Embed Size (px)
DESCRIPTION
Citation preview

RIEMA Grant Programs
State Administrative Agency (SAA) for all Homeland Security Grant Programs.

•State Homeland Security Grant Program (SHSP)State Homeland Security Grant Program (SHSP) •Urban Area Security Initiative (UASI)Urban Area Security Initiative (UASI)
•Emergency Management Performance Grant (EMPG)Emergency Management Performance Grant (EMPG) •Citizens Corp Program (CCP) Citizens Corp Program (CCP)
•Emergency Operation Center (EOC)Emergency Operation Center (EOC)
•Buffer Zone Protection Program (BZPP)Buffer Zone Protection Program (BZPP)
These Grants includeThese Grants include; ;

RIEMA Reimbursements• All RIEMA grants are reimbursement based.
The process is based upon State requirements and Audit recommendations
• All grants have certain conditions and assurances that are a requirement by the Federal Government if an entity is to receive Federal money.
• Signed Green Assurance Sheets must be returned within 60 days accepting grant, along with the signed blue Lobbyist Form and Single Audit Act Form.

Required Program Reports• Quarterly Progress Reports: A narrative
reflecting grant activity and status during last three months justifying program. Final quarterly will reflect project completed or carried over into future years funding.
• Quarterly Fiscal Reports: Form reflecting grant funds expended during period and balance available to spend. Final quarterly reflects money returned to RIEMA.

RHODE ISLAND EMERGENCY MANAGEMENT AGENCYHOMELAND SECURITY GRANT QUARTERLY PROGRESS REPORT
SUBGRANTEE: _ (City /Town/ Agency)___________ DATE: _____/_____/_____ ADDRESS: _________________________________________________________CITY: __________________________ STATE: RI ZIP CODE: ______________COMPLETED BY: _______(Should be project Coordinator)___________________
PHONE NUMBER: _______________________________________________________ SUBGRANT NUMBER __________ (Category/Fiscal Year/Project Letter) *located on grant award)
QUARTER OF FUNDING: PERIOD FROM: YEAR DATE DUE: __X__ 1st Quarter Jan. 1st – Mar. 31st _2011__ April 15th _____ 2nd Quarter April 1st – June 30th _______ July 15th _____ 3rd Quarter July 1st – Sept. 30th _______ Oct. 15th _____ 4th Quarter Oct. 1st – Dec. 31st _______ Jan. 15th
_____ Final Report All funds authorized spent and project completed.
Provide a short narrative to explain the federal expenditures, the project’sprogress, accomplishments and delays (additional page or attachments are acceptable):
(Please write the year next to the Period From Date)
______________________________________________________________ _______/_______/_______Authorized Agent Signature Date
PLEASE SEND REPORTS TO:Rhode Island Emergency Management Agency
645 New London AvenueCranston, RI 02920Attn: Richard Jones

RHODE ISLAND EMERGENCY MANAGEMENT AGENCYHOMELAND SECURITY GRANT QUARTERLY FISCAL REPORT
SUBGRANTEE: __ (City /Town/ Agency) ______________ DATE: _____/_____/_____ ADDRESS: ______________________________________________________________CITY: ____________________________________ STATE: RI ZIP CODE: _______________COMPLETED BY: _______________( Should be project Coordinator )_____________________PHONE NUMBER: _______________________________________________________________
SUBGRANT NUMBER –__00-125-FY10 SHSP__ (Category/Fiscal Year/Project Letter) *located on grant award
QUARTER OF FUNDING: PERIOD FROM: YEAR: DATE DUE: _____ 1st Quarter Jan. 1st – Mar. 31st __2011__ April 15th
__ X _ 2nd Quarter April 1st – June 30th ________ July 15th
_____ 3rd Quarter July 1st – Sept. 30th ________ Oct. 15th
_____ 4th Quarter Oct. 1st – Dec. 31st _________ Jan. 15th
_____ Final Report All funds authorized spent (See column b, cumulative).
TRANSACTIONS Previously Reported This Period Cumulativea. Amount paid out to vendors $3,000.00 $0 _____ $3,000.00b. Federal funds authorized __________ $10,000.00 _________c. Balance of funds not used $7,000.00
I have reviewed this fiscal report and certify that the information contained herein is true and correct to the best of my knowledge.
___________________________________ ____________________________________ Authorized Agent (Please Print) Signature
RIEMA USE ONLY_______________________________________________________________________________________________
Example Example

Quarterly Progress and Fiscal Reports Quarterly Progress and Fiscal Reports must be completed even if no funds must be completed even if no funds are expended or encumbered during are expended or encumbered during the quarter.the quarter.
Indicate in progress report that you Indicate in progress report that you are still using previous year grant are still using previous year grant funds or the reason your project start funds or the reason your project start has been delayed.has been delayed.

• Processing Reimbursements Requires:
1. RIEMA Reimbursement Form
2. Support Documents: A. Equipment: Detailed Invoices, Packing
Slips, Inventory Sheet and Cancelled Checks for purchases.
B. Training/Exercise: Syllabus, Signed Attendance Roster and Payroll Records/Checks for overtime/backfill.

RHODE ISLAND EMERGENCY MANAGEMENT AGENCY
GRANT REIMBURSEMENT REQUEST
Requesting Agency: Date Prepared:
Primary Contact: Federal Employer ID# (FEIN):
Address: State & Zip: Phone:
Sub-grant award # (application #): Project ID:
Fiscal Contact: Title: Phone:
Check One:
FY 2009
FY 2010
FY 2011
FY 2012
Solution Original Previous Current Balance Area Budget Reimbursement Request Remaining
A. Equipment
B. Planning
C. Training
D. Exercises
TOTALS
PAYMENT REQUEST AMOUNT Authorized Agency Official (Please Print) (Should equal total current reimbursement)
Signature (Please Sign in Blue Ink) I, the above signed, hereby certify that this request for reimbursement is in full accordance with the
approved project budget, as approved by the Rhode Island Emergency Management Agency.
PLEASE ATTACH COPIES OF BACKUP DOCUMENTS, RECEIPTS, INVOICES, ETC. TO THIS FORM

RHODE ISLAND EMERGENCY MANAGEMENT AGENCY
GRANT REIMBURSEMENT REQUEST
Requesting Agency: Grant Town Date Prepared: 1-11-11
Primary Contact: John Doe Chief Federal Employer ID# (FEIN):
Address: Main Street State & Zip: RI 02920 Phone: 401-555-5555 ext 555
Sub-grant award # (application #): 00-000-FY 00 SHSP Project ID: A
Fiscal Contact: Jane Doe Title: Finance Department Phone: 401-444-4444 ext 444
Check One:
FY 2009
FY 2010
FY 2011
FY 2012
Solution Original Previous Current Balance Area Budget Reimbursement Request Remaining
A. Equipment $100,000.00 $25,000.00 $25,000.00 $50,000.00
B. Planning $20,000.00 $0 $5,000.00 $15,000.00
C. Training $50,000.00 $10,000.00 $20,000.00 $20,000.00
D. Exercises $30,000.00 $30,000.00 $0 $0
TOTALS $200,000.00 $65,000.00 $50,000.00 $85,000.00
PAYMENT REQUEST AMOUNT Authorized Agency Official (Please Print) Chief John Doe (Should equal total current reimbursement)
$50,000.00 Signature (Please Sign in Blue Ink) I, the above signed, hereby certify that this request for reimbursement is in full accordance with the
approved project budget, as approved by the Rhode Island Emergency Management Agency.
PLEASE ATTACH COPIES OF BACKUP DOCUMENTS, RECEIPTS, INVOICES, ETC. TO THIS FORM
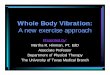
Example Example

Proof of attendance at training or exercise requires a sign in roster, or signed request for compensation by attendee.
Proof individual was paid monetary compensation by sub-grantee. Proof can be copies of actual payroll checks, detailed payroll sheets from finance department, or spread sheet indicating each persons hours and overtime rate signed by Finance Director.

Example of Example of spread sheet spread sheet signed by signed by finance finance director.director.
Training / Course Title: HAZMAT
Date: 1-10-11 Start Time 0800 AM End Time: 4:00 PM
Location of Training: 1 Main Street, Safeville, RI
Instructor's Name(s): Capt. Peebody & Lt. Sherman
Attendee's Name Rank On Duty OT Hrs Hrly Rate Total Pay
Smith, John Capt 8 $35.00 $280.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
Totals Personnel Costs $280.00
Request for Reimbursment $0.00
By my signature below, I attest to the fact that the employees above did each received
monetary compensation at their overtime rate for attending training on the above date(s).
(Finance Director's Name), Finance Director (City/Town of ) Date

By my signature below, I attest to the By my signature below, I attest to the fact that each employee listed above fact that each employee listed above did receive monetary compensation at did receive monetary compensation at their overtime rate for attending their overtime rate for attending training on the above date(s).training on the above date(s).
________________________________________________________________________________________________________ (Finance Director) (Date)(Finance Director) (Date)

Example of Example of sign in sheet sign in sheet signed by signed by instructorinstructor..

Food and Meals ReimbursementsFood and Meals Reimbursements
Nourishment and Hydration are eligible for Nourishment and Hydration are eligible for reimbursement if they meet one of the following criteria:reimbursement if they meet one of the following criteria:
• The training or exercise is eight or more hours in The training or exercise is eight or more hours in duration and it is logistically impractical to stop the duration and it is logistically impractical to stop the training or exercise to allow participates to obtain training or exercise to allow participates to obtain nourishment and hydration on their own.nourishment and hydration on their own.
OROR
•The training or exercise is eight or more hours and the The training or exercise is eight or more hours and the nourishment period is a “Working Lunch”. Working lunch nourishment period is a “Working Lunch”. Working lunch requires participants to continue working during the requires participants to continue working during the period by receiving training topic related instruction or a period by receiving training topic related instruction or a presentation pertaining to the exercise goals and presentation pertaining to the exercise goals and objectives.objectives.

Reimbursable Items?
•Responder Knowledge Base
RKB Website https://www.rkb.us/mel.cfm
Must provide documentation that item is Must provide documentation that item is allowable under the FEMA Responder allowable under the FEMA Responder Knowledge Base List.Knowledge Base List.

Generators>> >>Generators General | Grant Allowability | Previous Numbering This item is part of both the AEL and SEL.This equipment has been identified as requiring an Environmental Planning and Historic Preservation (EHP) review. Please refer to the EHP Program Page to the right, or consult your designated Program Analyst for guidance on your EHP submission. AEL / SEL Number: 10GE-00-GENR Title: Generators Description: Generators, varying types and sizes, including gasoline, diesel, propane, natural gas, alternator, gas turbine powered devices, etc. Important Features(Recommendations from IAB — NOT DHS requirement or part of DHS grant guidance): Portable or fixed. Operating Considerations(Recommendations from IAB — NOT DHS requirement or part of DHS grant guidance): Examine load capacity.Regular testing.Automatic transfer switch.Carbon monoxide detector.Heavy duty outdoor rated extension cords.Approved fuel storage containers.Fuel stabilizer.Run time (fuel capacity, fuel supply, resupply, etc.).Consider need for extended run time (greater than five days).Grounding needs, electrical connections (120/240 etc.).
* POD-List * Training Requirements (Recommendations from IAB — NOT DHS requirement or part of DHS grant guidance): Core Training: manufacturer's specification.Initial Training: Minimal (<1 day)Sustainment Training: Minimal (<1 day)
Example Example

Generators>> >>Generators General | Grant Allowability | Previous Numbering Print
Regular testing.Automatic transfer switch.Carbon monoxide detector.Heavy duty outdoor rated extension cords.Approved fuel storage containers.Fuel stabilizer.Run time (fuel capacity, fuel supply, resupply, etc.).Consider need for extended run time (greater than five days).Grounding needs, electrical connections (120/240 etc.).
* POD-List *
Initial Training: Minimal (<1 day)Sustainment Training: Minimal (<1 day) Operation Stonegarden Grant Program (OPSG): YES Interoperable Emergency Communications Grant Program (IECGP) : NO State Homeland Security Program / Urban Area Security Initiative (SHSP/UASI): YES Law Enforcement Terrorism Prevention Program (LETPP) or 2008 SHSP/UASI 25% Quota: YES Metropolitan Medical Response System (MMRS): YES Citizen Corps Program (CCP): NO Emergency Management Performance Grant (EMPG): YES Chemical Sector Buffer Zone Protection Program (Chem-BZPP) (2006 Only): YES Buffer Zone Protection Program (BZPP): YES Transit Security Grant Program (TSGP): YES Port Security Grant Program (PSGP): YES Intercity Bus Security Grant Program (IBSGP): YES Urban Areas Security Initiative-Nonprofit Security Grant Program (UASI-NSGP): NO Public Safety Interoperable Communications (PSIC): YES Emergency Operations Center Grant Program (EOC): YES
Knowledge Links
Related FEMA Grant(s) FEMA's FEMA's Environmental Environmental Planning and Planning and Historic Preservation Historic Preservation (EHP) Program(EHP) Program
Example Example

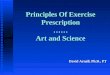
Other Assurance Requirements
• Identification of equipment purchased
• Inventory of equipment purchased
• NIMS ComplianceNIMSCAST ReportICS TrainingResource TypingCredentialing

•Equipment with a value of $500.00 or more Equipment with a value of $500.00 or more must be labeled and identified as being must be labeled and identified as being purchased with federal grant funds. purchased with federal grant funds.
•An Equipment Inventory List must be kept An Equipment Inventory List must be kept and copies of inventory lists must be and copies of inventory lists must be submitted with final quarterly reports.submitted with final quarterly reports.
•Inventory lists must be updated periodically Inventory lists must be updated periodically to reflect equipment that was damaged, lost to reflect equipment that was damaged, lost or liquidated. or liquidated.

NAME OF AGENCY SUBMITTING INVENTORY : North Providence Fire DECON
NAME OF RECIPIENT RESPONSIBLE FOR GRANT : Chief Leonard Albanese
PHONE NUMBER OF RESPONSIBLE RECIPIANT : 401-888-888
DATE INVENTORY COMPLETED OR UPDATED : 7/8/10
Item #Description of item purchased with DHS Funds with a value of
$500.00 or more.
Serial Number CostGrant
NumberGrant Year Purchase Date Disposal Date
160 Minute Scott Air Pack S326789-1278 3,300.0024-48 FY06 4/3/2006 6/1/2010
260 Minute Scott Air Pack S43790-289 3,500.0024-48 FYY09 5/25/2010
3Del Laptop Computer 647902bc679 1,500.0024-48 FY10 6/17/2010
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
Example Example

(National Information Management System)
NIMSCAST Report
All Federal Grants Require All Federal Grants Require Grantees to Be Grantees to Be NIMSNIMS Compliant Compliant
(NIMS Compliance Assistance Support Tool)
Every Local EMA Director must complete Every Local EMA Director must complete NIMSCAST each year by September 30NIMSCAST each year by September 30thth..
http://www.fema.gov/nimscast/ResetPasswordSubmit.do

Discipline IS 800 IS 700/100 IS 200ICS 300
ICS 400
IS 701
IS 702 IS 703
IS 704
Notes
Local/County Elected Officials X (700) 1
Local/ County Elected Officials involved in EM operations X X X X
Local Emergency Management Director X X X X X X
County Emergency Management Director X X X X X X X X
Public Works Director X X
Public Works/Road Commissioner X
School/Campus Emergency Team Leaders X X X 2
School/Campus Emergency Team X 7
Public Utilities Management X X 3
Public Utilities Worker X
Hospital Emergency Response Team HERT X X 4
Dept Heads/Deputies X X X X X X 8/9
Supervisors X X
Technicians/Operators X
State/County/Local Law Enforcement Dept Heads/Deputies X X X X X X 8/9
State/County/Local Law Enforcement Supervisors X X
State/County/Local Law Enforcement Officers X
Fire Service Dept Heads/Deputies X X X X X X 8/9
Fire Service Supervisors X X
Fire Service Firefighters X
DST/RRT HAZMAT Technicians X X X 5
DST/RRT HAZMAT Operations/ Responders X X
MACC/EOC Management X X X X X X X X
MACC/EOC Staff X X X X X X
IMAT Level III/IV X X X X X X X X 6
Public Information Officers/Designees X X X 6
Supervisor and Deputy Supervisor X

NIMS Requires Sub-Grantees to Resource Type all Equipment and Teams.
• Resource Typing is the categorization and description of response resources that are commonly exchanged in disasters through Mutual Aide Agreements.
• RIEMA is developing a Web EOC based data entry program that will be available to all cities and towns to utilize for Resource Typing.

NIMS Requires Sub-Grantees to “Credential” NIMS Requires Sub-Grantees to “Credential” Emergency Response Personnel.Emergency Response Personnel.
Credentialing is an evidence-based system that Credentialing is an evidence-based system that defines levels of proficiency for all of the FEMA’s defines levels of proficiency for all of the FEMA’s Disaster Workforce position commonly exchanged in Disaster Workforce position commonly exchanged in disasters through Mutual Aide Agreements.disasters through Mutual Aide Agreements.
Credentialing ensures that during the time of a Credentialing ensures that during the time of a disaster FEMA has prepared and qualified staff to disaster FEMA has prepared and qualified staff to execute its mission.execute its mission.
RIEMA is developing a Credentialing Process that it RIEMA is developing a Credentialing Process that it will share with the local cities and town to meet will share with the local cities and town to meet NIMS requirements.NIMS requirements.

RIEMA
• Questions?
• Comments?
• Concerns?