Embed Size (px)
Citation preview

E L S E V I E R European Neuropsychopharmacology 6 (1996) 85-91
EUROPEAN NEURO. PSYCHOPHARMACOLOGY
Response in chronic schizophrenia correlated with chlorpromazine, 7-OH- chlorpromazine and chlorpromazine sulfoxide levels
M. Chetty a'*, V.L. Pillay b, S.V. Moodley c, R. Mil l e r d
~Department of Pharmacy, Wits University Medical School, 7 York Road, Parktown 2193, South Africa hDepartment of Chemical Engineering, University of Natal, Durban, South Africa
~Fort Napier, Pietermaritzburg, South Africa dDepartment of Biopharmaceutics, Food & Drug Administration, Washington, DC. USA
Received 26 June 1994; accepted 4 July 1995
Abstract
The relationship between chlorpromazine, six of its metabolites and therapeutic response in chronic schizophrenic patients was investigated in this study. Logistic regression revealed no correlation between therapeutic response and four metabolites viz. Nor, chlorpromazine, Nor 2 chlorpromazine, chlorpromazine-N-oxide and Nor 2 chlorpromazine sulfoxide. A good correlation was seen between CPZ (P=0.036), 7-hydroxychlorpromazine (P=0.004), chlorpromazine sulfoxide (P=0.002) and therapeutic response. Good therapeutic response was correlated to high levels of chlorpromazine and its 7-hydroxy metabolite while high levels of the sulfoxide metabolite appeared to have a negative effect on therapeutic response. Poor responders who had high levels of chlorpromazine also had high levels of the sulfoxide metabolite. This suggests that the difference in response may lie in the difference in the metabolism of the drug.
Kevwords: Chlorpromazine; Metabolite; Therapeutic effect
1. Introduction
The clinical efficacy and safety of chlorpromazine (CPZ) may be enhanced by evaluation of its plasma- concentration-effect characteristics but little information is presently available on these properties of CPZ. Many authors have reviewed studies that have attempted to correlate levels of CPZ and its metabolites with clinical outcome in schizophrenics (May and Van Putten, 1978; Cooper, 1978; Midha et al., 1987; Cohen, 1984; Baldes- sarini et al., 1988; Dahl, 1986; Balant-Gorgia et al., 1993). However, most of the evidence on plasma-concentration- effect relationships of CPZ have been inconclusive and controversial. In a critical review, May and Van Putten (1978) have ascribed the failure to establish a definite correlation between plasma concentration and effect to factors such as technical problems in obtaining and prepar- ing the chemical analysis of plasma samples; heterogeneity of population samples with regard to age, acuteness or chronicity of disease, and duration of neuroleptic treat- ment; lack of distinct and specific clinical end points; lack
*Corresponding author. Fax: 011-6472052.
0924-977X/96/$15.00 © 1996 Elsevier Science B.V. All rights reserved SSDI 0 9 2 4 - 9 7 7 X ( 9 5 ) 0 0 0 4 7 - X
of a sensitive clinical psychiatric scale and the rote of CPZ metabolites.
With the shortcomings of previous studies in mind, this study was designed to investigate whether any correlation exists between plasma concentrations of CPZ, the major metabolites of CPZ and therapeutic response, in chronic schizophrenic patients who had relapsed and were treated with variable doses of CPZ (as determined by the psychiat- rist in attendance).
2. Research methodology
2.1. Patients
Ethical approval for this study was obtained from the University of Durban-Westville.
In-patients between the ages of 16 and 55 years with a diagnosis of schizophrenia (American Psychiatric Associa- tion, 1987), from the King George V Hospital and Fort Napier Hospital were included in the study. Informed consent was obtained from the patient, guardian or the medical superintendent. Patients presenting with an or-

86 M. Cheto' et al. / European Neuropsychopharmacology 6 (1996) 85-91
ganic disorder, e.g. hepatic, renal or gastrointestinal dis- ease, were excluded from the trial. Relapsed patients were included provided CPZ or its metabolites were not present in the plasma on admission to hospital.
The patient was withdrawn if there was evidence of non-compliance, administration of another antipsychotic agent or if the patient developed severe or unacceptable adverse reactions to CPZ.
Routine physical examination and clinical laboratory tests were performed on admission of the patient.
The patients were given sugar coated CPZ tablets. Dosage adjustment was based on the clinical judgement of the psychiatrist in attendance. Some patients were given anticholinergic medication at the request of the psychiat- rist. No other concurrent medication was permitted.
2.2. Blood sampling
Blood samples were drawn from the patients on entry into the study, to establish the absence of detectable levels of CPZ or its metabolites in plasma prior to inclusion in the study. Thereafter, 10 ml of blood was drawn from the median cubital vein of the patients weekly (for 3 weeks), 12 h after the evening dose. Heparinised tubes were used and contact with the rubber stopper was prevented. Any dosage change was made at least 5 days prior to the blood level being taken, to ensure that steady state was reached.
2.3. Plasma concentration analysis
Plasma samples were stored at -70°C and analysed by normal phase high performance liquid chromatography (HPLC), as described previously (Chetty and Miller, 1991). The metabolites that were measured are listed below, with the assay sensitivity for each metabolite given in square brackets.
7-Hydroxychlorpromazine (7-OH-CPZ) Nor I chlorpromazine (Nor~CPZ) Nor 2 chlorpromazine (Nor2CPZ) Chlorpromazine-N-oxide (CPZ-N-OXIDE) Chlorpromazine sulfoxide (CPZ Sulf) Nor 2 chlorpromazine sulfoxide (Nor2CPZ Sulf) The sensitivity for CPZ was 3 ng/ml.
[3 ng/ml] [5 ng/ml] [4 ng/ml] [5 ng/ml] [4 ng/ml] [6 ng/ml]
The synthetic metabolites were supplied by Dr S. Kennedy of the National Institute of Mental Health, Rockville, USA and Prof. K.K. Midha of the University of Saskatoon.
2.4. Pharmacodynamic assessments
Response to CPZ therapy was assessed by the Brief Psychiatric Rating Scale (BPRS) (Overall and Gorham, 1962). A baseline assessment was performed on inclusion
in the study. Thereafter the BPRS assessment was per- formed weekly, when blood samples were taken.
The BPRS factor score described below was used in the pharmacodynamic assessment (Overall and Gorham, 1988).
sum of composite items Factor score -
number of composite items
The scores, rated by the clinician, ranged from 1 (symp- toms not present) to 7 (symptoms extremely severe).
The BPRS assessments were made by the patients' therapist. Inter-rater reliability testing, as assessed by product-moment correlation, was shown to be favourable prior to commencement of the study.
2.5. Logistic regression
Logistic regressions of therapeutic response versus plasma concentrations of CPZ and six metabolites were carried out in this study. This method of data analysis was used to assess the frequency of patients responding (coded as 1) or not responding (coded 2) to varying plasma concentrations of CPZ and the metabolites. The technique is termed logistic regression because it investigates the linear dependence of the logistic transformation of the dependent variable (outcome or response) to several in- dependent variables (plasma concentrations) (Kirkwood, 1988). The logistic transformation (abbreviated as logit) is defined as:
proport ion Logit = log e i - ~ n
The model is fitted to the data using the maximum likelihood ratio technique for the binomial distribution of response or outcome.
Since there were many independent variables (time, plasma concentrations of CPZ and concentrations of six different metabolites), stepwise logistic regression was also used. Using this technique, predictor (independent) vari- ables were selected in a stepwise manner, and the co- efficients for logistic regression were estimated. At each step in the stepping process, a continuous variable (e.g. plasma concentration of a metabolite) or a set of variables (e.g. plasma concentrations of three metabolites) is added to or removed from the model. The step selections were based on the maximum likelihood ratio.
The output includes the log likelihood, the change in log likelihood from the previous step and three goodness-of-fit chi-square statistics. For each set of variables (metabolites) considered, the output includes frequency of success or failure, predicted probability, observed proportion and standardized residuals.
In the first step the log transformed concentrations of chlorpromazine and each of the metabolites were calcu- lated and each of these was used separately in a logistic regression.
Stepwise logistic regression (multiple logistic regres-

M. Chetty et al. / European Neuropsychopharmacology 6 (1996) 8.5-91 87
Table 1 Demographic characteristics
Number of patients 29 Number of samples 87 Age (years) 16-50 Weight (kg) 48-81 Male 18 Female 12 Dosage range (mg/day / 300-1200
0.0017) and therapeutic response. The relationship be- tween these plasma concentrations and therapeutic re- sponse can be represented by the following equation:
exp( - 11.27 + 3.18(1n CPZ) + 2.386(1n MI) - 4.48(1n M2)
pr - 1 + exp( - 11.27 + 3.18(In CPZ) + 2.386(1n MI ) - 4.48(1n M2))
where:
sion-backward elimination) was then used on all the above variables to determine which ones .contributed indepen- dently to the outcome.
All the above logistic regression analyses had time as a co-variant factor. Correlations were considered to be significant when P<0.05.
SAS software (version 6.03, SAS Institute Inc., North Carolina) was used to analyse data by logistic regression.
3. Results
Thirty patients of Asiatic origin were included in this study. One patient withdrew his consent to participate in the study a week after he had been included. The demo- graphic characteristics of the patients are presented in Table 1.
The 87 sets of data, consisting of plasma concentrations of CPZ and the metabolites and BPRS scores, that were used in the logistic regression analysis, are given in Appendix 1.
Inter-rater reliability testing (assessed by product-mo- ment correlation) produced the following favourable re- sults: r=0.85, P<0.001 for the following items: somatic concern, mannerisms and posturing, grandiosity, hostility, hallucinatory behaviour, motor retardation, unco-operative- ness, blunted affect, unusual thought content; r=0.71, P<0.002 for the following items: emotional withdrawal, guilt feelings, depressive mood, suspiciousness; and r= 0.67, P<0.03 for the remaining three items, i.e. anxiety, conceptual disorganisation and tension.
Results of logistic regression revealed no correlation between therapeutic response and four metabolites, viz. NorICPZ, NorzCPZ, CPZ-N-OXIDE and Nor 2 CPZ Sulf (Table 2). A good correlation was seen between CPZ (P=0.0362), 7-OH-CPZ (P=0.0037), CPZ Sulf (P=
Table 2 Results of logistic regression
Drug P value
CPZ 0.0362 CPZ-N-oxide 0.2230 7-OH-CPZ 0.0037 CPZ Sulf 0.0017 Nor~ CPZ 0.2160 Nor2CPZ 0.6025 NohCPZ Sulf 0.5032
p r
In M1
In M2
In CPZ
exp
=probability of therapeutic response =natural logarithm of the concentration of 7-OH-CPZ =natural logarithm of the the concentration of CPZ Sulf =natural logarithm of the concentration of CPZ = exponent
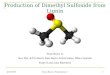
Fig. la is a graphical representation of the probability of response relative to all three components for the final regression model with one of the components, CPZ Sulf, fixed at 50 ng/ml. This graph illustrates that for a given concentration of CPZ Sulf (e.g. 50 ng/ml) the probability of CPZ treatment producing therapeutic improvement in 50% of the patients (i.e. pr=0.5) will depend on the relative concentrations of CPZ and 7-OH-CPZ. If the line corresponding to pr=0.5 is highlighted in Fig. la (see line i.e. contour representing P=0.5) and viewed from above, the contour in Fig. l b is obtained.
In Fig. l b the area above the curve represents the combinations of concentrations that would produce a >50% probability of improvement.
Contours similar to that in Fig. l b for CPZ Sulf concentrations ranging from 5 ng/ml to 125 ng/ml are presented in Fig. lc. These contour plots illustrate that as the concentration of CPZ Sulf increases, the area represent- ing pr>0.5 decreases ie. response to CPZ therapy de- creases and higher concentrations of CPZ and 7-OH-CPZ are required to produce a response with a probability greater than 50%.
4. Discussion
The results of this study suggest that the therapeutic outcome of CPZ therapy is influenced by the parent compound as well as two of the metabolites that were measured viz. CPZ Sulf and 7-OH-CPZ. Increasing con- centrations of 7-OH-CPZ and CPZ were associated with therapeutic improvement while increasing concentrations of CPZ Sulf were associated with diminished therapeutic response.
The results of many studies that have attempted to correlate the CPZ metaholite levels with therapeutic re- sponse to CPZ therapy concur with the observations made in this study. In a study of eight male schizophrenics treated long-term with high doses of CPZ (700-5000

88 M. Chetty et al. / European Neuropsychopharmacology 6 (I996) 8 5 - 9 t
(a)
pr
(b)
p = o.5 contmw ~
, ,\ ,
s?
;c
(c)
10 1Q0 20o 300 400 500 600
f 1 4nm to i~ii,~ d ~ e ~ ~ a a ~ ~lllan ~ a ~ W > 0.5 i
Fig+ 1. Graphical representation of the probability of response.

M. Chetty et al. / European Neuropsychopharmacology 6 (1996) 85-91 89
mg/day), the non-responders had levels of CPZ Sulf that were greater than their CPZ levels whereas the responders had lower levels of CPZ Sulf (Sakalis et al., 1973). This agrees with our finding that high levels of CPZ Sulf are associated with diminished therapeutic response.
Mackay et al. (1974) examined the relationship between global symptom control and plasma concentrations of CPZ, 7-OH-CPZ and CPZ Sulf in 86 chronic schizophre- nic patients. The CPZ Sulf concentrations were signifi- cantly lower in the good response group compared to those showing poorer control. The 7-OH-CPZ levels were higher in the good response group compared to those showing poorer control. The concentration of CPZ was not sig- nificantly different in good and poor responders. The ratio of 7-OH-CPZ/CPZ Sulf was significantly greater in well controlled patients than in poorly controlled patients. Good response was correlated to lower CPZ Sulf/CPZ ratios and higher 7-OH-CPZ/CPZ ratios. These findings are similar to those of the present study.
The findings of Sakurai et al. (1975) supported those of Mackay et al. (1974) when they reported that the CPZ Sulf to CPZ ratio appeared to be higher in the unchanged group of schizophrenics (nine patients) when compared to the slightly improved (10 patients) and improved (seven patients) groups. This lends further support to the findings of the present study.
Sakalis et al. (1972, 1973, 1977) examined the ratios of 'active' and 'inactive' compounds in responders and non- responders. Good responders had ratios of CPZ+7-OH- CPZ to CPZ Sulf that were greater than 1 while poor responders had ratios lower than 1. Here again CPZ Sulf appeared to be the 'inactivating' metabolite.
Although the above studies have provided a compelling body of evidence associating high concentrations of 7-OH- CPZ with therapeutic improvement and high concentra- tions of CPZ Sulf with diminished improvement, some researchers (Phillipson et al., 1977) were unable to detect 7-OH-CPZ in both good responders and poor responders. In a review on the plasma level monitoring of antipsy- chotic drugs, Cooper (1978) attributed the absence of 7-OH-CPZ in the above studies to technical difficulties in the assay procedure rather than the absence of the metabo- lite in the plasma of the patients.
The negative effect that high concentrations of CPZ Sulf appear to have on therapeutic improvement raises the following questions which warrant further investigation:
In the case of poor responders, is the target receptor in the brain occupied by a pharmacologically inactive metab- olite which acts like a competitive antagonist or a partial agonist?
Does a high concentration of CPZ Sulf effect changes that may modulate responsiveness of the D 2 receptor to the active compounds?
Does CPZ Sulf exert its inhibitory effect on therapeutic improvement via another receptor such as the D 3 receptor?
Why do some patients have higher CPZ Sulf/CPZ ratios than others?
Traficante et al. (1979) have focused on the last question when they suggested that sulfoxidation of chlorpromazine by human blood may represent a major metabolic route of drug inactivation in humans. These researchers found that small quantities of blood catalyse the formation of chlor- promazine sulfoxide from CPZ in a dose-dependent man- ner in vitro. An endogenous inhibitory protein 'regulates' sulfoxidation in vivo. Further preliminary studies by these researchers have suggested that schizophrenic patients who do not respond to CPZ and have high plasma levels of ring-sulfoxide appear to have much lower levels of this endogenous plasma protein factor than those patients who are known drug responders.
The proposed therapeutic window for CPZ is 30-350 ng/ml (Rivera-Calimlim et al., 1973, 1976; Curry, 1976). In this study a good response was associated with CPZ levels of 30 ng/ml to 380 ng/ml. However, some patients had relatively high levels of CPZ but failed to show good therapeutic response. Such patients are usually classified as being resistant to CPZ therapy, perhaps due to a particular subtype of schizophrenia. In this study, poor responders who had high levels of CPZ also had high levels of CPZ Sulf. This suggests that the difference in response in chronic schizophrenics may lie in the difference in the metabolism of the drug.
The observed relationship between plasma drug and metabolite concentrations and therapeutic outcome is very interesting to the researcher and the clinician. However, it is probably too complex to be useful in routine therapeutic monitoring of the drug. Measuring plasma CPZ Sulf levels relative to CPZ and 7-OH-CPZ levels may be useful in patients who do not show good response to CPZ. High concentrations of CPZ Sulf relative to the other two compounds may warrant the change of the drug rather than a dosage increase.
Acknowledgments
The authors would like to thank the Medical Research Council (SA) for the Research Grant and Prof. K.K. Midha of the University of Saskatchewan and Dr S. Kennedy of the U.S. National Institute of Mental Health for supplying the test samples of CPZ metabolites. The assistance of the nursing staff at the King George and Fort Napier Hospitals is appreciated. The authors are also grateful to Dr J.B. Carlile for his assistance in the design and initial im- plementation of the protocol. This study was conducted at the University of Durban-Westville.
Appendix I
Plasma concentrations of CPZ, the metabolites and therapeutic response

90 M. Chetty et at. / European Neuropsychopharmacology 6 (1996) 85-91
Patient
1 1 1 2 2 2 3 3 3 4 4 4 5 5 5 6 6 6 7 7 7 8 8 8 9 9 9 I0 10 10 11 11 11 12 12 12 13 13 13 14 14 14 15 15 15 16 16 16 17 17 t7 t8 18 t8 19 19 19 20 20 20 21 21 21 22
Concentration (ng /ml) CPZ CPZ-N-OXIDE
89.64 134.80 197.50 84.15 493.70 214.80 31.44 28,45 29.91 57.82 32.7t 3!.49 148.40 479.51 274.10 90.53 331,00 107.60 65.38 9.51 93.78 50.53 96.05 43,74 44.10 53.97 159.70 121.90 283.30 168.60 26,98 18.51 61.18 58.66 40.95 51.02 51.84 39.07 173.80 143.40 165.80 127,90 36.54 40.00 422.00 42.23 381.90 254.20 80.69 22.32 62.18 31,58 95.00 t 6.00 125.60 241.30 91.27 127.30 89.92 53.39 172.90 77~81 220.40 49.10 221.00 33.00 82.84 126,00 100.84 93.26 121.10 60.44 80.45 122.50 121.40 85.10 138.60 89.96 36.16 51.95 36.44 30.48 35.00 18.00 62.60 10.10 83.27 15.29 94.00 14.00 89,15 76.65 158.32 53,00 187.00 220.00 37.45 55,21 155.57 142.50 t 79.00 121.00 81.07 47.41 107.56 5.82 115.00 8.00 61.89 33A4 87,25 43.54 71.53 83.44 118.54 90.10 125.34 170,83 157.21 81.43 17.24 65.76 25.71 36.76 30,08 37.11 41.42 11.74
7-OH-CPZ CPZ Sulf NOR2CPZ NOR~CPZ NOR2CPZ Sulf
24.37 84.85 69.82 30.52 4.14 20.96 89.61 69.82 30.52 5.68 14,90 102,20 143.00 32.36 2.35 25.53 42.95 t 6.00 1 t .51 t 9,37 36.53 7,54 19.15 l 1.00 I9.37 35.53 6,22 15,06 1 t.38 21.47 13.26 479.5 t 10,95 5.85 BD 25.2.4 174.19 45.52 33.03 64.90 91.72 79.00 61. I 0 47.19 68.20 22.97 49.80 13.62 23.29 28.32 43.68 21.42 10.23 15.85 68.33 57.30 22.74 14.33 24.71 60.23 7.25 42.47 BD 12,25 BD 22,60 53.90 64.73 62.08 78.23 55.24 21.09 86.84 54.42 97.90 8.79 19.28 BD 11.73 23.84 84.47 8,35 24.69 23.67 1 t.38 62,60 6.88 19.27 19.53 14.14 11.49 138.86 5.21 15.99 26.74 23.59 125.10 28.83 39.07 40,11 2Z40 t 03.20 23.83 35. t 5 25.58 16.53 29.57 BD 12.34 BD 324.60 64.00 115.30 t 59.70 47.45 309,00 41.90 68.17 50.16 49,87 17.68 72.51 9.87 12.34 20.01 53.14 22.13 13.41 12.32 23 28 28.00 8.00 13,00 51.00 6~00 27.93 59.04 7.67 24.94 9.83 50.52 12.60 12.16 27.11 8.73 66.22 19.84 4,41 13.86 19.15 17.73 40.19 13.50 17.56 5.96 82.81 t 8.20 13.50 17,56 5.96 74.00 16.00 12.00 19.00 8.00 20.26 37.98 13.47 46.05 15.03 38.64 18.71 15.40 24.53 7.28 42.14 12.85 32.18 24.04 5.74 17,05 82.53 2.20 68.71 28.69 22.31 56.18 9.73 15.86 29.58 59,93 37.63 18.36 21.18 18.73 10,22 18.64 BD 16.0I 21.08 33.18 11.60 BD 11.51 28.37 9.00 5.00 16,00 21.00 20.00 32.32 15.51 BD 14.48 BD 42.25 23.36 8.14 14.85 BD 18,00 18.00 1 t .00 16.00 7.00 53.50 46.04 13.50 17.99 59,38 67.22 69.83 024 7,25 52.01 172.00 27.00 49.00 73,00 40.00 19.60 19.44 9.12 16.49 24.04 47.95 34.89 20.25 20.26 53.70 45~00 36.00 20.00 28.00 34.00 26.96 47.03 33.05 26.26 21.30 48.53 17,51 28.62 30.23 31.01 50.00 13.00 18.00 31.00 33.00 66.19 46.18 6.88 29.29 10,31 55.63 62.32 13.81 30.27 43.48 52.13 66.81 16.95 25.82 39.59 5.85 26.52 17.96 10.58 145,65 BD 21.67 BD 10.98 32.95 4,49 21,27 BD 21.68 40.36 BD 29.99 BD 19.99 50.2 I t 2,79 14.90 0.0O BD t 6.53 27.21 11.50 BD 19.55 t8,78 18.24 9.70 BD 14.06 50.20
Time (weeks)
Response

M. Chetty et al. / European Neuropsychopharmacology 6 (1996) 85-91 9l
Patient
22 22 23 23 23 24 24 24 25 25 25 26 26 26 27 27 27 28 28 28 29 29 29
Concentration (ng/ml) CPZ CPZ-N-OXIDE
32.11 12.35 38.36 9.82 53.25 41.68 140.00 18.80 137100 110.00 22.24 79.39 66.89 50.53 110.00 36.00 113.13 38.17 125.82 2.58 156.00 7.00 227.48 146.12 259.70 153.70 233.00 146.00 48.41 28.96 77.51 145.90 69.00 100.00 157.30 100.30 218.00 190.00 182.00 53.00 172.20 109.40 158.30 98.42 179.00 113.00
7-OH-CPZ CPZ Sulf NOR2CPZ NOR~CPZ NOR2CPZ Sulf Time Response (weeks)
18.84 4.60 BD 10.83 68.33 2 2 19.45 4.30 BD 10.81 66.65 3 I 21.87 52.25 8.63 9.61 15.68 I 2 96.16 24.97 12.05 13.59 71.4 2 l 21.00 6.00 16.00 19.00 49.00 3 1 20.96 36.18 9.25 17.84 29.22 I 2 51.25 33.15 5.73 18.54 43.80 2 1 35.00 25.00 7.00 17.00 27.00 3 1 24.61 29.20 7.89 13.23 66.97 I 2 119.89 25.03 5.15 12.43 41.59 2 I 106.00 69.00 7.00 5.00 31.00 3 1 3.20 95.06 42.44 42.82 191,30 1 2 211.32 86.42 50.30 38.75 156.21 2 1 103.00 36.00 39.00 48.00 101.00 3 1 30.34 233.12 7.44 15.55 31.37 1 2 279.20 254.00 157.70 136.40 692.20 2 2 273.00 140.00 99.00 53.00 557.00 3 2 20.53 41.20 20.53 20.36 125.21 I 2 43.00 25.00 BD 9.00 28.00 2 I 21.00 10.00 BD 9.00 28.00 3 1 94.97 98.60 28.46 31.02 159.47 1 2 33.42 133.40 31.20 29.62 119.63 2 2 104.00 27.00 30.00 70.00 130.00 3 2
References
American Psychiatric Association (1987) Diagnostic and Statistical Manual of Mental Disorders (DSM-III-R), 3rd edn. (revised). Ameri- can Psychiatric Association, Washington, DC.
Balant-Gorgia, A.E., Balant. L.E and Andreoli, A. (1993) Phar- macokinetic optimisation of the treatment of psychosis. Clin. Phar- macokinet. 25, 217-236.
Baldessarini, R.J., Cohen, R.M. and Teicher, M.H. (1988) Significance of neuroleptic dose and plasma level in the pharmacological treatment of psychoses. Arch. Gen. Psychiatry 45, 79-91.
Chetty, M. and Miller, R. (1991) Effect of storage on the plasma concentration of chlorpromazine and six of its metabolites. Ther. Drug Monit. 13, 350-355.
Cohen, B.M. (1984) The clinical utility of plasma neuroleptic levels. In: Stance (Ed.), Guidelines for the Use of Psychotropic Drugs. Spectrum, New York, pp. 245-260.
Cooper, T.B. (1978) Plasma level monitoring of antipsychotic drugs. Clin. Pharmacokinet. 3, 14-38.
Curry, S.H. (1976) Gas-chromatographic methods for the study of chlorpromazine and some of its metabolites in human plasma. Psycho- pharmac. Commun. 2, 1-15.
Dahl, S.G. (1986) Plasma level monitoring of antipsychotic drugs. Clin. Pharmacokinet. 11, 36-61.
Kirkwood, B.R. (1988) In: Essentials of Medical Statistics. Blackwell Scientific, London, pp. 105-106.
Mackay, A.V., Healy, A.F. and Bake, J. (1974) The relationship of plasma chlorpromazine to 7-hydroxy and sulfoxide metabolites in a large population of schizophrenics. Br. J. Clin. Pharmacol. 1, 425-430.
May, ER.A. and Van Putten, T. (1978) Plasma levels of chlorpromazine in schizophrenia. Arch. Gen. Psychiatry 35, 1081-1087.
Midha, K.K., Hawes, E.M., Hubbard, J.W. et al. (1987) The search for correlations between neuroleptic plasma levels and clinical outcome: a critical review. In: H.Y. Meltzer (Ed.), Psychopharmacology: The Third Generation of Progress. Raven, New York, pp. 1341-1351.
Overall, J.E. and Gotham, D.R. (1962) The Brief Psychiatric Rating Scale. Psychol. Rep. 10, 799-812.
Overall, J.E. and Gorham, D.R. (1988) The Brief Psychiatric Rating Scale (BPRS): Recent development in ascertainment and scaling. Psycho- pharmacol. Bull. 24, 97-99.
Phillipson, O.T., McKeown, J.M., Baker, J. and Healey, A.F. (1977) Correlation between plasma chlorpromazine and its metabolites and clinical ratings in patients with acute relapse of schizophrenic and paranoid psychosis. Br. J. Psychiatry 131, 172-184.
Rivera-Calimlim, L., Castaneda, L. and Lasagna, L. (1973) Effect of mode of management on plasma chlorpromazine in psychiatric pa- tients. Clin. Pharmacol. Ther. 14, 978-986.
Rivera-Calimlim, L., Nasrallah, H., Strass, J. and Lasagna, L. (1976) Clinical response and plasma levels: effect of dose, dosage schedule and drug interactions on plasma chlorpromaine levels, Am. J. Psychi- atry 133, 646-652.
Sakalis, G., Curry, S.H. and Mould, G.E (1972) Physiologic and clinical effects of chlorpromazine and their relationship to plasma level. Clin. Pharmacol. Ther. 13, 931-946.
Sakalis, G., Chan, T., Gershon, S. and Park, S. (1973) The possible role of metabolites in therapeutic response chlorpromazine treatment. Psychopharmacology 32, 277-284.
Sakalis, G., Chan, T.C., Sathanathan, G. et al. (1977) Relationships among clinical response, extrapyramidal syndrome and plasma chlor- promazine and metabolite ratios. Commun. Psychopharmacol. 1, 157- 166.
Sakurai, Y., Nakahara, T. and Takahashi, R. (1975) Prediction of response to CPZ treatment in schizophrenics. Psychopharmacology 44, 195- 203.
Traficante, L.J., Sakalis, G., Siekierski, J. et al. (1979) Rapid in vitro sulfoxidation of chlorpromazine by human blood: Inhibition by an endogenous plasma protein factor. Life Sci. 24, 337-346.