Embed Size (px)
Citation preview

Respiratory conditionsRespiratory conditions
Anne AspinAnne Aspin
20102010

EmbryologyEmbryology
Atresia of oesophagus with fistulaAtresia of oesophagus with fistula Atresia of trachea with fistulaAtresia of trachea with fistula Laryngo-tracheo-oesophageal cleftsLaryngo-tracheo-oesophageal clefts
System of folds, blocked pathwaySystem of folds, blocked pathway
Adriamycin (rat research)Adriamycin (rat research)

Defects caused by improper development Defects caused by improper development of the pleuro-peritoneal cavityof the pleuro-peritoneal cavity
Failure of muscularisation of the Failure of muscularisation of the lumbocostal and pleuro-peritoneal canal, lumbocostal and pleuro-peritoneal canal, weak part of diaphragm.weak part of diaphragm.
Pushing of intestine through foramen of Pushing of intestine through foramen of Bochdalek of diaphragm.Bochdalek of diaphragm.

Premature return of intestine to abdo Premature return of intestine to abdo cavity but canal still opencavity but canal still open
Abnormal persistance of lung in pleuro Abnormal persistance of lung in pleuro peritoneal cavity, preventing closure of peritoneal cavity, preventing closure of cavitycavity
Abnormal development of early lung.Abnormal development of early lung.

Of these theories failure of the pleuro-Of these theories failure of the pleuro-peritoneal membrane to meet the peritoneal membrane to meet the transverse septum is likely explanation for transverse septum is likely explanation for diaphragm herniationdiaphragm herniation
Lack of embryological evidenceLack of embryological evidence Day 13,(L) Day 14 (R), disturbed Day 13,(L) Day 14 (R), disturbed
development (rats) = 4-5/52 embryos.development (rats) = 4-5/52 embryos.

Lung hypoplasiaLung hypoplasia
From day 14 of deformation lung From day 14 of deformation lung hypoplasia caused by liver growing hypoplasia caused by liver growing through diaphragmatic defect into thoracic through diaphragmatic defect into thoracic cavity.cavity.
Liver grows at a faster rate than the lungs.Liver grows at a faster rate than the lungs.

Head and Neck ExaminationHead and Neck Examination
Respirations – 30 – 60 bpmRespirations – 30 – 60 bpm Abnormal < 30, > 60 bpm, nasal Abnormal < 30, > 60 bpm, nasal
flaring,intercostal recesssionflaring,intercostal recesssion
Apnoea, anoxia, alkalosisApnoea, anoxia, alkalosis Slow, weak, rapid signifies brain damageSlow, weak, rapid signifies brain damage Tachypnoea, congenital heart disease, resp Tachypnoea, congenital heart disease, resp
disease.disease. Asymmetry, phrenic nerve palsy, CDH, Asymmetry, phrenic nerve palsy, CDH,
atelectasisatelectasis

Examination of the noseExamination of the nose
Broad flat, chromosomal abnormalityBroad flat, chromosomal abnormality Patency, choanal atresia, tumourPatency, choanal atresia, tumour SneezingSneezing Bloody discharge, syphilisBloody discharge, syphilis

Examination of the mouth and Examination of the mouth and throatthroat
Excessive salivaExcessive saliva Abnormal structures, cleft lip and palate, Abnormal structures, cleft lip and palate,
micrognathia, large tongue, absent or micrognathia, large tongue, absent or unequal reflexes, prematurity or CNS unequal reflexes, prematurity or CNS anomalyanomaly
Distended neck veins indicate chest or Distended neck veins indicate chest or pneumomediastinal mass.pneumomediastinal mass.

Oesophageal atresiaOesophageal atresia
Bubbly secretionsBubbly secretions ApnoeaApnoea CyanosisCyanosis Immediate vomiting on feedingImmediate vomiting on feeding Unable to pass ng tubeUnable to pass ng tube Replogle tube, continual pharyngeal Replogle tube, continual pharyngeal
suctionsuction

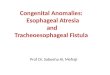
Types of oesophageal atresia Types of oesophageal atresia and fistulaand fistula
86% 7%4%

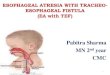
Types continuedTypes continued
1%<1
<1

Lungs and ThoraxLungs and Thorax
Crackles and rhonchi present first four Crackles and rhonchi present first four hours after birth.hours after birth.
Abnormal: decreased abdominal breathingAbnormal: decreased abdominal breathing Thoracic and asymmetrical breathing – Thoracic and asymmetrical breathing –
phrenic nerve damage, CDH,phrenic nerve damage, CDH, Hyperresonance may indicate Hyperresonance may indicate
pneumomediastinum, pneumothorax, CDHpneumomediastinum, pneumothorax, CDH

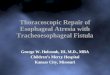
Thickened epiglottisThickened epiglottis

Oedematous narrowed sub Oedematous narrowed sub epiglottic tracheaepiglottic trachea

TracheobronchogramTracheobronchogram

Collapse of right main bronchusCollapse of right main bronchus

Indications for bronchoscopyIndications for bronchoscopy
Stridor Stridor Unexplained wheeze Unexplained wheeze Unexplained or persistent cough Unexplained or persistent cough
Haemoptysis Haemoptysis Suspected foreign bodySuspected foreign bodySuspected airway trauma, Suspected airway trauma,
chemical, or thermal injury chemical, or thermal injury Suspected tracheobronchial Suspected tracheobronchial
fistula fistula Suspected tracheobronchial Suspected tracheobronchial
stenosis stenosis Radiological abnormalities Radiological abnormalities Persistent or recurrent Persistent or recurrent
consolidation or atelectasis consolidation or atelectasis Recurrent or persistent infiltratesRecurrent or persistent infiltrates
Lung lesions of unknown Lung lesions of unknown aetiology aetiology
Immunosupressed patients Immunosupressed patients Identify cause of pneumonia Identify cause of pneumonia Recurrence of disease Recurrence of disease Cystic fibrosis Cystic fibrosis Identify cause of infection Identify cause of infection Intensive care Intensive care Examine for the position, patency, Examine for the position, patency, or damage related to or damage related to
endotracheal or tracheostomy endotracheal or tracheostomy tubes tubes
Facilitation of endotracheal Facilitation of endotracheal intubation intubation
Endobronchial stent placementEndobronchial stent placement

BronchoscopyBronchoscopy
Early dates, removal of foreign bodiesEarly dates, removal of foreign bodies
Rigid bronchoscope (telescope fits down), Rigid bronchoscope (telescope fits down), complete control of airway, ventilationcomplete control of airway, ventilation
Flexible bronchoscope (bundles of optical Flexible bronchoscope (bundles of optical fibres, light to the tips), children from 3yrsfibres, light to the tips), children from 3yrs

Complications of bronchoscopyComplications of bronchoscopy
Pneumothorax 8%Pneumothorax 8% Incidence reduced if bronchoscope Incidence reduced if bronchoscope
avoiding right middle lobeavoiding right middle lobe
Haemorrhage following biopsyHaemorrhage following biopsy Pyrexia, dyspnoeaPyrexia, dyspnoea

Choanal atresiaChoanal atresia
Complete or partialComplete or partial Bilateral or unilateralBilateral or unilateral Dyspnoea, apnoea when feedingDyspnoea, apnoea when feeding Thick mucus in nasal cavitiesThick mucus in nasal cavities Feeding difficultiesFeeding difficulties Blockage of catheter at 3cm.Blockage of catheter at 3cm. Stents are required.Stents are required.

Congenital laryngeal stridorCongenital laryngeal stridor
LaryngomalaciaLaryngomalacia Inspiratory stridorInspiratory stridor Suprasternal indrawingSuprasternal indrawing Noise increase with crying, decrease with Noise increase with crying, decrease with
sleepingsleeping
Cause: long, curved epiglottisCause: long, curved epiglottis Spontaneous recovery 2-3years.Spontaneous recovery 2-3years.

Common causesCommon causes
Laryngomalacia – 60%Laryngomalacia – 60% Congenital subglottic stenosisCongenital subglottic stenosis Vocal cord palsy - unilateral, birth trauma Vocal cord palsy - unilateral, birth trauma
– temporary– temporary Bilateral vocal cord palsy assoc other Bilateral vocal cord palsy assoc other
congenital anomaliescongenital anomalies

Morimoto et al (2004)Morimoto et al (2004)
97 patients 1991-200197 patients 1991-2001
Laryngomalacia 32%Laryngomalacia 32% Vocal cord palsy and laryngeal stenosis Vocal cord palsy and laryngeal stenosis
22%, within 2/12, severe dyspnoea22%, within 2/12, severe dyspnoea Haemangioma or papilloma 11%Haemangioma or papilloma 11% Cystic disease 7%Cystic disease 7%

contcont
2 / 31 of laryngomalacia and 2 / 22 VCP 2 / 31 of laryngomalacia and 2 / 22 VCP had neuromuscular disordershad neuromuscular disorders
3 of VCP complicated by laryngeal 3 of VCP complicated by laryngeal stenosisstenosis
33 / 97 Tracheostomy33 / 97 Tracheostomy
Sometimes stridor is the only presenting Sometimes stridor is the only presenting symptom. Past history importantsymptom. Past history important

Case historyCase history
6/12 girl6/12 girl Fever, coughingFever, coughing Inspiratory stridorInspiratory stridor Palpable neck swelling, bulging Palpable neck swelling, bulging
pharyngeal wallpharyngeal wall Limited movement of neckLimited movement of neck ? spasmodic croup, lymphadenitis coli? spasmodic croup, lymphadenitis coli Found to be retro pharyngeal abscessFound to be retro pharyngeal abscess

TreatmentTreatment
Oral incisionOral incision Drainage of abscessDrainage of abscess AntibioticsAntibiotics

Unilateral vocal cord paralysisUnilateral vocal cord paralysis
StridorStridor LaryngospasmLaryngospasm DyspnoeaDyspnoea
Cause by abnormal innervation of nerve Cause by abnormal innervation of nerve branches into adductor fibersbranches into adductor fibers

ResearchResearch
ObjectiveObjective
Determine stridor at rest after oral Determine stridor at rest after oral Prednisolone 1mg/kgPrednisolone 1mg/kg
And whether quick response after mild And whether quick response after mild croupcroup

MethodMethod
Retrospective explicit chart review of Retrospective explicit chart review of children over 1 year of age admitted to a children over 1 year of age admitted to a teaching hospitalteaching hospital
Patient demographicsPatient demographics Croup scores at AECroup scores at AE Duration of stridor at rest after steroidsDuration of stridor at rest after steroids

ResultsResults
188 cases analysed188 cases analysed Median duration at rest was 6.5 hrs, range Median duration at rest was 6.5 hrs, range
0.5 hrs- 82 hrs0.5 hrs- 82 hrs Patients with low score at AE recovered Patients with low score at AE recovered
quicker in response to steroids, early quicker in response to steroids, early discharge home.discharge home.

Amphotericin induced stridorAmphotericin induced stridor
Adverse effects reported Amphotericin BAdverse effects reported Amphotericin B DyspnoeaDyspnoea TachypnoeaTachypnoea BronchospasmBronchospasm HaemoptysisHaemoptysis hypoxiahypoxia

ObjectiveObjective
To review mechanism of action and To review mechanism of action and reports of respiratory adverse effects for reports of respiratory adverse effects for Amphotericin B, the liposomal Amphotericin B, the liposomal preparations for Amphotericin B and the preparations for Amphotericin B and the differential diagnosis of stridordifferential diagnosis of stridor
Medline search 1966 – 2002 looking for Medline search 1966 – 2002 looking for possible mechanisms and possible mechanisms and immunoregulatory effects of Ampho Bimmunoregulatory effects of Ampho B

ResultsResults
Amphotericin B shows increase in tumour Amphotericin B shows increase in tumour necrosis factor alpha (TNF alpha) necrosis factor alpha (TNF alpha) concentrations in macrophages.concentrations in macrophages.
Induces prostaglandin E2 synthesis, Induces prostaglandin E2 synthesis, increasing production of interleukin1 beta increasing production of interleukin1 beta in mononuclear cellsin mononuclear cells

ConclusionConclusion
Amphotericin B induces production of TNF Amphotericin B induces production of TNF alpha, interferon gamma and interleukin 1 alpha, interferon gamma and interleukin 1 beta which have toxic effects.beta which have toxic effects.

Medicines for childrenMedicines for children
Test dose infused over 30 mins – 100mcgTest dose infused over 30 mins – 100mcg Renal impairmentRenal impairment Low serum pott, mag, phosLow serum pott, mag, phos Lft’sLft’s arrhythmiasarrhythmias Pulmonary reactions if Amph and Pulmonary reactions if Amph and
leucocyte Tx.leucocyte Tx.

Subglottic stenosis, 1-8%Subglottic stenosis, 1-8%
TracheostomyTracheostomy
Cystic hygromaCystic hygroma
HaemangiomaHaemangioma

Case history 1Case history 1
Girl, 3.55kg, LSCS, 37/40Girl, 3.55kg, LSCS, 37/40 TTN, ett, ventilationTTN, ett, ventilation Day 3, pyrexia, measle like Day 3, pyrexia, measle like
exanthema,thrombocytopeniaexanthema,thrombocytopenia Diagnosis, toxic shock syndrome. Ax.Diagnosis, toxic shock syndrome. Ax. Day 5 yellow tracheal secretions, glottis Day 5 yellow tracheal secretions, glottis
red, not swollenred, not swollen MRSA, Day 13 extubated, stridor.MRSA, Day 13 extubated, stridor.

Case history 2Case history 2
Baby girl, 2.790kg, LSCS, 37/40.Baby girl, 2.790kg, LSCS, 37/40. At 3hrs, ett,ventilated, TTNAt 3hrs, ett,ventilated, TTN Day 3, pyrexiaDay 3, pyrexia Day 6 yellow secretions, epiglottis red, not Day 6 yellow secretions, epiglottis red, not
swollenswollen Diagnosis: laryngotracheitis, MRSADiagnosis: laryngotracheitis, MRSA TracheostomyTracheostomy

TracheomalaciaTracheomalacia
Normal struts of cartilage which maintain Normal struts of cartilage which maintain the trachea patent are either malformed the trachea patent are either malformed (OA,TOF) or compressed by vessels.(OA,TOF) or compressed by vessels.
Collapse of tracheaCollapse of trachea
Apnoea, resus (bag and mask opens Apnoea, resus (bag and mask opens airway)airway)

Where site of fistula repair in TOF:Where site of fistula repair in TOF:
Supporting cartilage framework not fully Supporting cartilage framework not fully formed, floppy airwayformed, floppy airway
Specialised lining cells (goblet and cilia) are Specialised lining cells (goblet and cilia) are replaced by squamous cells, less effective replaced by squamous cells, less effective in protecting airway.in protecting airway.

Severe tracheomalaciaSevere tracheomalacia
4-6mths age4-6mths age Excessive wheezeExcessive wheeze CyanosisCyanosis Particularly during feedParticularly during feed Near death episodesNear death episodes Trachea collapses, no air can pass Trachea collapses, no air can pass
throughthrough

Tests for tracheomalaciaTests for tracheomalacia
Radiography (side on)Radiography (side on) Barium mealBarium meal BronchoscopyBronchoscopy Respiratory function testsRespiratory function tests

Case history 1Case history 1
24/40, antenatal steroids 48hrs, wt 765g24/40, antenatal steroids 48hrs, wt 765g Ventilated 20 days, stridorVentilated 20 days, stridor At 100 days failure to extubate laryngo-At 100 days failure to extubate laryngo-
tracheobronchomalaciatracheobronchomalacia
90% occlusion lower trachea90% occlusion lower trachea 70% occlusion left main bronchus70% occlusion left main bronchus Unsuccessful aortapexy, cpap, tracheUnsuccessful aortapexy, cpap, trache At 18ths no malaciaAt 18ths no malacia

Case history 2Case history 2
25/40, 772g, male, hyaline membrane 25/40, 772g, male, hyaline membrane disease, curosurf x2disease, curosurf x2
Ventilated 6/52, recurrent stridorVentilated 6/52, recurrent stridor Subglottic stridor, Day 160 Subglottic stridor, Day 160
tracheobronchogram, collapse right tracheobronchogram, collapse right bronchusbronchus

Case history 3Case history 3
34/40, infant of diabetic mum, bw 1162g34/40, infant of diabetic mum, bw 1162g Moderate severe RDS, curosurf, vent 21/7Moderate severe RDS, curosurf, vent 21/7 Oxygen desats at one year, vented again.Oxygen desats at one year, vented again. Tracheobronchogram at 16mths, severe Tracheobronchogram at 16mths, severe
malacia of left main bronchusmalacia of left main bronchus
Cpap via tracheostomy.Cpap via tracheostomy.

Compressive disorderCompressive disorder
Double aortic arch, (embryiological)Double aortic arch, (embryiological) Compresses right main bronchus and Compresses right main bronchus and
lower trachealower trachea
This condition is result of failure of This condition is result of failure of posterior cricoid lamina and trachea posterior cricoid lamina and trachea oesophageal septum to fuseoesophageal septum to fuse
MRIMRI

Pulmonary artery slingPulmonary artery sling

CCAM CCAM
Chin and Tang (1949)Chin and Tang (1949) Proliferation of cysts resembling Proliferation of cysts resembling
bronchiolesbronchioles 25% of all lung lesions25% of all lung lesions

Pathogenesis and pathophysiologic Pathogenesis and pathophysiologic featuresfeatures
Focal arrest of fetal lung development Focal arrest of fetal lung development before 7before 7thth week development week development
Secondary to pulmonary insultsSecondary to pulmonary insults 4-26% associated with other congenital 4-26% associated with other congenital
anomaliesanomalies

Types of CCAMTypes of CCAM
Type 1. 2-10cm diameter, large cysts Type 1. 2-10cm diameter, large cysts accompanied by small cystsaccompanied by small cysts
Type 2. small relatively uniform cysts Type 2. small relatively uniform cysts resembling bronchioles, 0.5cm-2cm sizeresembling bronchioles, 0.5cm-2cm size
Type 3. Microscopic cysts, solidType 3. Microscopic cysts, solid
Type 2/3 assoc with pulmonary Type 2/3 assoc with pulmonary sequestration (arterial supply)sequestration (arterial supply)

Differential diagnosisDifferential diagnosis
Absence of bronchial cartilageAbsence of bronchial cartilage Absence of bronchial tubular glandsAbsence of bronchial tubular glands Presence of tall columnar mucus Presence of tall columnar mucus
epitheliumepithelium Over production of terminal bronchiolar Over production of terminal bronchiolar
structures without alveolistructures without alveoli Massive enlargement of the affected lobe Massive enlargement of the affected lobe
displacing other structures.displacing other structures.

Cystic adenomatoid malformationCystic adenomatoid malformation
Single or multi cystic mass in pulmonary Single or multi cystic mass in pulmonary tissue.tissue.
Cysts are lined with cuboid and columnar Cysts are lined with cuboid and columnar cells which appear as alimentary tract cells which appear as alimentary tract originorigin
Affects lower lobesAffects lower lobes Complete removal to avoid malignancy in Complete removal to avoid malignancy in
futurefuture

Mortality / morbidityMortality / morbidity
1: 25,000-35,000 Canada1: 25,000-35,000 Canada Type 3 extensiveType 3 extensive 56% regress when identified in utero56% regress when identified in utero Equal sexesEqual sexes

Congenital diaphragmatic herniaCongenital diaphragmatic hernia
1:3500 – 5000 births1:3500 – 5000 births Failure of closure of the pleuroperitoneal Failure of closure of the pleuroperitoneal
at 8-10 weekat 8-10 week Abdominal contents in chestAbdominal contents in chest Liver develops in chest, comes down to Liver develops in chest, comes down to
abdo cavity- lung hypoplasiaabdo cavity- lung hypoplasia

20% right sided20% right sided 1-4% bilateral1-4% bilateral 80% left sided80% left sided

Medical managementMedical management Surgery when conventional ventilationSurgery when conventional ventilation Pulmonary hypoplasiaPulmonary hypoplasia Hypoxia, hypercarbiaHypoxia, hypercarbia Pulmonary vasoconstrictionPulmonary vasoconstriction Pulmonary hypertensionPulmonary hypertension Poor gas exchange, right to left shunt.Poor gas exchange, right to left shunt.

Long term outcomesLong term outcomes
Recurrent chest infectionsRecurrent chest infections Gastro oesophageal refluxGastro oesophageal reflux Pulmonary hypertensionPulmonary hypertension Developmental delayDevelopmental delay DeafnessDeafness Recurrence of herniaRecurrence of hernia

Congenital lobar emphysemaCongenital lobar emphysema
UncommonUncommon Life threateningLife threatening Respiratory distress due to hyperinflationRespiratory distress due to hyperinflation
of the affected lobe, resulting in total of the affected lobe, resulting in total collapse of normal lung collapse of normal lung
Unilobar alveoli distensionUnilobar alveoli distension

StudyStudy
1995-2002 retrospective chart review1995-2002 retrospective chart review 5 boys, 3 girls with clinical and radiological 5 boys, 3 girls with clinical and radiological
diagnosis of CLEdiagnosis of CLE Age range 11 days- 10 yearsAge range 11 days- 10 years Five patients lobectomy, 3 medical Five patients lobectomy, 3 medical
managementmanagement

Like father like sonLike father like son Mothers and daughtersMothers and daughters InheritedInherited Antenatal scanAntenatal scan Decrease with ongoing pregnancyDecrease with ongoing pregnancy However, air trapping and RDS and need However, air trapping and RDS and need
lobectomy in somelobectomy in some Associated with congenital heart diseaseAssociated with congenital heart disease

ReferencesReferences Ankers D, Sajjad N, Green P, McPartland J (2010). Antenatal management Ankers D, Sajjad N, Green P, McPartland J (2010). Antenatal management
of pulmonary hyperplasia (congenital cystic adenomatoid malformation). of pulmonary hyperplasia (congenital cystic adenomatoid malformation). BMJ Case Reports. BMJ Case Reports. doi:10.1136/bcr.01.2010.2679doi:10.1136/bcr.01.2010.2679
Calvert J and Lakhoo K (2007). Antenatally suspected congenital cystic Calvert J and Lakhoo K (2007). Antenatally suspected congenital cystic adenomatoid malformation of the lung : postnatal investigation and timing of adenomatoid malformation of the lung : postnatal investigation and timing of surgery. surgery. Journal of Pediatric Surgery. Journal of Pediatric Surgery. Vol 42, Iss 2, p411 - 414Vol 42, Iss 2, p411 - 414
Congenital Cystic Adenomatoid Malformation.Congenital Cystic Adenomatoid Malformation. http://pediatrics.uchicago.edu/chiefs/AMreport/CCAM_files/outline.htmhttp://pediatrics.uchicago.edu/chiefs/AMreport/CCAM_files/outline.htm Mandell G (2003). Congenital Cystic Adenomatoid Malformation.Mandell G (2003). Congenital Cystic Adenomatoid Malformation. EE Medicine.Medicine. http://www.emedicine.com/radio/topic 186.htmhttp://www.emedicine.com/radio/topic 186.htm Marshall K, Blane C, Teitelbaum D, Leevuren K (2000).Marshall K, Blane C, Teitelbaum D, Leevuren K (2000). Congenital Cystic Adenomatoid Malformation. Impact of PrenatalCongenital Cystic Adenomatoid Malformation. Impact of Prenatal Diagnosis and Changing Strategies in the Treatment of the AsymptomaticDiagnosis and Changing Strategies in the Treatment of the Asymptomatic Patient. Patient. American Journal of Roentgenology.American Journal of Roentgenology. 175:1551-1554 175:1551-1554 Samuel M, Burge D (1999). Management of Ante-natally Diagnosed Samuel M, Burge D (1999). Management of Ante-natally Diagnosed
Pulmonary Sequestration Associated with Congenital Cystic Adenomatoid Pulmonary Sequestration Associated with Congenital Cystic Adenomatoid Malformation. Malformation. Thorax.Thorax. 54:701-70654:701-706
West D, Nicholson A, Colquhoun I, Pollock J (2006). Bronchioloaveolar West D, Nicholson A, Colquhoun I, Pollock J (2006). Bronchioloaveolar carcinoma in congenital cystic adenomatoid malformation of lung. carcinoma in congenital cystic adenomatoid malformation of lung. Annals of Annals of Thoracic Surgery. Thoracic Surgery. 83 : 687 - 68983 : 687 - 689