper>… E4 e surg1 rep no, no, show me on the machine E4 b rep surg1 we need to push this joint so it is on the axis <showing> E4 d 10:30 rep surg1 to put the camera in this position E4 e surg1 rep do I need to try to move it so we can see our whole field
of fiew? E4 a
surg1 surg2 can you move your arm down (robot arm)? E4 a surg1 surg2 again, again, again E4 b surg1 surg2 ok that’s it <stopped docking> WF e surg1 surg2 ok, its 11:06 WF e surg2 surg1 but here we didn’t put, do you want me to put the assis-
tant port? P3 a
surg1 surg2 yes, you need to push this blue button here E4 d surg2 surg1 do you want me to put it here? P4 a surg1 surg2 yes, at the same level as the other ones P4 d rep surg3 you need to push once to unlock the arm (for moving)
when it is blinking blue, you can move it however you want.
E4 b
surg2 surg1 wait wait, <he started manipulating the arms from the console>
P3 b
surg2 surg1 I didn’t put in the trocar yet, now I cannot see <he moved the camera>
E4 f
13:00 nurse1 surg1 one moment E4 b 14:23 surg2 surg1 ok that’s it E4 d
Case 2, Console:

143
Time Who To Who
Text VE Code
Bowers Code
2:40 surg1 nurse2 can I have the monopolar for the scissors E1 b
nurse2 surg1 yes its already there E1 d
surg2 nurse3 can you lower the screen E2 b
2:43 surg1 nurse3 can you lower the assistance for the scissors E2 b
nurse3 surg1 yes E2 c
nurse3 surg1 we put it at 30 E2 d
surg1 surg2 I. O g
surg2 surg1 yes O g
surg1 surg2 if you get <something> bigger than the other <something> O e
surg2 surg1 I seem to have fat in the retro calycene P4 a 2:45 nurse2 surg1 isn’t that the aorta? P4 a
surg1 nurse2 yes P4 c
surg1 surg2 we should start seeing something big? P4 a
surg2 surg1 well I think we are seeing the aorta P4 d
surg1 surg2 yes P4 c
surg1 surg2 yeah, yeah, maybe P4 c 2:47 surg2 surg1 we are in the right area P4 e
surg1 surg2 is it normal that the noise stopped? E4 a
surg1 surg1 so…ok (talking to self while operating O g
surg1 surg2 this is where … E4 e
surg2 surg1 totally, yeah E4 e
surg2 surg1 explaining where to grasp P2 e
surg1 nurse3 should I start cutting here? P2 a
nurse3 surg1 yes P2 c
surg1 nurse3 thanks P2 c
nurse3 surg1 You’re welcome P2 c
nurse3 surg1 maybe you should get more on the edge of it P3 b
surg1 nurse3 you mean almost there P3 d 2:49 nurse3 surg1 yes, totally P3 d
surg1 nurse3 asking for directions P4 a
nurse3 surg1 you can actually go directly to 7:00 (on clock face direc-tions) P4 d
surg1 surg2 is it this kind of tissue <names tissue type> P4 a
surg2 surg1 oh yeah, you have the artery there P4 d
surg1 surg2 wait, because if this is the aorta, and the artery is on this side, it means im not … P4 a
surg1 surg2 so this is not the aorta actually P4 a
surg2 surg1 discussing which one is aorta vs artery P4 d
nurse3 surg1 discussing which one is aorta vs artery P4 d
surg1 nurse3 well look if the aorta is this … P4 a
surg2 nurse3 discussing which one is aorta vs artery P4 d
nurse3 surg2 discussing which one is aorta vs artery P4 d
surg2 surg1 go back to 7 o clock to cut but first you need to push this or
else we won’t notice if we are on the good way P2 b
nurse3 surg2 yeah this is the ureter, I think he is suturing it P1 f
2:51 surg1 nurse3 can you tell me if I am on the right way because I haven’t seen the ureter P4 a
surg1 nurse3 so what you want is for me to suture it myself, right? P1 a
nurse3 surg1 no its sure to be the ureter P4 d
nurse2 surg1 yes the ureter is around 8 o clock, P4 d
nurse2 surg1 yes exactly that, you are right P1 d
nurse2 nurse3 you can see the ureter really well P4 f
surg1 nurse3 you see its really convincing P4 f
surg1 all what is everyone doing after <the surgery> O g 2:55 surg1 surg2 you haven’t put this tool yet P3 a
surg2 surg1 the grasper? P3 d
surg2 surg1 we need to try to get some room, clean the artery before P3 e
surg1 surg2 its difficult to be really straightforward with it <the robot> P3 e
surg1 surg2 I think this is the aorta because there is this thing there P4 a
surg2 surg1 it must be <horizontal / vert > P4 d
surg1 surg2 you can totally see it here P4 f
surg2 surg1 no no, you should go the opposite way P3 b
surg1 surg2 oh you mean like upward P3 d
surg2 surg1 no the opposite, downward P3 b

144
surg1 surg2 yea, but normally I would already see it P4 d
surg1 surg2 yeah that’s weird P4 e
surg1 surg2 oh no actually wait, its here P4 e
surg1 surg2 its here P4 e
surg1 surg2 yeah I think this is the aorta, but I am not seeing it really well P4 e
surg1 surg2 I think I am only seeing part of it P4 e
surg2 surg1 yeah, I am right there but you are not seeing me <with assistant port> P4 e
surg1 surg2 pull it up P2 b
surg1 surg2 do it P2 b
surg1 surg2 we cut it, or do you want to pull it up a bit more P2 a 3:00 surg1 surg2 we are okay? P2 a
surg1 surg2 do you agree, I.? P2 a
surg2 surg1 yep P2 c
surg1 surg2 is this <something>? P4 a
3:02 surg1 surg2 the higher we will go, the easier it will be for you to help me P3 e
surg1 surg2 yeah P3 e
surg1 surg2 how are we going to arrange it P3 a
surg2 surg1 looking for graspers P2 e 3:03 surg1 surg2 I think the aorta is there P4 e
surg1 nurse2 can you grasp a bit of it (tissue) P2 b
nurse2 nurse4 it will be good if I can have new gauze E1 b
surg1 rep I think this is the <anatomy> P4 a
rep surg1 yeah we see it really good P4 d
surg2 surg1 yes P4 c
surg3 nurse2 there is café au lait (another surgeon in room) O g
nurse2 surg3 what? O a
surg3 nurse2 there is café au lait coming out of the belly O d 3:06 surg1 surg3 P.? O a
surg3 surg1 what O d
surg1 surg3 its not normal O a
surg3 surg1 no its not O d
surg3 surg1 from a scatological point of view, it doesn’t seem normal O e
surg3 nurse2 keep track of the bfn P6 b
nurse2 surg3 yes P6 c
surg1 surg2
so this is the part that will be interesting for I., because we are in the second part of <something - procedure or anat-omy>
P3 e
surg1 nurse3 this is not co-something grasper? E4 a
nurse3 surg1 no its not E4 d
surg1 nurse3 hello? E1 a
nurse3 surg1 yes yes, it is there E1 d
surg1 nurse2 right now we should be in the space between <something> P4 e 3:09 nurse2 surg1 you are getting closer from the left part of the aorta P4 e
surg1 nurse3 can you come here P3 a
surg1 nurse2 can you come here please P3 a
surg1 nurse2 can you hold this ? (leaves) P3 a
surg1 all what is stupid is that … O g
surg1 surg2 I.? O a
surg2 surg1 yes? O c
surg1 surg2 can you please … P1 a
surg2 surg1 suction? P1 c
surg1 surg2 the liquid P3 a
nurse2 surg1 I think I did not do a good job with the trocar P3 a
surg1 nurse2 really what do you mean? P3 d
nurse2 surg1 yeah totally, it looks like if … P3 e
nurse2 surg1 its ok but could have been better, it should have been in the same direction as the instruments and not rotated P3 e
surg1 nurse2 yeah because right now it is messing with us and it am
totally lost P3 e
surg1 nurse2 I will still try to do it P3 e
surg1 nurse2 oh, yeah, of course that’s it, it’s right there P3 e
surg1 nurse2 ok I understand P3 e
nurse2 surg1 is it okay? P3 a
surg1 nurse2 yeah there is no problem anymore, I am the problem P3 d

145
surg1 nurse2 I didn’t understand that we are that way P3 a
nurse2 surg2 yeah I think if we follow the aorta, we will surely find … P3 d
nurse2 surg2 this is shady because I don’t know if … I mean it’s really … P3 g
surg2 nurse2 this is not really problematic (looking at screen) P3 e
surg1 surg2 we should get ready before orienting all the stuff P3 b
3:14 surg2 surg1 yes, this is an important artery so that’s why its more diffi-cult P3 d
surg2 nurse2 is he going to the left or to the right P3 a
surg1 surg2 yes look the liver is here P4 b
surg1 surg2 so since the liver is here, if we continue, we go directly to the ligament <name of ligament>, which means we are to the right
P4 e
surg1 surg2 the problem is, since she has already been operated on .. P4 e
surg2 surg1 yeah, yeah P3 c
surg1 surg2 I., we should pass soon the aorta, prepare yourself psycho-logically P3 b
surg1 nurse3 can you see <?> P3 a
nurse3 surg1 no P3 c
surg1 nurse3 oh I thought I did P3 e
nurse3 surg1 yeah, it happens sometimes, it feels like it, but there is definitely a space P3 e
surg1 nurse3 yeah I don’t know if … P3 e
nurse2 surg1 yeah I don’t know if it is because <?>, but I don’t under-stand, it feels like its going to the left, but there is only one P3 e
nurse2 surg1 I am lost P3 e
nurse2 surg1 I am lost P3 e
surg1 surg2 so we are on the aorta P4 e
surg2 surg1 you will lower it to be able to orient yourself better? E2 a
surg1 nurse2 and now we are good right E2 d
nurse2 surg1 yeah so this is the artery P4 a
surg1 nurse2 this is the artery, this is ligament, and this is the aorta P4 d
nurse2 surg2 this is the artery P4 f
nurse2 surg2 these are the suturing knots E1 f
nurse2 surg1 and can you look a bit to the left P3 b
surg2 nurse2 we should check to the left? P3 a
nurse2 surg2 yes to the left P3 d
nurse2 surg2 up yeah, here it is P3 f 3:17:08 surg1 surg2 here you are at the level of <something> P4 f
surg1 surg2 and there you just have to move a bit to find the aorta, no? P3 a
surg1 surg2 or is it something that opened, because its really thin P4 a
surg1 surg2 did it open because it was really thin or was it already there before? P4 a
surg2 surg1 I don’t know P4 d
surg1 surg2 and you see what I mean, this <indicating>? P4 a
surg1 surg2 its blue under, P4 d
surg2 nurse2 maybe it will be better to the left P4 e
nurse2 surg2 he could also go look under P4 e
surg1 surg2 we are following the aorta axis, and this is the artery P4 e
surg1 surg2 because you have an branch there and so here is the aorta P4 e
surg1 surg2 and you see the other branch there P4 e
surg1 surg2 you see? P4 a
surg2 surg1 mhmm P4 c
surg1 surg2 no? P4 a
surg1 surg2 I think this is the artery P4 d
surg1 surg2 and now we just put <something> for the aorta P4 e
surg1 surg2 from there to there P4 e
surg1 surg2 I can't go further P3 e
surg1 surg2 would it be possible to move one of them so that I can
access the grasper E2 b
surg2 surg1 yeah E2 c
surg2 surg1 yeah I can try E2 d
surg2 surg1 but it will be difficult E2 d
3:23 nurse2 surg2 you can put it between these two graspers, but internal P3 e
surg2 nurse2 or maybe you should lower it E2 e
nurse2 surg2 oh no look P3 e
surg1 surg2 it’s not at the same latitude than as this area P3 e

146
surg1 nurse3 is B. around here? E4 a
nurse3 surg1 wait I'll get him E4 d
rep surg1 because the grasper is … E4 a
surg1 rep yep E4 c
surg1 nurse2 which one is it, is it the third one E4 a
nurse2 surg1 yes it’s the third one E4 d
surg1 nurse2 yes because … wait so which one is this tool? E4 a
nurse2 surg1 it’s because it’s not internal E4 d
surg1 nurse2 I will need you to do it like this E4 b
nurse2 surg1 oh yes, it’s on this side? E4 d
surg1 rep no no no, actually the right arm I can’t use it right now be-cause the objective was for it to go to the bottom of the lady and right now it is around there
E4 e
rep surg1 yes we have to take it back E4 e
3:24:50 surg1 rep so we'll take it back and put it more on this side and hope-fully we'll manage this way E4 e
surg2 rep is it okay bertrand? E4 a
rep surg2 yes because right now its oriented to work on that side E4 d
surg2 rep so can I pull it off to check E4 e
surg1 surg2 so there you have … <something> … isa E4 e
rep surg2 press the blue button to get it E4 b
surg1 surg2 so that you can take control E4 b
surg2 surg1 yeah but I don’t have any bearings (lost). I am lost. P4 d
surg1 surg2 I think you will see it better at the console P4 b
surg1 surg2 I cant even see where are the left and right P4 d
surg1 surg2 if you can see the aorta, it will be easier P4 e
surg2 surg1 no even with the aorta I will not be able to orient myself P4 e
surg1 nurse2 go further E2 b
surg1 nurse2 stop E2 b
surg1 nurse2 so wait … E2 g
surg1 nurse2 you keep this grasper and do it like this E4 b
surg1 surg2 I.? P3 b
surg2 surg1 yes? P3 c
surg1 surg2 actually do you see this is the aorta we are at the level of
the liver P4 a
surg2 surg1 the left? P3 d
surg1 surg2 the right? P3 a
surg1 surg2 yes P3 c
surg1 surg2 we have the aorta there and we have the bifurcations of the
aorta … until there ... P4 e
surg1 surg2 then it goes up P4 e
surg1 surg2 and we can see that it goes in the direction of the ligament P4 e
surg2 surg1 yes P4 e
surg1 surg2 and so we are arriving in the area of this artery P4 e
surg2 surg1 and you don’t see the left side? P3 a
surg1 surg2 the left side is here P3 d
nurse3 surg1 no P3 c
surg1 surg2 I mean right side, right side P3 e
surg2 surg1 yeah but we need to see the left side P3 e
surg1 surg2 yeah but we need to do one thing at a time P3 e
surg1 surg2 we still need to see the left side P3 e
surg2 surg1 yeah P3 e 3:28 surg1 surg2 now I would like to start seeing the <something> there P4 e
surg2 surg1 we see it better P4 e
surg1 surg2 are you going to make it, will you be okay? (surgeons
switching places at console) O a
surg1 surg2 are you already sitting down? O a
surg2 surg1 yes I am O d
surg1 surg2 no no, don’t move O b
nurse2 nurse3 talking about moving the camera E2 e
surg1 surg2 hey! O g
surg1 surg2 wait, I.? O a
surg2 surg1 yes? O c
surg1 surg2 no no, its okay, just go. O b
surg1 surg2 Its just that I was thinking at your left it can’t be bifurca-
tion/branching P4 e

147
surg1 surg2 it must be the illiac from the left going down and the right going … I mean the illiac from the left going up and the invert going right
P4 e
surg1 surg2 and this is the aorta P4 e
surg1 surg2 these are the scissors E1 e
surg2 surg1 oh yes E1 c
surg1 surg2 here you go E1 e
surg1 nurse2 at some point we can try to push this one for I. P3 e
nurse2 surg1 do you want me to move the camera? E2 a
surg1 surg2 wait a bit I. P3 b
surg1 surg2 wait don’t move P3 b
surg1 surg2 going to push it and put it on the block in the back side P3 e
surg1 nurse2 or else we can free some space there P3 e
surg2 surg1 and so now I take back the other grasper? E4 a
surg1 surg2 press with your left foot laterally E4 d
surg1 surg2 you need to do it laterally E4 b
surg1 surg2 you see the kind of leash that you have near your left foot? E4 a
3:31 surg2 surg1 I can’t deal with the adherence if I have these two instru-ments
E4 d
surg1 surg2 oh, you can change instruments if you prefer E4 e
nurse3 surg2 and we can also change the place of the instruments E4 e
nurse3 surg2 you need to penetrate from … E4 e
surg1 surg2 it is the peritoneum adhering to the internal surface of the aorta because someone else has already been there be-fore us
P4 e
surg1 surg2 ok like that P3 e
surg1 surg2 hold on, be careful P3 b
nurse2 surg1 I am going to penetrate … P3 d
surg2 surg1 I would like ot have two hands and each arm too E4 e
surg1 surg2 wait, stop on this side and we are going to change the instrument E1 b
surg1 surg2 let’s change the instrument E1 e
nurse2 surg2 where do you want to grasper? Do you want it instead of the scissors? E1 a
surg2 nurse2 can I have the grasper on the blue one? E1 a
surg1 nurse2 ok remove the scissors and put in the grasper instead E1 d
nurse2 surg1 I will connect the grasper instead E1 e
nurse2 surg2 I am going to remove <something> E1 b
surg1 nurse2 no! E1 c
nurse3 nurse2 no! E1 e
surg1 nurse2 we are going to remove the scissors and put them on the
table, and you put another grasper in E1 e
nurse2 surg2 I’m removing the scissors E1 e
surg1 nurse2 a third grasper E1 e
nurse2 surg1 this kind of grasper? E1 a
surg1 nurse2 yes E1 c
surg1 surg3 we disconnected the scissors E1 e
surg1 surg3 we are not supposed to be at the aorta, but … P4 e
surg1 surg2 the third grasper is coming E1 e
surg2 surg1 there there is an artery P4 f
3:34 surg1 surg2 I wonder if we should lower it closer to the other P3 a
surg2 surg1 yeah that’s what I would like to see P3 d
surg1 surg2 wait, because what are you freeing right now P3 a
surg2 surg1 it must be the artery P4 d
surg2 surg1 I don’t really manage to see/grasp P2 a
nurse2 surg1 yeah I think the artery is there P4 d
surg1 surg2 the rubbing/scraping is working well P2 e
surg2 surg1 is it scraping? P2 a
surg1 surg2 its sticking E4 d
surg1 surg2 the tools are dangerous E4 f
surg2 surg1 are you afraid because I am the one doing it E4 a
surg1 surg2 no I was afraid since the beginning E4 d
nurse2 surg2 yeah that’s why he's asking you to do it E4 e
surg2 surg1 why did it shake (the camera) E4 a
surg1 surg2 its because you are touching the camera E4 d
surg2 surg1 yeah but that’s not supposed to happen E4 a

148
surg1 surg2 yeah, now you understand E4 d
surg1 surg2
I., B. is going to give you some advice about how to move the tools because its better if you make wide gestures because its translated as small gestures and it gets more accurate
E4 e
rep surg2 is it ok if I give you some advice E4 b
rep surg2 giving tips about how to make it more precise E4 b
3:3 surg1 surg2 while you are doing that, we can prepare the other tools for you E4 e
rep nurse2 can you stay focused on the important part? E4 a
surg1 nurse2 can you move it a bit in this direction P3 b
surg1 rep B., can we move this joint of the arm in that direction? E1 a
nurse2 surg1 if I do this, I can’t put it in the right direction E1 e
surg2 surg1 do you want to take back control? O a
surg1 surg2 yeah sure O c
surg1 surg2 we are going to try and free a bit more P3 e
surg1 surg2 you can start now P3 e 3:38 surg1 surg2 as for the cancer cells, they are … P3 e
surg2 surg1 there P3 e
surg2 surg1 now we have cleared the artery quite well P4 e
surg2 surg1 it’s there P3 e
surg2 rep it looks like the movement hurts more P3 e
rep surg2 how is it? P3 a
surg2 rep its worse P3 d
rep surg2 yeah it seems like it is P3 f
3:39 surg2 rep we will need to put it back as it was before P3 e
surg2 rep there is too much cyano when I try to separate E4 e
surg2 rep do you see what I mean E4 a
rep surg2 yeah I think they might be too close to the camera E4 d
surg2 rep yeah I think they might be too close to the camera E4 d
nurse2 surg2 yeah im going to pull back the camera, it will free some space for you E2 b
surg2 nurse2 yep E2 c
surg2 nurse2 yeah now there is a problem there is… P3 a
nurse2 surg2 you are between <anatomy> and <anatomy> P4 d
surg2 nurse2 so it will mean that <anatomy> will be there <pointed with tool> P4 a
3:41:15 surg2 nurse2 now can we cut or not P3 d
surg2 nurse2 I don’t know I feel like I am rolling the dice P3 a
surg2 nurse2 yeah that’s why I am asking for J.M. P3 d
nurse2 surg2 nope, he isn't here P3 d
nurse2 surg2 is the problem that you have trouble looking at it P3 a
surg2 nurse2 yeah I just can’t see it P3 d
nurse2 surg2 maybe I can orient the #2 differently <robotic arm> E2 e
surg2 nurse2 yeah I really can’t see anything P3 e
nurse2 surg2 yeah that’s what I was saying, maybe I can reorient the number 2 closer to the right arm? E2 d
nurse2 surg2 do you want me to try E2 a
nurse2 surg2 don’t move I am trying E2 d
surg2 nurse2 now I still don’t see anything P3 e 3:42 rep nurse2 maybe we should use the 30 E1 a
nurse2 rep yeah I was thinking of doing it but I don’t know if… E1 d
nurse2 rep if I put it like this, you should have more space for the three
of them P3 e
surg2 nurse2 ok what I am going to go is that honestly I will just ask to stop it P3 e
nurse2 nurse3 is he back yet? O a
nurse3 nurse2 not yet O d
nurse2 nurse3 yeah he's coming O d
surg1 surg2 so have you already done everything? P3 a
surg2 surg1 nothing P3 c
surg1 surg2 huh? P3 a
surg2 surg1 yeah I can’t orient myself at all, it’s not … P3 d
surg1 surg2 its not the same patient? P3 a
surg2 surg1 yep P3 c
surg1 surg2 oh sorry I didn’t notice that you actually stopped already P3 e

149
surg1 surg2 so I will just come take it back P3 e
surg2 surg1 yeah I don’t know where I am I just can’t orient myself P3 e
surg1 surg2 ok so wait, we are inside the inflation? P3 a
surg2 surg1 the artery is there P4 d
surg1 surg2 she's pouting P4 e
surg1 surg2 so ok we are there P4 e
surg1 surg2 ok so wait, what I am going to do first, I’m going to do this
one P3 e
3:45 surg1 surg2 you see I. after a while you don’t need your land-marks/guides to see where you are, you just know P3 e
surg2 surg1 yeah but I am too afraid, even right now I wouldn’t do it like
you are doing P3 e
surg2 surg1 yeah an furthermore, couldn’t go to the left P3 e
surg1 surg2 you want to go to the left, it’s a conservative point of view P3 e
surg1 nurse2 oh, now I've done <something> let’s hope it works because the next step is euthanizing P3 e
nurse2 surg1 oh at least I will be useful for something P3 e 3:46 surg1 nurse2 so now we are reaching the end <the right spot?> P3 a
nurse2 surg1 yes P3 c
surg1 nurse2 so what I am proposing we are doing … P3 e
surg2 surg1 so we don’t … <?> P3 g
surg1 surg2 yep, exactly, because … P3 g
surg2 surg1 yeah we don’t <?> but the thing is that we know well how you are and you will want to try anyway P3 e
surg1 surg2 yeah but if you help put me right on the artery, I would have done it already P3 e
surg2 surg1 yeah it seems it is truncated P3 e
surg1 surg2 yeah truncated, it’s because that’s how you see she has been operated on before P3 e
3:47 surg2 surg1 discussing that she didn’t see anything, it looks simpler now, but was different when she was in the console and the camera being so close was a pain
P3 e
surg1 surg2 yeah but that’s weird, because right now, it doesn’t trouble
me at so I think it must be because of the location P3 e
surg1 surg2 yeah its starting to get long, its starting to piss me off P3 e
surg1 surg2 <something> woo! O g
surg1 nurse2 is I. still there? O a
nurse2 surg1 no, she left already O d
surg1 nurse3 S.? O a
nurse3 surg1 yes im still here O d
surg1 nurse3 S.? O a
nurse3 surg1 yes O c
surg1 nurse3 S.? O a
nurse3 surg1 yes O c
surg1 nurse3 can you remove this thing? P1 a
nurse3 surg1 yeah but the problem is the trocar is to far from the … P1 d
nurse3 surg1 oh I don’t know where I am P4 a
nurse3 surg1 and there I am <camera moved> P4 a
surg1 nurse3 oh there you are, hi! P4 d
surg1 nurse3 don’t move don’t move <trying to pass a piece of tissue> P1 b
surg1 nurse3 ok grab it P1 b
surg1 nurse3 I think it was a good idea to put 3 graspers P3 e
nurse3 surg1 it was a good idea to what? P3 a
surg1 nurse3 it was a good idea to put 3 graspers P3 d
surg1 nurse3 yeah at least I think so P3 e
nurse3 surg1 yeah we can see better P3 e
nurse2 surg1 yeah it feels like we are seeing the depression P3 e
nurse2 nurse3 I am having trouble aspirating P1 a
nurse3 nurse2 yeah we are too close P3 d
nurse2 nurse3 no but I think… P3 e
nurse3 nurse2 yeah but we have to pass between the tools and the cam-
era, I don’t know how are going to do it E4 e
nurse3 nurse2 can’t we orient it… E4 a
nurse3 nurse2 cat we use it from that side E4 a
nurse2 nurse3 we need to check with B. E4 d
surg1 nurse2 woohoo <ready to help grasp the aspirator> P1 g

150
3:51 nurse3 surg1 you have <something> right there P1 e
nurse3 surg1 yeah but the problem is that the aspirator is … P1 e
surg1 nurse3 it will need to end there <indicating> P1 e
nurse3 surg1 there? P1 a
surg1 nurse3 theeeere P1 c
nurse3 surg1 yeah I know but P1 e
surg1 nurse3 theeeere P1 e
nurse3 nurse2 maybe we should insert it through the robot E4 a
nurse2 nurse3 yeah wait, because there is the plastic n the robot, maybe I can remove it E4 d
surg1 nurse2 I.? O a
surg2 surg1 yeah O c
surg1 surg2 can you totally remove the aspirator and insert it through a
different port, because I need you to aspirate there E1 a
surg1 surg2 I’m waiting for you, during that time I will start cleaning up P3 e
surg2 nurse3 yeah you can remove it because its not working E4 a
nurse3 surg2 yeah I don’t know maybe you want to try E4 d
surg2 nurse3 oh no no E4 c
surg2 nurse3 no I see that in this situation it’s not possible E4 e
surg2 nurse3 we will remove it from the trocar E4 e 3:52 nurse3 surg2 ok just wait a bit E4 e
surg2 nurse3 I., can you give me the <something> E1 a
nurse3 surg2 yeah I am trying with this trocar, but I cant get closer than
that E1 d
nurse3 surg2 do I move it? E2 a
surg2 nurse3 yeah remove everything E2 d
nurse3 surg2 ok wait, because I need to … P3 e
nurse3 surg2 discussing the options of where to put a new port P3 e
nurse2 nurse3 do you want some light S.? E2 a
nurse3 nurse2 wait I will need a grasper E1 b
surg1 surg2 what’s worrying me is that on that side we still haven’t seen the <something, devil?> P3 e
surg1 surg2 so we are not progressing as before P3 e
surg2 nurse2 we can place it …< the new trocar> P3 e
nurse2 surg2 yeah but if we place it this way … P3 e
surg1 nurse2 can you tell me where you are thinking about placing it? P3 a
surg2 nurse2 do you want to insert it this way S.? E4 a
surg2 nurse2 we need to insert it either this way or this way to optimize E4 d
surg1 nurse2 so what’s going on? E4 a
nurse2 surg1 we need to move a bit to see where we are P3 d
surg1 nurse2 you’re going in through which side? P3 a
nurse2 surg1 the left P3 d
3:56:00 surg1 nurse2 ok P3 c
nurse2 surg1 there? <putting trocar in> P3 a
surg1 nurse2 yeah its good P3 d
surg1 surg2 and do you manage to see? P3 a
surg2 surg1 it looks good P3 d
nurse2 surg1 ok they are in P3 e
surg1 nurse2 ah, super P3 e
surg1 nurse2 yeah the most important part is there P3 e
surg1 nurse2 oh, aspirate in the bottom of this part P1 b
nurse2 nurse3 do you think is possible to push it a bit so I can orient my-self better E2 a
nurse3 nurse2 yeah of course I’m coming E2 d
surg1 surg2 I.? O a
surg2 surg1 yeah? O c
3:58 surg1 surg2 I think your problem with it was that at the intersection there is too much of <something - not scar tissue, but something similar>
P3 e
surg2 surg1 oh, will you be able to remove these ones? P3 a
nurse2 surg2 yeah I think there has been an incident because of the problem before P3 c
surg2 nurse2 yeah it depends it’s a problem with the camera E4 e
surg2 rep yeah we had to pass it through the other side because we
couldn’t reach it this way P3 e
surg1 surg2 you see isa, what I meant is that from there oyu see as well P4 e

151
the right side of the aorta, which branches this way
surg1 surg2 it means we are right on the lesion P4 e
surg2 surg1 yeah and I think its totally flat which is why we can't see it P4 e
surg1 surg2 oh yeah I see P4 e
surg2 surg1 yeah and I think it’s totally flat and that’s why you can’t see it P4 e
surg1 surg2 oh yeah I see P4 e 4:00 surg1 surg2 and from that we can locate the lymph node P4 e
nurse2 surg1 oh yeah there is a clear conflict between the arm of the camera and the aspirator E3 e
surg1 surg2 ok lets stop, we progressed a lot for the next time P3 e
surg1 surg2 however, since we … I.? O a
surg2 surg1 yeah? O c
4:00 surg1 surg2 so we can see where the inflammation is with a lateral landmark P4 e
surg2 surg1 yeah, good learning P3 e
surg2 surg1 are you stopping now WF a
surg1 surg2 yeah I’m stopping WF d

152
APPENDIX C: NOTES FROM SURGEON INTERVIEW
Notes from a semi-structured interview with French robotic surgeon.
Background questions: What is your role at the hospital?
1. Attending surgeon / Obstetrician / Gynecologist 2. Resident Surgeon / Obstetrician / Gynecologist - Fellow Surgeon 3. Robotic Assistant 4. Scrub Nurse 5. Scrub Technician 6. Circulating Nurse 7. Other ____________________________ How many years of experience in this profession?
9 years – resident. Residencies in France are 5 years + 2 years for specializa-tion
How many times have you worked in a non-robotic surgery? Specify gynecology
1. Less than 25 2. 26 – 50 – for genecology 3. 51 – 75 4. 76 – 100 5. 101 +
How many times have you worked previously (in surgery) with the other mem-bers of the robotic surgery team?
More than 50 times. In the surgery videos, I noticed the team members communicating with each other frequently. I’m not sure whether this is common or is unique to robotic surgery. Compared to other non-robotic surgeries you have participated in, would you say the amount of communication during robotic surgery is …
Less About the same More n/a
It depends on the surgeon. J.M. generally talks a lot – he talks more in laparo-scopy procedures, but talks a lot in general. He talks less in robotic cases be-cause the surgeons are not face to face. There is a lack of visual (eye) contact. When it’s difficult, there is not a lot of talking/communication – communica-tion w/ facial expression. Need to talk behind console….but don’t want to re-veal the difficulty.

153
Surgeon shown a video excerpt from a French robotic surgery; a scene where the team members were having difficulty positioning the patient on the operating ta-ble in preparation for surgery.
Robot is new, no efficiency. Nobody was leading the positioning. Everybody has a different idea of how to do it. Different than when 1 new in laparoscopy, here everyone is new. Need a picture of how to position. Anesthesia is not very self confident with the robot – they don’t see point of the robot.
Surgeon shown a video excerpt from a French robotic surgery; a scene where the team members were performing port placement for the surgery.
Port placement is difficult because robotic arms block the patient, and if we need to change ports, it’s difficult. In laparoscopy, you don’t really check the scans to plan ports, but would be good for port planning in robotic surgery. Would be good to see 3D geometry - to know how big the uterus is, intestines, stomach etc.
Surgeon shown a video excerpt from a French robotic surgery; a scene where the nurse was having difficulty changing an instrument on the robot during the con-sole phase of surgery
Left can mean many things – it’s a problem with common language. Surgeon can’t go in and help them should practice without the patient, or should learn more skills. No system to train without the patient. Need to practice as a team in a mock surgery.

154
APPENDIX D: STATISTICAL ANALYSIS FOR EXPERIMENT 1
Novice Statistics
Split-plot ANOVA
Time Fact A (time) p=.104, F=2.95 Fact B (camera) p<.0001, F=50.56 Interaction p=.1828, F=2.06
Communication Fact A (comm) p=.8510, F=.16 Fact B (camera) p<.0001, F=48.11 Interaction p=.4193 F=.96
Ratio Fact A (ratio) p=.3435, F=1.21 Fact B (camera) p<.1969, F=1.94 Interaction p=.5392, F=.66
Note. Alpha=0.05 Note. Data were tested for normality using the Shapiro-Wilk statistic Note. Statistics were performed in SAS

155
APPENDIX E: STATISTICAL ANALYSIS FOR EXPERIMENT 2
Time ANOVA p=.2832, F=1.40, Fcrit=3.89, Alpha=0.05
Communication Volume: Kruskal-Wallis non-parametric test k=3, N=15, n=5 H=1.54 Hcrit = 5.7 for p=0.05
Ratio: Kruskal-Wallis non-parametric test
k=3, N=15, n=5 H=.1975 Hcrit = 5.7 for p=0.05
Spatial Ability Test:
Test for Equal Variance t-tests Assuming Equal Vari-ance (two-tailed)
2D Test 3D Test 2D Test 3D Test
Grid vs. Cardinal
p=.402 F=1.18 Fcrit=3.18
p=.44 F=.909 Fcrit=.315
p=.22 t=1.27 tcrit=2.1
p=.95 t=.05 tcrit=2.1
Grid vs. None
p=.051 F=3.177 Fcrit=3.178
p=.39 F=.837 Fcrit=.315
p=.025 t=2.43 tcrit=2.1
p=.20 t=1.32 tcrit=2.1
Cardinal vs. None
p=.08 F=2.68 Fcrit=3.18
p=.45 F=.921 Fcrit=.315
p=.33 t=.987 tcrit=2.1
p=.23 t=1.24 tcrit=2.1
Note. All data were tested for normality using the Shapiro-Wilk statistic. Note. Analysis performed in SAS, Excel, and by hand.

156
References
Bainbridge, L. (1983). Ironies of automation. Automatica, 19(6), 775-779.
Ballantyne, G. H. (2002). Robotic surgery, telerobotic surgery, telepresence, and telementoring. Surgical Endoscopy, 16(10), 1389-1402.
Boruk, M., Chernobilsky, B., Rosenfeld, R. M., & Har-El, G. (2005). Age as a prognostic factor for complications of major head and neck surgery. Archives of Otolaryngology--Head & Neck Surgery, 131(7), 605-609.
Bowers, C. A., Jentsch, F., Salas, E., & Braun, C. C. (December 1998). Analyzing communication sequences for team training needs assessment. Human Fac-tors: The Journal of the Human Factors and Ergonomics Society, 40, 672-679(8).
Cannon-Bowers, J. A., Salas, E., & Converse, S. A. (1993). Shared mental models in expert team decision making. In J. Castellan N.J. (Ed.), Current issues in individual and group decision making (pp. 221-246). Hillsdale, NJ: Erlbaum.
Cao, C. G. L. (2004). Hand-eye co-ordination in simulated laparoscopic surgery. Journal of Sport & Exercise Psychology, 26(S47)
Catchpole, K., Mishra, A., Handa, A., & McCulloch, P. (2008). Teamwork and error in the operating room: Analysis of skills and roles. Annals of Surgery, 247(4)
Chapanis, A. (1996). Human factors in systems engineering. New York: Wiley & Sons.
Chellali, A., Milleville-Pennel, I., & Dumas, C. (2008). Elaboration of a common frame of reference in collaborative virtual environments. Proceedings of the 15th European Conference on Cognitive Ergonomics: The Ergonomics of Cool Interaction, Funchal, Portugal. 21:1-21:8.
Christian, C. K., Gustafson, M. L., Roth, E. M., Sheridan, T. B., Gandhi, T. K., Dwyer, K., . . . Dierks, M. M. (2006). A prospective study of patient safety in the operating room. Surgery, 139(2), 159-173.
Clark, H. H., & Marshall, C. E. (1981). Definite reference and mutual knowledge. In A. K. Joshi, & B. L. Webber (Eds.), Elements of discourse understanding (pp. 10--63). Cambridge, England: Cambridge University Press.
157
Clark, H. H., & Brennan, S. E. (1991). Grounding in communication. In L. B. Resnick, J. M. Levine & S. D. Teasley (Eds.), Perspectives on socially shared cognition. (pp. 127-149) Washington, DC, US: American Psychologi-cal Association.
Clark, H. H., & Wilkes-Gibbs, D. (1986). Referring as a collaborative process. Cognition, 22(1), 1-39.
Cook, R., & Woods, D. (1996). Adapting to new technology in the operating room. Human Factors, v38(n4), p593(21).
Cramton, C. D. (2001). The mutual knowledge problem and its consequences for dispersed collaboration. Organization Science, 12(3), 346-371.
Davies, B. (2000). A review of robotics in surgery. Proceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine, 214(1), 129-140.
Ekstrom R.B., French J.W., Harman H.H., Dermen D. (1976). Manual for kit of factor-referenced cognitive tests. Princeton, NJ: Educational Testing Service.
Fleishman, E. A., & Zaccaro, S. J. (1992). Toward a taxonomy of team perform-ance functions. In Teams: Their training and performance. (pp. 31-56) Westport, CT, US: Ablex Publishing.
Gallagher, A. G., & Smith, C. D. (2003). Human-factors lessons learned from the minimally invasive surgery revolution. Surgical Innovation, 10(3), 127-139.
Gallstones and laparoscopic cholecystectomy. (1992). NIH Consensus Statement, 10(3), 1-28.
Gaver, W. W., Sellen, A., Heath, C., & Luff, P. (1993). One is not enough: Multi-ple views in a media space. Proceedings of the INTERACT '93 and CHI '93 Conference on Human Factors in Computing Systems, Amsterdam, The Netherlands. 335-341.
Gawande, A. A., Thomas, E. J., Zinner, M. J., & Brennan, T. A. (1999). The inci-dence and nature of surgical adverse events in colorado and utah in 1992. Surgery, 126(1), 66-75.
Goodman, R. A., & Goodman, L. P. (1976). Some management issues in tempo-rary systems: A study of professional development and manpower-the theater case. Administrative Science Quarterly, 21(3), 494-501.
158
Guerlain, S., Turrentine, F. E., Bauer, D. T., Calland, J. F., & Adams, R. (2008). Crew resource management training for surgeons: Feasibility and impact. Cogn.Technol.Work, 10(4), 255-264. doi:10.1007/s10111-007-0091-y
Gugerty, L., & Brooks, J. (2004). Reference-frame misalignment and cardinal di-rection judgments: Group differences and strategies. Journal of Experimental Psychology: Applied, 10(2), 75-88.
Healey, A., & Benn, J. (2009). Teamwork enables remote surgical control and a new model for a surgical system emerges. Cognition, Technology & Work, 11(4), 255-265.
Healey, M. A., Shackford, S. R., Osler, T. M., Rogers, F. B., & Burns, E. (2002). Complications in surgical patients. Arch Surg, 137(5), 611-618.
Hegarty, M., Montello, D. R., Richardson, A. E., Ishikawa, T., & Lovelace, K. (2006). Spatial abilities at different scales: Individual differences in aptitude-test performance and spatial-layout learning. Intelligence, 34(2), 151-176.
Helmreich, R. L., & Merritt, A. C. (2001). Culture at work in aviation and medi-cine: National, organizational and professional influences. Burlington: Ash-gate.
Helmreich, R. L., & Schaefer, H. (1994). Team performance in the operating room. In M. S. Bogner (Ed.), Human error in medicine (pp. 225-253). Hills-dale, NJ: Lawrence Earlbaum.
Helmreich, R. L., Wilhelm, J. A., Klinect, J. R., & Merritt, A. C. (2001). Culture, error, and crew resource management. In E. Salas Bowers, & E. C.A. E. (Eds.), Improving teamwork in organizations, applications of resource man-agement training (). New Jersey: Lawrence Erlbaum.
Helmreich, R. L. (2000). On error management: Lessons from aviation. BMJ, 320(7237), 781-785.
Hollnagel, E., & Woods, D. (2005). Joint cognitive systems: Foundations of cog-nitive systems engineering. Boca Raton, FL: CRC Press.
Jordan, N. (1963). Allocation of functions between man and machines in auto-mated systems. Journal of Applied Psychology, 47(3), 161-165.
Keehner, M. M., Tendick, F., Meng, M. V., Anwar, H. P., Hegarty, M., Stoller, M. L., & Duh, Q. (2004). Spatial ability, experience, and skill in laparoscopic surgery. The American Journal of Surgery, 188(1), 71-75.

159
Kohn, L., Corrigan, J., & Donaldson, M. (2000). To err is human: Building a safer health system. Washington, D.C.: National Academy Press.
Kraut, R. E., Fussell, S. R., & Siegel, J. (2003). Visual information as a conversa-tional resource in collaborative physical tasks. Hum.-Comput.Interact., 18(1), 13-49.
Landrigan, C. P., Parry, G. J., Bones, C. B., Hackbarth, A. D., Goldmann, D. A., & Sharek, P. J. (2010). Temporal trends in rates of patient harm resulting from medical care. The New England Journal of Medicine, 363(22), 2124-2134.
Leape, L. L. (1994). Error in medicine. JAMA: The Journal of the American Medical Association, 272(23), 1851-1857.
Lee, J. D. (2006). Human Factors and Ergonomics in Automation Design. In G. Salvendy (Ed.), Handbook of Human Factors and Ergonomics (pp. 1570-1596). Hoboken, NJ: John Wiley & Sons, Inc.
Lee, E., Rafiq, A., Merrell, R., Ackerman, R., & Dennerlein, J. (2005). Ergonom-ics and human factors in endoscopic surgery: A comparison of manual vs tel-erobotic simulation systems. Surgical Endoscopy, 19(8), 1064-1070.
Likert, R., & Quasha, W. H. (1970). Manual for the revised minnesota paper form board test. New York: The Psychological Corporation.
Lingard, L., Espin, S., Rubin, B., Whyte, S., Colmenares, M., Baker, G. R., . . . Reznick, R. (2005). Getting teams to talk: Development and pilot implemen-tation of a checklist to promote interprofessional communication in the OR. Qual.Saf.Health.Care., 14(5), 340-346.
Lingard, L., Espin, S., Whyte, S., Regehr, G., Baker, G., Reznick, R., . . . Grober, E. (2004). Communication failures in the operating room: An observational classification of recurrent types and effects. Qual.Saf.Health.Care., 13(5), 330-334. doi:10.1136/qshc.2003.008425 [doi]
Lingard, L., Reznick, R., Espin, S., Regehr, G., & DeVito, I. (2002). Team com-munications in the operating room: Talk patterns, sites of tension, and impli-cations for novices. Academic Medicine, 77(3)
Lirici, M. M., Papaspyropoulos, V., & Angelini, L. (1997). Telerobotics in medi-cine and surgery. Minimally Invasive Therapy & Allied Technologies, 6(5-6), 364-378.
160
Lohman, D. F., & Nichols, P. D. (1990). Training spatial abilities: Effects of prac-tice on rotation and synthesis tasks. Learning and Individual Differences, 2(1), 67-93.
Macedo, J. A., Kaber, D. B., Endsley, M. R., Powanusorn, P., & Myung, S. (1998). The effect of automated compensation for incongruent axes on teleoperator performance. Human Factors: The Journal of the Human Fac-tors and Ergonomics Society, (4), 541.
Mathieu, J. E., Heffner, T. S., Goodwin, G. F., Salas, E., & Cannon-Bowers, J. A. (2000). The influence of shared mental models on team process and perform-ance. The Journal of Applied Psychology, 85(2), 273-283.
Meyerson, D., Weick, K. E., & Kramer, R. M. (1996). Swift trust and temporary groups. In R. M. Kramer, & T. R. Tyler (Eds.), Trust in organizations (pp. 166-195). Thousand Oaks, CA: Sage Publications.
Miller, G. A. (1956). The magical number seven, plus or minus two: Some limits on our capacity for processing information. The Psychological Review, 63(2), 81-97.
Moray, N. (2004). Culture, context, and performance. In M. Kaplan (Ed.), Cul-tural ergonomics (pp. 31-59). Amsterdam: Elsevier.
Nagpal, K., Vats, A., Lamb, B., Ashrafian, H., Sevdalis, N., Vincent, C., & Moor-thy, K. (2010). Information transfer and communication in surgery: A sys-tematic review. Annals of Surgery, 252(2), 225-239 10.1097/SLA.0b013e3181e495c2.
Norman, D. (1998). The Psychology of Everyday Things. New York: Basic Books.
Nyssen, A., & Blavier, A. (2010). In Palanque P., Vanderdonckt J. and Winckler M.(Eds.), Integrating collective work aspects in the design process: An analysis case study of the robotic surgery using communication as a sign of fundamental change Springer Berlin / Heidelberg.
Orasanu, J., & Connolly, T. (1993). The reinvention of decision making. In G. A. Klein, J. Orasanu, R. Calderwood & C. E. Zsambok (Eds.), Decision making in action: Models and methods (pp. 3-20). Norwood, NJ: Ablex.
Oxford, E. D."Communication, n.". Retrieved
Parker, S. H., Wadhera, R., Wiegmann, D., & Sundt, T. M. (2009). The impact of protocolized communication during cardiac surgery. Human Factors and Er-gonomics Society Annual Meeting Proceedings, , 53(11) 684-688.
161
Reason, J. T. (1990). Human error. Cambridge: Cambridge University Press.
Risucci, D., Geiss, A., Gellman, L., Pinard, B., & Rosser, J. (2001). Surgeon-specific factors in the acquisition of laparoscopic surgical skills [Abstract]. American Journal of Surgery, 181(4) 289-293.
Rosser, J., Young, S., & Klonsky, J. (2007). Telementoring: An application whose time has come. Surgical Endoscopy, 21(8), 1458-1463.
Salas, E., Dickinson, T. L., Converse, S. A., & Tannenbaum, S. I. (1992). Toward an understanding of team performance and training. In R. W. Swezey, & E. Salas (Eds.), Teams: Their training and performance (pp. 3--29). Norwood, NJ: Ablex.
Schafer, W. A., & Bowman, D. A. (2004). Evaluating the effects of frame of ref-erence on spatial collaboration using desktop collaborative virtual environ-ments Springer London.
Schober, M. F. (1995). Speakers, addressees, and frames of reference: Whose ef-fort is minimized in conversations about locations? Discourse Processes, 20(2), 219-247.
Schostek, S., Schurr, M. O., & Buess, G. F. (2009). Review on aspects of artificial tactile feedback in laparoscopic surgery. Medical Engineering & Physics, 31(8), 887-898.
Sexton, J. B., & Helmreich, R. L. (2000). Analyzing cockpit communications: The links between language, performance, error, and workload. Human Per-formance in Extreme Environments : The Journal of the Society for Human Performance in Extreme Environments, 5(1), 63-68.
Shannon, C. E., & Weaver, W. (1949). The mathematical theory of communica-tion. Urbana, Ill.: University of Illinois Press.
Shepard, R. N., & Metzler, J. (1971). Mental rotation of three-dimensional ob-jects. Science, 171(3972), 701-703.
Sheridan, T. B. (2002). Humans and automation: System design and research is-sues. New York, NY, USA: John Wiley & Sons, Inc.
Smith, K. U., & Smith, W. M. (1962). Perception and motion Oxford, England: W. B. Saunders.
Stransky, D., Wilcox, L. M., & Dubrowski, A. (2010). Mental rotation: Cross-task training and generalization. Journal of Experimental Psychology.Applied, 16(4), 349-360.

162
Strauss, A. (2011). Minimally Invasive Surgery at University Hospitals. Retrieved from: http://www.mdnews.com/news/2011_03/05737_marapr2011_minimally-invasive-surgery
Tendick, F., Jennings, R. W., Tharp, G., & Stark, L. (1992). Sensing and manipu-lation problems in endoscopic surgery: Experiment, analysis, and observa-tion. Presence, 2, 66-81.
Trist, E. (1981). The evolution of socio-technical systems a conceptual framework and an action research program. In A. H. Van de Ven, & W. F. Joyce (Eds.), Perspectives on organization design and behavior (). New York: Wiley.
Trist, E., & Bamforth, K. (1951). Some social and psychological consequences of the long wall method of coal getting. Human Relations, 4(1), 3-38.
Webster, J. L., & Cao, C. G. L. (2006). Lowering communication barriers in op-erating room technology. Human Factors: The Journal of the Human Fac-tors and Ergonomics Society, 48(4), 747-758.
Wickens, C. D., & Carswell, C. M. (2006). Information processing. In Handbook of human factors and ergonomics (pp. 111-149) John Wiley & Sons, Inc.
Williams, R. G., Silverman, R., Schwind, C., Fortune, J. B., Sutyak, J., Horvath, K. D., . . . Dunnington, G. L. (2007). Surgeon information transfer and com-munication: Factors affecting quality and efficiency of inpatient care. Annals of Surgery, 245(2), 159-169.
World Health Organization. (2011). New scientific evidence supports WHO find-ings: A surgical safety checklist could save hundreds of thousands of lives. Retrieved from http://www.who.int/patientsafety/safesurgery/checklist_saves_lives/en/index.html




























