-
7/30/2019 Respiratory 3 Rd Handout Pg 56- 69
1/16
VENTILATOR ASSESSMENT
The following should be included in your initial assessment and
documentation of aventilated patient:
ETT size, length at lip or teeth (teeth is frequently better in
trauma patientsdue to swelling of lips), position in mouth, and
date of insertion
If a patient is trached, note the size of the trach, date of
insertion, stomacondition, presence of oozing around site; dressing
condition
Cuff Pressure (< 25 mm Hg is optimal)
Vent parameters - both set and measured
Breathing: Spontaneous resps over ventilator?
Tolerance (synchrony, work of breathing, comfort)
Suctioning: Colour, amount, viscosity
Alarms
Hourly assessments include all values:
Peak Pressures
Resp Rate any spontaneous breaths?
Tidal Volumes
Minute Volumes
WOB
Dont accept CIS data from the ventilator unless you have
reviewed it. Its veryimportant that you are aware of changing
measurements so that you can interveneas appropriate. Look for
changes up or down and relate these to the patientscondition.
Recognize how these changes may affect his ventilation or
oxygenation you may need to do an ABG.
When you change the ETT position you need to document where you
moved it toand whether it remains at the same marker level at the
lip/teeth. Before retapingthe tube you must listen for equal
bilateral breath sounds to ensure you have notdislodged it. When
you do your trach dressing you need to document how youcleaned it
and what the site looks like, and if you took any additional
measures (ienotified the MD if it appears infected).
Additional items to note during your assessment:
How much dead space is there? Can the tube be trimmed? Can the
cathetermount be shrunk?
Is the patient trying to initiate his own breaths but
unsuccessful? Have yourRT look at the sensitivity level and adjust
if necessary or, if the patient is notsupposed to be breathing,
consider increased sedation
Graphics: Use this workbook and study your graphics daily to see
if you canrecognize issues with ventilation. Ive placed a
Ventilator Graphics Handoutin your shared folder.
RECRUITMENT MANOEUVERS (RMs)
-
7/30/2019 Respiratory 3 Rd Handout Pg 56- 69
2/16
Recruitment manoeuvres are done by creating a sustained increase
in pressure as ameans of recruiting the collapsed alveoli.
Recruitment manoeuvres are doctor-ordered and done by the doctor or
the RT at this time.
There are 3 parts to a recruitment manoeuvre:
1. Inflation: this step helps to open as much of the lung as
possible. Its done byincreasing the pressures for a sustained
period. This can be done a few ways:
a. Sustained CPAP of 30-40 for about 40 secondsb. Inspiratory
Hold: While patient is inhaling you hold the air in, delaying
exhalation and thereby keeping the alveoli expanded for a bit
longerc. Set the pressure to 20 above the PEEP for 10-12 breaths,
then increase
PEEP so Peak Pressure is 40 for about 40-60 secondsd. Increase
PEEP by 5 for several minutes
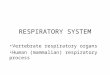
2. Deflation: By looking at the graphs, this helps you determine
the pressurewhere most units re-collapse
A= Point of collapse of alveoliduring
ExhalationB= Point of opening of alveoli
duringInspiration
3. Re-inflation: You can now choose your new PEEP settings based
on the above-
measured deflation value
RMs should be done at least once per shift. However, good
ventilation therapyincludes doing a recruitment manoeuvre every
time PEEP is broken, followingsuction, or following a leak in the
system.Caution: This increases intrathoracic pressure for up to 60
seconds so beware ofbarotrauma.
-
7/30/2019 Respiratory 3 Rd Handout Pg 56- 69
3/16
In summary, study the ventilator daily. Look at the ventilator
readings regularlyand with each nursing intervention to see how
your patient reacts. Interpret yourABGs and decide how you would
adjust the ventilator, and then see if it coincideswith what the RT
or the MD does. Does this change make sense based on the
biggerpicture? Remember, you are the only one who will know that
because you are theonly one at the beside for 12 hours. Ventilation
affects all other systems andinfluences the speed of recovery. By
ensuring you are optimizing ventilation youcan help your patient
recover faster and avoid complications. Understanding
ventilation is the difference between an average ICU nurse and
an exceptional one.
WEANING
Weaning from ventilation should be done as soon as possible to
avoidcomplications. There are certain basic criteria for
weaning:
1. Reason for Intubation: Has the original reason for intubation
resolved?Always consider why the patient was intubated in the first
place. It theseissues are still present, weaning is not
recommended.
2. Measurable Criteria: There are certain measurable parameters
one canlook at to determine readiness for weaning. Some of these
are directly
related to ventilation measurements while others relate to a
patients overallcondition. For instance:
CLINICAL PARAMETERS:
Acid-base balanceAnemiaTempCardiac issuesElectrolyte balance
Exercise tolerance(up in chair)Fluid balancePain
Psychological issuesSleep deprivationInfectionGlycemic
stabilityLevel of
ConsciousnessAbility to protectand clear airway
VENTILATION PARAMETERS:
-
7/30/2019 Respiratory 3 Rd Handout Pg 56- 69
4/16
Minute Volume