Embed Size (px)
Citation preview

Risk Stratification to Decrease Unnecessary Diagnostic Imaging for Acute AppendicitisHolly Depinet, MD, MPH, Daniel von Allmen, MD, Alex Towbin, MD, Richard Hornung, PHD, Mona Ho, MS, Evaline Alessandrini, MD, MSCE
Cincinnati Children’s Hospital Medical Center, Cincinnati,
Ohio
Dr Depinet conceptualized and designed the
study, oversaw enrollment and data management,
analyzed data, and drafted the initial manuscript;
Drs von Allmen and Towbin participated in study
design, analyzed the data, and revised the initial
manuscript; Dr Hornung and Ms Ho participated
in study design, carried out the initial analyses,
and reviewed and revised the manuscript; Dr
Alessandrini conceptualized and designed the
study, analyzed the data, and revised the initial
manuscript; and all authors approved the fi nal
manuscript as submitted.
DOI: 10.1542/peds.2015-4031
Accepted for publication May 19, 2016
Address correspondence to Holly Depinet, MD,
MPH, Division of Emergency Medicine, CCHMC,
3333 Burnet Ave, Cincinnati, OH 45229. E-mail: holly.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,
1098-4275).
Copyright © 2016 by the American Academy of
Pediatrics
FINANCIAL DISCLOSURE: The authors have
indicated they have no fi nancial relationships
relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors
have indicated they have no potential confl icts of
interest to disclose.
Identifying the small number of
patients with appendicitis among the
many presenting to the emergency
department (ED) for evaluation
of pediatric abdominal pain 1 is
challenging. Although the accuracy
of clinical factors for diagnosing
appendicitis is reported at 70% to
87%, 2, 3 the use of diagnostic imaging
including computed tomography (CT)
has become widespread, increasing
141% from 1996 to 2005. 4 Despite
the current recommendation for
ultrasound as the preferred first
diagnostic imaging modality5 and
the small increase in lifetime risk of
malignancy associated with ionizing
radiation, 6 CT is still commonly used
in some areas for initial diagnostic
imaging. 7
abstractBACKGROUND: There has been an increase in the use of imaging modalities
to diagnose appendicitis despite evidence that can help identify children
at especially high or low risk of appendicitis who may not benefit. We
hypothesized that the passive diffusion of a standardized care pathway
(including diagnostic imaging recommendations) would improve the
diagnostic workup of appendicitis by safely decreasing the use of
unnecessary imaging when compared with historical controls and that an
electronic, real-time decision support tool would decrease unnecessary
imaging.
METHODS: We used an interrupted time series trial to compare proportions
of patients who underwent diagnostic imaging (computed tomography
[CT] and ultrasound) between 3 time periods: baseline historical controls,
after passive diffusion of a diagnostic workup clinical pathway, and after
introduction of an electronic medical record–embedded clinical decision
support tool that provides point-of-care imaging recommendations (active
intervention).
RESULTS: The moderate- and high-risk groups showed lower proportions of
CT in the passive and active intervention time periods compared with the
historical control group. Proportions of patients undergoing ultrasound
in all 3 risk groups showed an increase from the historical baseline. Time
series analysis confirmed that time trends within any individual time
period were not significant; thus, incidental secular trends over time did not
appear to explain the decreased use of CT.
CONCLUSIONS: Passive and active decision support tools minimized
unnecessary CT imaging; long-term effects remain an important area of
study.
QUALITY REPORTPEDIATRICS Volume 138 , number 3 , September 2016 :e 20154031
To cite: Depinet H, von Allmen D, Towbin A,
et al. Risk Stratifi cation to Decrease Unnecessary
Diagnostic Imaging for Acute Appendicitis.
Pediatrics. 2016;138(3):e20154031
by guest on June 23, 2020www.aappublications.org/newsDownloaded from

DEPINET et al
Clinical scoring systems have been
developed to identify patients
at especially high or low risk of
appendicitis based on clinical features,
including the 10-point Pediatric
Appendicitis Score (PAS). 8 Initially,
a single scoring cutoff was used, but
subsequent studies found better
validity when scores delineated 3 risk
strata. Specifically, high-risk scores
(≥7) have a specificity of 95% to
98%, 9, 10 and low-risk scores (≤3)
have a negative predictive value
of 98%, 10 identifying cases where
diagnostic imaging could be avoided.
Evidence-based clinical pathways
often standardize care and use
clinical decision support (CDS) tools
or systems to achieve their goals. 11 – 16
Studies have shown that CDS tools
that are presented to the clinician
through active interventions showed
improved outcomes, and early
evidence indicates that computerized
CDS systems that present
recommendations at the point of care
also increase adherence to specific
clinical recommendations. 17
We hypothesized that the passive
diffusion of a standardized care
pathway (including diagnostic
workup recommendations)
would safely decrease the use of
unnecessary imaging when compared
with baseline historical controls and
that an active intervention at the
point of care would decrease the use
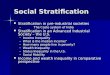
of unnecessary imaging ( Fig 1).
METHODS
Setting
This study was conducted at an
urban tertiary care hospital with
a pediatric ED with 90 000 annual
visits and ~500 cases of appendicitis
per year. There is 24-hour availability
of surgical subspecialty consultation,
anesthesia, and radiology (including
ultrasound and CT). The ED used a
well-established electronic medical
record (EMR) system with decision
support capabilities throughout the
study period.
Study Design
This was a prospective, interrupted
time series trial comparing imaging
use during 3 time periods: a historical
e2
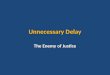
FIGURE 1Diagnostic pathway for patients age 3 to 21 with suspected acute (<72 hours) appendicitis.
by guest on June 23, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 138 , number 3 , September 2016
baseline, after traditional passive
diffusion of a clinical pathway, and
after implementation of an active
CDS intervention that used the same
clinical pathway ( Fig 2).
Interventions
Historical Controls (January–December 2010)
We used a cohort with clinical
characteristics that approximated
those of our study sample, to
determine baseline rates of outcomes
before any interventions were
made. 18
Passive Intervention (January 2012–October 2012)
We developed a clinical pathway
for the diagnostic evaluation of
suspected acute appendicitis that
was based on the well-validated PAS
and incorporated our standardized
ultrasound report templates and
test characteristics. 19 The pathway
recommended minimizing imaging
in the high- and low-risk groups
and encouraged ultrasound over CT
use in the moderate risk category.
The passive intervention (typical
evidence dissemination) included
conventional passive diffusion of
the clinical pathway via review at
divisional meetings and educational
conferences, posted copies of the
pathway in clinical areas and on
our divisional Web site, and e-mail
reminders.
Active Intervention (October 2012–June 2013)
We implemented a real-time,
computerized CDS tool that
integrated the above appendicitis
clinical pathway at the point of
care in the EMR. The tool was
technically simple, and physicians
had used similar tools in our setting
previously. Workflow analysis and
focus groups with key stakeholders
informed the development of a CDS
tool with 3 interacting components,
which were extensively tested:
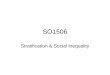
• EMR-based data collection template: An alert (which fired
in response to chief complaints:
vomiting and abdominal pain)
triggered clinicians to enter
elements of the PAS in a timely
fashion without interrupting their
clinical workflow; laboratory and
fever data were automatically
incorporated ( Fig 3). The tool
was iterative; if elements were
changed by the user or a more
senior physician, new data were
incorporated.
• CDS engine: The CDS engine
the above data and provided the
individualized risk score, strata,
and recommendations.
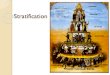
• EMR feedback interface: A
feedback interface provided the
results and recommendations
e3
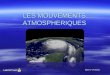
FIGURE 2Number meeting inclusion and exclusion criteria in all 3 time intervals.
by guest on June 23, 2020www.aappublications.org/newsDownloaded from

DEPINET et al
to clinician users in a clear,
visually simple manner at a
logical point in the ED workflow;
recommendations were associated
with automatic orders (based on
age, gender, and PAS risk strata)
for the appropriate testing or
treatment, which the physician
could accept or modify ( Fig 4).
Study of the Intervention
Inclusion and Exclusion Criteria and Population Identifi cation
Our study included 3 time periods:
historical baseline, passive
intervention, and active intervention.
During the active and passive
intervention phases, we included
a convenience sample of patients
age 3 to 21, with symptoms for
<72 hours, where the ED attending
physician had a clinical suspicion for
appendicitis or the patient had right
lower quadrant pain. We excluded
patients with significant abdominal
trauma, outside institution imaging,
or an underlying medical condition
that can confound the diagnosis of
appendicitis.
A paper data collection tool was
used to collect prospective data
for analysis (PASs determined by a
combination of attending physician
impression of clinical variables
at the time of their first physical
examination and laboratory and vital
sign data) during both intervention
phases for 2 reasons. First, this step
ensured that the data in both time
periods were measured similarly;
additionally, it allowed us to study
the active intervention (the CDS
tool) itself by comparing scores
obtained from the CDS tool with
the prospective data. To minimize
the influence of this data collection
tool (ie, limit the possibility that it
would serve as an intervention itself),
we included extraneous variables
and had a run-in period before the
passive intervention started. Because
our clinical pathway did not firmly
recommend a complete blood cell
count (CBC) for low-risk patients, in
cases where a CBC was not ordered,
we analyzed the PAS without
complete data.
To find historical controls that
represented the true baseline before
the clinical pathway was developed
(the pathway was developed during
the year before the interventions),
thus before any clinicians had
knowledge of its recommendations,
we sought a population cared for
>1 year before our study began.
Identifying such a population is
challenging, because patients with
issues of diagnostic accuracy 20
such as “potential appendicitis” are
difficult to identify retrospectively.
e4
FIGURE 3Chief complaint–based alert notifying clinicians to use the CDS tool (top) and data collection screen in the CDS tool (bottom).
FIGURE 4Automatic orders generated by the CDS tool (based on patient age, gender, and PAS risk strata).
by guest on June 23, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 138 , number 3 , September 2016
To identify a historical population
that would accurately approximate
our study sample, we used a database
of ED patients with abdominal pain,
from a 1-year period that preceded
our study by 13 months, who had
PAS assigned and validated by chart
review by pediatric emergency
medicine providers as part of another
study. 18 To select the patients in
this database who were as similar
as possible to our study population,
we additionally analyzed charts
to determine whether patients
would have met study inclusion and
exclusion criteria.
Specifically, ED physician notes
were analyzed via a natural
language processing program to
identify any mention of concern for
appendicitis; this is a well-validated
technique to extract relevant clinical
information from free text notes, and
in a previous study that used this
database, it performed comparably
to physician chart reviewers in
identifying clinical elements of the
PAS. 18 Additionally, we reviewed
imaging orders and indications. This
database fully sampled patients
with a diagnosis of appendicitis
and also included a random sample
of other patients with abdominal
pain. Therefore, the moderate- and
high-risk patients in the historical
control group approximate the same
groups in our study sample well. The
low-risk group was proportionally
larger in the historical sample, but it
includes patients with a low risk of
appendicitis based on our criteria.
Measurement
Outcome Variables
Our primary outcome of interest
was the proportion of patients
who underwent CT as part of their
evaluation for suspected appendicitis.
Outcomes were calculated overall
and stratified by high, moderate, or
low risk for appendicitis. Secondary
outcomes were proportion
undergoing ultrasound and ED length
of stay (LOS).
Additional process measures
included use of the CDS tool,
agreement between the CDS tool
and prospectively collected data
elements, and presence of a CBC.
Balancing measures include negative
appendectomy rate and missed
diagnosis rate (based on 1-month
follow-up review).
Covariates included age, gender,
race, shift of arrival (day, evening,
or overnight), resident physician
involvement (yes or no), and
referral status (referred or not
referred).
Analysis
Outcomes were examined via
statistical process control analyses,
logistic regression, and a time series
analysis to assess for trends within
each time period. Specifically, we
used p-charts, which are a type of
Shewhart chart (commonly called
a control chart) used to graphically
display trends and explore variation
in binomial data (eg, CT no CT). 21
We ran separate multivariable
logistic regression models for the
outcomes of CT and ultrasound
by using separate 3-level dummy
variables for the variable
representing PAS risk group (high,
moderate, or low) and intervention
time interval (historical, passive
diffusion, or active intervention)
across time intervals and stratified
by risk group, controlled for all
covariates.
Time series analyses assessed for
secular trends in major outcomes
between study time periods
(via comparison of means) and
within each study time period (via
comparison of slopes). This was
done to expand on the results of the
regression analyses and determine
whether our outcomes were stable
within each time period or changing
incrementally over time and thus
help determine whether the changes
we saw between time periods
were probably attributable to our
intervention or to secular trends
already under way.
We determined frequency of CDS
use and compared PAS risk strata
generated by the CDS tool with risk
strata determined by the prospective
data collection. ED LOS was reported
for each time period, stratified by
PAS risk group.
RESULTS
Our final sample included 809
patients in the historical group,
588 in the passive intervention
group, and 489 in the active
intervention group ( Fig 2). Groups
were similar with respect to age,
gender, and race; however, patients
in the active and passive groups
were more likely to have had a
resident physician involved in their
care, to have been referred to the
ED, and to have presented to the
ED earlier in the day compared with
historical controls. Additionally,
the historical group had a higher
proportion of patients in the low-risk
strata ( Table 1).
The CDS tool was used 61% of time in
the active study time period; the final
PAS strata assigned by the CDS tool
(including patients where all clinical
PAS elements were completed by the
physician user) were in agreement
with the prospectively assigned PAS
84.5% of the time; however, in 16%
of cases the CDS tool had ≥1 missing
or unknown clinical variable ( Table 1).
P-charts showed a decrease in the
proportion of patients with CT from
the historical baseline to the passive
and active intervention phases, in the
moderate-risk (from 22.3% to 10.2%
and 12.2%) and high-risk (from 25.2%
to 15.7% and 14.4%) strata ( Figs 5
and 6). There were too few patients
in the low-risk strata to create control
charts. Ultrasound increased in all
groups combined (we combined this
graphical display for all 3 groups
because similar statistically significant
increases were seen in all groups over
e5 by guest on June 23, 2020www.aappublications.org/newsDownloaded from

DEPINET et al
time) from 59.5% in the historical
group to 83.7% in the passive group
and 88.8% in the active group ( Fig 7).
In the regression analysis, moderate-
and high-risk patients during both
the active and passive phases had
significantly lower proportions of
CTs than those in the historical time
period (but neither differed from
passive to active phases); all risk
groups during both the active and
passive phases had significantly
higher proportions of ultrasounds
than those in the historical time
period ( Table 2).
Time series analyses found that
a comparison of the slopes of the
proportion of patients with imaging
within each time period was
nonsignificant, so changes seen were
not thought to be attributable to
secular trends occurring incidentally.
In the time series comparison of the
e6
TABLE 1 Characteristics of the Study Population (With 95% Confi dence Intervals)
Historical, n = 809 Passive, n = 588 Active, n = 489
Age, y (median) 12 12 12
Gender, % male 48.2% (44.8–51.7) 43.5% (39.5–47.5) 46.6% (42.2–51.1)
Race, % white 78.1% (75.3–81.0) 76.6% (73.1–79.9) 77.9% (74.2–81.6)
Resident involved, % yes 29.5% (26.4–32.7) 70.6% (66.9–74.3) 77.5% (73.8–81.2)
Referral, % yes 15.6% (13.1–18.1) 56.8% (52.8–60.8) 58.7% (54.3–63.1)
PAS distribution
Low risk 18.9% (16.2–21.6) 10.4% (7.9–12.8) 6.8% (4.5–9.0)
Moderate risk 38.8% (35.5–42.2) 51.9% (47.8–55.9) 60.5% (56.2–64.9)
High risk 42.3% (38.9–45.7) 37.8% (33.8–41.7) 32.7% (28.6–36.9)
Time of day of arrival
Day 42.4% (39.0–45.8) 60.4% (56.4–64.3) 58.5% (54.1–62.9)
Evening 41.9% (38.5–45.3) 34.9% (31.0–38.7) 34.4% (30.1–38.6)
Overnight 15.7% (13.2–18.2) 4.8% (3.0–6.5) 7.2% (4.9–9.4)
% of time CDS tool used n/a n/a 61.6% (57.2–65.9)
% with CBC 62.8% (59.5–66.1) 71.9%(68.3–75.6) 76.9% (73.2–80.1)
Negative appendectomy ratea 17.2% (10.7–23.7) 8.6% (4.6–12.6) 16.8% (12.9–20.7)
Missed appendicitis rateb n/a 0 0
n/a, not applicable.a Based on operative histology.b Based on 1-mo follow-up.
FIGURE 5P-chart for proportion of patients with CT imaging over time in high-risk patients (subgroups of 20).
by guest on June 23, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 138 , number 3 , September 2016 e7
FIGURE 6P-chart for proportion of patients with CT imaging over time in moderate-risk patients (subgroups of 20).
FIGURE 7P-chart for the proportion of patients with ultrasound over time in all risk groups (subgroups of 20).
by guest on June 23, 2020www.aappublications.org/newsDownloaded from

DEPINET et al
means between study time periods,
only the proportion of CT in the
moderate risk group decreased
(P = .03).
Analysis of ED LOS showed no
appreciable change over the 3 time
periods ( Table 3).
DISCUSSION
We found lower rates of CT imaging
the moderate- and high-risk strata,
in the passive diffusion and active
intervention groups compared
with historical controls, and an
unintended consequence of an
increase in the use of ultrasound.
The additional ultrasounds could
be explained by several factors:
Some patients in the final high-risk
category did not have laboratory
results ready at the time of ordering
an ultrasound, and so they appeared
to be in the moderate-risk category
until their CBC was completed
(the CDS tool was iterative and
would have given preliminary
recommendations for imaging even
without final data); also, trainees
may have scored the patients
higher than attending physicians.
Finally, some high-risk patients
may have appropriately had
ultrasound ordered after
surgical consultation.
The CDS tool was used 61% of
the time in the active time period,
and the CDS-assigned risk strata
correlated with prospective data
collected 84.4% of the time. Although
the CDS tool offered patient-tailored
recommendations at the point
of care, challenges of real-world
implementation may have led to
less than ideal practice (eg, missing
or unknown variables entered
into the CDS tool). For instance,
clinicians may have believed that
the PAS strata were simple enough
to memorize, and therefore they
did not need decision support, or
the many rotating trainees from
various institutions may have been
less familiar with CDS tools or not
reliably trained to use them. Also,
the firing of the CDS tool each time
there was a chief complaint related
to appendicitis may have led to alert
fatigue. Overall, more work is needed
to introduce a culture of standardized
care in which such a decision support
tool could work optimally.
Although these results showed
improved care in the direction
we thought was most important
(minimizing diagnostic imaging
associated with ionizing radiation),
we did not see more improvement
in imaging rates from the passive to
the active intervention time periods,
as we hypothesized we would. Active
interventions, especially those
embedded in the EMR at the point
of decision making, have shown
improved outcomes over guidelines
alone. 15, 22 – 24 It is possible that the
initial positive effect of traditional
passive diffusion of knowledge
extinguishes over time25; because our
passive pathway was present for only
9 months before the introduction of
the active pathway, it was still fairly
novel to clinicians, and its effects
did not have time to extinguish.
Additionally, it is possible that all
the preliminary work that occurred
in the year between the historical
control period and the passive and
active intervention periods, which
enabled development of the clinical
pathway for implementation (eg,
obtaining consensus among specialty
services about imaging goals,
changes in workflow and processes
for multiple divisions to support
the pathway, education about the
utility of the PAS and improved
test characteristics with standardized
ultrasound interpretations),
changed our practice in a way that
is more sustainable than an
individual pathway. We did not
see a significant difference in
e8
TABLE 2 Multivariablea Regression for the Outcomes of CT and Ultrasound
Historical Controls, n = 809 Passive Diffusion, n = 588 Active Intervention, n = 489
OR OR 95% CI OR 95% CI
CT
Low riskb 1.0 3.27 0.85–12.6 3.71 0.77–17.5
Moderate risk 1.0 0.38 0.24–0.61 0.48 0.31–0.75
High risk 1.0 0.55 0.36–0.85 0.49 0.3–0.82
Ultrasound
Low risk 1.0 10.5 5.0–22.0 10.8 4.2–27.5
Moderate risk 1.0 8.4 4.8–14.7 17.8 9.5–33.3
High risk 1.0 14.9 7.4–29.8 18.3 8.6–39
CI, confi dence interval; OR, odds ratio.a Adjusted for age, gender, race, shift of arrival (day, evening, or overnight), resident physician involvement (yes or no), and referral status (referred or not referred).b All risk strata based on our institutional pathway.
TABLE 3 ED LOS for Patients in All Risk Strata Across Time Intervals
Historical Controls,
n = 809
Passive Diffusion,
n = 588
Active Intervention,
n = 489
Mean (95% CI) Mean (95% CI) Mean (95% CI)
LOS, min, high risk 355.5 (339.4–371.6) 367.8 (350.4–385.3) 372.9 (351.4–394.4)
LOS, min, moderate risk 354.3 (337.9–370.6) 336.5 (321.8–351.2) 371.3 (355.7–386.9)
LOS, min, low risk 251.7 (234.6–268.7) 325.4 (284.5–366.3) 289.6 (244.0–335.1)
CI, confi dence interval.
by guest on June 23, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 138 , number 3 , September 2016
ED LOS between the time intervals;
however, this factor is affected by
many variables other than the
targets of our interventions
(eg, hospital boarding, changes in
available rooms due to construction,
other initiatives).
One challenge in studies of diagnostic
accuracy 20 is the difficulty with
population identification. Unlike
in studies of children with known
diagnoses such as asthma or diabetes,
there is no simple way to identify
patients with “possible diagnoses, ”
such as appendicitis, intussusception,
or sepsis. Our method of population
identification for the active and
passive samples (asking the
attending physician whether he or
she is considering appendicitis) has
been used successfully in previous
studies of pediatric appendicitis and
other types of studies. 26, 27 However,
there is a risk that this method may
introduce bias (toward the null) by
prompting the ED attending use the
pathway.
Additionally, we believe that the
low-risk population, in which
the clinician has some thought of
appendicitis but has ruled it out
clinically, may be underrepresented
in the passive and active diffusion
phases because of the hesitation to
identify a patient as having some
risk of appendicitis (however low)
despite not planning to do any more
evaluation. Thus, the historical
sample, with its population identified
by less subjective methods, may
represent a truer low-risk sample
than the prospectively identified
samples.
Challenges with population
identification also led to the need
to approximate the historical
control group differently than the
intervention groups, which may
introduce bias. For instance, the
historical group included more
patients seen overnight, fewer
patients cared for by resident
physicians, and patients from all
areas of the ED (whereas the active
and passive study populations
were not drawn from urgent
care areas). These factors could
have affected imaging outcomes
in the historical group, although
this effect is minimized by close
supervision of learners, introduction
of the pathway to residents, and
constant availability of ultrasound.
Additionally, some of these factors
would theoretically have introduced
bias in differing directions (ie, some
would bias toward and some away
from the null), but we believe that
our stringent selection criteria for
historical controls minimized this
possibility and that the moderate-
and high-risk groups were similar
across study periods.
Additionally, although a decrease in
CT was temporally correlated with
our interventions, it is possible that
other more global factors, such as
nationally disseminated knowledge
about the risks of CT, were partially
responsible for the decrease in CT
that we observed.
Finally, generalizability may be
limited to institutions with the
specific capabilities needed for
the intervention: 24-hour availability
of surgeons and radiologists,
acceptable test characteristics
of ultrasound, and EMRs with
decision support capabilities
and the technical resources to
program them.
CONCLUSIONS
Overall, we saw an improvement
in the use of CT from our historical
baseline, although CT use did not
differ between active and passive
intervention groups, and we saw an
unintended consequence of increased
use of ultrasound. Additional work
is needed to determine whether
this effect will diminish over time.
Additionally, this study demonstrates
the value of standardized care
pathways in reducing variation
in imaging in cases of diagnostic
accuracy.
REFERENCES
1. Pitts SR, Niska RW, Xu J, Burt CW.
National Hospital Ambulatory Medical
Care Survey: 2006 emergency
department summary. Natl Health Stat
Report. 2008;(7)1–38
2. Andersson RE. Meta-analysis
of the clinical and laboratory
diagnosis of appendicitis. Br J Surg.
2004;91(1):28–37
3. Toorenvliet BR, Wiersma F, Bakker
RF, Merkus JW, Breslau PJ, Hamming
JF. Routine ultrasound and limited
computed tomography for the
diagnosis of acute appendicitis. World
J Surg. 2010;34(10):2278–2285
4. Pines JM. Trends in the rates of
radiography use and important
diagnoses in emergency department
patients with abdominal pain. Med
Care. 2009;47(7):782–786
5. Howell JM, Eddy OL, Lukens TW,
Thiessen ME, Weingart SD, Decker
WW; American College of Emergency
Physicians. Clinical policy:
critical issues in the evaluation
and management of emergency
department patients with suspected
appendicitis. Ann Emerg Med.
2010;55(1):71–116
6. Brenner D, Elliston C, Hall E, Berdon W.
Estimated risks of radiation-induced
fatal cancer from pediatric CT.
AJR Am J Roentgenol. 2001;176(2):
289–296
7. Fullerton KT, Depinet H, Iyer S, Boeck
RN, Herr S, Morton I. Imaging variation
in the diagnosis of acute appendicitis.
AAP National Conference & Exhibition;
October 2015; Washington, DC
8. Samuel M. Pediatric appendicitis
score. J Pediatr Surg.
2002;37(6):877–881
9. Goldman RD, Carter S, Stephens D,
Antoon R, Mounstephen W, Langer JC.
e9
ABBREVIATIONS
CBC: complete blood cell count
CDS: clinical decision support
CT: computed tomography
ED: emergency department
EMR: electronic medical record
LOS: length of stay
PAS: Pediatric Appendicitis Score
by guest on June 23, 2020www.aappublications.org/newsDownloaded from

DEPINET et al
Prospective validation of the pediatric
appendicitis score. J Pediatr.
2008;153(2):278–282
10. Bhatt M, Joseph L, Ducharme FM,
Dougherty G, McGillivray D. Prospective
validation of the pediatric appendicitis
score in a Canadian pediatric
emergency department. Acad Emerg
Med. 2009;16(7):591–596
11. Bergman DA. Evidence-based
guidelines and critical pathways for
quality improvement. Pediatrics.
1999;103(1 suppl E):225–232
12. Institute of Medicine. To Err Is Human:
Building a Safer Health System.
Washington, DC: National Academy
Press; 1999
13. Chaudhry B, Wang J, Wu S, et al.
Systematic review: impact of health
information technology on quality,
effi ciency, and costs of medical care.
Ann Intern Med. 2006;144(10):742–752
14. Osheroff JA, Teich JM, Levick D, et
al. Improving Outcomes With Clinical
Decision Support: An Implementer’s
Guide. Chicago, IL: Healthcare
Information and Management Systems
Society; 2005
15. Osheroff JA, Teich JM, Middleton
B, Steen EB, Wright A, Detmer DE. A
roadmap for national action on clinical
decision support. J Am Med Inform
Assoc. 2007;14(2):141–145
16. Wright SW, Trott A, Lindsell CJ, Smith C,
Gibler WB. Evidence-based emergency
medicine. Creating a system to
facilitate translation of evidence
into standardized clinical practice: a
preliminary report. Ann Emerg Med.
2008;51(1):80–86, 86.e1–86.e8
17. Shojania KG, Jennings A, Mayhew A,
Ramsay CR, Eccles MP, Grimshaw J.
The effects of on-screen, point of care
computer reminders on processes and
outcomes of care. Cochrane Database
Syst Rev. 2009; (3):CD001096
18. Deleger L, Brodzinski H, Zhai H,
et al. Developing and evaluating
an automated appendicitis risk
stratifi cation algorithm for
pediatric patients in the emergency
department. J Am Med Inform Assoc.
2013;20(e2):e212–e220
19. Larson DB, Trout AT, Fierke SR,
Towbin AJ. Improvement in diagnostic
accuracy of ultrasound of the
pediatric appendix through the use
of equivocal interpretive
categories. AJR Am J Roentgenol.
2015;204(4):849–856
20. Iyer S, Reeves S, Varadarajan K,
Alessandrini E. The acute care model:
a new framework for quality care
in emergency medicine. Clin Pediatr
Emerg Med. 2011;12(2):91–101
21. Provost LP. Murray SK. Heath Care Data
Guide. San Francisco, CA: Jossey-Bass;
2011
22. Bates DW, Kuperman GJ, Wang S,
et al. Ten commandments for effective
clinical decision support: making the
practice of evidence-based medicine
a reality. J Am Med Inform Assoc.
2003;10(6):523–530
23. Sintchenko V, Coiera E, Iredell JR,
Gilbert GL. Comparative impact of
guidelines, clinical data, and decision
support on prescribing decisions:
an interactive Web experiment with
simulated cases. J Am Med Inform
Assoc. 2004;11(1):71–77
24. Kawamoto K, Houlihan CA, Balas EA,
Lobach DF. Improving clinical practice
using clinical decision support
systems: a systematic review of trials
to identify features critical to success.
BMJ. 2005;330(7494):765
25. Yang CW, Yen ZS, McGowan JE,
et al. A systematic review of
retention of adult advanced life
support knowledge and skills in
healthcare providers. Resuscitation.
2012;83(9):1055–1060
26. Kuppermann N, Holmes JF, Dayan
PS, et al; Pediatric Emergency Care
Applied Research Network (PECARN).
Identifi cation of children at very
low risk of clinically-important
brain injuries after head trauma: a
prospective cohort study. Lancet.
2009;374(9696):1160–1170
27. Yen K, Kuppermann N, Lillis K.
Interobserver agreement in the clinical
assessment of children with blunt
abdominal truma. Acad Emerg Med.
2013;20(5):426–432
e10 by guest on June 23, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2015-4031 originally published online August 23, 2016; 2016;138;Pediatrics
Evaline AlessandriniHolly Depinet, Daniel von Allmen, Alex Towbin, Richard Hornung, Mona Ho and
AppendicitisRisk Stratification to Decrease Unnecessary Diagnostic Imaging for Acute
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/138/3/e20154031including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/138/3/e20154031#BIBLThis article cites 23 articles, 2 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/surgery_subSurgerysubhttp://www.aappublications.org/cgi/collection/quality_improvement_Quality Improvement_management_subhttp://www.aappublications.org/cgi/collection/administration:practiceAdministration/Practice Managementfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on June 23, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2015-4031 originally published online August 23, 2016; 2016;138;Pediatrics
Evaline AlessandriniHolly Depinet, Daniel von Allmen, Alex Towbin, Richard Hornung, Mona Ho and
AppendicitisRisk Stratification to Decrease Unnecessary Diagnostic Imaging for Acute
http://pediatrics.aappublications.org/content/138/3/e20154031located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2016has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on June 23, 2020www.aappublications.org/newsDownloaded from