Embed Size (px)
Citation preview

Revista de Gastroenterología de México. 2013;78(4):255---260
REVISTA DEGASTROENTEROLOGIA
DE MEXICO´
´
www.elsevier.es/rgmx
SCIENTIFIC LETTERS
Idiopathic sclerosing mesenteritis in thepediatric patient: A case report�
mild duodenitis, and nodular colitis. Biopsies demonstratedmicro-abscesses at the distal duodenal level and special
strsowtfiacitd«
wbpw
nicttw
atc
mtti
Mesenteritis esclerosante idiopática en la edadpediátrica: presentación de un caso clínico
Sclerosing mesenteritis makes up part of a spectrum of rareidiopathic conditions characterized by chronic inflamma-tion of the mesentery and fibrosis.1 It was first describedin 1924.2 Clinical presentation varies from an asymptomaticabdominal mass to acute systemic syndromes manifested asfever, weight loss, general malaise, bowel obstruction, orintestinal ischemia.
Tomography is a sensitive diagnostic tool, but surgicalbiopsy is usually necessary for making the diagnosis andruling out other pathologies. Few patients require surgi-cal treatment, which is generally directed at secondarycomplications such as bowel obstruction. The epidemiol-ogy of sclerosing mesenteritis is unknown. A prevalence of0.6% has been described from more than 7,000 abdominalcomputed axial tomography scans.3 The disease is regardedas rare in the pediatric age and only 17 cases have beenreported up to the present date.4 Even though there arereports on children under 3 years of age, the majority ofpatients are in the fifth to seventh decades of life.1
We present the case herein of a 25-month-old male childwith a 15-day progression of symptoms that began withabdominal bloating, soft stools, and pain, for which he washospitalized in order to be tested. An abdominal comput-erized tomography scan was taken (Fig. 1) that showedimportant ascites. Paracentesis with fluid analysis was doneto look for tuberculosis, but only one positive criterion wasfound: tuberculin 10 mm (the rest were negative), for whichlatent tuberculosis was diagnosed.
Given that there were no other paraclinical findings toexplain the ascitic process, the patient underwent surgerythat revealed abundant clear peritoneal fluid, marked dis-tension of the intestinal segments, and whitish patches on
the peritoneum from diaphragmatic recesses. Upper gas-trointestinal endoscopy and total video colonoscopy wereperformed that showed grade III esophagitis, antral gastritis,� Please cite this article as: Parra-Buitrago A, Valencia-Zuluaga N,Rivera-Echeverry J, Contreras-Ramírez M, Vélez-Hoyos A. Mesen-teritis esclerosante idiopática en la edad pediátrica: presentaciónde un caso clínico. 2013;78:255---257.
ihrsivtpTt
2255-534X/$ – see front matter © 2014 Asociación Mexicana de Gastroente
tains were negative.Two weeks after surgery and with no clear diagnosis,
he patient’s symptoms of abdominal bloating and painecurred. A control abdominal ultrasound was done thathowed evidence again of free fluid in the cavity. A sec-nd surgery was decided upon and diagnostic laparoscopyas performed in which samples of the entire thickness of
he intestine were taken; this had not been possible in therst surgery because the distension of the segments had notllowed for adequate visualization. Surgery revealed criti-al stricture of the ileum with severe hardening in almostts entirety. Samples were taken for histopathology andhe macroscopic results were: the serous membrane of theistal ileum presented with thickened fibrous areas like abreastplate», compressing it.
Microscopically: the mucosa, submucosa, and muscleere normal; the serous membrane had a thickened fibrousand that entirely covered the distal ileum resulting in com-lete stricture and compression. Diagnosis in the distal ileumas idiopathic sclerosing mesenteritis (Figs. 2 and 3).
Systemic steroid therapy was begun, along with iso-iazid for 9 months for treating the latent tuberculosisnfection. Due to the severity of the clinical symptoms,yclophosphamide was added. Once treatment was started,he patient progressed adequately, he tolerated oral intake,here were no febrile peaks, and the ascites and distensionere resolved.
Given the atypical nature of the clinical symptomsnd the immediate improvement, it was decided to con-inue the steroids for 6 complete weeks, without prolongingyclophosphamide administration.
It has been suggested in the literature that sclerosingesenteritis is a rare entity in children and adolescents due
o the lower quantity of mesenteric fat,5 and even thoughhe precise etiology is still unexplained, mechanisms includ-ng previous abdominal trauma or surgery, autoimmunity,nfection, and ischemia have been proposed.6 A reasonableypothesis is that this subgroup of patients has abnormalesponses in the cicatrization and repair of connective tis-ue. This inflammatory and fibrotic process can affect thentegrity of the gastrointestinal lumen and the mesentericessels through a mass effect, causing a variety of gastroin-
estinal and systemic manifestations that include abdominalain, nausea and vomiting, diarrhea, weight loss, and fever.herefore a high degree of suspicion is necessary for makinghe diagnosis.2rología. Published by Masson Doyma México S.A. All rights reserved.

256 SCIENTIFIC LETTERS
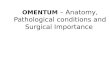
Figure 1 Abdominal tomography scan: A great quantity of ascites of undetermined cause; the liver, pancreas, and kidneys have anormal aspect and size; there is no primary tumor or metastasis and ncaliber and there are no lesions in the digestive tract.
Fml
pbg
Fdc
Ca
al
igi
iaaoptcse
igure 2 Histopathology, hematoxylin and eosin stain: serousembrane of the intestine with a fibrous band obliterating the
umen.
Diagnosis is established through histologic evaluation;lain x-ray is non-specific. Ultrasound imaging can aid inetter visualizing the mesenteric fat. Computerized tomo-raphy scan is the most sensitive image for detection.
igure 3 Histopathology, immunohistochemistry: a more evi-ent fibrous band is observed that is strictured and completelyompresses the lumen of the distal ileum.
F
N
C
T
R
o adenomegaly or masses. The vascular structures have normal
alcifications are present in approximately 20% of the lesionss a result of fat necrosis or vascular obstruction.7,8
Pathologic confirmation should be obtained in all cases,s was the case with our patient. It was the basis for estab-ishing the definitive diagnosis.
There is no standard therapy and treatment should bendividualized. In the large majority of cases, complete sur-ical resection is impossible due to the associated vascularnvolvement and disease extension.
A number of pharmaceutical agents have been usedn an attempt to stabilize the disease. Glucocorticoids,zathioprine, methotrexate, colchicine, cyclophosphamide,nd/or radiotherapy have been proposed as therapeuticptions.1,9,10 The patients with a greater inflammatory com-onent, with fever, weight loss, and general malaise appearo be the most receptive to glucocorticoids, alone or inombination. In the case of our patient, the use of theteroid and cyclophosphamide had favorable results in dis-ase improvement and modulation.
inancial disclosure
o financial support was received in relation to this article.
onflict of interest
he authors declare that there is no conflict of interest.
eferences
1. Akram S, Pardi DS, Schaffner JA, et al. Sclerosing mesenteri-tis: clinical features, treatment, and outcome in ninety-twopatients. Clin Gastroenterol Hepatol. 2007;5:589---96.
2. Vettoretto N, Doenico-Roberto D, Poiatti R, et al. Occasionalfinding of mesenteric lipodystrophy during laparoscopy: A diffi-cult diagnosis. World J Gastroenterol. 2007;13:5394---6.
3. Daskalogiannaki M, Voloudaki A, Prassopoulos P, et al. CT eval-uation of mesenteric panniculitis: Prevalence and associated
diseases. AJR Am J Roentgenol. 2000;174:427---31.4. Viswanathan V, Murray KJ. Idiopathic sclerosing mesenteritis inpaediatrics: Report of a successfully treated case and a reviewof literature. Pediatr Rheumatology. 2010;8:5.

257
5. Adams JT. Abdominal wall, omentum, mesentry, and retroperi-toneum. In: Schwartz S, Shires F, Spencer F, editors. Principlesof Surgery. 6 th ed. New York: McGraw Hill; 1994. p. 1485.
6. Tedeschi CG, Botta GC. Retractile mesenteritis. N Engl J Med.1962;266:1035---40.
7. Horton KM, Lawler LP, Fishman EK. CT findings in sclerosingmesenteritis (panniculitis): Spectrum of disease. Radiographics.2003;23:1561---7.
8. Roson N, Garriga V, Cuadrado M, et al. Sonographic findingsof mesenteric panniculitis: Correlation with CT and literaturereview. S J Clin Ultrasound. 2006;34:169---76.
9. Bala A, Coderre SP, Johnson DR, et al. Treatment of scleros-ing mesenteritis with corticosteroids and azathioprine. Can JGastroenterol. 2001;15:533---5.
10. Munoz-Juárez M, Luque-de León E, Moreno-Paquentin E, et al.Sclerosing mesenteritis: A disease of malignant appearance. RevGastroenterol Mex. 1998;63:224---30.
A. Parra-Buitragoa,∗, N.A. Valencia-Zuluagaa,J.A. Rivera-Echeverryb, M. Contreras-Ramírezb,A. Vélez-Hoyosc
a Residentes de Pediatría, Universidad PontificiaBolivariana, Medellín, Colombiab Servicio de Gastroenterología y Endoscopia,Hospital Pablo Tobón Uribe, Medellín, Colombiac Servicio de Patología, Hospital Pablo Tobón Uribe,Medellín, Colombia
∗ Corresponding author: Carrera 79 N.◦ 35-43 Medellín.Código Postal: 050034. Phone: (574) 4114745 --- 4168537.E-mail address: [email protected](A. Parra-Buitrago).
Capsule endoscope aspiration: A commoncomplication?�
Aspiración de cápsula endoscópica:¿complicación frecuente?
Obscure gastrointestinal bleeding (OGIB) is defined as occultbleeding or it manifests as bleeding of unknown origin afternegative endoscopy and colonoscopy. OGIB can present asoccult bleeding characterized by anemia, iron deficiencyand/or fecal occult blood, or it can manifest as hema-tochezia or melena, with no evidence of the bleeding sitethrough conventional studies. Approximately 5% of gastroin-testinal bleeding occurs between the Treitz ligament andthe ileocecal valve.1 Diagnosis and treatment of patientswith OGIB are often long and difficult processes.2 Cap-sule endoscopy (CE) has been shown to be a cornerstonein evaluating the patient with OGIB. The benefits of CEinclude the fact that it is a painless, invasive method thatis widely accepted by the patient for studying the smallbowel (SB).1 All the patient has to do is swallow the capsuleendoscope. Despite its being a minimally invasive method,several complications must be taken into account, such asretention of the capsule endoscope (0.7%), impaction inthe cricopharyngeus or diverticula, and aspiration into therespiratory tract.3---8 Only a few cases of capsule endoscopeaspiration have been reported worldwide 6---8 and none inMexico. Therefore, we believe it is of interest to report thepresent case, so that the physicians carrying out this typeof study are aware of this possible complication.
A 78-year-old man had no past history of chronic degener-ative diseases and no complaints of dysphagia or swallowingdisorders. He was hospitalized 3 years prior due to uppergastrointestinal bleeding from a gastric ulcer secondary to
with postprandial fullness, a weight loss of 14 kg during thatyear, and fecal occult blood on 2 occasions. Panendoscopyrevealed a hiatal hernia and chronic gastropathy of the bodyand antrum. Colonoscopy showed uncomplicated diverticu-lar disease of the descending colon and the sigmoid colon.The patient was referred for CE as part of the approach toOGIB. A bowel transit time test was done on the patientbefore he was given the capsule endoscope to swallow, andit was normal. There were no complications in relation tothe preparation for CE.
The patient was programmed for the CE study with themodified PillCam COLON 1 technique for studying the SB.The patient had some difficulty in swallowing the capsuleendoscope, but he was able to do so. Immediately afterswallowing it he had the sensation of a foreign body in histhroat and a coughing spell of 2 min. He did not complainof dyspnea or any other symptom and physical examinationshowed no cyanosis. He drank water again and had the sensa-tion of having swallowed the capsule. However, one minutelater his cough was exacerbated and he expelled the capsuleinto his mouth. He was given water, he swallowed the cap-sule with no incident, and the study was completed with noapparent complication. The images were downloaded andwhen the study was examined, it was seen that the capsulehad been aspirated, taking photograms of the respiratorytract (figs. 1 and 2); the capsule was then expelled into themouth and swallowed again, evaluating the usual trajectoryin its entirety. The capsule was passed 8 hours later and thecause of the bleeding was identified.
CE has currently become the method of choice for study-ing the patient with OGIB. It has been approved in the UnitedStates by the Food and Drug Administration for the study ofthese patients, and it is also indicated in the study of Crohn’sdisease and polyps, among others.9
The present case showed the aspiration of a capsule
NSAID ingestion for which he received satisfactory com-bined endoscopic treatment. He continued with occasionalNSAID ingestion. One year ago the patient began to present
� Please cite this article as: Sánchez-Chávez X, Martínez-GarcíaC. Aspiración de cápsula endoscópica: ¿complicación frecuente?.2013;78:257---258.
etswbnco
ndoscope and the successful and non-invasive recovery ofhe patient. The first reported case of aspiration requiredurgical extraction,8 in another published case extractionas carried out through rigid bronchoscopy, using a foreignody forceps and basket, 7 and in another, the patient didot require any invasive recovery procedure,6 as with our
ase. Our patient did not present with the classic symptomsf acute aspiration or any symptom of respiratory distress.