Embed Size (px)
Citation preview

ANESTH ANALG 1 Y83;62:76'-76
764
Review Article
Influence of Aging on Lung Function-Clinical Significance of Changes from Age Twenty
W. M. Wahba, MB, BCh, DA, MSc, FRCP(C)
There has been a progressive increase in the number of patients aged 65 years and over presenting for sin- gle or multiple anesthetics. In order to provide ade- quate care, a clear understanding of the physiological changes that occur with aging is needed. This review will examine the literature dealing with the effects of aging on pulmonary physiology and discuss their clinical implications as follows: mechanical properties of the lungs, gas exchange, control of breathing, and postoperative lung function. Because smoking, obe- sity, and chronic heart disease adversely affect lung function, the effects of these diseases also will be examined.
There are no longitudinal studies in the literature that examine all aspects of lung function. Therefore, we gathered data pertaining to different age groups and used regression analysis limiting extrapolation beyond the range of ages in any particular study.
Pulmonary Mechanics, Lung Volumes, and Capacities (Table 1) There are four basic changes that affect lung function as aging occurs. They are decrease in motor power, decrease in elastic recoil of lung tissue, stiffening of the chest wall, and decrease in the size of the inter- vertebral spaces. Their effects may be exerted singly or in combination.
Received from the Department of Anaesthesia, McGill Univer- sity, Montreal, Quebec, Canada. Presented at the 12th Connecticut Postgraduate Anesthesia Seminar, April 1982, and the Seventh Annual Spring Meeting of the New York State Society of Anes- thesiologists, May 1981. Accepted for publication March 1, 1983.
Address correspondence to Dr. Wahba, Queen Elizabeth Hos- pital of Montreal, 2100 Marlowe Avenue, Montreal, Quebec, H4A 3Lh. Canada.
Lung Compliance and Volumes The changes in lung volumes and mechanics are due to the decrease in elastic recoil of the lungs and pro- gressive stiffening of the chest wall. The loss of elastic recoil means that less pressure for expansion is re- quired, i.e., increased static compliance. The lung tends to assume a larger volume, i.e., increased functional residual capacity (FRC), at resting transpulmonary pressure (Ptp). The latter decreases progressively with age (81). However, the concomitant change in the chest wall elastic properties (progressive stiffening and calcification of costal cartilage) counteract this trend for the lung to assume a larger FRC, which thus re- mains constant (42,81).
Figure 1(A) depicts static pressure-volume rela- tionship of the lungs for a 20- and a 70-year-old seated healthy person. The general shape of the curve is not dissimilar, but the position of the curve for older sub- jects is shifted to the left (i.e., more compliant). Figure 1(B) graphically illustrates the expected change with aging of various measurements related to the elastic properties of the lungs.
Although the ratio of FRC to total lung capacity (TLC) tends to increase with age (102), the absolute FRC, which is a direct function of height, changes little with age (42,81). Specific lung compliance (i.e., CL/L FRC), therefore, increases with age. The reduced elastic recoil of the lung is not due to decreased elastin content, which does not change with age (83). The tensile strength of the lung is not reduced by aging (83). Cross linkage and rearrangement of the collagen fibrils and elastin occur with aging; this rearrange- ment explains the increased static compliance without loss of tensile strength. But this rearrangement is probably regional rather than evenly distributed, which may create some areas of high and others of low com- pliance with zones of different time constants. Dy-
C 1983 by the Internat~onal Anesthesia Research Societv

AGING AND LUNG FUNCTION ANESTH ANALG 765 1983;62:76476
Table 1. Useful Prediction Equations for Lung Volume, Capacities, Mechanics, and Oxygen Consumption
Measurement Reference Equation SD Condition of study and comments
Vital capacity (ml)
Total lung capacity (ml)
Functional residual capacity (ml)
Residual volume (ml)
RV/TLC%
Static recoil pressure (60% TLC) (cm H,O) Static transpulmonary pressure (cm H,O) Maximum inspiration pressure (cm H,O)
Forced expiratory volume (ml) in 1.0 s
Oxygen consumption (ml/min)
50.8 H - 32.0 A - 3020 33.0 H - 23.0 A ~ 1400 94.0 H - 15.0 A - 9167 79.0 H - 8.0 A - 7490 81.0 H - 1792 S - 7110 53.0 H - 17.0 W - 4740 46.4 H - 6040 27.0 H + 17.0 A - 3450 32.0 H + 9.0 A - 3900
0.343 A + 16.7 0.265 A + 21.7
9.92 - 0.0957A 27.1 - 0.1327 A 143 - 0.55 A (M) 104 - 0.51 A (F)
36.0 H - 27.0 A - 1650 25.0 H - 22.0 A - 620
& Male Female 10 167s 159 S 15 160 S 139 S 20 143 S 126 S 60 1 2 4 s 113s
? 450 f 460 f 648
? 580 ? 470
f 390 2 370 2 4.8 f 5.7
-
2 19.9 f 14.6 249.0 ? 400
403 M, standing 481 F, standing 44 M, sitting 50 F, sitting 44 M, sitting 50 F, sitting 59 M, supine 44 M, sitting 50 F, sitting 44 M, sitting 50 F, sitting 44 M and F, sitting 26 M, sitting 60 M, 60 F, 20-86 years old
298 M, standing 481 F, standing
Abbreviations: A, age (years); H, height (crn); W, weight (kg); S, surface area (I$); M, males; F, females,
namic lung compliance (i. e., compliance measured during active breathing) becomes quite frequency- dependent with age (37). At more rapid breathing rates, lung expansion may become less effective and may increase the maldistribution of ventilation rela- tive to perfusion.
The intervertebral spaces decrease in size with age leading to a decrease in total height. This height loss may account for the 10% reduction in TLC between the ages of 20 and 70 years (42), but a decrease in motor power also may play a role. The maximal pres- sure that can be generated by a full inspiration or expiration decreases with age (7) (Fig. l (B)) . This
1 a[
Figure 1. Pulmonary mechanics. (A) Re- constructed compliance (pressure:
old person, seated. Data from (102). (B) The expected change in various mea-
80 volume) curves in a 20- and a 70-year-
surements of lung mechanics (81,102) and
- 5 e s E 60 2
0 >
- maximum inspiratory pressures with
are measured at about 60% TLC, at which - aging (7). Static elastic recoil pressures cn 3 -1
40 volume the pressure measured reflects lung recoil alone. Transpulmonary pres- sure is measured at TLC. Note the log- arithmic scale for elastance (the recip- rocal of compliance) and that the scale decreases upwards. 20
decrease reflects the limitation to expansion imposed by the structural and motor power effects of aging and is of a greater magnitude in men (7).
The tendency for the lung to assume a larger rest- ing volume and the limitations imposed by a stiffer chest wall with a decrease in motor power result in a change in the subdivision of TLC (Fig. 2). From age 20, vital capacity (VC) decreases progressively ( - 20 to -30 ml/yr) while residual volume (RV) increases (+ 10 to + 20 ml/yr) (42). In fact, the ratio of RV to TLC increases from 25% at 20 years of age to about 40% in a 70-yr-old man (Fig. 2), which gives the chest wall a barrel-like appearance.
0 25 50 Static Pulmonary Elastic Recoil Pressure (cm H,O)
Age (Years)

ANESTH ANALG 766 1983,62:76&76
7 -
6 -
5 -
- 4 -
2 3 -
2 -
1 -
0 -
- - E 9
WAHBA
TLC , ,
FRC __
R", , ,
20 Years
RV/TLC 25% 40%
vc 1
FEVl o/FVC 80% 75 %
Fivure 2 Lung volumes and capacities. The expected values of TLC, FRC, RV, VC, and FEV, (plus various ratios) in a 20- and a 70-year-old of normal habitus and free of disease. The equations are given in Table 1. The hatched areas represent expected closing capacity .
Dynamic lung volumes and capacities decrease progressively with age [e.g., forced expiratory volume in 1 s, (FEVI o) (Fig. 2) (33) and maximal midexpiratory flow rate (MMEF) (62)]. This reduction is due largely to the decrease in motor power of the accessory mus- cles of breathing and to decreased expansion of the chest wall. We noted before that maximal inspiratory force decreases with age and is related to sex. This difference also is seen in the changes in FEV, o, which decreases by about 27 mliyr in men but by only 22 ml/yr in women (33). The percent change in the two sexes may, however, be the same because men start off with higher absolute values of this measurement.
Smoking has significant effects on lung volumes and capacities. For instance, a 20-pacWyr history (i.e., one pack per day for 20 years) leads to a marked decrease in FEV, O r VC, FEVNC%, and maximal breathing capacity over the reduction due to aging alone (110). The ratio of RV to TLC also increases. The annual decrease in FEVl,o can be increased nine- fold by heavy smoking (52). However, it is interesting to note that not all smokers will exhibit such changes. In some, no changes in FEVl.o may be noted and increased airway closure may be the only abnormality seen (12). It should be mentioned here that aged lungs have some, but certainly not all, of the features of chronic obstructive lung disease, e.g., increased RV and RVITLC%, reduced VC and FEV, o, and fre- quency dependence of compliance.
Lung and chest wall compliance, FRC, ERV, and VC are markedly reduced by obesity (64). Conse- quently, the work of breathing is increased. The in- fluence of obesity (or large weight-to-height ratios) on gas exchange will be examined later.
Airway Resistance In normal humans, flow resistance is largely due to the more central airways. The contribution of small peripheral airways (i.e., beyond the 10th to 12th air- way generation) is very small. With aging, the larger and more central airways increase in diameter as noted by an increase in anatomic (87) and physiologic dead space (100). Beyond age 40, the diameter of the small airways decreases significantly (75); however, airway resistance, as measured by currently available meth- ods, remains unchanged (10,17). It is possible that the method used is not sensitive enough to detect small changes in resistance. It also is possible that the in- crease in distal resistance and the decrease in proximal resistance cancel each other, giving a constant value. Specific resistance (i.e., resistance/L FRC) remains unchanged.
Airway Closure Small airways without cartilagenous support with diameter less than 1 mm are kept open by the guy- rope effect of the elastic tissue surrounding them and by subatmospheric intrapleural pressure (Ppl). Air- way stability is promoted by airway surfactant (65). The decrease of elastic recoil with age reduces the stability of small airways, leading to a tendency for these airways to close. The diameter of small periph- eral airways, as noted in postmortem specimens, also tends to decrease after age 40 (75). The extent of air- way closure (closing volume or capacity, CV, CC) has been shown to increase with age (11). The value of Ppl also is related to age with mean Ppl = -6.3 +- 2.7 cm HZO in children (47), whereas in adults (60-80 years old) mean Ppl is -4.8 -+ 2.0 cm H20 (37). In- trapleural pressure depends on posture, increasing by about 4-5 cm H20 when changing from the seated to the supine position (32), suggesting that small air- ways may lose some stability in the supine position. The decreased ventilation of basal lung units in obese subjects was attributed to airway closure occurring in these basal units (54). Indeed, subjects with a rela- tively large weight/height ratio tend to have CC/FRCs that are greater than that predicted on the basis of age alone (Fig. 3). This suggests that body build plays an important role in determining the extent of airway closure that becomes physiologically significant when CC exceeds FRC (20).
In cigarette smokers, closing volume increases dis- proportionately to age (12), while other tests of small airway function may be normal. It is sometimes im- possible to detect the change in slope necessary to measure CC in heavy smokers (71). The influence of airway closure on gas exchange will be examined later.

AGING AND LUNG FUNCTION ANESTH ANALG 767 1983;62: 76676
. .
. . . Wetght/Height
0 e 43 . , 43
0 0
. B , 0
y1 z 1 5 5 2o 30 40 50 bO I D so I 1 1
Age (Years)
Figure 3. Closing capacitylfunctional residual capacity v age. Data from published (20,24,25) and unpublished work (undertaken with Drs. H. F. Don and D. B. Craig). All subjects were supine. Those with a weight/height ratio greater than 0.43 had CClFRC greater than that accounted for by age alone. The CC/FRC:age relationship, determined by least squares regression, is CC/FRC = 0.64 + 0.1 age; r = 0.66. Inclusion of individual weightlheight ratios improved the coefficient of correlation. The equation is CClFRC = 0.29 + 0.1 age + 0.93 ratio; I = 0.79.
Changes during Anesthesia We have very little information on whether pulmo- nary mechanics during anesthesia are influenced by age alone. The following is a brief statement of current knowledge relating patient factors to intraoperative lung function.
Upon assuming the supine position, there is a re- duction in FRC (20) and hence an increase in airways resistance. Compliance may become less (32). After induction of anesthesia, FRC and compliance are re- duced and airways resistance is increased. However, an increase in airways resistance has not always been noted. The changes in FRC and compliance occur dur- ing or shortly after induction, at which time imped- ance to inspiratory gas flow is significantly increased (38). The reductions in compliance and FRC are not progressive with time. There is a striking similarity in the features of reduced FRC and compliance; in- deed, these changes may be due to the same mech- anism. The decrease in lung compliance is greater in obese subjects but is not related to age (41). The re- duction in FRC, which may be the initial and critical event, has been reported to be of greater magnitude in the aged (48), the more obese (23), and patients with low FEVl.o (51). Such patients should have more severe derangements of gas exchange during anes- thesia. Indeed, the increase in V/Q mismatching dur- ing anesthesia is a direct function of preoperative pul- monary status (27). Intraoperative gas exchange is related to the extent of decreased FRC (44,48,49,51),
the ratio of preoperative CC to intraoperative FRC (108), and preoperative lung function, specifically FEV1.o (84,103). The magnitude of enlargement of P[A - a]02 during anesthesia has not been shown to be clearly a function of the patient’s age alone.
The decrease in lung compliance during anesthesia should entail an increase in elastic recoil. Because air- way closure is in part due to loss of elastic recoil, one could anticipate that closing capacity will be less dur- ing anesthesia. However, there is no agreement on what happens to CC during anesthesia. Two earlier studies, using the resident gas technique, reported no change in closing capacity (39,44) (Fig. 4). Because this method may give wrong results in anesthetized patients, the study was repeated using the foreign gas technique, which is believed to avoid this error. One group reported a proportionate decrease in CC and FRC (Fig. 4), such that CC/FRC ratios in the 28 subjects studied remained age-related (57) (Fig. 5). Their data suggest that CC decreases to the same degree in all patients, but that FRC decreases to a lesser extent in younger patients (Fig. 5). The other group (45), however, reported that CC does not change and that CC/FRC is of a larger magnitude during anes- thesia (Fig. 4), confirming their previous report (44). The reasons for differing results is not clear and we must await further elucidation.
The change in airways resistance during general anesthesia also requires clarification because not all reports confirm the expected increase. The inverse relationship between airway resistance and FRC sug- gests that the former should increase during anesthesia.
Can positive airway pressure reverse airway clo- sure? The transpulmonary pressure at which airways close or open is the closing or opening pressure (CP,
Figure 4. Summary graph of intraoperative closing capacity. The figure shows mean CC and FRC values before and during general anesthesia (39,44,45,51). Note that in three reports, CC was un- changed while FRC was less during anesthesia. CCiFRC increased in these studies. In one report, both capacities were proportionately less. The reason for this difference in results is still not fully or satifactorily explained.
,Resident Gas Technique, ,Foreign Gas Technique, I I
cc FRC B

ANESTH ANALG 1983:62:761-76
768 WAHBA
1 6 I- -.5
" Y U I I I I I I
20 30 40 50 60 70 80
Age (Years)
FiRure 5. Intraoperative CC, CCIFRC, and age. Results of regres- sion analysis of age against CC and CCiFRC before and during anesthesia (57) (Table 1). Note the decrease in intercept but lack of change in the slope in the age:CC relationship. Between age and CC/FRC, there is a small difference in intercept and slope that makes a small difference in the change at both ends of the range of ages studied.
OP). During active breathing, C? in young subjects is about - 1.25 cm H20, and OP is + 2.5 cm H20, the difference being hysteresis (53). The values for CP and OP in subjects aged 65-75 years are 0 and 4.5 cm H20, respectively (53). During anesthesia with con- trolled ventilation, the opening pressure is about 6 cm H20 (6). In order to reopen such airways with positive end-expiratory pressure (PEEP), the system pressure must be sufficiently high to deliver such pressures to the closed airways and also must over- come chest wall resistance. The effectiveness of PEEP in clinical circumstances will, therefore, be limited (111) by this and by the effects of PEEP on cardiac output and pulmonary blood flow distribution.
Alveolar Gas Exchange (Table 2) Gas Exchange in the Awake State The efficiency of alveolar gas exchange decreases pro- gressively with age for a number of reasons. The small increase in anatomic dead space (35,100) alone cannot account for the uneven pattern of distribution of in- spired gas in older subjects that contrasts with the more even distribution in younger subjects (36). The closure of basal lung units during tidal breathing whenever closing capacity exceeds functional residual capacity is a very attractive explanation (53). In older subjects the pressure across basal lung units may be positive rather than subatmospheric. Thus during quiet breathing, inspired gases will preferentially go to the more distensible upper lung units leading to an un-
even distribution of gases (53). When older subjects take larger and slower breaths, creating a more sub- atmospheric intrapleural pressure throughout and opening closed airways, inspired gases are more evenly distributed (29), as is seen in young subjects. During quiet breathing, gas trapping behind closed airways occurs and is a direct function of age (53). Upon as- suming the supine position, a maneuver whose effect on Ppl was noted above, FRC decreases while CC does not change (20). Under such circumstances, gas trapping behind closed airways increases by a mea- surable amount (24). These studies lend support to the belief that the uneven distribution of inspired gas is largely due to airway closure. Unless the distri- bution of pulmonary blood flow changes appropri- ately, VlQ mismatching will occur. A significant cor- relation between CC/FRC and P[A - a]02 exists (Table 2).
The transfer of carbon monoxide across the alveolar membrane, a measure of diffusion, decreases with age (26). This loss, which is presumably due to struc- tural changes, is relatively greater in men than it is in women (0.24 ml/torr/year 7.1 0.16 ml/torr/year) (5). In smokers, the loss is accelerated (110). Alveolar sur- face area also decreases with age from about 75 m2 at age 20 years to about 60 m2 at age 70 years (101).
Beyond the alveolar surface, a number of factors contribute to the derangement in gas exchange. Al- though blood volume does not change with age p), that present in the pulmonary circulation at any one moment decreases with age (31). Hemoglobin content decreases with age. There also is evidence that the distribution of pulmonary blood flow changes with aging, promoting V/Q mismatching (109). Alveolar dead space, which is a good index of the distribution of pulmonary blood flow (93)' increases with age (87). One can speculate about the cause of the lack of ap- propriate change in pulmonary blood flow distribu- tion to restore VlQ matching. Pulmonary vascular resistance at rest is not age-dependent, but, during exercise, is higher in older subjects (30). The more rigid pulmonary vasculature in the aged probably re- sults in blunting of the hypoxic pulmonary vaso- constrictor (HPV) reflex. The efficiency of vascular distensibility and recruitment probably is decreased. The loss of physical support of surrounding pulmo- nary elastic tissue may be a contributing factor.
Cardiac output under basal conditions decreases progressively with age (9). This will certainly play a role in determining pulmonary blood flow and in ar- terial oxygenation. The relationship between cardiac output (Qt), oxygen consumption (Vo2) and the ar- terio-venous O2 content difference [C(a - +)02] is Fick's equation. Because both Voz (8) and Qt decrease with

AGING AND LUNG FUNCTION ANESTH ANALG 769 1983;62:76&76
Table 2. Gas Exchange Equations
Measurements Ref. Equation Comments
Alveolar-arterial 0, tension difference and arterial 0, tension
Physiological shunt (% cardiac Output)
Physiological dead space (%)
(40) P(A-a)o, = 19.3 + 0.46 A - 1.0 Paco, + 0.17 W
Pao, = 99.3 - 0.47 A - 3.17 smoking - 33.2 W/H
P(A - a)@ = 2.5 + 0.21 A Pao, = 104.2 - 0.27A
+ 2.95 smoking SEE = 10.6
+ 0.23 Pao, SEE = 10.6 (72)
(20) P(A - a)02 = 1.85 + 0.51 A r = 0.79
(107) Pao, = 102 - 0.498A r = 0.68 = 95 - 0.228 W M r = 0.25 = 111.65 - 0.44A - 29.62 WM r = 0.73
NB: Other equations (pre- and postoperative) can be found in (69) (68) = 0.102 A + 0.074 r = 0.74
= -13.88 + 34.99 CC/FRC r = 0.73
(20) = 0.26 A - 1.69 (20) (72) = 24.6 + 0.17age
= 18.63 + 0.22 age r = 0.81 r = 0.48
337 supine surgical patients. Smoking score: 0 = nil; 1 = light; 2 = heavy.
10 premedicated surgical
23 supine subjects 23 supine subjects 80 healthy, seated subjects,
15-75 years old
patients
Abbreviations as in Table 1.
age [cardiac index (L/m/m2) = 4.16 - 0.02 age (pooled data)], C(a - V)O, will remain the same so long as the same percent decrease occurs in both other measure- ments. No published data could be found to give age- related values of C(a -V)02 . The net result of all these factors is an increase in VlQ mismatch. Therefore,we get a progressive increase in all the measurements indicating the inefficiency of gas exchange (Table 2, Fig. 6).
An important question is what other factors aug- ment the influence of aging on arterial oxygenation. Body build and smoking history adversely affect Paol (40). Arterial Po, also is influenced by low FEVl.o (105). Arterial Pco, has been reported not to be influenced by age (91). Another study, however, reported a small but significant increase in Paco, with a corresponding small decrease in alveolar PO, (PAo,) (40).
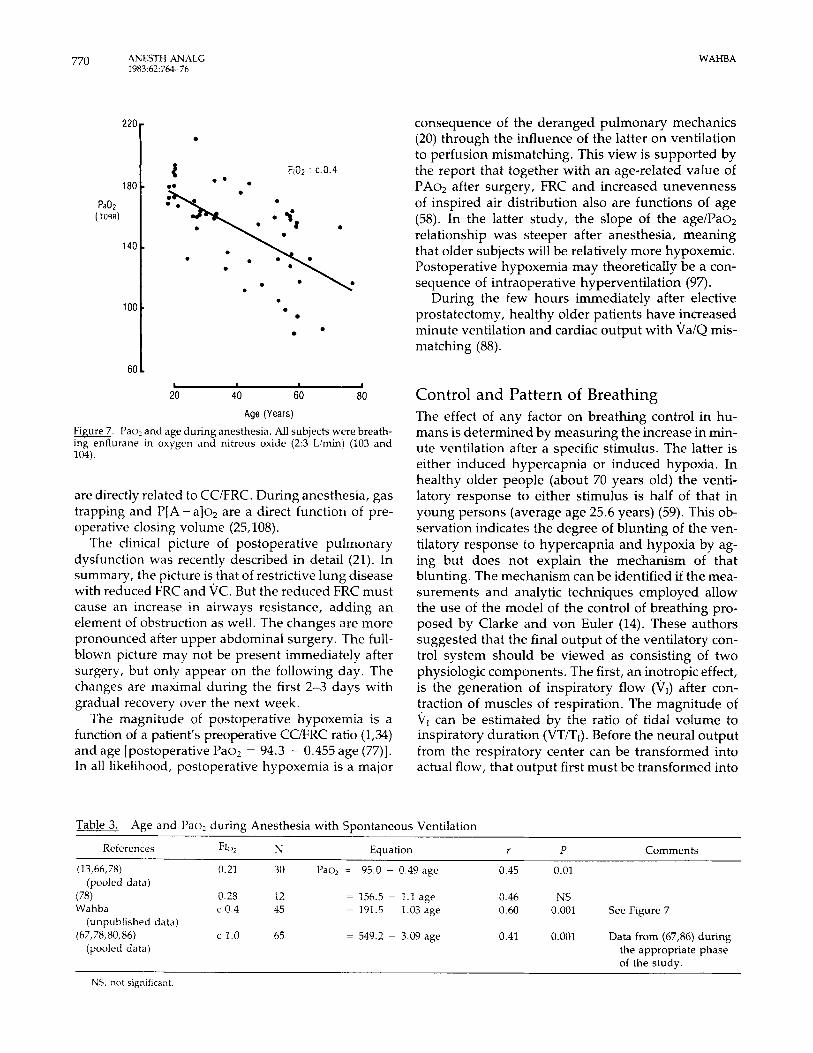
lntra- and Postoperative Gus Exchange Alveolar gas exchange during and after anesthesia almost invariably becomes less efficient. A major cause of this is believed to be an increase in V/Q mismatch- ing. The average Pao2/PAo2 in a number of studies analyzed was approximately 0.5 (77). The question now is whether or not Pao, during anesthesia is re- lated to age. The pooled data from studies dealing with spontaneously breathing patients were analyzed and an inverse relationship between age and Po, was found (Fig. 7 and Table 3). In studies where venti- lation was controlled, a similar relationship could be found only in three reports (13,108,111). The influ- ence of controlled ventilation on cardiac output ex-
plains the lack of a relationship between age and Pao2 in the other reports examined.
To what extent is the gas exchange derangement in surgical patients due to airway closure? Upon as- suming the supine position, P[A - a]02 and gas trap- ping behind closed airways increase (2024). The per- cent increase is less in subjects whose CWRC is greater than 1.25 than in subjects with values of 0.1-1.25. However, P[A - a]o, and the volume of gas trapped
Figure 6. Gas exchange and age. Data from the same subjects while supine (20). Equations are given in Table 2.
.
n I I I I I I ./
Age (Years) 20 30 40 50 60 70 80
WAHBA
180.
Pa02 (TORR)
140
100
22Or
-
-
60 L
0
0
b I
20 40 60 80
Age (Years)
Figure 7. Pao, and age during anesthesia. All subjects were breath- ing enflurane in oxygen and nitrous oxide (2:3 Limin) (103 and 104).
are directly related to CCiFRC. During anesthesia, gas trapping and P[A - a]oz are a direct function of pre- operative closing volume (25,108).
The clinical picture of postoperative pulmonary dysfunction was recently described in detail (21). In summary, the picture is that of restrictive lung disease with reduced FRC and VC. But the reduced FRC must cause an increase in airways resistance, adding an element of obstruction as well. The changes are more pronounced after upper abdominal surgery. The full- blown picture may not be present immediately after surgery, but only appear on the following day. The changes are maximal during the first 2-3 days with gradual recovery over the next week.
The magnitude of postoperative hypoxemia is a function of a patient's preoperative CCFRC ratio (1,34) and age [postoperative Pao, = 94.3 - 0.455 age (77)]. In all likelihood, postoperative hypoxemia is a major
consequence of the deranged pulmonary mechanics (20) through the influence of the latter on ventilation to perfusion mismatching. This view is supported by the report that together with an age-related value of PAo, after surgery, FRC and increased unevenness of inspired air distribution also are functions of age (58). In the latter study, the slope of the age/Pao2 relationship was steeper after anesthesia, meaning that older subjects will be relatively more hypoxemic. Postoperative hypoxemia may theoretically be a con- sequence of intraoperative hyperventilation (97).
During the few hours immediately after elective prostatectomy, healthy older patients have increased minute ventilation and cardiac output with ValQ mis- matching (88).
Control and Pattern of Breathing The effect of any factor on breathing control in hu- mans is determined by measuring the increase in min- ute ventilation after a specific stimulus. The latter is either induced hypercapnia or induced hypoxia. In healthy older people (about 70 years old) the venti- latory response to either stimulus is half of that in young persons (average age 25.6 years) (59). This ob- servation indicates the degree of blunting of the ven- tilatory response to hypercapnia and hypoxia by ag- ing but does not explain the mechanism of that blunting. The mechanism can be identified if the mea- surements and analytic techniques employed allow the use of the model of the control of breathing pro- posed by Clarke and von Euler (14). These authors suggested that the final output of the ventilatory con- trol system should be viewed as consisting of two physiologic components. The first, an inotropic effect, is the generation of inspiratory flow (V,) after con- traction of muscles of respiration. The magnitude of V1 can be estimated by the ratio of tidal volume to inspiratory duration (VT/TI). Before the neural output from the respiratory center can be transformed into actual flow, that output first must be transformed into
Table 3 . Age and Pao2 during Anesthesia with Spontaneous Ventilation
References F~oz N Equation r P Comments
(13,66,78) 0.21 30 Paoz = 95.0 - 0.49 age 0 45 0.01 (pooled data)
(78) 0.28 12 = 156.5 - 1.1 age 0.46 NS Wahba c 0.4 45 = 191.5 - 1.03 age 0.60 0.001 See Figure 7
(unpublished data) (67,78,80,86) c 1.0 65 = 549.2 - 3.09 age 0.41 0.001 Data from (67,86) during
(pooled data) the appropriate phase of the studv.
NS, not significant

AGING AND LUNG FUNCTION ANESTH ANALG 771 1983;62:76476
pressure due to muscle contraction. The pressure gen- erated at the mouth in the first 0.1 s during intentional occlusion of the airway during inspiration [occlusion pressure (Po,.l)] is a valid index of central neuro- muscular drive to breathing (73). Measuring Poo.l will enhance the investigative methodology because oc- clusion pressure is not influenced by pulmonary me- chanics, which is the case for V,. Also, the ratio of Po to V, (effective impedance) is a valuable, simple, and noninvasive index of pulmonary mechanics. The other component is a phase-duration timer (i-e., chrono- tropic activity), which determines inspiratory, expi- ratory, and total cycle duration (TI, TE, and TTOT).
Factors that influence ventilation can effect one or both components by acting on the gain of either out- put. The model and analytic technique needed can be easily understood by referring to Figure 8. The mechanism whereby aging leads to reduced ventila- tory response to hypoxia and hypercarbia has been defined by this approach (82).
The influence of both stimuli on frequency, TI, and TI/TToT in young normal subjects (mean age 24.4 years)
FiPure 8. Control of breathing: physiologic model. The two basic outputs are ventilatory drive and phase timing. Ventilatory drive can be measured by actual flow (V,) or mean flow (VTTI) and by occlusion pressure (PO). Occlusion pressure is not affected by lung mechanics at the time of measurement, as is flow rate. But occlusion pressures do not differentiate between central drive and ventilatory pump function. In awake subjects we can only use the pressure at 0.1 s after the start of inspiration. The duration of the phases are read off the horizontal.axis of the tracing. Any change in V, could be due to a change in VI, with a constant TI, or a change in TI with a constant V,, or by combinations. Changes in T T o T will be noted as changes in frequency because f = 60/TToT. The ratio of TI to TT,, indicates the portion of each breath during which inspiratory gas flow occu~s. Minute volume (Ve) = VT/TI X TI/TTOT X 60. The ratio of Po to V, is effective impedance, while that of V T / P is effective elastance, the reciprocal of compliance. [See (38) for more details.] Inspiratory flow probably originates from the dorsal and ventral respiratory groups of neurones (DRA, VRG) in the medulla (4). The timing mechanism is probably related to the pontine pneu- motaxic center (4).
Ventilatory Drive Timing I\
, \ # ,
I I \ I
Neuromuscular j I'
output ( P O ) ; j T* 1101 j
inspiratory j I I
.8r 1 8 I
, I I I
I I I
Flow (Vd ; j, V i = 0.5
I I
I
rn
s I
m 'c1 . 2 i= I
I I
0 0.5 1.0 1.5 2.0 2 5 3.0
I I
I
rn
s I
m 'c1 . 2 i= I
I I
0 0 5 1.0 1.5 2.0 2 5 3.0 Time (s)
- T V -1E- . T~ar=6O/ f .
is very similar to that in older healthy subjects (mean age 73.3 years). However V1, and hence minute vol- ume, is significantly greater in younger subjects. Thus the lesser increase in ventilation in older subjects is not due to a change in the response of the timing mechanism. Occlusion pressure and the resulting flow are of a lesser magnitude in the aged. This could be due either to a reduced central output or to a reduced responsiveness by the ventilatory pump (chest wall and diaphragm). The rib cage contribution to tidal volume is less, but not significantly so, in the younger group. We do not know whether or not the abdominal muscles and diaphragm responded differently in the two groups. An interesting observation can be made when the mean values ( ? SEM) of Po and V, for both groups are plotted along effective impedance iso- pleths. Surprisingly, older patients operate along lesser impedance isopleths (5 cm H20/L/s), (Fig. 9(A)). These studies were performed with subjects in the seated position. They may have been able, therefore, to breathe more freely than if they had been supine. The values of Po in 28 awake unpremedicated supine sur- gical patients (38) are shown in Figure 9(B), together with the calculated best-fit line. There is clearly a trend for Po to decrease with age. In summary, older sub- jects generate less ventilatory driving pressure both at rest and during hypoxia and hypercapnia.
The increase in ventilation during hypoxia and hy- percapnia is a useful clinical sign and also a homeo- static response. The fact that these responses are blunted in older subjects indicates that simple clinical observation of ventilatory frequency and chest move- ment with breathing may not be sufficient. The car- diovascular responses under these circumstances (heart rate and blood pressure increases) also are blunted with aging (28,59).
The clinician will realize that together with these age-related reduced responses in the awake state, the ventilatory responses to hypercapnia are reduced by narcotic premedication (50),and by thiopentone and narcotic and inhalational anesthetics in a dose-related manner (50). Subjects with chronic resistive loads [i.e., low forced expiratory volume (FEV,.,)], have a lesser response than normal patients (84). The decrease in FRC during general anesthesia is greater in patients with low FEVl.o (51), such that their ventilatory pump is less efficient. One must wonder to what extent ventilatory mechanics play a role in the reduced re- sponse to hypercapnia that patients with chronic ob- structive lung disease exhibit. However, not all pa- tients with chronic obstructive lung disease respond identically to added ventilatory loads. This may de- pend on the relative absence or presence of endog- enous endorphin elaboration (92). Drug therapy also

ANESTH ANALG 1983;62:764?6
772 WAHBA
Eflective Impedance (cm H20/l/sec) 2.00
1.75 h u v)
1 1.50
2 1.25 3
v
Q1 c
0
> 0
!z 1.00 L - 2 0.75 .- a v) c - 0.50
0.25
5
4 h
0, = 3
- 2 0
E, Y
a 1
n
a .
a
a . '--. .. a \.\. a a a
a -. -. *-% .. --- z
-- --- a . a a -------a,
a
I 1 I I I I 1
a
LI 1 I I I I 1
0 2 4 6 8 1 0 20 30 Occlusion Pressure (cm H,O)
Figure 9 lnspiratory flow rates, occlusion pressures, and age. (A) Mean ( 2 SEM) values of V, and I"' during induced hypoxia and hypercapnia. The fine, radially displayed lines are the effective impedance isopleths. Full details in text. Data taken from (82). (B) Occlusion pressure for 28 supine patients. The data indicate an age-related decrease in I?' at rest. Data taken from (38).
has an influence. Patients on beta adrenergic blockers (89) and dopamine (79) have blunted cardiovascular and ventilatory responses.
The breathing pattern in eupneic humans was ex- amined in a large study (56). Beginning at age 20 years, tidal volume decreases while frequency in- creases. The duration of expiration decreases with age, as does the ratio of TI to TTOT. Minute ventilation, however, does not change. These trends probably reflect the adaptation to progressive stiffness of the chest wall. Therefore, a slightly reduced tidal volume with a moderate tachypnea is to be expected in healthy, older subjects. The study also examined the influence of absolute body weight. Tidal volume increases while frequency decreases with body weight irrespective of age.
The authors reported that, irrespective of the val- ues of tidal volume and frequency, V, in all age groups (classified by decades) is nearly the same, 0.32-0.35 Lis. This observation indicates that the final interac- tion between neural drive and ventilatory response is the generation of a very specific inspiratory flow common to all age groups.
Postoperative Management The mortality in elderly patients after surgery has been reported to be about 3.5-6.2% (22,74). In these
40 50 60 70 80 Age (Years)
two reports, deaths due to pulmonary factors consti- tuted 33% and 48%, respectively. The close exami- nation of these two and other reports (15,16) reveals very interesting information. The mortality in patients over 60 years of age is almost three times that in patients less than 60 years old. Emergency operations increase mortality risk threefold in older patients. Preexisting disease (if controlled beforehand) in- creases the mortality fourfold, but if the concomitant disease is acute, mortality increases by 44.1%. There is no data to suggest that age alone increases risk. Indeed, the unfavorable prognosis may be almost en- tirely due to the concomitant disease rather than age or the scheduled operation. Cardiopulmonary causes, together with sepsis/peritonitis account for about 50% of the deaths (16). These considerations raise two questions: why are older patients at such risk and how should we manage these patients? The causes can be grouped under the following four headings.
Preoperative Pulmonary Status. The fact that older patients have some of the features of chronic obstruc- tive pulmonary disease(C0PD) should not imply that they should be considered as having COPD. Chronic bronchitis and obesity however, do increase the risk, as does chronic left-heart disease.
Postoperative Lung Function. This essentially con- sists of a mix of restrictive and obstructive lung dis- ease. The whole picture may not be apparent im- mediately after surgery, but the changes are present maximally during the first 2-3 days after the opera- tion. However, other factors may be present in the recovery period that will increase the risk. These pa-

AGING AND LUNG FUNCTION 773 ANESTH ANALG 1983;62:764-76
tients may be hypoxemic and they are breathing at a mechanical disadvantage. The risk is increased by the supine position and by the use of narcotic analgesics in an age group that already has blunted ventilatory reflexes to hypoxia and hypercapnia. Any residual anesthetic also will exert an effect. The elimination of narcotics and muscle relaxants may be delayed due to the impaired renal function in older patients (3). The effects of large volumes of crystalloid infusion may manifest in the recovery room (60).
Cardiopulmonary Reserve. Normal, older subjects have decreased ability to increase and maintain ven- tilation at high levels during periods of increased de- mand for oxygen (76). Ventilatory muscle fatigue is quite likely to occur early due to the altered physi- ology of voluntary muscle (95). Older patients have a reduced cardiac index (9) and a reduced ability to increase heart rate under such circumstances (2,91). Therefore, they cannot efficiently increase oxygen transport. Accordingly, the increased oxygen extrac- tion may lead to an enlarged arterio-venous oxygen content difference that will further increase hypox- emia. The period during which this extra demand is made is when the patient’s ventilatory apparatus is maximally disadvantaged. Most cardio-pulmonary complications occur at that time. The oxygen demand increases when there is hypoxemia, acidemia, hypo- or hyperthermia, or when cardiac output is low. The ability to increase ventilation will be limited by any
coexistent pulmonary disease. A low fixed cardiac output due to disease also will limit the response to increased oxygen requirements. Additionally, older patients perceive and respond to increased loads (be they resistive or elastic) less efficiently than younger patients (98,99). The limited ability of older patients to maintain higher levels of ventilation and circula- tion, particularly if cardio-pulmonary disease also is present, can lead to ventilatory inadequacy and fail- ure. Obviously this is more likely to occur after major abdominal surgery. The subjective feature of venti- latory inadequacy is dyspnea. Dyspnea is related to the peak subatmospheric intrapleural pressure during maximal inspiration (70). This relationship is the physio- logic basis of the use of peak inspiratory force as a test of instituting or discontinuing controlled ventilation. It seems reasonable to assume that older patients will be dyspneic earlier for any given ventilatory load.
Protective Airway Reflexes. Older patients have fewer cilia and their tracheo-bronchial tree is less able to recognize the presence of foreign bodies or noxious substances (85). Coughing is less efficient in terms of volume, force, and flow rate. In view of the above discussion designed to emphasize the added risk in geriatric anesthesia, particularly in patients with con- comitant disease, we now look at what can be done to prevent postoperative pulmonary complications.
The first step must be an adequate assessment and the correction of any abnormality noted in the phys-
Table 4. Functional Classification and Suggested Management (43,90,94) I I1 111 IV
Evaluation tests Spirometry
FEV,,/FVC FEF 25% to 75% FVC (% predicted) plus FEVl,o (%VC) FVC
Pao, Shunt PaCo2 (torr) VDJVT
Blood gases
Intraoperative management
Postoperative management
>50%
> 150 >loo >45% predicted
>65% predicted
>25% <25%
<loo <lo0 and FVC <10ml/kg <45% predicted
>65% predicted
Normal >75% predicted >50% predicted <50% predicted Normal Normal <48 >48
37 * 10% 48 -C 2%
The critical factor has to be the anesthesiologist rather than the agent or technique
Incentive spirometry sPEEP physiotherapy plus ?CMV + PEEP supplemental Oz
Posture: sitting up ?CMV 2 PEEP
Consider the value of continuous epidural analgesia (narcotics or anesthetics) u continuous or intermittent intravenous analgesia
CMV, continuous mandatory ventilation; PEEP, positive end-expiratory pressure; sPEEP, same during spontaneous ventilation

774 ANESTH ANALG 1983;62:761-76
WAHBA
ical examination and laboratory tests. For operations other than pulmonary resection, the assessment should consist of the determination of expiratory volumes and flow rates and arterial blood gases. That infor- mation can be used to classify the patient into one of four possible groups (Table 4). Some also measure an index of left ventricular stroke work (63). The anes- thetic technique and agents are of less importance than the degree of preparedness and the acumen of the anesthesiologist. The anesthetic requirements de- crease with age (96). The management of the patient after major abdominal or orthopedic surgery will de- pend on the preoperative classification, For patients in groups I and 11, a stir-up regimen, incentive spi- rometry, and oxygen-enriched air in age-dependent doses (61) may be sufficient. The need to institute any measure that restores FRC even partially must be stressed. The seated position increases FRC and could be the equivalent of 10 cm H20 positive-end expira- tory pressure (PEEP) (15). The seated position can improve gas exchange (20). Epidural analgesia with adequate intravenous hydration has no detrimental effects on FRC, VC, and gas exchange (106) and may be useful, although the restoration of FRC and VC is not complete (21).
For patients in groups I11 and IV, one must seri- ously consider instituting either controlled ventilation with PEEP or the latter with spontaneous ventilation (sPEEP) preemptively. In this context, a knowledge of CCiFRC may be useful in order to provide an in- spiratory lung volume (FRC plus tidal volume) that is greater than CC (108). For patients scheduled for pulmonary resection, the assessment also should in- clude tests that indicate whether the remaining lung tissue would be adequate for gas exchange.
The patient’s nutritional status also is very impor- tant. There is clear evidence that undernourished pa- tients breathe shallowly, have poor ventilatory re- sponses to COz, and do not sigh. This situation is reversed after appropriate dietary intake (Rosenbaum SH, Askanazi J, Hyman AI, Silverberg BA, Milic-Emili J, knney JM. Respiratory patterns in profound nu- tritional depletion (Abstracts). Anesthesiology 1979; 51 :S366).
D. B. Craig, 8. E. Marshall, D. Bevan, and D. M. M. Gillies gave me very valuable advice during the preparation of this text that I very gratefully acknowledge.
References 1. Alexander JI, Spence AA, Parikh RK, Stuart B. The role of
airway closure in postoperative hypoxaemia. Br J Anaesth 1973;45:34-40.
2. Astrand P-0. Human physical fitness with special reference to sex and age. Physiol Rev 1956;36:307-35.
3. Bender AD. Pharmacodynamic principles of drug therapy in the aged. J Am Geriatr SOC 1974;22:296-303.
4. Berger AJ, Mitchell RA, Severinghaus JE. Regulation of res- piration. N Engl J Med 1977;297:92-7.
5. Billiet L, Baisier W, Naedts JP. Effet de la taille, du sexe et de l’dge sur la capacite de diffusion pulmonaire de l’adulte normal. J Physiol (Pans) 1963;55:199-200.
6. Bindslev L, Hedenstierna G, Santesson J, Norlander 0, Gram I. Airway closure during anaesthesia and its prevention by positive end expiratory pressure. Acta Anaesth Scand 1980; 22: 199-205.
7. Black LF, Hyatt RE. Maximal respiratory pressure: normal val- ues and relationship to age and sex. Am Rev Respir Dis 1969;99:696-702.
8. Boothby WM, Berkson J, Dunn HL. Studies of the energy of metabolism of normal individuals: a standard for basal metab- olism with a nomogram for clinical application. Am J Physiol
9. Brandfonbrenner M, Landowne M, Shock NW. Changes in cardiac output with age. Circulation 1955;12:557-66.
10. Briscoe WA, DuBois AB. The relationship between airway re- sistance, airway conductance and lung volume in subjects of different age and body size. J Clin Invest 1958;37:1279-85.
11. Buist AS, Ross BB. Predicted values for closing volumes using a modified single breath nitrogen test. Am Rev Respir Dis 1973;107:744-52.
12. Buist AS. Early detection of airway obstruction by the closing volume technique. Chest 1973;64:495-9.
13. Campbell EJM, Nunn JF, Peckett BW. A comparison of artificial ventilation and spontaneous respiration with particular refer- ence to ventilation-blood flow relationship. Br J Anaesth 1958;30: 166-75.
14. Clark F, von Euler C. On the regulation of depth and rate of breathing. J Physiol (London) 1972;222:267-95.
15. Cogbill CL. Operation in the aged. Arch Surg 1967;94:202-5. 16. Cole WH. Medical differences between the young and the aged.
J Am Geriatr SOC 1970;18:589-614. 17. Cohn JE, Donoso H. Mechanical properties of lung in normal
men over 60 years old. J Clin Invest 1963;42:1406-10. 18. Cohn JE, Shock NW. Blood volume studies in middle-aged and
elderly males. Am J Med Sci 1949;217:388-91. 19. Cotes JE, Rossiter CE, Higgins ITT, Gilson JC. Average normal
values for the forced expiratory volume in white Caucasian males. Br Med J 1966;1:1016-9.
20. Craig DB, Wahba WM, Don HF, Couture JG, Becklake MR. “Closing volume” and its relationship to gas exchange in seated and supine positions. J Appl Physiol 1971;31:717-21.
21. Craig DB. Postoperative recovery of pulmonary function. An- aesth Analg 1981;60:46-52.
22. Djokovic JL, Hedley-Whyte J. Prediction of outcome of surgery and anesthesia in patients over 80. JAMA 1969;242:2301-6.
23. Don HF, Wahba WM, Cuadrado L, Kelkar K. The effect of anesthesia and 100 percent oxygen on the functional residual capacity of the lungs. Anesthesiology 1970;32:521-9.
24. Don HF, Craig DB, Wahba WM, Couture JG. The measurement of gas trapped in the lungs at functional residual capacity and the effects of posture. Anesthesiology 1971;35:582-90.
25. Don HF, Wahba WM. Craig DB. Airway closure, gas trapping and the functional residual capacity during anesthesia. Anes- thesiology 1972;36:533-9.
26. Donevan RE, Palmer WH, Varvis CJ, Bates DV. Influence of
1936;116:468-84.
AGING AND LUNG FUNCTION ANESTH ANALG 775 1983;62:764-76
age on pulmonary diffusing capacity. J Appl Physiol1959;14483- 92.
27. Dueck R, Young I, Clausen J, Wagner PD. Altered distribution of pulmonary ventilation and blood flow following induction of inhalational anesthesia. Anesthesiology 1980;52:113-25.
28. Duke PC, Wade JG, Hickey RF, Larson CP. The effects of age on baroreceptor reflex function in man. Can Anaesth SOC J
29. Edelman NH, Mittman C, Norris AH, Shock NW. Effects of respiratory pattern on age differences in ventilation uniformity. J Appl Physiol 1968;24:49-53.
30. Emirgil C, Sobol BJ, Campodonico S, Herbert WM, Mechkati R. Pulmonary circulation in the aged. J Appl Physiol1967;23:631- 40.
31. Englert M. Le reseau capillaire pulmonaire chez l’homme; etude physiopathologique. Paris: Masson et Cie, 1967.
32. Ferris BG, Frank NR, Mead J. Effect of body position on esoph- ageal pressure and measurement of pulmonary compliance. J Appl Physiol 1959;14:521-4.
33. Ferris BG, Anderson DO, Zickmantel R. Prediction values for screening tests of pulmonary function. Am Rev Respir Dis 1965;91:252-61.
34. Fibush EE, Rehder K, Sessler A. Preoperative CCiFRC ratio and postoperative hypoxemia. Anesthesiology 1975;43:481-5.
35. Fowler WS. Lung function studies V. Respiratory dead space in old age and in pulmonary emphysema. J Clin Invest 1950;29:1439-44.
36. Fowler WS, Cornish ER, Kety SS. Lung function studies VIII. Analysis of alveolar ventilation by pulmonary N, clearance curves. J Clin Invest 1952;31:40-50.
37. Frank NR, Ferris BG, Mead J. The mechanical behavior of the lungs in healthy elderly persons. J Clin Invest 1957;36:1680-7.
38. Germain MG, Wahba WM, Gillies DMM. Ventilation following induction of general anaesthesia with thiopentone. Can An- aesth SOC J 1982;29:100-4.
39. Gilmour J, Burnham M, Craig DB. Closing capacity measure- ment during general anesthesia. Anesthesiology 1976;45:477- 82.
40. Gillies IDS, Petrie A, Morgan M, Sykes MK. Analysis of pos- sible factors influencing Pao2 and (PAo, - Pao,) in patients awaiting surgery. Br J Anaesth 1977;49:427-37.
41. Gold M, Helrich M. Pulmonary compliance during anesthesia. Anesthesiology 1965;26:281-8.
42. Goldman HI, Becklake MR. Respiratory function tests: normal values at median altitudes and the prediction of normal results. Am Rev Tuberculosis 1959;79:457-67.
43. Gracey DR, Divertie MB, Didier EP. Preoperative pulmonary preparation of patients with chronic obstructive pulmonary disease. Chest 1979;76:123-9.
44. Hedenstierna G, McCarthy G, Bergstrom M. Airway closure during mechanical ventilation. Anesthesiology 1976;44:114-23.
45. Hedenstierna G, Santesson J. Airway closure during anes- thesia: a comparison between resident gas and argon-bolus techniques. J Appl Physiol 1979;47874-81.
46. Heinonen AO, Karvonen MJ, Kihlberg J. Subdivision of total lung volume and the maximum breathing capacity in firemen: age changes and correlation to body size. Ann Med Intern Fenn
47. Helliesen PJ, Agathon S, Cook CD, Friedlander L. Studies of respiratory physiology in children. I: mechanics of respiration and lung volumes in 85 normal children 5-17 years of age. Pediatrics 1958;22: 80-93.
48. Hewlett AM, Hulands GH, Nunn JG, Heath JR. Functional
1976;23: 11 1-24.
1962;51(~~pp 39): 1-13.
residual capacity during anaesthesia. 2. Spontaneous respira- tion. Br J Anaesth 1974;46:486-94.
49. Hewlett AM, Hulands GH, Nunn JF, Milledge IS. Functional residual capacity during anaesthesia. 3. Artificial respiration. Br J Anaesth 1974;46:495-503.
50. Hickey RF, Severinghaus JW. Regulation of breathing: drug effects in: Hornbein TF, ed. Regulation of breathing, Part 11. New York: Marcel Dekker Inc, 1981:1251-312.
51. Hickey RF, Visick W, Fairley HB, Fourcade HE. Effects of hal- othane anesthesia on functional residual capacity and alveolar- arterial oxygen tension difference. Anesthesiology 1973;38:20- 4.
52. Higgins I T , Oldham PD. Ventilatory capacity in miners. A five-year follow-up study. Br J Indust Med 1962;19:65-76.
53. Holland J, Milic-Emili J, Macklem PT, Bates DV. Regional dis- tribution of pulmonary ventilation and perfusion in elderly subjects. J Clin Invest 1968;47:81-92.
54. Holley HS, Milic-Emili J, Becklake MR, Bates DV. Regional distribution of pulmonary ventilation and perfusion in obesity. J Clin Invest 1967;46:475-81.
55. Hsu HO, Hickey RF. Effect of posture on functional residual capacity postoperatively. Anesthesiology 1976;44:520-1.
56. Jammes Y, Auran Y, Gouvernet J, Delpierre S, Grimaud, C. The ventilation pattern of conscious man according to age and morphology. Bull Eur Physiopathol Respir 1979;15:527-40.
57. Juno P, Marsh HM, Knopp TJ, Rehder K. Closing capacity in awake and anesthetized-paralyzed man. J Appl Physiol 1978;44:238-44.
58. Kitamura H, Sawa T, Ikezomo E. Postoperative hypoxemia: the contribution of age to the maldistribution of ventilation. Anes- thesiology 1972;36:244-52.
59. Kronenberg RS, Drage GW. Attenuation of the ventilatory and heart rate responses to hypoxia and hypercapnia with aging in normal man. J Clin Invest 1973;52:1812-9.
60. Laver MB, Hallolwell P, Goldblatt A. Pulmonary dysfunction secondary to heart disease. Anesthesiology 1970;33:161-92.
61. Leigh JM. Postoperative oxygen administration. Br J Anaesth 1975;47: 108-12.
62. Leuallen EC, Fowler WS. Maximal mid-expiratory flow. Am Rev Tuberculosis 1955;72:783-800.
63. Lewin I, Lerner AG, Green SH, DelGuercio LRM. Physical class and physiologic status in prediction of operative mortality in the aged sick. Ann Surg 1971;174;217-31.
64. Luce JM. Respiratory complications of obesity. Chest 1980;78:626- 31.
65. Macklem PT, Proctor DF, Hogg JC. The stability of peripheral airways. Respir Physiol 1969-70;8:191-203.
66. Marshall BE, Grange RA. Changes in respiratory physiology during etherlair anaesthesia. Br J Anaesth 1966;38:329-38.
67. Marshall BE. Physiological shunting and dead-space during spontaneous respiration with halothane-oxygen anaesthesia and the influence of intubation on the physiologcal dead-space. Br J Anaesth 1966;38:912-22.
68. Marshall BE, Cohen PJ, Klingenmaier CH, Aukberg S. Pul- monary venous admixture before, during, and after halothane- oxygen anesthesia in man. J Appl Physiol 1969;27:653-7.
69. Marshall BE, Wyche MQ Jr. Hypoxemia during and after anes- thesia. Anesthesiology 1972;37:178-209.
70. Marshall R, Stone RW, Christie RV. The relationship of dysp- nea to respiratory effort in normal subjects, mitral stenosis and emphysema. Clin Sci 1954;13:625-31.
71. McCarthy DS, Spencer R, Greene R, Milic-Emili J . Measure- ment of “closing volume” as a simple and sensitive test for

WAHBA
earl\, detection 01 small airway disease. Am J Med 7972;52:717- 53.
72. Mellemgaard K. The alveolar-arterial oxygen difference: its size and c-onipontmts in normal man. Acta Physiol Scan 1966;67:10- 20.
73 Milic-Emili J , Whitelaw WA, Derenne JPh. Occlusion pressure: a simple measure c)f the respiratory center's output. N Engl J Med 1975;293.102Y-30.
71 Morgan RM. Hirata RM, Jacques DA, Hoopes JE. Head and neck stirgerv in the aged. Am J Surg 1982;144:4.19-31,
77, Niervoehncr DE. Kleinerman J . Morphologic basis of pulmo- nary rtwstance in the human lung and effects of aging. J Appl Phvsioi 1Y74;36:.112-8
7h Norris AH, Shock NM', Yiengst MJ. Age differences in venti- lation and gas exch'3nge responses to graded exercises in males. J Geron to1 1958; 10: 143-55.
77. Nunn IF. Applied respiratory physiol. 2nd ed. London: But- terivorths. 1977:434-7.
7X. Nunn I F . Factor.; influencing the arterial oxygen tension during halothme maesthesia ivith spontaneous respiration. Br J An- aesth li)64,3h:327-11
79. Olson ILG, Hcmsley MJ, Saunders MA. Ventilate? respon- si\>ent+i to hypercapnic hypoxia during dopamine infusion in humans. Am Rev Respir Dis 1982;126:783-7.
HI). Panda\ J , Nunn J F Failure to demonstrate progressiLre falls of artvrial PO during anaesthesia. Anaesthesia 1968;23:38-46.
X I Permutt S, Martin HB. Static pressure-volume characteristics ot lungs in normal males J Appl Physiol 1960;15:819-25.
82. Peterson DD, Pack Al, Silage DA, Fishman AP. Eftect of aging on ventilatory and occlusion pressure responses to hypoxia and hypercapnia Am Rev Respir Dis 1981;124:387-91.
83. Pierce 1.4. Tensile .;treng:th of the human lung. J Clin Invest 196i,66:652-K.
X.1. Pietak S . M'twng CS. Hickey RF, Fairley HB. Anesthetic effects on ventilation in patients with chronic obstructive pulmonan disease. Anesthesiology 1975;12:160-6.
K5. Poiituppidan HH, Beecher HK. Progressive loss of protective reflew5 in the airiva!. with the advance of age. JAMA 1960; 1 Y 71:2209-13
Hh. Prys-Robert5 C, Kelman GR, Greenbaum R, Kain ML, Bay J . Hernodynamics and al\wdar-arterial Po, difference at varying Pac (1: in anestlietircd man. J Appl Physiol 1968;25:80-7.
87. Rainr [M, Bishop JM. A - a difference in 0, tension and phys- iological de'id space in normal man. J Appl Physiol 1963;18: 284-8.
8X. Renck t j . The elderly patient after anaesthesia and surgery. Acta Anae5th Scand 1969;13(supp 34):l-136.
XY. Richardson DW, Kontos HA, Raper AG, Patterson JL. Modi- fication b!' beta-adrenergic blockade of the circulatory response t o aciitc hvpokia in man J Clin Invest 1967;16:77-85.
90 Rigg J l i A , Jones NL Clinical assessment of respiratory func- tion. Hr J Anaesth 197H;50:3-13.
91. Robinson S kkperimental studies of physical fitness in relation t o age Arltt.it.;phv..iolc)gie 1938;10:251-323.
92. Santiago TV, Remolina C, Scoles V 111, Edelman NH. Endor- phins and the control of breathing. N Engl J Med 1981;304:1190- 5.
93. Severinghaus JW, Stupfel M. Alveolar dead space as an index of distribution of blood flow in pulmonary capillaries. J Appl Physiol 1957;10:335-48.
94. Shapiro BA. Interpretation of pulmonary function tests. ASA Refresher Course Lectures, 1981, No. 212.
95. Shock NW. Physiological aspects of aging in man. Annu Rev Phvsiol 1961;23:97-122.
96. Stel'ens U'C, Dolan WM, Gibbons CT, et al. Minimum alveolar concentrations (MAC) of isoflurane with and without nitrous oxide in patients of various ages. Anesthesiology 1975;42:197- 200.
97. Sullivan SF, Patterson RW. Posthyperventilation hypoxic: the- oretical considerations in man. Anesthesiology 1968;29:981- 6.
98. Tack M, Altose MD, Cherniack NS. Effect of aging on respi- ratory sensations produced by elastic loads. J Appl Physiol 1981;50:846-50.
99. Tack M. Altose MD Cherniack NS. Effect of aging on the perception of resistive ventilatory loads. Am Rev Respir Dis 1982;126:.163-7.
100. Tenney SM, Miller RM. Dead space ventilation in old age. J Appl Physiol 1956;9:321-7.
101. Thurlebeck WM. Internal surface area and other measure- ments in emphysema. Thorax 1967;22:483-96.
102. Turner JM, Mead J, Wohl ME. Elasticity of human lungs in relation to age. J Appl Physiol 1968;25:664-71.
103. Wahba WM. Influence of airways resistance and ventilatory pattern on Paco, during enflurane anaesthesia. Br J Anaesth 197951: 123-6.
10.1. Wahba U'M, Sadkova J . Atropine reversal of hypercarbia dur- ing enflurane anaesthesia. Br J Anaesth 1979;51:221-6.
105. Wahba WM. Factors influencing arterial oxygen tension. Br J Anaesth 1978;50:409.
106. Wahba Whl, Craig DB, Don HF, Becklake MR. The cardio- respiratory effects of thoracic epidural anesthesia. Can An- aesth Soc J 1972;19:8-19.
107. LVahba WM. Body build and preoperative arterial oxygen ten- .;ion. Can Anaesth Soc J 1975;22:653-8.
108. Weenig CS, Pietak S, Hickey RF, Fairley HB. Relationship of preoperative closing volume to functional residual capacity and alveolar-arterial oxygen difference during anesthesia with controlled \,entilation. Anesthesiology 1974;41:3-7.
109. West JB . Blood flow to the lung and gas exchange. Anesthe- siology 197.1;41:124-38.
110. Wilson RM, Meadow RS, Jay BE, Higgins E. The pulmonary pathologic physiology of persons who smoke cigarettes. N Engl J Med 1960;262:956-61.
111. M'yche MQ, Teichner RL, Kallos T, Marshall BE, Smith TC. Etfects of continuous positive pressure breathing on func- tional residual capacity and arterial oxygenation during intra- dbdomiiiai operations. Anesthesiology 1973;38:68-74.





























