Embed Size (px)
Citation preview

REVIEW: CLINICAL VARIABILITY AND GENETIC HETEROGENEITYIN MULTIPLE EPIPHYSEAL DYSPLASIA
Kathryn L. Chapman and Michael D. Briggs u WellcomeTrust Centre for Cell-
Matrix Research, School of Biological Sciences, University ofManchester,Manchester,
United Kingdom
Geert R. Mortier u Department ofMedical Genetics, University Hospital of Ghent,
Ghent, Belgium
u This review reports on multiple epiphyseal dysplasia (MED), ¢rst described clinically in the early part
of the 20th century. Over 50 years later, we are now beginning to unravel the mystery behind the genetic
mutations involved in triggering the changes in cartilage observed in this condition. In the past decade con-
siderable progress has been made in identifying the underlying genetic defect in some forms of MED.
Understanding the precise e¡ect that these molecular changes have on the integrity of the cartilage extra-
cellular matrix will lead the way in identifying the complex disease pathophysiology that de¢nes MED.
In addition, a greater understanding of the role and interactions of speci¢c cartilage molecules may reveal
the basis of more widespread cartilage disorders such as osteoarthritis.
Skeletal development in the embryobeginswith the formation of a hyaline cartilagemodel and through endochondral ossi¢cation this template of the vertebrate skele-ton is replaced by bone. Cartilage persists in the epiphyseal growth plate until pub-erty where the continuous proliferation, maturation, and hypertrophy ofchondrocytes result in long bone growth. In adults, articular cartilage remains atthe surface of bones, where it provides a smooth surface andconfers weight-bearingstrength to the joints. The extracellular matrix (ECM) secreted by chondrocytesprovides the fundamental structure of cartilage.The theory that this matrix is inerthas long since been dispelled, and even subtle alterations can signi¢cantly changethe properties and strength of cartilage. In addition to providing tensile strength,various functional components present in the matrix sequester diverse factors thatare involved in cell and matrix interactions. Defects in cartilage formation andmaintenance can lead to phenotypes ranging from relatively rare chondrodyspla-sias to the common degeneration of articular cartilage resulting in osteoarthritis.
Address correspondence to Michael D. Briggs,WellcomeTrust Centre for Cell-Matrix Research, School ofBiological Sciences, University of Manchester, 2.205 Stopford Building, Oxford Road, Manchester, M13 9PT,UK. E-mail: [email protected]
Pediatric Pathology andMolecular Medicine 22: 53^75, 2003Copyright# 2003 Taylor & Francis1522-7952/03 $12.00 + .00DOI: 10.1080/15227950390168183
53
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

HISTORICAL NOTE
Multiple epiphyseal dysplasia (MED) was initially recognized as a distinct os-teochondrodysplasia by Sir Thomas Fairbank, who published his comprehensivefindings in 1947 [1]. He described MED ‘‘as a rare congenital development errorcharacterised by mottling or irregularity in density and outline of several of the de-veloping epiphyses, dwarfism and stubby digits.’’He further stated that ‘‘hereditaryand familial influences are not in evidence as a rule, but one case apparently inher-ited it from his mother, and two sisters and also twin brothers are included in ourseries.’’ Hence from the outset, the genetic basis of MED appeared intricate. Since1947 numerous familial cases of MED have been reported and as early as 1955Maudsley pointed to an autosomal dominant basis for MED, stating that ‘‘thedefect appeared to be due to aMendelian unifactorial dominant gene [2].’’
CLINICAL FEATURES
Multiple epiphyseal dysplasia is primarily anautosomaldominant chondrodys-plasia, althoughautosomal recessive formshavebeendescribed [3,4].The conditionwas initially classified into the mild ‘‘Ribbing’’ and severe ‘‘Fairbank’’ types, but itsoonbecame clear that these two forms in fact definedabroadphenotypic spectrum[5]. In contrast to most other chondrodysplasias, the condition usually is not char-acterized by significant short stature [6]. The disorder can present in early child-hood with complaints of a waddling gait, easy fatigue, or joint pain after exercise.Generally the hips and knees aremost commonly affected [7], but ankles, shoulders[8], wrists, and hands also can be involved. In adulthood, the diagnosis is usuallymade because of early-onset osteoarthrosis [7]. Physical examination of affectedchildren may reveal a normal to mildly short statute, limited articular mobility,and waddling gait. Hands and feet are usually short and genu varum or genu val-gummay be present [5].
Radiographic evaluation shows a predominantly epiphyseal involvement andradiographic abnormalities can be present before the onset of physical symptoms.During the initial stage of thedisease, epiphysealossificationdelay is observed,whilelater on, with the appearance of the epiphyses, the ossification centers are usuallysmall and sometimes fragmentedwith irregular contours (Figure1). Inaddition, theadjacentmetaphysealbordersmaybe slightlyabnormal. Inadulthood, the articularsurfaces of the joints may be flattened and dysplastic with early features of osteo-arthrosis (Figure1) [7].Usually the epiphyses of thehips andknees aremost affectedbut ivory epiphyses in the hands, Schmorl nodes in the spine, and a double-layeredpatella [9, 10] are other radiographic signs of the condition.The absence of severespinal involvement andminimal metaphyseal defects allow differential diagnosis ofMED from other diseases with similar clinical features (e.g., spondyloepimetaphy-seal dysplasia (SEMD) and spondyloepiphyseal dysplasia (SED)).
Clinical variability occurs both within the same family and between differentfamilies, a single disease causing mutation can lead to hip involvement in one
54 K. L. Chapman et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

affected individual but not in another even though they may have an identical mu-tation. Therefore, it seems likely that environmental or additional genetic factorscontribute to the MED phenotype.
MOLECULAR GENETICS OF MED
Mutations in the cartilage oligomeric matrix protein (COMP) [11] gene, lo-cated on chromosome 19p12 [12], were the first to be identified in MED (EDM1)[13], and these studies also established that some forms of MED were allelic withpseudoachondroplasia [13, 14], a disease that shares some clinical features withMED [15]. Subsequently point mutations in the three type IX collagen genes
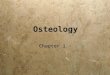
FIGURE 1. Radiographic evaluation of a family with multiple epiphyseal dysplasia. (a) Family pedigree.(b) Flattening and dysplasia of both femoral heads of II-2 at 38 years of age, and (c) bilateral deformed jointsurfaces of the knees withmultiple loose bodies in the joint space (osteochondritis dissecans) of II-2 at 22 years ofage. (d) Flattening andmild sclerosis of right femoral headwith osteophytosis at the uppermargin and £atteningof left femoral head, of II-3 at age 38 years, and (e) bilateralmildly deformed joint surfaces of the knees (partially£attening of the femoral surfaces) with solitary loose body in the left joint space of II-3 at 25 years of age.(f ) Abnormal acetabular contours, small femoral epiphyses, and irregular ossi¢ed epiphyses of trochanter majorof III-1at 8 years of age, and (g) bilateral irregular ossi¢ed and fragmented knee epiphyses.The medial part ofthe tibial metaphysis shows a lucent area, III-1at 8 years of age.
Molecular Genetics ofMultiple Epiphyseal Dysplasia 55
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

(COL9A1, COL9A2, and COL9A3, located on chromosomes 6q13, 1p33-p32.2, and20q13.3, respectively) were shown to cause a milder MED phenotype (EDM2,EDM3, and EDM6, respectively) [16^23]. Furthermore, a form of MED recentlyhas been shown to result from mutations in gene encoding matrilin-3 (EDM5)[24]. Finally, recessive forms ofMED (EDM4) have been shown to result frommu-tations in the gene-encoding diastrophic dysplasia sulphate transporter (DTDST)located on chromosome 5q32-q33.1 [25].
The pursuit of additionalMED-causingmutations has emerged as challengingandwide-ranging, in asmuch as the genetic basis has yet tobe elucidated in thema-jority of MED cases. Because five of the current candidate genes for autosomaldominant MED (COMP, COL9A1, COL9A2, COL9A3, and MATN3 ) have beensearched exhaustively, without success, in a number of patients, it seems likely sev-eral more disease-causing genes must contribute modestly to the overall prevalenceof MED. Alternatively, there could be a single gene, yet to be identified, mutationsin which result in the largest proportion of MED cases.
CARTILAGE OLIGOMERIC MATRIX PROTEIN (EDM1)
Cartilage oligomeric matrix protein (COMP) is a pentameric glycoproteincomposed of five identical 110kDa monomers (Figure 2a.) The amino terminus ofeachmonomer contributes to the oligomerization domain and pentamerization oc-curs intracellularly [26] by an a-helical coiled-coil arrangement that is stabilizedby interchain disulphide bonds [27]. Adjacent to the amino terminal domain arefour type 2 (EGF-like) repeats, followed by eight type 3 (calmodulin-like) repeats,anda globular carboxyl-terminal (C-terminal) domain.The type 3 repeats are un-ique to the thrombospondin family, of which COMP is the fifth member, and havebeen shown to bind Ca2þ with high affinity and in a cooperative manner [28].The secondary structure of this region of COMP is likely to be determined in partby numerous intrachain disulphide bonds and also by binding Ca2þ to the type 2and type 3 repeats. Indeed COMP assumes a more compact conformation in thepresence of Ca2þ, confirming that Ca2þ-binding is essential for correct folding ofthe molecule [28, 29]. COMP is expressed predominately in cartilage, tendon,and ligament, which explains why mutations in the COMPgene can cause a carti-lage disorder with significant joint laxity. Cation-dependent interactions betweenthe thrombospondins and othermatrix molecules have been demonstrated; specifi-cally, COMP is capable of binding to type I collagen, type II collagen [30], andtype IX collagen [31, 32] with high affinity. These interactions require Zn2þ, areindependent of Ca2þ, and are mediated by the C-terminal domain of COMP. Ro-tary shadowing transmission electronmicroscopy and real-time biomolecular ana-lysis (BIAcore) have shown that the C-terminal domain of COMP bindsspecifically to the noncollagenous domains of type IX collagen (Figure 2c) [31].Furthermore, the precise folding of COMP, mediated by Ca2þ-binding, is
56 K. L. Chapman et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

necessary for binding to type II and type IX collagen, and these interactions aredisrupted by mutations in the type 3 repeats [32].
The precise biological function of COMP remains to be determined; however,its prominent C-terminal domains are positioned ideally for binding to severalma-trix molecules simultaneously, which implies that it plays an essential interactiverole in the ECM, such as coordinating collagen fibrillogenesis. Indeed it has beenproposed that COMP may act as a molecular chaperone, bringing different col-lagen molecules together to form heterotypic fibrils. In addition, preliminary evi-dence has indicated that COMP can also bind to cells via an integrin-mediatedmechanism, suggesting the intriguing possibility that COMP can directly regulatecollagen fibril assembly through cellular regulation of procollagen synthesis.
Mutations in COMP
Mutations in COMP can cause MED and a phenotypically related osteochon-drodysplasia, pseudoachondroplasia (PSACH). PSACH results exclusively frommutations in COMP, whereas MED can result from mutations in at least five othergenes [3]. The majority of COMP mutations identified to date occur in the Ca2þ
-binding (type 3) domain of COMPand are either in-frame deletions or insertions
FIGURE 2. Rotary shadowing transmission electron microscopy of individual (a) COMP. (b) Type IX col-lagen molecules, whereas (c) shows a COMP molecule interacting with the NC2 domain of a type IX collagenmolecule via its C-terminal domain.The scale bar represents 100 nm.
Molecular Genetics ofMultiple Epiphyseal Dysplasia 57
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

(of 3, 6 or 9 nucleotides), or point mutations that are predicted to result in aminoacid substitutions [13, 33^39]. Interestingly, no nonsense or frameshift mutationshave been identified, which would ultimately result in nonsense-mediated mRNAdegradation. This observation, and the location of mutations exclusively in func-tionally important regions, suggests that mutations in COMP cause a qualitativerather than a quantitative defect.
A ‘‘Hot-Spot’’ for COMP Mutations
Themost commonmutation, found in 36%of all PSACHcasesbut in noMEDcase to date, is the in-frame deletion of 3 bp froma region of theCOMPgene that en-codes for five consecutive aspartic acid residues (TGC GAC GAC GAC GAC GAC
AAT) [14, 37]. The severity of the phenotype suggests that deletion of an asparticacid may affect both the Ca2þ-binding affinity of COMP and tertiary structure ofthe type 3 domain [40]. However, an expansion of this GAC repeat from (GAC)5to (GAC)6 or (GAC)7 results inMEDand PSACH, respectively [38]. Initial inter-pretation suggests that within this region the insertion of an aspartic acid residuehas a least deleterious effect than the deletion of the same residue, although expan-sion of the region by two aspartic acid residues manifests as PSACH. Only high-resolution structural studies using x-ray crystallography will provide the answersto these intriguing questions.
Aspartic Acid Residues Most Frequently Mutated
The most common amino acid substitutions are those for conserved asparticacid residues in the type 3 repeats and are postulated to alter the Ca2þ-bindingaffinity of this domain (Table 1). A cooperative effect on the remaining sevenCa2þ-binding domains, rendering the Ca2þ-binding region dysfunctional [28, 29],may result in a decreased ability of COMP to interact with other matrix mole-cules [32]. Of particular interest is how the substitution of a conserved asparticacid residues can cause either MED or PSACH. It is apparent that both theposition and the nature of the amino acid substitution are of great significance indetermining the severity of the phenotype. Whereas the majority of Asp?Tyrand Asp?Val changes cause MED, the other changes (Asp?His, Asp?Asn,Asp?Gly, Asp?Ala) exclusively cause PSACH. One possible explanation isthat tyrosine and valine residues are tolerated to a greater extent in the Ca2þ-binding domains. The substitution of cysteine, glycine, and asparagine also arecommon mutations and are predicted to have equally deleterious effects on thestructure of this region of COMP and ultimately the binding of Ca2þ. The pre-dominance of mutations occurring at these four particular amino acid residuessuggests that they are essential for coordinating the structure of the type 3repeats.
58 K. L. Chapman et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

Mutations in the C-Terminal Domain
A number of interesting mutations have been identified in the C-terminal do-main of COMP and recent studies on the binding of COMP to various collagenshave now shown these to be highly significant. Four amino acid substitutions havebeen identified in a five-residue segment of the C-terminal domain, namelyE583K, T585R, T585M, and H587R, and one of these substitutions, T585R,has been identified in two unrelated individuals [37, 39, 41]. Of particular interestis the phenotypic effect of these specific mutations: T585R results in an unclassi-fied form of MED, whereasT585M results in a mild form of PSACH but showingclear phenotypic overlap with MED [37]. T585R is a conserved amino acid sub-stitution, whereas T585M is a nonconserved substitution and this may have agreater effect on the local structure or charge environment of this region of theC-terminal domain. The other mutations, E583K and H587R, result in aPSACH phenotype with typical radiographic and clinical features [39, 41]. Allthese mutations occur in a region of the C-terminal domain that coordinateshigh-affinity binding to type IX collagen (Figure 2c) [31], suggesting that disrup-tions to these important interactions may be a contributing factor to the pathoge-netic mechanism of this bone dysplasia family.
TABLE 1. AminoAcid Substitutions in Exons Encoding theType 3 Repeats of COMP
Amino acid Codon Domain Phenotype Reference Number
Asp-His 271 type 3 #1 PSACH 39511 type 3 #8 41518 type 3 #8 39
Asp-Asn 290 type 3 #1 PSACH 36446 type 3 #6 43473 type 3 #7 41475 type 3 #7 41518 type 3 #8 36
Asp-Val 302 type 3 #2 MED 39361 type 3 #4 36
Asp-Tyr 342 type 3 #3 MED 13361 type 3 #4 35408 type 3 #5 35472 type 3 #7 PSACH 14
Asp-Gly 349 type 3 #3 PSACH 36437 type 3 #6 39473 type 3 #7 36482 type 3 #8 34507 type 3 #8 41509 type 3 #8 41
Asp-Ala 509 type 3 #8 PSACH 41
Molecular Genetics ofMultiple Epiphyseal Dysplasia 59
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

CELL MATRIX PATHOLOGY OF COMP DISEASES
One Mutant Monomer Affects Majority of Pentameric Molecules
In many ECM macromolecules, a dominant-interference effect occurs whenmutant monomers are incorporated into higher order multimeric structures, suchas triple helical collagen molecules or COMP pentamers. The incorporation ofmutant monomers into a pentamer such as COMP will disrupt the majority ofpentameric molecules. Assuming that mutant monomers are randomly incorpo-rated into COMP pentamers, it follows that only 3% of COMP pentamers wouldconsist of five normal COMPmonomer chains. Furthermore, if the mutantCOMPpentamers are secreted from the cell and incorporated into the ECM, they alsomay negatively interact with the 3% of normal pentamers in the matrix.
Action of COMP Mutations
There are no data to suggest that haploinsufficiency of COMPat themRNA le-vel occurs in either MED or PSACH. Indeed mutant and normal COMP mRNAis translated at similar levels and appears to show no difference in stability [26].Furthermore, the mutations found in COMP are all predicted to alter the functionof the protein, rather than affectmRNAexpression and stability. AbnormalCOMPmonomers can be incorporated into pentamers, even though they show reducedCa2þ-binding and are conformationally altered [28, 38].Therefore, the most com-prehensible mechanism by which COMP mutations exert their effect is via a domi-nant-interference mechanismwhere incorporation of mutant chains effects 97% ofCOMP pentamers.
This dominant negative interference mechanism may occur by the accumula-tion of pentameric COMP in the rough endoplasmic reticulum (RER) of chondro-cytes. Abnormally folded COMP is retained in the RER of cells, possible by theaction of specific molecular chaperones during the unfolded protein recognitionpathway (Figure 3). In many cases the accumulation of misfolded COMP in theRERof chondrocytes results in a characteristic lamellar appearance [42].This pe-culiar pattern, exhibiting alternating electron light and electron dense layers, hasbeen shown to be partly due to accumulation of COMP that appears to localize tothe electron dense region [43].This lamellar appearance is seen in the majority ofPSACH chondrocytes [44] and also in a fewMED chondrocytes [45], although inmost MED chondrocytes the accumulated material has a less organized appear-ance.Type IX collagenandaggrecan alsoare present in the expandedRERvesiclesof these cells [43, 45].The accumulation of abnormal COMP in the RERof tendonand ligament cells is not a consistent feature of these diseases [43], but it has beenobserved on a number of occasions (Figures 3c and 3d) [26]. However, patientswith COMP mutations have joint laxity, suggesting that mutant COMP does havea pathological effect in tendon and ligament.Type IX collagen is not expressed in
60 K. L. Chapman et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

tendon; therefore, the accumulation observed in tendon cells must consist of a dif-ferent set of matrix molecules than those found in cartilage [38].
The accumulation of other ECMmolecules may result from abnormal COMPobstructing the protein secretary pathway in a generalized fashion. If this werethe case, one would expect to see an extensive range of ECM molecules retainedwithin the RER. However, type IIcollagen, which has been shown to interact withCOMP in vitro [30] is not present in the RER versicles in PSACH chondrocytes[43].The absence of type II collagen in the RERmay be due to the different secre-tary pathways for these two molecules, as previously suggested [46]. Alternatively,the accumulation of otherECMmoleculesmaybe the result of specific intracellularinteractions. Some of the molecules that normally bind to COMP in the ECMmay be interacting in this intracellular environment to form largemacromolecularstructures prior to their secretion. For example, type IX collagen may be retainedalongside COMP because it interacts with COMP in the ECM. Subsequently, mo-lecules that interact with type IX also could be prevented from passing throughthe RER resulting in a cascade of accumulation, which ultimately would affectthe amount of various matrix molecules present in the ECMand consequently theseverity of the phenotype.
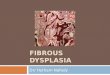
FIGURE 3. Electron micrographs of (a) cartilage and (d) ligament cells from a patient with MED and (b)cartilage and (c) ligament cells from a patient with PSACH. The patient with MED is III-1 from the familyshown in F|gure 1 and has an N489K substitution in COMP. The PSACH patient is case 3 in Newman et al.2000 [84] and has a G465S substitution in COMP. Note the large prominent inclusion bodies in the cartilageand ligament cells, that are indicated with an asterisk. The ligament cell from the PSACH patient shows mor-phologic signs of apoptotic cell death, but there is a large insoluble aggregate of misfolded COMP in the remnantof the RER.
Molecular Genetics ofMultiple Epiphyseal Dysplasia 61
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

It has been suggested that the accumulation of abnormal COMP (and otherproteins) in the RER of PSACH cells eventually leads to cell death in vitro
(Figure 2c)[47]. If the samewere true in vivo, cell deathmay result in a dramatic de-crease in viable chondrocytes, thereby disturbing endochondral ossification thatin turn may contribute to the short statute phenotype. However, ultrastructuralanalysis of growth plate cartilage from patients with COMP defects has failed toidentify a significant level of cell death in vivo. In contrast, cell death appears to oc-cur mostly in articular cartilage where cell division occurs only infrequently.Thispathological process, in addition to the abnormalities found within the extracellu-lar matrix, such as abnormal (or fused) collagen fibrils, may explain some of theclinical features of PSACH and EDMI, such as the premature osteoarthritis. Thelevel of COMP found in the extracellular matrix of PSACH and MED tissues re-mains controversial. In cartilage from PSACH patients, most of the mutant mole-cules appear to be retained in the RER and very little COMP is detected in theECM [43,48]. However, COMP is secreted from cultured PSACH chondrocytesand is present in the matrix surrounding these cells, suggesting that it could exert
FIGURE 4. Schematic showing type IX collagen and those mutations in COL9A2, COL9A3, and COL9A1 thatcauseMED (EDM2, EDM3, and EDM6, respectively).The three collagenous domains (COL1^COL3) of typeIX collagen are separated by noncollagenous domains (NC1^NC4). Note that the NC4 domain is derivedentirely from the a1(IX) chain [a1IX(NC4)]. The point mutations in the splice donor and acceptor sites ofCOL9A2 and COL9A3 are shown, as is the insertion of an adenine at position þ 3 of the splice acceptor site ofexon 8 of COL9A1.
62 K. L. Chapman et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

a dominant-interference effect in the ECM [26, 28], by disrupting cartilage ultra-structure and homeostasis.
In vitro studies have demonstrated that although there is a decrease in the levelsof COMP in the ECM secreted by cultured PSACH chondrocytes, the matrix ar-chitecture does appear normal [47]. As mutant COMP appears to be secreted atnormal levels in in vitro fromPSACHandMEDchondrocyte cell cultures, the cellu-lar environment in vivomay contribute to the accumulation of COMP in the RERand its absence from the ECM. Overall, subtle differences in two dominant-inter-ference mechanismsRaccumulation of COMP (and other proteins) in the RERand the presence in the ECMof abnormal COMPRmay explain some of the phe-notypic differences in the PSACH=EDM1disease spectrum.
TYPE IX COLLAGEN (EDM2, EDM3, AND EDM6)
Type IX and Type II Collagen in Cartilage ECM
Type IX collagen is a fibril-associated collagen with interrupted triple helices(FACIT). It is heterotrimer [a1(IX)a2(IX)a3(IX)] with three collagenous do-mains; COL1,COL2, andCOL3 separatedby four noncollagenous (NC) domainsNC1-4 (Figure 2b). A single chondroitin sulphate chain located at a serine residuein the NC3 domain of a2(IX) denotes its classification as a proteoglycan, in addi-tion to that of a collagen [49]. Type IX collagen exists as either a ‘long form,’ inwhich the NC4 domain is present, or a short form in which the NC4 domain is ab-sent [50].The long formof type IX collagen is the predominant species in cartilage,while the vitreous of the eye contains only the short form.The NC4 domain is de-rived exclusively from the a1(IX) chain and through alternative splicing and thesubsequent use of an alternative start codon in the COL9A1gene, the vitreous formof type IX collagen lacks the entire a1(IX) NC4 domain.
Expression of type IX collagen hasbeen shown in cartilage, brain, and skin tis-sue of mice. However, expression in cartilage appeared tobemore tightly regulatedthan in other tissues [51]. In the chick, the short form of collagen type IX is foundin the developing peripheral nervous system, the notochord, and the vitreous[52^55].The alternate long form is identified in cartilage both during developmentand in adult tissues [56]. All chondrocytes, except terminal hypertrophic chondro-cytes, synthesize type IX collagen. In the cartilage ECM, type IX collagen inter-acts covalently with type II collagen fibrils and is located on the type II collagenfibril surface [57].The COL3 and globular NC4 domains project out from the sur-face of the collagen fibril and are therefore in an ideal position to interact with othermatrix molecules, such as COMP (Figure 2c). The position of type IX collagenand its potential tobind to othermatrix components have implicated it in determin-ing the surface properties and interactions of the type II collagen fibrils. Conse-quently, type IX collagen may play an important role in preserving the structuralintegrity of articular cartilage and=or sustaining cartilage homeostasis [57].
Molecular Genetics ofMultiple Epiphyseal Dysplasia 63
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

Type IX Collagen Mutations Result in Exon Skipping
All type IX collagen gene mutations are clustered in the splice-donor site ofexon 3 of COL9A2 [16, 17], the splice-acceptor site of exon 3 of COL9A3 [18, 19, 21]or the splice-acceptor site of exon 8 of COL9AI [23].These mutations result in theskipping of exon 3 of COL9A2 and COL9A3 or exon 8 and=or 10 of COL9A1duringRNA splicing (Figure 4).The resulting 36bp deletion in the mRNA from COL9A2
and COL9A3 gives rise to a 12 amino acid in-frame deletion from the a2(IX) ora3(IX) chains.The in-frame deletion of 75, 63, or 138 bp in COL9A1gives rise to a25, 21, or 49 amino acid in-frame deletion from the a1(IX) chain. All these dele-tions are located in the equivalent region of the COL3 domain of type IX collagen,and this precise location demonstrates the importance of this domain. Interestingly,the location of the mutation in the splice donor site determines the stability ofthe mRNA from the mutant allele. Ex3[�1]G?A and IVS3DS[þ6]T?G, bothidentified in COL9A2, appear to result in decreased levels of mutant mRNA. In thecase of Ex3[�1]G?A, this was shown to be the result of mRNA degradation butthe precise levels andmechanism of this degradation remain to be determined. ForIVS3DS[þ6]T?G, no mechanism could be assigned; however, the location of themutation in position þ 6 of the splice-donor sitemight lend itself to correct splicingof the mutant mRNA in a proportion of the transcripts.The relatively mild MEDphenotype seen in both of these families may well result from the decreased levelsof mutant mRNA, albeit by different mechanisms, that it available for translation.
Collagen Type IX Mutations and Milder Forms of MED
All themutations identified in the COL9AI, COL9A2, and COL9A3 genes to dateresult in a similar deletion from the COL3 domain of type IX collagen, suggestingthat this region of the molecule is important for its structure and=or function. Itwould be expected that the disease progression in the affected individuals of eachof these families should show some phenotypic similarities. In this respect, themoststriking comparison, in the five families studied, is the absence or reduced incidenceof hip dysplasia [22]. In addition, severe knee pain and deformity also appear tobe a consistent feature, often requiring such surgical intervention as osteotomies.This is in direct contrast to MED that results from mutations in the COMP gene,which manifests with severe hip dysplasia and in the more severe cases dispropor-tionate short stature [22].
The obvious difference between these two forms of MED is that COMP is ex-pressed at high levels in tendon and ligament and that these patients suffer fromjoint laxity, which possibly acts as a major factor in the development of early onsetosteoarthritis in the hips of these patients. The observation that COL9AI is asso-ciated with hip osteoarthritis in females is puzzling [58], particularly when thereis little or no involvement of the hips in MED patients with COL9A2 and COL9A3
mutations, and this observation certainly requires further investigation. One
64 K. L. Chapman et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

further point that is noteworthy:Two of three families reported exhibiting COL9A3
mutations showed osteochondritis dissecans caused by incorrect ossification [18,29, 21], whereas this has not been described in any of the families with COL9A2mu-tations. The link between multiple epiphyseal dysplasia and osteochondritis hasnot been fully explored [59, 60], but it is sufficiently common to warrant greaterinvestigation.
OTHER FACTORS CAUSING PHENOTYPIC VARIABILITY
Two families have been described with identical COL9A3 mutations (IV-S2AS[�1]G?A) [19, 21] and show similar symptoms, including joint pain, stiff-ness, and mild myopathy that results in difficulties in walking. However, the age ofonset, from age 3 to age 20, varied among affected individuals. This difference inphenotypic expression might best be explained by degradation of mRNA from themutant allele through incomplete or aberrant splicing, resulting in a less severephe-notype. Indeed, in two families inwhich a reduction in the levels of mutant COL9A2
mRNAwas observed, affected individuals presented with normal height and wereclinically less severe than affected individuals in other families with normal levelsof COL9A2mRNA [17, 20].
Environmental or other genetic changes alsomay contribute to the phenotypicvariability of MED. As observed with type IX collagen gene mutations, there alsois significant intrafamilial and interfamilial variability in MED patients withCOMP mutations. The same genetic polymorphisms could modify the severity ofMED phenotypes regardless of whether the primary disease-causing mutation isin the COMP or type IX collagen genes.
There are numerous polymorphisms in the type IX collagengenes, withinbothexons and introns, which do not appear directly to cause MED (KLC and MDBunpublished results, J. Loughlin and L. Ala-Kokko, personal communications). How-ever, these nucleotide changes, which include point mutations and small deletions,might be predicted to alter mRNA processing and splicing. Alternatively, theymay result in the substitution of conserved residues that are important for the struc-ture and=or function of type IX collagen, such as coordinating binding to otherproteins of the ECM.
CELL MATRIX PATHOLOGY
Type IX collagen is made up of three separate gene products.Therefore, it fol-lows that amutation in only one of the three genes would cause a less deleterious ef-fect on heterotrimeric type IX collagen than observed with pentameric COMP.Atmost only half of the collagenmolecules would be expected to incorporate amu-tant a chain. However, if the mutant COL9A2mRNA is degraded, then a decreasein the amount of a1(IX) would lead to an overall reduction in the amount ofheterotrimeric type IX collagen, proportional to the amount of mutant COL9A2
Molecular Genetics ofMultiple Epiphyseal Dysplasia 65
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

mRNA degraded. Therefore, some patients exhibiting a mutation in the COL9A2
gene would be expected to have both abnormal type IX present compounded by adecrease in the total amount of type IX collagen in the ECM.
Action of Type IX Collagen Mutations
It has been suggested that COL9A2 and COL9A3 could exert their effect at themRNA level by altering the stability of themutantmRNA so that it is degraded re-sulting in haploinsufficiency for one of the three type IX collagen chains. AlteredstabilityofmRNAor incomplete skippingof exon3hasbeen reported intwo familieswithMEDandappears to dependonthe positionof themutation inthe splice donorand acceptor sites [20, 61]. Lack of a1(IX) leads to a complete absence of type IXcollagen heterotrimers in the mouse [62]. Therefore, it is probable that expressionof all three type IX collagen chains is necessary for assembly of type IX heterotri-mers. A decrease in the amount of mRNAof one a-chain subsequently may cause areduction in the overall amount of heterotrimeric type IX collagen in the ECM.
Deletion of COL3
Association of the three type IX collagena-chains andtheir subsequent trimer-ization occurs from the carboxy to amino terminal direction preceding the deletionin the COL3 domain. Therefore, exclusion of these 12 amino acid residues is notpredicted to influence folding of the majority of the type IX collagen molecule.Additionally, the interaction of type IX collagen with type II collagen also is notthought to be affected by this deletion because these covalent interactions occur inthe COL2 domain of type IX collagen [63, 64]. However, the COL3 and NC4 do-mains project from the collagen fibril surface into the cartilage extracellular matrixwhere they are accessible to interact with other matrix molecules, either structuralmolecules such as COMPor other proteins, for example, growth factors. A deletionof 12 amino acids within this domain may alter the conformation of the moleculeand then subsequently the ability of the NC4 domain to interact with moleculeswithin the ECM.
Alternatively, a dominant interference effect at the level of secretion wouldcause accumulation of mutant protein in the RER.Whether mutant type IX col-lagen is retained byMED chondrocytes remains uncertain. If the type IX collagenprotein is not secreted, then it would not effect fibril formation or interactions inthe extracellularmatrix, unless collagen fibrillogenesis was initiated intracellularly.A recent study showing that an a3(IX)COL3 deletion results in defective cross-linking of type IX collagen andaccumulation of materialwithin chondrocytes sug-gest thatmultiple steps of collagen synthesis andassembly are disturbedby the dele-tion in the a3(IX)COL3 domain [21]. In contrast, no abnormalities were detectedin extracellular fibrils or RER in chondrocytes from a patient with a mutation inthe type IX collagen a2 chain [65].
66 K. L. Chapman et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

MATRILIN-3 (EDM5)
Recently mutations in the A-domain of matrilin-3 have been shown to cause adistinctive mild MED phenotype [24, 66]. Two missense mutations (R121WandV194D) were identified in exon 2 of MATN3, which involve residues that are lo-cated within b-sheet regions of the A-domain (bB and bD, respectively), and thesesubstitutions are predicted to disrupt the structure and=or function of theA-domainofmatrilin-3 [24].To date, there are no datapertaining to the cell-matrixpathophy-siology of MED caused byMATN3mutations. Interestingly, the clinical expressiv-ity of MED caused by mutations in MATN3, which appears to primarily affectskeletal development rather than the long-term integrity of the articular cartilage[24, 66], mirrors the expression pattern ofMATN3 during joint development [67].
Matrilin-3 is the third member of a family of oligomeric multidomain ECMproteins comprising matrilin-1, -2, -3, and -4 [68^70].The domain structure of thematrilin family of proteins is similar, each consists of one or two vWFA domains, avarying number of EGF-like repeats, and a coiled-coil domain, which facilitatesoligomerization [71^73]. Matrilins have been found in collagen-dependent and-independent filament networks within the tissues that they are expressed andmay perform analogous functions in these different tissues [74, 75]. Furthermore,matrilin-3 can form heteroligomers with matrilin-1 [76, 77], implicating MATN1
as a candidate gene for phenotypes within the MED disease spectrum. Recently, acomprehensive analysis of a matn1 knock-out mouse failed to identify a detectablephenotype or ECM abnormality [78], highlighting the need to generate targetedknock-in mutations to studyMED disease pathways.
DIASTROPHIC DYSPLASIA SULPHATE TRANSPORTER (EDM4)
The only recessive forms ofMED (rMED) that have been confirmedby genet-ic analysis result from mutations in the gene-encoding diastrophic dysplasia sul-phate transporter (DTDST) protein (EDM4) [25]. This form of MED ischaracterized by joint pain and stiffness (usually in the hips and knees in child-hood) and deformities of the hands (mild brachydactyly), feet (clubfoot), and knees(double layered patella in 50% of patients). Usually there is only very mild shortstature in adulthood. DTDST mutations were originally described in the dia-strophic dysplasia group, which also includes achondrogenesis1B, and atelosteogen-esis type II. In all the cases of rMED caused by mutations in DTDST, affectedindividuals are homozygous for a R279Wsubstitution. R279Wis themost commonDTDST mutation, and yet individuals with the more severe diastrophic dysplasiaachondrogenesis 1B and atelosteogenesis type II phenotype are all compound het-erozygotes.This suggests that R279W is the mildest of the DTDSTmutations.
Analysis of the transmembrane protein, DTDST, has indicated that it is a Naþ-independent sulphate=chloride antiporter [79, 80]. The expression pattern ofDTDST was originally shown to be ubiquitous [79]-however, its increased
Molecular Genetics ofMultiple Epiphyseal Dysplasia 67
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

expression in cartilage and small intestine has now been demonstrated [80]. Theimportance of DTDST’s role in the sulphation of cartilagematrix proteins has beenconfirmed in cultured chondrocytes isolated from a patient with achondrogenesistype1B [81] inwhich a decrease in the expression ofDTDSTresults in a correspond-ing decrease in the level of sulfation.
Themajor proteoglycans in cartilage such as aggrecan are sulphated and this isessential for their function (reviewed in [82]). Similarly, type IX collagen has achondroitin sulphate GAG-side chain and therefore mutations in DTDST, whichresult in MED, may exhibit their effect through altering the sulfation pattern oftype IX collagen, thereby altering its function. This is the first mutation to be iden-tified in the MED=PSACH disease spectrum that does not occur in a structuralmacromolecule. It seems likely that the undersulfation of core proteoglycans in theECM could potentially alter their function, which in turn would alter the ultra-structure of cartilage leading to the MED phenotype.
CONCLUSIONS AND FUTURE PERSPECTIVES
MED is clinically and genetically heterogeneous and may be caused by muta-tions in a variety of cartilage ECM genes. The phenotypic similarity may be theresult of a common disease pathophysiology, such as a general disruption to chon-drocyte differentiation and maturation or reduced structural integrity of the car-tilage ECM, although the primary mechanism of initiation may differ betweenthe various MED phenotypes. Alternatively, genes, whose protein products eitherinteract within the ECM or act to modify other proteins in some way, may causethe spectrum of MED phenotypes. High-affinity binding of COMP to type IIcollagen and type IX collagen has recently been described, and DTDST is keyto the sulfation of many glycoproteins, including type IX collagen.The identifica-tion of further genes involved in the initiation of the multiple epiphyseal dyspla-sias will assist in unravelling the complex ECM architecture necessary forcartilage function.
Through extensive mutation screening and genetic linkage analysis, it is esti-mated that less than 50% of MED is caused by mutations in the COMP, type IXcollagen, matrilin-3, or DTDST genes. Future studies will likely concentrate onidentifying other genes and=or mutations that are involved in the initiation ofMED. In some families there is distinct intrafamilial variability, particularly ageof onset, suggesting that other genetic factors could modify the severity of theMED phenotype. Conservative and nonconservative amino acid substitutions inregions of type IX collagen known to bind COMPare postulated to have a pheno-typic effect by decreasing or abolishing these specific interactions. Confirming thatthese changes do in fact reduce or abolish binding will require extensive biochem-ical and biophysical investigation. In addition, intronic polymorphisms that arepredicted to alter gene expression and RNA splicing, thereby having an effect onmRNA stability, also have been found. The study of these DNAvariations within
68 K. L. Chapman et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

families will provide important insights into the howother genetic factors canmod-ify the severity of the MED phenotype.
Interestingly, but not surprisingly, some of the DNA variations identified inMED patients have been identified in apparently unaffected individuals. An inves-tigation into the capacityof these changes tomodify the severityof theMEDpheno-type may provide important insights into the pathogenetic mechanisms of morecommon conditions such as osteoarthritis [58], Perthes disease (osteochondritis),and vertebral disc diseases [83] and potentially identify predisposing alleles forthese diseases.
In some instances, specific phenotypic characteristics are related to certain gen-etic mutations [22], which ultimately assist in targeting a particular gene for muta-tion screening when molecular diagnosis is sought [3, 84]. The more mutationsthat are identified in a variety of different genes, the moremeaningful the genotypeto phenotype correlations will be.
The first mutations inMEDwere identified in1995, subsequently screening formutations in the type IX collagen and COMP genes over the past five years hasproved worthwhile. Overall, screening has helped to determine the true contribu-tion of these genes to MED and to predict important domains in these proteins[3]. It is likely that other MED-causing genes will be identified in the near future;their unearthing undoubtedly will pose more questions but ultimately will providefurther understanding of the complex interactions in the cartilage extracellularmatrix.
REFERENCES
1. FairbankT. Dysplasia epiphysialis multiplex. Proc R Soc Med (Ortho Sec) 1947;39:315^317.
2. Maudsley RH. Dysplasia epiphysialis multiplex. J Bone Joint Surg 1955;37B:228^240.
3. Briggs MD, Chapman KL. Pseudoachondroplasia and multiple epiphyseal dyspla-sia: Mutation review, molecular interactions, and genotype to phenotype correla-tions. HumMutat 2002;19:465^478.
4. Unger S, Hecht JT. Pseudoachondroplasia and multiple epiphyseal dysplasia: Newetiologic developments. AmJMed Genet 2001;106:244^250.
5. Rimoin DL, Lachman RS. Chondrodysplasias. In Rimoin DL, ConnorJM, PyeritzRE, eds. Emery and Rimoin’s Principles and Practice of Medical Genetics, Edin-burgh: Churchill Livingstone,1997;2779^2816.
6. Haga N, Nakamura K,Takikawa K, Manabe N, Ikegawa S, Kimizuka M. Statureand severity in multiple epiphyseal dysplasia. J Pediatr Orthop1998;18:394^397.
7. Treble NJ, Jensen FO, Bankier A, Rogers JG, ColeWG. Development of the hip inmultiple epiphyseal dysplasia. Natural history and susceptibility to premature os-teoarthritis. J BoneJoint Surg [Br] 1990;72:1061^1064.
8. Ingram RR. Early diagnosis of multiple epiphyseal dysplasia. J Pediatr Orthop1992;12:241^244.
Molecular Genetics ofMultiple Epiphyseal Dysplasia 69
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

9. YochumTR, Sprowl CG, Barry MS. Double patella syndrome with a form of multi-ple epiphyseal dysplasia. JManipulative PhysiolTher1995;18:407^410.
10. She⁄eld EG. Double-layered patella in multiple epiphyseal dysplasia: A valuableclue in the diagnosis. J Pediatr Orthop1998;18:123^128.
11. Hedbom E, Antonsson P, Hjerpe A, Aeschlimann D, PaulssonM, Rosa-Pimentel E,SommarinY,Wendel M, Oldberg A, Heinegard D. Cartilage matrix proteins. Anacidic oligomeric protein (COMP) detected only in cartilage. J Biol Chem1992;267:6132^6136.
12. Newton G, Weremowicz S, Morton CC, Copeland NG, Gilbert DJ, Jenkins NA,Lawler J. Characterization of human and mouse cartilage oligomeric matrix pro-tein. Genomics1994;24:435^439.
13. Briggs MD, Ho¡man SM, King LM, Olsen AS, Mohrenweiser H, Leroy JG,Mortier GR, Rimoin DL, Lachman RS, Gaines ES, et al. Pseudoachondroplasiaand multiple epiphyseal dysplasia due to mutations in the cartilage oligomeric ma-trix protein gene. Nat Genet 1995;10:330^336.
14. Hecht JT, Nelson LD, Crowder E,Wang Y, Elder FF, HarrisonWR, FrancomanoCA, Prange CK, Lennon GG, Deere M, et al. Mutations in exon 17B of cartilageoligomeric matrix protein (COMP) cause pseudoachondroplasia. Nat Genet1995;10: 325^329.
15. Rimoin DL, Rasmussen IM, Briggs MD, Roughley PJ, Gruber HE,Warman ML,Olsen BR, HsiaYE,YuenJ, Reinker K, et al. A large family with features of pseudo-achondroplasia and multiple epiphyseal dysplasia: Exclusion of seven candidategene loci that encode proteins of the cartilage extracellular matrix. Hum Genet1994;93:236^242.
16. Muragaki Y, Mariman EC, van Beersum SE, Perala M, van Mourik JB,WarmanML,Olsen BR,Hamel BC. Amutation in the gene encoding the alpha 2 chain of the¢bril-associated collagen IX, COL9A2, causes multiple epiphyseal dysplasia(EDM2). Nat Genet 1996;12:103^105.
17. Holden P, Canty EG,MortierGR,Zabel B, SprangerJ, CarrA,GrantME, LoughlinJA, Briggs MD. Identi¢cation of novel pro-alpha2(iX) collagen gene mutations intwo families with distinctive oligoepiphyseal forms of multiple epiphyseal dysplasia.AmJHum Genet 1999;65:31^38.
18. PaassiltaP,LohinivaJ,AnnunenS,BonaventureJ,LeMerrerM,PaiL,Ala-KokkoL.COL9A3: A third locus for multiple epiphyseal dysplasia. Am J Hum Genet1999;64:1036^1044.
19. Lohiniva J, Paassilta P, Seppanen U,Vierimaa O, Kivirikko S, Ala-Kokko L. Spli-cing mutations in the COL3 domain of collagen IX cause multiple epiphyseal dys-plasia. AmJMed Genet 2000;90:216^222.
20. Spayde EC, Joshi AP,WilcoxWR, Briggs M, Cohn DH, Olsen BR. Exon skippingmutation in the COL9A2 gene in a family with multiple epiphyseal dysplasia.Matrix Biol 2000;19:121^128.
21. Bonnemann CG, Cox GF, Shapiro F,Wu JJ, Feener CA, ThompsonTG, AnthonyDC, Eyre DR, Darras BT, Kunkel LM. A mutation in the alpha 3 chain of type IXcollagen causes autosomal dominant multiple epiphyseal dysplasia with mild myo-pathy. Proc Natl Acad Sci USA 2000;97:1212^1217.
70 K. L. Chapman et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

22. Unger SL, Briggs MD, Holden P, Zabel B, Ala-Kokko L, Paassilta P, Lohiniva J,RimoinDL, LachmanRS, CohnDH.Multiple epiphyseal dysplasia: Radiographicabnormalities correlated with genotype. Pediatr Radiol 2001;31:10^8.
23. Czarny-Ratajczak M, Lohiniva J, Rogala P, Kozlowski K, Perala M, Carter L,SpectorTD, Kolodziej L, Seppanen U, Glazar R, Krolewski J, Latos-Bielenska A,Ala-Kokko L. Amutation in COL9A1causes multiple epiphyseal eysplasia: Furtherevidence for locus heterogeneity. AmJHum Genet 2001;69:5.
24. Chapman KL, Mortier GR, Chapman K, Loughlin J, Grant ME, Briggs MD.Mutations in the region encoding the vonWillebrand factorA domain of matrilin-3are associated with multiple epiphyseal dysplasia. Nat Genet 2001;28:393^396.
25. Superti-Furga A, Neumann L, RiebelT, Eich G, Steinmann B, SprangerJ, KunzeJ.Recessivelyinheritedmultipleepiphysealdysplasiawithnormalstature,clubfoot,anddouble layeredpatellacausedbyaDTDSTmutation. JMedGenet1999;36:621^624.
26. Delot E, Brodie SG, King LM,WilcoxWR, Cohn DH. Physiological and patholo-gical secretion of cartilage oligomericmatrix proteinby cells in culture. J Biol Chem1998;273:26692^26697.
27. MalashkevichVN, Kammerer RA, E¢movVP, Schulthess T, Engel J. The crystalstructure of a ¢ve-stranded coiled coil in COMP: A prototype ion channel? Science1996;274:761^765.
28. Chen H, Deere M, Hecht JT, Lawler J. Cartilage oligomeric matrix protein is acalcium-binding protein, and amutation in its type 3 repeats causes conformationalchanges. J Biol Chem 2000;275:26538^26544.
29. Maddox BK,Mokashi A, Keene DR, Bachinger HP. A cartilage oligomeric matrixprotein mutation associated with pseudoachondroplasia changes the structural andfunctional properties of the type 3 domain. J Biol Chem 2000;275:11412^11417.
30. Rosenberg K, Olsson H, Morgelin M, Heinegard D. Cartilage oligomeric matrixprotein shows high a⁄nity zinc-dependent interaction with triple helical collagen.J Biol Chem1998;273:20397^20403.
31. Holden P, Meadows RS, Chapman KL, Grant ME, Kadler KE, Briggs MD. Car-tilage oligomeric matrix protein interacts with type IX collagen, and disruptions tothese interactions identify a pathogenetic mechanism in a bone dysplasia family.J Biol Chem 2001;276:6046^6055.
32. Thur J, Rosenberg K, Nitsche DP, Pihlajamaa T, Ala-Kokko L, Heinegard D,Paulsson M, Maurer P. Mutations in cartilage oligomeric matrix protein causingpseudoachondroplasia and multiple epiphyseal dysplasia a¡ect binding of calciumand collagen I, II, and IX. J Biol Chem 2001;276:6083^6092.
33. BalloR, BriggsMD,CohnDH,KnowltonRG, Beighton PH,RamesarRS.Multipleepiphyseal dysplasia, Ribbing type: A novel point mutation in the COMPgene in aSouth African family [published erratum appears in AmJ Med Genet 1997;7:494]AmJMed Genet 1997;68:396^400.
34. Susic S, McGrory J, Ahier J, ColeWG. Multiple epiphyseal dysplasia and pseudo-achondroplasia due to novel mutations in the calmodulin-like repeats of cartilageoligomeric matrix protein. Clin Genet 1997;51:219^224.
35. Loughlin J, Irven C, Mustafa Z, Briggs MD, Carr A, Lynch SA, Knowlton RG,Cohn DH, Sykes B. Identi¢cation of ¢ve novel mutations in cartilage oligomeric
Molecular Genetics ofMultiple Epiphyseal Dysplasia 71
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

matrix protein gene in pseudoachondroplasia and multiple epiphyseal dysplasia.HumMutat1998;Suppl: S10^7.
36. Ikegawa S, Ohashi H, Nishimura G, Kim KC, Sannohe A, Kimizuka M,FukushimaY, Nagai T, NakamuraY. Novel and recurrent COMP (cartilage oligo-meric matrix protein) mutations in pseudoachondroplasia and multiple epiphysealdysplasia. HumGenet1998;103:633^638.
37. BriggsMD,Mortier GR, ColeWG, King LM, Golik SS, BonaventureJ, Nuytinck L,De Paepe A, Leroy JG, Biesecker L, Lipson M,WilcoxWR, Lachman RS, RimoinDL, Knowlton RG, Cohn DH. Diverse mutations in the gene for cartilage oligo-meric matrix protein in the pseudoachondroplasia-multiple epiphyseal dysplasiadisease spectrum. AmJHumGenet1998;62:311^319.
38. Delot E, King LM, Briggs MD,WilcoxWR, Cohn DH. Trinucleotide expansionmutations in the cartilage oligomeric matrix protein (COMP) gene. Hum MolGenet1999;8:123^128.
39. Deere M, Sanford T, Francomano CA, Daniels K, Hecht JT. Identi¢cation of ninenovel mutations in cartilage oligomeric matrix protein in patients with pseudo-achondroplasiaandmultipleepiphysealdysplasia.AmJMedGenet1999;85:486^490.
40. Kleerekoper Q, HechtJT, PutkeyJA. Disease-causing mutations in cartilage oligo-meric matrix protein cause an unstructured Ca2þ binding domain. J Biol Chem2002;277:10581^10589.
41. Deere M, Sanford T, Ferguson HL, Daniels K, Hecht JT. Identi¢cation of twelvemutations in cartilage oligomeric matrix protein (COMP) in patients with pseudo-achondroplasia. AmJMed Genet1998;80:510^513.
42. Maynard JA, Cooper RR, Ponseti IV. A unique rough surfaced endoplasmic re-ticulum inclusion in pseudoachondroplasia. Lab Invest 1972;26:40^44.
43. Maddox BK, Keene DR, Sakai LY, Charbonneau NL, Morris NP, Ridgway CC,Boswell BA, Sussman MD, HortonWA, Bachinger HP, Hecht JT.The fate of carti-lage oligomeric matrix protein is determined by the cell type in the case of a novelmutation in pseudoachondroplasia. J Biol Chem1997;272:30993^30997.
44. Cohn DH, Briggs MD, King LM, Rimoin DL, Wilcox WR, Lachman RS,Knowlton RG.Mutations in the cartilage oligomeric matrix protein (COMP) genein pseudoachondroplasia and multiple epiphyseal dysplasia. Ann N Y Acad Sci1996;785:188^194.
45. Stanescu R, StanescuV, Muriel MP, Maroteaux P. Multiple epiphyseal dysplasia,Fairbank type: morphologic and biochemical study of cartilage. AmJ Med Genet1993;45:501^507.
46. Vertel BM, Velasco A, LaFrance S, Walters L, Kaczman-Daniel K. Precursors ofchondroitin sulfate proteoglycan are segregated within a subcompartment of thechondrocyte endoplasmic reticulum. JCell Biol1989;109:1827^1836.
47. HechtJT, Montufar-Solis D, Decker G, LawlerJ, Daniels K, Duke PJ. Retention ofcartilage oligomeric matrix protein (COMP) and cell death in redi¡erentiatedpseudoachondroplasia chondrocytes. Matrix Biol 1998;17:625^633.
48. Hecht JT, Deere M, Putnam E, ColeW,Vertel B, Chen H, Lawler J. Characteriza-tion of cartilage oligomeric matrix protein (COMP) in human normal and pseudo-achondroplasia musculoskeletal tissues. Matrix Biol 1998;17:269^278.
72 K. L. Chapman et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

49. Mayne R. Cartilage collagens.What is their function, and are they involved in ar-ticular disease? Arthritis Rheum1989;32:241^246.
50. Nishimura I, Muragaki Y, Olsen BR. Tissue-speci¢c forms of type IX collagen-proteoglycan arise from the use of two widely separated promoters. J Biol Chem1989;264:20033^20041.
51. Perala M, Savontaus M, Metsaranta M, Vuorio E. Developmental regulation ofmRNA species for types II, IX and XI collagens during mouse embryogenesis.BiochemJ1997;324:209^216.
52. Ring C, LemmonV, HalfterW.Two chondroitin sulfate proteoglycans di¡erentiallyexpressed in the developing chick visual system. Dev Biol 1995;168:11^27.
53. Ring C, HassellJ, HalfterW. Expression pattern of collagen IXand potential role inthe segmentation of the peripheral nervous system. Dev Biol 1996;180:41^53.
54. Swiderski RE, Solursh M. Localization of type II collagen, long form alpha 1(IX)collagen, and short form alpha 1(IX) collagen transcripts in the developing chicknotochord and axial skeleton. Dev Dyn1992;194:118^127.
55. Brewton RG,Wright DW, Mayne R. Structural and functional comparison of typeIX collagen-proteoglycan from chicken cartilage and vitreous humor. J Biol Chem1991;266:4752^4757.
56. Abe N,Yoshioka H, Inoue H, NinomiyaY. The complete primary structure of thelong form of mouse alpha 1(IX) collagen chain and its expression during limb de-velopment. Biochim Biophys Acta1994;1204:61^67.
57. Olsen BR. Collagen IX. IntJ Biochem Cell Biol 1997;29:555^558.58. Mustafa Z, ChapmanK, Irven C, CarrAJ, ClipshamK, ChitnavisJ, SinsheimerJS,
Bloom¢eld VA, McCartney M, Cox O, Sykes B, Loughlin J. Linkage analysis ofcandidate genes as susceptibility loci for osteoarthritis-suggestive linkage ofCOL9A1to female hip osteoarthritis. Rheumatology (Oxford) 2000;39:299^306.
59. Andersen PE Jr, Schantz K, Bollerslev J, Justesen P. Bilateral femoral head dys-plasia and osteochondritis. Multiple epiphyseal dysplasia tarda, spondylo-epiphyseal dysplasia tarda, and bilateral Legg-Perthes disease. Acta Radiol1988;29:705^709.
60. Versteylen RJ, Zwemmer A, Lorie CA, Schuur KH. Multiple epiphyseal dysplasiacomplicated by severe osteochondritis dissecans of the knee. Incidence in two fa-milies. Skeletal Radiol 1988;17:407^412.
61. Holden P, NewmanW, Jones CJP, Grant ME, Briggs MD. COMP gene mutationsresult in abnormal collagen ¢bril morphology. AmJHum Genet 1999;65:A301.
62. Hagg R, Hedbom E, Mollers U, Aszodi A, Fassler R, Bruckner P. Absence of thealpha1(IX) chain leads to a functional knock-out of the entire collagen IX proteinin mice. J Biol Chem1997;272:20650^20654.
63. WuJJ,Woods PE, Eyre DR. Identi¢cation of cross-linking sites in bovine cartilagetype IX collagen reveals an antiparallel type II-type IXmolecular relationship andtype IX to type IX bonding. J Biol Chem1992;267:23007^23014.
64. Diab M,Wu JJ, Eyre DR. Collagen type IX from human cartilage: A structuralpro¢le of intermolecular cross-linking sites. BiochemJ1996;314:327^332.
65. van MourikJB, Buma P,WilcoxWR. Electron microscopical study in multiple epi-physeal dysplasia type II. Ultrastruct Pathol1998;22:249^251.
Molecular Genetics ofMultiple Epiphyseal Dysplasia 73
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

66. MortierGR,ChapmanK, LeroyJL, BriggsMD.Clinical and radiographic featuresof multiple epiphyseal dysplasia not linked to the COMPor type IX collagen genes.EurJ Hum Genet 2001;9:606^612.
67. Segat D, Frie C, Nitsche PD, Klatt AR, Piecha D, Korpos E, Deak F,Wagener R,PaulssonM, Smyth N. Expression of matrilin-1, -2 and -3 in developingmouse limbsand heart. Matrix Biol 2000;19:649^655.
68. Wagener R, Kobbe B, Paulsson M. Primary structure of matrilin-3, a new memberof a family of extracellular matrix proteins related to cartilage matrix protein(matrilin-1) and vonWillebrand factor. FEBSLett 1997;413:129^134.
69. Deak F,Wagener R, Kiss I, PaulssonM.Thematrilins: A novel family of oligomericextracellular matrix proteins. Matrix Biol 1999;18:55^64.
70. Paulsson M, Piecha D, Segat D, Smyth N,Wagener R. The matrilins: A growingfamily of A-domain-containing proteins. Biochem SocTrans1999;27:824^826.
71. Belluoccio D, SchenkerT, Baici A,Trueb B. Characterization of human matrilin-3(MATN3). Genomics1998;53:391^394.
72. Klatt AR, Nitsche DP, Kobbe B, Macht M, Paulsson M,Wagener R. Molecularstructure, processing, and tissue distribution of matrilin-4. J Biol Chem2001;276:17267^17275.
73. Muratoglu S, Krysan K, Balazs M, Sheng H, Zakany R, Modis L, Kiss I, Deak F.Primary structure of human matrilin-2, chromosome location of the MATN2 geneand conservation of an AT-AC intron in matrilin genes. Cytogenet Cell Genet2000;90:323^327.
74. PiechaD,MuratogluS,MorgelinM,HauserN,StuderD,Kiss I,PaulssonM,DeakF.Matrilin-2, a large, oligomericmatrix protein, is expressedby a great variety of cellsand forms ¢brillar networks. J Biol Chem1999;274:13353^13361.
75. Chen Q, ZhangY, Johnson DM, Goetinck PF. Assembly of a novel cartilage matrixprotein ¢lamentous network: Molecular basis of di¡erential requirement of vonWillebrand factorA domains. Mol Biol Cell 1999;10:2149^2162.
76. Zhang Y, Chen Q. Changes of matrilin forms during endochondral ossi¢cation.Molecular basis of oligomeric assembly. J Biol Chem 2000;275:32628^32634.
77. WuJJ, Eyre DR. Matrilin-3 forms disul¢de-linked oligomers with matrilin-1 in bo-vine epiphyseal cartilage. J Biol Chem1998;273:17433^17438.
78. Aszodi A, Bateman JF, Hirsch E, Baranyi M, Hunziker EB, Hauser N, Bosze Z,Fassler R. Normal skeletal development of mice lacking matrilin 1: Redundantfunction of matrilins in cartilage? Mol Cell Biol 1999;19:7841^7845.
79. HastbackaJ, de la Chapelle A, Mahtani MM, Clines G, Reeve-Daly MP, Daly M,Hamilton BA, Kusumi K,Trivedi B,WeaverA, et al.The diastrophic dysplasia geneencodes a novel sulfate transporter: Positional cloning by ¢ne-structure linkagedisequilibriummapping. Cell 1994;78:1073^1087.
80. Satoh H, Susaki M, Shukunami C, Iyama K, NegoroT, HirakiY. Functional ana-lysis of diastrophic dysplasia sulfate transporter. Its involvement in growth regu-lation of chondrocytes mediated by sulfated proteoglycans. J Biol Chem 1998;273:12307^12315.
81. Rossi A, van der Harten HJ, Beemer FA, KleijerWJ, Gitzelmann R, Steinmann B,Superti-Furga A. Phenotypic and genotypic overlapbetween atelosteogenesis type 2and diastrophic dysplasia. Hum Genet1996;98:657^661.
74 K. L. Chapman et al.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.

82. Wallis GA. Cartilage disorders. The importance of being sulphated. Curr Biol1995;5:225^227.
83. Paassilta P, LohinivaJ, Goring HH, Perala M, Raina SS, KarppinenJ, Hakala M,PalmT, Kroger H, Kaitila I,Vanharanta H, OttJ, Ala-Kokko L. Identi¢cation of anovel common genetic risk factor for lumbar disk disease. JAMA 2001;285:1843^1849.
84. Newman B, Donnah D, Briggs MD. Molecular diagnosis is important to con¢rmsuspected pseudoachondroplasia. JMed Genet 2000;37:64^75.
Molecular Genetics ofMultiple Epiphyseal Dysplasia 75
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
0/26
/14
For
pers
onal
use
onl
y.