Embed Size (px)
Citation preview

Retroperitoneal hematoma after cardiac catheterization: Prevalence, risk factors, and optimal management K. Craig Kent , MD, Mauro Moscucci, MD, Kathleen A. Mansour , MD, Susan DiMatt ia , RN, BSN, Susan Gallagher, RN, MSN, Richard Kuntz , MD, and John J. Skillman, MD, Boston, Mass.
Purpose: Retroperitoneal hematoma is an unusual, but potentially serious, complication after cardiac catheterization. The predisposing factors, typical presentation, and clinical course of this iatrogenic complication are identified, and the role of surgery in its treatment is defined. Methods: A retrospective review of 9585 femoral artery catheterizations over a 5-year period aUowed identification and evaluation of all patients with retroperitoneal hemor- rhage. Results: Retroperitoneal hematoma developed in 45 patients (overall prevalence 0.5%), with the highest frequency after coronary artery stenting (3%). In the group of patients who underwent coronary artery stenting, statistically significant predictors of this complication included protocol for sheath removal, female sex, nadir platelet count, and excessive anticoagulation. Signs and symptoms included suprainguinal tenderness and fullness in 100%, severe back and lower quadrant pain in 64%, and femoral neuropathy in 36%. Most patients were treated successfully with transfusion alone. Seven patients (16%) required operation; in four, hypotension unresponsive to volume resuscitation developed early after catheterization; and, in three, a progressive fall in hematocrit level led to surgery 24 to 72 hours after catheterization. Conclusions: Retroperitoneal hematoma after cardiac catheterization can usually be treated by transfusion alone. A small subset of patients who have development of hypotension unresponsive to volume resuscitation require urgent operation. (J VAsc SURG 1994;20: 905-13.)
As the number and complexity of diagnostic and therapeutic cardiac catheterizations continue to in- crease, there is a parallel increase in the complications that arise from femoral artery puncture. 1,2 Most often these complications, which include false aneurysm, hematoma, arteriovenous fistula, or femoral artery occlusion, are confined to the femoral artery and groin. 3-7 However, hematomas of the retroperito-
From the Harvard Medical School (Drs. Kent, Mansour, Kuntz, and Skillman), and the Departments of Surgery (Drs. Kent and Skillman and Mses. DiMattia and Gallagher) and Cardiovascular Medicine (Drs. Moscucci, Mansour, and Kuntz), Beth Israel Hospital, Boston.
Supported by the Beth Israel Surgical Trust. Presented at the Eighth Annual Meeting of the Eastern Vascular
Society, Montr&l, Quebec, Canada, May 12-15, 1994. Reprint requests: K. Craig Kent, MD, Department of Surgery,
Beth Israel Hospital, 330 Brookline Ave., Boston, MA 02215. Copyright © 1994 by The Society for Vascular Surgery and
International Society for Cardiovascular Surgery, North Ameri- can Chapter.
0741-5214/94/$3.00 + 0 24/6/59849
neum are being observed with increasing fre- quency, s,9 These hematomas are believed to arise: from inadvertent puncture of the distal external iliac, artery. The clinical spectrum ranges from a benign limited process that requires transfusion only, to one', in which uncontrolled hemorrhage with hypotension requires urgent operation. 9~1
Management decisions can be difficult. Because most of these patients have coexisting heart disease:, a retroperitoneal operation may cause significant: morbidity. The proper treatment of patients with retroperitoneal hematoma after cardiac catheteriza- tion has not been well defined. To more clearly understand this entity, we conducted a retrospective review of all patients at this institution who had[ development of retroperitoneal hematoma after car-. diac catheterization over the past 5 years.
M A T E R I A L A N D M E T H O D S
From July 1988 to July 1993, 9284 cardiac: catheterizations were performed at Beth Israel Hos-.
905

JOURNAL OF VASCULAR SURGERY 9 0 6 Kent et aL December 1994
pital. Patients who had development of a retroperi- toneal hematoma were identified by reviewing the cardiology registry and logs of two vascular surgeons (J.J.S. and K.C.K.) who were routinely called to evaluate this complication. The diagnosis of a retro- peritoneal hematoma was made by physical exami- nation in all cases and confirmed by computed tomography (CT) scanning in selected cases. Data were collected by review of hospital records and the clinical computing database. Data regarding the type of catheterization were available from the entire population of patients undergoing cardiac catheter- ization. Extensive data, including baseline demo- graphic variables, history of hypertension, sheath size, degree of anticoagulation and baseline, and follow-up laboratory data, were available for a subgroup of patients who underwent coronary artery stenting. In this subgroup, predictors of rettoperito- neal hematoma were identified with univariate logis- tic regression. Independent predictors of retroperi- toneal hematoma were identified on the basis of the tmivariant model by use of multivariate logistic regression.
RESULTS
Forty-five patients had development of retroperi- toneal hematoma during the course of this study period (prevalence 0.47%). The average age of patients with retroperitoneal hematoma was 64, compared with an average age of 58 for the entire cohort of patients who underwent catheterization. In the group of patients with retroperitoneal hematoma, 27 were women (60%), compared with a 27% prevalence of female sex in all patients who under- went catheterization.
Physical examination revealed suprainguinal ten- derness and fullness in all. These findings were usually associated with a decrease in hematocrit level that was not attributable to any other source of hemorrhage. CT scans were obtained in 30 patients, and all confirmed the presence of a retroperitoneal he- matoma. Sixty-four percent of patients experienced
*Assuming that a 3-point fall in hematocrit (Hct) is equivalent to one unit of blood, the estimated blood loss (in units) for each patient was derived as follows:
Admission Hct - Discharge Hct + Units transfused
3 points/unit This formula estimates the total blood loss for each patient during the entire hospital stay and includes losses from sources other than retroperitoneal hematoma.
significant back or flank pain usually requiring narcotics for relief. Femoral neuropathy developed in 36% of patients. The estimated blood loss was 4.6 units (range 1 to 38).* The median number of units transfused was 4.0 (range 0 to 37). All patients except four, were given a full course of heparin for varying periods beyond the initial catheterization. Twenty- four percent of patients received thrombolytic drugs, 27% were treated with dextran, and all received aspirin. Thirty percent of patients, who had subse- quent development of retroperitoneal hematoma, initially were admitted to the cardiology service with myocardial infarction. Thus these patients were severely ill even before the development of retroperi- toneal hematoma.
The prevalence of rettoperitoneal hematoma varied with the type of catheterization. Placement of a coronary artery stent was associated with the highest prevalence 10 of 5956 (3%), > percutaneous transluminal angioplasty 23/2829 (0.81%), > diag- nostic catheterization 13/433 (0.17%), > coronary atherectomy 0/367 (0%). All of these differences were statistically significant (p < 0.05).
Potential risk factors for retroperitoneal hemor- rhage were evaluated in the subset of 376 patients who had placement of a coronary artery stent. All patients treated with coronary artery stents were given a flail course of anticoagulant after the proce- dure. During the course of this study, the protocol for management of anticoagulation during femoral ar- tery sheath removal in these patients was formally changed on two occasions (Table II). Table I displays the baseline demographics, procedure variables, and laboratory data of the 376 patients treated with coronary artery stents. In a univariate analysis, factors that predisposed to the development of retroperito- neal hematoma included female sex, nadir platelet count, number of hours that the partial thrombo- plastin time (PTF) was greater than 100 seconds, and sheath removal protocol (allp values < 0.03). Mul- tivariate analysis identified nadir platelet count, female sex, and sheath removal protocol as indepen- dent predictors of retroperitoneal hemorrhage.
Seven of 45 patients with retroperitoneal he- matoma required operation (16%). Four underwent urgent operation when hypotension unresponsive to fluid replacement developed within several hours of the catheterization. Two patients had an excessive fall in hematocrit level within 24 hours of catheteriza- tion, leading to the decision for operation. In neither patient was heparin discontinued until the decision

JOURNAL OF VASCULAR SURGERY Volume 20, Number 6 Kent et al. 9 0 7
Table I. Baseline demographics, procedure variables, and laboratory data in the 376 patients treated with coronary artery stents
Retroperitoneal hematoma
No Yes p Value
Baseline demographics No. of procedures 363 13 Age 61 + 12 58 + 12 0.42 Sex (% female) 18 46 0.005 Diabetes (%) 20 8 0.285 Hypertension (%) 53 62 0.554 Unstable angina (%) 70 62 0.779 Multivessel disease (%) 64 46 0.199
Procedure variables Multiple Studies (%) 26 23 0.786 Lysis (%) 7 15 0.221 Sheath removal (% Protocol 3) 75 46 0.022
Laboratory data Peak BUN (mg/dl) 17.6 + 11.04 21.1 + 11.2 0.28 Peak creatinine (mg/dl) 1.4 -+ 0.8 1.7 + 0.85 0.19 Hematocrit drop 7.2 + 4.00 15.8 + 0.85 < 0.001 Nadir platelet count (K/~I) 181.0 + 57.2 126.5 + 40.9 <0.001 Hours o fPTT > 100 sec 4.8 +- 8.3 11.7 +-- 12.5 <0.01
BUN, Blood urea nitrogen.
Table II. Sheath removal protocols in the subgroup of patients who underwent coronary artery stenting
Protocol 1 Continuous intravenous heparin administered until removal of the vascular sheaths the morning after catheterization, hep-
arin resumed 2 hours after achievement of hemostasis (31 procedures) Protocol 2
No additional heparin administered after catheterization, sheaths removed 4 hours later, heparin resumed 2 hours after achievement of hemostasis (68 procedures)
Protocol 3 No additional heparin administered after catheterization, sheaths removed when ACT < 180 seconds, heparin resumed 2
hours after achievement of hemostasis (177 procedures)
ACT, Activated clotting time.
for surgery had been made. The final patient treated with surgery had a gradual fall in hematocrit level over 3 days. In this patient, administration ofheparin was also continued until the day of operation. None of the last three patients had development of hy- potension.
In all patients who required operation, the PTF was elevated to a level greater than 150 seconds during the 24 hours before the operative procedure. Of the patients who did not require operation, only 50% had an elevation of the PTT greater than 150 seconds at any point during the first 3 days after catheterization (p < 0.05).
General anesthetic and a transverse suprainguinal incision were used in all. This allowed proximal control of the external iliac artery before exposing the
arterial laceration. In six of seven patients a second longitudinal femoral incision was necessary either 1~o remove a femoral arterial or venous catheter (n = 2) or to gain more adequate exposure for suturing the arterial laceration (n = 4). The laceration was always located within 2 cm of the inguinal ligament and was found in the external ihac artery in three patients, and in the common femoral artery in four.
The laceration was anterior in five instances and posterior in two instances. Anficoagulation with heparin was continued in four patients after opera- tion at the request of the cardiology service. One patient receiving heparin after operation had contin- ued hemorrhage, eventually requiring a total of 37 units transfusion.
Postoperative complications included death in

JOURNAL OF VASCULAR SURGERY 9 0 8 K e n t et al. December 1994
one patient related to a stroke, myocardial isch- emia/kidney failure in another, and arrhythmia re- quiring pacemaker placement in a third patient. All patients were evaluated by a vascular surgeon on at least one occasion after hospital discharge, and most patients were monitored routinely by the cardiology service. No late complications were observed.
DISCUSSION
Although retroperitoneal hemorrhage after car- diac catheterization is an event that occurs with a relatively low frequency, patients who have develop- ment of this complication often have coexisting myocardial disease, which makes prompt diagnosis and treatment essential. Back, flank, or suprainguinal pain occurred in most patients and was frequently severe enough to require intravenous or intramuscu- lar narcotics. Neuropathies involving the femoral, obturator, and lateral femoral cutaneous nerves were also common. Although these neuropathies were often initially disabling, symptoms eventually re- solved in almost all patients. 12 Pressure on nerves by an enlarging hematoma involving the psoas or iliopsoas muscle appeared to be the cause of neural dysfunction, which developed in 36% ofpatients.12,13
Several patients were symptom free, and either hypotension or a fall in hematocrit level led to suspicion of a retroperitoneal hematoma. However, because hemorrhage was usually adjacent to the inguinal ligament, careful physical examination uni- formly revealed either a suprainguinal mass or diffuse fullness above the inguinal ligament that was always at least mildly tender. CT scanning, although fre- quently ordered, was often unnecessary. 11,14 All patients in this study in whom CT scanning identified a hematoma had physical findings. The size of the hematoma on CT scanning did not influence therapy because decisions regarding the need for transfusion or operation were based on the hemodynamic stability of each patient and changes in hematocrit level. However, CT scanning may be a valuable diagnostic aid in the occasional patient with hypoten- sion or a falling hematocrit level in whom the diagnosis of retroperitoneal hematoma is not readily evident by physical examination.
The true prevalence of retroperitoneal hematoma is likely to be higher than the 0.5% that we have reported. Because this was a retrospective study, we recognize that a number of patients may have had subclinical hemorrhage. In other patients, appropri- ate signs and symptoms may not have been attributed to a retroperitoneal hematoma. Hypotension is not an infrequent event after cardiac catheterization and
may result from dehydration, a vasovagal episode, myocardial ischemia, or hemorrhage at another site (such as the groin). In a patient with hypotension a retroperitoneal hematoma may be missed if the clinician does not search for appropriate physical signs.
Factors that predisposed patients to retroperito- heal hemorrhage, in the subgroup of patients who underwent coronary artery stenting, were a low platelet count, female sex, sheath removal protocol, and prolonged elevation of the PTT. A diminished platelet count was presumably an effect rather than a cause of hemorrhage, because of platelet consump- tion. Women were much more likely to have development of retroperitoneal hematoma than men in the subgroup of patients treated with stents. In the overall cohort of patients with retroperitoneal he- matoma, 60% were women, which is quite dispro- portionate to the 3:1 male/female ratio for all patients undergoing cardiac catheterization at .this institution. The reason for the female predisposition for the development of this complication is unclear.
Excessive anticoagulation was a very strong predictor of retroperitoneal hemorrhage. Although patients receiving coronary artery stents had the highest prevalence of this complication, this associa- tion was probably related to the aggressive antico- agulation regimen to which these patients were subjected. All patients who received coronary artery stents were given anticoagulant continuously with heparin, dextran, aspirin, dipyridamole, and warfarin (Coumadin).
Early recognition of the role of anticoagulation in the development of complications after coronary artery stenting led to two formal changes in our method of sheath removal. The net effect of these two changes was to allow partial reversal of anticoagula- tion before removal of the femoral artery sheath. Each new protocol resulted in statistically fewer retroperitoneal hemorrhages than the prior method. Reversal of anticoagulation which allows adequate thrombosis at the arterial puncture site, appears to be crucial to prevent further hemorrhage from this site. Although anticoagulation is indisputably necessary for patients with unstable angina and after selected interventional procedures, we interpret the data from this analysis to suggest that vigilant and appropriate regulation of anticoagulation could reduce the preva- lence of retroperitoneal hematoma.
Although, the clinical course of patients with retroperitoneal hemorrhage can vary, most patients in this series did not require operation. However, transfusion requirements were high; an average of 4

JOURNAL OF VASCULAR SURGERY Volume 20, Number 6 K e n t et al. 90'9
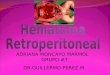
Fig. 1. CT scanning shows extensive retroperitoneal hematoma that developed after placement of coronary artery stent. Laceration in distal external iliac artery was surgically repaired.
units transfusion were necessary for each patient. The retroperitoneal space can sequester a large quantity of blood, which can dissect from a laceration in the common femoral or external iliac artery around the kidney and as far cephalad as the liver or spleen.
Seven patients in this series required operation. The most significant risk factor predicting the need for surgery was excessive anticoagulation. All seven patients requiring operation were found to have a PTT greater than 150 seconds during the 24-hour period before the procedure.
It is possible that operation could have been avoided in the three patients treated surgically for a gradual fall in hematocrit level, particularly if antico- agulation had either been stopped or reversed when the retroperitoneal hemorrhage was first identified. Our experience suggests that tamponade will even- tually occur in virtually all patients if hemorrhage is gradual and blood replacement is adequate. Unfor- tunately, the price for this nonoperative approach is a rather large requirement for transfusion in some patients. With the presumption that transfusion of these patients is of less overall risk than the general anesthetic associated with a retroperitoneal incision, we conclude that operation should be reserved for the small subset of patients with retroperitoneal hemor- rhage, who have development of hypotension that is not responsive to volume resuscitation within the first 4 hours after catheterization.
Surprisingly, the laceration was most frequently (4 of 7) found distal to the inguinal ligament in the
common femoral artery. This accounted for the nced in these patients to expose the common femoral artery with a separate longitudinal femoral incision. Even when the puncture site was found in the external iliac artery, it was always located within 2 cm of the inguinal ligament. These findings raise the possibility that patients, with retroperitoneal hemor- rhage who require surgery, can be initially ap- proached through a femoral incision. Such an ap- proach would ignore the surgical dictum of proximal control. However, hemorrhage from an arterial puncture related to femoral artery catheterization is rarely torrential and is usually easily controlled by digital pressure. Use of a femoral incision, with transection of the inguinal ligament for exposure of the external iliac artery when necessary, will avoid the need for two incisions and may have the added benefit of allowing at least 50% of repairs (those confined to the femoral artery) to be performed with the patient receiving local anesthetic. Since the conclusion of this study, the authors have successfully performed exploration in two patients with retro- peritoneal hematoma through a femoral incision. In one patient, the laceration was found within the common femoral artery and in a second patient the inguinal ligament was transected with the aid of a general anesthetic.
In conclusion, retroperitoneal hematoma is an infrequent complication of cardiac catheterization, which, under most circumstances, can be controlled by volume resuscitation and transfusion. Operation

JOURNAL OF VASCULAR SURGERY 910 Kent et al. December 1994
shou ld be reserved for the small subset o f pat ients w h o have d e v e l o p m e n t o f hypo tens ion unrespons ive to vo lume resusci ta t ion early after catheter izat ion.
REFERENCES 1. Popma JJ, Sailer LF, Pichard AD, et al. Vascular complica-
tions after balloon and new device angioplasty. Circulation 1993;86:1569-78.
2. Muller DW, Shamir KJ, Ellis SG, Topol El. Peripheral vascular complications after conventional and complex percu- taneous coronary interventional procedures. Am J Cardiol 1991 ;69:63-8.
3. Kim D, Orron DE, Skillman JJ, et al. Role of superficial femoral artery puncture in the development of pseudoaneu- rysm and arteriovenous fistula complicating percutaneous transfemoral cardiac catheterization. Cathet Cardiovasc Diagn 1992;25:91-7.
4. Kent KC, McArdle CR, Kennedy B, Balm DS, Anninos E, Skillman JJ. Accuracy of clinical examination in the evaluation of femoral false aneurysms and AV fistulas. J Cardiovasc Surg 1993;1:504-7.
5. Kent KC, McArdle CR, Kennedy B, Bairn DS, Anninos E, Skillman JJ. A prospective study of the clinical outcome of femoral pseudoaneurysms and AV fistulae induced by arterial puncture. J VASC SUWG 1993;17:125-33.
6. McCann RL, Schwartz LB, Pieper KS. Vascular complica- tions of cardiac catheterization. J VASC SURG 1991;13:328- 36.
7. Glaser RL, McKellar D, Scher KS. Atteriovcnous fistulas after cardiac catheterization. Arch Surg 1989;124:1313-5.
8. Sreeram S, Lumsden AB, Miller IS, Salam AA, Dodson TF, Smith RB. Retroperitoncal hcmatoma following femoral arterial catheterization: a serious and often fatal complication. Am Surg 1993;59:94-8.
9. Moscucci M, Mansour KA, Kent KC, Kuntz RE, Senerchia C, Bairn DS, Carrozza JP Jr. Peripheral vascular complications of directional coronary atherectomy and stenting: Predictors, management and outcome. Am J Cardiol 1994;74:448-53.
10. Mills JL, Wiedeman J-E, Robison IG, Hallett JW. Minimizing mortality and morbidity from iattogenic arterial injuries: The need for early recognition and prompt repair. J VASC SUING 1986;4:22-7.
11. Inescas FF, Baker ME, McCann R, Cohan R_H, Silverman PM, Dunnick NR. CT evaluation of retroperitoneal hemor- rhage associated with femoral atteriography. Am J Roent- gcnol 1986;146:1289-92.
12. Kent KC, Moscucci M, Gallagher SG, DiMattia ST, Skillman JJ. Neuropathy after cardiac catheterization: incidence, clini- cal patterns, and long-term outcome. J VASC SURG 1994;19: 1008-14.
13. Cianci P, Piscatelli RL. Femoral neuropathy secondary to retroperitoneal hemorrhage, lAMA 1969;210:1100-1.
14. Abaskaron M, King N. CT demonstration of retroperitoneal hematoma caused by high inguinal arterial puncture during angiography. J Ky Med Assoc 1986;84:354-5.
Submitted June 2, 1994; accepted Aug. 13, 1994.
DISCUSSION
Dr. Richard K. Spence (Camden, N.J.). As our colleagues in cardiology have become increasingly aggres- sive in their use of catheter-directed diagnosis and treat- ment of acute coronary artery events, a new spectrum of vascular surgical problems has arisen. Consider, for ex- ample, pseudoaneurysms of the femoral artery, a previously uncommon lesion associated with prosthetic grafts, but one that we now treat frequently, and usually as an emergency, after cardiac catheterization. Dr. Kent has now added to this problem an important and potentially more lethal one, retroperitoneal hematoma. He and his colleagues have given us an insightful description of the incidence, factors associated with development of the lesion, and approach to treatment of this problem.
A major predictor of retroperitoneal hematoma in your series was the anticoagulation status. I assume this includes those patients who have been treated with lytic agents followed by administration ofheparin. Is this combination a particularly dangerous one? If so, is there any hope of convincing the cardiologists of this? Sheath protocol was a significant predictor of vessel injury. Do you believe this is
associated with catheter size, or is it technique? Our angiographers seem able to place stents and perform angioplasty without causing this problem. What do you think is the difference? I 'm concerned about your recom- mendation that these lesions can be watched with the understanding that most will stop without further bleeding and subsequent tamponade. Is the price we pay in doing this worth it, both in terms of blood transfusions and the potential for disaster? How many of your patients were converted from an urgent to an emergency status by following this wait-and-see approach? Along that line, do your cardiologists consult you as soon as there are problems, or do they usually watch over them a day or 2 and then call you when the horse is clearly out of the barn?
Dr. K. Craig Kent. I think the most important question is the last one. We actually have a very close relationship with our cardiologists. Closer than I 'd want, considering how often they call us to see their patients. But we are very often consulted early and are able to monitor these patients very closely. The approach of wait and see, or wait and watch has worked very well for us. As you can see,

JOURNAL OF VASCULAR SURGERY Volume 20, Number 6 K e n t et al. 9 1 1
84% of our patients were able to be treated without surgery and without any deleterious complications.
Probably this is because we were able to lend our expertise about how to transfuse and when to transfuse. Clearly, in a situation where people who don't have that expertise are treating patients, getting behind in the resuscitation will lead to serious complications. So I think that this nonoperative approach that we are proposing is probably the right approach, but it certainly requires close cooperation between a vascular surgeon, who has an understanding of how to transfuse and resuscitate a patient, and the cardiologist.
In response to some of your other questions, the addition of lyrics to anticoagulation did not statistically increase the risk for development of a retroperitoneal hematoma. But clearly, anticoagulation was the over- whelming major predictor of this problem.
Even though we have a close association with our cardiologist we can't convince them to stop the anticoagu- lation. Most of these patients had placement of coronary artery stents. Our cardiologists believe that the patency of the stents is closely associated with the use of anticoagu- lants. Of course in their minds, and they are probably correct, the patency of the stent is far more important than a catheterization complication. However, if there could be more scrupulous control of anticoagulation I think the incidence of this problem would clearly decrease.
With regard to the sheath removal protocol, antico- agulation is the most important factor, not sheath size. We were able to show this by modifying our protocol and stopping the anticoagulation for an appropriate period of time before the sheath is removed.
In terms of your comment about female predisposition, I wish I knew why women are more likely to have development of retroperitoneal hematoma. But I think your suggestion that their arteries are smaller and that the laceration is larger and more traumatic is probably valid. We have actually found an increased predisposition for other catheterization complications in women in addition to retroperitoneal hematomas.
So in summary, these patients can be treated frequently without operation. These patients need to be monitored very closely and they need to have adequate volume resuscitation to allow this to happen. The retroperitoneal space clearly is a defined space, and it can "fill up." Only in situations where patients abruptly have hypotension after the initial catheterization is surgery really indicated.
Dr. Frank J. Veith (Bronx, N.Y.). We see retroperi- toneal hematomas after interventional radiology proce- dures. We have not been able to make the diagnosis simply on the basis of clinical grounds alone. We have actually had a couple of deaths because of massive retroperitoneal bleeding with no manifestation in the groin whatsoever. So I think this is a very serious problem and one that is not always easily detected and managed.
Second, we have had problems with sheath removal. What is remarkable to me is the size of the sheaths that can be put in arteries and then removed safely. These are huge holes that are made in the arteries. One of the things that we have done in patients who have undergone lyric therapy, and we did not want to stop the heparin because of the precarious nature of the out flow tract, is take the patient to the operating room and, with the patient receiving local anesthetic, make a little anterior exposure of the femoral artery and just put in a U stitch. With this procedure the heparin does not have to be stopped. I think the morbidity rate from this is virtually nonexistent. You don't even have to dissect the entire artery out and get clamp control. Just the anterior surface is exposed. There is a letter to the editor in the JOURNAL OF VASCULAR SURGERY that describes how to do this. I think there are times when it is important to keep up the anticoagulation. There is a way to do this if you work collaboratively with your cardiologists. What is your comment about that?
Dr. Kent. The first question that you posed relates to the diagnosis ofretroperitoneal hematoma. I am convinced that the diagnosis of retroperitoneal hematoma can always be made by use of physical examination by someone with experience. The key is making sure these experienced individuals are in fact evaluating the patient at the appropriate time.
Regarding the thought of removing these catheters by an open technique with the patient receiving local anaes- thetic, I think this is an excellent approach. Very often in a patient who is given anticoagulant, who has jus t finished receiving lytic therapy, or in whom the cardiologists have had some difficulty with the catheterization, we use this approach.
Dr. Thomas F. Panetta (Brooklyn, N.Y.). Have you used duplex ultrasonography? Should we be using this routinely to make the diagnosis if it is difficult? Have you used this in the treatment? I didn't hear you answer with regard to the size of the puncture hole. Your incidence of retroperitoneal hemorrhage for stents was higher than angioplasty, which was likewise higher than diagnostic procedures. This may be related to the puncture hole size: 7F to 9F for a stent placement, 5F for an angioplasty, and 3F for a diagnostic catheter. Could you comment on that! Our interventional radiologists and cardiologists fre- quently do a double-wall puncture. They go through the posterior wall and then pull back to place their catheters. Does this have any effect? Is the posterior hole significant? Should our radiology and cardiology colleagues be doing just anterior wall punctures?
Dr. Kent. Regarding your first question, ultrasonog- raphy in the diagnosis of the retroperitoneal hematoma probably isn't of use. We use duplex scanning all of the time in the diagnosis and the actual treatment of patients who have false aneurysms and arteriovenous fistulas. But with regard to a retroperitoneal hematoma, again we believe that

JOURNAL OF VASCULAR SURGERY 9 1 2 K e n t et al. December 1994
we can make the diagnosis by physical examination. Whether ultrasonography or CT scanning verifies that diagnosis seems to be of little consequence.
With regard to catheter size, it is difficult to sort out exactly whether this relates to the development of retro- peritoneal hematoma. There are many different factors and a lot of different variables: anticoagulation, catheter size, type of procedure, and variety of people performing the procedure. My impression, based on our statistical analysis, is that the most important factor is anticoagulation. But I can't deny that the larger size sheaths used for stents could also contribute to the increased incidence of this compli- cation with that particular procedure.
The naive, first-year vascular surgeon approaches the femoral artery and puts a stitch in the anterior laceration and gets called an hour later to take his patient back to the operating room because of bleeding from a posterior hole not detected at the original operation. You only have to see this once and you never make that mistake again. Very frequently what I do is dissect out the entire artery after repairing the anterior laceration to make sure there isn't the potential of hemorrhage from a posterior hole. I thought when we first started evaluating patients with retroperito- heal hematomas, that a large number of them might be bleeding from a posterior hole, above the inguinal liga- ment. We found this to be the case in one instance. But in most cases the hole was in the common femoral artery. In three cases where it was in the external iliac artery, two were on the anterior side and one was on the posterior side.
Discussant unknown. We had the same kind of problems as you described, and one of the things that we noticed was that there was a correlation between the method of holding the puncture site and the number of complications. It was common practice among most cardi- ologists to put a sandbag at the puncture site or put the so-called C clamp. Both of these techniques are atrocious. Our experience has been that if you make the cardiology fellow hold direct finger pressure exactly where the punc- ture hole is for a certain duration, depending on anticoagu- lation, the incidence was much lowered. So that is what we try to practice. I would like your comment about that.
Dr. Kent. There is little doubt in my mind that, when the sheath is first pulled, you have an opportunity to get control of that laceration. If you lose that control anywhere within the first 20 minutes, then the cow is out of the barn. So that is a very essential time. Manual control over that period of time is far more important than use of the C clamp or sandbag for pressure.
Dr. Enrico Ascer (Brooklyn, N.Y.). Have you looked at hypertension as a variable to induce bleeding after puncture ?
Dr. Kent. In the subset of the 376 patients who had placement of coronary artery stents, we evaluated hyper- tension and found no statistical increase of the incidence of retroperitoneal hematoma in the patients who had hyper- tension. Although I must say that hypertension is an elusive variable to be looking at. How long does the blood pressure
have to be up? How high should it be? We set criteria and didn't find a correlation. But I guess I am not completely convinced that there might not be a correlation.
Dr. John J. Ricotta (Buffalo, N.Y.). We have seen a couple of patients recently who have not had any groin manifestations and presented simply with decreasing he- matocrit level and retroperitoneal bleeding. One of these patients was actually in the cardiology service but had not undergone catheterization yet. They had been treated with high-dose anticoagulation as part of their initial protocol. Spontaneous retroperitoneal hemorrhage can occur. How do you handle a patient where there is not an obvious groin source? If there is no groin hematoma, do you treat that patient differently? What would the role be for angiogra- phy in a patient where it appears that all of the blood is up above the inguinal ligament?
Do you have follow-up on patients who did not undergo operation, in terms of whether they have devel- opment of false aneurysms later? I think when you don't operate on these people, it is awfully hard to figure out whether they are going to have development of an aneurysm because you just have a massive hematoma in the thigh. I wondered how many of these people have gone on to have development of aneurysms? What is the incidence of infection? What steps do you take to prevent infection in a patient who has a couple of units of blood in their retroperitoneum extending down into the groin in which you plan an open procedure?
Dr. Kent. To answer your first question, we had one patient during that 5-year period of time who had development of a spontaneous retroperitoneal hem- orrhage. There is a reason that these patients will have hypotension and not have physical findings. The hematoma is usually very high in the muscular area and not evident just above the inguinal ligament, as is the case with hemorrhage after cardiac catheteri- zation.
With regard to your question on follow-up, I thought that a lot of these patients might have development of pseudoaneurysms. We have very close long-term follow-up on all 45 patients whom we evaluated. They all did very well. So if they do have development of pseudoaneurysms, they all must spontaneously thrombose.
No infections in any of these patients were related to retropetitoneal hematoma.
Dr. Harry L. Bush, Jr. (New York, N.Y.). I just have one further question. I am a little concerned you had a relatively high incidence of nerve symptoms, specifically femoral neuropathy.
Do you feel comfortable in advising merely observation for neuropathy when only about 50% of them showed resolution of symptoms over time. In general if you do explore them and decompress the major portion of the hematoma, wouldn't the symptoms from nerve compres- sion resolve? I f it's because of infikration of blood into the adjacent muscle, obviously some of the symptoms would persist and then resolve. In the 18% that you explored, did

JOURNAL OF VASCULAR SURGERY Volume 20, Number 6 K e n t et al. 913
those people also happen to have nerve symptoms to a large extent or not?
Dr. Kent. We actually reported our experience with peripheral neuropathy of the neurovascular bundle about a year ago and that was the whole gist of the study) 2 What would be the optimal management? Should these people be treated in a nonoperative fashion? Will their symptoms resolve spontaneously or do they need to undergo decom- pression? Our approach through the 5-year period of time
was not to operate on the patients and see what their natural history would be. In patients treated without operation, there was a 50% reduction in symptoms by 2, months and by the end of the 24-month period of time, no patients had motor neuropathy. Six patients had very minor residual sensory neuropathy. We did operate on three patients in that series for other reasons, and the neuropathy did not resolve immediately after operation in any of these patients.
1 - 8 0 0 - 5 5 - M O S B Y
This number links you to the full text of literally every article ever published in Mosby journals. MOSBY Document Express TM, a rapid response information retrieval service, provides quick turnaround, 24-hour availability, and speedy delivery methods. For inquiries and pricing information, call our toll-free, 24-hour order line: 1-800-55-MOSBY; outside the United States: 415-259-5046; fax: 415-259-4019; E-mail: [email protected].
MOSBY Document Express TM is offered in cooperation with Dynamic Information Corp.












![caso-21 [Modo de compatibilidad] - GERIATRIA HCSC · agresivas y NO REALIZAR PAAF. 04/07/2010 06/07/2010. DIAGNOSTICO DIFERENCIAL DE MASA RETROPERITONEAL Hematoma Masa inflamatoria](https://img.dokumen.tips/doc/110x75/5ba3701e09d3f280548b609d/caso-21-modo-de-compatibilidad-geriatria-hcsc-agresivas-y-no-realizar-paaf.jpg)