-
Review ArticleThe Role of mTOR Inhibitors in Liver
Transplantation:Reviewing the Evidence
Goran B. Klintmalm1 and Björn Nashan2
1 Baylor Simmons Transplant Institute, Baylor University Medical
Center, 3410 Worth Street, Suite 950,Dallas, TX 75246, USA
2Department of Hepatobiliary Surgery and Visceral
Transplantation, University Medical Center Eppendorf,Martinistra𝛽e
52, 20246 Hamburg, Germany
Correspondence should be addressed to Goran B. Klintmalm;
[email protected]
Received 30 May 2013; Revised 20 September 2013; Accepted 21
September 2013; Published 25 February 2014
Academic Editor: Andreas Zuckermann
Copyright © 2014 G. B. Klintmalm and B. Nashan. This is an open
access article distributed under the Creative CommonsAttribution
License, which permits unrestricted use, distribution, and
reproduction in any medium, provided the original work isproperly
cited.
Despite the success of liver transplantation, long-term
complications remain, including de novomalignancies, metabolic
syndrome,and the recurrence of hepatitis C virus (HCV) and
hepatocellular carcinoma (HCC).The currentmainstay of treatment,
calcineurininhibitors (CNIs), can also worsen posttransplant renal
dysfunction, neurotoxicity, and diabetes. Clearly there is a need
forbetter immunosuppressive agents that maintain similar rates of
efficacy and renal function whilst minimizing adverse effects.
Themammalian target of rapamycin (mTOR) inhibitors with a mechanism
of action that is different from other immunosuppressiveagents has
the potential to address some of these issues. In this review we
surveyed the literature for reports of the use of mTORinhibitors in
adult liver transplantation with respect to renal function,
efficacy, safety, neurological symptoms, de novo tumors, andthe
recurrence of HCC andHCV.The results of our review indicate that
mTOR inhibitors are associated with efficacy comparable toCNIs
while having benefits on renal function in liver transplantation.
We also consider newer dosing schedules that may limit sideeffects.
Finally, we discuss evidence that mTOR inhibitors may have benefits
in the oncology setting and in relation to HCV-relatedallograft
fibrosis, metabolic syndrome, and neurotoxicity.
1. Introduction
One-year survival rates for liver transplantation currentlystand
at more than 80% in the US and Europe [1, 2]; however,the demand
for liver transplants far outstrips the number ofavailable donor
livers as increasing numbers of patients arereferred for
transplantation. Moreover, the global incidenceof conditions that
may ultimately require a liver transplant(hepatocellular carcinoma
(HCC), nonalcohol fatty liverdisease, and cirrhosis) is predicted
to increase [3–6], whichwould further drive demand for the
procedure. This maybe balanced by a reduction in liver transplants
requiredowing to hepatitis C virus (HCV) as a result of the use
ofnew potent antivirals. The success of liver transplantation
islimited by shortages of suitable donor organs, adverse eventsof
immunosuppressive drugs, and recurrence of disease.
Although transplant surgery was an area of great interestin the
1960s and 70s, the mortality rate for liver transplanta-tion in
1978, using azathioprine and prednisone immunosup-pression, was
approximately 75%. Cyclosporine, a calcineurininhibitor (CNI),
changed the face of transplantation, andin a few years the survival
rate of liver transplantation hadreached 80% [7]. The search for
new and safer immuno-suppressants continued and in 1989, reports
were publishedon the successful use of tacrolimus, another CNI, in
livertransplantation [8]. CNIs have been the cornerstone
ofmaintenance immunosuppression in liver transplantation[9], but
their nephrotoxic effects are an important sourceof morbidity
[10–13]. Several other factors are implicatedin the development of
renal dysfunction following livertransplantation, including
increased age, diabetes mellitus,hypertension, and preexisting
kidney disease [14]. Data from
Hindawi Publishing CorporationJournal of TransplantationVolume
2014, Article ID 845438, 45
pageshttp://dx.doi.org/10.1155/2014/845438
-
2 Journal of Transplantation
the United Network for Organ Sharing demonstrate thatalmost 20%
of liver transplant recipients have chronic renalfailure 5 years
after transplantation [14]. High rates of renaldysfunction
associated with the preexisting liver disease andwith the use of
CNIs are compounded by the use of theModelfor End-Stage Liver
Disease score for allocating transplantssince it favors liver
transplantation in individuals with renaldysfunction.
In addition to renal dysfunction, long-term complica-tions
associated with liver transplantation include the devel-opment of
de novomalignancies and the recurrence of HCVand HCC. Recurrence of
HCC occurs in approximately 20%of liver recipients [15] and is
associated with poor prognosis[16]. In patients who receive a
transplant due to HCV-relatedend-stage liver disease, graft
reinfection is almost universaland a significant percentage of
patients develop chronic hep-atitis in the graft [17–19]; 5-year
survival rates after primaryliver transplantation are significantly
reduced among HCV-positive patients compared to HCV-negative
patients [19].A four-fold greater risk of developing de novo
malignanciesposttransplant compared to the general population has
alsobeen reported [20].
Another concern relates to adverse effects of the
immuno-suppressants that are required to maintain the graft.
Forexample, new-onset diabetes mellitus (NODM) has beenestimated to
occur in 5–27%of liver transplant recipients [21–23] and is
associated with a negative impact on patient andgraft survival
[24]. CNIs, particularly tacrolimus, have beenshown to increase the
risk of developing NODM [21, 25, 26]and are also associated with an
increase in the incidence ofmalignancies are transplantation [20,
27, 28] and with casesof neurotoxicity [28–30]. In addition,
metabolic syndrome,which refers to the combination of abdominal
obesity, hyper-tension, hyperglycemia, and hyperlipidemia, is
common afterliver transplantation and has been reported to affect
43–58% of liver transplant recipients [31]. Hypertension is
alsoassociated with CNIs, particularly with cyclosporine [32].
Taken together, an unmet need clearly remains foridentifying
alternative immunosuppressive regimens that (1)maintain
antirejection efficacy with substantially reducedCNI exposure; (2)
optimize renal function, both short- andlong-term, by minimizing
CNI nephrotoxicity; (3) avoidor minimize CNI-associated adverse
events; (4) reduce therecurrence of HCV and HCC; (5) reduce the
occurrenceof de novo posttransplant malignancies. The
mammaliantarget of rapamycin (mTOR) inhibitors could
potentiallymeet these criteria, in part because they allow the use
ofimmunosuppressive regimens that include reduced doses ofCNIs. The
mTOR inhibitors also possess a mechanism ofaction that is different
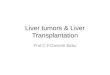
from other classes of immunosup-pressants: sirolimus and everolimus
engage FKBP12 to createcomplexes that engage and inhibit the target
of rapamycinbut cannot inhibit calcineurin (Figure 1). Inhibition
of thetarget of rapamycin blocks signal 3 by preventing
cytokinereceptors from activating the cell cycle [33]. In
addition,mTOR inhibitors may promote tolerance through actions
onregulatory T-cells and dendritic cells [34, 35].
Two mTOR inhibitors are currently approved for use
intransplantation. Everolimus is approved by the FDA for renal
and liver transplantation and by the EMA for renal, heartand
liver transplantation (Certican and Zortress, NovartisPharma AG;
Basel, Switzerland) [36, 37]. Clinical experiencewith everolimus in
liver transplantation is limited by the factthat it was only
recently approved for liver transplantationand it was not approved
for renal transplantation in the EUuntil 2003 and in the US until
2010. Sirolimus is approvedby the European Medicines Agency (EMA)
and the US Foodand Drug Administration (FDA) for renal
transplantation(Rapamune, Pfizer, NY, USA) [38, 39]. In the US,
sirolimuswas approved for renal transplantation in 1999. Although
notapproved for liver transplantation, it has still been used
inseveral centres in liver transplant recipients.
Everolimus is a derivative of sirolimus, differing by oneextra
hydroxyethyl group at position 40 [40]. In humanstudies, everolimus
has a shorter half life (30 hours) comparedto the 62 hours of
sirolimus and a quicker time to steady state(4 days versus 6 days)
[36, 38]. Both everolimus and sirolimusare substrates in the
p-glycoprotein and cytochrome P450-3A4 pathways [40, 41].
Therefore, the absorption and clear-ance of mTOR inhibitors may be
influenced by drugs thataffect cytochrome P450-3A4 and/or
p-glycoprotein, includ-ing common drugs such as fluconazole,
azithromycin, andprotease inhibitors [36, 38, 39]. An important
interactionof mTOR inhibitors is with cyclosporine, with
simultaneousadministration leading to increases in blood levels of
mTORinhibitor [42, 43], although this appears to be more
pro-nounced with sirolimus than with everolimus, necessitatingthe
administration of sirolimus 4 hours after cyclosporine[38, 39].
Initial enthusiasm for the use of mTOR inhibitors in
livertransplantation was tempered when the FDA issued a blackbox
warning for de novo sirolimus use in liver transplantationafter two
studies reported hepatic artery thrombosis (HAT)[38, 44]. In 2009,
the FDA issued a second black boxwarning, after a trial that
compared conversion from CNIs tosirolimus versus continued CNI use
showed that the numberof deaths (3.8% (15/393) versus 1.4% (3/214))
was higherin the conversion group, although this was not
significant.In addition, the rates of premature study
discontinuation,overall adverse events (specifically infections),
and biopsy-proven acute liver graft rejection at 12 months were
allsignificantly higher in the conversion group compared to
thegroup continuing with CNIs [38]. Unfortunately, it was notuntil
recently that the complete data that led to thesewarningswere
published [45] allowing them to be properly scrutinized[46].
Notwithstanding the warnings, the Scientific Registryof Transplant
Recipients (SRTR) indicates that between 1999and 2008 in the US,
sirolimus and everolimus were used in8.8% and 0.2% of liver
transplant recipients, respectively, asmaintenance therapy from the
period of discharge to 1 yearafter transplantation [47]. Given the
large amount of dataavailable on the use of mTOR inhibitors in
liver transplanta-tion and the controversy surrounding the black
boxwarnings,we have revisited the use of mTOR inhibitors in liver
trans-plantation. To this end, we searched the literature from
2001to 2012 to determine whether the clinical evidence supportsa
role for this class of immunosuppression with respect toefficacy,
safety, and the ability to address unmet clinical needs.
-
Journal of Transplantation 3
Cell membrane
Interleukin-15Interleukin-2
Anti-CD25mAb
Anti-CD154mAb
Sirolimus,everolimus
CTLA-4-lg
Antigen
CalcineurinMAP kinases
IKK
NFAT AP-1 NF-𝜅B
Costimulation
Antigen-presenting cell
T cell
MHC/peptides
Signal 1
Signal 2
Signal 3
TCR/CD3
PI-3K
Nucleus mRNA
JAK3JAK3
PI-3K
PI-3K
Nucleotidesynthesis
G2Cellcycle
S
M
G1
mTORSynap
se
JAK3
Anti-CD3mAb
inhibitor
MPA
CD52(depletion)
Cellmembrane
Cyclosporine,tacrolimus
CD80, 86
CD154
CD25CD40
CD28
Anti-CD52mAb
CDK/cyclins
Azathioprine
Figure 1: Sites of action of immunosuppressive drugs (adapted
from [33] with permission).
2. Methods
2.1. Identification of Published Clinical Data regarding the
UseofmTOR Inhibitors in Liver Transplantation. We searched
thebibliographic database, PubMed, for studies published
fromJanuary 2001 to April 2012.The following search criteria
wereused in the PubMed search: “everolimus liver transplanta-tion”
OR “sirolimus liver transplantation” OR “everolimusliver
transplant” OR “sirolimus liver transplant.” Prospec-tive or
retrospective clinical studies and reviews of singletransplantation
centers were considered. We only includedstudies that met the
following criteria: (1) focus on adultliver transplant recipients
receiving immunosuppressionwithmTOR inhibitors, (2) publication in
English, and (3) a patientsample size of at least 𝑛 = 7 in the mTOR
inhibitortreatment group. The studies identified were not
subjectedto a systematic review but are summarized and
discussedbased on the combined clinical experience of the authors.
DrKlintmalm has been involved in the use of mTOR inhibitorsin over
1,500 patients at the Simmons Transplantation Insti-tute at Baylor
University Medical Center, including 650 livertransplant recipients
converted to an mTOR inhibitor, 525liver transplant recipients who
received de novo therapy, andover 375 kidney transplant recipients.
Professor Nashan hasbeen using mTOR inhibitors (both de novo and
conversion)in liver and renal transplantation for the last 17 years
and inthat time has been involved in numerous key clinical trials
ofmTOR inhibitors for both indications.
2.2. Identification of Pertinent Studies Presented at
RecentLiver Transplant Congresses. Weretrieved abstracts
reporting
results from trials pertaining to liver transplantation
andeverolimus or sirolimus that were presented at the
followingcongresses: the American Transplant Congress, 2011;
The62nd and 63rdAnnualMeetings of the AmericanAssociationfor the
Study of Liver Diseases (AASLD), 2011 and 2012; 15thCongress of the
European Society for Organ Transplantation,2011; 23rd International
Congress of the TransplantationSociety, 2010; the 2011 Joint
International Congress of theInternational Liver Transplantation
Society (ILTS); the Euro-pean Liver and Intestine Transplant
Association; the LiverIntensive Care Group of Europe.
2.3. Identification of Ongoing Clinical Trials on the Useof mTOR
Inhibitors in Liver Transplantation. The onlinedatabase
ClinicalTrials.gov was searched for ongoing clinicaltrials
investigating mTOR inhibitors in liver transplantation.
2.4. Organization of Studies by Dosage Level and DosingStrategy.
We divided the studies according to their statedmode of mTOR
inhibitor administration, that is, de novo(given from the time of
transplantation) or conversion(where liver transplant recipients
were converted to anmTORinhibitor). In a small number of studies
mTOR inhibitorswere not given de novo but at some point after
transplantationwithout the previous immunosuppression being stated;
theseare termedmaintenance.We further classified the
conversionstudies according to whether sirolimus or everolimus
wasstarted “early” or “late,” because evidence suggests that
thetimepoint at which conversion takes place has an impacton renal
function [10]. NODM and hypertension are alsoassociated with the
use of CNIs (see Introduction 1), so
-
4 Journal of Transplantation
early conversion would also be expected to have a positiveimpact
on these endpoints. We defined early conversion asadministration of
anmTOR inhibitor at 3months or less aftertransplant and late
conversion as conversion after 3 monthsafter transplant, in line
with other studies [48–50]. All studieswere also classified
according to a scoring system taking intoaccount mTOR inhibitor
dosage level and the strength ofthe study design. Dosage level was
included in the scoringsystem since serious adverse events appear
to be associatedwith higher doses of sirolimus and everolimus [44,
45, 51, 52].We therefore based our dosage cut-off points on levels
thatare associated with less serious adverse events [46, 52]. For
denovo and maintenance studies, the following criteria scoredone
point each: (a) inclusion of a control arm; (b) sirolimusor
everolimus dose of ≤2mg/day; and (c) serum levels of≤10 ng/mL for
sirolimus or ≤12 ng/mL for everolimus. Inthe case of conversion
studies, the following criteria scoredone point each: (a) a
predefined conversion timepoint of ≤3months after transplantation;
(b) inclusion of a control arm;(c) specified dose of mTOR inhibitor
(see above); and (d)specified serum level of mTOR inhibitor (see
above). Thestudies were then classified as low (0-1 point), medium
(2points), or high (≥3 points) quality.
3. Results
Our literature search retrieved 40 studies on sirolimus useand
16 studies on everolimus use (Tables 1(a)–1(d)). Weanalyzed these
studies according to renal function, efficacy,safety, metabolic
syndrome, HCC, neurological symptoms,HCV recurrence/fibrosis
progression, and de novo tumors.
3.1. Efficacy of mTOR Inhibitors
3.1.1. Sirolimus. A retrospective study evaluating the use of
denovo sirolimus versus CNIs found that patients who
receivedsirolimus (𝑛 = 252) exhibited similar rates of patient and
graftsurvival in comparison to liver transplant recipients
receivingCNIs (𝑛 = 291). The percentage of patients who
developedacute cellular rejection or those with BPAR was
significantlylower in patients receiving sirolimus compared with
thoseon CNIs (Table 2(a)) [53]. In a large retrospective studythat
included de novo sirolimus use in liver transplantationcompared
with a CNI control group there were no significantdifferences in
rates of mortality or graft loss during the firstyear after liver
transplant (Table 2(a)) [54].
In a high quality retrospective study assessing conversion(early
versus late conversion), rejection rates in the sirolimusgroups
(early conversion: 35%; late conversion: 38%) werecomparable to
those in the CNI group (43%) [48]. In anotherretrospective study
assessing conversion (medium quality),BPAR among patients converted
at various times was 3.4%[67], while a medium quality review of a
prospectivelymaintained database revealed an acute cellular
rejection rateof 17.2% for those treated de novo with sirolimus
versus 2.8%for those converted at various timepoints to sirolimus
inresponse to rising serum creatinine concentrations [69].
Two single-arm prospective studies and one random-ized study
(Table 2(a)) have shown that late conversion tosirolimus in liver
transplant recipients is associated withgenerally low rates of
acute rejection: 4.8% [83], 6.7% [82]and 7.7% [78]. In addition, a
high quality retrospective studydemonstrated low rates of acute
rejection: 5% among patientsconverted to sirolimus versus 4% for
matched control groupmaintained on reduced-dose CNIs alone [72].
However, in alarge, prospective randomized trial in which liver
transplantrecipients were converted late (more than 50% of patients
ineach group entered the study at least 3 years
posttransplan-tation) and abruptly (within 24 hours) from CNI
treatmentto sirolimus, there were detrimental effects on efficacy
andsafety, suggesting that an overlap period is necessary [45].The
rate of BPAR (11.7% versus 6.1%) at 12 months afterrandomization (𝑃
= 0.02) and overall treatment failure (acutecellular rejection or
discontinuation; 48.3% versus 26.7%;𝑃 < 0.001) was significantly
higher in the sirolimus groupcompared to the control group who
received CNI for upto 6 years. In addition, significantly more
patients in thesirolimus group experienced ≥1 treatment-emergent
adverseevent during the study compared to the CNI group (𝑃 =0.005)
[45].
3.1.2. Everolimus. In a study in which de novo liver
transplantrecipients were randomized to receive cyclosporine
pluseverolimus (𝑛 = 89) at either 1, 2 or 4mg per day, BPAR
rateswere 32.1%, 26.7%, and 25.8%, respectively, versus 40% forthe
30 patients receiving cyclosporine plus placebo, althoughthis
difference was not significant [52]. There was evidenceof a dose
relationship for treated acute rejection throughoutthe double-blind
study period, with higher rates of acuterejection observed in
patients on lower doses of everolimus(particularly the lowest dose
of 1mg/day). In this study, therewere few deaths with patient
survival reported as 83.3%,82.1%, 96.7%, and 87.1% in liver
transplant recipients whoreceived placebo or everolimus at 1, 2, or
4mg per dayrespectively; no deaths were considered to be
treatment-related [52]. Rejection rates at 1 year after
transplantation ina prospective, randomized study in which patients
receivedeither de novo everolimus or tacrolimus were 11% versus
3%,respectively [88]. In a high quality maintenance study inwhich
liver transplant recipients were randomized at 1 monthafter
transplant to either everolimus-facilitated eliminationof
tacrolimus, everolimus-facilitated reduction of tacrolimus,or
standard-dose tacrolimus, withdrawing tacrolimus didnot provide
sufficient efficacy with a BPAR rate of 19.9%(although everolimus
did allow substantial tacrolimus reduc-tion in de novo liver
transplant recipients while resulting in asignificantly lower rate
of BPAR at 1 year) [87].
In five early conversion studies (Table 2(b)), all of whichwere
high quality, prospective, randomized trials, efficacywaseither
similar to [50, 89, 91] or better than [87, 90] controlgroups. One
of these investigated whether everolimus couldbe used to withdraw
or reduce immunosuppression withtacrolimus in de novo liver
transplant recipients [87]. Theresults of this study showed that
withdrawing tacrolimus didnot provide sufficient efficacy with a
BPAR rate of 19.9%.
-
Journal of Transplantation 5
Table1:(a)Sirolim
ustrials(den
ovoa
ndmaintenance
dosin
g)retrievedfro
mPu
bMed/con
gresssearch,(b)siro
limus
conversio
ntrialsretrievedfro
mPu
bMed/con
gresssearch,(c)everolim
ustrials(den
ovodo
sing)
retrievedfro
mPu
bMed/con
gresssearch,(d)e
verolim
usconversio
ntrialsretrievedfro
mPu
bMed/con
gresssearch.
(a)
Participants
Stud
ydesig
naDurationof
study
Sirolim
usdo
sing
Streng
thof
study
desig
nbased
ondefin
edcriteria
b
Den
ovodo
sing
Chinnakotla
etal.LiverTran
spl.
2009;15:1834–4
2[55]
𝑁=227recipients
(i)𝑛=121(SRL
)(ii)𝑛=106(TAC
)R/P
5years
2mgorally,
once
daily.Levels
maintained
at5–8n
g/mLforthe
first3mon
thsa
ndat
5ng/mLthereafte
rHigh
Asthanae
tal.Ca
nJ
Gastro
enterol.2011;25:28–34
[56]
𝑁=141recipients
(i)𝑛=88
(den
ovoSR
L)(ii)𝑛=53
(CNI)
R12
mon
ths
Maintainedat8–12ng
/mL
Medium
McK
enna
etal.A
mJT
ranspl.
2011;11:2379–87[57]
𝑁=455recipients
(HCV
-positive)
(i)𝑛=173(SRL
)(ii)𝑛=282(SRL
-free)
R/P
2years
2mgdaily
with
outa
loadingdo
sebeginn
ingon
thefi
rstp
ostoperativ
eday
Medium
Wagnere
tal.Int
Immun
opharm
acol.2010;10:
990–
3[58]
𝑁=67
recipients
(HCV
-positive)
(i)𝑛=39
(SRL
)(ii)𝑛=28
(CNI)
P,C
12mon
ths
Trou
ghlevelswerem
aintainedbetween3
and8n
g/mL
Medium
Zhou
etal.TransplantP
roc.2008;
40:3548–553[59]
𝑁=73
recipients(H
CCexceedingMilancriteria
)(i)𝑛=27
(SRL
)(ii)𝑛=46
(TAC
)
R2years
Given
1mon
thaft
ertransplant:initia
ldo
seof
3mg/m
2adjuste
dover
timeto
achieves
teady-sta
tetro
ughlevelsof
≈5–8n
g/mL
Medium
Asthanae
tal.Presentedat
AASLD2011(A
bstract184)[60]
𝑁=100recipients(recurrent
HCV
)(i)𝑛=40
(SRL
)(ii)𝑛=35
(TAC
)(iii)𝑛=24
(cyclosporine)
(iv)𝑛=36
lostto
follo
wup
P,C
Medianof
77.6
mon
ths
Not
stated
Low
-
6 Journal of Transplantation
(a)Con
tinued.
Participants
Stud
ydesig
naDurationof
study
Sirolim
usdo
sing
Streng
thof
study
desig
nbased
ondefin
edcriteria
b
Campsen
etal.J
Tran
splant.2011;
2011:913094[54]
𝑁=672recipients
(i)𝑛=328(C
NI+
MPS
attim
eof
discharge)
(ii)𝑛=135(C
NI+
MPS
attim
eof
discharge;SR
Laddedwith
inthefi
rst6
mon
thsa
ndcontinued
throug
hthefi
rstyear)
(iii)𝑛=15
(CNI+
MPS
attim
eof
discharge;SR
Lwas
added
with
inthefi
rst6
mon
thsa
nddiscon
tinuedbefore
thefi
rst
year)
(iv)𝑛=156(SRL
asprim
ary
immun
osup
pressio
n)(v)𝑛=38
(SRL
asprim
ary
immun
osup
pressio
nand
discon
tinuedbefore
thefi
rst
year)
R1y
ear
Not
stated
Low
Dun
kelbergetal.LiverTran
spl.
2003;9:463–8
[61]
𝑁=350recipients
(i)𝑛=170(SRL
)(ii)𝑛=180(historiccontrols)
R12
mon
ths
6mgon
day0,and2m
g/daythereafte
rno
targetlevelw
asspecified
Low
Jiménez-Rom
eroetal.
Hepatogastro
enterology.2011;58:
115–21
[62]
𝑁=16
recipientswho
developed
denovo
tumors
Allsw
itchedfro
mCN
I/MMF
toSR
Lmon
otherapy
P,S
Meanof
15.7mon
ths
Loadingdo
se:4
mg,follo
wed
by2m
g/day
until
8–12
days,thereaft
erdo
seadjuste
dto
achievetargetb
lood
levelof
5–10ng
/mL
Low
Knetem
anetal.LiverTran
spl.
2004;10:1301–11[63]
𝑁=40
recipients(H
CC)
AllgivenSR
LP,S
4years
Adjuste
dto
achievetargetlevels
of12–20n
g/mL
Low
Maram
attom
and
Wijd
icksNe
urology.2004;63:
1958–9
[64]
𝑁=202recipients
Allreceived
SRL
R18
mon
ths
Loadingdo
se:6
mg,thereafte
r:1–10mg/daywith
targetbloo
dlevelof
8–15ng
/mL
Low
Molinarietal.Tran
splIntl.2010;
23:155–6
8[53]
𝑁=543recipients
(i)𝑛=252(SRL
)(ii)𝑛=291(C
NI)
R5years
Orald
osea
djustedto
keep
theb
lood
levelsin
ther
ange
of10–15n
g/mLdu
ring
thefi
rst3–6
mon
thsa
ndthen
inthe
rangeo
f5–10n
g/mLaft
erwards
Low
Toso
etal.H
epatology.2010;51:
1237–4
3[65]
𝑁=2491
recipients(H
CC)
(i)𝑛=109(SRL
)(ii)𝑛=2382
(SRL
-free)
R5years
Not
stated
Low
-
Journal of Transplantation 7
(a)Con
tinued.
Participants
Stud
ydesig
naDurationof
study
Sirolim
usdo
sing
Streng
thof
study
desig
nbased
ondefin
edcriteria
b
Wiesner
etal.A
mJT
ransplant.
2002;2
(s3):464
(Abstract1294)
[44]
𝑁=163recipients
(i)𝑛=111(SRL
+Cs
A)
(ii)𝑛=52
(con
centratio
n-controlledTA
C(tr
ough
levels5–15ng
/mL)
+corticosteroids)
P,Ra
6mon
ths
Fixed-do
seof
5mg/day
Low
Zimmerman
etal.LiverTran
spl.
2008;14:633–8[15]
𝑁=97
recipients(cirr
hosis
+concom
itant
HCC
)(i)𝑛=45
(SRL
)(ii)𝑛=52
(stand
ardregimen
inclu
ding
CNIs,M
MF,and
corticosteroids)
R5years
Bolusd
oseo
f6mgon
day0andgivenon
2mg/daythereafte
rLo
w
Com
binatio
nof
denovo
andmaintenance
dosin
g
Kazimietal.Tran
splantation.
2010;90(2S):697
(Abstract1950)
[66]
𝑁=114recipients
(i)𝑛=65
(SRL
)(ii)𝑛=49
(CNI)
R1111±800days
Not
stated
Low
(b)
Participants
Stud
ydesig
naDurationof
study
Sirolim
usdo
sing
Streng
thof
study
desig
nbased
oncriteria
b
Early
conversio
n(≤3mon
thsa
ftertransplantatio
n)
Rogersetal.C
linTran
splant.
2009;23:887–96
[48]
𝑁=82
recipients
(i)𝑛=42
(SRL
)(ii)𝑛=40
(CNI)
R12
mon
ths
TargetSR
Llevelsforthe
firstthree
mon
thsa
fterc
onversionwere8
–10n
g/dL
,6–
8ng/dL
form
onths3
–6,and
5–6n
g/dL
after
mon
th12
High
Harpere
tal.Tran
splantation.
2011;91:128–32
[67]
𝑁=148recipients
Allconvertedto
SRL
RMedianof
1006
days
Con
versionfro
mCN
ItoSR
Lperfo
rmed
with
anoverlap
.SRL
givenat2m
g/day
andCN
Iwith
draw
nwhenSR
Lreached
5–8n
g/mL
Medium
McK
enna
etal.ILT
S.2011
(AbstractO
-17)
[68]
𝑁=1078
recipients
(i)𝑛=202(SRL
)(ii)𝑛=876(SRL
-free)
R10
years
Not
stated
Medium
-
8 Journal of Transplantation(b)Con
tinued.
Participants
Stud
ydesig
naDurationof
study
Sirolim
usdo
sing
Streng
thof
study
desig
nbased
oncriteria
b
Schleicher
etal.TransplantP
roc.
2010;42:2572–5
[49]
𝑁=57
recipients
(i)𝑛=11
(earlyconversio
n,im
paire
dperio
perativ
erenal
functio
n;SR
L=7,EV
L=4)
(ii)𝑛=7(earlyconversio
n,no
rmalperio
perativ
erenal
functio
n;SR
L=6,EV
L=1)
(iii)𝑛=23
(lateconversio
n,im
paire
dperio
perativ
erenal
functio
n,SR
L=15,E
VL=8)
(iv)𝑛=16
(lateconversio
n,no
rmalperio
perativ
erenal
functio
n;SR
L=12,E
VL=4)
R12
mon
ths
Initialdo
seof
10mg/day.Doses
were
adjuste
dsuccessiv
elyto
maintaintro
ugh
levelsof
5–10ng
/mL
Medium
Sancheze
tal.Tran
splant
Proc.
2005;37:44
16–23[69]
𝑁=64
recipients
(i)𝑛=29
(denovoSR
L)(ii)𝑛=35
(con
versionSR
L)P,C
2years
Inrecipientswith
HCC
orautoim
mun
edisorders,SR
Ldo
sesu
sedweretypically
either
a5mgor
3mgloadingdo
sefollo
wed
by2m
geach
day
Afte
rcon
version,
SRLlevelswere
maintainedat10–15n
g/mLwhenused
with
in3mon
thso
ftransplantatio
nandat
5–10ng
/mLaft
er3mon
thsa
fter
transplantation
Medium
Forgacse
tal.Tran
splant
Proc.
2005;37:1912–4
[70]
𝑁=7recipients
Allconvertedto
SRL
RUpto
425days
Not
stated
Low
Lateconversio
n(>3mon
thsa
ftertransplantatio
n)
Campb
elletal.Clin
Tran
splant.
2007;21:377–84
[71]
𝑁=179recipients
(i)𝑛=79
(SRL
conversio
n)(ii)𝑛=100(C
NIcon
trols)
RMedianof
359days
2mgdaily,dosea
djustedun
tiltarget
levelsof
5–8n
g/mLachieved
High
DuB
ayetal.LiverTran
spl.2008;
14:651–9
[72]
𝑁=114recipients(w
ithrenal
insufficiency)
(i)𝑛=57
(SRL
)(ii)𝑛=47
(low-doseC
NIs)
R12
mon
ths
Recipientson
CNIm
onotherapy
were
startedon
SRL1m
g/dayandtheC
NI
dose
was
halved.A
t1week,theC
NIw
assto
pped,and
theS
RLdo
sewas
adjuste
don
theb
asisof
thes
erum
levels.
For
recipientson
combinatio
ntherapy,the
CNIw
assto
pped,and
SRLwas
started
onthes
amed
ayat2m
g/daywhilethe
antim
etabolite
orste
roid
dosesw
ere
maintainedattheirc
urrent
levels.
Inbo
thgrou
pstheS
RLdo
sewas
adjuste
dto
maintaintro
ughlevelsof
5–15𝜇g/day
High
-
Journal of Transplantation 9
(b)Con
tinued.
Participants
Stud
ydesig
naDurationof
study
Sirolim
usdo
sing
Streng
thof
study
desig
nbased
oncriteria
b
Herlenius
etal.TransplantP
roc.
2010;42:44
41–8
[73]
𝑁=25
recipients(w
ithchronic
kidn
eydisease)
(i)𝑛=12
(SRL
)(ii)𝑛=13
(MMF)
P,Ra
12mon
ths
Asin
gleb
olus
dose
of10mgSR
Lfollo
wed
bythreec
onsecutiv
edailydo
seso
f8mg.
Targettro
ughconcentrationof
10ng
/mL
Medium
Lam
etal.D
igDisSci.2004;49:
1029–35[74]
𝑁=28
recipients(w
ithrenal
insufficiency
after
transplantation)
Allconvertedto
SRL
P,S
Meanof328±57
days
SRLinitiated
at2m
g/day.Doses
adjuste
dto
achievetargetlevelof
4–10ng
/mL
Medium
Morardetal.LiverTran
spl.2007;
13:658–6
4[75]
𝑁=48
recipients
(i)𝑛=16
(SRL
)(ii)𝑛=19
(SRL
+MMF)
(iii)𝑛=7(SRL
+prednisone)
(iv)𝑛=2(SRL
+CN
I)(v)𝑛=4(SRL
+MMF+
prednisone)
RMedianof22.6±11
mon
ths
Loadingdo
se:6
mg(day
1)follo
wed
by2m
g/day(day
2–7).SRL
dose
adjuste
dto
maintaintro
ughlevelsof
5–10ng
/mL
Medium
Shenoy
etal.Transplantatio
n.2007;83:1389–92[76]
𝑁=40
recipients(w
ithrenal
dysfu
nctio
n)(i)𝑛=20
(SRL
)(ii)𝑛=20
(CNI)
P,Ra
12mon
ths
5mgloadingdo
se,followed
by3m
gSR
Lon
cedaily.L
evels
maintained6–
10ng
/mL
Medium
Uhlmannetal.E
xpClin
Tran
splant.2012;10:30–
8[77]𝑁=25
recipients
Allconvertedto
SRL
P,S
75.6mon
ths
SRLsta
rted
at1m
g/day,do
seadjuste
dto
maintaintro
ughlevelsat69
ng/m
LMedium
Watsonetal.LiverTran
spl.2007;
13:1694–
702[78]
𝑁=27
recipients
(i)𝑛=13
(SRL
)(ii)𝑛=14
(CNI)
P,Ra
12mon
ths
CNIw
asdiscon
tinuedthee
vening
before
conversio
n,andrecipientsweres
tarted
on2m
g/daySR
Lon
thefollowingday.
Targetrangeo
f5–15n
g/mL
Medium
Steinetal.P
resented
atthe
American
Transplant
Con
gress
2011(A
bstract8
17)[79]
𝑁=40
recipients(received
transplant
forH
CV)
(i)𝑛=18
(SRL
conversio
n)(ii)𝑛=22
(TAC
)
R5years
Not
stated
Low
Vivarelli
etal.TransplantP
roc.
2010;42:2579–8
4[80]
𝑁=78
recipients
(i)𝑛=38
(SRL
)(ii)𝑛=40
(SRL
+CN
I)R
510±366days
5mg/m
2for1stday,then
2mg/daily,
adjuste
dto
troug
hbloo
dlevel<
10ng
/mL
Low
DiB
enedetto
etal.Transplant
Proc.200
9;41:1297–9[81]
𝑁=31
recipients
Allconvertedto
SRL
RMeanof
27.5mon
ths
(range:2–71.2
mon
ths)
SRLataloading
dose
of0.1m
g/kg
onday
1ofthe
switch,then
0.05
mg/kg
forthe
next
fewdays.D
osea
djustedto
maintain
troug
hlevelsof
8–10ng
/mL
Low
-
10 Journal of Transplantation
(b)Con
tinued.
Participants
Stud
ydesig
naDurationof
study
Sirolim
usdo
sing
Streng
thof
study
desig
nbased
oncriteria
b
Abdelm
alek
etal.A
mJ
Tran
splant.2012;12:694–705
[45]
𝑁=607recipients
(i)𝑛=393(SRL
conversio
n)(ii)𝑛=214(C
NIcon
tinuatio
n)P,Ra
Upto
6years
Loadingdo
seof
SRL:10–15m
g.Firstd
ose
given≥4h
after
thelastC
NId
ose;second
dosesg
iven
12hlater.Onstu
dydays
2–6,
SRLdo
seso
f3–5
mg/daywereg
iven.
Thereafter,SR
Ldo
sesm
aintainedto
achieveb
lood
levelsof
6–16ng
/mL
(chrom
atograph
ic)a
ndsubsequentlyto
8–16ng
/mL(chrom
atograph
ic)o
r10–20n
g/mL(im
mun
oassay)
Low
Bäckman
etal.C
linTran
splant.
2006;20:336–
9[82]
𝑁=15
recipients
Allconvertedto
SRL
P,S
6mon
ths
Loadingdo
seof
15mgSR
Lon
days
1and
2,then
8mg/dayandadjuste
dto
achieve
troug
hlevelsof
13–22and10–22n
g/mL
Low
Fairb
anks
etal.LiverTran
spl.
2003;9:1079–
85[83]
𝑁=21
recipients(develop
edrenald
ysfunctio
nwhileon
CNI
therapy)
Allconvertedto
SRL
P,S
Meanof66.8±38.9
weeks
Initially1-2
mg/dayandincreasedweekly
by1m
gto
achievetherapeuticlevels
(9–12n
g/mL)
Low
Naire
tal.LiverT
ranspl.2003;9:
126–
9[84]
𝑁=16
recipients
Allconvertedto
SRL
R6mon
ths
Loadingdo
seof
5mgon
day1,follo
wed
by2m
g/day.Atro
ughlevelof
5–10ng
/mLwas
maintained
Low
Neff
etal.TransplantP
roc.2003;
35:3029–
31[85]
𝑁=14
recipients
Allconvertedto
SRL
R90
days
Meansta
rtingdo
seof
SRL(10m
g/day)
adjuste
dto
maintaintro
ughlevelsof
8–12ng
/mLdu
ringfirstmon
thand
subsequently3–5n
g/mLforrecipientso
nmaintenance
combinatio
ntherapywith
SRL
Low
Wadeietal.Transplantatio
n.2012;93:1006–12[86]
𝑁=102recipients
Allconvertedto
SRL
RMedianof
3.1y
ears
CNId
oser
educed
by50%un
tiltarget
SRLlevelof8–12n
g/mLachieved
Low
Search
term
swere“sirolim
usliver
transplantation”
OR“siro
limus
liver
transplant.”
CNI:calcineurin
inhibitor;HCC
:hepatocellularc
arcino
ma;HCV
:hepatitisC
virus;ILTS
:2011Joint
InternationalC
ongresso
fthe
InternationalL
iver
TransplantationSo
ciety;MMF:mycop
heno
latem
ofetil;SR
L:sirolim
us;TAC
:tacrolim
us.
a Study
desig
n:C:
coho
rt;P
:prospectiv
e;R:
retro
spectiv
e;Ra
:rando
mized;S:single-arm.
b See
Section2ford
escriptio
nof
howcriteria
ared
efined.
-
Journal of Transplantation 11(c)
Participants
Stud
ydesig
naStud
ydu
ratio
nEv
erolim
usdo
sing
Streng
thof
study
desig
nbased
oncriteria
b
DeS
imon
eetal.Am
JTransplant.
2012;12:3008–20[87]
𝑁=719recipients
(i)𝑛=245(EV
R+TA
C-RD
)(ii)𝑛
=231(EV
R+TA
C-WD)
(iii)𝑛=243(TAC
-SD)
P,Ra
12mon
ths
ForE
VR+TA
C-WD,E
VRinitiated
ata
dose
of1.0
mgb.i.d
.with
in24
hof
rand
omizationwith
thed
osea
djusted
from
day5on
ward,to
maintainC0
3–8n
g/mLun
tilmon
th4aft
ertransplantation,
after
which
thetarget
rang
eincreased
to6–
10ng
/mL
IntheE
VR+TA
C-RD
arm,EVRinitiated
andmon
itoredas
forE
VR+TA
C-WD,
butthe
initialtargetrangeo
f3–8
ng/m
Lmaintainedthroug
hout
thes
tudy
High
Grazietal.P
resented
atILTS
;2011(A
bstractP
-256)[88]
𝑁=64
recipients(H
CV-related
cirrho
sis)
(i)𝑛=28
(EVR+Bm
ab+
steroids)
(ii)𝑛=36
(TAC
+Bm
ab+
steroids)
P,Ra
1year
Not
stated
Low
Levy
etal.Liver
Transpl.2006;
12:164
0–8[52]
𝑁=119recipients
(i)𝑛=28
(EVR1.0
mg)
+CN
I(ii)𝑛=30
(EVR2.0m
g)+CN
I(iii)𝑛=31
(EVR4.0m
g)+CN
I(iv
)𝑛=30
(placebo
)+CN
I
P,Ra
36mon
ths
1,2or
4mg/day
Low
Search
term
swere“everolim
usliver
transplantation”
OR“everolim
usliver
transplant.”
Maintenance
therapyrefersto
immun
otherapy
forthe
lifetim
eofthe
graft
.Con
versiontherapyiswhere
liver
transplant
recipientswerew
ithdraw
nfro
mCN
Isandsw
itchedto
everolim
us.
Bmab:basiliximab;C
NI:calcineurin
inhibitor;EV
R:everolim
us;H
CV:hepatitisC
virus;SR
L:sirolim
us;TAC
:tacrolim
us.
a Study
desig
n:P:
prospective;R:
retro
spectiv
e;Ra
:rando
mized.
b See
Section2ford
escriptio
nof
howcriteria
ared
efined.
(d)
Participants
Stud
ydesig
naStud
ydu
ratio
nEv
erolim
usdo
sing
Streng
thof
study
desig
nbased
oncriteria
b
Early
conversio
n(≤3mon
thsa
ftertransplantatio
n)
DeS
imon
eetal.Am
JTransplant.
2012;12:3008–20[87]
𝑁=719recipients
(i)𝑛=245(EVR+TA
C-RD
)(ii)𝑛=231(EV
R+TA
C-WD)
(iii)𝑛=243(TAC
-SD)
P,Ra
12mon
ths
ForE
VR+TA
C-WD,E
VRinitiated
ata
dose
of1.0
mgb.i.d
.with
in24
hof
rand
omizationwith
thed
osea
djusted
from
day5on
ward,to
maintainC0
3–8n
g/mLun
tilmon
th4aft
ertransplantation,
after
which
thetarget
rang
eincreased
to6–
10ng
/mL.
IntheE
VR+TA
C-RD
arm,EVRinitiated
andmon
itoredas
forE
VR+TA
C-WD,
butthe
initialtargetrangeo
f3–8
ng/m
Lmaintainedthroug
hout
thes
tudy
High
-
12 Journal of Transplantation
(d)Con
tinued.
Participants
Stud
ydesig
naStud
ydu
ratio
nEv
erolim
usdo
sing
Streng
thof
study
desig
nbased
oncriteria
b
Fischere
tal.Am
JTransplant.
2012;12:1855–6
5[50]
𝑁=203recipientson
CNI
with
/out
corticosteroids
(i)𝑛=101(EVR)
(ii)𝑛=102(C
NIcon
tinuatio
n)
P,Ra
12mon
ths
EVRsta
rted
at1.5
mgb.i.d
.and
adjuste
dto
achievea
targettro
ughlevelof
5–12ng
/mL(8–12n
g/mLin
patie
ntso
ntre
atmentw
ithCs
A),whenCN
Iwas
taperedby
70%of
theinitia
lCNId
ose
High
Masettietal.A
mJT
ransplant.
2010;10:2252–6
2[89]
𝑁=78
recipients
(i)𝑛=52
(EVR)
(ii)𝑛=26
(CsA
)P,Ra
12mon
ths
Initialdo
se:2.0mg/day,tro
ughlevelof
6–10ng
/mL.WhenCs
Adiscon
tinued,
troug
hlevel:8–12ng
/mLun
tilendof
mon
th6and6–
10ng
/mLthereafte
r
High
Salib
aetal.AASLD2012
[90]
𝑁=719recipientsfro
mDe
Simon
eetal.Am
JTransplant.
2012
[40]
(i)𝑛=245(EVR+TA
C-RD
)(ii)𝑛=231(EVR+TA
C-WD)
(iii)𝑛=243(TAC
-SD)
P,Ra
24mon
ths
Samea
sDeS
imon
eetal.Am
JTran
splant.2012[40]
High
Schlitt
etal.A
ASLD2012
[91]
𝑁=81
recipientsfro
mFischere
tal.A
mJT
ransplant.2012
(i)𝑛=41
(EVRwith
/out
corticosteroids)
(ii)𝑛=40
(CNIw
ith/out
corticosteroids)
P,Ra
35mon
ths
Samea
sFisc
here
tal.Am
JTransplant.
2012
[43]
High
Lateconversio
n(>3mon
thsa
ftertransplantatio
n)
Bilbao
etal.T
ransplantP
roc.
2009;41:2172–6
[92]
𝑁=25
recipients
Allconvertedto
EVR
RMeanof10±9
mon
ths
Inrefractory
rejection:
initialdo
se0.5m
g/12h.Trou
ghlevels5n
g/mL.Fo
rCN
I-relatedadversee
vents,EV
Rsta
rted
at0.5m
gon
ceor
twicea
day.Fo
rmalignancy,EV
Rintro
ducedat
0.5m
g/day,adjusting
troug
hlevelsto
<3n
g/mL
Medium
Casano
vase
tal.Tran
splant
Proc.
2011;43:2216–9
[93]
𝑁=35
recipients
Allconvertedto
EVR
P,S
Meanof
134mon
ths
Initialdo
se0.25
mg/12hforthe
first4
days.Targettroug
h3–5n
g/mL
Medium
Castr
oagudı́netal.LiverTran
spl.
2009;15:1792–7
[94]
𝑁=21
recipients(chron
icrenal
dysfu
nctio
n)Allconvertedto
EVR
P,S
Medianof
19.8
mon
ths
0.75
mgb.i.d
.,with
targettro
ughlevelsof
3–8n
g/mL
Medium
-
Journal of Transplantation 13
(d)Con
tinued.
Participants
Stud
ydesig
naStud
ydu
ratio
nEv
erolim
usdo
sing
Streng
thof
study
desig
nbased
oncriteria
b
DeS
imon
eetal.Tran
splInt.
2009;22:279–
86[95]
𝑁=40
recipients
P,S
12mon
ths
EVR1.5
mg/day.Trou
ghlevelof
3–8n
g/mL
Medium
DeS
imon
eetal.LiverT
ranspl.
2009;15:1262–9
[96]
𝑁=145recipients
(i)𝑛=72
(EVRtherapywith
CNIreductio
nor
discon
tinuatio
n)(ii)𝑛=73
(CNIcon
tinuatio
n)
P,Ra
12mon
ths
Initial:3
mg/day×2on
day1.Afte
rweek
2:EV
Rtro
ughlevelm
aintainedat
3–8n
g/mLdu
ringconcom
itant
CNI
administratio
nand6–
12ng
/mLifCN
Ielim
inated
Medium
Bilbao
etal.P
resented
atILTS
;2011(A
bstractP
-68)
[97]
𝑁=62
recipients
Allreceived
EVR
RMedianof
12mon
ths
EVRtro
ughlevelat∼
3ng/mL
Low
Salib
aetal.LiverT
ranspl.2011;
17:905–13[98]
𝑁=240maintenance
recipients
Allreceived
EVR
R12
mon
ths
Intro
ducedatmean2.4m
g/day.Th
emeantro
ughlevel=
7.3ng
/mLatmon
th1
and8.1n
g/mLatmon
th12
acrosstotal
popu
lation,
with
high
ervalues
inmon
otherapy
coho
rt(8.8ng
/mLat
mon
th12)
Low
Vallinetal.C
linTran
splant.2011;
25:660–9
[99]
𝑁=94
recipients
Allreceived
EVR
RMeanof12±7
mon
ths
Initialdo
se0.75–1.5mgb.i.d
.Troug
hadjuste
dto
3–8n
g/mL
Low
𝑃values
areincludedwhere
available.
Search
term
swere“everolim
usliver
transplantation”
OR“everolim
usliver
transplant.”
AASLD:A
nnualM
eetin
gsof
theA
merican
Associatio
nforthe
Stud
yof
LiverD
iseases;b.i.d.:twiced
aily;C
NI:calcineurin
inhibitor;Cs
A:cyclosporin
A;E
VR:
everolim
us;ILT
S:2011JointInternatio
nalC
ongress
oftheInternatio
nalL
iver
TransplantationSo
ciety;TA
C:tacrolim
us;TAC
-RD:reduced-dosetacrolim
us;TAC
-SD:stand
ard-do
setacrolim
us;TAC
-WD:tacrolim
uswith
draw
n.a Study
desig
n:P:
prospective;R:
retro
spectiv
e;Ra
:rando
mized;S:single-arm.
b See
Section2ford
escriptio
nof
howcriteria
ared
efined.
-
14 Journal of Transplantation
Table2:(a)E
fficacy
ofsirolim
us,(b)
efficacy
ofeverolim
us.
(a)
Patie
ntsurvivalrate(%
)Graftrejectionrate(%
)Ac
uter
ejectio
nrate(%
)BP
AR(%
)
Acutec
ellularrejectio
nrate
6mon
ths
1year
Crud
emortality
rate/10
00person
-mon
ths
Crud
egraft
failu
rerate/10
00person
-mon
ths
1year
(%)
ACR/1000
person
-mon
ths
Steroid-resistant
rejection/1000
person
-mon
ths
Den
ovodo
sing
Sancheze
tal.
Tran
splant
Proc.2005;
37:4416–
23[69]
17.2
Molinarietal.
Tran
splIntl.2010;23:
155–68
[53]
95versus
94(SRL
versus
CNI)
92versus
91(SRL
versus
CNI)
0versus
0(SRL
versus
CNI)
32.5versus
44.1(SRL
versus
CNI,
𝑃=0.03)
46.7versus
58.9(SRL
versus
CNI,
𝑃=0.003)
Campsen
etal.J
Tran
splant.2011;2011:
913094
[54]
∗Seefoo
tnotefor
grou
ps
2.39
(group
1),
1.96and3.88
(SRL
conversio
ngrou
ps2and3),
1.82and2.13
(SRL
denovo
grou
ps4and5).
AllNS
2.68
(group
1),
2.15
and3.88
(SRL
conversio
ngrou
ps2and3),
1.82and2.13
(SRL
denovo
grou
ps4and5).
AllNS
12.5(group
1),
13.4,12.9(SRL
conversio
ngrou
ps2,3,
𝑃=NSversus
control),
6.5,5.2
(SRL
denovo
grou
ps4,5;𝑃≤
0.0001,𝑃=
0.0007
versus
controls)
3.48
(group
1),
4.29,3.88(SRL
conversio
ngrou
ps2,3,
𝑃=0.03,𝑃=
NSversus
controls),1.58,
1.54(SRL
denovo
grou
ps4,
5;𝑃<
0.001,𝑃=0.04
versus
controls)
Lateconversio
n(>3mon
thsa
ftertransplantatio
n)
DuB
ayetal.Liver
Tran
spl.2008;14:
651–9[72]
5versus
4(SRL
versus
control)
Shenoy
etal.
Tran
splantation.2007;
83:1389–
92[76]
5versus
5(SRL
versus
control)
Watsonetal.Liver
Tran
spl.2007;13:
1694–702
[78]
7.7versus
0(SRL
versus
CNI)
-
Journal of Transplantation 15(a)Con
tinued.
Patie
ntsurvivalrate(%
)Graftrejectionrate(%
)Ac
uter
ejectio
nrate(%
)BP
AR(%
)
Acutec
ellularrejectio
nrate
6mon
ths
1year
Crud
emortality
rate/10
00person
-mon
ths
Crud
egraft
failu
rerate/10
00person
-mon
ths
1year
(%)
ACR/1000
person
-mon
ths
Steroid-resistant
rejection/1000
person
-mon
ths
Abdelm
alek
etal.A
mJT
ransplant.2012;12:
694–
705[45]
(Low
)
93.4versus
94.4(SRL
versus
CNI)
0versus
0(SRL
versus
CNI)
6.4versus
1.9(SRL
versus
CNI)
11.7versus
6.1
(SRL
versus
CNI,
𝑃=0.02)
Bäckman
etal.C
linTran
splant.200
6;20:
336–
9[82]
6.7
DiB
enedetto
etal.
Tran
splant
Proc.200
9;41:1297–9[81]
12.9
Fairb
anks
etal.Liver
Tran
spl.2003;9:
1079–85[83]
4.8
Naire
tal.Liver
Tran
spl.2003;9:
126–
9[84]
0
Con
versiontim
escompared
Rogersetal.Clin
Tran
splant.2009;23:
887–96
[48]
35,38,43
(early,
late
conversio
nSR
Land
CNI)
Varia
blec
onversiontim
es
Harpere
tal.
Tran
splantation.2011;
15;91:128–32
[67]
3.4
Sancheze
tal.
Tran
splant
Proc.2005;
37:4416–
23[69]
2.8
𝑃values
areincludedwhere
available.
ACR:
acutec
ellularrejectio
n;BP
AR:
biop
sy-provenacuter
ejectio
n;CN
I:calcineurin
inhibitor;NS:no
nsignificant;SR
L:sirolim
us.
∗Ke
yto
grou
ps:
(1)C
NI+
MPS
attim
eofd
ischarge.
(2)C
NI+
MPS
attim
eofd
ischarge;SR
Laddedwith
inthefi
rst6
mon
thsa
ndcontinuedthroug
hthefi
rstyear.
(3)C
NI+
MPS
attim
eofd
ischarge;SR
Lwas
addedwith
inthefi
rst6
mon
thsa
nddiscon
tinuedbefore
thefi
rstyear.
(4)S
RLas
prim
aryim
mun
osup
pressio
n.(5)S
RLas
prim
aryim
mun
osup
pressio
nanddiscon
tinuedbefore
thefi
rstyear.
-
16 Journal of Transplantation
(b)
Patie
ntsurvivalrate(%
)Graftrejectionrate(%
)Ac
ute
rejectionrate
(%)
BPAR(%
)
6mon
ths
1year
Other
time
points
6mon
ths
1year
3years
6mon
ths
1year
Other
time
points
Den
ovo/maintenance
dosin
g
DeS
imon
eetal.Am
JTran
splant.2012;12:
3008–20[87]
96.3versus
97.5(EVR+
TAC-
RDversus
TAC-
SD,
𝑃=NS)
2.4versus
1.2(EVR+
TAC-
RDversus
TAC-
SD,
𝑃=NS)
4.1v
ersus10.7
(EVR+
TAC-
RDversus
TAC-
SD,
𝑃=0.005)
Grazietal.P
resented
atILTS
;2011(Ab
stract
P-256)
[88]
Levy
etal.Liver
Tran
spl.2006;12:
1640
–8[52]
(Low
)+CN
I
82.1,
96.7,
87.1
forE
VR1,2
and
4mg/day∗†
0,13.3and3.2
forE
VR1,2
and
4mg/day∗†
39.3,30.0and
29.0forE
VR
1,2and
4mg/day∗†
32.1,
26.7,
and
25.8forE
VR
1,2and,
4mg/day∗†
39.3,30.0,and
29.0forE
VR1,
2,and
4mg/day∗†at3
years
Early
conversio
n(≤3mon
thsa
ftertransplantatio
n)
Fischere
tal.Am
JTran
splant.2012;12:
1855–1865[50]
95.8versus
95.9(EVR
versus
CNI
controlat11
mon
ths,
𝑃=NS)
2.1v
ersus2
.0(EVRversus
CNIcon
trol
at11mon
ths)
17.7versus
15.3
(EVRversus
CNIcon
trolat11
mon
ths)
Schlitt
etal.A
ASLD
2012
[91]
95.7versus
90.0
(EVRversus
CNIcon
trolat
35mon
ths,
𝑃=NS)
24.4versus
15.8
(EVRversus
CNIcon
trolat
35mon
ths,
𝑃=NS)
Masettietal.A
mJ
Tran
splant.2010;10:
2252–6
2[89]
92.3versus
92.3(EVR
versus
CsA,
𝑃=NS)
90.4versus
88.5(EVR
versus
CsA,
𝑃=NS)
5.7at40–87
days
after
transplant
versus
7.7atdays
41–240
after
transplant
CsA
(𝑃=NS)
-
Journal of Transplantation 17(b)Con
tinued.
Patie
ntsurvivalrate(%
)Graftrejectionrate(%
)Ac
ute
rejectionrate
(%)
BPAR(%
)
6mon
ths
1year
Other
time
points
6mon
ths
1year
3years
6mon
ths
1year
Other
time
points
DeS
imon
eetal.Am
JTran
splant.2012;12:
3008–3020[87]
96.5versus
96.3versus
97.5(TAC
elim
versus
EVR+
TAC-
RDversus
TAC-
SD)
2.2versus
2.4
versus
1.2(TAC
elim
versus
EVR+
TAC-
RDversus
TAC-
SD)
19.9versus
4.1
versus
10.7
(TAC
elim
versus
EVR+
TAC-
RDversus
TAC-
SD)
Salib
aetal.AASLD
2012
[90]
6.1v
ersus13.3;
delta
risk:−7.2
%(95%
CI:
−13.5%,−
0.9%
;𝑃=0.010.
EVR+
TAC-
RDversus
TAC-
SDat24
mon
ths)
Lateconversio
n(>3mon
thsa
ftertransplantatio
n)
Casano
vase
tal.
Tran
splant
Proc.2011;
43:2216–
9[93]
94.3
Castr
oagudı́netal.
LiverT
ranspl.200
9;15:1792–7[94]
0
DeS
imon
eetal.
Tran
splInt.200
9;22:
279–
86[95]
100
015
DeS
imon
eetal.Liver
Tran
spl.2009;15:
1262–9
[96]
98.6versus
100(EVR
versus
CNI)
95.8versus
95.9(EVR
versus
CNI)
0versus
0(EVRversus
CNI)
1.4versus
1.4(EVRversus
CNI)
4.2versus
4.1
(EVRversus
CNI)
Salib
aetal.Liver
Tran
spl.2011;
17:
905–13
[98]
1.6
Vallinetal.C
linTran
splant.2011;25:
660–
9[99]
9
𝑃values
areincludedwhere
available;∗𝑃:not
significantfor
allefficacy-related
eventsversus
placebo;otherw
ise,w
here
notstated.
†Timepoint
refersto
timea
fterimmun
osup
pressio
nwas
initiated.
AASLD:Th
eLiverMeetin
g62n
dAnn
ualM
eetin
gofthe
American
Associatio
nforthe
Stud
yofLiverDise
ases;BPA
R:biop
sy-provenacuterejectio
n;Cs
A:cyclosporinA;C
NI:calcineurin
inhibitor;EV
R:everolim
us;
NS:no
nsignificant;TA
Celim;tacrolim
uselimination;
TAC-
RD:reduced
dose
tacrolim
us(C0:3–5n
g/mL);T
AC-SD:stand
ard-do
setacrolim
us(C0:6–
10ng
/mL).
-
18 Journal of Transplantation
However, everolimus did allow substantial tacrolimus reduc-tion
in de novo liver transplant recipients while resulting in
asignificantly lower rate of BPAR at 1 year (4.1% versus
10.7%:everolimus + reduced-dose tacrolimus versus
standard-dosetacrolimus, 𝑃 = 0.005). The lower rate of BPAR
wasmaintained at 24 months (6.1% versus 13.3%, 𝑃 = 0.010)[90]. In a
second study, at 1 year there were similar rates ofpatient survival
(95.8% versus 95.9%), graft loss (2.1% versus2.0%), and BPAR (17.7%
versus 15.3%) in patients convertingto everolimus versus those
remaining on CNI treatment [50].Similarly, in the extension phase
of this study, at 35 monthstherewere similar rates of patient
survival (EVR: 95.7%versusCNI: 90.0%, 𝑃 = 0.535), BPAR (24.4%
versus 15.8%, 𝑃 =0.434), and efficacy failure (29.8% versus 28.2%,
𝑃 = 0.903)[91].
In four late-conversion studies (two prospective and
tworetrospective; Table 2(b)), the incidence of BPAR up to 1
yearafter conversion was 1.6% [98], 2.8% [96], 9% [99] and
15%[95].
3.2. The Effect of mTOR Inhibitors on Renal Function
3.2.1. Sirolimus. In two large retrospective studies (one
highquality and one low quality) in which patients
receivedsirolimus as de novo therapy, there were reductions in
theglomerular filtration rate (GFR) up to 1 year [54] or up to5
years after transplant [55]. In contrast, in a third de
novo,retrospective (low quality) study, modest improvements inrenal
function in patients receiving sirolimus were recordedat both 6 and
12months after transplant, with creatinine levelsdecreasing by 0.22
and 0.28 mg/dL, respectively, compared toincreases in creatinine of
0.61 and 0.35 mg/dL, respectively,in a control group receiving a
standard immunosuppressionregimen [15] (Table 3(a)).
Four retrospective studies (two high quality and twomedium
quality) reported renal function in liver transplantrecipients
converted early to sirolimus from CNI treatment(Table 3(b)) [48,
49, 67, 68]. Two of these studies includeda control group. In the
first retrospective study in which72 liver transplant recipients
converted to sirolimus fromCNI treatment were stratified according
to whether theyhad been converted
-
Journal of Transplantation 19
Table3:(a)E
ffecton
renalfun
ctionof
denovo
mTO
Rim
mun
osup
pressio
n(b)effecton
renalfun
ctionof
convertin
gto
sirolim
us(c)effecton
renalfun
ctionof
convertin
gto
everolim
us(d)
associationof
mTO
Rim
mun
osup
pressio
nwith
proteinu
ria.
(a)
mTO
Rinhibitor
Change
inGFR
(mL/min/1.73
m2 )aft
erconversio
nCh
ange
inserum
creatin
inec
oncentratio
n(m
g/dL
)afte
rcon
version
Change
inCr
Cl(m
L/min)
from
baselin
eat
postc
onversiontim
epoint
3mon
ths
6mon
ths
1year
2years
5years
6mon
ths
1year
6mon
ths
1year
Levy
etal.
Liver
Tran
spl.
2006;
12:
1640
–8[52]
EVR
EVR:
1,2,and
4mg/day
versus
placebo:
−18.7,−36.5,
and−33.2
versus−37
EVR:
1,2,and
4mg/dayversus
placebo:−20.2,
−43.0,and−36.9
versus−36.9
Chinnakotla
etal.
Liver
Tran
spl.
2009;
15:1834–
1842
[55]
SRL
−46
.5versus
−41.0(SRL
versus
TAC)
−39.5versus
−30.0(SRL
versus
TAC)
−43.5versus
−31.5(SRL
versus
TAC)
−38.5versus
−37.0(SRL
versus
TAC)
Campsen
etal.
JTran
splant.2
011;2011:
913094
[54]
SRL
−2.85
versus−9.6
6(C
NIv
ersusS
RL,
𝑃=0.0465)
−6.29
versus
−13.32
(CNI
versus
SRL,
𝑃=0.0320)
Zimmerman
etal.
Liver
Tran
spl.
2008;
14:633–8
[15]
SRL
−0.22
versus
+0.61(SR
Lversus
CNIs,
𝑃=0.0021)
−0.28
versus
+0.35(SRL
versus
CNIs,
𝑃<0.0001)
𝑃values
areincludedwhere
available.
CNI:calcineurin
inhibitor;Cr
Cl:creatininec
learance;E
VR:
everolim
us;G
FR:glomerular
filtrationrate;m
TOR:
mam
maliantargetof
rapamycin;SRL
:siro
limus;TAC
:tacrolim
us.
(b)
Change
inGFR
(mL/min/1.73
m2 )aft
erconversio
nCh
ange
inserum
creatin
inec
oncentratio
n(𝜇m/L)a
fterc
onversion
Change
in24
hCr
Cl(m
L/min)a
fterc
onversion
3mo
6mo
1year
2years
3years
1mo
3mo
6mo
1year
2years
3years
3mo
1year
Early
conversio
n(≤3mon
thsa
ftertransplantatio
n)
McK
enna
etal.
ILTS
.2011
(AbstractO
-17)
[68]
-
20 Journal of Transplantation
(b)Con
tinued.
Change
inGFR
(mL/min/1.73
m2 )aft
erconversio
nCh
ange
inserum
creatin
inec
oncentratio
n(𝜇m/L)a
fterc
onversion
Change
in24
hCr
Cl(m
L/min)a
fterc
onversion
3mo
6mo
1year
2years
3years
1mo
3mo
6mo
1year
2years
3years
3mo
1year
Rogersetal.C
linTran
splant.2009;
23:887–9
6[48]
+29.7
versus
+18.5
(early
versus
latec
on-
version,
𝑃<0.05)
+28.7
versus
+12.4
(early
versus
latec
on-
version,
𝑃<0.05)
+25.5versus
+14.7(early
versus
late
conversio
n,𝑃<0.05)
Harpere
tal.
Tran
splantation.
2011;91:128–32
[67]
+10.6versus
baselin
e(𝑃<0.05)
Schleicher
etal.
Tran
splant
Proc.
2010;42:2572–5
[49]
+15
versus
+9(early
versus
latec
on-
version,
𝑃=0.04)
+16
versus
+10(early
versus
latec
on-
version,
𝑃=0.05)
+22†
versus
+12†
(early
versus
late
conversio
n,𝑃=0.04)
−0.7‡
(early
conversio
nversus
baselin
e,𝑃=0.01)
−0.6‡
(late
conversio
nversus
baselin
e,𝑃=0.05)
Lateconversio
n(>3mon
thsa
ftertransplantatio
n)
Campb
elletal.
Clin
Tran
splant.
2007;21:377–84
[71]
0‡(SRL
versus
CNI)
DiB
enedetto
etal.
Tran
splant
Proc.
2009;41:1297–9
[81]
DuB
ayetal.Liver
Tran
spl.2008;14:
651–9[72]
-
Journal of Transplantation 21(b)Con
tinued.
Change
inGFR
(mL/min/1.73
m2 )aft
erconversio
nCh
ange
inserum
creatin
inec
oncentratio
n(𝜇m/L)a
fterc
onversion
Change
in24
hCr
Cl(m
L/min)a
fterc
onversion
3mo
6mo
1year
2years
3years
1mo
3mo
6mo
1year
2years
3years
3mo
1year
Herlenius
etal.
Tran
splant
Proc.
2010;42:44
41–8
[73]
+12versus
baselin
e(𝑃=0.03)
Lam
etal.D
igDis
Sci.2004;49:
1029–35[74]
−0.32‡
versus
baselin
e(𝑃=0.029)
+0.12‡,
versus
baselin
e(𝑃=NS)
Sancheze
tal.
Tran
splant
Proc.
2005;37:44
16–23
[69]
+8.2,
𝑃=0.05
versus
case
control
+20.2,NS
versus
case
control
+16.1,NS
versus
case
control
−0.1
00
Shenoy
etal.
Tran
splantation.
2007;83:1389-92
[76]
+12versus
−4,NS
versus
CNI
Uhlmannetal.
ExpC
linTran
splant.2012;
10:30–
8[77]
+11.9
versus
baselin
e(𝑃<0.05)
−27
versus
baselin
e(𝑃<0.05)
Watsonetal.Liver
Tran
spl.2007;13:
1694–702
[78]
+7.7
versus
baselin
e(𝑃=0.001)
+6.1versus
baselin
e(𝑃=0.024)
Abdelm
alek
etal.
AmJT
ransplant.
2012;12:694–
705
[45]
−4.45
versus
−3.07
(SRL
versus
CNI,
𝑃=0.34)
Bäckman
etal.
Clin
Tran
splant.
2006;20:336–
9[82]
+6.4
(𝑃=NS
from
baselin
e)
Fairb
anks
etal.
LiverT
ranspl.2003;
9:1079–85[83]
+9∗versus
baselin
e(𝑃=0.01)
-
22 Journal of Transplantation(b)Con
tinued.
Change
inGFR
(mL/min/1.73
m2 )aft
erconversio
nCh
ange
inserum
creatin
inec
oncentratio
n(𝜇m/L)a
fterc
onversion
Change
in24
hCr
Cl(m
L/min)a
fterc
onversion
3mo
6mo
1year
2years
3years
1mo
3mo
6mo
1year
2years
3years
3mo
1year
Naire
tal.Liver
Tran
spl.2003;9:
126–
9[84]
−0.45‡
versus
baselin
e(𝑃=0.001)
Neff
etal.
Tran
splant
Proc.
2003;35:3029–31
[85]
+11.3
versus
baselin
e
Vivarelli
etal.
Tran
splant
Proc.
2010;42:2579–8
4[80]
+18
versus
baselin
e†
+19
versus
baselin
e†+19versus
baselin
e†
Wadeietal.
Tran
splantation.
2012;93:1006–12
[86]
+3.5†versus
baselin
e(𝑃=0.03)
−0.1v
ersus
baselin
e(𝑃=0.25)
𝑃values
areincludedwhere
available.
∗MedianeG
FR,m
eanof
67weeks;†mL/min;‡mg/dL
.CN
I:calcineurin
inhibitor;Cr
Cl:creatininec
learance;G
FR:glomerular
filtrationrate;m
o:mon
th;N
S:no
nsignificant;SR
L:sirolim
us.
(c)
Change
inGFR
(mL/min/1.73
m2 )aft
erconversio
nCh
ange
inserum
creatin
inec
oncentratio
n(𝜇mol/L)a
fterc
onversion
Change
inCr
Cl(m
L/min)
from
baselin
eatp
ostcon
version
timep
oint
6mon
ths
1year
Other
timep
oints
3mon
ths
6mon
ths
1year
6mon
ths
1year
Early
conversio
n(≤3mon
thsa
ftertransplantatio
n)
Fischere
tal.Am
JTran
splant.2012;
12:1855–65
[50]
11-mon
thdata(EVR
versus
CNI):
CG-G
FR:m
eanchange
from
baselin
e:+4.4±27.1
versus0.9±29.2
LSmeandifference±
SE:
−2.923±
3.920(𝑃=0.457 )
§
MDRD
-GFR
:mean
change
from
baselin
e:+2.0±23.2versus
−2.8±23.1LS
mean
difference±
SE:−7.778±
3.338(𝑃=0.021 )
§
-
Journal of Transplantation 23(c)Con
tinued.
Change
inGFR
(mL/min/1.73
m2 )aft
erconversio
nCh
ange
inserum
creatin
inec
oncentratio
n(𝜇mol/L)a
fterc
onversion
Change
inCr
Cl(m
L/min)
from
baselin
eatp
ostcon
version
timep
oint
6mon
ths
1year
Other
timep
oints
3mon
ths
6mon
ths
1year
6mon
ths
1year
Schlitt
etal.
AASLD2012
[91]
35mon
ths:
differenceineG
FRbetweenEV
Rand
CNI:
Cockcroft-Gault:
−10.5mL/min
(𝑃=0.096)
and
Nankivellform
ula:
−10.5mL/min
(𝑃=0.015)
Masettietal.A
mJ
Tran
splant.2010;
10:2252–62
[89]
+6.1versus−16.5
(EVRversus
CsA,
𝑃<0.001
comparis
onof
absolutevalues)
+5.9versus−14.8(EVR
versus
CsA,𝑃<0.001
comparis
onof
absolute
values)
DeS
imon
eetal.
AmJT
ransplant.
2012;12:3008–20
[87]
EVR+TA
C-RD
(adjusted
meandifferenceineG
FRchange
forE
VR+
TAC-
RDversus
TAC-
SD:
+8.50±2.12;𝑃<0.001)
Salib
aetal.
AASLD2012
[90]
24mon
ths:
EVR+TA
C-RD
versus
TAC-
SD:
meandifferencein
eGFR
change:
+6.66(97.5
%CI
:+1.9,+11.42;𝑃=
0.0018)
Lateconversio
n(>3mon
thsa
ftertransplantatio
n)
Castr
oagudı́netal.
LiverT
ranspl.2009;
15:1792–7[94]
+3.99(N
Sversus
baselin
e)+7.65(𝑃=0.016versus
baselin
e)−0.09
(NS
versus
baselin
e)
−0.22‡
(𝑃<0.05
versus
baselin
e)
+5.18
(NSversus
baselin
e)+9
.82(𝑃=0.025
versus
baselin
e)
DeS
imon
eetal.
Tran
splInt.200
9;22:279–86[95]
+4.03
-
24 Journal of Transplantation(c)Con
tinued.
Change
inGFR
(mL/min/1.73
m2 )aft
erconversio
nCh
ange
inserum
creatin
inec
oncentratio
n(𝜇mol/L)a
fterc
onversion
Change
inCr
Cl(m
L/min)
from
baselin
eatp
ostcon
version
timep
oint
6mon
ths
1year
Other
timep
oints
3mon
ths
6mon
ths
1year
6mon
ths
1year
DeS
imon
eetal.
LiverT
ranspl.2009;
15:1262–9[96]
EVR:
+1.0;
controls:
+2.3
(NS)
Salib
aetal.Liver
Tran
spl.2011;
17:
905–13
[98]
+6.6chronicr
enal
failu
resubp
opulation
versus
baselin
e(𝑃=0.0002)
+4.2overallversus
baselin
e(𝑃=0.007)
+8.6chronicr
enalfailu
resubp
opulationversus
baselin
e(𝑃=0.02)
−11versus
baselin
e(𝑃=0.04)
−9versus
baselin
e(𝑃=NS)
−6versus
baselin
e(𝑃=NS)
𝑃values
areincludedwhere
available.
∗MedianeG
FR;†mL/min;‡mg/dL
.§ B
etween-grou
pdifference(calculated
asCN
Igroup
minus
everolim
usgrou
p)atmon
th11aft
erbaselin
e;results
basedon
ANCO
VAmod
el.CG
-GFR
:GFR
calculated
with
theC
ockcroft-Gaultform
ula;CN
I:calcineurin
inhibitor;Cr
Cl:creatininec
learance;C
sA:cyclosporin
A;EVR:
everolim
us;G
FR:glomerular
filtrationrate;LS:leastsqu
are;MDRD
:mod
ificatio
nof
dietin
renald
isease;MDRD
-GFR
:GFR
calculated
usingtheM
DRD
form
ula;NS:no
nsignificant;SE
:stand
arderror;TA
C-RD
:reduced-dosetacrolim
us(C0:3–5n
g/mL);TAC
-SD:stand
ard-do
setacrolim
us(C0:6–
10ng
/mL).
(d)
Proteinu
ria(afte
rcon
versionun
lessotherw
isesta
ted),%
recipients
Sirolim
usstu
dies
Early
conversio
n(≤3mon
thsa
ftertransplantatio
n)Harpere
tal.Tran
splantation.2011;91:128–32
[67]
Proteinu
ria:preconversio
n:45;6
mon
ths:72;3
years:63;5
years:58
Lateconversio
n(>3mon
thsa
ftertransplantatio
n)DuB
ayetal.L
iverTran
spl.2008;14:651–9[72]
7versus
4(SRL
versus
CNI)
Herlenius
etal.T
ransplantP
roc.2010;42:44
41–8
[73]
8.3versus
7.7(SRL
versus
MMF)
Morardetal.L
iverTran
spl.2007;13:658–64
[75]
Album
inuria:36
Uhlmannetal.E
xpClin
Tran
splant.2012;10:30–
8[77]
Proteinu
riaincreasedat6mon
thsa
fterc
onversion(𝑃<0.05)
Wadeietal.Transplantatio
n.2012;93:1006–12[86]
81Ev
erolim
usstu
dies
Early
conversio
n(≤3mon
thsa
ftertransplantatio
n)DeS
imon
eetal.Am
JTransplant.2012;12:3008–20[87]
EVR+TA
C-RD
versus
TAC-
SD:2.9versus
0.4(RR:
6.89,95%
CI0.85,55.54)
Fischere
tal.Am
JTransplant.2012;12:1855–6
5[50]
EVRversus
CNI:9.9
versus
2.0
Lateconversio
n(>3mon
thsa
ftertransplantatio
n)Ca
stroagudı́netal.LiverTran
spl.2009;15:1792–7
[94]
38.1
Salib
aetal.LiverT
ranspl.2011;17:905–13[98]
5.4
Vallinetal.C
linTran
splant.2011;25:660–9
[99]
13versus
29(pre-v
ersusa
fterc
onversion,𝑃<0.05)
𝑃values
areincludedwhere
available.
CNI:calcineurin
inhibitor;EV
R:everolim
us;M
MF:mycop
heno
latem
ofetil;SR
L:sirolim
us;R
R:relativerisk
;95%
CI:95%
confi
denceinterval;T
AC:tacrolim
us;TAC
-RD:reduced-dosetacrolim
us(C
0:3–5n
g/mL);
TAC-
SD:stand
ard-do
setacrolim
us(C0:6–
10ng
/mL).
-
Journal of Transplantation 25
(𝑛 = 89) or placebo (𝑛 = 30) to liver transplant
recipientsreceiving cyclosporine, there was no improvement in
renalfunction, with liver transplant recipients receiving
everolimusshowing a decrease in creatinine clearance at 6 months
aftertransplant (Table 2(c)) [52].
Four high quality, prospective, randomized studiesshowed good
results in liver transplant recipients convertedearly to everolimus
from CNI treatment (Table 3(c)) [50,87, 89, 91]. One of these
evaluated whether early CNIwithdrawal and initiation of everolimus
monotherapy in denovo liver transplantation patients would lead to
superiorrenal function, compared to the cyclosporine control, at
12months after transplantation [89]. At randomization, themean eGFR
value calculated by the modification of diet inrenal disease (MDRD)
formula was 81.7 ± 29.5mL/min/1.73m2 in the everolimus group and
74.7 ± 24.6mL/min/1.73m2in the cyclosporine group (𝑃 = 0.30). At 6
and 12 months,respectively, the mean eGFR values in the everolimus
groupwere 87.8 ± 36.7 and 87.6 ± 26.1mL/min versus 58.2 ± 17.9
and59.9 ± 12.6mL/min in the cyclosporine group (𝑃 < 0.001
forboth the 6- and 12-month comparisons). In a
per-protocolanalysis, the incidence of stage ≥3 chronic kidney
disease(estimated GFR < 60mL/min) was significantly lower in
theeverolimus group at 1 year after liver transplant (52.2%
versus15.4%, in the cyclosporine group, respectively, 𝑃 =
0.005)[89]. More recently, results from an 11-month,
multicenter,prospective, open-label trial were published in which
livertransplant recipients with good renal function at 4 weeksafter
transplant were randomized to either continue CNItreatment
with/without corticosteroids (𝑛 = 102) or switchto everolimus
with/without corticosteroids (𝑛 = 101) [50].There was a significant
difference between treatments usingthe MDRD formula (−7.8mL/min in
favor of everolimus,𝑃 = 0.021), although this was not significant
whenusing the Cockcroft-Gault formula (−2.9mL/min in favor
ofeverolimus, 𝑃 = 0.46) [50]. Results of the extension phase in81
patients demonstrated that everolimus maintained betterrenal
function at 35 months (difference in eGFR betweeneverolimus and CNI
arms: Cockcroft-Gault: −10.5mL/min,𝑃 = 0.096 and Nankivell formula:
−10.5mL/min, 𝑃 = 0.015)[91].
In the fourth early-conversion prospective, randomized,high
quality study (Table 3(b)) [87], 719 de novo livertransplant
recipients were given a 30-day run-in periodwith tacrolimus-based
immunosuppression (± mycophe-nolate) and then randomized to the
following groups:everolimus (trough concentration, C0: 3–8 ng/mL)
plusreduced-exposure tacrolimus (TAC-RD, C0: 3–5 ng/mL; 𝑛 =245);
everolimus (C0: 6–10 ng/mL) with tacrolimus beingwithdrawn (TAC-WD,
𝑛 = 231) at 4 months or standard-exposure tacrolimus (TAC-SD, C0:
6–10 ng/mL, 𝑛 = 243).Enrolment in the TAC-WD arm was stopped
prematurelydue to a higher incidence of biopsy-proven acute
rejection(BPAR) around the time of tacrolimus elimination.
However,renal function at 1 year post-randomization improved
sig-nificantly with everolimus plus TAC-RD, with an adjustedmean
difference in eGFR change of +8.5mL/min/1.73m2
(97.5% confidence interval (CI) 3.74, 13.27mL/min/1.73m2)
versus that observed in patients in the TAC-SD group (𝑃
<0.001). The recent publication of final results from this
trialdemonstrates that significantly better renal function
withTAC-RD was maintained at 24 months (mean difference ineGFR
change: 6.66mL/min/1.73m2 (97.5% CI: 1.9, 11.42; 𝑃 =0.0018))
[90].
Of four late-conversion studies involving everolimus(Table
3(b)), two prospective, single-arm studies and oneretrospective
study demonstrated a benefit [94, 95, 98].The other, a prospective,
randomized, multicenter, mediumquality study that involved
administering everolimus withCNI reduction or discontinuation to 72
liver transplantrecipients experiencing CNI-related renal
impairment, failedto show a significant improvement in renal
function frombaseline or when compared to renal function in 73
CNIcontrols [96, 100]. A number of confounding factors werenoted by
the authors that may have potentially contributed tothe negative
result, including low CNI exposure at baselinedue to previous
efforts by the clinical team to improverenal function, and the fact
that the extent of CNI dosereductions in the control group was
higher than expected fora maintenance population.
Proteinuria was reported in four everolimus (two highquality and
two low quality) studies identified in the literaturesearch (Table
3(d)), occurring with incidences of 2.9% [87],5.4% [98], 9.9% [50]
and 29% [99]. One of these was aprospective randomized study that
compared liver transplantrecipients who received CNIs with/without
corticosteroids(𝑛 = 102) to those who were switched early to
everolimuswith/without corticosteroids (𝑛 = 101). The incidence
ofproteinuria at 11 months post-randomization was higher inthe
everolimus group (9.9%) compared to the CNI group(2%), although six
out of ten cases were mild with theremaining cases being moderate
[50]. In another largeprospective randomized high quality trial, in
which patientswere converted to everolimus early, proteinuria was
observedin the everolimus plus reduced tacrolimus dose group
duringa 12-month followup period, but the maximum mean valuesfor
urinary protein to creatinine ratio were below 0.3 g/g,
andpreexisting cases of proteinuria did not worsen [87].
3.3. Safety of mTOR Inhibitors
3.3.1. Hepatic Artery Thrombosis (HAT)
Sirolimus. Two multicenter randomized studies in de novoliver
transplant recipients suggested that the use of sirolimusin
combination with cyclosporine or tacrolimus was associ-ated with an
increase in HAT [38, 44]. In subsequent studies(a mixture of
quality and trial designs) that reviewed the useof sirolimus in
liver transplant recipients, increased rates ofHAT have not been
observed (Table 4(a)) [15, 45, 48, 53, 55,57, 61]. In fact, two of
these studies recorded significantlylower incidences of HAT among
patients receiving sirolimuscompared to controls [53, 57]. In these
studies, sirolimus wasgiven at 2mg per day without a loading dose,
and sirolimuslevels were targeted at