Embed Size (px)
Citation preview

Reversal Agents for NOACs(Novel Oral Anticoagulants)
CSRC Symposium Washington DCOct 18, 2016
Current status and future challenges
Paul A Reilly, PhDClinical Research, Boehringer Ingelheim, Inc

Atrial fibrillation
• AF is the most common arrhythmia in clinical practice1
– In 2007, 6.3 million people in the US, Japan, Germany, Italy, Spain, France and the UK were living with diagnosed AF2
• The number of AF patients is predicted to rise3
– It is estimated 1 in 4 individuals aged 40 years or older will develop AF4
1. Go AS et al. JAMA 2001; 285:2370–2375. 2. Decision Resources. Atrial Fibrillation Report. December 2008. 3. Miyasaka Y et al. Circulation 2006; 114:119–125. 4. Lloyd-Jones DM et al. Circulation 2004; 110:1042–1046
CM-3
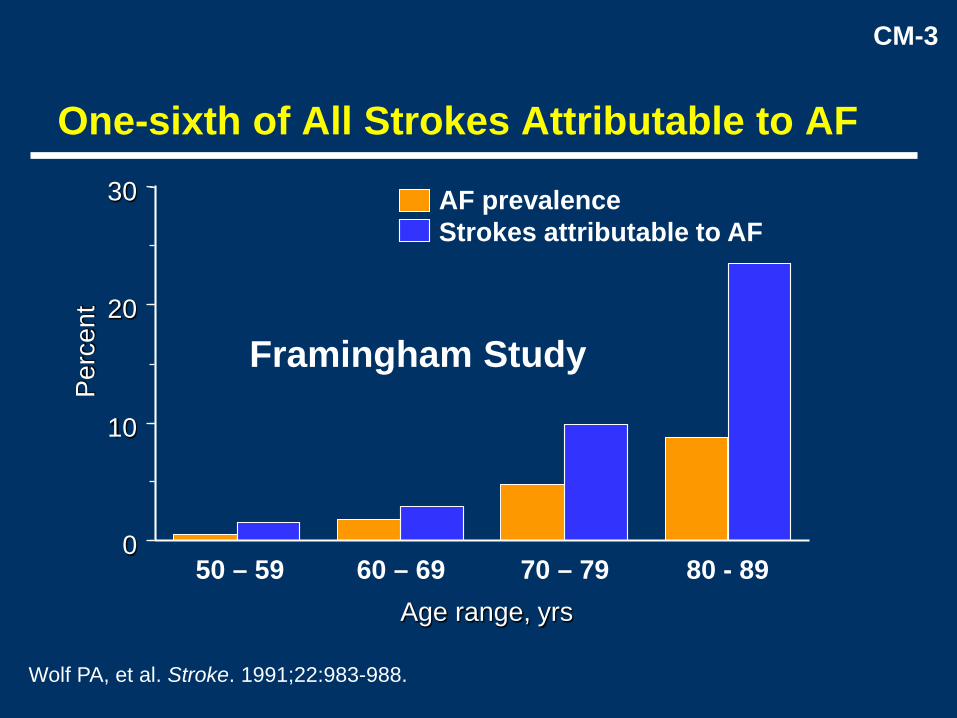
0
10
20
30
Perc
ent
AF prevalenceStrokes attributable to AF
Age range, yrs
One-sixth of All Strokes Attributable to AF
Framingham Study
50 – 59 60 – 69 70 – 79 80 - 89
Wolf PA, et al. Stroke. 1991;22:983-988.

CM-4
Study YearAFASAK I 1989; 1990
SPAF I 1991BAATAF 1990
CAFA 1991SPINAF 1992
EAFT 1993
All trials (n = 6)N = 2,900
Favors warfarin Favors placeboor control
100% 50% 0 −50% −100%
Hart RG, et al. Ann Intern Med. 2007;146:857-867.
Efficacy of Warfarin for Stroke ReductionCompared With Placebo or Control in 6 Studies
Relative risk reduction (95% CI)
Two Placebo controlled trials: CAFA and SPINAF

National Estimates of Medications Commonly Implicatedin Emergency Hospitalizations for Adverse Drug Events
In Older U.S. Adults, 2007-2009Annual National Proportion of
Medication Estimate of Emergency Dept.Hospitalizations Visits Resulting in
(N=99,628) Hospitalization
No. % (95% CI) %Most commonly implicated medications
Warfarin 33,171 33.3 (28.0-38.5) 46.2Insulins 13,854 13.9 (9.8-18.0) 40.6Oral antiplatelet agents 13,263 13.3 (7.5-19.1) 41.5Oral hypoglycemic agents 10,656 10.7 (8.1-13.3) 51.8Opioid analgesics 4,778 4.8(3.5-6.1) 32.4
Budnitz DS et al. NEJM, 2011

Why Use NOACs?
• As an alternative to warfarin– NOACs have a favourable benefit-risk profile
compared to warfarin, based on outcomes data from >71,000 patients
– Ruff et al. Lancet 2014; 383: 955-962

Stroke or systemic embolic events
Ruff et al. Lancet 2014; 383: 955-962

Major Bleeding
Ruff et al. Lancet 2014; 383: 955-962

Major Bleeding in Phase III Trials (per 100 patient-years)
Warfarin NOACRE-LY 3.6 3.3, 2.9
ROCKET 3.45 3.6
ARISTOTLE 3.1 2.1
ENGAGE 3.4 2.8, 1.6

Fatal Bleeds
Majeed et al. Circulation 2013; 128: 2325-2332

The Treatment Gap
• 3 to 4 million people in the US have AF• Of those with additional risk factors for
stroke, half are not treated with oral anticoagulants
• Of these, 5% per year experience a stroke• Of these, 70% are preventable• Over 50,000 preventable strokes each year in
the US

Can We Improve Treatment Rates?
• Fear of bleeding?– Absence of reversal agents may impede
the uptake of NOACs by both patients and physicians

Time to Reversal:Oral Versus IV Vitamin K
Lubetsky A et al. Arch Intern Med 2003;163:2469-2473

Normalizing INR with Prothrombin Complex Concentrates (PCCs)
Sarode et al. Circulation 2013; 128: 1234-1243
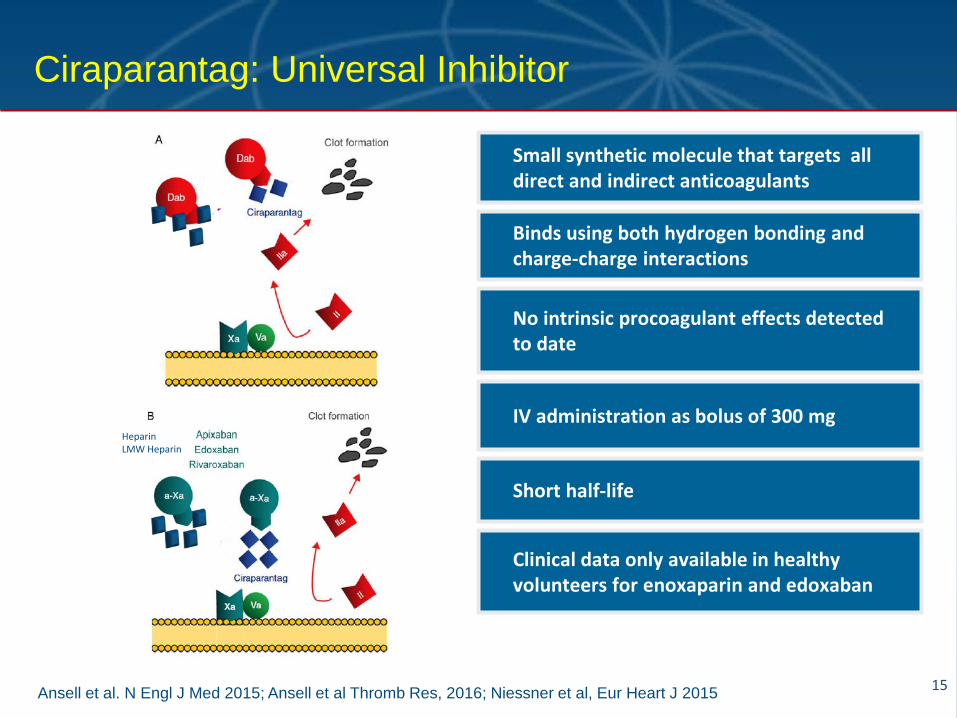
Ansell et al. N Engl J Med 2015; Ansell et al Thromb Res, 2016; Niessner et al, Eur Heart J 2015
Ciraparantag: Universal Inhibitor
15
Small synthetic molecule that targets all direct and indirect anticoagulants
Binds using both hydrogen bonding and charge-charge interactions
No intrinsic procoagulant effects detected to date
Short half-life
IV administration as bolus of 300 mgHeparinLMW Heparin
Clinical data only available in healthy volunteers for enoxaparin and edoxaban

Ansell et al NEJM 2014; Ansell et al, Thromb Res 2016
Reversal of Edoxaban and Enoxaparin in Healthy Volunteers with Ciraparantag
Reversal measured using whole blood assay
Enoxaparin Edoxaban

Ciraparantag: Opportunities & Challenges
Opportunities• Small molecule• Universal antidote
– Apixaban– Rivaroxaban– Edoxaban– Heparins– Dabigatran
Challenges• Whole blood clotting time
(WBCT): companion diagnostic?
• By 12 h reversal effect is gone
• Highly charged cationic molecule drug-drug interactions?
• Dose-related minor AEs

Lu G et al. Nat Med 2013; Siegal DM et al. N Engl J Med 2015;
Andexanet alfa: Factor Xa reversal agent
18
Factor Xa
Andexanet alfa
Recombinant modified activated FXa, competitive binding with direct FXa inhibitors –acts as a decoy
Similar binding affinity as with endogenous FXa; binds FXa inhibitors and inactivates them
Requires reconstitution prior to IV administration; bolus + infusion
Short half-life (30–60 min)
Increased thrombin generation during andexanet alfa in healthy volunteers

Siegal DM et al. N Engl J Med 2015
Effect of andexanet alpha in reversing anticoagulant effect of factor Xa inhibitors
19
Apixaban (Annexa-A) Rivaroxaban (Annexa R)
End of bolus End of infusion
100
75
50
25
00 0.2 0.4 0.6 1 2 3 4 5 6 7 8 9 10 1211
Time after bolus (h)
Ant
i-FXa
(%)
Placebo (Part 1, n=9)
400 mg bolus + 480 mg x 2-h infusion (n=23)
Placebo (Part 2, n=8)400 mg bolus (n=24)
400
0 0.2 0.4Time after bolus (h)
Anti-
FXa
(ng/
mL)
1 2 3 4 5 6 7 8 9 10
300
200
100
0
End of bolus End of infusion
0.6
Placebo (Cohorts 1–3, n=9)
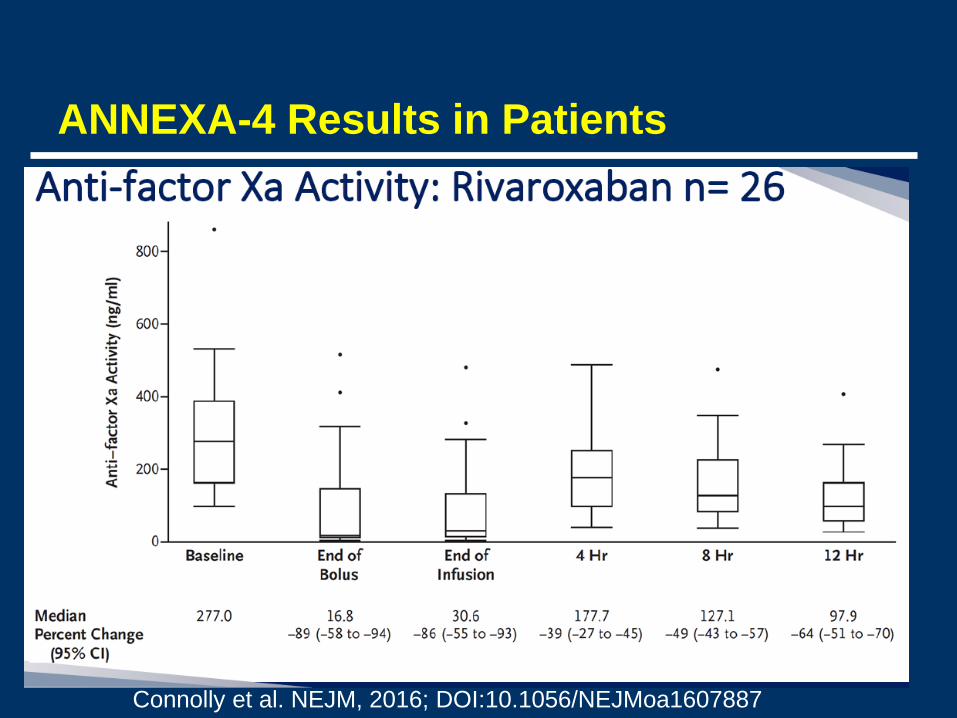
ANNEXA-4 Results in Patients
Connolly et al. NEJM, 2016; DOI:10.1056/NEJMoa1607887

Siegal DM et al. N Engl J Med 2015
Endogenous thrombin potential (ETP) with andexanet alfa in volunteers
21
2500
2000
1500
1000
500
0Baseline 0.0 0.2 0.4 0.6 2 4 6 8 10 12 14 16 2218 20
Time after bolus (h)
ETP
(nM
.min
)
Baseline range
End of bolus End of infusion Placebo (n=8)400 mg bolus + 480 mg x 2-hr infusion (n=23)
• Increase of ETP with andexanet alfa bolus
• Significant increase in thrombin generation (p<0.001)
• ETP returns to baseline range a few hours after bolus injection
• The mechanism is not clear –related to tissue factor pathway inhibitor

Andexanet: Opportunities & Challenges
Opportunities• Factor Xa antidote
– Apixaban– Rivaroxaban– Edoxaban– LMWH
• Peak reversal effect 89-93% within minutes
• Hemostasis excellent or good @12 h in 79%
Challenges• By 4 h reversal effect is
30-39%• Different dose regimens
for different agents• Possible procoagulant
effect? (thrombotic events in 18% within 30 days)
• CMC issues?
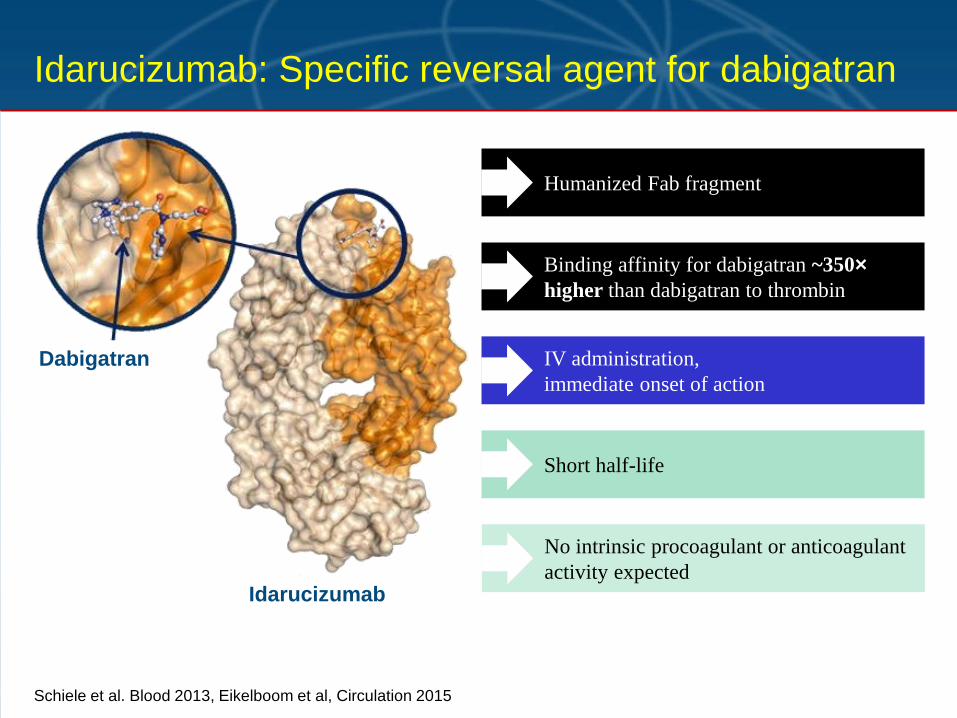
Schiele et al. Blood 2013, Eikelboom et al, Circulation 2015
Idarucizumab: Specific reversal agent for dabigatran
Dabigatran
Idarucizumab
Humanized Fab fragment
Binding affinity for dabigatran ~350×higher than dabigatran to thrombin
No intrinsic procoagulant or anticoagulant activity expected
IV administration,immediate onset of action
Short half-life
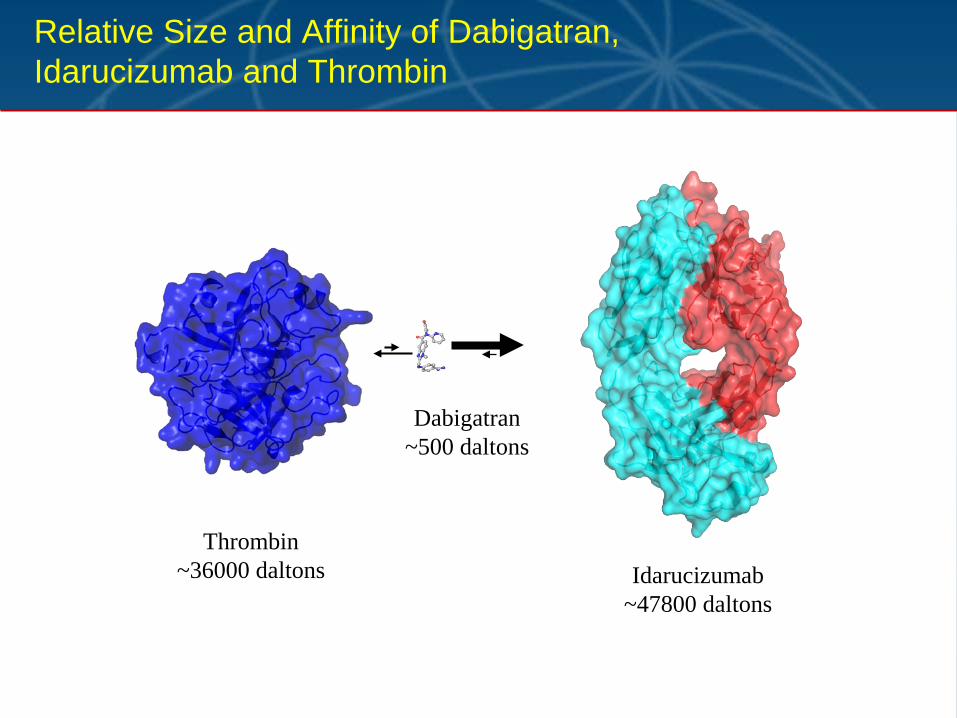
Relative Size and Affinity of Dabigatran, Idarucizumab and Thrombin
Thrombin~36000 daltons Idarucizumab
~47800 daltons
Dabigatran~500 daltons

Glund et al, Lancet 2015:S0140-6736(15)60732-2
Reversal of Dabigatran Anticoagulationby Idarucizumab in Healthy Volunteers
25
Dabigatran alone
121086420-2 24 36 48 60 72
Time after end of infusion (h)
70
65
60
55
50
45
40
35
30
dTT
(s)
+ placebo+ 1 g Fab+ 2 g Fab+ 4 g FabNormal upper limit Mean baseline
End of Idarucizumab injection (5 min infusion)
(8-9 healthy volunteers per group)
• Dabigatran prolonged clotting times of dTT, ECT, aPTT and TT
• Mean clotting times were reversed to baseline immediately after end of Fab infusion
• The effect was sustained for the 2000 and 4000 mg doses
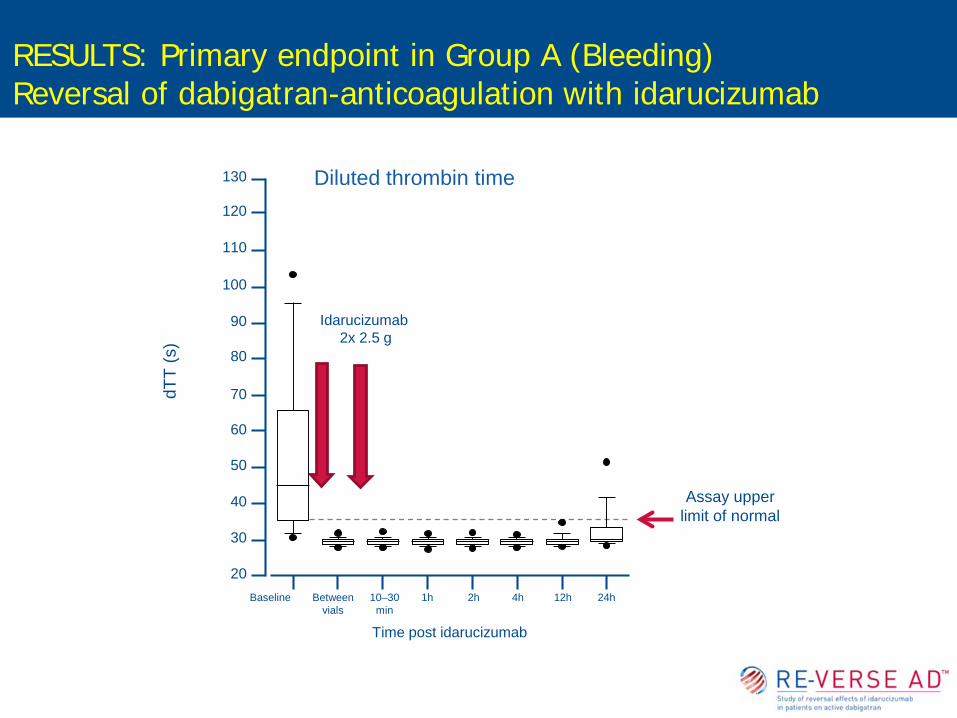
Assay upper limit of normal
Diluted thrombin time
Idarucizumab 2x 2.5 g
dTT
(s)
130
110
70
60
50
40
30
20
120
100
90
80
1h 2h 4h 12h 24hBaseline Betweenvials
10–30min
Time post idarucizumab
RESULTS: Primary endpoint in Group A (Bleeding)Reversal of dabigatran-anticoagulation with idarucizumab

Group A (n = 51)Active Bleeding
Group B (n = 39)Urgent Surgery
Unb
, dab
igat
ran
(ng/
mL)
1500
700
300
200
100
0
1000
600
500
400
1h 2h 4h 12h 24hBaseline Betweenvials
10-30min
Time post idarucizumab
Unb
, dab
igat
ran
(ng/
mL)
01h 2h 4h 12h 24hBaseline Between
vials10-30min
Time post idarucizumab
1500
700
300
200
100
1000
600
500
400
Dabigatran levels were below 20ng/ml in 89/90 patients already after infusion of first vial
Idarucizumab 2x 2.5 g
Idarucizumab 2x 2.5 g
Dabigatran levels before and after treatment with idarucizumab

No cases of hypersensitivity were observed
Five thrombotic events occurred (5 of 90=5.6%)– 1 early event (DVT + PE) within 72 hours of
idarucizumab administration
– 4 patients had events after 72 hours of idarucizumab administration (DVT, DVT+PE+LA thrombus, MI, ischemic stroke)
– None of these 5 patients was receiving any antithrombotic therapy when the events occurred
18 deaths occurred (9 in each Group)– Related to presenting index event and comorbidities
Safety
Idarucizumab: Opportunities & Challenges
Opportunities• Available in > 35
countries• Peak effect of 100%
reversal within minutes, sustained for 12-24 h
• Normal hemostasis in 93% of emergency surgery cohort
Challenges• Complete Phase III trial
as condition of approval

What specific reversal agents for NOACs are availableor in development?
Phase IIOngoing
Phase I/II
Ciraparantag(PER977)1Target: universal
Widespread availabil ity (>5500 hospitals worldwide)following local approval
ApprovalFDAOct 20154
EMANov 20155
etc.
Submitted to EMA/FDAand othersFeb/Mar 2015
Study in patients requiring urgent surgery/with major bleeding; started May 20142,3
Studies in healthy volunteers
Idarucizumab1
Target: dabigatran
Complete response letterby FDA, Aug 20168
Accepted for review by EMAAug 20169
Submitted to FDADec 20157
Study in patientswith major bleeding only; started Jan 20156
Studies in healthy volunteers
Andexanet alfa1
Target:FXa inhibitors
Idarucizumab is not approved in all countries. Please check your local prescribing information for details. Andexanet alfa is an investigational compound and is not approved in any country. 1. Adapted from Greinacher A et al. Thromb Haemost 2015; 2. Pollack C et al. N Engl J Med 2015; 3. Pollack C et al. Thromb Haemost 2015; 4. US FDA 2015 press release, 16 October 2015; 5. European Commission Community Register of Medicinal Products for Human Use 2015; 6. ClinicalTrials.gov Identifier: NCT02329327; 7. Portola Pharmaceuticals press release, 18 Dec 2015; 8. Portola Pharmaceuticals press release 17 August 2016; 9. Portola Pharmaceuticals press release 19 August 2016

Regulatory Framework (clinical)Accelerated approval
• Phase I/II trials demonstrate reversibility in volunteers– Placebo control group– Dose response– Pharmacodynamic endpoint (clotting test)
• Data in patients– Uncontrolled trial– Clinical efficacy cannot be established
• Completion of patient study for safety evaluation as post-marketing requirement
Clinical Outcomes in Reversal Trials
• Uncontrolled or life-threatening bleedingcessation of bleeding
• Emergency surgery Perioperative bleeding• Thrombotic events (DVT, PE, MI, ischemic
stroke)• Mortality • Hypersensitivity reactions

Is there a Therapeutic Benefit?
• Absent a controlled trial in the target patient population, powered to demonstrate reduction in mortality or other improvement in clinical outcomes (duration or extent of bleeding), pharmacologic endpoints are the primary basis for efficacy
• After >50 years, there is still no data to demonstrate the clinical benefit of reversal of VKAs with Vitamin K + plasma/PCCs

A Possible Indirect Benefit
• If the availability of reversal agents increases the comfort level of the physician and/or the patient, it will increase the likelihood that untreated patients will be treated with a NOAC
• An increase in the number of patients with AF who are anticoagulated may represent the true therapeutic benefit of reversal agents





























