Embed Size (px)
Citation preview

RESPIRATORY SYSTEM

FUNCTIONAL ANATOMY OF
THE RESPIRATORY SYSTEM• Respiratory System:
– Pulmonary ventilation: movement of air into and out of the lungs so that gases there are continuously changed and refreshed (commonly called breathing)
– External respiration: movement of oxygen from the lungs to the blood and of carbon dioxide from the blood to the lungs
• Circulatory System:– Transport of respiratory gases:
• Transport of oxygen from the lungs to the tissue cells of the body• Transport of carbon dioxide from the tissue cells to the lungs• Accomplished by the cardiovascular system using blood as the
transporting fluid– Internal respiration: movement of oxygen from blood to the
tissue cells and of carbon dioxide from tissue cells to blood

FUNCTIONAL ANATOMY OF
THE RESPIRATORY SYSTEM
• Respiratory and circulatory systems are closely coupled, and if either system fails, the body’s cells begin to die from oxygen starvation
• Because it moves air, the respiratory system is also involved with the sense of smell and with speech

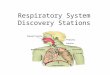
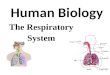
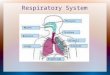
RESPIRATORY ORGANS
• The respiratory system includes:– Nose
– Nasal cavity
– Pharynx
– Larynx
– Trachea
– Bronchi
– Bronchioles
– Lungs
– Alveoli

RESPIRATORY SYSTEM
• Two Zones:– Conducting:
• Includes all the passageways that provide rigid conduits for air to reach the gas exchange locations
• Cleanses, humidifies, and warms incoming air
– Respiratory:• Actual site of gas exchange, is composed of the
respiratory bronchioles, alveolar ducts, and alveoli
• All microscopic structures

RESPIRATORY ORGANS

EXTERNAL NOSE

NOSE
• The nose is divided into the external nose, which is formed by hyaline cartilage and bones of the skull, and the nasal cavity, which is entirely within the skull

INTERNAL NASAL CAVITY• Divided by a midline nasal septum
– Anteriorly cartilage– Posteriorly vomer and ethmoid
bone• Continuous posteriorly with the nasal
portion of the pharynx through the posterior nasal apertures (internal nares)
• Roof of the nasal cavity is formed by the ethmoid and sphenoid bones of the skull
• Floor is formed by the palate, which separates the nasal cavity from the oral cavity
– Anterior: maxillary processes and palatine bone
– Posterior: muscular and soft

INTERNAL NASAL CAVITYVESTIBULE
• The part of the nasal cavity just superior to the nostrils
• Lined with skin containing sebaceous and sweat glands and numerous hair follicles
• Hairs (vibrissae) filter coarse particles (dust, pollen) from inspired air

INTERNAL NASAL CAVITYTWO TYPES OF MUCOSA
• Olfactory: – Lines the slitlike superior region– Contains smell receptors
• Respiratory:– Mucous glands: secrete mucus– Serous glands: secrete a watery
fluid containing enzymes– Epithelial cells: secrete defensins
(natural antibiotics that help get rid of invading microbes)
• The sticky mucus traps inspired dust, bacteria, and other debris, while lysozyme attacks and destroys bacteria chemically
• High water content of the mucus film acts to humidify the inhaled air

INTERNAL NASAL CAVITYRESPIRATORY MUCOSA
• Ciliated cells create a gentle current that moves the sheet of contaminated mucus posteriorly toward the throat, where it is swallowed and digested by stomach juices– Cold air causes them to
become sluggish• Mucus accumulates and
dribbles out the nostrils• Richly supplied with sensory
nerve endings:– Contact with irritating particles
triggers a sneeze reflex—forcing air outward in a violent burst

INTERNAL NASAL CAVITYRESPIRATORY MUCOSA
• Rich plexuses of capillaries and thin-walled veins underlie the nasal epithelium and warm incoming air as it flows across the mucosal surface

INTERNAL NASAL CAVITY
• Protruding medially from each lateral wall of the nasal cavity are three curved scroll-like mucosa-covered projections: increase the mucosal surface area exposed to the air and enhance air turbulence in the cavity – Superior conchae– Middle conchae– Inferior conchae
• Groove inferior to each concha is a meatus

THE NOSE AND
PARANASAL SINUSES
• The nose provides a resonance chamber for speech
• The nasal cavity is surrounded by paranasal sinuses within the frontal, maxillary, sphenoid, and ethmoid bones that serve to lighten the skull, warm and moisten air, and produce mucus which drains into the nasal cavity
– The suctioning effect created by nose blowing helps drain the sinuses

HOMEOSTATIC IMBALANCE
• Rhinitis: inflammation of the nasal mucosa accompanied by excessive mucus production, nasal congestion, and postnasal drip– Caused by cold viruses, streptococcal bacteria, and various
allergens• Sinusitis: inflamed sinuses
– Since the nasal mucosa is continuous with the sinuses infections can easily spread to the sinuses
• Sinus headache: when the passageways connecting the sinuses to the nasal cavity are blocked with mucus or infectious material, the air in the sinus cavities is absorbed resulting in a partial vacuum (localized over the inflamed areas)

THE PHARYNX
• The pharynx connects the nasal cavity and mouth superiorly to the larynx and esophagus inferiorly
• Commonly called the throat
• Muscular pharynx is composed of skeletal muscle

Nasopharynx
• Serves as only an air passageway
• During swallowing, the soft palate and its pendulous (hanging loosely) uvula move superiorly, an action that closes off the nasopharynx and prevents food from entering the nasal cavity
• Contains the pharyngeal tonsil (adenoids), which traps and destroys airborne pathogens

HOMEOSTATIC IMBALANCE
• Infected and swollen adenoids (pharyngeal tonsils) block air passage in the nasopharynx, making it necessary to breathe through the mouth– Air is not properly
moistened, warmed, or filtered before reaching the lungs

HOMEOSTATIC IMBALANCE
• The pharyngotympanic (auditory) tubes, which drain the middle ear cavities and allow ear pressure to equalize with atmospheric pressure, open into the lateral walls of the nasopharynx
• A ridge of pharyngeal mucosa, referred to as a tubal tonsil, arches over each of these openings– Help protect the middle ear
against infections likely to spread from the nasopharynx
– The pharyngeal tonsil also plays this protective role

NASOPHARYNX

OROPHARYNX
• Is an air and food passageway that extends inferiorly from the level of the soft palate to the epiglottis
– Air and food mix– Both swallowed food and inhaled
air pass through• Epithelium is adapted for increased
frictional and greater chemical trauma accompanying food passage
• Two kinds of tonsils lie embedded in the mucosa:
– Paired palatine tonsils lie in the lateral walls
– Lingual tonsil covers the base of the tongue

LARYNGOPHARYNX
• Is an air and food passageway that lies directly posterior to the epiglottis, extends to the larynx, and is continuous inferiorly with the esophagus
• The esophagus conducts food and fluids to the stomach
• Air enters the larynx anteriorly• During swallowing, food has
the “right of way”, and air passage temporarily stops


MIDSAGITAL SECTION OF THE HEAD AND NECK

UPPER RESPIRATORY TRACT

THE LARYNXBASIC ANATOMY
• The larynx (or voice box) attaches superiorly to the hyoid bone, opening into the laryngopharynx, and attaches inferiorly to the trachea– From 4th to 6th vertebra
• Three functions:– Provide an open airway– Switching mechanism to route
air and food into the proper channels
– Because it houses the vocal cords. The 3rd function is voice production

THE LARYNX
• The larynx consists of hyaline cartilages:– Thyroid:shield-shaped
• Midline laryngeal prominence (Adam’s Apple)
– Cricoid: ring shaped– Paired arytenoid,
corniculate, and cuneiform– Epiglottis, which is elastic
cartilage• Covered by mucosa-
containing taste buds

LARYNX

POSTERIOR ASPECT OF LARYNX

CARTILAGINOUS FRAMEWORK OF LARYNX
• During swallowing, the larynx is pulled superiorly and the epiglottis tips to cover the laryngeal inlet

VOCAL CORDS
• Vocal ligaments attach the arytenoid cartilages to the thyroid cartilage– These ligaments composed
largely of elastic fibers form the core of mucosal folds, called the vocal folds (true vocal cords)
• Which vibrate as air passes over them to produce sound
• Superior to the vocal cords are the false vocal cords– No part in sound production
but help to close the glottis when we swallow

VOCAL CORDS

VOCAL CORDS
• Below the vocal folds the epithelium is a pseudostratified ciliated columnar type that acts as a dust filter
• The power stroke of its cilia is directed upward toward the pharynx so that mucus is continually moved away from the lungs
• We help to move mucus up and out of the larynx when we “clear our throats”

VOICE PRODUCTION• Voice production involves the
intermittent release of expired air and the opening and closing of the glottis
• The length of the true vocal cords and the size of the glottis change with the action of the intrinsic laryngeal muscles that clothe the cartilage
• As the length and tension of the cords change, the pitch (depends on the frequency and loudness: height of wave) of the sound varies
– The tenser the cords, the faster they vibrate and the higher the pitch
• (b) the glottis is wide when we produce deep tones and narrows to a slit for high-pitched sounds
– Male larynx enlarges during puberty• Vocal cords become longer and thicker
causing them to vibrate slower (voice becomes deeper)

VOICE PRODUCTION
• Loudness of the voice depends on the force with which the airstream rushes across the vocal cords:– The greater the force, the stronger the vibration and the louder the sound– The power source for creating the airstream is the muscles of the chest,
abdomen, and back• Vocal folds actually produce buzzing sounds
– The perceived quality of the voice depends on the coordinated activity of many structures above the glottis
• The entire length of the pharynx acts as a resonating chamber, to amplify and enhance the sound quality
• Oral, nasal, and sinus cavities also contribute to vocal resonance• Good enunciation depends on the shaping of sound into
recognizable consonants and vowels by muscles in the pharynx, tongue, soft palate, and lips

HOMEOSTATIC IMBALANCE
• Laryngitis– Inflammation of the vocal folds– Vocal folds swell, interfering with their
vibrations– Produces a change in the voice tone,
hoarseness, or in severe cases inability to speak above a whisper

THE LARYNX
• The vocal folds and the medial space between them are called the glottis
• Under certain conditions, the vocal folds act as a sphincter that prevents air passage– Valsalva’s maneuver is a behavior in which the glottis
closes to prevent exhalation and the abdominal muscles contract, causing intra-abdominal pressure to rise
• Defecation: helps empty the rectum and can also stabilize the body trunk when one lifts a heavy load


THE TRACHEA
• The trachea, or windpipe, descends from the larynx through the neck into the mediastinum, where it terminates by dividing into the two primary bronchi at midthorax
• Cilia continually propel debris-laden mucus toward the pharynx

Cross-sectional view of the trachea, illustrating its relationship to the
esophagus and the position of the supporting cartilage rings

TRACHEA
• 16-20 C-shaped cartilage rings:– Prevents the trachea
from collapsing despite the pressure changes in breathing

HOMEOSTATIC IMBALANCE
• Smoking inhibits and ultimately destroys cilia, after which coughing is the only means of preventing mucus from accumulating in the lungs– For this reason, smokers with respiratory
congestion should avoid medications that inhibit the cough reflex

HOMEOSTATIC IMBALANCE
• Tracheal obstruction is life threatening
• Heimlich maneuver, a procedure in which air in the victim’s lungs is used to “pop out”, or expel, an obstructing piece of food– Cracked ribs are a distinct possibility when
done incorrectly

BRONCHIAL TREEBRONCHI and SUBDIVISIONS
• Site where conducting zone structures give way to respiratory zone structures

THE BRONCHIAL TREE
• The conducting zone consists of right and left primary bronchi that enter each lung and diverge into secondary bronchi that serve each lobe of the lungs
• The right primary bronchus is wider, shorter, and more vertical than the left and is the more common site for an inhaled foreign object to become lodged
• By the time incoming air reaches the bronchi, it is warm, cleansed of most impurities, and saturated with water vapor

Conducting Zone Structures
• Once inside the lungs, each primary bronchus subdivides into secondary (lobar) bronchi—three on the right and two on the left—each supplying one lung lobe
• Secondary bronchi branch into several orders of smaller tertiary bronchi, which ultimately branch into bronchioles– Cilia are sparse, and mucus-producing cells are absent in the
bronchioles• Thus, most airborne debris found at or below the level of the bronchioles
is removed by macrophages in the alveoli• Amount of smooth muscle in the walls increases as the passageways
become smaller– A complete layer of circular smooth muscle in the bronchioles and the
lack of supporting cartilage (which would hinder constriction) allows the bronchioles to provide substantial resistance to air passage under certain conditions

CONDUCTING RESPIRATORY PASSAGES

THE BRONCHIAL TREERESPIRATORY TREE
• The respiratory zone begins as the terminal bronchioles feed into respiratory bronchioles that terminate in alveolar ducts within clusters of alveolar sacs, which consist of alveoli
• Approximately 300 million gas-filled alveoli in the lungs account for most of the lung volume and provide a tremendous surface area for gas exchange

RESPIRATORY ZONE STRUCTURES

ALVEOLI
• Consists of a single layer of squamous epithelium, type-I cells, surrounded by a basal lamina:– The thinness of their walls
is hard to imagine, but a sheet of tissue paper is much thicker
• External surfaces of the alveoli are densely covered with pulmonary capillaries

RESPIRATORY MEMBRANE

THE RESPIRATORY MEMBRANE
• The alveolar and capillary walls and their fused basal laminae form the respiratory membrane, an air-blood barrier that has gas on one side and blood flowing past on the other

THE RESPIRATORY MEMBRANE
• Gas exchanges occur readily by simple diffusion across the respiratory membrane—O2 passes from the alveolus into the blood, and CO2 leaves the blood to enter the gas-filled alveolus
• The type I cells also are the primary source of angiotensin converting enzyme, which plays a role in blood pressure regulation

RESPIRATORY MEMBRANE

RESPIRATORY MEMBRANE
• Interspersed among the type-I cells are cuboidal type-II cells that secrete surfactant:– Reduces the surface
tension of the alveolar fluid

RESPIRATORY MEMBRANE
• Alveoli have 3 other significant features:– They are surrounded by
elastic fibers– They contain open alveolar
pores connecting adjacent alveoli allowing air pressure throughout the lung to be equalized and provide alternate air routes to any alveoli whose bronchi have collapsed
– They have remarkably efficient alveolar macrophages

RESPIRATORY MEMBRANE

THE LUNGS AND PLEURAEGROSS ANATOMY
• The lungs occupy all of the thoracic cavity except for the mediastinum; each lung is suspended within its own pleural cavity and connected to the mediastinum by vascular and bronchial attachments called the lung root
• Because the apex of the heart is slightly to the left of the median plane, the two lungs differ slightly in shape and size
• The left lung is smaller than the right, and the cardiac notch—a concavity in its medial aspect—is molded to and accommodates the heart

THORACIC CAVITY

THE LUNGS AND PLEURAEGROSS ANATOMY
• The left lung is subdivided into upper and lower lobes by the oblique fissure
• The right lung is partitioned into upper, middle, and lower lobes by then oblique and horizontal fissures

THE LUNGS AND PLEURAEGROSS ANATOMY
• Each lobe contains a number of pyramid-shaped bronchopulmonary segments (9-10) separated from one another by connective tissue septa

BRONCHIAL TREE

LOBULES
• Smallest subdivisions of the lung
• Appear at the lung surface as hexagons
• Each is served by a large bronchiole and its branches
• In most city dwellers and in smokers, the connective tissue that separates the individual lobules is blackened with carbon

THORACIC CAVITY

THE LUNGS AND PLEURAEGROSS ANATOMY
• Each lobe contains a number of bronchopulmonary segments, each served by its own artery, vein, and tertiary bronchus

LUNGSGROSS ANATOMY
• Lung tissue consists largely of air spaces, with the balance of lung tissue, its stroma, comprised mostly of elastic connective tissue
• Soft, spongy, elastic organs that together weigh just over 1 Kg (2.5 pounds)

Blood Supply and Innervation of the Lungs
• There are two circulations that serve the lungs:– Pulmonary
circulation– Bronchial
circulation

TRANSVERSE SECTION OF THORAX

Blood Supply and Innervation of the Lungs
• The pulmonary network:– Carries systemic venous
blood (pulmonary arteries) to the lungs for oxygenation
– Freshly oxygenated blood is conveyed from the respiratory zones of the lungs to the heart by pulmonary veins
– Large-volume, low pressure

Blood Supply and Innervation of the Lungs
• The bronchial arteries provide systemic blood to the lung tissue:– Arise form the aorta– Run along the branching bronchi, supplying all lung tissues except
the alveoli (these are supplied by the pulmonary circulation)– Small-volume, high pressure
• Although some systemic venous blood is drained from the lungs by the tiny bronchial veins, there are multiple anastomoses between the two circulations, and most venous blood returns to the heart via the pulmonary veins

Blood Supply and Innervation of the Lungs
• The lungs are innervated by parasympathetic and sympathetic motor fibers, and visceral sensory fibers
• These nerve fibers enter each lung through the pulmonary plexus on the lung root and run along the bronchial tubes and blood vessels in the lungs
• Parasympathetic fibers constrict the air tubes• Sympathetic fibers dilate the airways

PLEURAE
• Thin, double-layered serosa• Parietal pleura covers the
thoracic wall, superior face of the diaphragm, and continues around the heart between the lungs, forming the lateral walls of the mediastinal enclosure and snugly encloses the lung root
• Visceral pleura covers the external lung surface, following its contours and fissures

PLEURAE

PLEURAE
• Produces pleural fluid, which fills the slitlike pleural cavity between the parietal and visceral pleurae
• Lubricating secretion allows the lungs to glide easily over the thorax wall during our breathing movements

HOMEOSTATIC IMBALANCE
• Pleurisy: inflammation of the pleurae– Often results from pneumonia– Less pleural fluid
• Pleural surfaces become dry and rough, resulting in friction and stabbing pain with each breath
– Conversely, excessive fluid might be produced• Exerts pressure on the lungs• Hinders breathing movements, but is much less painful than
the dry rubbing type
• Pleural effusion:– Blood fluid accumulation

MECHANICS OF BREATHING
• Breathing (pulmonary ventilation) consists of two phases:– Inspiration: period when air flows into the
lungs– Expiration: period when gases exit the lungs

Pressure Relationship in the Thoracic Cavity
• Respiratory pressures are always described relative to atmospheric pressure (Patm), which is the pressure exerted by the air (gases) surrounding the body– At sea level: 760mm Hg (pressure exerted by a column of
mercury 760mm high)• Can also be expressed in atmosphere units: 760mm Hg = 1
atm– A negative respiratory pressure, such as -4mm, indicates
that the pressure in that area is lower than atmospheric pressure
» 760-4= 756mm Hg– A positive respiratory pressure is higher than atmospheric
pressure– Zero respiratory pressure is equal to atmospheric pressure

Intrapulmonary Pressure (P pul)
• Is the pressure in the alveoli, which rises and falls during respiration, but always eventually equalizes with atmospheric pressure

Intrapleural Pressure (P ip)
• Is the pressure in the pleural cavity– It also rises and falls during respiration, but is always
about 4 mm Hg less than intrapulmonary pressure
• The pressure in the pleural cavity, the intrapleural pressure (Pip), also fluctuates with breathing phases
• It is always about 4 mm Hg less than Ppul
• Hence, Pip is negative relative to both the intrapulmonary and atmospheric pressures

Intrapleural Pressure (P ip)
• How is this negative pressure established and maintained?– There are opposing forces acting– Forces act to pull the lungs (visceral pleura) away from the thorax
wall (parietal pleura) and cause lung collapse:• The lungs’ natural tendency to recoil
– Always assumes the smallest size possible
• The surface tension of the alveolar fluid– Constantly acts to draw the alveoli to their smallest possible
dimension
– These lung-collapsing forces are opposed by the natural elasticity of the chest wall, a force that tends to pull thorax outward and to enlarge the lungs

Intrapleural Pressure (P ip)
• WHO WINS????– Neither in a healthy person, because of the strong
adhesive force (attraction between unlike molecules) between the parietal and visceral pleura
• Pleural fluid secures the pleurae together in the same way a drop of water holds two glass slides together
• The pleurae slide from side to side easily, but they remain closely apposed, and separating them requires extreme force
• Net result of the dynamic interplay between these forces is a negative Pip

Intrapleural Pressure (P ip)
• The importance of negative pressure in the intrapleural space and the tight coupling of the lungs to the thorax wall cannot be overemphasized– Any condition that equalizes Pip with the
intrapulmonary (or atmospheric) pressure causes immediate lung collapse
– It is the transpulmonary pressure—the difference between the intrapulmonary and intrapleural pressures ( Ppul – Pip ) –that keeps the air spaces of the lungs open (keeps them from collapsing)

INTRAPULMONARY and INTRAPLEURAL PRESSURE RELATIONSHIPS

HOMEOSTATIC IMBALANCE
• Atelectasis: lung collapse – Commonly occurs when air enters the pleural cavity through a
chest wound, but it may result from a rupture of the visceral pleura, which allows air to enter the pleural cavity from the respiratory tract
– Common sequel to pneumonia• Pneumothorax: presence of air in the intrapleural space
– Reversed by closing the “hole” and drawing air out of the intrapleural space with chest tubes, which allow the lung to reinflate and resume its normal function
• Because the lungs are in separate cavities, one lung can collapse without interfering with the function of the other

Pulmonary Ventilation: Inspiration and Expiration
• Pulmonary ventilation is a mechanical process causing gas to flow into and out of the lungs according to volume changes in the thoracic cavity
• Volume changes lead to pressure changes—pressure changes lead to the flow of gases to equalize the pressure
• Boyle’s law states that at a constant temperature, the pressure of a gas varies inversely with its volume: P1V1 = P2V2
– Where P is the pressure of the gas in millimeters of mercury, V is its volume in cubic millimeters, and subscripts 1 and 2 represent the initial and resulting conditions respectively

INSPIRATION
• Gases always fill their container• During quiet inspiration, the diaphragm and
intercostals contract, resulting in an increase in thoracic volume, which causes intrapulmonary pressure to drop below atmospheric pressure, and air flows into the lungs
• Ppul drops about 1mm Hg relative to Patm– Anytime the intrapulmonary pressure is less than the atmospheric
pressure (Ppul < Patm, air rushes into the lungs along the pressure gradient
– Inspiration ends when Ppul = Patm
– During the same period Pip declines to about -6 mm Hg relative to Patm

Changes in thoracic cavity during Inspiration and Expiration

INSPIRATION
• During forced inspiration, accessory muscles of the neck and thorax contract, increasing thoracic volume beyond the increase in volume during quiet inspiration

EXPIRATION
• Quiet expiration is a passive process that relies mostly on elastic recoil of the lungs as the thoracic muscles relax– As the inspiratory muscles relax and resume their resting length,
the rib cage descends and the lungs recoil• Thus, both the thoracic and intrapulmonary volume decreases
compressing the alveoli• Ppul rises to about 1 mm Hg above atmospheric pressure• Ppul > Patm, the pressure gradient forces gases to flow out of the lungs
• Forced expiration is an active process relying on contraction of abdominal muscles to increase intra-abdominal pressure and depress the ribcage

Changes in thoracic cavity during Inspiration and Expiration

Changes in Intrapulmonary and Intrapleural Pressures during Inspiration and Expiration
Notice that normal atmospheric pressure (760mmHg) is given a value of 0 on the scale

Physical Factors Influencing Pulmonary Ventilation
• Lungs are stretched during inspiration and recoil passively during expiration
• Inspiratory muscles consume energy to enlarge the thorax
• Energy is also used to overcome various factors that hinder air passage and pulmonary ventilation:– Airway resistance– Alveolar surface tension forces– Lung compliance (elasticity)

Airway Resistance
• Major nonelastic source of resistance to gas flow is friction, or drag, encountered by air in the airways
• Gas flow is reduced as airway resistance increases• The relationship between gas flow (F), pressure (P),
and resistance (R) is given by the following equation:– F = ∆P/R
• The amount of gas flowing into and out of the alveoli is directly proportional to ∆P, the difference in pressure, or the pressure gradient, between the external atmosphere and the alveoli

Airway Resistance
• Gas flow changes inversely with resistance– Gas flow decreases as resistance due to friction
increases:• As with the cardiovascular system, resistance in the respiratory
tree is determined mostly by the diameters of the conducting tubes
• However, as a rule, airway resistance is insignificant for two reasons:
– 1. Airway diameters in the first part of the conducting zone are huge
– 2. Gas flow stops at the terminal bronchioles ( where small airway diameters might start to be a problem) and diffusion takes over as the main force driving gas movement

Airway Resistance
• Airway resistance peaks in the medium-sized bronchi and then declines sharply as the total cross-sectional area of the airway increases rapidly

Resistance of the various segments of the Respiratory Passageways

HOMEOSTATIC IMBALANCE
• Inhaled irritants and inflammatory chemicals (histamine, bronchoconstrictors) activate a reflex of the parasympathetic division of the nervous system causing vigorous constriction of the bronchioles and dramatically reduce air passageways– Example: acute asthma attack can stop pulmonary ventilation
almost completely, regardless of the pressure gradient• Conversely, epinephrine released during sympathetic
nervous system activation or administered as a drug dilates bronchioles and reduces airway resistance
• Local accumulations of mucus, infectious material, or solid tumors in the passageways are important sources of airway resistance in those with respiratory disease

Alveolar Surface Tension Forces
• Alveolar surface tension due to water in the alveoli acts to draw the walls of the alveoli together, presenting a force that must be overcome in order to expand the lungs
• At any gas-liquid boundary, the molecules of the liquid are more strongly attracted to each other than to the gas molecules
– This unequal attraction produces a state of tension at the liquid surface, called surface tension
• Draws the liquid molecules closer together and reduces their contact with the dissimilar gas molecules
• Resists any force that tends to increase the surface area of the liquid

Alveolar Surface Tension Forces
• Water is composed of highly polar molecules and has a very high surface tension
• Because water is the major component of the liquid film that coats the alveolar walls, it is always acting to reduce the alveoli to their smallest possible size– If the film was pure water, the alveoli would collapse between breaths– But the alveolar film contains surfactants, a detergent-like complex of
lipids and proteins produced by the type II alveolar cells• Surfactant decreases the cohesiveness of water molecules, much the
way a laundry detergent reduces the attraction of water for water, allowing water to interact with and pass through fabric
• As a result, the surface tension of alveolar fluid is reduced, and less energy is needed to overcome those forces to expand the lungs and discourage alveolar collapse

HOMEOSTATIC IMBALANCE
• Infant respiratory Distress Syndrome (IRDS)– Condition peculiar to premature babies– Since inadequate pulmonary surfactant is produced
until the last two months of fetal development, babies born prematurely often are unable to keep their alveoli inflated between breaths
• Treated by:– Positive-pressure respirators that force air into the alveoli ,
keeping them open between breaths» Bronchopulmonary dysplasia: damage to delicate lungs by
use of respiators– Spraying natural or synthetic surfactant into the newborn’s
respiratory passageways also helps

Lung Compliance
• Healthy lungs are unbelievably stretchy, and this distensibility (swell, expand) is referred to as lung compliance
• Lung compliance (CL) is a measure of the change in lung volume (∆VL) that occurs with a given change in the transpulmonary pressure [∆(Ppul-Pip)]
– CL = ∆VL / ∆(Ppul – Pip)

Lung Compliance
• Lung compliance is determined by:– Distensibility of lung tissue and the surrounding
thoracic cage
– Alveolar surface tension
• Because lung (and thoracic) distensibility is generally high and alveolar surface tension is kept low by surfactant, the lungs of healthy people tend to have high compliance, which favors efficient ventilation

Lung Compliance
• Compliance is diminished by factors with any of the following effects:– 1.Reduce the natural resilience of the lungs as fibrosis
• E.g., development of nonelastic scar tissue in tuberculosis– 2.Block the smaller respiratory passages
• E.g., with fluid (pneumonia) or mucus (chronic bronchitis)– 3.Reduce the production of surfactant– 4.Decrease the flexibility of the thoracic cage or its
ability to expand• The lower the lung compliance, the more
energy is needed just to breathe

HOMEOSTATIC IMBALANCE
• Deformities of the thorax, ossification of the costal cartilages (common during old age), and paralysis of the intercostal muscles all reduce lung compliance by hindering thoracic expansion

Respiratory Volumes and Pulmonary Function Tests
• Respiratory volumes and specific combinations of volume, called respiratory capabilities, are used to gain information about a person’s respiratory status
• The four respiratory volumes of interest are: tidal, inspiratory, expiratory reserve, and residual

Respiratory Volumes and Capacity
• The values recorded represent normal values for a healthy 20 year old male weighing about 70 Kg (155 pounds)

Respiratory Volumes and Capacities

Tidal Volume
• Tidal volume is the amount of air that moves in and out of the lungs with each breath during normal
• About 500 ml of air (quiet breathing)

Inspiratory Reserve Volume (IRV)
• The inspiratory reserve volume is the amount of air that can be forcibly inspired beyond the tidal volume
• 2100 to 3200 ml of air

Expiratory Reserve Volume (ERV)
• The expiratory reserve volume is the amount of air that can be evacuated from the lungs after tidal expiration
• Normally 1,000 to 1,200 ml of air

Residual Volume (RV)
• Residual volume is the amount of air that remains in the lungs after maximal forced expiration
• About 1,200 ml of air remains in the lungs
• Helps to keep the alveoli open and to prevent lung collapse

Respiratory Volumes and Capacity

Respiratory Capacities
• Include inspiratory capacity, functional residual capacity, vital capacity, and total lung capacity
• Respiratory capacities always consist of two or more lung volumes

Respiratory Volumes and Capacities

Inspiratory Capacity (IC)• Inspiratory capacity is the sum of tidal volume
and inspiratory reserve volume, and represents the total amount of air that can be inspired after a tidal expiration
• Sum of TV and IRV

Functional Residual Capacity (FRC)
• Functional residual capacity is the combined residual volume and expiratory reserve volume, and represents the amount of air that remains in the lungs after a tidal expiration
• Sum of RV and ERV

Vital Capacity (VC)
• Vital capacity is the sum of tidal volume, inspiratory reserve and expiratory reserve volumes, and is the total amount of exchangeable air
• Sum of TV,IRV, and ERV
• In healthy young males approximately 4800 ml

Total Lung Capacity (TLC)
• Total lung capacity is the sum of all lung volumes
• Normally around 6000 ml in males

Respiratory Volumes and Capacities

Dead Space
• Some of the inspired air fills the conducting respiratory passageways and never contributes to gas exchange in the alveoli
• The volume of these conducting zone conduits, which make up the anatomical dead space, typically amounts to about 150 ml– 1 ml per pound of body weight
• In a healthy young adult of 150 pounds– TV is 500 ml, only 350 ml is involved in alveolar ventilation– The remaining 150 ml of tidal breath is in the anatomical dead
space– The anatomical dead space is the volume of the conducting
zone conduits, which is a volume that never contributes to gas exchange in the lungs

Respiratory Volumes and Pulmonary Function Tests
• The measuring device, a spirometer, is a simple instrument utilizing a hollow bell inverted over water– The bell moves as the patient breathes into a connecting
mouthpiece, and a graphic recording is made on a rotating drum– Cannot provide a specific diagnosis, it can distinguish between
obstructive pulmonary disease involving increased airway resistance (chronic bronchitis) and restrictive disorders involving a reduction in total lung capacity resulting from structural or functional changes in the lungs (tuberculosis, fibrosis due to exposure to certain environmental agents such as asbestos)
– Pulmonary function tests evaluate losses in respiratory function using a spirometer to distinguish between obstructive and restrictive pulmonary disorders

Respiratory Volumes and Pulmonary Function Tests
• More information can be obtained about a patient’s ventilation status by assessing the rate at which gas moves into and out of the lungs– Minute Ventilation: total amount of gas that flows into or out of the
respiratory tract in 1 minute• Normal quiet breathing: 6L/min (500 ml per breath multiplied by 12
breaths per minute)• Vigorous exercise: 200L/min
– Alveolar Ventilation Rate (AVR): better index of effective ventilation• Takes into account the volume of air wasted in the dead space and
measures the flow of fresh gases in and out of the alveoli during a particular time interval
– AVR (ml/min) = frequency (breaths/min) X (TV – dead space) (ml/breath)
– In a healthy person:» AVR = 12 breaths/minute X (500-150 ml/breath)» AVR = 4200 ml/min

Nonrespiratory Air Movements
• Cause movement of air into or out of the lungs, but are not related to breathing: (coughing, sneezing, crying, laughing, hiccups, and yawning)
• Most result from reflex activity, but some are produced voluntarily

BASIC PROPERTIES OF GASESDALTON’S LAW
• Dalton’s law of partial pressure states that the total pressure exerted by a mixture of gases is the sum of the pressures exerted independently by each gas in the mixture– PN2
is 78.6% X 760 mm Hg = 597 mm Hg
– PO2 is 20.9 % X 760 mm Hg = 159 mm Hg
• At higher altitudes, pressure decreases (each partial pressure decreases proportionally to the values at sea level)
• Below sea level (under water), pressure increases– Pressure increases 1 atm (760 mm Hg) for each 33 feet of descent
• Thus at 99 feet below sea level, the total pressure is 4 atm ( 3040 mm Hg) (partial pressure for each gas is also quadrupled)

BASIC PROPERTIES OF GASESHENRY’S LAW
• Henry’s law states that when a mixture of gases is in contact with a liquid, each gas will dissolve in the liquid in proportion to its partial pressure
• How much of a gas will dissolve in a liquid at any given partial pressure also depends on the solubility of the gas in the liquid and on the temperature of the liquid– Carbon dioxide is most soluble– Oxygen is only 1/20 as soluble as CO2
– Nitrogen is practically insoluble
• The effect of increasing the liquid’s temperature is to decrease gas solubility

BASIC PROPERTIES OF GASESHENRY’S LAW
• Hyperbaric oxygen chambers: provide clinical applications of Henry’s Law– Chambers contain O2 at pressures higher than 1
atm and are used to force greater-than-normal amounts of O2 into the blood of patients suffering from carbon monoxide poisoning, circulatory shock, gas gangrene, tetanus poisoning from anaerobic bacteria, or asphyxiation (lack of O2 or excess CO2)

HOMEOSTATIC IMBALANCE
• Although breathing O2 gas at 2 atm is not a problem for short periods, oxygen toxicity develops rapidly when PO2
is greater than 2.5-
3 atm
• Excessively high O2 concentrations generate huge amounts of harmful free radicals, resulting in profound CNS disturbances, coma, and death

COMPOSITION OF ALVEOLAR GAS
• The gaseous makeup of the atmosphere is quite different from that in the alveoli– The atmosphere is almost entirely O2 and N2
– The alveoli contain more CO2 and water vapor and much less O2
• The relative proportions of gases in the alveoli reflect gas exchange occurring in the lungs, humidification of air by conducting passages, and mixing of alveolar gas that occurs with each breath

External RespirationPulmonary Gas Exchange
• Three factors influencing the movement of oxygen and carbon dioxide across the respiratory membrane are:– 1. Partial pressure gradients and gas solubilities
– 2.Matching of alveolar ventilation and pulmonary blood perfusion
– 3.Structural characteristics of the respiratory membrane
• External respiration involves O2 uptake and CO2 unloading from hemoglobin in red blood cells

External RespirationPartial Pressure Gradients and Gas Solubilities
• Because the PO2 of venous
blood in the pulmonary arteries is only 40 mm Hg, as opposed to a PO2
of
approximately 104 mm Hg in the alveoli, a steep oxygen partial pressure gradient exists, and O2 diffuses rapidly from the alveoli into the pulmonary capillary blood

Partial Pressure Gradients Promoting Gas Movements In The Body

External RespirationPartial Pressure Gradients and Gas Solubilities
• Equilibrium—that is, a PO2
of 104 mm Hg on both sides of the respiratory membrane—usually occurs in 0.25 second, which is about 1/3 the time a red blood cell is in a pulmonary capillary
• Blood can flow through the pulmonary capillaries 3x as quickly and still be adequately oxygenated

Oxygenation of Blood in the Pulmonary Capillaries

External RespirationPartial Pressure Gradients and Gas Solubilities
• Carbon dioxide moves in the opposite direction along a much gentler partial pressure gradient of about 5 mm Hg ( 45 mm Hg to 40 mm Hg) until equilibrium occurs at 40 mm Hg
• Carbon dioxide is then expelled gradually from the alveoli during expiration
• Even though the O2 pressure gradient for oxygen diffusion is much steeper than the CO2 gradient, equal amounts of these gases are exchanged because CO2 is 20 times more soluble in plasma and alveolar fluid than O2

External RespirationPartial Pressure Gradients and Gas Solubilities
• The difference in the degree of the partial pressure gradients of oxygen and carbon dioxide reflects he fact that carbon dioxide is much more soluble than oxygen in the blood
• A steep partial pressure gradient exists between blood in the pulmonary arteries and alveoli, and O2 diffuses rapidly from the alveoli into the blood, but carbon dioxide moves in the opposite direction along a partial pressure gradient that is much less steep

External RespirationVentilation-Perfusion Coupling
• For gas exchange to be efficient, there must be a close match, or coupling, between ventilation (the amount of gas reaching the alveoli) and perfusion (the blood flow in pulmonary capillaries
• Ventilation-perfusion coupling ensures a close match between the amount of gas reaching the alveoli and the blood flow in the pulmonary capillaries

External RespirationVentilation-Perfusion Coupling
• In alveoli where ventilation is inadequate, PO2
is low:– The terminal arterioles
constrict, and blood is redirected to respiratory areas where PO2
is high and oxygen pickup may be more efficient
– In alveoli where ventilation is maximal, pulmonary arterioles dilate, increasing blood flow into the associated pulmonary capillaries

VENTILATION-PERFUSION COUPLING

External RespirationVentilation-Perfusion Coupling
• While changes in alveolar PO2
affect the diameter of pulmonary blood vessels (arterioles), changes in alveolar PCO2
cause changes in the diameters of the bronchioles
– Passageways servicing areas where alveolar CO2 levels are high dilate, allowing CO2 to be eliminated from the body more rapidly, while those serving areas where PCO2
is low constrict
• As a result of modifications made by these two systems, alveolar ventilation and pulmonary perfusion are synchronized

VENTILATION-PERFUSION COUPLING

Partial Pressure Gradients Promoting Gas Movements In The Body

External RespirationThickness and Surface Area of the Respiratory Membrane
• The respiratory membrane is normally very thin (0.5 to 1 um), and presents a huge surface area for efficient gas exchange

HOMEOSTATIC IMBALANCE
• If the lungs become waterlogged and edematous (excess amount of fluid) as in pneumonia:– The exchange membrane thickens dramatically– Under such conditions, even the total time (0.75
s) that red blood cells are in transit through the pulmonary capillaries may not be enough for adequate gas exchange, and body tissues begin to suffer from oxygen deprivation

HOMEOSTATIC IMBALANCE
• In certain pulmonary diseases, the alveolar surface area actually functioning in gas exchange is drastically reduced:– Emphysema
• The walls of adjacent alveoli break through and the alveolar chambers become larger with a loss in elasticity
– Tumors, mucus, or inflammatory material blocks gas flow into the alveoli

Internal Respiration: Capillary Gas Exchange in the Body Tissues
– The diffusion gradients for oxygen and carbon dioxide are reversed from those for external respiration and pulmonary gas exchange
– The partial pressure of oxygen in the tissues is always lower than the blood, so oxygen diffuses readily into the tissues, while a similar but less dramatic gradient exists in the reverse direction for carbon dioxide
– Gas exchange that occur between the blood and the alveoli and between the blood and the tissue cells take place by simple diffusion driven by the partial pressure gradients of O2 and CO2 that exist on the opposite sides of the exchange membranes

Partial Pressure Gradients Promoting Gas Movements In The Body

TRANSPORT OF RESPIRATORY GASES BY BLOOD
• Oxygen Transport:– Since molecular oxygen is poorly soluble in the blood,
only 1.5 % is dissolved in plasma, while the remaining 98.5% must be carried on hemoglobin
• Up to four oxygen molecules can be reversibly bound to a molecule of hemoglobin– one oxygen on each iron
• The affinity of hemoglobin for oxygen changes with each successive oxygen that is bound or released, making oxygen loading and unloading very efficient

GAS EXCHANGES AT THE BODY TISSUES

GAS EXCHANGES IN THE LUNGS

Association of Oxygen and Hemoglobin
• The hemoglobin-oxygen combination, called oxyhemoglobin, is written HbO2
• Hemoglobin that has released oxygen is called reduced hemoglobin, or deoxyhemoglobin (HHb)
» Lungs
• HHb + O2 ↔ HbO2 + H+
» Tissues

Influence of PO2 on Hemoglobin Saturation
• The relationship between the degree of hemoglobin saturation and the PO2
of blood is not linear
• This S-shaped curve has a steep slope between 10 and 50 mm Hg PO2
and then flattens out between 70 and 100 mm Hg
• Remember, PO2 measurement
indicates only the amount of O2 dissolved in plasma, not the amount bound to hemoglobin

OXYGEN-HEMOGLOBIN DISSOCIATION CURVE

Influence of PO2 on Hemoglobin Saturation
• A hemoglobin saturation curve reveals important facts:– Hb is almost completely saturated at a PO2
of 70 mm Hg, and further increases in PO2
produce only small increases in O2 binding– The adaptive value of this is that O2 loading and delivery to the
tissues can still be adequate when the PO2 of inspired air is well
below its usual levels, a situation common at higher altitudes and in those with cardiopulmonary disease
– Most O2 unloading occurs on the steep portion of the curve, where the partial pressure changes very little, only 20-25% of bound oxygen is unloaded during one systemic circuit, and substantial amounts of O2 are still available in venous blood (venous reserve)
• Thus, if O2 drops to very low in the tissues, as might occur during vigorous exercise, much more O2 can dissociate from hemoglobin to be used by the tissue cells without any increase in respiratory rate or cardiac output

OXYGEN-HEMOGLOBIN DISSOCIATION CURVE

Influence of Other Factors on Hemoglobin Saturation
• The rate at which Hb reversibly binds or releases O2 is regulated by PO2
, temperature, blood pH, PCO2, and blood
concentration of an organic chemical called BPG (2,3-bisphosphoglycerate)– BPG is produced by red blood cells (RBCs) as they break
down glucose by the anaerobic process called glycolysis– These factors interact to ensure adequate deliveries of O2
to tissue cells– All these factors influence Hb saturation by modifying its
three-dimensional structure, and thereby its affinity for O2

Influence of Other Factors on Hemoglobin Saturation
• Increase in temperature, PCO2
, H+ content of the
blood, or BPG levels in blood decreases Hb’s affinity for O2 and causes the oxygen-hemoglobin dissociation curve to shift to the right
• This enhances oxygen unloading from the blood

Effects of Temperature, PCO2, and Blood pH on the Oxygen-Hemoglobin Dissociation Curve

Influence of Other Factors on Hemoglobin Saturation
• A decrease in in temperature, PCO2
, H+
content of the blood, or BPG levels in blood increases hemoglobin’s affinity for oxygen and shifts the dissociation curve to the left

Effects of Temperature, PCO2, and Blood pH on the Oxygen-Hemoglobin Dissociation Curve

The Hemoglobin-Nitric Oxide Partnership in Gas Exchange
• Nitric oxide (NO), secreted by lung and vascular endothelial cells, is a well-known vasodilator that plays an important role in blood pressure regulation
• Hemoglobin, on the other hand, has a formidable reputation as a vasoconstrictor because it is a NO scavenger—its iron-containing heme group destroys NO– Yet, there is a PARADOX: local vessels dilate where gases are
being unloaded and loaded:• It appears that as O2 is unloaded so is NO, which dilates the
local vessels and aid oxygen delivery• Then as deoxygenated hemoglobin picks up CO2, it also picks
up any circulating NO in the area and carries these gases to the lungs where they are unloaded

Effects of Temperature, PCO2, and Blood pH on the Oxygen-Hemoglobin Dissociation Curve

HOMEOSTATIC IMBALANCE
• Hypoxia: any conditions in which there is inadequate oxygen delivery to body tissues
• Anemic hypoxia: reflects poor O2 delivery resulting from too few RBCs or from RBCs that contain abnormal or too little Hb
• Ischemic (stagnant) hypoxia: results when blood circulation is impaired or blocked– Congestive heart (pumping efficiency depressed) circulation may
cause body-wide ischemic hypoxia– Emboli (mass of undissolved matter transmitted in the blood to a
location) or thrombi (blood clot that obstructs a vessel) block oxygen delivery only to tissues distal to the obstruction

HOMEOSTATIC IMBALANCE
• Histotoxic hypoxia: occurs when body cells are unable to use O2 even though adequate amounts are delivered– Consequence of metabolic poisons, such as cyanide
• Hypoxemic hypoxia: indicated by reduced arterial PO2– Possible causes include imbalances in the ventilation-
perfusion coupling mechanism– Pulmonary diseases that impair ventilation– Breathing air that containing scant (barely sufficient)
amounts of Oxygen

HOMEOSTATIC IMBALANCE
• Carbon Monoxide Poisoning: unique type of hypoxemic hypoxia:– Leading cause of death from fire– CO is an odorless, colorless gas that competes
vigorously with O2 for heme binding sites• Affinity for CO is more than 200 times greater than
its affinity for oxygen

Carbon Dioxide Transport• Blood transports CO2 from
the tissue cells to the lungs in three forms:
• 1. Dissolve in plasma (7-10%): dissolved in plasma
• 2. Chemically bound to hemoglobin (20%): carried as carbaminohemoglobin– CO2 + Hb ↔ HBCO2
(carbaminohemoglobin)• Does not require an enzyme• CO2 binds directly to the
amino acids of globin (not to the heme)
– Does not compete with the oxyhemoglobin (or NO) transport mechanism

GAS EXCHANGES AT THE BODY TISSUES

GAS EXCHANGES IN THE LUNGS

Carbon Dioxide Transport• 3. As bicarbonate ion in
plasma (70%): – Most carbon dioxide molecules
entering the plasma quickly enter RBCs, where most of the reactions that prepare carbon dioxide for transport as bicarbonate ions (HCO3
-) in plasma occur
– When CO2 diffuses into the RBCs, it combines with water, forming carbonic acid (H2CO3)
– H2CO3 is unstable and quickly dissociates into hydrogen ions and bicarbonate ions:
• CO2 + H2O ↔ H2CO3 ↔ H+ + HCO3
-

GAS EXCHANGES AT THE BODY TISSUES

Carbon Dioxide Transport
– Although this reaction also occurs in plasma, it is thousands of times faster in RBCs because they (and not plasma) contain carbonic anhydrase, an enzyme that reversibly catalyzes the conversion of carbon dioxide and water to carbonic acid
• Hydrogen ions released during the reaction bind to Hb, triggering the Bohr ( alters the structure of hemoglobin and release of oxygen) effect; thus, O2
release is enhanced by CO2 loading (as HCO3-)

Carbon Dioxide Transport
• Once generated, HCO3- diffuses quickly
from the RBCs into the plasma, where it is carried to the lungs:– To counterbalance this chloride ions (Cl-) move
from the plasma into the RBCs• This ion exchange is called the chloride shift

Carbon Dioxide Transport• In the lungs the process is
reversed• As blood moves through the
pulmonary capillaries– PCO2
declines from 45 mm Hg to 40 mm Hg
• For this to occur, CO2 must first be freed from its bicarbonate state
– HCO3- renters the RBCs (Cl-
moves into the plasma) and binds with H+ to form carbonic acid, which is then split by carbonic anhydrase to release CO2 and water
– This CO2, along with that released from hemoglobin and from solution in plasma, then diffuses along its partial pressure gradient from the blood into the alveoli

GAS EXCHANGES IN THE LUNGS

GAS EXCHANGES AT THE BODY TISSUES

HALDANE EFFECT• The lower the PO2
, and the lower the extent of Hb saturation with oxygen, the more CO2 that can be carried in the blood
• Reflects the greater ability of reduced hemoglobin to form carbaminohemoglobin and to buffer H+ by combination with it
• As CO2 enters the systemic bloodstream, it causes more oxygen to dissociate from Hb (Bohr effect), which allows more CO2 to combine with Hb and more HCO3
- to be formed (Haldane effect)

HALDANE EFFECTThe lower the degree of Hb saturation, the greater the amount
of CO2 that can be transported by the blood

HALDANE EFFECT• In the pulmonary
circulation, the situation is reversed—uptake of O2 facilitates release of CO2
• As Hb becomes saturated with O2, the H+ released combines with HCO3
-, helping to unload CO2 from the pulmonary blood
• The Haldane effect encourages CO2 exchange in both the tissues and lungs

GAS EXCHANGES IN THE LUNGS

Influence of CO2 on Blood pH
• The H+ released during carbonic acid dissociation is buffered by Hb or other proteins within the RBCs or in plasma
• The HCO3- generated in the red blood cells diffuses into
the plasma, where it acts as the alkaline reserve part of the blood’s carbonic acid-bicarbonate buffer system– This system is very important in resisting shifts in blood pH– Example:
• If hydrogen ion concentration in blood begins to rise, excess H+ is removed by combing with HCO3
- to form carbonic acid ( a weak acid that dissociates very little at either physiological or acidic pH)
• If H+ concentration drops below desirable levels in blood, carbonic acid dissociates, releasing hydrogen ions and lowering the pH again

Influence of CO2 on Blood pH
• Changes in respiratory rate or depth can produce dramatic changes in blood pH by altering the amount of carbonic acid in the blood– Slow, shallow breathing allows CO2 to accumulate in the blood
• Carbonic acid levels increase and blood pH drops
– Rapid, deep breathing quickly flushes CO2 out of the blood, reducing carbonic acid levels and increasing blood pH
• Respiratory ventilation can provide a fast-acting system to adjust blood pH (and PCO2
) when it is disturbed by metabolic factors
• Respiratory adjustments play a major role in the acid-base balance of the blood

Control Of RespirationNeural Mechanisms and Generation of Breathing
Rhythm• Medullary Respiratory
Centers– The medulla oblongata
contains:• The dorsal respiratory group,
or inspiratory center– With neurons that act as the
pacesetting group– Neurons mostly involved in
inspiration• And the ventral respiratory
group– Which functions mostly
during forced breathing– Contains a more even mix
of neurons involved in inspiration and expiration

NEURAL PATHWAYS

Dorsal Respiratory Group (DRG)
• Appears to be the pacesetting respiratory center• Inspiratory center• When its neurons fire, impulses travel along the phrenic and
intercostal nerves to excite the diaphragm and external intercostal muscles– The thorax expands and air rushes into the lungs– The DRG becomes dormant
• Expiration occurs passively as the inspiration muscles relax and the lungs recoil
• This cyclic on/off activity of the inspiratory neurons repeats continuously and produces a respiratory rate of 12-15 breaths per minute, with inspiratory phases lasting for about 2 seconds followed by expiratory phases lasting about 3 seconds

NEURAL PATHWAYS

Ventral Respiratory Group (VRG)
• A network of neurons that extends in the ventral brain stem from the spinal cord to the pons-medulla junction
• Contains a more even mix of neurons involved in inspiration and expiration
• Which functions mostly during forced breathing (especially forced expiration) when more strenuous breathing movements are needed

Pons Respiratory Centers
• Appears to smooth out the transitions from inspiration to expiration, and vice versa
• The pontine respiratory group (PRG) continuously transmits inhibitory impulses to the inspiratory center of the medulla
• The pons modifies the breathing rhythm and prevents overinflation of the lungs through an inhibitory action on the medullary respiration centers

NEURAL PATHWAYS

Genesis of the Respiratory Rhythm
• Origin of the Normal Respiratory Rhythm ????????????
• It appears to be the result of reciprocal inhibition of interconnected neuronal networks in the medulla– On the part of the different respiratory centers
• The medullary centers maintain the normal rhythm of breathing

Factors Influencing Breathing Rate and Depth
• The respiratory centers in the medulla and pons are sensitive to both excitatory and inhibitory stimuli

Pulmonary Irritant Reflexes
• Lungs contain receptors that respond to an enormous variety of irritants
• Accumulated mucus, dust, noxious fumes:– Reflex constriction when present in the
bronchioles– Cough when present in the trachea– Sneeze when present in the nasal cavity

The Inflation ReflexHering-Breuer Reflex
• The visceral pleurae and conducting passages in the lungs contain numerous stretch receptors (baroreceptors) that are vigorously stimulated when the lungs are inflated
• These receptors signal the medullary respiratory centers, sending inhibitory impulses that end inspiration and allow expiration to occur
• As the lungs recoil, the stretch receptors become quiet, and inspiration is initiated once again
• Is a protective response (prevents excessive stretching of the lungs) rather than a normal regulatory mechanism

Influence of Higher Brain Centers Hypothalamic Controls
• Acting through the limbic system, strong emotions, and pain activate sympathetic centers in the hypothalamus, that can modify respiratory rate and depth by sending signals to the respiratory centers:– Touch something cold and gaped– Breath holding when we are angry– Increased respiratory rate when excited– Rise in body temperature increases respiratory rate– Drop in body temperature decreases respiratory rate– Dip in cold water causes cessation of breathing or gasping

Influence of Higher Brain CentersCortical Controls
• The cerebral cortex can exert voluntary control over respiration by bypassing the medullary centers and directly stimulating the respiratory muscles

Influence of Higher Brain CentersChemical Factors
• The most important are changing levels of CO2, O2, and H+ in arterial blood
• Central chemoreceptors located bilaterally in the ventrolateral medulla and peripheral chemoreceptors found in the great vessels of the neck respond to these chemicals

Excitatory influences (+) increases the frequency of impulses sent to the muscles of respiration and
result in deeper, faster breathing

Inhibitory influences (-) decrease the frequency of impulses to the muscles of respiration and result
in shallow, slower breathing

Impulses may be excitatory or inhibitory (+/-) depending on which receptors or brain regions
are activated

Influence of Higher Brain CentersInfluence of PCO2
• Of all the chemicals influencing respiration, CO2 is the most potent and the most closely controlled

Influence of Higher Brain CentersInfluence of PCO2
• CO2 diffuses easily from the blood into the cerebrospinal fluid, where it is hydrated and forms carbonic acid– As the acid dissociates, H+ is liberated:
• This same reaction occurs when CO2 enters RBCs• Unlike RBCs or plasma, cerebrospinal fluid contains no proteins that
can buffer the added H+
• Thus, as PCO2 levels rise, a condition referred to as hypercapnia
– Cerebrospinal fluid pH drops, exciting the central chemoreceptors – Causes an increase in rate and depth of breathing
» This breathing pattern is called hyperventilation which enhances alveolar ventilation and quickly flushes CO2 out of the blood, increasing blood pH

Influence of Higher Brain CentersInfluence of PCO2
• Notice that while rising CO2 levels act as the initial stimulus, it is rising H+ levels that prod the central chemoreceptors into activity
• In the final analysis, control of breathing during rest is aimed primarily at regulating the H+ concentration in the brain

NEGATIVE FEEDBACK MECHANISMS

HOMEOSTATIC IMBALANCE
• A person experiencing an anxiety attack may hyperventilate involuntarily to the point where he or she becomes dizzy or faints
• This happens because low CO2 levels in the blood (hypocapnia) cause cerebral blood vessels to constrict, reducing brain perfusion and producing cerebral ischemia
• Such attacks may be averted by breathing into a paper bag because then the air being inspired is expired air, rich in carbon dioxide, which causes carbon dioxide to be retained in the blood

HOMEOSTATIC IMBALANCEHypoventilation
• When PCO2 is abnormally low, respiration is
inhibited and becomes slow and shallow

HOMEOSTATIC IMBALANCEHyperventilation
• Sometimes swimmers voluntarily hyperventilate so that they can hold their breath longer during swim meets
• This is incredibly dangerous for the following reasons:– Blood O2 content rarely drops below 60% of normal during
regular breath-holding, because as PO2 drops, PCO2
rises enough to make breathing unavoidable
– However, strenuous hyperventilation can lower PCO2 so much that
a lag period occurs before it rebounds enough to stimulate respiration again
– This lag may allow oxygen levels to fall well below 50 mm Hg, causing the swimmer to black out (and perhaps drown) before he or she has the urge to breathe

Influence of PO2
• Cells sensitive (oxygen sensors) to arterial O2 levels are found in the peripheral chemoreceptors of the aortic arch and carotid arteries
• Blood PO2 affects breathing indirectly by influencing chemoreceptors sensitivity to changes in PCO2

OXYGEN CHEMORECEPTORS

Influence of PO2
• Peripheral chemoreceptors monitor plasma PO2 and stimulate an increase in ventilation when PO2 drops below 60 mm Hg

HOMEOSTATIC IMBALANCE
• In people who retain CO2 because of pulmonary disease (e.g., emphysema and chronic bronchitis), arterial PCO2
is chronically elevated and, as a result, chemoreceptors become unresponsive to this chemical stimulus
• In such cases, a declining PO2 acting on the oxygen-
sensitive peripheral chemoreceptors provides the principal respiratory stimulus, the hypoxic drive
• Thus, gas mixtures administered to such patients during respiratory distress are only slightly enriched with O2 because inspiration of pure oxygen would stop their breathing by removing their respiratory stimulus (low PO2
levels)

Influence of Arterial pH
• As arterial pH declines, the respiratory system attempts to compensate by causing an increase in rate and depth of breathing– Attempt to compensate and raise the pH by
eliminating CO2 (and carbonic acid) from the blood
– Mediated by the peripheral chemoreceptors

SUMMARY
• Rising CO2 levels are the most powerful respiratory stimulant– As CO2 is hydrated in cerebrospinal fluid,
liberated H+ acts directly on the central chemoreceptors, causing a reflexive increase in breathing rate and depth
– Low PCO2 levels depress respiration

SUMMARY
• Under normal conditions, blood PO2 affects
breathing only indirectly by influencing chemoreceptor sensitivity to changes in PCO2
• Low PO2 augments PCO2
effects
• High PO2 levels diminish the effectiveness of
CO2 stimulation

SUMMARY
• When arterial PO2 falls below 60 mm Hg, it
becomes the major stimulus for respiration, and ventilation is increased via reflexes initiated by the peripheral chemoreceptors
• This may increase O2 loading into the blood, but it also causes hypocapnia (low PCO2
blood
levels) and an increase in blood pH, both of which inhibit respiration

SUMMARY
• Changes in arterial pH resulting from CO2 retention or metabolic factors act indirectly through the peripheral chemoreceptors to promote changes in ventilation, which in turn modify arterial PCO2
and pH
• Arterial pH does not influence the central chemoreceptors directly

RESPIRATORY ADJUSTMENTSAdjustments During Exercise
• During vigorous exercise, deeper and more vigorous respirations, called hyperpnea, ensure that tissue demands for oxygen are met
• The respiratory changes seen in hypernea match metabolic demands and so do not lead to significant changes in blood O2 and CO2 levels– By contrast, hyperventilation may provoke excessive ventilation, resulting
in low PCO2 and alkalosis
– The abrupt increase in ventilation that occurs as exercise begins reflects interaction of three neural factors:
• 1. Psychic stimuli: our conscious anticipation of exercise• 2. Simultaneous cortical motor stimulation of skeletal muscles and respiratory
centers• 3. Excitatory impulses to the respiratory areas from proprioceptors in active
muscles, tendons, and joints• The small but abrupt decrease in ventilation that occurs as exercise
ends reflects the shutting off of the neural control mechanisms

RESPIRATORY ADJUSTMENTSAdjustments at High Altitude
• Acute mountain sickness (AMS) may result from a rapid transition from sea level to altitudes above 8000 feet– Air density and PO2
are lower
– Headache, shortness of breath, nausea, and dizziness– In severe cases of AMS, lethal pulmonary and cerebral edema may
occur
• A long-term change from sea level to high altitudes results in acclimatization of the body, including an increase in ventilation rate, lower than normal hemoglobin saturation, and increased production of erythropoietin

SCUBA GEAR
• Self-contained underwater breathing apparatus– Has freed divers to explore the ocean depths
• Heavy pressurized suits permits continual equalization of the air pressure (produced by the mixture of compressed air in the tank) with the water pressure– Air enters the lungs at a higher-than-normal pressure
– Descent is not usually a problem, unless below 100 feet

SCUBA GEAR• Nitrogen ordinarily has little effect on body functioning
– Hyperbaric (being exposed to gas pressure greater than atmospheric pressure) conditions for an extended time force so much nitrogen into solution in the blood that it provokes a narcotic effect called nitrogen narcosis
• Nitrogen is far more soluble in lipids than in water, so it tends to concentrate in lipid-rich tissues such as the central nervous system, bone marrow, and fat deposits
• Divers become dizzy, giddy, and appear to be intoxicated• Most ascend to the surface gradually
– Dissolved nitrogen gas can be driven out of the tissues and eliminated by the lungs without problems
• Ascent is too rapid, the PN2 decreases abruptly and the poorly soluble
nitrogen gas appears to “boil” from the tissue and out of solution in the body
– Gas bubbles in the blood (lethal emboli): bends• Decompression sickness can also strike at high altitudes
– Unpressurized aircraft flying above 18,000 feet

DECOMPRESSION

HOMEOSTATIC IMBALANCES OF
THE RESPIRATORY SYSTEM
• Chronic obstructive pulmonary diseases (COPD):– Seen in patients that have a history of
smoking• Result in progressive dyspnea
– Difficult or labored breathing
• Coughing and frequent pulmonary infections• Respiratory failure
– Accompanied by hypoxemia (low oxygen levels), CO2 retention, and respiratory acidosis

PATHOGENESIS OF COPD

HOMEOSTATIC IMBALANCES OF
THE RESPIRATORY SYSTEM
• Obstructive emphysema is characterized by permanently enlarged alveoli and deterioration of alveolar walls– Chronic inflammation leads to lung fibrosis, and invariably the
lungs lose their elasticity• Airways collapse during expiration and obstruct the outflow of air
– Bronchioles open during inspiration but collapse during expiration– Surprisingly gas exchange remains adequate until late in the disease
• Chronic bronchitis: inhaled irritants– Results in excessive mucus production, as well as inflammation
and fibrosis of the lower respiratory mucosa• Pulmonary infections are frequent because bacteria thrive in the
stagnant pools of mucus

PATHOGENESIS OF COPD

HOMEOSTATIC IMBALANCES OF
THE RESPIRATORY SYSTEM
• Asthma is characterized by coughing, dyspnea difficult or labored breathing), wheezing, and chest tightness—alone or in combination– Brought on by active inflammation of the airways
• Immune response under the control of TH2 cells (subset of lymphocytes) that recruit eosinphils to the site
• Bronchoconstriction• Common triggers: allergens
– Mites, cockroaches, cats, dogs, and fungi
– Marked by acute exacerbations (more violent) followed by symptom-free periods

HOMEOSTATIC IMBALANCES OF
THE RESPIRATORY SYSTEM
• Tuberculosis (TB) is an infectious disease caused by the bacterium Mycobacterium tuberculosis and spread by coughing and inhalation– Mostly affects the lungs but can spread through the lymphatics to
affect other organs– TB test depends on detecting anti-TB antibodies in the patient
• 1/3 of the world’s population is infected, but most people never develop active TB because a massive inflammatory and immune response usually contains the primary infection in fibrous, or calcified, nodules (tubercles) in the lungs
– However, the bacteria survive in the nodules and when the person’s immunity is low, they may break out and cause symptomatic TB, involving fever, night sweats, weight loss, a racking cough, and spitting up blood

HOMEOSTATIC IMBALANCES OF
THE RESPIRATORY SYSTEM• Lung Cancer:
– In both sexes, lung cancer is the most common type of malignancy, and is strongly correlated with smoking
• 90% of lung cancer patients were smokers– Because lung cancer is aggressive and metastasizes rapidly and widely,
most cases are not diagnosed until they are well advanced– Squamous cell carcinoma arises in the epithelium of the bronchi, and
tends to form masses that hollow out and bleed– Adencarcinoma originates in peripheral lung areas as nodules that develop
from bronchial glands and alveolar cells– Small cell carcinoma contains lymphocyte-like cells that form clusters
within the mediastinum and rapidly metastasize– Some small cell carcinomas cause problems beyond their effects on the
lungs because they become ectopic sites of hormone production• Some secrete ACTH (leading to Cushing’s disease) or calcitonin
(hypocalcemia)

DEVELOPMENTAL ASPECTS OF
THE RESPIRATORY SYSTEM• By the fourth week of development, the olfactory placodes are present and
give rise to olfactory pits that form the nasal cavity• The nasal cavity extends posteriorly to join the foregut, which gives rise to an
outpocketing that becomes the pharyngeal mucosa• By the eighth week of development, mesoderm forms the walls of the
respiratory passageways and stroma of the lungs• As a fetus, the lungs are filled with fluid, and vascular shunts are present that
divert blood away from the lungs; at birth, the fluid drains away, and rising plasma PCO2 stimulates respiratory centers
• Respiratory rate is highest in newborns, and gradually declines to adulthood; in old age, respiratory rate increases again
• As we age, the thoracic wall becomes more rigid, the lungs lose elasticity, and the amount of oxygen we can use during aerobic respiration decreases
• The number of mucus glands and blood flow in the nasal mucosa decline with age, as does ciliary action of the mucosa, and macrophage

EMBRYONIC DEVELOPMENT OF THE RESPIRATORY SYSTEM

HOMEOSTATIC IMBALANCE• Cystic fibrosis
– Most common lethal genetic disease in the U.S.• 1 out of 2400 births
– Oversecretion of a viscous mucus that clogs the respiratory passages, providing a breeding ground for airborne bacteria that predisposes the child to fatal respiratory infection that can be treated only by a lung transplant
– Impairs food digestion by clogging ducts that deliver pancreatic enzymes and bile to the small intestine
– Sweat glands produce an extremely salty perspiration– Conventional therapy:
• Mucus-dissolving drugs• Clapping the chest to loosen thick mucus• Antibiotics to prevent infection
– Cause: faulty gene that codes for a cystic fibrosis transmembrane conductance regulator protein
• Lacks an essential amino acid• Enzyme remains stuck in the endoplasmic membrane and does not reach the plasma membrane to
perform its function– Consequently less Cl- is secreted and less water follows, resulting in the thick mucus typical of CF
– Unable to reach the bacteria embedded in the mucus, immune cells begin to attack the lung tissue, turning the air sacs into bloated cysts

DECOMPRESSION