Embed Size (px)
Citation preview

Retinal laser Doppler velocimetry: toward itscomputer-assisted clinical use
Benno L. Petrig and Charles E. Riva
Clinical use of laser Doppler velocimetry of absolute red blood cell velocity Vmax in the center of major retinalvessels becomes possible with recent advances in microcomputer technology. Speed and automation ofDoppler photocurrent analysis and identification of proper laser beam positioning are the major requirementsin making direct quantitative assessment of retinal hemodynamics a routine diagnostic tool. We discuss ourefforts toward achieving this goal and illustrate our current capabilities with examples of changes in retinalblood flow in response to physiologic maneuvers. In veins, Vmax can now be determined on-line. In arteries,current computing speed only supports intermittent on-line data acquisition.
1. Introduction
The retina is among the few tissues of the humanbody where blood circulation can be observed directlyand noninvasively. This has facilitated a detailed de-scription of the morphological changes of the retinalvasculature caused by many systemic and ocular dis-eases. In spite of the accessibility of the retinal vascu-lature and the obvious importance of blood flow, aquantitative method for routine measurement of reti-nal hemodynamics is not available to the clinician now.Assessments of normal or low flow based on fluoresceinangiography remain qualitative, and the fluoresceindye dilution technique has had limited success.
Laser Doppler velocimetry (LDV), when applied toretinal blood vessels, provides a noninvasive, direct,and absolute measurement of the maximum (centerline) red blood cell velocity Vmax in individual arteriesand veins as small as 40 /,m.lA In this paper wediscuss why LDV, despite its advantages over othermethods, is not yet a clinically available technique.We define requirements for its clinical application,describe some of our recent progress toward this goal,and show several examples of the current capabilitiesof LDV. These include the study of the reactivity ofthe retinal vasculature to breathing 100% oxygen and
The authors are with University of Pennsylvania, OphthalmologyDepartment, Scheie Eye Institute, Philadelphia, Pennsylvania19104.
Received 30 June 1987.0003-6935/88/061126-09$02.00/0.© 1988 Optical Society of America.
the investigation of the effect of acutely and chronical-ly decreased perfusion pressure on retinal blood flow.
II. Methods
A. Basic Principles
A low power laser beam, e.g., He-Ne at = 632.8 nm,is introduced through the dilated pupil into the eyeand focused on a retinal vessel. Measurement sites aretypically chosen within one to two disk diameters fromthe center of the optic disk. Laser light is scatteredback out of the pupil both by moving red blood cellsand by stationary structures (e.g., vessel wall). Someof this scattered light is collected along two directionsand guided to separate light detectors. Each detectorproduces a photocurrent signal, which is amplified,filtered, and either recorded on tape or fed into acomputer.
In accordance with the Doppler effect, laser lightscattered by red blood cells is shifted in frequency withrespect to that of stationary objects by an amountproportional to their relative velocity. These frequen-cy shifts can be measured by optical autodyne detec-tion,5 a special form of heterodyne detection applica-ble in our case.6 Because at any given time there aremany red cells moving at different velocities, the scat-tered light contains a spectrum of shifts. When mixedon the photodetector surface with light scattered bythe vessel wall, the photocurrent yields a spectrum ofbeat frequencies, which is directly related to the veloci-ty spectrum of the red blood cells.
For one scattering direction we can, therefore, calcu-late the power spectrum of the photocurrent signal anddetermine the maximum Doppler shift fmax, also calledcutoff frequency. Vmax is proportional to fmax, but theproportionality constant is unknown because it de-
1126 APPLIED OPTICS / Vol. 27, No. 6 / 15 March 1988

pends on the scattering geometry internal to the eye.Thus unidirectional LDV can only produce a relativemeasure of Vmax provided the scattering geometry re-mains unchanged. Using the bidirectional approach,the corresponding center line red cell velocity can becalculated in absolute terms as follows:
Vmax = klfmax,1 - fmax,21. (1)
Here k is a known constant for a given eye, andfmax,ifmax,2 are the cutoffs for the two directions mea-sured simultaneously. The factor k depends only onthe wavelength of the laser, the axial length of the eye,the index of refraction of the flowing medium, and thegeometry of the optical pathways in the detection sys-tem of the fundus camera, which is readily deter-mined. 1,3
B. Cutoff Analysis by Visual Inspection
Until recently cutoffs were determined by visualinspection of power spectra obtained with a hardwarespectrum analyzer and displayed on an oscilloscope,one spectrum at a time. Each estimate of Vmax (meanand standard deviation) was based on 10-20 pairs ofcutoffs.
Thus analysis of cutoffs by visual inspection is a verytime-consuming procedure already in the case of reti-nal veins where flow is usually nonpulsatile, and onevalue of Vmax is sufficient to determine venous bloodflow. In retinal arteries, however, several Vmax esti-mates at different phases of the heart cycle are neededto obtain the average arterial blood flow velocity. Toeliminate bias, the examiner was masked with respectto the kind of patient studied and the experimentalprotocol used, adding further time to the analysis pro-cedure. Clearly, the visual inspection method is notsuitable for routine clinical application.
C. Requirements for Clinical Use of LDV
Speed and automation of measurements are twoimportant factors in the routine clinical use of anydiagnostic method. A brief LDV procedure avoidspatient fatigue and maximizes the number of vesselsthat can be measured in a given time period. Auto-mated data collection and analysis procedures reducethe number of operators needed and ensure standard-ization of the technique across different clinics.
We estimated how the total measurement time isspent to perform the various tasks involved in LDVmeasurements based on visual inspection. Assumingthat the patient's pupil is already dilated, the initialstep including the alignment of the laser delivery andlight detection system can be done in a few minutes.Occasionally the apparatus needs to be realigned, andthe patient's fixation target has to be readjusted dur-ing the session.
Actual data collection (photocurrent sampling) timethereafter is only a fraction of a second for a single pairof power spectra. This means that the natural bloodflow pulsatility in arteries during the cardiac cyclecould be followed accurately. Furthermore, a photo-current signal of only 1.6-s duration is needed when
measuring Vmax in a vein based on, for example, twentypairs of spectra and frequency domain averaging withN = 4 (corresponding to a total of eighty raw spectrapairs). Analyzing these data takes -10-20 min.Clearly, much more time is spent finding those por-tions of the tape where the laser beam was well cen-tered on the vessel and analyzing the cutoffs than forthe acquisition of the underlying Doppler signals.
Therefore, the signals cannot be analyzed by thevisual inspection method as they are acquired, and asecond operator frequently checks the power spectraof the signal and decides when enough signal has beenrecorded to reliably determine Vmax later. This deci-sion is usually made very conservatively, and, there-fore, data collection can extend over a considerablylonger time period than needed to obtain a sufficientamount of data.
Thus one of the foremost goals is to reduce the timeneeded for cutoff analysis. Because of the complexityof the task, computer analysis of cutoffs is the pre-ferred way of automating and accelerating the mea-surement of Vmax in retinal vessels. As an added bene-fit, automation eliminates the variability of resultsobtained by the same observer due to short- and long-term shifts of the criteria applied in the analysis. Italso allows comparison of results obtained in differentlaboratories.
Most patients cannot maintain adequate fixation tokeep the laser beam on the vessel for more than a fewseconds. When the laser beam is off the vessel, theassumptions underlying retinal vessel LDV are nolonger applicable. Another requirement is, therefore,to identify those time periods when the laser beam isproperly focused and centered on the vessel.
The power spectra originating from a laser beamwell centered on the vessel and one located to the sideor completely off the vessel are distinctly different.The former case is characterized by a flat spectrumwith a sharp drop in both the mean and variance of thespectral density as the Doppler shift frequency in-creases. In the latter case, most of the power is con-centrated at very low frequencies, and the falloff inspectral density is gradual, lacking a well-defined cut-off point. One way to differentiate between the twocases is, therefore, based on the shape of the DSPS, i.e.,how well the model is able to account for the data. Aparameter to this effect is defined below.
D. Computer Analysis of Doppler Shift Power Spectra
To automate the analysis of the cutoff frequency ofDoppler shift power spectra (DSPS), a computer algo-rithm was developed 7 based on a theoretical modeldescribed in detail elsewhere.2 The algorithm pro-vides the best fit of this model to a given DSPS usingthe least-squares criterion. Briefly, this simple model,which is based on single light scattering of laser light byred blood cells,8 assumes a flat spectrum from dc tosome cutoff frequency and includes a constant powerdensity contribution originating from the inherentshot noise of the light detection system. In the experi-mental condition of short measuring time, this model
15 March 1988 / Vol. 27, No. 6 / APPLIED OPTICS 1127

Chl - Data l Random Array
Ch2 - A/D Acquisition Access ProcessorPulse * / Processor Memory
FFT
l SpectrumI ~~~~~Anacys~s
0/A Fr eque ncyAnaysis
Graphics IDisplay
Processor
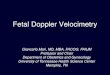
Fig. 1. Block diagram of MCS-561 computer system. The mainCPU (Motorola 68010) controls three slave processors (dashedlines). The data acquisition processor handles A-D conversion ofphotocurrent and pulse signals. It also makes the time course ofselected parameters available through D-A converters for hard copyrecording. The data path is indicated by wide arrows. The arrayprocessor takes the signal from main memory buffers, calculatesFFT, power spectrum, and cutoff frequency for each channel, andreturns results to main memory. The display processor plots power
spectra and time course of results on-line on a graphics monitor.
seems to be justified on the basis of previous resultsobtained in vitro and in vivo2 and the typical spectrashown in Figs. 2 and 3.
Originally developed on a PDP-11/34, the timespent just for a two-channel cutoff analysis alone was45 s. A recent adaptation of the algorithm to an arrayprocessor coupled with a Masscomp MCS-561 micro-supercomputer brought about a massive speed im-
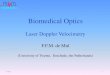
Fig. 2. Partial view of the graphics monitor during measure-ments in a human retinal vein. The upper two panels show theinstantaneous unaveraged power spectrum in each channel. The xaxes are scaled according to the selected photocurrent signal band-width. In this case, horizontal divisions represent 2.5 kHz. The yaxes are adjusted to show the maximum power spectral density ofeach channel at full scale. The vertical and horizontal lines drawnon top of the spectra show the automatically determined cutofffrequency and the linear fit of the data below the cutoff, respectively.The lower panel shows a wraparound trace of the 512 most recentvalues of the average center line red cell velocity ( Vmax) as a functionof time. (Vmax) is calculated as the running average of the eightmost recent values of Vmax derived from single pairs of power spec-tra. The x-axis scale depends on the frequency of Vmax analysis
(6.4 s, full scale); the y axis is calibrated in cm/s/div.
provement. This system needs only 80 ms to digitizethe signals, calculate the fast Fourier transforms(FFT) and power spectra, in addition to the cutoffanalysis.
As indicated by the dashed lines in the block dia-gram in Fig. 1, the main processor (CPU, Motorola
Fig. 3. Partial view of the graphics monitor during measurements in a human retinal artery as seen at the systolic (A) and diastolic (B) phaseof the cardiac cycle. Similar to Fig. 2, panels show instantaneous power spectra (5kHz/horizontal division) and (Vmax). An additional panelon the bottom shows a trace of the pulse wave. The signal saturated while it was recorded but still indicates the systolic and diastolic phases.
Blinks or inappropriate fixation cause a disturbance of Vmax during the latter portion of (B).
1128 APPLIED OPTICS / Vol. 27, No. 6 / 15 March 1988

Table 1. Theoretical Constraints on Maximum Rate of Cutoff Analysis
NbSignal 1 2 4 8
bandwidth fsmpla Tacqc 7anaT Tacq fana Tacq fana Tacq fana(kHz) (kHz) (ms) (Hz) (Ms) (Hz) (ms) (Hz) (ms) (Hz)
100 204.8 5 200 10 100 20 50 40 2550 102.4 10 100 20 50 40 25 80 12.525 51.2 20 50 40 25 80 12.5 160 6.2512.5 25.6 40 25 80 12.5 160 6.25 320 3.136.25 12.8 80 12.5 160 6.25 320 3.13 640 1.56
a fsmnpl, sampling frequency per channel.b N, number of spectra averaged in the frequency domain.
Tacq, duration of data acquisition.d fana, maximum possible rate of cutoff analysis.
68010) controls three slave processors. The first, thedata acquisition processor, samples and digitizes thetwo photocurrent signals and deposits the 12-bit bina-ry data, 1024 samples/channel, directly into randomaccess memory buffers. The heart pulse signal is ac-quired through a third channel. The data paththrough the system is illustrated by wide arrows. Thisprocess can handle signals at a maximum bandwidth of100 kHz/channel. The second, a tightly coupled arrayprocessor, continuously transfers the acquired databuffers from main memory to its local memory wherethe FFTs and the power spectra are calculated, and thecutoff frequencies are determined. In addition, a pa-rameter related to the goodness of fit between themodel and the data is computed for each spectrum.All results are returned into main memory. The third,the graphics display processor, performs all the graph-ics display functions needed during LDV recordings.As shown in Fig. 2 for a retinal vein and Fig. 3 for anartery, the instantaneous power spectrum of eachchannel can be monitored continuously, and the timecourse of Vmax and the heart pulse can be observed overa time period covering the most recent 512 data points.The entire time course of the above parameters and thegoodness of fit parameter are also available at the D-Aconverter output for recording on a hard copy devicesuch as a strip chart recorder.
The theoretical constraints on the sampling fre-quency of Vmax imposed by the bandwidth of the pho-tocurrent signal are summarized in Table I. Also in-cluded in the data are the effects of frequency domainaveraging of N Doppler shift power spectra before thecutoff analysis. This procedure provides a smoothpower spectrum estimate at the expense of loweringthe maximum rate at which arterial Vmax can be mea-sured. Table II shows the computational constraintsof the MCS-561 computer system which can sustain amaximum continuous rate of Vmax measurements of12.5 Hz without averaging and at least 6.5 Hz whenaveraging up to eight power spectra before determin-ing the cutoffs. This means that 35% of the possiblecombinations of bandwidth and extent of averaginglisted in Table I are available in real time. Specifical-ly, when measuring retinal veins with N = 8, the systemis able to determine Vmax on-line, provided the photo-current signal bandwidth does not exceed 25 kHz. Us-
Table 11. Computational Constraints on Maximum Rate of Cutoff Analysis
FanabNa (Hz)
1 12.52 10.54 8.58 6.5
a N, number of spectra averaged in frequency domain.b Fana, rate of cutoff analysis the computer can sustain.
ing a fundus camera based velocimeter, fmax rarely goesbeyond 20 kHz in either channel. Since venous bloodflow is considered constant throughout the heart cycle,choosing N = 8 is advantageous because it results invery smooth DSPS and considerable noise reductionboth below and above fmax and still requires only 160ms of signal acquisition time. Thus, just a few secondsof steady fixation per vessel are enough to obtain areproducible estimate of venous Vmax, as indicated bythe flat trace on the graphics screen (Fig. 2, bottom)during data collection.
In cases where photocurrent signals are recorded ontape and can be played back 2, 4, or 8 times slower foranalysis, our MCS-561 machine can be boosted to aneffective performance covering 90% of all combina-tions listed in Table I. Since much of the Vmax datashown in this paper are from arteries, the traces wereobtained in this manner to increase the details of thewaveforms.
E. Assessment of Doppler Signal Quality
To help identify those times during which the laserwas appropriately centered on the vessel and duringwhich the application of the model is justified, a pa-rameter qj based on the shape of the power spectrumfor the jth scattering direction has been defined asfollows (for the derivation of this formula see Appen-dix):
1 I i= 1,2, (2)1 + (M 1 - 1) * SI + (M2 - 1) S2
M, . d + M2 d 21~~~~ 2
where Ml and M 2 are the number of data points belowand above the previously determined cutoff frequency;sl and s2 are the standard deviations of the power
15 March 1988 / Vol. 27, No. 6 / APPLIED OPTICS 1129
qj =

density, and d, and d2 are the differences between thefitted model power density and the average powerdensity over the entire spectrum. Indices 1 and 2denote the frequency region below and above the cut-off, respectively. It should be noted that the parame-ter q does not vary with changes in the gain of thephotocurrent since it is normalized by the averagespectral power density. In its currently presentedform, however, there is a dependence on the cutofffrequency because the variance in the two regions canbe markedly different (see Fig. 7), and their weightdepends on the position of the cutoff. This parameterwill approach unity as the data points move closer tothe model value and zero as they move away from themodel. Since both scattering directions must providesharp cutoffs, the product
q = q 2 (3)
is used as an, indicator of the goodness of the model fitin some of the data shown later. We are currentlystudying variations of this parameter to eliminate thedependency on the cutoff frequency.
Another approach which is useful in measuring arte-rial Vmax stems from the pulsatility of blood flow.Since one can expect most patients to fixate for aduration of three or four heartbeats one can applyautocorrelation techniques to pick out those sectionsof Vmax which show a repeatable flow profile or cross-correlation between Vmax and the pulse wave to findwhether the flow profile is in phase with the pulseprofile. These techniques are currently under investi-gation.
F. Intermittent Data Acquisition
The ability to sustain real-time data analysis for anindefinite length of time may not be essential for clini-cal applicability. Quite frequently there are pausesduring the data collection session because the patienthas to blink or needs to rest or the camera has to bereadjusted. During these times data acquisition ismeaningless and could be stopped while data analysiscontinues until all data are analyzed.
Again consulting Tables I and II, we can see thatdata analysis is at worst 16 times but usually only 8, 4,or 2 times slower than data acquisition. Depending onbandwidth, this means that a pause of 15, 7, 3, or 1 s isrequired for every second of acquired signal. Thus, incontrast to continuous data acquisition and analysis,the intermittent approach permits all combinations ofbandwidth and averaging of Table I with a reasonableanalysis delay.
The total time span that can be covered in this waydoes not depend on computational speed but only onthe amount of memory available to store the databuffers until they can be analyzed. Table III showsthe amount of memory required to store 5 s of signal onall three channels at different bandwidths. This timeperiod seems to be required when measuring fromretinal arteries because it covers several heart cycles.A consistent and repeatable waveform during thistime, found either by visual inspection or automatical-
Table Ill. Data Storage Requirements for 5 s of Signal (All Channels)
Bandwidth Memory(kHz) (kB)
100 600050 300025 150012.5 7506.25 375
ly by autocorrelation of Vmax or cross-correlation ofVmaX with the pulse wave, will help decide whether thelaser beam was well centered.
Thus, when using the MCS-561-based LDV signalacquisition and analysis system in retinal veins, wherethe highest required bandwidth is 25 kHz, we can nowperform on-line Vmax measurements. In retinal arter-ies, intermittent data acquisition and pausing for addi-tional data analysis time are required but in our viewacceptable in a clinical situation, providing quasi on-line performance for short periods of time. New gen-erations of computers may offer more speed and even-tually be able to do continuous LDV analysis at allbandwidths. If the signals were recorded on tape andplayed back slower, all LDV signals could be analyzed,but this approach is not satisfactory in a clinical settingsince it is slow and would again require a second opera-tor to assist in the data collection phase.
Ill. Applications
Several examples of using the MCS-561 based LDVanalysis system follow. In each case the data are froma different subject. All data on venous Vmax wereobtained in real time. To increase the details of thearterial Vmax waveforms we chose to play photocurrentsignals back from tape 8 times slower than the record-ing speed and without frequency domain averaging.Furthermore, each data point shown for Vmax repre-sents the running average of the eight most recentlydetermined values. The other parameters shown as afunction of time are not subject to a running average.
A. Oxygen Reactivity in the Miniature Pig
In this example a photocurrent signal was recordedonly in one direction from an anesthetized miniaturepig where the laser beam could be centered on a vesselfor the duration of the experiment. In such casesunidirectional LDV measurements are sufficient toshow relative changes over time. Figure 4 shows thetime course of relative arterial Vmax as the animal wentfrom breathing air to breathing 100% 02. Trace (A)shows the pulsatility of Vmax, whereas trace (B) shows alow-pass (0.1-Hz) filtered version of trace (A). Thusthe time course of systolic, diastolic, and mean velocitycan be determined accurately. A new equilibrium isreached after -2-3 min of pure oxygen breathing witha decrease in the above quantities of 60, 72, and 62%,respectively. Small portions of the signal during airand oxygen breathing in Fig. 4 are depicted in Fig. 5 onan expanded time scale illustrating the details of thewaveform.
1130 APPLIED OPTICS / Vol. 27, No. 6 / 15 March 1988

I I I I**I 1 1 1 1 i i ._ 1.:l 1 '-
4- -t~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~4
... ,,,. .I7 _ ::tT .. ,. _ .... _ _ . _ _ _ _ _ _ _ _ _ _ _ , ... .,. T .'... I'. .... . .U X s ,i~g, = _= , _ _ = == _= = ===- ==- --''1' 1''1:'1'''1'''1'''1'''I1'J.
-. , T.,,,, I, A..M _ ., _ _ - = = =_ = === =-== _ .- = '1'''1''1:':1':1' '''1' I''Al. a. i. Wr.......Cg___i. ======-- ::
0 1 2 3 4Minutes of 100% 02 breathing
Fig. 4. Effect of oxygen breathing on retinal blood flow in the miniature pig. Relative red cell velocity (given by the cutoff frequency fmaxmeasured with a unidirectional system) is shown in an anesthetized animal going from air to 100% oxygen breathing. The diastolic andsystolic limits (A) and the time average (B) of fnax are presented. After -2 min of inhaling pure oxygen a new equilibrium is reached between
60 and 72% below the base line value.
A Air40 F PI 9IM- OU I t I.,!! jjEi
1 MIl I' I 'l.0: 1
L L i0
B 100% 0240 ri~~4tl~i~}!-il'Ii
I T l0.,I ill
"1I
ii
A Air
Fig. 5. Portions of Vmax redrawn from Fig. 4 on an expanded timescale to illustrate the waveform at base line (A) and at 5 min of 02breathing (B). These data demonstrate the regularity of Vmax mea-surements in the well-stabilized conditions of an animal experiment
as opposed to those in a human subject shown in Fig. 6.
B. Oxygen Reactivity in the Human
Figure 6 shows arterial Vmax measurements over afew heart cycles in a normal human volunteer (A)during air breathing and (B) at 5 min of inhaling 100%02. Diastolic and systolic Vmax decrease from -1.9and 4.5 cm/s at base line to -1 and 3 cm/s, respectively,during oxygen breathing. In keeping with earlier de-tailed studies of 02 reactivity, 9 this subject shows asimilar decrease in red blood cell velocity of -40%.
There is some variation in the shape of the Vmaxwaveform between different pulses. This is mostlydue to small variations in the fixation and to noise in
10
E
IE
0-B
E I
E a
0 -l
F.
100% 02q-' 4-iTl
isFig. 6. Effect of oxygen breathing on blood flow in the normalhuman retina. Arterial Vmax is shown during air breathing (A) andat 5 min of 100% 02 breathing. A decrease of -40% can be noted.
the determination of the cutoffs, indicating the neces-sity to average several pulses to obtain an estimate ofmean arterial blood velocity or the true Vmax wave-form.
C. Acute Changes in Perfusion Pressure in Humans
In a different subject the effect of increased intra-ocular pressure (IOP) induced by applying pressure onthe temporal sclera using a suction cup device is illus-trated in Figs. 7 and 8. Figure 7 shows fmax (relativeVmax) using a unidirectional infrared LDV system.10
Both traces are drawn on the same vertical scale tosimplify comparison. Traces (A) and (B) show fmax at
15 March 1988 / Vol. 27, No.6 / APPLIED OPTICS 1131
A20-
NIS
E I
0
B20-
N
I
E
0
Air5 6
d1L1L :1U_1ETFr,
llilll:g-ili: l' ill' iEll.lq
gWqW I4Sl!: 1 ll!:tizELL|,!t-jj,,. ......
1 <1 l!1:! t!!!l1 Ills
,!!f1U 'Ii
I
11 l.I
LN

blinkA
B
20 -_Z _2O:I _
I-I
L_
20Y fE7 _-.
1 2I _-
II0
i I I I i i i i i
isII. l.. I11 I.. II I I
isFig. 7. Effect of acute elevation of intraocular pressure on bloodflow in the normal human retinal artery. Relative red cell velocityfmax is plotted at rest (A) and at an intraocular pressure elevated todiastolic retinal artery pressure (B) by means of a scleral suction cup.The cutoff frequency at diastole is reduced to about zero, while thesame at systole is increased over its base line value, suggesting thatthe retinal vasculature is counteracting the change in perfusionpressure. Nevertheless, time-averaged velocity is decreased. Note
that the effect of blinks lasts only for a short time.
A 5
E
E
0 :I:A. I I
10S
0 U
d i dastolic 1 i -Tr iu !'''-:ih -:|'i:-4 - 1- --
Fig. 8. Effect of acute elevation of intraocular pressure on bloodflow in a normal human retinal vein. On-line absolute Vmax mea-surements are shown before and after an acute increase induced bysuction cup (A) and before and after releasing the suction (B). Vmaydecreases from '-1.5 to 0.5 cm/s after pressure elevation to 38 mm Hg(A). Raising the pressure to diastolic (B) causes Vma to approachzero. After the cup is released Vmax, quickly increases to 2.5 cm/s and
returns to base line after -'1 min.
rest and at an intraocular pressure equal to the centralretinal artery diastolic blood pressure, respectively.We see that relative Vmax is practically zero at diastolewhile being increased above its resting value duringsystole. Since the vessel diameter at the site of LDVmeasurements did not change significantly in theseconditions (compensatory vasodilatation must haveoccurred distally to the measured vessels),"1 this clear-ly demonstrates the presence of an autoregulatorymechanism, which counteracts the acute change inperfusion pressure. It appears, however, that the defi-cit in diastolic flow cannot be completely recoveredduring the systolic phase which supports our earlierfinding that blood flow is reduced before the intraocu-lar pressure reaches the diastolic pressure level.1112
Occasional blinks cannot be avoided, but they contam-inate the trace only for a brief moment.
The effect of acute elevation of IOP on a small reti-nal vein (60 ,gm in diameter) draining the macularregion is demonstrated in the same subject (Fig. 8) for aconsiderably longer time period, covering -1 min be-fore and after placing the suction cup and removing itagain. The Vmax data were obtained in real time at abandwidth of 25 kHz with frequency domain averagingof N = 8 and a running average on the Vmax trace usinga window size of W = 10.
The base line [Fig. 8(A)] shows some fluctuationaround a value of -1.5 cm/s mostly due to fixationaldrifts and blinks. When the cup is placed on the sclera(cup on) and the IOP is raised to -38 mm Hg, Vmaxdrops to around 0.5 cm/s. As the IOP is further raised[Fig. 8(B)] and reaches diastolic pressure (diastolic),Vmax is practically down at zero. After the cup isreleased (cup off), Vmax jumps to 2.5 cm/s to returngradually to the base line value within -1 min.
D. Chronic Alterations in Perfusion Pressure
As the last example, measurements in a patient suf-fering from severe bilateral carotid occlusion are de-picted in Fig. 9. The top and middle traces show Vmaxin a major retinal artery and the finger pulse wave,respectively, as a function of time. Even though thesedata were obtained in resting conditions we noted arather high pulse rate of 107 beats/min and high pulsa-tility with almost zero blood flow velocity at diastoleand elevated velocity at systole. There is a strikingsimilarity between this chronic hemodynamic statusand the acutely induced one shown before, indicatingthat a considerable portion of the autoregulatory ca-pacity of this patient may already be utilized at rest.Thus blood flow in this patient may already be reducedor its regulatory mechanisms may no longer be able tomeet additional demand during further hemodynamicstress situations.
The bottom trace shows the goodness-of-fit parame-ter q as defined in Eqs. (2) and (3) combining bothdirections of light scattering. A higher value indicatesbetter agreement between data and model indicatingbetter positioning of the laser beam. As mentionedabove there is a dependence of this factor on the cutofffrequency because the higher variance of the powerspectral density below the cutoff is weighted more atsystole (M1 large) than at diastole (M1 small). Thuswhen applied to arteries the parameter q fluctuatesinversely with Vmax.
In the left half of Fig. 9 both Vmjx and q are fairlyregular, whereas on the right, beginning at the arrow, qremains at a low level over several cycles indicatingthat the laser beam is no longer placed properly. Eventhough the computer continues to calculate cutoffsand determine Vmax, q remains at a low level throughseveral heart cycles and may help in deciding whatparts of the signal should be taken as originating froman artery. It appears, however, that q is not very goodat distinguishing spectra taken during systole fromspectra recorded off the vessel. Additional work isneeded in this regard to remove the dependency of q onthe cutoff and improve its performance during systole.
1132 APPLIED OPTICS / Vol. 27, No. 6 / 15 March 1988

~~~~~~~~~~~. . ... ::..:. .il ....* :"'l''-h B ' --
g~~~~~~~~A -: r <t: , r ll
X a.,F T_ T.. n17-..v Eku
:X.1::0 :1::!-::!: : .1: 1y' l q :: K :
1 k 1 -R .A 1 k AA: 10 '0 k0 0 A0
1..:.' 1'--1 1'1 1 1 1- 1 :1 1 : 1 11 1
1'1:.1~~ ~~~~ 1 :-1i:10 11 1 ..1: I1 .-1'1.--. ... .. 1 .. .. .. .. .. .. .. ..I
. w ilM..:tw: M..:l-w.. l a~. ... ... ... a l
is Time
I Al 1- A .1I 1 1 1 1 -1' :1 A I I: 1 -
1 1.1.H71 1 1 1 11 1 1 1 1.;.1 1 1:.,1''' 1 . L
0 |" | '|_ ; .| | ,| .. !l l
'1 -1 ' - _ ..I - .1 1 :' 1 1 1 ':k ; I. l: : lI v l l l. I I - -. | t -
f ;14 1 , -1i 1 1 1 0 :.1 1.11' 1 2:' ::.'':1-Sb_ l _ _
t
Fig. 9. Effect of chronic decrease in perfusion pressure on retinal blood flow. Arterial Vm.. (top trace), pulse pressure (middle), and the
goodness of fit parameter q (bottom) are shown for a patient with carotid occlusion. The horizontal divisions of the chart paper do not align inall traces because these were combined from two sequential strips of a two-channel chart recorder, but all signals are aligned in time. On the
left, Vmax follows a regular waveform over several cardiac cycles. Parameter q (see text) rises periodically during diastole. On the right, when
fixation is no longer maintained as indicated by the arrow, the q value remains low over several pulses providing an objective means to
determine those time periods when signal is recorded from a well-centered laser beam.
IV. Conclusion
We have shown that today's computer technologyapproaches the capability to automate and perform atreal-time speed most of the tasks that have until nowprevented the routine clinical application of laserDoppler velocimetry in retinal vessels. In addition, wedescribed methods dealing with the fact that the typi-cal patient cannot be expected to fixate adequately formore than a few seconds at a time. More work is stillneeded on this last issue to find the optimal approachto address this important factor in the clinical environ-ment.
Several examples showed the application of the en-hanced capabilities of the MCS-561 microcomputer inthe analysis of LDV photocurrent signals obtainedfrom retinal arteries and veins. Specifically, detailedanalysis of the blood velocity waveform now becomespossible and could permit the investigation of the dis-tensibility and the vasomotor state of the retinal vas-culature. These advances may help in making LDVwidely available in the clinical assessment of the hemo-dynamic status of patients in the monitoring of treat-ment efficacy and in the evaluation of pharmacologicagents.
The authors thank Juan Grunwald who obtained theLDV photocurrent signals in the patient presented in
the last example and Joan Baine for her skilled techni-cal assistance.
This work was supported by the Whitaker Founda-tion, Camp Hill, PA 17011 by NIH grant EY-03242from the National Eye Institute, by the Gretel andEugene Ormandy Teaching and Research Fund, andby the Vivian Simkins Lasko Retinal Vascular Re-search Fund.
Appendix
The parameter qj for the scattering direction j isderived from the variable gj defined below, which is ameasure of how well the model used in our cutoffanalysis can account for the power spectral densitydata. The quantitygj represents the variance betweenthe data and the fitted model (X2 del) normalized bythe variance of the data alone (Xnorm) so that qj be-comes a dimensionless quantity independent of signalgain. Thus we define
X2model
bj 2Xnorm
(Al)
Since 0 ( XmodeW < Xorm, it can be seen thatgj will varybetween 0 (indicating that the model fits the dataexactly) and 1. (The model does not account for thedata at all.) Let
15 March 1988 / Vol. 27, No. 6 / APPLIED OPTICS 1133
10
E
1EI
U,)
1I
0

xij, < i < N (A2)
be the spectral density data and
{ A},B M 0<N. (A3)
denote the model, where M represents the cutoff,M-1
M E i0
is the sum of Doppler shift power density and shotnoise below M, and
N-1B= N M E XiN1 M I x
M
is the shot noise power above M.Using Eqs. (A2) and (A3) in Eq. (Al) yields
M-1 N-1
i (Xi-A)2 + E (Xi-B)2
0 M
N-iE (xi- C)2
0
whereN-1
C =NEXi.0
Substituting d, = A - C and d2 = C - B, and with
M-1 N-1
(Xi -A and s NM (xi-B),0 M
the latter being the spectral variance below and abovethe cutoff, respectively, Eq. (A4) can be rewritten as
(M - 1)s2+ (N-M-1)s2
g (M - 1)I + Md2 + (N - M-1)s2 + (N-M)d2
Note that g reaches a maximum of 1 when di = 0, d2 =0, and s, 5# 0 or s2 0 0 and a minimum of 0 when si = 0,S2 = 0, d, # 0, and d2 # 0. Leading to the equationgiven in the text we define
qj = 1 -g
so that qj is 1 when the model fits theand 0 when the fit is inappropriate.
data perfectly
References1. C. E. Riva, G. T. Feke, B. Eberli, and V. Benary, "Bidirectional
LDV System for Absolute Measurement of Blood Speed inRetinal Vessels," Appl. Opt. 18, 2301 (1979).
2. C. E. Riva and G. T. Feke, "Laser Doppler Velocimetry inthe Measurement of Retinal Blood Flow," in The BiomedicalLaser: Technology and Clinical Application, L. Goldmann,Ed. (Springer-Verlag, New York, 1981), pp. 135-161.
3. C. E. Riva, J. E. Grunwald, S. H. Sinclair, and K. O'Keefe,"Fundus Camera Based Retinal LDV," Appl. Opt. 20, 117(1981).
4. C. E. Riva, J. E. Grunwald, S. H. Sinclair, and B. L. Petrig,"Blood Flow Velocity and Volumetric Flow Rate in HumanRetinal Vessels," Invest. Ophthalmol. Vis. Sci. 26, 1124(1985).
5. D. U. Fluckiger, R. J. Keyes, and J. H. Shapiro, "Optical Auto-dyne Detection: Theory and Experiment," Appl. Opt. 26, 318(1987).
6. We now use the term autodyne detection rather than heterodynedetection to describe our technique. In heterodyne detection,light scattered by moving targets is mixed with a local oscillatormost often derived directly from the same laser source. Thedisadvantage is that the matching of polarization and spatialmode character between these two laser beams is very critical,especially when dealing with a signal beam coming from a hu-man eye. Autodyne detection does not depend on a local oscilla-tor. Rather itis a direct detection scheme involving self-beatingbetween the various frequency components of the received sig-nal beam. In this application a relatively large portion of thesignal beam originates from light scattered by the vessel wall andsurrounding quasi-stationary tissue and is mixed with the signallight scattered by the red cells.
7. B. L. Petrig, C. E. Riva, and J. E. Grunwald, "Computer Analysisof Laser Doppler Measurements in Retinal Blood Vessels," In-vest. Ophthalmol. Vis. Sci. 25 (Suppl.), 7 (1984).
8. C. E. Riva, J. E. Grunwald, and B. L. Petrig, "Laser DopplerMeasurement of Retinal Blood Velocity: Validity of the SingleScattering Model," Appl. Opt. 24, 605 (1985).
9. C. E. Riva, J. E. Grunwald, and S. H. Sinclair, "Laser DopplerVelocimetry Study of the Effect of Pure Oxygen Breathing onRetinal Blood Flow," Invest. Ophthalmol. Vis. Sci. 24,47 (1983).
10. C. E. Riva, B. L. Petrig, and J. E. Grunwald, "Near InfraredRetinal Laser Doppler Velocimetry," Lasers Ophthalmol. 1,211(1987).
11. C. E. Riva, J. E. Grunwald, and B. L. Petrig, "Autoregulation ofHuman Retinal Blood Flow: an Investigation with Laser Dopp-ler Velocimetry," Invest. Ophthalmol. Vis. Sci. 27, 1706(1986).
12. B. Petrig, E. B. Werner, C. E. Riva, and J. E. Grunwald, "Re-sponse of Macular Capillary Blood Flow to Changes in Intraocu-lar Pressure as Measured by the Blue Field Simulation Tech-nique," in Proceedings, Sixth International Visual Field Sym-posium, A. Heijl and E. L. Greve, Eds. (Dr. W. Junk Publishers,Dordrecht, The Netherlands, 1985), pp. 447-451.
0
1134 APPLIED OPTICS / Vol. 27, No. 6 / 15 March 1988
g =