Embed Size (px)
Citation preview

1
Risk Adjustment Methodology 101: How to Make Sense of It All
Brett Senor, MD, CRC, CCDSMedical DirectorEnjoinAsheville, NC
22
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

3
Polling Question
Which best represents your organization?
1.ACO
2. Provider in physician office setting
3.Hospital/health system
4. Consulting organization
5.Other
3
4
Learning Objectives
• At the completion of this educational activity, the learner will be able to:
– Understand the framework of Hierarchical Condition Categories (HCC)
– Recognize the differences between the 2019 and 2020 CMS‐HCC methodology
– Identify the new HCC categories and documentation tips to support capture
– Acknowledge additional upcoming changes
– Describe the key documentation elements for accurate and valid HCC capture
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

5
HHS Goal: Reward Value, Not Volume
• HHS framework categorizes healthcare payment according tohow providers receive payment for care
• Categories 1–4
• Moving toward higher categories entails two shifts:– (1) Increasing accountability for both quality and total cost of care
– (2) A greater focus on population health management as opposed to payment for specific services
6
Risk Adjustment Evolution
Acronyms:RAPS ‐ Risk Adjustment Processing SystemRA – Risk AdjustmentMA – Medicare Advantage
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

7
So Many Changes
• Implementation of extrapolation for RADV findings
• “Pathways to Success” for ACOs
• Special Supplemental Benefits for Chronically Ill (SSBCI)
• Social Determinants of Health (SDoH)
• Changes to CMS‐HCC methodology
8
Methodology Changes Within the Bigger Picture
ICD‐10 codes
Methodologies: Risk adjustment (e.g., HCC risk scores)
Programs: ACO, Medicare Advantage, CPC+, MIPS, etc.
Documentation
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

9
Current Methodology
10
Current CMS‐HCC Model CharacteristicsCharacteristic Descriptions
Prospective model Uses diagnostic information from a base year to predict Medicare benefit costs for the following year
Site neutral Model does not distinguish payment based on site of care
Diagnostic sources Model recognizes diagnoses from hospital inpatient, hospital outpatient, and physician settings
Multiple chronic diseases considered
Risk‐adjusted payment based on assignment to disease groups (Condition Categories [CC])• Most CCs represent chronic conditions
Models are additive Individual risk scores calculated by adding coefficients associated with each beneficiary’s demographic factors and CCs
Demographic variables Demographic factors include age, sex, original reason for entitlement, Medicaid or low‐income status, disability status
Adapted from: Centers for Medicare and Medicaid Services. Medicare Managed Care Manual. Chapter 7 – Risk Adjustment, 70 – Risk Adjustment Models – Overview.
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
11
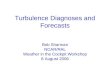
Current CMS‐HCC Model Structure
Structure Details
Hierarchical 65% of all HCCs exist in clinically related family of HCCs that are ranked by severity or cost dominance within a hierarchy• When > 2 HCCs within a hierarchy are reported for a patient in a calendar
year, only highest ranked/most severe HCC that is triggered is reported for a patient each year• Process is called “trumping”
Additive Unrelated HCCs are cumulative
Disease interactions
Certain combinations of diseases have been demonstrated to increase costs of careThe model incorporates additional relative factors for disease interactions• Are additive factors and increase payment accuracy
Adapted from: Watson, M. "Documentation and Coding Practices for Risk Adjustment and Hierarchical Condition Categories." Journal of AHIMA 89, no.6 (June 2018): extended online version.
12
Risk Adjustment: CMS‐HCC Model
• A coefficient or “weight” is assigned to each category of chronic complex diagnoses as well as severe acute diagnoses
• HCCs involving unrelated conditions are cumulativeHCC
Category Description Label Coefficient
HCC 1 HIV/AIDS 0.344
HCC 2 Septicemia, Sepsis, Systemic Inflammatory Response Syndrome/Shock 0.428
HCC 6 Opportunistic Infections 0.446
HCC 8 Metastatic Cancer and Acute Leukemia 2.654
HCC 9 Lung and Other Severe Cancers 1.027
HCC 10 Lymphoma and Other Cancers 0.675
HCC 11 Colorectal, Bladder, and Other Cancers 0.309
HCC 12 Breast, Prostate, and Other Cancers and Tumors 0.153
HCC 17 Diabetes with Acute Complications 0.307
HCC 18 Diabetes with Chronic Complications 0.307
HCC 19 Diabetes without Complications 0.106
HCC 21 Protein‐Calorie Malnutrition 0.554
HCC 22 Morbid Obesity 0.262
HCC 23 Other Significant Endocrine and Metabolic Disorders 0.212
HCC 27 End‐Stage Liver Disease 0.913
HCC 28 Cirrhosis of the Liver 0.381
0.307+0.554+0.2121.073
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

13
Current CMS‐HCC Model Structure
• A coefficient or “weight” is assigned to each category of chronic complex diagnoses as well as severe acute diagnoses
• Each unrelated HCC that applies is additive
Age, sex, disability status, etc.
Health status
Adjusts future
payments
0.307+0.554+0.2121.0730.73
14
Current CMS‐HCC Model Structure (cont.)
• A coefficient or “weight” is assigned to each category of chronic complex diagnoses as well as severe acute diagnoses
• Each unrelated HCC that applies is additive
1.803
Risk Adjustment Factor (RAF) Score
Age, sex, disability status, etc.
Health status
Adjusts future
payments
0.307+0.554+0.2121.0730.73
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
15
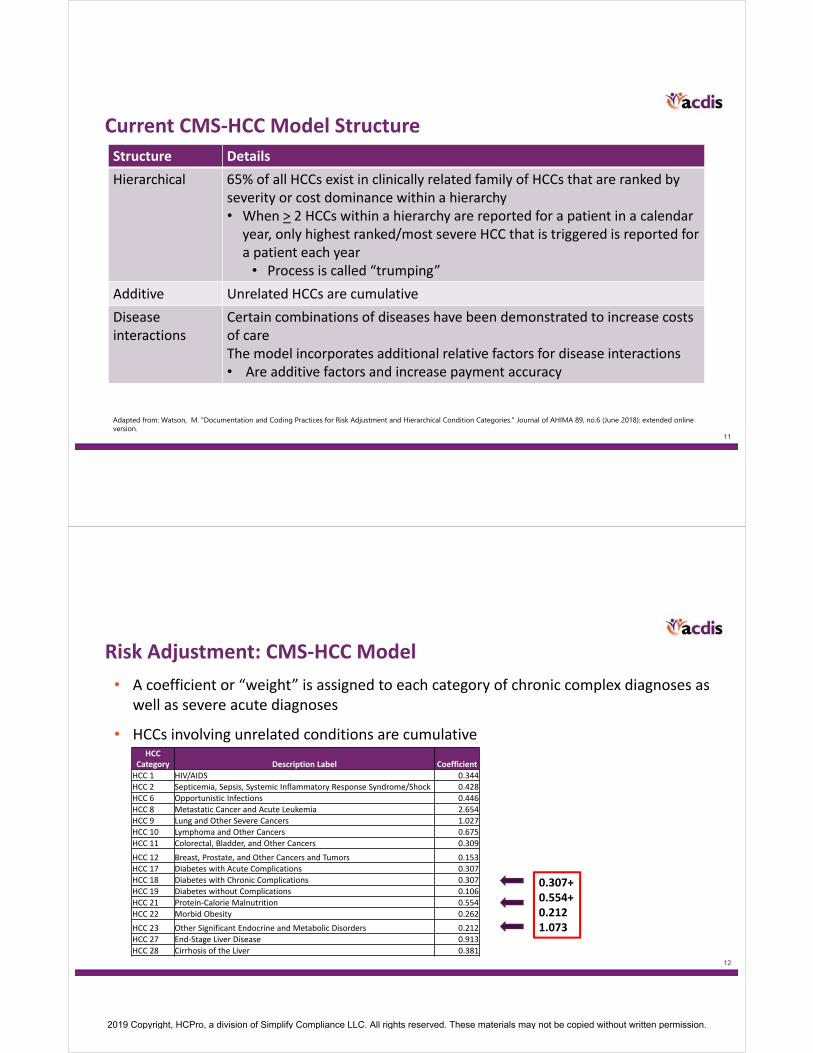
All conditions precisely documented
84 year old female – nondual aged
.540
COPD J44.9 (HCC 111) .335
Diabetes w/ diabetic CKD E11.22 (HCC 18)
.307
CKD stage 5 N18.5 (HCC 136) .284
Chronic diastolic CHF I50.32 (HCC 85)
.310
Disease interaction (DM + CHF) .152
Disease interaction (CHF + RF) .202
Disease interaction (CHF + COPD)
.191
Total RAF score 2.321
PMPM payment $1,857
Annual payment $22,282
Roberta Smith’s clinical picture: Type 2 diabetic with CKD stage 5, chronic diastolic CHF, & COPD
Demographics
Diagnoses supported in encounter
documentation
Interaction coefficients
added by CMS
Risk score
Risk adjustment payment
Provider impact –based on specificity and comprehensive documentation
Current 2019 v.23 $800 base rate
How It All Adds Up!
16
2020 Methodology Changes
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

17
Key Changes That Impact Risk Adjustment
• Alternative Payment Condition Count model (APCC)
• Additional HCCs added to the model
– Ensuring capture and validation of diagnoses
• Risk score calculation percentages
18
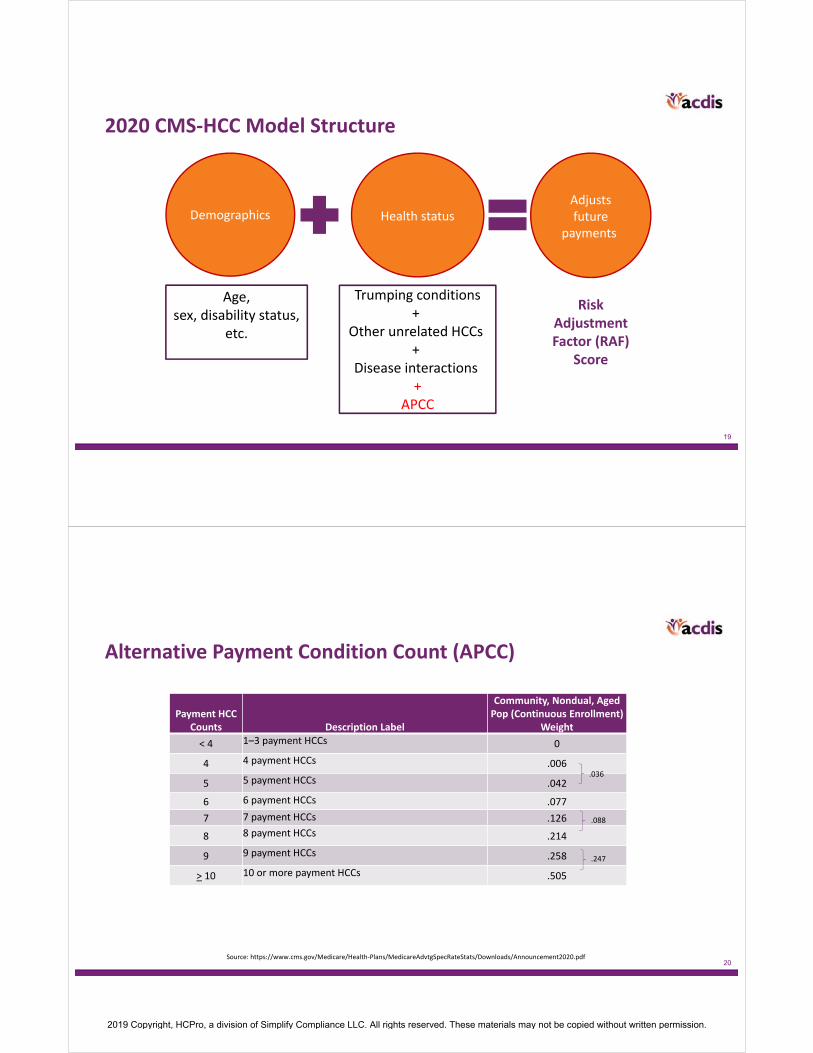
2019 CMS‐HCC Model Structure
Risk Adjustment Factor (RAF)
Score
Demographics Health status
Trumping conditions+
Other unrelated HCCs+
Disease interactions
Age, sex, disability status,
etc.
Adjusts future
payments
2019 CMS‐HCC Model Structure
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
19
2019 CMS‐HCC Model Structure
Risk Adjustment Factor (RAF)
Score
Demographics Health status
Trumping conditions+
Other unrelated HCCs+
Disease interactions+
APCC
Age, sex, disability status,
etc.
Adjusts future
payments
2020 CMS‐HCC Model Structure
20Source: https://www.cms.gov/Medicare/Health‐Plans/MedicareAdvtgSpecRateStats/Downloads/Announcement2020.pdf
Alternative Payment Condition Count (APCC)
Payment HCC Counts Description Label
Community, Nondual, Aged Pop (Continuous Enrollment)
Weight
< 4 1–3 payment HCCs 0
4 4 payment HCCs .006
5 5 payment HCCs .042
6 6 payment HCCs .077
7 7 payment HCCs .126
8 8 payment HCCs .214
9 9 payment HCCs .258
> 10 10 or more payment HCCs .505
.036
.088
.247
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

21
All conditions precisely documented
84 year old female – nondualaged
.528
COPD J44.9 (HCC 111) .335
Diabetes w/ diabetic CKD E11.22 (HCC 18)
.302
CKD stage 5 N18.5 (HCC 136) .289
Chronic diastolic CHF I50.32 (HCC 85)
.331
Disease interaction (DM + CHF) .121
Disease interaction (CHF + RF) .156
Disease interaction (CHF + COPD) .155
D4 – 4 payment HCCs .006
Total RAF score 2.223
PMPM payment $1,778
Annual payment $21,341
Roberta Smith’s clinical picture: Type 2 diabetic with CKD stage 5, chronic diastolic CHF, & COPD
Demographics
Diagnoses supported in encounter
documentation
Interaction coefficients
added by CMS
Risk score
Risk adjustment payment
Provider impact –based on specificity and comprehensive documentation
$800 base ratev.23 w APCC
Condition count
How It All Adds Up!
22
Hierarchy involving new HCCs for dementia and pressure ulcers
HCC HCC Title Trumps
51 Dementia with Complications (2020 HCC) 52
52 Dementia without Complications (2020 HCC) none
157 Pressure Ulcer of Skin with Necrosis Through to Muscle, Tendon, or Bone
158, 159, 161
158 Pressure Ulcer of Skin with Full Thickness Skin Loss
159, 161
159 Pressure Ulcer of Skin with Partial Thickness Skin Loss (2020 HCC)
161
161 Chronic Ulcer of Skin, Except Pressure noneSource: https://www.cms.gov/Medicare/Health‐Plans/MedicareAdvtgSpecRateStats/Downloads/Announcement2020.pdf
2020 Changes to CMS‐HCC Risk Adjustment Methodology: Alternative Payment Condition Count Model (APCC)
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

23Source: https://www.cms.gov/Medicare/Health‐Plans/MedicareAdvtgSpecRateStats/Downloads/Announcement2020.pdf
Key Changes That Impact Risk Adjustment
• Data used to calculate risk scores
• 50% calculated with 2017 CMS‐HCC model and diagnoses submitted on RAPS and FFS claims
• 50% calculated with alternative payment condition count model, using diagnoses submitted on encounter data records, RAPS inpatient records, and FFS claims
24
Key Changes: Encounter Data TransitionTransition plan
2015
RAPS EDS
2016
RAPS EDS
2017
RAPS EDS
2018
RAPS EDS
2019
RAPS EDS
2020
RAPS EDS
2015
RAPS EDS
2016
RAPS EDS
2017
RAPS EDS
2018
RAPS EDS
2019
RAPS EDS
Actual
Centers for Medicare & Medicaid Services’ Transition from Risk Adjustment Processing System (RAPS) Data to Medicare Advantage (MA) Encounter Data for Risk Score Calculation; GAO‐17‐223Medicare Advantage Rates & Statistics; Announcements 2015‐2020; https://www.cms.gov/Medicare/Health‐Plans/MedicareAdvtgSpecRateStats/Announcements‐and‐Documents.html?DLSort=2&DLEntries=10&DLPage=1&DLSortDir=descending.
2020
RAPS EDS
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

25
What’s the Effect of the Transition?
• Study conducted in 2017 with eight Medicare Advantage payers accounting for approx. 1 million beneficiaries to compare difference in scores and HCC capture based on methodologies
RAPS• Prevalence rate for top 10 HCCs
‒ 11.5% in 2014 ‒ 12.2% in 2015
• % of HCCs per patient‒ 28.2% with 0 HCCs‒ 25.3% with 1 HCC‒ 15.5% with 2 HCCs‒ 29.0% with 3 or more HCCs
EDS• Prevalence rate for top 10 HCCs
‒ 6.9% in 2014‒ 9.2% in 2015
• % of HCCs per patient‒ 39.3% with 0 HCCs‒ 24.7% with 1 HCC‒ 15.3% with 2 HCCs‒ 20.7% with 3 or more HCCs
RAPS to EDS Collaboration: A Data‐Driven Analysis; National Medicare Advantage Summit; April 2017
26
Ensuring HCC Capture
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

27
Hierarchy involving new HCCs for dementia and pressure ulcers
HCC HCC Title Trumps
51 Dementia with Complications (2020 HCC) 52
52 Dementia without Complications (2020 HCC) none
157 Pressure Ulcer of Skin with Necrosis Through to Muscle, Tendon, or Bone
158, 159, 161
158 Pressure Ulcer of Skin with Full Thickness Skin Loss
159, 161
159 Pressure Ulcer of Skin with Partial Thickness Skin Loss (2020 HCC)
161
161 Chronic Ulcer of Skin, Except Pressure noneSource: https://www.cms.gov/Medicare/Health‐Plans/MedicareAdvtgSpecRateStats/Downloads/Announcement2020.pdf
2020 Changes to CMS‐HCC Risk Adjustment Methodology: Alternative Payment Condition Count Model (APCC)
28
CMS‐HCCs 51 and 52: Dementia With and Without Complications
HCC 51: Dementia with ComplicationsExamples:• Vascular dementia with behavioral disturbance
• Dementia in other diseases classified elsewhere with behavioral disturbance
• Unspecified dementia with behavioral disturbance
• Hydrocephalus – multiple types
‒ Includes normal pressure hydrocephalus
HCC 52: Dementia without Complications Examples: • Alzheimer's disease
‒ Early onset‒ Late onset‒ Other Alzheimer's disease‒ Unspecified
• Dementia with Lewy bodies• Vascular dementia without behavioral disturbance • Unspecified dementia without
behavioral disturbance• Dementia in other diseases classified elsewhere
without behavioral disturbance • Pick's disease• Creutzfeldt‐Jakob disease
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

29
CMS‐HCC 159: Pressure Ulcer of Skin with Partial Thickness Skin Loss
Pressure‐induced injury staging:
Stage 1 – Skin intact but with nonblanchable redness
• Non‐HCC
Stage 2 – Partial‐thickness loss of skin with exposed dermis
• New HCC
Stage 3 – Full‐thickness loss of skin, in which adipose (fat) is visible in the ulcer and granulation tissue and epibole (rolled wound edges) are often present
• HCC 158
Stage 4 – Full‐thickness skin and tissue loss with exposed or directly palpable fascia, muscle, tendon, ligament, cartilage, or bone in the ulcer
• HCC 157
Unstageable ulcers (HCC 158)
30
Step 1Document diagnosis with specificity
Step 2Link diagnosis to MEAT criteria component in note
Step 3Submit diagnosis with proper ICD‐10‐CM code to claim
Monitor EvaluateAssessTreat
Or
Or
Or
Documentation Requirements for HCC Assignment
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

31
Diagnosis
Documentation demonstrating your addressed
diagnosis
The Importance of Linking: The MEAT Criteria
32
Monitor
Evaluate
Assess
Treat
Examples:
• Essential HTN: Stable on lisinopril (assess and treat)
• Chronic systolic heart failure: Well compensated (assess)
• COPD: Worsening sx, will check PFTs, add inhaled steroid (evaluate, assess, treat)
Or
Or
Or
Documentation Requirements for HCC Assignment
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

33
Documentation Scenario
CC: Weight loss
HPI: 68‐year‐old female with carotid stenosis, HTN, and hyperlipidemia who has residual right hemiplegia since 2013 stroke. Has been frequently bedbound with minimal help with ADLs for past 6 months. Didn't like home health caregivers so fired them after 3 weeks. Poor po intake with unintentional 14 lb. weight loss over this same period.
PMH:
Stroke 2013
HTN
Hyperlipidemia
34
Documentation Scenario
ROS: As above. Otherwise was evaluated by wound care team recently.
Exam: BP 150/60 HR 68 reg R 16 T afebrile BMI 17
General: Cachectic‐appearing pale female.
CV: Cor RRR with occasional ectopy. Pulses diminished at feet.
Neuro: Right upper extremity with 3/5 grip and arm strength. RLE 2/5 strength throughout.
Skin: Coccyx with pink, moist wound bed measuring 4x5 cm (wider than 4 months ago). Partial‐thickness skin loss with no exposed adipose or deeper tissue. No infectious signs.
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

35
Documentation Scenario
Visit diagnoses:
1. Cachexia
2. Coccyx pressure injury with partial‐thickness skin loss
3. Stroke 2013
4. Right hemiplegia due to above
Plan:
1. Encouraged to increase caloric intake
2. Refer for home health caregiver
3. F/u with wound care team
36
Documentation Scenario
Ques ons:
• Is MEAT sa sfied for the coccyx pressure injury? ‒ Yes. The wound was assessed and described adequately.
• Skin: Coccyx with pink, moist wound bed measuring 4x5 cm (wider than 4 months ago). Partial‐thickness skin loss with no exposed adipose or deeper tissue. No infectious signs.
• Does a partial‐thickness (stage 2) pressure ulcer trigger an HCC in 2019? ‒ Not yet. It will in 2020 as part of the APCC implementa on .
• What additional step should providers be encouraged to do to enhance likelihood of HCC capture? ‒ Submit proper code for each diagnosis satisfying MEAT criteria.
• L89.152 Pressure ulcer of sacral region, stage 2
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

37
What’s Coming?
38
• Implementation of extrapolation for RADV findings• Different platforms for patient engagement
‒ Home/mobile care‒ Telehealth‒ Retail care‒ Telephone support
• Social Determinants of Health (SDoH)‒ Are there codes for that?
Other Buzz in the Industry
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

39
Is There a Code for That?
Z56.0 Unemployment, unspecified
Z59.0 Homelessness
Z59.1 Inadequate housing
Z59.4 Lack of adequate food and safe drinking water
Z59.5 Extreme poverty
Z59.6 Low income
Z59.7 Insufficient social insurance and welfare support
Z59.8 Other problems related to housing and economic circumstances
Z59.9 Problem related to housing and economic circumstances, unspecified
40
• Implementation of extrapolation for RADV findings
• Different platforms for patient engagement ‒ Home/mobile care‒ Telehealth‒ Retail care‒ Telephone support
• Social Determinants of Health (SDoH)‒ Are there codes for that? YES, although vague‒ Additional codes with specificity proposed for 2020
• Z59.61 Unable to pay for prescriptions• Z59.64 Unable to pay for transportation• Z60.82 Inadequate social interaction
https://www.cdc.gov/nchs/data/icd/Topic‐packet‐March‐2019‐Part‐2Vs3.pdf
Other Buzz in the Industry
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

41
• Engage your providers!‒ How do you do that?
• Keep apprised of changes‒ How do you do that?
• Start education now for 2020 changes‒ Why do that?
• Start building processes to support HCC capture‒ Why do that?
What Should You Be Doing Now?
42
References• Centers for Medicare and Medicaid Services. Medicare Managed Care Manual. Chapter 7 – Risk Adjustment, 70 – Risk Adjustment Models – Overview.
• CMS.gov HHS‐Developed Risk Adjustment Model Algorithm "Do It Yourself (DIY)" Software Instructions.
• Gilmer, T. Risk Adjustment Using CDPS. Research Data Assistance Center; cdps.ucsd.edu
• Medicare Advantage Rates & Statistics; “Announcements” 2015–2020. https://www.cms.gov/Medicare/Health‐Plans/MedicareAdvtgSpecRateStats/Announcements‐and‐Documents.html?DLSort=2&DLEntries=10&DLPage=1&DLSortDir=descending.
• Murrin, S. “Medicare Advantage Encounter Data Show Promise for Program Oversight, But Improvements Are Needed.” DHHS Office of Inspector General (OEI‐03‐15‐00060), January 2018. https://oig.hhs.gov/oei/reports/oei‐03‐15‐00060.asp
• Palmetto GBA. “Medicare Advantage & Part D Communications Handbook.” August 2018. https://www.csscoperations.com/internet/cssc4.nsf/files/Medicare%20Advantage%20Communications%20Handbook%2020180810.pdf/$FIle/Medicare%20Advantage%20Communications%20Handbook%2020180810.pdf
• Risk Adjustment for EDS & RAPS User Group. April 19, 2018. https://www.csscoperations.com/internet/cssc4.nsf/DocsCat/CSSC~CSSC%20Operations~Medicare%20Advantage%20Encounter%20Data%20and%20RAPS%20Data~User%20Group~AZJ8PF0127?open&navmenu=Medicare^Advantage^Encounter^Data^and^RAPS^Data||||
• Risk Adjustment for EDS & RAPS User Group. May 17, 2018. https://www.csscoperations.com/internet/cssc4.nsf/DocsCat/CSSC~CSSC%20Operations~Medicare%20Advantage%20Encounter%20Data%20and%20RAPS%20Data~User%20Group~AZJ8TX8643?open&navmenu=Medicare^Advantage^Encounter^Data^and^RAPS^Data||||
• Swadi, A. “RAPS to EDS Collaboration: A Data‐Driven Analysis.” National Medicare Advantage Summit. April 6, 2017. http://www.ehcca.com/presentations/medadvsummit/swadi_ms2.pdf
• The Henry J. Kaiser Family Foundation. “Medicare Advantage” Fact Sheet. October 2017. https://www.kff.org/medicare/fact‐sheet/medicare‐advantage/
• United States Government Accountability Office. “Medicare Advantage: Limited Progress Made to Validate Encounter Data Used to Ensure Proper Payments.” GAO‐17‐223, January 2017. https://www.gao.gov/assets/690/682145.pdf
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

43
Thank you. Questions?
In order to receive your continuing education certificate(s) for this program, you must complete the online evaluation. The link can be found in the continuing education section of the program guide.
2019 Copyright, HCPro, a division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.