Embed Size (px)
Citation preview

Revista de la
Sociedad Argentina de DiabetesSociedad Argentina de DiabetesRevista de la
Sociedad Argentina de DiabetesAño 50 • Vol. 50 • Nº Especial Scientifi c IADPSG Meeting 2016 • Marzo de 2016ISSN 0325-5247 (impresa) ISSN 2346-9420 (en lí nea)
Scientific IADPSG Meeting 2016
MARCH 21-23, 2016 • BUENOS AIRES • ARGENTINA
Abstracts of the lectures, hot topics, workshop, clinical updates, oral presentations and poster presentations presented at the
International Association of the Diabetes and Pregnancy Study Groups (IADPSG) Meeting 2016.
Universidad Católica Argentina, Buenos Aires, Argentina
Rev
ista
de
la S
ocie
dad
Arg
enti
na
de D
iabe
tes
• A
ño
50
• V
ol.
50
• N
º Esp
ecia
l Sci
enti
fi c IA
DP
SG
Mee
ting
20
16
• M
arzo
de
20
16

Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 A1
Comité Editorial
Directores: Dr. Pablo Arias. Médico Especialista en Endocrinología; Doctor en Medicina (Universidad de Ulm, R.F. de Alemania); Profesor Titular Ordinario de Fisiología Humana, Facultad de Ciencias Médicas, Universidad Nacional de Rosario, Santa Fe, Argentina.Dr. Julio César Bragagnolo. Médico Especialista en Medicina Interna y Nutrición. Jefe de la Unidad de Nutrición y Diabetes del Hospital J.M. Ramos Mejía; Docente Asociado de la Universidad de Buenos Aires (UBA), Ciudad Autónoma de Buenos Aires (CABA), Argentina. Dr. Gustavo Frechtel. Médico Especialista en Nutrición, Doctorado en la UBA; Profesor Asociado de la Cátedra de Nutrición, De-partamento de Medicina (UBA); Jefe de División Genética del Hospital de Clínicas (UBA); Jefe del Servicio de Nutrición y Diabetes, Hospital Sirio Libanés, CABA, Argentina.
Secretario: Dr. Alejandro De Dios. Especialista Universitario en Medicina Interna (UBA); Médico de Planta del Servicio de Clínica Médica del Hospi-tal Carlos G. Durand (CABA); Médico de la División Genética del Hospital de Clínicas José de San Martín (CABA), Argentina.
Integrantes:Dra. Gabriela Krochik. Especialista en Pediatría; Especialista en Nutrición Pediátrica; Asistente Adjunta del Servicio de Nutrición del Hospital de Pediatría J. P. Garrahan; Docente Adscripta Facultad de Medicina (UBA), CABA, Argentina.Dr. Claudio González. Profesor Titular de Farmacología de las Universidades Austral y Favaloro, y del Instituto Universitario CEMIC; Profesor de Metodología de la Investigación y Bioestadística de la Universidad Católica; Coordinador de la Carrera de Médicos Espe-cialistas en Farmacología (UBA), CABA, Argentina.Dr. Fabio Zambon. Jefe del Servicio Nutrición y Diabetes, Sanatorio de la Trinidad Mitre; Titular de la Unidad de Evaluación Tecnologías Sanitarias, OSECAC; Coordinador Académico, Universidad ISALUD; Subdirector Centro Médico Medeos, CABA, Argentina.Dra. Velia Lobbe. Médica Especialista en Nutrición; Jefa de la Unidad de Nutrición del Hospital de Gastroenterología Dr. C. Bonorino Udaondo; Profesora Titular de Fisiopatología I-II (Instituto Universitario de Ciencias de la Salud Fundación H. A. Barceló), CABA, Argentina.Dra. Laura Pomares. Médica Clínica; Especialista en Nutrición (UBA), Especializada en Diabetología (Sociedad Argentina de Diabetes, SAD); Médica de Planta del Servicio de Endocrinología y Diabetes del Hospital Juan Pablo II, Corrientes Capital, Coordinadora el Comi-té de Graduados en Diabetes de la SAD, Argentina.Dra. Estrella Menéndez. Médica Especialista en Nutrición; Medica de planta del Servicio de Diabetes y Nutrición CEMIC, CABA, Argentina.Dr. Luis Grosembacher. Jefe de la Sección Diabetes del Servicio de Endocrinología, Hospital Italiano de Buenos Aires, CABA, Argentina.Dra. Marianela Ackermann. Médica Especialista en Medicina Interna; Especialista en Nutrición; Magister en Diabetes; Docente e Investigadora de la Cátedra III de Medicina Interna de la Universidad Nacional del Nordeste (UNNE); Directora Asociada del Curso de Postgrado Obesidad Universidad Favaloro-Nutrinfo; Directora Asociada del Curso de Postgrado Nutrición Bariátrica (Sociedad Argentina de Nutrición, SAN), CABA, Argentina.Dra. Graciela Fuente. Médica Especialista en Nutrición, Especializada en Diabetes; Jefa de la Unidad de Nutrición del Hospital Carlos Durand; encargada de enseñanza de la materia Nutrición, Unidad Docente Hospitalaria Durand (UBA); Asesora del Comité de Neuro-patía Diabética, SAD, CABA, Argentina.Dr. Pablo René Costanzo. Investigador; Asistente en la Carrera de Investigador del Hospital Italiano; Especialista en Andrología acre-ditado por la Sociedad Argentina de Andrología; Jefe de Trabajos Prácticos del Departamento Académico de Medicina del Instituto Universitario del Hospital Italiano de Buenos Aires, CABA, Argentina.
Propietaria:Sociedad Argentina de Diabetes Asociación Civil
Domicilio Legal de la Revista:Paraguay 1307, piso 8º ofic. 74 (C1057AAU), CABA, ArgentinaRegistro en la Dirección Nacional de Derecho de Autor: Exp. No 5266320. Registro de la marca “Revista de la Sociedad Argentina de Diabetes - Asociación Civil” No de concesión 2.605.405 y No de disposición 1.404/13, Instituto Nacional de la Propiedad Industrial. La Revista de la SAD está indizada en la Base de Datos LILACS (Literatura Latinoamericana y del Caribe en Ciencias de la Salud) y en el Catálogo de Latindex, Sistema Regional de Información en Línea para Revistas Científicas de América Latina, el Caribe, España y Portugal. Periodicidad: cuatrimestral.ISSN 0325-5247 (impresa)ISSN 2346-9420 (en línea)
Edita:Sello Editorial Lugones® de Editorial Biotecnológica S.R.L. Socio Gerente: Facundo Lugones. Jefa de Redacción: Lic. María Fernanda Cristoforetti. Diseño gráfico: Marisa Kantor.Av. Acoyte 25, 4º piso, ofic. E (C1405BFA), CABA, Argentina. Tel.: (011) 4903-1090/2210. E-mail: [email protected]
Año 50 • Volumen 50 • Número Especial Scientific IADPSG Meeting 2016 • Marzo de 2016 •ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Año 50 • Volumen 50 • Número Especial Scientific IADPSG Meeting 2016 • Marzo de 2016
Imprenta: Gráfica Offset. Domicilio: Santa Elena 328, CABA, ArgentinaLa presente Edición está impresa en papel libre de cloro
Revista de laSociedad Argentina de Diabetes

Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientifi c IADPSG Meeting 2016 Marzo de 2016 A2
ComisiÓn dirECtiVa
Sociedad Argentina de Diabetes Paraguay 1307, piso 8º ofi c. 74, (C1057AAU), Ciudad de Buenos Aires, Argentina.
Tel./fax: (5411) 4816-2838/4815-1379. E-mail: sad@fi bertel.com.ar Sitio web: www.diabetes.org.ar
Presidente: Dra. María Cristina Faingold
Vicepresidente: Dra. Graciela Fuente
Secretario: Dr. Cristián Suárez Cordo
Tesorera: Dra. Carla Musso
Prosecretaria:Dra. Miriam Tonietti
Vocales Titulares:Dr. Nelson Rodríguez Papini
Dra. Susana SalzbergDr. Carlos Buso
Dr. Adrian Proietti
Vocales Suplentes:Dra. Mariana PrietoDr. Gabriel MinuchinDr. Osvaldo Fretes
Revisores de Cuentas Titulares:Dr. Isaac Sinay
Dr. Jorge Alvariñas
Revisor de Cuentas Suplente:Dr. Guillermo Burlando

Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientifi c IADPSG Meeting 2016 Marzo de 2016
Comité orGaniZador
Comité CiEntÍfiCo
ChairMaría Cristina Faingold
Co-ChairAlicia Jawerbaum
Vice-ChairSilvia Gorbán de Lapertosa
DPSG-SAD CoordinadoraGabriela Rovira
MiembrosSusana SalzbergLiliana Glatstein
María Elena RodríguezNatalia BasualdoIngrid Di Marco
Secretaria del Comité LocalEvangelina Capobianco
LOC Diabetes and Pregnancy Study Group of the Argentina Society of Diabetes
Alicia Jawerbaum, Jorge Alvariñas
LOC Saredia International AssociationJacinto Lang
Canadian Diabetes in Pregnancy Study GroupLois Donovan
DPSG of EASDAnne Dornhorst
Diabetes in Pregnancy Study Group IndiaVijayam Balaji, Seshiah V
Japanese Association of Diabetes and Pregnancy
Yasue Omori
West Coast USA DPSG David Sacks, Jed Friedman
Australasian Diabetes in Pregnancy SocietyAidan McElduff
Society MFM USAPat Catalano
A3
sCiEntifiC iadPsG mEEtinG 2016
DEL 21 AL 23 DE MARZO CIUDAD AUTÓNOMA DE BUENOS AIRES
ChairDavid McIntyre

Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 A4
Año 50 • Vol. 50 • Número Especial Scientific IADPSG Meeting 2016 • Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Revista de laSociedad Argentina de Diabetes
taBlE of ContEnts
•Editorial 1
•lectures 3
•Workshop 8
•Hot topics 13
•Clinical Updates 21
•oral Presentations 29
•Poster Presentations 33
•index of authors 77

1
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
1
BiEnVEnidos al iadPsG 2016
EDITORIAL
La diabetes es la alteración metabólica que con mayor frecuencia complica el embarazo influenciando el futuro de la madre y su hijo.
En los últimos años se inició un debate acerca de los criterios diagnósticos y en relación a la definición de la diabetes gestacional (DG).
El Grupo Internacional de Estudio de la Diabetes en el Embarazo (IADPSG, según sus siglas en inglés) a la luz del estudio Hiperglucemia y Embarazo Resultado Adverso (HAPO, sus siglas en inglés) que estudió a 24 mil mujeres gestantes, determinó nuevos criterios diagnósticos.
Este grupo se reúne cada cuatro años y en esta oportunidad tuvimos el gran honor que la Argentina haya sido elegida como sede de esta reunión científica, cuyo objetivo principal es proporcionar un foro en el que los médicos y científicos de todo el mundo puedan reunirse para presentar y discutir los últimos hallazgos en el área de la diabetes y la gestación, abordando una importante variedad de temas multidisciplinarios en los que es necesario actuar para mejorar el cuidado materno y fetal en la diabetes.
Haber participado en la coordinación de este encuentro científico del IADPSG en Argentina fue un placer enorme y una experiencia sumamente enriquecedora. El programa científico cuyo desarrollo llevó casi un año, intentó abarcar todo el espectro de temas relacionados con la Diabetes y el Embarazo, yendo desde lo mole-cular hasta lo estrictamente tecnológico, sin descuidar por supuesto los aspectos clínicos de esta patología.
Esperamos puedan disfrutar de esta reunión, que por primera vez se realiza en Latinoamérica y que nos acerca a figuras internacionales sumamente destacadas en el área de la Diabetes y Embarazo
Dra. María Cristina FaingoldPresidente Congreso IADPSG 2016
Es en base a muchos años de interacción con los grupos de estudio de diabetes y embarazo de diversos países del mundo que la Argentina, hoy miembro de la Asociación Internacional de Grupos de Estudio de Dia-betes y Embarazo (IADPSG), a través de la Sociedad Argentina de Diabetes, ha sido elegida como sede de este evento internacional: el Congreso IADPSG 2016.
Este evento tiene la particularidad de reunir personalidades destacadas de todo el mundo que trabaja en temas básicos, clínicos y traslacionales en diabetes y embarazo.
Fue un desafío realizar este evento en Latinoamérica y en especial en la Argentina, sorteando los inconve-nientes propios vinculados a nuestra realidad económica y social. Es por ello que hoy miramos con placer el inicio de este evento donde nuestro objetivo primordial fue brindar un programa científico y social como base que habilite a una profunda interacción entre especialistas latinoamericanos y del resto del mundo en el campo de estudio.
Nuestro objetivo especial fue mejorar la interacción entre especialistas básicos y clínicos, intentando de-mostrar que de esta interacción pueden surgir nuevos proyectos y desafíos que faciliten el progreso en el cuidado de la salud de todas las mujeres gestantes que padecen diabetes. En Latinoamérica, esta interacción es un camino que necesita ser más transitado y por ello resulta una oportunidad valiosa contar aquí con un gran número de especialistas en diabetes y gestación del mundo en áreas básicas, traslacionales y clínicas, que sabemos están totalmente dispuestos a interaccionar con los especialistas latinoamericanos y ayudarnos a transitar este camino.
A los invitados extranjeros, nuestro agradecimiento por participar en este encuentro y facilitar esta interac-ción con los delegados de todo el mundo.
A todos los delegados, agradecemos su participación, los próximos serán días de intensa actividad que mar-carán el avance en todas las áreas vinculadas a la salud materna y fetal en la gestación complicada con diabetes. Esperamos que puedan aprovechar y disfrutar de este encuentro.
Sean todos bienvenidos al IADPSG 2016.
Dra. Alicia Jawerbaum Co-Presidente Congreso IADPSG 2016

2 Editorial
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
2
Diabetes is a metabolic impairment that frequently complicates pregnancy, influencing the future of the mother and her offspring.
In the last years, the diagnostic criteria of this diseases as well as the definition of gestational diabetes (GDM) has been intensively debated.
The International Association of Diabetes in Pregnancy Study Groups (IADPSG), based on the Hyperglyce-mia and Adverse Pregnancy Outcome (HAPO) Study (HAPO), evaluated 24.000 pregnant women and determi-ned new diagnostic criteria.
This International Group meets every 4 years, and, in this opportunity, it is a great honor to say that Argentina has been selected as the headquarters for this Scientific Meeting. The main goal is to provide a forum where clinicians and basic scientists from all over the world can come together to present and discuss leading edge work on Diabetes and Pregnancy, addressing a major array of multidisciplinary issues on which action is requi-red to improve maternal care and fetal outcome in diabetes.
It has been a great pleasure and an extremely enriching experience to have had the chance to lead the coordination of this Scientific Meeting of IADPSG in Argentina. The elaboration of the scientific program took almost one year, and was intended to cover all the range of subjects related to Diabetes and Pregnancy, from the molecular to the strictly technological aspects, and taking into account of all the clinical aspects of this pathology.
We hope you enjoy this meeting, which, for the first time, is held in Latin America and allow us to be close to international highly outstanding scientists and clinicians in the field of Diabetes and Pregnancy.
Dra. María Cristina FaingoldChair IADPSG 2016 Meeting
As a result of several years of interaction with the Diabetes and Pregnancy Study Groups of different coun-tries in the world, Argentina, a novel member of the International Association of the Diabetes and Pregnancy Study Groups (IADPSG) through the Argentine Society of Diabetes, has been selected as the headquarters for this international event, the IADPSG 2016 Meeting.
This Congress brings together distinguished specialists from all over the world, who work in basic, clinical, translational and basic sciences in diabetes and pregnancy.
It has been a challenge to organize this event in Latin America, in particular in Argentina, considering our economic and social reality. Today, we look forward to the beginning of this event. In this Meeting, our main aim is to bring a scientific and social program as a base to promote a profound interaction between Latin-American specialists and those working in this field around the world.
Our special objective is to improve the interaction between clinical and basic specialists, aiming to demons-trate that new projects and challenges can arise from this interaction and thus facilitate the progress in the care of the health of all the pregnant women with diabetes. In Latin America, this interaction should be improved. Therefore, it is worth knowing that important specialists from all over the world, working in clinical, translational and basic sciences in diabetes and pregnancy will be present in this meeting and will be happy to interact and help Latin American delegates to improve this interaction.
Our thanks to the foreign Speakers for participating in this Meeting and facilitating the interaction with the delegates from all over the world.
To all the delegates, thank you for your participation. The next days will be of an intense activity and will mark the degree of advance in all the areas related to maternal and fetal health in pregnancies complicated with diabetes. We hope you are able to enjoy and take advantage of this meeting.
Welcome to IADPSG 2016.
Dra. Alicia Jawerbaum Co-Chair IADPSG 2016 Meeting
WElComE to iadPsG 2016

3
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Lectures 3
rEsúmEnEs dE las PrEsEntaCionEs dEl ConGrEso iadPsG 2016
AbsTRAcT Of ThE PREsEnTATIOns IADPsG 2016 MEETInG
lECtUrEs
oPEninG lECtUrEs: BasiC and translational sCiEnCEs in diaBEtEs & PrEGnanCy
ConGEnital malformationsUlf J. ErikssonDepartment of Medical Cell Biology. Uppsala University, Sweden
Despite increased clinical efforts to improve glycemic control during diabetic pregnancy, the rate of conge-nital malformations remains increased in studies of type 1 and type 2 gestational diabetes. In two recent large meta-studies, it was found that the malformation rates in type 1 diabetic pregnancy did not differ from that of type 2 diabetic pregnancy; both rates were estimated to be around 5-6%. The similar rates of malformation may relate to the increased age and concomitant adiposity in type 2 diabetic women, both of which may increase the incidence in this group.
The cell biological reason for the teratogenic effect of the maternal diabetic state is not known. Howe-ver, both environmental factors (maternal diabetic state and intrauterine conditions) and genetic predisposition seem to be of importance in diabetic embryopathy, i.e., diabetic teratogenesis is an environment–gene interac-tion process.
It has been suggested that the absence of a specific malformation pattern for diabetic embryopathy signals the presence of several teratological factors and mechanisms in diabetic pregnancy. Likewise, the number of different teratogenic agents identified would indicate that diabetic embryopathy is of complex etiology.
Several studies have suggested that diabetic embryopathy is associated with oxidative stress. Also, there are experimental evidence that diabetic embryopathy is associated with alterations of various signaling systems that control intracellular developmental conditions. These are nitrosative stress, ER stress, hexosamine stress and AGE/RAGE activity, as well as altered PKC and JNK activities. In addition, enhanced embryonic apoptosis has been regarded as a component of diabetic embryopathy.
Understanding the interrelationships and ”cross-talk” between these teratological events is important, pre-sumably crucial, for the understanding of the development of congenital malformations in diabetic pregnancy, and, consequently, for our ability to design future anti-teratological treatments to avoid diabetic embryopathy.
PlaCEntal CHanGEs in diaBEtEs mEllitUs: ContriBUtors to fEtal PHEnotyPE or adPatiVE rEsPonsEs?Gernot Desoye, Birgit Hirschmugl, Carolin Besenboeck, Ursula Hiden, Christian WadsackDepartment of Obstetrics and Gynaecology, Medical University of Graz, Graz, Austria
Owing to its position between mother and fetus, the placenta has long been speculated to contribute to the phenotype associated with maternal diabetes i.e., fetal/neonatal adiposity. The underlying assumption has been an augmented maternal-to-fetal nutrient transfer, especially of glucose and fatty acids. Molecular changes of placental glucose transporters such as GLUT1 and GLUT3 as well as of placental fatty acids transporters are accompanied by changes in glucose and fatty acid uptake into the trophoblast seemingly lending support to the hypothesis of placental involvement. However, ex vivo placental perfusion experiments as well as in vivo stable isotope studies have failed to provide any evidence for a placental contribution to augmented maternal-to-fetal glucose and fatty acid transfer at the end of gestation. Thus, the concentration gradients between the maternal and fetal circulation determine transplacental fluxes. An overflow of glucose and perhaps fatty acids into the fetus in conditions of maternal overnutrition then results from a steepened concentration gradient. Fetal
l1
l2

4
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Lectures4
hyperinsulinemia stimulates glucose extraction into insulin-sensitive fetal tissues and thereby contributes to a steepening of the concentration gradient, at least to that of glucose (‘fetal glucose steal phenomenon’).
Structural and functional compartimentalization of the placenta may explain absence of placental contribu-tion to nutritional overflow despite diabetes-associated molecular and functional changes in the placenta. These changes can be regarded as adaptive responses to protect the fetus from the adverse effects of the maternal and fetal environment. Insulin is one of the fetal signals mediating these responses. Examples are placental 1) hypervascularization to cover enhanced fetal oxygen demand, 2) upregulation of placental endothelial phospho-lipid-transfer protein (PLTP) to facilitate cholesterol depletion from the fetal circulation through HDL2 formation for uptake into the fetal liver, and 3) insulin-stimulation of lipoprotein-associated phospholipase A2 (LpPLA2) activity in placental macrophages to cleave oxidized placental phospholipids as a protective mechanism against oxidative stress.
Collectively, at the end of gestation the placenta does not seem to play an active role in determining the neonatal phenotype. 70 years after Jorgen Pedersen, his concept still remains unrefuted.
fEtal ExosomEs from GEstational diaBEtEs CaUsE fEtoPlaCEntal EndotHEliUm dysfUnCtion in normal PrEGnanCiEs Tamara Sáez1,2, Marijke Faas2, Luis Sobrevia 1,3,4
1Cellular and Molecular Physiology Laboratory (CMPL), Division of Obstetrics and Gynaecology, School of Medicine, Faculty of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile. 2Immunoendocrinology, Division of Medical Biology, Department of Pathology and Medical Biology, University of Groningen, University Medical Center Groningen (UMCG), Groningen, The Netherlands. 3Department of Physiology, Faculty of Pharmacy, Universidad de Sevilla, Seville E-41012, Spain. 4University of Queensland Centre for Clinical Research (UQCCR), Faculty of Medicine and Biomedical Sciences, University of Queensland, Herston QLD 4029, Queensland, Australia
Gestational diabetes mellitus (GDM) associates with macro and microvascular endothelial dysfunction in the human placenta. In the GDM placenta increased human cationic amino acid transporter 1 (hCAT-1)–mediated L-arginine transport, nitric oxide (NO) synthesis and endothelial NO synthase (eNOS) expression are found. Exosomes are nanoparticles involved in the modulation of trophoblast function in the human fetoplacental unit. However, the role of exosomes derived from the human umbilical vein endothelial cells (HUVECs) from GDM is unknown. In primary cultures of HUVECs from normal or GDM pregnancies the exo-somes released to the culture medium were collected and used to challenge HUVECs looking at L-arginine transport and NO synthesis. The L-arginine transport in HUVECs from normal pregnancies was increased in a concentration–dependent manner (half-maximal effect (ED50) ~0.5 μg/mL) when cells were exposed to exosomes from GDM pregnancies. However, exosomes from normal pregnancies reverted the GDM–increa-sed L-arginine transport to values in cells from normal pregnancies. Similar results were obtained for hCAT-1 protein abundance. However, total eNOS (i.e., non-phosphorylated and phosphorylated) protein abundance was unaltered by exosomes in both cell types, while exosomes from HUVECs from normal pregnancies re-verted the GDM–associated increase in eNOS phosphorylation at Ser1177, without altering its phosphorylation at Thr495. These findings suggest that HUVECs–derived exosomes from GDM could change L-arginine/NO signalling pathway in HUVECs from normal pregnancies to values in GDM. The findings show that exosomes released from HUVECs in the fetoplacental unit are a mechanism most likely involved in the aetiology of GDM in humans. Support: Fondo Nacional de Desarrollo Científico y Tecnológico (FONDECYT 1150377, 1150344), Chile. TS holds Comisión Nacional de Investigación en Ciencia y Tecnología (CONICYT), Chile, and UMCG, University of Groningen, The Netherlands-PhD fellowships.
tHE mECHanisms UndErlyinG adaPtiVE CHanGEs in β-CEll mass dUrinG PrEGnanCy in tHE moUsEDavid J. Hill, Linhao Zhong, Sandra Szlapinski , Christine Beamish, Brenda StruttLawson Health Research Institute, Western University, London, Ontario, Canada
The relative insulin resistance encountered during pregnancy is compensated for by an adaptive increase
l3
l4

5
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Lectures 5
in the maternal pancreatic β-cell mass and greater insulin availability. Failure to complete this adaptive change can contribute to gestational diabetes. The proliferative capacity of β-cells in adults outside of pregnancy is extremely low. Therefore an understanding of how β-cell expansion can occur during pregnancy could result in prevention strategies for gestational diabetes, as well as diabetes reversal more generally. We have previously shown that insulin-expressing but glucose-transporter-2-low (Ins+Glut2LO) multi-potent progenitor cells are pre-sent in high numbers in the neonatal mouse and human pancreas, and decrease with age. These cells are pre-dominantly located in extra-islet β-cell clusters and contribute to the regeneration of the endocrine pancreas fo-llowing directed pharmacological ablation. We therefore studied the role of Ins+Glut2LO cells in β-cell expansion during normal pregnancy, and in mice where this has been compromised through feeding a low protein diet.
Pancreata were collected from pregnant C57Bl/6 mice fed a control or low protein (8%) diet at gestational days (GD) 6, 9, 12, 15, and 18, and postpartum D 7 (n=4) and compared to control, non-pregnant animals (n>6). The β-cell mass, anatomical location of β-cells, proliferation rate (Ki67+ labeling), and proportion of Ins+Glut2LO
cells were measured using immunohistochemistry and confocal microscopy. An intravenous glucose tolerance test was performed at GD18. One-way ANOVA with Tukey’s Post Test was used to analyze data.
Beta cell mass was three times greater at GD 18 compared to non-pregnant mice. Total β-cell proliferation peaked at GD12, occurring both within islets (>6 β-cells) and in small β-cell clusters (1-5 β-cells). The proportion of Ins+Glut2LO cells also increased significantly during pregnancy and this preceding the increase in β-cell mass and proliferation, peaking at GD9 for both the islet and cluster compartments. Moreover, these Ins+Glut2LO cells themselves had a high proliferative rate at GD9. The increased proportion of Ins+Glut2LO Ki67+ cells persisted from GD6 -15 within clusters, and the overall number of clusters was increased significantly at GD9. In mice exposed to a low protein diet during pregnancy the adaptive change in β-cell mass was significantly impaired, and the number and proliferative rate of Ins+Glut2LO cells in clusters was significantly reduced compared to mice fed control diet. This resulted in poorer glucose tolerance.
These results indicate that Ins+Glut2LO β-cell progenitors likely contribute to β-cell expansion during pregnan-cy through an increased rate of proliferation and differentiation into new, functional β-cells, and that an induced reduction in β-cell compensatory mass resulted in impaired glucose tolerance.
ClosinG lECtUrEs: PrEGnanCy, oBEsity & diaBEtEs
diffErEnt imPliCation of liPids in nEonatal Body WEiGHt and fat mass BEtWEEn GEstational diaBEtiC and HEaltHy motHErsEmilio Herrera, Henar Ortega-SenovillaUniversity San Pablo CEU, Madrid, Spain
At term and under conditions of normal glucose tolerance maternal serum glucose, nonesterified fatty acids (NEFA) and glycerol but not triacylglycerides (TAG) correlate with these variables in cord blood serum whereas only maternal glucose correlate with neonatal weight or fat mass. Besides, cord blood glucose, TAG and NEFA correlated with neonatal weight, BMI or fat mass. However in gestational diabetes mellitus (GDM) maternal or cord blood glucose does not correlate with neonatal anthropometric parameters but cord serum insulin correlate positively with neonatal fat mass whereas cord TAG correlated negatively with neonatal BMI or fat mass and maternal NEFA, TAG and glycerol correlated positively with neonatal weight, BMI and fat mass. Although the mother can convert dietary essential fatty acids (linoleic acid, LA, and alpha-linolenic acid, ALA) to their long-chain polyunsaturated fatty acids (LCPUFA) derivatives like arachidonic acid (AA) and docosahexaenoic acid (DHA) respectively, these LCPUFA are essential for fetal development but the fetus can’t synthesize them and therefore have to come from maternal circulation where they are mainly carried in their esterified form associated to different lipoproteins. Despite that the placenta doesn’t have mechanisms to directly transfer these lipoproteins to fetal circulation it allows those fatty acids to become available to the fetus where at term the proportion of both AA and DHA are even higher than in their mother. In control neonates there are positive lineal correlations between the concentration of most individual fatty acids in cord serum versus both birth weight and fat mass. However in neonates of GDM mothers such correlations are not significant or appear negative as it is the case for LA, ALA and AA. Besides, the proportion of AA and DHA in umbilical arterial serum appears lower in GDM than in controls whereas no difference between the two groups is found in umbilical venous plasma, indicating an altered metabolism of LCPUFA by the fetus of GDM mothers. Thus whereas in controls maternal glucose is more important than lipids in controlling neona-
l5

6
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Lectures6
tal body weight, in GDM maternal lipids and their more efficient utilization by the fetus play a critical role in neonatal body, BMI and fat mass. It is therefore proposed that altered maternal lipid metabolism rather than hyperglycemia constitutes a risk for macrosomia in GDM.
matErnal PrE-PrEGnanCy oBEsity/ExCEssiVE GEstational WEiGHt Gain: EffECt on mEtaBoliC HEaltH of tHE offsPrinGPatrick M. CatalanoCenter for Reproductive Health, Case Western Reserve University, Cleveland, OHIO USA
Maternal obesity is the most common metabolic disorder in pregnancy. In the United States ~30% of women are obese and the percentage is higher in African American and Hispanic populations. Excessive gesta-tional weight gain is associated with accrural of adipose tissue in contrast to lean body mass. Maternal obesity is associated with increased insulin resistance before and during pregnancy affecting carbohydrate and lipid metabolism and is associated with meta-inflammation. This combination results in increased nutrient avail-ability for the fetus and fetal overgrowth and metabolic dysfunction. The infant of the obese women is heavier at delivery as compared with the normal weight women because of a preferential increase in adipose tissue and inflammation. There is a wide overlap in the percentage body fat of term neonates born appropriate for gestational age as compared with neonates born small or large for gestational age. The increase in adiposity at birth is a significant risk factor for childhood obesity. Further increased fat in contrast to lean mass accrural in the first 8 months of life is associated with childhood adiposity. In women with gestational diabetes, maternal pregravid obesity may be the more significant contributor to childhood obesity. Lifestyle interventions in obese women to decrease adverse perinatal morbidity in the offspring have largely been unsuccessful. We believe this may be related to early (first trimester) maternal hyperinsulinemia in obese women affecting placental gene expression and function. Lifestyle intervention prior to conception needs to be examined as a potential preven-tive treatment option.
oBEsityMaría Inés SchmidtFaculdade de Medicina, Universidade Federal Do Rio Grande Do Sul, Brazil
The nutritional transition manifested over the last decades worldwide has led to sharp increases in obesity rates globally. The rise occurs at all ages, and maternal obesity emerges as an important medical and obstetric problem with consequences to the future health and well-being of both mother and child. Traditionally conside-red a problem of high-income countries, maternal obesity has reached low and middle income countries, and frequently the so-called “double burden” of both low and excessive maternal weight challenges the implemen-tation of effective public policies.
Maternal obesity is associated with medical and obstetric complications including pregnancy loss, congenital anomalies, gestational diabetes, preeclampsia, cardiac dysfunction, proteinuria, sleep apnea, non-alcoholic fatty liver disease, failed trial of labor, cesarean delivery, endometritis, wound rupture/dehiscence, neonatal injury, in-creased length of labor, postpartum atonic hemorrhage and anemia. Obese women breastfeed less frequently and terminate breastfeeding earlier. The infant of the obese women is at increased risk of being premature, large for gestational age and is at increased risk of developing the metabolic syndrome and childhood obesity.
I will present these issues and will discuss the feasibility and effectiveness of interventions to be offered to obese women during pregnancy, including lifestyle and pharmacological interventions. I will also address possi-ble interventions to be given shortly after delivery and for the treatment of pre-conceptual obesity.
l6
l7

7
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Lectures 7
KEynotE lECtUrEs: tHE PanCrEas, tHE PlaCEnta & tHE Brain
insUlin sECrEtion-BEta CEll dysfUnCtionChristopher Nolan The Canberra Hospital and the Australian National University Medical School, Canberra, Australian Capital Territory, Australia
Major adaptations in the islet occur in normal pregnancy, including β-cell mass expansion, lowering of the glucose set-point for glucose-stimulated insulin secretion and a markedly augmented secretory response to glucose. While these adaptations are often considered to be compensatory to the physiological insulin resis-tance of later pregnancy, they begin much earlier and are likely to be important to the process of facilitated anabolism by which maternal energy stores are increased in early to mid-pregnancy. It is well recognised that failure of islet β-cell adaptation to pregnancy contributes to the pathogenesis of gestational diabetes.
There has been considerable progress made in understanding the mechanisms that underlie pregnancy-related islet adaptation. Hormonal factors, as well as changes in the nutrient mix in maternal blood, are involved. Prolactin and placental lactogens, acting via the prolactin receptor and the JAK2-STAT5 signalling pathway have a major role. This pathway has recently been shown to cause marked up-regulate of tryptophan hydrolase 1 and 2 increasing β-cell serotonin production. Also, prolactin increases β-cell Survivin (also known as Birc5) which is likely to be important for the β-cell expansion. Down-regulation of β-cell miRNA 338-3p, possibly via oestrogen action through the GPR30 oestrogen receptor, also occurs during pregnancy resulting in the increased expression of β-cell proliferation and survival genes.
Maternal blood lipids increase in normal pregnancy. We have shown that fatty acid augmentation of insulin secretion in islets of pregnant rats is enhanced, particularly late in pregnancy. This is associated with reduced islet fatty acid oxidation and very active glucose-stimulated glycerolipid fatty acid cycling (fatty acid esterifica-tion and lipolysis) and reduced islet triglyceride content.
An improved knowledge of the complexities of islet adaptation to pregnancy is not only key to better understanding of the pathophysiology of gestational diabetes, it also provides insight into the mechanisms involved in the regulation of β-cell mass and function in general.
PlaCEntal nUtriEnt sEnsinG in normal PrEGnanCy and PrEGnanCiEs ComPliCatEd By GEstational diaBEtEs Thomas Jansson Department of OB/GYN, Division of Reproductive Sciences, University of Colorado Anschutz, Medical Campus, Aurora, CO, USA
The placenta mediates maternal-fetal exchange and has historically been regarded as a passive conduit for nutrients. However, emerging evidence suggests that the placenta actively responds to nutritional and metabo-lic signals from the mother and the fetus. We have proposed that the placenta integrates a multitude of mater-nal and fetal nutritional cues with information from intrinsic nutrient sensing signaling pathways to match fetal demand with maternal supply by regulating maternal physiology, placental growth and nutrient transport. This process, which we have called placental nutrient sensing, ensures optimal allocation of resources between the mother and the fetus to maximize the chances for propagation of parental genes without jeopardizing maternal health. Placental mechanistic target of rapamycin (mTOR) signaling is likely to be an important component of placental nutrient sensing. We suggest that these mechanisms have evolved due to the evolutionary pressures of maternal under-nutrition, which result in decreased placental growth and down-regulation of nutrient trans-porters, thereby limiting fetal growth to ensure maternal survival. These regulatory loops may also function in response to maternal over-nutrition, leading to increased placental growth and nutrient transport in some cases of maternal obesity or gestational diabetes (GDM). Emerging evidence shows that fetal overgrowth in GDM is associated with activation of placental mTOR signaling and increased nutrient transport activity in the placental barrier, consistent with the placental nutrient sensing model. In summary, the placental nutrient sensing model predicts that the placenta plays a critical role in regulating fetal growth and mediating fetal programming, the-reby determining lifelong health. In GDM, it is critical to consider placental responses to better understand the influence of the disease and current treatment modalities on fetal short- and long-term outcomes.
K1
K2

8
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Workshop8
CoGnitiVE fUnCtion in tHE offsPrinGPeter DammCenter for Pregnant Women with Diabetes at Rigshospitalet, Copenhagen, Denmark
Exposure to maternal diabetes in utero may have well described negative longterm implications for meta-bolic functions in the offspring. Actually, increased risks for overweight, the metabolic syndrome and type 2 diabetes in the offspring have been described.
Development of the central nervous system is a result of complex processes initiated in utero and conti-nuing until late adolescence and adulthood. These processes are vulnerable to a number of adverse environ-mental factors associated with an increased risk of neurological and psychiatric disorders in later life. Thus a hyperglycemic intrauterine environment may exert an adverse influence on the development of the fetal brain with implications for the long-term cognitive function.
Studies on cognitive function in offspring of women with diabetes are relatively limited and often not easy to interprete. An update of our knowledge will be given primarily based on recent Danish studies in adolescent and adult offspring of women with diabetes during pregnancy (type 1 diabetes and gestational diabetes).
WorKsHoP: Gdm diaGnosis
Basis for tHE diaGnosis of GdmBoyd E. Metzger MD, Tom D. Spies Professor of Nutrition and Metabolism Emeritus. Northwestern University Feinberg School of Medicine, Chicago, IL, USA
Case reports that likely represented examples of gestational diabetes mellitus (GDM) were published in 19th century; however, the concept of GDM as we currently view hyperglycemia that is first recognized during pregnancy developed in the 1950s as part of a preoccupation of investigators with what was identified as “pre-diabetes”, that is the interval before development of diabetes mellitus. Retrospective historical evidence indica-ted that a significant proportion of women with adult onset diabetes had adverse pregnancy outcomes during their prediabetic years that were similar to such outcomes in pregnant women with pre existing diabetes. A clinical trial was initiated to determine in treatment with insulin would reduce adverse outcomes in women with “prediabetes”. However, the criteria that were proposed by O’Sullivan and Mahan in 1964 for interpretation of an oral glucose tolerance test during pregnancy focused on the level of risk for the later development of diabetes in the mother.
GDM has been recognized as a specific disorder of carbohydrate metabolism during pregnancy for more than 3 decades amidst controversy about the value of its detection and treatment. Two issues have been of ma-jor concern. The first is whether the adverse outcomes in pregnancies complicated by GDM are independently linked to maternal hyperglycemia or to confounding factors such as obesity or higher maternal age. The second is whether treatment of hyperglycemia in GDM reduces adverse outcomes. In the past decade, results of the “Hyperglycemia & Adverse Pregnancy Outcome (HAPO) Study showed that associations between maternal glycemia and linear and continuous and two large randomized clinical trials of treatment of mild GDM establis-hed that treatment of hyperglycemia can reduce frequencies of some adverse perinatal outcomes.
In 2010, an “expert” panel of the IADPSG published recommendations for the diagnosis and classification of hyperglycemia in pregnancy. IADPSG diagnostic thresholds are based on associations between plasma glucose concentrations from a 75 gm 2-hr OGTT and frequency of birth weight, infant adiposity and newborn cord C-peptide level each greater than the 90th percentile. These diagnostic recommendations have been accepted by many groups including the WHO. However, others have not and in some instances more treatment trials have been recommended. Thus, controversy about GDM continues.
W1
K3

9
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Workshop 9
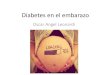
diaGnosis of GEstational diaBEtEs (Gdm). tHE intErnational fEdEration of GynEColoGy and oBstEtriCs (fiGo) initiatiVE on GEstational diaBEtEs mEllitUs: a PraGmatiC GUidE for diaGnosis, manaGEmEnt, and CarEDavid H. McIntyre1, Moshe Hod2, Anil Kapur2, David A. Sacks2, Eran Hadar2, Mukesh Agarwal2, Gian Carlo Di Renzo2, Luis Cabero Roura2, Harold David McIntyre2, Jessica L. Morris2, Hema Divakar2
1Professor, Mater Medical Research Institute, The University of Queensland, South Brisbane, QLD 4101, Australia. 2For the FIGO GDM Workgroup
The International Federation of Gynecology and Obstetrics (FIGO) has recently published a pragmatic guide to the diagnosis, management and care of women with GDM. This presentation will deal primarily with issues regarding diagnosis. FIGO recommends that all women should be tested for hyperglycemia during pregnancy and encourages its member associations to develop strategies to achieve this goal, adapted to local conditions. Whilst FIGO has primarily endorsed the WHO (2013) and IADPSG (2010) criteria for GDM based on a one step diagnostic 75 gram OGTT, it is recognised that, due to resource constraints, particularly in the developing world, local strategies may vary and should be considered equally acceptable. In this context, the diagnostic approaches promoted by DIPSI for India, the Ministry of Health for China, EBCOG for Europe, Latin American authorities for South America, ADIPS for Australia, NICE for the United Kingdom and local clinical practice in the Middle Eastern countries are specifically documented and acknowledged as representative of evidence or consensus based standards of care relevant to their local health care contexts.
FIGO recommends that the diagnosis of GDM should ideally be based on venous plasma samples properly collected and transported and tested in an accredited lab subject to external quality control. However, in primary care settings particularly in the developing world where proper facilities to test or store and transport blood sam-ples to a distant lab may not exist, a plasma glucose calibrated hand held glucometer with properly stored test strips to measure plasma glucose is considered an acceptable alternate. Using a glucose meter in this situation maybe more reliable than lab tests done on samples that have been inadequately handled and transported.
Beyond questions of GDM diagnosis, the FIGO document offers a pragmatic approach to major issues in the management of GDM, accompanied by a comprehensive assessment of such strategies using the GRADE framework.
Considering future priorities for GDM diagnosis, FIGO recommends further research regarding point of care testing and alternatives to the OGTT for GDM detection, studies of pre-pregnancy markers of GDM risk and careful definition of the potential costs and benefits associated with early pregnancy diagnosis of GDM. Long term observational studies to more clearly define the postpartum risks and cost effectiveness relating to a GDM diagnosis for both mother and baby are also recommended. The potential roles of metabolomics, the mi-crobiome and epigenetic factors including micro RNAs in defining GDM phenotype and influencing immediate pregnancy outcomes and longer term health risks are also recognized as a research priority.
tHE iadPsG diaGnostiC CritEria for HyPErGlyCaEmia in PrEGnanCy: a CommEntaryAidan McElduffThe Discipline of Medicine, The University of Sydney, Sydney, 2006, NSW, Australia
The new WHO/IADPSG criteria for the diagnosis of hyperglycaemia in pregnancy including gestational dia-betes (GDM) are based on the risk of fetal adiposity derived from the HAPO study although they also identify other neonatal and maternal risks (Diabetes Care 2010;33:676–682, Diabetes Res Clin Pract 2014;103:364–372). These new criteria will increase the prevalence of GDM in some but not all populations depending on the preva-lence of fasting or post load hyperglycaemia in the population. They have not been subjected to an RCT although the RCTs, which have been performed, have relatively similar glucose values for the diagnosis of GDM. The lack of RCT evidence of benefit has led to criticism particularly with regard to cost benefit. The NICE guidelines, which purport to examine the evidence for benefit, analyse 1 mmol/L variations in fasting plasma glucose on a variety of endpoints that do not include fetal adiposity. This analysis has been criticised as it can include only ~80 pairs of women from the ACHOIS study and individual patient data was not available to the NICE committee. Retrospective studies from before and after the change to the IADPSG criteria have shown benefit and cost savings in some populations. With regard to the diagnosis of GDM in early pregnancy the IADPSG has publish a
W2
W3

10
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Workshop
statement highlighting the need for more data and the current uncertainty about an appropriate fasting plasma glucose value for an early diagnosis (Diabetes Care DOI: 10.2337/dc15-1887).
tHE latin amEriCa diaBEtEs assoCiation (alad) diaGnosis of GdmSusana SalzbergSpecialist in Nutrition and Diabetes, Coordinator of Diabetes and Pregnancy working groups in the Latin Ame-rican association of Diabetes (ALAD) and the Argentine Society of Diabetes (SAD), Member of SAD Directive Committee, Buenos Aires, Argentina
Up today we failed to get universal consensus with regard to the diagnosis of gestational diabetes mellitus (GDM).Since 2007 ALAD Diabetes and Pregnancy Study Group considered appropriate for gestational diabetes
diagnosis the cutoff 100 mg/dl (5.6 mmol/l) in fasting plasma glucose (FPG) and 140 mg/dl or over (7.8 mmol/l) in 120 minutes p75 test. In 2013 we added other criteria in accordance with IADPSG and WHO, that pregnant with FPG of 126 or more are considered as to have diabetes mellitus.
We hoped HAPO Study would have brought a cutoff point for diagnosis, but this did not happen. This trial showed that there is a continuous association of maternal glucose levels with increased birth weight and increa-sed cord-blood serum C-peptide levels.
Diabetes and Pregnancy Committee of Argentine Diabetes Society developed a multicenter trial comparing maternal and neonatal outcomes in patients between IADPSG criteria and ALAD 2013
Preliminary report of 1037 (from 4000) pregnant women who have delivered their babies showed (Table 1):
Gdm PrEValEnCE maCrosomia
total PoPUlation no 7.23%
alad-Gdm 9.86% 12.74%
iadPsG 24.8% 11.24%
table 1
No significant difference (p=0.71) was observed in macrosomia between ALAD and IADPSG-diagnosed gestational diabetes mellitus patients. However both GDM (ALAD and IADPSG criteria) had a significant diffe-rence on macrosomia compared to total population (p<0.05). This preliminary data led the ALAD study group to the decision not to innovate the diagnosis criteria. Therefore, in the last workshop (2015) the ALAD Group confirmed that criteria, waiting for cost-benefit assessment.
The algorithm proposed for diagnosis of gestational diabetes is as follows (Figure 1):
figure 1: Dx algorithm. OGTT: oral glucose tolerance test; RF: risk factor.
There is a group of pregnant women at risk of developing GDM: obese pregnant with FPG between 85 and 99 mg/dl (4.72 mmol/l and 5.5 mmol/l). We recommend to follow up this group with diet plan and physical activity to prevent the development of gestational diabetes.
10
W4
≥ 126 First trimester fasting glucose
Repeat
≥ 126100 to 125
Diabetes
Gestational diabetes
≥ 126
≥ 140
≥ 140
< 140
< 100
RF = YES
24 - 28 week OGTT
No RF
Absence of GDM
OGTT 31 - 33 week
DIAMU 2013 ALAD 2015
100 to 125
dx algorithm

11
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Workshop 11
Gdm diaGnosis in UKAnne DornhorstImperial College, Hammersmith Hospital, London W12 0HS
In 2015 The National Institute for Health and Care Excellence (NICE) updated its guidance on Diabetes and Pregnancy (www.nice.org.uk/guidance/NG3). This guidance included recommendations for the diagnosis of gestational diabetes to be a fasting plasma glucose of 5.6 mmol/l (100 mg/dl or above and a 2 hour plasma glucose on a 75 gm. OGTT of 7.7 mmol/l (160mmol/l) or above.
These criteria followed an analysis of the impact of different diagnostic criteria on real patient data sets taken from 4 of the original HAPO centres1 (UK and Australia) and one from Norwich, UK.
The impact of different diagnostic criteria were considered using a prediction model looking at the impact of different diagnostic criteria on 3600 women for 6 predefined pregnancy outcomes (see table below).
- Shoulder dystocia (proxy for serious perinatal complications).- Jaundice.- Neonatal intensive care unit admission.- Induction of labour.- Caesarean section.- Pre-eclampsia.
dx thresholdnº
diagnosedshoulder dystocia
sPC CsniCU
admissionsJaundice Preeclampsia iol
No treatment 0 49 67 759 345 219 146 974
Fasting 5.6/2hs 8.5 413 43 59 745 332 213 130 995
Fasting 5.5 /2hs 8.5 450 43 59 744 331 213 129 996
Fasting 5.4/2hs 8.5 488 42 58 743 330 212 128 999
IADPSG 2.00 494 43 59 743 331 212 128 999
WHO 1999 558 41 57 741 328 212 126 1.002
Fasting 5.3/2hs 8.5 565 42 57 741 329 212 126 1.002
Fasting 5.6/2hs 7.8 629 41 56 739 326 211 123 1.006
Fasting 5.5/2hs 7.8 659 41 56 738 326 210 123 1,007
Fasting 5.4/2hs 7.8 688 40 56 737 325 210 122 1.009
Fasting 5.3/2hs 7.8 757 40 55 735 323 209 120 1,012
IADPSG 1.75 774 40 55 735 324 209 120 1.013
IADPSG 1.75 (incl 1hr) 912 39 54 731 321 207 117 1.019
IADPSG 1.50 1.063 38 52 727 317 206 113 1.027
Table 1: Modeling treatment and diagnosis of GDM. Clinical outcomes per 3,500 women with risk factors (SPC serious perinatal com-plications, CS Caesarean Section, NICU neonatal intensive care unit, IOL induction of Labour).
In addition a Health Economics cost effectiveness with general effectiveness analysis was undertaken that modelled outcomes and costs to obtain aggregated total costs and benefits across individual patients. For each threshold for each patient in the analysis to determine whether they would be diagnosed with gestational dia-betes. If no, they are not treated and they had a baseline risk for each outcome in the model. If yes, a treatment effect (relative risk) was applied to baseline risk based using ACHOIS2 and/or Landon3 Randomised Trial data. This analysis showed a fasting plasma glucose of 5.6 mmol/l (100mg/dl) and a 2hour OGTT glucose of 7.8 mmol/l (160mg/dl) to be highly cost effective.
REFEREnCES1. Group HSCR, Metzger BE, et al. Hyperglycemia and adverse pregnancy outcomes. The New England journal of medicine. 2008 May 8;358(19):1991-2002.2. Crowther CA, et al. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. The New England journal of medi-cine. 2005 Jun 16;352(24):2477-86. 3. Landon, et al. A multicenter, randomized trial of treatment for mild gestational diabetes. The New England journal of medicine. 2009 Oct 1;361(14):1339-48.
W5

12
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Workshop12
GEstational diaBEtEs (Gdm) diaGnosis in EUroPEFidelma DunneProfessor, School of Medicine and Galway Diabetes Research Centre (GDRC), National University of Ireland, Galway (NUIG), Ireland
The burden of GDM is rising globally as the prevalence of type 2 diabetes and obesity increases. In addition, rising maternal reproductive age is another important contributor. GDM can be effectively managed and the intervention, mainly medical nutritional therapy (MNT) and exercise, is of low cost for the majority of women. Effective management is associated with improved pregnancy outcomes for those treated with MNT and/or insulin. More importantly indentifying women with this condition is of public health concern as it allows inter-ventions to be initiated that can reduce maternal risk of progression to type 2 Diabetes by up to 50%. For the offspring, the growing literature on the association with Autism Spectrum Disorders (ASD), and the burden of adolescent obesity and diabetes compels us to identify women with GDM as efficiently as possible to improve the immediate and long term health of the offspring.
In Europe GDM may be diagnosed using various diagnostic criteria. A recent survey by the European Board and College of Obstetrics and Gynecology (EBCOG) of national affiliated societies identified that 75% of natio-nal societies are using the cut -offs recommended by WHO (2013) based on the HAPO study of 5.1, 10.0 and 8.5 mmol/l for fasting, 1 hour and 2 hour glucose post a 75g oral glucose tolerance test (OGTT). Interestingly, of the societies that have not implemented these guidelines, 50% intend to do so in the future. Other criteria used for diagnosis in Europe are in the minority and include the 1999 WHO (8.7%), the European Association for the Study of Diabetes (EASD) (8.7%), the Carpenter & Coustan (4.4%) and the National Diabetes Data Group (NDDG) criteria (4.4%). Most European countries implement selective screening based on risk factors with only a minority adopting a universal approach.
The known prevalence of GDM using WHO (2013) cut-offs in Europe varies depending on whether scree-ning is selectively or universally applied. In Ireland the prevalence is 12.4% on universal screening of a regional population while Belfast and Manchester had rates of 17% and 24% respectively recorded in the HAPO study.
The use of common diagnostic criteria for GDM by the majority of national societies is an important first step towards achieving uniformity in GDM diagnosis across Europe. In so doing it provides the infrastructure for comparative cohort studies in European populations and randomized trials to examine options for 1 step or 2 step screening programmes.
tHE statUs of GEstational diaBEtEs mEllitUs (Gdm) in asiaYasue OmoriDirector of Diabetes Center, Ebina General Hospital. Emeritus Prof. of Tokyo Women’s Medical University, Japan
In 1985, Hadden DR published the paper titled “Geography ethnic and racial variations in the incidence of gestational diabetes mellitus”. Wherein, he pointed out these differences were caused by, not only the ethnicity, but also the diagnostic criteria or glucose load volume relative to GTT.
In 2010, the newly completed diagnostic criteria and definition of GDM by IADPSG internationally brought benefit to the field of clinical practice and research, especially, for countries in which type 2 diabetes is pre-dominant.
In my country, Japan, so far, some doctors have followed the definition of GDM created by the ADA. There-fore, it was very confusing, and clinical data could not be compared according to region. The Japanese Society of Diabetes and Pregnancy, the Japan Society of Diabetes and the Japan Society of Obstetrics and Gynecology quickly accepted the new diagnostic criteria and definition developed by the IADPSG as early as in 2010, July. We, Japanese doctors adopted it smoothly because it is a very simple and clear definition, even if prevalence increased compared with previous criteria from 4.1% to 12.8%, because GDM is a pre-stage of type 2 diabetes, so we can find type 2 diabetes earlier.
Although getting information of the GDM status in Asia was attempted, the response rate was only 33,3%, therefore a few assumptions about the status of GDM in Asia can only be done by analysis of published papers.
The results will be presented at the congress in Argentina. Additionally, the problem of abnormal carbohydra-te metabolism in the first trimester of pregnancy, which is named GDM, is not exaggerated by pregnancy, but which was existing before pregnancy, will be discussed.
W6
W7

13
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Hot Topics 13
Hot toPiCs
Hot toPiCs sEssion 1: nUtrition in diaBEtEs & PrEGnaCy
ControVErsiEs in diEt rECommEndations in GEstational diaBEtEs to imProVE infant oUtComEsLinda Barbour Professor of Medicine and Obstetrics and Gynecology. Divisions of Endocrinology, Metabolism, and Diabetes and Maternal-Fetal Medicine. Co-Director Colorado Program for Nutrition and Healthy Development. Director OB Diabetes and Co-Director High Risk OB Clinics, University of Colorado School of Medicine, USA
Determining the optimal macronutrient composition for dietary management of gestational diabetes mellitus (GDM) has tremendous potential to improve perinatal outcomes, especially given a GDM prevalence of 10-30% using new diagnostic criteria recommended by the IADPSG. Diet therapy may result in significant cost savings if effective in deterring the need for expensive medical management within this growing population. Furthermore, fetal metabolic programming from excess maternal nutrient availability including glucose, triglycerides (TG), and free fatty acids (FFAs) has been strongly implicated in human epidemiologic studies and animal models as an in-dependent predictor for the development of obesity, metabolic syndrome, and diabetes in the offspring. However, there remains no consensus on the optimal diet for GDM women to minimize both the need for medication and prevent excess fetal overgrowth, and in the vast majority of studies, birth weight is used as a surrogate for the degree of infant fat development at birth. Surprisingly, there are less than a dozen RCT diet trials in GDM women and no large trials directly providing the maternal diet which better ensure compliance given the limited accuracy of dietary questionnaires and food records from adherence difficulties and recall bias. Although historically, diet therapy has focused on lowering simple carbohydrates to blunt the postprandial glucose excursion, women often substitute fat for carbohydrates since protein content is held remarkably constant at 15-20% of total calories. In addition to maternal glucose, studies support that maternal TG and FFAs can be used by the placenta and may be a stronger predictor of excess fetal fat accretion than maternal glucose, raising the question as to whether glyce-mia should be the sole criteria for diet recommendations. Furthermore, the substitution of carbohydrate with fat, especially saturated fat, may worsen maternal insulin resistance, resulting in a flux of all nutrients (glucose, lipids, amino acids) across the placenta and driving fetal overgrowth. A high fat diet has also been shown in non-human primates to result in lipid deposition in the fetal liver in addition to changes in the offspring metabolome and appe-tite regulation. The effect of a high fat diet on the microbiome may also be associated with endotoxin release (LPS) resulting in worsening maternal inflammation and an “obesogenic” microbiome. Overall, the available evidence would support that a diet higher in complex carbohydrate and fiber, low in simple sugar (low glycemic index), and lower in saturated fat may be effective in blunting maternal postprandial hyperglycemia and the worsening of maternal insulin resistance and preventing excess fetal growth. However, the use of diet therapy in the rapidly growing population of women with GDM or obesity is an area in grave need for high quality RCTs.
WEiGHt Gain dUrinG PrEGnanCy: a CritiCal issUE in sHort and lonG tErm fEto-matErnal HEaltHJorge AlvariñasAssessor of Diabetes and Pregnancy working groups in the Latin American association of Diabetes (ALAD) and the Argentine Society of Diabetes (SAD), Buenos Aires, Argentina
Adequate weight gain on pregnancy and prenatal body mass index (prenatal BMI) are critically important variables to follow pregnancy evolution and prevent pathologies in the mother and newborn which are someti-mes not taken in account.
Base on this, in 1990 and 2009, the Institute of Medicine (IOM), USA, published recommendations that were accepted by the World Health Organization (WHO) related to weight gain according to the prenatal BMI (Table 1).
Prepregnancy nutritional state recommended weight gain on pregnancy
Normal weight (BMI 18.5-24.9) 11.5 a 16 Kg (25-35 pounds)
Overweight (BMI 25-29,9) 7.0 a 11.5 Kg (15-25 pounds)
Obesity (BMI ≥ 30) 5 a 9 Kg (11-20 pounds)
Table 1: Recommended weight gain during the pregnancy (adapted from Rasmussen et al. 2009).
H1
H2

14
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Hot Topics14
Weight gain in women with normal BMI is 0.5 to 2 kg in the first trimester. An excessive weight gain in this first trimester is a predictor of a greater weight than the one indicated by the actual recommendations.
From the second trimester it is recommended a weight gain of 400 gr/week. It is recommended to follow the weight with the weight curve of Rosso-Mardones (ALAD).During a normal pregnancy with a 12-13 Kg weight gain, this weight corresponds to 7 kg of water, 7 kg of
fat and 1 kg of proteins. From the proteins, a 50% belongs to the fetus, suggesting the relevance of assuring the necessary protein intake.
But, are the weight recommendations followed? In 2000-2009 in United States, 35.8% of women showed the recommended weight gain, 44.8% showed a weight gain greater than recommended and 19.8% showed a weight gain lower than recommended.
A similar situation is found in different countries. In Argentina, from 991 overweight/obese women studied, only 45% achieved the goals.
Why does this happen? According to ION, from 3.661 healthy women studied, 27% did not receive any indication. Although the remaining 73% received the indications, 18% were indicated to gain less weight than that recommended and 22% received the indication to gain more weight than that recommended.
Other relevant aspect is nutrition. In the National Enquire in Nutrition and Health in Argentina (2007), those pregnant women with deficiency in selected nutrients were: energy 64%, proteins 29%, calcium 88% and ferrum 59%. This demonstrates the needs for education in national nutrition plans.
Which is the impact of not accomplishing these rules? In the mother, an increase in prenatal BMI increases in risks of preeclampsia (0.54% increase /1 kg/m2 increase in BMI), gestational diabetes, infections, hemorrha-ges and cesarean section.
In the newborn, the prenatal BMI increases the risks of malformations, increase in weigh for gestational age, admission to neonatal intensive therapy unit, and macrosomia. The latter pathologies correlate with an increase in obesity and type 2 diabetes in newborn´s later life.
We have studied mitochondrial DNA content in newborns from elevated and low weight for gestational age, finding that mitochondrial DNA content is lower in those newborns with weight alterations compared to normal weight newborns.
We speculate that the observed mitochondrial DNA depletion is a possible link between abnormal fetal growth and metabolic and cardiovascular alterations in later life.
In other work, we found that methylation of PPARgamma Coactivator 1A is correlated with prenatal BMI. Methylation of this coactivator is involved in mitochondrial biogenesis, is increased in pancreatic islets and related to FTO (fat mass and obesity associated) gene and obesity. Thus, its methylation has a potential role in intrauterine programming.
Recently, we showed that telomere length is related to abnormal fetal growth, suggesting that telomere length can also be programmed in the intrauterine environment.
Considering all this, weight control in the pregnancy through a nutritional plan and phyisical activity is impor-tant, and a beginning to prevent adverse future events.
REFEREnCES- Rasmussen, Kathleen M, Ann L. Yaktine. “Committee to Reexamine IOM Pregnancy Weight Guidelines.” Food and Nutrition Board, Board on Children, Youth and Families, Institute of Medicine, National Research Council. Weight gain during pregnancy: reexamining the guidelines. Washington, DC: National Academies Press (2009)- Cochrane Review. Published in 2015, issue 6.- Gemma C, et al. Obesity 2006; 14: 2193-2199. - Gemma C, et al. Obesity 2009; 17: 1032-1039.- Gilmore LA, et al. Seminars in Perinatology 2015; 39: 296-303.- Johnson J. Am J Obstet Gynecol 2015; 212: 806-18.- Telechea M et al. Sci Rep. 2015; 5:7869.
Vitamin d, oBEsity and diaBEtEs in PrEGnanCyDavid Simmons Western Sydney University, Campbelltown, Sydney, Australia
Vitamin D includes a number of fat soluble secosteroids involved in calcium and phosphate metabolism. Inactive forms of vitamin D are either produced endogenously following exposure of the skin to sunlight or fo-llowing consumption of some foods including fish, egg yolks, fish liver oils and fortified dairy and grain products.
H3

15
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Hot Topics 15
Activation of cholecalciferol (from endogenous sources) and ergocalciferol (from plant sources) is through hy-droxylation in the liver, and then the kidney to produce 1,25 hydroxy vitamin D. The definition of biologically im-portant low concentrations of vitamin D is debated with some using a definition of 25 OH Vitamin D <50nmol/l and others using <75nmol/l. The prevalence of low vitamin D concentrations varies across different populations and with seasoinality. Although many women take multivitamin supplements, including in pregnancy, vitamin D deficiency remains common.
Within non-pregnant and pregnant women, vitamin D concentrations are lower in the presence of obesity. In pregnant women, fetal vitamin D concentrations correlate with maternal concentrations. The implications of this remain unclear, but maternal Vitamin D deficiency has been associated with adverse outcomes related to the skeletal health of the offspring including low birth weight, small for gestational age and preterm delivery in some studies. Low maternal vitamin D concentrations in pregnancy are also associated with maternal ges-tational diabetes and pre-eclampsia. Whether these associations are causal, remains disputed. There is some evidence that that vitamin D is involved with pancreatic islet function, providing a putative mechanism behind the association.
Randomised controlled trials to date have not clearly shown that Vitamin D supplementation is associated with the prevention of GDM or indeed diabetes outside of pregnancy with doses of up to 4000iu/day. A small number of studies have suggested that vitamin D supplementation might reduce insulin resistance (measured as HOMA IR), but these require confirmation. Trials are currently underway to test the benefits of vitamin D supplementation on insulin resistance and the risk of GDM.
In summary-diabetes, obesity and vitamin D in pregnancy: epiphenomenon or causal pathway? Still unanswered.
mEditErranEan diEt and inCidEnCE of GEstational diaBEtEsEleni AnastasiouDirector, Endocrine Section-Diabetes Center. Alexandra General Hospital, Greece
The traditional Mediterranean diet (MedDiet) is, literally, the dietary pattern prevailing among the people of the olive tree-growing areas of the Mediterranean basin before the 1960’s. It has entered the medical literature by the pioneering Seven Countries Study conducted by Ancel Keys and his colleagues which showed that the adherence to the MedDiet pattern was associated with less cardiovascular disease risk in men of Crete, island of Greece, Italy and Spain. Further studies have confirmed this finding, and additionally have found other bene-ficial associations, including, inter alia, the prevention of DM2 and the metabolic syndrome, lower incidence of some cancers (as gastric, colorectal and breast cancers), and possibly lower incidence of hip fractures.
Although there is no specific single pattern of MedDiet, its main characteristics, as currently determined, are the following: high intake of vegetables, legumes, unprocessed cereals, fruits and nuts; a high intake of olive oil but a low intake of saturated and trans lipids; a moderate consumption of fish; a low to moderate consumption of dairy products in the form of low fat yoghurt and cheese; a low intake of meat (preferable white instead of red meat). An important component of the MedDiet is the regular, moderate consumption of wine during meals.
It is well documented that the prevalence of Gestational Diabetes Mellitus (GDM) is increasing as obesity among women of the reproductive age is rising globally. Further, there are a few studies that have examined the association of individual nutrients or foods with GDM risk. A positive correlation was found between GDM incidence and saturated fat intake, red and processed meat products and food with high glycemic load.
However, nutrients are not consumed in isolation; therefore, determining an “eating pattern” has the advanta-ge of taking into account the complex interaction and cumulative effects of various nutrients within the entire diet.
In an observational study the MedDiet pattern of eating was explored in relation to the incidence of GDM in more than a thousand pregnant women from ten Mediterranean countries. In all women, during the OGTT-75g, the dietary habits were assessed by a validated questionnaire, and a MedDiet Index was computed. The incidence of GDM defined by either Carpenter and Coustan or IADPSG criteria was lower in women with the higher MedDiet index (which denotes better adherence to MedDiet) after adjustment for age, BMI, diabetes in family, weight gain and energy uptake. Furthermore, better adherence to MedDiet was associated with a better degree of glucose tolerance in pregnant normoglycemic women.
Nevertheless, the mechanisms underlying the protective effects of the MedDiet are not clear. The high ratio of monounsaturated fatty acids to saturated fatty acids, the low content of trans fatty acids and the high content of fiber, anti-oxidants, polyphenols and magnesium may contribute to the anti-inflammatory properties of the MedDiet, and may also help prevent metabolic deterioration by opposing free radicals and decreasing systemic oxidative stress.
H4

16
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Hot Topics16
Hot toPiCs sEssion 2
EPiGEnEtiC rEGUlation in diaBEtiC EmBryoPatHyMary R. Loeken, Ph.D.Section on Islet Cell and Regenerative Biology, Joslin Diabetes Center. Department of Medicine, Harvard Medical School, Boston, MA USA
Maternal pregestational diabetes significantly increases risk for congenital malformations, a diabetic compli-cation known as “diabetic embryopathy”. Neural tube defects (NTDs) are among the most common malforma-tion seen in diabetic embryopathy. We have used a mouse model in which NTDs are significantly increased by maternal diabetes. The defects resemble those that occur with 100% penetrance in the mouse strain, Splotch, (Pax3Sp/Sp) which carry loss-of-function Pax3 alleles. We found that Pax3 expression is significantly reduced in embryos of diabetic mice. This is not due to general inhibition of neuroepithelial/neural crest gene expression, as Pax7 and Pax6, which are also expressed in the neural tube, are not inhibited. Thus, while there could be many processes during neural tube closure that are disturbed by maternal diabetes, simply reducing Pax3 ex-pression below a critical threshold is sufficient to cause a NTD. We have elucidated a pathway, showing how maternal diabetes induces oxidative stress, and how oxidative stress inhibits Pax3 expression, and how Pax3 insufficiency causes NTDs.
An important question is how maternal hyperglycemia and embryo oxidative stress inhibits Pax3 expression at the level of transcription. We recently showed that a Pax3 CpG island is highly methylated in blastocysts and un-differentiated embryonic stem cells (ESC), prior to the onset of Pax3 expression, and that hypomethylation of the Pax3 CpG island is necessary for induction of Pax3 expression in the neurulating embryo and differentiating ESC. Use of shRNA directed against each of the DNA methyltransferase (Dnmt) mRNAs demonstrated that DNMT3B is responsible for methylation and silencing of Pax3 prior to differentiation and in response to oxidative stress. While expression of Dnmt3b was not affected by oxidative stress, DNA methyltransferase activity was stimulated by oxidative stress. These results indicate that hyperglycemia-induced oxidative stress stimulates DNMT3B activi-ty, thereby inhibiting chromatin modifications necessary for induction of Pax3 expression during neurulation. This provides a molecular mechanism for defects caused by Pax3 insufficiency in diabetic embryopathy.
transGEniC moUsE modEls sHEd liGHt on tHE rolE of ProlaCtin on food intaKEDamasia Becu-VillalobosSenior Researcher CONICET. Director of the Institute of Biology and Experimental Medicine. Head of the Labora-tory of Pituitary Regulation. IBYME. Buenos Aires, Argentina
High prolactin levels observed in pregnancy and lactation may contribute to a hyperphagic state probably sustained by leptin resistant hypothalamic centers controling food intake. The presence of prolactin receptors in brain areas associated with the regulation of energy balance and food intake, as well as in white and brown adipose tissue, liver and pancreas raises the possibility that prolactin is involved in energy balance acting at different levels.
To unravel the role of elevated prolactin levels, lactotrope specific dopamine receptor type 2 (D2R) knockout (lacDrd2KO) female mice provide a unique model. Because dopamine acting on lactotrope D2Rs inhibits prolac-tin synthesis and secretion, female lacDrd2KO mice have chronically elevated serum prolactin levels, pronoun-ced lactotrope hyperplasia, and increased pituitary weight and prolactin content. They are subfertile and have altered estrous cycles. Importantly, in lacDrd2Ko mice there is increased food intake and body weight, specially in females, and marked adiposity. In correlation with adiposity accretion serum leptin is markedly elevated in 11 month-old female lacDrd2KO mice, but high leptin levels do not induce higher levels of anorexigenic peptides indicating leptin resistance. Hypothalamic Pomc mRNA levels, as well as intermediate pituitary levels of aMSH, which are anorexigenic, are not modified. Furthermore mRNA levels of the orexigenic neuropeptide Y (Npy), which are usually downregulated by leptin are increased, while the precursor of orexins (Ppo) is not modified. These results reinforce the occurrence of leptin insensitivity in the presence of high prolactin levels.
Furthermore, hyperprolactinemic lacDrd2KO mice have glucose intolerance, hyperinsulenemia, and a blun-ted insulin response to glucose, pointing to an imbalance of glucose homeostasis. In lacDrd2KO female mice not only heavier gonadal and retroperitoneal fat pads, but also heavier livers were observed. Adipocytes were
H5
H6

17
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Hot Topics 17
bigger, and increased adiposity correlated with higher serum triglycerides and non esterified fatty acids with no changes in cholesterol or adiponectin levels.
In the heavier livers of lacDrd2KO mutants, abundant fat droplets were evidenced, as well as higher triglyce-ride content. This high fat content in the liver could not be explained by alterations of the expression of lipogenic or lipolytic enzymes such as Fas, Atgl, Lpl and Hsl). Therefore altered glucose homeostasis, and glucose-indu-ced lipogenesis may be causally related to increased liver fat observed.
Results in lacDrd2KO provide clear evidence that chronic high prolactin levels promote food intake, adiposity and glucose intolerance. This may represent a hallostatic hallmark in pregnancy, but also may posit a diabetoge-nic risk during treatments with antisychotic medications or in patients with prolactinomas.
matErnal diEt and dEVEloPmEnt of tHE matErnal-infant miCroBiomE Jacob E. FriedmanUniversity of Colorado School of Medicine, Aurora Colorado, USA
It is becoming increasingly clear that the gut microbiome in newborns and infants plays a significant role in gut health and therefore child development. Maternal obesity and diabetes dramatically increase the long-term risk for obesity in the next generation, and primary prevention during pregnancy and lactation, including changes in the microbiome may be possible to break the obesity cycle. The gut bacteria is established during the first 1-3 years of life and is dramatically altered by the components of breast feeding and early infant diets. Alteration of the early infant gut microbiome has been correlated with the development of childhood obesity and autoimmu-ne conditions, including asthma, allergies, and more recently type 1 diabetes. Pre-existing obesity or diabetes in mothers can affect the early colonization of the infant microbial landscape but it’s causative role in the future composition of both the childand adult microbiota and metabolic, gastrointestinal, and autoimmune disease risk later is unknown. This is likely due to complex interactions between mode of delivery, antibiotic use, maternal diet, components of breastfeeding, and a network of regulatory events involving both the innate and adaptive immune systems within the infant host. Each of these factors are critical for informing microbiome develop-ment and can impact immune signaling, toxin release, and metabolic signals that regulate appetite, metabo-lism, and inflammation, including short-chain fatty acids and possibly bile acids. Early results also suggest that an individual’s genome, in part, shapes the microbiome, which in turn can influence host metabolism. Several randomized controlled trials have administered probiotics to target the microbiome during pregnancy to impro-ve maternal and infant health. However, there are limited studies examining the long-term effects of microbial therapy on infant body composition, and are often confounded by mode of delivery, antibiotic use, ethnicity, infant gender, maternal health, and length of exposure. Understanding how nutritional exposures affect the assembly and development of both maternal and infant microbial communities may aid in identifying targeted interventions to reduce adverse outcomes in infants born to mothers with obesity or diabetes and slow the maternal-infant transmission of obesity risk to the next generation.
Hot toPiCs sEssion 3
GlyBUridE trEatmEnt in GEstational diaBEtEs is assoCiatEd WitH inCrEasEd PlaCEntal GlUt1 ExPrEssion and HiGHEr BirtH WEiGHt.Paula Díaz, Genelyn Dimasuay, Soumini Vasan, Theresa PowellUniversity of Colorado, USA
Introduction: gestational diabetes (GDM) is treated by diet modification, oral insulin sensitizers or insulin. Use of sulfonylureas, such as glyburide, to treat GDM has raised concern about neonatal side effects such as hyperinsulinemia and increased birth weight (Amin M, Clin Drug Investig 2015:35). In the placenta, ATP-sensiti-ve K+ channels (KATP; Kir6.2) and sulfonylurea receptor (SUR2) are localized to the syncytiotrophoblast. In other cell types, sulfonylureas inhibit KATP channel activity causing depolarization and Ca++ influx. Sulfonylureas stimulate glucose uptake by increasing glucose (GLUT) transporters (Tsiani E, Endocrin 1995:136). The effects of glyburide on placental function have not been adequately studied. We tested the hypothesis that glyburide in pregnancy causes increased trafficking of glucose transporters to the syncytiotrophoblast plasma membranes.
Methods: we collected placentas from GDM pregnancies treated with either diet modification (n=15) or gly-
H7
H8

18
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Hot Topics18
buride (n=8) who delivered at term. We isolated syncytiotrophoblast microvillous (MVM) and basal (BM) plasma membranes and determined expression of nutrient transporters for glucose, amino acids and fatty acids in the MVM and BM by Western blot. Birth size parameters were also evaluated. GLUT1 transporter expression was evaluated by confocal microscopy in cultured primary human trophoblast (PHT) cells after exposure to glyburide.
Results: birth weight was higher when mothers were treated with glyburide (3.4 vs 3.7 kg, P<0.05). GLUT1 expression was significantly increased in both the MVM (+50%) and BM (+75%) of the syncytiotrophoblast in mothers treated with glyburide compared to those treated by diet (P<0.01). Placental amino acid and fatty acid transporter expression were not altered by glyburide therapy. Exposure to glyburide (20 and 100 µM) increased membrane expression of GLUT1 in cultured trophoblast cells.
Conclusions: glyburide treatment of GDM was associated with increased birth weight as previously des-cribed. The increased GLUT 1 expression in MVM and BM in response to glyburide will result in enhanced fetal glucose delivery leading to accelerated fetal growth. This may provide a possible explanation for the association between glyburide treatment and increased birth weight.
inCrEtin ExPrEssion is altErEd in tHE offsPrinG of rats fEd WitH a satUratEd fat diEt: PossiBlE rolE of lEPtinVerónica White, María Belén Mazzucco, Evangelina Capobianco, Alicia JawerbaumLaboratory of Reproduction and Metabolism, CEFYBO-CONICET, University of Buenos Aires, Buenos Aires, Argentina
Introduction: in a rat model of maternal overweight, induced by an overload of saturated fat in the diet, we have previously found several metabolic alterations in mothers, fetuses and offspring, as well as hyperglycemia, hyperinsulinemia, hyperleptinemia and liver leptin resistance in fetuses from these rats. Recently, we found al-terations in the gene expression of the incretins gastric inhibitory peptide (GIP) and glucagon-like peptide (GLP) in the fetal intestine. Nutrients, as well as leptin, are well-known stimulators of incretin production. We aimed to analyze whether an overload of saturated fat in the maternal diet induces impairments in leptin-induced intesti-ne GIP and GLP gene expression in the fetus and whether these impairments persist in the offspring’s later life.
Methods: female Wistar rats were fed with either a standard (5% fat) (controls) or a saturated fat diet (28% fat) from 6 weeks of age (SFD rats). After 8 weeks of diet, they were mated with control males. Control and SFD pregnant rats were euthanized at 21 days of gestation and fetal intestines obtained and either preserved or cultured (3 h) with or without leptin (100 ng/ml). Another group of control and SFD rats were allowed to deliver, their offspring euthanized at 21 or 140 days of age and the proximal portion of their intestine obtained. GIP and GLP expression were assessed by PCR.
Results: the intestines from control male and female fetuses cultured with leptin showed higher GIP and GLP expression (p<0.05) compared with no addition. In contrast, the intestines from SFD fetuses cultured with leptin showed no changes in GIP or GLP expression suggesting intestine resistance to leptin activity in the SFD group. Moreover, the intestines from the 21-day-old female and male offspring (p<0.05) and in the 140-day-old female offspring (p<0.05) from SFD rats showed lower GIP expression than those from controls. The intestines from the 140-day-old male and female offspring from the SFD group (p<0.05) also showed lower GLP expres-sion than those from controls.
Conclusions: saturated fat in the maternal diet induces a down-regulation of intestine gene expression of incretins in the offspring. Leptin resistance in incretin expression begins during fetal life and may be responsible for impairments in GLP and GIP intestine expression in the offspring’s later life.
Early PrEdiCtors of GEstational diaBEtEs in GinGiVal CrEViCUlar flUid and ExaCErBatinG faCtors of PEriodontal disEasE dUrinG PrEGnanCyAlejandra Chaparro1, Valeria Ramírez1, Edgardo Zuñiga1, José Galaz1, Juan Pedro Kusanovic1, Carolina Inostroza1, Manuel Varas-Godoy1, Carlos Salomon2, Gregory Rice2, Sebastián Illanes1
1Department of Obstetrics and Gynaecology, Faculty of Medicine, University of Los Andes, Chile. 2Centre for Clinical Diagnostics, Royal Brisbane and Women’s Hospital, University of Queensland, Australia
Background: gestational diabetes mellitus (GDM) affects around 10% of all pregnancies. The current ‘gold standard’ for the diagnosis of GDM is performed at 24-28 weeks of gestation. When GDM is diagnosed in
H9
H10

19
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Hot Topics 19
the late second or early third trimester of pregnancy the ‘pathology’ is most likely well established and the possibility to reverse or limit potential adverse effects on perinatal outcomes may be limited. Early detection of predisposition to and/or onset of GDM are the first step in developing, evaluating and implementing efficacious preventive treatment.
Aim(s): to explore biomarkers in gingival crevicular fluid (GCF) early in pregnancy (11-14 weeks gestation) and determine their association with the GDM development and with the severity of periodontal disease.
Methods: we recruited 80 pregnant women, and with Sotero del Río Hospital and Universidad de los Andes ethics committee approval and patients signed consent, we took GCF samples early in pregnancy (11-14 weeks) and completed a questionnaire for maternal, periodontal and obstetric history. We measured two biomarkers in GCF. Additionally, we evaluated a complete periodontal condition and anthropometric variables. All significant variables were integrated in a multiparametric model by logistic regression analysis.
Results: 80 pregnant patients were included, 17,5% (n=14) of them developed GDM. The BMI observed in the first trimester was 32.23Kg/m2 in GDM group and 26.15Kg/m2 in healthy pregnancies (p value = 0.0022). Periodontal surface inflamed area was 904.45mm2 in patients that developed GDM and 854.1mm2 in the control group. The mean values observed of biomarker 1 in GCF for patients that developed GDM was 12.19 ng/mL compared with 4.93ng/ml in the healthy pregnancies (p-value = 0.0919). Biomarker 2 levels were 0.76ng/ml in healthy patients and 4.24pg/ml in the case group (p-value = 0.0252). Area under the ROC curve observed was 0.8185, when combining BMI with GCF levels of these biomarkers.
Conclusions: women that will develop GDM showed significant differences in comparison with healthy pregnancies in the selected biomarkers detected in the GCF during the first trimester of pregnancy. A multiparametric model could predict the development of GDM, although this model needs further validation.
atlantiC diP: PrEPrEGnanCy CarE, PrEGnanCy and BEyond. an EValUation of WomEn WitH diaBEtEs 12 montHs Post-PartUmAoife Egan, Louise Carmody, Breda Kirwan, Fidelma DunneGalway Diabetes Research Centre, National University of Galway, Ireland
Introduction: many patients with type 1 and 2 diabetes struggle to meet therapeutic targets. However, during pregnancy women are highly motivated to achieve tight glycaemic goals and typically receive intensive education and support from a specialist service. Those who attend prepregnancy care (PPC) benefit from addi-tional input for approximately 6 months prior to pregnancy.
Objective: this study sought to assess the impact of pregnancy and PPC on long term treatment goals in women with diabetes.
Methods: we included women with type 1 and 2 diabetes who attended the Atlantic DIP programme for PPC and antenatal care between January 2006 and December 2014. Women were evaluated at six months prepregnancy (or at first PPC visit), and again at twelve months post-partum.
Results: in total 269 women were included, 177 (66%) with type 1 diabetes and 92 (34%) with type 2 diabetes. One hundred and seventeen (44%) attended prepregnancy care. At 12 months post-partum, 70 (26%) were again attending PPC, 26 (9.7%) were pregnant again, 40 (14.9%) were lost to follow up and the remaining 133 (49.5%) were attending routine diabetes clinics. For all women despite achieving tight glycae-mic control in the first trimester of pregnancy (mean HbA1c 7.2±1.6%), there was no significant difference in HbA1c before and twelve months after pregnancy (before: 7.8±1.9%, after: 7.6±1.7%, p=0.26). Furthermore, there was no difference in mean systolic/diastolic blood pressure (SBP/DBP), lipid profile, albumin-creatinine ratio (ACR) or weight in women before and after pregnancy. However, at 12 months post partum, those who attended PPC in preparation for pregnancy had a lower SBP (126.3±14.6mmHg vs 119.8±17.0mmHg, p=0.001), DBP (77.6±9.9mmHg vs 74.8±8.0mmHg, p=0.04) and weight (75.0±14.4kg vs 81.0±20kg, p=0.04) than those who did not attend PPC. In addition, women who achieved a first trimester HbA1c of <7.0% after PPC continued to demonstrate superior glycaemic control at 12 months post-partum (6.8±1.3% vs 8.4±1.8%, p<0.001).
Conclusions: despite intensive education and personal motivation during pregnancy, women with diabetes do not have a sustained improvement in measures of diabetes control and weight at 12 months post-partum. However, the benefits of PPC continue beyond pregnancy with women who have attended PPC continue to have better glycaemic control, lower BP and lower weight at 12 months post-partum. Our challenge now is to engage all women in PPC so that these long term benefits can be gained by all women with established diabetes.
H11

20
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Hot Topics20
dEVEloPmEnt of a risK sCorE for HyPErtEnsion PrEdiCtion in WomEn WitH a History of GEstational diaBEtEs mEllitUsJames Carey, Julia Wenger, Jennifer Huynh, Ravi Thadhani, Rhonda Bentley-LewisMassachusetts General Hospital, USA
Introduction: gestational diabetes mellitus is associated with increased maternal cardiovascular disease (CVD) risk manifest as hypertension subsequent to pregnancy. The impacts of dysglycemia and race/ethnicity on hypertension risk have been examined; however, the study of other putative risk factors has been limited. We aimed to develop a risk score that predicts hypertension subsequent to pregnancy accounting for degree of dysglycemia.
Methods: we identified a population of 23,223 women who presented for prenatal care to the Massa-chusetts General Hospital Obstetrical Department between September 1998 and January 2007. We selected women aged 18 to 40 years free of CVD or pregestational diabetes with complete glycemic and demographic data who delivered a singleton, live birth, and were free of CVD or pregestational diabetes. Each woman’s initial pregnancy was selected in order to not violate the independence assumption. The population was next strati-fied by incident hypertension subsequent to pregnancy. Logistic regression models (with and without stepwise selection) were used to identify significant maternal risk factors based on predictive performance. Finally, the risk prediction score was developed from β coefficients in multivariable Weibull models.
Results: the study sample comprised 11,161 women; 547 (4.9%) women developed hypertension during 4.2 years (median) follow-up. Significant predictors of hypertension included age, body mass index, systolic and diastolic blood pressures, parity, dysglycemia, and race/ethnicity. These factors were used to develop a risk score for subsequent hypertension risk. The final risk score achieved a c-statistic of 0.76, indicating moderate discriminative ability (Figure 1).
Conclusions: we have developed a risk score that may be used in clinical settings to identify patients with an elevated risk of hypertension subsequent to a pregnancy complicated by dysglycemia. Further external vali-dation is warranted to determine generalizability and clinical effectiveness.
Figure 1: Receiver operatin characteristic curves (ROC) for detection of hypertension based on different combinations of risk factors.
H12

21
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Clinical Updates 21
CliniCal UPdatEs
CliniCal UPdatE 1: monitorinG in diaBEtEs & PrEGnanCy
PostPrandial monitorinG in PrEGnanCy WitH diaBEtEsGloria López-StewartDirector Postdraduate Diabetes Program, Faculty of Medicine, University of Chile, Chile
Glucose monitoring is crucial for a successful outcome of pregnancy in women with pregestational, type 1, type 2 and gestational diabetes. There is controversy around the optimal levels to be attained. There is a continuous association between glucose levels and maternal and fetal outcomes, and this relationship is sig-nificant with fasting, 1 hour and 2 hours post glucose load. From a pathophysiologic perspective, postprandial hyperglycemia is the most frequent metabolic alteration in gestational diabetes. Diabetic patients, particularly type 1 diabetics, run with pre- and postprandial disorder. In the clinical setting, there is good data showing the role of postprandial glucose monitoring in the treatment of diabetes in pregnancy. Besides the fact that prandial state contributes more to the mean glucose level than fasting, it is accompanied by potentially detrimental alterations such as proinflammation and procoagulation. Besides, prandial glucose excursion is tightly related to glucose variability and there is data that suggest a negative correlation of this variability with fetal outcomes. The best time after the meal for the testing to be performed is also a matter of controversy. Main results will be presented and discussed. There is evidence of the relevance of both 2 and 1 hour monitoring. Traditionally, the 2 hour sample was the most utilized. More recently, the 1 hour testing became frequent and comparative studies were published. Some showed a similar correlation and others a better correlation for the 1 hour postprandial measurement. These results lead to several guidelines to recommend this sampling time.
HyPoGlyCaEmia in diaBEtiC PrEGnanCyElisabeth R MathiesenProfessor, Chief Physician. Dep. of Endocrinology, Rigshospitalet, Copenhagen, Denmark
Prevalence, predictors and pathophysiological factors involved in episodes of severe hypoglycaemia during pregnancy will be covered.
In women with type 1 diabetes, severe hypoglycaemia (hypoglycaemia with the need of help from third person) occurs three to five times more frequently in early pregnancy than in the period prior to pregnancy. Risk factors for severe hypoglycaemia during pregnancy include a history with severe hypoglycaemia in the year preceding pregnancy and impaired hypoglycaemia awareness. Pregnancy-induced nausea and vomiting seem not to be contributing factors. Severe hypoglycaemia is also seen in insulin treated women with type 2 diabetes.
Possible pathophysiological mechanisms involved in increased risk of severe hypoglycameia during pregnan-cy will be covered.
Pre-conception counselling, education with focus on the risk of hypoglycaemia, carbohydrate counting, use of insulin analogues, continuous subcutaneous insulin infusion (insulin pump) therapy and real-time continuous glucose monitoring with alarms for low glucose values might be relevant tools to obtain near-normoglycaemia without episodes of severe hypoglycaemia.
A decline in the prevalence of severe hypoglycaemia during pregnancy in women with type 1 diabetes with dedicated education of patients and caregivers and the use of modern insulin treatment has been documented.
ClosEd looP in PrEGnanCyHelen Murphy Professor of Medicine, University of East Anglia (UEA) & Honorary Consultant Physician Cambridge University NHS Foundation Trust, United Kingdom
Continuous glucose monitoring (CGM) has highlighted the gap that exists between our expectations of tight metabolic control and the realities of actually achieving this, particularly during type 1 diabetes pregnancy.
C1
C2
C3

22
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Clinical Updates22
Longitudinal measurements indicate that despite overall “good” HbA1c levels, pregnant women with type 1 diabetes spend 8 hours per day with blood glucose levels above the recommended targets. New closed-loop (CL) or artificial pancreas approaches integrate insulin pump delivery (CSII) with continuous glucose monitoring (CGM) via computerized algorithms.
The vital component of a CL system for use during pregnancy is a control algorithm which can function safely despite the physiological changes in glucose turnover, endogenous glucose production and insulin ki-netics. We have defined these changes in type 1 diabetes pregnancy and completed proof-of-concept studies evaluating overnight CL, in early (12-16 weeks) and late (28-32 weeks) gestation. Pilot feasibility studies de-monstrated near-normal overnight glucose control (85-100% time within the target range of 3.5-7.8mmol/l), during early and late gestation. In a subsequent 24-hour crossover study comparing CL vs. conventional CSII, CL achieved excellent overnight control (95-100% time in target), with 80% overall time in target, during meals, snacks and physical activity. Home studies evaluating the feasibility, safety and efficacy of CL in real-life home settings are underway. Ongoing studies also suggest that CL can be safely used during in-patient admissions to hospital maternity units, to maintain glucose control following antenatal steroids for fetal lung maturation as well as before, during and after delivery.
oBEsity and GEstational diaBEtEs: tHE sEarCH for tHE missinG linKs ContinUEsSilvia DaherLaboratory of Obstetrics Investigation, Department of Obstetrics, Universidade Federal de São Paulo, Brazil
Obesity is a risk factor for adverse pregnancy outcome. Outside of gestation, obesity is associated with dyslipidemia; hyperinsulinemia; vascular dysfunction; and low-grade chronic inflammation. This inflammatory process, which is originated in the visceral adipose tissue (VAT), is related to infiltration of proinflammatory macrophages, and is considered a major cause of obesity-related insulin resistance.
Successful gestation involves a complex and well tuned interaction between genetic and environmental fac-tors, cells and mechanisms. Inflammation and insulin resistance are part of the physiological changes associa-ted with a normal pregnancy, and seem to be exacerbated in maternal obesity. Besides innate (macrophages, neutrophils, eosinophils, mast cells, NK cells) and adaptive (CD4 T cells, CD8 T cells, regulatory T cells and B cells) immune factors, the adipose tissue has been considered an important link between these phenomena. Different studies suggest that in obese individuals, inflammatory cells infiltrate adipose tissue leading to an unbalanced production of adipokines, such as leptin, resistin, adiponectin, IL-6 and TNF-A.
Gestational diabetes mellitus (GDM), the most frequent endocrine disorder on pregnancy, is usually associa-ted with high body mass index (BMI). Similar to obesity, GDM is a complex disease involving several mediators and mechanisms, including inflammation and increased insulin resistance. The link between inflammation and GDM seems to be related to the actions of cytokines such as interleukin-6 (IL-6) and tumor necrosis factor (TNF)-A, which induce insulin resistance and stimulate the acute phase inflammatory response.
Screening for GDM is usually performed between the 24-28 weeks gestation when there is a significant in-crease in the production of placental hormones that lead to insulin resistance. However, some women develop GDM at an earlier gestational age, for reasons that are still unclear. These cases are frequently more severe and may involve different pathophysiological mechanisms.
Despite several studies on the role of adipokines and other proinflammatory mediators, the physiopathology of GDM and maternal obesity remain unclear. We have been investigating the most relevant mediators in obese women who develop GDM. In addition, we have been looking for adipokines that might be associated with early-onset GDM.
CliniCal UPdatE 2: trEatmEnt in diaBEtEs & PrEGnanCy
mEtformin in PrEGnanCy and BEyondJanet Rowan1, Lindsay Plank2, Jun Lu3, Victor Oblonkin3, Elaine Rush3
1National Women’s Health, Auckland City Hospital, NZ. 2University of Auckland, NZ. 3Auckland University of Technology, New Zealand
C4
C5

23
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Clinical Updates 23
Background: studies using metformin in pregnancy for women with GDM demonstrate that metformin is a suitable treatment option with respect to pregnancy outcomes. However, metformin crosses the placenta and there are limited offspring follow up data. Animal data report beneficial effects of metformin for the offspring if the fetus is in an environment of over-nutrition (obese mother, high fat diet) but adverse effects if metformin is administered to a normal mother.
Methods: in the Metformin in Gestational diabetes: The Offspring Follow Up (MiG: TOFU) study, offspring of women who were randomised to either metformin or insulin for treatment of GDM have been followed. Between September 2012 and June 2015, 99 offspring in the Auckland MiG cohort were seen at 8.9 years of age. Background information, maternal and child anthropometry, bioimpedence, child DXA, abdominal MRI, liver MRS and fasting bloods were collected.
Results: there were 54 and 45 offspring of the 733 women randomised to insulin or metformin, respec-tively, in the MiG trial. In this follow up subgroup, at enrolment, there were fewer Caucasian and more Asian women in the insulin vs metformin group (38.9% vs 55.6% Caucasian and 48.1% vs 31.1% Asian). The mothers in the insulin group had a lower recruitment BMI (32.0(6.3)kg/m2 vs 35.4(11.3)kg/m², p=0.08) and fasting plasma glucose (5.0(0.6)mmol/l vs 5.3(0.8) mmol/l, p=0.1). In the children, at 8.9(0.4) years of age, there were more male offspring in the insulin vs metformin group, 51.9% vs 37.8%, p=0.2. Overall, the insulin children were smaller, with BMI 17.7kg/m2 vs 19.3kg/m2, p=0.03. Body fat percent was 30.3% vs 32.0%, p=0.28 by DXA and abdominal fat percent was 32.3(10.9)% vs 36.0(14.1)%, p=0.16 by MRI. Fasting plasma glucose was 4.9(0.3)mmol/l vs 4.7(0.4)mmol/l. HbA1c was 35(3)mmol/mol in both groups, p=0.8.
Conclusion: at 8.9 years of age, offspring of women treated with metformin in the MiG cohort were bigger but had similar body fat percent compared with offspring of women treated with insulin alone. Measures of glucose tolerance were similar. These data support the safety of metformin treatment for women with GDM.
insUlin analoGUEsMaría Cristina FaingoldHead of the Endocrinology Service at Cesar Milstein Hospital. Director of the Endocrinology Career (Buenos Aires University). President of the Argentine Diabetes Society. Buenos Aires, Argentina
It is well established that poor control of glycosylated hemoglobin A1c (HbA1c), fasting plasma glucose, and postprandial glucose during pregnancy is associated with poor pregnancy outcomes1-2 and the frequency of pregnancy complications in women with pre-existing diabetes remains high3. Optimal glycemic control is cen-tral to reducing the likelihood of poor outcome but must be balanced against the risk of maternal hypoglycemia4, which can be a serious complication even resulting in maternal death, and is therefore one of the main concerns of treatment of pregnant women with diabetes
Short-acting soluble human insulin and intermediate-acting neutral protamine hagedorn (NPH) insulin have been and are being used in diabetic pregnancy given the label indication. However, the development of rapid-acting insulin analogues has provided greater choice for patients, with the potential benefits of less hypogly-cemia, better glycemic control5, and allow for more flexibility in mealtime administration than human insulins.
One large prospective randomized controlled trial has demonstrated the efficacy and safety of insulin aspart versus soluble human insulin, both used with NPH insulin, in pregnant women with type 1 diabetes5. This study resulted in a change in category from C to B for the use of insulin aspart in pregnancy as recommended by the Food and Drug Administration (FDA). A much smaller randomized controlled trial has compared insulin lispro (also category B) with soluble human insulin in 33 pregnant women with type 1 diabetes.
Both basal insulin analogues, insulins detemir and glargine, were currently category C.In 2011 was published the data of Insulin detemir in pregnancy-study6, that was a prospective study com-
paring insulin detemir with NPH in 310 pregnant women, and it demostrated that Insulin detemir can be used in pregnancy and is associated with less fasting hyperglycaemia than human insulin. With this study the EMA approved insulin detemir for its use in pregnancy and finally on march 2012 the FDA changed its category from C to B.
We can conclude that insulin lispro, aspart and detemir are safety for their use in pregnancy, but the final decision of which insulin is better must be taken together with the mother after informing her about risks and benefits of the available insulin preparations.
C6

24
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Clinical Updates24
REFEREnCES1. Suhonen L, Hiilesmaa V,Teramo K. Glycaemic control during early pregnancy and fetal malformations in women with type I diabetes mellitus. Diabetologia 2000; 43(1): 79-82.2. HAPO Study Cooperative Research Group; Metzger BE, Lowe LP, Dyer AR, et al. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med 2008; 358(19): 1991–2002.3. Dunne FP, Avalos G, Durkan M, et al. ATLANTIC DIP collaborators. ATLANTIC DIP: pregnancy outcome for women with pregestational diabetes along the Irish Atlantic seaboard. Diabetes Care 2009; 32(7): 1205-1206.4. Nielsen LR, Pedersen-Biergaard U, Thorsteinsson B, Johansen M, Damm P, Mathiesen ER. Hypoglycemia in pregnant women with type 1 diabetes: predictors and role of metabolic control. Diabetes Care 2008; 31: 9-1.5. Mathiesen ER, Kinsley B, Amiel SA, et al.; Insulin Aspart Pregnancy Study Group. Maternal glycemic control and hypoglycemia in type 1 diabetic pregnancy: a randomized trial of insulin aspart versus human insulin in 322 pregnant women. Diabetes Care 2007; 30(4): 771-776. 6. Mathiesen ER, Damm P, Jovanovic L, McCance DR, Thyregod C, Jensen AB, Hod M. Basal insulin analogues in diabetic pregnancy: a literature review and baseline results of a randomised, controlled trial in type 1 diabetes. Diabetic Medicine, Vol. 27, No. 6, 2011, p. 543-51.
trEatmEnt of Gdm WitH PartiCUlar EmPHasis on maCrosomia. tHE danisH ExPEriEnCEPer Ovesen Professor, Department of Obstetrics and Gynecology, Aarhus University Hospital, Skejby, 8200 Aarhus N, Denmark
From 1997 to 2010 the prevalence of gestational diabetes mellitus (GDM) has increased from 1.0% to 3.2% of all pregnancies in Denmark and is paralleling the obesity epidemic.
Women with GDM, including those who are treated, are at increased risk of having a macrosomic infant. At birth these neonates haves increased adiposity and are at risk for birth injury. Furthermore, these babies are at increased risk for developing obesity and glucose intolerance later in life. Fetal macrosomia therefore has been used as a primary outcome measure in the management of GDM.
Diet is the mainstay of treatment in GDM regardless whether pharmacologic therapy is introduced. Dietary control with a reduction in fat intake and the substitution of complex carbohydrates for refined carbohydrates seeks to achieve and maintain the maternal blood glucose profile essential during gestation.
The amount and distribution of carbohydrate should be based on clinical outcome measures as hunger, plasma glucose levels, weight gain and ketone levels but a minimum of 175 g carbohydrate per day should be provided. Carbohydrate should be distributed throughout the day in three small-to-moderate-size meals and in between two to four snacks. Because of the increased morning insulin resistance carbohydrate is often less well tolerated at breakfast than other meals. An evening snack may be needed to prevent accelerated ketosis overnight. If nutrition therapy fails to achieve normal blood glucose levels, insulin treatment is initiated.
Regular physical activity can help lower fasting and postprandial plasma glucose concentrations and may be used as an adjunct to improve maternal glycaemia.
Weight loss is not recommended in pregnancy however, for obese women with GDM, modest energy restriction by 30 % of estimated energy needs may improve glycemic control without ketones and reduce maternal weight gain.
The percentage of macrosomia infants weighing ≥4,500 g increased in Denmark (N=2.501.908 singletons) from 1.5% in 1973 to 4.3% in 2000. Hereafter there has been a fall in the percentage of macrosomic babies to 2.6% in 2013. This decrease in the number of macrosomic children in Denmark coincides with a national tighte-ning of treatment guidelines of GDM patients.
In a retrospective analysis of data from 1518 singleton pregnancies from our department, examining the effect of limited gestational weight gain after the diagnose of GDM on fetal growth, we found a gradual decrea-se from 2004 to 2014 in both birth weight (BW) and z-score for BW (taking gestational age and sex into account) with a fall from 0.60 to 0.09 or almost normal weight.
These observations show that it is possible to reduce the risk of macrosomia not only locally but also on a national scale, and thus contribute to prevent the obesity epidemic.
diaBEtEs and tHyroid aUtoimmUnity dUrinG PrEGnanCyJorge H. MestmanDepartment of Medicine and Obstetrics and Gynecology. Keck School Of Medicine, University Of Southern California, USA
C7
C8

25
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Clinical Updates 25
Since early pregnancy, the thyroid gland, starting at 4-6 gestation, increases the secretion of thyroid hormo-nes by 30 to 50% from basal, owing mainly to the hCG stimulating effects on the maternal thyroid gland. Thyroid hormones, thyroxine (T4) and Triiodothyronine (T3) cross the placenta, but only T4 is taking up by the fetal brain receptors. The fetal Hypothalamic- Pituitary-Thyroid axis becomes functionally active after gestational week 12 and is fully operative by week 18. The normal maternal thyroid gland is able to compensate for the increase in thyroid hormones demands, but in cases of thyroid gland pathology, such as chronic thyroiditis or previous thyroid ablation or iodine insufficiency, hypothyroidism develops. Some of the maternal, fetal and neonatal com-plications of untreated maternal hypothyroidism include: premature delivery, gestational hypertension, placental previa, children intellectual impairment, and brain structural changes later in life. The most common etiology of primary hypothyroidism is Chronic or Hashimoto’s Thyroiditis (CT); the incidence of euthyroid chronic thyroiditis in women during reproductive age varies between 5 and 15%. However the incidence of CT is significantly increased in women with DM1, it is estimated that 20-25% of them are affected. The American Diabetes Association (American Diabetes Association, Clinical Practice 2015) recommends screening for autoimmune thyroid disease at the time of DM1 diagnosis and periodically thereafter. The recommended blood tests are serum TSH and Thyroid Peroxidase Antibodies (TPOAb). If the serum TSH is outside reference range, the patient should be treated accordingly. In the presence of serum TSH within reference range but elevated TPOAb titers, it is recommended to repeat serum TSH every 6-12 months, since the presence of elevated serum TPOAb ti-ters is diagnostic of thyroid autoimmunity (CT) and a risk factor for development of thyroid dysfunction, mostly hypothyroidism. It is important to keep in mind the occurrence of other autoimmune endocrine diseases in patients with DM1, such as primary adrenal and ovary insufficiency, part of the Polyglandular Syndrome, the frequency in DM1 significantly less than thyroid autoimmunity.
One other complication frequently reported is postpartum thyroiditis, requiring a proper medical history and thyroid tests every 3 months for the first year after delivery.
In order to prevent pregnancy hypothyroidism in women at risk, a pre-pregnancy serum TSH ~1.0 IU/L is suggested, and the diagnosis of subclinical hypothyroidism in the first trimester of pregnancy is made, in most countries, when the serum TSH is >2.5 IU/L.
CliniCal UPdatE 3: tHE fEtUs and tHE offsPrinG
matErnal and PErinatal oUtComEs in PrEGnanCiEs WitH mild HyPErGlyCEmiaIracema Mattos Paranhos CalderonObstetrics Full Professor from Botucatu Medical School-Unesp, Brazil. Coordinator of the Reference Center of Diabetes and Pregnancy/Botucatu Medical School-Unesp (RCDP/BMS-Unesp), Brazil
Mild hyperglycemia in pregnancy is not defined, and much less a consensus. Gabe defined mild gestational diabetes mellitus (GDM) as OGTT-100g with two abnormal results and fasting glucose < 95mg/dL, and highlight the importance to treat Mild GDM to reduces fetal overgrowth, shoulder dystocia, and preeclampsia1.
Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study described the continuous association bet-ween maternal glucose concentrations and increasing birthweight, cord blood serum C-peptide levels. These associations were present at glucose levels currently lower than those used to diagnose GDM2.
Rudge et al. (1990)3 described a group of pregnant women with normal results of OGTT-100g and abnor-mal glycemic daily profile (GP), with fasting glucose ≥ 90 mg/dL and/or postprandial levels ≥ 130 mg/dL. Ac-cording these two tests, the pregnant women were classified into four groups: I-A, not diabetes, with normal OGTT and GP (N = 79, 41.2%); I-B, mild gestational hyperglycemia (MGH), with normal OGTT and abnormal GP (N = 63, 32.8%); II-A, GDM, with abnormal OGTT and normal GP (N = 18, 9.4%), and II-B, also GDM, with abnormal OGTT and GP (N = 32, 16.7%). Large for gestational age (LGA) newborns were similar in I-A and II-A groups (25.6 and 28.6%, respectively), and in the I-B (MGH) and II-B (GDM) groups (53.8 and 51.9% respectively). The authors proposed that MGH should be treated like GDM pregnant women, with a diet and exercise, and insulin when necessary, to achieves normal blood glucose levels3. Thus, since 1990, the RCDP/BMS-Unesp, Brazil, maintains the OGTT associated to GP as a routine to diagnosis of GDM and MGH, and treat MGH like GDM women4.
In Rudge’s I-B or MGH group perinatal mortality rate is 41‰, similar to that observed in diabetic group and 10 times higher than that found in non-diabetics pregnant women; the placental villi and villous vessels architecture are different from those seen in non-diabetic and diabetic groups, and suggest adjustment to keep
C9

26
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Clinical Updates26
up functional oxygen maternal-fetal exchange; maternal risk for hypertension, obesity and hyperglycemia are high and seemed to reproduce a model of metabolic syndrome, and finally, exhibits 16,7% of DM2, 10-12 years after index-pregnancy4-7 .
The results of HAPO study2 clearly revealed that levels of maternal hyperglycemia in the range of those used to establish the diagnosis of GDM and even lower do pose a health risk to the offspring of pregnant women. The new GDM diagnostic protocol, proposed by IADPSG8, was introduced in our RCDP/BMS-Unesp on August 15th, 2011, but the GP was maintained in association to OGTT-75g. With this new protocol, we asked if all I-B group or MGH pregnant women were classified into new criteria of GDM, the GP would not be necessary.
The results of a Master thesis compared the prevalence of GDM and MGH three years before and three years after IADPSG-protocol associated to GP (August, 2008-August, 2014). These results show an increasing in women with GDM (32,5 to 41.3%) similar to others studies, and no change in the MGH rates (22.5 to 18.6%) (data not yet published). Considering that the new limits and criteria of TTG-75g are not enough to identify all pregnant women at risk for hyperglycemia, we still keep the association OGTT-75g8 and GP) for GDM and MGH diagnostic, and treat MGH like GDM pregnant women.
REFEREnCES1. Landon MB. Is there a benefit to the treatment of mild gestational diabetes mellitus? Am J Obstet Gynecol. 2010 Jun; 202(6):649-53.2. Metzger BE, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, Coustan DR, Hadden DR, McCance DR, Hod M, McIntyre HD, et al: Hyper-glycemia and adverse pregnancy outcomes. N Engl J Med 2008, 358:1991-2002.3. Rudge MV, Peraçoli JC, Berezowski AT, Calderon IM, Brasil MA. The oral glucose tolerance test is a poor predictor of hyperglycemia during pregnancy. Braz J Med Biol Res. 1990;23(11):1079-89.4. Rudge MV, Calderon IM, Ramos MD, Abbade JF, Rugolo LM. Perinatal outcome of pregnancies complicated by diabetes and by ma-ternal daily hyperglycemia not related to diabetes. A retrospective 10-year analysis. Gynecol Obstet Invest. 2000;50(2):108-12.5. Rudge MV, Calderon IM, Ramos MD, Brasil MA, Rugolo LMS, Bossolan G, Odland JØ. Maternal daily hyperglycemia diagnosed by glycemic profile: a maternal and perinatal public health problem. Rev Bras Ginecol Obstet. 2005;27(11):691-7.6. Calderon IM, Damasceno DC, Amorin RL, Costa RA, Brasil MA, Rudge MV. Morphometric study of placental villi and vessels in wo-men with mild hyperglycemia or gestational or overt diabetes. Diabetes Res Clin Pract. 2007 Oct;78(1):65-71.7. Negrato CA, Jovanovic L, Tambascia MA, Calderon I de M, Geloneze B, Dias A, Rudge MV. Mild gestational hyperglycaemia as a risk factor for metabolic syndrome in pregnancy and adverse perinatal outcomes. Diabetes Metab Res Rev. 2008 May-Jun; 24(4):324-30.8. Metzger BE, Gabbe SG, Persson B, Buchanan TA, Catalano PA, Damm P, Dyer AR, Leiva A, Hod M, Kitzmiler JL, et al: International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in preg-nancy. Diabetes Care 2010,33:676-682).
fEtal sEx and BirtH WEiGHtRosa CorcoyServei d’Endocrinologia i Nutrició, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain. Departament de Medi-cina, Universitat Autònoma de Barcelona, Spain
Birth weight is an important pregnancy outcome since high and low values -crude or assessed after custo-mized growth charts- are predictors of health problems in the neonatal period and later in life. The simplicity of its measurement adds to its importance.
Birth weight is the sum of multiple factors. It is influenced by fetal genome, maternal factors (conveying environmental influences) and function of placenta (which shares fetal genome and is a mediator of maternal factors). Sex is one of the elements of fetal genome affecting birth weight. On the other hand, birth weight is one of the numerous pregnancy outcomes influenced by fetal sex (including congenital malformations, preterm delivery, cord problems, and perinatal mortality).
Differences in birth weight according fetal sex has being recognized for long time with term male newborns weighing on average ≈125 g more than female newborns. It can be intuitively hypothesized that male and female fetuses exhibit a differential response to factors influencing growth. Current evidence supports this hypothesis but maternal characteristics do not have uniform additive effects. In a study that addressed single-ton uncomplicated pregnancies, increasing maternal weight and height had a higher influence on birth weight in males than in females. The associations were non-linear and the main influence was displayed at different periods of pregnancy. A number of interactions did also take place with male newborns being more sensitive to maternal weight among shorter mothers and more responsive to maternal height among lighter mothers.
In pregnancies affected by comorbidities, birth weight is not homogenously affected in male and female fetuses. The risk of high birth weight in mothers with gestational diabetes is higher in male fetuses with di-vergent reports in pregestational diabetes. On the other side, the risk of intrauterine growth restriction has a
C10

27
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Clinical Updates 27
sex-dimorphic pattern that differs according to the condition: male fetuses are more susceptible to tobacco and caffeine while female fetuses are more sensitive to the growth restricting effects of hypertension.
Although mechanisms are incompletely understood, we have some insights that point to hormones (andro-gens, IGF axis, insulin sensitivity and response to glucocorticoids) and cytokines. Interestingly, the gender gap in birth weight has been reported to display a negative temporal trend, tentatively attributed to antiandrogenic endocrine disruptors.
dEliVEry in diaBEtiC WomEnNatalia BasualdoChief of Tocogynecology Department, Sanatorio Anchorena, Member of SAD and SOGIBA Committees. Buenos Aires, Argentina
The delivery in women with diabetes requires an integrated and evidence-based management. A balance
between fetal lung maturity, gestational age, glycemic control obstetric history, estimated fetal weight, fetal and maternal comorbidities and preferences of the family.
1. Fetal lung maturation: maternal hyperinsulinemia and hyperglycemia inhibit fetal cortisol, decreasing pro-duction of fetal lung surfactant. Respiratory Distress Syndrome Newborn (SDR) is the leading cause of morbidi-ty, mortality and admission to neonatal units in this group of patients. Documented a delay in biochemical and physiological processes, it is estimated that pregnant women with diabetes, surfactant production is guaran-teed only after the 38.5 weeks. In cases where termination of pregnancy is 34 weeks before the administration of betamethasone improved perinatal outcome. It must be controlled by the risk of hyperglycemia.
2. Gestational age: between 37 and 38.6 weeks increases neonatal morbidity. Birth in week 39 is conside-red as a good practice, especially in women with a favorable cervix. If the cervix is unfavorable , glycemic control is good ,and there is not other obstetric pathology, the spontaneus onset of labor can expect until 40 weeks. In women with pre-gestational diabetes with vascular complications consider delivery between weeks 37 and 39.
3. Monitoring glycemic: it is essential to know the metabolic status of these women.4. Obstetric history: consider the parity, previous fetal mortality, preterm children, number of previous C-
sections.5. Fetal weight: estimation by ultrasound has an error of 15%, however, performing a fetal weight estimation
by ultrasound around 38 weeks is recommended.6. Comorbidities: the association with other diseases, such as preeclampsia or vascular disease worsens
the prognosis and increases the rate of cesarean sections.7. Preferences families: from the paradigm family centrered care is basic to know the preferences, family
values and fears in order to allows, greater confidence in the team and consensus decision-making and eviden-ce based.
Pregnancy termination criteria:- Poor metabolic regulation.- Bishop Score >6.- Obstetrical pathology that requires birth.- Severe fetal maternal comorbidity .- 40 weeks.Birth:- If the PFE is greater than 4500 grams a c-section is the choice.- In women with fetal weight calculation between 4000-4499 grams, consider obstetric history, pelvimetry
and progress of labor.- The vaginal delivery of a big baby in the context of a patient with diabetes is associated with an increased
risk of intrapartum trauma.- Expectant management has proven to be cost effective.- Is not more effective elective termination.- No more effective caesarean section.- Diabetes is not a contraindication for vaginal delivery in women with a previous cesarean.- The need to agree on all decisions on pregnancy termination, detailing the risks and benefits to mothers
and their families is strongly recommended.
C11

28
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Clinical Updates28
imPaCt of EdUCational ProGramsSilvia Gorbán de LapertosaFull Professor, Nutrition and Education for Health, Medicine School, Northeast National University, Argentina. Vice Chairman, Diabetes & Woman Group, IDF. Vice president, Diabetes & Pregnancy Group, ALAD
World Healht Organization’s action plan for noncommunicable diseases prevention and control during 2013-2020 has the objective: To reduce the preventable and avoidable burden of morbidity, mortality and disability due to noncommunicable diseases by means of multisectoral collaboration and cooperation at national, regional and global levels, so that populations reach the highest attainable standards of health and productivity at every age and those diseases are no longer a barrier to well-being or socioeconomic development. These objectives should be considered throughout the lifecycle, empowering people and communities with strategies based on scientific evidence, being therapeutic education a valid tool for achieving these objectives.
The fulfillment of planned objectives could be achieved throughout education of mothers to prevent the de-velopment of gestational diabetes and diabetes in the future and also, working for the scheduled pregnancy and promotion of lifestyle changes for children and adolescents who had high or low birth weight assist in meeting objectives. Therapeutic education is an ongoing process that must be done by the health team and treatment should be integrated. Therapeutic education programs in pregnant women with diabetes focus on the person as protagonist of a permanent intervention that involves contact to a trained health team, enabling her to agree on a specific treatment plan. The person with diabetes needs to acquire extensive knowledge and develop skills, besides having positive attitudes that enable sound decisions regarding lifestyle, treatment and prevention of complications, to facilitate and improve control her illness and perinatal outcomes.
Education can be performed on individual high-risk obstetric outpatient consultation or group sessions of 3-8 hours. The contents are developed through participatory activities, demonstrations, educational games and physical activity. Meal plans are discussed with card games. We evaluate using knowledge questionnaires, de-pression (WHO5), quality of life (EQ-5D) and satisfaction before and after the educational intervention. Medical students make home visits to assess progress and appoint retesting visits. We evaluated process indicators, with reduced cesarean rates and hospitalization in neonatology.
Finally, a text message system with treatment adjustment is implemented by such means. This therapeutic strategy has a positive impact on health care costs by reducing hospital days, the workload of health workers and greater satisfaction for women and their families.
HyPErGlyCEmia in PrEGnanCy in tHE amEriCas: sitUation analysis and Call for aCtionAlberto BarcelóRegional Advisor, Pan American Health Organization/World Health Organization, Washington DC, USA
Worldwide, it is estimated that one in ten women who are pregnant develop hyperglycemia, 90% of which may be Gestational Diabetes Mellitus (GDM). The proportion of affected women may be as high as 30% of pregnancies, but many cases of GDM remain undiagnosed with potentially life-threatening consequences for mother and child. Data on the frequency of gestational diabetes is scarce, as there is no worldwide uniform approach towards screening and diagnosing gestational diabetes. In 2013, the World Health Organization (WHO) published the document Criteria for the Diagnosis and Classification of Hyperglycemia First Detected during Pregnancy. This guideline is aimed at health professionals who care for pregnant women, most often prima-ry care physicians, obstetricians and gynecologists. We conducted a cross sectional survey among all PAHO Member States on the different aspects of diabetes related to pregnancy. Data from 28 countries was received. Overall 50% of countries reported having policies in place to screen women for diabetes during pregnancy but only three countries reported GDM prevention programs on a national level. Six countries were implementing institutional GDM educational programs. The total number of live births reported by countries, with available national information, was 1,788,135. The total combined prevalence of LGA and SGA was 8.7% and 7.9% res-pectively. Among countries reporting national data, the percentage of diagnosed GDM varied between 0.8% in Belize and 6.5% in Canada, while the prevalence of DM during pregnancy varied between 5.3% in Chile and 0.4% in Cuba. The survey demonstrated a lack of data necessary for monitoring GDM in many countries. It was also observed that almost half of reporting countries did not have policies to screen women for GDM. Although
C13
C12

29
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Oral Presentations 29
educational programs targeting type 2 diabetes are widely available throughout the Americas, there is a lack of prevention and educational programs for GDM. A Call-for-Action was published recently encouraging countries to screen women for GDM as well as to start prevention and control programs.
oral PrEsEntations
CytoCHromE C oxidasE ExPrEssion in EmBryos from diaBEtiC rats is rEGUlatEd By matErnal trEatmEnts WitH CHia oil and idEBEnonERomina Higa, Sabrina Roberti, Ivana Linenberg, Alicia JawerbaumLaboratory of Reproduction and Metabolism, CEFYBO-CONICET, University of Buenos Aires, Buenos Aires, Argentina
Introduction: maternal diabetes induces an increase in embryo malformations, and oxidative stress seems to have a teratogenic role. COXIV is the last component of the electron transport chain in mitochondria. Dys-function of this complex is associated with increased mitochondrial reactive oxygen species production. Chia oil is enriched in linolenic acid, an n-3 PUFA that potently activates PPARdelta, a nuclear receptor involved in developmental and antioxidant processes. Idebenone is a coenzymeQ analogue, acting both as an antioxidant and as a transporter in the electron transport chain in mitochondria.
Aims: 1) to evaluate whether embryonic COXIV expression is modulated by a maternal 6% chia oil-supple-mented diet in control and diabetic pregnant rats. 2) To analyze the effect of idebenone administration to control and diabetic pregnant rats on COXIV and PPARdelta expression as well as on the apoptotic rate in embryos during early organogenesis.
Methods: diabetes was induced by neonatal streptozotocin administration (90 mg/kg). Adult control and dia-betic female rats were mated with healthy males. From days 0.5 to 10.5 of pregnancy rats, were treated with: 1) a diet supplemented or not with 6% chia oil, 2) idebenone (100 mg/kg) or vehicle. Embryonic expression of PPARdelta and COXIV was measured by PCR and apoptosis by TUNEL.
Results: we found decreased expression of PPARdelta and COXIV (p<0.05), and increased apoptotic rate (p<0.01) in embryos from diabetic rats compared to controls. Maternal treatments with chia oil (enriched in PPARdelta activators) increased COXIV expression (p<0.01) in embryos from diabetic rats. Maternal treatment with idebenone increased both PPARdelta and COXIV expression (p<0.05). In addition, maternal treatment with idebenone prevented the increased apoptotic rate (p<0.05) in embryos from diabetic rats.
Conclusion: alterations in COXIV expression were found in embryos from diabetic rats and can be mo-dulated by a diet enriched in PPARdelta activators, suggesting that maternal treatments with idebenone may restore COXIV via a PPARdelta pathway. Idebenone also reduced the diabetes-induced increase in the embryonic apoptotic rate, suggesting that mitochondrial-induced oxidative stress is a relevant component in diabetic embryopathy.
altErEd GlUCosE and liPid HomEostasis in adUlt rats rElatEd to sUCrosE-riCH diEt dUrinG Early staGE of lifE: EffECt of salBa (salVia HisPaniCa l) aftEr WEaninGMaría Alejandra Fortino, Silvia Rodríguez, Yolanda B. Lombardo, Adriana G. ChiccoUniversidad Nacional del Litorial, Argentina
Introduction: energy intake and macronutrient composition during preconception, pregnancy or pregnancy and lactation (P+L) have been related to nutritional programming. Previous studies showed that early life expo-sure (P+L) to a sucrose rich diet (SRD) is associated with changes in lipid and glucose metabolism, leading to an unfavorable profile in adulthood, regardless of whether offspring consumed an SRD after weaning. Although the alterations resulting from nutrient-fetal programming have been considered as irreversible changes, some studies have addressed the capacity of the postnatal environment, to either exacerbate or attenuate program-med outcomes. In this regard n-3 polyunsaturated fatty acids (PUFAs) from marine source, consumed from weaning to adulthood, overcome dyslipidemia and liver steatosis induced by maternal and post-weaning SRD. Another important source of n-3PUFAs is alpha linolenic acid (ALA, 18:3 n-3) which derives from plant source. ALA administration is associated with decreased plasma lipid concentration and increased peripheral insulin
o1
o2

30
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Oral Presentations30
sensitivity. The seed of Salba, commonly named chia seed, contains the richest botanic oil source of ALA.Objective: analyze whether the effect of dietary chia seed during post-weaning result in an amelioration of
fetal programming induced by a maternal sucrose-rich diet.Materials and methods: during P+L, female rats were fed either a SRD or a standard powdered rodent
commercial diet (reference diet: RD). Energy% was: 60 sucrose; 23 corn-oil (rich in n-6 fatty acids), 17 protein in SRD and 60 starch, 23 corn oil, 17 protein in RD. After weaning, male offspring from SRD dams were fed a RD, SRD or SRD in which chia seed replaced corn oil as fat source (SRD-C). All groups were fed up to 150 days of age, forming the SRD-RD, SRD-SRD and SRD-SRDC groups respectively. The offspring from RD dams conti-nued with RD, forming the RD-RD group. At 150 days of age in offspring of each group we analyzed: anthropo-metric measurements, visceral adiposity (VA), carcass composition, plasma triglyceride (Tg), FFA, and glucose levels; VLDL-Tg secretion rate, intravenous fat tolerance test (K2 %min-1), glucose and insulin tolerance test.
Results: the results showed: 1- body weight, energy intake and anthropometric measurements were similar in all groups, although VA and carcass fat content were higher (p<0.01) in the offspring from SRD dams inde-pendently of the post-weaning diet. 2- Plasma Tg values were (mM): RD-RD: 0.70±0.05; SRD-SRD: 1.42±0.12; SRD-RD: 1.20±0.11; SRD-SRDC: 0.72±0.05 (p<0.05 SRD-SRD and SRD-RD vs RD-RD and SRD-SRDC). The nor-malization of plasma Tg in the SRD-SRDC group was in agreement with VLDL-Tg secretion rate and a K2 %min-1. The increased levels of plasma FFA observed in the SRD-SRD group was significant decreased (p<0.05) when RD or SRD-C were consumed after weaning. However, in both groups, (SRD-RD and SRD-SRDC) plasma FFA were still significant different from RD-RD group. Plasma glucose levels return to normal values only when chia seed was present after weaning. Values expressed as mean ± SEM (n=8) (mM): 6.19±0.26 in RD-RD, 7.49± 0.26 in SRD-SRD, 7.17± 0.29 SRD-RD and 6.59 ± 0.40 in SRD-SRDC (p< 0.05 SRD-SRD and SRD-RD vs RD-RD and SRD-SRDC). These results were accompanied by a complete normalization of KITT and a significant ame-lioration of Kg only in SRD-SRDC group.
Conclusion: taking all the results together this work signals that the incorporation of chia seed as source of fat (rich in 18:3 n-3 fatty acids, fibers, proteins, mineral, antioxidants and isoflavons) after weaning is a feasible interventional strategy that could prevent and/or reduce the outcomes induced by a sucrose-rich diet from the onset of pregnancy until adulthood in offspring.
rEdUCEd insUlin sEnsitiVity PrEdiCts adVErsE oUtComEs in WomEn WitH GEstational diaBEtEs mEllitUsCamille Powe1, Catherine Allard2, Marie Claude Battista2, Myriam Doyon2, Luigi Bouchard2, Patrice Perron2, José Florez1, Ravi Thadhani3, Marie France Hivert41Diabetes Unit, Massachusetts General Hospital. 2Universite de Sherbrooke, Quebec, Canada. 3Department of Population Medicine, Harvard Pilgrim Healthcare Institute. 4Harvard Medical School, USA
Introduction: hyperglycemia in both pregnant and non-pregnant individuals results from insufficient insulin secretion, reduced insulin sensitivity, or a combination of both processes. However, the relative degree to which insufficient insulin secretion and/or reduced insulin sensitivity contribute to gestational diabetes mellitus (GDM) pathogenesis has not been firmly established.
Objectives: 1) to define pathophysiologic subtypes of GDM, according to the presence of insufficient in-sulin secretion and/or reduced insulin sensitivity. 2) To determine whether pregnancy outcomes differ among these subtypes.
Methods: among 809 pregnant women in the Gen3G cohort (Quebec, Canada) we obtained multiple blood glucose and insulin measurements during a 75 g OGTT performed at 24-30 weeks gestation. The Matusda index and the Stumvoll 1st phase estimate were used as estimates of insulin sensitivity and insulin secretion, respectively. In women with GDM (determined by IADPSG criteria), we considered a defect in insulin sensitivity and/or secretion to be present if insulin sensitivity and/or secretion was below the 25th percentile, defined in women with normal glucose tolerance (NGT). Women were placed in the GDM-Sensitivity group if there was an isolated insulin sensitivity defect, the GDM-Secretion group if there was an isolated insulin secretion defect, and the GDM-Mixed group if both defects were present.
Results: of 67 women with GDM, 51% were in the GDM-Sensitivity group, 30% were in the GDM-Secre-tion group, and 18% were in the GDM-Mixed group. Compared to women with NGT, the GDM-Sensitivity group had higher 1st trimester BMI (median [IQR], 30.1 [26.9-37.7] kg/m2, NGT: 23.9 [21.5-27.5] kg/m2, P<0.001) and higher fasting glucose (90 [81-94], NGT: 76 [70-79] mg/dl; P<0.001), while the GDM-Secretion group had a trend
o3

31
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Oral Presentations 31
toward lower 1st trimester BMI (21.9 [20.7-26.0] kg/m2, P=0.15 versus NGT) and normal fasting glucose (76 [72-79] mg/dl, P=0.91 versus NGT). Infants of GDM-Sensitivity women had higher birth weight z-scores than the infants of NGT women (0.57 [-0.01-1.37] versus 0.03 [-0.53-0.52] in the NGT group, p=0.001), were more likely to be large for gestational age (LGA) (26.5% versus 6.3% in the NGT group, P<0.001), and were more likely to be delivered by cesarean-section (33.3% versus 15.2% in the NGT group, P=0.03). After adjustment for 2nd trimester BMI, the increased risk of cesarean section in the GDM-Sensitivity group (as compared to the NGT group) was attenuated (P=0.06), while differences in birth weight z-score, and risk of LGA remained significant (P<0.03 for both compared to NGT group). Infants of GDM-Secretion women (compared to NGT women) had similar birth weight z-scores (0.20 [-0.54-0.86], P=0.71 versus NGT), similar risk of LGA (10.0%, P>0.99 versus NGT), and were not significantly more likely to be delivered by cesarean-section (20%, P>0.99 versus NGT). Lower insulin sensitivity was associated with higher infant birth weight among women without GDM, indepen-dent of maternal BMI (P=0.01).
Conclusions: there is pathophysiologic heterogeneity among women with GDM with regard to underlying insulin sensitivity and insulin secretion defects. GDM with reduced insulin sensitivity carries an increased risk of adverse perinatal outcomes.
Funding: fonds de recherche du Québec en santé #20697 (M.-F.H.); Canadian Institute of Health Research #MOP 115071 (M.-F.H.); Diabète Québec grant (P.P.); ADA Accelerator Award #1-15-ACE-26 (M.-F.H.); NIDDK T32 DK007028-41(C.E.P).
PrEValEnCE of Gdm and maCrosomia in an arGEntinian CoHort aCCordinG to alad and iadPsG diaGnosis CritEriaStella M. Sucani1, María Natalia Maccio1, Irene Coniberti1, Adriana Bartolin1, Estrella Silvia Zamory1, María Laura Lewin2, Darío Aguera2, Rosana Fullone2, Mercedes García Richter2, Graciela Murno2, Corina Yanarella2, María Inés Argerich3, Raúl David3, Silvia Gorbán de Lapertosa4, Claudia Pare4, María Marta Curet5, Mónica Rosana Virga6, Mónica Chiocconi6, María Celeste Goedelmann6, Patricia Glikman6, Alicia Gauna6, Alejandro Hakim6, Susana Martínez6, Gabriela Malfetano6, Gustavo Pintos6, Gabriela Portunato6, Claudia Scalise6, Magdalena Rey7, Josefina Bomarito7, María Paula Esteban7, Ricardo H Illia7, Guillermo Lobenstein7, María Pía Lozano Bullrich6, María Paz Martínez7, Magdalena Menises7, Josefina Pozzo7, Silvana Maniá8, Fabiana Masjoan9, Carolina Fux Otta10, Rodolfo Mengual10, Liliana Cervetta10, José María Ochandorena Martin11, Liliana Propato11, Sandra Rove-da11, Lorna Gómez Ponce11, Marta Gómez Flores11, Carolina Farias12, Celina Bertona13, Jorge Alvariñas14, María Cristina Faingold14, Myriam Liliana Glatstein14, Claudio Daniel González14, Susana Salzberg14, Alicia Jawer-baum14, Gabriela Rovira15
1Hospital Materno Provincial Dr. R. F. Lucini, Córdoba. 2Hospital Municipal Dr. R. Santamarina, Bs. As. 3Hos-pital Perrupato San Martín, Mendoza. 4Hospital JR Vidal, Corrientes. 5Hospital Regional Ramón Carrillo, San-tiago del Estero. 6Hospital Ramos Mejía, Bs. As. 7Hospital Alemán, Bs. As. 8Maternidad Municipal Eva Perón Malvinas Argentinas, Bs. As. 9Hospital JB Iturraspe, Santa Fe. 10Hospital Universitario de Maternidad y Neona-tología, Córdoba. 11Hospital Materno Neonatal Dr. Ramón Carrillo, Córdoba. 12Maternidad Provincial 25 de Mayo.13Coordinadora Mendoza. 14Comité Asesor .15Comité de Diabetes y Embarazo
Introduction: GDM diagnosis is a controversial issue. The Argentine Society of Diabetes recommend the use of ALAD guidelines for GDM diagnosis and to perform studies designed to address whether maternal and fetal risks varies according to the GDM diagnostic criteria in our population. The purpose of this work was to evaluate prevalence of macrosomia and GDM following both ALAD and IADPSG criteria in 1037 pregnancies in Argentina.
Methods: prevalence of GDM and macrosomia was evaluated in a prospective cohort including 1037 pregnancies, in Argentinian pregnant women. The 1037 pregnant women belong to different Argentinian cen-ters. OGTT (75 g glucose-time 0, 60 min and 120 min) was performed on 24-28 weeks of pregnancy and if negative, repeated in those with risk factors at 31-33 weeks of gestation. For diagnosis and treatment ALAD guidelines were followed: 2 fasting glucose values greater than or equal to 100mg/dl o OGTT values at 120 min postcharge greater than or equal to 140mg/dl detects ALAD-diagnosed GDM patients. IADPSG diagnosis was performed with two fasting values greater than or equal to 92 mg/dl and < 126 mg/dl, or with OGTT values at 0 min greater than or equal to 92 mg/dl, at 60min greater than or equal to 180 mg/dl or at 120min greater than or equal to 153 mg/dl.
Results: GDM prevalence was 9.86% following ALAD criteria and 24.8% following IADPSG criteria (Kappa
o4

32
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Oral Presentations32
coefficient 0.49, p<0.001). Macrosomia was observed in 7.23% of the studied pregnant woman (total studied population), in 12.74% of the ALAD-diagnosed GDM patients (p<0.05 vs total population) and in 11.24% of the IADPSG-diagnosed GDM patients (p<0.05 vs total population). No significant difference (p=0.71) was observed in macrosomia between ALAD and IADPSG-diagnosed GDM patients. All macrosomic babies in ALAD-diagno-sed GDM group were also IADPSG positive. Macrosomia in women who had fasting glucose levels between 92 and 99 mg/dl was 9.9% (p=0.34 vs total population). Only 4% of macrosomia was detected by the 60 min OGTT value in the IADPSG-diagnosed group. Positive predictive value of macrosomia was 17.9% in ALAD-diagnosed patients and 11.2% in IADPSG-diagnosed patients.
Conclusions: despite an important increase in GDM prevalence in the IADPSG- diagnosed group, no di-fference in macrosomia rate was detected compared to the ALAD-diagnosed group. This was observed even when only those women that were diagnosed by ALAD criteria were treated. Considering this and that positive predictive values are higher with ALAD criteria, our results do not suggest beneficial effects of using IADPSG criteria to detect macrosomia as a common adverse fetal outcome, although other adverse fetal and maternal outcomes deserves further research.
fEEdinG PraCtiCEs and tHEir assoCiation WitH adiPosity dUrinG tHE first yEar of lifE Ameyalli Rodríguez Cano, Karina Caballero Guzman, María Angélica Reyes López, Otilia Perichart Perera, Cinthya Muñóz ManriqueInstituto Nacional de Perinatología, México
Introduction: the first 1.000 days of life is a critical period where diet could influence adiposity and risk of chronic diseases later in life.
Objective: to evaluate the association between feeding practices and adiposity during the first year of life. Methodology: we studied the newborns from a prospective cohort of healthy pregnant women at the
National Institute of Perinatology (México City). All children included were healthy, full term babies. Adiposity markers were performed at 1, 3, 6 and 12 months: weight, waist circumference (WC), subscapular, triceps and biceps skinfold thickness (SFT), body mass index for age (BMI) and fat mass percentage (%FM). A feeding practices questionnaire was applied to mother at all visits to identify breast (BF), formula (FF) or mixed (MF) feeding, and the time of initiation of complementary feeding (CF). Descriptive statistics and frequencies were performed and mean differences were analyzed using Student´s t-test or U Mann-Whitney. A p-value <0.05 was considered statistically significant.
Results: a total of 105 babies were included. At birth, 6.2% of infants presented overweight risk; none had overweight/obesity. The prevalence of overweight risk was: 7.5%, 16.9%, 12.1% and 12.9% for 1, 3, 6 and 12 months; and prevalence of overweight/obese was: 1.3%, 4.9%, 6% and 6% respectively. BF rate decline over time: at 1m 93.6% received breast milk; at 3m 81.5%; 66.7% at 6m; and 31.6% at 12m. Conversely, FF increa-sed: 54% at 1m, 60.3% at 3m; 65.9% at 6m; and 40.2% at 12m. Before 4m, 28.9% had started CF, 64.8% started between 4-6m and 6.3% started after 6m. There were no differences between adiposity and type of lactation at 1m. At 3m, BF children had higher %FM (26.7%) compared with FF infants (22.3%), and also higher than those receiving MF (23.5%) (BF vs FF p=0.009, BF vs MF p=0.019). At 6m, WC, BMI and %FM were also higher in the BF group compared to the FF group (WC-cm: BF 40.7 ±3.14, FF 38.9 ±2.42, p=0.01; BMI-z score: BF 0.47 ±1.22, FF -0.11 ±1.09, p=0.042; %FM: BF 28.5 ±5.35, FF 22.9 ±6.07, p=0.00). At 12m, there were no differences between children who were still receiving breastfeeding and those were not. At 12m, WC was hig-her in children who started complementary feeding before 4m (<4m 42.6 ±3.62 vs 4-6m 40.6 ±2.74, p=0.009).
Conclusion: breastfeeding promotes increased adiposity during the first 6m of life, which might be a pro-tective factor. The early start of complementary feeding seems to increase WC at 12m.
PHasE 1 BiomarKEr trial: idEntifiCation and Validation of matErnal Plasma Exosomal BiomarKErs in PrEGnanCiEs diaGnosEd WitH GEstational diaBEtEs mEllitUsGregory Rice1, Katherin Scholz Romero1, Sherri Longo2, Gregory Duncombe1, Sebastián Illanes3, Carlos Salomon1
1Exome Biology Laboratory, UQ Centre for Clinical Research, Brisbane, Australia. 2Maternal-Fetal Medicine, De-partment of Obstetrics and Gynecologu, Ochsner Clinic Foundation. 3Department of Obstetric and Gynaecology, Universidad de Los Andes, Chile
o5
o6
33
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations 33
Currently, there is no reliable early detection test available to identify pregnant women who are at risk of developing gestational diabetes mellitus (GDM). The aim of this project is to test the hypothesis that women at risk of developing gestational diabetes can be identified at 11 to 14 weeks of pregnancy using a multivariate index assay that combines maternal biophysical and biochemical variables, and placental exosomal biomarkers. A prospective cohort of patients was recruited and blood collected at three time points during pregnancy for each patient (i.e. 11-14, 22-24 and 32-36 weeks gestation). Women (n=500) were recruited between January 2008 and December 2010 with informed, written consent, by research midwives from the Hospital Parroquial de San Bernardo, Santiago, Chile. A retrospectively stratified study was designed involving normal healthy preg-nant women (n=13) and GDM (n=7) patients, matched for age, gestational age, parity and BMI. Gestational age and pregnancy status were identified as significant factors contributing to variation in plasma exosome concen-tration (ANOVA, p<0.05). Post-hoc analyses established that PdE concentrations increased during gestation in both normal and GDM pregnancies, however, the increase was significantly greater in GDM (~2.2-fold, ~1.5-fold and ~1.8-fold greater at each gestational age compared to normal pregnancies). The sensitivity and specificity of exosomes number as a predictor for GDM was also examined by performing ROC curve analysis. The number of observations (i.e. 7 GDM and 13 normal pregnant women) in the present study limit the generation of robust estimates of Sensitivity and Specificity. We, however, as a proof-of-principle exercise, generated a multivariate index assay based on exosome number (placental and total) and gestational age (trimester). The model delivers an area under the curve of >0.95 and at a cut-off value on 0.49 (predicted posterior probability value) has a sensitivity = 85.7% and specificity = 89.7%. The model was cross-validated (2-fold) and as anticipated (given the small number of observations) degraded slightly (AUC= 0.78, sensitivity=0.89, specificity = 0.68). While the role of exosomes during GDM remains to be fully elucidated, exosome profiles may be of diagnostic utility for screening asymptomatic populations.
PostEr PrEsEntations
sEssion a: Gdm: diaGnosis and PrEValEnCE
tHE PrEValEnCE of GEstational diaBEtEs in a soUtH afriCan PoPUlationSumaiya Adam, Paul RheederUniversity of Pretoria, South Africa
Introduction: the prevalence of gestational diabetes (GDM) is increasing as the prevalence of Type 2 diabe-tes mellitus and obesity increases. South Africa is now amongst one of the most obese nations in the world. Current national guidelines recommend risk factor based screening. There is no consensus on the method of screening with each centre choosing criteria on personal preference and experience. There is now global con-sensus on adopting the one-step 75g-2hour oral glucose tolerance test (OGTT) and using the IADPSG recom-mendations for diagnosis of GDM.
Objective: to describe the prevalence of GDM according to the IADPSG criteria (fasting glucose ≥5.1mmol/l, 1h glucose ≥10mmol/l, 2h glucose ≥8.5mmol/l) and compare it to that found with the commonly used in Sou-th Africa 1998 WHO criteria (fasting glucose ≥7.0mmol/l, 2h glucose ≥7.8mmol/l) and the 2006 WHO criteria (fasting glucose ≥5.3mmo/l, 1h glucose ≥10mmol/l, 2h glucose ≥8.6mmol/l). To investigate the sensitivity and specificity of traditional risk factors in identifying patients at risk of GDM.
Materials and methods: we enrolled 833 pregnant women in the study thus far. Non-diabetic pregnant wo-men were screened for GDM using a 75g-2h OGTT between 24 and 28 weeks gestation at an antenatal clinic in Johannesburg, South Africa. The currently is on-going.
Results: thus far 428 women have completed the OGTT. All patients in the study were Black Africans. The mean age was 27.2 years. The average HbA1c was 34.4mmol/mol (5.3%). Twenty two patients had an HbA1c ≥38.8mmol/mol (5.7%). According to the 1998 WHO criteria 32 patients (7.5%) had GDM. Thirteen patients had GDM according to the 2006 WHO criteria. When employing the IADPSG criteria 129 patients (29.4%) were diagnosed with GDM. Two hundred and eighty one patients (65.7%) had at least one risk factor (age ≥35years, obesity, glycosuria, history of stillbirth, congenital anomalies or GDM, or positive family history) present. The sensitivity of risk factors in screening for GDM was 0.690 and the specificity was 0.358.
Conclusion: the prevalence of GDM is increased 4-fold when using the IADPSG criteria. Risk factors are a poor screening tool. Larger studies are required to determine the prevalence of GDM in South Africa and to recommend suitable guidelines for the screening of GDM.
Pa1

34
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations34
sUrVEy By tHE EUroPEan Board and CollEGE of oBstEtriCs and GynaEColoGy on sCrEEninG for GEstational diaBEtEs in EUroPEKatrien Benhalima1, Van Assche André2, Peter Damm3, Mathieu Chantal1, Devlieger Roland2, Mahmood Tahir4, Dunne Fidelma5
1Department of Endocrinology, Uz Gasthuisberg, Ku Leuven, Belgium. 2Department of Obstetrics & Gynecology, Uz, Gasthuisberg Ku Leuven, Belgium. 3Department of Obstetrics, Rigshospitalet, University od Copenhagen, Denmark. 4Department of Obstetrics & Gynecology, Victoria Hospital, Kirkcaldy, Scotland, UK. 5Galway Diabe-tes Research Centre, National University of Galway, Ireland
Introduction: more uniformity is necessary in screening for gestational diabetes (GDM) across Europe. Recently a steering committee appointed by the European Board and College of Obstetrics and Gynaecology (EBCOG) recommended to use the 2013 WHO criteria for the diagnosis of GDM in Europe.
Objectives: the aims of this work are: 1) to evaluate the current recommendations for GDM screening across Europe; 2) to obtain more insight into how well GDM guidelines are implemented and (3) to determine whether national or regional societies have implemented the 2013 WHO criteria for GDM.
Materials and methods: between September and November 2015, EBCOG organized an online survey on the current national or regional recommendations for GDM screening in individual European states. The survey was completed by the national delegates of EBCOG or by members of the European Diabetic Pregnancy Study Group (DPSG) in the member countries.
Results: the survey was directed to the 33 European countries that are members of EBCOG. 21 countries responded, giving a response rate of 63.6%. The response rates were high in central Europe (100%), northern Europe (85.7%) and southern Europe (71.4%) with lower response rates in Eastern Europe (55.6%). From Belgium, data were separately obtained from the Dutch-and the French-speaking parts and from the UK data were also obtained from Scotland, leading to data from 23 responders. 91.3% of all countries have national guidelines for GDM and 8.7% have regional guidelines. 81.8% of responders feel that the guidelines are well implemented and 73.9% of societies already recommend the 2013 WHO criteria for GDM. Of the societies that do not yet recommend the 2013 WHO criteria (7), 42.7% plan to implement them in the future. 87% of guide-lines recommend screening for unknown diabetes at first prenatal visit and screening is mostly based on risk factors (66.7%). 69.6% of guidelines recommend to screen for GDM before 24 weeks of pregnancy, mostly ba-sed on risk factors (94.1%). 95.7% of guidelines recommend to screen for GDM ≥24 weeks, mostly between 24-28 weeks (90.5%), based on risk factors in 63.4% of cases and by universal screening in 36.4%. The most commonly used screening tests are a 2 hour 75g oral glucose tolerance test (OGTT) (77.3%), a random glucose (13.6%), a 50g glucose challenge test (GCT) (13.6%) and a fasting glucose (9.1%). An abnormal GCT is followed by a 2 hour 75g OGTT (66.7%). The most commonly used diagnostic criteria for GDM are the 2013 WHO crite-ria (69.6%), the 1999 WHO criteria (8.7%), the European Association for the Study of Diabetes (EASD) criteria (8.7%), the Carpenter & Coustan criteria (4.4%) and the National Diabetes Data group criteria (4.4%).
Conclusions: our survey shows that the majority of European societies now advise to use the 2013 WHO criteria for GDM screening . The majority of societies recommend screening based on risk factors or by a two--step approach. Only a minority recommend a one–step universal screening approach. The use of common diagnostic criteria for GDM by the majority of national societies is an important first step towards achieving uniformity in GDM screening across Europe.
trEnds in Gdm WomEn ProfilE: tHE iadPsG CritEria ComParEd to tHE BraZilian CritEria in tWo CoHorts 20 yEars aPartAngela Jacob Reichelt1, Letícia Schwez Weinert2, Lívia Silveira Mastella2, Vanessa Gnielka3, María Amélia Cam-pos4, María Inês Schmidt3, María Lúcia Oppermann3, Sandra Pinho Silveiro3, Vânia Naomi Hirakata1
1Hospital de Clínicas de Porto Alegre, Brazil. 2Postgraduate Program in MS: Endocrinology, Universidade Federal Do Rio Grande Do Sul, Brazil. 3Faculdade de Medicina, Universidade Federal Do Rio Grande Do Sul, Brazil. 4Hospital Nossa Senhora Da Conceição, Porto Alegre, Brazil
Introduction: the adoption of the IADPSG criteria may raise GDM prevalence to 18% in Brazil, a 2.5 fold increase. Could different GDM criteria identify, in fact, different pregnant women?
Objective: to describe clinical characteristics and pregnancy outcomes of women meeting only one or other
Pa3
Pa2

35
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations 35
of two GDM diagnosis criteria. Material and Methods: two GDM cohorts from the city of Porto Alegre (Brazil), 20 years apart, were com-
pared: 216 women from the Estudo Brasileiro de Diabetes Gestacional (Brazilian Study of Gestational Diabetes), held in the 1990s, here called as the GDM-EBDG cohort; and 375 women from a university hospital prenatal clinic (2009 to 2013), called GDM-HCPA. GDM was diagnosed with the 75-g oral glucose tolerance test (75-g OGTT); Brazilian criteria (fasting >= 110 mg/dl or 2-h glucose >= 140 mg/dl) and IADPSG criteria (fasting >= 92 mg/dl or 1-h >= 180 mg/dl or 2-h >= 153 mg/dl) were applied to both cohorts. Characteristics and pregnancy outcomes of women with diagnostic overlapping and of those meeting exclusively the Brazilian or the IADPSG criteria were compared.
Results: age (29.7 ± 5.7 years vs 31.1 ± 6.5 years, p<0.001), family history of diabetes (16.8% vs 51.2%, p<0.001), previous GDM (1.4% vs 13.9%, p<0.001), pre-pregnancy weight 62.6 ± 11.4 kg vs 75.8 ± 18, p<0.001) and obesity rates (15.2% vs 45.1%, p<0.001) were lower in the GDM-EBDG compared to the GDM-HCPA cohort. In the GDM-EBDG cohort, 66 (30.5%) women met both criteria, 17 (7.9%), the Brazilian-only and 133 (61.6%), the IADPSG-only criteria. In the GDM-HCPA cohort, 266 (71%) women met both criteria, 42 (11%), the Brazilian-only and 67 (18%), the IADPSG-only criteria. In both cohorts, pre-gestational weight and BMI, and the OGTT 2-h glucose were lower in the Brazilian-only compared to the IADPSG-only women; OGTT fasting glucose was higher in the IADPSG-only group. In the GDM-HCPA cohort, obesity rates were higher (58.5% vs 33.3%, p=0.031) in the IADPSG-only group compared to the Brazilian-only group, as well as mean birth weight (3,338 ± 506 g vs 3,087 ± 484 g, p=0.012), large for gestational age rates (15% vs 2.4%, p=0.009) and macrosomia (10% vs 0%, p=0.030).
Conclusions: pre-gestational weight and BMI increased significantly in GDM women in 20 years. Women meeting IADPSG-only criteria were heavier and had a lower OGTT 2-h glucose in both cohorts. Furthermore, in the contemporary cohort, women meeting IADPSG-only criteria were more frequently obese and delivered heavier babies. IADPSG criteria seemed to detect pregnancy complications mainly associated to obesity.
tHE imPaCt of tHE iadPsG diaGnostiC CritEria on tHE PrEValEnCE of Gdm ComParEd to niCE CritEriaJosip Djelmis, Marina IvanisevicSchool of Medicine, University of Zagreb, Croatia
Objective: to investigate the impact of the IADPSG diagnostic criteria on the prevalence of GDM compared to NICE criteria in period from 2013-2014. Further goal was to evaluate the frequency of obese women, cesa-rean deliveries, hypertensive disorders in the pregnant cohort with FPG ≥5.1mmol/L ≤5.5mmol/L.
Methods: a cohort of 2669 women who underwent diagnostic 2 hours glucose tolerance test (OGTT) for hyperglycemia in pregnancy were studied retrospectively. The criteria of the NICE for GDM include: FPG venous plasma ≥5.6mmol/L and/or the value of glucose concentration in venous plasma ≥7.8mmol/L measured 2 hours after 75g OGTT. According to IADPSG criteria it is necessary that at least one of glucose values in maternal plasma equals to or is above the upper limit which was set for: fasting ≥5.1mmol/L; one hour ≥10mmol/L and 2 hours ≥8.5mmol/L. IADPSG criteria for overt diabetes (OD) in pregnancy are when the concentration of glucose in fasting plasma is ≥7mmol/L, or after a load of 75 g OGTT is ≥11.1mmol/L or when the random concentration of glucose value is ≥ 11.1mmol/L.
Results: when IADPSG criteria were applied 1674 (40.2%) women had GDM and 50 (1.9%) OD. Using NICE criteria GDM was found in 826 (30.9%) women. According to both criteria (NICE and IADPSG) 1413 women had normal OGTT and served as a control group (CTRL). According to either or both, the NICE and IADPSG criteria, 1,206 (45.1%) women had GDM. According to fasting glucose values of 5.1mmol/L or more, 827 (31%) women had GDM, and 14 (0.52%) women were diagnosed with OD as they had fasting glucose values of 7 or more mmol/L. There were 430 (18.9%) women whose FPG was between 5.1-5.5mmol/L and 2-h OGTT value lower than 7.8mmol/L. This particular group of 430 women gave birth to 107 (24.9%) LGA newborns and 98 (22.9%) of them had delivered macrosomic newborns (≥4.000 g). Frequency of LGA newborns in the group of women who had FPG between 5.1-5.5mmol/L is statistically significantly higher when compared to LGA newborns born in the control group (24.9 % vs. 15.2%, P<0.0001). Out of 430 pregnant women with FPG 5.1-5.5mmol/L, 58 (16.1%) were obese (BMI>30), in comparison to CTRL group where 117 (8.3%) women were obese, and the difference is statistically significant (P=0.0025). The frequency of CS in CTRL was 15.1%, in the group with FPG 5.1-5.5mmol/L frequency of CS was 19.6% (P=0.0327). According to our results, in conclusion, we dare to say that further lowe-ring of FPG threshold for gestational diabetes should not happen as already proposed by UK NICE.
Pa4

36
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations36
HEtEroGEnEity of matErnal CHaraCtEristiCs and imPaCt on Gdm risK-imPliCations for UniVErsal Gdm sCrEEninG?Nora Grotenfelt1, Emilia Huvinen2, Johan Eriksson3, Kristiina Rönö2, Jelena Meinilä3, Anita Valkama3, Hannu Kautiainen3, Beata Stach-Lempinen4, Saila Koivusalo2
1Folkhälsan Research Centre, Helsinki, University of Helsinki, Finland. 2Obstetrics and Gynaecology, Helsinki University and Helsinki University Hospital, Helsinki, Finland. 3General Practice and Primary Health Care, University of Helsinki and Helsinki University Hospital. 4Obstetrics and Gynaecology, South Karelia Central Hospital, Lappeeranta, Finland
Introduction: the incidence of gestational diabetes mellitus (GDM) is increasing worldwide. Several in-terventions targeting GDM prevention have been undertaken but the results have been inconsistent. The he-terogeneity of type 2 diabetes is well known and has been the focus of several previous studies. In contrast, there has been little focus on the heterogeneity of GDM, and it has not been taken into account when planning strategies for GDM prevention or in previous GDM prevention trials. The purpose of the present study was to focus upon clinical characteristics of women at high risk for GDM. This may help to optimize individualized GDM prevention strategies in the future.
Objective: to study the incidence of gestational diabetes mellitus (GDM) in relation to phenotypic characte-ristics and gestational weight gain (GWG) among women at high risk for GDM.
Materials and methods: this is a secondary analysis of a GDM prevention study (RADIEL), a randomized controlled trial conducted in Finland. 269 women with a history of GDM and/or a pre-pregnancy body mass index (BMI) of 30 kg/m2 or more were enrolled before 20 weeks of gestation (mean 13) and divided into four groups according to parity, BMI and previous history of GDM. The main outcome was incidence of GDM.
Results: there was a significant difference in incidence of GDM between the groups (p<0.001). Women with a history of GDM and BMI < 30 kg/m2 showed the highest incidence (35.9%). At baseline they had fewer metabolic risk factors and by the second trimester they gained more weight. There was no interaction between GWG and GDM outcome and no significant difference in the prevalence of diabetes-associated antibodies.
Conclusion: despite a healthier metabolic profile at baseline the non-obese women with a history of GDM displayed a markedly higher cumulative incidence of GDM. GWG and the presence of diabetes-associated an-tibodies were not associated with GDM occurrence among these high-risk women.
Group A: primiparous, BMI >30 kg/m2.Group B: multiparous, no previous GDM, BMI >30 kg/m2.Group C: multiparous, previous GDM, BMI <30 kg/m2.Group D: multiparous, previous GDM, BMI >30 kg/ m2.
Figure 1: Gestational weight gain according to group and GDM outcome (adjusted for physical activity in second trimester and diet score in second trimester, age, years of education and family history of diabetes).
Pa5

37
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations 37
ComParison of laBoratory HBa1C and tHE alErE afinion HBa1C analysEr in PrEGnant WomEn in a rEal-World sEttinGSumaiya Adam, Paul RheederUniversity of Pretoria, South Africa
Introduction: the prevalence of gestational diabetes (GDM) is increasing and thus gaining more attention. A universal, standardised screening program for GDM is now recommended. The recommended glucose tole-rance test is inconvenient and cumbersome. Glycated haemoglobin (HbA1c) is being considered as a screening tool. Numerous studies have recommended HbA1c values,above which patients have a greater chance of de-veloping GDM. Pregnancy is a finite period. Patients often encounter barriers such as travel to the laboratory or attending follow-up visits. A point-of-care (POC) test is thus an attractive option.
Objective: to compare the laboratory HbA1c result to the POC HbA1c values obtained on the Afinion in a pregnant population.
Materials and methods: all non-diabetic pregnant women less than 28 weeks were recruited at an ante-natal clinic in Johannesburg, South Africa. HbA1c analysis was performed at recruitment at the laboratory with the TOSOH G8 analyser and on-site using the Afinion POC system. The POC test was performed by a non-labo-ratory trained nurse. Approval was obtained from the University of Pretoria Health Sciences Ethics Committee (180/2012). Data was analysed with XL-STAT and MedCalc Software.
Results: we collected 675 samples, of which 607 completed data sets were analysed. Incomplete data were due to lost samples or power failure interrupting Afinion use. The mean age was 26.7 years, mean HbA1c on the Afinion was 32.8mmol/mol (5.15%) and for the laboratory was 33.5mmol/mol (5.22%). Pearson’s corre-lation coefficient (p=0.66) and the Bland-Altman analysis [bias -0.06, standard error 0.29(CI -0.09 - -0.04), limits of agreement -0.64 - 0.51] showed a positive relationship between POC and laboratory tests. However the Deming regression had an intercept of 0.75 (CI 0.27 - 1.22) and slope coefficient of 0.84 (CI 0.75 to 0.94). The proportional difference excludes equality between tests. The within-subject coefficient of variation is 4% (CI 3.8 to 4.3) which is greater than the recommended 2% for interchangeability of test methods. Lin’s concordance coefficient is 0.65 (CI 0.60 to 0.69). The bias correcting factor is 0.98. This indicates poor agreement between the Afinion and the laboratory.
Conclusion: the Alere Afinion POC system cannot replace laboratory analysis of HbA1c.
tHE trUE faCts aBoUt diaBEtEs and PrEGnanCy trEatmEnt at EVa PEron HosPital loCatEd in san martÍn, ProVinCE of BUEnos airEs.Sandra Fabiana Geraci, Silvia Lara, Carlos Weschler, Nelson Sánchez, Liliana Macri, Mónica Biondi, Alejandra Kinsella, Gabriela BorgeseHospital Interzonal General de Agudos Eva Perón, General San Martín, Argentina
Introduction: we hereby present an observational retrospective study carried out at Eva Perón Higa (Gene-ral Hospital). This is a high complexity center located in the first suburban belt around the city of Buenos Aires where the patients are sent from other primary care centers.
Objective: the main objective of this study was to determine the week of pregnancy in which the patients go to the medical consultation. Other objectives of this study were to define the relationship with body weight, the checkup and treatment, the postpartum examination and reclassification.
Material and methods: for this study the Medical History of the listed patients who had been treated at the Nutrition Service were taken. The measurement was fulfilled between 07/2015 and 01/2011. We completed a registration form with some selected data in order to obtain just the data points related to the objectives. These points were pregnancy time in the first consultation, Body Mass Index, attendance to checkup, compliance with self-monitoring, diet and insulin therapy and postpartum consultation/ reclassification.
Results: 124 patients were evaluated and the consultation average was 30.4 weeks. 0-24 weeks 15.3 %, 24-28 weeks 5.6 %, 28-32 weeks 21.7%, 32-41 weeks 57.4%. Out of the whole, 102 patients were gestational diabetics (82.3%) and 22 were pre gestational diabetics (17.7%). Out of these 22, 14 were diabetes mellitus 2 and their first average consultation was in week 21.2 and the other 8 patients were diabetes mellitus 1 and their first average consultation was in week 11.7. Regarding the objectives in the second place, the BMI average of the whole was 31.9. Within the pre-gestational group, diabetes mellitus 1, BMI was 22.4 and diabetes mellitus 2 was 34.2. They were provided with an individual diet with a weekly checkup by a nutrition specialist. Self-mo-
Pa6
Pa7

38
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations38
nitoring was 96.7% out of the whole (120 patients). 57 patients (46%) needed insulin. Only 30 patients (24%) of this group attended postpartum consultation for checkup. 6 patients (4.84%) attended for reclassification.
Conclusions: our records do not coincide either with epidemiologic statistics or the standards proposed by different sanitary or academic organizations. Taking this into account, the 32-41 weeks group (57.4%) is a late derivation which exposes people to unnecessary risk. Considering sociodemographic characteristics, the IMC in the first consultation is too high. The self-monitoring and insulin therapy worked properly due to the fact that they were part of the free giving program. We consider the fact that patients did not attend for reclassification, despite education about diabetes, as a sanitary failure because of the future potential risk it implies.
sEssion B: ExPErimEntal WorKs
matErnal trEatmEnt WitH a mitoCHondrial antioxidant PrEVEnts matErnal diaBEtEs-indUCEd ProGramminG of HEart altErationsSabrina Roberti, Daiana Fornes, Alicia Jawerbaum, Romina HigaLaboratory of Reproduction and Metabolism, CEFYBO-CONICET, University of Buenos Aires, Buenos Aires, Argentina
Introduction: maternal diabetes induces a pro-inflammatory and pro-oxidant environment and can pro-gram metabolic and cardiovascular diseases in the offspring. Idebenone is a coenzymeQ analogue, acting as a transporter in the mitochondrial electron transport chain and as an antioxidant. Mitochondrial biogenesis and function, as well as antioxidant processes are regulated by peroxisome proliferator activated receptor coactiva-tor 1alpha (PGC-1alpha).
Aims: to analyze the effect of idebenone administration during pregnancy on pro-inflammatory and pro-oxidant markers and on PGC-1alpha protein expression in hearts of offspring from control and diabetic rats.
Methods: diabetes was induced by neonatal streptozotocin administration (90 mg/kg), leading to adult dia-betic animals with fasting glycemia values between 130 and 230 mg/dl. Control and diabetic adult females were mated with control males. During pregnancy rats were treated with idebenone (100 mg/kg, oral treatment) or vehicle (water). The heart was explanted in 21-day-old offspring for further evaluation of the levels of nitrotyro-sine (a marker of peroxynitrite-induced damage), MMP9 (matrix metalloproteinase-9), CTGF (connective tissue growth factor, a pro-inflammatory and pro-fibrotic marker) and PGC-1alpha by immunohistochemistry.
Results: the hearts of 21-day-old offspring from diabetic rats showed increased protein nitration (p<0.001), increased levels of MMP9 (p<0.001) and CTGF (p<0.001) and reduced concentrations of PGC-1alpha (p<0.01) compared to controls. Maternal treatment with idebenone decreased protein nitration (p<0.001), decreased MMP9 (p<0.001) and CTGF (p<0.001) levels, and increased PGC-1alpha protein expression (p<0.05) in the hearts of offspring from diabetic rats.
Conclusion: maternal diabetes programs increases in pro-oxidant and pro-inflammatory markers in the heart of 21-day-old offspring, which may be related to the observed reductions of PGC-1alpha protein expres-sion. Maternal treatments with idebenone prevent the observed alterations, showing protection of program-ming of the cardiac anomalies induced by maternal diabetes.
ExPErimEntal GEstational diaBEtEs mEllitUs (Gdm) indUCEd By intraUtErinE ProGramminG: EffECts of f0 trEatmEnts WitH mitoCHondrial antioxidantsIvana Linenberg, Verónica White, Alicia Jawerbaum, Evangelina CapobiancoLaboratory of Reproduction and Metabolism, CEFYBO-CONICET, University of Buenos Aires, Buenos Aires, Argentina
Introduction: in a mild model of diabetes induced by neonatal streptozotocin administration (F0), we have previously found that the female offspring, when mated with control males, develop GDM during pregnancy.
Objective: considering that an intrauterine pro-oxidant and pro-inflammatory environment is evident in both mild diabetic F0 pregnancies and GDM pregnancies, the AIM of this work was to address whether F0 maternal treatments with mitochondrial antioxidants reduce pro-oxidant and pro-inflammatory markers in GDM placen-tas (F1).
Methods: control and mild diabetic (glycemia 180-220 mg/dl) Wistar rats (F0) were treated with either vehicle or antioxidants (Idebenone (IDE, 100 mg/kg/day) or Mitoquinone (MitoQ, 17mg/kg/day)) from day 1 of gestation until parturition. No treatments were performed in the F1 generation. The female offspring (F1) from
PB1
PB2

39
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations 39
control and diabetic rats were mated with healthy males. On day 21 of pregnancy, rats were euthanized, the serum conserved for metabolic determinations and the placentas preserved for evaluation of a) levels of PPARγ, superoxide dismutase (SOD) and nitrotyrosine (a marker of protein nitration and peroxynitrite-induced damage), by immunohistochemistry, b) the production of nitric oxide, through quantification of nitrates/nitrites by the Griess reaction and c) apoptosis, by TUNEL.
Results: the offspring of diabetic rats had increased glycemia and insulinemia (p<0.01) and the F0 treatments with the mitochondrial antioxidants had no effect on these parameters. GDM placentas showed decreased PPARγ levels (p<0.01, 66%), which were unchanged by the maternal antioxidant treatments in the F0 ge-neration. The protein expression of SOD was decreased in GDM rats (p<0.05, 23%), and increased by both idebenone and mitoQ F0 treatments (p<0.05, 24-27%). Although the apoptosis rate was unchanged in the GDM placentas, nitric oxide production was increased in the GDM placentas when compared to controls, and decreased with F0 treatments with idebenone and mitoQ. Protein nitration was increased in GDM placentas (p<0.001, 190%), and decreased by both idebenone and MitoQ (p<0.01, 50-70%).
Conclusions: oxidative and nitrative stress was increased in GDM placentas and decreased by treatments with mitochondrial antioxidants during F0 diabetic pregnancies. This suggests that an adverse pro-oxidant and pro-inflammatory environment can be programmed in the uterus and reversed by F0 treatments.
is oxidatiVE strEss imPliCatEd in tHE tEratoGEnEsis assoCiatEd to oBEsity?Martín Alcala1, Isabel Sánchez-Vera1, Victoria Bolado1, Sonia Clapés2, Guillermo Sáez3, Francisco Dasí4, María Pilar Ramos1, Marta Viana1
1Universidad CEU San Pablo. 2Universidad de Ciencias Médicas de La Habana, ICBP Victoria de Girón, La Habana, Cuba. 3Hospital Clínico Universitario de Valencia. 4Instituto de Investigación Sanitaria Incliva, Valencia, España
Introduction: maternal obesity has fetal and neonatal deleterious consequences. In early pregnancy, obe-sity is a risk factor for spontaneous and recurrent abortion, and is associated with a high risk of congenital ano-malies, such as neural tube defects (NTD). The mechanism underlying the increased risk of NTD is unknown, however, a number of theories have been proposed including, nutritional deficits, metabolic alterations (hyper-glycemia, and hyperinsulinemia among others), inflammation and oxidative stress.
Objective: our aim was to study the effect of oxidative stress in an animal model of obese pregnant rats, its putative relation with congenital malformations, and evaluating the protective effect of antioxidants, such as vitamin E.
Methods: obesity was induced in Wistar rats by feeding with a high fat diet. The animals were divided in three groups: one was fed standard pellet diet, control group (L); two groups were fed with the high fat diet during 3 months, the first one without any supplementation (O) and the second was supplemented with 150 mg/d of vitamin E (OE) during all experiment. The animals were mated and sacrificed at day 11,5 of pregnancy. The embryos were dissected and the rate of malformation was recorded. Embryos not conforming to normal morphology were considered malformed. Blood and liver were collected and metabolic parameters and oxida-tive stress markers were analysed.
Results: obese rats showed an increased rate of embryo malformations (24%) compared with the C group (4%). When the animals were supplemented with vitamin E (OE) the rate of malformations decreased to 7%. After the diet period, the O rats presented an HOMA index higher than the L rats, whereas the supplementation with vitamin E reduces the obesity-induced insulin resistance to control levels. Circulating and hepatic AOPPs and hepatic 8-OH-dG concentration were significantly higher in the O group compare to C. Vitamin E supple-mentation had no effect in this markers. The mRNA expression of antioxidant enzymes such as SOD and Gpx were lower in the O compare with the C group. Vitamin E supplementation do not enhance antioxidant gene transcription in the liver of obese pregnant rats, but preserves hepatic glutathione levels that were lower in the O group. Vitamin E also are able to reduce the expression of the GCLC enzyme to control levels.
Conclusion: obesity during pregnancy is associated to an increased rate of embryo malformations, which is decreased with the administration of vitamin E. The obese animals presented insulin resistance that was prevented with the administration of vitamin E. The oxidative stress markers indicate higher oxidative stress in obesity, although vitamin E is not able to normalize all of them. We propose that the mechanism of vitamin E-mediated reduction in teratogenesis may involve a reduction in insulin resistance, TG, FFA, which agrees with the Freinkel’s fuel-mediated teratogenesis hypothesis. Another possible mechanism of Vitamin E could be the mediation in the preservation of GSH, critical for protein folding.
PB3

40
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations40
matErnal diaBEtEs diEt sUPPlEmEntEd WitH or WitHoUt oliVE oil diffErEntially imPaCts PanCrEas dEVEloPmEnt in malE and fEmalE offsPrinGElizabeth Pham1, Daniel Ramnath2, Evangelina Capobianco3, Alicia Jawerbaum3, Edith Arany1
1Lawson Health Research Institute, University of Western Ontario, Canada. 2Lawson Research Institute, Canada. 3Laboratory of Reproduction and Metabolism, CEFYBO-CONICET, School of Medicine, University of Buenos Aires, Argentina
Maternal type 1 diabetes mellitus (T1DM) impacts fetal development and results in glucose intolerance later in life. Previous research in our laboratory has shown that dietary supplementation with 6% olive oil (enriched with 34% oleic acid) given during pregnancy to mild diabetic rats increased the numbers of implanted embryos and decreased neonatal malformations by reducing the inflammatory intrauterine environment. This was related to the activation of PPARs, a family of nuclear receptors essential for placental development, embryonic stem cell proliferation and implantation. Oleic acid, the main component of olive oil, is a ligand of PPARs and has been shown to lower LDL and total cholesterol levels, and it has beneficial effects in terms of blood sugar control as well as reducing insulin resistance. In this study we examined the effects of maternal diabetes with or without olive oil supplementation on neonatal and adult pancreas development and its impacts in early adulthood. A mild diabetic rat model was used, injecting streptozotocin (STZ) (90 mg/kg) diluted with fresh citrate buffer or citrate buffer alone, 2 days after birth. Females with glycemia than 130 mg/ml were mated with normal male rats and at gestational day 0.5 were fed with control chow diet (D+C) or diet supplemented with 6% olive oil (D+O). A control non-diabetic group fed with (C) and (C+O) was also studied. Male and female body weight, pancreas weight, fasting glycemia and pancreas were collected at day 2 and 4 months of age. Differences in body and pancreas weight between all groups were not statistically significant. However, in males fasting glycemia was higher in the D+C and similar to C in the D+O at 4 months of age. No significant changes were seen in females. Dual immunohistochemistry was performed to detect alpha and beta-cells with the different PPARs in islets and morphometric analysis was carried out to study islet area, beta and alpha cell area, beta cell mass and islet distribution by size. Our data showed that the percentage of islet area, beta and alpha cell area and beta cell mass at day 2 postnatal was not statistically significant between all groups. However, males at 4 months of age showed that olive oil supplementation had a restorative effect on islet and beta cell area, as well as beta cell mass with a significant increase (P <0.05) in the number of large islets and beta cell clusters than D+C. PPAR alpha was detected in islets and was co-localized to alpha cells at day 2 and 4 months. PPAR gamma was only seen at day 2 and PPAR delta was co-localized in both and cells at both time points studied. Although we could determine their presence in the endocrine pancreas, future studies are needed to establish their role. Therefore, we conclude that maternal diabetes predisposes male offspring to an early onset of diabetes, but have fewer effects on females. Again, in males the introduction of olive oil in the maternal diet increased islet area, cell area, cell mass, number of islets and cell clusters and fasting glycemia was similar to C. These studies have further addressed the importance of understanding the mechanisms by which the in utero environmental milieu can affect males and females differently in the prevention or treatment of future adult disease. Overall, these findings addressed the importance of the quality of the diet in mothers with type 1diabetes to prevent early onset of glucose intolerance in males.
matErnal trEatmEnts WitH a mitoCHondrial antioxidant PrEVEnt tHE intraUtErinE ProGramminG of altErations in PParGamma and its CoaCtiVator PGC-1alPHa in tHE fEtal liVEr of rats tHat dEVEloP GEstational diaBEtEsDaiana Fornes, Romina Higa, Evangelina Capobianco, Alicia JawerbaumLaboratory of Reproduction and Metabolism, CEFYBO-CONICET, University of Buenos Aires, Buenos Aires, Argentina
Introduction: maternal diabetes induces a pro-inflammatory environment and impairments in PPARs signa-ling, evident in both fetuses and placentas. This has been observed in a newly developed experimental model of gestational diabetes (GDM) induced by intrauterine programming. PPARgamma and its coactivator PGC-1alpha regulate developmental, metabolic, anti-oxidant and anti-inflammatory processes. Idebenone is a coenzyme Q analog that works as an electron carrier in the electron transfer chain and as a mitochondrial antioxidant. Impro-per development of the fetal liver can lead to adult metabolic diseases.
PB4
PB5

41
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations 41
Aims: to evaluate whether maternal treatments with idebenone (F0) regulate PPARgamma, PGC-1alpha, peroxynitrite-induced damage and matrix metalloproteinase 2 (MMP-2) levels in the fetal liver of GDM rats (F1).
Methods: mild diabetes was induced in Wistar rats by neonatal streptozotocin administration (90 mg/Kg) (glycemia values 180-230 mg/dl) (F0), an experimental model of diabetes that programs GDM in the F1 gene-ration (glycemia values before pregnancy: 90-100 mg/dl; glycemia values on pregnancy: 130-150 mg/dl). F0 control and diabetic rats were treated with idebenone (100 mg/kg/day) or vehicle during pregnancy. F1 rats were mated with control males and received no treatment. On day 21 of gestation F1 rats were euthanized and the fetal livers isolated for evaluation of PPARgamma, PGC1alpha, nitrotyrosine (indicating protein nitration and peroxynitrite-induced damage) and MMP2 levels by immunohistochemistry.
Results: fetal livers from GDM rats showed a decrease in PPARgamma levels (30%, p<0.05) compared to controls and PPARgamma levels increased when F0 pregnancies were treated with idebenone (p<0.05). PGC-1alpha was also reduced in fetal livers from GDM rats (29%, p<0.05) compared to controls, and this alteration was prevented by F0 treatments with idebenone (p<0.05). MMP-2 was increased in fetal livers from GDM rats (300%, p<0.001) compared to controls, although not changed by F0 treatments with idebenone. Nitrotyrosine levels were increased in fetal livers from GDM rats (31%, p<0.05) and decreased in the fetal livers of GDM rats that were treated with idebenone during F0 pregnancies.
Conclusion: the observed reduction in the levels of PPARgamma and its coactivator PGC1alpha is probably related to the increased levels of pro-oxidant/pro-inflammatory markers in fetal livers of GDM rats. In addition, idebenone treatments in the F0 generation were able to prevent alterations in PPARs pathways in the F1 gene-ration, highlighting the ability of maternal treatments with a mitochondrial antioxidant to prevent programming of future alterations.
matErnal oBEsity indUCEs latEnt mEtaBoliC altErations in offsPrinG WHEn sUBJECtEd to a HiGH fat diEtMaría Victoria Bariani, Ana Paula Domínguez Rubio, Julieta Aisemberg, Ana María FranchiCentro de Estudios Farmacológicos y Botánicos. CEFYBO-CONICET-UBA, Buenos Aires, Argentina
The prevalence of maternal obesity has risen dramatically and could significantly impact the fetal development. Children from obese mothers have an increased risk of developing obesity as well as several diseases, including cardiovascular disease and hypertension. The endocannabinoid system (ECS) participates in the control of energy balance and regulates lipid metabolism and the accumulation of energy as fat. Therefore, a disregulation in the ECS might contribute to excessive visceral fat accumulation and to the onset of several metabolic risk factors associated with obesity. We had developed a high fat diet (HFD: standard food + 30% fat)-induced maternal obe-sity model in CD1 wild type (WT) and cannabinoid receptor type 1-knockout (CB1-KO) mice. The aim of this study was to evaluate the weight gain as well as several markers of obesity in offspring (both WT and CB1-KO) from HFD-treated and control mothers, when subjected to a HFD or standard diet. We observed that pups (both WT and CB1-KO) born to obese mothers had higher weight at birth and during lactation period (p<0.05). Moreover, we found an increased in serum cholesterol (CHOL) levels in postnatal day 1, but not in glucose and triglycerides levels, in these animals. After weaning, pups were fed with standard food or HFD during 3 months. Here, we found that the offspring from HFD and standard-diet mothers when subjected to a standard diet in adulthood showed no differences in several metabolic parameters, except for the increased weight and higher CHOL levels in CB1-KO animals. However, if animals were fed with a HFD, we found a higher weight and CHOL levels in the offspring from obese mothers (p<0.05). In addition, the offspring from obese mothers showed higher amount of abdominal adipose tissue (p<0.05). Our results suggest that the ECS is involved in the development of obesity and that maternal obesity induces short and long term metabolic alterations in their offspring.
matErnal satUratEd fat diEt indUCEs dECrEasEs in dEtoxifyinG EnZymEs and oxidatiVE tissUE damaGE in tHE liVErs of fEtUsEs and offsPrinGMaría Belén Mazzucco, Evangelina Capobianco, Alicia Jawerbaum, Verónica WhiteLaboratory of Reproduction and Metabolism, CEFYBO-CONICET, University of Buenos Aires, Buenos Aires, Argentina
Introduction: maternal overweight programs metabolic alterations in the liver of the offspring. In a rat mo-
PB6
PB7

42
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations42
del of saturated fat overload in the maternal diet, we have previously found increased oxidative stress parame-ters and alterations in the gene expression of some detoxifying liver enzymes in the fetuses and offspring. The transcription factors Nrf2 and PPARalpha are implicated in the antioxidant/detoxifying cell defense. This involves induction of gene expression of a) detoxifying enzymes such as multidrug resistance-related proteins (MRPs) and b) antioxidant enzymes. Plasma activity of the liver enzymes glutamate oxalacetate transaminase (GOT) and glutamate pyruvate transaminase (GPT) are markers of liver damage.
Objective: to investigate the effects of a saturated fat overload in the maternal diet on the livers from fetuses and 21- and 140-day-old offspring regarding a) Nrf2, PPARalpha and MRP3 gene expression, b) plasma GOT and GPT activity and c) nitrative-related tissue damage.
Methods: female Wistar rats were fed with either a standard (5% fat) or a saturated fat diet (28% fat) from 6 weeks of age (SFD rats). After 8 weeks of diet, they were mated with control males. Control and SFD pregnant rats were euthanized at 21 days of gestation, the fetal liver was explanted and fetal plasma obtained. Another group of control and SFD rats were allowed to deliver. The offspring were euthanized at 21 and 140 days of age, their plasma obtained and their livers explanted. All livers were preserved for the analysis of PPARalpha, Nrf2 and MRP3 gene expression (PCR), GOT and GPT activity (commercial kit) and 3-nitrotyrosine levels (immuno-histochemistry).
Results: Nrf2 expression in the livers from 21- and 140-day-old offspring (p<0.05) from SFD rats was lo-wer than in those from controls. MRP3 expression in the livers from 140-day-old offspring (p<0.05) from SFD rats was lower than in those from controls. Plasma GPT activity in fetuses (p<0.05) and plasma GOT activity (p<0.05) and liver nitrotyrosine levels in 140-day-old offspring (p<0.05) from SFD rats were higher than in those from controls.
Conclusions: maternal saturated fat diet induces a decrease in the gene expression of detoxifying enzymes in the fetal liver, which continues in the offspring, probably related to the decrease in Nrf2 expression. These alterations could contribute to the increased nitrative stress and subsequent oxidative liver damage observed in the SFD group.
EValUation of GastriC motility in PrEGnant diaBEtiC ratsJuliana Fernandes Matos1, Madileine Francely Américo2, Yuri Karen Sinzato3, Débora Cristina Damasceno3, José Ricardo de Arruda Miranda1
1Institute of Biosciences of Botucatu-UNESP. 2Institute of Biological Sciences and Health, Barra Do Garças-MT. 3Laboratory of Experimental Research on Gynecology and Obstetrics, Botucatu-UNESP, Brazil
Diabetes mellitus is a worldwide public health problem and is often associated with symptoms and gastroin-testinal motility disorders. As the incidence of diabetes continues to increase in individuals of all ages, women of fertile age also present risk for diabetes during pregnancy. The aim is to evaluate the mechanical profile of gastric motility in diabetic pregnant rats. The biosusceptometry of Alternating Current (BAC) is a fairly simple technique, low cost and versatile in research related to the human gastrointestinal tract and has recently been improved so that it could generate images of markers in both ferromagnetic vitro and in vivo, as it was proposed a new instrumentations to perform tomographic images. BAC is composed of magnetic sensors based in inductions coil. An electrode was inserted for measurement of electromyography (EMG), and a ferrite bead to measure the BAC in the rats (Figure 1). Severe diabetes was induced by a beta-cytotoxic agent (streptozotocin -40 mg/kg, ip) at adult rats. The control and diabetic rats were mated to obtain pregnant rats. The gastric emptying was conducted through the measurement of the concentration of magnetic material throughout the gastrointestinal tract by the sensor BAC. The gastric motility was evaluated during pregnancy. P<0.05 as statistical significance limit. The gas-tric contraction frequency decreased throughout pregnancy, especially at day 14 of pregnancy. Furthermore there is an increase in gastric emptying time on day 14 of gestation. There was a linear correlation between increase in progesterone concentration and decreased contraction frequency during pregnancy. The diabetic pregnant rats presented increased significant contraction frequency compared with control group (day 7). Furthermore, in qua-litative terms, there were irregular profile of signs of pregnant diabetic dams. Morphologically, it was a different sign, showing oscillations with higher periods and most acute peaks. The severe diabetic rats exhibited variations in the frequency of gastric contraction, delayed gastric emptying and irregularities in the signal profile during preg-nancy. Acknowledgement: FAPESP 2015/05045-8.
PB8

43
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations 43
Figure 1: Modified of Quini et al, 2012. Employment of a noninvasive magnetic method for evaluation of gastroin-testinal transit in rats. Journal of Biological Engineering.
CHaraCtEriZation of GastrointEstinal motility in ExPErimEntal modEl of HyPErGlyCEmia: PrEliminary rEsUltsJuliana Fernandes Matos1, Madileine Francely Américo2, Yuri Karen Sinzato3, Débora Cristina Damasceno3, José Ricardo de Arruda Miranda1
1Institute of Biosciences of Botucatu-UNESP. 2Institute of Biological Sciences and Health, Barra do Garças-MT. 3Laboratory of Experimental Research on Gynecology and Obstetrics, Botucatu-UNESP
In healthy individuals, plasma glucose concentration is highly regulated and kept within a narrow range and these concentrations also play a role in the regulation of gastrointestinal motility. Acute changes in glu-cose concentration in the blood have important effects on motor and sensory function of the upper GI, and at the same time, the upper intestine plays an important role in the regulation of postprandial blood. The aim is to characterize the profile of gastric motility in rats with severe diabetes model and moderate and evaluate the influence of glycemic variations in GI. Biosusceptometry of Alternating Current (BAC) is a fairly simple technique, low cost and versatile in research related to the human gastrointestinal tract and has recently been improved so that it could generate images of markers in both ferromagnetic vitro and in vivo, as it was propo-sed a new instrumentations to perform tomographic images. BAC is composed of magnetic sensors based in inductions coil. An electrode was inserted for measurement of electromyography (EMG), and a ferrite bead to measure the BAC in the rats. Severe diabetes was induced by a beta-cytotoxic agent (streptozotocin -40 mg/kg, ip) at adult rats. They were evaluated contractility and gastric emptying of serious control and diabetic animals. Concomitant to this experiment was also performed the hyperglycemic clamp in non-diabetic ani-mals to evaluate the hyperglycemic condition. P<0.05 as statistical significance limit. There was a significant decrease in contraction frequency and increase in gastric emptying time of the diabetic animals compared with control animals. As for the hyperglycemic clamp experiment no significant differences were gastric contraction rate during hyperglycemic period. However, morphologically there was a sign of irregularity ob-tained gastric motility during hyperglycemic time. These are preliminary results that can generate answers to questions not yet defined in the literature as the pathophysiological changes resulting from the glucose conditions and their relationships.
Acknowledgement: FAPESP 2015/05045-8 .
PB9

44
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations44
sEssion C: Gdm manaGEmEnt & folloW UP
faCtors assoCiatEd WitH tHE nEEd for insUlin tHEraPy in PatiEnts WitH GEstational diaBEtEs mEllitUs diaGnosEd By first Visit fastinG Blood GlUCosEAna Claudia Souza1, Rafaela Costa1, Cristiane Paganoti1, Marcelo Zugaib2, Rossana Francisco2
1Obstetrics Division of Hospital Das Clinicas Da FMSUP. 2Department of Obstetrics and Gynecology of Faculda-de de Medicina Da Universidade de São Paulo. Brazil
Introduction: since the proposition of the International Association of Diabetes and Pregnancy Study Group (IADPSG) consensus regarding diagnosis of GDM, the prevalence of this condition has increased among preg-nancies, particularly by the addition of a new group of hyperglycemic women: those diagnosed by altered fas-ting blood glucose (FBG) at the first prenatal visit.
Objective: to evaluate predictor variables of the insulin need in women diagnosed for GDM by the FBG at first prenatal visit.
Materials and methods: we performed an observational, retrospective cohort study by accessing clinical and laboratorial data from electronic medical chart of pregnant women that attended prenatal care in a tertiary teaching hospital in São Paulo city (Brazil) from 2012 to 2014. We included singleton pregnancies of women with GDM diagnosed by FBG according to IADPSG consensus (FBG >=92mg/dL) before 24 gestational wee-ks. Exclusion criteria were: subjects who lost follow-up to antenatal visits, incomplete medical records, use of corticosteroids during pregnancy and pregnancies that did not progress beyond 20 gestational weeks. Primary outcome was the requirement of insulin therapy to achieve blood glucose targets. According to the primary outcome (insulin or diet group) subjects were compared regarding clinical and laboratorial variables.
Results: a total of 354 women were identified and 299 were included for analysis. Among them, 117 (39%) needed insulin therapy. Compared to diet group, those who required insulin were older, had higher FPG levels at diagnosis, had greater pre pregnancy BMI, more frequently had prior GDM and family history of diabetes and presented higher HbA1c levels after diagnosis, as shown in Table 1.
Conclusions: over a third of pregnant women with GDM diagnosed by altered FBG require insulin to achie-ve blood glucose targets and older maternal age, higher levels of FBG, greater pre pregnancy BMI, prior GDM and higher levels of HbA1c are risk factors related to the insulin need in these pregnancies.
diet (n=182) insulin (n=117) P-value
Maternal age (years), mean ± SD 31.3 ± 6.1 33.7 ± 5.8 0.001
Primigravida, n (%) 51 (28.0) 22 (18.8) 0.057
Prepregnancy BMI (kg/m²), mean ± SD 29.6 ± 7.0 31,9 ± 6,3 0.005
Weight gain during pregnancy (kg), mean ± SD 7.7 ± 7.0 8.1 ± 6.2 0.604
Family history of diabetes, n (%) 103 (56.6) 83 (70.9) 0.015
Prior GDM, n (%) 6 (4.6) 25 (27.2) <0.001
Prior fetal macrosomia, n (%) 10 (7.6) 15 (15.8) 0.084
Smoking, n (%) 15 (8.3) 15 (12.9) 0.239
Chronic arterial hipertension, n (%) 47 (25.8) 38 (32.5) 0.238
Gestational age at diagnosis (weeks), mean ± SD 10.1 ± 3.9 10.6 ± 4.1 0.304
FBG at diagnosis (mg/dL), mean ± SD 96.8 ± 5.5 100.5 ± 7.4 <0.001
HbA1c at diagnosis (%), mean ± SD 5.1 ± 0.4 5.4 ± 0.7 <0.001
Table 1: Clinical and laboratorial profile of women with GDM, according to the IADPSG criteria.
GEstational diaBEtEs PatiEnts trEatEd at tHE aUstral UniVErsity HosPital diaBEtoloGia sErViCENoemí Passarin, María Cecilia Preiti, María Silvina Guaita, Fabiana Davila, Susana Beatriz Apoloni, Fabiana Vázquez, Rodolfo Fregonese, Ernesto BerutiHospital Universitario Austral
PC1
PC2

45
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations 45
Introduction: gestational diabetes (DG) is diagnosed during pregnancy for the first time and implies higher risk of complications for the mother and the child. For these reasons, all pregnant women treated at the Austral University Hospital (HUA) are tested for diagnosis.
Objective: to describe the frequency of diagnostic, demographic, clinical and biochemical characteristics, fetal and maternal complications of DG in patients treated at diabetes unit of the HUA.
Material and methods: there were requested to the HUA information systems department the number of caesarean and deliveries made between March 1, 2014 to 31 August 2015. A review was made of medical records of patients with diagnosis of DG (according to SAD criteria) treated at the Diabetologia service at the same period. Patients with diagnosis of pre-gestational DBT were excluded. DG was classified according to Freinkel Criteria. Chi square test was used to compare proportions.
Results: 196 cases of DG were analyzed. 3193 patients were hospitalized for labor (vaginal 1997 and 1196 caesarean) in a 18 months period; rate of 6,14 cases of DG per 100 deliveries. In 196 cases with DG, average age was 32, 56 ±5 and body mass index at the beginning of the pregnancy was 25,8±4; 8 patients had throm-bophilia (4.08%). The diagnosis of DG was made between 8 and 35 weeks of pregnancy (median = 25) and 158 DG were classified as A1 (80,61%), 36 as A2 (17.85%) and 3 as B (1.02%). In 37 patients (23.57%) type A1, 18 type A2 (50%) and 3 type B insulin was indicated (p < 0.0001). Pregnancy Complications: 9 cases with Cholestasis (4.64%); 19 with hypertension (9.69%); 5 pre-eclampsia (2.55%); and 2 toxoplasmosis. Childbirth took place by caesarean in 86 cases (43,88%) and in 10 cases before 36 weeks gestation (5.10%). There were 16 newborn babies with macrosomia (8.16%), 5 hyperbilirubinemia (2.55%), 1 hypoglycemia (0.51%). There were 3 neonatal deaths (two had malformations). A patient developed Diabetic Ketoacidosis before 6 weeks postpartum and was reclassified as diabetic type I. In 67 patients (34.18%) oral glucose tolerance test at 6 weeks post partum was done, 9 had impaired glucose tolerance, 4 had elevated fasting plasma glucose but in any diagnosis of diabetes was made.
Conclusions: the observed rate of DG was similar to that reported in other studies ranging from 1 to 28%, depending on the population studied and the diagnostic criteria used. In more than 80% of cases the diagnosis was performed by impared glucose tolerance test. The Group A2 and B presenting hyperglycemia of fasting showed greater requirement for insulin therapy. The most frequent complication was fetal macrosomia with numbers similar to other present patients series but less than what was reported in historical series prior to the implementation of detection and early treatment programs.
insUlin dynamiCs in JaPanEsE GEstational diaBEtiC WomEn: a diffErEnCE BEtWEEn lEan and oBEsE sUBJECtsIchiro Yasuhi, Yukari Kugishima, Hiroshi Yamashita, Sachie Suga, Misao Fukuoka, Yasushi Umezaki, Masashi Fukuda, Nobuko KusudaNHO Nagasaki Medical Center, Japan
Introduction: insulin dynamics depends on some characteristics including the degree of obesity, race, gen-der, age, etc.
Objective: the aim of this study was to demonstrate a difference between lean and obese women with gestational diabetes (GDM) in Japanese population.
Methods: in this retrospective study, we included Japanese singleton pregnant women with GDM, and measured immunoreactive insulin levels as well as glucose values in their diagnostic OGTT during mid-preg-nancy. We compared HOMA-insulin resistance (IR) and indices reflecting insulin secretion including HOMA-β, insulingenic index (II), and disposition index (DI) between lean (prepregnancy body mass index <18.5) (group L), normal weight (18.5-24.9) (group N), and obese (≥25.0) (group O) women.
Results: among 162 women included in this study, 18 (11%), 98 (61%), and 46 (28%) subjects were lean, normal weight, and obese, respectively. HOMA-IR was significant different between the groups: 0.9±0.6, 1.3±0.6, and 2.3±0.8, in the L, N, and O group, respectively (p<0.0001). Although HOMA-β did not differ between the groups, II in group L (0.35±0.15) was significantly lower than the other groups (0.58±0.33 in group N; 0.60±0.40, p<0.01). DI in group O (0.60±0.41) was significantly lower than those in group N (0.84±0.34, p<0.01).
Conclusion: in comparison with women normal prepregnancy BMI, prepregnant obese and lean women are characterized as more insulin resistant and decreased early phase insulin secretion, respectively. Therefore, not only obese but also lean Japanese women with a history of GDM are at high risk for the development of diabetes.
PC3

46
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations46
PrEGnanCy oUtComEs in GEstational diaBEtEs diaGnosEd BEforE and aftEr 28 WEEKsCecilia Fregozo Osuna, Jeddú Cruz Hernández, Jacinto Lang, Antonio Márquez GuillénNational Institute of Endocrinology, Havana, Cuba
Introduction: the time of diagnosis of gestational diabetes is associated with pregnancy outcomes. Objective: to determine whether gestational diabetes diagnosed before 28 weeks is associated with better
pregnancy outcomes, which subsequently diagnosed.Methods: descriptive study that included 302 women diagnosed with DG to <28 (group 1) or ≥ 28 weeks
(group 2) in the Gynecobstetric Hospital “America Arias”, Havana Cuba, during 2010-2012. Variables such as, fasting plasma glucose, time of therapeutic intervention, insulin requirement and pregnancy outcomes were analyzed. Chi-square and Fisher test was used to compare qualitative variables (percentage) and Student t test was used for quantitative variables (mean ± standard deviation). Significant <0.05 was assumed.
Results: 46.7% of women were aged ≥30 years and 5.6% were teenagers. 55.9% of the women to group 1 had a fasting plasma glucose between 4.4-5.5 mmol/L versus 35.5% of group 2 (p <0.0001). The mean diffe-rence of time of therapeutic intervention (24.20 ± 6.30 versus 32.42 ± 2.08 weeks) was statistically significant: p <0.0001. In group 1 more women required insulin: 91.9 versus 81.9% (p=0.0117) and had more preterm labor: 12.5 versus 1.8% (p=0.0002). The average birth weight of group 1 (3372.42 ± 614.85 g) was less than the group 2 (3565.46 ± 473.00): p = 0.0029.
Conclusions: early diagnosis of gestational diabetes was associated with early therapeutic intervention, but not improved pregnancy outcomes.
maCrosomia PrEdiCtors in infants Born to CUBan motHErs WitH GEstational diaBEtEsJeddú Cruz Hernández, Raiden Grandúa, Pilar Hernández, Jacinto Lang, Antonio Márquez Guillén, Liset Padilla, Suilbert RodríguezNational Institute of Endocrinology, Havana, Cuba
Introduction: fetal macrosomia is the most important complication in infants of women with gestational diabetes. Its occurrence is related to certain maternal and fetal conditions and negatively affects maternal and perinatal outcomes.
Objective: identify which maternal and fetal conditions could be macrosomia predictors in infants born to Cuban mothers with gestational diabetes.
Methods: a case-control study comprising 236 women with gestational diabetes who bore live infants (118 with macrosomia and 118 without) was conducted in the América Arias Maternity Hospital, Havana, Cuba, during 2002-2012. The dependent variable was macrosomia (birth weight ≥4000g). Independent maternal varia-bles included body mass index at pregnancy onset, overweight or obesity at pregnancy onset, gestational age at diabetes diagnosis, pregnancy weight gain, glycemic control, triglycerides and cholesterol. Fetal variables examined included third-semester fetal abdominal circumference, estimated fetal weight at ≥28 weeks, absolu-te and percentilized by Campbell and Wilkin, and Usher and McLean curves. Chi square was used to compare continuous variables (proportions) and the student t test (X ± SD) for categorical variables, with significance threshold set at p <0.05. ORs and their 95% CIs were calculated.
Results: significant differences between cases and controls were found in most variables studied, with the exception of late gestational diabetes diagnosis, total fasting cholesterol and hypercholesterolemia. The highest OR for macrosomia were for maternal hypertriglyceridemia (OR 4.80, CI 2.34-9.84), third-trimester fetal abdo-minal circumference >75th percentile (OR 7.54, CI 4.04–14.06), and estimated fetal weight >90th percentile by Campbell and Wilkin curves (OR 4.75, CI 1.42-15.84) and by Usher and McLean curves (OR 8.81, CI 4.25–18.26).
Conclusions: most variables assessed were predictors of macrosomia in infants of mothers with gestatio-nal diabetes. They should therefore be taken into account for future studies and for patient management. Wide confidence intervals indicate uncertainty about the magnitude of predictive power.
PC4
PC5

47
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations 47
PrEdiCtion modEl for insUlin tHEraPy rEQUirEmEnt in PatiEnts WitH GEstational diaBEtEs mEllitUs diaGnosEd By first Visit fastinG Blood GlUCosEAna Claudia Souza1, Rafaela Costa1, Cristiane Paganoti1, Marcelo Zugaib2, Rossana Francisco2
1Obstetrics Division of Hospital Das Clínicas Da FMUSP. 2Department of Obstetrics and Gynecology of Faculda-de de Medicina da Universidade de São Paulo, Brazil
Introduction: since the proposition of the International Association of Diabetes and Pregnancy Study Group (IADPSG) consensus regarding diagnosis of GDM, the prevalence of this condition has increased among preg-nancies, particularly by the addition of a new group of hyperglycemic women: those diagnosed by altered fas-ting blood glucose (FBG) at the first prenatal visit.
Objective: to evaluate predictor variables of the insulin need in women diagnosed for GDM by the FBG at first prenatal visit.
Materials and methods: we performed an observational, retrospective cohort study by accessing clinical and laboratorial data from electronic medical chart of pregnant women that attended prenatal care in a tertiary teaching hospital in Sao Paulo city (Brazil) from 2012 to 2014. We included singleton pregnancies of women with GDM diagnosed by FBG according to IADPSG consensus (>=92mg/dL) before 24 gestational weeks. Exclusion criteria were: subjects who lost follow-up to antenatal visits, incomplete medical records, use of corticosteroids during pregnancy and pregnancies that did not progress beyond 20 gestational weeks. Primary outcome was the requirement of insulin therapy to achieve blood glucose targets. According to the primary outcome (insulin or diet group) subjects were compared regarding clinical and laboratorial variables. We performed a logistic regression model to estimate the performance of these variables in predicting insulin need for GDM treatment.
Results: a total of 354 women were identified and 299 were included for analysis. Among them, 117 (39%) needed insulin therapy. At the logistic regression model, maternal age, pre pregnancy obesity (body mass index >= 30kg/m2), FBG and prior GDM were significant independent variables in prediction of insulin need. The pro-babilities of insulin need according to these variables are presented in figure 1.
Conclusions: in women with GDM diagnosed by the first visit FBG, the need for insulin therapy can be predicted by a logistic regression model that includes maternal age, level of FBG, the history of prior GDM and the diagnosis of pre-pregnancy obesity.
Figura 1: Comparison of clinical chracteristics and perinatal outcomes in women with GDM according to IADPSG criteria. (Sao Paulo, n= 241).
dEPrEssiVE symPtoms aCCordinG to tHE EdinBUrGH dEPrEssion sCalE in WomEn WitH GEstational diaBEtEs mEllitUsKadhija Abrahim Cherubini, Pâmella Goveia, Patrícia Kluwe Viégas Damé, Georgia Das Graças Pena, María Angélica Antunes NunesUniversidade Federal do Rio Grande Do Sul, Brazil
PC7
PC6

48
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations48
Introduction: perinatal depression is highly prevalent and may cause adverse outcomes to mother and child. Gestational diabetes mellitus (GDM) also causes adverse outcomes and is related to depressive symp-toms, which may affect adherence to GDM treatment and compound pregnancy outcomes.
Objective: to assess the frequency of depressive symptoms according to the Edinburgh scale and its rela-tionship with sociodemographic characteristics in women with GDM.
Materials and methods: follow up study of 818 women with GDM who attended tertiary prenatal care facilities within the National Health System (SUS). Structured interviews provided information regarding socio-demographics. Depressive symptoms were assessed by the Edinburgh Postnatal Depression Scale (EPDS) and rated on a scale of 0-30. A score on the EDPS more or equal to 12 was used to classify the presence of clinically relevant symptoms. A score of 18 or more indicated severity of the symptoms. Suicidal ideation was evaluated by one specific question of the questionnaire. We used Poisson regression to estimate prevalence ratios and their 95% Confidence Intervals (PR ±95% CI) for the presence of elevated depressive symptoms (EPDS more or equal to 12) and the relationship with sociodemographic characteristics.
Results: most women were 30 to 39 years old (50%), lived with a partner (88%) and had an unfavorable socioeconomic position. Only 39% finished high school, and 39% had a family income within 1-2 minimum wages. Most women were obese (47%) before pregnancy. The overall frequency of depressive symptoms was 31,3%, of severe depressive symptoms 9,9% and of suicidal ideation 8,3%. The frequency of depressive symp-toms was lower among women living with a partner (0.6; 0.5-0.8) and having a higher household income (0.6; 0.4-0.8). The frequency of depressive symptoms was higher among women of lower education (2.4; 1.4-4.0).
Conclusions: the high proportion of pregnant women with GDM presenting depressive symptoms is worri-some, given their negative impact on pregnancy outcomes. Our results suggests the need to consider depres-sive symptoms in the management of women presenting a pregnancy complicated by gestational diabetes, especially among more vulnerable population.
sEssion d: maCrosomia and oBEsity
PlaCEnta PatHoloGy and nEonatal oUtComEs in oBEsE WomEn aCCordinG to diaBEtEs statUsTamara Welham1, Jenny Chen2, Alison Kent3, Bruce Shadbolt2, Jane Dahlstrom4, Cristopher Nolan5
1ACT Pathology, The Canberra Hospital, Canberra, ACT, Australia. 2ANU Medical School, Canberra, ACT, Australia. 3Department of Neonatology, The Canberra Hospital and ANU Medical School, Canberra, ACT, Australia. 4ACT Pathology, The Canberra Hospital and ANU Medical School, Canberra, ACT, Australia. 5Department of Neonatology, The Canberra Hospital and ANU Medical School, Canberra, ACT, Australia
Introduction: maternal obesity is often associated with pregnancy complications which are often thought to be related to placental dysfunction which may be worsened by the presence of diabetes.
Aims: to assess the placenta pathological findings and baby outcomes of high BMI women by diabetes status. Methods: a 3 year prospective clinical audit was carried out on all placentas from women with a BMI > 39
kg/m2 delivering at our institution. Relevant clinical history including diabetes status, macro- and microscopic pla-cental pathologies were recorded. Statistical analyses were carried out using SPSS v22.0. Published percentile distributions on placenta weights and baby outcomes were compared to the study sample by diabetes status of the mother using χ2 tests. One-way ANOVA was used for comparing continuous data variables between groups.
Results: The cohort consisted of 205 women (age 31.5±5.9 yrs; gestational age at 37.8±3.0 wks; BMI 44.7±5.5 kg/m2 at delivery) having live singleton births (53.2% male). Of these 58.5% were not diabetic; 15.6% GDM-diet (D); 23.9% GDM-insulin (I) and 2% type 2 diabetes (T2D). Due to the low number of T2D patients (n=4), these pregnancies were excluded in the further analyses. Compared to normative data, 22.9%, 23.4% and 26.3% had, respectively, a birth weight, head circumference and placental disc weight >90th centile. Mo-thers without diabetes were more likely to have premature rupture of membranes (21%, 6%, 4%; no diabetes, GDM-D, GDM-I; p=0.007), acute chorioamnionitis (25%, 9%, 8%; p=0.013) and delivery <37 weeks (25%, 3%, 8%; p=0.002). However, chorioamnionitis was evident in only 11.4% of the premature births. Of those babies born ≥37 wks (n=170), there was no significant difference in birthweight (3679±539g, 3825±475g, 3569±518g; p=0.14), head circumference, placental disc weight (552±120g, 563±88g, 563±120g; p=0.94) or thickness, rates of chorangiosis, chronic villitis or villous dysmaturity.
Conclusions: obese women, irrespective of the presence of GDM-D or GDM-I, had higher rates of heavier
Pd1

49
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations 49
neonates and larger placentas than women of the general population. Women without diabetes had higher rates of premature birth and chorioamnionitis, but the chorioamnionitis was not significantly associated with premature birth. This may relate to closer management of obese women once GDM is diagnosed.
rElationsHiP BEtWEEn matErnal HyPErtriGlyCEridEmia and maCrosomia in GEstational diaBEtEsMaría Inés Argerich, Andrea Bochini, Raúl Alejandro David, Adriana Funez, Víctor PreviteraHospital Perrupato San Martín, Mendoza, Argentina
Objective: to determine the relationship between macrosomia and maternal hypertriglyceridemia in gesta-tional diabetes.
Methods: medical records were analized during october 2006 to october 2015. We classified pregnant GD women in order if the maternal serum triglyceride was over 250mg/dl or between 150mg/dl and 250mg/dl, and the presence of fetal macrosomia outcome in both groups.
Results: 137 medical reacord were included for the analisis. We detected a total of 20 macrosomic new borns (NB).The sample had the following distribution: 13 NB with macrosomia and maternal serum triglyceride less than 250mg/dl; 7 NB with macrosomia and maternal serum triglyceride over 250mg/dl; 77 NB without macrosomia and maternal serum triglyceride less than 250mg/dl and 40 NB without macrosomía and maternal serum triglyceride over 250mg/dl. The mean for maternal age was 30 years old (ESM: 0.53 IC 95%: 28,86-31,13 DS: 4,5-5,8); the mean pregastational BMI was 29,2 (ESM: 0,66 IC 95%: 27,97-30,53 DS: 5,38-7,53) the mean maternal serum tri-glyceride was 239,59 mg/dl (ESM: 9,98 IC 95%: 220,7-258,4 DS: 77,7-113,4) the mean of hba1c was 5,85 (ESM: 5,8 IC 95%: 5,69-6,02 DS: 0 ,66-0,95) The prevalence of macrosomia in this group was 14%. The AR of macroso-mia in the group that maternal serum triglyceride was over 250mg/dl is 14.8% while the AR of macrorsomia in the group that maternal serum triglyceride was less than 250mg/d is 14.4%. The RR is 1. The odds of macrsomia in the group that maternal serum triglyceride was over 250mg/dl is 17.5% while the odds in macrosomia in the group that maternal serum triglyceride was less than 250mg/dl is 16.8%. The OR: 1.04
Conclusions: the results of this análisis shows that; in this population; there is no relationship between ma-ternal serum triglyceride levels and macrosomía outcome in gestational diabetes with optimal glucose control.
rElationsHiP BEtWEEn fEtal maCrosomia and matErnal WEiGHt Gain dUrinG Gd PrEGnanCyMaría Inés Argerich, Raúl Alejandro David, Andrea Bochini, Víctor Previtera, Adriana FunezHospital Perrupato San Martín, Mendoza, Argentina
Objectives: to determine the risk of macrosomía in pregnancy with GD, BMI › 24 and its relation with exe-sive weigt gain.
Methods: medical records of GD patients have been evaluated by the clinic diabetic unit from October 2006 to October 2015. Only patients with BMI › 24 were included for the analysis. The group observed was categorized according to the weight gain (›10kg or ‹10kg) and macrosomia outcome (yes-no). SPSS v.19.0 was used for analysis.
Results: 104 patients with GD fullfilled the inclusion criteria. The gestational age mean of 1st diabetic con-sult is 30 weeks (ESM: 0.52 CI 95% 29.19 to 31.51 DS: 3.9-6.4) maternal age mean is 30.7 years old (ESM : 0.54 CI 95% 29.4-31.8 DS: 4.3-6.07) the BMI mean is 32 (ESM: 0.54 CI 95% : 30.4-33.01 DS: 4.23-6.66) HbA1c mean is 5.8 (ESM: 0.08 CI 95%: 5.6-6.0 DS 0.58 to 0.85). The prevalence of macrosomia is 16%; the sensitivity is 70%, specificity is 55%. The AR of macrosomia in the group that gained more than 10kg weight is 23% com-pared to 9.4% in the AR group that gained less than 10kg weight. The RR is 2.44. The odds of macrosomia in › 10kg weight gain is 30%. The odds of macrosomia in ‹ 10kg weight gain is 10%. The OR is: 3. The PPV is 23% and the NPV is 90% .
Conclusions: the HbA1c mean was 5.8 (ESM: 0.08 CI 95%: 5.6-6.0 DS 0.58 to 0.85) reflecting that this group reached HbA1c target parameters control, so macrosomia isn’t caused by glicemic control in this popula-tion. More than10 kgs maternal weight gain in DG with preconception BMI more than 24 is a marker of risk for the development of macrosomía so its detection and timely approach with adequate control of maternal weight gain during the course of pregnancy is indispensable to prevent adverse maternal and fetal consequences.
Pd2
Pd3

50
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
matErnal mEtaBoliC risK and oBEsity dUrinG PrEGnanCy: a lonGitUdinal stUdy in adUlt and adolEsCEnt mExiCan WomEnOtilia Perichart-Perera1, Cinthya Muñóz Manrique1, Angélica Reyes-López1, Maricruz Tolentino-Dolores1, Salva-dor Espino y Sosa2, María Cristina Ramírez González1
1Instituto Nacional de Perinatología. 2Instituto Nacional de Medicina Genómica, Ciudad de México, D.F., México
Introduction: obesity during pregnancy increases the risk of adverse clinical outcomes. Metabolic and inflammatory alterations have been reported in complicated pregnancies (gestational diabetes-GDM, obesity).
Objective: to describe prospectively metabolic and inflammatory markers during pregnancy and compare these markers by age, pregestational obesity and weight gain.
Materials and methods: prospective cohort; pregnant women <14 weeks of gestation, receiving prenatal care at National Institute of Perinatology (Mexico City, 2009-2013). Women were excluded if: multiple pregnan-cy, medication use that affect metabolism. Elimination criteria included: GDM, preeclampsia, and lacking two blood measurements. Women were followed up monthly. Serum analysis of glucose, insulin, lipid profile, leptin, adiponectin, TNF-alfa,IL-1b, IL-6 and CRP was done each trimester; HOMA index was calculated. Pregestational body mass index (p-BMI) and weight gain were evaluated (IOM,2009). Statistical analysis included descriptives, correlations Pearson/Spearman, mean differences-One way ANOVA, Student t-test, longitudinal differences (re-peated measures ANOVA) (SPSS, 20.0).
Results: a total of 180 women were studied (20.7% desertion, 23.7% elimination). Mean age was 27.8+-8.5 years old (25% were adolescents). Forty two percent of women were overweight or had obesity; 33% showed excessive weight gain. Differences were observed between adult and adolescent women: higher TC in adults (1st trimester); higher TAG, HDL-C, CRP, and lower leptin in adults (3rd trimester) (p<0.05). During pregnancy, insulin, lipids and leptin increased in all women (p<0.05). In adolescents, IL-6 was increased (p=0.008), and glucose showed a decrease during the 2nd trimester (p=0.017). Adiponectin was not decreased throughout pregnancy. BMI correlated with insulin and leptin in all trimesters (all r>0.232; p<0.01); and overweight/obese women showed higher TAG in 2nd and 3rd trimesters and higher CRP in 1st and 3rd trimesters (p<0.05). In the 3rd trimester, BMI correlated with CRP (r=0.229, p=0.004); weight gain correlated with insulin levels and HOMA (r=0.268 and r=0.302, p<0.001, respectively).
Conclusions: leptin, insulin and lipids are increased during pregnancy in Mexican women. In addition, some biomarkers appears to be different by age, pregestational body mass index and gestational weight gain in diffe-rent stages of pregnancy.
PHysiCal aCtiVity, sEdEntary BEHaVior and HaBits in adolEsCEnts of PataGonia: an oPPortUnity for Early PrEVEntion of oBEsityGraciela Ponce, Jorge García, María Rodríguez, Andrés QuezadaUniversidad Nacional de la Patagonia San Juan Bosco, Argentina
Introduction: the prevalence of overweight and obesity in childhood and adolescence in the developed world and much of the developing word is rising and continues to increase. The energetic imbalance that causes obesity is often due to a lack of control on the intake or on energetic expenditure.
Objective: to describe the lifestyle of a group of adolescents of Patagonia in relation to physical activity and eating habits.
Methods: 403 volunteers (280 females and 123 males) aged 12 to 16 were studied with their parent written consent. Using a validated survey data of physical activity (IPAQ International Physical Activity Questionnaire) that allowed the classification in inactive teenagers, regularly and irregularly active data assets; besides, eating habits were collected. Anthropometry, blood pressure and waist circumference were measured, and body mass index was calculated. Adolescents had fasting total cholesterol (CT), low-density lipoprotein choleste-rol (LDL-C), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C) and glucose assays (G) (photometry spectrum). The population was classified as eutrophic or overweight/obese by body mass index (BMI) (IOTF criteria) and waist circumference percentile (PcW) (WHO).
Results: 39% of the general population was overweight or obese by BMI and 21% when the PcW was con-siderated. Medians values and 25, 75 quartiles of quantitative variables studied were: systolic blood pressure (SBP): 114 (107-120), diastolic blood pressure (DBP): 65 (60-71), CT: 155 (140-175), LDL-C: 89 (73-103), TG: 63
50
Pd4
Pd5

51
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
(47-91), HDL-C: 53 (46-61) and G: 83 (77-90). The overweight and obese adolescents had higher levels of SBP and DBP, G and TG, and lower concentration of HDL-C (p<0.01). In relation to physical activity, 2 % were inactive, 42 % regularly active and 56% irregularly active. The average stay before screen was 5 hours. 17% didn´t have breakfast and 70% consumed sugary drinks, mainly cola, at least 3 days a week, with limited consumption of fruits and vegetables. 4 % informed the cigarettes habits.
Conclusions: based on the results obtained, it is observed that the studied adolescents are developing in an obesogenic environment which requires an immediately intervention. The infancy and adolescence could be ap-propriate times of health intervention for reduce the global prevalence of obesity and its future consequences.
risK faCtors assoCiatEd to fEtal maCrosomiaMaría Ortiz1, Pablo Pochettino2, Lina Capurro1, Laura Mercanzini2, Liliana Rodota3, Julieta Lofrano3
1Servicio de Endocrinología, Metabolismo y Medicina Nuclear, Hospital Italiano de Buenos Aires. 2Servicio de Obstetricia, Hospital Italiano Agustín Rocca. 3Servicio de Alimentación, Hospital Italiano Agustín Rocca, Argentina
Introduction: macrosomia is defined as birth weight greater than 4000 g. Related risk factors are gestatio-nal diabetes, maternal age, maternal height >1.65cm, preconceptional overweight, multiparity, >20kg of weight gain during pregnancy, overdue pregnancy, and history of macrosomia in previous pregnancies, among others. Macrosomia brings fetal complications such as shoulder dystocia at birth, broken collarbone, cephalohemato-ma, hypoxia and risk of metabolic syndrome in adulthood, and obstetric complications such as greater number of caesarean and perineal tears.
Objective: to describe the incidence of risk factors in our cohort of patients who delivered macrosomic children, and to determine predictors of fetal macrosomia.
Materials and methods: retrospective descriptive study of a transversal cohort of 127 pregnant patients with macrosomic newborns, in the period 9/2011 to 1/2015. Inclusion criteria: pregnant women with children born with >4000g, which had full anthropometric data from the beginning to the end of pregnancy. They had an OGTT done at week 24, unless they had a previous diagnosis of diabetes.
Results: of the total births in this period (n=3448), 200 were macrosomic (prevalence 5.8%). Of them, 127 fulfill inclusion criteria. Maternal age media 30.6 years (16 - 43 y/o); BMI media 26.27+/-4.42 k/m2; Gestational age at delivery 39.3+/-0.96 weeks. Risk factors: gestational diabetes 5,69% (n=7), previous gestational dia-betes 3 (3.03%), previous macrosomy 13.40% (n=13), weight gain during pregnancy 17.73kg +/-7.27; > 20kg weight gain during pregnancy 39.2% (n=49), preconceptional BMI >25: 53.17% (n=67), age >30 years 53.17% (n=67), multiparous 29.92% (n=38). In reference to the following risk factors (previous macrosomia, gestatio-nal diabetes previous pregnancies, gestational diabetes in this pregnancy, age> 30, BMI at baseline >25 and increase >20kg) 12.6% had no risk factors (n=16). 1 risk factor 33.07% (n=42), 2 risk factors 37.01% (n=47) 3 risk factors 15.75% (n=20) and 5 risk factors 1.57% (n=2). Caesarean section was done in 72.44% (n=92), whereas 26.77% (n=34) has vaginal delivery. 1 patient required use of forceps (0.79%). In the same period, 154 pregnant women had gestational or pre-gestational diabetes: 12 (7.79%) had diabetes diagnosed before pregnancy and 142 (92.21%) had gestational diabetes. Among diabetic women, only 7 delivered a macrosomic children (Frequency 4.54%). Gestational diabetes prevalence in the whole population of pregnant women in the studied period was 4.11%.
Conclusions: only 12.6% (n=16) of patients had no risk factor associated with macrosomia. The most com-mon risk factors were age> 30 years, BMI at baseline> 25 and an increase > 20kg of body weight during preg-nancy. Gestational diabetes occurred in only 5.69% of the patients. We found a 5.8% prevalence of macrosomia.
imPaCt of diaBEtEs and maCrosomia in tHE roBson’s 10 GroUPs ClassifiCation for CEsarEan sECtionClaudia Bolognani, Lilian Reis, Adriano Dias, Iracema de Mattos Paranhos CalderonFaculdade de Medicina de Botacatu, UNESP, Brazil
Introduction: maternal Diabetes Mellitus (DM) and fetal macrosomia, exclusively or in association, are important causes of cesarean section (CS) and, therefore, have contributed to their increase rates. Considering that Robson’s ten groups classification (RTGC) includes only obstetric characteristics it is justified to investigate the impact of these conditions on CS rates.
51
Pd6
Pd7

52
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
Objective: to assess the impact of DM and macrosomia association on the CS rates, using RTGC system. Methods: a cross-sectional study of all attended births, in one year period, in two maternity of Public Health
System (SUS), Brasilia, Brazil. We analyzed the prevalence of CS deliveries and the frequency of pregnant wo-men with and without DM (DM1, DM2, GDM) and/or macrosomia in each group of RTGC. CS relative frequency was compared among groups (Pearson chi-square test), and odds ratio (OR) and confidence interval (IC95%) were calculated in groups where DM and/or macrosomia impacted the CS indication (p < 0.05).
Results: among of 6579 births, 3181 (48.4%) were by CS. DM and/or macrosomia were associated with 174 indications (5.5%). Considering the RTGC, DM and/or macrosomia were associated with increased CS rates in G2 (28.7 vs 15.0%; p <0.001), G3 (11.5 vs 5.0%; p=0.009) and G4 (17.8 vs 6.6%; p<0.001) groups, with OR (IC95%) corresponding to 2.3 (1.67 - 3.21), 2.4 (1.489 - 3.996) and 3.0 (2.033 - 4.654), respectively.
Conclusion: the prevalence of CS was 48.4%. DM and/or macrosomia represented increased risk [two to three times] for CS in pregnant women with singleton pregnancy, cephalic presentation, and no previous CS. These results reinforce two important advices “avoid the first CS delivery to reduce high CS rates”, and “CS has no absolute indication, even in pregnancies complicated by DM and/or macrosomia”.
Group obstetric characteristcs dm-macrosomia total
yEs no p*
G1 Nulliparous, single cephalic, ≥ 37 weeks, spontaneous labor
38/174 (21.8%)
584/3007 (19.4%) 0.452 622
G2 Nulliparous, single cephalic, ≥ 37 weeks, induced or CS before labor
50/174 (28.7%)
452/3007 (15.0%) <0.001 502
G3 Multiparous (exscluding previous CS), single cephalic, ≥ 37 weeks, spontaneous labor
20/174 (11.5%)
152/3007 (5.0%) 0.009 172
G4 Multiparous (exscluding previous CS), single cephalic, ≥ 37 weeks, induced or CS before labor
31/174 (17.8%)
198/3007 (6.6%) <0.001 229
G5 Previous CS, single cephalic, term 33/174 (18.9%)
1045/3007 (34.8%) <0.001 1078
G6 All nulliparous breeches - 110/3007 (3.7%) - 110
G7 All multiparous breechs (including previous CS) 1/174 (0.5%)
91/3007 (3.0%) 0.061 92
G8 All multiple pregnancies (including previous CS) - 84/3007 (2.8%) - 84
G9 All abnormal lies (including previous CS) - 21/3007 (0.7%) - 21
G10 All single cephalic, £ 36 weeks (including previous CS)
1 (0.5%)
270/3007 (9.0%) <0.001 271
total 174/3181 (5.5%)
3007/3181 (94.5%) 3181
*Pearson Chi-Square test.
Table 1: Relative frequency of cesarean section, according to the association or not of diabetes mellitus (DM1, DM2, DMG) and/or macrosomia in Robson’s System.
Group obstetric characteristcs dm-macrossomia
or iC95%
G2 Nulliparous, single cephalic, ≥ 37 week, induced or CS before labor 2.3 1.67 - 3.213
G3 Multiparous (exscluding previous CS), single cephalic, ≥ 37 week, spontaneous labor 2.4 1.489 - 3.996
G4 Multiparous (exscluding previous CS), single cephalic, ≥ 37 week, induced or CS before labor 3.0 2.033 - 4.654
Table 2: Impact of DM and/or macrosomia at increased risk for cesarean section in Robson’s System.
52

53
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
matErnal and fEtal oUtComEs in PrEGnanCy ComBinEd WitH oVErWEiGHt and oBEsityJoice Vernini, Mariana Alvarez Arantes, Bianca Fioravanti Nicolosi Cassettari, Debora Cristina Damasceno, Maril-za Viera Cunha Rudge, Iracema de Mattos Paranhos CalderonFaculdade de Medicina de Butucatu, UNESP, Brazil
Introduction: overweight and obesity increases the risks of pregnancy complications and adverse perinatal outcomes, posing short- and long-term risks for maternal and child health.
Objective: to assess delivery, maternal and child outcomes in pregnancies associated with overweight and obesity.
Method: the descriptive prospective study included 258 pregnant women.According to prepregnancy body mass index (BMI), the women were classified into: normal weight, overweight and obese. Data were analyzed using the chi-square test and analysis of variance followed by the Tukey test, and logistic regression was perfor-med to calculate odds ratio and 95% confidence interval (p<0.05).
Results: most women ≥35 years old were overweight and obese (p<0.001). Prepregnancy diabetes was significantly associated with obesity (15.74%). Obese women showed the lowest weight gain (9.56 ± 7.50 Kg). Overweight and obese women practiced physical exercise more frequently (p=0.0100) than the other. A greater proportion of obese mothers (13.39%) had large for gestational age babies (p=0.0209), with higher thoracic cir-cumference (33.58 ± 2.01 cm) and abdominal circumference (31.60±2.30 cm). Overweight and obesity increa-sed the risk of developing gestational hypertension (OR: 2.11, CI 95%: 1.13-3.94), gestational diabetes mellitus (OR: 7.01, CI 95%: 3.10-15.88), and mild gestational hyperglycemia (OR: 5.52, CI 95%: 2.88-10.57). The infants born to obese mothers had longer hospital stay (3.86 ± 3.93) (p = 0.005).
Conclusion: the results confirm that obesity in pregnancy can lead to adverse outcomes and underscore the importance of identifying and treating inadequate weight status during pregnancy.
adiPoKinEs and insUlin in PrEGnanCy ComPliCatEd By oVErWEiGHt and oBEsity: PrEliminary rEsUltsJoice Vernini, Mariana Alvarez Arantes, Bianca Fioravanti Nicolosi Cassettari, Debora Cristina Damasceno, Maril-za Viera Cunha Rudge, Iracema de Mattos Paranhos CalderonFaculdade de Medicina de Butucatu, UNESP, Brazil
Objective: to evaluate maternal adipokine and insulin levels in pregnancies complicated by overweight and obesity and correlate them to maternal and fetal outcomes.
Methods: the cross-sectional study included 72 mother-newborn pairs, classified into normal weight (N=23); ober weight (N=18) and obese (N=31). Adiponectin, leptin, resistin and insulin levels at the end of preg-nancy were compared among weight classes, and correlated with maternal and perinatal outcomes. Data were analyzed by ANOVA and correlation tests, with at a significance level of p< 0.05.
Results: obese pregnant women showed higher leptin levels (p =0.0021), which correlated positively with prepregnancy BMI (r=0.57), gestational BMI (r = 0.39), hypertension (r=0.27), and hyperglycemia (0.31), and negatively with newborn abdominal perimeter (r=-0.25). Adipokine concentration correlated negatively with gestational BMI (r=-0.29) and newborn cephalic perimeter (r= -0.27) and positively with birth weight (r=0.23). Insulin concentrations correlated positively with prepregnancy BMI (r=0.38), gestational BMI(r=0.24) and ma-ternal hyperglycemia (r=0.26).
Conclusion: insulin and leptin levels are associated to maternal weight status and insulin resistance during pregnancy, and adiponectin is related to maternal weight status and intrauterine growth.
53
Pd8
Pd9

54
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
sEssion E: translational sCiEnCEs, BiomarKErs and intErVEntions
mECHanism of EndotHElial dysfUnCtion indUCEd By HiGH d-GlUCosE in HUman UmBiliCal EndotHEliUmMarcelo González, Cristina Valenzuela, Roberto Villalobos, David Gallegos, Susana RojasUniversidad de Concepción, Concepción, Chile
Introduction: nitric oxide (NO) synthesis depends of L-arginine uptake, which is mediated by the activity and subcellular distribution of the human cationic amino acid transporter 1 (hCAT-1). High D-glucose (25 mM) increases NO and reactive oxygen species (ROS) synthesis in human umbilical vein endothelial cells (HUVEC). Our aim was to describe the mechanisms underlie the effects of high D-glucose on NO and ROS synthesis.
Methods: HUVEC isolated (collagenase digestion) from human umbilical cords (ethics committee approval and informed patient consent were obtained) were cultured in medium 199 (M199) plus sera. After incubation (0-30min/0-24h) with 5 or 25 mM D-glucose, L-arginine transport (100 μM L-arginine, 2μCi/ml L-[3H]arginine, 1 min, 37°C), NO (DCF) and ROS (DAF) were determined. Gene and protein expressions were determined (RT-PCR, western blot and confocal microscopy). In some experiments proteins from plasma membrane were separated through ultracentrifugation or biotynilation of extracellular proteins.
Results: high D-glucose increased L-arginine uptake after 10 (3±0.7-fold) and 30 (3±0.6-fold) min. Acute incubation not alter ROS but increases NO levels 2.4-fold and 2.8-fold (10 and 30 min, respectively). Long term incubation increased L-arginine uptake (3-fold), ROS (1.8-fold) and NO (1.5-fold). High D-glucose increased mRNA (6-fold) and protein (2.7-fold) for hCAT-1 and mRNA (1.5-fold) and protein (1.7-fold) for catalytic subunit 4 of NADPH oxidase (NOX-4). The effects of high D-glucose (25 mM, 24 h) on ROS and gene expression were blocked with inhibitor of protein kinase C (PKC), p38mapk and NADPH oxidase. High D-glucose increases the hCAT-1 protein abundance in plasma membrane and biotinylated proteins (1.6-fold), without changes in cytosol. Confocal microscopy images showed high hCAT-1 expression in HUVEC exposed to high D-glucose (2.6-fold increase), with higher fluorescence in non-permeabilized cells.
Conclusions: acute effect of high D-glucose is related with increases of L-arginine/NO pathway, without changes in ROS levels. Long term incubation with high D-glucose maintains the activation of this pathway but there is a concomitant activation of NADPH oxidase/ROS pathway. The pathophysiological mechanism induced by high D-glucose includes a higher expression of hCAT-1 in plasma membrane and the activation of a signaling pathway that include activation of PKC and p38mapk.
sUPraPHysioloGiCal GEstational WEiGHt Gain WorsEns GEstational diaBEtEs mEllitUs-dECrEasEd adEnosinE transPort and nitriC oxidE syntHEsis in HUman UmBiliCal VEin EndotHEliUmFabián Pardo, L Silva, E Barros, R Salsoso, T Saez, R Villalobos, M Subiabre, C Sanhueza, A Leiva, L SobreviaDivision of Obstetrics and Gynaecology, Faculty of Medicine Pontificia, Universidad Católica de Chile, Santiago de Chile, Chile
Introduction: supraphysiological gestational weight gain (spGWG) regards with excessive GWG in mothers with normal pregestational body mass index. These women course with altered placental vascular function and show higher risk of developing gestational diabetes mellitus (GDM). GDM associates with increased nitric oxide (NO) synthesis, via endothelial NO synthase (eNOS), and mitogen–activated protein kinases 1 and 2 (MAPK1/2) activity, increased activity of C/EBP homologous protein 10 (hCHOP) at SLC29A1 (for hENT1) and reduced ade-nosine transport via human equilibrative nucleoside transporters 1 (hENT1).
Aims: to evaluate whether spGWG worsens GDM–associated endothelial dysfunction. Methods: human umbilical vein endothelial cells (HUVECs) were isolated from normal or GDM pregnancies
where the mother coursed without (N or GDM) or with spGWG (N+spGWG or GDM+spGWG). NO synthesis (as L-citruline formation) was measured in the absence or presence of 100 µmol/L NG-nitro-L-arginine methyl es-ter (NAME, NOS inhibitor). Adenosine transport (31–250 µmol/L, 3 µCi/mL, 25ºC, 20 seconds) was determined in the absence or presence of 10 µg/mL chlorpromazine (CPZ, endocytosis blocker) or 1 µmol/L nitrobenzylthioi-nosine (NBTI, hENTs inhibitor), hENT1 expression was detected by immunofluorescence, and total and Ser1177
54
PE1
PE2

55
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
(P-Ser1177eNOS) or Thr495 (P-Thr495eNOS) phosphorylated eNOS, hENT1, and hCHOP protein abundance in the absence or presence of 10 µmol/L PD-98059 (MAPK1/2 inhibitor), 100 µmol/L NAME or 100 µmol/L sodium nitroprusside (SNP, spontaneous NO donor) was evaluated by Western blots. Expression of mRNA was measu-red by qRT-PCR. hCHOP activity was measured by chromatin immunoprecippitation.
Results: hENT1–adenosine uptake was equally diminished in N+spGWG (~56%) and GDM (~42%), but fur-ther reduced in GDM+spGWG (~98%) compared with N, a result unaltered by CPZ. hENT1 protein abundance and mRNA expression were higher in N+spGWG (~1.7 and ~3-fold, respectively), but lower in GDM (~60 and 50%, respectively) and GDM+spGWG (~60 and 50%, respectively) compared with N. Lower hCHOP binding to SLC29A1 promoter (~52%), but higher total protein abundance (~1.6 fold), and reduced hENT1 protein abun-dance in response to SNP (~40%) was seen only in N+spGWG. NO synthesis and eNOS mRNA expression were lower in GDM+spGWG (~72 and ~90%, respectively) and N+spGWG (~91 and ~72%, respectively) compared with N or GDM. Higher P-Ser1177eNOS in GDM (~1.6 fold) and P-Thr495eNOS in N+spGWG (~2 fold), without changes in GDM+spGWG compared with N, was found. MAPK1/2 phosphorylation was higher in N+spGWG (~1.6 fold) and GDM+spGWG (~1.4 fold), an effect blocked by PD-98059. This inhibitor associates with higher P-Ser1177eNOS (~1.8-fold), without altering total eNOS protein abundance in GDM+spGWG, with no effect observed in the others groups.
Conclusion: spGWG is a condition that worsens GDM-associated fetoplacental endothelial dysfunction. Support: FONDECYT 11150083, 1150377, 1150344, 3140516, Chile. LS, RS, and TS hold CONICYT Chile-PhD
fellowships. LS, EB, and RS hold Faculty of Medicine, PUC-PhD fellowships. RV and MS hold Vicerectorate of Research, PUC-PhD fellowships.
CorrElation BEtWEEn CliniCal CHaraCtEristiCs, PErinatal oUtComEs and PlaCEntal VasCUlar rEaCtiVity in CHilEan WomEn diaGnosEd WitH GEstational diaBEtEs mEllitUsMarcela Cid, Katia Sáez, Luz Valdivia, Marcelo GonzálezUniversidad de Concepción, Concepción, Chile
Introduction: gestational diabetes mellitus (GDM) is the intolerance to the carbohydrates that starts or is recognized during pregnancy. GDM increases the risk of placental dysfunction and cardiometabolic diseases. Therefore, its identification and study is an important strategy of prevention and health promotion. Chile has a high prevalence of diabetes; nevertheless, there are no recent reports in Chilean population from Biobío region that correlates clinical parameters perinatal outcomes of GDM pregnant women.
Aim: analyze the correlation between clinic characteristics, perinatal results and placental vascular reactivity in women with GMD and normal pregnancies.
Methods: quantitative and observational study, made in with patients from Guillermo Grant Benavente Hos-pital (GGBH), in Concepción, Chile (ethics committee approval and informed patient consent were obtained). The sample studied considered 150 term pregnant women (37 weeks), of which 42 (28%) have GDM. Familiar and personal history, body mass index (BMI), birth’s type and newborn’s weight were analyzed. Placentas were obtained and a cotyledon was cannulated and continuously perfused with a Krebs solution (95% O2/5% CO2, pH 7.4, 37°C). After stabilization, effects of U46619 (vasoconstrictor) (5 nM) and/or insulin (0.1 nM) on perfusion pressure were determined. Also, total RNA was isolated from placental vessels to determine changes in gene expression of human cationic amino acid transporter 1 (hCAT-1).
Results: during the first semester of 2013, 9-10% of women attended in GGBH correspond to GMD diag-nostic, being this percentage almost the double of national report. Average age of the sample collected was 28.6 years, with a range between 18 and 44 years old. There was significant differences (p<0.0001) between GDM women and normal women with a media of 32.4 and 27.2 years old for each group, respectively. There are not significant differences in BMI between normal and GDM woman: average BMI at early pregnancy was 29.1±5.7 kg/m2, ranging between 18.7 and 49.3 kg/m2. In regard with family history, 69% of GDM wo-men had family history of diabetes, a higher percentage (p=0.0018) than normal pregnant with family history of diabetes (39.8%). The weight of newborns from GDM or non-diabetic mothers was similar with average weight of 3553±485 gr (2260-4700 gr) and average height of 50.9±1.9 cm. However, considering the nutritional classification of these infants, 35.7% of children from GDM were classified as large for gestational age (LGA), compared with the 14.8% of newborn from women without diabetes (p= 0.0173). Comparing the way of birth, cesarean intervention was required in 76.2% and 39.8% of GDM and normal pregnant women, respectively (p=0.0173). In GDM-placenta was registered a 3-fold higher (p<0.05) perfusion pressure with U46619 (10 nM)
55
PE3

56
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
and the normal relaxation induced by insulin was not observed. These alterations in vascular reactivity in GDM were associated with decreases of 48% and 17% in hCAT-expression in chorionic vein and chorionic artery of placenta, respectively.
Conclusions: there are a large percentage of overweight women in early pregnancy, independently if they develop GDM during pregnancy. This parameter could not be directly associated with GDM, but the family history of diabetes showed a strong correlation with GDM. In placenta, GDM induces an increases in vascular reactivity related with lower expression of hCAT-1, a key protein for endothelium-dependent vasodilatation. These adaptations could be a result of a gestational environment that, at the end, induces LGA babies and high rate of cesarean interventions. Supported by VRID-Asociativo 213.A84.014-1.0 (Universidad de Concepcion).
GEstational diaBEtEs mEllitUs lEads to inCrEasEd total and ldl CHolEstErol assoCiatEd WitH matErnal sUPraPHysioloGiCal HyPErCHolEstErolEmiaAndrea Leiva, Bárbara Fuenzalida, Rocío Salsoso, Fabián Pardo, Luis SobreviaPontificia Universidad Católica de Chicle, Santiago de Chile, Chile
Introduction: maternal supraphysiological hypercholesterolemia (MSPH) leads to placental endothelial dys-function a likely key phenomenon in MSPH-associated adult cardiovascular disease of the offspring.
Aim: since dyslipidemia has been described in pregnancies with gestational diabetes mellitus (GDM) the aim of this work was to evaluate if MSPH condition will be worsened by a metabolic condition as GDM.
Methods: total-(TC), low density lipoprotein-(LDL-C) and high density lipoprotein- cholesterol (HDL-C) as well as triglycerides were determined in each trimester of pregnancy in women from Hospital Clínico PUC with normal (N, n=100) or GDM pregnancies (n= 101). Both groups were sub-divided as maternal physiological hypercholesterolemia (MPH) or MSPH (cut-point >280 mg/dl for maternal total cholesterol at term) and the ma-ternal and newborn characteristics were tabulated. Values are mean and SEM. Significance: p<0.001, ANOVA and Bonferroni post-test.
Results: GDM was associated with increased glycemia 2 hours after glucose intake, HOMA and glycosyla-ted hemoglobin A1C at the second trimester of pregnancy compare with N. No differences were determined in maternal age, height or basal glycemia and weight, body mass index and systolic pressure in each trimester of pregnancy between the groups. Dyslipidemia was not determined in GDM compare with N in any trimester of pregnancy. However, when the groups were sub-divided in MPH and MSPH, GDM-MSPH (30% of the GDM population) was associated with increased TC and LDL-C (346±4.8 and 192± 4.4 mg/dl) compare with N-MSPH (301±4.6 and 160± 4.1 mg/dl).
Conclusion: the data suggest that MSPH is worsened in GDM a phenomenon that could be relevant in the endothelial dysfunction described in GDM.
Support: FONDECYT (1150344, 1150377, 11150083).
first trimEstEr mUltiParamEtriC modEl for PrEdiCtion of GEstational diaBEtEsPaula Correa1, Ignacio Valenzuela1, Pía Venegas1, Stephanie Acuña1, José Galaz1, María Jesús Chavarri1, Yasna Palmeiro1, Gregory Rice2, Sebastián Illanes1
1Department of Obstetrics and Gynaecology, Faculty of Medicine, Universidad de los Andes, Chile. 2Centre for Clinical Diagnostics, Royal Brisbane and Women’s Hospital, University of Queensland, Australia
Introduction: gestational diabetes (GDM), defined as carbohydrate intolerance with onset or first recogni-tion during pregnancy, has a prevalence of 9% and is a growing problem, specially related to obesity epidemic among young women. It is crucial to screen and make accurate diagnosis because of the short and long term complications. Macrosomia, a frequent consequence, carries a series of fetal and neonatal secondary adverse events. Long-term effects for the mother and child are high cardiovascular risk, with higher incidence of obesity, diabetes, dyslipidemia and hypertension. This could be explained by fetal programming in response to an adver-se intrauterine environment. Nowadays diagnosis is made during third trimester, and treatment reduces short--term complications. To impact long-term complications an early prediction of the pathology has to be made to allow early interventions.
Aim(s): to create a multiparametric prediction model applied during the first trimester in national unselected
56
PE4
PE5

57
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
population, based on maternal and family history, biophysical and biochemical variables. Methods: we recruited 200 women at their first pregnancy control and took blood samples and completed
a questionnaire for maternal medical and obstetric history. We measured cholesterol, LDL, HDL, triglycerides, plasma glucose, insulin, glycated hemoglobin, uric acid, liver enzymes, and inflammation markers. Factors were integrated in a multiparametric model.
Results: from the recruited patients 14.72% developed gestational diabetes. This group was significantly ol-der (29.68 vs 32.45, p<0.05), had lower levels of high density lipoprotein (HDL) (65 vs 59, p<0.05), higher levels of low density lipoprotein (LDL) (93.3 vs, p<0.05), higher insulin (7.8 vs 9.2, p<0.05), alanine aminotransferase (26 vs 32.5, p<0.05), and plasminogen activating factor (t-PA) (2.45 vs 3.82, p<0.05). In a multiparametric model including sex hormone binding globulin (SHBG) and t-PA, the area under the ROC curve for GDM prediction was 0.879.
Conclusions: multiparametric screening approach in the first trimester are promising in the prediction of patients that will develop GDM, although new evidence is needed to validate these early approaches and their clinical impact.
HyPErGlyCEmia diffErEntially affECts matErnal and fEtal dna intEGrity and dna rEPair EnZymEsJusciele Brogin Moreli1, Janine H Santos2, Aline Lorenzon-Ojea3, Simone Correa-Silva4, Clarissa R Rocha5, Maril-za Rudge6, Debora Damasceno7, Estela Bevilacqua8, Iracema de Mattos Paranhos Calderon 9
1Graduate Program in Gynecology, Obstetrics and Mastology, Botucatu Medical School, UNESP. 2Laboratory of Molecular Carciogenesis, National Institute of Environmental Health Sciences/Niehs. 3Department of Cell and Developmental Biology, Institute of Biomedical Sciences, USP. 4Graduate Program in Gynecology, Obstetrics and Mastology, Botucatu Medical School, UNESP. 5DNA Repair Laboratory, Department of Microbiology, Institute of Biomedical Sciences, USP. 6Graduate Program in Gynecology, Obstetrics and Mastology, Botucatu Medical School, UNESP. 7Graduate Program in Gynecology, Obstetrics and Mastology, Botucatu Medical School, UNESP. 8Department of Cell and Developmental Biology, Institute of Biomedical Sciences, USP. 9Graduate Program in Gynecology, Obstetrics and Mastology, Botucatu Medical School, UNESP, Brazil
Introduction: hyperglycemia leads to oxidative stress with consequent damage to proteins, lipids and DNA in mitochondria (mtDNA) and nuclear DNA (nDNA). Different processes can remove oxidized lipids and proteins; however, DNA has to be repaired or, in the case of some types of mtDNA damage, the genome must be re-moved.
Objective: investigate the DNA damage and DNA repair enzymes in blood samples from both mothers and the umbilical cord of pregnancies complicated by hyperglycemia.
Methods: this cross-sectional study included 144 pregnant women who underwent 75 g oral glucose tole-rance test (GTT-75g) and glycemic profile (GP), which were applied in parallel between the 24th and 28th weeks of pregnancy. Pregnant women were classified into the following groups: Non-diabetic (ND; normal GTT-75g and GP; n=46), Mild gestational hyperglycemia (MGH; normal GTT-75g and abnormal GP; n=30), Gestational diabetes mellitus (GDM; abnormal GTT-75g in pregnancy; n=45), and DM2 (abnormal GTT-75g prior to preg-nancy; n=23). Maternal glycemic control was evaluated by HbA1c levels (high-performance liquid chromatogra-phy) and the glycemia mean (GM) performed in GP. Peripheral blood mononuclear cell (PBMC) isolation and/or leukocytes from whole maternal and umbilical cord blood were obtained from all groups at delivery. Nuclear and mitochondrial DNA damage were measured by gene-specific quantitative PCR, and the expression of mRNA and proteins involved in the base excision repair (BER) pathway were assessed by real-time qPCR and Western blot, respectively.
Results: GDM and DM2 groups were characterized by an increase glucose levels and in nuclear and mito-chondrial DNA damage, and decreased expression of mRNA (APE1, POLB; and FEN1) and proteins (hOGG1, APE1) involved in BER pathway. Blood levels of DNA damage in umbilical cord were similar among the groups. Newborns of diabetic mothers had increased expression of BER mRNA (APE1, POLB; and FEN1) and proteins (hOGG1, APE1, POLB; and FEN1) (Figure 1 and Table 1).
Conclusions: our data show relevant asymmetry between maternal and fetal blood cell susceptibility to DNA damage and expression of BER proteins. Maternal cells seem to be more predisposed to changes in an adverse glucose environment. This may be due to differential ability in upregulating multiple genes involved in the activation of DNA repair response, especially the BER mechanism.
57
PE6

58
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
Figure 1: Nuclear [1] and mitochondrial [2] DNA damage from maternal [A] and umbilical cord blood [B]. DNA damage determined by gene-specific quantitative PCR (QPCR). Values as mean ± SEM, ** p<0.05 vs appointed study group. n=15 group.
nd mGH Gdm dm2
mrna Protein mrna Protein mrna Protein mrna Protein
mothers hoGGi nd nd nd ↓§ nd aPE-1 ↓* ↓ ↓*fEn-1 ns ns ↓*# ns ↓* nsPolβ ↓* ↓* ↓*
newborns hoGGi nd nd nd nd ↑*#aPE-1 ↑ ↑ fEn-1 ↑* ↑*# ↑*# Polβ ↑* ↑
↑ increase of expression or ↓ decrease of expression compared to all groups; * compared to ND group; # compared to MGH group; § compared to DM2 group. nd: not detected; ns: not significant. n=15 group in mRNA analysis and n=8 group in protein analysis.
Table 1: Summary results of mRNA and protein expression of BER.
tHyroid HormonE mEtaBolism is diffErEntially modifiEd in HUman PlaCEnta from GEstational diaBEtEs PrEGnanCiEsAxel Armella1, Carlos Veas1, Scarlett Araneda1, José Garcés1, Marcelo González2, Luis Sobrevia3, Enrique Guzmán-Gutiérrez1
1Facultad de Ciencias de Salud, Universidad San Sebastián. 2Facultad de Ciencias Biológicas, Universidad de Concepción. 3Laboratorio de Fisiología Celular y Molecular, Pontificia Universidad Católica de Chile, Chile
Objectives: to determine whether gestational diabetes alters levels of thyroid hormones, and mRNA and protein levels of thyroid hormone transporters and deiodinases from human placental cotyledons.
58
PE7

59
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
Methods: pregnant women and placentae were obtained from Hospital Guillermo Grant Benavente (Con-cepcion, Chile), previously having signed an informed consent. 100 mg of human placental cotyledon were used for mRNA and protein extraction. mRNA was extracted using Trizol® reactive. Extracted proteins were obtained from normal (n=8) and gestational diabetes (n=8) human placental cotyledons using a mortar in presence of a protease inhibitor. 70 ug of protein was added on SDS-PAGE (100V, 30 min), and transferred to a PVDF mem-brane. The membrane was exposed to primary antibodies anti-human deiodinase 3 (DIO3), anti-human LAT 2, anti-human OATP-E, and anti-human beta-actin, and secondary antibodies anti-rabbit IgG-HRP and anti-mouse IgG-HRP. mRNA expression was evaluated by real time PCR (2^(-deltadeltaCT)), using the StepOne™ thermo-cycler. Statistical analysis was realized using non-parametric ANOVA, and Bonferroni post test.
Results: free T4 levels were decreased in the first trimester of pregnancy in gestational diabetes, without changes in TSH levels. Free T4 levels in the first trimester of pregnancy were correlated with glycaemia post 2 hours in the second trimester of pregnancy. Moreover, in placenta from gestational diabetes pregnancies there was an increase for mRNA for LAT2 and OATP-E (4.2-fold and 2.3-fold, respectively) compared with normal human cotyledons. Also, an increase of mRNA levels for DIO3 (2.3-fold) was observed, compared with normal human placental cotyledons. Interestingly, protein levels of OATP-E increased (1.5-fold) in the gestational diabe-tes condition. However, protein levels of LAT2 and DIO3 did not change.
Conclusion: gestational diabetes courses with diminished free T4 in the first trimester of pregnancy, and alterations of the expression of thyroid hormone transporters (LAT2, OATP-E) and DIO3 in human placental cotyledons.
intEraCtion BEtWEEn rs10830963 PolymorPHism in mtnr1B GEnE and lifEstylE intErVEntion on PrEVEntion of GEstational diaBEtEsNora Grotenfelt1, Niko Wasenius2, Kristiina Rönö3, Hannele Laevuori3, Beata Stach-Lempinen4, Marju Orho-Me-lander5, Hannu Kautiainen1, Saila Koivusalo3, Johan Eriksson1
1General Practice and Primary Health Care, University of Helsinki and Helsinki, University Hospital XX. 2Folkhäl-san Research Centre, Helsinki, University of Helsinki, Finland. 3Obstetrics and Gynaecology, Helsinki University and Helsinki University Hospital, Helsink, Finland. 4Obstetrics and Gynaecology, South Karelia Central Hospi-tal, Lappeeranta, Finland. 5Department of Clinical Sciences, Lund University Diabetes Center, Lund University, Sweden
Introduction: the incidence of GDM is increasing worldwide as a result of both environmental and genetic factors. The G allele of intronic rs10830963 in Melatonin receptor 1B gene (MTNR1B) is associated with GDM, insulin resistance, and impaired insulin secretion. Previously, rs10830963 variant has also been shown to mo-dulate the individual response to weight loss interventions. Thus, variation in rs10830963 could plausibly explain why many intervention trials with the aim of reducing GDM have reported inconsistent and discouraging results.
Objective: the aim of this study was to assess the interaction between MTRN1B rs10830963 polymor-phism and prenatal lifestyle intervention on occurrence of GDM in pregnant women.
Materials and methods: this is a secondary analysis of the randomized controlled GDM prevention trial “RADIEL”, conducted between 2008 and 2014 in four maternity hospitals in Southern Finland. A total of 269 wo-men with previous GDM and/or a pre-pregnancy body mass index of 30 kg/m2 or over enrolled at less than 20 weeks of gestation (mean 13 weeks) and randomized into an intervention group receiving lifestyle counseling and a control group receiving standard antenatal care. The main outcome was incidence of GDM, defined as one or more pathological glucose value in a 75 g two-hour OGTT. We genotyped the participants regarding the MTNR1B rs10830963 for further analyses.
Results: no significant differences were found in the genotype frequencies between the intervention group and the control group. MTNR1B rs10830963 was significantly associated with the occurrence of GDM (unad-justed OR = 1.82, 95% confidence interval (CI) 1.10 – 3.02, p = 0.019) on pooled data. There was a significant interaction between the rs10830963 and the lifestyle intervention regarding age-adjusted occurrence of GDM (p = 0.041). The lifestyle intervention decreased the risk of GDM among homozygous carriers of the C allele of rs10830963 (-15%, 95% CI -28 – -3, p = 0.017) but not among heterozygous or homozygous carriers of the risk allele G (Figure 1).
Conclusions: the participants without melatonin receptor 1B risk alleles benefited from the lifestyle in-tervention, whereas the participants with risk alleles did not. Genetic risk should be taken into account when planning GDM prevention strategies.
59
PE8

60
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
Figure 1: Association between melatonin receptor 1B rs10890363 poly-morphism and age adjusted occurrence of gestational diabetes (GDM) according to intervention group in 226 women participating in the RA-DIEL trial. Error bars indicate 95% confidence intervals.
CHorioniC Villi HaVE an inflammatory ProfilE in HUman HyPErGlyCEmiC PrEGnanCiEsSimone Correia-Silva1, Aline Paixão-Alencar2, Jusciele Moreli1, Lessandra De Rosa1, Débora Damasceno1, Marilza Cunha Rudge1, Estela Bevilacqua2, Iracema de Mattos Paranhos Calderon1
1Graduate Program in Gynecology, Obstetrics and Mastology, Botucatu Medical School, UNESP. 2Department of Cell and Developmental Biology, Institute of Biomedical Sciences, USP, Sao Paulo, Brazil
Introduction: this study aimed to evaluate the placental inflammatory profile during hyperglycemic dysfunction. Method: this was a cross-sectional study that evaluated the inflammatory serum and placenta profile from
183 pregnant women. Based on glucose tolerance test (GTT) and glycemic profile (GP), pregnant women were classified into the groups: non diabetic (ND; normal 75-g GTT and GP; n=65), mild gestational hyperglycemia (MGH; normal 75-g GTT and abnormal GP; n=42), gestational diabetes mellitus (GDM; abnormal 75-g GTT du-ring pregnancy; n=20) and diabetes mellitus type 2 (DM2; abnormal 75-g GTT prior to pregnancy; n=56). Serum and placental concentrations of IL-1beta; IL-6 and MCP-1 were determined by ELISA and, gene expression of iNOS and MCP-1 by quantitative RT-PCR. Standard indirect immunoperoxidase technique was used on placental paraffin sections for MCP-1, iNOS and CD68 localization. The reactions were converted to digital images and quantified using Image J software. Groups were statistically compared using the Mann-Whitney U-test and considered statistically different at p<0.05.
Results: there was a significant association between serum and placenta increased levels of the proinflam-matory factors IL-1beta, IL-6, iNOS and MCP-1 in pregnancies complicated by hyperglycemia. In the chorionic villi, Hofbauer cells (HBCs, CD68 positive cells) were the main cell type reactive to iNOS and MCP-1 suggesting its participation in the inflammation pattern seen in placenta.
Conclusion: HBCs activation and cytokine unbalance at the chorionic villi caused by systemic maternal hyperglycemia and obesity may be of relevance for placental cellular machineries, which is fundamental to the successful placentation and embryogenesis.
sEssion f: matErnal & fEtal oUtComEs
EffiCaCy, safEty and matErnofEtal oUtComEs in 27 PrEGnant WomEn WitH tyPE 1 diaBEtEs mEllitUs in sEnsor aUGmEntEd PUmP tHEraPyAna Marín Gómez Medina, Lisseth Fernanda Marín Carrillo, Carol Arévalo Correa, Edward Andrés Cáceres Men-dez, Jaime Luis Silva HerreraHospital Universitario San Ignacio, Bogotá, Colombia
Objective: to assess the efficacy and safety of sensor-augmented pump (SAP) therapy in pregnant women with type 1 diabetes Mellitus (T1DM) and to describe maternofetal outcomes.
60
PE9
Pf1

61
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
Methods: the study describes an observational prospective cohort from august 2009 until august 2015 of 27 pregnant women with T1DM who started SAP therapy before or during pregnancy at Hospital San Ignacio, Colombia. The main indication was severe hypoglycemia and poor glycemic control. We registered efficacy, safety and outcome variables.
Results: 27 pregnant women with T1DM on SAP therapy were included (62% with low glucose suspend function). None of the pregnancies were planned and preconceptional glycemyc control was poor (8.3%). Reduction of HbA1c level from pre-pregnancy to third trimester was -1.9% (p=0,001) and between first and second trimester was -0.81% (p=0.000). 32% of patients achieved HbA1c <6% and 60% HbA1c <6.5% in second trimester and 13% and 56% respectiveley in third trimester. 27 pregnancies resulted in 27 infants. Maternal and fetal outcomes are described in table 1. 92% of women underwent cesarean section and the main reasons were fetal distress (5.20%), iterative cesarean (5.20%), macrosomia (4.16%) and pre-eclampsia (3.12%). 35.9 weeks was the mean gestational age at delivery and 11 pregnancies resulted in preterm delivery. Eight infants were macrosomic (>p90) and 24% of pregnancies were complicated by pre-eclampsia. We did not have maternofetal mortality.
Conclusions: SAP therapy was effective for improving glycemic control during early and late pregnancy without increasing risk of severe hypoglycemia. Despite a better control during late pregnancy maternal mor-bidity was significant. Neonatal morbidity was represented by macrosomia, hypoglycemia and need for ICU.
Variable n (%)
maternal outcomes
First trimester HbA1c (%) 7.2 (0.80) *
Second trimester HbA1c (%) 6.4 (0.68) *
Third trimester HbA1c (%) 6.54 (0.51) *
Severe hypoglycemia in first trimester 0
Severe hypoglycemia in second and third trimester 0
Ketoacidosis episodes 3 (12)
Pregnancy-induced hypertension 8 (32)
Preeclampsia 6 (24)
Intrapartum hypoglycemia (not severe) 2 (9.5)
48 hrs postpartum hypoglycemia 17 (80.9)
neonatal outcomes
Stillbirth 0 (0)
Preterm delivery (< 37 weeks) 11 (44)
Cesarean delivery rate 23 (92)
Gestational age at delivery (weeks) 35.9 (3.2) *
large for gestational age (> p 90) 8 (33.3)
Small for gestational age (< p 10) 0
Neonatal hypoglycemia 9 (36)
Need for intensive care unit (ICU) 14 (56)
Hyperbilirrubinaemia 5 (20)
Respiratory distress syndrome 4 (16)
Malformations 1 (4)
* mean (SD) Tabla 1: Martenal-fetal outcomes for 27 pregnant T1DM patients with SAP therapy.
CliniCal and PErinatal oUtComEs in WomEn WitH diaGnosis of Gdm aCCordinGto iadPsG CritEria, EitHEr By tHE first-Visit fPG or By tHE oGtt 75G at 24-28 GEstational WEEKs: a rEtrosPECtiVE CoHort and ComParison BEtWEEn GroUPsRafaela Costa1, Carolina Bittencourt1, Tatiana Zaccara1, Cristiane Paganoti1, Marcelo Zugaib2, Rossana Francisco2
1Department of Obstetrics and Gynecology oh Hospital Das Clínicas Da FMUSP. 2Faculdade de Medicina da Universidade de São Paulo, FMUSP, Brazil
61
Pf2

62
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
Introduction: although the International Association of the Diabetes and Pregnancy Study Groups (IADPSG) consensus was proposed to establish an universal way for diagnosing Gestational Diabetes Mellitus (GDM), many centers still do not consider the diagnosis of GDM when it is result of a single abnormal fasting plasma glucose (FPG) at the first prenatal visit, as suggested by the IADPSG consensus, claiming that this would lead to an excessive GDM diagnosing.
Objective: We aimed to describe the clinical and perinatal outcomes in women diagnosed for GDM by an abnormal FPG at first prenatal visit and to compare them to those of women diagnosed for GDM by the classic Oral Glucose Tolerance Test 75g (OGTT75g) at 24-28 gestational weeks.
Materials and methods: we performed an observational, retrospective cohort study, involving pregnant women who attended antenatal care visits at a tertiary teaching hospital in Sao Paulo city (Brazil) during the year of 2014. We included singleton pregnancies that were diagnosed with GDM according to IADPSG criteria, either by an abnormal first-visit FPG or by an abnormal OGTT 75g at 24-28 gestational weeks. We accessed clinical and laboratorial data from their electronic medical chart. Those subjects who lost follow-up to antenatal visits and those whose diagnostic tests results were incomplete in medical records were excluded. Women were classified according to the abnormal test that leaded to the diagnosis of GDM (either FPG or OGTT group) and were compared regarding maternal and perinatal outcomes.
Results: a total of 259 women were identified and 245 were included for analysis, n=104 for FPG group and n=141 for OGTT group. Groups were similar regarding maternal age, ethnicity, parity, smoking, family history of diabetes mellitus and coexistence of other diseases besides GDM. Women from FPG group had greater pre--pregnancy Body Mass Index (29.3 ± 6.70 vs. 7.2 ± 5.3 kg/m2, p=0.010) and more frequently history of GDM in previous pregnancies (12.2% vs. 3.9%, p=0.037). Clinical and perinatal outcomes are presented in table 1. Insulin need was more frequent in FPG group (30.0% vs. 13.5%, p=0.004), as well as macrossomia (7.7% vs. 1.6%, p=0.035).
Conclusions: women diagnosed for GDM by abnormal FPG during the first antenatal care visit have greater risk of needing insulin to achieve glycemic control and of delivering a macrosomic newborn.
fPG Group (n=100)
ottG75g Group (n=141)
P-value
Gestational age at diagnosis (weeks), mean (SD) 12.06 (5.77) 27.80 (3.55) <0.001
Need for insuline, n (%) 30 (28.8) 19 (13.5) 0.004
Gestational age at insuline introduction (weeks), mean (SD) 25.11 (5.98) 32.30 (2.61) <0.001
Gestational age at delivery (weeks), mean (SD) 38.69 (2.94) 38.02 (2.27) 0.517
Mode of delivery 0.705
Vaginal, n (%) 25 (26.9) 34 (26.2)
Forceps, n (%) 2 (2.2) 6 (4.6)
Cesarian, n (%) 66 (71.0) 90 (69.2)
Male newborn, n (%) 47 (51.1) 60 (46.5) 0.585
Birth weight (grams), mean (SD) 3067 (746) 2980 (619) 0.350
Low birthweight (<2500g), n (%) 15 (16.5) 25 (19.4) 0.861
Macrosomia (birthweight >4000g), n (%) 7 (7.7) 2 (1.6) 0.035
Neonatal hypoglycemia, n (%) 9 (19.1) 6 (8.7) 0.157
Neonatal respiratory distress, n (%) 7 (14.9) 6 (8.6) 0.371
5th minute apgar < 7, n (%) 2 (2.2) 1 (0.8) 0.572
Adequacy of weight to gestational age at birth 0.178
Small for gestational age, n (%) 11 (12.1) 20 (15.6)
Adequate for gestational age, n (%) 70 (76.9) 103 (79.8)
Large for gestational age, n (%) 10 (11.0) 6 (4.7)
Table 1: Comparison of clinical chracteristics and perinatal outcomes in women with GDM according to IADPSG criteria (Sao Paulo, n= 241).
62

63
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
ComParison of adVErsE PrEGnanCy oUtComEs BEtWEEn latin amEriCan diaBEtEs assoCiation and amEriCan diaBEtEs assoCiation CritEria for GEstational diaBEtEs mEllitUsSantiago De Loredo, María Eugenia Bazán Quiroga, Pablo Rodrigo Luján, Nilda Ruth Garces, Juan Manuel Alo-mar, Luis De LoredoHospital Privado de Córdoba, Córdoba, Argentina
Introduction: to compare differences on adverse pregnancy outcomes following the new American Dia-betes Association (ADA) and Latin American Diabetes Association (ALAD) diagnostic criteria in women with gestational diabetes mellitus (GDM) from Argentina.
Research design and methods: retrospective analysis of 517 pregnant women in 3 groups: No-GDM: Fas-ting plasma glucose (FPG) level <92 mg/dl and 2-hour plasma glucose level post OGTT <140 mg/dl. ADA: FPG level between 92-99 mg/dl and 2-hour plasma glucose level <140 mg/dl. ALAD: FPG level ≥100 mg/dl and/or 2-hour plasma glucose level ≥140 mg/dl. Variables Analyzed: Gestational Hypertension, Preeclampsia, Primary Cesarean Delivery, Birth weight above 90th percentile (LGA), Premature Delivery.
Results: comparisons were made between No-GDM and ADA, No-GDM versus ALAD and between ADA and ALAD. For No-GDM versus ADA, the odds ratios were: Gestational Hypertension 2.77 (95% CI, 1.52 - 5.07), Preeclampsia 2.51 (1.28 - 4.93), Primary Cesarean Delivery 1.46 (0.90 - 2.37), LGA 4.23 (1.96 - 9.12) and Pre-mature Delivery 2.16 (0.97 - 4.81). When comparing No GDM versus ALAD, the odds ratios were: gestational hypertension 0.79 (0.35 - 1.77), preeclampsia 0.67 (0.26 - 1.74), primary cesarean delivery 1.48 (0.88 - 2.31), LGA 2.60 (1.13 - 5.98) premature delivery 3.58 (1.72 - 7.46). For ADA versus ALAD, the odds ratios were: Gestational Hypertension 0.28 (95% CI, 0.13 - 0.63), Preeclampsia 0.27 (0.10 - 0.69), Primary Cesarean Delivery 0.97 (0.56 - 1.67), LGA 0.61 (0.29 - 1.30) Premature Delivery 1.65 (0.78 - 3.48).
Conclusions: we showed that there are increased adverse pregnancy outcomes in pregnant women who are considered No GDM patients by ALAD criteria and gestational diabetic patients by ADA.
Figure 1: Odds ratio between No-GDM vs ADA. Figure 2: Odds ratio between No-GDM vs ALAD.
matErnal CarE and PErinatal oUtComEs in PrEPrEGnanCy diaBEtEs PatiEnts ControllEd at a PUBliC HosPitalVirginia Mabel Bustos1, Paula Camin2, Leonardo Mezzabotta2, Ana María Nicolotti2, Adriana Osorio3, Lila Urzich3, Orlando Jimenez2, Roberto Votta2, V Baumberger, Mabel Poncelas2
1Servicio de Endocrinología, Hospital General de Agudos Cosme Argerich, Buenos Aires. 2Servicio de Obstetricia, Hospital General de Agudos Cosme Argerich, Buenos Aires. 3Servicio de Endocrinología, Hospital General de Agudos Cosme Argerich, Buenos Aires.
Objective: to evaluate maternal complications and perinatal outcomes in our Prepregnancy diabetes pa-tients during 1999-2015.
Methods: we retrospectively studied 262 singletone pregnancies in women with type 1 (121/262), and type 2 (141/262) diabetes from our medical records and processed by software programs: Access 2000 ad Excel 2010 (Microsoft), the significance level used was ›0.05.
63
Pf3
Pf4

64
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations64
Results: Maternal Baseline data: Median age type 1: 26.14±6,7 and type 2:33.97±5.7 (p0,0001), Pregesta-tional BMI 24.68±4.2 and 31.1±5.6 (p0.0001),Multiparous 39.6% and 69.5%, years of evolution 8.37±7.3 and 4.95±4.5 (p0.000) respectively.The 9.9% of type 1 and 2.1% of type 2 present Nephropathy (p0.02), Retino-pathy 4.13% and 2.8%(ns) and Hypertension 13.2% vs 34.04% (p0.000). There were no difference in planning pregnancy 11.5% vs 5.6% (p 0.1), Gestational Age at admission 16.42±9.21 vs 17.5±8 (p 0.3) and Glycemic Con-trol (HbA1c) in the first trimester: 8.04±1.8 vs 7.93±1.9 (p 0.6). On the contrary HbA1c in the second and third trimester was better in type 2 diabetes: 7.56±1.6 vs 6.88±1.5 (p 0.000) and 6.85±1.37 vs 6.44±1.05 (p 0.007) respectively. Table 1 shows Pregnancy complications and Perinatal Outcomes.
Conclusions: the Glycemic control was similar at Admission but it was significantly better in type 2 diabetes in the Second and Third trimester. Pregnancy induced hypertension was increased in type 1 diabetes because of poor metabolic control presumably. No difference was found in macrosomia, congenital malformations and perinatal mortality but neonatal morbidity was significantly increase in type 1 diabetes. We think that the worst outcome in type 1 may be due to the longer years of evolution, microangiopathy complications and the poor planning of pregnancies
type 1 type 2 P value
N 121 141
Pregnancy induced hypertension% 33 ( 27.2) 21 (14.8) 0.002
Preeclampsia 20 (16.5) 13 (9.2)
Caesarean delivery% 80 (66.1) 99 (70.2)
Perinatal mortality% 9 (7.4) 3 (2.1)
Congenital malformations 12 (9.9) 7 (4.9)
Gestational age (weeks) 35.86 ±4.3 37.4 ±2.25 0.007
Birth weight (gs) 3061 ± 939 3374 ±939 0.000
Prematurity 44 (39.2) 39 ( 28.8)
Macrosomia% 18 (16.07) 33 (24.4)
Small for gestational age 13 (11.6) 14 (10.3)
Neonatal jaundice 45 (40.2) 29 (21.5)
Respiratory difficulties 32 (28.5) 29 (21.5)
NICU admission 76 ( 67.8) 68 (50.3)
NICU (stay in days) 8.52 4.52
Neonatal morbility% 80 (71.4) 78 (57.7) 0.032
Table 1: Pregnancy complications and perinatal outcomes (1999 - 2015). Data are median or n (%). The total borns infants was 112 (Type 1) and 135 (Type 2).
atlantiC diP: HoW EffECtiVE is insUlin tHEraPy for WomEn WitH GEstational diaBEtEs mEllitUs diaGnosEd UsinG iadPsG CritEriaDelia Bogdanet1, Aoife Egan1, Oratile Kgosidialwa1, B Kirwan1, L Carmody1, Fidelma Dunne2
1Galway Diabetes Research Centre, National University of Galway, Ireland. 2College of Medicine, Nursing and Health Sciencis National University or Ireland, Galway, Ireland
Introduction: use of IADPSG diagnostic criteria for GDM diagnosis is now common in Europe. In Ireland the prevalence of GDM using these criteria is 12.4%. National guidelines recommend insulin if medical nutritional therapy fails. 40% of women require insulin to achieve target glucose levels in the Irish setting.
Objective: the aim of this study was to assess the effect of insulin on pregnancy outcomes in women with GDM and determine if the outcomes are comparable to women with normal glucose tolerance (NGT).
Materials and methods: this retrospective cohort study included 752 women with insulin treated GDM and 2496 women with NGT during pregnancy. All women were from the ATLANTIC DIP network database
Pf5

65
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations 65
covering antenatal centers along the Irish Atlantic seaboard. Maternal outcomes examined were preeclampsia, antepartum (APH) and postpartum hemorrhage (PPH), pregnancy-induced hypertension (PIH), polyhydramnios. Fetal outcomes examined were shoulder dystocia, congenital malformations, neonatal hypoglycemia, neonatal mortality, admission to neonatal intensive care unit (NICU), macrosomia, large for gestational age (LGA) and small for gestational age (SGA).
Results: infants of women with insulin treated GDM were more likely to be hypoglycemic at birth (adjusted odds ratio (aOR) 7.27, 95% CI 2.49- 21.22) and more likely to require admission to NICU (aOR 13.90 95%CI 10.23– 8.87). Neonatal mortality and rates of macrosomia, LGA and SGA infants (median birth weight+/- sd 3.58+/-0.6 GDM, 3.57+/-0.5 NGT, p=0.81) were similar to women with NGT. There were no differences in Apgar scores or gestational week of delivery (median+/-sd week of gestation; 39+/-2.4 GDM, 40+/- 1.7 NGT, p=0.18) between infants of women with GDM and those with NGT. Women with GDM had a significantly higher BMI (BMI >30 64.19% GDM; 20.41% NGT, p<0.01), a higher rate of family history of diabetes (68.05% GDM; 31.91% NGT, p<0.01) and a greater history of smoking (11.79% GDM; 6.89% NGT, P<0.01). Maternal rates of preeclampsia, PIH, APH and PPH were similar between women with insulin treated GDM and NGT. Women with GDM had a higher risk of polyhydramnios (aOR 8.52 95%CI 4.40-16.47).
Conclusions: insulin treatment for women with GDM is successful in normalizing rates of macrosomia, LGA and SGA in infants and maternal hypertensive disorders. Neonatal hypoglycaemia and maternal polyhydra-mnios remain excessive but this may merely reflect ascertainment bias. Despite these positive outcomes admission to NICU remains excessive and this warrant’s further investigation.
PErinatal matErnal and nEonatal oUtComEs in WomEn WitH GEstational diaBEtEs mEllitUs aCCordinG to diaBEtEs onsEtFabiana Noemí Guarneri, Natalia Cavallero, Gabriela Vecchi, Alicia ArizaHospital Materno Neonatal Dr. Ramón Carrillo, Córdoba, Argentina
Introduction: perinatal mortality has not decreased in gestational diabetic pregnancies during the last 30 ye-ars. Fetal deaths are five times and neonatal deaths three times higher compared with the general population.
Objective: the aim of this study is to analyze maternal and neonatal short term outcomes in pregnancies with gestational diabetes mellitus (GDM), according to gestational diabetes onset.
Material and method: this retrospective cohort study was conducted at Materno Neonatal Hospital. Ges-tational Diabetes subjects who were diagnosed and treated from July 2014 to August 2015 were classified as the Pregnancy and Diabetes consensus committee, from de Argentinean Diabetes Society (2008) guidelines for GDM. Evaluated maternal characteristics included anthropometrics, obstetric history, GDM diagnosis and characteristics. Primary neonatal outcome was a composite of any of the following: hypoglycemia, preterm delivery, admission to level 3 nursery, oxygen requirement, among others.
Results: a total of 132 pregnancies were included. Maternal characteristics were essentially similar in early and late onset GDM. Fourteen neonates (9.6%) had birth weight ≥4000 g. Maternal age was significantly hi-gher in early onset GDM (p=0.045) and gestational age at delivery was significantly lower for early onset GDM (p=0.03), compare with late onset GDM. Significantly more early onset GDM (p=0.019), was diagnoses in Obe-se patient (BMI >30), being 52.6% of women diagnosed before. Women with a history of stillbirths in previous pregnancies were more likely to have early onset GDM (p=0.020), as well as women with a history of GDM in others pregnancies (p= 0.019). We were not able to demonstrate that babies with early-onset GDM, have a worse prognosis or experience more hypoglycemia, hypomagnesemia, hypocalcemia or polycythemia, neither had longer hospitalization period.
Conclusion: we did not find evidence that gestational diabetes worsened pregnancy outcomes. In general, early onset GDM, is thought in obese women, together with women who had a stillbirth in a previous preg-nancy and history of GDM in another pregnancy. After this evidences, we would like to question the division between pre-gestational diabetes and gestational diabetes in terms of diagnosis and treatment.
Pf6

66
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations66
ratE and PErinatal oUtComEs in a risK faCtor PoPUlation for GEstational diaBEtEs EValUatEd WitH tWo diaGnosis CritEria: sad and iadsPGPaula Camin, Virgina Bustos, Leonardo Mezzabotta, Carolina Romero, Florencia Verdi Brusati, Adriana Osorio, Sara Andreucci, Roberto Votta, Lila Ursich, Mabel Poncelas, Ana NicolottiObstetrics and Endocrinology Department, Cosme Argerich General Hospital, Buenos Aires, Argentina
Objetives: 1- To evaluate the rate of gestational diabetes (GD) in our risk population using two diagnosis criteria: SAD (Argentine Diabetes Society) and IADSPG (International association of diabetes and pregnancy study groups). 2- To present our perinatal outcomes in patients with GD according to the two diagnosis criteria and compare them with the non diabetic risk factor population.
Methods: between January and December 2011 all patients with risk factors for GD according to SAD cla-sification were included: maternal age >= 30, previus medical history of GD mellitus, family history, perinatal morbidity or mortality of unknown cause, macrosomia, hypertension or BMI>=27. The SAD diagnosis criteria use the following values a) Two fasting glycemias >=100mg/% or b) Glucose tolerance test (GTT) with 75 grs. and cuts values of >=100 mg/% fasting glycemia and >=140 mg/% at 120 minutes. To analize the perinatal outcomes we compare the group of patients whose GTT results were normal for SAD and IADSPG diagnosis criteria (group 1, n:407) with those patients normal SAD but included in IADSPG criteria (fasting glucose level between 92-99 mg/% and two hours glycemia <140 mg/%) (group 2, n:33). Outcome measures were macrososmia (>=4000 grs.), cesa-rean rate and perinatal mortality. Data were processed using the following software programs: Access 2000 and Excel 2010 (Microsoft). A two tails Fisher exact test was use with significance level of p<0,05.
Results: a total of 511 patients with risk factors enter the study. The average gestational age at the GTT was 29.2 weeks. Of the total population, 440 did not have diabetes when tested with our current SAD diagnosis crite-ria, 71/511 (13.8%) had GD with this criteria and 81/511 (15.7%) with IADSPG one. In this, diagnosis was mainly made with fasting value: 74/81 (91.3%). Comparing patients without GD (n:440) and those with GD according to SAD crietria (n:71), macrosomia: 18.6% vs 11.2%, cesarean rate: 32% vs 38% and perinatal mortality: 0.68% vs 1.4% was respectively found. Finally we evaluate perinatal outcomes in group 1 and group 2 (Table 1).
Conclusions: when the two criterias were compared a 13.7% (IADSPG 15.7% vs SAD 13.8%) increase in GD diagnosis was found, being the totality of the patients in this subgroup with fasting hyperglycemia (>92mg/%). The analysis of perinatal outcomes in the different groups, show also a not significant increase of 33% (24.2% vs 18.2%) in the rate of macrosomia in group 2 compare group 1. In both groups no intervention was done because they were out of SAD diabetes diagnosis criteria. No differences were found in cesarean rates and in perinatal mortality. The results of this study let us infer the different prevalence of GD according to the diagnosis criteria used, although the perinatal outcomes do not allow us, possibly due to the small number of patients, to determi-nate the possible benefits of making any change in the current criteria use for our hospital population.
Group 1 Group 2 P value
N 407 33
Macrosomia 18.2% (74) 24.2% (8) 0.3
Cesarean 32.6% (133) 27% (9) 0.5
Perinatal mortality 0.68% (3) 0% (0) -
Table 1
sEssion G: PrEGEstational diaBEtEs & Early PrEGnanCy
GlyCatEd HEmoGloBin in first trimEstEr PrEGnant araB WomEn and its CorrElation WitH otHEr ParamEtErsGomathi Kadayam Guruswami1, Mawahib Abd Salman Al Biate2, Amal Hassan Abdel Aziz Hassan Ismail2, Palat Krishna Menon1, Tatjana Ille1, Prashant Hegde2, Ishtiyaq Ahmed Shaafie1, Zouhoor Mohamed Elbaz1
1Department of Biochemistry, Gulf Medical University Ajman, UAE. 2Department of Obstetrics and Gynecology, Gulf Medical College Hospital, Ajman, UAE. 3Centre for Biomedical Research and Innovation, Gulf Medical University, Ajman, UAE
Pf7
PG1

67
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations 67
Introduction: gestational diabetes mellitus (GDM) risk varies between ethnicities and United Arab Emirates (UAE) has a high prevalence of 7.9 to 37.7% based on the criteria adopted. Early detection in high risk groups can help to manage the condition with appropriate lifestyle/therapeutic interventions. Glycated hemoglobin (HbA1c) is an established and convenient measure of glycemia. Higher HbA1c levels in pregnancy are associated with poor pregnancy outcomes, however there is no consensus regarding the normal reference ranges for the three trimesters. Some studies suggest risk of adverse pregnancy outcomes increases when first trimester HbA1c is more than or equal to 5.7% while others have even suggested cutoffs of 5.4% for the first trimester.
Objective: to study first trimester HbA1c levels in pregnant Arab women and to correlate it with other pa-rameters.
Materials and methods: normal pregnant women of Arab ethnicity (11-13 weeks pregnant) were enrolled in a prospective study after informed written consent was obtained. The study was approved by the Institutional Ethics committee. Anthropometric parameters, medical histories were recorded and venous blood specimens collected. HbA1c (HPLC method), Hemoglobin, Pregnancy associated plasma protein-A (PAPP-A) and Free Beta hCG levels were measured using standard procedures in a College of American Pathologists accredited labora-tory. Data was entered into statistics software SPSS 22.0 and analyzed. T-test and Mann-Whitney was used for significance, Pearsons and Spearmans test for correlations.
Results: 108 normal pregnant women, gestation (Mean±SD) 83.9 ± 7.3 days participated. Age (Mean±SD) was 28.5 ±4.7 years and BMI (Mean±SD) was 25.7± 5.04 kg/m2. 24% had a family history of diabetes. He-moglobin ranged between 9.1 and 13.6 g% and Mean±SD was found to be 11.89± 1.05 g%. 33 % of women had Hemoglobin values less than 11.6 g%. HbA1c (Mean±SD) was 5.39± 0.41 % (i.e. 35.43±4.61 mmol/mol). Body mass index (BMI) correlated weakly (r= 0.277) but significantly (2-tailed, p =0.004) with HbA1c levels. Both HbA1c and BMI correlated negatively and significantly with PAPPA levels (r = -0.238 and -0.258; 2-tailed p = 0.013 and 0.008 respectively). Free beta hCG did not show any correlation with HbA1c or BMI. HbA1c levels were found >/= 5.7% in 24 %, and >/= 5.4% in 51% of the women. Significant differences were seen in the BMI (24.34 ±4.38 vs 27.08± 5.29, p=0.005) between women with HbA1c <5.4% and those with HbA1c >/= 5.4%. None of the other parameters were found to be significantly different between the groups.
Conclusion: many pregnant women were overweight or obese. 1 in 3 women was found to be anemic. HbA1c levels were found to be >/= 5.7% in 24 % of women. HbA1c levels correlated negatively with both BMI and hemoglobin levels. Iron deficiency anemia is known to be elevate HbA1c levels and more studies are needed to understand HbA1c levels in pregnant women in countries with high prevalence of anemia such as the UAE. Acknowledgements: this study was funded by the Al Jalila foundation, UAE.
EValUation of tyPE 2 diaBEtEs mEllitUs and PostPartUm GlUCosE intolEranCE ratEs in WomEn WitH GEstational diaBEtEs mEllitUsCristiane Paganoti1, Juliana Souza1, Rafaela Costa1, Marcelo Zugaib2, Rossana Francisco2
1Obstetrics Division of Hospital Das Clínicas Da Fmusp. 2Department of Obstetrics and Gynecology of Faculdade de Medicina da Universidade de São Paulo, Brazil
Introduction: there is a strong relationship between Gestational Diabetes Mellitus (GDM) and the long-term development of type 2 diabetes mellitus (DM2) and impaired glucose tolerance. It is known that 50% of women with GDM will develop DM2 in the first five years postpartum. This data shows the importance of adopting the tracking of patients in the postpartum period, through oral glucose tolerance test performed six to 12 weeks after delivery, and identifying risk and protective factors for these outcomes.
Objective: we aimed to evaluate the incidence of DM2 and oral glucose intolerance diagnosed in the pos-tpartum period in patients who presented GDM and to identify risk and protection factors associated to these diagnoses.
Materials and methods: we developed an observational, retrospective case-control study, which evaluated clinical and laboratory data from 148 pregnant women diagnosed with GDM according to IADPSG criteria in the period from January to December 2014, who attended antenatal care visits and performed postpartum oral glucose tolerance test (OGTTp) 75g at a tertiary teaching hospital in Sao Paulo city (Brazil). The patients were di-vided into two groups according to the results of the OGTTp: normal OGTTp group and abnormal OGTTp group for statistical analysis. Abnormal OGTTp was considered when either fasting blood glucose (FBG) was greater than 100mg/dL or 2h after overload greater than 140mg/dL. Groups were compared with regard to clinical and laboratorial data.
PG2

68
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations68
Results: abnormal OGTTp was observed in 25 (16.9%) of the 148 patients included in the study, namely 4 (2.7%) of DM2 and 21 (14.2%) of impaired glucose tolerance. Women who presented abnormal OGTTp had more frequently personal history of GDM (OR 7.8; 95%CI 2.1-28.2, p = 0.003), higher first trimester FBG and greater third trimester body mass index (BMI), as shown in table 1. Other identified risks for abnormal OGTTp were the requirement of insulin for glycemic control during pregnancy (OR 5.5; 95%CI 2.2-3.9, p<0.001) and earlier gestational age of insulin introduction. Patients who had GDM diagnosed by OGTT had a lower risk of abnormal OGTTp than those by FBG (OR 0.3; 95%CI 01-0.9, p 0.043).
Conclusion: the presence of a history of prior GDM, higher first trimester FBG, greater third trimester BMI, requirement and early introduction of insulin and the diagnosis of GDM by FBG are risk factors related to the development of oral glucose intolerance and DM2 after delivery.
normal oGttp (n=123)
abnormal otGGp (n=25) P-value
Prior GDM, n (%) 5 (4.1) 6 (25) 0.003
Third trimester BMI (kg/m²), mean (SD) 31.1 ± 5.8 33.8 ± 5.7 0.047
First trimester FBG (mg/dl), mean (SD) 87 ± 10 96 ± 13 0.006
Diagnosis test of GDM - FBG, n (%) 45 (36.6) 15 (50) 0.043
Diagnosis test of GDM - OGTT, n (%) 78 (63.4) 10 (40) 0.043
Treatment - diet, n (%) 103 (83.7) 12 (48) < 0.001
Treatment – insulin 20 (16.3) 13 (52) < 0.001
Gestational age at insulin introduction (weeks), mean (SD) 31.44 ± 2.84 21.46 ± 5.59 < 0.001
Results of OGTTp - FBG (mg/d1), mean (SD) 84.8 ± 6.3 99.5 ± 10.3 < 0.001
Results of OGTTp - second hour (mg/,dl), mena (SD) 98.4 ± 19.5 159.2 ± 35.1 < 0.001
Table 1: Clinical and laboratorial profile of women with GDM, according to the IADPSG criteria.
oVErt diaBEtEs: matErnal-fEtal oUtComEs in a HiGH risK oBstEtriC sErViCEFabiola Romero, María Lis Alarcon, Liliana Vigo, Liz Valinotti, Lilian Zorrilla, Alicia Gómez, Helen López, Car-men Echague, Diego Vera, Alba Guerrero, Francisco Cabrera, Nidia Villalba, Rosa Villalba, Alejandra Ocampo, Zumilda Ibarra, Carolina Acosta, María Celia MenoniInstituto Previón Social, Asunción, Paraguay
Introduction: hyperglycemia in the first half of gestation, to levels considered diagnostic DM outside preg-nancy, is classified by IADPGS as overt diabetes (OvD). WHO extends this classification to all over gestation time. More marked carbohydrate alteration could identify more severe pathophysiological changes, with increa-sed risk of maternal and fetal complications.
Objective: evaluate maternal and fetal morbidity and mortality of women diagnosed and treated OvD accor-ding IADPGS criteria, and compared with women with GDM and normal glucose tolerance (NGT).
Material and methods: prospective, longitudinal study of consecutive cases from High Risk Obstetrics Service- Hospital Central Instituto Previsión Social, Asuncion, Paraguay, from January to July 2013. According to 75 g OGTT plasma glucose levels, NGT: basal glucose ≤91, one hour ≤180, two hours ≤152 mg/dl; GDM: basal glucose ≥92 and ≤125, 1hr ≥180, 2hrs ≥153 and ≤199 mg/dl; OvD: basal glucose ≥126, two hours ≥200 mg / dl.
Results: of the 330 women studied were NGT 170 (51.5%), GDM 136 (41.2%) and OvD 24 (7.3%). Age 29 ± 6 NGT; 30 ± 5 GDM; 32 ± 4 years OvD (p=ns), and BMI 24 ± 4; 25.9 ± 4; 26 ± 4 kg / m2 respectively (p=ns) Risk factors: Age >30 years (42.4% NGT, 57.4% GDM, 66.7% OvD ) (p=0.008). Overweight / obesity (44.3% NGT, 50.4% GDM, 58.3% OvD) (p=ns). DM2 family history (25.4% NGT, 32.7% GDM, 55.4% OvD) (P = 0.03) previous DG/ macrosomia (2.3% NGT, 17.5% GDM, 16.7 % OvD (p = 0.005). No difference in other factors. OGTT at 30±4 weeks of gestation, basal glucose, 1 and 2 hours was significantly higher in the OvD group than the GDM group and NGT group. 84.7% and 68.4% of OvD and GDM groups respectively were treated with diet alone and 15.3% and 31.6% with diet and insulin (p=ns). Polyhydramnios was found in 8.2% NGT; 5.9% GDM; 20.8% OvD (p = 0.05). New born weight 2842 ± 715 NGT; 2975 ± 711 GDM; 3234 ± 665 grams OvD (p:
PG3

69
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations 69
0.02), and macrosomía/birth weight ≥90th percentile 3% NGT; 3.8% GDM; 17.4% OvD (p=0.02). No difference in other fetal/ maternal complications. Using stepwise multiple regressions for predicting the risk for macroso-mía, variable were not predictive. Only glycaemia levels were found predictive in the bivariate analysis (basal, 1hrs and two hrs).
Conclusions: age over 30 years old, family history of type 2 diabetes and a history of DG most important risk factors for OvD In OvD group, polyhydramnios was more frequent, with more birth weight and fetal macro-somia. Macrosomia was related to blood glucose levels in bivariate analysis.
PrEGnanCy and tyPE 2 diaBEtEsMaría Inés Vera1, Hugo Sanabria1, María Cristina Faingold2
1Instituto Cardiovascular de Buenos Aires. 2Unidad Asistencial Dr. César Milstein, Buenos Aires, Argentina
Introduction: we are facing a significant increase of women with pregestational type 2 (DM2), due to its onset at earlier ages, the growing incidence of obesity and as a result of lifestyle changes. In Argentina, 44.3% of women between 19 and 49 years old suffer overweight or obesity. The aim of this study was to determine the presence of pregestational DM2 in a group of women under treatment in a Medical Center specialized in Diabetes and Pregnancy from a Health Care Company, and establish whether the presence of such condition implied more risk for the mother and the fetus, and/or perinatal morbi-mortality.
Material and methods: we studied 167 patients derived from the Obstetrics and Gynecology department, between December 2012 and August 2015.
Results: from 167 women; 32.3% (n54) had pregestational diabetes, 42.4% (n23) had DM1, and 57.4% (n31) had DM2; the rest of them, 67.6% (n113) had gestational diabetes (GDM). During gestation, 74.2% of the women with DM2 received insulin therapy and 29.2% of the women with GDM did not respond to diet alone and need insulin therapy as well (p=0.01). The observed complications were miscarriages, premature rupture of membrane, biliary obstruction, placental abruption, eclampsia, and preeclampsia; we grouped them as “Mater-nal”; 41.7% (n10) of the DM2 women, 17.6% (n3) of the DM1 and 20.4% (n10) of the GDM, presented these complications. Neonatal hypoglycemia, macrosomia, brachial paralysis, and polyhydramnios, were grouped as “Fetal Complications”, 41.2% (n7) of them were seen in DM1 women, 12.5% (n3) in DM2,and 8.3% (n4) in GDM (p=0.01).
Conclusions: although the number of patients is small it can be observed that, the DM2 patients presented a higher maternal morbidity and miscarriages, but congenital malformations and perinatal mortality was not reported in them, in contrast with the data reported by the literature. We want to highlight the high prevalence of DM2 observed in our population, and the great number of patients that need to be treated with insulin in this group. Diabetes Care 28:323-328, 2005
Characteristic dm1 dm2 Gdm P
Age (years) 27 ± 6 35 ± 4 34 ± 5 0.01
Body mass index (Kg/m²) initial 23 ± 3 31 ± 7 27 ± 14 0.01
Initial weight 62.4 ± 10 86.2 ± 22 71.5 ± 14 0.01
Delta cheek of weight 8 ± 6 8 ± 6.9 9 ± 5.7 n/s
Delivery week 36.4 ± 1.2 37.4 ± 1.2 37.6 ± 1.4 0.05
Natural delivery 38.9% (n7) 28.6% (n6) 46.3% (n25) n/s
Cesarean section 61.1% (n11) 71.4% (n15) 53.7% (n29) n/s
New born’s weight (grams) 3545.7 ± 653.3 3453 ± 424.1 3321.1 ± 479.1 n/s
Table: Description of the population.
PG4

70
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations70
normoGlyCEmiC diaBEtiC KEtoaCidosis in PrEGnanCy: CasE rEPortMaría Margarita Rivas1, Claudia Belmar1, Marisel Figueroa1, Lía Miranda1, Carolina Pérez1, Pilar Durruty1, Gloria López1, Lilian Sanhueza2
1Hospital Clínico, Universidad de Chile. 2Hospital San Juan de Dios, Chile
Introduction: diabetic ketoacidosis (DKA) in pregnancy is a medical emergency, causing maternal and fetal mortality. Normoglycemic Diabetic Ketoacidosis in Pregnancy (NDKP), blood glucose is less than 180mg/dl, and represents 0.8-1.1% of all DKA. It´s cause is unknown, and the predisposing factors are: prolonged fasting and hyper emesis. The fetal consequences are: acidosis, hypoxia, distress, arrhythmias and neurologic impairment. Precocious interruption of pregnancy is associated to morbidity and mortality. Clinical Case: 39 year old woman, morbid obesity, primiparous woman, 32 week pregnancy. No médical history of metabolic disorder. She pre-sents with vomits and anorexia at the emergency room for the first time. She had arterial pressure of 184/115 mmHg, was afebrile, glycemia 120 mg/dl, neurologic exam was normal. She was hospitalized for pregnancy hypertensive syndrome. Her arterial pressures were normal later on. Obstetric evaluation: active fetus, biophy-sical profile 6/8, pulmonary maturity was induced. The patient kept vomiting, without abdominal pain, glycemia 213 mg/dl, metabolic acidosis, anion GAP 21, ketonemia +++, leukocytosis, proteinuria 0.64 mg/dl, renal func-tion and plasmatic electrolytes were normal. The internist diagnosed diabetes mellitus in pregnancy with DKA. She was managed with fluids, insulin and interruption of pregnancy. A caesarean section was performed and the patient was transferred to the ICU. She was hemodynamically stable, with metabolic acidosis, glycemia 172mg/dl. NDK was diagnosed, was managed with saline solution, 5% glucose infusion, insulin pump, and bicarbonate. 12 hours later DKA was resolved without obstetric complications. The diabetologist indicated NPH insulin. She was discharged in good condition and continued follow up. The newborn weight was 2650 grs, length 46 cm, big for gestational age, APGAR score 2-7, had perinatal asphyxia, and was later on discharged from the hospital in good condition.
Conclusion: NDKP must be suspected in diabetic pregnant patients with vomits and diminished oral intake. The acid-base status has to be evaluated, even though glycemia might be normal. It is necessary to accomplish metabolic balance before pregnancy is interrupted.
nEtWorK of diaBEtiC PrEGnanCy in dECEntraliZEd HosPitalClaudio Fabián Dituro, I. Somma, E. Tanda, R. Boragno and Laboratory of HIGA Junin. Hospital Descentralizado Región Sanitaria III, Junín, Prov. De Buenos Aires, Argentina
Aim: build a network of care for pregnant women with diabetes to improve perinatal outcomes. Improve the quality of their assistance.
Method and material: the dynamics of the network is high risk obstetric clinics, clinic Diabetology once a week with shifts in demand with residents of social work. They are referenced to different offices of Nutrition, Dentistry, Vaccination, Images, Laboratory (HbA1c Frustosamine, Oral glucose tolerance test) and mental he-alth. CLAP perinatal record. Diabetological and obstetric clinical histories. In 2014, 16 pregnant women were treated for diabetes, 13 gestational (GDM) and 3 pregestational (DMPG), three of them were stillborn; none reclassified; lack of reference of the patients was observed from the first level of care and other parties in the health region III level 3. A training workshop and update on Pregnancy and Diabetes was carried out for genera-lists, obstetricians, gynecologists, social workers of first level of attention and from the Hospital Interzonal Junin where the situational analysis of the Health Region III was exposed and the Diabetes and Pregnancy network is constituted as a strategy to reverse the situation, improve the quality of care and its accessibility. The high risk obstetric clinic is enabled, incorporating rotation of resident professionals of first level of care, favouring the-counter-reference between the two levels of care.
Results: one year after the creation of the network an assessment of the proceedings is made, collecting information from the medical perinatal records; 696 births are detected; 115 high-risk pregnancies, of which 46 had DM, 35 of them were treated in the network. Of the 35 pregnant women treated, 7 are in control and 28 terminated their pregnancies, of which 32 had DMG and 3 DMPG. Of the 28 births, 22 cesarean sections (78.6%); 1 preterm (32 weeks) and 27 (96.4%) with appropriate controls (> 5); 2 (7.14%) with birth weight (PRN) <2500 g and 5 (18%)> 4000 g; 9 (32%) required lung maturation; 20 pregnant women (71%) were treated with insulin. 12 patients (43%) were referenced from the Primary Care Centers (PCCs) and 15 (54%) from the same
PG6
PG5

71
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations 71
Interzonal Hospital of Junin and 1 (3%) from the private sector. 18 pregnant women (64%) and 3 infants (10.7%) required hospitalization. They were performed 21 (75%) determinations of HbA1c in the last quarter, 16 (76%) <6% and 5 (24%) between 6 and 7%; determining Fructosamine: 15 (71%) <230; 5 (24%) from 230 to 285 and 1 (5%)> 285. No perinatal mortality was recorded. 18 women (64%) were re classified.
Conclusions: the constitution of the network allows us to achieve a 96.4% of term pregnancies with proper controls, 43% were referenced PPCs, 18% of macrosomic, 76% with optimal metabolic control, 32% required fetal lung maturity. No perinatal mortality was recorded and a 64% was reclassified postpartum. These results encourage us to continue in training and strengthening the network to cover a larger number of women with diabetes.
sErUm alaninE lEVEls in Early PrEGnanCy CorrElatE WitH risK of sUBsEQUEnt GEstational diaBEtEsKristiina Rönö1, Saila Koivusalo1, Hannu Kautiainen2, Beata Stach-Lempinen3, Johan Eriksson2
1Obstetrics and Gynaecology, Helsinki University and Helsinki University Hospital, Helsinki, Finland. 2De-partment of General Practice and Primary Health Care, University of Helsinki, Helsinki, Finland. 3Obstetrics and Gynaecology, South Karelia Central Hospital, Lappeenranta, Finland
Introduction: branched chain amino acids (BCAA) have been reported to be metabolic predictors of insulin resistance and type 2 diabetes. Findings concerning the relationship between BCAA and aromatic amino acids and development of gestational diabetes mellitus (GDM) have been inconsistent. Objective: To assess the rela-tion between amino acid levels during pregnancy in a cohort of women at high risk for GDM and development of subsequent GDM.
Materials and methods: prospective cohort of 168 women recruited before 20 week’s of gestation (on ave-rage 13) in Finland. Participants were obese BMI ≥30 kg m2 and/or had a history of prior GDM, and had a normal 75 g 2-hr oral glucose tolerance test (OGTT), at baseline. Of the participants 36 developed GDM and they were compared to a group of 132 women who did not develop GDM (non-GDM). Diagnosis of GDM was based on OGTT performed around 24 to 28 weeks’ of gestation; the diagnostic thresholds were set according to ADA 2008 criteria. Fasting maternal serum samples were collected at 13 (baseline) and 23 weeks’ of gestation in both groups. Targeted nuclear magnetic resonance spectroscopy (NMR) was used to analyze the concentrations of nine amino acids (alanine, glutamine, glycine, histidine, isoleucine, leucine, valine, phenylalanine, and tyrosine).
Results: no difference was seen in age between GDM (32.5 years, SD 4.1 years) and non-GDM (31.6 years, SD 5.1 years) participants (p=0.32). No difference was seen in fasting plasma glucose level between GDM (4.95, SD 0.21) and non-GDM (4.87, SD 0.25) participants at baseline. Mean BMI at baseline was lower (29.7 kg/m2, SD 6.4) in GDM-group compared to non-GDM-group (32.5 kg/m2, SD 5.0) (p=0.005). GDM participants (75%, n=27) had more often at least one prior delivery compared to non-GDM participants (25%, n=9). At base-line alanine concentration was higher in GDM participants (0.366 mmol/l, SD 0.043) compared with non-GDM participants (0.349mmol/l, SD 0.040) (p=0.026). No difference was seen at 23 weeks’ of gestation between the groups (Fig1). In a logistic regression the risk of subsequent GDM incidence increased by 1.55 times (1.03 to 2.36; p=0.031, after adjustment with baseline age, BMI, glucose and parity) per one SD of alanine concentration at baseline. No difference was seen on any other amino acids analyzed, including BCAAs.
Conclusions: high-risk women who develop GDM have higher levels of alanine in early pregnancy compa-red to non-GDM women.
Table 1
PG7

72
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
sEssion H: lifEstylE, nUtrition, matErnal WEiGHt Gain & PostPartUm
lifE stylE intErVEntion dUrinG PrEGnanCy for WomEn WitH GEstational diaBEtEs. WHat Can WE lEarn in tErms of diaBEtEs PrEVEntion aftEr PrEGnanCy?Patrícia Damé1, Kadhija Cherubini1, Pâmella Goveia1, Leony Galliano2, Michele Drehmer1, María Inês Schmidt11Universidade Federal Do Rio Grande Do Sul, UFRGS. 2Universidade Federal de Pelotas, UFPEL, Brazil
Introduction: gestational diabetes (GDM) has been increasingly recognized globally as an important condi-tion for prenatal care. Although treatment during pregnancy is based on solid evidence base, the post-pregnan-cy orientation has received less investigation.
Objective: to assess lifestyle practices among women with GDM in terms of their meeting standard recom-mendations for a healthy life style and diabetes prevention.
Materials and methods: follow up study of 1799 women with GDM who attended tertiary prenatal care facilities within the National Health System (SUS). Structured interviews provided information regarding food ingestion, physical activity, sociodemographics and prepregnancy weight. Chart review provided information on height and weight.
Results: most women were 30 to 39 years old (51%), lived with a partner (89%) and had an unfavorable socioeconomic position (only 37%finished high school, and 40% had a family income within 1-2 minimum wages). Most were obese (46%) before pregnancy, and their average gestational weight gain was 9.4 kg while their weight gain up to enrollment was 8.4 kg. Within this scenario, only about half reported receiving advice to increase physical activity during pregnancy (45%), and only a few were classified as active in leisure (5.3%) and during commuting (29%). With regard to dietary orientation, the recommended consumption of fruits and vegetables was achieved by 70% and of beans by 55.3% of the women. Consumption of soft drinks or swee-tened juices five times per week or more was reported by 26%.
Conclusions: women with GDM seen in the SUS received little orientation with regard to physical activity, and their practice revealed a sedentary pattern of physical activity. Although the recommended consumption of fruits and vegetables was reached by most, a third did not, and the consumption of sweetened beverages was considerably high for this particular health condition. Considering the importance of healthy eating and mode-rate physical activity for both, GDM treatment and post-partum diabetes prevention, greater efforts should be given to such women during pregnancy to guide towards a more sustained healthy lifestyle.
BEnEfits of EdUCational GroUP intErVEntion in GEstational diaBEtEsM De la Cruz, María Teresa De Sagastizabal, N Gómez, Silvia Gorbán de Lapertosa, JP Gutiérrez, C López, V Ludman, MC Monzón Hernández, M Rosseberg, V Veglia, José Ramón Vidal, M Villagra, M Villasanti, María Florencia Yendrika, LY ZacaríasMedicine Faculty National Northeastern University, Argentina
Objective: to improve the quality of care and perinatal outcomes. Reduce incidence of maternal and neona-tal admissions related to treatment of this disease. Evaluate knowledge, skills and attitudes acquired after the implementation of an educational intervention in pregnant women with gestational diabetes (GD).
Materials and methods: observational study. Women with GD who attend clinic DG High Risk, during pe-riod July 2013-November 2015. Group Activity takes about eight hours with 8 pregnant overlook, it deals with topic such us through participatory activities, explanations, educational games, anthropometric measurements , blood pressure , glycemic profile, set treatment and physical activity, eating plans were discussed with card games. Attended by a multidisciplinary team. Knowledge questionnaires, Depression (WHO5), quality of life (EQ-5D) and satisfaction, analysis of medical records, consulting room and home visits. Contact by text messa-ge with insulin dose corrections or questions about your pregnancy was implemented. Control group formed for pregnant with Normatized care between 2009 /12. Statistical analysis: SPSS 20 and Epidat 3 program. Des-criptive statistics, Student t test and Kruskal Wallis and X² proof considered significant differences with p <0.05.
Results: 53 pregnant women with group education , age, X 31.8 ± 6.5, BMI X 32.5 ± 7.3, knowledge ques-tionnaires 13.8± 3.5 vs 16.8 ±2.6 (p<0.000) , welfare index 55.1 + 18.3 vs 65.7 ± 19.4 (p<0.000) , 88 % referred satisfaction with the activity , 57% used text messages to fit treatment with satisfactory results. Process indi-cators (BMI, fundus, ECG and urine protein), p<0.0005. Decreased incidence of hospitalization in neonatology
PH1
PH2

73
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
(OR 0.77 CI (95%) 0.27-2.18). Decreased the number of caesarean sections (OR.0.61 IC (95%) 0,22-1.68). Conclusions: the evaluation of knowledge, skills and attitudes for implementing the group education was
statistically significant (0.000), improved quality of care and hospitalizations decreased in neonatal IC OR 0.77 (95 %) 0.27-2.18 and number of caesarean sections OR 0.61 CI (95 %) 0.22-1.68).
PrEValEnCE of WEiGHt Gain adEQUaCy in WomEn WitH GEstational diaBEtEs: a mEta-analysisAngela Jacob Reichelt1, Luciana Reck Remonti1, Camila Viecelli1, Livia Silveira Matella2, Vanessa Gnielka3, María Lucía Oppermann3, Sandra Pinho Silveiro3
1Hospital de Clínicas de Porto Alegre, Brazil. 2Postgraduate Program in MS, Endocrinology, Universidade Federal Do Rio Grande Do Sul. 3Faculdade de Medicina, Universidade Federal Do Rio Grande Do Sul, Brazil
Introduction: inadequate (insufficient or excessive) gestational weight gain (GWG) is related to adverse pregnancy outcomes. No specific recommendations on weight gain are available for gestational diabetes (GDM) women. One objective of our meta-analysis was to describe frequencies of weight gain adequacy in GDM women according to the 1990 or the 2009 IOM recommendations.
Material and methods: we searched PubMed and EMBASE databases for studies that evaluated, in GDM women, the effects of GWG according to the 1990 or the 2009 IOM recommendations on pregnancy outco-mes; and also which described rates of adequate, excessive or insufficient weight gain. We included studies on GWG irrespective of GDM diagnostic criteria. We excluded studies with pre-gestational diabetes (type 1 or type 2) women. Prevalence and 95% confidence interval (CI) of GWG adequacy were calculated using WinPepi program. The study protocol is registered at Prospero International Prospective Register of Systematic Reviews site, http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42015024268.
Results: until November 2015, 1,471 potential studies met the strategy search; of these, 87 were fully re-vised. Eighteen studies, including 48,697 women, met inclusion criteria for the prevalence analysis. One study used the 1990 IOM recommendation and the other 17, the 2009 recommendation (one modified for Asian patients). One study included only obese women. GDM was diagnosed with NDDG criteria in 4 studies, Car-penter and Coustan in 4, IADPSG in 4 (in two, combined with previous criteria) and in one according to a local strategy; in 5 studies criteria was not described. GWG was classified as insufficient, adequate or excessive in 12 studies, as excessive or non-excessive in 4, and as excessive or adequate in 2 studies. Adequate weight gain occurred in 16,179 women (33.2%, 95% CI 32.8-33.6%); insufficient, in 14,000 (28.8 %, 95% CI 28.4-29.2%); excessive in 15,610 (32.1%, 95% CI 31.6-32.5%); and non-excessive, in 2,908 (5.9%, 95% CI 5,8-6.2% ). When we evaluated only studies based on the 2009 recommendation (17 studies including 17,623 women) prevalence was: adequate, N= 5,897 (33.5%, 95% CI 32.8-34.2%0); insufficient, N=3,067 (17.4%, 95% CI 16.9-18.0%); excessive, N= 5,751 (32.6%, 95% CI 31.9-33.3%); and non-excessive N=2,908 (16.5%, 95% CI 16.0-17.1%).
Conclusions: adequate GWG occurred in only one third of GDM women, excessive or insufficient gain being more common. Approaches to improve GWG adequacy in GDM pregnancies must be sought, as well as validation of current recommendations with specific GDM outcomes.
GlUCosE tolEranCE aBnormalitiEs at Post-PartUm folloWinG PrEGnanCy WitH GEstational diaBEtEs mEllitUs (Gdm)Cristina Dickie De Castilhos, Maria Inês Schmidt, Bruce Bartholow DuncanUniversidade Federal Do Rio Grande Do Sul (UFRGS), Argentina
Introduction: GDM has been increasingly recognized globally as an important condition for prenatal care. Although retesting at post-partum has been recommended in most guidelines, rates of performance remain poor. This raises the question as to whether all women with GDM should be equally reinforced to perform the test at early post-partum, while still adapting to recent motherhood, or if milder cases could receive a more flexible screening.
Objective: to assess glucose tolerance up to six months post partum among women with GDM who did not require insulin during pregnancy and thus presented a milder case of gestational hyperglycemia.
Materials and methods: follow up to at least 6 weeks postpartum of 1314 women with GDM. Structu-
PH3
PH4

74
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
red interviews provided information regarding food ingestion, physical activity, socio-demographics and pre-pregnancy weight. Chart reviews provided information on height and weight. Laboratory results were obtained directly from the laboratory or from the participant.
Results: Mean age was 31 years. Most had an unfavorable socioeconomic position (only 37% finished high school, and 40% had a family income between 1-2 minimum wages). Most had excess weight, 46% being obese before pregnancy. Of the 1075 women who did not use insulin for GDM treatment, 507 (47.2%) returned for an OGTT within 6 months post partum. Of these, 15 (3.0%) had diabetes, and 71 (14.0%) had pre-diabetes. With respect to pre-diabetes, 41 (8.1%) had fasting glucose >100mg/dl, and 44 (9.1%) had a two hour post-load glucose >140 mg/dl.
Conclusions: Even among women able to control GDM without insulin during pregnancy, post-partum testing identified a large proportion presenting either diabetes or pre-diabetes. These findings support the re-commendation to test all women with GDM in the post-partum period.
miCronUtriEnt intaKE in PrEGnant WomEn WitH GEstational diaBEtEs.Keine Pereira1, Lilian Reis2
1FEPECS, Secretaria de Saúde, Brasilia. 2Faculdade de Medicina de Botacatu, UNESP, Brazil
Objective: to evaluate the adequacy of macronutrients in the diet and micronutrient intake in pregnant wo-men with gestational diabetes treated in ambulatory diabetes Hospital Regional da Asa Norte (HRAN) Brasilia-Federal District, with specific analysis of quantitative adequacy of selenium, zinc, magnesium, calcium and vitamin D.
Method: descriptive observational study in which we analyzed the food intake of 34 pregnant women with gestational diabetes, by 24-hour recall, food frequency questionnaire and record food intake of 3 non-consecu-tive days.
Results: The mean percentage of nutrients found in food surveys were 21.7% protein , 51.7% carbohydrate and 26.4% fat, and mean values of dietary intake of micronutrients calcium, magnesium, zinc, the selenium and vitamin D were 725.1 mg 220.2 mg, 9.33 mg, 4.11 mcg and 76 mg, respectively. Selenium showed the highest frequency of suitability by pregnant women, unlike vitamin D and magnesium had the lowest levels.
Conclusion: The majority of diabetic pregnant women according to dietary surveys, showed inadequacies important below recommended calcium, vitamin D and magnesium. The average intake of selenium was ade-quate, while zinc showed the approximate values advocated. The average protein intake was considered the closest recommendation for gestational diabetes, and the average consumption of carbohydrates and lipids above suboptimal. Nutritional interventions to change food habits and diet quality should be applied to this po-pulation in order to promote health benefits of both mother and child.
assoCiation of nUtritional statUs WitH marKErs of mEtaBoliC syndromE and GlyCEmiC Control in GEstational diaBEtEs mEllitUsLilian Moreira Reis1, Claudia Vicari Bolognani1, Adriana Pederneiras Da Silva2, Adriano Dias1, Marilza Cunha Rudge1, Iracema Mattos Paranhos Calderon1
1Graduate Program un Gynecology, Obstetrics and Mastology, Botucatu Medical School, UNESP. 2Escola Supe-rior de Ciências da Saúde, ESCS/DF, Brasilia, Brazil
Introduction: Obesity, insulin resistance, metabolic syndrome (MS), and gestational diabetes mellitus (GDM) are naturally related, directly linked to maternal nutritional status, and might bring short or long-term maternal and perinatal complications.
Objective: to assess maternal nutritional status, and its potential association with markers of MS and glyce-mic control in pregnant women with GDM.
Method: a cross-sectional study including 65 pregnant women with GDM. Nutritional status was assessed based on prepregnancy body mass index (BMI), total energy intake (TEI) as assessed by the 24-h diet recall (24-hR) and the food frequency questionnaire (FFQ), and diet quality as assessed by the Healthy Eating Index (HEI) adapted for the Brazilian population. MS and glycemic control markers were also evaluated.
Results: prepregnancy BMI >=25 Kg/m2 was found in 67.7% of the women. Food intake was inadequate in
PH5
PH6

75
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations
70.3%, 76.6%, and 50% of the study participants according to 24-hR, FFQ, and HEI scores, respectively. Prepreg-nancy BMI >=25 Kg/m2 was associated with 5.6-fold and 3.9-fold higher risks for gestational BMI >=25 Kg/m2 and FG >85 mg/dl, respectively. Inadequate TEI/24-hR was associated with a 4.7 higher risk for gestational BMI >=25 kg/m2 and a 1.3-fold higher risk for HDL-cholesterol <50 mg/dl. Inadequate TEI/FFQ favored a 6.7-fold increased gestational BMI >=25 kg/m2, and HEI score < 65 was associated with a 1.1-fold higher risk of HbA1c >6.5%.
Conclusion: our results show that inadequate maternal nutritional status during pregnancy is associated with increased risk for MS and poor glycemic control.
Can matErnal WEiGHt Gain in GEstational diaBEtEs (Gdm) PrEdiCt BirtH WEiGHt adEQUaCy?Maria Lúcia Oppermann1, Livia Mastella2, Letícia Weinert2, Vanessa Gnielka3, Sandra Pinho Silveiro1, Vania Nao-mi Hirakata3, Angela Reichelt51Faculdade de Medicina Da Universidade Federal Do Rio Grande Do Sul. 2Postgraduate Programe n MS, Endo-crinology, Universidade Federal Do Rio Grande So Sul. 3Universidade Federal Do Rio Grande Do Sul (UFRGS). 4Grupo de Pesquisa e Pós-Graduação Do Hospital de Clinicas de Porto Alegre. 5Hospital de Clinicas de Porto Alegre, Brazil
Introduction: maternal body mass index (BMI) and gestational weight gain (GWG) are important deter-minants of birth weight. Excessive weight gain is associated with excessive fetal growth in normal and GDM pregnancies. Can we predict birth weight adequacy in GDM pregnancies from maternal weight gain?
Objective: to evaluate the predictive value of GWG on birth weight adequacy among women with GDM. Material and methods: prospective cohort of 362 GDM women classified according to pre-pregnancy BMI
categories. Gestational weight gain was considered insufficient, appropriate or excessive based on the 2009 Institute of Medicine recommendations. Newborns were classified as large, adequate or small for gestational age, according to Alexander’s chart. Receiver Operating Curves (ROC) were plotted to identify critical weight gain values that could predict birth weight adequacy.
Results: mean BMI was 30 ± 6.9 kg/m2; 94 (26%) had normal BMI, 106 (29%) were overweight and 162 (45%), obese. Average gestational weight gain was 10 ± 7.5 kg (-8.0 to 36.3 kg). Appropriate weight gain occu-rred in 25%, excessive in 37.5% and insufficient in 37.5% of women. Mean birth weight was 3.239 ± 575 g; 33 of the newborns (9.1%) were small for gestational age (SGA), and 44 (12%), large for gestational age (LGA). In obese women, the area under the curve (AUC) of GWG as predictor of LGA was 0.736 (95% CI 0.625-0.847, P=0.000); in normal BMI women, the AUC to predict SGA was 0.801 (95% CI 0.640-0.962, P = 0.001). In obese women, a weight gain of 11 kg or more predicted large newborns with sensitivity of 65%, and specificity of 81% while a weight gain of less than 5 kg predicted large neonates with sensitivity of 81% and specificity of 40%. In normal BMI women, a weight gain of 8 kg or less predicted small newborns with sensitivity of 73% and specificity of 84%.
Conclusions: in obese GDM women, a GWG higher than 11 kg predicted LGA; a weight gain of 5 kg avoided large babies without increasing the risk of SGA. In normal BMI women, a GWG lower than 8 kg was associated with SGA.
latE aBstraCts
EffECt of GEstational diaBEtEs mEllitUs on tHE fEtoPlaCEntal EndotHElial fUnCtion from motHErs sUBJECtEd to insUlin tHEraPyMario Subiabre1, Rocío Salsoso1,2, Bárbara Fuenzalida1, J Araos1, Fabián Pardo1, C Sanhueza1, Andrea Leiva1, Luis Sobrevia1,3,4 1Cellular and Molecular Physiology Laboratory (CMPL), Division of Obstetrics and Gynaecology, School of Medicine, Faculty of Medicine, Pontificia Universidad Católica de Chile, Santiago 8330024, Chile. 2Department of Physiology, Faculty of Pharmacy, Universidad de Sevilla, Seville E-41012, Spain. 3University of Queensland Centre for Clinical Research (UQCCR), Faculty of Medicine and Biomedical Sciences, University of Queensland, Herston, QLD 4029, Queensland, Australia
PH7
la1

76
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
Poster Presentations76
Introduction: gestational diabetes mellitus (GDM) is a disease that occurs during pregnancy and relates with maternal and fetal hyperglycaemia and fetoplacental endothelial dysfunction. Pregnant women with GDM subjected to diet present with normal glycaemia; however, increased L-arginine transport via the human cationic amino acid transporter 1 and nitric oxide (NO) synthesis via the endothelial NO synthase (eNOS), are still present. Some of these women under diet fail to control glycaemia and are subjected to insulin therapy. Nevertheless, it is unknown whether insulin therapy restores fetoplacental endothelial dysfunction seen in GDM.
Aims: to determine whether insulin therapy reverses fetoplacental endothelial dysfunction in pregnant women with GDM treated with diet.
Methods: Human umbilical vein endothelial cells (HUVECs) were isolated from normal pregnancies, GDM pregnancies where the pregnant woman was under diet (GDMd) or insulin therapy (GDMi, 0.5–0.65 U/kg). Cells were cultured up to passage 3 under standard conditions (5% CO2, M199 supplemented with 20% bovine sera, penicillin/streptomycin) and used when ~95% confluence. Kinetics of saturable L-arginine transport (Vmax, Km) were measured (0 – 1000 mmol/L L-arginine, 3 mCi/mL L-[3H]arginine, 1 minute, 37 ºC) in Krebs solution in the absence or presence of 1 nmol/L insulin (8 hours). Intracellular content of L-citrulline was measured by high-performance liquid chromatography (h.p.l.c.) and nitric oxide level was estimated by fluorescence using DAF-FM probe. Total and Ser1177 (P~Ser1117 eNOS) and Thr495 (P~Thr495 eNOS) phosphorylated eNOS protein abundance was estimated by Western blotting (b-actin was used as internal reference).
Results: in the absence of insulin L-arginine transport was higher (P<0.05, n=4) in cells from GDMi (Vmax/Km ~2.7 fold) and GDMd (Vmax/Km ~2.8 fold) compared with normal pregnancies (Vmax/Km = 0.0013 ± 0.0001 pmol/mprotein/minute/(mmol/L)). Insulin partially reversed the increase in L-arginine transport in GDMi (~34%) and GDMd (~36%). L-Citrulline content and NO level are higher in cells from GDMi (~7 and ~5.7 fold, respectively) and GDMd (~5.9 and ~3.7 fold, respectively) compared with cells from normal pregnancies in the absence of insulin. This hormone partially reversed the elevated L-citrulline content and NO level seen in GDMi (~38 and ~49%, respectively). Insulin also reversed the elevated NO level detected in GDMd (~51%). Total eNOS protein abundance was higher in GDMd (~6.3 fold) and GDMi (~1.2 fold) compared with cells from normal pregnancies. Insulin increased (~1.9 fold) eNOS protein abundance in cells from normal pregnancies, but reversed GDMd (~42%) and GDMi (~7%)–increase in eNOS. In the absence of insulin, the protein abundance for P~Ser1117 eNOS is higher in cells from GDMd (~1.5 fold) and GDMi (~1.6 fold) compared with cells from normal pregnancies. Insulin increased (~1.5 fold) P~Ser1117 eNOS in cells from normal pregnancies, but reversed GDMd (~29%) and GDMi (~60%)–associated increase. However, P~Thr495 eNOS was unaltered by GDMd, GDMi or insulin.
Conclusion: insulin therapy in pregnant women that course with GDM is an approach that results in normal maternal and fetal glycaemia, but seems inefficient in restoring this disease–associated fetoplacental endothelial dysfunction at term.
Support: Fondo Nacional de Desarrollo Científico y Tecnológico (FONDECYT 1150377, 1150344, 11150083, 3140516), Chile. RS holds a Comisión Nacional de Investigación en Ciencia y Tecnología (CONICYT), Chile– and Faculty of Medicine, PUC–PhD fellowships. MS holds Vicerectorate of Research, PUC–PhD fellowship.

77Index of authors
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
77
indEx of aUtHors
AUTOR UBICACIÓnAbrahim Cherubini, Kadhija PC7Acosta, Carolina PG3Acuña, Stephanie PE5Adam, Sumaiya PA1/PA6Agarwal, Mukesh W2Aguera, Darío O4Aisemberg, Julieta PB6Al Biate, Mawahib AS PG1 Alarcon, M Lis PG3Alcala, Martín PB3Allard, Catherine O3Alomar, Juan M PF3Alvarez Arantes, Mariana PD8/PD9Alvariñas, Jorge H2/O4Anastasiou, Eleni H4André, Van Assche PA2Andreucci, Sara PF7Antunes Nunes, M Angélica PC7Apoloni, Susana Beatriz PC2Araneda, Scarlett PE7Arany, Edith PB4Arévalo Correa, Carol PF1Argerich, María Inés O4/PD2/PD3Ariza, Alicia PF6Armella, Axel PE7Araoz J LA1Barbour, Linda H1Barceló, Alberto C13Bariani, María Victoria PB6Barros, E PE2Bartolin, Adriana O4Basualdo, Natalia C11Battista, M Claude O3Baumberger, V PF4Bazán Quiroga, M Eugenia PF3Beamish, Christine L4Becu-Villalobos, Damasia H6Belmar, Claudia PG5Benhalima, Katrien PA2Bentley-Lewis, Rhonda H12Bertona, Celina O4Beruti, Ernesto PC2Besenboeck, Carolin L2Bevilacqua, Estela PE6/PE9Biondi, Mónica PA7Bittencourt, Carolina PF2Bochini, Andrea PD2/PD3Bogdanet, Delia PF5Bolado, Victoria PB3Bolognani, Claudia PD7Bomarito, Josefina O4
AUTOR UBICACIÓnBoragno E PG6Borgese, Gabriela PA7Bouchard, Luigi O3Bustos, Virgina PF4/PF7Caballero Guzman, Karina O5Cabero Roura, Luis W2Cabrera, Francisco PG3Cáceres Mendez, Edward A PF1Calderon, Iracema C9/PD7/PD8/PD9/PE6/ PE9/PH6Camin, Paula PF4/PF7Campos, M Amélia PA3Capobianco, Evangelina H9/PB2/PB4/PB5/PB7Capurro, Lina PD6Carey, James H12Carmody, Louise H11/PF5Cassettari, Nicolosi PD8/PD9Castilhos, Cristina Dickie De PH4Catalano, Patrick M L6Cavallero, Natalia PF6Cervetta, Liliana O4Chantal, Mathieu PA2Chaparro, Alejandra H10Chavarri, María Jesús PE5Chen, Jenny PD1Cherubini, Kadhija PH1Chicco, Adriana G O2Chiocconi, Mónica O4Cid, Marcela PE3Clapés, Sonia PB3Coniberti, Irene O4Corcoy, Rosa C10Correa, Paula PE5Correa-Silva, Simone PE6/PE9Costa, Rafaela PC1/PC6/PF2/PG2Cruz Hernández, Jeddú PC4/PC5Cunha Rudge, Marilza PH6Curet, María Marta O4Daher, Silvia C4Dahlstrom, Jane PD1Damasceno, Débora PB8/PB9/PD8/PD9/ PE6/PE9Damé, Patrícia PH1Damm, Peter K3/PA2Das Graças Pena, Georgia PC7Dasí, Francisco PB3David, Raúl O4/PD2/PD3Davila, Fabiana PC2De la Cruz, M PH2De Loredo, Luis PF3De Loredo, Santiago PF3

78 Index of authors
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
78
AUTOR UBICACIÓnDe Rosa, Lessandra PE9De Sagastizabal, M Teresa PH2Desoye, Gernot L2Di Renzo, Gian Carlo W2Dias, Adriano PD7/PH6Díaz, Paula H8Dimasuay, Genelyn H8Dituro, Claudio Fabián PG6Divakar, Hema W2Djelmis, Josip PA4Domínguez Rubio, Ana P PB6Dornhorst, Anne W5Doyon, Myriam O3Drehmer, Michele PH1Duncan, Bruce B PH4Duncombe, Gregory O6Dunne, Fidelma H11/PF5/W6Durruty, Pilar PG5Echague, Carmen PG3Egan, Aoife H11/PF5Elbaz, Zouhoor M PG1 Eriksson, Johan PA5/PE8/PG7Eriksson, Ulf J L1Espino y Sosa, Salvador PD4Esteban, M Paula O4Faas, Marijke L3Faingold, M Cristina C6/O4/PG4Farias, Carolina O4Fernandes Matos, Juliana PB8/PB9Fidelma, Dunne PA2Figueroa, Marisel PG5Fioravanti, Bianca PD8/PD9Florez, José O3Fornes, Daiana PB1/PB5Fortino, M Alejandra O2Francely Américo, Madileine PB8/PB9Franchi, Ana María PB6Francisco, Rossana PC1/PC6/PF2/PG2Fregonese, Rodolfo PC2Fregozo Osuna, Cecilia PC4Friedman, Jacob E H7Fuenzalida, Bárbara PE4/LA1Fukuda, Masashi PC3Fukuoka, Misao PC3Fullone, Rosana O4Funez, Adriana PD2/PD3Fux Otta, Carolina O4Galaz, José H10/PE5Gallegos, David PE1Galliano, Leony PH1Garcés, José PE7Garces, Nilda Ruth PF3García Richter, Mercedes O4García, Jorge PD5Gauna, Alicia O4
AUTOR UBICACIÓnGeraci, Sandra F PA7Glatstein, Myriam L O4Glikman, Patricia O4Gnielka, Vanessa PA3/PH3/PH7Goedelmann, M Celeste O4Gómez Flores, Marta O4Gómez Medina, Ana Marín PF1Gómez Ponce, Lorna O4Gómez, Alicia PG3Gómez, N PH2González, Claudio Daniel O4González, Marcelo PE1/PE3/PE7Gorbán de Lapertosa, Silvia C12/O4/PH2Goveia, Pâmella PC7/PH1Grandúa, Raiden PC5Grotenfelt, Nora PA5/PE8Guaita, María Silvina PC2Guarneri, Fabiana N PF6Guerrero, Alba PG3Gutiérrez, JP PH2Guzmán-Gutiérrez, Enrique PE7Hadar, Eran W2Hakim, Alejandro O4Hedge, Prashant PG1 Hernández, Pilar PC5Herrera, Emilio L5Hiden, Ursula L2Higa, Romina O1/PB1/PB5Hill, David J L4Hirakata, Vânia N PA3/PH7Hirschmugl, Birgit L2Hivert, M France O3Hod, Moshe W2Huvinen, Emilia PA5Huynh, Jennifer H12Ibarra, Zumilda PG3Illanes, Sebastián H10/O6/PE5Ille, Tatjana PG1 Illia, Ricardo H O4Inostroza, Carolina H10Ismail, Amal Hassan AAH PG1 Ivanisevic, Marina PA4Jacob Reichelt, Angela PA3Jansson, Thomas K2Jawerbaum, Alicia H9/O1/O4/PB1/PB2/ PB4/PB5/PB7Jimenez, Orlando PF4Kadayam Guruswami, Gomathi PG1 Kapur, Anil W2Kautiainen, Hannu PA5/PE8/PG7Kent, Alison PD1Kgosidialwa, Oratile PF5Kinsella, Alejandra PA7Kirwan, Breda H11/PF5Kluwe Viégas Damé, Patrícia PC7

79Index of authors
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
79
AUTOR UBICACIÓnKoivusalo, Saila PA5/PE8/PG7Kugishima, Yukari PC3Kusanovic, Juan P H10Kusuda, Nobuko PC3Laboratory of Higa Junin PG6Laevuori, Hannele PE8Lang, Jacinto PC4/PC5Lara, Silvia PA7Leiva, Andrea PE2/PE4/LA1Lewin, M Laura O4Linenberg, Ivana O1/PB2Lobenstein, Guillermo O4Loeken, Mary R H5Lofrano, Julieta PD6Lombardo, Yolanda B O2Longo, Sherri O6López, C PH2López, Gloria PG5López, Helen PG3López-Stewart, Gloria C1Lorenzon-Ojea, Aline PE6Lozano Bullrich, M Pía O4Lu, Jun C5Ludman, V PH2Luján, Pablo Rodrigo PF3Maccio, María Natalia O4Macri, Liliana PA7Malfetano, Gabriela O4Maniá, Silvana O4Marín Carrillo, Lisseth F PF1Márquez Guillén, Antonio PC4/PC5Martínez, M Paz O4Martínez, Susana O4Masjoan, Fabiana O4Mastella, Livia PH3/PH7Mathiesen, Elisabeth R C2Mazzucco, María Belén H9/PB7Mcelduff, Aidan W3McIntyre, Harold D W2Meinilä, Jelena PA5Mengual, Rodolfo O4Menises, Magdalena O4Menon, Palat Krishna PG1 Menoni, María Celia PG3Mercanzini, Laura PD6Mestman, Jorge H C8Metzger, Boyd E W1Mezzabotta, Leonardo PF4/PF7Miranda, José R de Arruda PB8/PB9Miranda, Lía PG5Monzón Hernández, MC PH2Moreli, Jusciele PE6/PE9Morris, Jessica L W2Muñóz Manrique, Cinthya PD4/O5Murno, Graciela O4
AUTOR UBICACIÓnMurphy, Helen C3Nicolotti, Ana PF4/PF7Nolan, Christopher K1/PD1Oblonkin, Victor C5Ocampo, Alejandra PG3Ochandorena Martin, José M O4Omori, Yasue W7Oppermann, M Lucía PA3/PH3/PH7Orho-Melander, Marju PE8Ortega-Senovilla, Henar L5Ortiz, María PD6Osorio, Adriana PF4/PF7Ovesen, Per C7Padilla, Liset PC5Paganoti, Cristiane PC1/PC6/PF2/PG2Paixão-Alencar, Aline PE9Palmeiro, Yasna PE5Pardo, Fabián PE2/PE4/LA1Pare, Claudia O4Passarin, Noemí PC2Pederneiras Da Silva, Adriana PH6Pereira, Keine PH5Pérez, Carolina PG5Perichart Perera, Otilia O5/PD4Perron, Patrice O3Pham, Elizabeth PB4Pinho Silveiro, Sandra PA3Pintos, Gustavo O4Plank, Lindsay C5Pochettino, Pablo PD6Ponce, Graciela PD5Poncelas, Mabel PF4/PF7Portunato, Gabriela O4Powe, Camille O3Powell, Theresa H8Pozzo, Josefina O4Preiti, M Cecilia PC2Previtera, Víctor PD2/PD3Propato, Liliana O4Quezada, Andrés PD5Ramírez González, M Cristina PD4Ramírez, Valeria H10Ramnath, Daniel PB4Ramos, María Pilar PB3Reck Remonti, Luciana PH3Reichelt, Angela PH3/PH7Reis, Lilian PD7/PH5/PH6Rey, Magdalena O4Reyes López, M Angélica O5/PD4Rheeder, Paul PA1/PA6Rice, Gregory H10/O6/PE5Rivas, M Margarita PG5Roberti, Sabrina O1/PB1Rocha, Clarissa R PE6Rodota, Liliana PD6
80 Index of authors
Revista de la Sociedad Argentina de Diabetes Año 50 Vol. 50 Número Especial Scientific IADPSG Meeting 2016 Marzo de 2016 ISSN 0325-5247 (impresa) ISSN 2346-9420 (en línea)
AUTOR UBICACIÓnRodríguez Cano, Ameyalli O5Rodríguez, Silvia O2Rodríguez, María PD5Rodríguez, Suilbert PC5Rojas, Susana PE1Roland, Devlieger PA2Romero, Carolina PF7Romero, Fabiola PG3Rönö, Kristiina PA5/PE8/PG7Rosseberg, M PH2Roveda, Sandra O4Rovira, Gabriela O4Rowan, Janet C5Rudge, Marilza Viera Cunha PD8/PD9/PE6/PE9Rush, Elaine C5Sacks, David A W2Sáez, Guillermo PB3Sáez, Katia PE3Saez, Tamara L3/PE2Salomon, Carlos H10/O6Salsoso, Rocío PE2/PE4/LA1Salzberg, Susana O4/W4Sanabria, Hugo PG4Sánchez, Nelson PA7Sánchez-Vera, Isabel PB3Sanhueza, C PE2/LA1Sanhueza, Lilian PG5Santos, Janine H PE6Scalise, Claudia O4Schmidt, Maria Inês L7/PA3/PH1/PH4Scholz Romero, Katherin O6Schwez Weinert, Letícia PA3Shaafie, Ishtiyaq Ahmed PG1 Shadbolt, Bruce PD1Silva Herrera, Jaime Luis PF1Silva, L PE2Silveira Mastella, Lívia PA3Silveiro, Sandra Pinho PH3/PH7Simmons, David H3Sinzato, Yuri Karen PB8/PB9Sobrevia, Luis L3/PE2/PE4/PE7/LA1Somma, I PG6Souza, Ana Claudia PC1/PC6Souza, Juliana PG2Spies, Tom D W1Stach-Lempinen, Beata PA5/PE8/PG7Strutt, Brenda L4Subiabre, Mario PE2/LA1Sucani, Stella M O4Suga, Sachie PC3Szlapinski, Sandra L4Tahir, Mahmood PA2Tanda, E PG6Thadhani, Ravi H12/O3
AUTOR UBICACIÓnTolentino-Dolores, Maricruz PD4Umezaki, Yasushi PC3Ursich, Lila PF4/PF7Valdivia, Katia PE3Valenzuela, Cristina PE1Valenzuela, Ignacio PE5Valinotti, Liz PG3Valkama, Anita PA5Varas-Godoy, Manuel H10Vasan, Soumini H8Vázquez, Fabiana PC2Veas, Carlos PE7Vecchi, Gabriela PF6Veglia, V PH2Venegas, Pía PE5Vera, Diego PG3Vera, M Inés PG4Verdi Brusati, Florencia PF7Vernini, Joice PD8/PD9Viana, Marta PB3Vicari Bolognani, Claudia PH6Vidal, José Ramón PH2Viecelli, Camila PH3Vigo, Liliana PG3Villagra, M PH2Villalba, Nidia PG3Villalba, Rosa PG3Villalobos, R PE1/PE2Villasanti, M PH2Virga, Mónica R O4Votta, Roberto PF4/PF7Wadsack, Christian L2Wasenius, Niko PE8Weinert, Letícia PH7Welham, Tamara PD1Wenger, Julia H12Weschler, Carlos PA7White, Verónica H9/PB2/PB7Yamashita, Hiroshi PC3Yanarella, Corina O4Yasuhi, Ichiro PC3Yendrika, María Florencia PH2Zacarías, LY PH2Zaccara, Tatiana PF2Zamory, Estrella Silvia O4Zhong, Linhao L4Zorrilla, Lilian PG3Zugaib, Marcelo PC1/PC6/PF2/PG2Zuñiga, Edgardo H10