Embed Size (px)
Citation preview
RHABDOMYOSARCOMA
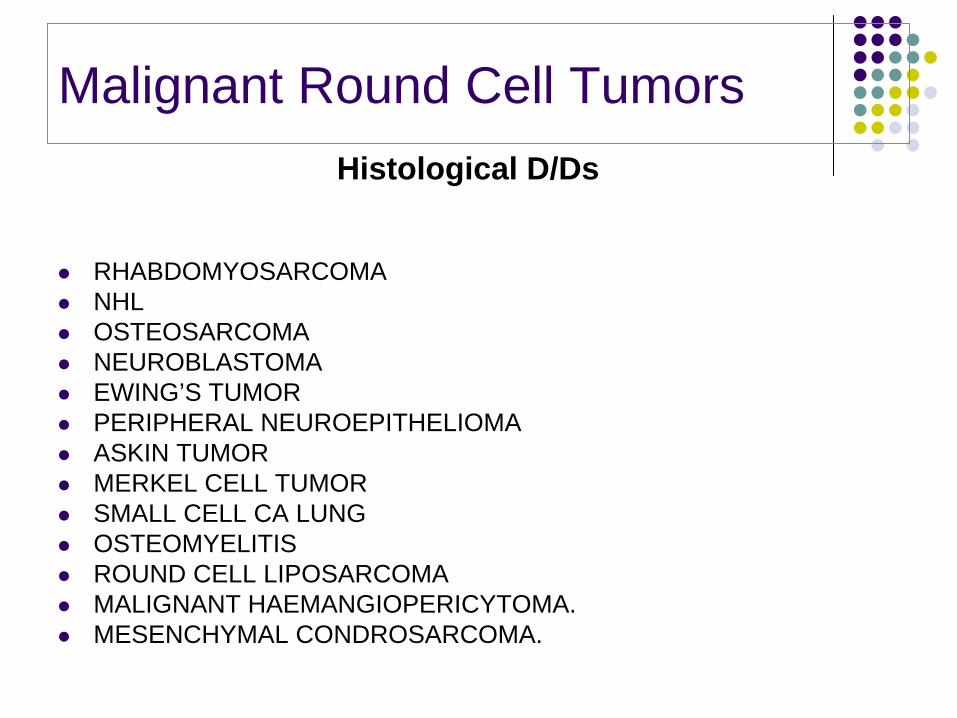
Malignant Round Cell Tumors
RHABDOMYOSARCOMANHLOSTEOSARCOMANEUROBLASTOMAEWING’S TUMORPERIPHERAL NEUROEPITHELIOMAASKIN TUMORMERKEL CELL TUMORSMALL CELL CA LUNGOSTEOMYELITISROUND CELL LIPOSARCOMAMALIGNANT HAEMANGIOPERICYTOMA.MESENCHYMAL CONDROSARCOMA.
Histological D/Ds
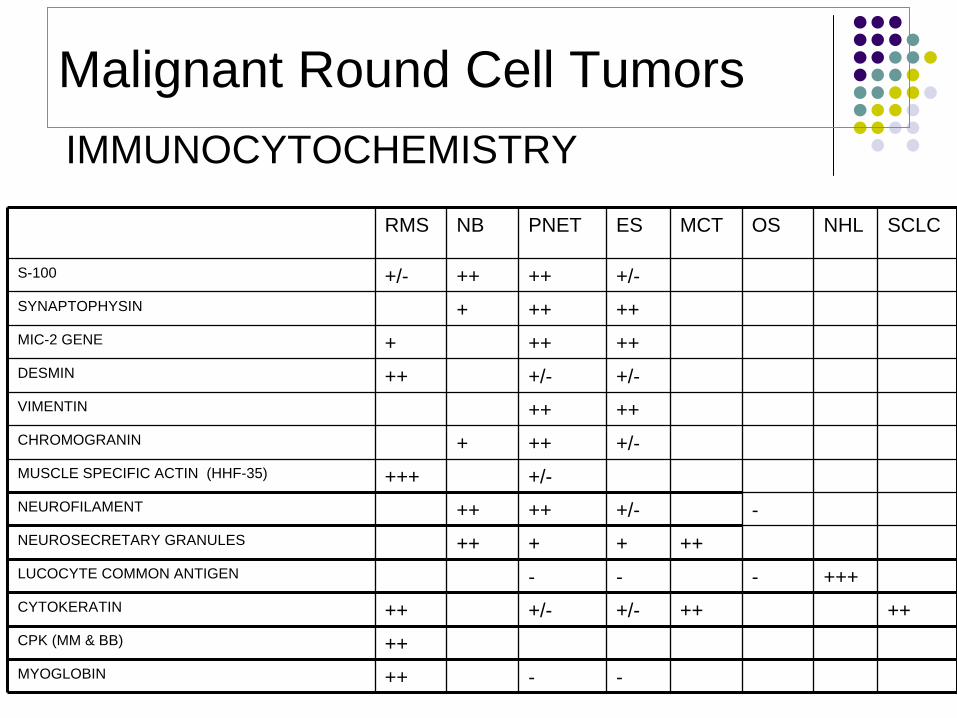
Malignant Round Cell TumorsIMMUNOCYTOCHEMISTRY
RMS NB PNET ES MCT OS NHL SCLC
S-100 +/- ++ ++ +/-SYNAPTOPHYSIN + ++ ++MIC-2 GENE + ++ ++DESMIN ++ +/- +/-VIMENTIN ++ ++CHROMOGRANIN + ++ +/-MUSCLE SPECIFIC ACTIN (HHF-35) +++ +/-NEUROFILAMENT ++ ++ +/- -NEUROSECRETARY GRANULES ++ + + ++LUCOCYTE COMMON ANTIGEN - - - +++CYTOKERATIN ++ +/- +/- ++ ++CPK (MM & BB) ++MYOGLOBIN ++ - -
RHABDOMYOSARCOMA
Highly malignant STS that arises from unsegmented, undifferentiated mesoderm or myotome derived skeletal muscle.Different pathobiologic entities linked by common propensity to develop neoplastic skeletal musclesHeterogeneous group, clinicopathologic entities based on morphologic appearance and genetic make up.Mid 1900, Horn and enterline divided into Embryonal, Alveolar, Botryoid, Pleomorphic subtimesMore recently- spindle cell, anaplastic, and refinements such as Undifferentiated and Solid Alveolar.
Highly malignant STS that arises from unsegmented, undifferentiated mesoderm or myotome derived skeletal muscle.Different pathobiologic entities linked by common propensity to develop neoplastic skeletal musclesHeterogeneous group, clinicopathologic entities based on morphologic appearance and genetic make up.Mid 1900, Horn and enterline divided into Embryonal, Alveolar, Botryoid, Pleomorphic subtimesMore recently- spindle cell, anaplastic, and refinements such as Undifferentiated and Solid Alveolar.
Histology of these neoplasms is analogous with myogenesis in the developing embryo
more correct to define RMS as a tumor derived from primitive mesenchyme and exhibiting a profound tendency towards myogenesis
RHABDOMYOSARCOMA
EPIDEMIOLOGY
Most common pediatric STS (approximately 50%)3.5% of all malignancies under age of 15; 2% of all malignancies in 15-19 age group90 % of all RMS in individuals < 25 years; 60-70% in <10 years, 5% are infants.Peak age 2- 5 years & adolescenceMale preponderance (1.5:1)Racial predisposition (White children 4 times as likely as black children)
1/3 of RMS patients have other congenital abnormalitiesGI, GU, CV, CNS
Majority of cases are sporadic; but some are associated with genetic conditions
Li Fraumeni (p53 mutation)NF 1Beckwith – Wiedemann
Though it may occur at any site, most frequently involved are….
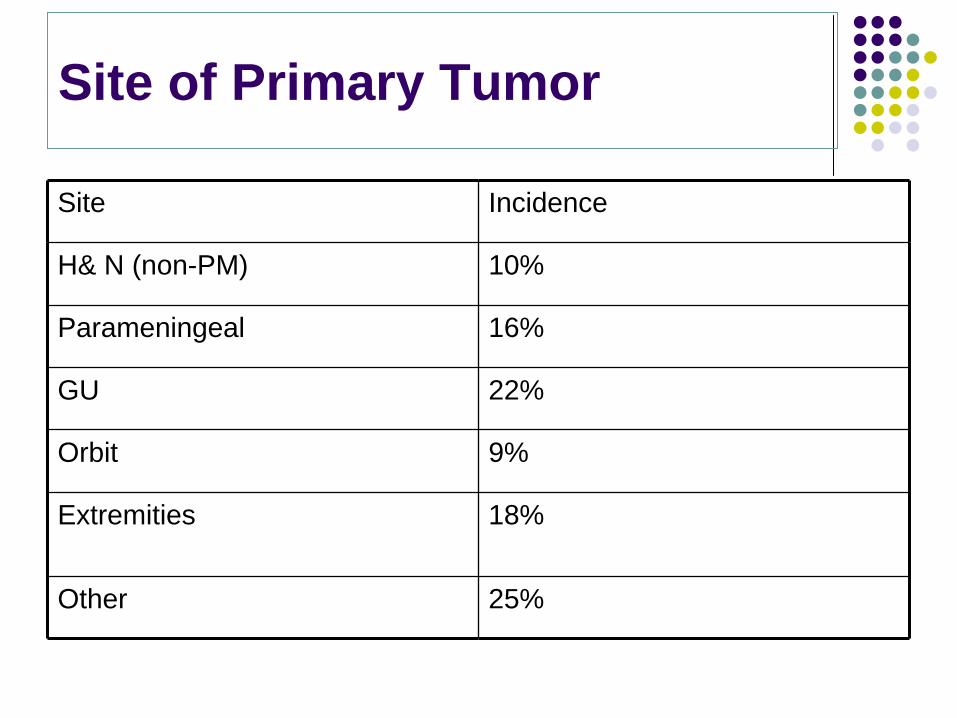
Site of Primary Tumor
Site Incidence
H& N (non-PM) 10%
Parameningeal 16%
GU 22%
Orbit 9%
Extremities 18%
Other 25%
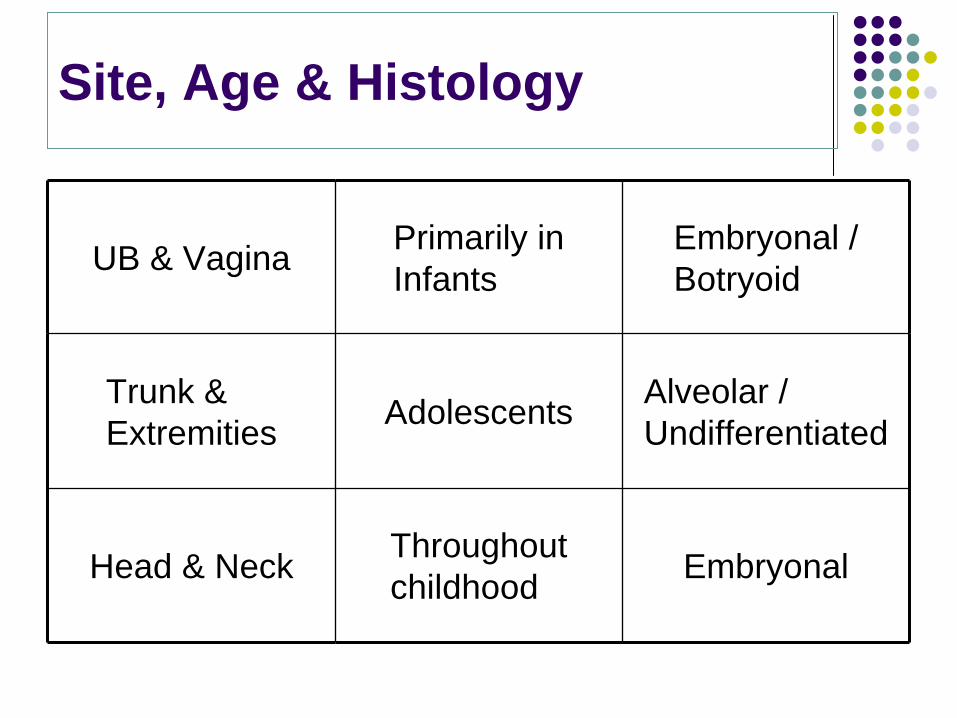
Site, Age & Histology
UB & Vagina Primarily in Infants
Embryonal / Botryoid
Trunk & Extremities Adolescents Alveolar /
Undifferentiated
Head & Neck Throughout childhood Embryonal
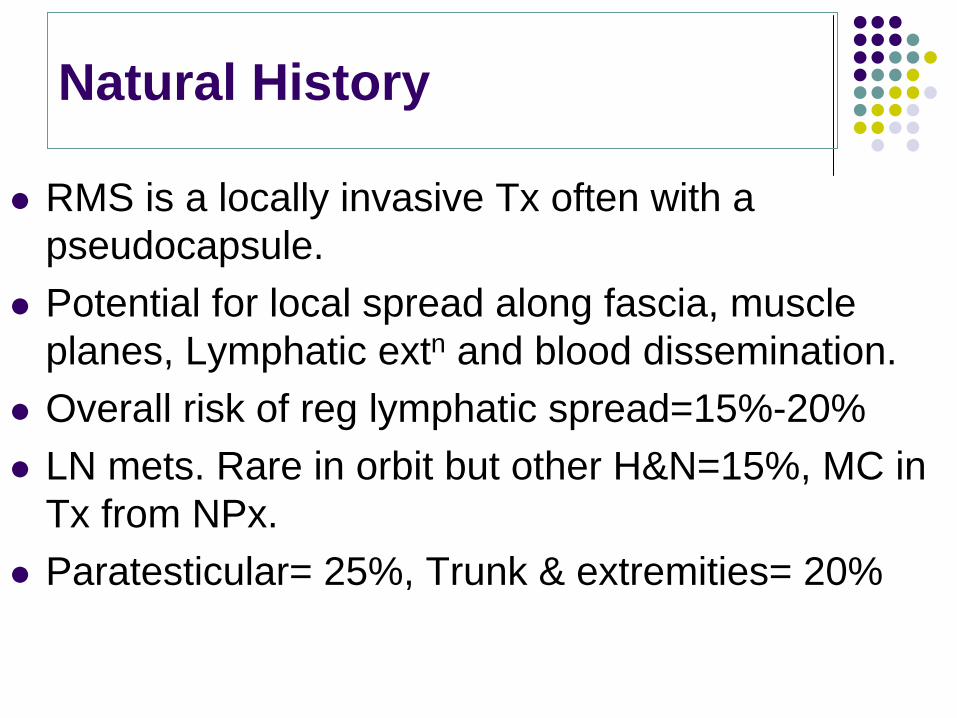
Natural History
RMS is a locally invasive Tx often with a pseudocapsule.Potential for local spread along fascia, muscle planes, Lymphatic extn and blood dissemination.Overall risk of reg lymphatic spread=15%-20%LN mets. Rare in orbit but other H&N=15%, MC in Tx from NPx.Paratesticular= 25%, Trunk & extremities= 20%
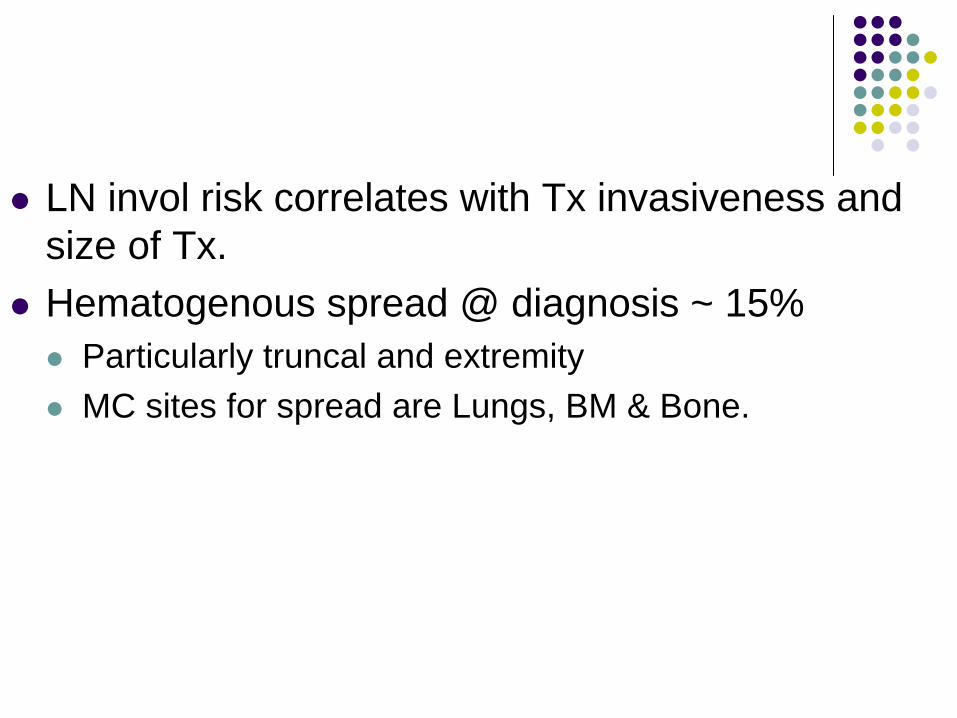
LN invol risk correlates with Tx invasiveness and size of Tx.Hematogenous spread @ diagnosis ~ 15%
Particularly truncal and extremityMC sites for spread are Lungs, BM & Bone.
Histopathology
Standard classificationHorn & Enterline ( 1958 )
Cytohistological ( Palmer) ClassificationBeckwith & Palmer ( 1978 )
SIOP classificationCaillaud et al ( 1989 )
NCI classificationTsokos et al ( 1990 )
International ClassificationNewton & Colleagues
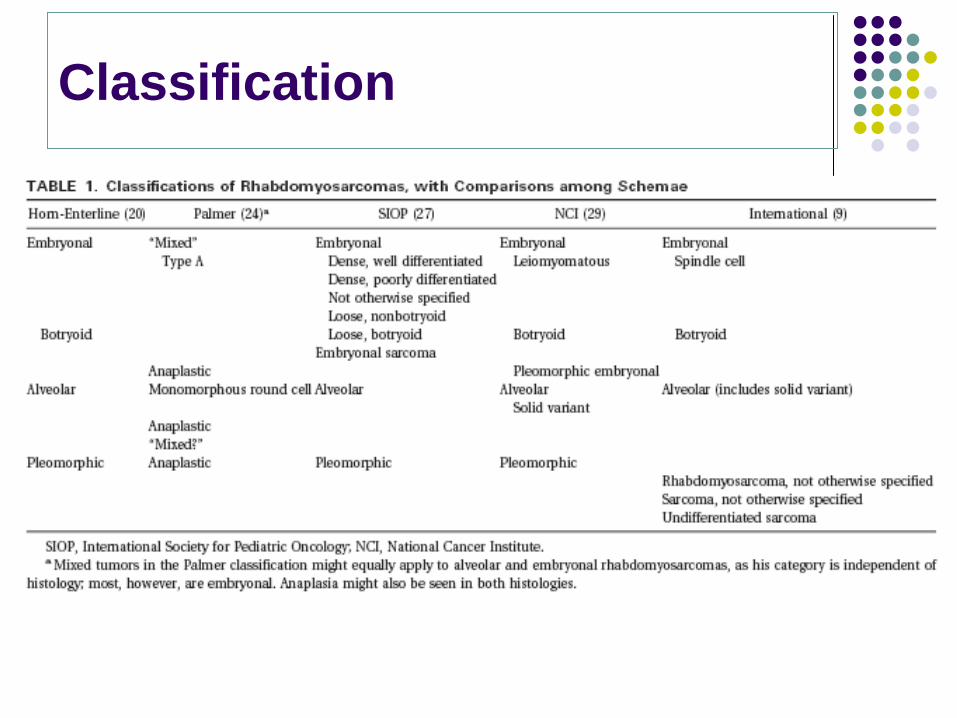
Classification
EMBRYONAL
So named by Berard ( 1894 )tumeur embryonnaire du muscle striae.CHILDREN(60-70%)Most common subtype
Most common in children, in head & neck, GU sites
So named by Berard ( 1894 )tumeur embryonnaire du muscle striae.CHILDREN(60-70%)Most common subtype
Most common in children, in head & neck, GU sites
EMBRYONAL
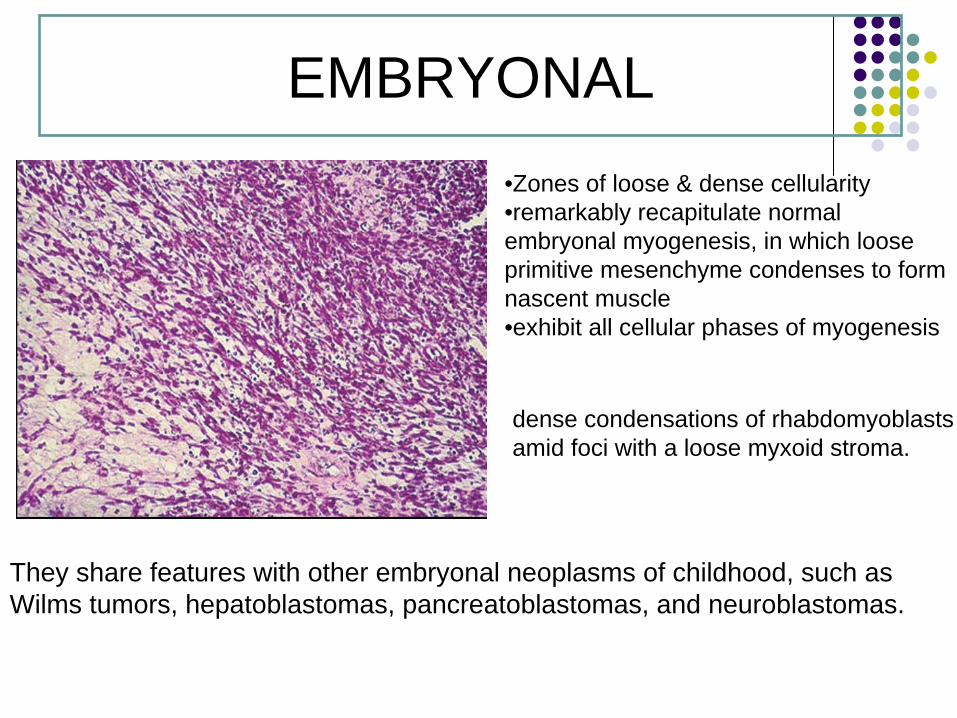
dense condensations of rhabdomyoblasts amid foci with a loose myxoid stroma.
•Zones of loose & dense cellularity•remarkably recapitulate normalembryonal myogenesis, in which loose primitive mesenchyme condenses to form nascent muscle•exhibit all cellular phases of myogenesis
They share features with other embryonal neoplasms of childhood, such as Wilms tumors, hepatoblastomas, pancreatoblastomas, and neuroblastomas.
ALVEOLAR
Riopelle and Theriault (1956)20% of RMS< 1 Yr --- >10 Yr ( Adolescents)Extremities, trunk, perianal, perinealMORE AGGRESSIVEMETASTATIC DISEASE
Riopelle and Theriault (1956)20% of RMS< 1 Yr --- >10 Yr ( Adolescents)Extremities, trunk, perianal, perinealMORE AGGRESSIVEMETASTATIC DISEASE
ALVEOLAR RHABDOMYOSARCOMA
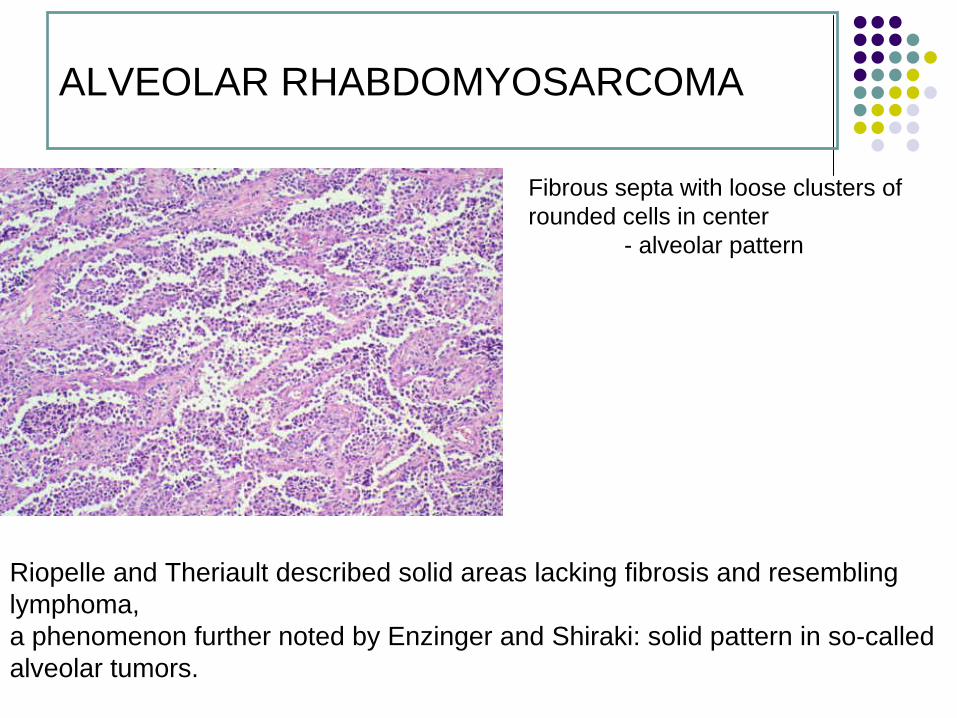
Fibrous septa with loose clusters of rounded cells in center
- alveolar pattern
Riopelle and Theriault described solid areas lacking fibrosis and resembling lymphoma, a phenomenon further noted by Enzinger and Shiraki: solid pattern in so-called alveolar tumors.
BOTRYOID TYPE
Termed by Guersant’ssarcoma botryoides
Subtype of Embryonal10% of all Childhood RMSMucosal Surface
VaginaBilliaryBladderNasopharynx
Most common in hollow visceral organs - GU tract
Superior Prognosis
Termed by Guersant’ssarcoma botryoides
Subtype of Embryonal10% of all Childhood RMSMucosal Surface
VaginaBilliaryBladderNasopharynx
Most common in hollow visceral organs - GU tract
Superior Prognosis
BOTRYOID RHABDOMYOSARCOMA
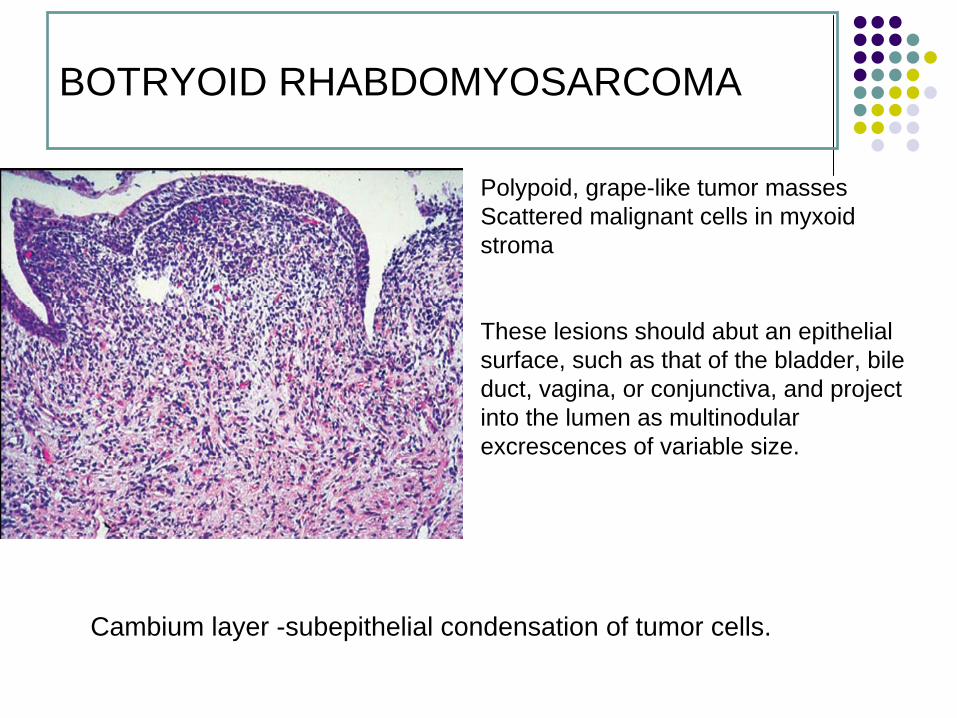
Polypoid, grape-like tumor masses Scattered malignant cells in myxoid stroma
These lesions should abut an epithelial surface, such as that of the bladder, bile duct, vagina, or conjunctiva, and project into the lumen as multinodular excrescences of variable size.
Cambium layer -subepithelial condensation of tumor cells.
SPINDLE CELL
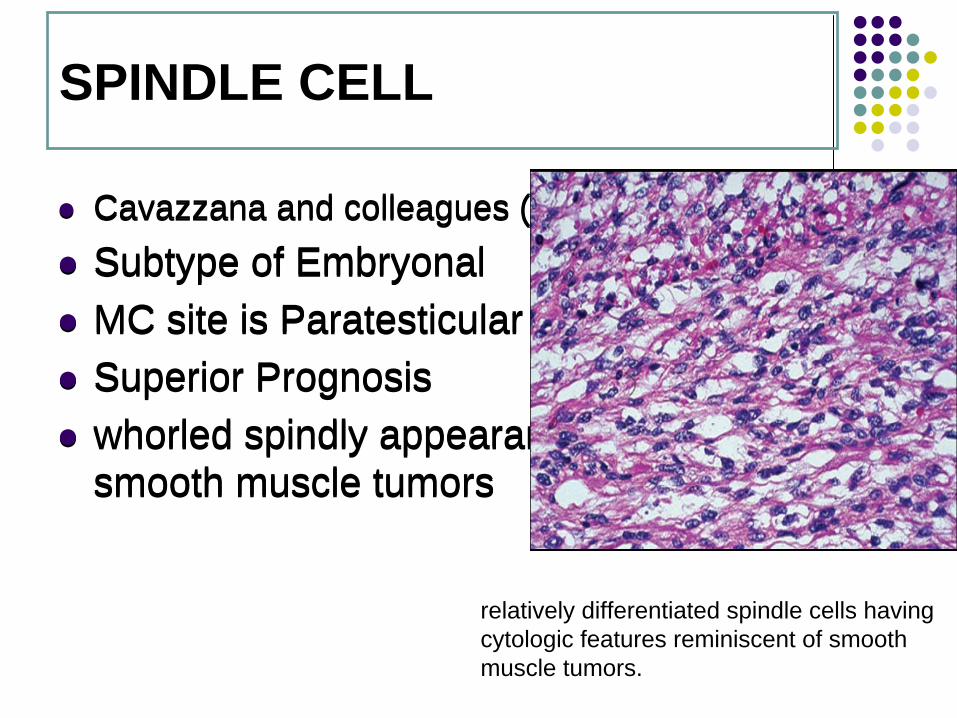
Cavazzana and colleagues ( 1992 )Subtype of EmbryonalMC site is ParatesticularSuperior Prognosiswhorled spindly appearance akin to that of smooth muscle tumors
Cavazzana and colleagues ( 1992 )Subtype of EmbryonalMC site is ParatesticularSuperior Prognosiswhorled spindly appearance akin to that of smooth muscle tumors
relatively differentiated spindle cells havingcytologic features reminiscent of smooth muscle tumors.
Diagnosis of exclusionPreviously called PleomorphicRare in childrenMore common in Adults ( 30-50 Yrs)In skeletal muscles of older people, thigh
Marked pleomorphismIrregularly arranged cellsMultinucliated giant cells
UNDIFFERENTIATED
UNDIFFERENTIATED
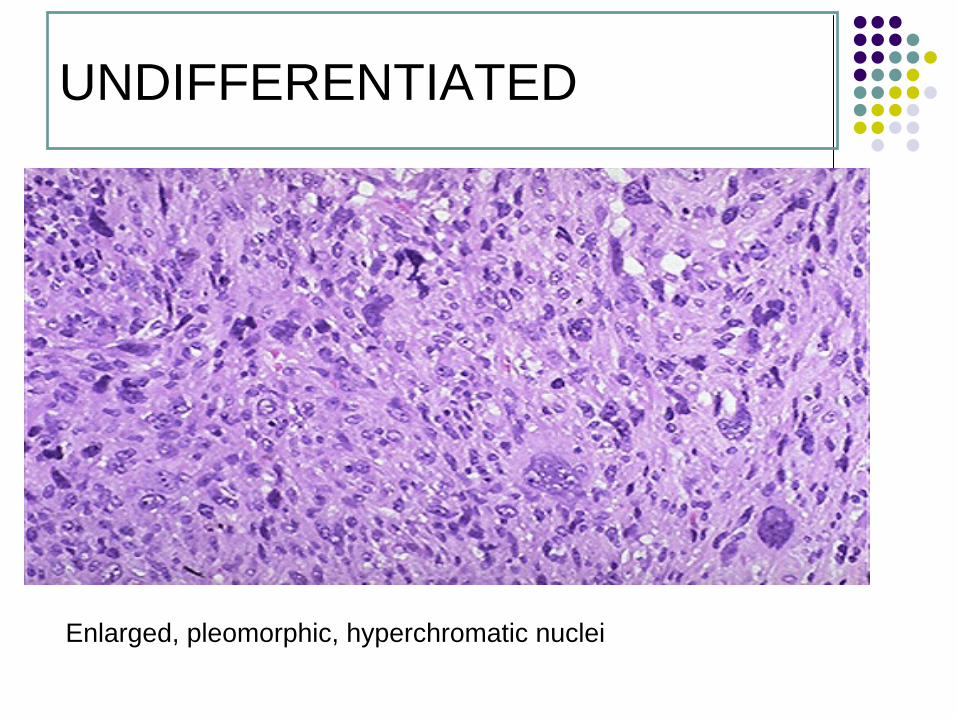
Enlarged, pleomorphic, hyperchromatic nuclei
Cytogenetics
Alveolar RhabdomyosarcomaT(2,13)(p35;q14)
70% of all alveolar RMSFuses PAX3:FKHR
T(1,13)(p36:q14)20% all alveolar RMSFuses PAX7:FKHROccurs in younger children, better prognosis
Genomic amplificationMDM2, CDK4
Near-tetraploidy
Cytogenetics
EmbryonalRhabdomyosarcoma
Loss of heterozygosity at 11pLoss of amplificationHyperploidy
Cell cycle controlMyogenesis = Mesenchymal fibroblast Skeletal muscleControlled by MyoD protein family (Myogenin, MYF5, MYF6)Can stain RMS cells with anti-MyoD Ab
Tumor Suppressor Genes
P53 mutation
ProtooncogenesN-myc amplification Especially seen in alveolar histology
Cytogenetics
The prognostic value of DNA ploidy and proliferative index (PI) DNA hyperdiploid and tetraploidrhabdomyosarcomas had a favorable prognosiswhile DNA diploid and polyploid tumors had a poor prognosis.
Am J Clin Pathol 2004;121:358-365
Clinical Presentation
Occurs in multiple primary sitesUsually presents as a asymptomatic masssymptoms relate to mass effect on asso. OrganOrbital
Proptosis, ophthalmoplegiaParameningial
Nasal, Aural or sinus obstruction, CN Palsies & headache etc.
GenitourinaryHematuria, Urinary obstruction or constipation.
LocationDeep lesions tend to be malignant--Superficial lesions - benign
SizeLarger tumors tend to be malignant
Growth patternRapidly growing - malignant-Infiltrating - malignant
Metastasis
Sites
Head & NeckOrbitNon-ParameningialParameningial
TrunkRetroperitonialParatesticularGenitourinary
Extremities
Head & Neck (Para-meningeal)
Sites: Nasopharynx, Nasal cavity, PNS, Middle ear, Pterygopalatine fossa.Have propensity for base skull invasion & intracranial extension.Common histological subtype: ERMS.Incidence of lymph node involvement (IRS III): <20%.Possibility of complete surgical excision (IRS III): <25%.
Sites: Nasopharynx, Nasal cavity, PNS, Middle ear, Pterygopalatine fossa.Have propensity for base skull invasion & intracranial extension.Common histological subtype: ERMS.Incidence of lymph node involvement (IRS III): <20%.Possibility of complete surgical excision (IRS III): <25%.
Head & Neck (Non-parammeningeal)
Sites: Parotid, Oral cavity, Oropharynx and Larynx.Common histological subtype: Embryonal RMS.Buccal mucosa: Alveolar RMSScalpIncidence of lymph node involvement (IRS III): <20%. Prophylactic / Elective nodal irradiation not recommended.
Sites: Parotid, Oral cavity, Oropharynx and Larynx.Common histological subtype: Embryonal RMS.Buccal mucosa: Alveolar RMSScalpIncidence of lymph node involvement (IRS III): <20%. Prophylactic / Elective nodal irradiation not recommended.
Pelvic RMS:
Urinary Bladder Common histologic subtype: Embryonal RMSLymph node involvement: 20% (Hypogastric &
Ext. iliac)IRS III - Chemo + Radiotherapy → Surgery for residual diseaseIRS III - Bladder preservation: 55% with 90% survival
Urinary Bladder Common histologic subtype: Embryonal RMSLymph node involvement: 20% (Hypogastric &
Ext. iliac)IRS III - Chemo + Radiotherapy → Surgery for residual diseaseIRS III - Bladder preservation: 55% with 90% survival
Paratesticular
Along spermatic cord; from interscrotal area through the inguinal canal.Lymph node involvement: 30% (paraaortic / renal hilar) If LN +ve (radiological): Ipsilateral. Nerve sparing LN dissn./ Regional nodal irradn.
i) dissect entire s.cord after orchidectomyii) sample abdominopelvic nodes, except for Gr. Iiii) scrotal violation / involvement: need scrotal RT.
Along spermatic cord; from interscrotal area through the inguinal canal.Lymph node involvement: 30% (paraaortic / renal hilar) If LN +ve (radiological): Ipsilateral. Nerve sparing LN dissn./ Regional nodal irradn.
i) dissect entire s.cord after orchidectomyii) sample abdominopelvic nodes, except for Gr. Iiii) scrotal violation / involvement: need scrotal RT.
Orbit
Common histological subtype: Embryonal RMSGeneral treatment policy: Incisional Biopsy for diagnosis → Chemo+ RT Radiotherapy volume: Entire orbit need not be included. Shield lachrymal gland & duct.
Significant role of 3D CRT / IMRT.Survival: 90-95% at 5years (with CT + RT).
Common histological subtype: Embryonal RMSGeneral treatment policy: Incisional Biopsy for diagnosis → Chemo+ RT Radiotherapy volume: Entire orbit need not be included. Shield lachrymal gland & duct.
Significant role of 3D CRT / IMRT.Survival: 90-95% at 5years (with CT + RT).
Extremity
Common histological subtype: Alveolar RMS Lymph node involvement: 27-30% General treatment policy: W/E + LN sampling →Chemo + RT .Radiotherapy: No RT if R0 & N0 & ≤ 5cm tumor(primary surgery).Entire LN region irradiated if sampling +ve.Strip of tissue spared for lymph drainage.
Common histological subtype: Alveolar RMS Lymph node involvement: 27-30% General treatment policy: W/E + LN sampling →Chemo + RT .Radiotherapy: No RT if R0 & N0 & ≤ 5cm tumor(primary surgery).Entire LN region irradiated if sampling +ve.Strip of tissue spared for lymph drainage.
Retroperitoneal:
Common histological subtype: Alveolar RMSGeneral treatment policy: W/E + Chemo + RT Poor prognosis: 5year survival - 40%.
Common histological subtype: Alveolar RMSGeneral treatment policy: W/E + Chemo + RT Poor prognosis: 5year survival - 40%.
Diagnostic Evaluation
Thorough physical examinationRoutine Blood examinationHistopathologic evaluation
BiopsyImmunohistochemistry – Cytokeratin, Vimentin, Smooth muscle Actin, Desmin, S100, CD31,34
FISHRT PCR
CT/MRI of primary
Diagnostic Evaluation
Site specificH&N, Parameningial- CSF examinationGU - Examination under anesthesiaIntravenous pyelography for retroperitoneal tumorsCystoscopy
Metastatic workupChest X rayBone marrow biopsyBone scan
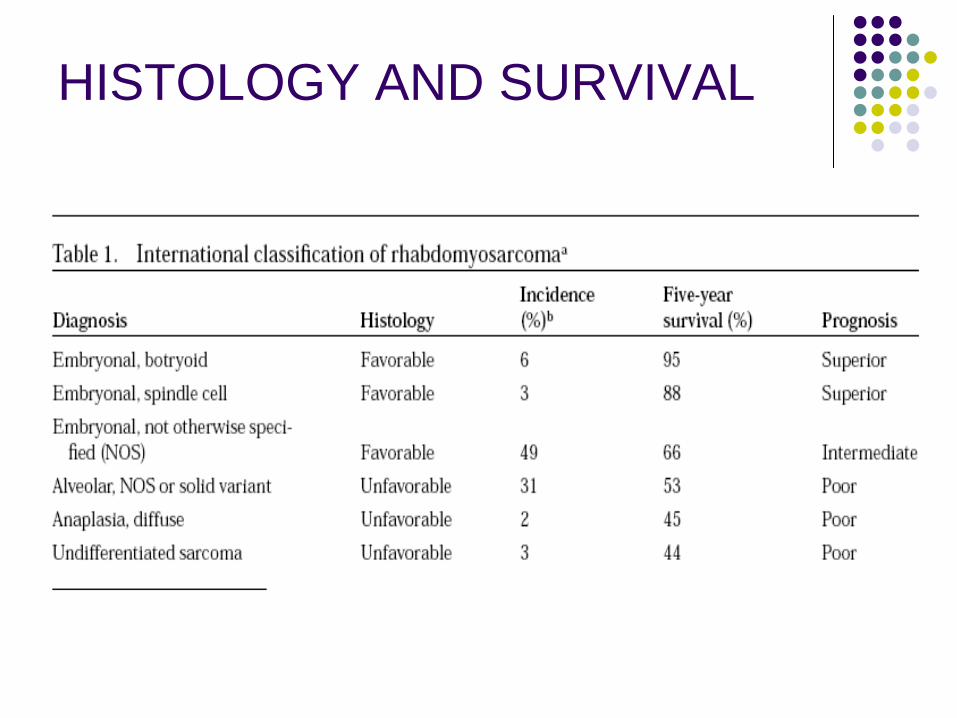
HISTOLOGY AND SURVIVAL
Grouping
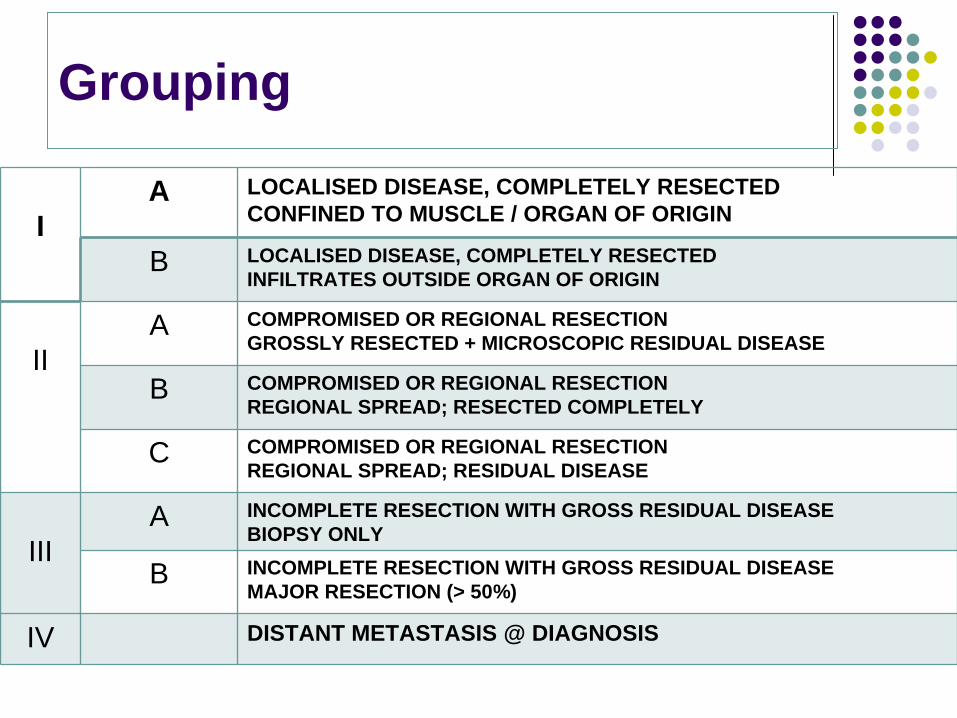
IA LOCALISED DISEASE, COMPLETELY RESECTED
CONFINED TO MUSCLE / ORGAN OF ORIGIN
B LOCALISED DISEASE, COMPLETELY RESECTED INFILTRATES OUTSIDE ORGAN OF ORIGIN
IIA COMPROMISED OR REGIONAL RESECTION
GROSSLY RESECTED + MICROSCOPIC RESIDUAL DISEASE
B COMPROMISED OR REGIONAL RESECTIONREGIONAL SPREAD; RESECTED COMPLETELY
C COMPROMISED OR REGIONAL RESECTIONREGIONAL SPREAD; RESIDUAL DISEASE
IIIA INCOMPLETE RESECTION WITH GROSS RESIDUAL DISEASE
BIOPSY ONLY
B INCOMPLETE RESECTION WITH GROSS RESIDUAL DISEASEMAJOR RESECTION (> 50%)
IV DISTANT METASTASIS @ DIAGNOSIS
Group
Group Incidence
I 16%
II 20%
III 48%
IV 16%
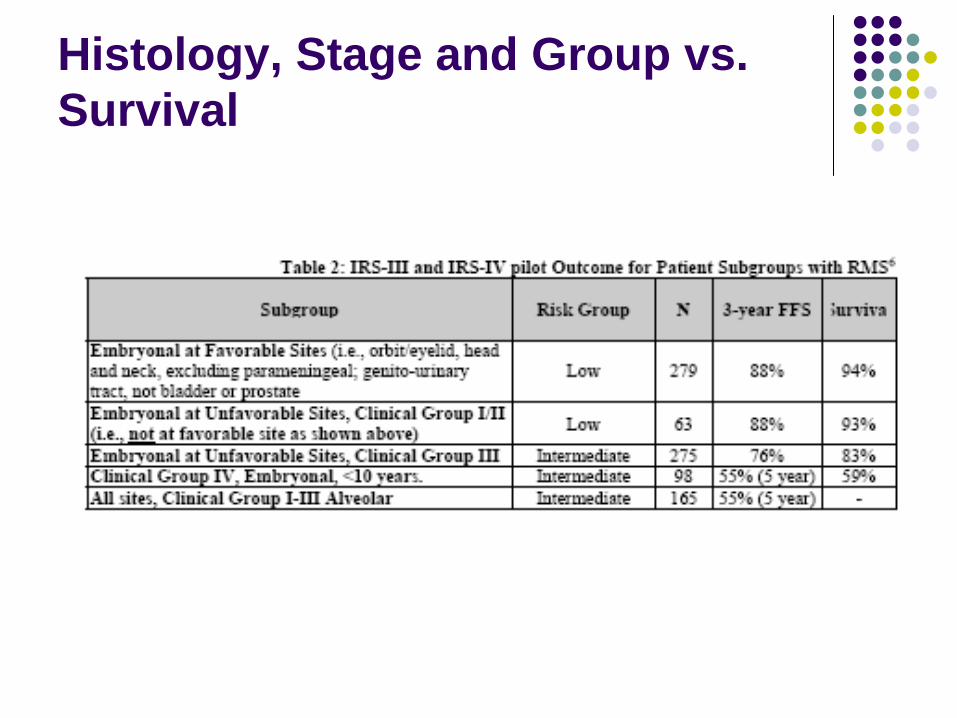
Histology, Stage and Group vs. Survival
Staging
Stage ISites
OrbitH&N (excluding parameningeal) GU (non-bladder, non-prostate)Biliary tract
Tumor invasiveness: T1 or T2Tumor Size: a or bLymph node status: any NMetastasis: M0
(T1: confined to anatomic site of origin; T2: extension; a: <5 cm in diameter; b: >5 cm in diameter; N0: no clinically involved LN; N1: clinically involved LN; M1: metastasis present)
Stage II
Stage IISites
ParameningealNasopharynx/Nasal CavityMiddle Ear and Mastoid regionParanasal SinusesInfratemporal fossaPterygopalatine fossaParapharyngeal space
Bladder or ProstateExtremity
Stage IITumor Invasiveness: T1 or T2Tumor size: aLymph node status: N0 or NxMetastasis: M0
Stage III & IV
Stage IIISites: Same as Stage IITumor Invasiveness: T1 or T2Tumor size and Lymph Node status
a N1b any N
Metastasis: M0
Stage IVSites: AllMetastasis: M1
RHABDOMYOSARCOMA Part-II
Dr. Pramod Tike ,JR-IIDr. Kanhu Patro, SR-II
Dept. Of Radiation Oncology, TMH
TREATMENT
RHABDOMAYOSARCO MA
TREATMENT SEQUENCE
CHEMOTHERAPY REGIMEN
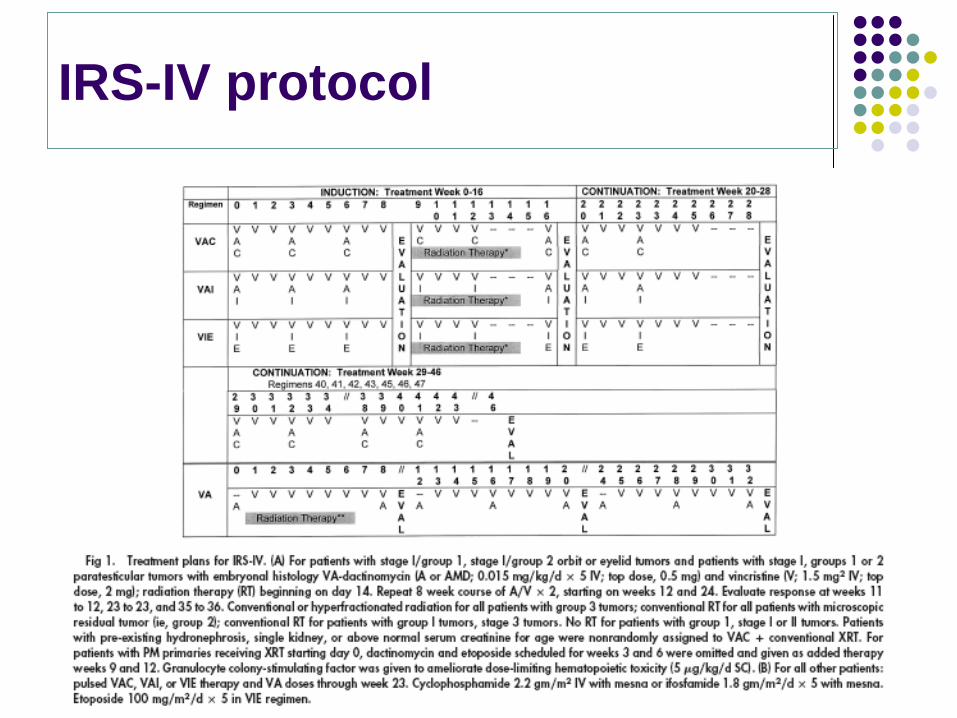
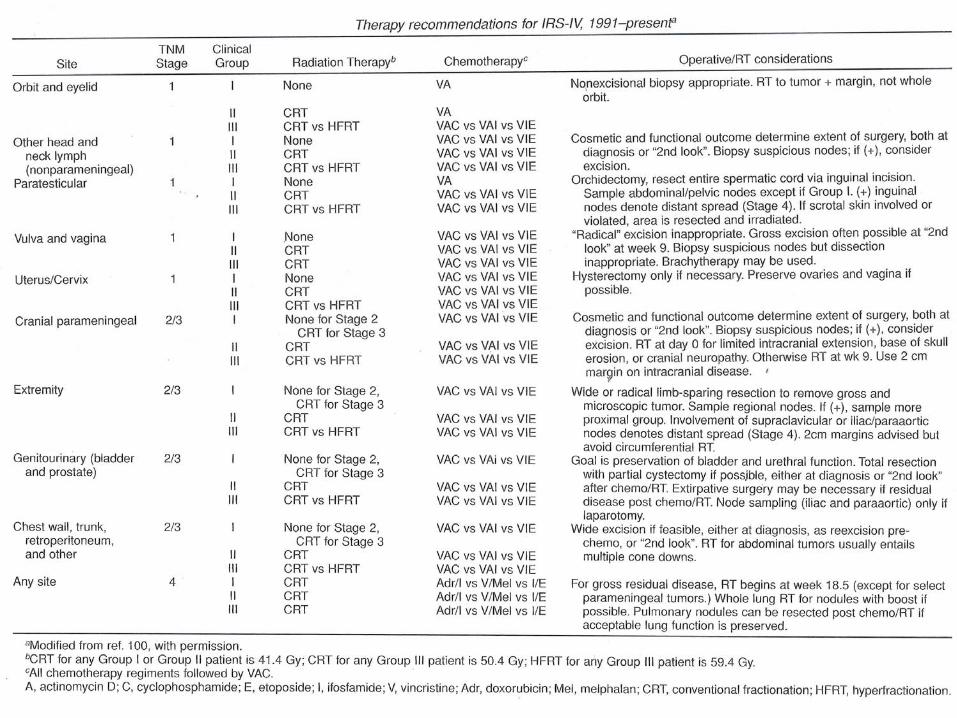
IRS-IV protocol
LOCAL THERAPY
SURGERY GUIDELINES
If wide resection is possible surgery with resection and suitable reconstruction.
If chemotherapy has not been very effective (as judged from clinical response, post chemo MRI) and wide resection is not feasible ablative surgery in the form of an amputation is recommended. Maintenance chemotherapy is subsequently used.
Surgery should be reasonable i.e.: removal of tumor bulk with maximum preservation of organ & function.
If wide resection is possible surgery with resection and suitable reconstruction.
If chemotherapy has not been very effective (as judged from clinical response, post chemo MRI) and wide resection is not feasible ablative surgery in the form of an amputation is recommended. Maintenance chemotherapy is subsequently used.
Surgery should be reasonable i.e.: removal of tumor bulk with maximum preservation of organ & function.
RADIOTHERAPY
INDICATIONALL STAGE EXCEPT GR-1 EMBRYONAL HISTOLOGYDOSEMARGINTIMING
INDICATIONALL STAGE EXCEPT GR-1 EMBRYONAL HISTOLOGYDOSEMARGINTIMING
RT-TIMING
Base skull erosion Cranial nerve palsy meningeal invasion
None of the above features - "week 9".
Base skull erosion Cranial nerve palsy meningeal invasion
None of the above features - "week 9".
DAY- 0
RADIOTHERAPY-MARGIN
Gross pre-chemotherapy volume + 2cm. Modified in special sites adjacent to critical structuresIn sites where tumor grows into body cavities: post-chemo volume + 2cm.Microscopic disease (IRS group I & II) -
Gross pre-chemotherapy volume + marginGross disease (IRS group III) –
Phase I - Gross pre-chemotherapy volume + marginPhase II - Post-chemotherapy / volume + margin*
Gross pre-chemotherapy volume + 2cm. Modified in special sites adjacent to critical structuresIn sites where tumor grows into body cavities: post-chemo volume + 2cm.Microscopic disease (IRS group I & II) -
Gross pre-chemotherapy volume + marginGross disease (IRS group III) –
Phase I - Gross pre-chemotherapy volume + marginPhase II - Post-chemotherapy / volume + margin*
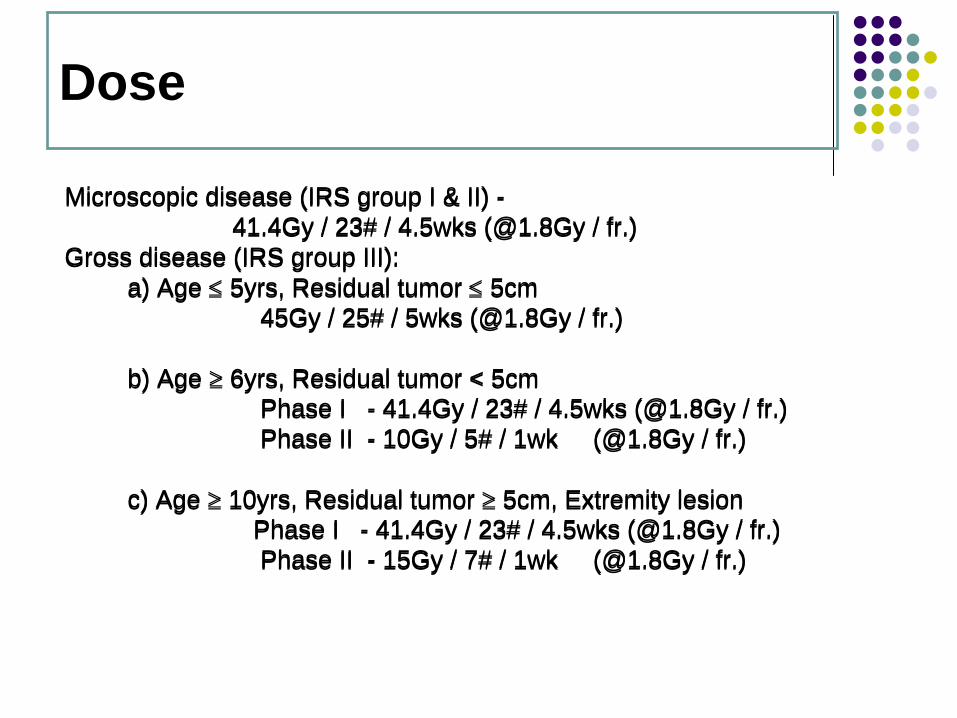
Dose
Microscopic disease (IRS group I & II) -41.4Gy / 23# / 4.5wks (@1.8Gy / fr.)
Gross disease (IRS group III): a) Age ≤
5yrs, Residual tumor ≤
5cm 45Gy / 25# / 5wks (@1.8Gy / fr.)
b) Age ≥
6yrs, Residual tumor < 5cmPhase I - 41.4Gy / 23# / 4.5wks (@1.8Gy / fr.)Phase II - 10Gy / 5# / 1wk (@1.8Gy / fr.)
c) Age ≥
10yrs, Residual tumor ≥
5cm, Extremity lesionPhase I - 41.4Gy / 23# / 4.5wks (@1.8Gy / fr.)Phase II - 15Gy / 7# / 1wk (@1.8Gy / fr.)
Microscopic disease (IRS group I & II) -41.4Gy / 23# / 4.5wks (@1.8Gy / fr.)
Gross disease (IRS group III): a) Age ≤
5yrs, Residual tumor ≤
5cm 45Gy / 25# / 5wks (@1.8Gy / fr.)
b) Age ≥
6yrs, Residual tumor < 5cmPhase I - 41.4Gy / 23# / 4.5wks (@1.8Gy / fr.)Phase II - 10Gy / 5# / 1wk (@1.8Gy / fr.)
c) Age ≥
10yrs, Residual tumor ≥
5cm, Extremity lesionPhase I - 41.4Gy / 23# / 4.5wks (@1.8Gy / fr.)Phase II - 15Gy / 7# / 1wk (@1.8Gy / fr.)
FOLLOW-UP- Frequency
Every 3 monthly for the 1st yrEvery 6 monthly for the 2nd & 3rd yrYearly thereafter
Every 3 monthly for the 1st yrEvery 6 monthly for the 2nd & 3rd yrYearly thereafter
FOLLOW UP- Investigations
Relevant History Physical examination & documentationHaematological evaluation:
Hb, TC, PlateletLiver Function Tests (LFT)Renal Function Tests (RFT)Radiological evaluation: CXR
X-ray of local partBone scans CT chest
Bone Scan/ CT scan chest is done every 6 months for the first 2 years and every year for the next 3 years.Other investigations (MRI/ CT Scan of local part) to be done as specified after discussion in the Pediatric joint clinic.
Relevant History Physical examination & documentationHaematological evaluation:
Hb, TC, PlateletLiver Function Tests (LFT)Renal Function Tests (RFT)Radiological evaluation: CXR
X-ray of local partBone scans CT chest
Bone Scan/ CT scan chest is done every 6 months for the first 2 years and every year for the next 3 years.Other investigations (MRI/ CT Scan of local part) to be done as specified after discussion in the Pediatric joint clinic.
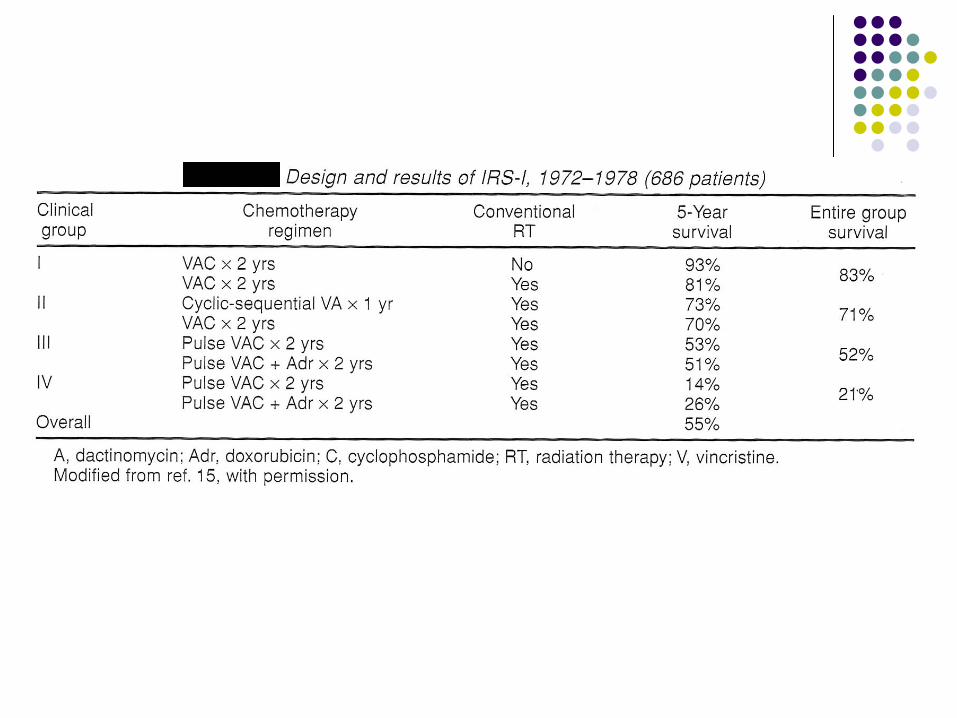
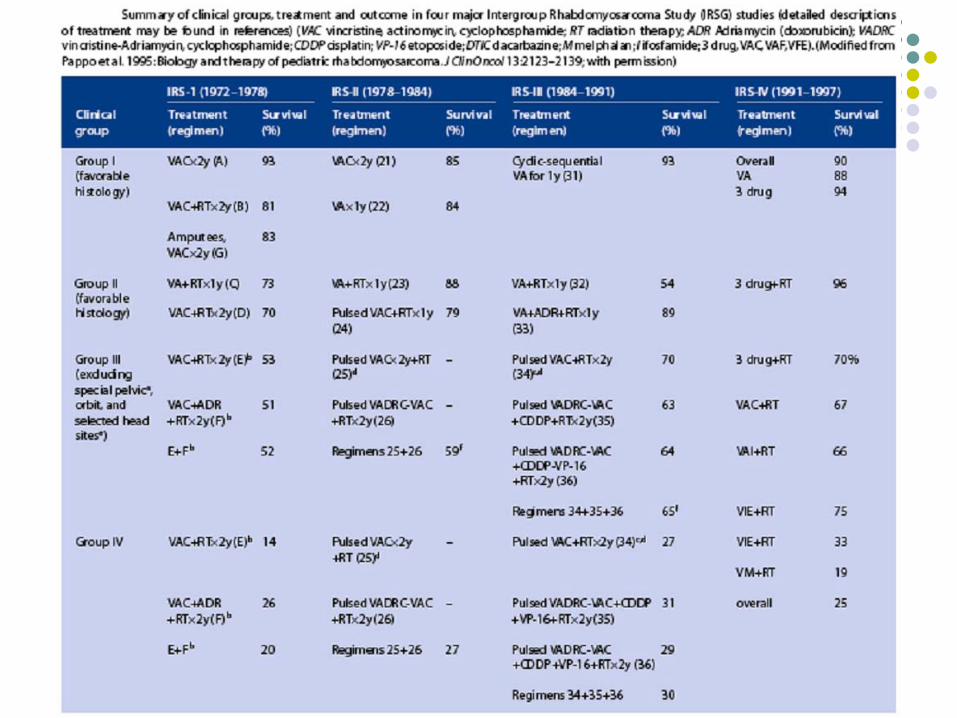
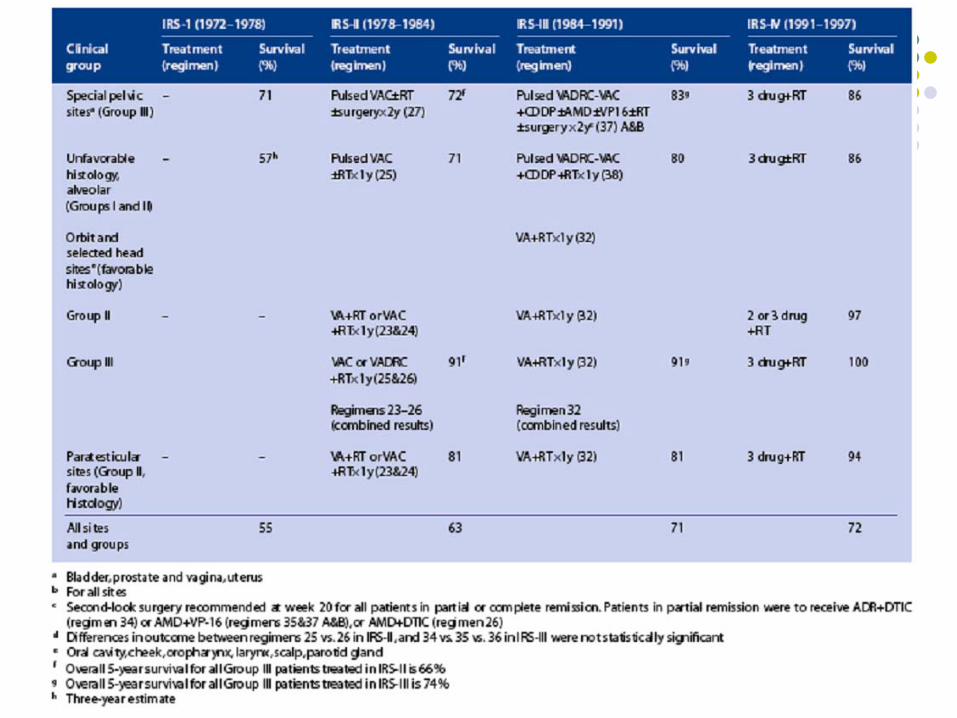
Intergroup Rhabdomyosarcoma Study Group
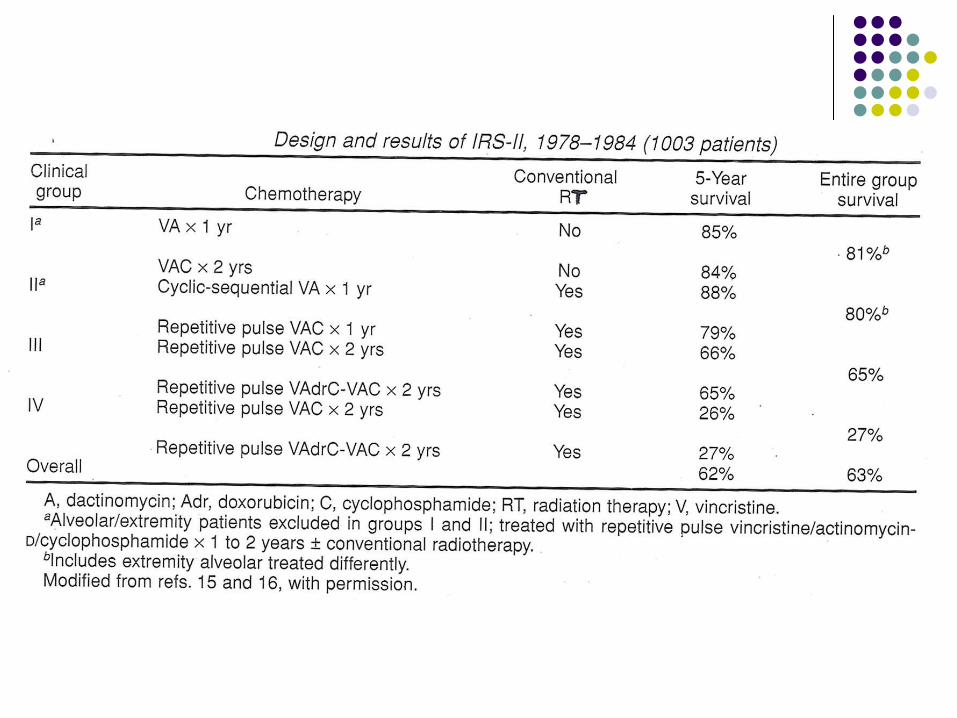
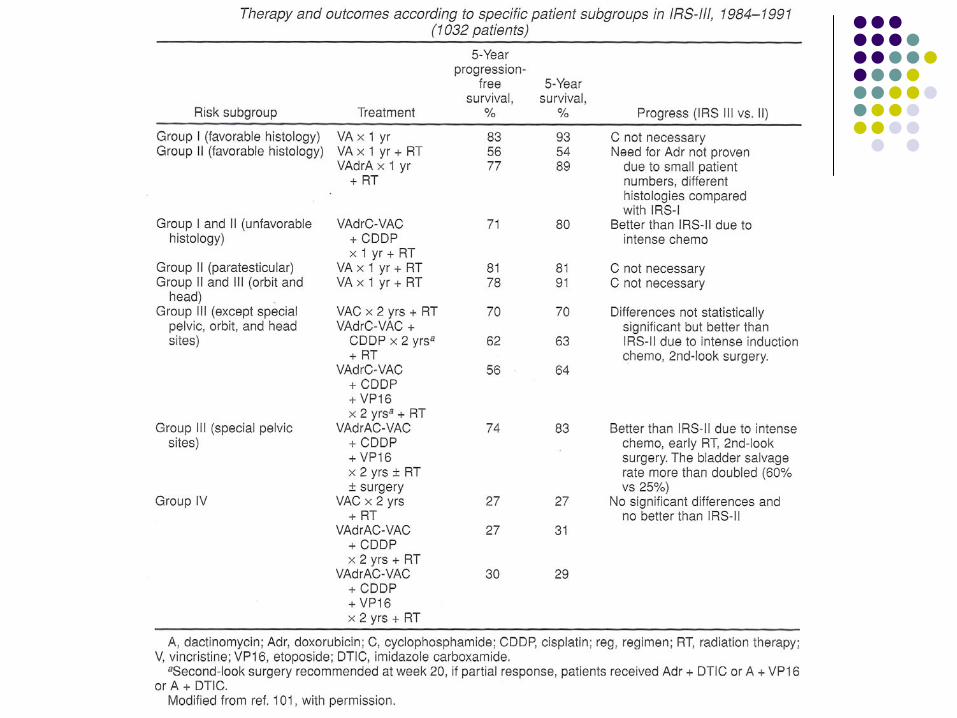
COG, CCG, POGIRS I (1972 – 1978) OS 55%IRS II (1978 – 1984) OS 63%IRS III (1984 – 1991) OS 71%IRS IV (1991 – 1997) OS 71%IRS V (1998 – present)
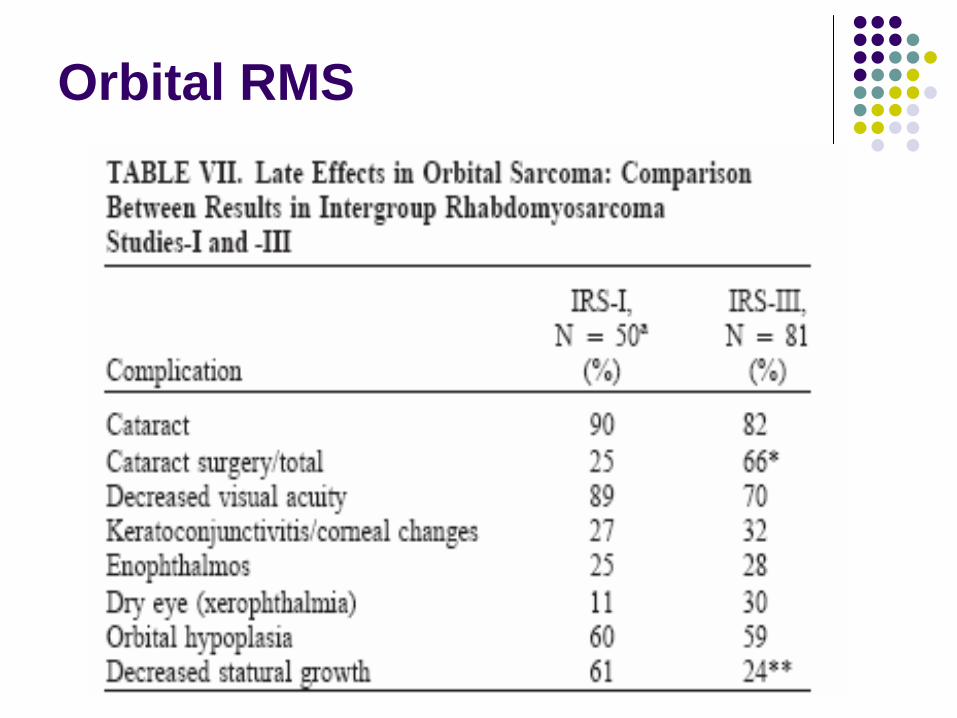
Orbital RMS
9% of all RMSMost common single H&N siteUsually diagnosed early; presents with eye swelling, globe displacement2/3 of cases are Group III
Can invade meningesvia SOF84% Embryonal; 10% Alveolar5 y OS for Embryonal94%; for Alveolar 74%
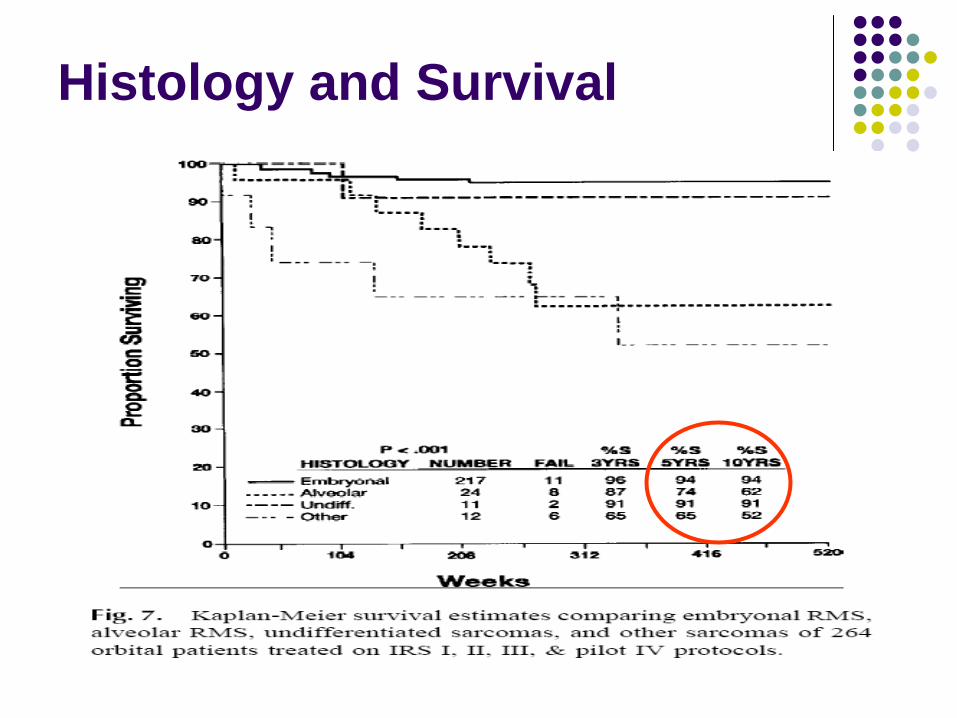
Histology and Survival
Historical management
Orbital Exenteration was standard treatment until mid 1960s
High rate of local failurePoor survival
Late 1960s, Cassady et al. showed that RT after biopsy offered local control in 4/5 patients
Orbital RMS
IRS IGroup I patients randomized to VAC +/- RTGroup II VA + RT +/- CGroup III/IV VAC + RT +/- AdriamycinPts with Group II or III disease 85-94% OS @ 6 years5 y OS 89%; 3/6 deaths 2/2 other causesComplete or Partial surgical excision no longer recommended standard of care
Orbital RMS
IRS IIGroup I VA or VAC (no RT)Group II VA + RT +/- CGroup III VAC +RT +/- AdriamycinNo improvement in any of the more intensive chemotherapy armsOS/FFS better in all arms compared to IRS I
Orbital RMS
IRS IIIGroup I VA onlyGroups II and III, VA +RTNo difference in OS or FFS compared to IRS II3 y/o FFS 92% and OS 100%
IRS IVGroup I VA onlyGroup II VA + CD RTGroup III VAC vs. VAI vs. VIE AND CD RT vs. HF XRT
RT doses 50.4 Gy vs. 59.4 GyGroups I & II pts. 3 y FFS 91%, OS 100% (no change compared to IRS III
Orbital RMS
IRS IVGroup III, 3 y FFS 94%, OS 98%No difference in the 3 chemotherapy arms or the 2 RT armsHowever, when compared to IRS III, pts. with 3 drug chemotherapy regimens did better than VA regimen
IRS VDue to concern for treatment related toxicities
Chemotherapy C/I/E dropped; back to VART dose decreased to 45 Gy
SIOP MMT 84 trial
Evaluated eliminating radiation in Group II/III patients34 patients treated initially with VA aloneRT reserved for those who did not achieve a complete response22 patients initially did not get radiation 11 failed locally
10/11 salvaged with RT + chemotherapy3/11 developed distant mets 2 died
4 y/o EFS 62%; 4y/o OS 84%
Orbital RMS
Conclusions
Total surgical extenteration no longer standard of careChemotherapy alone in Group I patients is effectiveChemo + RT for Group II and III patientsFuture trend for RT
Dose reductionElectrons, ProtonsIMRT treatment planning
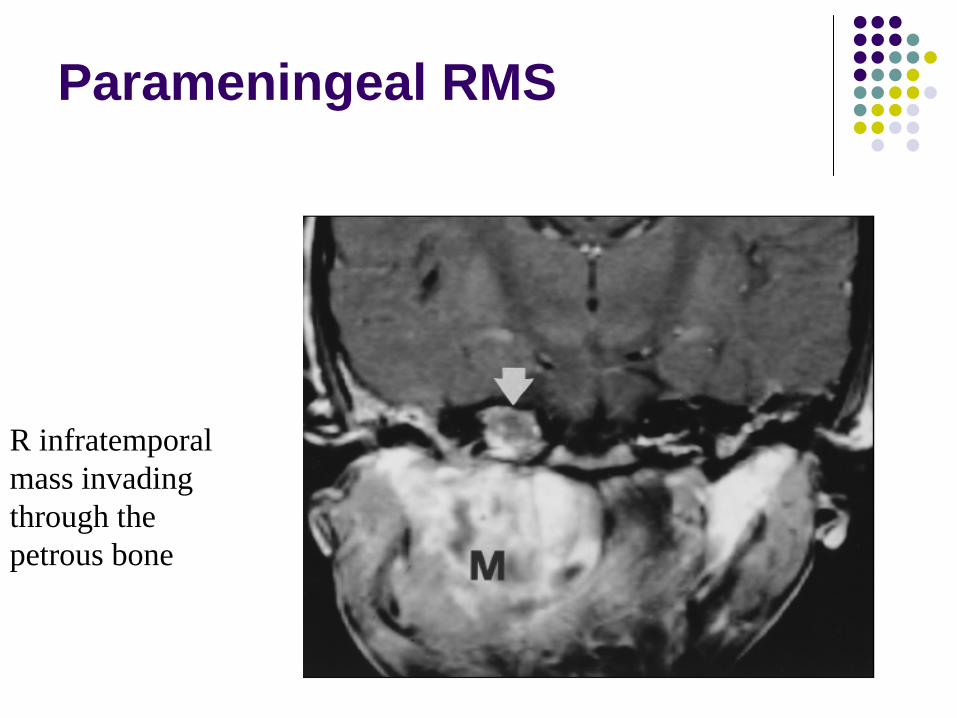
Parameningeal RMS
R infratemporal mass invading through the petrous bone
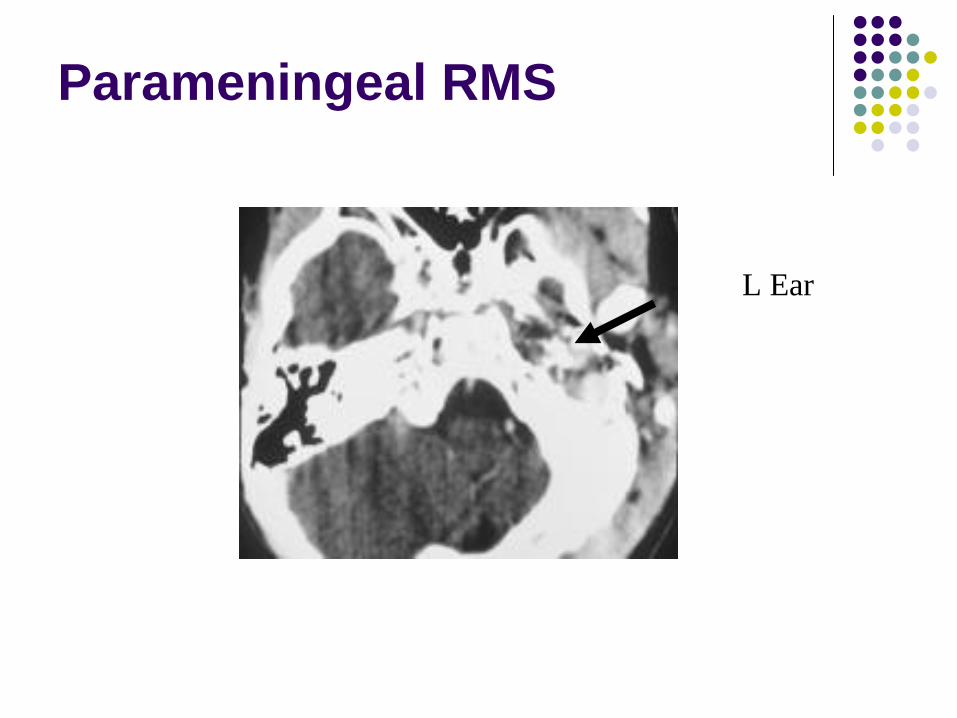
Parameningeal RMS
L Ear
Parameningeal RMS
16 % of all RMS41 % of all H&N RMSMost cases in children < 8 -10 years of ageCan extend intra-cranially and produce neoplasticmeningitis (35% of all PM RMS)<20% have LN involvement (IRS III)Most have favorable histology (Embryonal: Alveolar 4:1)
Parameningeal RMS
Meningeal penetration and leptomeningealtumor cell seeding must be assessed Complete surgical extirpation almost never possible76% are Group III (IRS III)Hence, surgery is generally either a biopsy or subtotal resection
Parameningeal RMS - Sites
Nasal Cavity/Nasopharynx/Paranasal Sinuses can invade through basal foramina, sinus roofsMiddle Ear can extend through tegmentympani into the middle cranial fossa or through posterior mastoid into the posterior cranial fossaParapharyngeal spacePterygopalatine / Infratemporal fossa
PM RMS
IRS I3 y PFS 46%
Orbit 91 %Non-PM H&N 75%
Meningeal extension occurred in 35% of cases at a median time of 5 months after diagnosisMeningeal extension was likely fatal 90%Associated with inadequate margins and doses < 50 Gy
PM RMS – IRS II -III
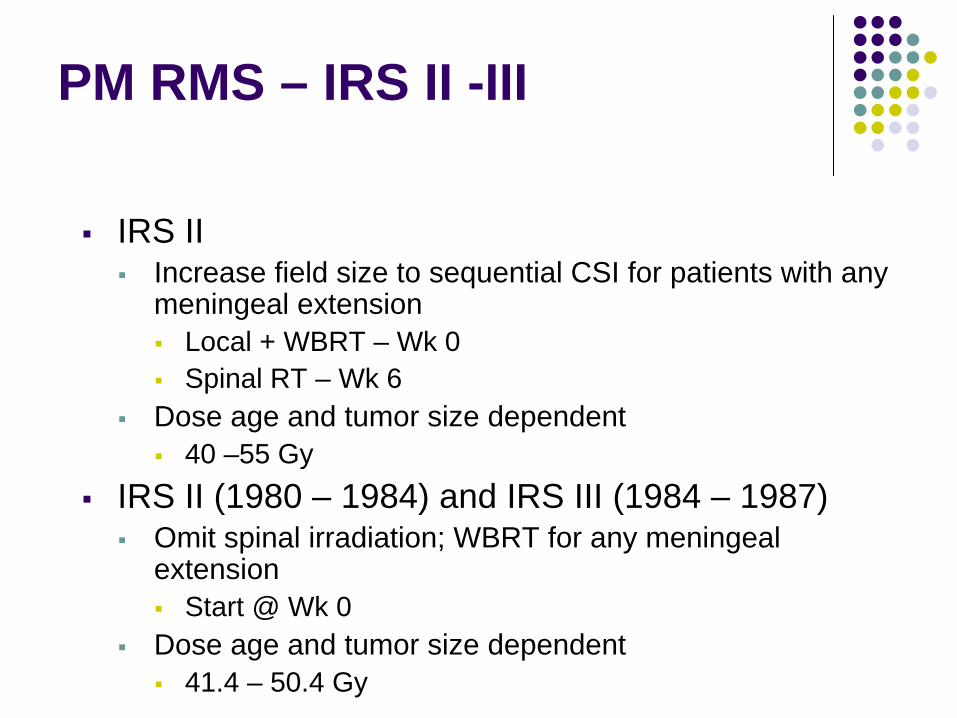
IRS IIIncrease field size to sequential CSI for patients with any meningeal extension
Local + WBRT – Wk 0Spinal RT – Wk 6
Dose age and tumor size dependent40 –55 Gy
IRS II (1980 – 1984) and IRS III (1984 – 1987)Omit spinal irradiation; WBRT for any meningealextension
Start @ Wk 0Dose age and tumor size dependent
41.4 – 50.4 Gy
PM RMS – IRS IV
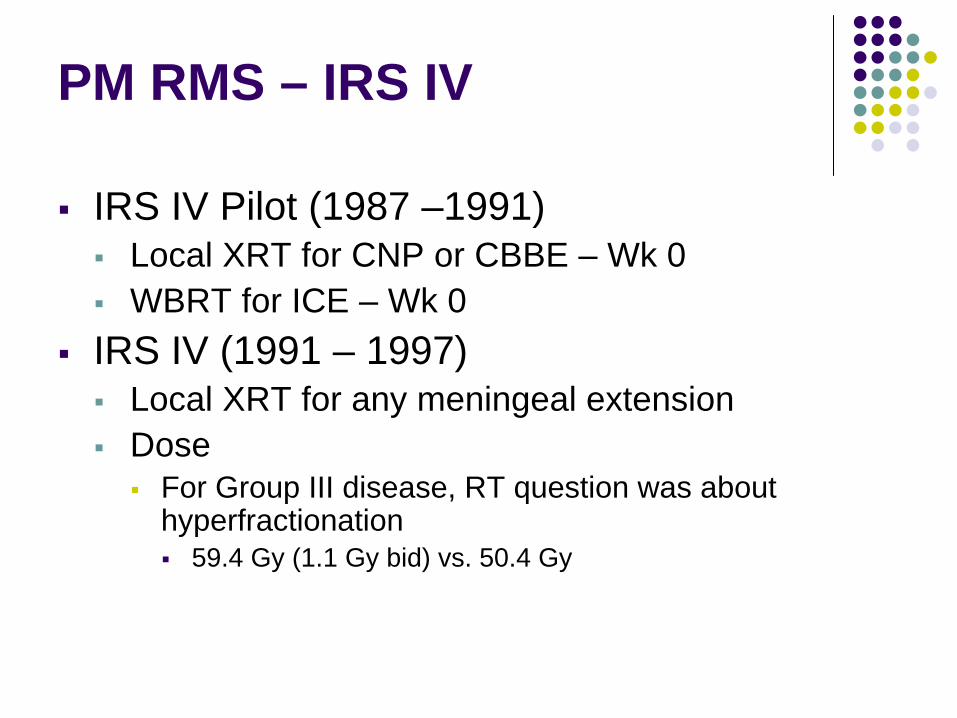
IRS IV Pilot (1987 –1991)Local XRT for CNP or CBBE – Wk 0WBRT for ICE – Wk 0
IRS IV (1991 – 1997)Local XRT for any meningeal extensionDose
For Group III disease, RT question was about hyperfractionation
59.4 Gy (1.1 Gy bid) vs. 50.4 Gy
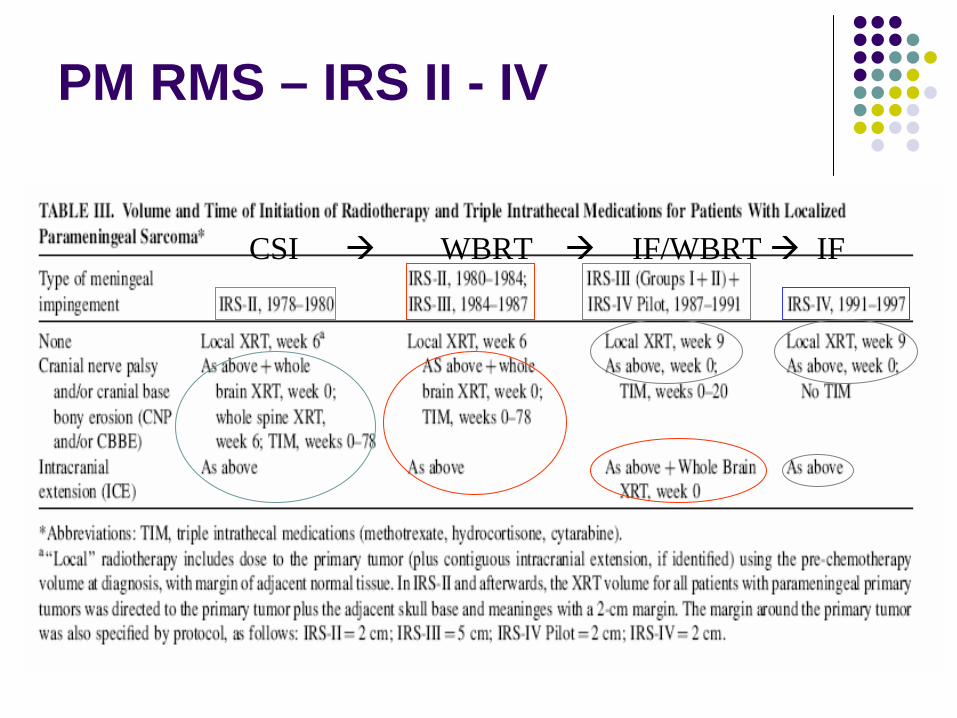
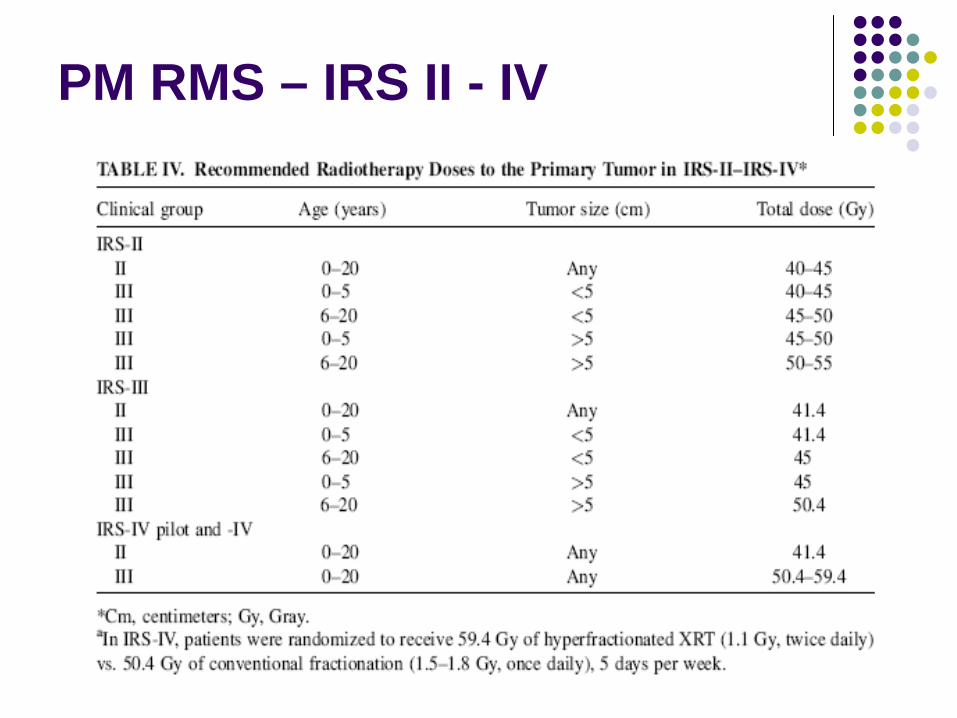
PM RMS – IRS II - IV
CSI WBRT IF/WBRT IF
PM RMS – IRS II - IV
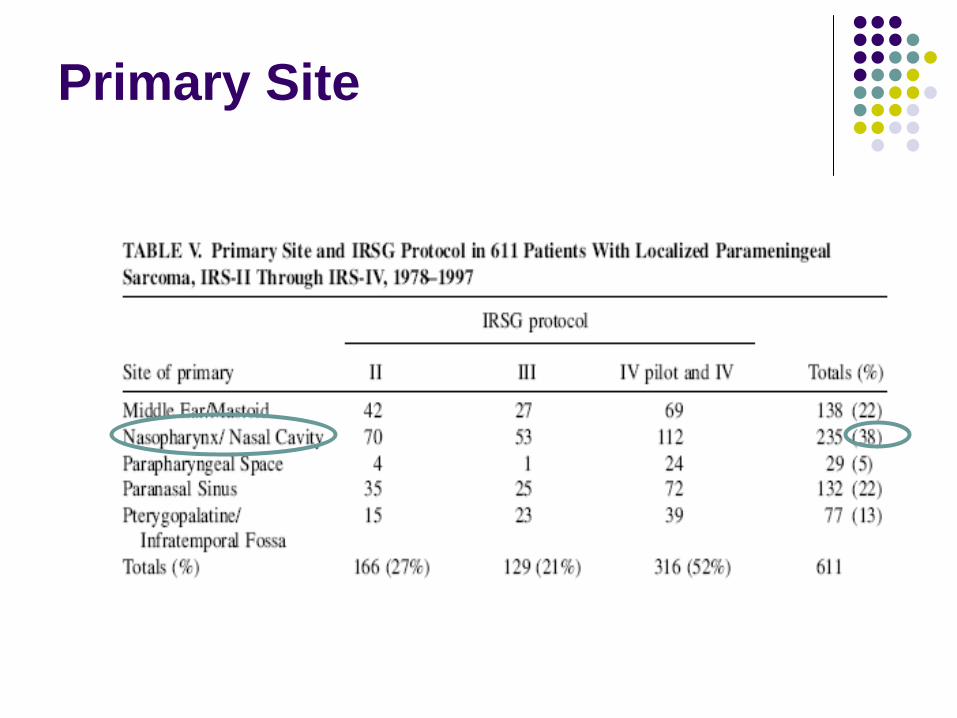
Primary Site
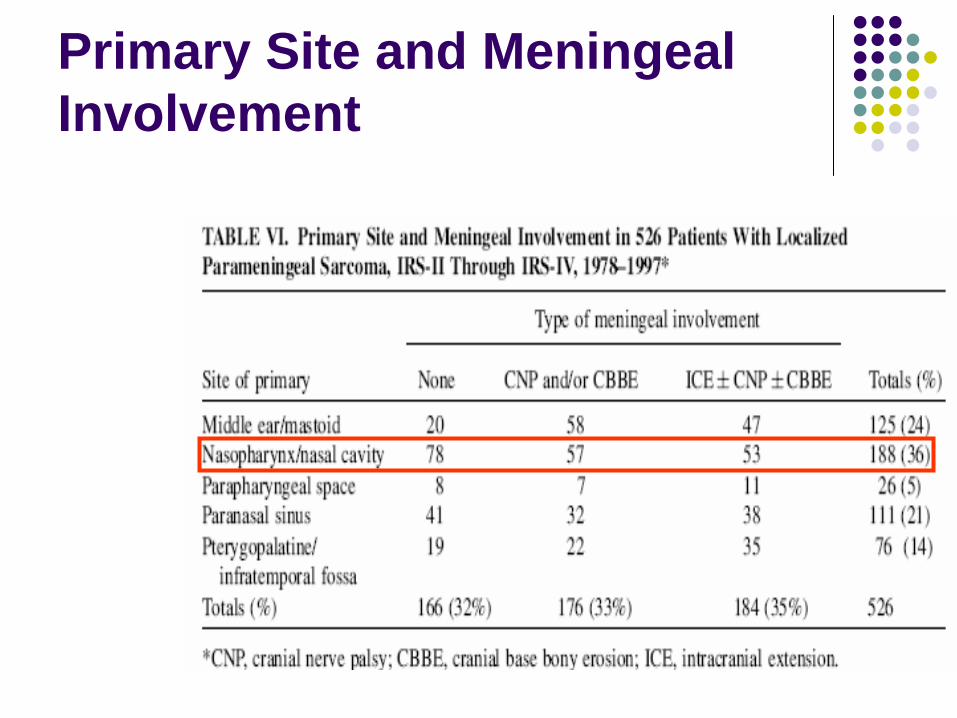
Primary Site and Meningeal Involvement
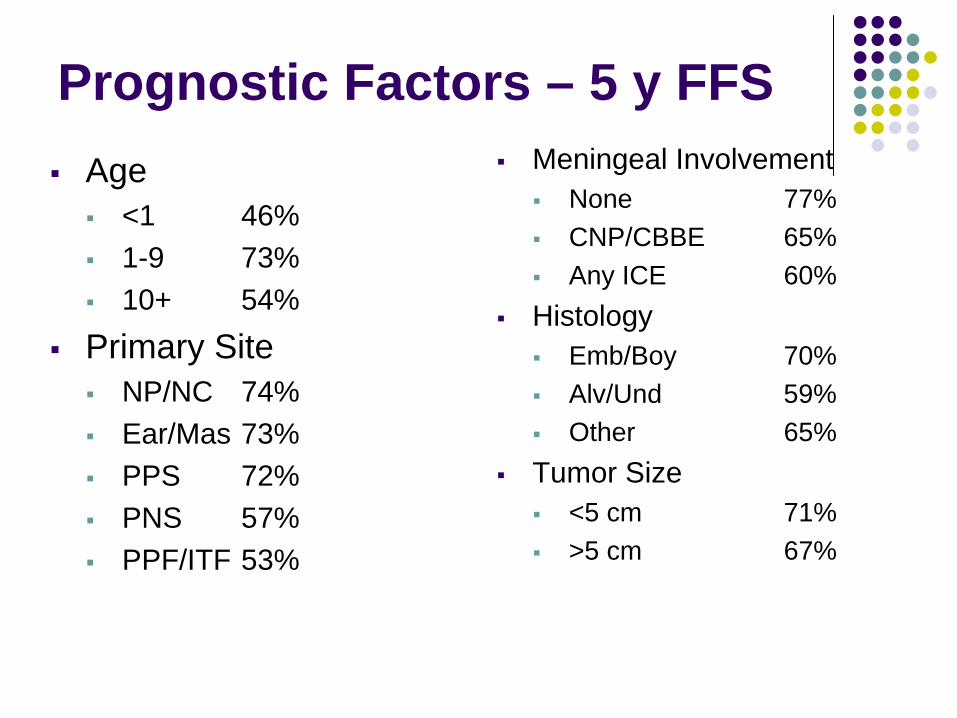
Prognostic Factors – 5 y FFSAge
<1 46%1-9 73%10+ 54%
Primary SiteNP/NC 74%Ear/Mas 73%PPS 72%PNS 57%PPF/ITF 53%
Meningeal InvolvementNone 77%CNP/CBBE 65%Any ICE 60%
HistologyEmb/Boy 70%Alv/Und 59%Other 65%
Tumor Size<5 cm 71%>5 cm 67%
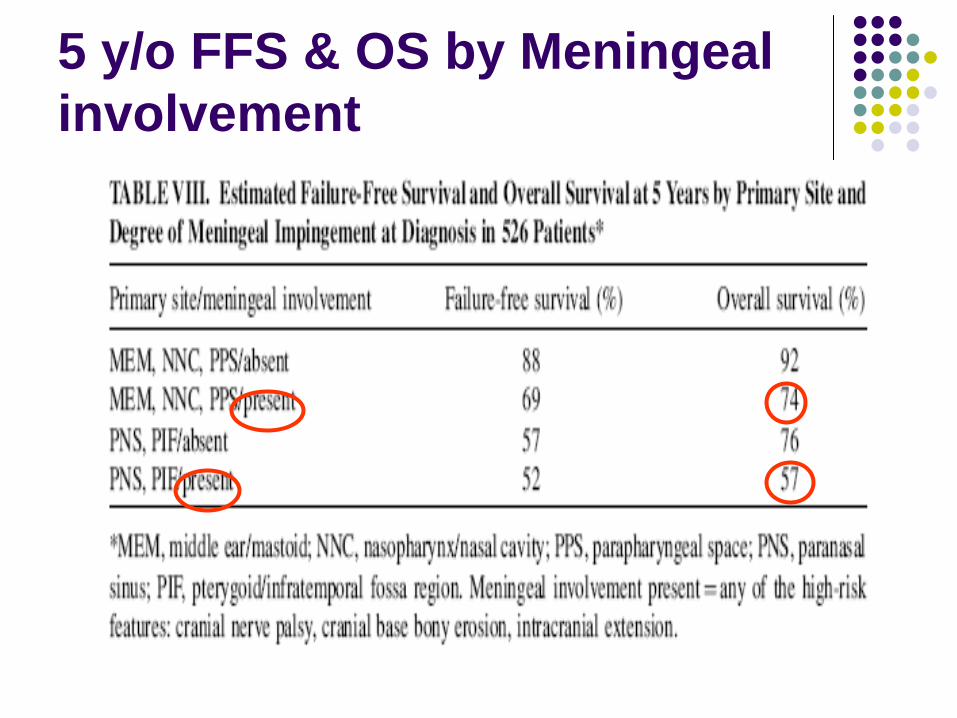
5 y/o FFS & OS by Meningeal involvement
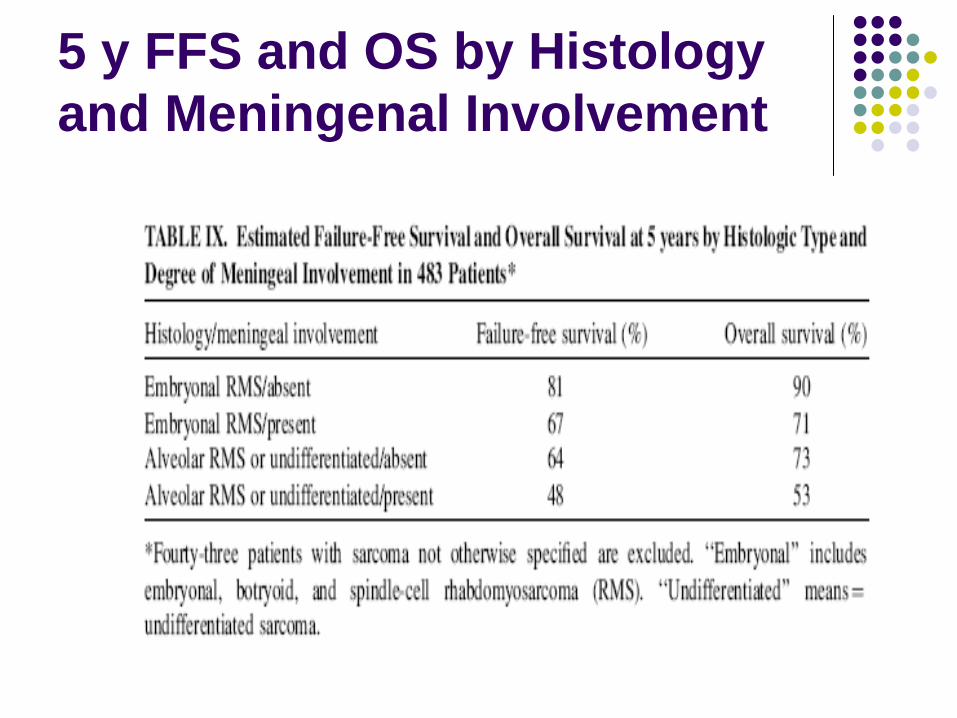
5 y FFS and OS by Histology and Meningenal Involvement
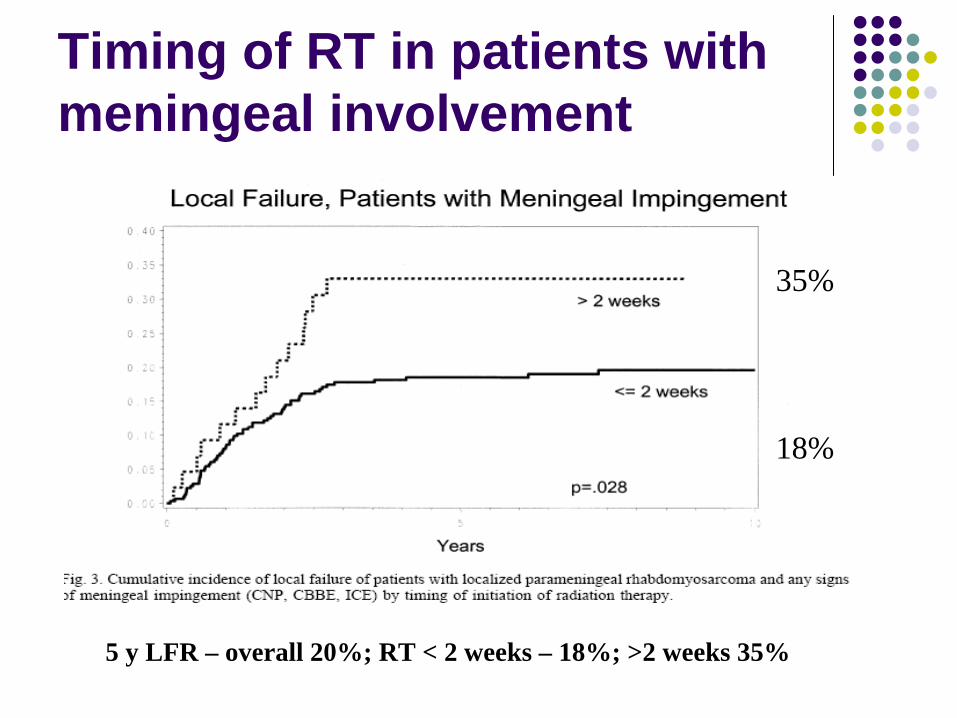
Timing of RT in patients with meningeal involvement
5 y LFR – overall 20%; RT < 2 weeks – 18%; >2 weeks 35%
35%
18%
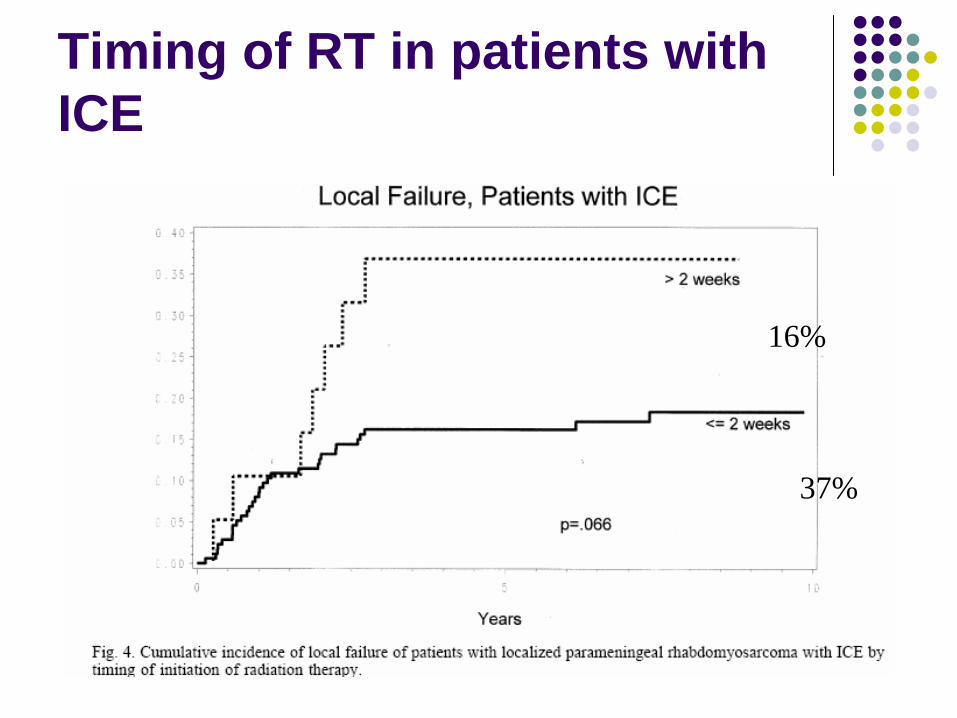
Timing of RT in patients with ICE
16%
37%
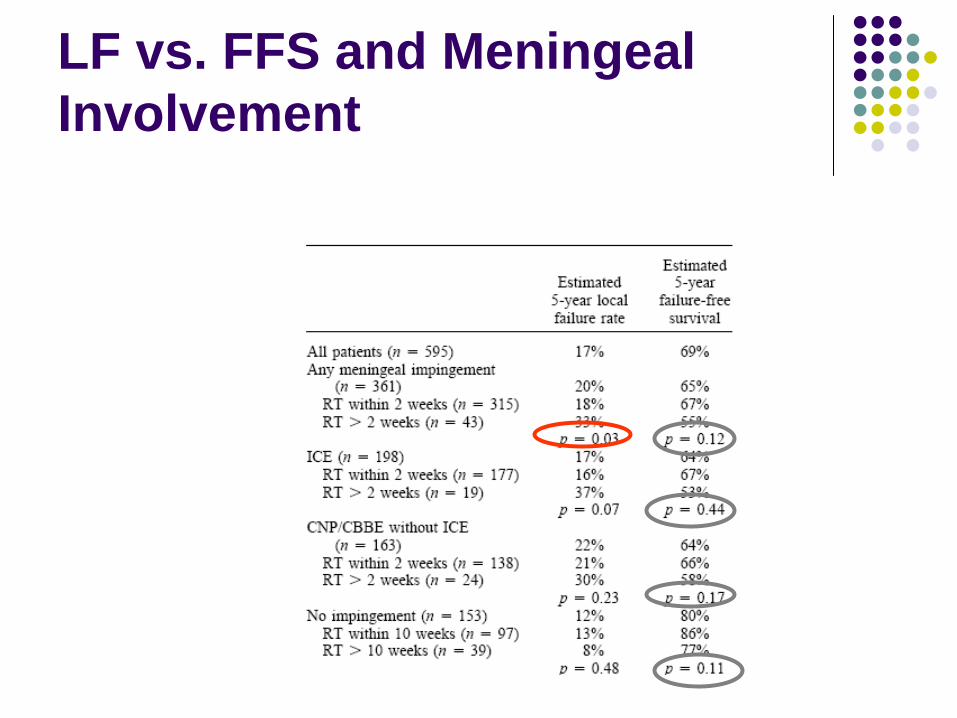
LF vs. FFS and Meningeal Involvement
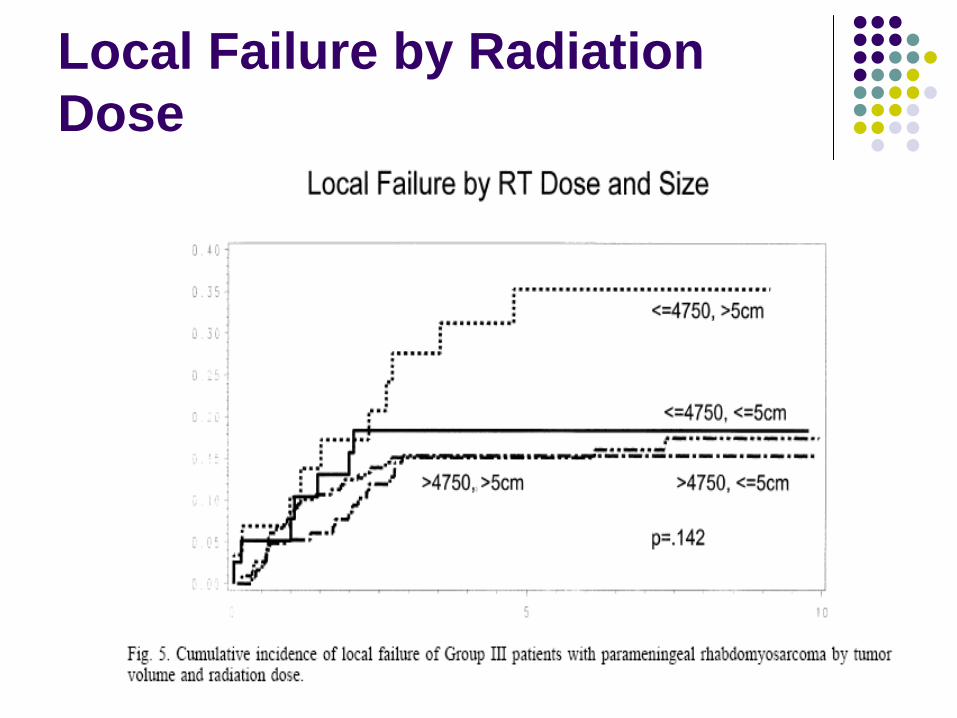
Local Failure by Radiation Dose
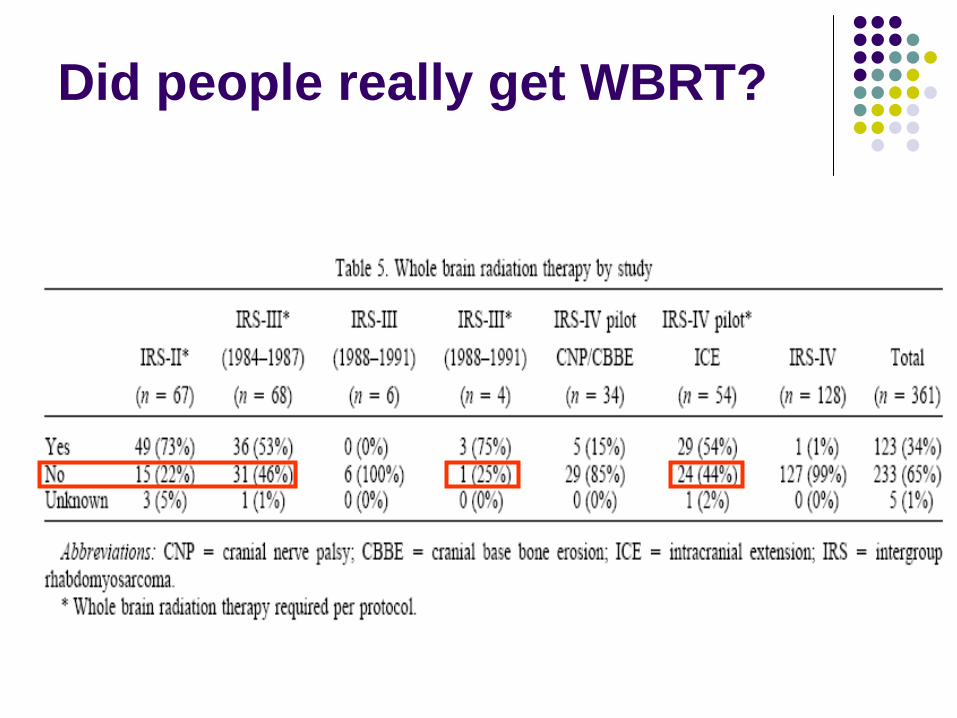
Did people really get WBRT?
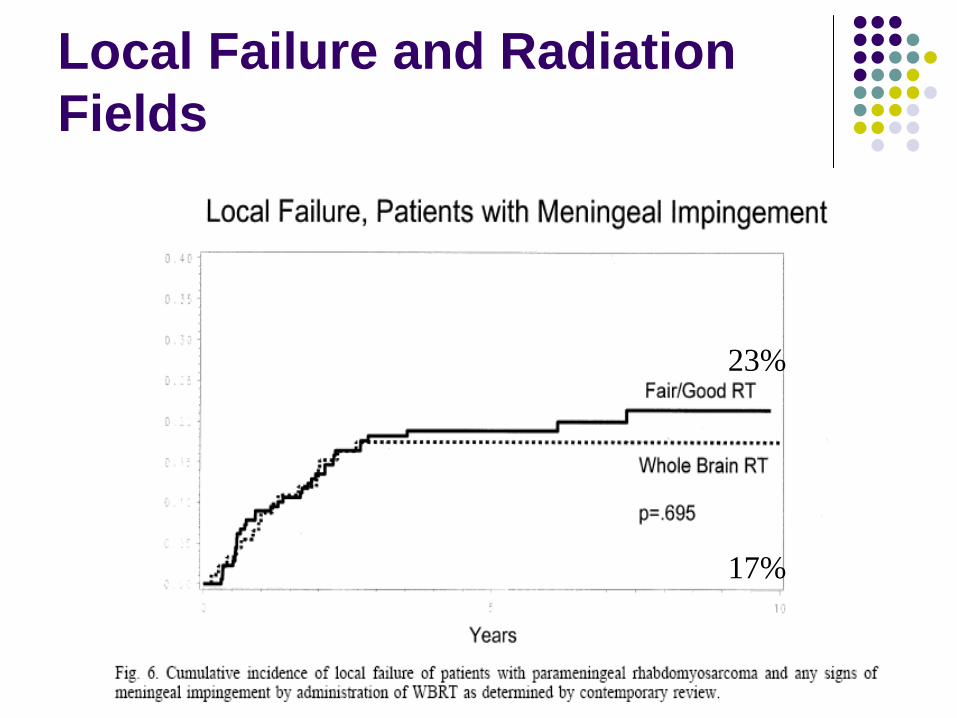
Local Failure and Radiation Fields
23%
17%
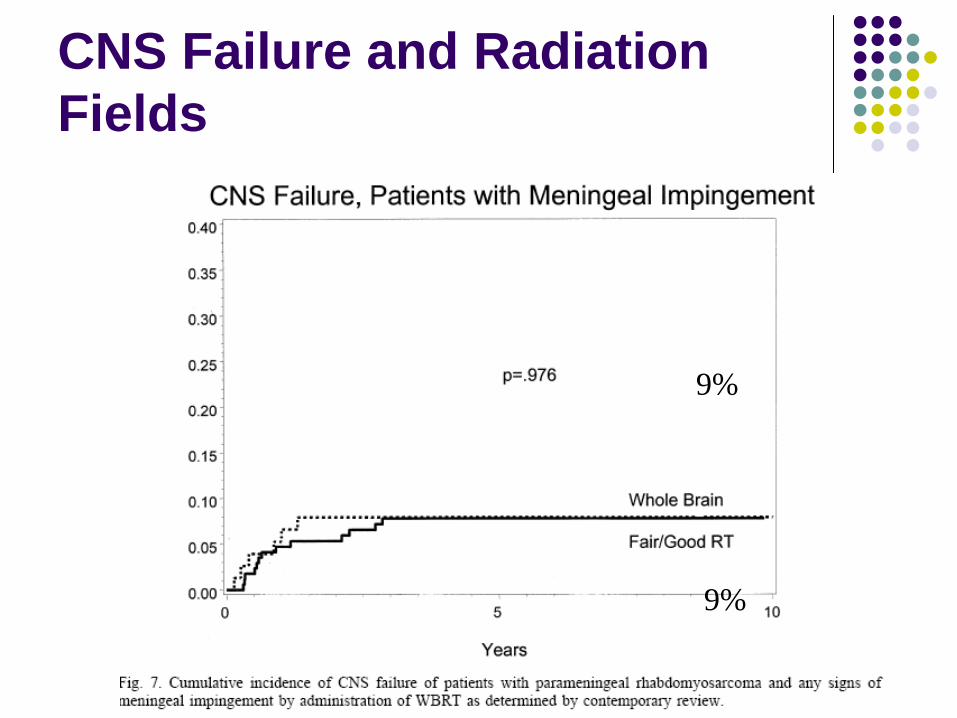
CNS Failure and Radiation Fields
9%
9%
Multivariate analysis
Statistically significant worse prognostic factors controlling for tumor size
Age > 10 (p = 0.002)RT dose <47.5 Gy (p = 0.01)Meningeal Impingement (p =0.001)
Timing of RT was NOT a significant factor
Conclusions
Availability of cross-sectional imaging improved ability to diagnose ICE and hence led to better treatment planning and earlier delivery of RTPatients with tumors > 5 cm benefited from dose > 47.5 GyWBRT not necessary to achieve high control rates; but good planning is!Timing of RT – impacted LF rates but not FFS; not significant on multivariate analysis
Background
IRS II and IRS III showed local relapse rate of 16% and LR relapse rate of 32 % respectively in Group III patientsRCT comparing hyperfractionation vs. conventional fractionation in Group III patientsHyperfractionation = More than 1 fraction a dayGoal to improve LCR by 10% without increasing late side effectsRationale based on 10-15% improvement seen in LRC in other H&N cancers in adults with HF
Criteria / Treatment Logistics
Stage 1, 2, and 3 and Group III patientsCF = 50.4 Gy in 1.8 Gy/fraction given dailyHF = 59.4 GY in 1.1 Gy/fraction given bid atleast 6 hours apartPre-op/Pre-chemo volume + 2 cm marginRT started week 9 or week 0 if cord compression or any meningeal involvement
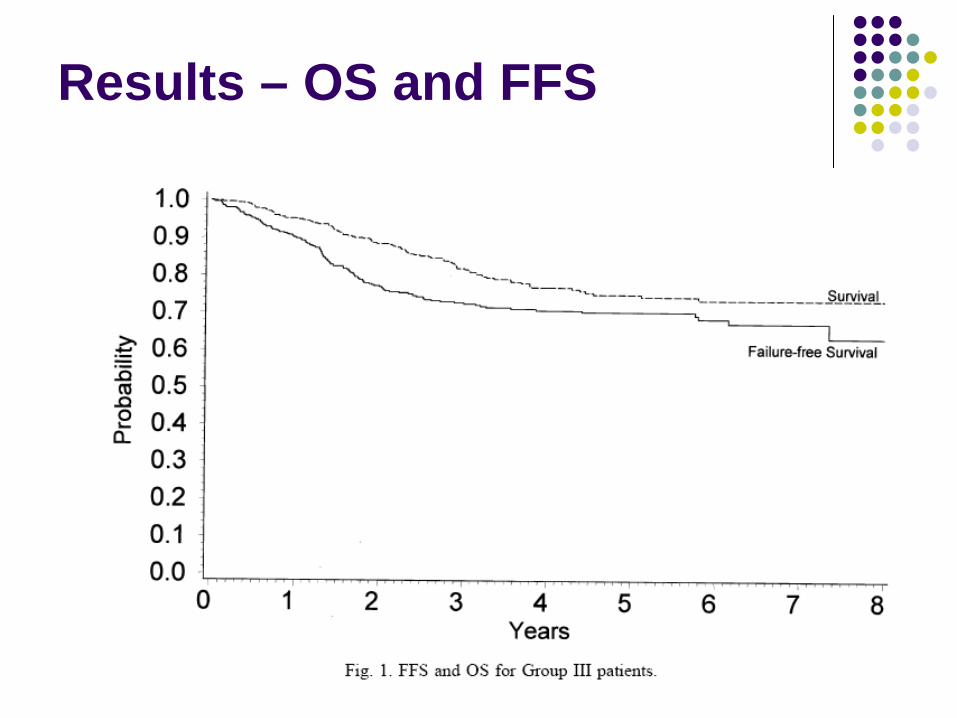
Results – OS and FFS
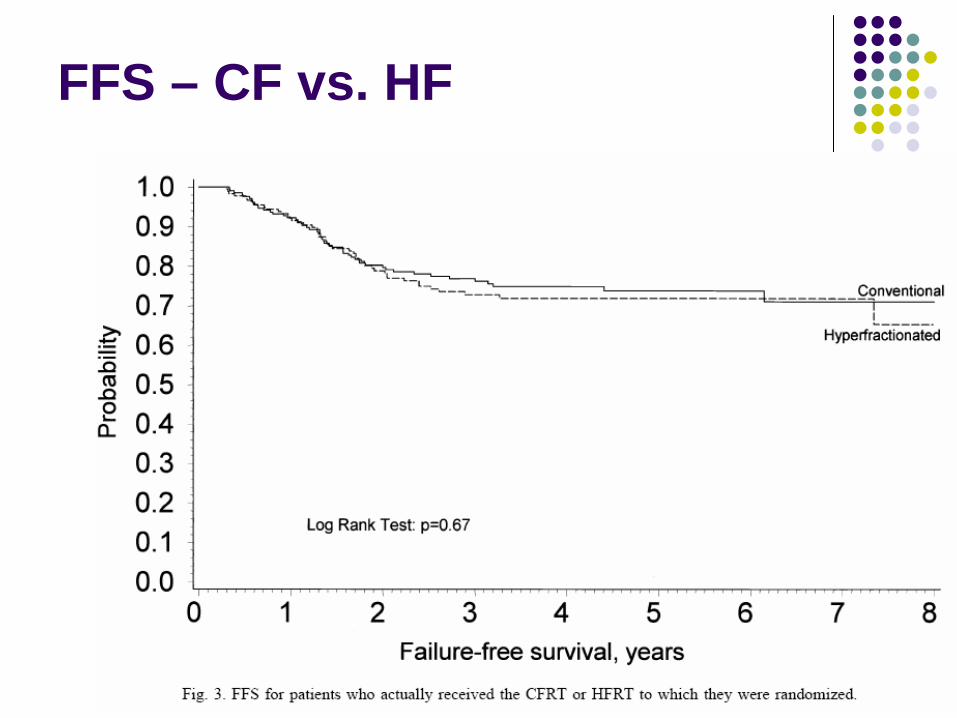
FFS – CF vs. HF
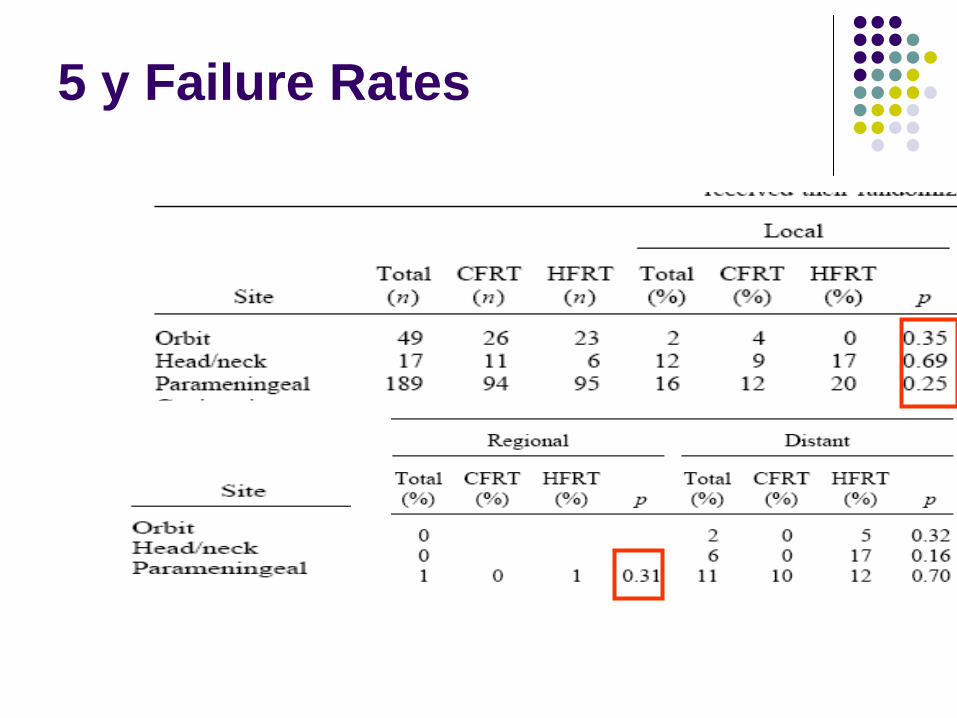
5 y Failure Rates
Conclusion
Hyperfractionation did NOT improve local, regional or distant control over conventional fractionation for Group III tumors
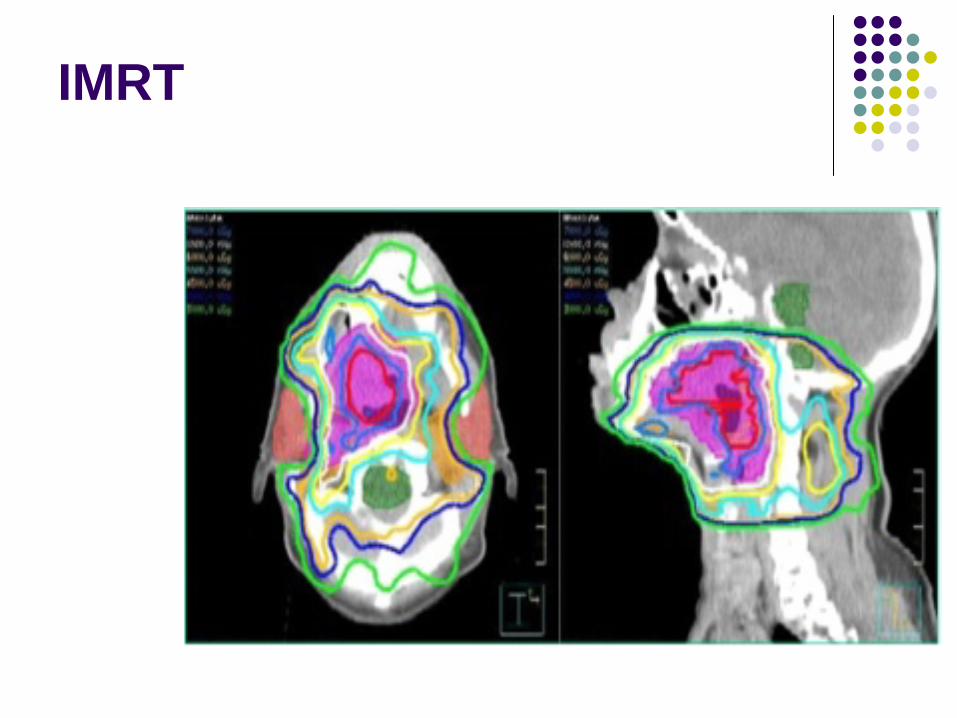
IMRT
IMRT
The next step in radiation treatment planning after 3DInverse planning with computer-assisted optimizationDose painting
Sharp dose fall off outside target volume with selective avoidance of critical structures and tissues
Multiple FieldsDose modulation within each field
Better immobilization, longer treatment time
IMRT
IMRT
Patient Characteristics
28 patients21 parameningeal, 3 orbit, 4 other H&N7% Group II, 89% Group III, 4% Group IV21% Stage I, 21% Stage 2, 54% Stage 3, 4% Stage 457% Embryonal, 32% Alveolar, 11% Undifferentiated
Median RT dose 50.4 Gy (41.4 – 55.8 Gy)Median F/U 2 years
Results
3 y/o LCROrbit 100%Non PM H&N 100%PM 95%
1 patient with Stage IV failedAlveolar/paranasal sinus Local/Regional/Distant mets irradiated
Failed Locally
3 y/o RCROverall 93%Orbit 100%Non PM H&N 100%PM 93%
3 y/o DFSOverall 65%PM 60%Other sites 80%
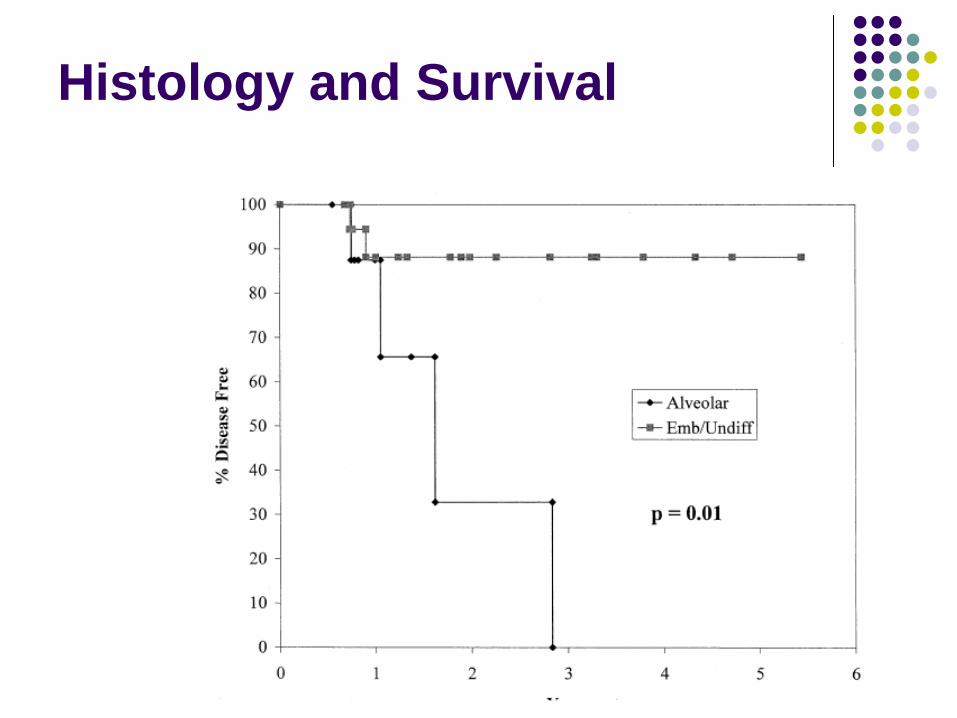
Histology and Survival
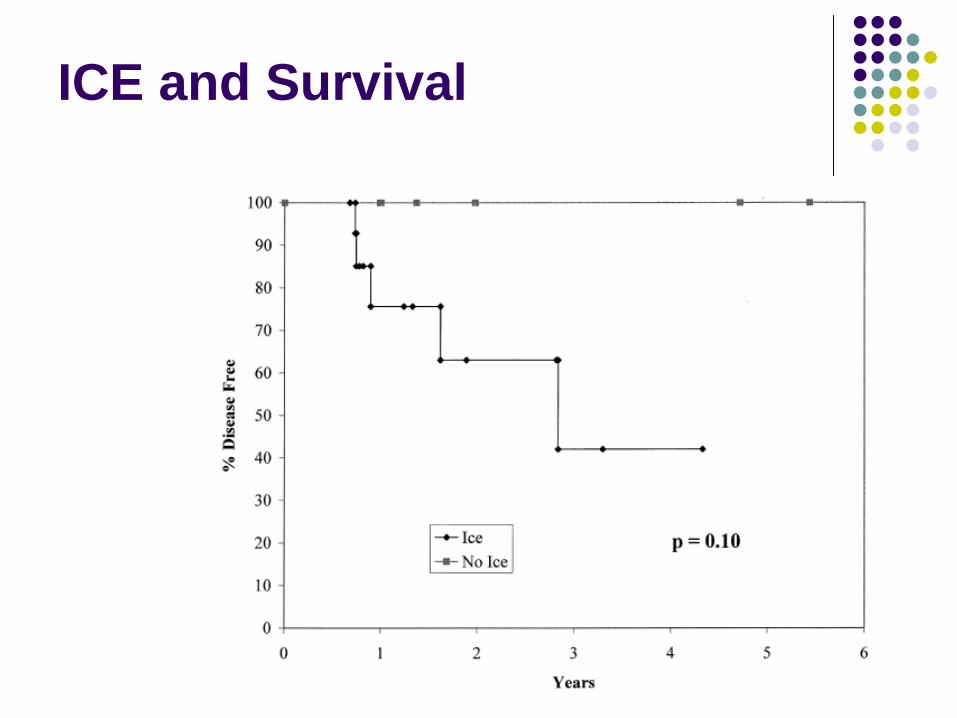
ICE and Survival
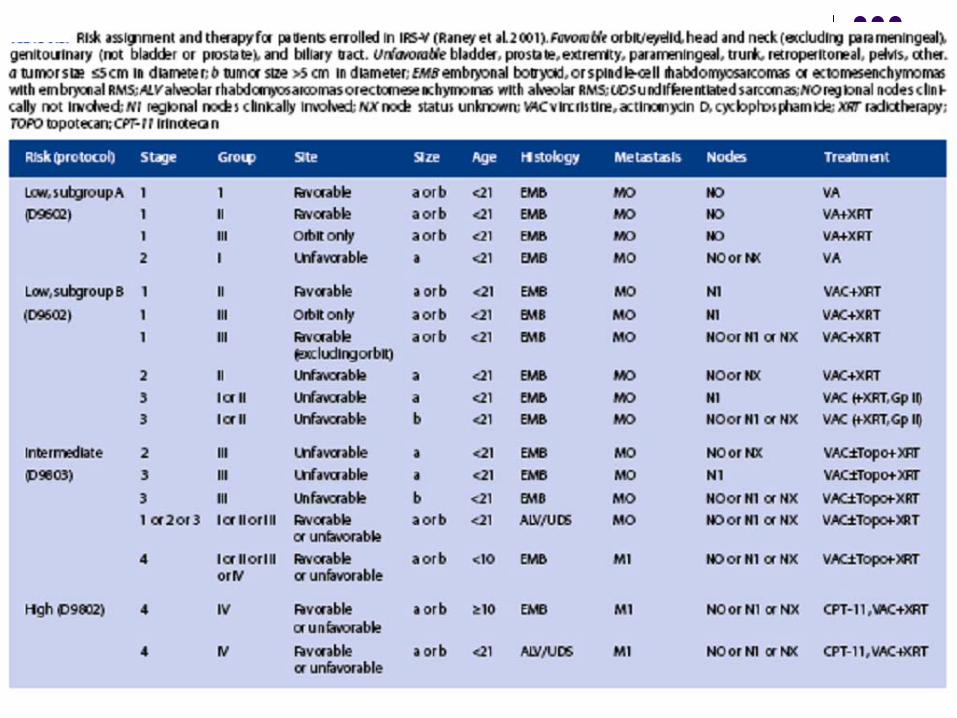
IRS V
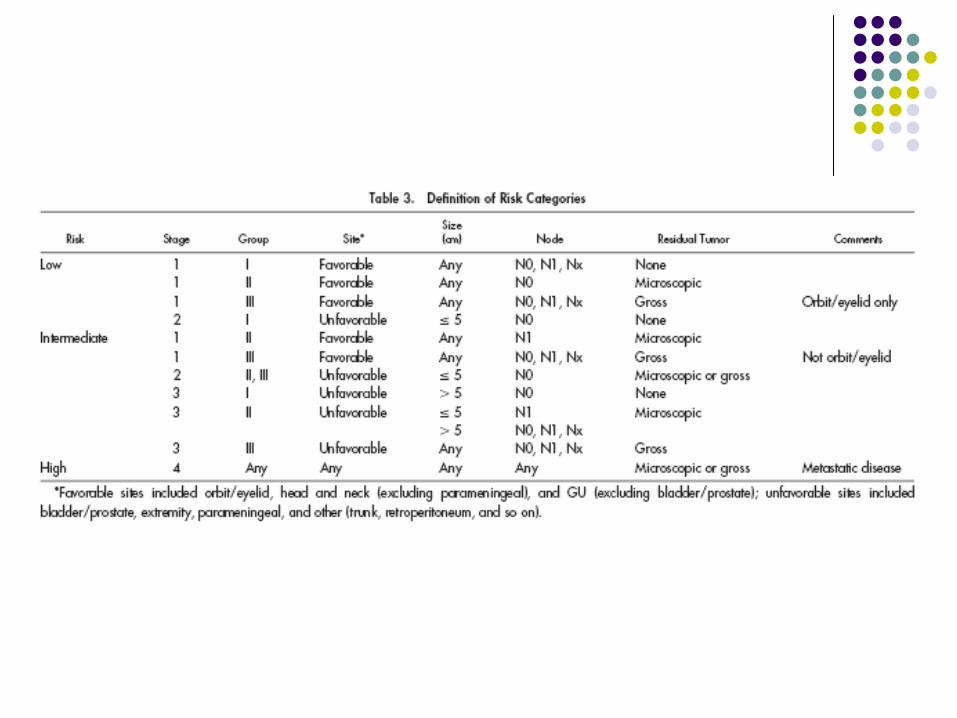
Low Risk
Sub-group AHistology: Embryonal / BoytroidStage 1, Groups I, II(N0)Stage 1, Group III(N0) Orbit onlyStage 2, Group I(N0)
Low Risk
Subgroup BHistology: Embryonal /BoytroidStage 1, Grp II (N1) – microscopic residual dz.Stage 1, Grp III (N1) orbit only – gross residual dz.Stage 1, Grp III (N0 or N1) – gross residual dz.Stage 2, Grp II (N0) – microscopic residual dz, ≤ 5cm primaryStage 3, Grp I or II (N0 or N1) - ≤ 5cm with + LN or > 5cm primary regardless of LN status, - margins or microscopic residual dz.
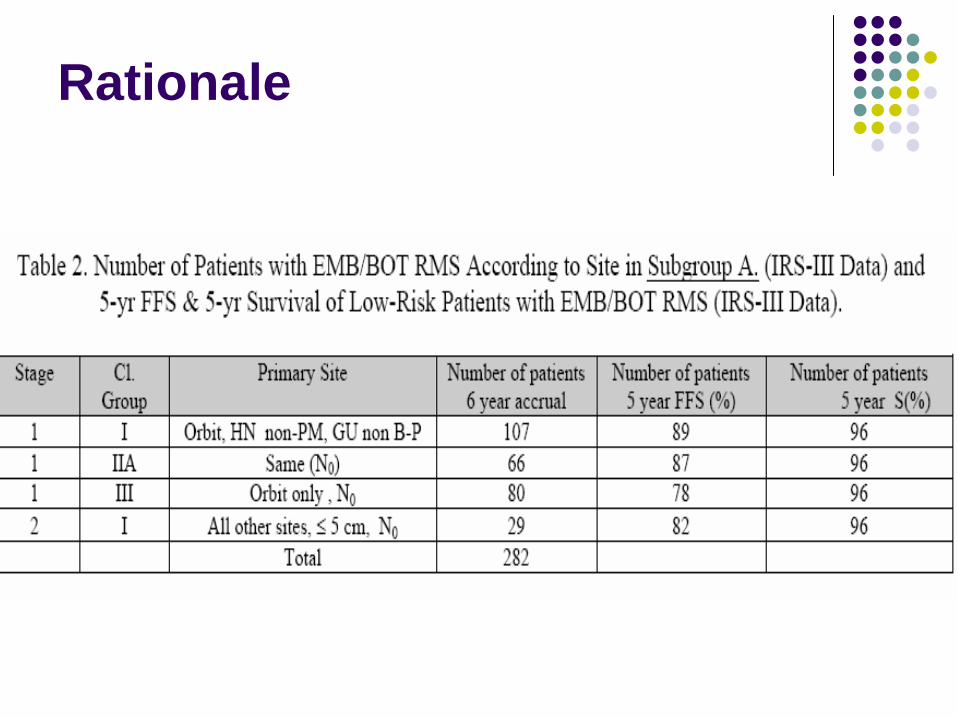
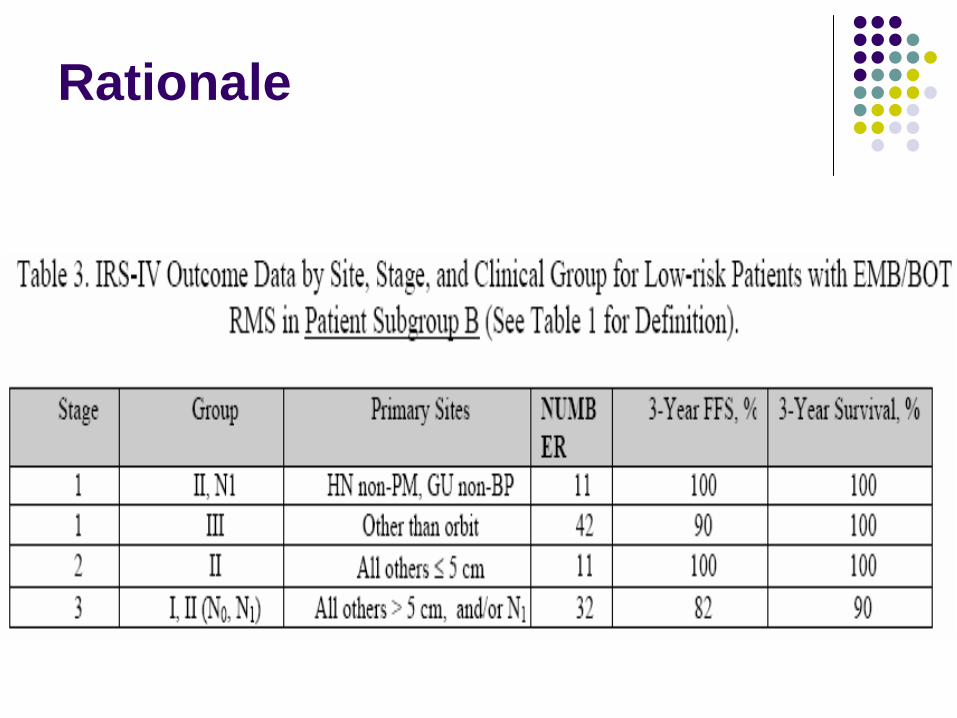
Rationale
5 y OS (IRS – IV) 90-95%5 y FFS 78-89%Primary site, Tumor size and T stage were not prognostic
Rationale
Rationale
IRS V
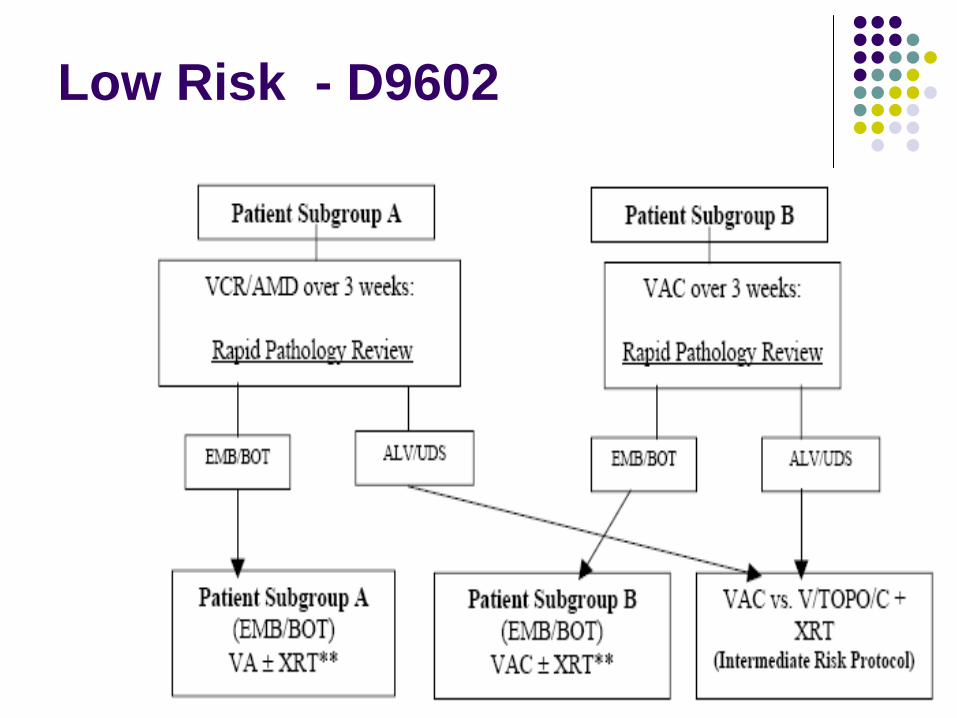
Low Risk - D9602
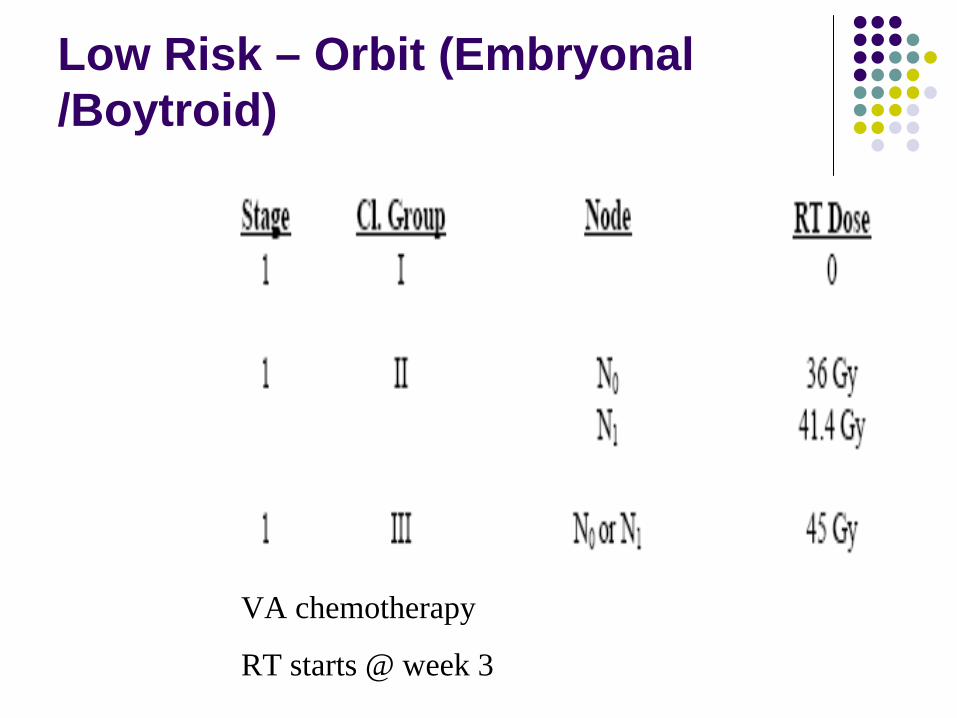
Low Risk – Orbit (Embryonal /Boytroid)
VA chemotherapy
RT starts @ week 3
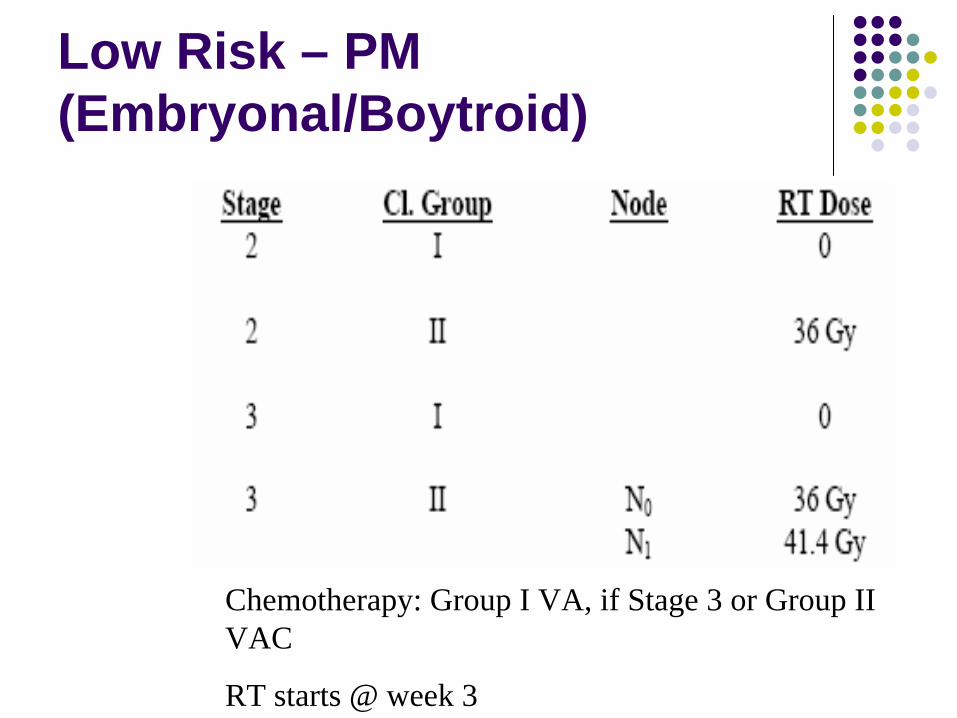
Low Risk – PM (Embryonal/Boytroid)
Chemotherapy: Group I VA, if Stage 3 or Group II VAC
RT starts @ week 3
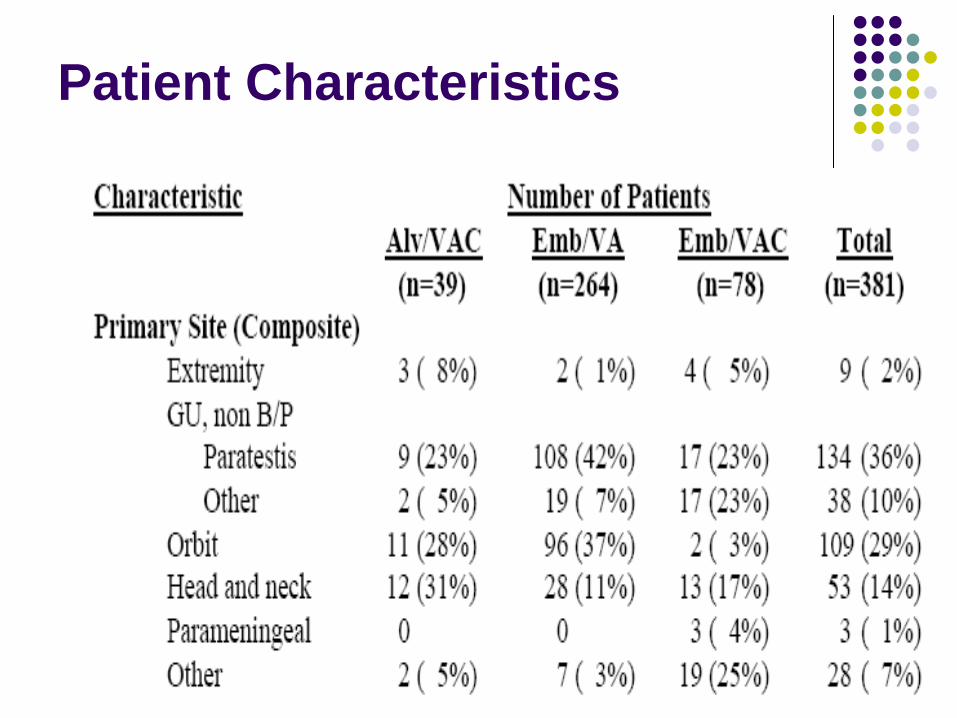
Patient Characteristics
Stage 1, Group IIA
XRT dose reduction from IRS IV41.4 Gy 36 Gy60 pts accruedVA ChemotherapyDecrease in FFS/OS currently attributed to less chemotherapy when compared to IRS IV
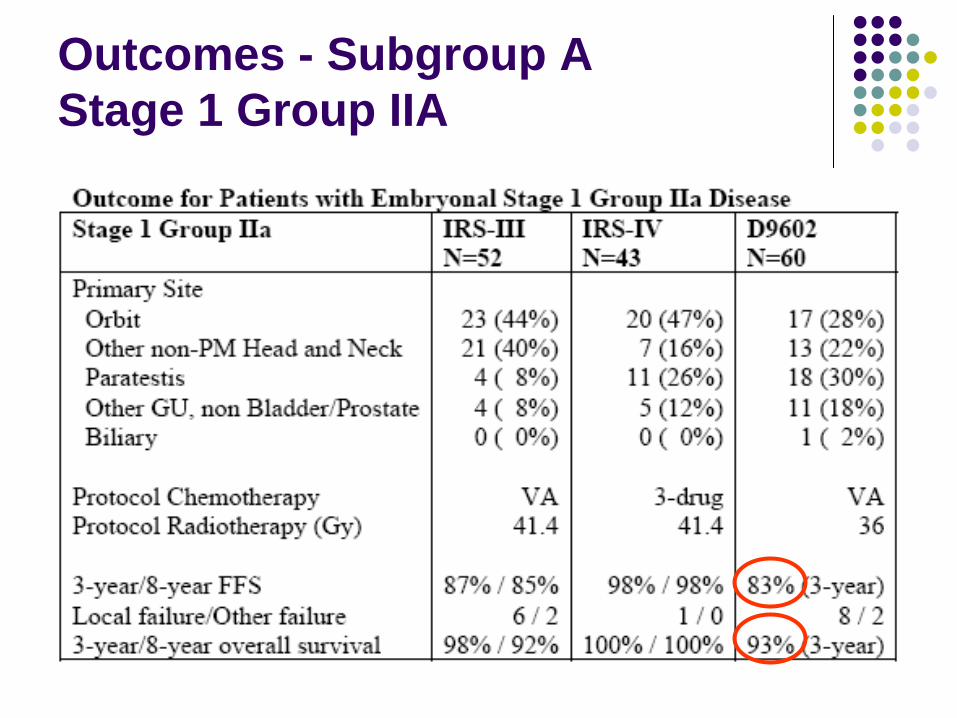
Outcomes - Subgroup A Stage 1 Group IIA
Subgroup A – Stage 1 Group III Orbit
77 patients assigned to VA therapy and reduced RT doseXRT dose reduced from 50.4 /59.4 from IRS IV to 45 Gy10 relapses (all had a local failure component); 3 deathsFFS and OS @ 3 years – 88% and 97%The decrease in FFS/OS in IRS V compared to IRS IV partly attributed to less chemotherapyIt is similar to results from IRS III with VA chemotherapy
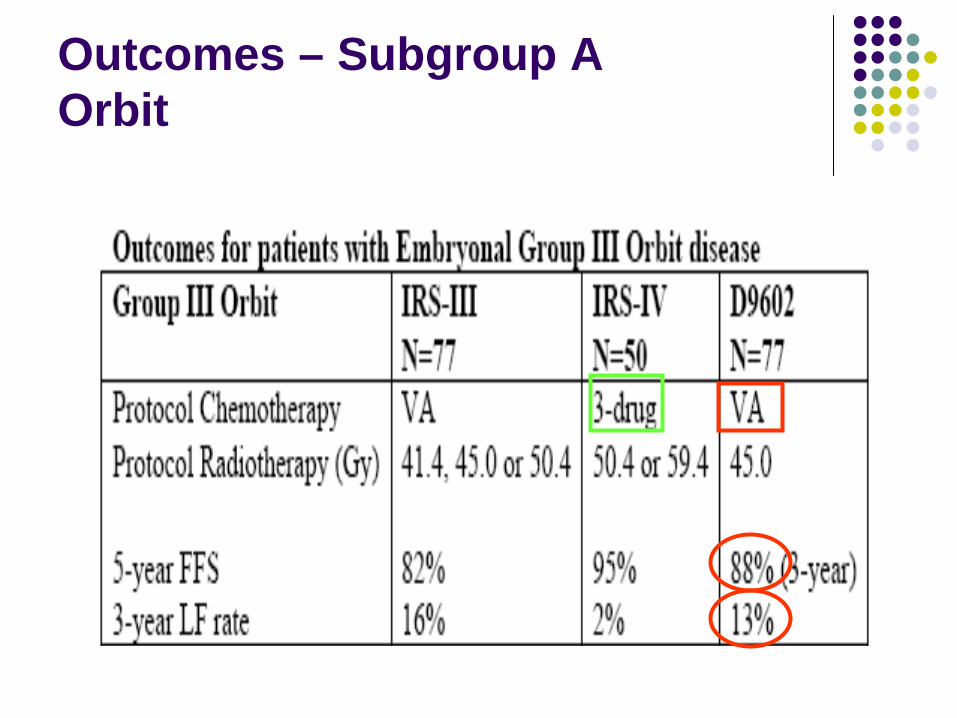
Outcomes – Subgroup A Orbit
Subgroup B – Stage 2/3 Group IIA (N0)
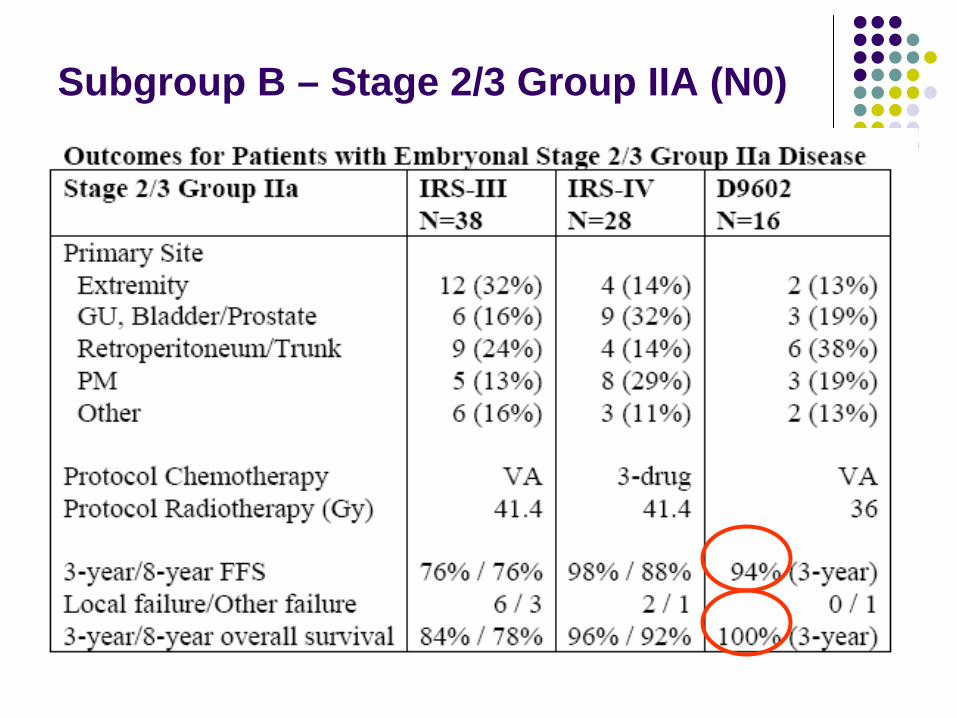
16 patients accrued; treated with VAC chemotherapy and reduced dose RTRT dose reduced from 41.4 Gy 36 GyNo impact on FFS with reduced dose RT
Subgroup B – Stage 2/3 Group IIA (N0)
Intermediate Risk – D9803
Chemotherapy
Randomizes patients to VAC vs. VTCT – Topotecan
Topoisomerase I inhibitorS – phase specific

Orbit – Alveolar/Undiff
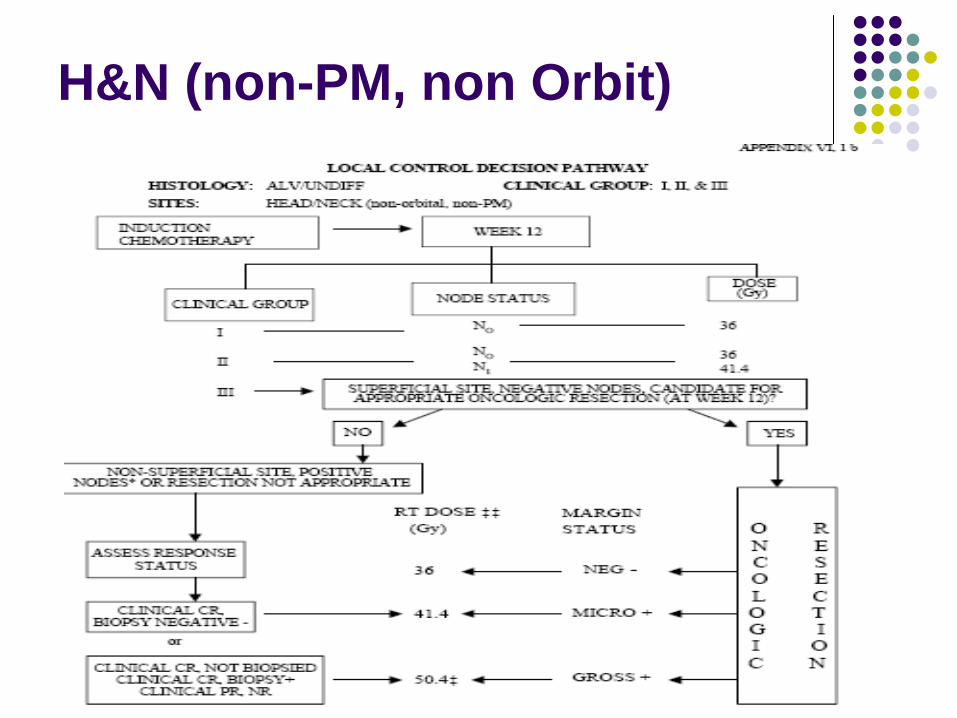
H&N (non-PM, non Orbit)
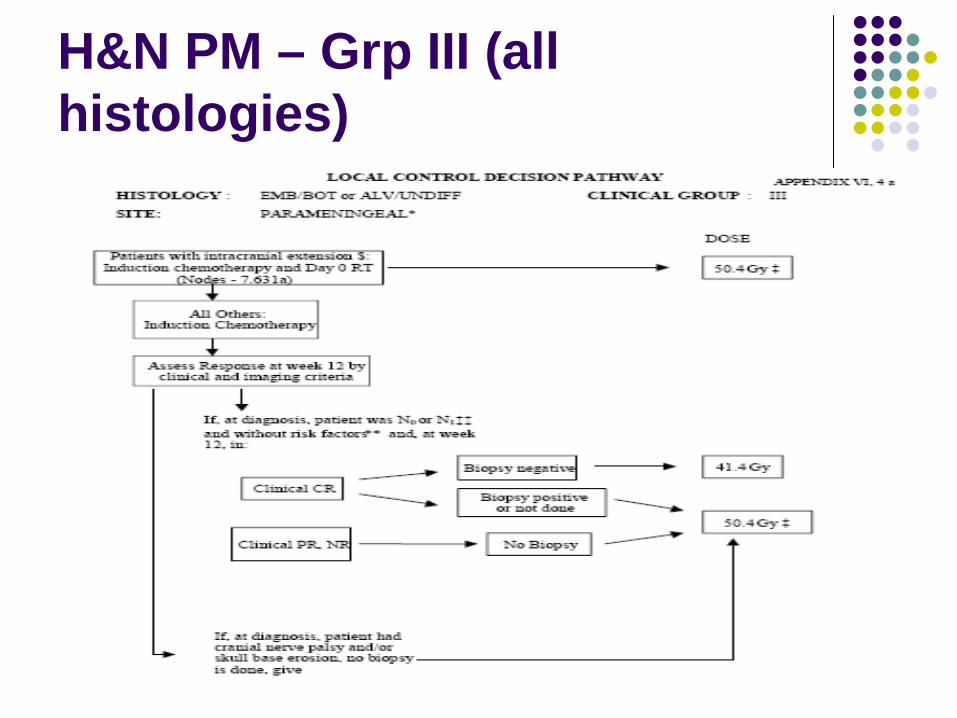
H&N PM – Grp III (all histologies)
High Risk – D9802
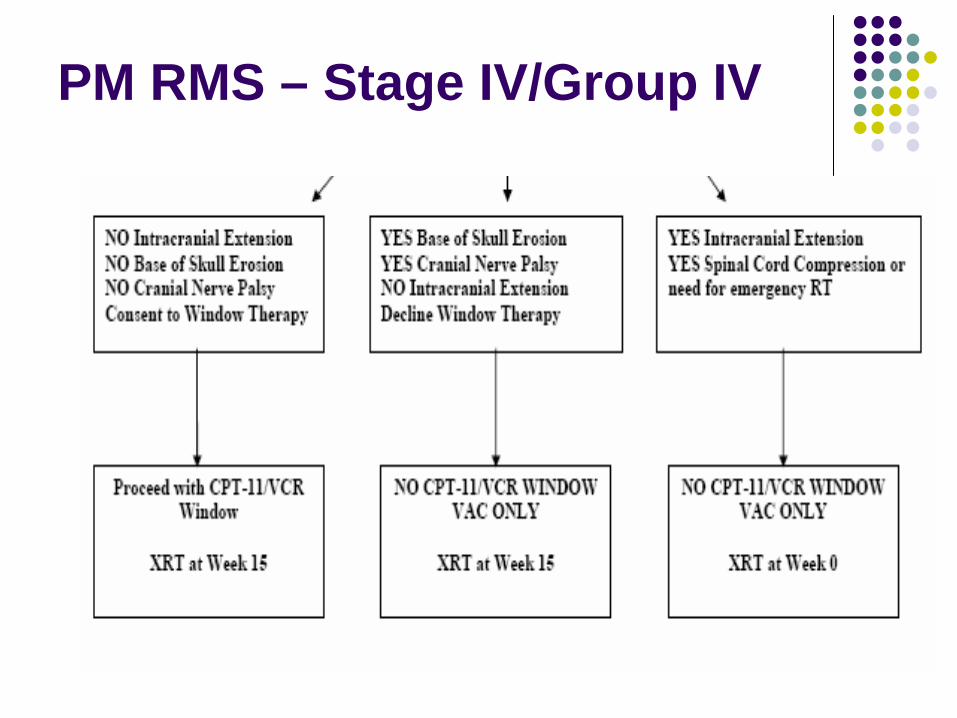
PM RMS – Stage IV/Group IV
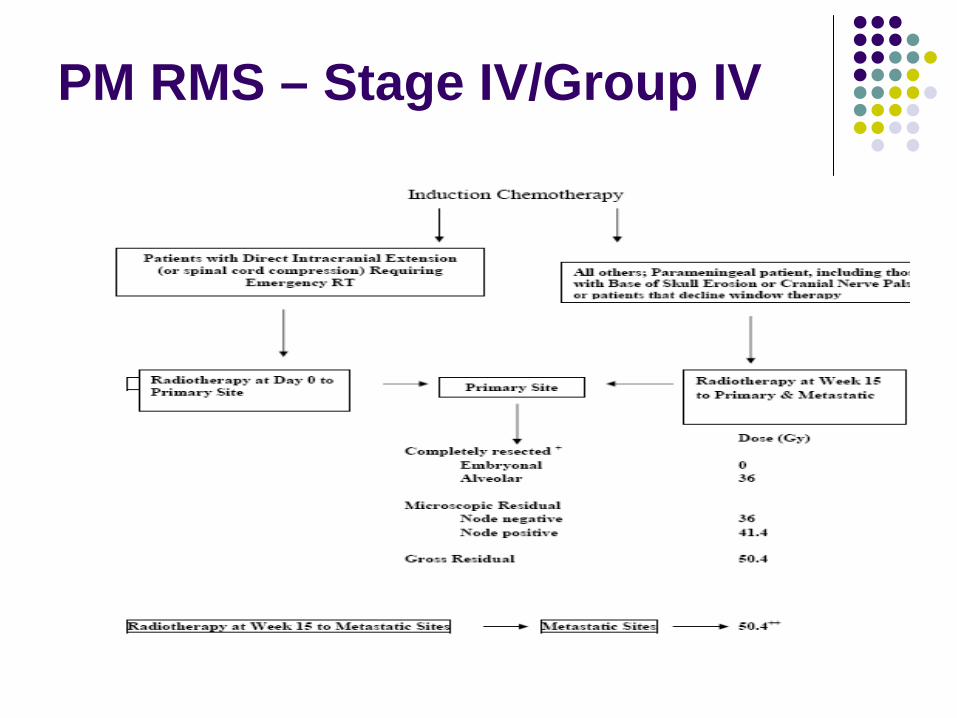
PM RMS – Stage IV/Group IV





























