Embed Size (px)
Citation preview
Responsiveness in interactions of mothers and sons with ADHD: Relations to maternal and child characteristics - attention-deficit hyperactivity disorder - Statistical Data Included
Journal of Abnormal Child Psychology, Feb, 2002 by Charlotte
Johnston, Candice Murray, Stephen P. Hinshaw, William E. Pelham,
Jr., Betsy Hoza
Charlotte Johnston (1,5)
Candice Murray (1)
Stephen P. Hinshaw (2)
William E. Pelham Jr. (3)
Betsy Hoza (4)
**********
It is widely known that children with attention-deficit/hyperactivity
disorder (ADHD) have difficulties in interactions with their parents
(Johnston & Mash, 2001). However, experts agree that parenting is
unlikely to be the ultimate cause of ADHD (Barkley, 1998). Instead,
studies have suggested that parenting variables are most closely
related to the presence of comorbid oppositional defiant (ODD) or
conduct disordered (CD) behavior among children with ADHD
(Whalen & Henker, 1999). It has also been hypothesized that
problems in parent--child interactions are associated with
exacerbations or continuation of ADHD symptoms (Barkley, 1998;
Biederman et al., 1996). It is important to note that many studies of
the associations between parenting and increased child ADHD
symptoms or ODD/CD behaviors do not directly address causality.

The theoretical model most often used is transactional, with child
symptoms and parenting behavior reciprocally related, and exerting
mutual influences over time (Campbell, 1994). We sim ilarly adopt a
transactional approach and do not imply that our correlational
findings speak to the causes of either child symptoms or parenting
behavior.
Previous studies of parent--child interactions in families of children
with ADHD consistently demonstrate that in contrast to nonproblem
children (a) ADHD children are less compliant and more negative in
parent--child interactions, and (b) their parents use more
commands, more negative statements, and less praise (e.g.,
Cunningham & Barkley, 1979; Mash & Johnston, 1982). As noted
above, recent studies suggest that although ADHD children and
parents usually show more interaction difficulties than controls, the
greatest problems are often among ADHD children with comorbid
ODD/CD behavior. At both elementary-school ages and in
adolescence, studies have found higher levels of observed child
negative behavior and maternal directiveness and negativity in
families of children with comorbid ADHD and conduct problems,
compared to children with only ADHD or to control children (Barkley,
Anastopoulos, Guevremont, & Fletcher, 1992; Gomez & Sanson,
1994). Anderson, Hinshaw, and Simmel (1994) also found that
observed mater nal negativity predicted conduct problems in sons
with ADHD over a 1-2-month period, even with the effects of
maternal psychopathology and child negative behavior controlled.
Thus, although these observational findings are not entirely
consistent (e.g., Johnston, 1996), most studies support an
association between negative parenting behaviors and child conduct
problems.

Despite the contributions of this previous research, a focus on
discrete parenting behaviors may not capture the complex,
multidimensional nature of parent-child interactions. Theorists have
argued that combined patterns of parenting behaviors, or parenting
styles, are more strongly related to child behaviors than are discrete
parenting behaviors (Darling & Steinberg, 1993) and some empirical
support for this argument has been presented (Rothbaum & Weisz,
1994). The classic works in this area are those of developmental
psychologists such as Baumrind (1968, 1983), who differentiated
authoritarian, authoritative, and permissive styles of parenting
control, and Maccoby and Martin (1983), who conceptualized
parenting behaviors as falling along dimensions of responsiveness
and demandingness. Using meta-analysis, Rothbaum and Weisz
(1994) identified responsiveness-acceptance and restrictiveness as
the two important dimensions of parenting, with responsiveness
being the more important and the most strongly related t o child
externalizing behavior. Based on factor analytic studies, these
authors include variables such as parental approval of the child,
synchrony, affection, and noncoercive or authoritative control within
the construct of responsive parenting.
We argue that responsive parenting is particularly relevant in
understanding parent-child interactions among ADHD children.
Monitoring and interpreting ongoing child behavior as the basis for
adapting one's own behavior is more difficult when interacting with a
child who, by definition, displays impulsive, disorganized, and poorly-
regulated behavior. Also, given that responsive parenting has been
posited as a prerequisite for the child's development of self-
regulation skills (Kochanska, 1997; Winsler, 1998), we hypothesize
that diminished maternal responsiveness may be associated with the

severity of both ADHD and ODD/CD symptoms in children with
ADHD.
Some existing research supports this hypothesized link between an
unresponsive style of parenting and ADHD and ODD child behaviors,
particularly in high-risk samples. Among lower socioeconomic status
families followed from infancy to early school years, Carlson,
Jacobvitz, and Sroufe (1995) found that early ratings of maternal
insensitivity and overstimulating or nonresponsive physical intimacy
predicted distractible and hyperactive child behavior. However, this
study did not include children with formal diagnoses of ADHD.
Comparing the mother-child teaching task interactions of a small
group of boys with ADHD (primarily without ODD/CD problems) to
controls, Winsler (1998) found less effective maternal scaffolding in
the ADHD dyads. Scaffolding was defined as including elements such
as whether mothers modified task demands and their level of
assistance to be appropriate to the child's skill. Together, these
studies suggest a link between child ADHD symptoms and low
maternal responsiveness, but the results are limited by
nondiagnosed or small samples and the measurement of
responsiveness only at young child ages or in teaching-type
situations.
Other studies have looked at the relations between maternal
responsiveness and both ADHD and CD child behaviors. Campbell
and colleagues (Campbell, Breaux, Ewing, & Szumowski, 1986;
Campbell & Ewing, 1990) followed a sample of hard-to-manage
children from age 3 to 9, and reported that negative maternal control
(including inappropriateness of direction, lack of enjoyment of the
child, and mother-child conflict) when the child was 3 was positively
related to both ADHD and ODD/CD child behaviors at ages 6 and 9.

Only a few studies have examined maternal responsiveness in
samples of children who meet formal diagnostic criteria for ADHD or
ODD/CD. Wakschlag and Hans (1999), in a high-risk sample of
African American children, reported that maternal responsiveness as
rated in infancy negatively predicted subsequent ODD or CD
diagnoses for the child, even after controlling for the effects of
concurrent parenting and a variety of biological and family risk
factors. However, responsiveness was not related to child ADHD
symptoms. Similarly, comparing nonproblem boys and boys rated by
parents as meeting criteria for ADHD, ODD, and both ADHD and
ODD, Lindahl (1998) found that parents in all three clinical groups
were rated as showing more rejection-coercion and directiveness
than control parents. In contrast, family cohesion (including
elements of parental responsiveness) was problematic only in the
ODD and comorbid groups. Summarizing this research, it appears
that maternal responsiveness has a negative association with child
conduct problems, although only the Lindahl study included children
classified according to diagnostic criteria. Unfortunately, in that
study, observations of responsiveness were combined with other
aspects of family functioning. The current study will add important
information regarding the link between maternal responsiveness and
child behavior in school-aged children meeting diagnostic criteria for
ADHD. We predict that maternal responsiveness will be negatively
related to both ODD/CD problems and AD HD symptom severity in
boys with ADHD.
In addition to child characteristics, maternal responsiveness also has
been related to parental difficulties such as depressed mood. Using
unfamiliar children to eliminate effects due to one's own child,
Goldsmith and Rogoff (1995) reported that dysphoric women showed
less sensitivity to children than nondysphoric women. Harnish,

Dodge, Valente, and the Conduct Problems Prevention Research
Group (1995) reported that in first-grade children, the relation
between maternal depressive symptoms and child externalizing
problems was partially mediated by the level of maternal
unresponsiveness in mother-child interactions. Although not
examined extensively in prior research, impulsive or inattentive
characteristics in the parent also may interfere with the ability to
monitor and respond sensitively to child behavior. For example, in a
case report, Evans, Vallano, and Pelham (1994) found positive
associations between a mother's own ADHD symptoms and her
difficulties managing her child's behavior. In this study, we pre dict
that maternal responsiveness will be negatively related to mothers'
depressive symptoms and history of ADHD symptoms.
Many existing measures of responsiveness focus on mothers of
infants and preschool-aged children and the measures used with
older children have assessed limited aspects of responsiveness or
have combined responsiveness with other aspects of family
functioning. Therefore, one challenge for this study was to adapt
existing measures to create an observational system for maternal
responsiveness that would be developmentally appropriate for
parents of elementary-school-aged children. Based on previous
measures, as well as theoretical considerations, we examined several
dimensions of parenting behavior, including style of control,
sensitivity and responsiveness, acceptance of the child, affection,
and involvement. We assessed the validity of the observations by
examining differences in parenting behavior across situations with
different demands and correlating the behaviors with maternal
reports of family functioning. We predicted that play interactions,
because of their low structure and demands, would reveal high levels
of maternal affection and low levels of authoritarian control. In

situations where the mother was busy, we predicted low involvement
with the child. The teaching nature of a pencil-paper task situation
was expected to elicit maternal sensitivity and responsiveness to the
child's abilities and needs, and the demands of a clean-up task were
expected to lead to high levels of control. In addition, we predicted
that observed responsiveness would be related to mothers' reports of
the parent-child relationship and of parenting practices.
METHOD
Participants
Videotaped interactions of 136 mothers and their sons with ADHD
were used in this study. The data were from baseline observations
conducted at the University of California at Berkeley (n = 71) and
the University of Pittsburgh (n = 65), two of six sites involved in the
Multimodal Treatment Study of Children with ADHD (MTA). The
choice of only two sites was based on a balance between obtaining a
sufficient sample size and practical limitations on the amount of data
that could be coded. Mother-daughter interactions were excluded
because of the relatively small sample of girls. Recruitment and
assessment procedures are described in detail in previous
publications (Hinshaw et al., 1997). Although treatment outcome
data from the MTA study have been published (MTA Cooperative
Group, 1999), this investigation employs only baseline data and
focuses on pretreatment relations among maternal and child
variables.
All boys in the sample met DSM-IV criteria for ADHD, combined type.
Thirty-eight percent of the sample had comorbid ODD, 3% had
comorbid CD, 21% were comorbid for both ODD and CD, and 38%
had ADHD alone. Sixty-five percent of the mothers identified their

child's ethnicity as white, 25% as African American, 2% as
Latino/Latina, and 8% as mixed. Demographic characteristics for the
sample are presented in Table I.
Procedure
Videotaped mother-son interactions were part of the baseline
assessment battery used in the MTA study. Interactions were
conducted in furnished laboratory rooms (e.g., equipped with a table
and chairs, magazines, toys) and were videotaped through a one-
way mirror or with a camera mounted in the upper corner of the
room. Each mother-son interaction lasted 17 min and consisted of
four situations designed to elicit typical child-rearing interactions:
free play (4 min), parent busy (3 min), a paper and pencil task (5
min), and clean-up (5 min).
Mothers received verbal and written instructions for each of the four
situations. For the free-play period, with toys and magazines
available in the room, mothers engaged in an activity of their choice
with their sons.
During the parent-busy period, mothers completed questionnaires
and had their sons sit quietly in a chair, without interrupting them.
For the paper and pencil period, mothers instructed their sons to
work on either a math or a handwriting task. Last, for the clean-up
period, mothers had their sons pick up small paper dots from the
floor, put the toys away, and place the materials from the paper and
pencil task on a small table.
Measures
Observations

Maternal behavior was assessed by observation of the videotaped
mother-son interactions. Observers considered maternal behavior in
the context of the child's needs, developmental level, and the
situation. Responsiveness was conceptualized as a multidimensional
construct that included several aspects of parenting behavior. The
coding manual was derived from work of others (Campbell et al.,
1986; Carlson et al., 1995; Goldsmith & Rogoff, 1995; Harnish et al.,
1995; Kochanska, 1997) with modifications to increase the
appropriateness of the definitions for mothers' interactions with their
7-10-year-old sons. (6)
Six dimensions of maternal behavior were observed. Each dimension
was measured on a 7-point rating scale, with higher scores reflecting
more of the construct measured:
1) Authoritative Control reflected the extent to which the mother
used an authoritative method of controlling the child's behavior.
Mothers rated low on this dimension imposed high levels of structure
on their child's activities, using control strategies ranging from direct,
harsh commands (without explanations) to physical restraint. In
contrast, mothers rated as high in authoritative control encouraged
their children to participate in decision making and offered
explanations for commands. (7)
2) Sensitivity of Control measured the degree to which mothers
exerted control in a manner that was sensitive to the child's needs
and abilities. As some situations naturally require more control (e.g.,
clean up) than others (e.g., free play), and some children need more
assistance than others, this rating involved an assessment of how
much direction the child required. Mothers who were low on
Sensitivity of Control made demands that were unreasonable for the
situation (e.g., too much control in free play or too little structure in
clean up). Mothers who were high in Sensitivity of Control were able
to match their instructions to the child's level and only intervened
when their child needed assistance.
3) Responsiveness referred to the mother's overall ability to
appropriately adapt her behavior to her child's abilities, needs,
requests, and interests, as well as his ongoing behavior. Mothers low
in Responsiveness were intrusive and operated according to their
own agenda. They appeared unaware of their child's needs and their
behavior was not congruent with their child's (e.g., changed the
child's activity during play even though the child was content). In
contrast, mothers high in Responsiveness synchronized their
behavior with the affect, ability, or desire of their child, even if this
meant deviating from the instructions given.
4) Positive Affect reflected the mother's verbal and nonverbal
emotional expression in the interaction. A low score indicated that
the mother displayed frequent and/or intense negative affect (e.g.,
anger, sadness), whereas a high score indicated frequent and/or
intense positive affect (e.g., happiness, warmth). Neutral scores
reflected relatively equal amounts of negative and positive affect or
neutral affect.
5) Acceptance of the Child was based on the degree to which the
mother approved, praised, and/or showed affection toward her son.
Mothers with low scores were rejecting and cold toward their sons.
They made negative comments or expressed disapproval of their
sons' behavior in a derogatory manner. Mothers high on Acceptance
displayed genuine positive feelings for their sons, praising their
efforts regardless of the outcome.

6) Involvement with Child was assessed as the amount of time the
mother spent in verbal and nonverbal interactions with her child.
Mothers rated low on Involvement may have read magazines while
their child played whereas mothers who were high in Involvement
stayed in close proximity or engaged in conversations with their
child.
A seventh behavior category (Percent No Control) was created from
the Authoritative Control dimension and reflected the percentage of
intervals in which no maternal control was exercised.
Coders began by watching the entire interaction to gain an
understanding of the child's needs and abilities. Then, coders
watched the interaction a second time, stopping at 1-min intervals to
rate the mother's behavior across the seven categories. Coders were
trained to rate each of the dimensions of behavior independently so
that a high score on one dimension did not imply a high score on
another dimension. Two undergraduate students and the first two
authors were trained to use the coding system, through reading the
coding manual and attending regular coding meetings. Training
continued until a minimum of 80% agreement (defined as ratings
within 1-point of each other on the 7-point scale) across the
dimensions was reached between independent coders. Then,
reliability checks between independent coders continued throughout
the coding process. Thirty-five percent of the interactions were coded
independently to check for reliability. Cohen's kappas calculated for
each of the four situations ranged from .79 to . 86 for
Responsiveness, .84 to .92 for Authoritative Control, .75 to .87 for
Sensitivity of Control, .97 to .99 for Positive Affect, .96 to .99 for
Acceptance of Child, and .80 to .89 for Involvement with Child. All

coders were blind to the mothers' and children's scores on the other
measures used in the study.
Maternal Characteristics
The level of depressive symptoms in mothers was measured using
the Beck Depression Inventory (BDI; Beck, Rush, & Emery, 1979).
The BDI is a 21-item, self-report scale designed to assess adult
depressive symptoms in cognitive, somatic, and affective realms. The
BDI has high test-retest reliability (rs = .60-.90) and high internal
consistency ([alpha] = .81; Beck, Steer, & Garbin, 1988).
The level of childhood ADHD symptomatology in mothers was
measured using the Wender Utah Rating Scale (WURS; Ward,
Wender, & Reimherr, 1993). The WURS is a 5-point, 61-item, self-
report scale used to assess adults' recall of childhood levels of
inattentiveness, impulsivity, hyperactivity, oppositional behavior,
medical problems, and learning difficulties. The 25-items from this
scale that best discriminate adults with ADHD from non-problem and
psychiatric controls were used in this study. (8) The 25-item scale
has high split-half reliability (r = .90), correlates with parents'
ratings, and predicts response to medication (Ward et al., 1993). It
also correlates with current adult ADHD symptoms (Greenfield et al.,
2001; Nigg et al., 2001).
Child Characteristics
Children's levels of ADHD symptoms were assessed using both
mothers' and teachers' reports on the SNAP-IV (Swanson, 1992).
The SNAP-IV uses a 4-point scale for rating the child on the nine
inattentive and nine impulsive-hyperactive symptoms from the DSM-
IV symptom list for ADHD. Scores were added across all 18 items.
Although psychometrics have not been reported for the SNAP-IV, the
Disruptive Behavior Rating Scale, which is similar in content and
format, yields high test-retest reliability (r = .85) and internal
consistency ([alpha] = .92; DuPaul, Power, Anastopoulos, & Reid,
1998).
The child's level of conduct disordered behavior was assessed by
both mothers and teachers using the Conduct Problem scale from the
Conners' Parent Rating Scale (CPRS; Conners, 1990) and the
Conners' Teacher Rating Scale (CTRS; Conners, 1990). The Conners'
rating scales measure problematic behaviors in 4--12-year-old
children by using a 4-point scale. The manual for the Conners' scales
reports reasonable internal consistency, interrater agreement, and
test-retest reliability for the scales.
Maternal Reports of the Parent--Child Relationship and Parenting
Practices
The quality of the relationship between mothers and sons and the
level of maternal power assertion were assessed using the brief
version of the Parent--Child Relationship Questionnaire (PCRQ;
Furman & Giberson, 1995). This is a 40-item scale that assesses
parental perceptions of the quality of the parent--child relationship
on a 5-point scale. The measure includes five subscales, and three,
Personal Relationship, Warmth, and Power Assertion, were chosen
for the present study. These subscales have high levels of internal
consistency ([alpha]s > .85).
The Alabama Parenting Questionnaire (APQ; Shelton, Frick, &
Wootton, 1996) is a 42-item measure of parenting practices and
uses a 5-point scale. The Parental Involvement and Positive
Parenting subscales were used in the current study and both have

acceptable internal consistencies ([alpha]s > .80). In addition, the 3-
item Corporal Punishment subscale was used despite its lower
internal consistency ([alpha] = .46). The validity of this subscale is
suggested by its negative correlations with child age and SES and its
ability to distinguish normal and disturbed families (Shelton et al.,
1996).
RESULTS
Descriptive Information
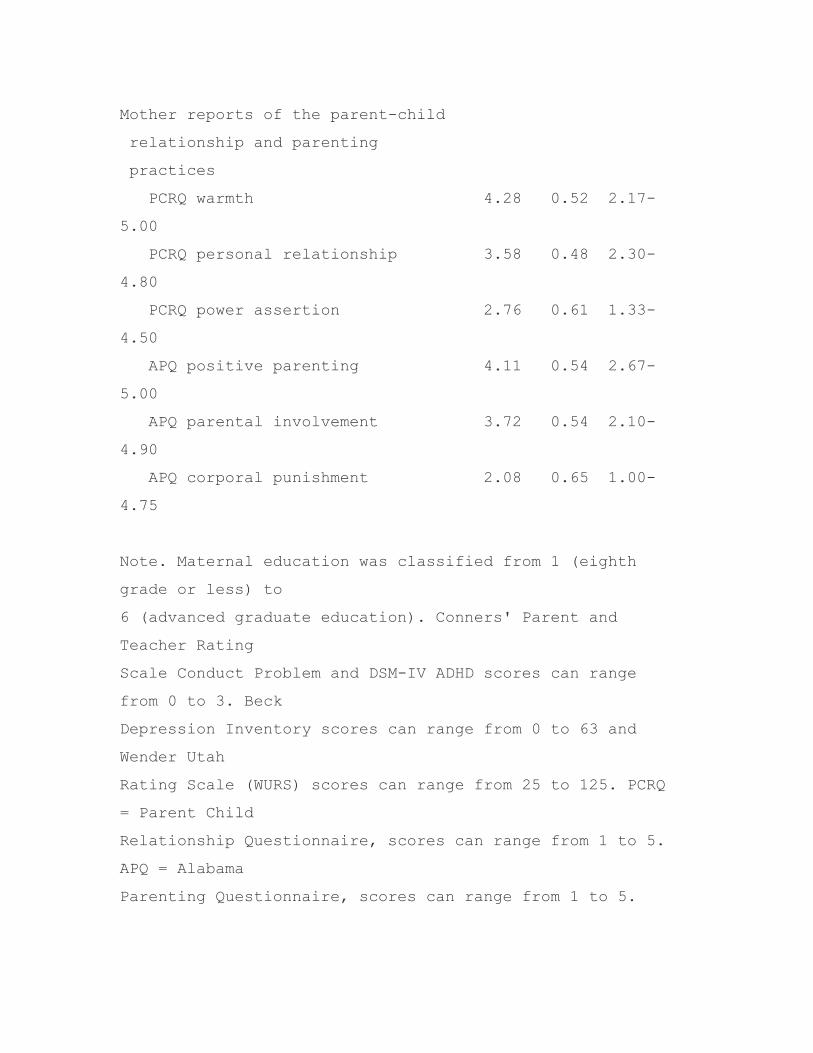
Means, standard deviations, and ranges for variables indexing
mothers' reports of the parent--child relationship, and maternal and
child characteristics are presented in Table I.
Situational Effects on Maternal Behavior
Prior to correlating observations of maternal behavior with maternal
and child characteristics, we investigated cross-situational differences
in behavior. Using the average rating across the 1-min intervals on
each of the seven maternal behavior dimensions as dependent
measures, we tested for differences across the free-play, parent-
busy, pencil-paper task, and clean-up task periods by using a
repeated-measures MANOVA.
The overall effect for situation was significant, F(21, 112) = 27.10, p
< .001. At the univariate level, situational differences were found for
Authoritative Control, F(3, 396) = 6.63, p < .001, Sensitivity of
Control, F(3, 396) = 6.08, p < .001, Responsiveness, F(3, 396) =
4.50, p < .004, Positive Affect, F(3, 396) = 32.57, p < .001,
Acceptance of Child, F(3, 396) = 2.85, p < .04, Involvement with
Child, F(3, 396) = 115.84, p < .001, and Percentage of Intervals

with No Control, F(3, 396) = 23.56, p < .001. The situation
differences for each dimension, as revealed through post hoc tests,
are shown in Table II. In general, these differences are consistent
with expectations and support the validity of the coding system.
During free play, mothers used the most authoritative methods of
control and showed the most positive affect. Free-play and parent-
busy situations were similar in that mothers used less control in
them (more intervals with no control) than in the other situations.
Parent-busy periods were charac terized by the least involvement
and by less positive affect than the other two task periods (clean-up
and pencil-paper). The teaching context of the pencil-paper task
elicited the highest levels of sensitive control and responsiveness,
and the clean-up task was characterized by the fewest intervals with
no control and by less responsiveness than other situations involving
structured tasks.
Data Reduction for Observational Measures
To reduce the number of maternal behaviors, principal components
analyses with varimax rotations were conducted on the seven
dimensions of behavior coded during each Situation (free-play,
parent-busy, pencil-paper task, and clean-up task). In each of the
four situations, the first component, labeled Responsiveness, had an
eigenvalue between 3.34 and 3.87 and accounted for approximately
half of the variance (48-55%). Authoritative Control, Sensitivity of
Control, Responsiveness, Positive Affect, and Acceptance of Child
loaded above .60 on this component, with Responsiveness and
Sensitivity of Control having the highest loadings (.80-.90 range).
Factor loadings are shown in Table III. In the free-play situation,
Involvement with Child also loaded primarily on this component.
Across the four situations, a second component emerged with
eigenvalues between 1.10 and 1.70, which accounted for 15-24% of
additional variance. Involvement and the Percentage of Intervals
with No Control generally loaded on this component , typically in the
.80-.90 range, and the component was labeled Involvement. Across
the four situations, no other components emerged with eigenvalues
above 1.
Using items with factor loadings above .60 and unit weighting of
items, a factor score was calculated for the Responsiveness
component for each situation. Across the four situations, correlations
among Responsiveness scores ranged from .58 to .81, and all were
significant at p < .01. Thus, mothers who were more responsive in
one situation, were also more responsive in the other situations.
Internal consistency for a Responsiveness score summed across the
four situations was .94. Therefore, an overall Responsiveness score
was calculated for each mother-son dyad by summing across the
four situations (M = 75.01, SD = 11.09, range 36.05-100.64). For
Involvement, because the two items loading above .60 on the
component were measured with different metrics, scores were
standardized and the control item was reversed before they were
summed to form an Involvement score for each situation.
Correlations for Involvement scores across the situations were low to
moderate (rs = .05-.49) and four of six were significant at the p <
.01 level. The alpha for an Involvement score summed across the
situations was only .68, and was not improved by omitting any
behaviors or situations. Because the Involvement score captured
only two of the coding categories and produced lower crosssituational
agreement and internal consistency than desired, we excluded it
from further analyses.
Responsiveness and Demographic Characteristics

Mothers' overall Responsiveness scores were related to the
demographic variables of child age, mother age, mother education,
and maternal marital status. Both mother age and education were
related to Responsiveness, r(129) .19, p = .03 and r(127) = .33, p <
.001, respectively. Older and better-educated mothers were more
responsive with their sons. t tests indicated that marital status (two-
parent vs. single-parent) also was related to Responsiveness, t(l,
127) = 2.02, p = .05. Single mothers were less responsive with their
sons.
Responsiveness and Reports of the Parent-Child Relationship and
Parenting Practices
To further assess the validity of the observations of maternal
behavior, Responsiveness scores were correlated with mothers'
reports of the parent-child relationship and parenting practices.
Partial correlations were used to control for mother age, education,
and marital status. Responsiveness was significantly, negatively
related to reports of harsh parenting strategies, as measured by both
questionnaires; for the Power Assertion scale of the PCRQ, r(107) = -
.35, p < .001, and for the Corporal Punishment scale of the APQ,
r(107) = -.51, p < .001. Responsiveness was not significantly related
to maternal reports of Warmth, Personal Relationship, Involvement,
or Positive Parenting (rs = .01 to -.08).
Responsiveness and Reports of Maternal and Child Characteristics
Partial correlations between maternal Responsiveness and maternal
and child characteristics were also conducted, controlling for mother
age, education, and marital status. Although controlling for the
demographic variables reduced the strength of the predicted
associations, many of the correlations confirmed predictions.

Maternal depressive symptoms, but not maternal childhood ADHD,
were negatively related to Responsiveness in interactions with their
children; for the BDI, r(92) = -.23, p = .02, and for the WURS, r(92)
= -.15, p = .16. In addition, Responsiveness was inversely related to
mothers' reports of child conduct problems, r(92) = -.26, p = .01.
The correlation between Responsiveness and teachers' reports of
conduct problems was significant at the bivariate level, r(l01) = -.23,
p = .0l, but was reduced, r(92) = -.13, p = .23, when demographic
variables were controlled. Responsiveness was not related to child
ADHD symptoms (rs = -.03 and -.01 for mothers' and teachers'
reports, respectively).
Regression Analyses
The unique contributions of maternal and child characteristics to
predicting Responsiveness were tested. Four blocks of variables were
created containing (1) relevant demographics, (2) maternal
depressive and maternal childhood ADHD symptoms, (3) child ADHD
symptoms as rated by the mother and teacher, and (4) child conduct
problems as rated by the mother and teacher. A series of regression
analyses were conducted, with each block forced into the prediction
model in last place to see if it could account for unique variance in
observed Responsiveness. This method allowed us to test the unique
contribution of each block of variables, over and above the variance
accounted for by all other predictor variables. The full regression
model was significant, but only the blocks of demographic
characteristics and child conduct problems made significant unique
contributions once all other variables were entered in the model,
F(3,87) = 2.93, p = .04, [DELTA][R.sup.2] = .07 and F(3,87) =
3.06, p = .05, [DELTA][R.sup.2] = .0 5, respectively. Thus, child
conduct problems were uniquely and negatively related to maternal

Responsiveness. Standardized beta coefficients from the full model
are shown in Table IV. Maternal education and mother's reports of
conduct problems were significant individual predictors of
Responsiveness, as was maternal depressive symptoms, even
though the maternal characteristics block as a whole did not
contribute unique variance.
DISCUSSION
We hypothesized that a stylistic aspect of parenting, responsiveness,
would be related to maternal and child characteristics in families of
ADHD children. Results confirmed that maternal responsiveness was
negatively and uniquely related to child conduct problems and also
was negatively, although not uniquely, related to maternal
depressive symptoms. Maternal responsiveness, however, was not
related to the severity of the child's ADHD symptoms. Thus, this
study adds to existing literature, suggesting that parenting
difficulties are most closely related to conduct problems in families of
children with ADHD.
As noted, mothers' responsiveness to the needs and behaviors of
their sons with ADHD was negatively related to child conduct
problems, even after the variance in responsiveness due to
demographic characteristics, maternal depressive and maternal
childhood ADHD symptoms, and severity of child ADHD symptoms
was controlled. Bivariate correlations also indicated that this
association was found, not just with mothers' reports of the child's
conduct problems, but also using teachers' reports. However, the
correlation with teachers' reports was reduced when demographic
variables were controlled and teachers' reports did not emerge as
significant predictors in the regression analyses. The link between
responsiveness and child conduct problems is consistent with
previous reports (e.g., Campbell & Ewing, 1990; Lindahl, 1998) and
likely reflects an interactive and transactional process. For example,
unresponsive parenting may be associated with increased difficulties
in child self-regulation that lead to oppositional or conduct problems
in children with ADHD, and these child problems in turn challenge
responsive parenting.
In contrast to conduct problems, child ADHD symptoms were not
related to maternal responsiveness. Although all children were
diagnosed with ADHD combined type, the standard deviations and
ranges, as well as inspection of score distributions, indicated that
there was considerable variability in the range of symptom severity.
Thus, restriction of range and distribution skew do not appear likely
explanations for the lack of association. Instead, this finding is
consistent with the emerging consensus that parental and family
characteristics are more closely related to comorbid ODD/CD
behavior, than to ADHD behavior (Johnston & Mash, 2001; Whalen &
Henker, 1999). Our findings are also consistent with the suggestion
that if an association is found between child ADHD behavior and
maternal unresponsiveness, it is most likely to occur in community
samples (e.g., Campbell & Ewing, 1990) or in structured teaching
tasks (e.g., Winsler, 1998). Although responsiveness was not related
to child ADHD symptoms, without the inc lusion of families of
nonproblem children or children with only ODD/CD behavior, we
cannot speak to whether responsiveness would discriminate among
such groups. Similarly, the present findings are limited to boys with
combined subtype of ADHD.
Also consistent with previous research (e.g., Harnish et al., 1995),
observed maternal responsiveness was negatively associated with

the maternal depressive symptoms. Mothers of children with ADHD
have been reported to experience elevated rates of depressive
symptoms (Whalen & Henker, 1999), and the present study suggests
that responsiveness in parenting may function as a mediating
mechanism through which depressive symptoms are linked to
conduct problems in children with ADHD. Specifically, a mother's
experience of depressive symptoms may interfere with her ability to
respond appropriately and sensitively to her child's behavior and this
lack of responsiveness may create or exacerbate problematic child
behavior. Although the average score on the Beck Depression
Inventory in this sample was in the nondepressed range, the highest
scores were well within the range typical of individuals with clinical
depression. However, caution must be exercised in distinguishing
reports of depressive symptoms from more formal clinical diagnoses
of depressive disorder. In contrast to the findings for depressive
symptoms, mothers' reports of their childhood symptoms of ADHD
were not related to observed parenting style. This may reflect the
limitations of the WURS as a measure of ADHD symptomatology,
including its focus on childhood rather than current symptoms and its
inclusion of symptoms that are not clearly aspects of ADHD.
In this study, we adapted previous measures of responsiveness to be
developmentally appropriate to mother-child interactions in 7-10-
year-old children, and presented evidence of the reliability and
validity of this observational measure of parenting style. In addition
to usual measures of interrater reliability, the ratings of maternal
responsiveness were internally consistent and stable across the four
observational situations. A comparison of the dimensions of maternal
behavior across four different interaction contexts supported the
validity of the measure. For example, mothers were rated as using
the most authoritative style of control and showing the most positive

affect in free play, a situation with few demands. In addition to
situational effects, the validity of the responsiveness observations
was supported by their inverse correlations with maternal reports of
harsh discipline techniques. However, responsiveness was not
related to more positive dimensions of parenting style, such as
warmth or involve ment. We speculate that the discrepancy in
relations for positive and negative aspects of reported parenting
behavior may arise because of a difference in how responsiveness
was observed versus how parenting is assessed in questionnaires. An
integral aspect of our observational measure was that maternal
behavior was coded depending on the child behavior (e.g., needs or
abilities). For example, mothers were rated as responsive if they
provided a level of instruction that was appropriate for the child's
needs. For some, this meant providing a great deal of instruction,
but for others the child needed little instruction. In contrast,
questionnaire measures are more likely to assess the absolute
quantity of a parent behavior (e.g., how often do you give
instructions). Thus, the lack of association between responsiveness
and reports of positive parenting may reflect this difference in
methods of assessment. In contrast, for harsh discipline, it can be
argued that any amount of this behavior is inappropriate and no
nresponsive and hence, the quantitative assessment offered by
questionnaires corresponds more closely to the observational
assessment.
Unexpectedly, a second component emerged in the observation
ratings that reflected aspects of the mothers' involvement with their
children. In contrast to Responsiveness, the Involvement component
accounted for less variance in the observations and revealed
relatively low internal consistency and cross-situational stability. For
these reasons, we did not include the Involvement score in our
analyses and suggest that future research is needed to explore the
meaning of observational ratings of involvement as a dimension of
parenting style.
Obviously, the correlational nature of the investigation cannot offer
evidence regarding the direction of the operative effects. We suspect
that the most likely possibility is that child conduct problems,
maternal depressive symptoms, and maternal responsiveness are
linked in a reciprocal and transactional fashion, with each component
influencing the development of each other component over time
(Sameroff & Fiese, 2000). It seems plausible that mothers who are
experiencing depressive symptoms will be impaired in their ability to
monitor and respond appropriately to their child's behavior, and that
it is harder for mothers to be responsive to children who are
oppositional and difficult to manage, and that over time, the
presence of unresponsive parenting, maternal psychological
dysfunction, and child conduct problems will fuel the maintenance of
each other. Obviously, alternate explanations are possible. More
complex, longitudinal designs that marry assessment of
environmental and genetic influences are needed to address these
possibilities. In addition, more work is needed to specify the
particular individual or relational characteristics that trigger the cycle
of difficult child behaviors and nonresponsive parenting. However,
recognition of the concurrent associations among parenting style and
parent and child characteristics in families of children with ADHD
provides a starting point for this research and for potential
interventions.
One implication of the current findings is that psychosocial
interventions in families of children with ADHD may benefit from
inclusion of more content designed to improve parental

responsiveness. Such content would not be intended to target the
ADHD symptomatology, but rather to lessen or prevent child
difficulties with comorbid conduct problems. Available data already
suggest that psychosocial treatments for children with ADHD are
particularly important for targeting child oppositional behavior and
problems in the parent-child relationship (MTA Cooperative Group,
1999). Although behavioral parenting programs often include some
degree of responsiveness training (e.g., positive attending),
additional training in this aspect of parenting may be important.
Preliminary research (e.g., Wahler & Bellamy, 1997; Wendland-
Carro, Piccinini, & Millar, 1999) demonstrates the promise of such an
approach.
ACKNOWLEDGMENTS
We extend our sincere appreciation to the entire MTA group for their
willingness to allow us to use data from that project for this report.
In addition, we thank all the families who participated in the study.
Finally, we thank Irene Kim and Catherine McDonald who offered
invaluable assistance with data coding and entry.
This work was supported by a grant from the University of British
Columbia, Hampton Fund to Dr Johnston. Dr Pelham was supported
by Grant Nos. AA06267, MH50467, MH48157, MH45576, and
MH53554; Dr Hinshaw by Grant Nos. MH50461 and MH45064; and
Dr Hoza by Grant Nos. MH47390, MH48157, and MH50467 from the
National Institute of Mental Health.
The Multimodal Treatment Study of Children with Attention-
Deficit/Hyperactivity Disorder Cooperative Group Principal
Collaborators: National Institute of Mental Health, Rockville, MD:
Peter S. Jensen, MD (Office of the Director); L. Eugene Arnold, MD

(Department of Psychiatry, Ohio State University); John E. Richters,
PhD (Developmental Psychopathology and Prevention Research
Branch); Joanne B. Severe, MS (Research Projects and Publications
Branch); Donald Vereen, MD (Office of Drug Control Policy); and
Benedetto Vitiello, MD (Child and Adolescent Treatment and
Preventive Interventions Research Branch). Office of Special
Education Programs, U.S. Department of Education, Washington, DC:
Ellen Schiller, PhD. Principal Investigators and Coinvestigators
University of California, Berkeley/University of California, San
Francisco: Stephen P. Hinshaw, PhD (Department of Psychology,
University of California, Berkeley); Glen R. Elliott, MD, PhD
(Department of Psychiatry, University of California, San Francisco).
Duke U niversity, Durham, NC: C. Keith Conners, PhD, Karen C.
Wells, PhD, and John March, MD (Department of Psychiatry and
Behavioral Sciences). University of California, Irvine/University of
California at Los Angeles: James Swanson, PhD, and Timothy Wigal,
PhD (Department of Pediatrics and Cognitive Science, University of
California, Irvine); Dennis P. Cantwell, MD (deceased) (Department
of Psychiatry, Neuropsychiatric Institute, University of California at
Los Angeles). Long Island Jewish Medical Center, New York,
NY/Montreal Children's Hospital, Montreal, Quebec: Howard B.
Abikoff, PhD (Department of Psychiatry, New York University School
of Medicine); Lily Hechtman, MD (Department of Psychiatry, McGill
University, Montreal). New York State Psychiatric Institute/Columbia
University/Mount Sinai Medical Center, New York, NY: Laurence L.
Greenhill, MD (Department of Psychiatry, Columbia University);
Jeffrey H. Newcorn, MD (Department of Psychiatry, Mount Sinai
School of Medicine). University of Pittsburgh, Pittsburg h, PA: William
E. Pelham, PhD (Department of Psychology, State University of New
York at Buffalo); Betsy Hoza, PhD (Department of Psychological

Sciences, Purdue University, West Lafayette, IN). Statistical and
Design Consultation Helena C. Kraemer, PhD (Department of
Psychiatry and Behavioral Science, Stanford University, Palo Alto,
CA).
Table I
Sample Characteristics
Variable (a) M SD Range
Demographic characteristics
Child age in months 100.46 10.47 84-124
Maternal age in years 37.70 6.95 24-60
Maternal education 4.12 1.19 1-6
Percent two-parent families 65
Child characteristics
Conduct problem
Mother report 1.34 0.55 0.21-
2.81
Teacher report 1.30 0.76 0.00-
2.92
ADHD symptoms
Mother report 1.99 0.62 0.61-
3.00
Teacher report 2.04 0.57 0.57-
2.96
Maternal characteristics
Beck Depression Inventory 7.03 6.47 0-30
Wender Utah Rating Scale 48.45 18.09 25-
103
Mother reports of the parent-child
relationship and parenting
practices
PCRQ warmth 4.28 0.52 2.17-
5.00
PCRQ personal relationship 3.58 0.48 2.30-
4.80
PCRQ power assertion 2.76 0.61 1.33-
4.50
APQ positive parenting 4.11 0.54 2.67-
5.00
APQ parental involvement 3.72 0.54 2.10-
4.90
APQ corporal punishment 2.08 0.65 1.00-
4.75
Note. Maternal education was classified from 1 (eighth
grade or less) to
6 (advanced graduate education). Conners' Parent and
Teacher Rating
Scale Conduct Problem and DSM-IV ADHD scores can range
from 0 to 3. Beck
Depression Inventory scores can range from 0 to 63 and
Wender Utah
Rating Scale (WURS) scores can range from 25 to 125. PCRQ
= Parent Child
Relationship Questionnaire, scores can range from 1 to 5.
APQ = Alabama
Parenting Questionnaire, scores can range from 1 to 5.

(a)Sample size varies slightly across measures because of
missing
information.
Table II
Observed Maternal Behavior in Free Play, Parent Busy,
Pencil-Paper Task,
and Clean-Up Task
Behavior Free play Parent busy
Authoritative Control 3.20 (a) (0.63) 2.96 (b) (0.73)
Sensitivity of Control 3.61 (a) (0.97) 3.74 (a) (1.12)
General Responsiveness 3.83 (a,c) (1.16) 3.99 (a,b)
(0.93)
Positive Affect 4.28 (a) (0.58) 3.80 (b) (0.50)
Acceptance of Child 4.04 (a) (0.59) 3.94 (b) (0.43)
Involvement with Child 5.19 (a) (1.28) 3.07 (b) (1.16)
Percent No Control (a) 26 (a) (26) 26 (a) (27)
Behavior Pencil-paper Clean-up
Authoritative Control 3.07 (b) (0.58) 2.98 (b) (0.72)
Sensitivity of Control 3.98 (b) (1.11) 3.68 (a) (1.12)
General Responsiveness 4.07 (b) (1.11) 3.76 (c) (1.12)
Positive Affect 3.97 (c) (0.44) 3.93 (c) (0.55)
Acceptance of Child 4.09 (a) (0.57) 4.02 (a,b) (0.63)
Involvement with Child 5.18 (a) (1.18) 4.65 (c) (1.23)
Percent No Control (a) 13 (b) (20) 01 (c) (15)

Note. Ratings are on a 1-7 scale, Higher ratings indicate
more
authoritative control, more sensitive control, more
responsiveness, more
positive affect, greater acceptance of the child, and more
involvement
with the child. Means with different superscripts differ
statistically
at p < .05.
(a)The percentage of intervals in which control ratings
were not made
because the mother did not engage in control of the
child's behavior.
Table III
Factor Loadings for Observational Ratings of Maternal
Behavior
Free play
Parent busy
Rating Resp. Invol. Resp.
Invol.
Authoritative Control .73 -.01 .68
-.27
Sensitivity of Control .84 -.14 .81
-.08
Responsiveness .87 -.21 .89
.16

Positive Affect .63 .07 .85
.17
Acceptance of child .80 -.04 .84
.03
Involvement with Child .61 -.55 .07
-.88
Percent No Control .06 .94 .10
.89
Pencil-Paper
Clean-up
Rating Resp. Invol. Resp.
Invol.
Authoritative Control .77 .21 .67
.04
Sensitivity of Control .89 .01 .89
.01
Responsiveness .92 .03 .89
-.01
Positive Affect .76 .07 .79
.13
Acceptance of child .83 .05 .79
.07
Involvement with Child .44 .73 .26
.77
Percent No Control .15 -.91 .14
-.86

Note. Resp.: Responsiveness; Invol.: Involvement. Loadings
above .60 are
given in italics.
Table IV
Regression Analyses Indicating contribution of Maternal
and Child
Characteristics to the Prediction of Maternal
Responsivensess
Predictor [beta] p
Marital status -.07 ns
Mother's age .11 ns
Mother's education .24 .02
Mother's depressive symptoms -.21 .04
Mother's ADHD symptoms -.04 ns
Child ADHD symptoms
Mother's report .19 ns
Teacher's report -.09 ns
Child conduct problems
Mother's report -.29 .03
Teacher's report -.04 ns
Note. Full model: F(9,87) = 3.47, p = .001, [R.sup.2] =
.26. [beta]s and
significance levels from the full regression model.
Received October 26, 2000; revision received March 22, 2001;
accepted May 17, 2001

(1.) Department of Psychology, University of British Columbia,
Vancouver, British Columbia, Canada.
(2.) Department of Psychology, University of California, Berkeley,
California.
(3.) Department of Psychology, University of New York, Buffalo, New
York.
(4.) Department of Psychological Sciences, Purdue University, West
Lafayette, Indiana.
(5.) Address all correspondence to Charlotte Johnston, Department
of Psychology, 2136 West Mall, University of British Columbia,
Vancouver, British Columbia Canada V6T 1Z4; e-mail:
(6.) The coding manual is available from the first author on request.
(7.) The Authoritative Control dimension was originally constructed
to also include a permissive style of control, with autocratic control
rated 1, authoritative control rated 4, and permissive control rated 7.
However, only 2% of ratings on this dimension were higher than 4.
Therefore, the dimension is reconceptualized as ranging from 1
(autocratic) to 4 (authoritative).
(8.) Analyses were also conducted using the full 61-item Wender
Utah Rating Scale and the Attention Problem Scale derived from
factor analyses by Stein et al. (1995). Results were identical across
the three measures.
REFERENCES

Anderson, C. A., Hinshaw, S. P., & Simmel, C. (1994). Mother-child
interactions in ADHD and comparison boys: Relationships with overt
and covert externalizing behaviors. Journal of Abnormal Child
Psychology, 22, 247-265.
Barkley, R. A. (1998). Attention deficit hyperactivity disorder: A
handbook for diagnosis and treatment (2nd ed.). New York: Guilford
Press.
Barkley, R. A., Anastopoulos, A. D., Guevremont, D. C., & Fletcher,
K. E. (1992). Adolescents with attention deficit hyperactivity
disorder: Mother adolescent interactions, family beliefs and conflicts,
and maternal psychopathology. Journal of Abnormal Child
Psychology, 20, 263-288.
Baumrind, D. (1968). Authoritarian vs. authoritative parental control.
Adolescence, 3, 255-272.
Baumrind, D. (1983). Rejoinder to Lewis's reinterpretation of
parental firm control effects: Are authoritative families really
harmonious? Psychological Bulletin, 93, 132-142.
Beck, A. T., Rush, A. J., & Emery, G. (1979). Cognitive therapy of
depression. New York: Guilford Press.
Beck, A, T., Steer, R. A., & Garbin, M. G. (1988). Psychometric
properties of the Beck Depression Inventory: Twenty-five years of
evaluation. Clinical Psychology Review, 8, 77-100.
Biederman, J., Faraone, S., Milberger, S., Curtis, S., Chen, L., Marrs,
A., et al. (1996). Predictors of persistence and remission of ADHD
into adolescence: Results from a four-year prospective follow-up

study. Journal of the American Academy of Child and Adolescent
Psychiatry, 35, 343-351.
Campbell, S. B. (1994). Hard-to-manage preschool boys:
Externalizing behavior, social competence, and family context at two-
year followup. Journal of Abnormal Child Psychology, 22, 147-166.
Campbell, S. B., Breaux, A. M., Ewing, L. J., & Szumowski, E. K.
(1986). Correlates and predictors of hyperactivity and aggression: A
longitudinal study of parent-referred problem preschoolers. Journal
of Abnormal Child Psychology, 14, 217-234.
Campbell, S. B., & Ewing, L. J. (1990). Follow-up of hard-to-manage
preschoolers" Adjustment at age 9 and predictors of continuing
symptoms. Journal of Child Psychology and Psychiatry, 31, 871-899.
Carlson, E. A., Jacobvitz, D., & Sroufe, L. A. (1995). A developmental
investigation of inattentiveness and hyperactivity. Child
Development, 66, 37-54.
Conners, C. K. (1990). Conners' Rating Scales Manual. Toronto,
Canada: Multi-Health Systems.
Cunningham, C. E., & Barkley, R. A. (1979). The interactions of
normal and hyperactive children with their mothers in free play and
structured tasks. Child Development, 50, 2 17-224.
Darling, N., & Steinberg, L. (1993). Parenting style as context: An
integrative model. Psychological Bulletin, 113, 487-496.
DuPaul, G. J., Power, T. J., Anastopoulos, A. D., & Reid, R. (1998).
ADHD Rating Scale-IV: Checklists, norms, and clinical interpretation.
New York: Guilford Press.

Evans, S. W., Vallano, G., & Pelham, W. E. (1994). Treatment of
parenting behavior with a psychostimulant: A case study of an adult
with attention deficit hyperactivity disorder. Journal of Child and
Adolescent Psychopharmacology, 4, 63-69.
Furman, W., & Giberson, R. S. (1995). Identifying the links between
parents and their children's sibling relationships. In S. Shulman
(Ed.), Close relationships in social-emotional development (pp. 95-
108). Norwood, NJ: Ablex.
Goldsmith, D. F., & Rogoff, B. (1995). Sensitivity and teaching by
dysphoric and nondysphoric women in structured versus
unstructured situations. Developmental Psychology, 31, 388-394.
Gomez, R., & Sanson, A. V. (1994). Mother child interactions and
noncompliance in hyperactive boys with and without conduct
problems. Journal of Child Psychology amid Psychiatry, 35, 477-490.
Greenfield, B., Hechtman, L., Bouffard, R., Minde, K., Looper, K.,
Ochs, E., et al. (2001, June). Correspondence between self and
"significant other" reports of childhood and current adult ADHD
symptoms. Poster presented at the International Society for
Research in Child and Adolescent Psychopathology, Vancouver.
Hamish, J. D., Dodge, K. A., Valente, E., & the Conduct Problems
Prevention Research Group. (1995). Mother-child interaction quality
as a partial mediator of the roles of maternal depressive
symptomatology and socioeconomic status in the development of
child behavior problems. Child Development, 66, 739-753.
Hinshaw, S, P., March, J. S., Abikoff, H., Arnold, L. E., Cantwell, D.
P., Conners, C. K., et al. (1997), Comprehensive assessment of

childhood attention-deficit hyperactivity disorder in the context of a
multisite, multimodal clinical trial. Journal of Attention Disorders, 1,
217-234.
Johnston, C. (1996). Parent characteristics and parent-child
interactions in families of nonproblem children and ADHD children
with higher and lower levels of oppositional-defiant behavior. Journal
of Abnormal Child Psychology, 24, 85-104.
Johnston, C., & Mash, E. J. (2001). Families of children with
attention-deficit/hyperactivity disorder: Review and
recommendations for future research. Clinical Child and Family
Psychology Review, 4, 183-208.
Kochanska, G.(1997). Multiple pathways to conscience for children
with different temperaments: From toddlerhood to age 5.
Developmental Psychology, 33, 228-240.
Lindahl, K. M. (1998). Family process variables and children's
disruptive behavior problems. Journal of Family Psychology, 12, 420-
436.
Maccoby, E. E., & Martin, J. A. (1983). Socialization in the context of
the family: Parent-child interactions. In P. H. Mussen (Series Ed.) &
E. M. Hetherington (Vol. Ed.), Handbook of child psychology: Vol. 4.
Socialization, personality, and social development (4th ed., pp. 1-
101). New York: Wiley.
Mash, E. J., & Johnston, C. (1982). A comparison of the mother-child
interactions of younger and older hyperactive and normal children.
Child Development, 53, 1371-1381.

Multimodal Treatment Study of Children with ADHD Cooperative
Group. (1999). A 14-month randomized clinical trial of treatment
strategies for attention-deficit/hyperactivity disorder. Archives of
General Psychiatry, 56, 1073-1086.
Nigg, J. T., John, O. P., Blaskey, L., Huang-Pollock, C., Willcutt, E.
G., Hinshaw, S. P., et al. (2001). Big five dimensions and ADHD
symptoms: Links between personality traits and clinical symptoms.
Unpublished manuscript.
Rothbaum, F., & Weisz, J. R. (1994). Parental caregiving and child
externalizing behavior in nonclinical samples: A meta-analysis.
Psychological Bulletin, 116, 55-74.
Sameroff, A. J., & Fiese, B. H. (2000). Models of development and
developmental risk. In C. H. Zeanah, Jr. (Ed.), Handbook of infant
mental health (2nd ed., pp. 3-19). New York: Guilford Press.
Shelton, K. K., Frick, P. J., & Wootton, J. (1996). Assessment of
parenting practices in families of elementary school-age children.
Journal of Clinical Child Psychology, 25, 317-329.
Stein, M. A., Sandoval, R., Szumowski, E., Roizen, N., Reinecke, M.
A., Blondis, T. A., et al. (1995). Psychometric characteristics of the
Wender Utah Rating Scale (WURS): Reliability and factor structure
for men and women. Psychopharmacology Bulletin, 31, 425-433.
Swanson, J. M. (1992). School-based assessments and interventions
for ADD students. Irvine, CA: KC Publications.
Wahler, R. G., & Bellamy, A. (1997). Generating reciprocity with
conduct problem children and their mothers: The effectiveness of

compliance teaching and responsive parenting. Journal of Social and
Personal Relationships, 14, 549-564.
Wakschlag, L. S., & Hans, S. L. (1999). Relation of maternal
responsiveness during infancy to the development of behavior
problems in high-risk youth. Developmental Psychology, 35, 569-
579.
Ward, M. F., Wender, P. H., & Reimherr, F. W. (1993). The Wender
Utah Rating Scale: An aid in retrospective diagnosis of childhood
attention deficit hyperactivity disorder. American Journal of
Psychiatry, 150, 885-890.
Wendland-Carro, J., Piccinini, C. A., & Millar, W. S. (1999). The role
of early intervention on enhancing the quality of mother-infant
interactions. Child Development, 70, 713-721.
Whalen, C. K., & Henker, B. (1999). The child with attention deficit
hyperactivity disorder in family contexts. In H. C. Quay & A. E.
Hogan (Eds.), Handbook of disruptive behavior disorders (pp. 139-
155). New York: Plenum.
Winsler, A. (1998). Parent-child interactions and private speech in
boys with ADHD. Applied Developmental Science, 2, 17-39.
COPYRIGHT 2002 Plenum Publishing Corporation
COPYRIGHT 2002 Gale Group