Embed Size (px)
Citation preview

Spronk, I., Korevaar, J.C., Burgers, J.S., Albreht, T., Schellevis, F.G. Review of guidance on recurrence risk management for general practitioners in breast cancer, colorectal cancer and melanoma guidelines. Family Practice: 2017, 34(2), 154-160
This is a NIVEL certified Post Print, more info at http://www.nivel.eu
Postprint
Version
1.0
Journal website https://academic.oup.com/fampra/article-abstract/34/2/154/2992963/Review-of-guidance-on-recurrence-risk-management?redirectedFrom=fulltext
link
DOI 10.1093/fampra/cmw140
This is a NIVEL certified Post Print, more info at http://www.nivel.eu
Review of guidance on recurrence risk
management for general practitioners in breast
cancer, colorectal cancer and melanoma guidelines
INGE SPRONKA , JOKE C KOREVAAR
A , JAKO S BURGERS
BC , TIT ALBREHT
D, FRANÇOIS G
SCHELLEVISA
a NIVEL, Netherlands Institute for Health Services Research , Utrecht, The Netherlands
b Dutch College of General Practitioners , Utrecht , The Netherlands
c School CAPHRI, Department Family Medicine, Maastricht University , Maastricht , The Netherlands
d Centre for Health System Analyses, National Institute of Public Health , Ljubljana, Slovenia
ABSTRACT
Background.
General practitioners (GPs) will face cancer recurrences more frequently due to
the rising number of cancer survivors and greater involvement of GPs in the
follow-up care. Currently, GPs are uncertain about managing recurrence risks
and may need more guidance.
Objective.
To explore what guidance is available for GPs on managing recurrence risks for
breast cancer, colorectal cancer and melanoma, and to examine whether
recurrence risk management differs between these tumour types.
Methods.
Breast cancer, colorectal cancer and melanoma clinical practice guidelines were
identified via searches on internet and the literature, and experts were
approached to identify guidelines. Guidance on recurrence risk management that
was (potentially) relevant for GPs was extracted and summarized into topics.
Results.
We included 24 breast cancer, 21 colorectal cancer and 15 melanoma
guidelines. Identified topics on recurrence risk management were rather similar
among the three tumour types. The main issue in the guidelines was recurrence
detection through consecutive diagnostic testing. Guidelines agree on both
routine and nonroutine tests, but, recommended frequencies for follow-up are
inconsistent, except for mammography screening for breast cancer. Only six
guidelines provided targeted guidance for GPs.
Conclusion.

Spronk, I., Korevaar, J.C., Burgers, J.S., Albreht, T., Schellevis, F.G. Review of guidance on recurrence risk management for general practitioners in breast cancer, colorectal cancer and melanoma guidelines. Family Practice: 2017, 34(2), 154-160
This is a NIVEL certified Post Print, more info at http://www.nivel.eu
This inventory shows that recurrence risk management has overlapping areas
between tumour types, making it more feasible for GPs to provide this care.
However, few guidance on recurrence risk management is specific for GPs.
Recommendations on time intervals of consecutive diagnostic tests are
inconsistent, making it difficult for GPs to manage recurrence risks and
illustrating the need for more guidance targeted for GPs.
INTRODUCTION
The number of cancer survivors is rising as a result of the increasing incidence of
cancer and the advances in treatment and early detection (1,2). In 2012, there were
almost 32.5 million cancer survivors worldwide (3). The World Cancer Research
Fund estimates that this number will grow to almost 70 million survivors in 2050 (4).
On completion of curative cancer treatment, patients usually receive follow-up care
in secondary care settings by medical specialists (5,6). Due to the rising number of
cancer survivors, the limited capacity of secondary care facilities to provide follow-
up care, and the increasing costs, general practitioners (GPs) are increasingly
involved in the follow-up care (7–9). An important component of follow-up care is
detecting recurrence (5).
Recurrences regularly occur between scheduled follow-up visits and are often
initially presented as symptoms to the GP (10–12). In addition, recurrences that
occur many years after the initial treatment are probably also first presented to the
GP.
It is expected that GPs will face cancer recurrences more frequently in particular, in
follow-up care of common tumour types with high survival rates and with
recurrences occurring many years after treatment, such as breast cancer, colorectal
cancer and melanoma (13–15). It is important that GPs are able to detect recurrence
and refer patients in time to secondary care for treatment.
In order to provide optimal recurrence risk management, GPs need more applicable
guidance (16–22). GPs are especially uncertain about the type and, frequency of
tests, and the length of maintaining a test scheme during the follow-up (21). Besides,
GPs expect that providing this care increases their workload (23–25) and that they
need more expertise and formal training (16,23–27). A recent study on evidence-
based recommendations on care for breast cancer survivors in five recent evidence-
based guidelines showed that these guidelines are insufficiently helpful for GPs (28).
This stimulates the need of including guidelines not evidence based.
To uncover what guidance is available for GPs on managing recurrence risks in
patients with breast cancer, colorectal cancer and melanoma, and to examine whether
recurrence risk management differs between these tumour types, we made an
inventory of existing clinical practice guidelines originating from Australia, Canada,
European countries, New Zealand and USA and created an overview of presented
guidance.
METHODS
Two strategies were used to collect guidelines. As part of the European Union Joint
Action Cancer Control (CanCon; www.cancercontrol.eu), a Joint Action (29) which
aims to contribute to reducing the cancer burden in the European Union, an inventory
of existing clinical practice guidelines in European countries via national experts was

Spronk, I., Korevaar, J.C., Burgers, J.S., Albreht, T., Schellevis, F.G. Review of guidance on recurrence risk management for general practitioners in breast cancer, colorectal cancer and melanoma guidelines. Family Practice: 2017, 34(2), 154-160
This is a NIVEL certified Post Print, more info at http://www.nivel.eu
undertaken and in addition internet and scientific literature was searched to complete
the inventory of guidelines.
Inventory of guidelines via experts
In Autumn 2014, experts from the European Union Member States and four other
non-EU countries (Norway, Switzerland, Iceland and Turkey) were asked to supply
existing national and/or regional guidelines from their own country. Experts were
delegates from national primary care associations, nursing associations, universities
with a medical department and CanCon associated partners. At least three experts per
country were approached. In December 2014, also delegates were approached from
the Cancer and Primary Care Research International Network (CA-PRI), the
European Forum for Primary Care (EFPC), the European Society of General
Practice/Family Medicine (WONCA Europe) and CanCon collaborating partners
from nonresponding countries. Inclusion criteria were that guidelines needed to
contain guidance on care for adult cancer survivors, subsequent to curative treatment,
and that they were (potentially) relevant to GPs.
Internet and literature search
A bibliographical database search using the terms ‘guideline’, ‘breast cancer’,
‘colorectal cancer’, ‘colon cancer’, ‘rectum cancer’, ‘melanoma’ was conducted in
January 2015 to complete the inventory of clinical practice guidelines. Databases
included Embase and Medline. Also, the National Guideline Clearinghouse website,
the Guidelines International Network (G-I-N) website and cancer agency websites
were searched for relevant tumour-specific guidelines (see Supplementary Table 1
for all websites that were searched). Guidelines with a publication date from 2000 to
2015 were included and searches were conducted without any language restriction.
Guidelines were required to contain guidance on care for cancer survivors that was
(potentially) relevant to GPs, subsequent to curative treatment.
Guideline selection
Guidelines obtained from literature and internet searches were selected on basis of
title. Screening of guidelines was done by one researcher (IS). We included
guidelines focusing on adults and originating from western countries, as mentioned
above, and Australia, Canada, New Zealand and USA. We excluded older versions
of guidelines, duplicates, those that were specifically made for oncologists, and those
that only focussed on early detection, screening, treatment or palliative care,
advanced cancer or metastasis, or on specific patients groups, e.g. hereditary cancer
survivors and childhood cancer survivors.
Data extraction and content analysis
Data were extracted on the target audience of the guideline, the clinical content and
the supporting evidence. Evidence was defined as one or more references to
scientific, peer reviewed sources. Translations were used for data extraction from
guidelines written in other languages than English or Dutch. The data from Croatian,
Danish, Finnish, Norwegian and Polish guidelines were validated by the expert who
provided the guidelines. Translations of data from the French, German and Italian
guidelines were validated by researchers from the NIVEL institute who were native
speakers or who speak the specific language. Extracted data were categorized into
‘guidance on recurrence risk management’ and ‘other guidance’ by two researchers
independently (IS and JK). Subsequently, it was assessed whether the

Spronk, I., Korevaar, J.C., Burgers, J.S., Albreht, T., Schellevis, F.G. Review of guidance on recurrence risk management for general practitioners in breast cancer, colorectal cancer and melanoma guidelines. Family Practice: 2017, 34(2), 154-160
This is a NIVEL certified Post Print, more info at http://www.nivel.eu
recommendations were relevant for GPs; recommendations on diagnostic tests
performed in a secondary care setting were excluded.
Based on the relevant guidance, a clinical topic list for each tumour type was
composed. The topic lists were composed by one researcher (IS) and checked by a
second researcher (JK). Guidance was independently allocated to topics by two
researchers (IS and JK). If guidance did not fit into the predefined topics, a new topic
was created by discussion. Disagreements on categorization or allocation into topics
were resolved by discussion with a third researcher (FS).
RESULTS
Included guidelines
Twelve countries indicated that there were no tumour-specific guidelines containing
information on care for cancer survivors (potentially) relevant for GPs. From other
countries, we received at least one tumour-specific guideline on breast cancer (n =
16), colorectal cancer (n = 17) or melanoma (n = 13). Thirty of these guidelines were
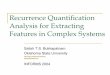
considered eligible and were included. Excluded guidelines were duplicates (n = 3),
translated versions of included guidelines (n = 3) and guidelines specifically
targeting oncologists (n = 10) (Fig. 1).
[FIGURE 1.]
The database search yielded 639 results, the National Guideline Clearinghouse
website 547 results and the G-I-N website 246. In total, in the databases and on the
cancer agency websites, 30 additional relevant guidelines were found. Overall, 60
guidelines were deemed eligible, including 24 breast cancer guidelines, 21 colorectal
cancer guidelines and 15 melanoma guidelines (Supplementary Table 2). The colon
cancer and rectal cancer guideline from the United States included the same
guidance, therefore only the colon cancer guideline was used. Included guidelines
were published between 2003 and 2015 and originated from Europe (n = 45), Canada
(n = 7), United States (n = 5) and Australia and New Zealand (n = 3). Twenty-eight
guidelines were not published in English: five were published in Dutch, five in
German, three in Danish, three in Finnish, three in French, three in Polish, two in
Croatian, two in Italian and two in Norwegian. Three guidelines were specifically
made for GPs (30,31) and three guidelines provided a summarized guide explicitly
for GPs (32–34). Furthermore, 23 other guidelines mentioned the GP explicitly as
part of their target audience.
Identification of topics
Eight topics were identified in the breast cancer and melanoma guidelines (Fig. 2). In
colorectal guidelines, seven of these topics were covered; self-examination was not
mentioned. For all tumour types, most attention was given to recurrence detection by
recommendations on diagnostic testing. Physical examination was recommended for
each of the three tumour types. Self-examination by patients was recommended in
87% of the melanoma and in 29% of the breast cancer guidelines. Additional,
diagnostic imaging (mammography) for breast cancer and laboratory diagnostic
testing [carcinoembryonic antigen testing (CEA)] for colorectal cancer was
recommended. Another topic that was often highlighted was awareness of cancer
recurrence; it was mentioned in 67% of the breast cancer, 73% of the melanoma and

Spronk, I., Korevaar, J.C., Burgers, J.S., Albreht, T., Schellevis, F.G. Review of guidance on recurrence risk management for general practitioners in breast cancer, colorectal cancer and melanoma guidelines. Family Practice: 2017, 34(2), 154-160
This is a NIVEL certified Post Print, more info at http://www.nivel.eu
80% of the colorectal cancer guidelines. In contrast, specific signs and symptoms of
recurrence received limited attention; these were reported in 15% of the colorectal
cancer, 21% of the breast cancer and 33% of the melanoma guidelines. Differences
in coverage of topics between guidelines from the tumour types were also observed.
Risk of recurrence/second cancer was pointed out in most breast cancer (67%) and
melanoma guidelines (73%), but in less colorectal cancer guidelines (40%).
Recommendations on organization of care were provided in 67% of the breast cancer
guidelines, in 50% of the colorectal cancer guidelines and in 33% of the melanoma
guidelines.
[FIGURE 2.]
Recommendations on frequency of diagnostic testing
Breast cancer
Recommendations on the frequency of physical examination were provided in 20 out
of 24 guidelines and all 24 guidelines reported a recommended frequency of
mammography (Table 1). Broad consensus existed on annual mammography.
Additionally, 10 guidelines stated that the first mammogram after breast conserving
therapy should take place after at least 6 months. Less agreement was observed on
the frequency of physical examination ranging from one to four times a year in the
first 3 years after treatment. In the 3 subsequent years, most guidelines recommended
(semi-)annually examinations. Guidelines agreed on an annual examination after 3
years.
[TABLE 1.]
Colorectal cancer
Eighteen out of 20 guidelines contained recommendations on time intervals between
consecutive physical examinations and nineteen on time intervals between
consecutive CEA testing. Eleven guidelines recommended the same frequency for
both tests. Overall, there was some agreement among guidelines on the time intervals
between consecutive tests. Recommended time intervals were 3- to 6-monthly in the
first 3 years and 6- to 12-monthly in the 4th and 5th year (Table 2). All, except one
guideline, agreed that there is no need for diagnostic testing after 5 years.
[TABLE 2.]
Melanoma
Guidance on time intervals between consecutive physical examinations was provided
by 12 out of 15 melanoma guidelines, two other guidelines stated that the frequency
and the duration of follow-up should be tailored to each individual patient.
Recommended time intervals in eight guidelines were dependent on the stage of the
melanoma as the risk of recurrence/second cancer is related to the primary tumour
thickness (35). Recommendations were inconsistent on the time intervals between
consecutive tests for both stage I and stages II and III, ranging from one to four times
a year in the first 5 years after treatment (Table 3). Most guidelines (67%) stressed

Spronk, I., Korevaar, J.C., Burgers, J.S., Albreht, T., Schellevis, F.G. Review of guidance on recurrence risk management for general practitioners in breast cancer, colorectal cancer and melanoma guidelines. Family Practice: 2017, 34(2), 154-160
This is a NIVEL certified Post Print, more info at http://www.nivel.eu
that the more advanced the disease the shorter the time intervals should be in the first
2 years. Most guidelines (83%) agreed on continuing testing during 5 to 10 years
after the initial treatment. After 10 years, there was disagreement whether to stop or
continue testing.
[TABLE 3.]
Evidence regarding recurrence risk management
Eighteen out of 59 reviewed guidelines did not include any references to scientific
evidence related to cancer recurrence risk management. Among the guidelines that
included references, the range in the number of references was one to 54. Only few
guidelines provided evidence-based recommendations on time intervals; five on
physical examination and ten on mammography for breast cancer, three on both
physical examination and CEA testing for colorectal cancer and five on physical
examination for melanoma. Evidence-based recommendations showed the same
discrepancies in preferred time intervals as the recommendations were not evidence
based (data not shown).
DISCUSSION
This is the first inventory evaluating guidance on recurrence risk management
available in existing breast cancer, colorectal cancer and melanoma guidelines that is
(potentially) relevant to GPs. It demonstrates that the topics on recurrence risk
management were rather similar among the three tumour types and that few guidance
on recurrence risk management is targeted to GPs. Most attention was given to
recurrence detection often by highlighting the importance of the diagnostic tests. For
each tumour type, there is consensus among the guidelines about the preferred type
of diagnostic tests, but, recommended frequencies for follow-up are inconsistent,
except for mammography screening for breast cancer, reflecting the lack of evidence
in this field.
The guidance on recurrence risk management of three tumour types could be
summarized into identical topics with similar components. This facilitates GPs to
provide follow-up care because the same pattern applies for different tumour types.
However, GPs still need more knowledge on details, like on diagnostic tests, which
are specific per tumour type.
Overall, the main focus in the guidelines is recurrence detection through consecutive
diagnostic testing. Guidelines agree on both routine and nonroutine tests, but, except
for mammography screening for breast cancer, recommendations on time intervals
are inconsistent. This diversity reflects the lack of high quality evidence available;
recommendations are mainly based on expert opinion. Although, the evidence-based
recommendations showed the same discrepancies in preferred time interval. Thus the
lack of agreement not only arises from expert opinions. The discrepancies in
recommended time intervals make it difficult for GPs to determine the frequency of
follow-up. This problem was confirmed by a study investigating the views of GPs on
follow-up care (21). Most common problems among GPs were uncertainty about the
type and frequency of diagnostic tests and duration of follow-up. Even when
guidance is univocal and evidence based, its implementation is crucial to improve the
quality of care and, subsequently, the survival of cancer. Further research is needed
to examine the facilitators and barriers of implementing the guidance on recurrence

Spronk, I., Korevaar, J.C., Burgers, J.S., Albreht, T., Schellevis, F.G. Review of guidance on recurrence risk management for general practitioners in breast cancer, colorectal cancer and melanoma guidelines. Family Practice: 2017, 34(2), 154-160
This is a NIVEL certified Post Print, more info at http://www.nivel.eu
risk management in daily practice and whether this leads to better cancer survival in
respective countries.
Awareness of cancer recurrence is also often mentioned in the guidelines. However,
specific signs and symptoms that may indicate recurrence are reported by few
guidelines and only one guideline provided EB guidance on signs of recurrence (33).
Signs of recurrence also receive little attention in the scientific literature as there is a
paucity of research in this field, especially in the primary care setting. Until now,
only one study examined the signs of recurrence in primary care (36). This study
showed that the symptoms of recurrence in primary care were very different from
those reported by secondary care, reflecting the need for specific guidance on signs
of recurrence for primary care. More research in primary care is needed to fill the
knowledge gap.
Most melanoma and breast cancer guidelines report the risk of recurrence and state
which patients have an increased risk of recurrence, but only few colorectal cancer
guidelines discuss this, although the risk of recurrence is not significantly lower in
colorectal cancer (37–40). In addition to detection of recurrence by health care
providers, recurrences are also detected by the patients themselves (41,42). Almost
all melanoma guidelines provide instructions on self-examination to patients,
whereas only 29% of the breast cancer guidelines recommend this. This is in
accordance with the current literature; regular self-examination does not reduce
breast cancer morbidity or mortality and it is associated with an increased number of
physician visits and high rates of benign biopsies (43–45). For melanoma, self-
examination is promoted (46,47) as evidence suggests that self-examination is
associated with reduced mortality (48) and the vast majority of melanomas and
melanoma recurrences are found by patients themselves (41,49,50). Besides,
melanomas found by self-examination have been shown to be thinner than those
found incidentally (51).
A previous study from our group focussing just on evidence-based recommendations
on care for cancer survivors in five recent evidence-based breast cancer guidelines
showed that these guidelines are not helpful to GPs (28). We used the same method
as in the current study and restricted the inclusion to evidence-based guidelines and
identified the same topics, except for signs of recurrence. Signs of recurrence were
never covered by the evidence-based recommendations. Recommendations on the
frequency of mammography screening were the same as in the current study, but, in
contrast to the lack of agreement on the recommended frequency of physical
examination in the current study, the evidence-based recommendations agreed on the
frequency of physical examination. However, a limitation was that only two
guidelines provided a recommendation on physical examination and three on
mammography. This limited number of evidence-based guidelines stimulated the
need to include guidelines not evidence-based as is done in the current study.
All guidelines in our study included both evidence-based recommendations as well
as opinion based recommendations. The lack of clear and uniform data to support
recommendations calls for expert opinions, which could explain differences between
the guidelines. However, we also found discrepancies between evidence-based
recommendations, showing the influence of interpretation of research findings is not
always straightforward.
Our study showed limited applicability of cancer guidelines for GPs, which was also
highlighted by an earlier study focussing on breast cancer, colorectal cancer and

Spronk, I., Korevaar, J.C., Burgers, J.S., Albreht, T., Schellevis, F.G. Review of guidance on recurrence risk management for general practitioners in breast cancer, colorectal cancer and melanoma guidelines. Family Practice: 2017, 34(2), 154-160
This is a NIVEL certified Post Print, more info at http://www.nivel.eu
prostate cancer guidelines (19). Another recent publication focussing on the role of
the GP in aftercare, also found that recommendations in guidelines are often not
targeted toward GPs (52). Involvement of GPs in the development of guidelines
could raise the number and relevance of recommendations to GPs (19). However, it
may be argued whether this is sufficient. Due to the limited applicability of current
guidelines for GPs, it seems the right time to develop GP specific guidelines. These
could address specific topics that are relevant in the GP care setting, where care is
more holistic and includes personalised care for patients’ comorbidities. A first
example that a GP guideline is feasible, is a recent guideline on care for breast cancer
survivors as developed in the United Stated (53). This guideline is, where possible,
based on research in primary care.
A strength of this inventory is the input of 45 experts from all 32 approached
countries. We gained information from all European Union countries and collected
additional information from other Western countries. Therefore, we were able to
create a fairly complete overview of guidance on recurrence risk management for
GPs.
A limitation of present study is the inclusion of guidelines older than 5 years. It is has
been demonstrated that almost half of the guidelines are outdated after 5 years (54).
Although, no differences were seen in both included topics and guidance between the
older and newer guidelines. This might indicate a low availability of new evidence
on recurrence risk management in the recent years.
Conclusion
This inventory represents the guidance on recurrence risk management (potentially)
relevant for GPs provided in breast cancer, colorectal cancer and melanoma
guidelines. It shows that care on recurrence risk management has overlapping areas
between tumour types, making it more feasible for GPs to provide this care.
However, only little guidance on recurrence risk management is specific for GPs and
recommendations between time intervals of consecutive diagnostic tests are
inconsistent, making it hard for GPs to know how to manage recurrence risks and
illustrating the need for more guidance targeted for GPs. Besides, all guidelines to
some extent provided recommendations that were opinion based, reflecting the need
of more high quality studies on cancer recurrence risk management.
SUPPLEMENTARY MATERIAL
Supplementary data are available at Family Practice online.
DECLARATION
Funding: Joint Action CanCon as part of the Health Programme of the European
Union.
Ethical approval: none.
Conflict of interest: IS, JCK, JSB, TA and FGS declare that they have no conflict of
interest.
ACKNOWLEDGEMENTS
We gratefully acknowledge Anne-Vicky Carlier, Marianne Heins, Pekka Honkanen,
Anne Kari Knudsen, Roar Maagaard, Mario Sekerija and Elzbièta Senkus-Konefka

Spronk, I., Korevaar, J.C., Burgers, J.S., Albreht, T., Schellevis, F.G. Review of guidance on recurrence risk management for general practitioners in breast cancer, colorectal cancer and melanoma guidelines. Family Practice: 2017, 34(2), 154-160
This is a NIVEL certified Post Print, more info at http://www.nivel.eu
for validating our translations. We would also like to acknowledge all experts who
provided us response.
REFERENCES 1 Jemal A Bray F Center MM Ferlay J Ward E Forman D . Global cancer statistics. CA
Cancer J Clin 2011 ; 61 : 69 – 90 . 2 Lu WL Jansen L Post WJ Bonnema J Van de Velde JC De Bock GH . Impact on survival
of early detection of isolated breast recurrences after the primary treatment for breast cancer: a meta-analysis . Breast Cancer Res Treat 2009 ; 114 : 403 – 12
3 International Agency for Research on Cancer . GLOBOCAN 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012 . 2012 . http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx ( accessed on 18 August 2015).
4 Marmot M Atinmo T Byers T et al Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective . Washington, DC : American Institute for Cancer Research , 2007 .
5 Hewitt M Greenfield S Stovall E . From Cancer Patient to Cancer Survivor: Lost in Transition. Committee on Cancer Survivorship: Improving Care and Quality of Life, Institute of Medicine and National Research Council . Washington, DC: The National Academies Press; 2005.
6 Lewis RA Neal RD Williams NH et al Follow-up of cancer in primary care versus secondary care: systematic review . Br J Gen Pract 2009 ; 59 : e234 – 47
7 Lewis R Neal RD Williams NH et al Nurse-led vs. conventional physician-led follow-up for patients with cancer: systematic review . J Adv Nurs 2009 ; 65 : 706 – 23
8 Taplin SH Rodgers AB . Toward improving the quality of cancer care: addressing the interfaces of primary and oncology-related subspecialty care . J Natl Cancer Inst Monogr
2010 ; 2010 : 3 – 10 9 Lichtenfeld L . Cancer care and survivorship planning: promises and challenges . J Oncol Pract 2009 5 : 116 – 8 10Auckland R Wassell P Hall S Nicolson MC Murchie P . Exploring patterns of recurrent
melanoma in Northeast Scotland to inform the introduction a digital self-examination intervention . BMC Dermatol 2014 ; 14 : 4 .
11 de Bock GH Bonnema J van der Hage J Kievit J van de Velde CJ . Effectiveness of routine visits and routine tests in detecting isolated locoregional recurrences after treatment for early-stage invasive breast cancer: a meta-analysis and systematic review . J Clin Oncol 2004 ; 22 : 4010 – 8 .
12 Grunfeld E Mant D Yudkin P et al Routine follow up of breast cancer in primary care: randomised trial . BMJ 1996 ; 313 : 665 – 9
13 Montgomery DA Krupa K Cooke TG . Locoregional relapse after breast cancer: most relapses occur late and are not clinically detected . Breast J 2009 ; 15 : 163 - 7
14 Turner RM Bell KJ Morton RL et al Optimizing the frequency of follow-up visits for patients treated for localized primary cutaneous melanoma . J Clin Oncol 2011 ; 29 : 4641 – 6 .
15 Kobayashi H Mochizuki H Sugihara K et al Characteristics of recurrence and surveillance tools after curative resection for colorectal cancer: a multicenter study . Surgery 2007 ; 141 : 67 – 75
16 Bober SL Recklitis CJ Campbell EG et al Caring for cancer survivors . Cancer 2009 ; 115 : 4409 – 18 .
17 Lawrence RA McLoone JK Wakefield CE Cohn RJ . Primary care physicians’ perspectives of their role in cancer care: a systematic review . J Gen Intern Med
. 2016 ; 31 : 1222 – 36 . 18 Zitzelsberger L Grunfeld E Graham ID . Family physicians’ perspectives on practice
guidelines related to cancer control . BMC Fam Pract 2004 ; 5 : 25 . 19 Dahlhaus A Semlitsch T Jeitler K Horvath K Siebenhofer A . Relevance to family
practice of English-language guidelines on breast, colorectal and prostate cancer: a review . Fam Pract 2015 ; 32 : 483 – 91
20 Del Giudice ME Grunfeld E Harvey BJ Piliotis E Verma S . Primary care physicians’ views of routine follow-up care of cancer survivors . J Clin Oncol 2009 ; 27 : 3338 – 45 .

Spronk, I., Korevaar, J.C., Burgers, J.S., Albreht, T., Schellevis, F.G. Review of guidance on recurrence risk management for general practitioners in breast cancer, colorectal cancer and melanoma guidelines. Family Practice: 2017, 34(2), 154-160
This is a NIVEL certified Post Print, more info at http://www.nivel.eu
21 Nissen MJ Beran MS Lee MW Mehta SR Pine DA Swenson KK . Views of primary care providers on follow-up care of cancer patients . Fam Med 2007 ; 39 : 477 – 82
22 Meiklejohn JA Mimery A Martin JH et al The role of the GP in follow-up cancer care: a systematic literature review . J Cancer Surviv . 2016 ; 10 : 990 – 1011
23 Greenfield DM Absolom K Eiser C et al Follow-up care for cancer survivors: the views of clinicians . Br J Cancer 2009 ; 101 : 568 – 74.
24 Johnson CE Lizama N Garg N Ghosh M Emery J Saunders C . Australian general practitioners’ preferences for managing the care of people diagnosed with cancer . Asia Pac J Clin Oncol 2014 ; 10 : e90 – 8
25 Roorda C Berendsen AJ Haverkamp M van der Meer K de Bock GH . Discharge of breast cancer patients to primary care at the end of hospital follow-up: a cross-sectional survey . Eur J Cancer 2013 ; 49 : 1836 – 44 .
26 Wind J Duineveld LA van der Heijden RP van Asselt KM Bemelman WA van Weert HC . Follow-up after colon cancer treatment in the Netherlands: a survey of patients, GPs, and
colorectal surgeons . Eur J Surg Oncol 2013 ; 39 : 837 – 43 27 Fidjeland HL Brekke M Vistad I . General practitioners’ attitudes toward follow-up after
cancer treatment: a cross-sectional questionnaire study . Scand J Prim Health Care . 2015 ; 33 : 223 – 32 . 28 Spronk I Korevaar J Schellevis F Albreht T Burgers J . Evidence based guidelines for
breast cancer survivors insufficiently helpful for primary care physicians . J Clin Oncol . 2016 . 29 European Commission . Funding Under the 3rd Health Programme 2014–2020 .
http://ec.europa.eu.proxy.library.uu.nl/chafea/documents/health/hp-factsheets/joint-actions/factsheets-hp-ja_en.pdf.
30 National Cancer Control Programme . Follow-up Care Plan After Treatment for Breast Cancer: A Guide for General Practitioners . Dublin, Ireland : National Cancer Control Programme ; 2013 . 31 Österreichische Gesellschaft für Allgemein- und Familienmedizin .
Tumornachsorge in der allgemeinmedizinischen Praxis . Vienna, Autria : AllMed , 2007 . 32 Aitken JF Barbour A Burmeister B Taylor S Walpole E Smithers BM . Clinical Practice
Guidelines for the Management of Melanoma in Australia and New Zealand . Cancer Council Australia and Min Health New Zealand , 2008 .
33 Cancer Australia . Recommendations for Follow-up of Women with Early Breast Cancer . Australian Government , 2010 . 34 Integraal kankercentrum Nederland .
Mammacarcinoom. Landelijke richtlijn , Versie: 2.0. Oncoline , 2012 . 35 Francken AB Accortt NA Shaw HM et al Follow-up schedules after treatment for
malignant melanoma . Br J Surg 2008 ; 95 : 1401 – 7 36 Hamilton W Barrett J Stapley S Sharp D Rose P . Clinical features of metastatic cancer
in primary care: a case-control study using medical records . Br J Gen Pract 2015 ; 65 : e516 – 22
37 Ferrone CR Ben Porat L Panageas KS et al Clinicopathological features of and risk factors for multiple primary melanomas . JAMA 2005 ; 294 : 1647 – 54 .
38 Bartelink H Horiot J-C Poortmans PM et al Impact of a higher radiation dose on local control and survival in breast-conserving therapy of early breast cancer: 10-year results of the randomized boost versus no boost EORTC 22881 -10882 trial . J Clin Oncol 2007 ; 25 : 3259 – 65 .
39 van den Brink M Stiggelbout AM van den Hout WB et al Clinical nature and prognosis of locally recurrent rectal cancer after total mesorectal excision with or without preoperative radiotherapy . J Clin Oncol 2004 ; 22 : 3958 – 64
40 Rex DK Kahi CJ Levin B et al Guidelines for colonoscopy surveillance after cancer resection: a consensus update by the American Cancer Society and US Multi-Society Task Force on Colorectal Cancer . CA Cancer J Clin 2006 ; 56 : 160 – 7
41 Francken AB Shaw HM Accortt NA Soong SJ Hoekstra HJ Thompson JF . Detection of first relapse in cutaneous melanoma patients: implications for the formulation of evidence-based follow-up guidelines . Ann Surg Oncol 2007 ; 14 : 1924 – 33 .
42 Montgomery DA Krupa K Cooke TG . Follow-up in breast cancer: does routine clinical examination improve outcome? A systematic review of the literature . Br J Cancer 2007
; 97 : 1632 – 41 .

Spronk, I., Korevaar, J.C., Burgers, J.S., Albreht, T., Schellevis, F.G. Review of guidance on recurrence risk management for general practitioners in breast cancer, colorectal cancer and melanoma guidelines. Family Practice: 2017, 34(2), 154-160
This is a NIVEL certified Post Print, more info at http://www.nivel.eu
43 Hackshaw AK Paul EA . Breast self-examination and death from breast cancer: a meta-analysis . Br J Cancer 2003 ; 88 : 1047 – 53 .
44 Baxter N , Care CTFoPH . Preventive health care, 2001 update: should women be routinely taught breast self-examination to screen for breast cancer? CMAJ 2001 ; 164 1837 – 46 .
45 Kösters JP Gøtzsche PC . Regular self‐examination or clinical examination for early detection of breast cancer . Cochrane Libr . 2003 .
46 Hamidi R Cockburn MG Peng DH . Prevalence and predictors of skin self-examination: prospects for melanoma prevention and early detection . Int J Dermatol 2008 ; 47 : 993 – 1003
47 Murchie P Allan JL Brant W et al Total skin self-examination at home for people treated for cutaneous melanoma: development and pilot of a digital intervention . BMJ Open 2015 ; 5 : e007993 .
48 Berwick M Begg CB Fine JA Roush GC Barnhill RL . Screening for cutaneous melanoma by skin self-examination . J Natl Cancer Inst 1996 ; 88 : 17 – 23
49 Brady MS Oliveria SA Christos PJ et al Patterns of detection in patients with cutaneous melanoma . Cancer 2000 ; 89 : 342 – 7
50 Richard MA Grob JJ Avril MF et al Delays in diagnosis and melanoma prognosis (I): the role of patients . Int J Cancer 2000 ; 89: 271 – 9 .
51 McPherson M Elwood M English DR Baade PD Youl PH Aitken JF . Presentation and detection of invasive melanoma in a high-risk population . J Am Acad Dermatol 2006 ; 54 : 783 – 92 .
52 Rubin G Berendsen A Crawford SM et al The expanding role of primary care in cancer control . Lancet Oncol 2015 ; 16 : 1231 – 72 .
53 runowicz CD Leach CR Henry NL et al American Cancer Society/American Society of Clinical Oncology Breast Cancer Survivorship Care Guideline . J Clin Oncol 2016 ; 34 : 611 – 35 .
54 Shekelle PG Ortiz E Rhodes S et al Validity of the Agency for Healthcare Research and Quality clinical practice guidelines: how quickly do guidelines become outdated? JAMA 2001 ; 286 : 1461 – 7
TABLES AND FIGURES

Spronk, I., Korevaar, J.C., Burgers, J.S., Albreht, T., Schellevis, F.G. Review of guidance on recurrence risk management for general practitioners in breast cancer, colorectal cancer and melanoma guidelines. Family Practice: 2017, 34(2), 154-160
This is a NIVEL certified Post Print, more info at http://www.nivel.eu

Spronk, I., Korevaar, J.C., Burgers, J.S., Albreht, T., Schellevis, F.G. Review of guidance on recurrence risk management for general practitioners in breast cancer, colorectal cancer and melanoma guidelines. Family Practice: 2017, 34(2), 154-160
This is a NIVEL certified Post Print, more info at http://www.nivel.eu

Spronk, I., Korevaar, J.C., Burgers, J.S., Albreht, T., Schellevis, F.G. Review of guidance on recurrence risk management for general practitioners in breast cancer, colorectal cancer and melanoma guidelines. Family Practice: 2017, 34(2), 154-160
This is a NIVEL certified Post Print, more info at http://www.nivel.eu

Supplementary table 1. Literature and internet searches
Literature search
EMBASE (2000 to 2015) Search 1
1. 'breast cancer':ti
2. guideline:ti
3. [humans]/lim
4. [2000-2015]/py
5. 1 AND 2 AND 3 AND 4
Search 2
1. 'melanoma':ti
2. guideline:ti
3. [humans]/lim
4. [2000-2015]/py
5. 1 AND 2 AND 3 AND 4
Search 3
1. 'colorectal cancer':ti
2. guideline:ti
3. [humans]/lim
4. [2000-2015]/py
5. 1 AND 2 AND 3 AND 4
Search 4
1. 'rectal cancer':ti
2. guideline:ti
3. [humans]/lim
4. [2000-2015]/py
5. 1 AND 2 AND 3 AND 4
Search 5
1. 'colon cancer':ti
2. guideline:ti
3. [humans]/lim
4. [2000-2015]/py
5. 1 AND 2 AND 3 AND 4
Medline (2000 to 2015) Search 1
1. breast cancer[Title] 2. limit to guideline 3. limit to publication date from 2000/01/01
Search 2 1. melanoma[Title] 2. limit to guideline 3. limit to publication date from 2000/01/01
Search 3 1. colorectal cancer[Title] 2. limit to guideline 3. limit to publication date from 2000/01/01
Search 4 1. rectal cancer[Title] 2. limit to guideline 3. limit to publication date from 2000/01/01
Search 5 1. colon cancer[Title] 2. limit to guideline 3. limit to publication date from 2000/01/01

Internet search
National guideline clearinghouse (January 2015) http://www.guideline.gov/search/search.aspx?term=melanoma http://www.guideline.gov/search/search.aspx?term=breast+cancer http://www.guideline.gov/search/search.aspx?term=colorectal+cancer http://www.guideline.gov/search/search.aspx?term=rectal+cancer http://www.guideline.gov/search/search.aspx?term=colon+cancer Guidelines International Network (G-I-N) (January 2015) http://www.g-i-n.net/library/international-guidelines-library/@@guideline_search_results?type=basic&basic-searchable-text=breast+cancer http://www.g-i-n.net/library/international-guidelines-library/@@guideline_search_results?type=basic&basic-searchable-text=melanoma http://www.g-i-n.net/library/international-guidelines-library/@@guideline_search_results?type=basic&basic-searchable-text=colorectal+cancer http://www.g-i-n.net/library/international-guidelines-library/@@guideline_search_results?type=basic&basic-searchable-text=rectal+cancer http://www.g-i-n.net/library/international-guidelines-library/@@guideline_search_results?type=basic&basic-searchable-text=colon+cancer Cancer agency websites (January 2015) Alberta Health Services (http://www.albertahealthservices.ca/) American Cancer Society (http://www.cancer.org/) American Society for Clinical Oncology (ASCO) (http://www.asco.org/) British Colombia Cancer Agency (BCCA) (http://www.bccancer.bc.ca/) Cancer Care Ontario (https://www.cancercare.on.ca/) Cancer Council Australia (http://www.cancer.org.au/health-professionals/clinical-guidelines/) Comprehensive Cancer Centre the Netherlands (IKNL) (http://www.oncoline.nl/) European Society for Medical Oncology (ESMO) (http://www.esmo.org/) Haute Autorité de Santé (http://www.has-sante.fr) National Comprehensive Cancer Network (NCCN) (http://www.nccn.org/) National Institute for Health and Clinical excellence (NICE) (https://www.nice.org.uk/) New Zealand Guidelines Group (NZGG) (http://www.health.govt.nz/about-ministry/ministry-health-websites/new-zealand-guidelines-group) Saskatchewan Cancer Agency (http://www.saskcancer.ca/) Scottish Intercollegiate Guidelines Network (SIGN) (http://www.sign.ac.uk/) Sociedad Espanola de Oncologia Medica (SEOM) (http://www.seom.org/)

Supplementary table 2. Included guidelines
Table 1. Included guidelines
Country Year Title
Breast cancer (n=24)
Australia 2010 Recommendations for follow-up of women with early breast cancer*
Austria 2007 Tumour aftercare in general practice†
Belgium 2013 Breast cancer in women: diagnosis, treatment and follow-up Canada 2005 Clinical practice guidelines for the care and treatment of breast cancer: 9.
Follow-up after treatment for breast cancer (2005 update) Canada – Alberta 2013 Follow-up care for early-stage breast cancer Canada – British Columbia
2013 Breast Cancer: Management and Follow-Up
Canada - Saskatchewan 2012 Breast Cancer Treatment Guidelines Croatia 2012 Clinical guideline for the diagnosis, treatment and monitoring of patients with
non-invasive breast cancer Denmark 2012 Breast cancer guideline Europa 2013 Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis,
treatment and follow-up Finland 2014 Breast cancer France 2010 Breast cancer Germany 2012 Interdisciplinary S3 guideline for the diagnosis, treatment and aftercare of
breast cancer Ireland 2013 Follow-up care plan after treatment for breast cancer - A guide for General
Practitioners†
Italy 2014 Breast cancer guideline Netherlands 2012 Breast cancer. National guideline version 2.0
§
New Zealand 2009 Management of Early Breast Cancer Norway 2014 National action program with guidelines for diagnosis, treatment and
monitoring of patients with breast cancer Poland 2014 Control tests after treatment in the most common solid tumours in adults Spain 2013 SEOM Clinical Guidelines for the systemic treatment of early breast cancer
2013 Spain - Catalonia 2009 Breast Cancer Guideline United Kingdom 2009 Early and locally advanced breast cancer: diagnosis and treatment United States 2013 Breast Cancer Follow-Up and Management After Primary Treatment: American
Society of Clinical Oncology Clinical Practice Guideline Update United States 2014 Breast Cancer
Colorectal cancer (n=21)
Austria 2007 Tumour aftercare in general practice*
Belgium 2014 Colon Cancer Belgium 2004 Rectum Cancer Canada - British Columbia
2013 Follow-up of Colorectal Polyps or Cancer
Canada - Ontario 2012 Follow-up Care, Surveillance Protocol, and Secondary Prevention Measures for Survivors of Colorectal Cancer
Canada – Saskatchewan
2011 Provincial Colorectal Cancer Treatment Guidelines
Croatia Clinical guideline for the diagnosis, treatment and monitoring of patients with colorectal cancer
Denmark 2012 Colorectal cancer guideline Europe 2013 Early colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment
and follow-up Finland 2013 Colorectal cancer France 2012 Colorectal cancer and adenocarcinoma Germany 2014 S3 guideline colorectal cancer

Italy 2014 Colorectal cancer guideline Netherlands 2014 Colorectal cancer. National guidelines version 3.0 Poland 2014 Control tests after treatment in the most common solid tumours in adults Spain - Catalonia 2009 Colorectal Cancer guideline Switzerland 2007 Revised consensus recommendations for aftercare
after colonoscopy and after curative surgery for colorectal cancer United Kingdom 2011 Colorectal cancer
The diagnosis and management of colorectal cancer USA 2015 Colon Cancer USA 2015 Rectal Cancer
Melanoma (n=15)
Australia and New Zealand
2008 Clinical Practice Guidelines for the Management of Melanoma in Australia and New Zealand
*
Belgium 2007 National guidelines for clinical practice: Melanoma Denmark 2012 Melanoma guideline Europe 2012 Cutaneous melanoma: ESMO Clinical Practice Guidelines for diagnosis,
treatment and follow-up Europe 2012 Diagnosis and treatment of melanoma. European consensus-based
interdisciplinary guideline – Update 2012 Finland 2012 Melanoma France 2012 Cutaneous melanoma Germany 2013 Malignant Melanoma S3 guideline "Diagnosis, treatment and aftercare of
melanoma" Netherlands 2012 Melanoma. National guideline version 2.0 Norway 2013 National action program with guidelines for diagnosis, treatment and follow-up
of malignant melanomas Poland 2014 Control tests after treatment in the most common solid tumours in adults Scotland 2003 Cutaneous Melanoma - A national clinical guideline Switzerland 2011 Updated Swiss guidelines for the treatment and follow-up of cutaneous
melanoma United Kingdom 2011 Improving outcomes for people with skin tumours including melanoma:
Evidence Update October 2011 United States 2015 Melanoma *This clinical guideline provided a guide for general practitioners. This guide refers to the clinical guideline for more
information. Therefore, the clinical guideline is included.
†This guideline
was specifically made for general practitioners.
§A part of the information reported in the multidisciplinary guideline is copied to the general practitioners guide ‘diagnosis
of breast cancer’. This guide refers to the multidisciplinary guideline. Therefore, the multidisciplinary guideline is included.