Embed Size (px)
Citation preview

Results of the 2012 Survey of theAmerican Association of Academic
Chief Residents in Radiology
Steven Sauk, MD, MS, Clinton Jokerst, MD, Jennifer Gould, MD, Ronald Evens, MDAc
FrWLoPrco
ªht
32
Rationale and Objective: Every year, the American Association of Academic Chief Residents in Radiology conducts a survey of the chief
residents in accredited radiology training programs in North America. The survey serves as a tool for gathering information, sharing ideas,
and voicing opinions.
Materials and Methods: An online survey was made available to the chief residents from 187 training programs in North America. Ques-
tions were presented in multiple-choice and free response formats, designed to address many issues ranging from program structure to
on-call policies, changes for the new board examination format and fellowships, and the effects of health care reform on radiology prac-
tices. The results of the survey were tabulated and responses to the repeated questions were compared with those from earlier surveysdating to 2003.
Results: Among those surveyed, 185 individual responses representing 135 unique programs were completed, yielding a 73% response
rate. Thirty-eight percent of programs responded from the northeast and 17% of programs responded from the southeast. Nineteen per-cent of responses were from central United States, 14% of responses were from western United States, and 12% of responses were from
Canada.
Conclusions: There is an increasing number of programs, which cover more hospitals, during the past decade. There are more programsproviding ultrasound and magnetic resonance services after hours, with an associated increase in after-hours attending physician cover-
age. Many changes are being made for the future board examination format. Health care reform is affecting how residents are preparing
themselves for their future practices.
Key Words: Resident education; staffing; call; health care.
ªAUR, 2013
he American Association of Academic Chief Resi- Mallinckrodt Institute of Radiology. Questions are added or
T dents in Radiology (A3CR2) includes chief residents
from all accredited radiology programs, including uni-
versity, community, and military hospitals. The organization
meets annually to discuss issues related to the training of diag-
nostic radiology residents. In addition, the A3CR2 conducts
an annual survey of resident training programs and presents
the data at the annual A3CR2 meeting held in conjunction
with the Association of UniversityRadiologists meeting (1–11).
The survey has been conducted since 1971, and the database is
maintained at the Mallinckrodt Institute of Radiology (11). The
survey is intended to not only to analyze trends regarding resi-
dency programs but also address the current issues that radiology
programs face and provide information regarding the changes
that many programs are making in the future (12–15). Survey
questions are generated by the chief residents at the
ad Radiol 2013; 20:320–331
om the Department of Radiology, Mallinckrodt Institute of Radiology atashington University, 510 South Kingshighway, Campus Box 8131, Stuis, MO 63110. Received May 12, 2012; accepted September 3, 2012.esented at the A3CR2 Meeting, San Antonio, TX, April 18, 2012. Addressrrespondence to: S.S. e-mail: [email protected]
AUR, 2013tp://dx.doi.org/10.1016/j.acra.2012.09.024
0
changed by the chief residents and several faculty members of
Mallinckrodt to address residency program issues that are
discussed at A3CR2 throughout the year. These questions are
then proposed to the Steering Committee of the A3CR2 for
final changes. Programs with more than one chief resident
were asked to select one representative to state their institution’s
name and answer program-specific questions. Any duplicate
answers from the same institution were removed after responses
were collected. The following data represent the results from
the survey conducted from February 14–24, 2012, discussing
trends in program characteristics, resident benefits, chief resident
roles, call structure, the effects of the changing board examina-
tion, fellowships, the impact of the current economy and health
care reform, and performance and quality improvement projects.
In the following sections, unless otherwise noted, there are no
changes in the data compared to the previous year’s data.
PROGRAM INFORMATION
Program structures were assessed to characterize the increas-
ing volume of studies that hospitals face in the current era of
rapidly advancing technology and the current trends in radiol-
ogy resident demographics.

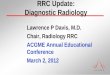
Figure 1. Percentage of programs per-
forming a given number of studies per yearin 2004, 2009, and 2012. (k indicates 1000.)
Academic Radiology, Vol 20, No 3, March 2013 A3CR2 2012 SURVEY RESULTS
Seventy-six percent of programs report that a medical
school or university is responsible for the residency pro-
gram. Twenty-five percent and 26% of programs cover
one and two hospitals, respectively, whereas 21% of
programs cover three hospitals. There is an increase in the
percentage of programs that cover more hospitals, with
15% of programs covering four hospitals and 13% of pro-
grams covering five or more hospitals (respective 2005 val-
ues were 9% and 9% in 2005). This year, 82% of programs
are a part of Level 1 Trauma centers and dedicated Stroke
Centers, 53% are National Institutes of Health–designated
cancer centers, and 54% have separate pediatric emergency
departments, covered by residents. When asked about the
number of radiologic studies performed per year, which
includes radiographs, fluoroscopic studies, nuclear medi-
cine, ultrasound, and magnetic resonance (MR) and com-
puted tomographic (CT) studies, 2% of programs perform
<100,000 studies (8% and 1% in 2004 and 2009, respec-
tively), 14% perform between 100,000 and 250,000 studies
(45% and 21% in 2004 and 2009, respectively), 33% per-
form 250,000 to 500,000 studies (30% and 42% in 2004
and 2009, respectively), 23% perform 500,000 to 750,000
studies (5% and 15% in 2004 and 2009, respectively), and
29% of programs perform >750,000 studies (12% and
21% in 2004 and 2009, respectively) (Fig 1).
A number of studies have looked at the differences between
the genders in radiology. Data from the Association of Amer-
ican Medical Colleges show an increase in the number of
women residents entering radiology, from 24% in 1999 to
27% in 2009 (16). Based on the A3CR2 Survey, among the
radiology residents in 2012, 29% are women, increased from
23% in 2003. In 2012, the average number of residents per
training program is 27 residents, increased from 21 residents
in 2003.
RESIDENT BENEFITS
Information regarding resident compensation and benefits
was gathered in an attempt to better understand the financial
obligations and constraints on residents, which are important
in future discussions regarding resident career choices (17).
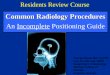
The median first-year radiology resident salary for the
2011–2012 academic year is $50,344 ($47,211 in 2009), rang-
ing from $42,000 to $100,000 (ranging from $38,000 to
$65,000 in 2009). The median fourth-year resident salary
for the 2011–2012 academic year is $56,652 ($52,944 in
2009), ranging from $48,000 to $100,000 (ranging from
$42,000 to $100,000 in 2009). Resident salaries have
increased 6.6% and 7% for first- and fourth-year residents
between 2009 and 2012, respectively. The average inflation
rate from 2009 to 2012 is estimated at 6.9% (18) (Fig 2).
Ninety-four percent of programs provide paid family leave
for residents who are pregnant during their residency (80% in
2008), but 54% require them to be taken from the pool of vaca-
tion or ‘‘sick’’days (in whole or in part). Seventy-six percent of
programs offer up to 9 weeks of family leave for residents who
are pregnant. For residents who are significant others of
spouses who had just undergone delivery (also known as
‘‘paternity’’ leave), 79% of programs offer family leave, with
57% programs taking these days from the pool of vacation or
‘‘sick’’ days (in whole or in part). Sixty-one percent of pro-
grams offer up to 2 weeks of family leave for these residents.
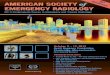
Regarding resident benefits this year, 86% of programs offer
book funds, 76% provide travel stipends for conferences, 68%
reimburse for conference fees, and 71% allocate time for con-
ferences (2008 values were 76%, 76%, 7%, and 7%, respec-
tively). The survey reports that 94% residents attend the
course offered at the Armed Institute of Radiologic Pathology
(AIRP), formerly known as the Armed Forces Institute of
Pathology. Ninety-one percent of programs offer tuition
reimbursement for residents attending AIRP, whereas 77%
programs offer reimbursements for housing and/or travel
costs (in 2008, 93% and 78%, respectively). The average
amount allotted to residents in the country is $1793 (range,
$300 to $6000). Forty-three percent of programs offer per-
sonalized lead aprons for their residents. Forty-seven percent
of programs reimburse residents for oral boards review course
tuitions and/or travel costs (Fig 3).
Internet resources have become almost invaluable to resi-
dents and their education. Ninety-three percent (146 of 157)
of programs are subscribed to STAT Dx (www.amirsys.com/
statdx.php, Amirsys Inc., Salt Lake City, UT), 34% (54 of
321

Figure 2. The median salaries (and inter-
quartile ranges) of first- and fourth-year radi-
ology residents (postgraduate year 2 and 5,respectively), in 2009 and 2012.
Figure 3. The percentage of programs that offered specific benefits to radiology residents in 2008 and 2012. ABR, American Board of Radi-
ology; AFIP, Armed Forces Institute of Pathology; AIRP, Armed Institute of Radiologic Pathology; e-Anatomy, e-Anatomy (www.imaios.com/en/
e-Anatomy); RAD, RAD Primer (www.radprimer.com); STAT Dx, STAT Dx (www.amirsys.com/statdx.php).
SAUK ET AL Academic Radiology, Vol 20, No 3, March 2013
157) are subscribed to RAD Primer (www.radprimer.com,
Amirsys Inc., Salt Lake City, UT), and 17% (26 of 157) are sub-
scribed to e-Anatomy (www.imaios.com/en/e-Anatomy,
IMAIOS SAS, France). Other benefits not included in the sur-
vey questions but commented on by those surveyed include
iPads (Apple, Cupertino, CA) for residents, gym memberships,
coverage for insurance co-payments, and meals.
CHIEF RESIDENT
Sixty-one percent of programs in the country have two chief
residents, with a range of one to six residents simultaneously
holding the position. Chief resident selection varied greatly
322
between programs and consisted of input from residents,
faculty, program directors, and the department chair. Chief
residents are offered a variety of responsibilities and benefits,
all of which have not changed dramatically since 2007.
Chief resident responsibilities remain largely administrative
(Fig 4). Ninety-five percent of chief residents are responsible
for creating the call schedule, and 80% of programs have their
chief residents create the resident rotation schedule. Seventy-
three percent of programs will designate the chief residents to
create the vacation schedule. Seventy-nine percent of pro-
grams involve the chief residents for resident recruiting and
selection. Teaching duties are less common, with 62% and
48% of programs asking chief residents to teach residents

Figure 4. The percentage of chief resi-
dents with specific responsibilities in 2012.
Figure 5. The percentage of programs that provided certain typesof reports while on-call in 2011 and 2012. Prelim, preliminary.
Academic Radiology, Vol 20, No 3, March 2013 A3CR2 2012 SURVEY RESULTS
and medical students, respectively. Regarding the curriculum,
62% programs have chief residents develop and evaluate the
training program curriculum, and 49% of programs have chief
residents create the attending lecture/conference schedule.
Chief residents were responsible for organizing the institu-
tion’s board review schedule at 42% of programs. Miscellane-
ous duties including social events and managing disputes are
handled by the chief residents in 73% and 93% of programs,
respectively.
Survey respondents reported several benefits associated
with the chief resident position. Fifty-three percent of chief
residents are allotted extra time away from clinical duties to
attend national conferences and meetings. Conference fees
and travel costs were reimbursed by residency programs for
60% of programs surveyed. Forty-three percent of programs
offer their chief residents time off-service to perform chief res-
ident duties, something that many participants in the survey
indicated would help them better fulfill their obligations as
chief resident and make the position more attractive.
Thirty-seven percent of respondents had either their own
office or a shared office with the other chief residents.
Seventy-five percent of programs offer their chief residents a
salary bonus, with a median of $1500 per year, which has
increased from $1000 in 2008.
CALL STRUCTURE
Call structures are varied and complex across all programs,
intertwining the higher demands for imaging in today’s med-
ical practices with the schedules of the technicians, residents,
and attending physicians.
On-call residents are responsible for previewing and/or
dictating studies from numerous locations, from both the
emergency department and inpatient services performed
overnight. Sixty percent of programs provide complete pre-
liminary reports to clinicians while on call (unchanged from
2011) (Fig 5). Twenty percent of programs provide abbrevi-
ated preliminary reports, answering only the clinical question
and/or incidental findings that impact the patient’s immediate
management (19% in 2011). There has been a decrease in the
programs that provide oral reports from 5% in 2009 to 1% in
2012, with an increase in final reports provided by the resident
and attending or the attending alone, from 16% in 2011 to
19% in 2012. There are several programs that have variability
in the type of report given, depending either on the type of
study (ie, only neuroradiology studies are provided with a
short preliminary report), the level of training of the on-call
resident (ie, the junior resident provides a complete
preliminary report while the senior resident provides a short
preliminary report), and the time of the day or week.
Since 2009, there has been a general trend for more ultra-
sound coverage throughout the country (Fig 6a). This year,
323

Figure 6. (a) The percentage of programs
in 2009 and 2012 that offered 24-hour so-nographers, home-call sonographers, and
residents who perform the ultrasound (US)
examinations and those programs that
have nonradiologists perform the examina-tion and that do not offer after-hours ultra-
sound examinations. (b) The percentage of
programs in 2012 that offered ultrasoundexaminations for the emergency depart-
ment (ED), inpatient services for emergent
indications, and inpatient services for rou-
tine indications.
SAUK ET AL Academic Radiology, Vol 20, No 3, March 2013
46% of programs have a trained sonographer in-house 24
hours, 7 days a week, which has increased from 29% in
2009. Thirty-eight percent of programs have a trained sonog-
rapher who is on-call but is contacted while at home, which
has decreased from 44% in 2009. Having the sonographer
take call in-house or while at home can vary depending on
the hospital covered and the day of the week. Sixteen percent
of programs will have the on-call resident perform the ultra-
sound study, increased from 13% in 2009. Every program in
the country performs emergency department ultrasound
studies after hours, including gallbladder, appendix, and scro-
tal examinations. Eighty-eight percent of programs provide
emergent inpatient studies after hours such as transplant organ
Doppler studies, and 29% of programs provide routine inpa-
tient studies after hours (Fig 6b). There are exceptions to
the ultrasound examinations performed overnight; where
many programs have the obstetrics/gynecology service per-
form and interpret pelvic and pregnancy-related ultrasound
examinations and have the vascular surgery service perform
and interpret venous Doppler studies in the evaluation for
deep venous thromboses.
324
With more clinicians aware of the increased risks of radia-
tion in medical imaging and with advances in its technology,
MR imaging (MRI) has increased in volume during the past
decade. Within those hospitals that do provide MR services
after regular business, there is variability in the types of exami-
nations performed and, depending on the urgency and
whether the patient is from the emergency department, in
whether they are performed in an outpatient or inpatient set-
ting. Ninety percent of programs provide neuroradiology
(brain and spine) services after regular business hours (after
5:00 PM). Body, musculoskeletal, and vascular studies are per-
formed in 65%, 54%, and 47% of programs, respectively,
across the country (Fig 7a). Four percent of programs do
not provide MRI studies after regular business hours. The
interpretations of MR examinations are made by the on-call
residents in 95% of programs (Fig 7b). Fourteen percent of
programs have the fellows interpret the MR examinations
with or without the resident. Twelve percent of programs
have the attendings interpret the MR examination with or
without the resident. Six percent of programs do not interpret
the MR examinations overnight. The reports given to the

Figure 7. (a) The percentage of programs
in 2012 that offered specific types of mag-
netic resonance (MR) examinations afterhours. (b) The percentage of programs in
2012 that provided interpretations for MR
examinations performed after hours, by
on-call residents, fellows, and/or attend-ings, and those that did not interpret MR ex-
aminations performed overnight.
Academic Radiology, Vol 20, No 3, March 2013 A3CR2 2012 SURVEY RESULTS
clinician may vary depending on the type of examination (ie,
only body cases are given in oral report form), on the com-
plexity of the study, and on whether the clinician calls for
the results.
The process for reviewing studies at the end of the call shift
varies across the country and may depend on the type exami-
nation performed and the level of training of the resident. The
face-to-face readout gives the opportunity for the attending
and resident to discuss each case and its findings in person.
Forty-nine percent of programs perform face-to-face read-
outs with an attending or fellowmost or all of the time. Fifteen
percent of programs perform face-to-face readouts some of
the time. No face-to-face readouts are performed in 21% of
programs.
Throughout the United States, training programs are
pressured to provide more final reports, thereby requiring
attendings to cover radiology services after hours (Fig 8).
This may depend on the type of study and the day of the
week or on some combination of being in-house and at
home depending on the time of the day. Currently, 46%
of programs have the attendings go home at the end of
the work day, which is decreased from 54% in 2010. Attend-
ings remain in-house for extended hours (ie, from 5:00 to
10:00 PM) to read out the on-call studies in 45% of programs,
previously 46% in 2010. Twenty percent of programs have
an attending in-house overnight to finalize studies, which
is increased from 15% in 2010. Attendings review cases
from home in 3% of programs, which is unchanged from
2010. Attendings review cases after hours only if the on-
call resident calls them for a specific question in 35% of
programs, which is decreased from 52% in 2010. Twelve
percent of programs hire an external teleradiology service
to read out the studies read by the on-call resident
(previously 10% in 2010).
325

Figure 8. The percentage of programs
from 2009 to 2012 that have attending
physicians go home at the end of the workday, stay in-house for extended hours (ie,
5:00 to 10:00 PM), stay in-house overnight 7
days a week, review cases at home, reviewcases that residents call about in the middle
of the night, and have external teleradiology
services read on-call studies. Other meth-
ods include having attendings read onlyneuroradiology studies after hours and hav-
ing attendings read studies after hours on
different days of the week.
SAUK ET AL Academic Radiology, Vol 20, No 3, March 2013
Routine services are sometimes performed over the week-
end, depending on the hospital and program and the available
faculty (Fig 9). Nineteen percent and 16% of programs pro-
vide half-day coverage on Saturdays and Sundays, respectively.
Full-day coverage is provided on Saturdays and Sundays in
58% and 49% of programs, previously 55% and 49% in
2010, respectively. There has been a decrease in the number
of programs that do not provide weekend routine services
(originally 27% in 2010, now 23% in 2012).
Figure 9. The percentage of programs that provide routine service
coverage for half- or full-day Saturdays and Sundays, as well as the
percentage of programs that do not provide routine service coverageover the weekend.
CHANGING BOARD EXAMINATION
In 2008, the American Board of Radiology (ABR) issued a
change in the way diagnostic radiology residents are board
certified, moving from the three-examination model (includ-
ing a physics examination, clinical examination, and oral
examination) to a two-examination model, where a ‘‘core
examination’’ is given at the end of the third year of radiology
training and a certifying examination is given 15 months after
the completion of residency (19). With this, the ABR has
determined that mastery of the core components of diagnostic
radiology must be demonstrated at the qualifying step at the
end of the third year of training, leading to many programs
switching to a ‘‘three + one’’ curriculum, where the trainee
finishes all of the core requirements for board certification
at the end of the third year of training, allowing the fourth
year of training to be dedicated to focus on subspecialties.
Ten percent of those surveyed thought this change was pos-
itive, expressing that this new board format incorporates
physics into clinical knowledge, removes the block of time
off-service for studying in the fourth year of radiology,
encourages more trainees to pursue fellowships, and allows
more focused training during the fourth year. Thirty
percent of those surveyed thought this change to be negative,
326
expressing that the new board format decreases emphasis on
effective verbal communication skills and makes it more diffi-
cult to find a job because board certification cannot be
attained until 15 months after graduating residency. The
majority of those surveyed, 62%, had mixed sentiments
regarding the new board format.
Since 2010, there has been a dramatic increase in the num-
ber of programs that have established a ‘‘three + one’’ curric-
ulum, from 5% to 41% (Fig 10). Thirty-five percent of
programs plan to have a ‘‘three + one’’ curriculum established
by 2013, increased from 19% in 2010. Seven percent of pro-
grams plan to have this new curriculum established after
2013, decreased from 18% in 2010. There is no change in
the number of programs that do not plan to change to a ‘‘three
+ one’’ curriculum, accounting for 17% of programs.

Figure 10. The percentage of programsfrom 2010 to 2012 that already have, plan
to have, or do not plan to have a 3-year
‘‘core’’ curriculum in place for the newboard
examination planned for 2013.
Figure 11. The percentage of programs in 2011 and 2012 that are
making changes for preparing radiology residents for the future‘‘core’’ board examination.
Academic Radiology, Vol 20, No 3, March 2013 A3CR2 2012 SURVEY RESULTS
Although 23% of programs have not yet decided what the
fourth-year residents will do once the new board examina-
tion is in place, 26% of programs plan to continue normal
rotations. Sixty percent of programs plan to implement
selectives, or ‘‘mini-fellowships,’’ in which residents are
allowed several months to concentrate on specific subspecial-
ties of interest. Seven percent of programs are allowing
residents who plan to matriculate into fellowships at the
same institution of their residents to begin their fellowship
training earlier and for 2 years, as opposed to the conven-
tional 1 year (ie, ‘‘three + two’’ curriculum). Twelve percent
of programs will use the fourth year to fill in deficits from
the first 3 years, and 17% of programs plan to use a combi-
nation of implementations.
In preparation for the new ‘‘core’’ examination, many
programs are offering a variety of ways for residents to study
(Fig 11). Twenty-five percent of programs are allowing those
studying for the examination time off-service to study,
which is increased from 21% in 2011. Residents will be
taken out of the call pool for a varying amount of time
(�2 to 3 months) in 50% of programs, which is increased
from 40% in 2011. Thirteen percent of programs will not
give residents any protected time, and 36% of programs
are not sure how they will structure their curriculum for
the class taking the ‘‘core’’ examination. Some programs
are planning to place those studying for the examination
on rotations that demand less time on-service or allowing
afternoons off to study.
Currently, 84% of programs offer internal board review for
the oral board examination. Thirteen percent do not offer an
internal board review but allow time off-service for external
board review. Three percent of programs do not offer internal
board reviews and do not allow time off for external board
reviews. With the new ‘‘core’’ examination, 15% of programs
plan to keep their internal board review with few or no
changes. Thirteen percent of programs plan to dramatically
change their internal board review format to match the style
of the ‘‘core’’ examination. Four percent of programs plan to
stop their internal board review, allowing time for external
review. Twelve percent of programs plan to continue allowing
time off-service for residents to attend external board reviews.
Two percent of programs plan to stop all board review ses-
sions. The majority of programs, representing 67% of those
surveyed, are not sure how they will prepare their residents
for the ‘‘core’’ examination.
With the advent of the new ‘‘core’’ curriculum format,
many programs are planning to adapt their teaching methods
to reflect the multiple-choice format of the examination. One
method includes the use of audience response systems (ARS),
which require audience members to use a clicker to enter the
answer to a multiple-choice question that the lecturer pro-
vides. At the end of a designated time limit, the results from
the polled audience are displayed, which allows the lecturer
to discuss explain the correct and incorrect answers. Nine per-
cent of programs frequently use ARS, whereas 35% rarely use
it. Fifty-two percent of programs do not use an ARS. Among
those programs that do use ARS, 36% of their residents find it
to be a valuable tool, whereas 6% find that ARS detract from
learning. Twenty-one percent of those surveyed have mixed
sentiments about the use of ARS.
327

Figure 12. The distribution of residents in
the United States who matriculated and
plan to matriculate into fellowships in 2009
and 2012, respectively. ‘‘Other’’ fellowshipsinclude emergency radiology and combined
fellowship programs. MRI, magnetic reso-
nance imaging; MSK, musculoskeletal;
NeuroIR, neurologic interventional radiol-ogy; Nucs, nuclear medicine; Peds, pedia-
trics; VIR, vascular interventional radiology.
SAUK ET AL Academic Radiology, Vol 20, No 3, March 2013
FELLOWSHIPS
Especially with the changes in the curriculum with the new
board examination format, more residents are planning to
pursue fellowship subspecialty training. Ninety-one percent
of the chief residents who were surveyed plan to enter a fel-
lowship after graduating residency, whereas 3% plan to enter
a private practice, 3% plan to enter an academic position,
and 3% plan to enter the military service.
Data from polling the rest of the chief residents throughout
the country show that interventional radiology is themost pop-
ular of fellowships, with 22% of residents in the country plan-
ning to go into it for the next year, which is increased from
15% in 2009 (Fig 12). Twenty percent of residents plan to go
into neuroradiology (increased from 15% in 2009); 14% plan
to go into musculoskeletal radiology (decreased from 19% in
2009); and 11% plan to go into breast imaging (decreased
from 13% in 2009). Pediatric radiology is planning to have
5% of this year’s fourth-year residents enter its fellowship
(increased from 2% in 2009); nuclear medicine is expecting
2% of the current fourth-year resident class to enter its fellow-
ship (increased from1% in 2009); and a stable 4% percent of res-
idents are entering a cardiothoracic imaging fellowship this year
compared with 2009. Body MR fellowships are seeing a
decrease, from 6% in 2009 to 4% this year. Seventeen percent
of residents are planning to enter either an abdomen or a
body fellowship, separate from a Body MR fellowship. One
percent of residents are planning to enter other fellowships
such as neurointerventional or emergency radiology.
There is also some variability in what percentage of the
fellowship positions are offered to external applicants. Data
from the chief resident survey show that within interventional
radiology, 25% of the fellows are from an outside institution;
within neuroradiology, 68%; within musculoskeletal
radiology, 47%; within breast imaging, 55%; within
328
abdomen/body and body MRI, 65% and 50%, respectively;
and within cardiothoracic, nuclear medicine, and pediatric
radiology, 50% of fellows are from outside institutions.
With input from the A3CR2 and the Association of
ProgramDirectors in Radiology, the Society of Chairs in Aca-
demic Radiology Departments has decided that, beginning
with radiology fellowships with start dates of July 2014, all fel-
lowships must limit their interviewing season from the begin-
ning of February of the resident’s junior year (which would
therefore correspond initially to spring 2013) and that offers
to external candidates not be made until May 1 of the third
year of residency (corresponding to May 1, 2013). Thirty per-
cent of those surveyed agree with the change as it will make
the process of interviewing for fellowships more fair.
Twenty-eight percent agree with the change but think that
it will be difficult to enforce these new limitations. Eight per-
cent disagreewith the change, and 35% of those surveyed have
no strong opinion either way. Several comments were made
that the interview season will occur at the same time as
‘‘core’’ examination preparation starting in 2014.
Currently, only neuroradiology and interventional radiol-
ogy have their fellowship applicants apply using the National
Resident Matching Program, which enforces when residents
may apply, interview, and be ranked for the match, which typ-
ically occurs every June. With the new Association of
ProgramDirectors in Radiology and Society of Chairs in Aca-
demic Radiology Departments decision for when fellowships
applicants may interview regardless of the subspecialty,
residents were surveyed regarding their preference for the fel-
lowship application process. Twenty-three percent prefer the
same application process, with priority given to internal appli-
cants and with varying application deadlines. Forty-six
percent prefer a common deadline for all fellowships applica-
tions. Five percent prefer a match process for all fellowship
positions, beyond neuroradiology and interventional

Academic Radiology, Vol 20, No 3, March 2013 A3CR2 2012 SURVEY RESULTS
radiology. Twenty-six percent prefer a combination of a
match process and a common deadline.
HEALTH CARE ECONOMICS AND THE JOBMARKET
Health care reform, falling reimbursements, and a recent eco-
nomic downturn have contributed to large changes in radiol-
ogy, especially the job market. There is increasing concern
regarding the current job market for radiologists, with 95%
of chief residents feeling at least a little worried about finding
a job after residency or fellowship. Twenty-five percent of
chief residents have already started looking for a job and 8%
already have one before graduation. To obtain a job, 60%
are willing to accept a lower salary, 50% are willing to have
less vacation time, 48% are willing to move to a less ideal loca-
tion, 44% are willing to take more call shifts, and 36% are
willing to take more weekend shifts.
Chief residents were asked about career plans following
completion of their training in radiology. Despite the inherent
selection bias from polling only chief residents and the large
number of academic training programs represented in the
results, the motivations for pursuing a particular career path
are important to evaluate. After fellowship training, 27% of
chief residents plan to enter academics, 38% plan to enter
private practice, 3% plan to enter the military service, and
32% are undecided.
The current economic environment influences career plans
in a variety of ways. Forty-five percent of chief residents
believe that there is little or no influence. Twenty-five percent
think that academics has become more appealing as a result,
whereas 10% believe that private practice has become more
appealing. Forty-two percent and 3% believe that the envi-
ronment has increased and decreased interest in training in a
fellowship program, respectively. Sixteen percent think that
the current economic environment influences one’s
fellowship choice.
When asked about the effects health care reform will have
on the field of radiology, 86% think practices will try to
increase their volume to maintain a similar salary, despite
the lower reimbursement rates. Sixty-five percent believe it
will discourage top-tier medical students from choosing radi-
ology. Thirty-six percent think that practices are going to be
looking for radiologists trained in more than one fellowship.
As far as training residents in health care economics and
radiology business, 30% of residents think their programs offer
adequate training, 34% think that their training is inadequate,
and 36% of residents report there is no training given in this
area.
The poor economic climate has led to budget issues at
some programs, especially programs that have more trainees
than its training ‘‘cap,’’ paying for a certain number of train-
ees out of pocket. As a result, such programs are looking at
the need for downsizing the number of trainees. In 2012,
51% of programs have an equal number of trainees as their
training cap. Thirteen percent of programs have more
trainees than their training cap. In the 2012–2013 academic
year, 16% of programs are planning on increasing the num-
ber of trainees, whereas 4% are planning on decreasing the
number of trainees.
PERFORMANCE AND QUALITY IMPROVEMENTPROJECTS
During the past decade, the ABR has mandated that radiolog-
ists document participation in at least three successful per-
formance and quality improvement (PQI) projects every 10
years tomaintain board certification. Sixty-two percent of res-
idents find that their programs are adequately preparing them
for this requirement. Twenty percent think they are getting
inadequate training, whereas 18% of residents are finding
that they are not getting any training in PQI projects. Among
the programs that do support residents on PQI projects, 60%
provide faculty advisors, 48% provide resources such as data-
bases and research tools, 18% provide time off-service, and
2% provide financial support. Twenty-two percent of pro-
grams do not provide any of the aforementioned methods of
support for residents pursuing a PQI project.
DISCUSSION
This year’s survey included a number of questions focusing on
the changes that are being made in anticipation for the new
board examination format. The majority of the programs
have already instituted or plan to institute a 3-year ‘‘core’’ cur-
riculum. To allow enough study time for the first class taking
the ‘‘core’’ examination, half of the programs in the country
are planning to take the class out of their call pool and some
programs are either taking residents off-service or putting
them on less time-demanding rotations, although how pro-
grams will balance this with the remaining residents remains
to be worked out on a individual program basis. Additionally,
most programs are not sure how they plan to prepare their res-
idents for the ‘‘core’’ examination, partly due to the uncer-
tainty of how the examination will appear. In June 2013,
the ABR is planning to administer a ‘‘pilot’’ examination for
the third-year residents who are eligible to take the ‘‘core’’
examination in October 2013, to provide performance feed-
back for residents and to make appropriate adjustments in the
content and scoring of the new examination. It is hoped that
after the administration of this pilot examination, programs
will have a better idea of how to prepare their residents for
passing their ‘‘core’’ examinations.
As shown in this survey, with the increasing volume of
radiologic studies in this era of rapidly advancing technology,
combined with the higher demands for attending coverage
beyond the regular work hours, programs are trying to
balance the needs for their individual hospitals without
compromising the experience of residents working inde-
pendently to train effectively for their future practices. There
has been an increase in the percentage of programs that offer
329

SAUK ET AL Academic Radiology, Vol 20, No 3, March 2013
24-hour trained sonographer coverage after hours, which
may partly be due to current campaigns to reduce patients’
exposure to radiation to as little as reasonably achievable.
With the advent of faster and more efficient MR protocols,
it is expected that there will be an increase in the volume of
MR studies performed after hours as well. Currently, 95% of
residents are interpreting MR examinations while on-call.
With more clinicians being aware of the risks of exposing
patients to radiation from CT examinations, there may be
an increase in the volume of MR studies performed.
Combined with the pressures for final reads while on-call
throughout the country, many programs are considering
readjusting how examinations are read on-call. Already,
this survey has shown an increase in the number of programs
that are providing either extended-hour or 24-hour attend-
ing coverage for studies performed on-call from 2009 to
2012. It is uncertain up to what point programs will have
attendings cover the workflow after hours before resident
training is at risk for being compromised. Future survey
results will be needed to provide more information regarding
this trend.
Given the current economic environment and the contin-
ued evolution of health care reform, there is increasing
concern among residents in the United States regarding the
current job market, with nearly all residents in the country
seeking to train in a fellowship before practicing in an aca-
demic or private practice job. Although the impacts of the
economy on the business of radiology remain uncertain, the
majority of residents in the United States think they are either
inadequately or not trained in health care economics, some-
thing that can be considered for change in program curricula
in future years.
A study was conducted in 2007 that demonstrated an expo-
nential increase in the number of CT scans performed during
the past decade, with >62 million CT scans performed in
2007 (20). Hospital coverage and the volume of radiologic
studies are continually changing over the past decade. There
is an increase in the number of programs that cover four or
more hospitals, with an associated increase in the number of
programs that perform >750,000 radiologic studies per year.
This may be due to a combination of factors, including the
increasing use of imaging for patient management and
hospitals needing to support falling reimbursement rates by
merging to support their budgets given the current economic
environment.
The residency class sizes have increased by 29% since 2003.
There is an associated 16% increase in women residents enter-
ing radiology. The reasons behind this pattern are not clear.
However, data from the Association of American Medical
Colleges indicate an increase in the number of women
residents entering other medical specialties such as allergy
and immunology, medical genetics, surgery, and surgical
subspecialties, out of proportion to the small increase in the
number of women residents choosing to enter radiology (16).
Radiology resident benefits continue to increase since
2009. Resident salaries have increased 6.6% and 7% for
330
first- and fourth-year radiology residents since 2009, respec-
tively, keeping up with the national inflation rate of 6.9%
and reflecting how sources of funding continue to adapt to
the changes in the economy. Residents are receiving increas-
ing benefits in regard to book and travel funds, conference
fees, and support for attending the AIRP conferences.
Most programs are offering support for residents who
request family leave, with more than half of the programs
taking at least some of the days of family leave from vacation
and/or sick days.
Chief residents continue to be largely responsible for
administrative duties such as schedule generation and curric-
ulum development.With the changes being made for the new
‘‘core’’ examination, chief residents will play an important role
in designing a schedule that matches the needs of residents
preparing for the examination with the program needs to
cover the various clinical services.
In conclusion, the A3CR2 survey provided data on chief
radiology residents’ perceptions concerning residency
training, changes in the curriculum with the new board
examination format, on-call policies, fellowships, and health
care economic trends. The responses provide a tool that allows
for comparison among various training programs and among
different time periods.
REFERENCES
1. Evert MB, Schertz LD, Wilson AJ, et al. Results of the 1990 survey of the
American Association of Academic Chief Residents in Radiology
(A3CR2) emphasizing data about chief residents in radiology. Invest Radiol
1991; 26:773–776.
2. Bower BL, Engels JT, Evens RG. Results of the 1989 survey of the
American Association of Academic Chief Residents in Radiology. Invest
Radiol 1991; 26:99–102.
3. Perry MA, Smith DK, Wilson AJ, et al. Results of the 1991 survey of the
American Association of Academic Chief Residents in Radiology. Invest
Radiol 1992; 27:402–405.
4. Horstman WG, Kang E, Wilson AJ, et al. Results of the 1992 survey of the
American Association of Academic Chief Residents in Radiology. Invest
Radiol 1993; 28:96–99.
5. Oser AB, Baker SM, Wilson AJ, et al. Results of the 1993 survey of the
American Association of Academic Chief Residents in Radiology. Acad
Radiol 1994; 1:154–158.
6. Duncan JR, Derdeyn CP, Evens RG. Results of the 1994 survey of the
American Association of Academic Chief Residents in Radiology. Acad
Radiol 1996; 3:72–76.
7. VanWagenen FK, Weidman ER, Duncan JR, et al. Results of the 1996
survey of the American Association of Academic Chief Residents in Radi-
ology. Acad Radiol 1997; 4:132–137.
8. Heck DV, Vaughan TE, Duncan JR, et al. Results of the 1997 survey of the
American Association of Academic Chief Residents in Radiology. Acad
Radiol 1998; 5:224–231.
9. Ruhs SA, Fromke MK, Evens RG. Results of and comments on the 1998
survey of the American Association of Academic Chief Residents in
Radiology. Acad Radiol 1999; 6:706–709.
10. Lawler LP, Fromke J, Jost RG, et al. Results of and comments on the 2000
survey of the American Association of Academic Chief Residents in Radi-
ology. Acad Radiol 2001; 8:777–781.
11. Evens RG. Report on a survey of chief residents in Academic Departments
of radiology. Invest Radiol 1972; 7:61–62.
12. Minocha J, Yaghmai V, Hammond N, et al. Cardiac imaging training in
radiology residency programs: A survey of radiology chief residents.
Acad Radiol 2010; 17:795–798.
13. Horowitz JM, Yaghmai V, Miller FH, et al. Will CT ordering practices
change if we educate residents about the potential effects of radiation

Academic Radiology, Vol 20, No 3, March 2013 A3CR2 2012 SURVEY RESULTS
exposure? Experience at a large academic medical center. Acad Radiol
2011; 18:1447–1452.
14. Chiunda AB, Mohammed TL. Knowledge of ACR thoracic imaging Appro-
priateness Criteria� among trainees: One institution’s experience. Acad
Radiol 2012; 19:635–639.
15. Petscavage JM, Paladin AM, Wang CL, et al. Current status of residency
training of allergic-like adverse events to contrast media. Acad Radiol
2012; 19:252–255.
16. Distribution of residents by specialty, 1999 compared to 2009. (2010). Ac-
cessed May 12, 2012, from www.aamc.org.
17. Kerr JR, Brown JJ. Costs of a medical education: Comparison with
graduate education in law and business. J Am Coll Radiol 2006; 3:
122–130.
18. US Inflation Calculator. (2012) Accessed on May 12, 2012, from http://
www.usinflationcalculator.com/.
19. Alderson PO, Becker GJ. The new requirements and testing for American
Board of Radiology certification in diagnostic radiology. Radiology 2008;
248:707–709.
20. Brenner DJ, Hall EJ. Computed tomography—an increasing source of
radiation exposure. N Engl J Med 2007; 357:2277–2284.
331