Embed Size (px)
Citation preview

© 2013 Mayo Foundation for Medical Education and Research
Courtney M. Tomblinson, MD; S. Santino Cervantes, MD; April M. Landry, MD;
Richard E. Hayden, MD; Michael L. Hinni, MD
Department of Otolaryngology - Head and Neck Surgery – Mayo Clinic Hospital - Phoenix, Arizona
• The tubed submental flap is an additional
neopharyngeal reconstructive option for
patients with total laryngopharyngectomy.
• Large defects can be repaired in a single-
stage operation, reliably and rapidly.
• Donor site morbidity is low, as the tubed
submental flap is harvested from the same
surgical wound and does not require a
second surgical team nor microvascular
reconstruction
Conclusions
1. Howard BE, Nagel TH, Donald CB, Hinni ML, Hayden
RE. Oncologic safety of the submental flap for
reconstruction in oral cavity malignancies. Otolaryngol
Head Neck Surg 2013;149:40 .
2. Wang WH, Hwang TZ, Chang CH, Lin YC.
Reconstruction of pharyngeal defects with a submental
island flap after hypopharyngeal carcinoma ablation.
ORL 2012;74:304-309.
3. Patel UA, Bayles SW, Hayden RE. The submental flap:
a modified technique for resident training. Laryngoscope
2007;117:186-189.
4. Chu PY, Chang SY. Reconstruction after resection of
hypopharyngeal carcinoma: comparison of the
postoperative complications and oncologic results of
different methods. Head & Neck. 2005;27(10):901-8
5. Espitalier F et al. Results after U-shaped pectoralis
major myocutaneous flap reconstruction of
circumferential pharyngeal defects. Laryngoscope
2012;122:2677-2682
6. Lopez F et al. Outcomes following
pharyngolaryngectomy with fasciocutaneous free flap
reconstruction and salivary bypass tube. Laryngoscope
2012;123:591-596.
References
Discussion
Patients requiring total, circumferential laryngo-
pharyngectomy had limited options for reconstruction in
the past. These options include pectoralis major
myocutaneous flap, anterolateral thigh free flap, and free
jejunal interposition grafts. Significant morbidity is
associated with these reconstructions.
We submit a novel technique for circumferential total
laryngopharyngectomy reconstruction using a tubed
myocutaneous submental pedicled flap that decreases
morbidity and has acceptable functional outcome. To our
knowledge, this is the first successful application of this
technique. Previous studies report its use with partial
defects.
Technique
The pedicle of our submental flap consisted of venous drainage by the external jugular vein and was arterially based on the the submental artery, a branch of the facial artery. The skin paddle, measuring 15 cm in length by 8 cm in width, was carefully elevated, beginning with the superior incision, dissecting to the inferior border of the mandible to avoid cutaneous perforating vessels and releasing the mylohyoid muscle down.
The lesion, shown in Figure 2, crossed midline posteriorly and only a thin, 1 cm strip of pharyngeal mucosa could be salvaged. This was excised to prevent a second vertical anastamosis, completing the total laryngopharyngectomy. An 8cm defect remained between the native pharynx and the cervical esophagus.
The submental flap was rotated inferiorly, formed into a tube with the squamous epithelium lining the inner surface of the tube. The superior and inferior anastamoses were sutured closed. A nasogastric tube was placed to serve as a conduit. The final anastamosis was zippered shut from superior to inferior over the nasogastric tube.
The mylohyoid and digastric muscles were incorporated into the flap so as to add extra bulk on the superficial portion of the neopharyngeal reconstruction once tubed. After a left selective neck dissecion of levels II-V, the stoma was matured and the neck was closed primarily without extraneous tissue or grafting.
Introduction
82 year old male with a six-month history of non-
productive cough and odynophagia and a previously
resected and irradiated T1 right glottic tumor. Endoscopic
examination revealed a left piriform sinus lesion with
apparent involvement of the left cricoarytenoid joint and
immobility of the left true vocal cord. PET scan revealed
avidity in the left side of the larynx and hypopharynx.
The tumor was visualized via direct laryngoscopy and
esophagoscopy, spanning from the left piriform sinus onto
the left arytenoid and extending into the party wall. The
burden was too extensive to be performed via an
endoscopic approach and the patient underwent total
laryngopharyngectomy, left selective neck dissection, and
neopharyngeal reconstruction with a myocutaneous
submental pedicled flap. A nasogastric feeding tube was
placed to serve as a conduit for the newly formed tubed
neopharynx.
A PEG tube was placed and tube feeds were started 24
hours later. The nasogastric tube conduit was removed
prior to discharge. The patient began an oral diet on POD
17. He did not experience any localized infection and no
evidence of leak.
He completed adjuvant radiation three months post-
operatively and has experienced dysphagia since
radiation. Exam at his last visit reveals a mildly stenotic
inlet at the superior anastamosis and a second stenosis
at the inferior anastamotic suture line of the neopharynx.
He underwent esophageal dilation with significant
improvement in the neopharyngeal lumen.
Case Report
Figure 3. A Esophagram five months post-operatively at
the level of the tubed submental flap revealing patent
neopharynx with ample passage of contrast material.
B Lateral view of repair at eleven months post-operatively
with positive aesthetic outcome.
Figure 2. A Surgical planning of submental flap skin paddle with an extended incision planned for a right neck dissection. Reprinted from Patel et al.
B Elevation of skin paddle with a right-sided vascular pedicle, mylohyoid as part of the submental flap, ipsilateral geniohyoid (thin arrow) and
contralateral digastric muscle (thick arrow). Reprinted from Patel et al. C Gross specimen, total laryngopharynx. D Superior is to the right, inferior to
the left. Immediately prior to total laryngopharyngectomy showing extensive tumor involvement in the party wall and crossing midline. E Zippered
lateral closure with superior and inferior anastomosis. Nasogastric tube has been placed as a conduit. F Complete closure of tubed submental flap
with mylohyoid muscle on the anterior surface of the neopharynx.
A
A B C
D E F
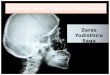
Figure 1. Axial CT demonstrating a left hypopharyngeal
mass with obliteration of the esophagus, invasion of the
larynx, and contralateral tumor extension.
A B
Hypopharyngeal carcinomas are commonly diagnosed
at advanced stages with a poor prognosis. Surgical
ablation may render a large defect, often requiring total
laryngopharyngectomy; the reconstruction of which is
challenging. Classically, options for the reconstructive
portion include anterolateral thigh free flap, pectoralis
major myocutaneous flap, and free jejunal flap.
The tubed submental flap offers an option that has the
advantage of being both pedicled and from a single
surgical wound, thereby decreasing donor site morbidity.
Additionally, the submental flap reconstruction can be
performed in a single-stage procedure and eliminates
the need for a two-team approach.
In our experience, the tubed submental flap is reliable
and is advantageous in that it can be rapidly harvested,
has a favorable arc of rotation, eliminates the need for
microvascular surgery, and permits size variability
during design. When necessary, a large paddle
measuring up to 6 x 18 cm can be harvested depending
on the defect. In addition, the pliability of the submental
flap allows for easy tube formation.
Inclusion of the ipsilateral mylohyoid muscle with the
digastric muscle during flap harvest aids in protection of
the vascular pedicle during dissection, can reduce
operative time, and can add bulk when desired. This
may be desirable when contemplating adjuvant
radiotherapy in an attempt to decrease fistula formation.
The Submental Myocutaneous Flap for
Circumferential Neopharyngeal Reconstruction:
A Novel Technique