Embed Size (px)
Citation preview

274
THE PLACE OF RESPIRATORY FUNCTIONTESTS IN CLINICAL MEDICINE
D. V. BATES, M.D., M.R.C.P.First Assistant, Mledical Unit, St. Bartholomew's Hospital, London, E.C.i
IntroductionIt is difficult to settle on a precise date for the
introduction of objective methods of measurementinto clinical medicine. Perhaps a good case canbe made out for the year I867 when CliffordAllbutt arranged for the first clinical thermometerto be manufactured. This technique survived theridicule with which it was greeted, but perhapseven then it was realized that the substitution of athermometer for the sensitive hand of the physicianwas a dangerous precedent, likely eventually tolead to the substitution of one technique of diag-nosis by another. It is important that certainerroneous preconceptions are cleared away there-fore, before the particular question of the place ofrespiratory function tests is considered. Thedays when a vain search was made for tests whichwere infallible in the diagnosis of this or thatcondition, have passed. It is quite clear that thebest contemporary practice assembles its informa-tion, the history, the physical examination, theX-ray, the blood count, etc., with care and withknowledge of what may be misleading in each ofthem; and then reaches a diagnosis by puttingthis information together as neatly and as co-herently as it will allow, guided by its experience.No-one expects the blood urea to diagnose chronicnephritis, so there need be no surprise if the vitalcapacity does not diagnose emphysema. Furtherone can recall that all investigations, from themeasurement of the body temperature onwards,have started essentially as research investigationsused only by one or two laboratories by one or twophysicians. A general application of the methodhas followed a general understanding of itsusefulness. Some contemporary investigationsare in the border country between being' research 'and ' clinical' investigations; the electro-encephalogram, the serum lipo-proteins perhapsbeing examples of these. To the question, therefore, should every hospital have facilities forstudying the serum lipo-proteins, the answermight be that it should be available in any depart-ment where vascular disease is particularly
studied, but not necessarily elsewhere. Thereseems little doubt that the full range of con-temporary respiratory function tests should beavailable to every chest hospital, but this is not thesame as suggesting that every hospital should havea pulmonary function laboratory.
Lastly, there are some difficulties that parti-cularly apply to respiratory function tests. Theco-operation of the patient is required, thoughthis very rarely presents a problem. Indeed Ihave come to the conclusion that if the patientcomplains of dyspnoea, the idea of measuring hislung performance seems at the moment morelogical and reasonable to the patient than it does tothe physician. Some of the recent techniques ofmeasurement of respiratory function are compli-cated and all of them require trained staff. Weneed not be deterred by the fact that these testscannot be applied in every doctor's consultingroom. The value of simple tests, like the maximalbreathing capacity, tends to be overstressedbecause they can be easily measured, and it ismost important that the practical value of the testin clinical practice receives very critical attention,since if nothing is going to be learned of real valueto the physician, any test, however simple, is awaste of time.The last ten years have seen the completion of a
great deal of the essential foundation work in thestudy of pulmonary physiology. These advanceshave been most excellently brought together andsimply described in a recent book by J. H. Comroeand his colleagues. The purpose of this articleis, firstly, to describe contemporary tests offunction and to discuss the information they arecapable of yielding; and secondly to discuss theclinical situations in which this information isimportant.What Aspects of Pulmonary Function can beMeasured ?
Trotter in 1933, pointed out that ' up to thepresent time, medicine has almost wholly avoidedthe burden of measurement.' Recent research
by copyright. on D
ecember 15, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.32.368.274 on 1 June 1956. Dow
nloaded from

June 1956 BATES: The Place of Respiratory Function Tests in Clinical Medicine 275
has given us an exact knowledge of what consti-tutes normal lung function, and what the derange-ments are in certain diseases. The following' compartments' of pulmonary function can beseparately measured.
I. Total ventilation-ability to move airnormally in and out.
2. Measurement of the subdivision of lungvolume-volume of gas normally 'residual'or displaceable.
3. Measurement of evenness of gas distributionwithin the lungs-the air breathed in is almostperfecly divided between alveoli in normal lungs.
4. Measurement of physical characteristics ofthe lungs-normally the lungs are easily dis-tensible, and the bronchial resistance to airflowis low.
5. Measurement of the efficiency of gas transferacross the lung-measurement of the rate ofoxygen diffusion which indicates principally eitherloss of surface area of exposed blood, or somebarrier to gas diffusion between alveoli and thered cell haemoglobin.
6. Direct measurement of pressure in thepulmonary artery.
7. Measurement of tensions of oxygen and CO2in the blood.
8. Ability to measure certain aspects oflung function in each lung individually-bronchospirometry.
Recent work has emphasised the value of makingsome of these measurements while the patient isexercising, as this will often show more clearlythe degree of defect present. This list presents aformidable array, and it is interesting to note thattechniques for the measurement of Nos. 3, 4, 5, 6,7 and 8 have all been developed within the last15 years, and those used to measure the remainingtwo have been simplified and clarified during thepast few years.In What Clinical Situations is the Measure-ment of Pulmonary Function Useful ?
It would be surprising indeed if at this stageit were possible to define clearly all the situationsin which these tests of function are of value.The use of these tools in research is evident, andneed not be stressed here; but much of the worknecessary before a final verdict can be given ontheir clinical application, remains to be done.Comroe has described a few clinical cases illustra-tive of some of the clinical problems in whichfunction tests may be useful, and enough hasperhaps, been learned to permit certain con-clusions about the value of these tests in clinicalmedicine. The field of study being potentially solarge, each worker in it has inevitably mainly givenhis attention to particular problems, and for this
reason I will stress those situations in whichpersonal experience has indicated the usefulnessof these methods of study.(a) In Accurate Diagnosis of Emphysema.The pathological condition that leads to the
most gross defects of all aspects of pulmonaryfunction is emphysema. It is sometimes errone-ously thought that because the classical fullydeveloped condition is easy to recognize, thereforethere is no diagnostic problem. In my experience,difficulty is likely to arise in three distinctsituations.
I. If there has been minimal antecedent bronchitis.In this country, the majority of patients developemphysema secondary to obvious chronic bron-chitis, and it is therefore sometimes forgotten thatemphysema may occur without any convincinghistory of bronchitis and without any sputum.The patients are often younger than those whoseemphysema has followed chronic bronchitis, andthe diagnosis may easily be missed. In two suchcases in my experience, the patients have beenreferred to the psychiatrist, the dyspnoea havingbeen diagnosed as' functional.' In one other, thedyspnoea was vaguely attributed to 'left ventri-cular strain' (in the absence of hypertension andwith a normal ECG). This type of patient doesnot have large bullae in the lungs, and the postero-anterior X-ray film may look relatively normal.Occasionally, these cases are seen as patientswith evidence of right ventricular failure of whichthe cause is clinically obscure.
2. When polycythemia is present, with minimalbronchitis. There is no defect of respiratoryfunction in patients with primary polycythemiarubra vera. The presence of bronchitis raises thequestion of the possibility of whether the poly-cythemia is secondary to emphysema. In certainpatients this problem can only be finally solved bythe use of function tests.
3. In the assessment of severity and response totreatment. There is evidence that the prognosisin emphysema is related to the level of impairmentof gas diffusion. This defect is due to a progressiveloss of surface of lung parenchyma and from thefunctional point of view constitutes the mostcharacteristic impairment of emphysema. Thestage of chronic bronchitis and bronchospasm isdistinguished from it by the maintenance ofrelatively normal gas diffusion together with thesame evidence of ventilatory obstruction. By theuse of tests Nos. I, 2, 4 and 5 therefore, in anygiven patient an estimate can be made of his statusin respect of irreversible change. This distinctionis at the moment mainly of research value, and is ofuse in classifying more accurately the response totreatment of patients generally labelled as 'chronicbronchitis and emphysema.'
C
by copyright. on D
ecember 15, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.32.368.274 on 1 June 1956. Dow
nloaded from

276 POSTGRADUATE MEDICAL JOURNAL June I956
4. In alleged ' emphysema.' Of these, perhapsthe most interesting is the study of patients whopresent with one large ' emphysematous' bulla inthe lung. The nature of these lesions is obscure,but pulmonary function tests before and aftersurgery enable an accurate opinion to be given ofthe normality of the rest of the lungs. In myexperience, sometimes the remainder of the lungsis quite normal, but in one patient, in spite ofnormal X-rays, there was clearly a generalizeddefect involving the apparently normal lungs afteroperation (see Fig. 3).(b) In the Study of Pulmonary Infiltrations andFibrosis
In this highly confused field of medicine, it isimportant to recognize that severe function defectmay be present with little radiological change, andthat evident radiological change may not beaccompanied by more than slight functional defect.For instance, in following the treatment of a caseof acute miliary tuberculosis, it was found thatnine months after treatment was begun, the lungswere still twice as' stiff' as normal and the rate ofgas diffusion was half normal. The patient camewith the comment that she had no disability andthe X-rays of her lung fields was completelynormal: both these comments were correct andyet the lungs had clearly not returned to normal(see Fig. 2a). The systematic study of the use ofACTH (for instance) in sarcoidosis, in chronicdiffuse interstitial fibrosis, or in collagen diseases,necessarily involves the use of tests of function ifit is to be complete, just as in the ' nephrotic syn-drome' the effect of treatment may be followedby routine tests of renal function or plasma proteinestimation. It is difficult to convince chest physi-cians that the following of treatment with functiontests in cases of lung disease is no less and no moreunreasonable than to follow the progress of renalor hepatic disease with appropriate objective tests.Certain types of pulmonary fibrosis, such as in-dustrial pneumoconiosis, present special problemswhich have yet to be tackled with modern tech-niques of study.(c) In the Study of the Effect of Lung Surgery andin Pre-operative AssessmentThe effect of surgical procedures on lung
function can only be accurately assessed by meansof tests of function. A recent investigation hasshown how complex is the problem of disabilityafter pneumonectomy, and it is already clear thatfurther work is required to clarify the relationshipbetween' over-inflation 'and 'emphysema.' Someof the controversial points about preferentialoperations from the point of view of functioncould be settled by a careful study of differentgroups of patients with the function tests nowavailable. More complex problems, such as the
results of lung denervation or the effect of removalof bullae in the lung, can quite clearly only beapproached intelligibly with the assistance offunction tests. Bronchospirometry is fairlygenerally used on the continent in the pre-operativeassessment of function of the two lungs separately.It has not yet been used in conjunction withmeasurements of lung mechanics or gas diffusion,but it may be expected that these will add to itsvalue.
(d) In the Study of Rare and Obscure DiseasesIt is often said that it is only in rare and
interesting' diseases that the use of pulmonaryfunction tests is of value. Unless the disordersmentioned above are all in this category, this isclearly not true. It is true that they are of valuein obscure cases, such as arterio-venous fistulain the lung, but in my experience these casesconstitute a small fraction of those in which thesetests are useful.
(e) As Research InvestigationsPhysicians, particularly if they have no interest
in nor aptitude for experimental work, are veryapt to forget that all clinical investigations startedlife as esoteric research methods. Once the'neighbours ' use them, as it were, they take theirplace as respectable clinical tools. One shouldnot have to stress the research aspect of the use oftests of function in the light of the experimentalwork published in the last ten years. There isno doubt but that they will be increasingly used inthe study of respiratory disorders.
What Facilities and Apparatus are Required ?It is evident that the facilities and equipment
required depends entirely on the scope of the workto be undertaken. In the case of a large hospitaldealing exclusively with respiratory disease of alltypes, the size of the department of appliedphysiology should be limited only by the financialsupport such a department can receive-there willalways be plenty for it to do. It is not, in my view,unreasonable to maintain that such major centresshould be equipped to undertake complete functionstudies when required. The correct balancebetween purely research studies and purely routineinvestigations is not an easy one to define, but itbecomes easier as physicians and surgeons under-stand the type of problem in which function testsare of real assistance. In my experience aminimum team for such work, able to study fullyperhaps I2 patients a week, requires one full timeand one half time research worker, both fullytrained, and two fully trained technicians as aminimum. It takes perhaps about a year to trainsomeone with an aptitude for this type of work inthe ' routine ' studies and a further year before heis fully conversant with the field. It must be
by copyright. on D
ecember 15, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.32.368.274 on 1 June 1956. Dow
nloaded from

June 1956 BATES: The Place of Respiratory Function Tests in Clinical Medicine 277
.:. ....: ....:
FIG:. .aT 1 Ibi
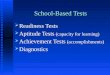
FIGa. xa FIG. ibFIG. I.-Both these X-rays are of men in their fifties, each with polycythemia (Hb = 30 per cent.). In the case of
(a), all pulmonary function tests were normal, as is usual in polycythemia rubra vera. Although the respiratoryhistory in the case of (b) was insignificant, there was a marked impairment of gas diffusion and a reduced maximalbreathing capacity-suggesting that the lung condition (? emphysema) was probably responsible for thepolycythemia.
'":,~ii.~!?11i':'iii
...::.
............ ...
.... .'.m- :......: !.
..... .:.-
..: ... ...:.
FIG. 2aFIG. 2a is the X-ray of a girl, aged 19, seven months
after treatment of severe acute miliary tuber-culosis of the lungs. At this time she wassymptom-free and this X-ray was consideredto be clear. Lung function tests showed thatthe lungs were still twice as 'stiff' as normaland the diffusing capacity was only half thenormal value.
....... .·
mbi~~
FIG. 2bFIG. 2b.-Man, aged 57. 20-year intermittent
exposure to silica (grinding). Recovered ffomattack of right ventricular failure. X-rayevidence of fibrosis slight but definite. Pul-monary function tests showed extreme reduc-tion in lung compliance (= very stiff), andsevere interference with gas diffusion, indi-cating a much more severe degree of lungchange than would have been judged from theX-ray appearance.
by copyright. on D
ecember 15, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.32.368.274 on 1 June 1956. Dow
nloaded from

278 POSTGRADUATE MEDICAL JOURNAL June I956
...... i;"ii
·l
.....
.: :i::
-E........... ...:::
.: ..
........ .... . ....... :.............. :.....". ................:;FIG. 3a FIG. 3b
FIG. 3.-These X-rays are of the same man (aged 30), before and after removal of the cyst in the left upper lobe.There was a moderate degree of impairment of lung function before operation, and afterwards there was noimprovement in the test results. The low rate of gas diffusion, in particular, suggests strongly that the cystwas part of a generalized lung change (? rarefaction) present in both lungs. In other similar cases, the findingof normal function oost-operativelv Dresumablv indicates that the cyst is a solitary phenomenon.
emphasized that the measurement of purelyventilatory tests of function (see No. i above) byonie technician, is unlikely to lead to the collectionof much information of real value or assistance tothe physician; and it does not seem to me helpfulto suggest that the consultant should be en-couraged to make these observations-howeversimple the equipment-in his consulting room.These single ventilatory tests are of value asresearch tools in the study, for instance, of theeffect of broncho-dilator drugs, but in my experi-ence their usefulness is very limited in the solutionof any problem of any complexity.Conclusion
There is little doubt that modern tests ofrespiratory function are of considerable value inthe study, management and diagnosis (perhaps inthat order) of cases of lung disease. The next20 years will probably see an increasing applicationof these methods of investigation, and enable the
exact scope of their use to be more precisely defined.Figs. I to 3, show X-rays of five patients in whichtests of function contributed materially to theclinical management. It may be well to end withanother quotation from Trotter: ' Moreover,with all its opportunities, observation has at itsbest been able to disclose but little of the funda-mental processes of disease, of the exact meaningof morbid phenomena, of the precise mechanismslying behind symptoms; whereas experiment hasa remarkable series of successes of these very kindsalready to its credit. In view of such considera-tions as these, it may well be asked whether thetime has not come when it should be recognized,with all the practical consequences that wouldfollow, that observation can no longer be regardedas able to effect serious advances in medicine.'
COMROE, J. H. and others (I955), ' The Lung,' The Year BookPublishers.
TROTTER, W., 'The Collected Papers of Wilfrid Trotter,F.R.S.,' (I941), Oxford Medical Publications, II2, 194.
BACK NUMBERS OF THE POSTGRADUATE MEDICAL JOURNAL
If any subscribers have copies, in good condition, of MARCH and APRIL 1952,the Fellowship of Postgraduate Medicine, 60 Portland Place, London, W.I, will be
glad to purchase them.
by copyright. on D
ecember 15, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.32.368.274 on 1 June 1956. Dow
nloaded from