Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Response of urinary liver-type fatty acid-binding proteinto contrast media administration has a potential to predictone-year renal outcome in patients with ischemic heart disease
Daishi Fujita • Masao Takahashi • Kent Doi • Mitsuru Abe • Junichi Tazaki •
Arihiro Kiyosue • Masahiro Myojo • Jiro Ando • Hideo Fujita • Eisei Noiri •
Takeshi Sugaya • Yasunobu Hirata • Issei Komuro
Received: 13 November 2013 / Accepted: 31 January 2014
� Springer Japan 2014
Abstract Urinary liver-type fatty acid-binding proteins
(uL-FABP) have recently been recognized as a useful
biomarker for predicting contrast-induced nephropathy.
Although accumulating studies have evaluated short-term
outcomes, its prognostic value for long-term renal prog-
nosis in patients undergoing coronary angiography (CAG)
has not been fully examined. This study aimed to evaluate
the predictive value of uL-FABP for long-term renal out-
come in patients with ischemic heart disease (IHD). Con-
secutive 24 patients with impaired renal function (serum
creatinine [1.2 mg/dL) who underwent CAG were
enrolled. uL-FABP was measured before CAG, 24 and
48 h after CAG. The changes in estimated glomerular fil-
tration rate (eGFR) throughout CAG and at 1 year later
were compared with the uL-FABP levels. The patients with
a greater decrease in eGFR 1 year later had higher uL-
FABP levels at all points, but only the value at 48 h after
CAG reached statistical significance (lower vs. higher
decreased eGFR group, 4.61 ± 3.87 vs. 17.71 ± 12.96;
P \ 0.01). Measurement of uL-FABP at 48 h after CAG
(48h-uL-FABP) showed better correlation with the change
in eGFR (pre-CAG uL-FABP vs. 48h-uL-FABP: R = 0.27,
P = 0.20 vs. R = 0.65, P \ 0.01). Moreover, the high-pre
and high-48h-uL-FABP group showed a significantly lar-
ger decrease in eGFR compared with the high-pre and low-
48h-uL-FABP group (change in eGFR; 8.12 ± 4.06 vs.
1.25 ± 2.23 mL/min/1.73 m2, P \ 0.01), although the
baseline eGFR levels were similar between these two
groups. In this pilot study, measurement of uL-FABP levels
at 48 h after CAG may be useful in detecting renal damage,
and in predicting 1-year renal outcome in IHD patients
undergoing CAG.
Keywords Urinary liver-type fatty acid-binding proteins
(uL-FABP) � Renal prognosis � Coronary angiography
(CAG) � Contrast-induced nephropathy (CIN)
Abbreviations
uL-FABP Urinary liver-type fatty acid binding protein
DM Diabetes mellitus
CKD Chronic kidney disease
CAG Coronary angiography
IHD Ischemic heart disease
CIN Contrast-induced nephropathy
sCr Serum creatinine
eGFR Estimated glomerular filtration rate
Electronic supplementary material The online version of thisarticle (doi:10.1007/s00380-014-0484-9) contains supplementarymaterial, which is available to authorized users.
D. Fujita � M. Takahashi (&) � A. Kiyosue � M. Myojo �J. Ando � H. Fujita � I. Komuro
Department of Cardiovascular Medicine, Graduate School
of Medicine, The University of Tokyo, Hongo 7-3-1,
Bunkyo-ku, Tokyo 113-8655, Japan
e-mail: [email protected]
K. Doi � E. Noiri
Division of Nephrology, Graduate School of Medicine,
The University of Tokyo, Hongo 7-3-1, Bunkyo-ku,
Tokyo 113-8655, Japan
M. Abe
Department of Cardiology, Kyoto Medical Center, Kyoto, Japan
J. Tazaki
Department of Cardiovascular Medicine, Graduate School
of Medicine, Kyoto University, Kyoto, Japan
T. Sugaya
CMIC Company, Limited, Tokyo, Japan
Y. Hirata
Tokyo Teishin Hospital, Tokyo, Japan
123
Heart Vessels
DOI 10.1007/s00380-014-0484-9

Introduction
Liver-type fatty acid-binding protein (L-FABP) is a 14.4-
kDa protein expressed in the proximal tubule of human
kidney [1]. It binds to free fatty acids (FFA), which are
reported to be overloaded in the proximal tubule in various
conditions leading to tubulointerstitial damage, such as
massive proteinuria, ischemia, and toxic insults. FFAs
induce L-FABP gene expression, and L-FABP is thought to
be the regulator of FFA homeostasis in the cytoplasm.
Because measuring urinary L-FABP (uL-FABP) enables us
to monitor renal tubulointerstitial damage [2, 3], uL-FABP
has recently been recognized as a useful biomarker for
renal impairment. A number of clinical studies that eval-
uated uL-FABP have been reported with cohorts of patients
with diabetes mellitus (DM) [4–7], chronic kidney disease
(CKD) [8], kidney transplantation, cardiovascular surgery
[9, 10], and under critical care [11–14].
Coronary angiography (CAG) has become indispensable
to the evaluation and management of patients with ischemic
heart disease (IHD). Renal impairment is an important risk
factor for IHD, but many patients with coronary ischemia
have renal impairment. Although prophylactic measures for
contrast-induced nephropathy (CIN) have been widely
explored and its efficacies have been shown, it is still dif-
ficult to determine the risks and benefits of performing CAG
in each individual patient. uL-FABP has been reported as a
promising prognostic indicator for CIN occurrence [15–19],
but its effect on renal function over a longer period has not
been evaluated. Many patients undergo CAG several times,
and a useful biomarker that can predict future progression of
renal injury due to contrast medium administration is
important. We measured periprocedural uL-FABP in CAG
patients and examined whether measuring uL-FABP would
be useful in detecting patients who are susceptible to tubu-
lointerstitial damage after contrast medium administration.
We also evaluated the performance of uL-FABP for pre-
dicting the long-term renal outcomes of patients who were
exposed to contrast media.
Methods
Study design and patient enrollment
This study was designed as a part of the BLOCKADE
study (UMIN-CTR ID C000000419), in which the effect of
intravenous sodium hydrogen carbonate (NaHCO3) for the
prevention of CIN was examined. Patients suspected of
having IHD with serum creatinine (sCr) levels above
1.2 mg/dL and who underwent elective CAG at our insti-
tute were enrolled. Exclusion criteria were acute coronary
syndrome, planned dialysis, severe heart failure not toler-
ating hydration, and administration of contrast medium
within 72 h of CAG. To prevent CIN, CAG was performed
under either intravenous 0.9 % sodium chloride (NaCl;
1 mL/kg/h, 12 h before CAG until 12 h after CAG), or
intravenous NaHCO3 (3 mL/kg/h for 1 h before CAG and
1 mL/kg/h for 6 h after CAG). N-acetylcysteine
(704.8 mg/day; twice a day) was administered at the phy-
sician’s discretion on the previous day and the day of CAG.
CIN was defined as a relative increase in sCr concentration
of at least 25 % or an absolute increase in sCr of 0.5 mg/dL
at 48 h after CAG. The levels of uL-FABP were measured
on the day before CAG (pre-uL-FABP), 24 h after CAG
(24h-uL-FABP), and 48 h after CAG (48h-uL-FABP) by
specific enzyme-linked immunosorbent assay. sCr was
measured on the same day of uL-FABP. After discharge,
the patients were followed up at our outpatient clinic and
their clinical outcomes and sCr were analyzed. Estimated
glomerular filtration rate (eGFR) was calculated using the
Japanese equation for eGFR [20]. Diabetes was defined as
HbA1c [6.5 % in accordance with the National Glycohe-
moglobin Standardization Program and/or taking anti-dia-
betic agents including insulin-use regardless of fasting
glucose levels. Patients were diagnosed with hypertension
when their systolic/diastolic blood pressure on admission
was [140/90 mmHg or when they were under treatment
with antihypertensive agents. Left ventricular ejection
fraction (LVEF) was calculated by echocardiography.
The study protocol was approved by the Institutional
Review Board of the University of Tokyo Hospital
(P2008026-11X). All patients provided written informed
consent before participation.
uL-FABP analysis
For each patient, three urine samples were obtained and
then frozen at -80 �C within 12 h of collection. Urinary
L-FABP was measured using commercially available
ELISA kits (Human L-FABP Assay Kit; CMIC Co Ltd.,
Tokyo, Japan). Briefly, a sandwich is formed of the
L-FABP antigen between the anti-L-FABP antibody coated
at the bottom of a microplate and the free anti-L-FABP
antibody conjugated with peroxidase. Its optimal density is
measured after incubation with substrate to determine the
L-FABP concentration. Urinary L-FABP levels were
evaluated by correction with urine creatinine concentration
as previously described [12].
Data analysis and statistics
Data are presented as the mean ± SD. The Student t test or
Mann–Whitney test was used to compare two groups.
Heart Vessels
123

Univariate and multivariate analyses were performed to
clarify the factors that correlated with the change of eGFR.
These calculations were performed using Dr. SPSS II for
Windows (SPSS Japan, Inc, Tokyo). P \ 0.05 was con-
sidered to be statistically significant.
Results
From January 2009 to March 2010, 24 patients were
enrolled in this study. The clinical backgrounds of these
patients are shown in Table 1. All the enrolled patients
were diagnosed as CKD based on the KDIGO guideline
(i.e., eGFR \60 mL/min/1.73 m2). The underlying disor-
der for CKD was either DM or hypertension in all patients.
There were no significant differences in uL-FABP levels at
any point and eGFR at 1 year later between the NaCl group
and NaHCO3 group (data not shown). The average amount
of contrast medium used for CAG was 60.0 ± 17.9 mL.
The patients who were required the later PCI amounted
to 11. And there was no significant difference in baseline
and followed eGFR levels between required and not
required PCI patients (Supplement Table; eGFR change
rate; no PCI vs. later PCI = 0.96 ± 5.68 vs. 3.20 ± 5.56,
P = 0.34).
Table 2 shows the baseline and follow-up data for renal
function and uL-FABP. There was no CIN occurrence
within the observation period of 48 h in this study. At
1 year from CAG, renal impairment had progressed by
0.10 ± 0.20 mg/dL in sCr and by 2.0 ± 5.5 mL/min/
1.73 m2 in eGFR. The time course of uL-FABP in each
patient is shown in Fig. 1a. In 8 patients, the uL-FABP level
did not change at all, whereas in the remaining 16 patients
the level was significantly increased at 24 h after CAG. The
levels of uL-FABP had almost reverted to the baseline at
48 h after CAG. The patients were divided into two groups
by the median value of eGFR change at 1 year (median;
-1.05 mL/min/1.73 m2). Although both higher and lower
progression in eGFR groups exhibited similar time courses
in terms of uL-FABP values (Fig. 1b, c), the greater eGFR
progression group had higher uL-FABP levels at all points.
In this group, only the 48h-uL-FABP value reached statis-
tical significance. Previous reports showed uL-FABP levels
were positively correlated with urinary albumin levels [21].
We did not collect the levels of the urinary albumin in all
patients, but only 8 patients were available the urinary
albumin levels. In these patients, the pre-uL-FABP had a
correlation with urinary albumin values (supplemental fig-
ure: R = 0.90, P = 0.003). Urinary albumin value reflected
the pre-uL-FABP, as well as previous report.
Regression analysis revealed the following parameters
to be risk factors for a long-term decrease in eGFR for
1 year: higher 48h-uL-FABP levels and higher baseline
Cystatin C level (Table 3). Pre-uL-FABP and 24-h-uL-
FABP levels were not statistically significant, although
levels of 48h-uL-FABP were significantly correlated with a
decrease in eGFR (Fig. 2a, b, c). The amount of contrast
medium was not a significant risk for renal outcome in our
analysis.
To confirm the predictive value of uL-FABP for renal
outcome at 1 year, the patients were divided into two
groups by the median value of uL-FABP measured at each
time point, and the changes in eGFR were compared
(Table 4). The patients in the higher uL-FABP group
showed a significantly larger decrease of eGFR compared
Table 1 Background of patients in this study
Patients background
n 24
Age 69.9 ± 8.5
Female 2 (8 %)
Height (cm) 163.0 ± 6.4
Weight (kg) 65.3 ± 12.9
BMI 24.5 ± 4.2
DM 16 (66.7 %)
CHF 3 (12.5 %)
HTN 24 (100 %)
PAD 3 (12.5 %)
pPCI 15 (62.5 %)
pCABG 3 (12.5 %)
Diseased vessels
Average 2.17
1 5
2 10
3 9
ACE-I 6 (25 %)
ARB 16 (66.7 %)
Diuretics 5 (20.8 %)
NSAIDS 2 (8.3 %)
Statin 19 (79.2 %)
Baseline sCr (mg/dL) 1.37 ± 0.20
eGFR (mL/min/1.73 m2) 40.83 ± 7.96
Cystatin C (mg/L) 1.20 ± 0.24
Hb (g/dL) 12.39 ± 1.29
CRP (g/dL) 0.23 ± 0.27
BNP (pg/mL) 87.1 ± 107.5
Overt urinary protein 9 (37.5 %)
LVEF (%) 68.0 ± 9.6
Contrast medium (mL) 60.0 ± 17.9
N-acetylcysteine 21 (87.5 %)
DM diabetes mellitus, CHF congestive heart failure, HTN hyperten-
sion, PAD peripheral artery disease, ACE-I angiotensin-converting
enzyme inhibitors, ARB angiotensin receptor blockers, NSAIDS non-
steroidal anti-inflammatory drugs, BNP brain natriuretic peptide,
LVEF left ventricular ejection fraction
Heart Vessels
123

with the lower group at all time points, although there was
no statistical difference in the baseline eGFR levels
between the groups.
To confirm that the patients with prolonging increase in
uL-FABP have poor renal outcome, the patients with high
(n = 12) and low pre-uL-FABP (n = 12) were further
divided into two groups according to the ratios of their uL-
FABP levels at 24 and 48 h after CAG to pre-uL-FABP
levels (Table 5). The median ratios of 24h- and 48h-uL-
FABP to pre-uL-FABP were 2.8 and 2.0, respectively, in
the lower pre-uL-FABP group. There was no difference in
eGFR change at 1 year among the subgroups in the lower
pre-uL-FABP group. Among the higher pre-uL-FABP
subgroups, the higher 48h-uL-FABP subgroup exhibited a
significant change in eGFR at 1 year, while the higher 24h-
uL-FABP group did not (Table 5; Fig. 3a, b). The median
ratios of 24h- and 48h-uL-FABP to pre-uL-FABP were 1.8
and 0.8, respectively, in the high pre-uL-FABP group. The
high-pre and high-48h-uL-FABP level groups showed a
significantly larger decrease in eGFR over a year compared
with the high-pre and low-48h-uL-FABP level groups
(Table 5), although the baseline eGFR levels were similar
between these two groups. The patient backgrounds for
these two groups are shown in Table 6. Although the high-
pre and high-48h-uL-FABP groups were slightly older and
had higher brain natriuretic peptide levels, there was no
significant difference in risk factors for renal outcome
between the two groups.
Table 2 Baseline and follow
up renal functionPre CAG 24 h 48 h 1 year
sCr (mg/dL) 1.37 ± 0.20 1.34 ± 0.23 1.41 ± 0.28 1.47 ± 0.31
eGFR (mL/min/1.73 m2) 40.83 ± 7.96 40.77 ± 10.48 42.53 ± 9.72 38.84 ± 9.67
uL-FABP (lg/gCr) 11.82 ± 15.32 24.97 ± 29.33 11.16 ± 11.59
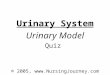
Fig. 1 a uL-FABP levels in study patients at each time point. On
average, uL-FABP levels had doubled at 24 h after CAG and returned
to baseline at 48 h. b uL-FABP levels in 12 patients in which the
eGFR did not decline at 1 year. The average uL-FABP levels were
6.24 ± 10.48 (pre CAG), 13.36 ± 15.88 (24 h), and 4.61 ± 3.87
(48 h). All data are the average ± SD. c uL-FABP levels in 12
patients with worsened eGFR at 1 year. The average uL-FABP levels
were 17.40 ± 17.24 (pre CAG), 36.58 ± 34.63 (24 h), and
17.71 ± 12.96 (48 h). Both groups exhibited a similar time course
change in uL-FABP levels after CAG, but only the uL-FABP level at
48 h was statistically significant (lower vs. higher change in eGFR
group, 4.61 ± 3.87 vs. 17.71 ± 12.96; *P \ 0.01)
Heart Vessels
123

Discussion
Urinary L-FABP is a recently developed renal biomarker
that changes dramatically with contrast medium adminis-
tration. In accordance with a previous report, our data
confirmed a large increase in uL-FABP levels after contrast
medium usage and its levels recovered towards baseline
after 48 h from CAG [15]. uL-FABP has been reported as a
useful marker for predicting the occurrence of CIN, which
is defined by a modest but significant elevation of sCr [22].
The results obtained in this study indicated that this sen-
sitive biomarker would also be useful in detecting mild
renal damage which would not change sCr or eGFR. In
addition, sustained elevation of uL-FABP for 48 h after
CAG was an indicator of poor renal outcome at 1 year.
In this study, CIN, which is defined by an elevation of
sCr, was not observed. This is possibly because the amount
of contrast medium was quite low and sufficient preventive
measures such as N-acetylcysteine and intravenous NaCl or
NaHCO3 administration were taken. Although there was no
significant difference in baseline renal function among the
patients, uL-FABP levels before and after CAG varied
markedly. It is of note that patients with a higher pre-uL-
FABP level or post-uL-FABP level had worse renal out-
come at 1 year. On the other hand, patients whose uL-
FABP levels recovered after CAG had a better long-term
renal outcome. These results may suggest that uL-FABP
could reflect mild renal damage which would not affect
eGFR immediately but have a significant impact on long-
term renal prognosis. It is well known that renal tubular
cell injury will induce inflammatory cell infiltration and
fibrosis and subsequently promote renal dysfunction
Table 3 Univariate and multivariate analyses of eGFR change
Univariateanalysis
Multivariateanalysis
R P value R P value
Gender (female) 0.24 0.25
Age -0.11 0.60
DM 0.15 0.48
Baseline sCr 0.001 1.00
Baseline eGFR 0.002 0.99
Baseline Cystatin C 0.45 0.03 0.39 <0.01
Amount of contrast medium 0.21 0.32
ACE-I -0.25 0.24
ARB 0.33 0.12
Statin 0.27 0.21
Overt urinary protein 0.60 <0.01 0.006 0.712
uL-FABP
Pre CAG 0.27 0.20
24 h 0.27 0.21
48 h 0.65 <0.01 0.46 <0.01
Statistically significant P values are in bold
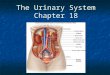
Fig. 2 a Correlation between change in eGFR and pre-uL-FABP
levels (regression coefficient R = 0.27, P = 0.20). b Correlation
between change in eGFR and uL-FABP level at 24 h (regression
coefficient R = 0.26, P = 0.21). c Correlation between change in
eGFR and uL-FABP level at 48 h (regression coefficient R = 0.65,
P \ 0.01). The levels of uL-FABP at 48 h showed better correlation
with change in eGFR than uL-FABP levels at other time points
Heart Vessels
123

independently from a glomerular lesion. Because L-FABP
in urine is dominantly derived from renal tubular cells, it is
quite possible that the measurement of uL-FABP will
enable clinicians to monitor the stress or injury to renal
tubular cells [21, 23, 24].
Although eGFR did not change through CAG in this
study, uL-FABP can detect minor impairment in kidney
and can clinically be important for the management of
patients with CKD. We speculate that measuring uL-FABP
after CAG enables us to identify the high-risk patients who
would have further renal dysfunction 1 year later. In our
study, uL-FABP levels at 48 h after CAG seemed to be the
most reliable indicator. The pre-uL-FABP and 24h-uL-
FABP levels varied greatly, and there may have been many
influencing factors such as temporary dehydration through
the CAG and excess salt intake during the pre-hospital-
ization. The measured values of 48h-uL-FABP were stable,
perhaps because the measurement conditions were rela-
tively uniform. Forty-eight hours is long enough for the
contrast medium used to be washed out of the patient’s
Table 4 eGFR change according to the uL-FABP levels
uL-FABP N eGFR (mL/min/1.73 m2) P value
Baseline 1 year D
Pre
High 12 38.54 ± 10.47 33.87 ± 10.24 -4.68 ± 4.75 0.02
Low 12 43.12 ± 2.58 43.83 ± 5.68 0.71 ± 4.83
24 h
High 12 40.08 ± 10.02 35.64 ± 10.68 -4.44 ± 5.78 0.03
Low 12 41.58 ± 5.02 42.04 ± 7.24 0.46 ± 3.87
48 h
High 12 37.85 ± 9.42 33.41 ± 9.09 -4.44 ± 4.82 0.03
Low 12 43.82 ± 4.49 44.28 ± 6.71 0.46 ± 5.01
eGFR levels at baseline and 1 year for each subgroup are shown. The patients were divided into two groups according to the median value of uL-FABPlevels at each point. The median uL-FABP levels were as follows: pre 3.09, 24 h 13.89, 48 h 6.48, respectively. At every time point, the high groupshowed a larger change in Egfr. There were no statistically significant differences among the baseline eGFR values
Statistically significant P values are in bold
Table 5 eGFR change according to the uL-FABP levels, subgroup analysis
uL-FABP N eGFR (mL/min/1.73 m2) P value
Baseline 1 year D
Pre low
24 h
High 6 43.34 ± 2.40 42.52 ± 7.54 -0.82 ± 6.52 0.33
Low 6 42.91 ± 3.19 45.14 ± 4.04 2.24 ± 2.80
48 h
High 6 43.52 ± 2.36 43.87 ± 7.01 0.35 ± 5.18 0.82
Low 6 42.73 ± 3.18 43.80 ± 5.30 1.06 ± 5.37
Pre high
24 h
High 6 39.20 ± 10.29 35.91 ± 11.39 -3.29 ± 4.18 0.47
Low 6 37.88 ± 10.60 31.80 ± 8.47 -6.08 ± 4.87
48 h
High 6 39.83 ± 10.09 31.72 ± 7.72 -8.12 ± 4.06 <0.01
Low 6 37.25 ± 10.68 36.00 ± 11.88 -1.25 ± 2.23
eGFR values at baseline and 1 year for each subgroup are shown. The patients were divided according to their pre-uL-FABP and then by their post-uL-FABP/pre uLFABP ratio at the median. The pre-low groups had only slight changes in eGFR at 1 year, regardless of their uL-FABP levels at 24 or 48 h. Inthe higher pre-uL-FABP group, patients with high 48h-uL-FABP levels showed the largest and a significant change in eGFR (-8.12 ± 4.06; P \ 0.01).The higher pre and lower 48h-uL-FABP level groups had a favorable renal prognosis. Median ratios of post- to pre-uL-FABP: low-pre and 24 h was 2.8,low-pre and 48 h was 2.0, high-pre and 24 h was 1.8, high-pre and 48 h was 0.8. There were no statistically significant differences among the baselineeGFR
Statistically significant P value is in bold
Heart Vessels
123

body. Furthermore, at 48 h the body fluid volume and salt
intake were relatively constant, so it is also an appropriate
time for measurement from this perspective. Forty-eight
hours after CAG seems to be the right timing for detecting
prolonged damage. Patients with high levels of 48h-uL-
FABP should preferably undergo an examination that does
not use contrast medium, such as RI scintigraphy. The
measurement of 48h-uL-FABP can be useful in optimizing
our method of follow-up after percutaneous coronary
intervention in patients with renal impairment. Conversely,
patients with low uL-FABP levels through CAG may be
able to tolerate repeated contrast medium administration.
Our study has some limitations. First, the conditions in
which each patient’s urine was obtained were not strictly
unified. Basically, the first urine in the morning of day 1 and
day 2 was obtained, but water intake was not limited and the
degree of dehydration may have differed among patients.
We attempted to standardize this by urine creatinine levels.
Our study population was rather small and was limited to
patients with risk factors for IHD. All patients had
hypertension and many patients had DM, and they were
administered the optimal medications. This may have been
the reason why the already known risk factors such as DM
did not reach statistical significance for progression in renal
impairment in our study. A longer period of time is perhaps
needed for other risk factors to become prominent. In
addition, a large-scale multicenter prospective study is
necessary to confirm the result of this study. Despite these
limitations, our results still show that 48h-uL-FABP levels
are a very strong predictor of renal outcome at 1 year after
CAG in patients suspected of having IHD.
In conclusion, the measurement of 48h-uL-FABP levels
may be useful for detecting renal damage after contrast
Fig. 3 Patients with high pre-uL-FABP were further divided into two
groups according to their post-uL-FABP levels: a Subgroups divided
by their uL-FABP levels at 24 h. There was no significant difference
between the two groups in eGFR change at 1 year (-6.08 ± 4.87 vs.
-3.29 ± 4.18, P = 0.47). b Subgroups divided by their uL-FABP
levels at 48 h. While the low 48h-uL-FABP subgroup had good renal
outcome, the high 48h-uL-FABP subgroups showed as much as
-8.12 ± 4.06 change in eGFR at 1 year. *P \ 0.01
Table 6 Background of high pre- and low 48h-uL-FABP group, and
high pre and high 48h-uL-FABP group
Patients background High-low High–high P value
n 6 6
Age 67.7 ± 13.7 72.3 ± 9.8 0.5
Female 1 (16.7 %) 1 (16.7 %) n.s.
Height (cm) 158.6 ± 9.5 161.6 ± 3.7 n.s.
Weight (Kg) 63.4 ± 19.8 62.7 ± 7.7 n.s.
BMI 24.9 ± 6.5 24.1 ± 3.4 n.s.
DM 4 (66.7 %) 4 (66.7 %) n.s.
CHF 1 (16.7 %) 1 (16.7 %) n.s.
HTN 6 (100 %) 6 (100 %) n.s.
PAD 0 (0 %) 2 (33.3 % 0.5
pPCI 3 4 n.s.
pCABG 2 3 n.s.
Average diseased
vessels
2.17 2.33 n.s.
1 2 1
2 1 2
3 3 3
ACE-I 2 (33.3 %) 1 (16.7 %) 0.5
ARB 3 (50 %) 4 (66.7 %) 0.6
Diuretics 2 (33.3 %) 2 (33.3 %) n.s.
NSAIDS 0 (0 %) 0 (0 %) n.s.
Statin 4 (66.7 %) 6 (100 %) 0.5
Baseline sCr (mg/dL) 1.51 ± 0.27 1.38 ± 0.26 0.4
eGFR (mL/min/1.73 m2) 37.25 ± 11.70 39.83 ± 11.05 0.7
Cystatin C (mg/L) 1.20 ± 0.24 1.35 ± 0.19 0.23
Hb (g/dL) 11.93 ± 1.15 12.60 ± 2.00 0.5
CRP (g/dL) 0.36 ± 0.43 0.19 ± 0.15 0.38
BNP (pg/mL) 66.7 ± 75.9 157.9 ± 140.0 0.19
Overt urinary protein 4 (66.7 %) 5 (83.3 %) 0.5
LVEF (%) 67.0 ± 7.5 65.8 ± 6.9 0.8
Contrast medium (mL) 67.5 ± 22.1 65.8 ± 6.9 n.s.
N-acetylcysteine 5 (83.3 %) 4 (66.7 %) 0.5
Later PCI 4 (66.7 %) 4 (66.7 %) n.s.
The abbreviations are listed in Table 1
Heart Vessels
123

medium administration and for predicting 1-year renal
outcome in patients undergoing CAG.
Conflict of interest There are no conflicts of interest, and there was
no source of support for this article.
References
1. Kamijo-Ikemori A, Sugaya T, Kimura K (2006) Urinary fatty
acid binding protein in renal disease. Clin Chim Acta 374:1–7
2. Kamijo A, Sugaya T, Hikawa A, Okada M, Okumura F, Yama-
nouchi M, Honda A, Okabe M, Fujino T, Hirata Y, Omata M,
Kaneko R, Fujii H, Fukamizu A, Kimura K (2004) Urinary
excretion of fatty acid-binding protein reflects stress overload on
the proximal tubules. Am J Pathol 165:1243–1255
3. Yokoyama T, Kamijo-Ikemori A, Sugaya T, Hoshino S, Yasuda
T, Kimura K (2009) Urinary excretion of liver type fatty acid
binding protein accurately reflects the degree of tubulointerstitial
damage. Am J Pathol 174:2096–2106
4. von Eynatten M, Baumann M, Heemann U, Zdunek D, Hess G,
Nawroth PP, Bierhaus A, Humpert PM (2010) Urinary L-FABP
and anaemia: distinct roles of urinary markers in type 2 diabetes.
Eur J Clin Invest 40:95–102
5. Kamijo-Ikemori A, Sugaya T, Yasuda T, Kawata T, Ota A,
Tatsunami S, Kaise R, Ishimitsu T, Tanaka Y, Kimura K (2011)
Clinical significance of urinary liver-type fatty acid-binding
protein in diabetic nephropathy of type 2 diabetic patients. Dia-
betes Care 34:691–696
6. Chou KM, Lee CC, Chen CH, Sun CY (2013) Clinical value of
NGAL, L-FABP and albuminuria in predicting GFR decline in
type 2 diabetes mellitus patients. PLoS One 8:e54863
7. Panduru NM, Forsblom C, Saraheimo M, Thorn L, Bierhaus A,
Humpert PM, Groop PH (2013) Urinary liver-type fatty acid-
binding protein and progression of diabetic nephropathy in type 1
diabetes. Diabetes Care 36(7):2077–2083
8. Ivanisevic I, Peco-Antic A, Vulicevic I, Hercog D, Milovanovic
V, Kotur-Stevuljevic J, Stefanovic A, Kocev N (2013) L-FABP
can be an early marker of acute kidney injury in children. Pediatr
Nephrol 28(6):963–969
9. Matsui K, Kamijo-Ikemori A, Sugaya T, Yasuda T, Kimura K
(2012) Usefulness of urinary biomarkers in early detection of
acute kidney injury after cardiac surgery in adults. Circ J
76:213–220
10. Liu S, Che M, Xue S, Xie B, Zhu M, Lu R, Zhang W, Qian J, Yan
Y (2013) Urinary L-FABP and its combination with urinary
NGAL in early diagnosis of acute kidney injury after cardiac
surgery in adult patients. Biomarkers 18:95–101
11. Doi K, Negishi K, Ishizu T, Katagiri D, Fujita T, Matsubara T,
Yahagi N, Sugaya T, Noiri E (2011) Evaluation of new acute
kidney injury biomarkers in a mixed intensive care unit. Crit Care
Med 39:2464–2469
12. Katagiri D, Doi K, Honda K, Negishi K, Fujita T, Hisagi M, Ono
M, Matsubara T, Yahagi N, Iwagami M, Ohtake T, Kobayashi S,
Sugaya T, Noiri E (2012) Combination of two urinary biomarkers
predicts acute kidney injury after adult cardiac surgery. Ann
Thorac Surg 93:577–583
13. Cho E, Yang HN, Jo SK, Cho WY, Kim HK (2013) The role of
urinary liver-type fatty acid-binding protein in critically ill
patients. J Korean Med Sci 28:100–105
14. Tsigou E, Psallida V, Demponeras C, Boutzouka E, Baltopoulos
G (2013) Role of new biomarkers: functional and structural
damage. Crit Care Res Pract 2013:361078
15. Nakamura T, Sugaya T, Node K, Ueda Y, Koide H (2006) Uri-
nary excretion of liver-type fatty acid-binding protein in contrast
medium-induced nephropathy. Am J Kidney Dis 47:439–444
16. Kato K, Sato N, Yamamoto T, Iwasaki YK, Tanaka K, Mizuno K
(2008) Valuable markers for contrast-induced nephropathy in
patients undergoing cardiac catheterization. Circ J 72:1499–1505
17. Bachorzewska-Gajewska H, Poniatowski B, Dobrzycki S (2009)
NGAL (neutrophil gelatinase-associated lipocalin) and L-FABP
after percutaneous coronary interventions due to unstable angina
in patients with normal serum creatinine. Adv Med Sci
54:221–224
18. Malyszko J, Bachorzewska-Gajewska H, Poniatowski B, Mal-
yszko JS, Dobrzycki S (2009) Urinary and serum biomarkers
after cardiac catheterization in diabetic patients with stable
angina and without severe chronic kidney disease. Ren Fail
31:910–919
19. Manabe K, Kamihata H, Motohiro M, Senoo T, Yoshida S,
Iwasaka T (2012) Urinary liver-type fatty acid-binding protein
level as a predictive biomarker of contrast-induced acute kidney
injury. Eur J Clin Invest 42:557–563
20. Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, Ya-
magata K, Tomino Y, Yokoyama H, Hishida A (2009) Revised
equations for estimated GFR from serum creatinine in Japan. Am
J Kidney Dis 53:982–992
21. Abe M, Maruyama N, Suzuki H, Inoshita A, Yoshida Y, Okada
K, Soma M (2013) L/N-type calcium channel blocker cilnidipine
reduces plasma aldosterone, albuminuria, and urinary liver-type
fatty acid binding protein in patients with chronic kidney disease.
Heart Vessels 28(4):480–489
22. Katoh H, Nozue T, Kimura Y, Nakata S, Iwaki T, Kawano M,
Kawashiri M, Michishita I, Yamagishi M (2013) Elevation of
urinary liver-type fatty acid-binding protein as predicting factor
for occurrence of contrast-induced acute kidney injury and its
reduction by hemodiafiltration with blood suction from right
atrium. Heart Vessels. doi:10.1007/s00380-013-0347-9
23. Remuzzi G, Benigni A, Remuzzi A (2006) Mechanisms of pro-
gression and regression of renal lesions of chronic nephropathies
and diabetes. J Clin Invest 116:288–296
24. Nath KA (1992) Tubulointerstitial changes as a major determi-
nant in the progression of renal damage. Am J Kidney Dis
20:1–17
Heart Vessels
123