Embed Size (px)
Citation preview
Rheumatoid Arthritis2013
Jeffrey Carlin, MD
Section Head,
Division of Rheumatology
Virginia Mason Medical Center
Rheumatoid Arthritis Symmetric, inflammatory polyarthritis,
involving large and small joints Serological studies may be negative at onset
and may remain negative in 15-20%! RA is a clinical diagnosis, no laboratory test is
diagnostic, just supportive!
Rheumatoid Arthritis:Patterns of Onset
Acute polyarticular Acute, severe onset 10-15 % Subacute 20%
Additive Palindromic
The Challenges of RA• Reliable diagnosis of early RA
– RA is a heterogeneous disease that differs substantially from patient to patient in presentation and progression
• Detection of early inflammatory arthritis• Detection of the earliest events that predictably
lead to destructive synovitis
Early RA: A problematic diagnosis
Most patients will not meet ACR criteria Most patients will not be sero-positive ( 19- 45%) Most patients will not seek medical care Most PCPs prefer to evaluate, rather than refer Many patients will remit with symptomatic Rx Histopathology similar: RA, ERA, UPA Few features to distinguish RA vs UPA
Duration, # Jts, RF+, CCP+, ESR/CRP

Longitudinal Course of RA
Klareskog L et al, Lancet 2009;373:659-672

The Natural History of RA
at presentation after 5 years after 15 years
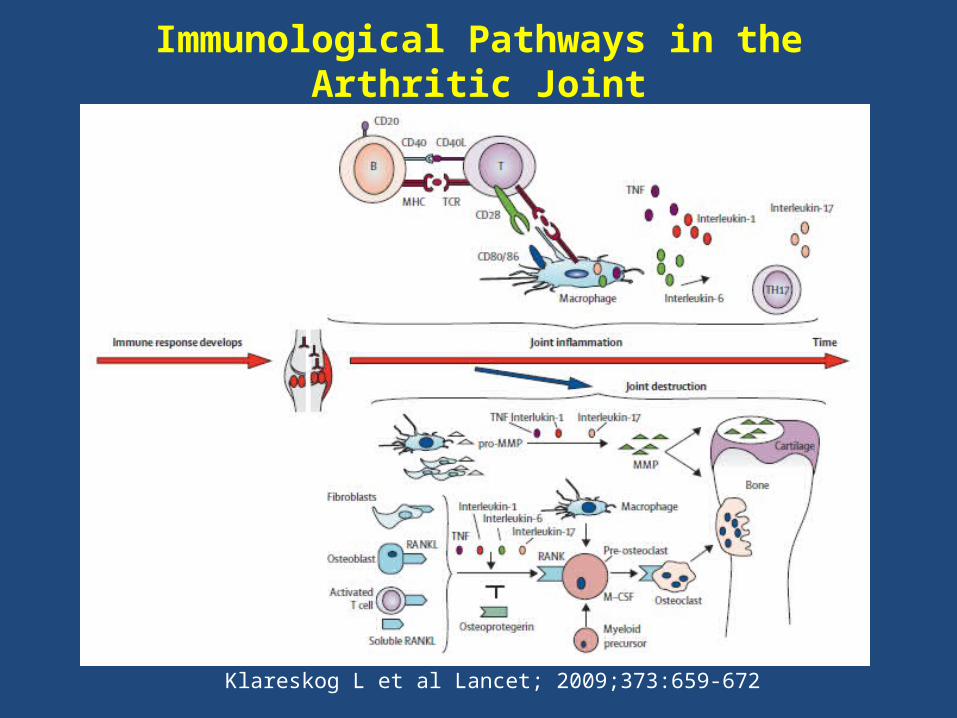
Immunological Pathways in the Arthritic Joint
Klareskog L et al Lancet; 2009;373:659-672
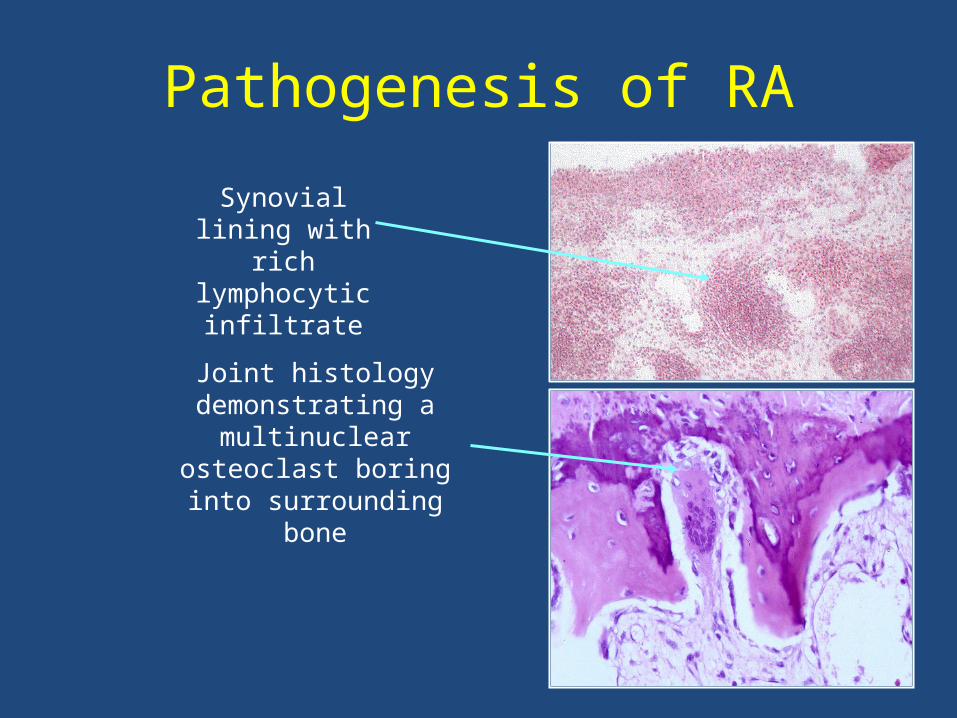
Pathogenesis of RA
Joint histology demonstrating a
multinuclear osteoclast boring into surrounding
bone
Synovial lining with rich
lymphocytic infiltrate
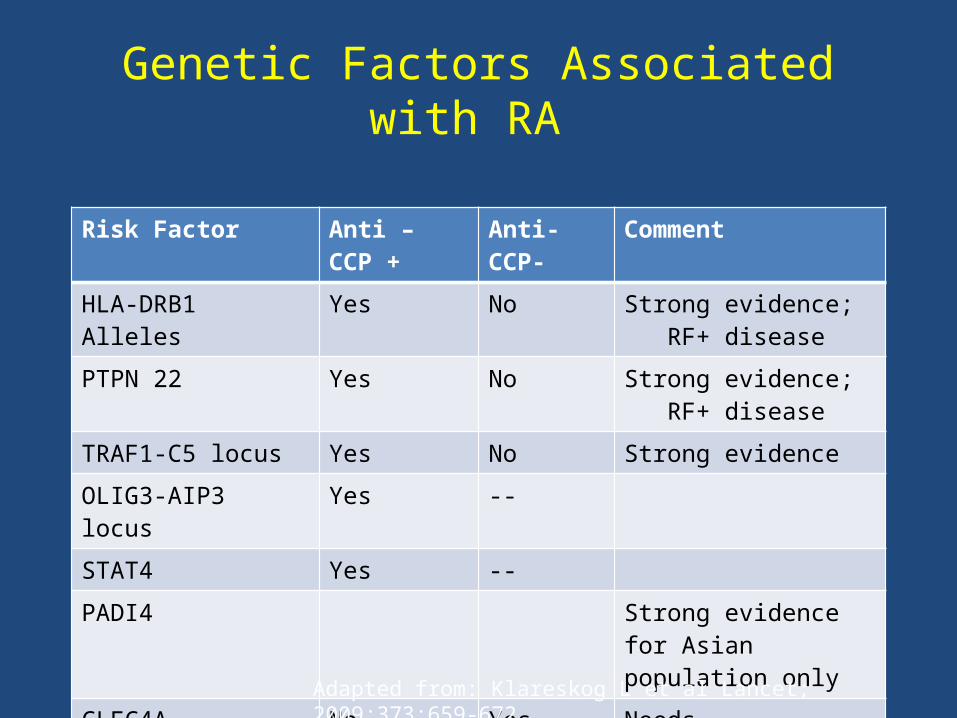
Genetic Factors Associated with RA
Risk Factor Anti – CCP +
Anti- CCP-
Comment
HLA-DRB1 Alleles Yes No Strong evidence; RF+ disease
PTPN 22 Yes No Strong evidence; RF+ disease
TRAF1-C5 locus Yes No Strong evidence
OLIG3-AIP3 locus Yes --
STAT4 Yes --
PADI4 Strong evidence for Asian population only
CLEC4A No Yes Needs confirmation
IRF5 No Yes Needs confirmation
Adapted from: Klareskog L et al Lancet; 2009;373:659-672
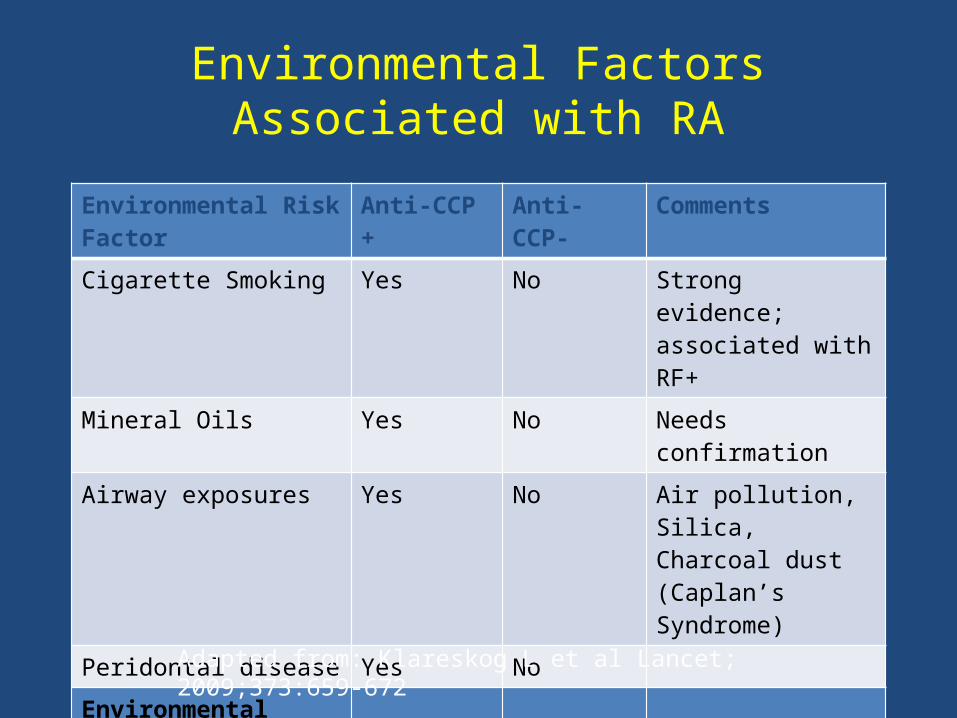
Environmental Factors Associated with RA
Environmental RiskFactor
Anti-CCP + Anti-CCP- Comments
Cigarette Smoking Yes No Strong evidence; associated with RF+
Mineral Oils Yes No Needs confirmation
Airway exposures Yes No Air pollution, Silica, Charcoal dust (Caplan’s Syndrome)
Peridontal disease Yes No
Environmental Protective Factor
Alcohol Yes Yes Needs confirmation
Adapted from: Klareskog L et al Lancet; 2009;373:659-672
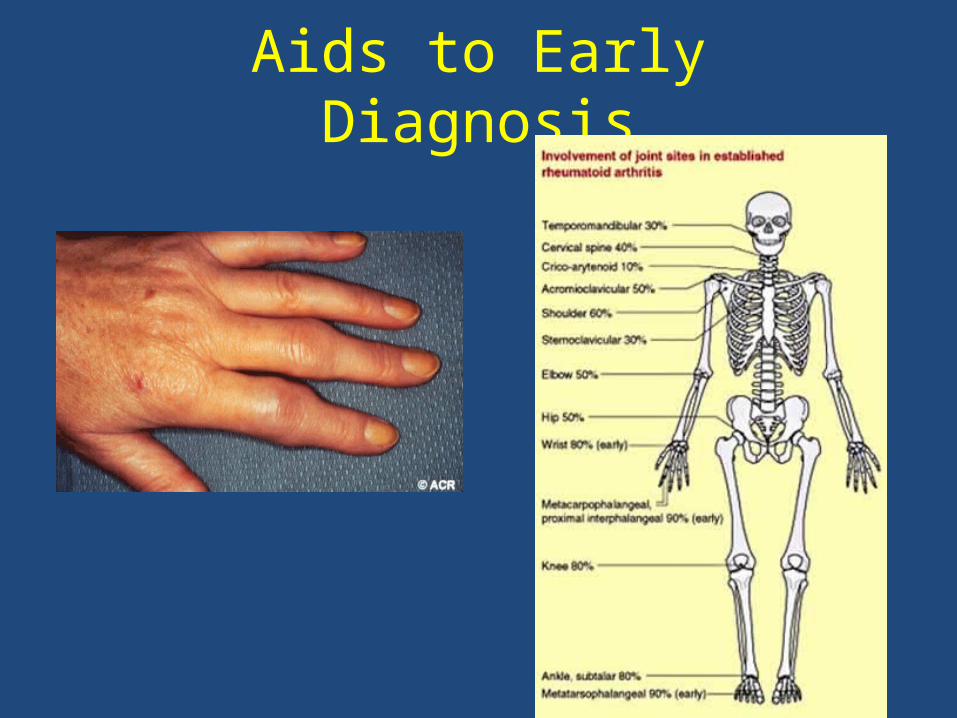
Aids to Early Diagnosis
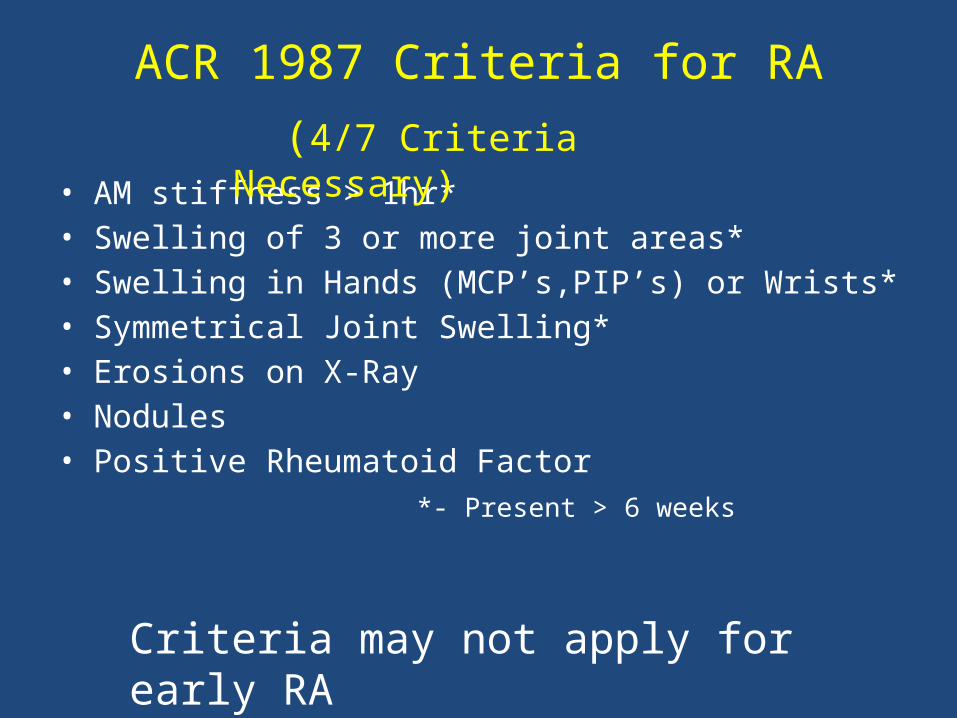
ACR 1987 Criteria for RA
• AM stiffness > 1hr*• Swelling of 3 or more joint areas*• Swelling in Hands (MCP’s,PIP’s) or Wrists*• Symmetrical Joint Swelling*• Erosions on X-Ray• Nodules• Positive Rheumatoid Factor
*- Present > 6 weeks
Criteria may not apply for early RA
(4/7 Criteria Necessary)
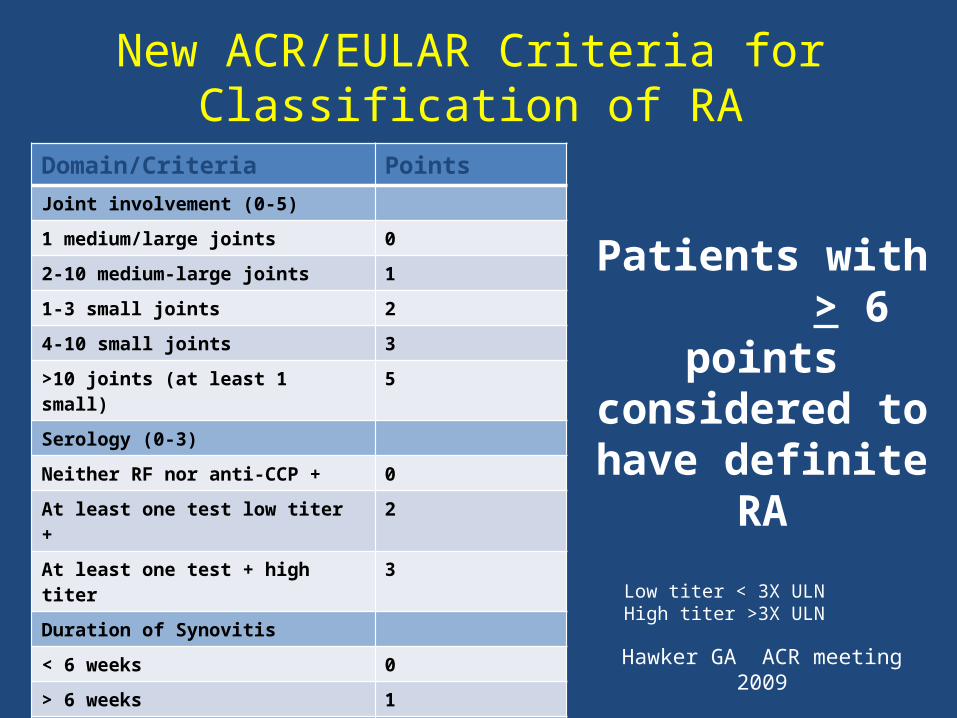
New ACR/EULAR Criteria for Classification of RA
Domain/Criteria PointsJoint involvement (0-5)
1 medium/large joints 0
2-10 medium-large joints 1
1-3 small joints 2
4-10 small joints 3
>10 joints (at least 1 small) 5
Serology (0-3)
Neither RF nor anti-CCP + 0
At least one test low titer + 2
At least one test + high titer 3
Duration of Synovitis
< 6 weeks 0
> 6 weeks 1
Acute Phase Reactants
Neither CRP or ESR elevated 0
Abnormal ESR/CRP 1
Patients with > 6 points
considered to have definite RA
Hawker GA ACR meeting 2009
Low titer < 3X ULNHigh titer >3X ULN
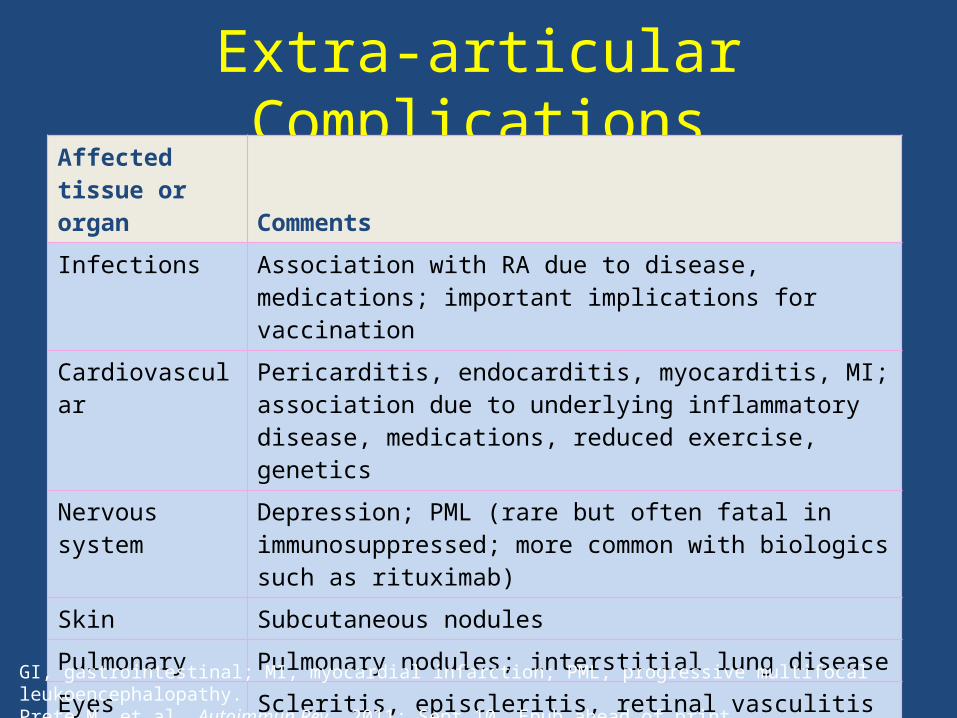
Extra-articular ComplicationsAffected tissue or organ Comments
Infections Association with RA due to disease, medications; important implications for vaccination
Cardiovascular Pericarditis, endocarditis, myocarditis, MI; association due to underlying inflammatory disease, medications, reduced exercise, genetics
Nervous system Depression; PML (rare but often fatal in immunosuppressed; more common with biologics such as rituximab)
Skin Subcutaneous nodules
Pulmonary Pulmonary nodules; interstitial lung disease
Eyes Scleritis, episcleritis, retinal vasculitis
Other Vasculitis, diabetes, GI bleeding, cancer (e.g., lymphoma)
GI, gastrointestinal; MI, myocardial infarction; PML, progressive multifocal leukoencephalopathy.Prete M, et al. Autoimmun Rev. 2011; Sept 10. Epub ahead of print.
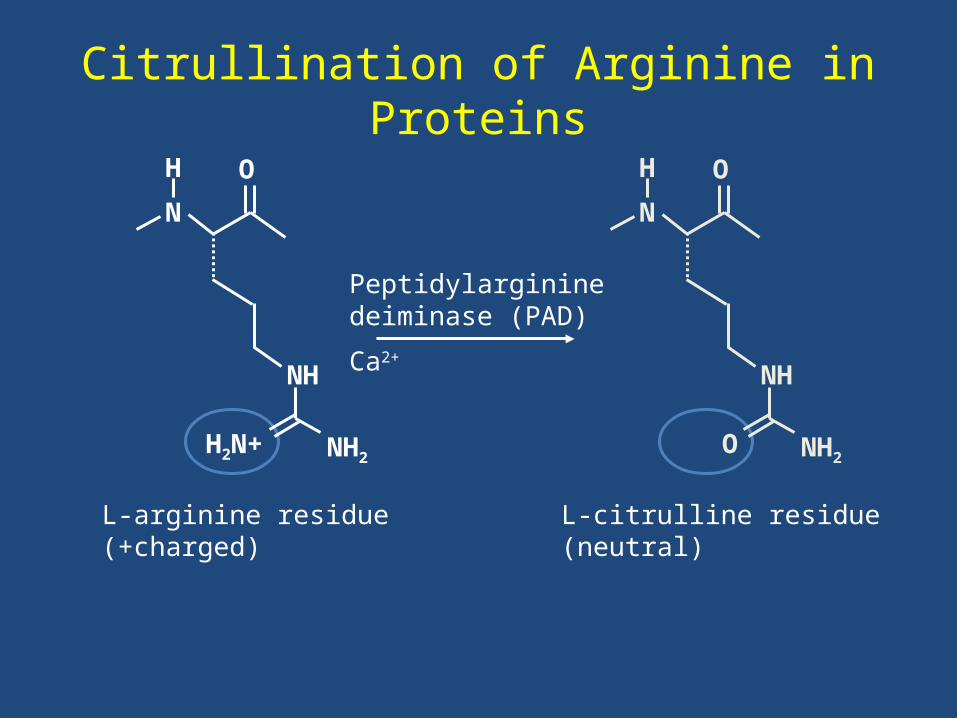
Citrullination of Arginine in Proteins
L-arginine residue(+charged)
L-citrulline residue(neutral)
Peptidylargininedeiminase (PAD)
Ca2+
H
N
O
NH
NH2H2N+
H
N
O
NH
NH2O
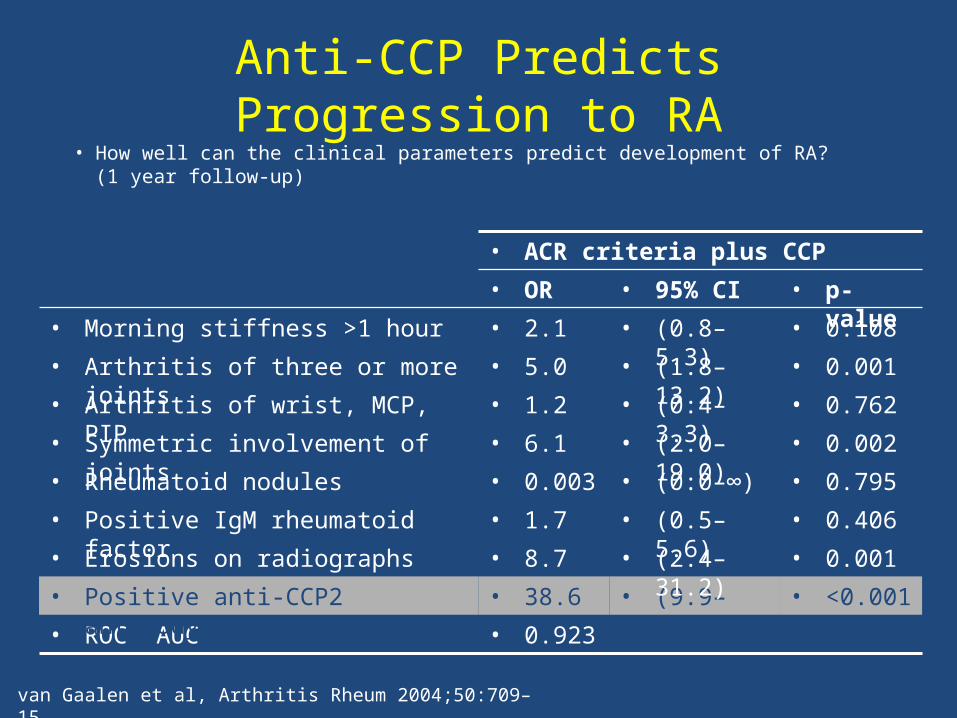
Anti-CCP Predicts Progression to RA• How well can the clinical parameters predict development of RA?
(1 year follow-up)
• ACR criteria plus CCP
• 0.923• ROC AUC
• <0.001• (9.9–151.0)
• 38.6• Positive anti-CCP2 antibody
• 0.001• (2.4–31.2)• 8.7• Erosions on radiographs
• 0.406• (0.5–5.6)• 1.7• Positive IgM rheumatoid factor
• 0.795• (0.0–∞)• 0.003• Rheumatoid nodules
• 0.002• (2.0–19.0)• 6.1• Symmetric involvement of joints
• 0.762• (0.4–3.3)• 1.2• Arthritis of wrist, MCP, PIP
• 0.001• (1.8–13.2)• 5.0• Arthritis of three or more joints
• 0.108• (0.8–5.3)• 2.1• Morning stiffness >1 hour
• p-value• 95% CI• OR
van Gaalen et al, Arthritis Rheum 2004;50:709–15
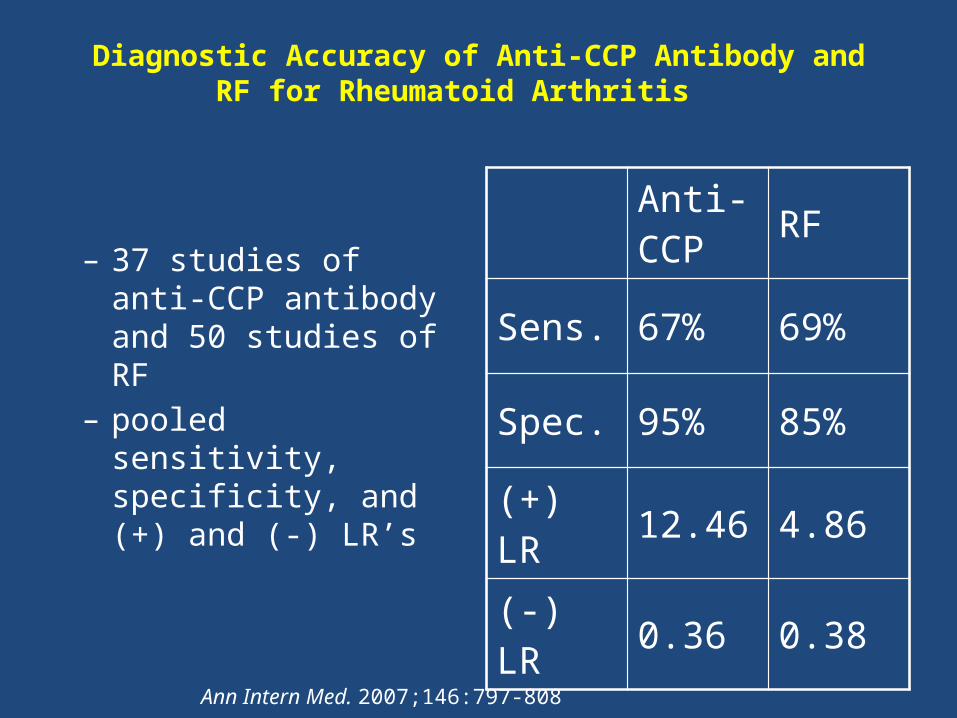
Diagnostic Accuracy of Anti-CCP Antibody and RF for Rheumatoid Arthritis
– 37 studies of anti-CCP antibody and 50 studies of RF
– pooled sensitivity, specificity, and (+) and (-) LR’s
Anti-CCP RF
Sens. 67% 69%
Spec. 95% 85%
(+) LR 12.46 4.86
(-) LR 0.36 0.38
Ann Intern Med. 2007;146:797-808
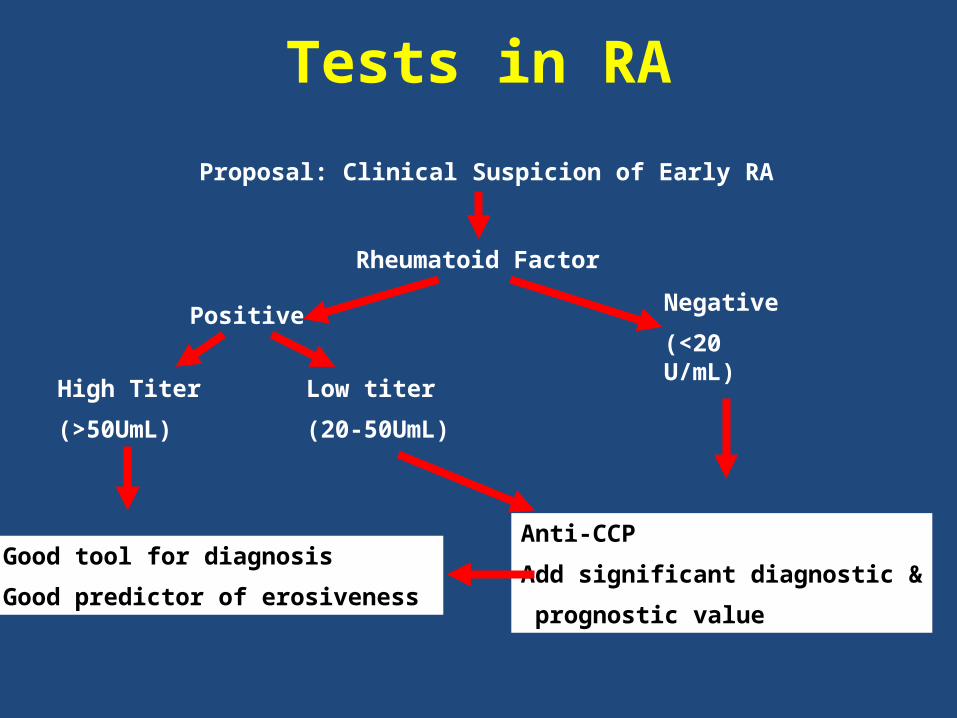
Tests in RA
Proposal: Clinical Suspicion of Early RA
Rheumatoid Factor
Negative
(<20 U/mL)
Positive
Low titer
(20-50UmL)
High Titer
(>50UmL)
Anti-CCP
Add significant diagnostic &
prognostic value
Good tool for diagnosis
Good predictor of erosiveness
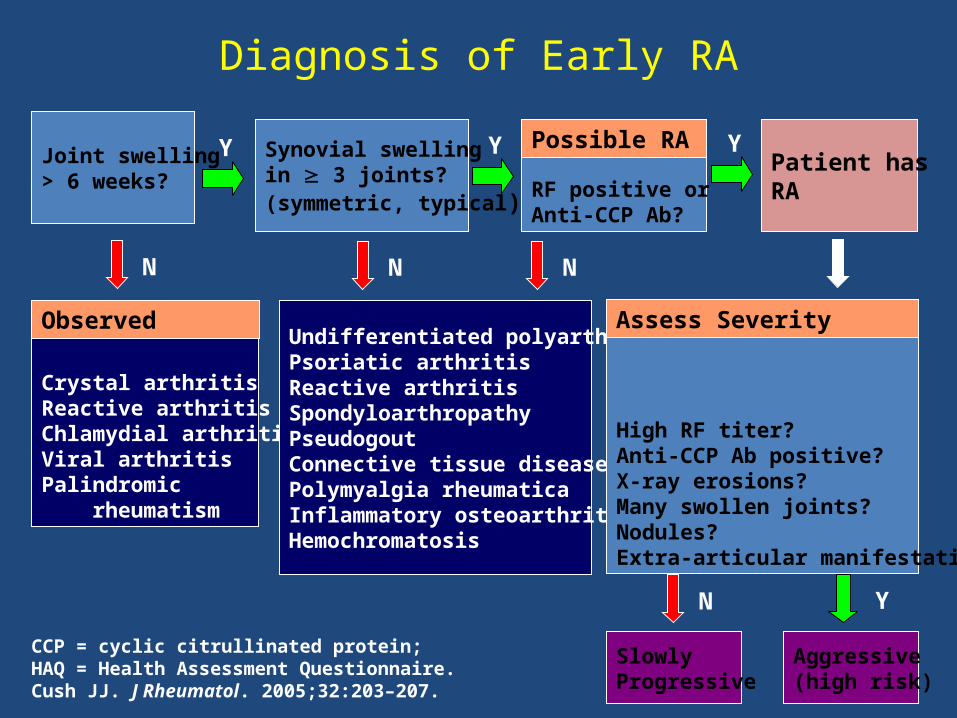
Diagnosis of Early RA
Joint swelling> 6 weeks?
N
Synovial swellingin 3 joints?(symmetric, typical)
Crystal arthritisReactive arthritisChlamydial arthritisViral arthritisPalindromic rheumatism
Y
Observed
Patient hasRA
Y
N
SlowlyProgressive
Aggressive(high risk)
N Y
CCP = cyclic citrullinated protein; HAQ = Health Assessment Questionnaire.Cush JJ. J Rheumatol. 2005;32:203–207.
RF positive orAnti-CCP Ab?
Undifferentiated polyarthritisPsoriatic arthritisReactive arthritisSpondyloarthropathyPseudogoutConnective tissue diseasePolymyalgia rheumaticaInflammatory osteoarthritisHemochromatosis
Y
N
Possible RA
High RF titer?Anti-CCP Ab positive?X-ray erosions?Many swollen joints?Nodules?Extra-articular manifestation?
Assess Severity
RA Therapy
Goals of RA Treatment
• Improvement in Pain, Stiffness, and Constitutional Complaints
• Prevention of Joint Damage/Disability• Normal Quality of Life• Prevention of Co-Morbidities
– Cardiovascular Disease– Osteoporosis– Infections– Malignancies
Treatment Challenges in Early RA
• Defining Who Is At Risk for Progression• Deciding What is the Appropriate Rx for
the Individual
Factors Suggesting Poor Prognosis
• >20 swollen joints• High RF titer• Elevated anti-CCPs• Elevated Sed Rate• Elevated CRP• Late implementation of
treatment
• Joint erosions• Presence of rheumatoid
nodules• Socioeconomic
characteristics• Smoking• Poor functional status
RA Therapeutic Classes• NSAIDS• Corticosteroids• DMARD’s
– Hydroxychloroquine, Sulfasalazine• Immunosuppressive Agents
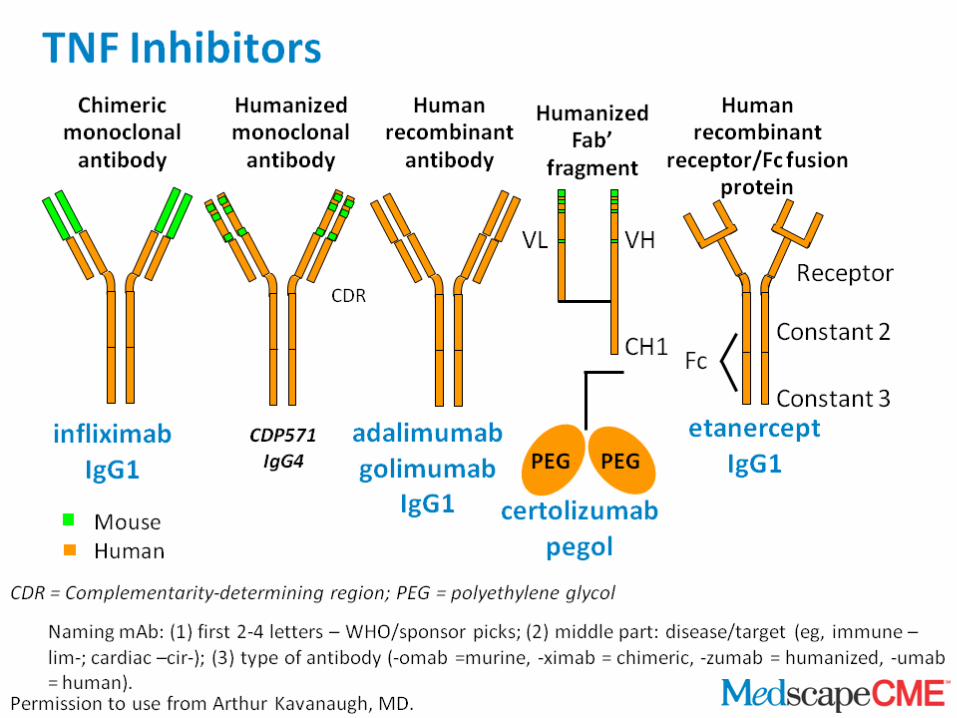
– Methotrexate, Leflunomide, Azathioprine• Biological Agents
– Anti TNF Agents• Etanercept, Infliximab, Adalimumab, Golimumab,
Certolizumab – New Biologics
• Abatacept, Rituximab,Tociluzimab, Tofacinitib
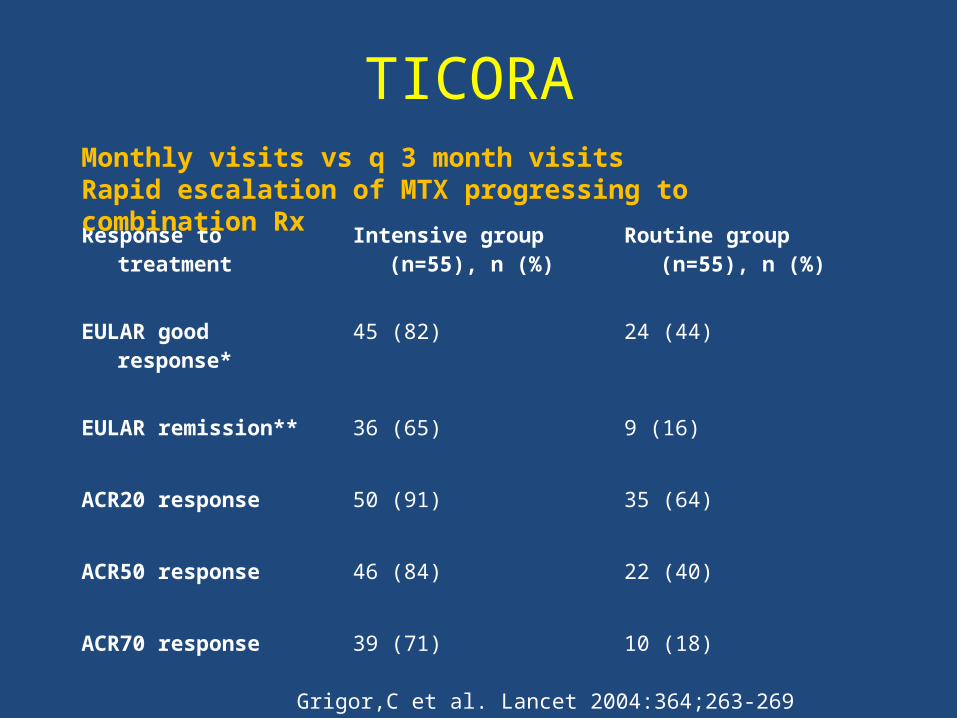
TICORA
Response to treatment
Intensive group (n=55), n (%)
Routine group (n=55), n (%)
EULAR good response*
45 (82) 24 (44)
EULAR remission** 36 (65) 9 (16)
ACR20 response 50 (91) 35 (64)
ACR50 response 46 (84) 22 (40)
ACR70 response 39 (71) 10 (18)
Monthly visits vs q 3 month visitsRapid escalation of MTX progressing to combination Rx
Grigor,C et al. Lancet 2004:364;263-269
Biological Agents
– Anti TNF Agents• Etanercept, Infliximab, Adalimumab, Golimumab,
Certolizumab
– T Cell Co-stimulation inhibitor• Abatacept
– B-cell inhibitor• Rituximab
– IL-6 Inhibitor• Tociluzimab
– Signal molecule inhibitors• Tofacitinib- Jak-3 • Experimental-
– LY3009104- Jak- ½– Fostamatinib- Syk
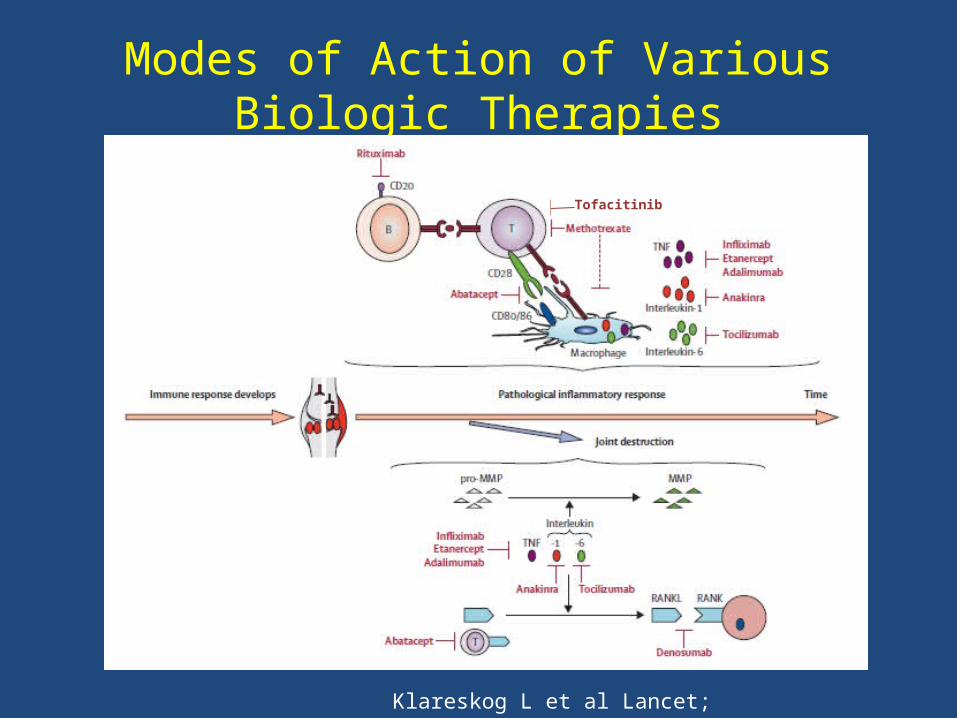
Modes of Action of Various Biologic Therapies
Klareskog L et al Lancet; 2009;373:659-672
Tofacitinib
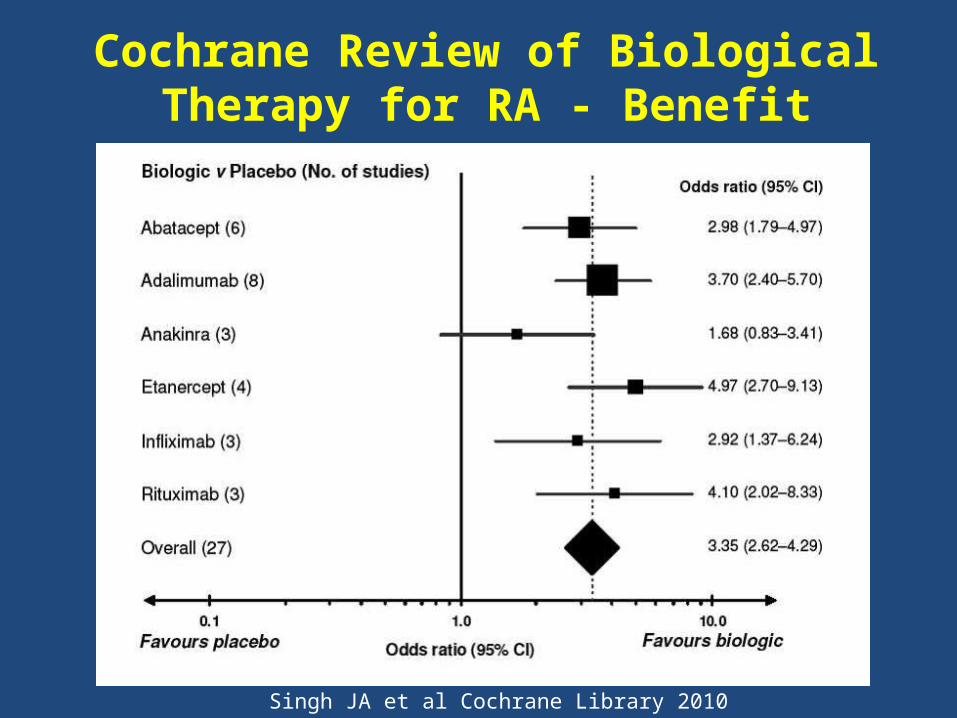
Cochrane Review of Biological Therapy for RA - Benefit
Singh JA et al Cochrane Library 2010
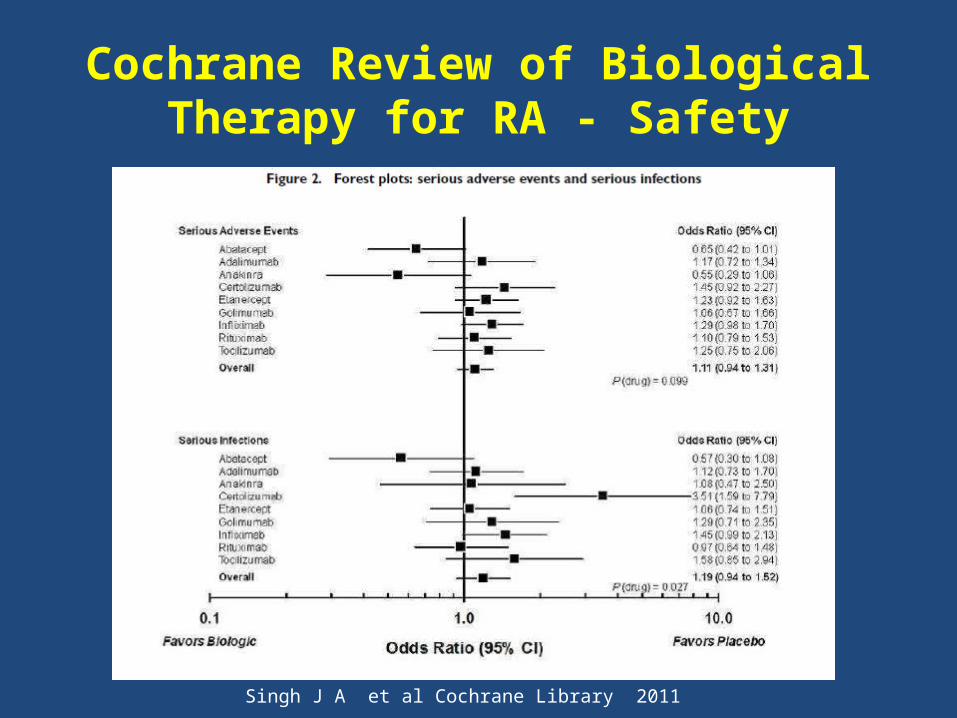
Cochrane Review of Biological Therapy for RA - Safety
Singh J A et al Cochrane Library 2011
2
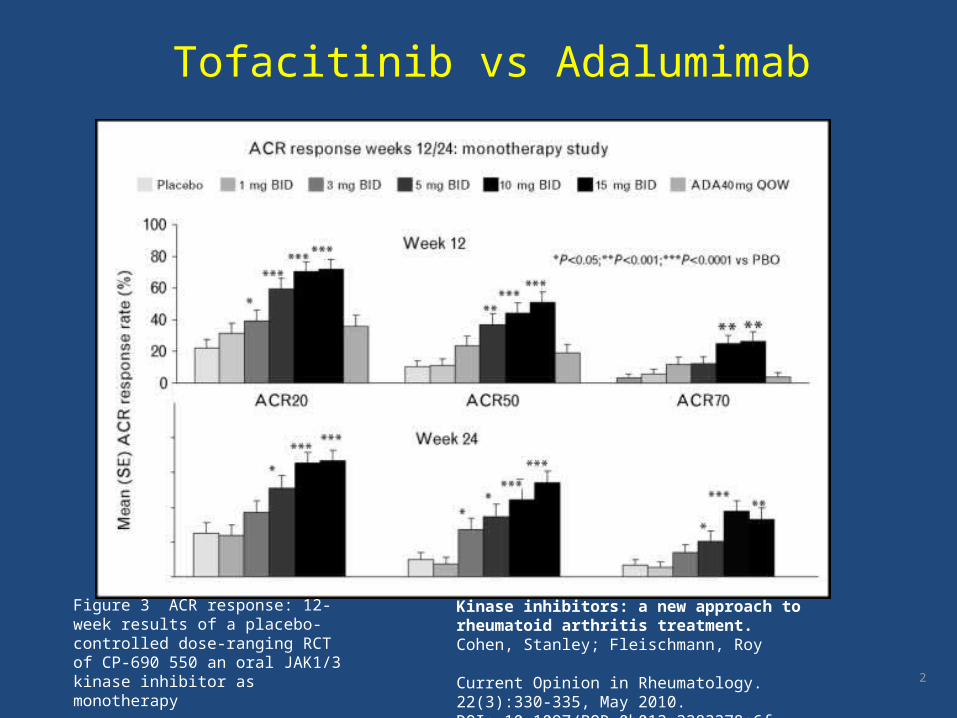
Kinase inhibitors: a new approach to rheumatoid arthritis treatment.Cohen, Stanley; Fleischmann, Roy
Current Opinion in Rheumatology. 22(3):330-335, May 2010.DOI: 10.1097/BOR.0b013e3283378e6f
Figure 3 ACR response: 12-week results of a placebo-controlled dose-ranging RCT of CP-690 550 an oral JAK1/3 kinase inhibitor as monotherapy
Tofacitinib vs Adalumimab
Side Effects of Tofacitinib
• Neuro- headache, light-headedness• GI- abdominal pain, nausea• Liver- abnormal LFT’s• Renal- mild elevation of creatinine• Infections- influenza, URI’s, UTI’s• Hematologic- anemia, leukopenia• Metabolic- hypercholesterolemia
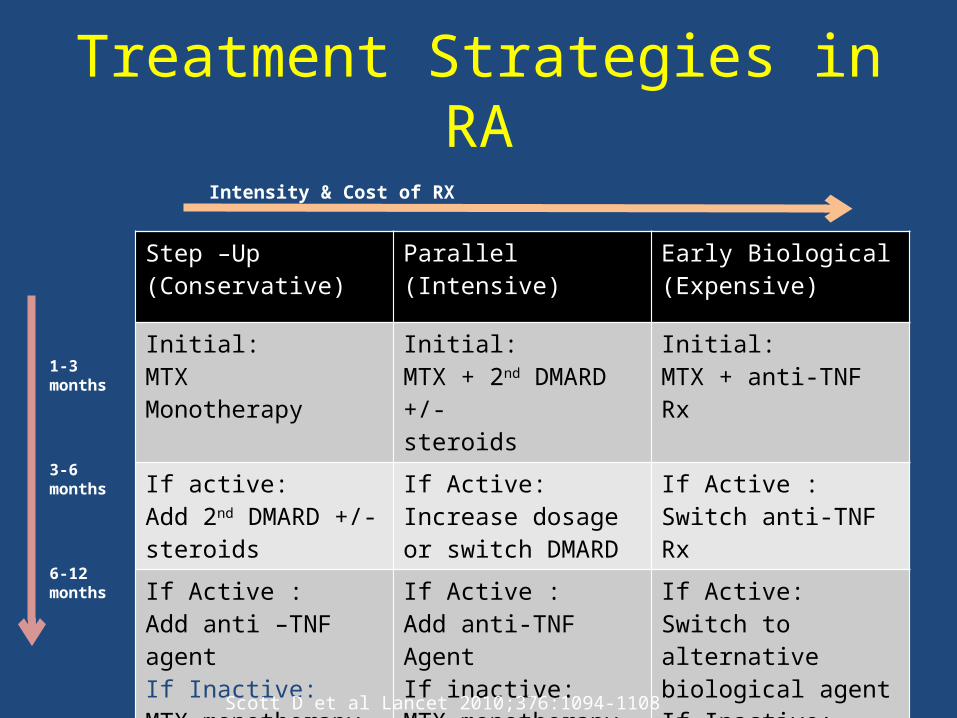
Treatment Strategies in RA
Step –Up (Conservative)
Parallel(Intensive)
Early Biological(Expensive)
Initial:MTXMonotherapy
Initial:MTX + 2nd DMARD +/-steroids
Initial:MTX + anti-TNF Rx
If active:Add 2nd DMARD +/- steroids
If Active:Increase dosage or switch DMARD
If Active :Switch anti-TNF Rx
If Active :Add anti –TNF agentIf Inactive:MTX monotherapy
If Active :Add anti-TNF AgentIf inactive:MTX monotherapy
If Active:Switch to alternative biological agentIf Inactive:MTX monotherapy
Intensity & Cost of RX
1-3 months
3-6 months
6-12months
Scott D et al Lancet 2010;376:1094-1108
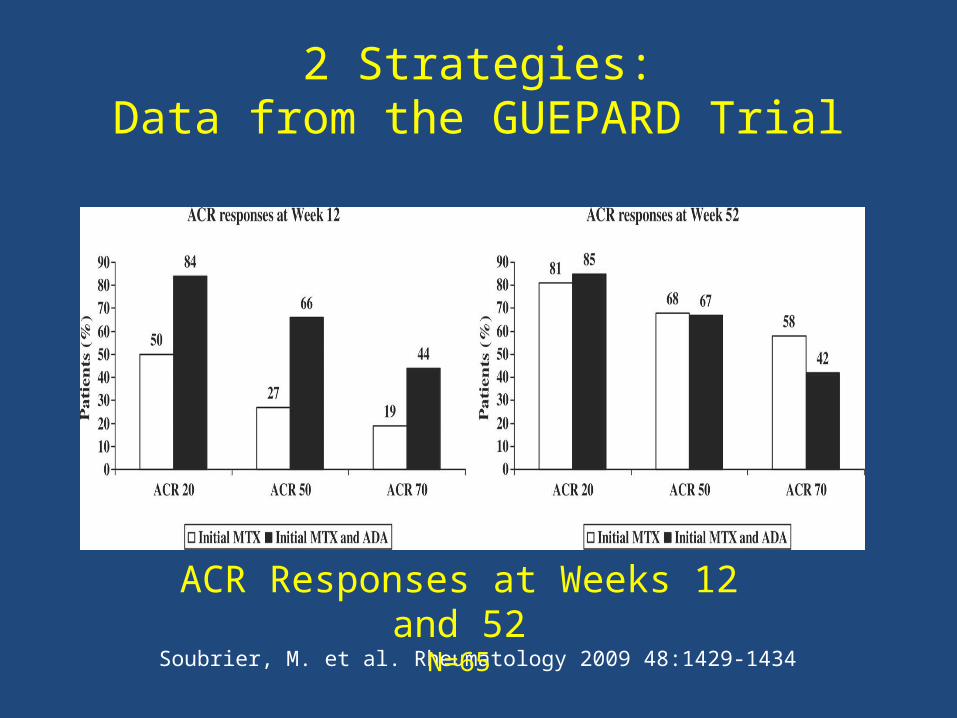
Soubrier, M. et al. Rheumatology 2009 48:1429-1434
ACR Responses at Weeks 12 and 52
N=65
2 Strategies:Data from the GUEPARD Trial
Recommendations from GUEPARD
• Initial therapy with TNF inhibitor is not justified
• If there is persistent disease activity on MTX mono therapy at 12 weeks, TNF inhibitors should be added
• Regardless of the strategy, tight control is effective
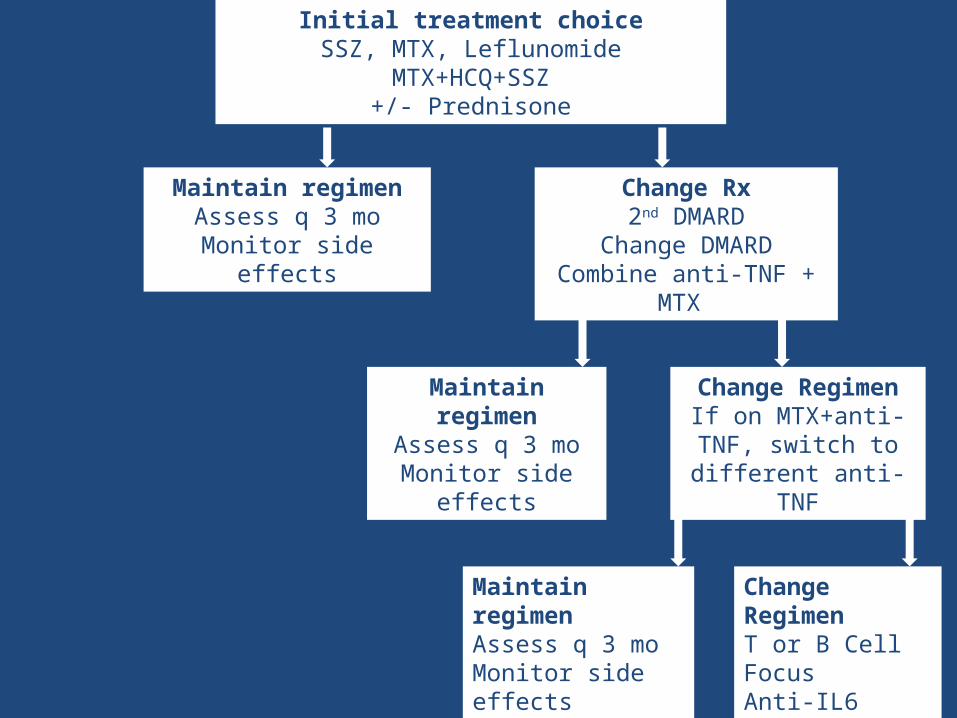
Initial treatment choiceSSZ, MTX, Leflunomide
MTX+HCQ+SSZ+/- Prednisone
Maintain regimenAssess q 3 mo
Monitor side effects
Change Rx2nd DMARD
Change DMARDCombine anti-TNF + MTX
Maintain regimenAssess q 3 mo
Monitor side effects
Change RegimenIf on MTX+anti-TNF,
switch to different anti-TNF
Maintain regimenAssess q 3 moMonitor side effects
Change RegimenT or B Cell FocusAnti-IL6
Rheumatoid Arthritis Treatment Strategies
• Things we agree on:– Early diagnosis is good– Early institution of DMARD therapy is good– Tight control improves outcomes– “Treat-to- Target”
• Unanswered questions:– Optimal treatment strategy in early disease
• ? Monotherapy with step up• ? Initial combination therapy• ? Early institution of biologics • How much steroid initially
CBC, complete blood count; DMARD, disease-modifying antirheumatic drug; LFT, liver function test; TB, tuberculosis. Saag KG, et al. Arthritis Rheum. 2008;59:762-784.
Before Starting Therapy• Obtain CBC, LFTs, creatinine level, HIV
and hepatitis B and C status– Repeat at regular intervals depending on
the therapy
• Vaccinations• TB screening for biologic DMARDs
CRP, C-reactive protein; CV, cardiovascular; DXA, dual-emission X-ray absorptiometry; ESR, erythrocyte sedimentation rate; FRAX, fracture risk estimation; PLT, platelet. Saag KG, et al. Arthritis Rheum. 2008;59:762-784.
• Assess disease activity regularly– Labs: ESR, CRP, PLT, CMR etc. every 1-3 months
– Joint examination: 28-joint count
– MHAQ, RAPID-3, DAS28
– Disease flares
• Monitor treatment-specific side effects
• Monitor comorbidities– CV: lipid profile, tobacco use, etc
– Osteoporosis: DXA, calcium, vitamin D, exercise, FRAX
– Mental health
Ongoing Monitoring
Conventional DMARD Safety Concerns
• Reproductive• MTX, Leflunomide
• Pulmonary• MTX, Leflunomide
• Allergic• SSZ, HCQ
• Cutaneous• Leflunomide
• Lymphoma• MTX, Leflunomide, Azathioprine
• Hematologic • All
• Host Defense• MTX, Leflunomide, Azathioprine
• Hepatic • MTX, Leflunomide, Azathioprine
• Gastro-intestinal• All
• Ocular • HCQ
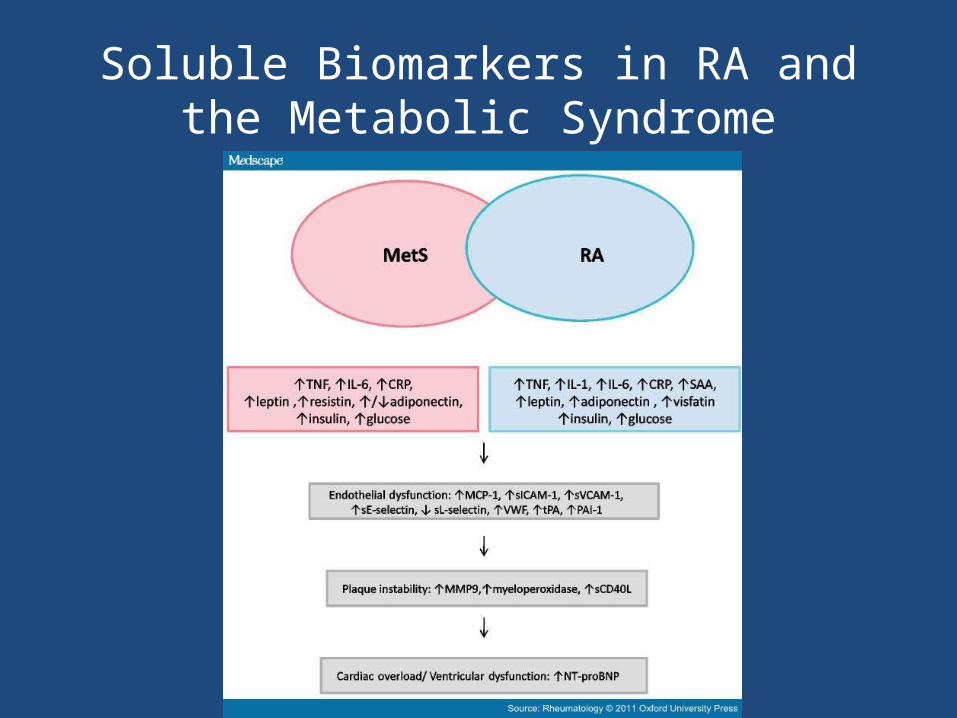
Soluble Biomarkers in RA and the Metabolic Syndrome
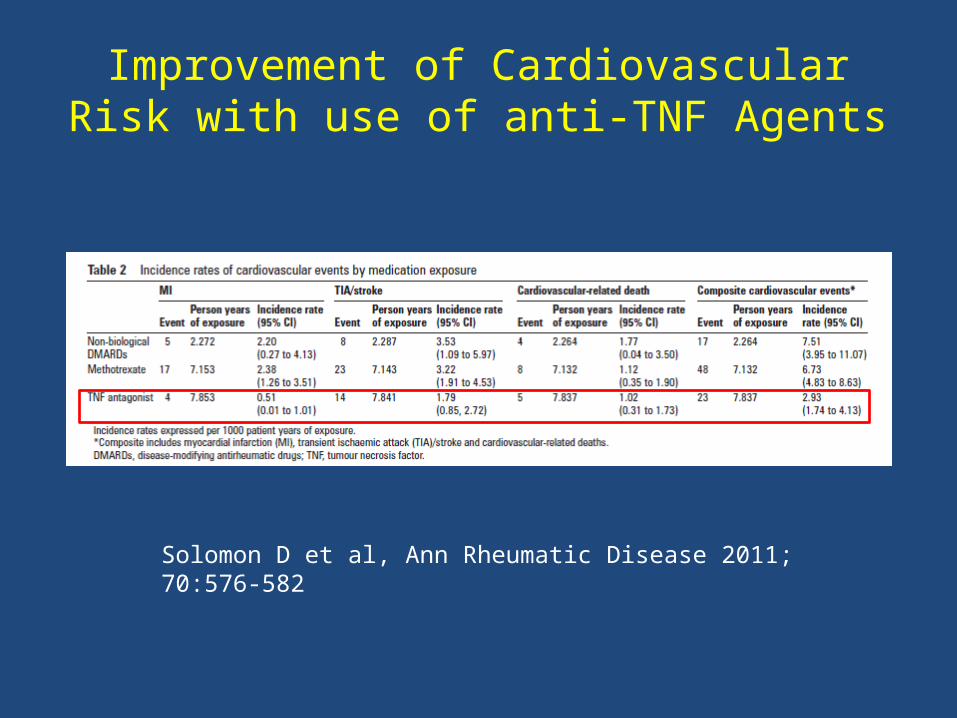
Improvement of Cardiovascular Risk with use of anti-TNF Agents
Solomon D et al, Ann Rheumatic Disease 2011; 70:576-582
Additional Interventions• Exercise recommended for all RA patients to:
– Keep joints loose, support affected joints– Maintain/improve balance and strength– Ward off depression/improve mood
• Smoking cessation• Stress management• Foot health• Vaccination
– Yearly influenza vaccine– Pneumococcal vaccine when indicated
• Risk factor assessment for cardiovascular disease– Lifestyle modification – Glucose and lipid monitoring
Saag KG, et al. Arthritis Rheum. 2008;59:762-784.
Thank you!

Potential Contraindications to DMARD Treatment
• Infectious disease: bacterial infection, TB, shingles, serious fungal infection, or pneumonitis (ILD)
• Hematologic and oncologic • Cardiac: class III-IV heart failure• Liver: abnormal LFTs, hepatitis B or C• Renal • Neurologic: MS• Pregnancy and breastfeeding • Perioperative infectious risk
DMARDs, disease-modifying antirheumatic drugs; ILD, interstitial lung disease; LFT, liver function test; MS, multiple sclerosis; TB, tuberculosis.Saag KG, et al. Arthritis Rheum. 2008;59:762-784.
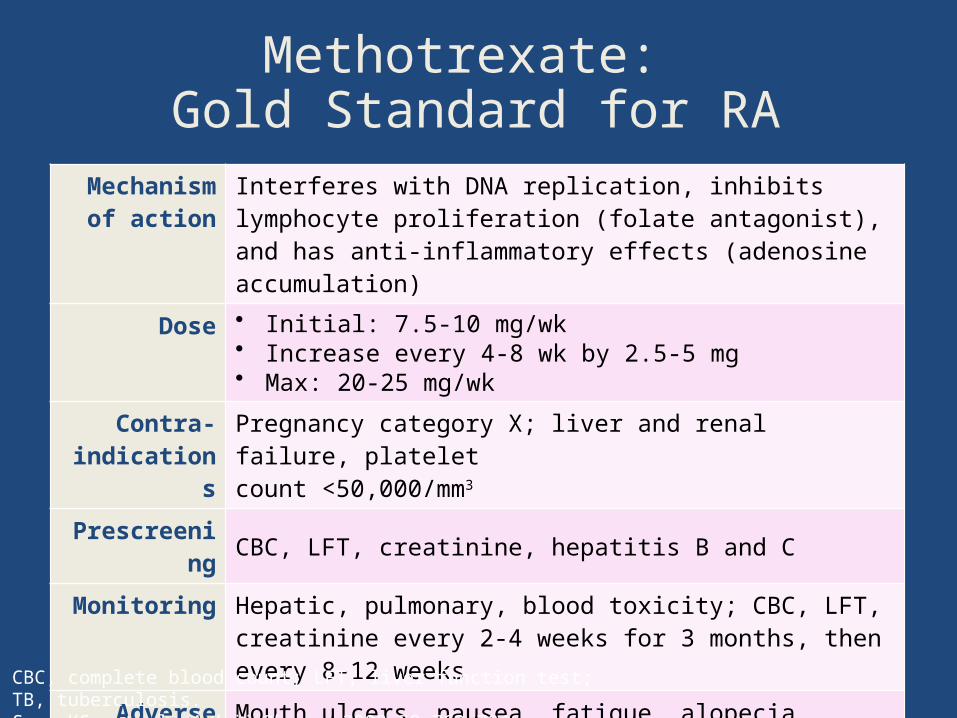
Methotrexate: Gold Standard for RA
Mechanism of action
Interferes with DNA replication, inhibits lymphocyte proliferation (folate antagonist), and has anti-inflammatory effects (adenosine accumulation)
Dose • Initial: 7.5-10 mg/wk• Increase every 4-8 wk by 2.5-5 mg• Max: 20-25 mg/wk
Contra-indications
Pregnancy category X; liver and renal failure, platelet count <50,000/mm3
Prescreening CBC, LFT, creatinine, hepatitis B and C
Monitoring Hepatic, pulmonary, blood toxicity; CBC, LFT, creatinine every 2-4 weeks for 3 months, then every 8-12 weeks
Adverse reactions
Mouth ulcers, nausea, fatigue, alopecia, diarrhea, achiness, irritability
Other Consider folic acid supplementation; no alcohol; >180 mg/day caffeine reduces efficacy; high alert for incorrect dosing
CBC, complete blood count; LFT, liver function test; TB, tuberculosis.Saag KG, et al. Arthritis Rheum. 2008;59:762-784.
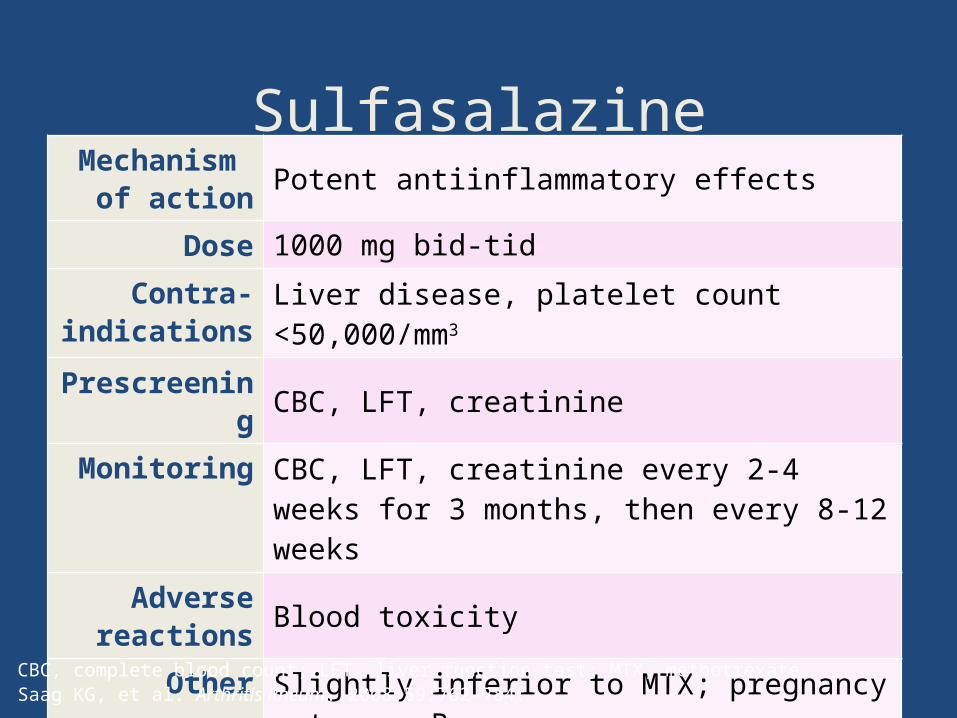
SulfasalazineMechanism
of action Potent antiinflammatory effects
Dose 1000 mg bid-tid
Contra-indications Liver disease, platelet count <50,000/mm3
PrescreeningCBC, LFT, creatinine
Monitoring CBC, LFT, creatinine every 2-4 weeks for 3 months, then every 8-12 weeks
Adverse reactions Blood toxicity
Other Slightly inferior to MTX; pregnancy category B
CBC, complete blood count; LFT, liver function test; MTX, methotrexate.Saag KG, et al. Arthritis Rheum. 2008;59:762-784.
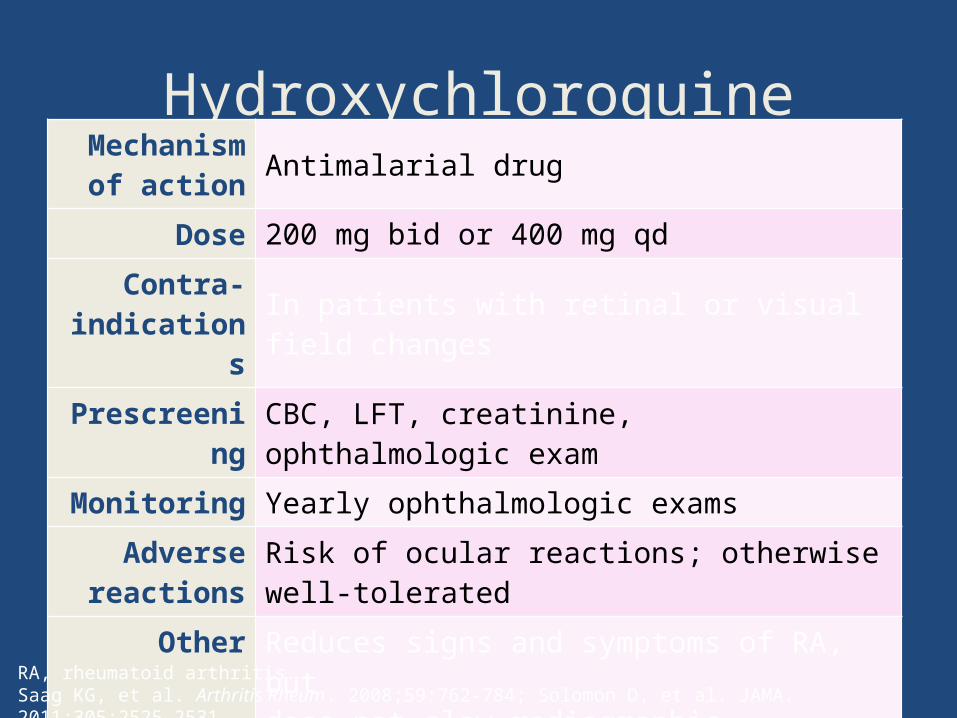
HydroxychloroquineMechanism
of action Antimalarial drug
Dose 200 mg bid or 400 mg qd
Contra-indications In patients with retinal or visual field changes
Prescreening CBC, LFT, creatinine, ophthalmologic exam
Monitoring Yearly ophthalmologic exams
Adverse reactions
Risk of ocular reactions; otherwise well-tolerated
Other Reduces signs and symptoms of RA, but does not slow radiographic progression as monotherapy; reduces the risk of new-onset diabetes
RA, rheumatoid arthritis.Saag KG, et al. Arthritis Rheum. 2008;59:762-784; Solomon D, et al. JAMA. 2011;305:2525-2531.
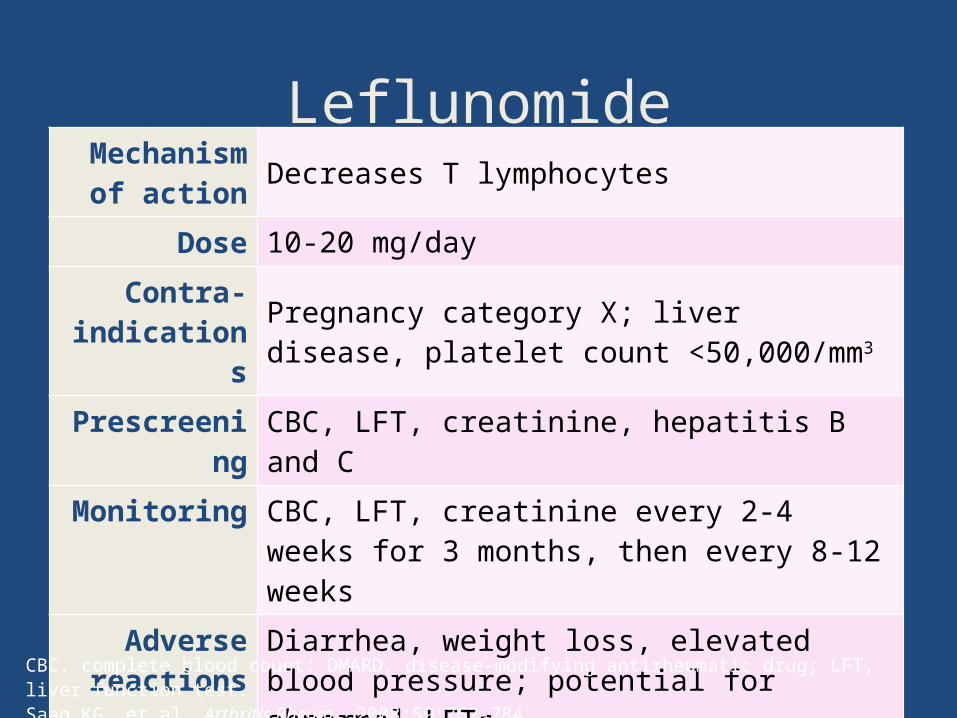
LeflunomideMechanism
of action Decreases T lymphocytes
Dose 10-20 mg/day
Contra-indications
Pregnancy category X; liver disease, platelet count <50,000/mm3
Prescreening CBC, LFT, creatinine, hepatitis B and C
Monitoring CBC, LFT, creatinine every 2-4 weeks for 3 months, then every 8-12 weeks
Adverse reactions
Diarrhea, weight loss, elevated blood pressure; potential for abnormal LFTs
Other Newer nonbiologic DMARD
CBC, complete blood count; DMARD, disease-modifying antirheumatic drug; LFT, liver function test.Saag KG, et al. Arthritis Rheum. 2008;59:762-784.
Biologic DMARDs: Overview• Considerations for injectable agents:
– Rotate injection sites– Some needle covers made from latex; caution in latex allergy
• Adverse reactions– Injection-site or infusion reactions– Infections: TB, hepatitis, fungal, and bacterial (sepsis)– Rare: lupus and MS
• Contraindications – Active or recurrent cancer – Untreated infection, active or latent TB– Cannot receive live virus vaccinations– Severe heart failure (class III-IV)
MS, multiple sclerosis; TB, tuberculosis.Saag KG, et al. Arthritis Rheum. 2008;59:762-784.
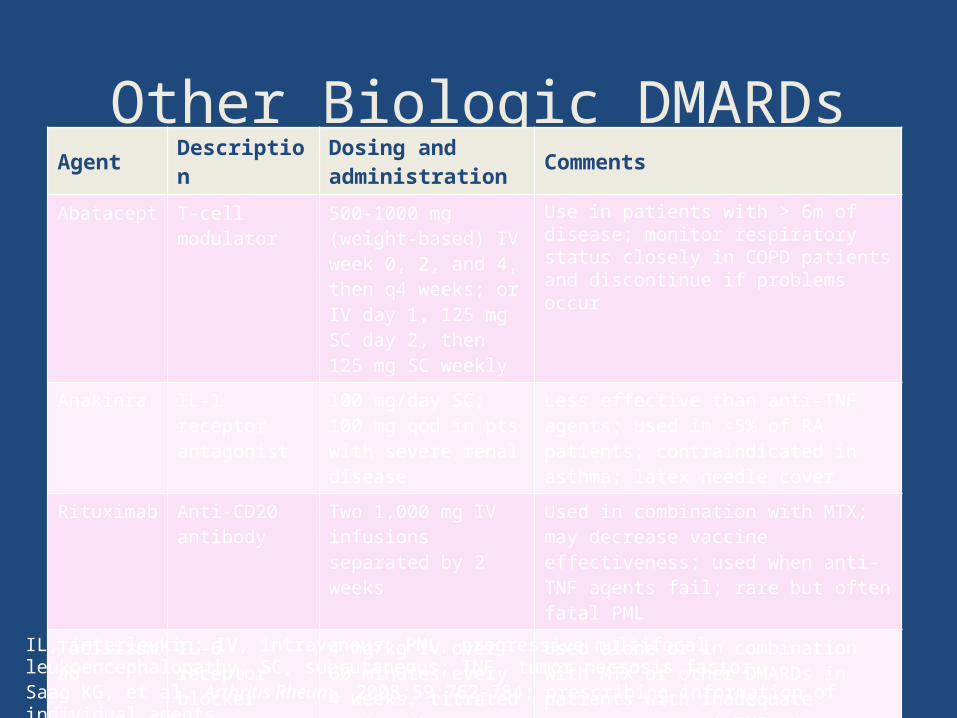
Other Biologic DMARDsAgent Description Dosing and
administration Comments
Abatacept T-cell modulator
500-1000 mg (weight-based) IV week 0, 2, and 4, then q4 weeks; or IV day 1, 125 mg SC day 2, then 125 mg SC weekly
Use in patients with > 6m of disease; monitor respiratory status closely in COPD patients and discontinue if problems occur
Anakinra IL-1 receptor antagonist
100 mg/day SC; 100 mg qod in pts with severe renal disease
Less effective than anti-TNF agents; used in <5% of RA patients; contraindicated in asthma; latex needle cover
Rituximab Anti-CD20 antibody
Two 1,000 mg IV infusions separated by 2 weeks
Used in combination with MTX; may decrease vaccine effectiveness; used when anti-TNF agents fail; rare but often fatal PML
Tocilizumab IL-6 receptor blocker
4 mg/kg IV over 60 minutes every 4 weeks, titrated to 8 mg/kg as needed
Used alone or in combination with MTX or other DMARDs in patients with inadequate response to anti-TNF therapy
IL, interleukin; IV, intravenous; PML, progressive multifocal leukoencephalopathy; SC, subcutaneous; TNF, tumor necrosis factor. Saag KG, et al. Arthritis Rheum. 2008;59:762-784; prescribing information of individual agents.
Other Agents: NSAIDs• Help with inflammation & pain• No disease-modifying capability• Contraindicated in patients with renal
disease• Caution in patients with heart disease
& peptic ulcer disease• Increased incidence of heart attack,
stroke, GI disease, renal disease
GI, gastrointestinal; NSAID, nonsteroidal antiinflammatory drug.Saag KG, et al. Arthritis Rheum. 2008;59:762-784; Trelle S, et al. BMJ. 2011;342:c7086.
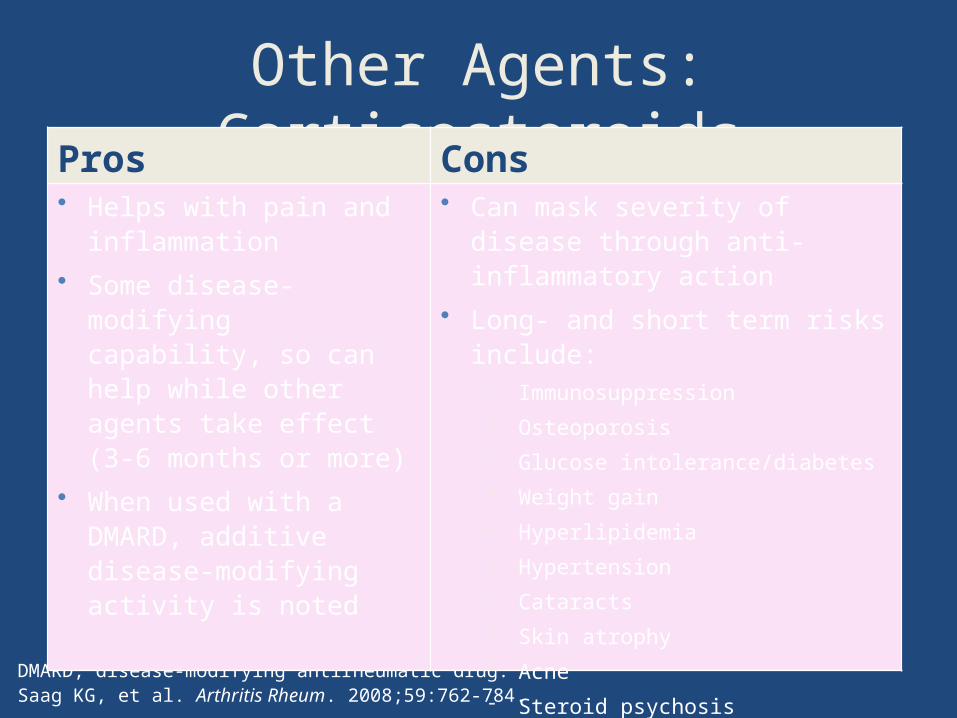
Other Agents: Corticosteroids
DMARD, disease-modifying antirheumatic drug.Saag KG, et al. Arthritis Rheum. 2008;59:762-784.
Pros Cons• Helps with pain and
inflammation• Some disease-modifying
capability, so can help while other agents take effect (3-6 months or more)
• When used with a DMARD, additive disease-modifying activity is noted
• Can mask severity of disease through anti-inflammatory action
• Long- and short term risks include: Immunosuppression Osteoporosis Glucose intolerance/diabetes Weight gain Hyperlipidemia Hypertension Cataracts Skin atrophy Acne Steroid psychosis
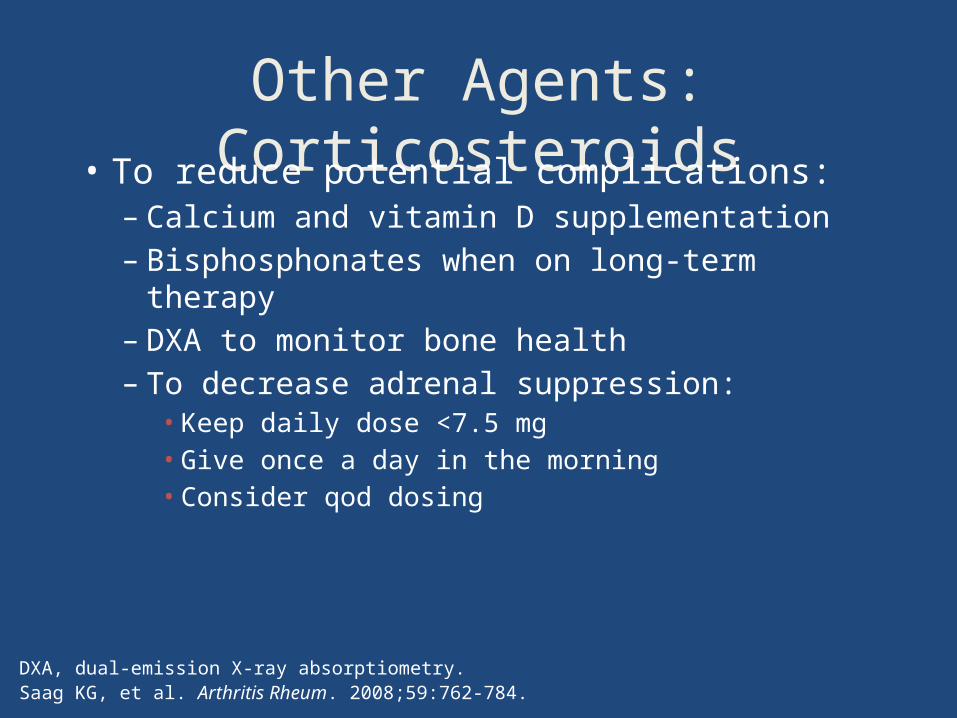
Other Agents: Corticosteroids• To reduce potential complications:
– Calcium and vitamin D supplementation– Bisphosphonates when on long-term
therapy– DXA to monitor bone health– To decrease adrenal suppression:
• Keep daily dose <7.5 mg• Give once a day in the morning• Consider qod dosing
DXA, dual-emission X-ray absorptiometry.Saag KG, et al. Arthritis Rheum. 2008;59:762-784.
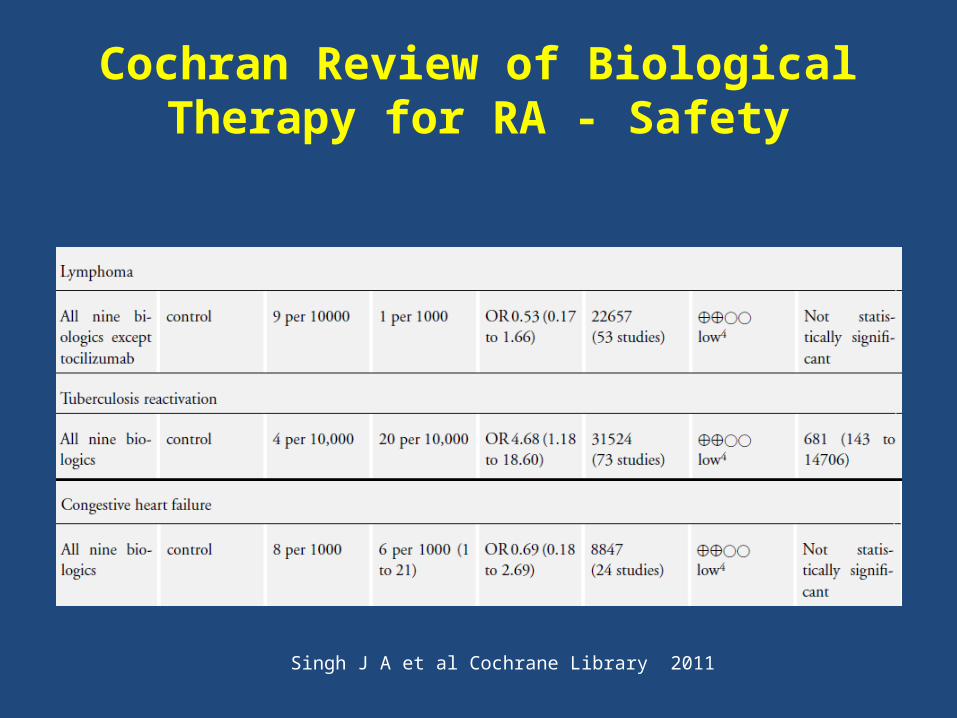
Cochran Review of Biological Therapy for RA - Safety
Singh J A et al Cochrane Library 2011
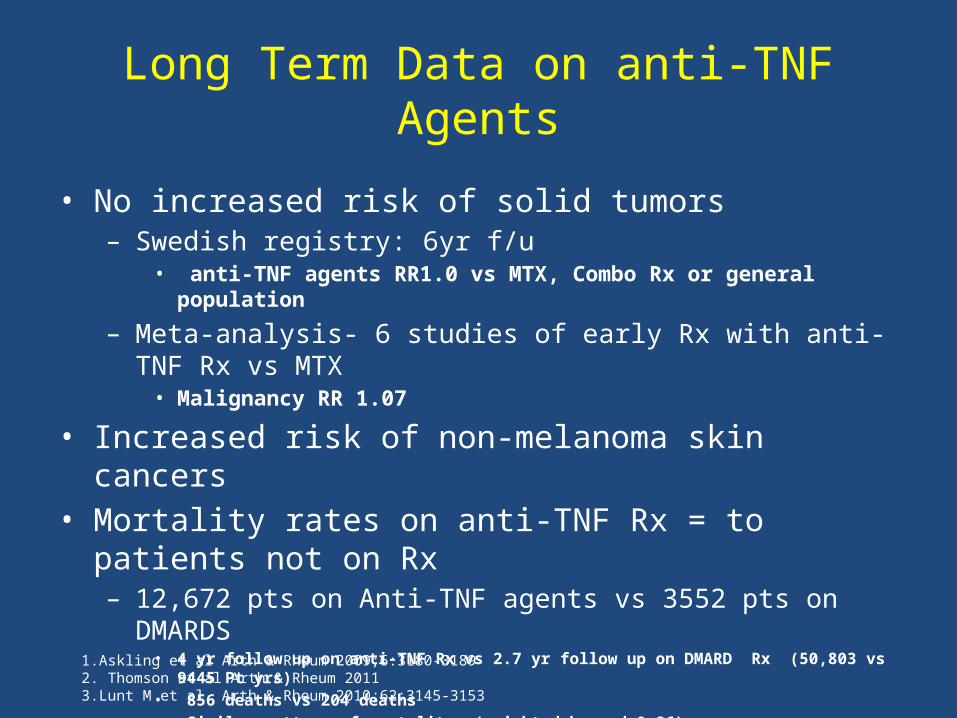
Long Term Data on anti-TNF Agents
• No increased risk of solid tumors– Swedish registry: 6yr f/u
• anti-TNF agents RR1.0 vs MTX, Combo Rx or general population
– Meta-analysis- 6 studies of early Rx with anti-TNF Rx vs MTX• Malignancy RR 1.07
• Increased risk of non-melanoma skin cancers• Mortality rates on anti-TNF Rx = to patients not on Rx
– 12,672 pts on Anti-TNF agents vs 3552 pts on DMARDS• 4 yr follow up on anti-TNF Rx vs 2.7 yr follow up on DMARD Rx (50,803 vs 9445 Pt yrs) • 856 deaths vs 204 deaths • Similar pattern of mortality- (weighted hazard 0.86)• Deaths: circulatory, neoplasm, respiratory
1.Askling et al Arth & Rheum 2009;6:3180-31892. Thomson et al Arth & Rheum 20113.Lunt M et al, Arth & Rheum 2010;62:3145-3153
Who to Treat? Who to Refer?• Patients with features of an early
inflammatory arthritis:
- joint swelling
- symmetric distribution of symptoms
- MCP and MTP involvement
- significant early morning stiffness (>1 hr)
- a good anti-inflammatory response
- family history
Principles of RA Therapy
• More aggressive therapy
• Early institution of DMARD therapy
• Maximization of MTX dosing
• Combination therapy
• Addition of biologic agents for persistent
activity





























