-
Hindawi Publishing CorporationEvidence-Based Complementary and
Alternative MedicineVolume 2013, Article ID 213407, 16
pageshttp://dx.doi.org/10.1155/2013/213407
Review ArticleTibetan Medicine: A Systematic Review of the
Clinical ResearchAvailable in the West
K. Philip Reuter, Thorolf E. R. Weißhuhn, and Claudia M.
Witt
Institute for Social Medicine, Epidemiology and Health
Economics, Charité-Universitätsmedizin, 10098 Berlin, Germany
Correspondence should be addressed to K. Philip Reuter;
[email protected]
Received 12 December 2012; Revised 17 February 2013; Accepted 18
February 2013
Academic Editor: Myeong Soo Lee
Copyright © 2013 K. Philip Reuter et al.This is an open access
article distributed under theCreative CommonsAttribution
License,which permits unrestricted use, distribution, and
reproduction in any medium, provided the original work is properly
cited.
Background. Little is known about Tibetan medicine (TM),
inWestern industrialized countries.Objectives. To provide a
systematicreview of the clinical studies on TM available in the
West. Data Sources. Seven literature databases, published
literature lists,citation tracking, and contacts to experts and
institutions. Study Eligibility Criteria. Studies in English,
German, French, or Spanishpresenting clinical trial results.
Participants. All patients of the included studies. Interventions.
Tibetan medicine treatment. StudyAppraisal and Synthesis Methods.
Included studies were described quantitatively; their quality was
assessed with the DIMDI HTAchecklist; for RCTs the Jadad score was
used. Results. 40 studies from 39 publications were included.They
were very heterogeneousregarding study type and size, treated
conditions, treatments, measured outcomes, and quality.
Limitations. No Russian, Tibetan,or Chinese publications were
included. Possible publication bias. Conclusions. The number of
clinical trials on TM available in theWest is small; methods and
results are heterogeneous. Implications of Key Findings. Higher
quality larger trials are needed, as is ageneral overview of
traditional usage to inform future clinical trials. Systematic
Review Registration Number. None.
1. Background
Traditional Tibetan medicine (TM), sometimes called“Lamaist” or
“Buddhist” medicine, has developed in 1200years into a unique
medical system [1–3]. In TM, disease isunderstood as an imbalance
of the three “Nyes-pa” (princi-ples) consisting of one or two
elements: “rLung” (air, wind),“mKhris-pa” (fire), and “Bad kann”
(earth and water) [4].Buddhist philosophy as well as shamanic
origins of Tibetanculture form a background of cosmological,
mind-body, andspiritual dimensions [1–3]. Treatment may consist of
medi-cines (usually preparations of plants [5], seldom minerals
oranimals), physical treatments (e.g., massage, baths), life
anddiet regulation, or spiritual techniques [4]. Standardizationof
the originally individualized medicines, separation fromthe
underlying philosophies, and discontinuation of sometechniques
(e.g., Tibetan dental medicine, cauterization)have led to
derivative forms of TM [6]. We will use theterm “Tibetan medicine”
for the traditional TM (with itsindividual life style advice, diet,
physical, and spiritualmeans) as well as larger or smaller subsets
or varieties of it,down to single formulas.
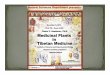
Besides the regions of the historical Tibet, very similarmedical
traditions are practised since the Mongolian con-quest of Tibet in
the 13th century in Mongolia, adjacentSiberia, and in the Russian
province Kalmykia (Figure 1)[7]. Especially with traditional
Mongolian medicine, TM hasa substantial similarity. TM use in
Western industrializedcountries (the “West”) originates in a line
of descendants ofa Buryat physician migrating westward in the 19th
century(Figure 1) [8, 9]. Still, there is little awareness of TM
inthe general Western public. Following the rising interest
intraditional Chinese medicine (TCM) and complementaryor
alternative medicine (CAM) in general, more demandfrom Western
countries can be expected in the future. Theamount of available
research in the West is small. A Medlinesearch up to December 31,
2010, for example, for “Tibetanmedicine” returned 371 hits, 0.0183
times the number for “tra-ditional Chinese medicine.”The existing
literature indicates apalliative, possibly curative potential,
especially for chronicdiseases [10], but studies on its multimodal
individualizedapproach are scarce and systematic reviews exist only
for oneTM product [11–15]. Therefore, we attempted to present
inthis paper a systematic overview of clinical research
currently
-
2 Evidence-Based Complementary and Alternative Medicine
TM core regions todayChina: Tibet autonomous regionand partly
Qinghai, Sichuan,Yunnan and GansuIndia: LadakhNepal: MustangIndia:
SikkimBhutanMongoliaRussia: BuryatiaRussia: Kalmykia
Regions where TM is practicedregularlyRussia:TuvaUst-Ordynski
BuryatAgin BuryatChita OblastAmur OblastKhabarovsk KraiChina:Inner
Mongolia autonomousregion
(8th–11th century)TM expansion after Mongolianconquest of Tibet
(13th century)Spread of Mongolian culture
Asian TM Schools today. North to South: Ulan-Ude, Ulaanbaatar,
Xining, Leh, Dharamsala, Lhasa, Thimphu, Darjeeling, and
Sarnath
(17th-18th century)
Badmaev family members (19th-20th century)
12
3
4 5
6
7
8
ab
cd
ef
g
II
I
II
IIIIII
III
(1)
(2)(3)(4)(5)(6)(7)(8)
(a)(b)(c)(d)(e)(f)
(g)
(I)
(II)
(III)
TM core regions todayChina: Tibet autonomous regionand partly
Qinghai, Sichuan,Yunnan and GansuIndia: LadakhNepal: MustangIndia:
SikkimBhutanMongoliaRussia: BuryatiaRussia: Kalmykia
Regions where TM is practicedregularlyRussia:TuvaUst-Ordynski
BuryatAgin BuryatChita OblastAmur OblastKhabarovsk KraiChina:Inner
Mongolia autonomousregion
(8th–11th century)TM expansion after Mongolianconquest of Tibet
(13th century)Spread of Mongolian culture
Asian TM Schools today. North to South: Ulan-Ude, Ulaanbaatar,
Xining, Leh, Dharamsala, Lhasa, Thimphu,
(17th-18th century)
Badmaev family members (19th-20th century)
12
3
4 5555
6
7
8
abbbbbbbbbbbbb
cccccccddddddd
ef
g
II
I
II
IIIIIIIIIIIIIIIIIIIIIIIIII
IIIIIIIIIIII
(1)
(2)(3)(4)(5)(6)(7)(8)
(a)(b)(c)(d)(e)(f)
(g)
(I)
(II)
(III)
Historical development:Main cultural influences on TM
Figure 1: Tibetan medicine in geography and history. Map based
on [7, 8, 17–22].
available in theWest onTibetanmedicine, and aim to
providedetails on methods and study quality. Some preliminary
datacan be found in [16].
2. Methods
A preliminary list of 15 literature databases was tested
usingthe search terms “Tibetan medicine,” “Himalaya
medicine,”“Tibetan herbal,” and “Lamaistic medicine.” The
databaselist had been compiled from recommendations by experts,by
Ovid [23], and by Deutsches Institut für Medizinis-che
Dokumentation und Information (DIMDI) [24]. Thosereturning the most
hits were used for the literature search,together with databases
that were recommended by expertsor appeared relevant in their
characterization on the websitesof DIMDI or the Charité library
[25]. We finally searchedseven databases up to publication date
December 31, 2010:ABIM (accessed via Rijksuniversiteit Groningen),
AMED(DIMDI), CAMbase (cambase), CCmed (DIMDI),
CochraneCollaborative Library (OVID), Embase (OVID),
andMedline(PubMed). The search term “(Tibet OR Himalaya OR
Mon-golia OR Buddhist) AND (herbal ORmedicine) AND study”
was adapted as necessary to database language and syntax.Similar
searches were used on the medical informationservices of DIMDI [24]
and ZB MED [26] and by adding“AND clinical study” on Google scholar
[27]. The publishedliterature lists [28, 29]were screened.We also
contacted Euro-pean experts, research departments of TM medical
faculties(Mentsekhang) in Lhasa and Dharamsala, and Europeancentres
for TM [30–32]. All identified literature was furtherscreened for
relevant citations. Duplicate references wereeliminated throughout
the process; of multiple publicationsof a study the most recent one
was included. Included papershad to be written in English, German,
French, or Spanish andhad to present clinical trial results on a
clinical outcome. Nofurther restrictions were applied.
One of the authors (K. P. Reuter) used a predefined formto
extract descriptive study data intoMS Access 2003 andMSExcel 2003
[33, 34] data bases, including bibliographic data,and study
parameters such as type, methods (including diag-nostics,
randomization, and blinding), and patient numbers.Furthermore, data
regarding treated diseases, interventions,outcomes, and types of
outcome measures (clinical symp-toms, tests, and laboratory
parameters) were extracted. If no
-
Evidence-Based Complementary and Alternative Medicine 3
Additionally from other sources(unique) 𝑛 = 398
Returns from 7 indexes𝑛 = 1488
Unique records𝑛 = 985
Screened records total𝑛 = 1383
Language (DE, EN, FR, SP)𝑛 = 1179
Topic (Tibetan medicine)𝑛 = 159
Method (clinical study)𝑛 = 40
Included publications𝑛 = 39
Included studies𝑛 = 40
Figure 2: The literature search. References from indexing
serviceswere collected first, then other sources were added.
primary outcome was defined, the first outcome mentionedin the
title or the abstract was extracted, unclear cases werediscussed
with another author (C. M. Witt) until consensuswas reached.
Methodological quality of the studies was determinedwith a DIMDI
checklist (Table 1) that is used to evaluatestudies for
in-/exclusion in health technology assessments(HTA) in Germany
[35]. The checklist has up to 31 itemssorted into 7 categories and
was used on a descriptive basis.Randomized controlled trials (RCTs)
were further evaluatedwith the Jadad score [36, 37]. Descriptive
statistics werecalculated using MS Access 2003 andMS Excel 2003
[33, 34].
3. Results
From 1383 screened records, we identified 40 studies reportedin
39 publications (one contains 2 studies [38]), see Figure 2.An
additional search without the terms “herbal,” “Buddhist,”and
“Mongolian” did not result in fewer relevant
publications.Thirty-five of the publications were journal articles,
twowere book chapters, and one is treated in this paper as asingle
Internet publication, although different findings hadbeen published
in several online media reports [39]. Only18 publications were
found by the initial data base searches.Most of the others were
indeed indexed, as a reverse search(for already known publications)
revealed.Written in Englishwere 53.8% (𝑛 = 21) of the publications,
the other 46.2% (18)were in German. Most publications came from
Poland andSwitzerland (30.8% or 𝑛 = 12 each, all on products of
PadmaAG). The Asian studies were from India (15.4%, 𝑛 = 6) orChina
(5.1%, 𝑛 = 2).The earliest publication appeared in 1970.Since 1990
every 5 years about 3 new RCTs were publishedand, less evenly
distributed, most of the observational studies
(total 𝑛 = 14). The 5 nonrandomized controlled trials
werepublished between 1986 and 1991, and the 6 case studies orcase
series in 1998 or later (Table 2). The setting of 7 studies(17.5%)
was multicentred [40–46]. Four studies (10.0%) wereretrospective
[40, 45, 47, 48].
In the RCTs included were 2028 patients, 1020 of themreceived
the Tibetan medicine treatment. Study durationranged from 14 days
to 12 months (mean = 114 days). MostRCTs investigated Padma 28 (𝑛 =
9) (the first study in[38], and [49–56]) or Padma Lax (𝑛 = 1) [57].
A wholemedical system approach with a complex traditional
TMintervention was applied in 3 studies on diabetes mellitus[43],
arthritis, [58] or hepatitis B [59]. Tibetan yoga inlymphoma
patients [60] and a single TM preparation (ZhiByed 11) for
postpartum haemorrhage [44] were each thesubject of 1 RCT. One
study [61] was declared an RCT butlacked randomization.
From those publications including herbalmedicines, fourdid not
provide details on the used medication [42, 58, 59,62], two
provided the name of the preparations but notthe ingredients [43,
48], and two provided the name ofthe preparation and ingredients,
but no information on thequantity of the ingredients [44, 63]. Data
on both ingredientsand their quantitywas only available for Padma
28 andPadmaLax.
The duration of the non-randomized controlled trials wasbetween
6 weeks and 6months (mean = 43 d), 54% of the 678patients received
the verumPadma 28. Four non-randomizedcontrolled trials included
children with chronic respiratorytract infections [46, 64, 65] or
juvenile arthritis [66]. One trialon adults included angina
pectoris patients [61].
In the observational studies included, there were 1824patients.
The observation duration ranged from 15 days to 2years (mean= 217
days). In someof the publications, the studyduration was not
clearly stated (the second study in [38],and [41]) or varied
between participants [42, 45, 63]. Sevenobservational studies
investigated Padma 28 (the secondstudy in [38], and [47, 67–71]).
One study each investigatedPadma Lax [41] or a jewel pill (Byu-Dmar
13) [63]. ComplexTM treatment was applied in 5 studies [39, 42, 45,
48, 62].
Theduration of the case studies/series rangedwidely fromseveral
days to 13.5 years [40]. Padma 28 was investigated in4 case studies
[40, 72–74], Padma Lax in 1 [75], and complexTM in another
[76].
All studies included a total of 4684 patients, ranging from1 to
967 per trial (mean = 117, SD = 187). Ten studies didnot state the
patients’ sex (𝑛 = 1648, 35.2% of all patientsin the present
review) [40–42, 47, 56, 63, 65, 67, 71, 77].From the other studies,
1080 patients (23.1%) were male and1956 (41.8%) female. Data on age
was available in 31 of 39studies. Children (age 10 months to 16
years, 𝑛 = 955) onlywere included in 5 studies [46, 64, 65, 70,
71]. Only 2 studiesreported on ethnicity (Tibetan patients in both)
[42, 58]. In 32studies, dropouts were reported ranging from 0% (15
studies)to 53% [45] with a mean dropout rate of 15%. In 21 of the
28trials of Padma 28 or Padma Lax, the mean drop out rate
was6%.
The checklist results for quality assessment are presentedat
item level in Table 3 for each study. Depending on study
-
4 Evidence-Based Complementary and Alternative Medicine
Table 1: DIMDI HTA checklist items.
Item∗ Item no. (label)∗∗
(A) Selection of participants Participants(1) Were the criteria
for in-/exclusion defined sufficiently and clearly? A1
(in-/exclusion)(2) Were the criteria for in-/exclusion defined
before intervention? A2 (predefined)(3) Was the health status
recorded in a valid and reliable way? A3 (health status)(4) Were
the diagnostic criteria of the disease described? A4 (diagnostic
criteria)(5) Were the studied/exposed patients representative for
the majority of the exposed population or the “standardusers” of
the intervention? A5 (representativity)
(B) Allocation and study participation Allocation(1) Were the
exposed/cases and nonexposed/controls from the same base
population? B1 (basic population)(2) Were intervention/exposed and
control/nonexposed groups comparable at baseline? B2
(comparable)(3) Was allocation randomized, with a standardized
procedure? B3 (randomization)
(4) Was randomization blinded? B4 (blindedrandomization)(5) Were
known/possible confounders considered at baseline? B5
(confounders)(C) Intervention/exposition Intervention(1) Were
intervention or exposition recorded in a valid, reliable, and
similar way? C1 (recording)(2) Apart from intervention, were
intervention and control groups treated similarly? C2 (similar
treatment)(3) In case of other treatments, were they recorded in a
valid and reliable way? C3 (other treatments)(4) For RCTs: were
placebos used for the control group? C4 (placebo use)
(5) For RCTs: was the way of placebo administration documented?
C5 (placebodocumented)(D) Study administration Administration(1)
Are there indications for “overmatching”? D1 (overmatching)(2) In
multicentre studies: were the diagnostic and therapeutic methods
and the outcome recording in the centresidentical? D2
(multicentre)
(3) Was if assured that participants did not crossover between
intervention and control group? D3 (no crossover)(E) Outcome
recording Outcome(1) Were patient-centred outcome parameters used?
E1 (patient-centred)(2) Were the outcomes recorded in a valid and
reliable way? E2 (recording)(3) Was outcome recording blinded? E3
(blinded outcomes)(4) For case series: was the distribution of
prognostic factors recorded sufficiently? E4 (prognostic
factors)(F) Drop-outs Drop-outs(1) Was the response rate in
intervention/control group sufficient, or, for cohort studies,
could a sufficient part ofthe cohort be tracked for the full study
duration? F1 (evaluable number)
(2) Were the reasons for the dropouts of participants stated? F2
(reasons)(3) Were the outcomes of dropouts described and included
in the analysis? F3 (outcomes)(4) If differences were found: were
they significant? F4 (significance)(5) If differences were found:
were they relevant? F5 (relevance)(G) Statistical analysis
Statistics(1) Were the described analytic methods correct and the
information sufficient for a flawless analysis? G1 (correct)(2)
Were confidence intervals given for means and for significance
tests? G2 (CIs given)(3) Were the results presented in graphical
form, and were the underlying values stated? G3
(graphics)∗Translated from [35], ∗∗used in Table 3.
type and setting, 10 to 26 items could be answered. Had
theassessment been for HTA purposes, only 1 case study [76]and 1
RCT [55] would have been eligible for inclusion in aHTA. Ignoring
only one item (G2, provision of confidenceintervals) would have
raised that number to 13, including 8
RCTs that the Jadad score rated as good or very good quality.The
Jadad score of the 15 RCTs (Table 4) reached a mean± SD of 3.40 ±
1.35 (median = 4). Randomization scored1.40 ± 0.51 (median = 1),
blinding 1.20 ± 1.01 (median =2), and drop-out reporting 0.80 ±
0.41 (median = 1). Studies
-
Evidence-Based Complementary and Alternative Medicine 5Ta
ble2:Inclu
dedstu
dies.
Stud
yTy
pe∗
Cou
ntry
Dise
ase(diagno
stic
syste
m)∗∗
Participants
(meanage),
drop
-outs∗∗∗
Durationof
interventio
nor
study
kind
,doseo
fintervention∗∗∗∗
(1)M
ainou
tcom
e(2)O
ther
outcom
esNotes
Ascho
ffetal.1997
OS
Germany
Migraine(BM
)I:22;D
:06mon
ths(andlonger?)
Byu-Dmar
13jewelpill,1U
/d
(1)S
everity
ofattacksreduced
by82%
(2)F
requ
ency
ofattacksu
nchanged;lessu
seof
analgesic
sinmostp
artic
ipants
Very
briefd
ocum
entatio
n;on
lysubjectiv
eoutcomes
Bommeli
etal.2001
rCS(M
C)Sw
itzerland
Vario
us(78%
patie
nts
w/arteriosclerosis
)(BM,T
M)
I:147;D:18
From
fewdays
to13.5years
P28,varyingdo
ses(∼50%of
patie
nts3×
2U/d)
(1)Improvem
ento
fcom
plaintsin%of
patie
nts:
perip
heralarteryocclu
sived
iseasein94%,
coronary
heartd
iseasein92%,chron
icveno
usinsufficiency
in91%,arthrosisin
80%
Patie
ntsfrom
15ph
ysicians,
nodemograph
ics,no
mon
otherapy,successno
tcle
arlyattributableto
P28
Brun
ner-La
Roccae
tal.2005
RCT(5)
Switzerland
Mild
hypercho
leste
ro-
laem
ia(BM)
I:30;C
:30;
D:0
4weeks
+15dfollo
wup
I:P2
8,3×2U
/dC:
potato
starch
(1)T
otalcholesterolu
nchanged
(2)O
ther
bloo
dlip
idsu
nchanged
Participantsno
ttypical
patie
nts
Brzoskoetal.1991
CT(4
arms)
Poland
Chronicjuvenile
arthritis(BM)
I1:12(11
years);I2:7;
C1:10
(health
y);C
2:10
(inremission)
I1:6
weeks;I2:4weeks
I1:P
28,2–4
U/d
I2:Th
ymus
extract,1sup
positorium/day
(1)Joint
pain
andsw
ellin
g(RitchieInd
ex):
improved
in75%–83%
ofP2
8patie
nts,in
86%of
thym
usextractp
atients
(2)Improvem
ent(comparedto
healthycontrol)of
sedimentatio
nrate,IgG
,IgM
,serom
ucoid,
CD8-Lymph
ocytes,C
D4/CD
8-qu
otient
Con
trolisn
osta
ndard
therapy;comparis
onwith
healthyprob
ands;
immun
ologicalparameters
notveryrelevant
for
contem
porary
diagno
stics
Brzoskoand
Jank
owski1992
OS(M
C)Po
land
HepatitisB
(BM)
I:178
inclu
ding
52child
ren
2years(interventio
n),10years(stu
dy)
I:P2
8,3×2U
/d
(1)“Biochemicalmarkers”(no
tspecified)
improved
in∼90%
(2)Improvem
entsin
Tlymph
ocytes
(CD3,CD
4,CD
8,andCD
4/CD
8)in
90%,hepatocellularv
irus
elim
inated
in15%,improvem
entsin
immun
ohistochemistry
(HBe
-Akincrease
in70%),andclinicalfi
ndings
(in90%)
Very
briefd
escriptio
nof
patie
ntsa
ndou
tcom
es;n
ostatem
entabo
utother
therapies
Changbar
1998
CS India
Chronica
plastic
anaemia(BM,T
M)
I:1m
an(63);
D:0
15mon
ths
Rinchenyusnying
25special,1o
nalternatingdays;Z
hiru,2×on
alternating
days;G
urgu
m8special,4×/d;Se‘bruku
nbd
e,3×
/d;A
gar8
,4×/d;dietary
recommendatio
ns
(1)H
aemoglobin(in
crease
from
3.1to10.4mg/dL
)(2)C
linicalim
provem
ent,redu
ctionof
comedication
Coh
enetal.200
4RC
T(2)
USA
Mentalsym
ptom
saccompanying
lymph
omas
(BM)
I:19;C
:19;D:
9
7weeks
+3mon
thsfollow-up
7weeklysessions
ofguided
yoga
(Tsa
lung
trul
khor
yoga)
(1)S
leep
disorder
improved
(2)D
espair,
anxiety,depressio
n,fatig
ueno
tsig
nificant,patie
nt’sappraisalp
ositive
Manyou
tcom
esin
small
popu
latio
nincreased
prob
abilityof
significant
results
caused
byrand
omvaria
tions;highdrop
-out
rate;low
compliance
Feldhaus
2004
CS Switzerland
Perip
heralarterial
occlu
sived
isease
(BM,unspecified
CAM)
I:1w
oman
(61);D
:0
1year
P28,3×2U
/d;intestin
alcle
ansin
g(in
testinalhydrotherapy
andmicrobacterial
treatment),
chelationtherapy,oxygenation
therapy,orthom
olecular
treatment,IV
treatmentw
ithrib
onucleicacid
(1)G
eneralcond
ition
muchim
proved
after
8mon
ths
(2)W
alking
distance
improved
(<100m
to>2000
m)
Noattributionof
effectto
TMpo
ssible
-
6 Evidence-Based Complementary and Alternative Medicine
Table2:Con
tinued.
Stud
yTy
pe∗
Cou
ntry
Dise
ase(diagno
stic
syste
m)∗∗
Participants
(meanage),
drop
-outs∗∗∗
Durationof
interventio
nor
study
kind
,doseo
fintervention∗∗∗∗
(1)M
ainou
tcom
e(2)O
ther
outcom
esNotes
Feldhaus
2006
CS Switzerland
Chronicc
onstipatio
nof
tetraplegicp
atients
(BM,unspecified
CAM)
I:3;D:0
1–3mon
ths
I:PL
,1×1-2
U/d;
intestinalcle
ansin
g(in
testinal
hydrotherapy
andmicro
bacterial
treatment),
chelationtherapy,otherC
AM
(1)C
onstipatio
ncuredin
allcases
Noattributionof
effectto
TMpo
ssible
FlückandBu
bb1970
OS(M
C)Sw
itzerland
Chronicc
onstipatio
n(BM)
I:285(256
outpatients,
29inpatie
nts)
“Several”
weeks
PL,1×1U
/d(1)S
ymptom
simproved
in82%
(2)U
nwantedeffectsin
6.3%
Insufficientd
escriptio
nof
popu
latio
n,inclu
sion
criteria
,and
diagno
stics
Füllemann2006
OS
Switzerland
Chronicd
ental
pulpitis(BM
)I:53;D
:415
days
P28,2×2U
/d
(1)P
ain-fre
ewith
in1m
onth
in55%
(2)E
xtractionor
root
canaltreatmentn
otnecessaryin
82%
Com
paris
onwith
expectationfro
mexperie
nce;4drop
-outs
becauseo
fincom
pliance
might
have
caused
false
positiver
esult
Gladysz
etal.1993
OS
Poland
HepatitisB
(BM)
I:34
12mon
ths
P28,3×2U
/d
(1)S
erologicalandliver
functio
nparameters
improved
in76.5%,liver
biop
syim
proved
in55.9%
(2)O
ther
parameters(GGT,GPT
,bilirubin,
and
albu
min)u
nchanged
Authorsc
laim
elim
ination
potentialfor
HBe
Agand
HBV
-DNAsim
ilarto
interfe
ronstandard
therapy;un
wantedeffects
notstated
Gün
sche
2005
CS Switzerland
Bipo
larD
isorder
(BM)
I:1w
oman
(44);D
:011mon
ths
P28,3×2U
/dfor6
weeks,then3×1/d
(1)a
nd(2)D
aytim
esleepiness,concentration
difficulties,and
apathy
muchim
proved
with
in6
weeks,cured
after
11mon
ths
Onlysubjectiv
eoutcomes
Hürlim
ann1979/1
RCT(3)
Switzerland
Perip
heralarterial
occlu
sived
isease
(BM)
I:13;C
:11;D:
0
12weeks
I:P2
8,3×2U
/dC:
Placebo
(1)P
ainfre
ewalking
distance
improved
by54%
(2)O
ther
symptom
simproved
in69%,n
ochange
inplethysm
ograph
y
Goo
dstu
dydesig
n,ho
mogenou
sgroup
s,very
briefp
resentationof
results,
valid
results
Hürlim
ann1979/2
OS
Switzerland
Perip
heralarterial
occlu
sived
isease
(BM)
I:10;D
:0Durationno
tstated
P28,3×2U
/d.
(1)R
estp
ainim
proved
in70%
Very
briefp
resentation,
duratio
nno
tstated
Jank
owskietal.1986
OS
Poland
Recurrentrespiratory
tractinfectio
ns(BM)
I:61
(2years);
D:0
8weeks
P28,3×1U
/dor
3×0.5U
/ddepend
ingon
age,4weeks
P28—
2weeks
pause—
2weeks
P28
(1)F
requ
ency
andintensity
ofinfections
redu
ced
in80%
(2)Immun
oglobu
linsa
ndBcells
unchanged,T
cells
norm
alized,phagocytic
activ
ityof
leucocytes
increased,appetiteincreased
Immun
ologicalanalysisdid
notinclude
allp
articipants
Jank
owskietal.1991
CT Poland
Recurrentrespiratory
tractinfectio
ns(BM)
I:19;C
:10
(health
y);(3
years);D
:0
8weeks
P28,3×1U
/d,4
weeks
P28—
2weeks
pause—
2weeks
P28
(1)B
acteric
ideind
ex(“spon
taneou
sbacteric
idal
activ
ity”)im
proved
in84%
Effectn
otcle
arly
attributablebecauseo
fhealthycontrols;
teste
dbacteriano
ttypicalfor
disease;un
usualoutcome
parameter
-
Evidence-Based Complementary and Alternative Medicine 7
Table2:Con
tinued.
Stud
yTy
pe∗
Cou
ntry
Dise
ase(diagno
stic
syste
m)∗∗
Participants
(meanage),
drop
-outs∗∗∗
Durationof
interventio
nor
study
kind
,doseo
fintervention∗∗∗∗
(1)M
ainou
tcom
e(2)O
ther
outcom
esNotes
Jank
owskietal.1992
OS
Poland
Recurrentrespiratory
tractinfectio
ns(BM)
I:305(4
years)
10weeks
P28,3×1U
P28or
3×0.5U
depend
ingon
age
(1)F
requ
ency
andintensity
ofinfections
redu
ced
in72%
(2)IncreaseinCD
2+,C
D4+
lymph
ocytes,and
CD4/CD
8qu
otient
Possiblyrepu
blish
eddata
from
earlier
studies;
immun
ologicalresults
from
48participantson
ly(rando
mized?)
Korw
in-Piotro
wska
etal.
1992
RCT(2)
Poland
Multip
leSclerosis
(BM)
I:50;C
:50;
D:0
12mon
ths
I:P2
8,3×2U
/dC:
Placebo,symptom
atictre
atment
(1)C
linicalcourse
(relapse
frequ
ency
orprogression)
improved
in44
%(2)E
vokedpo
tentials:
visualim
proved
in33%,
acou
sticu
nchang
ed
Other
treatmentinplacebo
grou
p
Leem
anetal.2001
OS
USA
Breastcancer
(BM,
TM)
I:11;D
I:2
1year
2–4herbalpreparations,2–6×/d;diet,
lifestyleregulation,
prayer;every
3–4
mon
thsa
djustm
ento
fprescrip
tion
(1)N
oun
wantedeffectsgradeIIIor
IV(2)1
patie
nt’stumor
regressed,2weres
tablefor
>12
mon
ths,6progressed
Nopeer-reviewed
publication;
nostatem
ents
abou
tdrop-ou
t’sou
tcom
es(possib
lydiseasep
rogress)
Li2001
OS(M
C)Lh
asaP
refecture,
China
Helicobacter
pylori
associated
gastr
itis
(BM,T
M)
I:86
Max.8
weeks,follow-upof
24patie
ntsa
fter
5mon
ths
TM,m
ax.8
weeks
(1)H
elicobacter
testno
tchanged
(2)C
linicalparametersimproved
in76.3%–100%
(depending
oncategory),symptom
intensity
improved
Therapyaccordingto
Tibetandiagno
sticsin9
“medicationgrou
ps”;
selectionof
follo
wup
grou
pno
tstated
Mansfe
ld1988
CT Switzerland
Recurrentrespiratory
tractinfectio
ns(BM)
I:218;C:
205;
(11y
ears);D:
3
6weeks,thenob
servationfor6
–12mon
ths
I:P2
8,3×
1U/d,biomedicinew
henneeded,
mou
ntainairc
ure
C:biom
edicinew
henneeded,m
ountainair
cure
(1)F
requ
ency
andseverityof
infections
tend
edto
improve(no
tsignificant)
(2)Immun
oglobu
lines
andinflammation
parametersn
otsig
nificant
Parentsa
ssessedinfection
severity;othertherapies
might
have
maskedP2
8effect
Mehlse
netal.1995
RCT(5)
Denmark
Perip
heralarterial
occlu
sived
isease
I:20;C
:20;
D:4
4mon
ths
I:P2
8,2×2U
/dC:
gelatine
(1)M
ax.w
alking
distance
improved
(2)P
ain-fre
ewalking
distance
improved,n
ochange
inbloo
dpressure
andbloo
dpressure
ratio
ankle/up
pera
rm
Excellent
study
desig
n
Miller
etal.200
9RC
T(5)(MC)
LhasaP
refecture,
China
Post-
partum
haem
orrhage(BM
,TM
)
I:480;C:
487;
D:7
Sing
ledo
seI:Zh
iByed11,
3U,and
placebo
C:Miso
prostol,60
0𝜇g,andplacebo
(1)M
isoprostolsup
eriortoZh
iByed11for:
Hem
orrhage,maternaldeath,needforu
terotonics
(2)N
osig
nificantd
ifference
form
eanandmedian
bloo
dloss
Nam
duletal.2001
RCT(1)(MC)
India
Type
2Diabetes(BM
,TM
)
I:100;C:
100;
D:88(64
after
12weeks)
24weeks
I:Ky
ura-6,Aru-18,Yu
ng-4,and
Sugm
el-19,
daily
+lifes
tyleregu
latio
n+dietaccording
toAmerican
DiabetesA
ssociatio
nC:
lifes
tyleregulation+dietas
above
(1)F
astin
gbloo
dglucoser
educed
(2)P
ostprand
ialblood
glucosea
ndHbA
1credu
ced,we
ight,blood
pressure,and
bloo
dlip
ids
unchanged
Interventio
ngrou
pmoreill
despite
rand
omization;
values
ofinterventio
ngrou
ptakenas
baselin
e;high
drop
-out
ratewith
out
furthera
nalyses
-
8 Evidence-Based Complementary and Alternative Medicine
Table2:Con
tinued.
Stud
yTy
pe∗
Cou
ntry
Dise
ase(diagno
stic
syste
m)∗∗
Participants
(meanage),
drop
-outs∗∗∗
Durationof
interventio
nor
study
kind
,doseo
fintervention∗∗∗∗
(1)M
ainou
tcom
e(2)O
ther
outcom
esNotes
Neshar2
000
OS
India
Diabetesm
ellitus
(BM,T
M)
I:82;D
:0(study
ofpatie
ntfiles)
Min.6
mon
ths
Yung
-4,K
yuru-6,C
hinn
i-Aru-18,and
Sugm
el-10,daily
+lifestyleanddiet
regu
latio
n
(1)B
lood
glucoseimproved
in70%,stabilized
in100%
(2)Improvem
entsin
subjectiv
esym
ptom
s(92%),
andneed
forb
iomedicinein68%
Regardinggeneral
improvem
ent
discrim
inationbetween
TMalon
eorw
ithadditio
nalbiomedicine:itis
notclear
whether
biom
edicinew
asgivenat
baselin
eorb
ecam
enecessarydu
ringstu
dy;
mostd
atar
efer
toa
subp
opulationof
24thatis
notd
escribed:selectio
nbias?
Neshar2
007
OS
India(
MC)
Cancer
(BM,T
M)
I:647;D:340
Varyingdu
ratio
nTradition
alTM
(not
furtherspecified)
(1)G
eneralhealth
statemuchim
proved
(2)Improvem
entsin
progression,
infections,pain,
sidee
ffectso
fchemotherapy
andradiationtherapy
Selectionof
patie
ntsn
otrepresentativ
e,high
drop
-out
rate
Pauw
vlietetal.1997
OS
Netherla
nds
Rheumaticdisorders
(BM,T
M)
I:35;D
:76mon
ths
Tradition
alTM
(not
furtherspecified)
(1)S
everity
ofdiseaseimproved
(2)Improvem
entsin
pain,num
bero
fdise
ased
partsg
eneralwell-b
eing
,and
mentalcom
plaints
Highdrop
-out
rate,4
ofthem
becauseo
faggravation;
prepub
lication
with
outlaboratorydata
Prusek
etal.1987
CT(6
arms)(M
C)Po
land
Recurrentrespiratory
tractinfectio
ns(BM)
I:30;C
1:23;
C2:10;C3
:29;C
4:25;
C5:20;(4
years);D
:0
11mon
ths
I:P2
8,3×1U
/dfor1
mon
thC1
:levam
isole,
3mg/kg:for
2×3d
C2:thymus
factorx,1m
g/kg
for3
weeks
C3:bacteria
llysate,3.5m
g/dfor3×10d
C4:clim
atec
urefor
6weeks
C5:health
yprob
ands
(1)F
requ
ency
andseverityof
infections
improved
in57%(le
ssthan
controls)
(2)Immun
oglobu
lines
notchanged,T
cells
improved
Com
parabilityof
grou
psun
clear
(allo
catio
nby
clinicalind
ication);
statistic
alevaluatio
nno
tsufficient
Rüttg
ers2
004
CS Switzerland
Chronicv
enou
sinsufficiency
(BM)
I:1;D:0
3mon
thsa
ndfollo
w-up
P28,3×1U
/dandbiom
edicalstandard
(no
prim
arily
angiological)therapy
(1)Infl
ammationim
proved
(2)O
edem
aand
pain
improved;rem
issionfor>
6mon
ths;healingfaste
rund
erP2
8
Ryan
1997
RCT(3)
India
Arthritis(BM
,TM)
I:15;C
:15;D:
2
3mon
ths
I:tradition
alTM
(not
furtherspecified)
C:biom
edicaltre
atment
(1)M
otilityof
extre
mities
improved,in86%of
the
matched
pairs
theT
Mpatie
ntbette
rthan
respectiv
econ
trol
Inclu
sionby
Tibetan
diagno
sis;nofurtherd
etails
tomatched
pairs
;onlytwo
pairs
ofarthritispatie
nts
Sallo
netal.1998
RCT(4)
Israel
Perip
heralarterial
occlu
sived
isease
(BM)
I:37;C
:35;D:
13
6mon
ths
I:P2
8,2×2U
/dC:
potato
starch
(1)A
nkle-brachial-ind
exun
changed
(2)Improved:pressured
ecrease,isc
haem
iatim
e,andpatie
nt’sassessment
Sallo
netal.2002
RCT(4)
Israel
Chronicc
onstipatio
n(BM)
I:42;C
:38;
D:19
12weeks
I:PL
,2×2U
/d,
C:po
tato
starch
(1)Improved
intestinalpassage
(2)Improved
abdo
minalpain
(physic
ian’s
assessment)andeveryday
activ
ity(patient’s
assessment)
Com
prehensiv
estudy
documentatio
n
-
Evidence-Based Complementary and Alternative Medicine 9
Table2:Con
tinued.
Stud
yTy
pe∗
Cou
ntry
Dise
ase(diagno
stic
syste
m)∗∗
Participants
(meanage),
drop
-outs∗∗∗
Durationof
interventio
nor
study
kind
,doseo
fintervention∗∗∗∗
(1)M
ainou
tcom
e(2)O
ther
outcom
esNotes
Samocho
wiece
tal.
1987
RCT(4)
Poland
Perip
heralarterial
occlu
sived
isease
(BM)
I:55;C
:45
4mon
ths
I:P2
8,2×2U
/dC:
lactose
(1)Improved
max.w
alking
distance
(2)U
pper
arm
bloo
dpressure
unchanged,
improved:totalbloo
dlip
ids,𝛽-lipo
proteins,
thrombo
cyteaggregationthreshold
Nopatie
ntdemograph
ics;
comparis
onon
lyto
baselin
e,no
tbetween
grou
ps
Sang
moetal.2007
RCT(2)
India
HepatitisB
(BM,T
M)
I:24;C
:25;
D:1
6mon
ths
I:SpecialT
M,(no
tfurther
describ
ed)
C:Tradition
alTM
(1)N
odifferences
betweengrou
ps(2)B
othgrou
pstend
edto
improvem
entsin
liver
functio
nandim
proved
clinically
SpecialT
Mgrou
pmoreill
atbaselin
e;almostn
oappraisalofresults;
possibly
overtesting
;very
comprehensiv
edo
cumentatio
nalso
ofTibetandiagno
stics
Schleicher
1990
OS
Germany
Acqu
iredim
mun
edeficiencysynd
rome
(BM)
I:15;D
:56mon
ths
P28,3×3U
/d
(1)T
otalTcells
stabilized
(2)S
tabilized:sup
pressor-cytotoxicc
ells,
helper-in
ducerc
ells,
andlymph
ocytes;
unchanged:Bcells
andkillerc
ells;
increase
ingranulocytes
andph
agocytosis
Nopatie
nt-centre
dparameters;progno
stically
mostrele
vant
CD4cell
coun
tand
viralloadno
tdo
cumented
Schrader
etal.1985
RCT(4)
Switzerland
Perip
heralarterial
occlu
sived
isease
(BM)
I:27;C
:26;
D:10
4mon
ths
I:P2
8,3×2U
/dC:
lactose
(1)Improved
max.w
alking
distance
(2)Improved
pain-fr
eewalking
distance
Smulskiand
Wojcicki1994
RCT(5)
Poland
Perip
heralarterial
occlu
sived
isease
(BM,T
M)
I:50;C
:50;
D:7
4mon
ths
I:P2
8,2×2U
/dC:
lactose
(1)M
ax.w
alking
distance
improved
(2)P
atient’sassessmentm
orep
ositive,improved
totalblood
lipids,triglycerid
es,low
density
lipop
roteins
Com
paris
onof
grou
pson
lyforw
alking
dista
nce
Split
etal.1998
RCT(2)
Poland
Apop
lexy
(BM)
I:60;C
:60
14days
I:P2
8,3×2U
/d+biom
edicalstandard
therapy
C:biom
edicalstandard
therapy
(1)B
etterg
eneralsta
tus(Ka
rnofskyfunctio
nal
efficiency
scale,KF
ES)
(2)B
etterT
cells,B
cells,and
clinicalprogress
Age
notstated,no
blinding
,no
placebo,comparis
onon
lyun
derstand
ablefor
KFES
,therapy
effectn
otdiscerniblefrom
placebo
effect
Wojcickietal.1986
CT Poland
Coron
aryheart
disease,angina
pectoris(BM)
I:50
6weeks
Placebo,2weeks—P2
8,2×2U
/d,2
weeks—placebo,2weeks
(1)N
itroglycerin
eneedredu
ced
(2)Improvem
ento
fexercise
capacity,platele
taggregation,
andbloo
dlip
ids
Norand
omization
(con
traryto
publication
statem
ent);
descrip
tion
difficultto
understand
;selectionof
patie
ntsfrom
larger
popu
latio
nno
tclear;
shortverum
perio
d∗
(r)C
S:(retrospectiv
e)case
study
;CT:
controlledtrial(no
trando
mized);OS:ob
servationalstudy
;RCT
:rando
mized
controlledtrial(with
Jadadsum
score);M
C:multic
entre
study.
∗∗
BM:B
iomedicine(the“
Western”“conventio
nal”medicine);T
M:T
ibetan
medicine;CA
M:com
plem
entary
oralternativem
edicine.
∗∗∗
I:interventio
ngrou
p(TM);C:
controlgroup
(other
treatment,placebo);D
:totaldrop
outs.
∗∗∗∗
U:unit(tablet,capsule,
orpill);/d:perd
ay;P
28:Padma2
8;PL
:PadmaL
ax.
-
10 Evidence-Based Complementary and Alternative MedicineTa
ble3:DIM
DIH
TAchecklist
results.
Participants
Allo
catio
nInterventio
nAd
ministratio
nOutcome
Drop-ou
tsStatistics
Stud
y
Itemno.(label)∗
A1(in-/exclusion)
A2(pre-defined)
A3(healthstatus)
A4(diagnosticcriteria)
A5(representativity)
B1(basicpopulation)
B2(comparable)
B3(randomization)
B4(blindedrandomization)
B5(confounders)
C1(recording)
C2(similartreatment)
C3(othertreatments)
C4(placebouse)
C5(placebodocumented)
D1(overmatching)
D2(multicentre)
D3(nocrossover)
E1(patient-centred)
E2(recording)
E3(blindedoutcomes)
E4(prognosticfactors)
F1(evaluablenumber)
F2(reasons)
F3(outcomes)
F4(significance)
F5(relevance)
G1(correct)
G2(CIsgiven)
G3(graphics)
Rand
omized
controlled
trials
Brun
ner-LaRo
ccae
tal.2005
YY
YY
YY
YY
YY
YY⋅
YY
N⋅
YN
YY⋅
YY
Y⋅⋅
YN
YCoh
enetal.200
4Y
YY
NY
YY
?Y
YY
Y⋅
N⋅
N⋅
YY
YN⋅
?Y
N⋅⋅
YY
NHürlim
ann1979/1
YY
YY
YY
YY
YY
YY⋅
YY
N⋅
YY
Y?⋅
Y⋅⋅⋅⋅
YN
NKo
rwin-Piotro
wskae
tal.1992
YY
YN
YY
Y?
NY
YN
NN⋅
N⋅
YY
Y?⋅
Y⋅⋅⋅⋅
YN
NMehlse
netal.1995
YY
YY
YY
YY
YY
YY⋅
YY
N⋅
YY
YY⋅
YY
N⋅⋅
YY
NMiller2009
YY
YY
YY
Y?
YY
YY⋅
YY
N?
YY
YY⋅
YY
N⋅⋅
YN
NNam
duletal.2001
YY
YY
YY
Y?
??
YY⋅
N⋅
NY
YY
Y?⋅
YN
N⋅⋅
YN
NRy
an1997
YY
YY
?Y
Y?
?Y
YY
YN⋅
N⋅
YY
YN⋅
YN
N⋅⋅
YN
NSallo
netal.1998
YY
YY
YY
YY
YY
YY⋅
YY
N⋅
YY
YY⋅
?Y
N⋅⋅
YY
YSallo
netal.2002
YY
YY
YY
YY
YY
YY⋅
YY
N⋅
YY
YY⋅
YY
N⋅⋅
YN
YSamocho
wiece
tal.1987
YY
YY
YY
YY
YY
YY⋅
YY
N⋅
YY
YY⋅
Y⋅⋅⋅⋅
YN
YSang
moetal.2007
YY
YY
YY
Y?
??
NY⋅
N⋅
N⋅
YY
YN⋅
YY
N⋅⋅
YN
NSchrader
etal.1985
YY
YY
YY
YY
YY
YY⋅
YY
N⋅
YY
YY⋅
YY
N⋅⋅
YN
NSm
ulskiand
Wojcicki1994
YY
YY
YY
YY
YY
YY⋅
YY
N⋅
YY
YY⋅
YY
N⋅⋅
YY
YSplit
etal.1998
YY
NN
?Y
Y?
??
YY⋅
N⋅
N⋅
YY
Y?⋅
Y⋅⋅⋅⋅
YN
N
Con
trolled
trials
Brzoskoetal.1991
YY
YY
YY
NN⋅
NY
Y⋅⋅⋅
N⋅
YY
YN⋅
Y⋅⋅⋅⋅
YN
NJank
owskietal.1991
YY
YY
YN
NN⋅
NY
N⋅⋅⋅
N⋅
YN
YN⋅
Y⋅⋅⋅⋅
YN
NMansfe
ld1988
YY
YN
YY
?N⋅
?Y
Y⋅⋅⋅
N⋅
YY
?N⋅
Y⋅⋅⋅⋅
YN
YPrusek
etal.1987
YY
YY
YY
NN⋅
NY
?⋅⋅⋅
NN
YY
?N⋅
Y⋅⋅⋅⋅
YN
NWojcickietal.1986
YY
YY
YY
YN⋅
YY
Y⋅⋅⋅
N⋅
YY
YN⋅
Y⋅⋅⋅⋅
YN
N
Observatio
nstu
dies
Ascho
ffetal.1997
YY
YY
Y⋅⋅⋅⋅
YY
NN⋅⋅⋅⋅⋅
YY⋅⋅
Y⋅⋅⋅⋅
YN
NBrzoskoandJank
owski1992
YY
?N
Y⋅⋅⋅⋅
?Y
?⋅⋅⋅⋅⋅⋅
YY⋅⋅
Y⋅⋅⋅⋅
YN
NFlückandBu
bb1970
YY
YY
Y⋅⋅⋅⋅
NY
?⋅⋅⋅⋅
Y⋅
YY⋅⋅
Y⋅⋅⋅⋅
YN
NFü
llemann2006
YY
YY
Y⋅⋅⋅⋅
YY
NN⋅⋅⋅⋅⋅
YY⋅⋅
YY
YN
NY
NN
Gladysz
etal.1993
YY
YY
Y⋅⋅⋅⋅
YY
Y⋅⋅⋅⋅⋅⋅
NY⋅⋅
Y⋅⋅⋅⋅
YN
NHürlim
ann1979/2
YY
YY
Y⋅⋅⋅⋅
?Y
?⋅⋅⋅⋅⋅⋅
YN⋅⋅
Y⋅⋅⋅⋅
YN
NJank
owskietal.1986
YY
YY
Y⋅⋅⋅⋅
NY
?⋅⋅⋅⋅⋅⋅
YY⋅⋅
Y⋅⋅⋅⋅
YY
N
-
Evidence-Based Complementary and Alternative Medicine 11
Table3:Con
tinued.
Participants
Allo
catio
nInterventio
nAd
ministratio
nOutcome
Drop-ou
tsStatistics
Stud
y
Itemno.(label)∗
A1(in-/exclusion)
A2(pre-defined)
A3(healthstatus)
A4(diagnosticcriteria)
A5(representativity)
B1(basicpopulation)
B2(comparable)
B3(randomization)
B4(blindedrandomization)
B5(confounders)
C1(recording)
C2(similartreatment)
C3(othertreatments)
C4(placebouse)
C5(placebodocumented)
D1(overmatching)
D2(multicentre)
D3(nocrossover)
E1(patient-centred)
E2(recording)
E3(blindedoutcomes)
E4(prognosticfactors)
F1(evaluablenumber)
F2(reasons)
F3(outcomes)
F4(significance)
F5(relevance)
G1(correct)
G2(CIsgiven)
G3(graphics)
Jank
owskietal.1992
YY
YY
Y⋅⋅⋅⋅
NY
Y⋅⋅⋅⋅⋅⋅
YY⋅⋅
Y⋅⋅⋅⋅
YN
NLeem
anatal.2001
YY
YN
Y⋅⋅⋅⋅
NN
NN⋅⋅⋅⋅⋅
YY⋅⋅
YN
N⋅⋅
YN
NLi
2001
YY
YY
Y⋅⋅⋅⋅
YN
Y⋅⋅⋅⋅
Y⋅
YY⋅⋅
Y⋅⋅⋅⋅
YN
NNeshar2
000
YN
YY
Y⋅⋅⋅⋅
NY⋅⋅⋅⋅⋅⋅⋅
YN⋅⋅
?⋅⋅⋅⋅
NN
NNeshar2
007
YY
?Y
?⋅⋅⋅⋅
?Y⋅⋅⋅⋅⋅
Y⋅
YY⋅
NY
NN⋅⋅
YN
NPauw
vlietetal.1997
YY
YY
Y⋅⋅⋅⋅
?Y
NY⋅⋅⋅⋅⋅
YY⋅⋅
Y⋅⋅⋅⋅
YN
NSchleicher1990
YY
YY
Y⋅⋅⋅⋅
NY
?N⋅⋅⋅⋅⋅
NY⋅⋅
?⋅⋅⋅⋅
YN
N
Case
studies
Bommeli
etal.2001
YY
YY
Y⋅⋅⋅⋅
YY
NN⋅⋅⋅
Y⋅
YY⋅
NY
YN⋅⋅
YN
NCh
angbar
1998
Y⋅
YY
N⋅⋅⋅⋅⋅
Y⋅⋅⋅
Y⋅⋅⋅
YY⋅
NY⋅⋅⋅⋅⋅⋅
NFeldhaus
2004
Y⋅
YY
N⋅⋅⋅⋅
?Y⋅⋅⋅⋅⋅⋅⋅
YY⋅
NY⋅⋅⋅⋅⋅⋅
NFeldhaus
2006
YY
YY
Y⋅⋅⋅⋅
?Y
N⋅⋅⋅⋅⋅⋅
YY⋅
NY⋅⋅⋅⋅⋅⋅
NGün
sche
2005
Y⋅
YY
N⋅⋅⋅⋅
YY⋅⋅⋅⋅⋅⋅⋅
YN⋅
NY⋅⋅⋅⋅⋅⋅
NRü
ttgers2
004
Y⋅
YY
N⋅⋅⋅⋅
NY⋅⋅⋅⋅⋅⋅⋅
YN⋅
NY⋅⋅⋅⋅⋅⋅
NY:
yes;N:no;?:un
clear/not
stated;⋅:not
applicable.
∗
Fullitem
text
inTable1.
-
12 Evidence-Based Complementary and Alternative Medicine
Table 4: Jadad Score Results for Included RCTs.Randomization
Blinding Drop-outs Sum score
Brunner-La Rocca et al. 2005 2 2 1 5Cohen et al. 2004 2 0 0
2Hürlimann 1979/1 1 2 0 3Korwin-Piotrowska et al. 1992 1 0 1
2Mehlsen et al. 1995 2 2 1 5Miller 2009 2 2 1 5Namdul et al. 2001 1
0 0 1Ryan 1997 2 0 1 3Sallon et al. 1998 1 2 1 4Sallon et al. 2002
1 2 1 4Samochowiec 1987 1 2 1 4Sangmo et al. 2007 1 0 1 2Schrader
et al. 1985 1 2 1 4Smulski and Wojcicki 1994 2 2 1 5Split et al.
1998 1 0 1 2
on Padma 28 or Padma Lax had higher Jadad scores thanstudies on
other treatments: 3.70 ± 1.06 (median = 4) versus2.60 ± 1.51
(median = 2).
All studies followed conventional “Western” medicaldiagnoses.
Additional traditional TM diagnostics wererecorded in 11 studies
that investigated the traditional mul-timodal treatment. In 9 of
them, the Tibetan diagnosis wasused to plan the therapy [39, 42,
43, 45, 48, 58, 59, 62, 76].
Thirty studies including 3497 patients (74.7% from allincluded
studies) investigated single formulations: Padma 28(𝑛 = 25
studies), Padma Lax (3), Byu-Dmar 13 (1), andZhi Byed 11 (1). The
complex traditional Tibetan treatmentwas studied in 9 trials that
included a total of 1140 (24.3%)patients.Here, and in the Padma 28
studies, the treated condi-tions varied widely. For example, Padma
28 was investigatedfor arteriosclerosis, infections, neurological
disorders, venousinsufficiency, arthritis, and
hypercholesteraemia.
Assessed outcomes included clinical outcomes such assymptom
scales (𝑛 = 37 studies), laboratory tests (19), clinicaltests (such
as ankle/brachial pressure index, blood pressure,or weight; 9), and
other (9), such as microbiology, histology,or the need for
conventional medication. The authors drewpositive conclusions on
their data in 34 studies. In 2 RCTs,TM was found to be inferior to
conventional medicine,but better than placebo [44, 46]. In one
study, only 1 of 5outcomes improved [60]; in 2 studies the primary
outcomedid not change significantly while secondary outcomes
did[42, 52]. The comparison of the traditional and a not
furtherspecified “special” Tibetan medicine [59] resulted in
compa-rable clinical improvements.The remaining studies found
nosignificant differences to controls [49, 65], or their
authorswere doubtful about the observed effects [39].
Statementsabout adverse effects were included in 23 studies, in 11
ofthem no adverse effects were reported, and 2 studies did
notmention the number of patients with adverse effects [39, 53].The
remaining 10 studies reported adverse effects with a rangefrom 5%
to 55% of the patients.
Some disease groups were researched in several trials.Peripheral
arterial occlusive disease was treated with Padma
28 in 9 studies (6 RCTs, (the first study in [38], [51–55]))1
observation study, (the second study in [38]) and 2 casestudies
[40, 72]. Maximum walking distance increased in 5studies (the first
study in [38], and [51, 53–55]). Both casestudies and the
observational study reported a general clinicalimprovement. The
ankle/brachial pressure index in 1 RCT[52] was unchanged. All
authors made a positive conclusionregarding Padma 28.
Five studies (3 non-randomized controlled trials [46, 53,65] and
2 observation studies [70, 71]) investigated Padma28 for recurrent
respiratory tract infections in children.Improvements were seen for
frequency of infections [70, 71]or spontaneous bacterial activity
[64]. In 1 of the controlledtrials, no significant difference to
standard therapy was found[65], and in another study, inferiority
to other therapies wasreported [46].
Osteoarthritis or rheumatoid arthritis was treated inthree
trials: 1 RCT [58] and 1 observational study [62] withthe
traditional multimodal approach, and with Padma 28in 1 controlled
trial [66]. All studies reported pre-/post-improvements or
superiority to controls regarding symptomseverity.
Padma Lax in chronic constipation was the subject ofthree
studies (1 RCT [57], 1 controlled trial [75], and 1 obser-vational
study [41]). All reported clinical improvements.
In 3 other trials, hepatitis B patients were either treatedwith
a “special” TM (that was not further specified) incomparison to
traditional TM (1 RCT [59]) or with Padma 28(2 observational
studies [47, 69]). All publications reportedpositive results for
laboratory outcomes. The comparison oftraditional and “special”
traditional TM found comparableimprovements but did not achieve
seroconversions.
4. Discussion
In this paper, we presented an overview of the clinicalresearch
on traditional Tibetan medicine (TM) that is cur-rently available
in the West. Three quarters of the includedstudies tested single
formulations, most of them products of
-
Evidence-Based Complementary and Alternative Medicine 13
a single company. One quarter investigated the
traditionalmultimodal TM approach. Studies were very
heterogeneousregarding study type and size, treated conditions,
treatments,measured outcomes, and quality.
In this, to our knowledge, first systematic overview ofclinical
TM research available in the West, we tried tominimize subjectivity
using pre-defined systematic methodswherever possible (data
extraction sheets, established qualityassessment tools). However,
the small number of trials scat-tered over a whole medical system
and very heterogeneoustreated diseases prohibitedmore formal or
in-depth analyses.
Despite the broad literature search, some studies may nothave
been identified, for various reasons. Although Mongo-lian and
Tibetan medicine are not completely identical, wehave included
“mongolian” in the search terms in order tofind asmuch relevant
literature as possible.We did not searchfor single TM interventions
such as bathing or bloodlettingand assumed that they are well
covered under the umbrellaterm “medicine.” Although we detected
with this search astudy on Tibetan yoga [60], we possibly missed
other studies.Furthermore, publication bias could have had
occurred, assome papers [11, 15, 58] indicated the existence of
studiesthat have not been published (or at least not in
indexedjournals) [77–82]. Several papers were not identified byour
search strategy in the literature databases, but couldhave been
found searching for “Padma 28” or “Padma Lax.”Clearer labelling of
TM studies in the future would behelpful. On the other hand, our
search seems to have beenpartly redundant, as all identified
publications could havebeen found with fewer search terms. The main
limitation isthat our language restriction excluded articles in
Russian,Tibetan, and Chinese. This literature was not accessiblefor
us. Furthermore, we learned from our field work andfrom discussions
with Western and Chinese manufacturersduring an interdisciplinary
symposium on TM [16] thatmost literature on clinical research
published in Tibetan isnot available in indexed journals and that
most researchpublished in Chinese addresses preclinical
questions.
The evaluated literature presented a high number ofstudies
without a control group. Only a few single productswere subject to
in-depth investigation. Both facts indicate anearly stage of
research in a new and largely unexplored fieldwhere only few
focused inquiries exist. The predominatingcountries of origin
(>2/3 European) and the 70% of studieson Padma products among
the included literature are conse-quences of the language
restrictions of our search as well asof the historical development
of TM utilization in the West.Although they are prescribed in a
standardized and nonindi-vidualized fashion, the Padma products are
a genuine Tibetanmedication according to manufacturers, study
authors, andindependent experts [17, 83, 84]. Adaptation of
constituentsto local situation and ecology is an accepted practice
in TM.It was done in one study when Tibetan physicians reducedthe
traditional Byu-Dmar 25 by 12 ingredients to comply withTibetan
pharmacopoeia and European regulations, resultingin Byu-Dmar 13
[63]. A similar strategymight have been usedin two other studies
[39, 62].
The heterogeneous nature of the included studiesdemanded the use
of quality assessment instruments that
were suitable for diverse study designs, but have the
generaldisadvantage of allowing only rough estimates of theassessed
quality. Nevertheless, they allowed spotting themore obvious
deficiencies that are symptomatic of researchat an early stage and
that future research can avoid withimproved methodology on the
grounds of evidence-basedmedicine. Case studies and observational
studies are usefulto gather information on traditional usage and
settings andto identify areas where controlled studies seem
promising.Then, to provide higher-level evidence, more RCTs willbe
needed. Methodological issues such as small samples,insufficiently
described populations in many studies,pre-/post-comparisons of
treatment within a group, orcomparator treatments without clinical
relevance all indicatethat TM research as seen through the Western
literatureis still at a nascent stage. Furthermore, the quality of
moststudies and the heterogeneity of interventions and outcomesmake
clear conclusions impossible.
5. Conclusion
The clinical research on traditional Tibetan medicine (TM)that
is available in Western industrialized countries is scarceand
scattered over a whole medical system, but showsinteresting
results. Better research methodology should beapplied, and larger
trials are needed, as is a general overviewof traditional usage to
inform future clinical research.
Acknowledgments
This work was supported within a grant of the Chair
forComplementary Medicine Research, funded by the Karl andVeronica
Carstens Foundation, Essen, Germany.The authorsstate that they have
no conflict of interests.
References
[1] T. Dunkenberger, Das Tibetische Heilbuch, Windpferd
Verlags-gesellschaft, Aitrang, Germany, 1999.
[2] P. Skinner, “Tibetan medicine,” in The Gale Encyclopedia
ofAlternative Medicine, T. Gale, Ed., Longe, Detroit, Mich, USA,2nd
edition, 2005.
[3] V. Dash, Tibetan Medicine: Theory and Practice, Sri
SatguruPublications, Delhi, India, 1997.
[4] G. Samel, TibetanMedicine, Little, Brown&Company,
London,UK, 2001.
[5] C.M.Witt, N. Berling, N.Thingo,M. Cuomo, and S.
N.Willich,“Evaluation of medicinal plants as part of Tibetan
medicine—prospective observational study in Sikkim and Nepal,”
Journalof Alternative and Complementary Medicine, vol. 15, no. 1,
pp.59–65, 2009.
[6] E. Asshauer, Tibets Sanfte Medizin: Heilkunst vom Dach
derWelt, Oesch, Zürich, Switzerland, 4th edition, 2003.
[7] B. B. Gaitonde and P. N. Kurup, “Regional overview:
South-EastAsia region,” inWHO Global Atlas of Traditional,
Complemen-tary and Alternative Medicine, G. Bodeker, C. Ong, C.
Grundyet al., Eds., pp. 75–82, World Health Organisation, Centre
forHuman Development, Kobe, Japan, 2005.
-
14 Evidence-Based Complementary and Alternative Medicine
[8] H. Schwabl, S. Geistlich, and E. McHugh, “Tibetische
Arznei-mittel in Europa: Historische, praktische und
regulatorischeAspekte,” Forschende Komplementärmedizin, vol. 13,
supple-ment 1, pp. 1–6, 2006.
[9] V. Badmaev Jr., “The continuation of the Badmaev family
tra-dition in its 5th generation,” AyurVijnana, vol. 7, 2000.
[10] R. Saller, “TibetischeHeilmittel bei chronischen
Erkrankungen,Einleitung,” in Tibetische Heilmittel bei Chronischen
Erkrankun-gen, Zürich, Switzerland, 2005.
[11] J. Melzer, R. Brignoli, C. Diehm et al., “Treating
intermittentclaudication with Tibetan medicine Padma 28: does it
work?”Atherosclerosis, vol. 189, no. 1, pp. 39–46, 2006.
[12] V. Badmaev, “Medicine tested by Science: an effective
botanicaltreatment for circulatory deficience due to
atherosclerosis,”Nutri-Cosme-Ceutici, 6.8.2.2002, Rome, Italy,
2002.
[13] F. Ueberall, D. Fuchs, and C. Vennos, “Das
anti-inflamma-torische Potential von Padma 28: Übersicht
experimentellerDaten zur antiatherogenen Wirkung und Diskussion des
Viel-stoffkonzepts,” Forschende Komplementärmedizin, vol. 13,
sup-plement 1, pp. 7–12, 2006.
[14] A. Weseler, R. Saller, and J. Reichling, “Comparative
investi-gation of the antimicrobial activity of Padma 28 and
selectedEuropean herbal drugs,” Forschende Komplementärmedizin
undKlassische Naturheilkunde, vol. 9, no. 6, pp. 346–351, 2002.
[15] M. B. Röösli, Systematische Übersichtsarbeit: Klinische
Stu-dien zur Wirksamkeit und Sicherheit des
phytotherapeutischenKombinationspräparats PADMA 28, Universität
Zürich, Zürich,Switzerland, 2009.
[16] C. M. Witt, S. Craig, and M. Cuomu, Tibetan
MedicineResearch—From Current Evidence to Future Strategies:
Advicefrom an Interdisciplinary Conference, KVC Verlag, Essen,
Ger-many, 2012.
[17] S. Geistlich and H. Schwabl, “Von der Tradition zur
‘evidence-based medicine’,” Schweizerische Zeitschrift für
Ganzheitsmedi-zin, vol. 15, pp. 133–140, 2003.
[18] B. Gerke, “Tradition and modernity in Mongolian
medicine,”The Journal of Alternative and ComplementaryMedicine,
vol. 10,no. 5, pp. 743–749, 2004.
[19] E. M. Plakun, “Psychiatry in Tibetan Buddhism: madness
andits cure seen through the lens of religious and national
history,”The Journal of the American Academy of Psychoanalysis
andDynamic Psychiatry, vol. 36, no. 3, pp. 415–430, 2008.
[20] M. Saxer, Journeys with Tibetan medicine [M.S. thesis],
2004,http://www.anyma.ch/journeys/doc/thesis.pdf.
[21] I. A. Navchoo and G. M. Buth, “Medicinal system of
Ladakh,India,” Journal of Ethnopharmacology, vol. 26, no. 2, pp.
137–146,1989.
[22] United Nations, “World, Map No. 4170,” October 2006,
http://www.scribd.com/doc/217671/Map-The-World.
[23] Wolters Kluwer,Ovid Technologies, 2010,
http://www.ovid.com.[24] DIMDI, Datenbanken A-Z, 2010,
http://www.dimdi.de/static/
de/db/dbinfo/index.htm.[25] Bibliothek der Charité,
Datenbanken, 2010, http://www.charite
.de/bibliothek/datenbanken.htm.[26] ZB MED,MedPilot, 2010,
http://www.medpilot.de.[27] Google, Google Scholar, 2010,
http://scholar.google.com.[28] A.G.
Padma,Padma28—Literaturverzeichnis 2/09, 2009, http://
www.padma.ch/Literature/Literature Padma28 Feb2009.pdf.[29] J.
Aschoff, Tibetische Medizin—Kommentierte Bibliographie,
Fabri, Ulm, Germany, 1996.
[30] Institut für Ost-West-Medizin, Kursreihe Einführung in
dieTibetische Medizin, 2008, http://www.ostwestmedizin.de/.
[31] Interessengemeinschaft Tibetische Medizin, Programm im
De-tail: der Ausbildung zur Therapeutin tibetische Medizin,
Interes-sengemeinschaft Tibetische Medizin, 2011,
http://www.ig-tibetische-medizin.ch/images/ausbildung/Ausbildung
Ueber-sicht.pdf.
[32] New Yuthog Institute, 4 year Tibetan Medicine course,
2011,http://www.newyuthok.it/en/ctibetanmedicine.html.
[33] Access, Microsoft, Redmond, Wash, USA, 2003.[34] Excel,
Microsoft, Redmond, Wash, USA, 2003.[35] M. Ekkernkamp, D.
Lühmann, and H. Raspe,Methodenmanual
für ,HTA-Schnellverfahren’ und exemplarisches ,Kurz-HTA’.
DieRolle der quantitativen Ultraschallverfahren zur Ermittlung
desRisikos für osteoporotische Frakturen, vol. 34, Asgard
Verlag,Sankt Augustin, Germany, 2003.
[36] D. Moher, A. R. Jadad, and P. Tugwell, “Assessing the
qualityof randomized controlled trials. Current issues and
futuredirections,” International Journal of Technology Assessment
inHealth Care, vol. 12, no. 2, pp. 195–208, 1996.
[37] A. R. Jadad, R. A. Moore, D. Carroll et al., “Assessing the
qualityof reports of randomized clinical trials: is blinding
necessary?”Controlled Clinical Trials, vol. 17, no. 1, pp. 1–12,
1996.
[38] F.Hürlimann, “Eine lamaistische Rezeptformel zur
Behandlungder peripheren arteriellen Verschlusskrankheit,”
SchweizerischeRundschau Fur Medizin, vol. 67, pp. 1407–1409,
1979.
[39] E. Leeman, Y. Dhonden, and M. Woolf, A Phase I Trial
ofTibetanMedicine for Advanced Breast Cancer, 2001,
http://www.cbcrp.org/research/PageGrant.asp?grant id=90.
[40] C. Bommeli, R. Bohnsack, and C. Kolb, “Praxiserfahrungenmit
einem Vielstoffpräparat aus der tibetischen
Heilkunde,”Erfahrungsheilkunde, vol. 50, no. 11, pp. 745–756,
2001.
[41] H. Flück and W. P. Bubb, “Eine lamaistische
Rezeptformelzur Behandlung der chronischen Verstopfung,”
SchweizerischeRundschau für Medizin Praxis, vol. 59, no. 33, pp.
1190–1193,1970.
[42] F. Li, “Ergebnisse der Behandlung von
symptomatischenPatien-ten mit tibetanischer Medizin, die an einer
Infektion mit Heli-cobacter Pylori (HP) leiden,” Deutsche
Zeitschrift für Akupunk-tur, vol. 44, no. 3, pp. 183–185,
2001.
[43] T.Namdul, A. Sood, L. Ramakrishnan et al., “Efficacy of
Tibetanmedicine as an adjunct in the treatment of type 2
diabetes,”Diabetes Care, vol. 24, no. 1, pp. 175–176, 2001.
[44] S. Miller, C. Tudor, V. Thorsten et al., “Randomized
doublemasked trial of Zhi Byed 11, a Tibetan traditional medicine,
ver-sus misoprostol to prevent postpartum hemorrhage in
Lhasa,Tibet,” Journal of Midwifery & Women’s Health, vol. 54,
no. 2,pp. 133.e1–141.e1, 2009.
[45] D. Neshar, “Clinical case Study of Cancer (Dres-ned)
patientstreated at Men-Tsee-Khang’s Bangalore Branch Clinic for
theperiod of 27 month from November 2002 to February 2005,”Journal
of Men-Tsee-Khang, vol. 4, no. 1, pp. 50–68, 2007.
[46] W. Prusek, A. Jankowski, G. Radomska et al.,
“Immunos-timulation in recurrent respiratory tract infections
therapy inchildren,”Archivum Immunologiae etTherapiae
Experimentalis,vol. 35, no. 3, pp. 289—2302, 1987.
[47] W. Brzosko and A. Jankowski, “PADMA 28 bei chronis-cher
Hepatitis B: Klinische und immunologische Wirkungen,”Schweizerische
Zeitschrift für Ganzheitsmedizin, vol. 7-8, supple-ment 1, pp.
13–14, 1992.
-
Evidence-Based Complementary and Alternative Medicine 15
[48] D. Neshar, “Efficacy of traditional Tibetan medicine
againstdiabetes mellitus,” Journal of Men-Tsee-Khang, vol. 2, no.
2, pp.25–35, 2000.
[49] H. P. Brunner-La Rocca, R. Schindler, M. Schlumpf et
al.,“Effects of the Tibetan herbal preparation Padma 28 on
bloodlipids and lipid oxidisability in subjects with mild
hypercholes-terolaemia,” VASA, vol. 34, no. 1, pp. 11–17, 2005.
[50] T. Korwin-Piotrowska, D. Nocon, A. Stankowska-Chomicz,
A.Starkiewicz, J. Wojcicki, and L. Samochowiec, “Experience ofPadma
28 in multiple sclerosis,” Phytotherapy Research, vol. 6,no. 3, pp.
133–136, 1992.
[51] J. Mehlsen, H. Drabaek, J. Petersen et al., “Der Effekt
einertibetischen Kräutermischung (Padma 28) auf die Gehstreckebei
stabiler Claudication intermittens,” Forschende
Komple-mentärmedizin und Klassische Naturheilkunde, vol. 2, no. 5,
pp.240–245, 1995.
[52] S. Sallon, G. Beer, J. Rosenfeld et al., “The efficacy of
Padma28, a herbal preparation, in the treatment of
intermittentclaudication: a controlled double-blind pilot study
with objec-tive assessment of chronic occlusive arterial disease
patients,”Journal of Vascular Investigation, vol. 4, no. 3, pp.
129–136, 1998.
[53] L. Samochowiec, J. Wojicki, and K. Kosminder,
“Wirksamkeit-sprüfung von Padma 28 bei der Behandlung von
Patienten mitchronischen arteriellen Durchblungsstörungen,”
PolbiopharmReports, no. 22, pp. 3–14, 1987.
[54] R. Schrader, B. Nachbur, and F. Mahler, “Die Wirkung
destibetanischen Kräuterpraparates Padma 28 auf die
Claudicatiointermittens,” Schweizerische Medizinische
Wochenschrift, vol.115, no. 22, pp. 752–756, 1985.
[55] H. S. Smulski and J. Wojcicki, “Plazebokontrollierte
Doppel-blindstudie zur Wirkung des tibetanischen
KräuterpräparatesPadma 28 auf die Claudication intermittens,”
Forschende Kom-plementärmedizin und Klassische Naturheilkunde,
vol. 1, pp. 18–26, 1994.
[56] W. Split, M. Szydlowska, andW. Brzosko, “The estimation of
theaction of Padma-28 in the treatment of ischaemic brain
stroke,”European Journal of Neurology, vol. 5, supplement 1, p. 9,
1998.
[57] S. Sallon, E. Ben-Arye, R. Davidson et al., “A novel
treatmentfor constipation-predominant irritable bowel syndrome
usingPadma Lax, a Tibetan herbal formula,” Digestion, vol. 65, no.
3,pp. 161–171, 2002.
[58] M. Ryan, “Efficacy of the Tibetan treatment for arthritis,”
SocialScience & Medicine, vol. 44, no. 4, pp. 535–539,
1997.
[59] R. Sangmo, D.Dolma, T. Namdul et al., “Clinical trial of
Tibetanmedicine in the treatment of chronic hepatitis B,” Journal
ofMen-Tsee-Khang, vol. 4, no. 1, pp. 32–49, 2007.
[60] L. Cohen, C. Warneke, R. T. Fouladi et al.,
“Psychologicaladjustment and sleep quality in a randomized trial of
the effectsof a Tibetan yoga intervention in patients with
lymphoma,”Cancer, vol. 100, no. 10, pp. 2253–2260, 2004.
[61] J. Wojcicki, L. Samochowiec, and C. Dolata,
“Controlleddouble-blind study of Padma 28 in angina pectoris,”
HerbaPolonica, vol. 32, no. 2, pp. 107–113, 1986.
[62] C. Pauwvliet, “A pilot study on the effect of Tibetan
medicineon patients with rheumatic diseases,” in Tibetan Medicine,
J.Aschoff and I. Rösing, Eds., pp. 39–49, Fabri, Ulm,
Germany,1997.
[63] J. Aschoff, T. Tashigang, and J. Maier, “Clinical trial in
migraineprophylaxis with amulticomponent Tibetan jewel-pill.
Transferproblems of Tibetan to Western medicine, demonstrated,
“pars
pro toto” on the Aconitemedical plants in our Tibetan
prescrip-tion,” in Tibetan Medicine,Verlag, J. Aschoff and I.
Rösing, Eds.,pp. 21–38, Fabri, Ulm, Germany, 1997.
[64] S. Jankowski, A. Jankowski, S. Zielinska, M. Walczuk, andW.
J. Brzosko, “Influence of Padma 28 on the spontaneousbactericidal
activity of blood serum in children suffering fromrecurrent
infections of the respiratory tract,” PhytotherapyResearch, vol. 5,
no. 3, pp. 120–123, 1991.
[65] H. Mansfeld, “Beeinflussung rezidivierender
Atemwegsinfektebei Kindern durch Immunostimulation,”Therapeutikon,
vol. 2,p. 707, 1988.
[66] W. J. Brzosko, A. Jankowski, W. Prusek, and H.
Ollendiek,“Influence of Padma 28 and the thymus extract on
clinicaland laboratory parameters of children with juvenile
chronicarthritis,” International Journal of Immunotherapy, vol. 7,
no. 3,pp. 143–147, 1991.
[67] P. Schleicher, “Wirkung von Padma 28 auf das Immun-system
bei Patienten mit Acquired Immunodeficiency Syn-drom im Stadium des
Pre-AIDS,” Schweizerische Zeitschrift fürGanzheitsmedizin, vol. 2,
p. 58, 1990.
[68] F. Füllemann, “Padma 28 in der Behandlung von chronis-chen
Zahnpulpitiden: Eine Praxisbeobachtung an 49 Fällen,”Forschende
Komplementärmedizin, vol. 13, supplement 1, pp.28–30, 2006.
[69] A. Gladysz, J. Juszczyk, and W. J. Brzosko, “Influence of
Padma28 on patients with chronic active hepatitis B,”
PhytotherapyResearch, vol. 7, no. 3, pp. 244–247, 1993.
[70] A. Jankowski, E. Drabik, Z. Szysko et al., “Die Behand-lung
rezidivierender Atemwegsinfektionen bei Kindern durchAktivierung
des Immunsystems,” Therapiewoche Schweiz, vol.2, no. 1, pp. 25–32,
1986.
[71] A. Jankowski, R. Jankowska, and W. Brzosko, “Behand-lung
infektanfälliger Kinder mit Padma 28,” SchweizerischeZeitschrift
für Ganzheitsmedizin, vol. 7-8, supplement 1, pp. 22–23, 1992.
[72] S. Feldhaus, “Ganzheitliches Therapiekonzept bei
pAVK,”Schweizerische Zeitschrift für Ganzheitsmedizin, vol. 16, p.
72,2004.
[73] M. Günsche, “Therapieresistenz bei Tagesmüdigkeit,
Antrieb-sschwäche und Konzentrationsschwierigkeit,”
SchweizerischeZeitschrift für Ganzheitsmedizin, vol. 17, p. 90,
2005.
[74] J. Rüttgers, “Crux medicorum: das offene Bein,”
SchweizerischeZeitschrift für Ganzheitsmedizin, vol. 16, pp.
278–280, 2004.
[75] S. Feldhaus, “Behandlung der chronischen Obstipation
einestetraplegischen Patienten mit dem tibetischen
ArzneimittelPadma Lax—ein Fallbericht,” Forschende
Komplementärmed-izin, vol. 13, supplement 1, pp. 31–32, 2006.
[76] S. Changbar, “Tibetan medicine in the treatment of
aplasticanaemia,” AyurVijnana, vol. 4, 1998.
[77] M. Ryan, “Measuring the efficacy of Tibetan treatment for
acutehepatitis,” inProceedings of the 10thAnnual Conference on
EthnicCulture and Folk Knowledge of Russian Acadamy of
Sciences,Moscow University Press, Moscow, Russia, 1994.
[78] S. Sommogy and P. Schleicher, “Therapie der
peripherenarteriellen Verschlusskrankheit (PAVK) mit Padma 28,”
Bericht26.6, Abteilung für Gefäßchirurgie, Technische
UniveritätMünchen und Zytognost GmbH, München, Germany,
1990.
[79] L. Samochowiec, J. Wojcicki, K. Kosmider et al.,
“Wirksamkeit-sprüfung von Padma 28 bei der Behandlung von
Patientenmit chronischen arteriellen Durchblutungsstörungen,”
HerbaPolonica, vol. 33, pp. 29–41, 1987.
-
16 Evidence-Based Complementary and Alternative Medicine
[80] K. Winther, A. Kharazmi, H. Himmelstrup, H. Drabaek, andJ.
Mehlsen, “PADMA-28, a botanical compound, decreasesthe oxidative
burst response of monocytes and improvesfibrinolysis in patients
with stable intermittent claudication,”Fibrinolysis, vol. 8, no. 2,
pp. 47–49, 1994.
[81] H. Panjwani and W. Brzosko, “Influence of selected
immuno-correcting drugs on intellectual function of the brain due
toarteriosclerosis,” Nowiny Lekarskie, vol. 5, pp. 665–670,
1998.
[82] J. Hasik, H. Klinkiewicz, K. Linke et al., “Effectiveness
ofduodenal ulcer disease treatment by PADMA 28,” NowinyLekarskie,
vol. 2, pp. 40–44, 1992.
[83] T. Kalsang, Interview with KPR [pers. comm.],
Dharamsala,India, October 2008.
[84] T. Tamdin, “Challenges and prospects of research in
Tibetanmedicine,” in Tibetische Heilmittel bei Chronischen
Erkrankun-gen, Zürich, Switzerland, November 2005.
-
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation
http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing
Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing
Corporationhttp://www.hindawi.com