Embed Size (px)
Citation preview

Research ArticleTrunk and Shoulder Kinematic and Kinetic andElectromyographic Adaptations to SlopeIncrease during Motorized Treadmill Propulsion amongManual Wheelchair Users with a Spinal Cord Injury
Dany Gagnon12 Annie-Claude Babineau12 Audrey Champagne12
Guillaume Desroches12 and Rachid Aissaoui3
1School of Rehabilitation Universite de Montreal Montreal QC Canada H3C 3J72Pathokinesiology Laboratory Centre for Interdisciplinary Research in Rehabilitation of Greater MontrealInstitut de Readaptation Gingras-Lindsay-de-Montreal 6300 Darlington Montreal QC Canada H3S 2J43Department of Automated Production Engineering Ecole de Technologie Superieure Montreal QC Canada H3C 1K3
Correspondence should be addressed to Dany Gagnon danygagnon2umontrealca
Received 15 May 2014 Revised 15 August 2014 Accepted 19 August 2014
Academic Editor Dan Ding
Copyright copy 2015 Dany Gagnon et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
The main objective was to quantify the effects of five different slopes on trunk and shoulder kinematics as well as shoulderkinetic and muscular demands during manual wheelchair (MWC) propulsion on a motorized treadmill Eighteen participantswith spinal cord injury propelled their MWC at a self-selected constant speed on a motorized treadmill set at different slopes(0∘ 27∘ 36∘ 48∘ and 71∘) Trunk and upper limb movements were recorded with a motion analysis system Net shoulder jointmoments were computed with the forces applied to the handrims measured with an instrumented wheel To quantify musculardemand the electromyographic activity (EMG) of the pectoralis major (clavicular and sternal portions) and deltoid (anterior andposterior fibers) was recorded during the experimental tasks and normalized against maximum EMG values obtained during staticcontractions Overall forward trunk flexion and shoulder flexion increased as the slope became steeper whereas shoulder flexionadduction and internal rotation moments along with the muscular demand also increased as the slope became steeper The resultsconfirm that forward trunk flexion and shoulder flexion movement amplitudes along with shoulder mechanical and musculardemands generally increase when the slope of the treadmill increases despite some similarities between the 27∘ to 36∘ and 36∘ to48∘ slope increments
1 Introduction
There has been a growing interest in motorized treadmillmanual wheelchair (MWC) propulsion in recent years inrehabilitation research environments and to a lesser extentin clinical practice since it seems to closely duplicateoverground MWC requirements [1] Motorized treadmillMWC propulsion also allows for propulsion in a restrictedspace during short (eg high intensity interval training) andprolonged (eg cardiorespiratory fitness training) periods oftime at different speed or slope parameters Moreover unlike
propulsion on a roller ergometer or a dynamometer MWCpropulsion on a motorized treadmill allows for greater free-dom of MWC movements and some inertial effect exposurelinked to the accelerationdeceleration of the wheelchair andhead-trunk-upper limb segments Hence motorized tread-mill MWC propulsion is a promising therapeutic alternativefounded on the principle of repetitive task-specific trainingand anticipated sensorimotor adaptations The quality andquantity of evidence currently available on motorized MWCpropulsion do not inform rehabilitation professionals abouthow to vary parameters that can be easily modulated (eg
Hindawi Publishing CorporationBioMed Research InternationalVolume 2015 Article ID 636319 15 pageshttpdxdoiorg1011552015636319
2 BioMed Research International
the speed or slope of the treadmill) and their effects duringmotorized treadmill MWC propulsion Stronger evidence isneeded to optimize assessment and training protocols
Propelling aMWCup slopes on amotorized treadmill hasbeen found to increase upper limb demand in a few recentstudies Richter et al [2] found among MWC users with aspinal cord injury (SCI) propelling at a self-selected velocityon amotorized treadmill that the speed was about 15 and 27times slower when pushing up 3∘ and 6∘ slopes respectivelyin comparison with the level surface (0∘ slope) Additionallythey also reported that the peak total force at the handrimwas about 17 and 22 times higher when pushing up 3∘ and6∘ slopes respectively in comparison with the level surface(0∘ slope) despite the reduced treadmill speed Yang et al[3] found among MWC users with a SCI propelling at animposed steady speed of 09ms on a motorized treadmillthat peak shoulder flexion increased by 9∘ while the total andtangential forces applied at the handrim were about 209 and238 times higher when pushing up a 3∘ slope (approximatelya 1 20 ratio) in comparison with the level surface whereasthe mechanical efficiency was only found to be 11 timeshigher More recently Gagnon et al [4] found among MWCusers with a SCI each propelling at a self-selected steadyspeed on a motorized treadmill up slopes set at 0∘ 27∘ 36∘48∘ and 71∘ that the total and tangential forces appliedat the handrim were at least 2 times greater as the slopebecame progressively steeper The greatest change observedwas between 0∘ and 27∘ while similarities were observedbetween 27∘ and 36∘ Such differences also support the needto gain a better understanding of the effects of steeper slopeson trunk and shoulder kinematics shoulder kinetics andshoulder muscular demand during uphill propulsion on atreadmill set at a steady speed among a group of experiencedMWC users
In addition few studies have investigated the effects ofvarying slopes during overground MWC propulsion overthe past decade Among those Chow et al [5] investigatedthe effects of various slopes (ie 0∘ 2∘ 4∘ 6∘ 8∘ 10∘ and12∘) on trunk kinematics handrim kinetics and upper limband upper trunk muscular demand among MWC users witha spinal cord injury Overall forward trunk flexion andmuscular demand (ie triceps brachii anterior deltoid andpectoralis major) were found to progressively increase asthe slope became steeper van Drongelen et al [6] com-pared shoulder net joint moments between overground leveland uphill (ie 3∘ slope) propulsion among MWC userswith paraplegia and tetraplegia The resultant net shouldermoments were about 2 times higher during uphill comparedto overground level MWC propulsion Arabi et al [7] com-pared relative mechanical demand during uphill propulsionacross three slopes (ie 27∘ 48∘ and 57∘) among a group ofable-bodied individuals who used a MWC They confirmedthat the relative mechanical demand significantly increasedas the slope became steeper and reached 161 257 and311 of their maximum isometric voluntary force generatingcapability for the three slopes tested respectively Last Kuliget al [8] compared shoulder net joint moments between leveloverground and uphill (slope = 47∘) MWC propulsion inindividuals with paraplegia They showed that the peak net
shoulder flexion adduction and internal rotation momentswere 22 22 and 27 times greater respectively whenascending a slope compared to level overground wheelchairpropulsion
The aim of this study was to quantify the trunk and non-dominant shoulder kinematic changes along with the non-dominant shoulder joint moments and electromyographicchanges during MWC propulsion on a motorized treadmillset at a self-selected natural speed on five different slopes (ie0∘ 27∘ 36∘ 48∘ and 71∘) It was expected that the nondom-inant shoulder and trunk range of motion and nondominantshoulder jointmoments andmuscle electromyographic activ-ity would gradually and significantly increase with each slopeincrement while the speed remained constant
2 Material and Methods
21 Description of Participants A convenience sample of 17men and 1 woman who sustained a SCI (American SpinalInjuryAssociation Impairment Scale [9] (AIS) =A B C orD)volunteered to participate in this study (Table 1) Participantswere included in the study if they had sustained a SCI atleast three months before the study had been dischargedfrom initial intensive inpatient rehabilitation were living inthe community and used their MWC for at least 4 hoursper day Participants also had to master basic and advancedwheelchair skills including the capability to propel up a 9-metre long access ramp meeting building code standardsin the province of Quebec in Canada (ie maximum slopeof 1 12 for slopes of a maximum length of 9 metres)[10] Participants were excluded if they presented associatedneurological conditions musculoskeletal impairmentspaincardiorespiratoryvascular conditions or any other impair-ments or disabilities that might have interfered with theperformance or safety of the experimental tasks The self-reported Wheelchair Userrsquos Shoulder Pain Index (WUSPI)questionnaire [11 12] was completed (grouprsquos mean score =089plusmn 10510) and reviewed by a physical therapist who askedspecific questions whenever pain was rated as interferingwith the performance of wheelchair mobility to further verifythat pain will not limit their ability to specifically com-plete the experimental tasks During a telephone interviewwith the potential participants the rehabilitation researchcoordinator reviewed the inclusion and exclusion criteriato determine eligibility before scheduling the clinical andlaboratory assessments All participants gave their writtenconsent to participate in the study after being informed ofthe objectives and nature of their participation in the studyThe Research Ethics Committee of the Centre for Interdisci-plinaryResearch inRehabilitation ofGreaterMontreal (CRIR715-0312) approved the present study
22 Clinical Evaluation Each participant underwent a clini-cal assessment completed by a physical therapist in order tocollect their personal characteristics measure their anthro-pometric parameters (height weight length and circumfer-ence of body segments) characterize the severity of the sen-sory and motor impairments (ASIA Impairment Scale [13])
BioMed Research International 3
Table 1 Description of participants
Participants Gender Ageyears
Heightm
Masskg
Time sinceinjury years
ASIAlowast WUSPIlowast
Neuro-logicallevel
AISlowast Sensory224
Motor100
Mean10
Propulsion10min10
Slope10
1 M 443 184 803 106 T7 A 117 50 019 00 002 M 464 170 802 46 T10 B 140 50 068 01 053 M 322 192 959 53 T10 A 140 50 000 00 004 M 358 180 771 118 T6 D 194 81 125 19 225 M 332 195 723 78 T12 C 162 56 019 00 006 M 526 177 1089 187 T9 A 132 50 114 24 347 M 599 188 998 50 T10 A 140 50 034 04 228 M 440 172 684 221 T4 B 183 35 007 09 009 M 412 178 727 61 C7 C 56 44 123 27 2710 M 284 185 666 106 T12 A 154 50 063 38 1911 M 390 176 1018 28 T10 A 72 50 365 55 6812 M 491 170 768 44 T7 A 88 52 097 15 2413 M 557 180 1031 49 T3 A 88 50 031 18 1614 M 328 175 619 89 T4 A 95 50 010 04 0415 F 281 165 475 48 T11 A 148 50 020 20 1016 M 330 165 665 53 T6 A 53 50 010 00 0317 M 527 173 782 89 T12 B 172 63 312 26 4818 M 258 183 592 49 T7 A 112 50 188 47 26Mean 408 178 787 82 1248 517 089 17 18SD 103 009 170 51 423 90 105 17 19lowastGender M = male F = female AIS = ASIA Impairment Scale A = no motor or sensory function is preserved below the neurological level B = sensoryfunction is preserved but motor function is not preserved below the neurological level C =Motor function is preserved below the neurological level and morethan half of key muscle functions below the single neurological level of injury have a muscle grade less than 35 and D =Motor Incomplete Motor function ispreserved below the neurological level and at least half of key muscle functions below the neurological levle of injury have a muscle grade gt or = 35 ASIA =American Spinal Injury Association WUSPI = Wheelchair Userrsquos Shoulder Pain Index
confirm the absence of debilitating UL musculoskeletalimpairment (ie WUSPI [11 12] UL joint ranges of motionUL staticmanualmuscle testing) and confirmULnondom-inance [9]
23 Motorized Treadmill Wheelchair Propulsion At the startof the laboratory assessment each participant was givena five-minute familiarization period of motorized tread-mill propulsion at various slopes that differed from thoseinvestigated in the present study during which rest peri-ods were allowed to avoid fatigue The motorized dualbelt instrumented treadmill (Bertec Corporation ColumbusOhio United States) (width = 084m length = 184m) wasadapted for safe MWC propulsion The MWC was anchoredwith elastic bands to a bilateral frictionless gliding safetysystem preventing excessive antero-posterior and rotationalmovements of theMWC (Figure 1)The imposed speed of thetreadmill was adjusted for each participant to mimic the self-selected natural propulsion speed measured during a timedperformance-based 20 meter MWC propulsion test This lasttest was performed three times with a two-minute rest takenbetween trials to compute the self-selected natural propulsionspeed Thereafter each participant first propelled their own
MWC on the motorized treadmill with a level ground (0∘)and then randomly at four different slopes 27∘ 36∘ 48∘and 71∘ reflecting an increase from one unit of height to20 16 12 and 8 units of length respectively For each angletested two trials lasting a maximum of one minute (ie20 consecutive pushes) and separated by a two-minute restperiod were recorded During each trial the last 10 completeconsecutive propulsion cycles recordedwere used to computethe measurements of interest (ie trunk and shoulder kine-matics shoulder kinetics and shoulder muscular demand)and were essential to confirm the successful completion foreach slope tested (ie two trialsslope) This study designwas selected to minimize systematic errors related to thetesting (eg learning) and temporarymaturation effects (egfatigue) associated with the experimental protocol and toconclude that the findings of the present study do not resultfrom these potential threats to internal validity Participantsrated their perceived nondominant localized UL effort usinga 10 cm visual analog scale ranging from ldquono effortrdquo (0 cm) toldquomaximum effortrdquo (10 cm) during the rest periods
24 Trunk and Shoulder Kinematics To capture the 3Dmovements of the trunk the nondominant UL and
4 BioMed Research International
(a) (b) (c)
Figure 1 Illustration of three slopes tested during motorized treadmill MWC propulsion (a) 0∘ slope (b) 36∘ slope and (c) 71∘ slope
the MWC a total of 27 skin-fixed light-emitting diodes(LEDs) were placed on specific anatomical landmarks whilefour LEDs were fixed to the MWC frame [14] The 3Dcoordinates of each LED within the laboratory coordinatesystem were collected at 30Hz with a motion capture systemincorporating four synchronised camera units (Optotrack3020 and Optotrack Certus Northern Digital Inc WaterlooOntario Canada httpwwwndigitalcom) Supplementarybony landmarks wheelchair and treadmill reference pointswere digitised to determine principal axes of segments andlocate articular joint centres for the trunk and nondomi-nant UL wheelchair position and treadmill slope Beforeinitiating the experimental tasks three abduction-adductionand three flexion-extension active movements were recordedto locate the shoulder articular centre with respect to thescapula using a quadratic sphere fitting procedure [15 16] Allmarker trajectories were visually inspected and interpolatedwhen coordinates were missing using a linear or a cubicspline method The marker trajectories were then filteredusing a 4th order zero-lag Butterworth filter with a cutofffrequency set at 6Hz The recommendations formulated bythe International Society of Biomechanics [17] were used todetermine segmental coordinate systems (head trunk armsforearms and hand) Relative motion between the humerusand clavicle used as a surrogate rigid segment for the scapulathat articulates with the humerus [17] was computed using aZX1015840Y10158401015840 cardanic rotation sequence to avoid gimbal lock andto interpret reconstructed shoulder movements according tothree anatomical movements commonly described in clinicalpractice (ie flexionextension abductionadduction inter-nal and external rotations) [18] The relative trunk forwardinclination angle (ie forward trunk flexion) was computedas the motion of the vertical axis of the trunk defined by
a unit vector created with the midpoint between the eighththoracic vertebra and the xiphoid process to the midpointbetween the seventh cervical vertebra and the sternal notchwith respect to the vertical axis of the laboratory coordinatesystem For the trunk forward flexionextension and theshoulder flexionextension adductionadduction and inter-nalexternal rotation the minimal and maximal movementsalong with their total excursion were the main outcomemeasures
25 Handrim Kinetics Each participantrsquos MWC wasequipped bilaterally with 2410158401015840 or 2610158401015840 instrumented wheels(SmartWheel (SmartWheel Out-Front (formerly ThreeRivers Holdings LLC) Mesa Arizona United Stateshttpwwwout-frontcom)) to measure the three dimen-sional components of the total force applied at the handrimduring MWC propulsion at a sampling frequency of 240Hz[19] While these instrumented wheels did not alter axleposition or other rear wheel spatial characteristics (egorientation and diameter of the handrim) they slightlyincreased wheelchair width and weight (48 kginstrumentedwheel) and may have affected rolling resistance (ieurethane tire) Three dimensional handrim kinetic datawere filtered with a 4th order Butterworth filter anda cutoff frequency of 20Hz and then downsampled to30Hz to fit the kinematic data using a custom MATLAB(MATLAB MathWorks Natick Massachusetts UnitedStates httpwwwmathworkscom) routine
26 Shoulder Kinetics Shoulder net joint moments werecomputed using an inverse dynamic method [20] The dataentered into a custom-made MATLAB algorithm included
BioMed Research International 5
the anthropometric characteristics as well as the UL kine-matics and the pushrim kinetics with respect to the labcoordinate system Shoulder net joint moments were thenexpressed in the same coordinate system used to expressshoulder joint kinematics and normalized against the bodymass of each participant In fact moderate to high associ-ations were found between body mass and mean and peakshoulder net joint moments when propelling with no slope(119903 = 0554 and 0577) and with slopes of varying degrees(119903 = 0713 to 0809) The peak and mean shoulder net jointmoments in the sagittal frontal and transverse plane werethe main outcome measures
27 Shoulder Muscular Demand The electromyographicactivity of the anterior and posterior portions of the del-toid along with the clavicular and sternal heads of thepectoralis major was recorded at the nondominant upperextremity at a sampling frequency of 1200Hz using a portabletelemetric system (NORAXON USA Inc Scottsdale Ari-zona Telemyo 900) Skin preparation and the placementof the surface electrodes (BlueSensor M AMBU BallerupDanmark) (AgAgCl sensor ndash132mm2 active surface area)were made in accordance with SENIAM recommendations(refer to httpwwwseniamorg) Following baseline noiseremoval all EMG signals recorded were visually inspectedbefore being filtered with a 4th order zero-lag Butterworthbandpass filter with low and high cut-off frequencies set at30 and 500Hz respectively Thereafter EMG patterns werefull-wave rectified and filtered with a 6Hz low-pass filterto generate EMG linear envelopes for each muscle studiedThe muscular utilization ratio (MUR ()) was calculatedfor each muscle studied by normalizing the amplitude ofthe EMG signals recorded during the experimental tasksagainst the peak EMG signal recorded over a 05 secondperiod during one of the two static maximum voluntarycontractions (MVC) Muscle-specific manual resistance wasapplied by a trained physiotherapist to generate the MVCswhile participants remained seated in their own wheelchairMeanwhile another research associate manually providedadditional trunk and wheelchair stability to participants Foreach muscle studied the peak and mean MURs as well as anindicator of muscle work (IMW) were calculated using theintegral of the MUR data were the main outcome measuresAll EMG signal processing was performed digitally using acustom-developed MATLAB algorithm
28 Statistical Analyses Descriptive statistics (mean plusmn SD)were calculated for the demographic and clinical character-istics of all participants as well as for the kinematic kineticand muscular demand outcome measures For these lastoutcome measures 10 propulsion cycles were averaged pertrial resulting in a total of 20 propulsion cycles for eachslope tested The kinematic kinetic and muscular demanddata recorded during the push phase of each cycle analyzedwere also time-normalized over 100 (ie 100 data points)to generate a profile for each participant and a mean groupprofile Shapiro-Wilk tests confirmed that the kinematickinetic and electromyographic outcome measures for all
slopes tested were normally distributed and justified the useof parametric statistical tests One-way repeated-measureanalyses of variance (ANOVA) with one within-subjectsfactor (slopes of 0∘ 27∘ 36∘ 48∘ and 71∘) using a generallinear model was used to determine the effect of the slopeson the kinematic and kinetic and electromyographic outcomemeasures and an eta-squared value was used to confirmif the proportion of the total variability attributable to theslope factor (ie effect size) was small (gt002) moderate(gt013) or large (gt026) Whenever an ANOVA revealedsignificant differences (main effect 119875 lt 005) after the resultof the Mauchlyrsquos test of sphericity of the covariance matrixwas taken into consideration Studentrsquos 119905-tests for pairedsamples were computed (post hoc tests) with a Bonferronicorrection setting the significance level at 119875 le 00125(119875 le 0054 pairwise comparisons) as a result of thefour possible slope increments (ie 0∘ to 27∘ 27∘ to 36∘36∘ to 48∘ and 48∘ to 71∘) All statistical analyses wereperformed with SPSS Statistics 170 software for WindowsNote that the kinematic and electromyographic data wereonly collected and computed at the nondominant UL sincequasi-symmetrical ULmovement strategies and efforts wereassumed in order to safely propel on a linear trajectory onthe motorized treadmill [21] and since the nondominant ULstrength generating capability is generally weaker than theone at the dominant UL possibly resulting in higher relativedemand at the nondominant UL during the performance ofa symmetrical functional task
3 Results
31 Completion Rate At a mean natural and constant self-selected propulsion speed of 117 plusmn 018ms [min = 091msmax = 165ms] all participants (completion rate = 100)were able to propel themselves on the 0∘ slope and up the27∘ slope (Table 2)The completion rate reached 889 (119873 =1618 participants) 778 (119873 = 1418 participants) and556 (119873 = 1018 participants) for the 36∘ 48∘ and 71∘slopes respectively (Table 2)
32 Temporal Parameters Table 3 summarizes the meanduration of the push and recovery phases and the totalduration of a propulsion cycle in seconds for the differenttreadmill slopes The average durations of the push phasewere similar for all tested slopes (ANOVA 119875 = 0267)whereas the average duration of the recovery phase declinedas the slope became steeper (post hoc tests 119875 le 0043) Thetotal duration significantly decreased as the slope becamesteeper (post hoc tests 119875 le 0001) except during the 27∘ to36∘ slope increment that remained similar
33 Trunk and Shoulder Kinematics The trunk and shouldermovement patterns are illustrated in Figures 2(a) 2(b) 2(c)and 2(d) whereas the minimum maximum and excur-sion of the trunk and shoulder movement amplitudes aresummarized in Table 4 The slopes of the treadmill signifi-cantly influenced most minimum maximum and excursiontrunk and shoulder movement amplitudes At the trunk all
6 BioMed Research International
Table 2 Description of self-selected comfortable propulsion speed experimental tasks completed and rate of perceived exertion
Participants Self-selected speed (ms) Slopes Rate of perceived exertion (10)0∘ 27∘ 36∘ 48∘ 71∘ 0∘ 27∘ 36∘ 48∘ 71∘
1 111 09 74 55 81 952 165 01 22 03 03 mdash3 105 13 13 39 44 714 118 08 17 37 48 785 120 17 48 25 59 796 091 30 63 77 mdash mdash7 148 09 97 mdash mdash mdash8 116 0 03 09 mdash mdash9 104 18 38 33 42 mdash10 127 0 0 0 0 011 139 10 15 33 27 3212 099 11 41 40 75 mdash13 106 42 88 mdash mdash mdash14 125 12 52 67 64 8515 103 00 06 19 36 mdash16 107 07 34 46 66 9217 106 07 62 26 65 8918 111 29 46 61 66 73Mean 117 119899 = 18 119899 = 18 119899 = 16 119899 = 14 119899 = 10 12 39 35 47 68SD 018 11 29 22 25 30
Table 3 Group average (SD) mean temporal parameter measured of the push phase measured at the nondominant handrim at the fivedifferent slopes tested
Slopes0∘ 27∘ 36∘ 48∘ 71∘
Temporal parameters (s)Push phase 048 plusmn 008 048 plusmn 008 049 plusmn 008 048 plusmn 007 048 plusmn 006Recovery phase 059 plusmn 022 027 plusmn 010 026 plusmn 009 022 plusmn 008 018 plusmn 005Total (cycle) 107 plusmn 023 075 plusmn 016 075 plusmn 014 070 plusmn 013 066 plusmn 010
minimum maximum and excursion movement amplitudessignificantly increased as the slope became steeper except forminimum and maximum values during the 27∘ to 36∘ slopeincrement that remained similar The greatest maximumforward trunk flexion (609∘) which was accompanied by thegreatest forward trunk excursion (224∘) was reached duringthe 71∘ slope At the shoulder the maximum shoulder flexionmovement amplitude significantly increased as the slopebecame steeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments The minimum maximum and excursion shoulderabduction movement amplitudes remained comparable asthe slope became steeper The minimum maximum andexcursion shoulder internal rotation movement amplitudesalso remained comparable as the slope became steeper with
the exception of the minimum and excursion values whichsignificantly increased during the 0∘ to 27∘ slope increment
34 Shoulder Kinetics The net shoulder flexion abductionand internal rotation moment patterns are illustrated inFigures 2(e) 2(f) and 2(g) while their mean and maximumvalues are summarized in Table 5 The greatest maximumshoulder moments were found during flexion across allslopes except for the 71∘ slope when the internal rotationgenerated the greatest moment All mean and maximumshouldermoments were significantly influenced by the slopesof the treadmill The mean and maximum flexion momentssignificantly improved as the slope increased except for the36∘ to 48∘ and 48∘ to 71∘ slope increments The meanadduction moments only significantly improved as the slopeincreased between 0∘ and 27∘ whereas the peak mean valueonly significantly improved as the slope increased between
BioMed Research International 7
0
10
20
30
40
50
60
70
80
Trun
k fle
xion
(+)
exte
nsio
n (minus
)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(a)
60
40
20
0
minus20
minus40
minus60
Shou
lder
flex
ion
(+)
exte
nsio
n (minus
)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(b)
0
10
20
30
40
50
60
Shou
lder
abdu
ctio
n (+
) ad
duct
ion
(minus)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(c)
0
10
20
30
40
50
60
70
0 20 40 60 80 100
Normalized time (100)Angle (∘)
Shou
lder
IR (+
) ER
(minus)
(d)
12
08
04
00
minus04
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder flexion (+) extension (minus)
(e)
04
02
00
minus02
minus04
minus06
minus08
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder abduction (+) adduction (minus)
(f)
Figure 2 Continued
8 BioMed Research International
10
08
06
04
02
00
minus02
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder IR (+) ER (minus)
(g)
Figure 2 Group averaged time-normalized profile (solid line) and standard deviation (dotted line) of the shoulder and trunk kinematics (ab c and d) and weight-normalised shoulder moments (e f and g) during the push phase for the five slopes tested at self-selected naturalspeed
the 0∘ to 27∘ 36∘ to 48∘ and 48∘ to 71∘ slope incrementsThemean and maximum internal rotation moments significantlyincreased as the slope became steeper except for the 36∘ to48∘ slope increment
35 Shoulder Muscular Demand The MUR patterns of themuscles studied are illustrated in Figure 3 while their meanand maximum values are summarized in Table 6 The meanIMWs of the muscles studied are summarized in Table 6 andillustrated in Figure 4 For allmuscles studied theirmean andmaximum MURs as well as their indicator of muscle workvalue significantly increased as the slope became steeperexcept for the posterior deltoid that remained comparablebetween the 27∘ to 36∘ slope increment
4 Discussion
This study quantified trunk and nondominant shoulderkinematic changes along with nondominant shoulder jointmoments and electromyographic changes during MWCpropulsion on a motorized treadmill set at a self-selectednatural speed on five different slopes (ie 0∘ 27∘ 36∘ 48∘and 71∘) Overall the MWC users with a SCI increasedforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increased during simulated uphillMWC propulsion on a motorized treadmill
41 Trunk and Shoulder Movement-Related Adaptations Themovement-related adaptations occurring at the trunk andshoulder partially support the hypothesis that their outcome
measures would gradually and significantly increase witheach slope increment while the speed remained constantAt the trunk the maximum forward trunk flexion and thetotal trunk excursion increased significantly as the slopebecame steeper except for the 27∘ to 36∘ slope incrementChow et al [5] obtained somewhat comparable resultsin terms of trunk kinematics although no difference wasrevealed when comparing 4∘ and 8∘ slopes This may beexplained by the fact that participants propelled at self-selected speeds that decreased progressively in their protocolas the slope increased Nonetheless the increased maximumforward trunk flexion coupled with the increased forwardtrunk excursion may allow MWC users to move their centreof mass further and faster anteriorly and to maintain itsprojection in front of the rear wheel axle in order toprevent backward tilt and falls as the slope increases Thismay also explain why maximum forward trunk flexion andforward trunk excursion became greater as the gravitationaleffects became harder to overcome with steeper slopes Thedecreasing success rate with a steeper slope may be explainedin part by the fact that some participants were classified asbeing overweight (body mass index gt 25) or class I obese(body mass index = 300ndash349) with associated abdominalobesity that limited their ability to increase forward trunkflexion to accommodate for the steeper slopes In fact 556of participants who were unable to propel up the 71∘ slopewere overweight (119873 = 3) or obese (119873 = 2) whereasonly 30 of participants who were able to propel up the 71∘slope were overweight (119873 = 2) or obese (119873 = 1) Henceabdominal circumference may deserve additional attentionwhen investigating wheelchair propulsion technique or man-ual wheelchair skills such as uphill propulsion
BioMed Research International 9
Table4Group
average(SD)totalexcursio
n(∘ )
and
maxim
umandminim
um(∘ )
kinematicvalues
measuredatthetrun
kandno
ndom
inantsho
uldera
tthe
fivedifferent
slopestestedas
wellasthe
results
oftheA
NOVA
andpo
stho
ccom
paris
ontest
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Jointangle(∘
)
Trun
kmdashflexion
(+)extension(minus)
Trun
kmdashflexion
(+)extension(minus)
Excursion
588
(212
)1267(340)
1456(277)
1761
(396)
2237
(600)lt0001
0907
lt0001
000
6lt0001
0003
Maxim
um1927(623)
3592(845)
3945(831
)4579(853
)6093(113
0)lt0001
0889
lt0001
0031
0002
0005
Minim
um1339
(614
)2326(775)
2490(805)
2818
(771)
3857(859)lt0001
0910
lt0001
0028
lt0001
lt0001
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Excursion
5567(920)
5817
(1092)
5963(901)
6019
(698)
6499(895)
0019
0296
0072
0183
0473
0217
Maxim
um1131
(934)
1800(820)
1935
(762)
2259(730)
3088(745)lt0001
0849
lt0001
0001
0054
lt0001
Minim
umminus44
36(935
)minus40
17(936)minus40
27(915
)minus3760(834)minus3410
(1036)lt0001
0651
lt0001
000
6lt0001
lt0001
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Excursion
935(343)
1227(716)
1348(661)
1488(756)
1965(118
8)0012
0337
0010
0363
0158
0047
Maxim
um3325(800)
3481(1065)
3540(1026)
3488(1057)
4060(1543)
0083
mdashmdash
mdashmdash
mdashMinim
um2390(627)
2253
(726)
2192(666)
2000(545)
2094(570)
0038
mdashmdash
mdashmdash
mdashShou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Excursion
2486(820)
3055(1024)
3335(883)
3452
(944)
4328(113
4)lt0001
0623
000
4004
00765
0013
Maxim
um3157(1682)
3789(1846
)40
15(19
17)
4302(1223)
4969(871)lt0001
0665
lt0001
0029
0855
0033
Minim
um671
(1357)
734(1510)
680
(1694)
850
(918
)641
(770)
0152
mdashmdash
mdashmdash
mdash
10 BioMed Research International
Table5Group
average(
SD)m
eanandpeak
weight-n
ormalise
dmom
ents(N
mkg)
measuredatthen
ondo
minantsho
uldera
tthe
fived
ifferentslopesa
swellasresultsof
theA
NOVA
and
postho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Normalisedmoments(Nmkg)
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Mean
0140(0056)
0226(0067)
0248(0081)
0233(0083)
0242(015
1)0027
0288
lt0001
0003
0433
0966
Peak
(maxim
um)
0292(010
9)0512(015
2)0546(016
7)0559(012
8)0733(0302)lt0001
0588
lt0001
000
40867
0049
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashaddu
ction(+)abdu
ction(minus)
Mean
minus0016(0023)minus006
0(0050)minus0069(0046
)minus0090(0043)minus0103(0036)lt0001
0623
lt0001
0414
0147
0366
Peak
(minim
um)minus0088(0041)minus0257(010
5)minus0278(010
4)minus0369(013
7)minus0494(013
3)lt0001
0797
lt0001
0149
0002
0002
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Mean
0097(0036)
0189(0050)
0222(0064
)0252(0065)
0344(010
1)lt0001
0726
lt0001
000
40191
0010
Peak
(maxim
um)
0196(0078)
0415(014
4)0456(012
9)0530(014
8)0780(018
4)lt0001
0801
lt0001
0001
0103
0001
BioMed Research International 11
00
02
04
06
08
10
Ant
erio
r delt
oid
(a)
00
02
04
06
08
10
(b)
00
02
04
06
08
10
(c)
00
02
04
06
08
10
12
Poste
rior d
eltoi
d
(d)
00
02
04
06
08
10
12
(e)
00
02
04
06
08
10
12
(f)
00
02
04
06
08
10
Clav
icul
ar h
ead
of p
ecto
ralis
maj
or
(g)
00
02
04
06
08
10
(h)
00
02
04
06
08
10
(i)
00
02
04
06
08
10
12
14
16
0 20 40 60 80 100
Ster
nal h
ead
of p
ecto
ralis
maj
or
Normalised time (100)Mean MUR pattern (1)
0∘
27∘
36∘
48∘
71∘
(j)
00
02
04
06
08
10
12
14
16
Mean MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(k)
00
02
04
06
08
10
12
14
16
Peak MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(l)
Figure 3 Group averaged time-normalized mean profile (solid line) and standard deviation (dotted line) (a d g and j) as well as group-average (SD) mean (b e h and k) and peak (c f i and l) muscle utilization ratio (MUR) during the push phase for the five slopes tested atself-selected natural speed
12 BioMed Research International
Table6Group
average(
1SD)meanmuscle
utilisatio
nratio
(MUR)peakMUR(1)and
indicatoro
fmuscle
work(IMW)v
aluesfor
each
muscle
assessed
atthen
ondo
minantsho
uldera
tfived
ifferentslope
angles
aswellasresultsof
theA
NOVA
andpo
stho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Anteriord
eltoid
Anteriord
eltoid
MeanMUR(1)
007
(004)
021
(009)
023
(012
)026
(010
)034
(013
)lt0001
0831
lt0001
0002
lt0001
0001
Peak
MUR(1)
014
(008)
044
(023)
048
(026)
054
(026)
068
(028)lt0001
0836
lt0001
0002
lt0001
lt0001
IMW
718(398)
2070(943)
2348(1237)
2606(1043)
3448(1304)lt0001
0829
lt0001
0003
lt0001
0002
Poste
riord
eltoid
Poste
riord
eltoid
MeanMUR(1)
008
(007)
020
(014
)024
(024)
023
(010
)027
(006)lt0001
0907
lt0001
0144
lt0001
lt0001
Peak
MUR(1)
020
(014
)052
(031
)062
(051)
060
(019
)077
(019
)lt0001
0894
lt0001
0027
0001
0005
IMW
795(692)
2036(1384)
2443(2381)
2335
(1047)
2734(648)lt0001
0906
lt0001
0143
lt0001
lt0001
Clavicular
fiberso
fpectoralis
major
Clavicular
fiberso
fpectoralis
major
MeanMUR(1)
007
(004)
018
(010
)020
(010
)027
(014
)035
(018
)lt0001
0754
lt0001
0003
lt0001
0005
Peak
MUR(1)
014
(009)
038
(022)
042
(023)
057
(031
)071
(029)lt0001
0814
lt0001
000
9lt0001
0001
IMW
700(426)
1837
(977)
2041(1046)
2704(14
32)
3528(175
7)lt0001
0752
lt0001
0003
lt0001
0005
Sternalfi
bersof
pectoralismajor
Sternalfi
bersof
pectoralismajor
MeanMUR(1)
012
(008)
030
(015
)032
(013
)037
(015
)053
(024)lt0001
0781
lt0001
0005
0001
000
6Peak
MUR(1)
021
(015
)054
(023)
059
(023)
071
(026)
101(042)lt0001
0829
lt0001
0003
lt0001
0002
IMW
1194(753)
3023(14
77)
3227(1323)
3753
(1511)
5280(2406)lt0001
0780
lt0001
0005
0001
000
6
BioMed Research International 13
0
10
20
30
40
50
60
70
80
Ant
erio
r delt
oid
Poste
rior d
eltoi
d
Clav
icul
ar h
ead
ofpe
ctor
alis
maj
or
Ster
nal h
ead
of
pect
oral
is m
ajor
IMW
0∘
27∘
36∘
48∘
71∘
Figure 4 Group averaged (SD) mean indicator of muscle work(IMW) during the push phase for the five slopes tested at self-selected natural speed
At the shoulder the maximum shoulder flexion move-ment amplitude significantly increased as the slope becamesteeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments It is possible that increasedmaximumshoulder flexionwas needed to accommodate for the increased forward trunkflexion and to apply most of the force tangentially on thehandrim to preserve mechanical efficiencyThe fact that onlythe duration of the recovery period drastically decreasedas the slope became steeper can also explain in part therelatively stable shoulder flexion-extension excursion (iesimilar push phase durations across slopes) This finding isconsistent to some extent with the work of Yang et al [3]who found comparable values of movement-related adap-tation at the shoulder when comparing level overgroundand uphill (ie 3∘ slope) MWC propulsions However theshoulder flexion-extension excursion significantly increasedon average by 937∘ and the shoulder extension remainedsimilar in their study contrary to the results of the presentstudy These discrepancies may be attributed to the fact thatparticipants used test wheelchairs that were not anchoredto a safety system when propelling up a 3∘ slope at 09mson a motorized treadmill the level surface propulsion (0∘slope) was performed overground and the shoulder kine-matic calculation differed from the work by Yang et al [3]Nevertheless all these results confirmed kinematic adapta-tions at the shoulder as the slope progressed Lastly theincreased forward trunk flexion coupled with an increasedshoulder flexion that modifies the orientation of the forcegenerated at the shoulder may increase posterior shoulderjoint forces and explain the elevated muscular demand at theposterior deltoid occurring towards the end of the push phase[22]
42 Shoulder Joint Mechanical and Muscular Effort Adap-tations The shoulder joint moments adaptations partiallysupport the hypothesis that their outcome measures wouldgradually and significantly increase with each slope incre-ment while the speed remained constant For two out of thethree shoulder net joint moments investigated most of themean and peak values for the shoulder flexor and internalrotator moments progressively increased as the slope becamesteeper aside from some outcomemeasures during the 27∘ to36∘ or the 36∘ to 48∘ slope increment The relative musculardemand adaptations and muscular work computed for allmuscles investigated fully support this hypothesis since theiroutcomemeasures gradually and significantly increased witheach slope increment while the speed remained constantHence once the results of these two approaches are com-bined it is clear that the shoulder mechanical and musculareffort increases are key contributors to the adaptation processassociated with the steeper slopes Moreover these resultsare in line with the perceived UL efforts expressed by theparticipants and may explain in part The decreasing successrate with a steeper slope as shoulder strength generatingcapability most likely becomes a determinant for propellingon steeper slopes
43 Implications for Clinical Practice With the use of a slopeor of a combination of slopes when a MWC user propelshimselfherself on a motorized treadmill therapists may beable to offer task-specific high-intensity short duration inter-val training programs to increase UL strength particularlyat the shoulders Cautiousness is advised with this practicesince the risk exposure (ie increased shoulder mechanicaland muscular demands) will progressively and significantlyincrease as the slope becomes steeper and will vary accordingto the strength-generating capability of each MWC user Inaddition since the risk exposure could trigger the develop-ment or exacerbation of secondary impairments at the ULparticularly at the shoulders such a program should alsobe accompanied by proper warm-up and cool-down periodsas well as by antagonist muscle strengthening to preventmuscle strength imbalance Alternatively therapists may alsooffer task-specific cardiorespiratory fitness training programswhen a MWC user propels on a motorized treadmill withno slope or minimal slope (lt27∘) with minimal demandsduring a prolonged period of time (ie cardiorespiratoryfitness training)
44 Limits of the Study The present study included a rela-tively small sample size (119899 = 18) of experienced MWC userswho have completed their rehabilitation process which maylimit the strength of the evidence and potential to generalizethe results with new MWCs respectively The fact that theparticipants used their personal wheelchairs during the studywarrants consideration as optimal wheelchair positioningand configuration parameters most likely differs across par-ticipants and impacts the outcome measures of interest inthe present study and the risk of the MWC tilting or fallingbackwards when propelling up a slope The use of the instru-mented wheels which slightly increase the width and weight
14 BioMed Research International
of the wheelchair along with rolling resistance may havemodified participantsrsquo propulsion technique (eg increasedshoulder abduction) and fatigue level (eg increased ULeffort) in comparison to propelling with their own wheelsThe self-selected natural treadmill speed determined for eachparticipant maintained across all slopes tested in an effort toisolate the effect of speed also requires consideration sinceMWCusers tend to reduce their speedwhen propelling uphillin daily life particularly on steep slopes [2] Finally thekinematic and kinetic and electromyographic variables solelyfocused on the trunk and nondominant shoulder prevent afull understanding of UL adaptations (ie elbow and wristnot studied) during motorized treadmill MWC propulsionacross different slopes
5 Conclusion
This study confirms that MWC users with a SCI increaseforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increase during simulated uphillMWC propulsion on a motorized treadmill Few similaritieswere found between the 27∘ to 36∘ and the 36∘ to 48∘ slopeincrements for shoulder flexion and adduction momentsFuture studies incorporating interactions with various slopesand velocities could strengthen the results of the presentstudy and provide additional evidence-based knowledge onwheelchair propulsion on a motorized treadmill
Abbreviations
AIS American Spinal Injury AssociationImpairment Scale
EMG ElectromyographyER External rotationLED Light-emitting diodeIMW Indicator of muscle workIR Internal rotationJCS Joint coordinate systemMUR Muscle utilization ratioMVC Maximum voluntary contractionMWC Manual wheelchairUL Upper limbWUSPI Wheelchair Userrsquos Shoulder Pain
Index
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors would like to thank Michel Goyette (Eng)Daniel Marineau (Technician) Youssef El Khamlichi(Research Associate) and Philippe Gourdou (ResearchAssociate) for their contributions to this project DanyGagnon holds a Junior 1 Research Career Award from
the Fonds de la recherche du Quebec-Sante (FRQ-S)Annie-Claude Babineau and Guillaume Desroches aresupported by a summer internship and a post-doctoralfellowship from the Canadian Institutes of Health Researchrespectively DanyGagnon andRachid Aissaoui aremembersof the Multidisciplinary SensoriMotor RehabilitationResearch Team (httpwwwerrsmca) supported bythe CIHR and the Quebec-Ontario Spinal Cord InjuryMobility (SCI-MOB) Research Group funded by theQuebec Rehabilitation Research Network (REPARhttpwwwreparca) and the Ontario NeuroTraumaFoundation (ONF httpwwwonforg) The project wasfunded in part by the Fonds de la recherche du Quebec-Sante(FRQS) The equipment and material required for theresearch completed at the Pathokinesiology Laboratory wasfinanced by the Canada Foundation for Innovation (CFI)
References
[1] B Mason J Lenton C Leicht and V Goosey-Tolfrey ldquoAphysiological and biomechanical comparison of over-groundtreadmill and ergometer wheelchair propulsionrdquo Journal ofSports Sciences vol 32 no 1 pp 78ndash91 2014
[2] W M Richter R Rodriguez K R Woods and P W AxelsonldquoStroke pattern and handrim biomechanics for level and uphillwheelchair propulsion at self-selected speedsrdquo Archives of Phys-ical Medicine and Rehabilitation vol 88 no 1 pp 81ndash87 2007
[3] Y-S Yang A M Koontz S-J Yeh and J-J Chang ldquoEffectof backrest height on wheelchair propulsion biomechanics forlevel and uphill conditionsrdquo Archives of Physical Medicine andRehabilitation vol 93 no 4 pp 654ndash659 2012
[4] D H Gagnon A-C Babineau A Champagne G Desrochesand R Aissaoui ldquoPushrim biomechanical changes with pro-gressive increases in slope during motorized treadmill manualwheelchair propulsion in individuals with spinal cord injuryrdquoJournal of Rehabilitation Research amp Development vol 51 no 5pp 789ndash802 2014
[5] J W Chow T A Millikan L G Carlton W-S Chae Y-T Lim and M I Morse ldquoKinematic and electromyographicanalysis of wheelchair propulsion on ramps of different slopesfor young men with Paraplegiardquo Archives of Physical Medicineand Rehabilitation vol 90 no 2 pp 271ndash278 2009
[6] S van Drongelen L H van Der Woude T W Janssen E LAngenot E K Chadwick and D H Veeger ldquoMechanical loadon the upper extremity during wheelchair activitiesrdquo Archivesof Physical Medicine and Rehabilitation vol 86 no 6 pp 1214ndash1220 2005
[7] H Arabi R Aissaoui J Rousseau D Bourbonnais and JDansereau ldquoEvaluation of minimal mechanical effort duringthe ramp access of manual wheelchairrdquo Ergonomia vol 26 no3 pp 253ndash259 2004
[8] K Kulig S S Rao S J Mulroy et al ldquoShoulder joint kineticsduring the push phase of wheelchair propulsionrdquo ClinicalOrthopaedics and Related Research no 354 pp 132ndash143 1998
[9] L J Chapman and J P Chapman ldquoThe measurement ofhandednessrdquoBrain andCognition vol 6 no 2 pp 175ndash183 1987
[10] Gouvernement du Quebec Regie du Batiment du Quebec(RBQ) Construction Code Building Act Chapter 1 Architec-tural and Transportation Barriers Compliance Board 2013
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 BioMed Research International
the speed or slope of the treadmill) and their effects duringmotorized treadmill MWC propulsion Stronger evidence isneeded to optimize assessment and training protocols
Propelling aMWCup slopes on amotorized treadmill hasbeen found to increase upper limb demand in a few recentstudies Richter et al [2] found among MWC users with aspinal cord injury (SCI) propelling at a self-selected velocityon amotorized treadmill that the speed was about 15 and 27times slower when pushing up 3∘ and 6∘ slopes respectivelyin comparison with the level surface (0∘ slope) Additionallythey also reported that the peak total force at the handrimwas about 17 and 22 times higher when pushing up 3∘ and6∘ slopes respectively in comparison with the level surface(0∘ slope) despite the reduced treadmill speed Yang et al[3] found among MWC users with a SCI propelling at animposed steady speed of 09ms on a motorized treadmillthat peak shoulder flexion increased by 9∘ while the total andtangential forces applied at the handrim were about 209 and238 times higher when pushing up a 3∘ slope (approximatelya 1 20 ratio) in comparison with the level surface whereasthe mechanical efficiency was only found to be 11 timeshigher More recently Gagnon et al [4] found among MWCusers with a SCI each propelling at a self-selected steadyspeed on a motorized treadmill up slopes set at 0∘ 27∘ 36∘48∘ and 71∘ that the total and tangential forces appliedat the handrim were at least 2 times greater as the slopebecame progressively steeper The greatest change observedwas between 0∘ and 27∘ while similarities were observedbetween 27∘ and 36∘ Such differences also support the needto gain a better understanding of the effects of steeper slopeson trunk and shoulder kinematics shoulder kinetics andshoulder muscular demand during uphill propulsion on atreadmill set at a steady speed among a group of experiencedMWC users
In addition few studies have investigated the effects ofvarying slopes during overground MWC propulsion overthe past decade Among those Chow et al [5] investigatedthe effects of various slopes (ie 0∘ 2∘ 4∘ 6∘ 8∘ 10∘ and12∘) on trunk kinematics handrim kinetics and upper limband upper trunk muscular demand among MWC users witha spinal cord injury Overall forward trunk flexion andmuscular demand (ie triceps brachii anterior deltoid andpectoralis major) were found to progressively increase asthe slope became steeper van Drongelen et al [6] com-pared shoulder net joint moments between overground leveland uphill (ie 3∘ slope) propulsion among MWC userswith paraplegia and tetraplegia The resultant net shouldermoments were about 2 times higher during uphill comparedto overground level MWC propulsion Arabi et al [7] com-pared relative mechanical demand during uphill propulsionacross three slopes (ie 27∘ 48∘ and 57∘) among a group ofable-bodied individuals who used a MWC They confirmedthat the relative mechanical demand significantly increasedas the slope became steeper and reached 161 257 and311 of their maximum isometric voluntary force generatingcapability for the three slopes tested respectively Last Kuliget al [8] compared shoulder net joint moments between leveloverground and uphill (slope = 47∘) MWC propulsion inindividuals with paraplegia They showed that the peak net
shoulder flexion adduction and internal rotation momentswere 22 22 and 27 times greater respectively whenascending a slope compared to level overground wheelchairpropulsion
The aim of this study was to quantify the trunk and non-dominant shoulder kinematic changes along with the non-dominant shoulder joint moments and electromyographicchanges during MWC propulsion on a motorized treadmillset at a self-selected natural speed on five different slopes (ie0∘ 27∘ 36∘ 48∘ and 71∘) It was expected that the nondom-inant shoulder and trunk range of motion and nondominantshoulder jointmoments andmuscle electromyographic activ-ity would gradually and significantly increase with each slopeincrement while the speed remained constant
2 Material and Methods
21 Description of Participants A convenience sample of 17men and 1 woman who sustained a SCI (American SpinalInjuryAssociation Impairment Scale [9] (AIS) =A B C orD)volunteered to participate in this study (Table 1) Participantswere included in the study if they had sustained a SCI atleast three months before the study had been dischargedfrom initial intensive inpatient rehabilitation were living inthe community and used their MWC for at least 4 hoursper day Participants also had to master basic and advancedwheelchair skills including the capability to propel up a 9-metre long access ramp meeting building code standardsin the province of Quebec in Canada (ie maximum slopeof 1 12 for slopes of a maximum length of 9 metres)[10] Participants were excluded if they presented associatedneurological conditions musculoskeletal impairmentspaincardiorespiratoryvascular conditions or any other impair-ments or disabilities that might have interfered with theperformance or safety of the experimental tasks The self-reported Wheelchair Userrsquos Shoulder Pain Index (WUSPI)questionnaire [11 12] was completed (grouprsquos mean score =089plusmn 10510) and reviewed by a physical therapist who askedspecific questions whenever pain was rated as interferingwith the performance of wheelchair mobility to further verifythat pain will not limit their ability to specifically com-plete the experimental tasks During a telephone interviewwith the potential participants the rehabilitation researchcoordinator reviewed the inclusion and exclusion criteriato determine eligibility before scheduling the clinical andlaboratory assessments All participants gave their writtenconsent to participate in the study after being informed ofthe objectives and nature of their participation in the studyThe Research Ethics Committee of the Centre for Interdisci-plinaryResearch inRehabilitation ofGreaterMontreal (CRIR715-0312) approved the present study
22 Clinical Evaluation Each participant underwent a clini-cal assessment completed by a physical therapist in order tocollect their personal characteristics measure their anthro-pometric parameters (height weight length and circumfer-ence of body segments) characterize the severity of the sen-sory and motor impairments (ASIA Impairment Scale [13])
BioMed Research International 3
Table 1 Description of participants
Participants Gender Ageyears
Heightm
Masskg
Time sinceinjury years
ASIAlowast WUSPIlowast
Neuro-logicallevel
AISlowast Sensory224
Motor100
Mean10
Propulsion10min10
Slope10
1 M 443 184 803 106 T7 A 117 50 019 00 002 M 464 170 802 46 T10 B 140 50 068 01 053 M 322 192 959 53 T10 A 140 50 000 00 004 M 358 180 771 118 T6 D 194 81 125 19 225 M 332 195 723 78 T12 C 162 56 019 00 006 M 526 177 1089 187 T9 A 132 50 114 24 347 M 599 188 998 50 T10 A 140 50 034 04 228 M 440 172 684 221 T4 B 183 35 007 09 009 M 412 178 727 61 C7 C 56 44 123 27 2710 M 284 185 666 106 T12 A 154 50 063 38 1911 M 390 176 1018 28 T10 A 72 50 365 55 6812 M 491 170 768 44 T7 A 88 52 097 15 2413 M 557 180 1031 49 T3 A 88 50 031 18 1614 M 328 175 619 89 T4 A 95 50 010 04 0415 F 281 165 475 48 T11 A 148 50 020 20 1016 M 330 165 665 53 T6 A 53 50 010 00 0317 M 527 173 782 89 T12 B 172 63 312 26 4818 M 258 183 592 49 T7 A 112 50 188 47 26Mean 408 178 787 82 1248 517 089 17 18SD 103 009 170 51 423 90 105 17 19lowastGender M = male F = female AIS = ASIA Impairment Scale A = no motor or sensory function is preserved below the neurological level B = sensoryfunction is preserved but motor function is not preserved below the neurological level C =Motor function is preserved below the neurological level and morethan half of key muscle functions below the single neurological level of injury have a muscle grade less than 35 and D =Motor Incomplete Motor function ispreserved below the neurological level and at least half of key muscle functions below the neurological levle of injury have a muscle grade gt or = 35 ASIA =American Spinal Injury Association WUSPI = Wheelchair Userrsquos Shoulder Pain Index
confirm the absence of debilitating UL musculoskeletalimpairment (ie WUSPI [11 12] UL joint ranges of motionUL staticmanualmuscle testing) and confirmULnondom-inance [9]
23 Motorized Treadmill Wheelchair Propulsion At the startof the laboratory assessment each participant was givena five-minute familiarization period of motorized tread-mill propulsion at various slopes that differed from thoseinvestigated in the present study during which rest peri-ods were allowed to avoid fatigue The motorized dualbelt instrumented treadmill (Bertec Corporation ColumbusOhio United States) (width = 084m length = 184m) wasadapted for safe MWC propulsion The MWC was anchoredwith elastic bands to a bilateral frictionless gliding safetysystem preventing excessive antero-posterior and rotationalmovements of theMWC (Figure 1)The imposed speed of thetreadmill was adjusted for each participant to mimic the self-selected natural propulsion speed measured during a timedperformance-based 20 meter MWC propulsion test This lasttest was performed three times with a two-minute rest takenbetween trials to compute the self-selected natural propulsionspeed Thereafter each participant first propelled their own
MWC on the motorized treadmill with a level ground (0∘)and then randomly at four different slopes 27∘ 36∘ 48∘and 71∘ reflecting an increase from one unit of height to20 16 12 and 8 units of length respectively For each angletested two trials lasting a maximum of one minute (ie20 consecutive pushes) and separated by a two-minute restperiod were recorded During each trial the last 10 completeconsecutive propulsion cycles recordedwere used to computethe measurements of interest (ie trunk and shoulder kine-matics shoulder kinetics and shoulder muscular demand)and were essential to confirm the successful completion foreach slope tested (ie two trialsslope) This study designwas selected to minimize systematic errors related to thetesting (eg learning) and temporarymaturation effects (egfatigue) associated with the experimental protocol and toconclude that the findings of the present study do not resultfrom these potential threats to internal validity Participantsrated their perceived nondominant localized UL effort usinga 10 cm visual analog scale ranging from ldquono effortrdquo (0 cm) toldquomaximum effortrdquo (10 cm) during the rest periods
24 Trunk and Shoulder Kinematics To capture the 3Dmovements of the trunk the nondominant UL and
4 BioMed Research International
(a) (b) (c)
Figure 1 Illustration of three slopes tested during motorized treadmill MWC propulsion (a) 0∘ slope (b) 36∘ slope and (c) 71∘ slope
the MWC a total of 27 skin-fixed light-emitting diodes(LEDs) were placed on specific anatomical landmarks whilefour LEDs were fixed to the MWC frame [14] The 3Dcoordinates of each LED within the laboratory coordinatesystem were collected at 30Hz with a motion capture systemincorporating four synchronised camera units (Optotrack3020 and Optotrack Certus Northern Digital Inc WaterlooOntario Canada httpwwwndigitalcom) Supplementarybony landmarks wheelchair and treadmill reference pointswere digitised to determine principal axes of segments andlocate articular joint centres for the trunk and nondomi-nant UL wheelchair position and treadmill slope Beforeinitiating the experimental tasks three abduction-adductionand three flexion-extension active movements were recordedto locate the shoulder articular centre with respect to thescapula using a quadratic sphere fitting procedure [15 16] Allmarker trajectories were visually inspected and interpolatedwhen coordinates were missing using a linear or a cubicspline method The marker trajectories were then filteredusing a 4th order zero-lag Butterworth filter with a cutofffrequency set at 6Hz The recommendations formulated bythe International Society of Biomechanics [17] were used todetermine segmental coordinate systems (head trunk armsforearms and hand) Relative motion between the humerusand clavicle used as a surrogate rigid segment for the scapulathat articulates with the humerus [17] was computed using aZX1015840Y10158401015840 cardanic rotation sequence to avoid gimbal lock andto interpret reconstructed shoulder movements according tothree anatomical movements commonly described in clinicalpractice (ie flexionextension abductionadduction inter-nal and external rotations) [18] The relative trunk forwardinclination angle (ie forward trunk flexion) was computedas the motion of the vertical axis of the trunk defined by
a unit vector created with the midpoint between the eighththoracic vertebra and the xiphoid process to the midpointbetween the seventh cervical vertebra and the sternal notchwith respect to the vertical axis of the laboratory coordinatesystem For the trunk forward flexionextension and theshoulder flexionextension adductionadduction and inter-nalexternal rotation the minimal and maximal movementsalong with their total excursion were the main outcomemeasures
25 Handrim Kinetics Each participantrsquos MWC wasequipped bilaterally with 2410158401015840 or 2610158401015840 instrumented wheels(SmartWheel (SmartWheel Out-Front (formerly ThreeRivers Holdings LLC) Mesa Arizona United Stateshttpwwwout-frontcom)) to measure the three dimen-sional components of the total force applied at the handrimduring MWC propulsion at a sampling frequency of 240Hz[19] While these instrumented wheels did not alter axleposition or other rear wheel spatial characteristics (egorientation and diameter of the handrim) they slightlyincreased wheelchair width and weight (48 kginstrumentedwheel) and may have affected rolling resistance (ieurethane tire) Three dimensional handrim kinetic datawere filtered with a 4th order Butterworth filter anda cutoff frequency of 20Hz and then downsampled to30Hz to fit the kinematic data using a custom MATLAB(MATLAB MathWorks Natick Massachusetts UnitedStates httpwwwmathworkscom) routine
26 Shoulder Kinetics Shoulder net joint moments werecomputed using an inverse dynamic method [20] The dataentered into a custom-made MATLAB algorithm included
BioMed Research International 5
the anthropometric characteristics as well as the UL kine-matics and the pushrim kinetics with respect to the labcoordinate system Shoulder net joint moments were thenexpressed in the same coordinate system used to expressshoulder joint kinematics and normalized against the bodymass of each participant In fact moderate to high associ-ations were found between body mass and mean and peakshoulder net joint moments when propelling with no slope(119903 = 0554 and 0577) and with slopes of varying degrees(119903 = 0713 to 0809) The peak and mean shoulder net jointmoments in the sagittal frontal and transverse plane werethe main outcome measures
27 Shoulder Muscular Demand The electromyographicactivity of the anterior and posterior portions of the del-toid along with the clavicular and sternal heads of thepectoralis major was recorded at the nondominant upperextremity at a sampling frequency of 1200Hz using a portabletelemetric system (NORAXON USA Inc Scottsdale Ari-zona Telemyo 900) Skin preparation and the placementof the surface electrodes (BlueSensor M AMBU BallerupDanmark) (AgAgCl sensor ndash132mm2 active surface area)were made in accordance with SENIAM recommendations(refer to httpwwwseniamorg) Following baseline noiseremoval all EMG signals recorded were visually inspectedbefore being filtered with a 4th order zero-lag Butterworthbandpass filter with low and high cut-off frequencies set at30 and 500Hz respectively Thereafter EMG patterns werefull-wave rectified and filtered with a 6Hz low-pass filterto generate EMG linear envelopes for each muscle studiedThe muscular utilization ratio (MUR ()) was calculatedfor each muscle studied by normalizing the amplitude ofthe EMG signals recorded during the experimental tasksagainst the peak EMG signal recorded over a 05 secondperiod during one of the two static maximum voluntarycontractions (MVC) Muscle-specific manual resistance wasapplied by a trained physiotherapist to generate the MVCswhile participants remained seated in their own wheelchairMeanwhile another research associate manually providedadditional trunk and wheelchair stability to participants Foreach muscle studied the peak and mean MURs as well as anindicator of muscle work (IMW) were calculated using theintegral of the MUR data were the main outcome measuresAll EMG signal processing was performed digitally using acustom-developed MATLAB algorithm
28 Statistical Analyses Descriptive statistics (mean plusmn SD)were calculated for the demographic and clinical character-istics of all participants as well as for the kinematic kineticand muscular demand outcome measures For these lastoutcome measures 10 propulsion cycles were averaged pertrial resulting in a total of 20 propulsion cycles for eachslope tested The kinematic kinetic and muscular demanddata recorded during the push phase of each cycle analyzedwere also time-normalized over 100 (ie 100 data points)to generate a profile for each participant and a mean groupprofile Shapiro-Wilk tests confirmed that the kinematickinetic and electromyographic outcome measures for all
slopes tested were normally distributed and justified the useof parametric statistical tests One-way repeated-measureanalyses of variance (ANOVA) with one within-subjectsfactor (slopes of 0∘ 27∘ 36∘ 48∘ and 71∘) using a generallinear model was used to determine the effect of the slopeson the kinematic and kinetic and electromyographic outcomemeasures and an eta-squared value was used to confirmif the proportion of the total variability attributable to theslope factor (ie effect size) was small (gt002) moderate(gt013) or large (gt026) Whenever an ANOVA revealedsignificant differences (main effect 119875 lt 005) after the resultof the Mauchlyrsquos test of sphericity of the covariance matrixwas taken into consideration Studentrsquos 119905-tests for pairedsamples were computed (post hoc tests) with a Bonferronicorrection setting the significance level at 119875 le 00125(119875 le 0054 pairwise comparisons) as a result of thefour possible slope increments (ie 0∘ to 27∘ 27∘ to 36∘36∘ to 48∘ and 48∘ to 71∘) All statistical analyses wereperformed with SPSS Statistics 170 software for WindowsNote that the kinematic and electromyographic data wereonly collected and computed at the nondominant UL sincequasi-symmetrical ULmovement strategies and efforts wereassumed in order to safely propel on a linear trajectory onthe motorized treadmill [21] and since the nondominant ULstrength generating capability is generally weaker than theone at the dominant UL possibly resulting in higher relativedemand at the nondominant UL during the performance ofa symmetrical functional task
3 Results
31 Completion Rate At a mean natural and constant self-selected propulsion speed of 117 plusmn 018ms [min = 091msmax = 165ms] all participants (completion rate = 100)were able to propel themselves on the 0∘ slope and up the27∘ slope (Table 2)The completion rate reached 889 (119873 =1618 participants) 778 (119873 = 1418 participants) and556 (119873 = 1018 participants) for the 36∘ 48∘ and 71∘slopes respectively (Table 2)
32 Temporal Parameters Table 3 summarizes the meanduration of the push and recovery phases and the totalduration of a propulsion cycle in seconds for the differenttreadmill slopes The average durations of the push phasewere similar for all tested slopes (ANOVA 119875 = 0267)whereas the average duration of the recovery phase declinedas the slope became steeper (post hoc tests 119875 le 0043) Thetotal duration significantly decreased as the slope becamesteeper (post hoc tests 119875 le 0001) except during the 27∘ to36∘ slope increment that remained similar
33 Trunk and Shoulder Kinematics The trunk and shouldermovement patterns are illustrated in Figures 2(a) 2(b) 2(c)and 2(d) whereas the minimum maximum and excur-sion of the trunk and shoulder movement amplitudes aresummarized in Table 4 The slopes of the treadmill signifi-cantly influenced most minimum maximum and excursiontrunk and shoulder movement amplitudes At the trunk all
6 BioMed Research International
Table 2 Description of self-selected comfortable propulsion speed experimental tasks completed and rate of perceived exertion
Participants Self-selected speed (ms) Slopes Rate of perceived exertion (10)0∘ 27∘ 36∘ 48∘ 71∘ 0∘ 27∘ 36∘ 48∘ 71∘
1 111 09 74 55 81 952 165 01 22 03 03 mdash3 105 13 13 39 44 714 118 08 17 37 48 785 120 17 48 25 59 796 091 30 63 77 mdash mdash7 148 09 97 mdash mdash mdash8 116 0 03 09 mdash mdash9 104 18 38 33 42 mdash10 127 0 0 0 0 011 139 10 15 33 27 3212 099 11 41 40 75 mdash13 106 42 88 mdash mdash mdash14 125 12 52 67 64 8515 103 00 06 19 36 mdash16 107 07 34 46 66 9217 106 07 62 26 65 8918 111 29 46 61 66 73Mean 117 119899 = 18 119899 = 18 119899 = 16 119899 = 14 119899 = 10 12 39 35 47 68SD 018 11 29 22 25 30
Table 3 Group average (SD) mean temporal parameter measured of the push phase measured at the nondominant handrim at the fivedifferent slopes tested
Slopes0∘ 27∘ 36∘ 48∘ 71∘
Temporal parameters (s)Push phase 048 plusmn 008 048 plusmn 008 049 plusmn 008 048 plusmn 007 048 plusmn 006Recovery phase 059 plusmn 022 027 plusmn 010 026 plusmn 009 022 plusmn 008 018 plusmn 005Total (cycle) 107 plusmn 023 075 plusmn 016 075 plusmn 014 070 plusmn 013 066 plusmn 010
minimum maximum and excursion movement amplitudessignificantly increased as the slope became steeper except forminimum and maximum values during the 27∘ to 36∘ slopeincrement that remained similar The greatest maximumforward trunk flexion (609∘) which was accompanied by thegreatest forward trunk excursion (224∘) was reached duringthe 71∘ slope At the shoulder the maximum shoulder flexionmovement amplitude significantly increased as the slopebecame steeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments The minimum maximum and excursion shoulderabduction movement amplitudes remained comparable asthe slope became steeper The minimum maximum andexcursion shoulder internal rotation movement amplitudesalso remained comparable as the slope became steeper with
the exception of the minimum and excursion values whichsignificantly increased during the 0∘ to 27∘ slope increment
34 Shoulder Kinetics The net shoulder flexion abductionand internal rotation moment patterns are illustrated inFigures 2(e) 2(f) and 2(g) while their mean and maximumvalues are summarized in Table 5 The greatest maximumshoulder moments were found during flexion across allslopes except for the 71∘ slope when the internal rotationgenerated the greatest moment All mean and maximumshouldermoments were significantly influenced by the slopesof the treadmill The mean and maximum flexion momentssignificantly improved as the slope increased except for the36∘ to 48∘ and 48∘ to 71∘ slope increments The meanadduction moments only significantly improved as the slopeincreased between 0∘ and 27∘ whereas the peak mean valueonly significantly improved as the slope increased between
BioMed Research International 7
0
10
20
30
40
50
60
70
80
Trun
k fle
xion
(+)
exte
nsio
n (minus
)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(a)
60
40
20
0
minus20
minus40
minus60
Shou
lder
flex
ion
(+)
exte
nsio
n (minus
)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(b)
0
10
20
30
40
50
60
Shou
lder
abdu
ctio
n (+
) ad
duct
ion
(minus)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(c)
0
10
20
30
40
50
60
70
0 20 40 60 80 100
Normalized time (100)Angle (∘)
Shou
lder
IR (+
) ER
(minus)
(d)
12
08
04
00
minus04
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder flexion (+) extension (minus)
(e)
04
02
00
minus02
minus04
minus06
minus08
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder abduction (+) adduction (minus)
(f)
Figure 2 Continued
8 BioMed Research International
10
08
06
04
02
00
minus02
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder IR (+) ER (minus)
(g)
Figure 2 Group averaged time-normalized profile (solid line) and standard deviation (dotted line) of the shoulder and trunk kinematics (ab c and d) and weight-normalised shoulder moments (e f and g) during the push phase for the five slopes tested at self-selected naturalspeed
the 0∘ to 27∘ 36∘ to 48∘ and 48∘ to 71∘ slope incrementsThemean and maximum internal rotation moments significantlyincreased as the slope became steeper except for the 36∘ to48∘ slope increment
35 Shoulder Muscular Demand The MUR patterns of themuscles studied are illustrated in Figure 3 while their meanand maximum values are summarized in Table 6 The meanIMWs of the muscles studied are summarized in Table 6 andillustrated in Figure 4 For allmuscles studied theirmean andmaximum MURs as well as their indicator of muscle workvalue significantly increased as the slope became steeperexcept for the posterior deltoid that remained comparablebetween the 27∘ to 36∘ slope increment
4 Discussion
This study quantified trunk and nondominant shoulderkinematic changes along with nondominant shoulder jointmoments and electromyographic changes during MWCpropulsion on a motorized treadmill set at a self-selectednatural speed on five different slopes (ie 0∘ 27∘ 36∘ 48∘and 71∘) Overall the MWC users with a SCI increasedforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increased during simulated uphillMWC propulsion on a motorized treadmill
41 Trunk and Shoulder Movement-Related Adaptations Themovement-related adaptations occurring at the trunk andshoulder partially support the hypothesis that their outcome
measures would gradually and significantly increase witheach slope increment while the speed remained constantAt the trunk the maximum forward trunk flexion and thetotal trunk excursion increased significantly as the slopebecame steeper except for the 27∘ to 36∘ slope incrementChow et al [5] obtained somewhat comparable resultsin terms of trunk kinematics although no difference wasrevealed when comparing 4∘ and 8∘ slopes This may beexplained by the fact that participants propelled at self-selected speeds that decreased progressively in their protocolas the slope increased Nonetheless the increased maximumforward trunk flexion coupled with the increased forwardtrunk excursion may allow MWC users to move their centreof mass further and faster anteriorly and to maintain itsprojection in front of the rear wheel axle in order toprevent backward tilt and falls as the slope increases Thismay also explain why maximum forward trunk flexion andforward trunk excursion became greater as the gravitationaleffects became harder to overcome with steeper slopes Thedecreasing success rate with a steeper slope may be explainedin part by the fact that some participants were classified asbeing overweight (body mass index gt 25) or class I obese(body mass index = 300ndash349) with associated abdominalobesity that limited their ability to increase forward trunkflexion to accommodate for the steeper slopes In fact 556of participants who were unable to propel up the 71∘ slopewere overweight (119873 = 3) or obese (119873 = 2) whereasonly 30 of participants who were able to propel up the 71∘slope were overweight (119873 = 2) or obese (119873 = 1) Henceabdominal circumference may deserve additional attentionwhen investigating wheelchair propulsion technique or man-ual wheelchair skills such as uphill propulsion
BioMed Research International 9
Table4Group
average(SD)totalexcursio
n(∘ )
and
maxim
umandminim
um(∘ )
kinematicvalues
measuredatthetrun
kandno
ndom
inantsho
uldera
tthe
fivedifferent
slopestestedas
wellasthe
results
oftheA
NOVA
andpo
stho
ccom
paris
ontest
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Jointangle(∘
)
Trun
kmdashflexion
(+)extension(minus)
Trun
kmdashflexion
(+)extension(minus)
Excursion
588
(212
)1267(340)
1456(277)
1761
(396)
2237
(600)lt0001
0907
lt0001
000
6lt0001
0003
Maxim
um1927(623)
3592(845)
3945(831
)4579(853
)6093(113
0)lt0001
0889
lt0001
0031
0002
0005
Minim
um1339
(614
)2326(775)
2490(805)
2818
(771)
3857(859)lt0001
0910
lt0001
0028
lt0001
lt0001
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Excursion
5567(920)
5817
(1092)
5963(901)
6019
(698)
6499(895)
0019
0296
0072
0183
0473
0217
Maxim
um1131
(934)
1800(820)
1935
(762)
2259(730)
3088(745)lt0001
0849
lt0001
0001
0054
lt0001
Minim
umminus44
36(935
)minus40
17(936)minus40
27(915
)minus3760(834)minus3410
(1036)lt0001
0651
lt0001
000
6lt0001
lt0001
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Excursion
935(343)
1227(716)
1348(661)
1488(756)
1965(118
8)0012
0337
0010
0363
0158
0047
Maxim
um3325(800)
3481(1065)
3540(1026)
3488(1057)
4060(1543)
0083
mdashmdash
mdashmdash
mdashMinim
um2390(627)
2253
(726)
2192(666)
2000(545)
2094(570)
0038
mdashmdash
mdashmdash
mdashShou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Excursion
2486(820)
3055(1024)
3335(883)
3452
(944)
4328(113
4)lt0001
0623
000
4004
00765
0013
Maxim
um3157(1682)
3789(1846
)40
15(19
17)
4302(1223)
4969(871)lt0001
0665
lt0001
0029
0855
0033
Minim
um671
(1357)
734(1510)
680
(1694)
850
(918
)641
(770)
0152
mdashmdash
mdashmdash
mdash
10 BioMed Research International
Table5Group
average(
SD)m
eanandpeak
weight-n
ormalise
dmom
ents(N
mkg)
measuredatthen
ondo
minantsho
uldera
tthe
fived
ifferentslopesa
swellasresultsof
theA
NOVA
and
postho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Normalisedmoments(Nmkg)
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Mean
0140(0056)
0226(0067)
0248(0081)
0233(0083)
0242(015
1)0027
0288
lt0001
0003
0433
0966
Peak
(maxim
um)
0292(010
9)0512(015
2)0546(016
7)0559(012
8)0733(0302)lt0001
0588
lt0001
000
40867
0049
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashaddu
ction(+)abdu
ction(minus)
Mean
minus0016(0023)minus006
0(0050)minus0069(0046
)minus0090(0043)minus0103(0036)lt0001
0623
lt0001
0414
0147
0366
Peak
(minim
um)minus0088(0041)minus0257(010
5)minus0278(010
4)minus0369(013
7)minus0494(013
3)lt0001
0797
lt0001
0149
0002
0002
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Mean
0097(0036)
0189(0050)
0222(0064
)0252(0065)
0344(010
1)lt0001
0726
lt0001
000
40191
0010
Peak
(maxim
um)
0196(0078)
0415(014
4)0456(012
9)0530(014
8)0780(018
4)lt0001
0801
lt0001
0001
0103
0001
BioMed Research International 11
00
02
04
06
08
10
Ant
erio
r delt
oid
(a)
00
02
04
06
08
10
(b)
00
02
04
06
08
10
(c)
00
02
04
06
08
10
12
Poste
rior d
eltoi
d
(d)
00
02
04
06
08
10
12
(e)
00
02
04
06
08
10
12
(f)
00
02
04
06
08
10
Clav
icul
ar h
ead
of p
ecto
ralis
maj
or
(g)
00
02
04
06
08
10
(h)
00
02
04
06
08
10
(i)
00
02
04
06
08
10
12
14
16
0 20 40 60 80 100
Ster
nal h
ead
of p
ecto
ralis
maj
or
Normalised time (100)Mean MUR pattern (1)
0∘
27∘
36∘
48∘
71∘
(j)
00
02
04
06
08
10
12
14
16
Mean MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(k)
00
02
04
06
08
10
12
14
16
Peak MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(l)
Figure 3 Group averaged time-normalized mean profile (solid line) and standard deviation (dotted line) (a d g and j) as well as group-average (SD) mean (b e h and k) and peak (c f i and l) muscle utilization ratio (MUR) during the push phase for the five slopes tested atself-selected natural speed
12 BioMed Research International
Table6Group
average(
1SD)meanmuscle
utilisatio
nratio
(MUR)peakMUR(1)and
indicatoro
fmuscle
work(IMW)v
aluesfor
each
muscle
assessed
atthen
ondo
minantsho
uldera
tfived
ifferentslope
angles
aswellasresultsof
theA
NOVA
andpo
stho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Anteriord
eltoid
Anteriord
eltoid
MeanMUR(1)
007
(004)
021
(009)
023
(012
)026
(010
)034
(013
)lt0001
0831
lt0001
0002
lt0001
0001
Peak
MUR(1)
014
(008)
044
(023)
048
(026)
054
(026)
068
(028)lt0001
0836
lt0001
0002
lt0001
lt0001
IMW
718(398)
2070(943)
2348(1237)
2606(1043)
3448(1304)lt0001
0829
lt0001
0003
lt0001
0002
Poste
riord
eltoid
Poste
riord
eltoid
MeanMUR(1)
008
(007)
020
(014
)024
(024)
023
(010
)027
(006)lt0001
0907
lt0001
0144
lt0001
lt0001
Peak
MUR(1)
020
(014
)052
(031
)062
(051)
060
(019
)077
(019
)lt0001
0894
lt0001
0027
0001
0005
IMW
795(692)
2036(1384)
2443(2381)
2335
(1047)
2734(648)lt0001
0906
lt0001
0143
lt0001
lt0001
Clavicular
fiberso
fpectoralis
major
Clavicular
fiberso
fpectoralis
major
MeanMUR(1)
007
(004)
018
(010
)020
(010
)027
(014
)035
(018
)lt0001
0754
lt0001
0003
lt0001
0005
Peak
MUR(1)
014
(009)
038
(022)
042
(023)
057
(031
)071
(029)lt0001
0814
lt0001
000
9lt0001
0001
IMW
700(426)
1837
(977)
2041(1046)
2704(14
32)
3528(175
7)lt0001
0752
lt0001
0003
lt0001
0005
Sternalfi
bersof
pectoralismajor
Sternalfi
bersof
pectoralismajor
MeanMUR(1)
012
(008)
030
(015
)032
(013
)037
(015
)053
(024)lt0001
0781
lt0001
0005
0001
000
6Peak
MUR(1)
021
(015
)054
(023)
059
(023)
071
(026)
101(042)lt0001
0829
lt0001
0003
lt0001
0002
IMW
1194(753)
3023(14
77)
3227(1323)
3753
(1511)
5280(2406)lt0001
0780
lt0001
0005
0001
000
6
BioMed Research International 13
0
10
20
30
40
50
60
70
80
Ant
erio
r delt
oid
Poste
rior d
eltoi
d
Clav
icul
ar h
ead
ofpe
ctor
alis
maj
or
Ster
nal h
ead
of
pect
oral
is m
ajor
IMW
0∘
27∘
36∘
48∘
71∘
Figure 4 Group averaged (SD) mean indicator of muscle work(IMW) during the push phase for the five slopes tested at self-selected natural speed
At the shoulder the maximum shoulder flexion move-ment amplitude significantly increased as the slope becamesteeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments It is possible that increasedmaximumshoulder flexionwas needed to accommodate for the increased forward trunkflexion and to apply most of the force tangentially on thehandrim to preserve mechanical efficiencyThe fact that onlythe duration of the recovery period drastically decreasedas the slope became steeper can also explain in part therelatively stable shoulder flexion-extension excursion (iesimilar push phase durations across slopes) This finding isconsistent to some extent with the work of Yang et al [3]who found comparable values of movement-related adap-tation at the shoulder when comparing level overgroundand uphill (ie 3∘ slope) MWC propulsions However theshoulder flexion-extension excursion significantly increasedon average by 937∘ and the shoulder extension remainedsimilar in their study contrary to the results of the presentstudy These discrepancies may be attributed to the fact thatparticipants used test wheelchairs that were not anchoredto a safety system when propelling up a 3∘ slope at 09mson a motorized treadmill the level surface propulsion (0∘slope) was performed overground and the shoulder kine-matic calculation differed from the work by Yang et al [3]Nevertheless all these results confirmed kinematic adapta-tions at the shoulder as the slope progressed Lastly theincreased forward trunk flexion coupled with an increasedshoulder flexion that modifies the orientation of the forcegenerated at the shoulder may increase posterior shoulderjoint forces and explain the elevated muscular demand at theposterior deltoid occurring towards the end of the push phase[22]
42 Shoulder Joint Mechanical and Muscular Effort Adap-tations The shoulder joint moments adaptations partiallysupport the hypothesis that their outcome measures wouldgradually and significantly increase with each slope incre-ment while the speed remained constant For two out of thethree shoulder net joint moments investigated most of themean and peak values for the shoulder flexor and internalrotator moments progressively increased as the slope becamesteeper aside from some outcomemeasures during the 27∘ to36∘ or the 36∘ to 48∘ slope increment The relative musculardemand adaptations and muscular work computed for allmuscles investigated fully support this hypothesis since theiroutcomemeasures gradually and significantly increased witheach slope increment while the speed remained constantHence once the results of these two approaches are com-bined it is clear that the shoulder mechanical and musculareffort increases are key contributors to the adaptation processassociated with the steeper slopes Moreover these resultsare in line with the perceived UL efforts expressed by theparticipants and may explain in part The decreasing successrate with a steeper slope as shoulder strength generatingcapability most likely becomes a determinant for propellingon steeper slopes
43 Implications for Clinical Practice With the use of a slopeor of a combination of slopes when a MWC user propelshimselfherself on a motorized treadmill therapists may beable to offer task-specific high-intensity short duration inter-val training programs to increase UL strength particularlyat the shoulders Cautiousness is advised with this practicesince the risk exposure (ie increased shoulder mechanicaland muscular demands) will progressively and significantlyincrease as the slope becomes steeper and will vary accordingto the strength-generating capability of each MWC user Inaddition since the risk exposure could trigger the develop-ment or exacerbation of secondary impairments at the ULparticularly at the shoulders such a program should alsobe accompanied by proper warm-up and cool-down periodsas well as by antagonist muscle strengthening to preventmuscle strength imbalance Alternatively therapists may alsooffer task-specific cardiorespiratory fitness training programswhen a MWC user propels on a motorized treadmill withno slope or minimal slope (lt27∘) with minimal demandsduring a prolonged period of time (ie cardiorespiratoryfitness training)
44 Limits of the Study The present study included a rela-tively small sample size (119899 = 18) of experienced MWC userswho have completed their rehabilitation process which maylimit the strength of the evidence and potential to generalizethe results with new MWCs respectively The fact that theparticipants used their personal wheelchairs during the studywarrants consideration as optimal wheelchair positioningand configuration parameters most likely differs across par-ticipants and impacts the outcome measures of interest inthe present study and the risk of the MWC tilting or fallingbackwards when propelling up a slope The use of the instru-mented wheels which slightly increase the width and weight
14 BioMed Research International
of the wheelchair along with rolling resistance may havemodified participantsrsquo propulsion technique (eg increasedshoulder abduction) and fatigue level (eg increased ULeffort) in comparison to propelling with their own wheelsThe self-selected natural treadmill speed determined for eachparticipant maintained across all slopes tested in an effort toisolate the effect of speed also requires consideration sinceMWCusers tend to reduce their speedwhen propelling uphillin daily life particularly on steep slopes [2] Finally thekinematic and kinetic and electromyographic variables solelyfocused on the trunk and nondominant shoulder prevent afull understanding of UL adaptations (ie elbow and wristnot studied) during motorized treadmill MWC propulsionacross different slopes
5 Conclusion
This study confirms that MWC users with a SCI increaseforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increase during simulated uphillMWC propulsion on a motorized treadmill Few similaritieswere found between the 27∘ to 36∘ and the 36∘ to 48∘ slopeincrements for shoulder flexion and adduction momentsFuture studies incorporating interactions with various slopesand velocities could strengthen the results of the presentstudy and provide additional evidence-based knowledge onwheelchair propulsion on a motorized treadmill
Abbreviations
AIS American Spinal Injury AssociationImpairment Scale
EMG ElectromyographyER External rotationLED Light-emitting diodeIMW Indicator of muscle workIR Internal rotationJCS Joint coordinate systemMUR Muscle utilization ratioMVC Maximum voluntary contractionMWC Manual wheelchairUL Upper limbWUSPI Wheelchair Userrsquos Shoulder Pain
Index
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors would like to thank Michel Goyette (Eng)Daniel Marineau (Technician) Youssef El Khamlichi(Research Associate) and Philippe Gourdou (ResearchAssociate) for their contributions to this project DanyGagnon holds a Junior 1 Research Career Award from
the Fonds de la recherche du Quebec-Sante (FRQ-S)Annie-Claude Babineau and Guillaume Desroches aresupported by a summer internship and a post-doctoralfellowship from the Canadian Institutes of Health Researchrespectively DanyGagnon andRachid Aissaoui aremembersof the Multidisciplinary SensoriMotor RehabilitationResearch Team (httpwwwerrsmca) supported bythe CIHR and the Quebec-Ontario Spinal Cord InjuryMobility (SCI-MOB) Research Group funded by theQuebec Rehabilitation Research Network (REPARhttpwwwreparca) and the Ontario NeuroTraumaFoundation (ONF httpwwwonforg) The project wasfunded in part by the Fonds de la recherche du Quebec-Sante(FRQS) The equipment and material required for theresearch completed at the Pathokinesiology Laboratory wasfinanced by the Canada Foundation for Innovation (CFI)
References
[1] B Mason J Lenton C Leicht and V Goosey-Tolfrey ldquoAphysiological and biomechanical comparison of over-groundtreadmill and ergometer wheelchair propulsionrdquo Journal ofSports Sciences vol 32 no 1 pp 78ndash91 2014
[2] W M Richter R Rodriguez K R Woods and P W AxelsonldquoStroke pattern and handrim biomechanics for level and uphillwheelchair propulsion at self-selected speedsrdquo Archives of Phys-ical Medicine and Rehabilitation vol 88 no 1 pp 81ndash87 2007
[3] Y-S Yang A M Koontz S-J Yeh and J-J Chang ldquoEffectof backrest height on wheelchair propulsion biomechanics forlevel and uphill conditionsrdquo Archives of Physical Medicine andRehabilitation vol 93 no 4 pp 654ndash659 2012
[4] D H Gagnon A-C Babineau A Champagne G Desrochesand R Aissaoui ldquoPushrim biomechanical changes with pro-gressive increases in slope during motorized treadmill manualwheelchair propulsion in individuals with spinal cord injuryrdquoJournal of Rehabilitation Research amp Development vol 51 no 5pp 789ndash802 2014
[5] J W Chow T A Millikan L G Carlton W-S Chae Y-T Lim and M I Morse ldquoKinematic and electromyographicanalysis of wheelchair propulsion on ramps of different slopesfor young men with Paraplegiardquo Archives of Physical Medicineand Rehabilitation vol 90 no 2 pp 271ndash278 2009
[6] S van Drongelen L H van Der Woude T W Janssen E LAngenot E K Chadwick and D H Veeger ldquoMechanical loadon the upper extremity during wheelchair activitiesrdquo Archivesof Physical Medicine and Rehabilitation vol 86 no 6 pp 1214ndash1220 2005
[7] H Arabi R Aissaoui J Rousseau D Bourbonnais and JDansereau ldquoEvaluation of minimal mechanical effort duringthe ramp access of manual wheelchairrdquo Ergonomia vol 26 no3 pp 253ndash259 2004
[8] K Kulig S S Rao S J Mulroy et al ldquoShoulder joint kineticsduring the push phase of wheelchair propulsionrdquo ClinicalOrthopaedics and Related Research no 354 pp 132ndash143 1998
[9] L J Chapman and J P Chapman ldquoThe measurement ofhandednessrdquoBrain andCognition vol 6 no 2 pp 175ndash183 1987
[10] Gouvernement du Quebec Regie du Batiment du Quebec(RBQ) Construction Code Building Act Chapter 1 Architec-tural and Transportation Barriers Compliance Board 2013
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 3
Table 1 Description of participants
Participants Gender Ageyears
Heightm
Masskg
Time sinceinjury years
ASIAlowast WUSPIlowast
Neuro-logicallevel
AISlowast Sensory224
Motor100
Mean10
Propulsion10min10
Slope10
1 M 443 184 803 106 T7 A 117 50 019 00 002 M 464 170 802 46 T10 B 140 50 068 01 053 M 322 192 959 53 T10 A 140 50 000 00 004 M 358 180 771 118 T6 D 194 81 125 19 225 M 332 195 723 78 T12 C 162 56 019 00 006 M 526 177 1089 187 T9 A 132 50 114 24 347 M 599 188 998 50 T10 A 140 50 034 04 228 M 440 172 684 221 T4 B 183 35 007 09 009 M 412 178 727 61 C7 C 56 44 123 27 2710 M 284 185 666 106 T12 A 154 50 063 38 1911 M 390 176 1018 28 T10 A 72 50 365 55 6812 M 491 170 768 44 T7 A 88 52 097 15 2413 M 557 180 1031 49 T3 A 88 50 031 18 1614 M 328 175 619 89 T4 A 95 50 010 04 0415 F 281 165 475 48 T11 A 148 50 020 20 1016 M 330 165 665 53 T6 A 53 50 010 00 0317 M 527 173 782 89 T12 B 172 63 312 26 4818 M 258 183 592 49 T7 A 112 50 188 47 26Mean 408 178 787 82 1248 517 089 17 18SD 103 009 170 51 423 90 105 17 19lowastGender M = male F = female AIS = ASIA Impairment Scale A = no motor or sensory function is preserved below the neurological level B = sensoryfunction is preserved but motor function is not preserved below the neurological level C =Motor function is preserved below the neurological level and morethan half of key muscle functions below the single neurological level of injury have a muscle grade less than 35 and D =Motor Incomplete Motor function ispreserved below the neurological level and at least half of key muscle functions below the neurological levle of injury have a muscle grade gt or = 35 ASIA =American Spinal Injury Association WUSPI = Wheelchair Userrsquos Shoulder Pain Index
confirm the absence of debilitating UL musculoskeletalimpairment (ie WUSPI [11 12] UL joint ranges of motionUL staticmanualmuscle testing) and confirmULnondom-inance [9]
23 Motorized Treadmill Wheelchair Propulsion At the startof the laboratory assessment each participant was givena five-minute familiarization period of motorized tread-mill propulsion at various slopes that differed from thoseinvestigated in the present study during which rest peri-ods were allowed to avoid fatigue The motorized dualbelt instrumented treadmill (Bertec Corporation ColumbusOhio United States) (width = 084m length = 184m) wasadapted for safe MWC propulsion The MWC was anchoredwith elastic bands to a bilateral frictionless gliding safetysystem preventing excessive antero-posterior and rotationalmovements of theMWC (Figure 1)The imposed speed of thetreadmill was adjusted for each participant to mimic the self-selected natural propulsion speed measured during a timedperformance-based 20 meter MWC propulsion test This lasttest was performed three times with a two-minute rest takenbetween trials to compute the self-selected natural propulsionspeed Thereafter each participant first propelled their own
MWC on the motorized treadmill with a level ground (0∘)and then randomly at four different slopes 27∘ 36∘ 48∘and 71∘ reflecting an increase from one unit of height to20 16 12 and 8 units of length respectively For each angletested two trials lasting a maximum of one minute (ie20 consecutive pushes) and separated by a two-minute restperiod were recorded During each trial the last 10 completeconsecutive propulsion cycles recordedwere used to computethe measurements of interest (ie trunk and shoulder kine-matics shoulder kinetics and shoulder muscular demand)and were essential to confirm the successful completion foreach slope tested (ie two trialsslope) This study designwas selected to minimize systematic errors related to thetesting (eg learning) and temporarymaturation effects (egfatigue) associated with the experimental protocol and toconclude that the findings of the present study do not resultfrom these potential threats to internal validity Participantsrated their perceived nondominant localized UL effort usinga 10 cm visual analog scale ranging from ldquono effortrdquo (0 cm) toldquomaximum effortrdquo (10 cm) during the rest periods
24 Trunk and Shoulder Kinematics To capture the 3Dmovements of the trunk the nondominant UL and
4 BioMed Research International
(a) (b) (c)
Figure 1 Illustration of three slopes tested during motorized treadmill MWC propulsion (a) 0∘ slope (b) 36∘ slope and (c) 71∘ slope
the MWC a total of 27 skin-fixed light-emitting diodes(LEDs) were placed on specific anatomical landmarks whilefour LEDs were fixed to the MWC frame [14] The 3Dcoordinates of each LED within the laboratory coordinatesystem were collected at 30Hz with a motion capture systemincorporating four synchronised camera units (Optotrack3020 and Optotrack Certus Northern Digital Inc WaterlooOntario Canada httpwwwndigitalcom) Supplementarybony landmarks wheelchair and treadmill reference pointswere digitised to determine principal axes of segments andlocate articular joint centres for the trunk and nondomi-nant UL wheelchair position and treadmill slope Beforeinitiating the experimental tasks three abduction-adductionand three flexion-extension active movements were recordedto locate the shoulder articular centre with respect to thescapula using a quadratic sphere fitting procedure [15 16] Allmarker trajectories were visually inspected and interpolatedwhen coordinates were missing using a linear or a cubicspline method The marker trajectories were then filteredusing a 4th order zero-lag Butterworth filter with a cutofffrequency set at 6Hz The recommendations formulated bythe International Society of Biomechanics [17] were used todetermine segmental coordinate systems (head trunk armsforearms and hand) Relative motion between the humerusand clavicle used as a surrogate rigid segment for the scapulathat articulates with the humerus [17] was computed using aZX1015840Y10158401015840 cardanic rotation sequence to avoid gimbal lock andto interpret reconstructed shoulder movements according tothree anatomical movements commonly described in clinicalpractice (ie flexionextension abductionadduction inter-nal and external rotations) [18] The relative trunk forwardinclination angle (ie forward trunk flexion) was computedas the motion of the vertical axis of the trunk defined by
a unit vector created with the midpoint between the eighththoracic vertebra and the xiphoid process to the midpointbetween the seventh cervical vertebra and the sternal notchwith respect to the vertical axis of the laboratory coordinatesystem For the trunk forward flexionextension and theshoulder flexionextension adductionadduction and inter-nalexternal rotation the minimal and maximal movementsalong with their total excursion were the main outcomemeasures
25 Handrim Kinetics Each participantrsquos MWC wasequipped bilaterally with 2410158401015840 or 2610158401015840 instrumented wheels(SmartWheel (SmartWheel Out-Front (formerly ThreeRivers Holdings LLC) Mesa Arizona United Stateshttpwwwout-frontcom)) to measure the three dimen-sional components of the total force applied at the handrimduring MWC propulsion at a sampling frequency of 240Hz[19] While these instrumented wheels did not alter axleposition or other rear wheel spatial characteristics (egorientation and diameter of the handrim) they slightlyincreased wheelchair width and weight (48 kginstrumentedwheel) and may have affected rolling resistance (ieurethane tire) Three dimensional handrim kinetic datawere filtered with a 4th order Butterworth filter anda cutoff frequency of 20Hz and then downsampled to30Hz to fit the kinematic data using a custom MATLAB(MATLAB MathWorks Natick Massachusetts UnitedStates httpwwwmathworkscom) routine
26 Shoulder Kinetics Shoulder net joint moments werecomputed using an inverse dynamic method [20] The dataentered into a custom-made MATLAB algorithm included
BioMed Research International 5
the anthropometric characteristics as well as the UL kine-matics and the pushrim kinetics with respect to the labcoordinate system Shoulder net joint moments were thenexpressed in the same coordinate system used to expressshoulder joint kinematics and normalized against the bodymass of each participant In fact moderate to high associ-ations were found between body mass and mean and peakshoulder net joint moments when propelling with no slope(119903 = 0554 and 0577) and with slopes of varying degrees(119903 = 0713 to 0809) The peak and mean shoulder net jointmoments in the sagittal frontal and transverse plane werethe main outcome measures
27 Shoulder Muscular Demand The electromyographicactivity of the anterior and posterior portions of the del-toid along with the clavicular and sternal heads of thepectoralis major was recorded at the nondominant upperextremity at a sampling frequency of 1200Hz using a portabletelemetric system (NORAXON USA Inc Scottsdale Ari-zona Telemyo 900) Skin preparation and the placementof the surface electrodes (BlueSensor M AMBU BallerupDanmark) (AgAgCl sensor ndash132mm2 active surface area)were made in accordance with SENIAM recommendations(refer to httpwwwseniamorg) Following baseline noiseremoval all EMG signals recorded were visually inspectedbefore being filtered with a 4th order zero-lag Butterworthbandpass filter with low and high cut-off frequencies set at30 and 500Hz respectively Thereafter EMG patterns werefull-wave rectified and filtered with a 6Hz low-pass filterto generate EMG linear envelopes for each muscle studiedThe muscular utilization ratio (MUR ()) was calculatedfor each muscle studied by normalizing the amplitude ofthe EMG signals recorded during the experimental tasksagainst the peak EMG signal recorded over a 05 secondperiod during one of the two static maximum voluntarycontractions (MVC) Muscle-specific manual resistance wasapplied by a trained physiotherapist to generate the MVCswhile participants remained seated in their own wheelchairMeanwhile another research associate manually providedadditional trunk and wheelchair stability to participants Foreach muscle studied the peak and mean MURs as well as anindicator of muscle work (IMW) were calculated using theintegral of the MUR data were the main outcome measuresAll EMG signal processing was performed digitally using acustom-developed MATLAB algorithm
28 Statistical Analyses Descriptive statistics (mean plusmn SD)were calculated for the demographic and clinical character-istics of all participants as well as for the kinematic kineticand muscular demand outcome measures For these lastoutcome measures 10 propulsion cycles were averaged pertrial resulting in a total of 20 propulsion cycles for eachslope tested The kinematic kinetic and muscular demanddata recorded during the push phase of each cycle analyzedwere also time-normalized over 100 (ie 100 data points)to generate a profile for each participant and a mean groupprofile Shapiro-Wilk tests confirmed that the kinematickinetic and electromyographic outcome measures for all
slopes tested were normally distributed and justified the useof parametric statistical tests One-way repeated-measureanalyses of variance (ANOVA) with one within-subjectsfactor (slopes of 0∘ 27∘ 36∘ 48∘ and 71∘) using a generallinear model was used to determine the effect of the slopeson the kinematic and kinetic and electromyographic outcomemeasures and an eta-squared value was used to confirmif the proportion of the total variability attributable to theslope factor (ie effect size) was small (gt002) moderate(gt013) or large (gt026) Whenever an ANOVA revealedsignificant differences (main effect 119875 lt 005) after the resultof the Mauchlyrsquos test of sphericity of the covariance matrixwas taken into consideration Studentrsquos 119905-tests for pairedsamples were computed (post hoc tests) with a Bonferronicorrection setting the significance level at 119875 le 00125(119875 le 0054 pairwise comparisons) as a result of thefour possible slope increments (ie 0∘ to 27∘ 27∘ to 36∘36∘ to 48∘ and 48∘ to 71∘) All statistical analyses wereperformed with SPSS Statistics 170 software for WindowsNote that the kinematic and electromyographic data wereonly collected and computed at the nondominant UL sincequasi-symmetrical ULmovement strategies and efforts wereassumed in order to safely propel on a linear trajectory onthe motorized treadmill [21] and since the nondominant ULstrength generating capability is generally weaker than theone at the dominant UL possibly resulting in higher relativedemand at the nondominant UL during the performance ofa symmetrical functional task
3 Results
31 Completion Rate At a mean natural and constant self-selected propulsion speed of 117 plusmn 018ms [min = 091msmax = 165ms] all participants (completion rate = 100)were able to propel themselves on the 0∘ slope and up the27∘ slope (Table 2)The completion rate reached 889 (119873 =1618 participants) 778 (119873 = 1418 participants) and556 (119873 = 1018 participants) for the 36∘ 48∘ and 71∘slopes respectively (Table 2)
32 Temporal Parameters Table 3 summarizes the meanduration of the push and recovery phases and the totalduration of a propulsion cycle in seconds for the differenttreadmill slopes The average durations of the push phasewere similar for all tested slopes (ANOVA 119875 = 0267)whereas the average duration of the recovery phase declinedas the slope became steeper (post hoc tests 119875 le 0043) Thetotal duration significantly decreased as the slope becamesteeper (post hoc tests 119875 le 0001) except during the 27∘ to36∘ slope increment that remained similar
33 Trunk and Shoulder Kinematics The trunk and shouldermovement patterns are illustrated in Figures 2(a) 2(b) 2(c)and 2(d) whereas the minimum maximum and excur-sion of the trunk and shoulder movement amplitudes aresummarized in Table 4 The slopes of the treadmill signifi-cantly influenced most minimum maximum and excursiontrunk and shoulder movement amplitudes At the trunk all
6 BioMed Research International
Table 2 Description of self-selected comfortable propulsion speed experimental tasks completed and rate of perceived exertion
Participants Self-selected speed (ms) Slopes Rate of perceived exertion (10)0∘ 27∘ 36∘ 48∘ 71∘ 0∘ 27∘ 36∘ 48∘ 71∘
1 111 09 74 55 81 952 165 01 22 03 03 mdash3 105 13 13 39 44 714 118 08 17 37 48 785 120 17 48 25 59 796 091 30 63 77 mdash mdash7 148 09 97 mdash mdash mdash8 116 0 03 09 mdash mdash9 104 18 38 33 42 mdash10 127 0 0 0 0 011 139 10 15 33 27 3212 099 11 41 40 75 mdash13 106 42 88 mdash mdash mdash14 125 12 52 67 64 8515 103 00 06 19 36 mdash16 107 07 34 46 66 9217 106 07 62 26 65 8918 111 29 46 61 66 73Mean 117 119899 = 18 119899 = 18 119899 = 16 119899 = 14 119899 = 10 12 39 35 47 68SD 018 11 29 22 25 30
Table 3 Group average (SD) mean temporal parameter measured of the push phase measured at the nondominant handrim at the fivedifferent slopes tested
Slopes0∘ 27∘ 36∘ 48∘ 71∘
Temporal parameters (s)Push phase 048 plusmn 008 048 plusmn 008 049 plusmn 008 048 plusmn 007 048 plusmn 006Recovery phase 059 plusmn 022 027 plusmn 010 026 plusmn 009 022 plusmn 008 018 plusmn 005Total (cycle) 107 plusmn 023 075 plusmn 016 075 plusmn 014 070 plusmn 013 066 plusmn 010
minimum maximum and excursion movement amplitudessignificantly increased as the slope became steeper except forminimum and maximum values during the 27∘ to 36∘ slopeincrement that remained similar The greatest maximumforward trunk flexion (609∘) which was accompanied by thegreatest forward trunk excursion (224∘) was reached duringthe 71∘ slope At the shoulder the maximum shoulder flexionmovement amplitude significantly increased as the slopebecame steeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments The minimum maximum and excursion shoulderabduction movement amplitudes remained comparable asthe slope became steeper The minimum maximum andexcursion shoulder internal rotation movement amplitudesalso remained comparable as the slope became steeper with
the exception of the minimum and excursion values whichsignificantly increased during the 0∘ to 27∘ slope increment
34 Shoulder Kinetics The net shoulder flexion abductionand internal rotation moment patterns are illustrated inFigures 2(e) 2(f) and 2(g) while their mean and maximumvalues are summarized in Table 5 The greatest maximumshoulder moments were found during flexion across allslopes except for the 71∘ slope when the internal rotationgenerated the greatest moment All mean and maximumshouldermoments were significantly influenced by the slopesof the treadmill The mean and maximum flexion momentssignificantly improved as the slope increased except for the36∘ to 48∘ and 48∘ to 71∘ slope increments The meanadduction moments only significantly improved as the slopeincreased between 0∘ and 27∘ whereas the peak mean valueonly significantly improved as the slope increased between
BioMed Research International 7
0
10
20
30
40
50
60
70
80
Trun
k fle
xion
(+)
exte
nsio
n (minus
)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(a)
60
40
20
0
minus20
minus40
minus60
Shou
lder
flex
ion
(+)
exte
nsio
n (minus
)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(b)
0
10
20
30
40
50
60
Shou
lder
abdu
ctio
n (+
) ad
duct
ion
(minus)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(c)
0
10
20
30
40
50
60
70
0 20 40 60 80 100
Normalized time (100)Angle (∘)
Shou
lder
IR (+
) ER
(minus)
(d)
12
08
04
00
minus04
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder flexion (+) extension (minus)
(e)
04
02
00
minus02
minus04
minus06
minus08
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder abduction (+) adduction (minus)
(f)
Figure 2 Continued
8 BioMed Research International
10
08
06
04
02
00
minus02
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder IR (+) ER (minus)
(g)
Figure 2 Group averaged time-normalized profile (solid line) and standard deviation (dotted line) of the shoulder and trunk kinematics (ab c and d) and weight-normalised shoulder moments (e f and g) during the push phase for the five slopes tested at self-selected naturalspeed
the 0∘ to 27∘ 36∘ to 48∘ and 48∘ to 71∘ slope incrementsThemean and maximum internal rotation moments significantlyincreased as the slope became steeper except for the 36∘ to48∘ slope increment
35 Shoulder Muscular Demand The MUR patterns of themuscles studied are illustrated in Figure 3 while their meanand maximum values are summarized in Table 6 The meanIMWs of the muscles studied are summarized in Table 6 andillustrated in Figure 4 For allmuscles studied theirmean andmaximum MURs as well as their indicator of muscle workvalue significantly increased as the slope became steeperexcept for the posterior deltoid that remained comparablebetween the 27∘ to 36∘ slope increment
4 Discussion
This study quantified trunk and nondominant shoulderkinematic changes along with nondominant shoulder jointmoments and electromyographic changes during MWCpropulsion on a motorized treadmill set at a self-selectednatural speed on five different slopes (ie 0∘ 27∘ 36∘ 48∘and 71∘) Overall the MWC users with a SCI increasedforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increased during simulated uphillMWC propulsion on a motorized treadmill
41 Trunk and Shoulder Movement-Related Adaptations Themovement-related adaptations occurring at the trunk andshoulder partially support the hypothesis that their outcome
measures would gradually and significantly increase witheach slope increment while the speed remained constantAt the trunk the maximum forward trunk flexion and thetotal trunk excursion increased significantly as the slopebecame steeper except for the 27∘ to 36∘ slope incrementChow et al [5] obtained somewhat comparable resultsin terms of trunk kinematics although no difference wasrevealed when comparing 4∘ and 8∘ slopes This may beexplained by the fact that participants propelled at self-selected speeds that decreased progressively in their protocolas the slope increased Nonetheless the increased maximumforward trunk flexion coupled with the increased forwardtrunk excursion may allow MWC users to move their centreof mass further and faster anteriorly and to maintain itsprojection in front of the rear wheel axle in order toprevent backward tilt and falls as the slope increases Thismay also explain why maximum forward trunk flexion andforward trunk excursion became greater as the gravitationaleffects became harder to overcome with steeper slopes Thedecreasing success rate with a steeper slope may be explainedin part by the fact that some participants were classified asbeing overweight (body mass index gt 25) or class I obese(body mass index = 300ndash349) with associated abdominalobesity that limited their ability to increase forward trunkflexion to accommodate for the steeper slopes In fact 556of participants who were unable to propel up the 71∘ slopewere overweight (119873 = 3) or obese (119873 = 2) whereasonly 30 of participants who were able to propel up the 71∘slope were overweight (119873 = 2) or obese (119873 = 1) Henceabdominal circumference may deserve additional attentionwhen investigating wheelchair propulsion technique or man-ual wheelchair skills such as uphill propulsion
BioMed Research International 9
Table4Group
average(SD)totalexcursio
n(∘ )
and
maxim
umandminim
um(∘ )
kinematicvalues
measuredatthetrun
kandno
ndom
inantsho
uldera
tthe
fivedifferent
slopestestedas
wellasthe
results
oftheA
NOVA
andpo
stho
ccom
paris
ontest
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Jointangle(∘
)
Trun
kmdashflexion
(+)extension(minus)
Trun
kmdashflexion
(+)extension(minus)
Excursion
588
(212
)1267(340)
1456(277)
1761
(396)
2237
(600)lt0001
0907
lt0001
000
6lt0001
0003
Maxim
um1927(623)
3592(845)
3945(831
)4579(853
)6093(113
0)lt0001
0889
lt0001
0031
0002
0005
Minim
um1339
(614
)2326(775)
2490(805)
2818
(771)
3857(859)lt0001
0910
lt0001
0028
lt0001
lt0001
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Excursion
5567(920)
5817
(1092)
5963(901)
6019
(698)
6499(895)
0019
0296
0072
0183
0473
0217
Maxim
um1131
(934)
1800(820)
1935
(762)
2259(730)
3088(745)lt0001
0849
lt0001
0001
0054
lt0001
Minim
umminus44
36(935
)minus40
17(936)minus40
27(915
)minus3760(834)minus3410
(1036)lt0001
0651
lt0001
000
6lt0001
lt0001
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Excursion
935(343)
1227(716)
1348(661)
1488(756)
1965(118
8)0012
0337
0010
0363
0158
0047
Maxim
um3325(800)
3481(1065)
3540(1026)
3488(1057)
4060(1543)
0083
mdashmdash
mdashmdash
mdashMinim
um2390(627)
2253
(726)
2192(666)
2000(545)
2094(570)
0038
mdashmdash
mdashmdash
mdashShou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Excursion
2486(820)
3055(1024)
3335(883)
3452
(944)
4328(113
4)lt0001
0623
000
4004
00765
0013
Maxim
um3157(1682)
3789(1846
)40
15(19
17)
4302(1223)
4969(871)lt0001
0665
lt0001
0029
0855
0033
Minim
um671
(1357)
734(1510)
680
(1694)
850
(918
)641
(770)
0152
mdashmdash
mdashmdash
mdash
10 BioMed Research International
Table5Group
average(
SD)m
eanandpeak
weight-n
ormalise
dmom
ents(N
mkg)
measuredatthen
ondo
minantsho
uldera
tthe
fived
ifferentslopesa
swellasresultsof
theA
NOVA
and
postho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Normalisedmoments(Nmkg)
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Mean
0140(0056)
0226(0067)
0248(0081)
0233(0083)
0242(015
1)0027
0288
lt0001
0003
0433
0966
Peak
(maxim
um)
0292(010
9)0512(015
2)0546(016
7)0559(012
8)0733(0302)lt0001
0588
lt0001
000
40867
0049
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashaddu
ction(+)abdu
ction(minus)
Mean
minus0016(0023)minus006
0(0050)minus0069(0046
)minus0090(0043)minus0103(0036)lt0001
0623
lt0001
0414
0147
0366
Peak
(minim
um)minus0088(0041)minus0257(010
5)minus0278(010
4)minus0369(013
7)minus0494(013
3)lt0001
0797
lt0001
0149
0002
0002
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Mean
0097(0036)
0189(0050)
0222(0064
)0252(0065)
0344(010
1)lt0001
0726
lt0001
000
40191
0010
Peak
(maxim
um)
0196(0078)
0415(014
4)0456(012
9)0530(014
8)0780(018
4)lt0001
0801
lt0001
0001
0103
0001
BioMed Research International 11
00
02
04
06
08
10
Ant
erio
r delt
oid
(a)
00
02
04
06
08
10
(b)
00
02
04
06
08
10
(c)
00
02
04
06
08
10
12
Poste
rior d
eltoi
d
(d)
00
02
04
06
08
10
12
(e)
00
02
04
06
08
10
12
(f)
00
02
04
06
08
10
Clav
icul
ar h
ead
of p
ecto
ralis
maj
or
(g)
00
02
04
06
08
10
(h)
00
02
04
06
08
10
(i)
00
02
04
06
08
10
12
14
16
0 20 40 60 80 100
Ster
nal h
ead
of p
ecto
ralis
maj
or
Normalised time (100)Mean MUR pattern (1)
0∘
27∘
36∘
48∘
71∘
(j)
00
02
04
06
08
10
12
14
16
Mean MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(k)
00
02
04
06
08
10
12
14
16
Peak MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(l)
Figure 3 Group averaged time-normalized mean profile (solid line) and standard deviation (dotted line) (a d g and j) as well as group-average (SD) mean (b e h and k) and peak (c f i and l) muscle utilization ratio (MUR) during the push phase for the five slopes tested atself-selected natural speed
12 BioMed Research International
Table6Group
average(
1SD)meanmuscle
utilisatio
nratio
(MUR)peakMUR(1)and
indicatoro
fmuscle
work(IMW)v
aluesfor
each
muscle
assessed
atthen
ondo
minantsho
uldera
tfived
ifferentslope
angles
aswellasresultsof
theA
NOVA
andpo
stho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Anteriord
eltoid
Anteriord
eltoid
MeanMUR(1)
007
(004)
021
(009)
023
(012
)026
(010
)034
(013
)lt0001
0831
lt0001
0002
lt0001
0001
Peak
MUR(1)
014
(008)
044
(023)
048
(026)
054
(026)
068
(028)lt0001
0836
lt0001
0002
lt0001
lt0001
IMW
718(398)
2070(943)
2348(1237)
2606(1043)
3448(1304)lt0001
0829
lt0001
0003
lt0001
0002
Poste
riord
eltoid
Poste
riord
eltoid
MeanMUR(1)
008
(007)
020
(014
)024
(024)
023
(010
)027
(006)lt0001
0907
lt0001
0144
lt0001
lt0001
Peak
MUR(1)
020
(014
)052
(031
)062
(051)
060
(019
)077
(019
)lt0001
0894
lt0001
0027
0001
0005
IMW
795(692)
2036(1384)
2443(2381)
2335
(1047)
2734(648)lt0001
0906
lt0001
0143
lt0001
lt0001
Clavicular
fiberso
fpectoralis
major
Clavicular
fiberso
fpectoralis
major
MeanMUR(1)
007
(004)
018
(010
)020
(010
)027
(014
)035
(018
)lt0001
0754
lt0001
0003
lt0001
0005
Peak
MUR(1)
014
(009)
038
(022)
042
(023)
057
(031
)071
(029)lt0001
0814
lt0001
000
9lt0001
0001
IMW
700(426)
1837
(977)
2041(1046)
2704(14
32)
3528(175
7)lt0001
0752
lt0001
0003
lt0001
0005
Sternalfi
bersof
pectoralismajor
Sternalfi
bersof
pectoralismajor
MeanMUR(1)
012
(008)
030
(015
)032
(013
)037
(015
)053
(024)lt0001
0781
lt0001
0005
0001
000
6Peak
MUR(1)
021
(015
)054
(023)
059
(023)
071
(026)
101(042)lt0001
0829
lt0001
0003
lt0001
0002
IMW
1194(753)
3023(14
77)
3227(1323)
3753
(1511)
5280(2406)lt0001
0780
lt0001
0005
0001
000
6
BioMed Research International 13
0
10
20
30
40
50
60
70
80
Ant
erio
r delt
oid
Poste
rior d
eltoi
d
Clav
icul
ar h
ead
ofpe
ctor
alis
maj
or
Ster
nal h
ead
of
pect
oral
is m
ajor
IMW
0∘
27∘
36∘
48∘
71∘
Figure 4 Group averaged (SD) mean indicator of muscle work(IMW) during the push phase for the five slopes tested at self-selected natural speed
At the shoulder the maximum shoulder flexion move-ment amplitude significantly increased as the slope becamesteeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments It is possible that increasedmaximumshoulder flexionwas needed to accommodate for the increased forward trunkflexion and to apply most of the force tangentially on thehandrim to preserve mechanical efficiencyThe fact that onlythe duration of the recovery period drastically decreasedas the slope became steeper can also explain in part therelatively stable shoulder flexion-extension excursion (iesimilar push phase durations across slopes) This finding isconsistent to some extent with the work of Yang et al [3]who found comparable values of movement-related adap-tation at the shoulder when comparing level overgroundand uphill (ie 3∘ slope) MWC propulsions However theshoulder flexion-extension excursion significantly increasedon average by 937∘ and the shoulder extension remainedsimilar in their study contrary to the results of the presentstudy These discrepancies may be attributed to the fact thatparticipants used test wheelchairs that were not anchoredto a safety system when propelling up a 3∘ slope at 09mson a motorized treadmill the level surface propulsion (0∘slope) was performed overground and the shoulder kine-matic calculation differed from the work by Yang et al [3]Nevertheless all these results confirmed kinematic adapta-tions at the shoulder as the slope progressed Lastly theincreased forward trunk flexion coupled with an increasedshoulder flexion that modifies the orientation of the forcegenerated at the shoulder may increase posterior shoulderjoint forces and explain the elevated muscular demand at theposterior deltoid occurring towards the end of the push phase[22]
42 Shoulder Joint Mechanical and Muscular Effort Adap-tations The shoulder joint moments adaptations partiallysupport the hypothesis that their outcome measures wouldgradually and significantly increase with each slope incre-ment while the speed remained constant For two out of thethree shoulder net joint moments investigated most of themean and peak values for the shoulder flexor and internalrotator moments progressively increased as the slope becamesteeper aside from some outcomemeasures during the 27∘ to36∘ or the 36∘ to 48∘ slope increment The relative musculardemand adaptations and muscular work computed for allmuscles investigated fully support this hypothesis since theiroutcomemeasures gradually and significantly increased witheach slope increment while the speed remained constantHence once the results of these two approaches are com-bined it is clear that the shoulder mechanical and musculareffort increases are key contributors to the adaptation processassociated with the steeper slopes Moreover these resultsare in line with the perceived UL efforts expressed by theparticipants and may explain in part The decreasing successrate with a steeper slope as shoulder strength generatingcapability most likely becomes a determinant for propellingon steeper slopes
43 Implications for Clinical Practice With the use of a slopeor of a combination of slopes when a MWC user propelshimselfherself on a motorized treadmill therapists may beable to offer task-specific high-intensity short duration inter-val training programs to increase UL strength particularlyat the shoulders Cautiousness is advised with this practicesince the risk exposure (ie increased shoulder mechanicaland muscular demands) will progressively and significantlyincrease as the slope becomes steeper and will vary accordingto the strength-generating capability of each MWC user Inaddition since the risk exposure could trigger the develop-ment or exacerbation of secondary impairments at the ULparticularly at the shoulders such a program should alsobe accompanied by proper warm-up and cool-down periodsas well as by antagonist muscle strengthening to preventmuscle strength imbalance Alternatively therapists may alsooffer task-specific cardiorespiratory fitness training programswhen a MWC user propels on a motorized treadmill withno slope or minimal slope (lt27∘) with minimal demandsduring a prolonged period of time (ie cardiorespiratoryfitness training)
44 Limits of the Study The present study included a rela-tively small sample size (119899 = 18) of experienced MWC userswho have completed their rehabilitation process which maylimit the strength of the evidence and potential to generalizethe results with new MWCs respectively The fact that theparticipants used their personal wheelchairs during the studywarrants consideration as optimal wheelchair positioningand configuration parameters most likely differs across par-ticipants and impacts the outcome measures of interest inthe present study and the risk of the MWC tilting or fallingbackwards when propelling up a slope The use of the instru-mented wheels which slightly increase the width and weight
14 BioMed Research International
of the wheelchair along with rolling resistance may havemodified participantsrsquo propulsion technique (eg increasedshoulder abduction) and fatigue level (eg increased ULeffort) in comparison to propelling with their own wheelsThe self-selected natural treadmill speed determined for eachparticipant maintained across all slopes tested in an effort toisolate the effect of speed also requires consideration sinceMWCusers tend to reduce their speedwhen propelling uphillin daily life particularly on steep slopes [2] Finally thekinematic and kinetic and electromyographic variables solelyfocused on the trunk and nondominant shoulder prevent afull understanding of UL adaptations (ie elbow and wristnot studied) during motorized treadmill MWC propulsionacross different slopes
5 Conclusion
This study confirms that MWC users with a SCI increaseforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increase during simulated uphillMWC propulsion on a motorized treadmill Few similaritieswere found between the 27∘ to 36∘ and the 36∘ to 48∘ slopeincrements for shoulder flexion and adduction momentsFuture studies incorporating interactions with various slopesand velocities could strengthen the results of the presentstudy and provide additional evidence-based knowledge onwheelchair propulsion on a motorized treadmill
Abbreviations
AIS American Spinal Injury AssociationImpairment Scale
EMG ElectromyographyER External rotationLED Light-emitting diodeIMW Indicator of muscle workIR Internal rotationJCS Joint coordinate systemMUR Muscle utilization ratioMVC Maximum voluntary contractionMWC Manual wheelchairUL Upper limbWUSPI Wheelchair Userrsquos Shoulder Pain
Index
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors would like to thank Michel Goyette (Eng)Daniel Marineau (Technician) Youssef El Khamlichi(Research Associate) and Philippe Gourdou (ResearchAssociate) for their contributions to this project DanyGagnon holds a Junior 1 Research Career Award from
the Fonds de la recherche du Quebec-Sante (FRQ-S)Annie-Claude Babineau and Guillaume Desroches aresupported by a summer internship and a post-doctoralfellowship from the Canadian Institutes of Health Researchrespectively DanyGagnon andRachid Aissaoui aremembersof the Multidisciplinary SensoriMotor RehabilitationResearch Team (httpwwwerrsmca) supported bythe CIHR and the Quebec-Ontario Spinal Cord InjuryMobility (SCI-MOB) Research Group funded by theQuebec Rehabilitation Research Network (REPARhttpwwwreparca) and the Ontario NeuroTraumaFoundation (ONF httpwwwonforg) The project wasfunded in part by the Fonds de la recherche du Quebec-Sante(FRQS) The equipment and material required for theresearch completed at the Pathokinesiology Laboratory wasfinanced by the Canada Foundation for Innovation (CFI)
References
[1] B Mason J Lenton C Leicht and V Goosey-Tolfrey ldquoAphysiological and biomechanical comparison of over-groundtreadmill and ergometer wheelchair propulsionrdquo Journal ofSports Sciences vol 32 no 1 pp 78ndash91 2014
[2] W M Richter R Rodriguez K R Woods and P W AxelsonldquoStroke pattern and handrim biomechanics for level and uphillwheelchair propulsion at self-selected speedsrdquo Archives of Phys-ical Medicine and Rehabilitation vol 88 no 1 pp 81ndash87 2007
[3] Y-S Yang A M Koontz S-J Yeh and J-J Chang ldquoEffectof backrest height on wheelchair propulsion biomechanics forlevel and uphill conditionsrdquo Archives of Physical Medicine andRehabilitation vol 93 no 4 pp 654ndash659 2012
[4] D H Gagnon A-C Babineau A Champagne G Desrochesand R Aissaoui ldquoPushrim biomechanical changes with pro-gressive increases in slope during motorized treadmill manualwheelchair propulsion in individuals with spinal cord injuryrdquoJournal of Rehabilitation Research amp Development vol 51 no 5pp 789ndash802 2014
[5] J W Chow T A Millikan L G Carlton W-S Chae Y-T Lim and M I Morse ldquoKinematic and electromyographicanalysis of wheelchair propulsion on ramps of different slopesfor young men with Paraplegiardquo Archives of Physical Medicineand Rehabilitation vol 90 no 2 pp 271ndash278 2009
[6] S van Drongelen L H van Der Woude T W Janssen E LAngenot E K Chadwick and D H Veeger ldquoMechanical loadon the upper extremity during wheelchair activitiesrdquo Archivesof Physical Medicine and Rehabilitation vol 86 no 6 pp 1214ndash1220 2005
[7] H Arabi R Aissaoui J Rousseau D Bourbonnais and JDansereau ldquoEvaluation of minimal mechanical effort duringthe ramp access of manual wheelchairrdquo Ergonomia vol 26 no3 pp 253ndash259 2004
[8] K Kulig S S Rao S J Mulroy et al ldquoShoulder joint kineticsduring the push phase of wheelchair propulsionrdquo ClinicalOrthopaedics and Related Research no 354 pp 132ndash143 1998
[9] L J Chapman and J P Chapman ldquoThe measurement ofhandednessrdquoBrain andCognition vol 6 no 2 pp 175ndash183 1987
[10] Gouvernement du Quebec Regie du Batiment du Quebec(RBQ) Construction Code Building Act Chapter 1 Architec-tural and Transportation Barriers Compliance Board 2013
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 BioMed Research International
(a) (b) (c)
Figure 1 Illustration of three slopes tested during motorized treadmill MWC propulsion (a) 0∘ slope (b) 36∘ slope and (c) 71∘ slope
the MWC a total of 27 skin-fixed light-emitting diodes(LEDs) were placed on specific anatomical landmarks whilefour LEDs were fixed to the MWC frame [14] The 3Dcoordinates of each LED within the laboratory coordinatesystem were collected at 30Hz with a motion capture systemincorporating four synchronised camera units (Optotrack3020 and Optotrack Certus Northern Digital Inc WaterlooOntario Canada httpwwwndigitalcom) Supplementarybony landmarks wheelchair and treadmill reference pointswere digitised to determine principal axes of segments andlocate articular joint centres for the trunk and nondomi-nant UL wheelchair position and treadmill slope Beforeinitiating the experimental tasks three abduction-adductionand three flexion-extension active movements were recordedto locate the shoulder articular centre with respect to thescapula using a quadratic sphere fitting procedure [15 16] Allmarker trajectories were visually inspected and interpolatedwhen coordinates were missing using a linear or a cubicspline method The marker trajectories were then filteredusing a 4th order zero-lag Butterworth filter with a cutofffrequency set at 6Hz The recommendations formulated bythe International Society of Biomechanics [17] were used todetermine segmental coordinate systems (head trunk armsforearms and hand) Relative motion between the humerusand clavicle used as a surrogate rigid segment for the scapulathat articulates with the humerus [17] was computed using aZX1015840Y10158401015840 cardanic rotation sequence to avoid gimbal lock andto interpret reconstructed shoulder movements according tothree anatomical movements commonly described in clinicalpractice (ie flexionextension abductionadduction inter-nal and external rotations) [18] The relative trunk forwardinclination angle (ie forward trunk flexion) was computedas the motion of the vertical axis of the trunk defined by
a unit vector created with the midpoint between the eighththoracic vertebra and the xiphoid process to the midpointbetween the seventh cervical vertebra and the sternal notchwith respect to the vertical axis of the laboratory coordinatesystem For the trunk forward flexionextension and theshoulder flexionextension adductionadduction and inter-nalexternal rotation the minimal and maximal movementsalong with their total excursion were the main outcomemeasures
25 Handrim Kinetics Each participantrsquos MWC wasequipped bilaterally with 2410158401015840 or 2610158401015840 instrumented wheels(SmartWheel (SmartWheel Out-Front (formerly ThreeRivers Holdings LLC) Mesa Arizona United Stateshttpwwwout-frontcom)) to measure the three dimen-sional components of the total force applied at the handrimduring MWC propulsion at a sampling frequency of 240Hz[19] While these instrumented wheels did not alter axleposition or other rear wheel spatial characteristics (egorientation and diameter of the handrim) they slightlyincreased wheelchair width and weight (48 kginstrumentedwheel) and may have affected rolling resistance (ieurethane tire) Three dimensional handrim kinetic datawere filtered with a 4th order Butterworth filter anda cutoff frequency of 20Hz and then downsampled to30Hz to fit the kinematic data using a custom MATLAB(MATLAB MathWorks Natick Massachusetts UnitedStates httpwwwmathworkscom) routine
26 Shoulder Kinetics Shoulder net joint moments werecomputed using an inverse dynamic method [20] The dataentered into a custom-made MATLAB algorithm included
BioMed Research International 5
the anthropometric characteristics as well as the UL kine-matics and the pushrim kinetics with respect to the labcoordinate system Shoulder net joint moments were thenexpressed in the same coordinate system used to expressshoulder joint kinematics and normalized against the bodymass of each participant In fact moderate to high associ-ations were found between body mass and mean and peakshoulder net joint moments when propelling with no slope(119903 = 0554 and 0577) and with slopes of varying degrees(119903 = 0713 to 0809) The peak and mean shoulder net jointmoments in the sagittal frontal and transverse plane werethe main outcome measures
27 Shoulder Muscular Demand The electromyographicactivity of the anterior and posterior portions of the del-toid along with the clavicular and sternal heads of thepectoralis major was recorded at the nondominant upperextremity at a sampling frequency of 1200Hz using a portabletelemetric system (NORAXON USA Inc Scottsdale Ari-zona Telemyo 900) Skin preparation and the placementof the surface electrodes (BlueSensor M AMBU BallerupDanmark) (AgAgCl sensor ndash132mm2 active surface area)were made in accordance with SENIAM recommendations(refer to httpwwwseniamorg) Following baseline noiseremoval all EMG signals recorded were visually inspectedbefore being filtered with a 4th order zero-lag Butterworthbandpass filter with low and high cut-off frequencies set at30 and 500Hz respectively Thereafter EMG patterns werefull-wave rectified and filtered with a 6Hz low-pass filterto generate EMG linear envelopes for each muscle studiedThe muscular utilization ratio (MUR ()) was calculatedfor each muscle studied by normalizing the amplitude ofthe EMG signals recorded during the experimental tasksagainst the peak EMG signal recorded over a 05 secondperiod during one of the two static maximum voluntarycontractions (MVC) Muscle-specific manual resistance wasapplied by a trained physiotherapist to generate the MVCswhile participants remained seated in their own wheelchairMeanwhile another research associate manually providedadditional trunk and wheelchair stability to participants Foreach muscle studied the peak and mean MURs as well as anindicator of muscle work (IMW) were calculated using theintegral of the MUR data were the main outcome measuresAll EMG signal processing was performed digitally using acustom-developed MATLAB algorithm
28 Statistical Analyses Descriptive statistics (mean plusmn SD)were calculated for the demographic and clinical character-istics of all participants as well as for the kinematic kineticand muscular demand outcome measures For these lastoutcome measures 10 propulsion cycles were averaged pertrial resulting in a total of 20 propulsion cycles for eachslope tested The kinematic kinetic and muscular demanddata recorded during the push phase of each cycle analyzedwere also time-normalized over 100 (ie 100 data points)to generate a profile for each participant and a mean groupprofile Shapiro-Wilk tests confirmed that the kinematickinetic and electromyographic outcome measures for all
slopes tested were normally distributed and justified the useof parametric statistical tests One-way repeated-measureanalyses of variance (ANOVA) with one within-subjectsfactor (slopes of 0∘ 27∘ 36∘ 48∘ and 71∘) using a generallinear model was used to determine the effect of the slopeson the kinematic and kinetic and electromyographic outcomemeasures and an eta-squared value was used to confirmif the proportion of the total variability attributable to theslope factor (ie effect size) was small (gt002) moderate(gt013) or large (gt026) Whenever an ANOVA revealedsignificant differences (main effect 119875 lt 005) after the resultof the Mauchlyrsquos test of sphericity of the covariance matrixwas taken into consideration Studentrsquos 119905-tests for pairedsamples were computed (post hoc tests) with a Bonferronicorrection setting the significance level at 119875 le 00125(119875 le 0054 pairwise comparisons) as a result of thefour possible slope increments (ie 0∘ to 27∘ 27∘ to 36∘36∘ to 48∘ and 48∘ to 71∘) All statistical analyses wereperformed with SPSS Statistics 170 software for WindowsNote that the kinematic and electromyographic data wereonly collected and computed at the nondominant UL sincequasi-symmetrical ULmovement strategies and efforts wereassumed in order to safely propel on a linear trajectory onthe motorized treadmill [21] and since the nondominant ULstrength generating capability is generally weaker than theone at the dominant UL possibly resulting in higher relativedemand at the nondominant UL during the performance ofa symmetrical functional task
3 Results
31 Completion Rate At a mean natural and constant self-selected propulsion speed of 117 plusmn 018ms [min = 091msmax = 165ms] all participants (completion rate = 100)were able to propel themselves on the 0∘ slope and up the27∘ slope (Table 2)The completion rate reached 889 (119873 =1618 participants) 778 (119873 = 1418 participants) and556 (119873 = 1018 participants) for the 36∘ 48∘ and 71∘slopes respectively (Table 2)
32 Temporal Parameters Table 3 summarizes the meanduration of the push and recovery phases and the totalduration of a propulsion cycle in seconds for the differenttreadmill slopes The average durations of the push phasewere similar for all tested slopes (ANOVA 119875 = 0267)whereas the average duration of the recovery phase declinedas the slope became steeper (post hoc tests 119875 le 0043) Thetotal duration significantly decreased as the slope becamesteeper (post hoc tests 119875 le 0001) except during the 27∘ to36∘ slope increment that remained similar
33 Trunk and Shoulder Kinematics The trunk and shouldermovement patterns are illustrated in Figures 2(a) 2(b) 2(c)and 2(d) whereas the minimum maximum and excur-sion of the trunk and shoulder movement amplitudes aresummarized in Table 4 The slopes of the treadmill signifi-cantly influenced most minimum maximum and excursiontrunk and shoulder movement amplitudes At the trunk all
6 BioMed Research International
Table 2 Description of self-selected comfortable propulsion speed experimental tasks completed and rate of perceived exertion
Participants Self-selected speed (ms) Slopes Rate of perceived exertion (10)0∘ 27∘ 36∘ 48∘ 71∘ 0∘ 27∘ 36∘ 48∘ 71∘
1 111 09 74 55 81 952 165 01 22 03 03 mdash3 105 13 13 39 44 714 118 08 17 37 48 785 120 17 48 25 59 796 091 30 63 77 mdash mdash7 148 09 97 mdash mdash mdash8 116 0 03 09 mdash mdash9 104 18 38 33 42 mdash10 127 0 0 0 0 011 139 10 15 33 27 3212 099 11 41 40 75 mdash13 106 42 88 mdash mdash mdash14 125 12 52 67 64 8515 103 00 06 19 36 mdash16 107 07 34 46 66 9217 106 07 62 26 65 8918 111 29 46 61 66 73Mean 117 119899 = 18 119899 = 18 119899 = 16 119899 = 14 119899 = 10 12 39 35 47 68SD 018 11 29 22 25 30
Table 3 Group average (SD) mean temporal parameter measured of the push phase measured at the nondominant handrim at the fivedifferent slopes tested
Slopes0∘ 27∘ 36∘ 48∘ 71∘
Temporal parameters (s)Push phase 048 plusmn 008 048 plusmn 008 049 plusmn 008 048 plusmn 007 048 plusmn 006Recovery phase 059 plusmn 022 027 plusmn 010 026 plusmn 009 022 plusmn 008 018 plusmn 005Total (cycle) 107 plusmn 023 075 plusmn 016 075 plusmn 014 070 plusmn 013 066 plusmn 010
minimum maximum and excursion movement amplitudessignificantly increased as the slope became steeper except forminimum and maximum values during the 27∘ to 36∘ slopeincrement that remained similar The greatest maximumforward trunk flexion (609∘) which was accompanied by thegreatest forward trunk excursion (224∘) was reached duringthe 71∘ slope At the shoulder the maximum shoulder flexionmovement amplitude significantly increased as the slopebecame steeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments The minimum maximum and excursion shoulderabduction movement amplitudes remained comparable asthe slope became steeper The minimum maximum andexcursion shoulder internal rotation movement amplitudesalso remained comparable as the slope became steeper with
the exception of the minimum and excursion values whichsignificantly increased during the 0∘ to 27∘ slope increment
34 Shoulder Kinetics The net shoulder flexion abductionand internal rotation moment patterns are illustrated inFigures 2(e) 2(f) and 2(g) while their mean and maximumvalues are summarized in Table 5 The greatest maximumshoulder moments were found during flexion across allslopes except for the 71∘ slope when the internal rotationgenerated the greatest moment All mean and maximumshouldermoments were significantly influenced by the slopesof the treadmill The mean and maximum flexion momentssignificantly improved as the slope increased except for the36∘ to 48∘ and 48∘ to 71∘ slope increments The meanadduction moments only significantly improved as the slopeincreased between 0∘ and 27∘ whereas the peak mean valueonly significantly improved as the slope increased between
BioMed Research International 7
0
10
20
30
40
50
60
70
80
Trun
k fle
xion
(+)
exte
nsio
n (minus
)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(a)
60
40
20
0
minus20
minus40
minus60
Shou
lder
flex
ion
(+)
exte
nsio
n (minus
)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(b)
0
10
20
30
40
50
60
Shou
lder
abdu
ctio
n (+
) ad
duct
ion
(minus)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(c)
0
10
20
30
40
50
60
70
0 20 40 60 80 100
Normalized time (100)Angle (∘)
Shou
lder
IR (+
) ER
(minus)
(d)
12
08
04
00
minus04
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder flexion (+) extension (minus)
(e)
04
02
00
minus02
minus04
minus06
minus08
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder abduction (+) adduction (minus)
(f)
Figure 2 Continued
8 BioMed Research International
10
08
06
04
02
00
minus02
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder IR (+) ER (minus)
(g)
Figure 2 Group averaged time-normalized profile (solid line) and standard deviation (dotted line) of the shoulder and trunk kinematics (ab c and d) and weight-normalised shoulder moments (e f and g) during the push phase for the five slopes tested at self-selected naturalspeed
the 0∘ to 27∘ 36∘ to 48∘ and 48∘ to 71∘ slope incrementsThemean and maximum internal rotation moments significantlyincreased as the slope became steeper except for the 36∘ to48∘ slope increment
35 Shoulder Muscular Demand The MUR patterns of themuscles studied are illustrated in Figure 3 while their meanand maximum values are summarized in Table 6 The meanIMWs of the muscles studied are summarized in Table 6 andillustrated in Figure 4 For allmuscles studied theirmean andmaximum MURs as well as their indicator of muscle workvalue significantly increased as the slope became steeperexcept for the posterior deltoid that remained comparablebetween the 27∘ to 36∘ slope increment
4 Discussion
This study quantified trunk and nondominant shoulderkinematic changes along with nondominant shoulder jointmoments and electromyographic changes during MWCpropulsion on a motorized treadmill set at a self-selectednatural speed on five different slopes (ie 0∘ 27∘ 36∘ 48∘and 71∘) Overall the MWC users with a SCI increasedforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increased during simulated uphillMWC propulsion on a motorized treadmill
41 Trunk and Shoulder Movement-Related Adaptations Themovement-related adaptations occurring at the trunk andshoulder partially support the hypothesis that their outcome
measures would gradually and significantly increase witheach slope increment while the speed remained constantAt the trunk the maximum forward trunk flexion and thetotal trunk excursion increased significantly as the slopebecame steeper except for the 27∘ to 36∘ slope incrementChow et al [5] obtained somewhat comparable resultsin terms of trunk kinematics although no difference wasrevealed when comparing 4∘ and 8∘ slopes This may beexplained by the fact that participants propelled at self-selected speeds that decreased progressively in their protocolas the slope increased Nonetheless the increased maximumforward trunk flexion coupled with the increased forwardtrunk excursion may allow MWC users to move their centreof mass further and faster anteriorly and to maintain itsprojection in front of the rear wheel axle in order toprevent backward tilt and falls as the slope increases Thismay also explain why maximum forward trunk flexion andforward trunk excursion became greater as the gravitationaleffects became harder to overcome with steeper slopes Thedecreasing success rate with a steeper slope may be explainedin part by the fact that some participants were classified asbeing overweight (body mass index gt 25) or class I obese(body mass index = 300ndash349) with associated abdominalobesity that limited their ability to increase forward trunkflexion to accommodate for the steeper slopes In fact 556of participants who were unable to propel up the 71∘ slopewere overweight (119873 = 3) or obese (119873 = 2) whereasonly 30 of participants who were able to propel up the 71∘slope were overweight (119873 = 2) or obese (119873 = 1) Henceabdominal circumference may deserve additional attentionwhen investigating wheelchair propulsion technique or man-ual wheelchair skills such as uphill propulsion
BioMed Research International 9
Table4Group
average(SD)totalexcursio
n(∘ )
and
maxim
umandminim
um(∘ )
kinematicvalues
measuredatthetrun
kandno
ndom
inantsho
uldera
tthe
fivedifferent
slopestestedas
wellasthe
results
oftheA
NOVA
andpo
stho
ccom
paris
ontest
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Jointangle(∘
)
Trun
kmdashflexion
(+)extension(minus)
Trun
kmdashflexion
(+)extension(minus)
Excursion
588
(212
)1267(340)
1456(277)
1761
(396)
2237
(600)lt0001
0907
lt0001
000
6lt0001
0003
Maxim
um1927(623)
3592(845)
3945(831
)4579(853
)6093(113
0)lt0001
0889
lt0001
0031
0002
0005
Minim
um1339
(614
)2326(775)
2490(805)
2818
(771)
3857(859)lt0001
0910
lt0001
0028
lt0001
lt0001
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Excursion
5567(920)
5817
(1092)
5963(901)
6019
(698)
6499(895)
0019
0296
0072
0183
0473
0217
Maxim
um1131
(934)
1800(820)
1935
(762)
2259(730)
3088(745)lt0001
0849
lt0001
0001
0054
lt0001
Minim
umminus44
36(935
)minus40
17(936)minus40
27(915
)minus3760(834)minus3410
(1036)lt0001
0651
lt0001
000
6lt0001
lt0001
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Excursion
935(343)
1227(716)
1348(661)
1488(756)
1965(118
8)0012
0337
0010
0363
0158
0047
Maxim
um3325(800)
3481(1065)
3540(1026)
3488(1057)
4060(1543)
0083
mdashmdash
mdashmdash
mdashMinim
um2390(627)
2253
(726)
2192(666)
2000(545)
2094(570)
0038
mdashmdash
mdashmdash
mdashShou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Excursion
2486(820)
3055(1024)
3335(883)
3452
(944)
4328(113
4)lt0001
0623
000
4004
00765
0013
Maxim
um3157(1682)
3789(1846
)40
15(19
17)
4302(1223)
4969(871)lt0001
0665
lt0001
0029
0855
0033
Minim
um671
(1357)
734(1510)
680
(1694)
850
(918
)641
(770)
0152
mdashmdash
mdashmdash
mdash
10 BioMed Research International
Table5Group
average(
SD)m
eanandpeak
weight-n
ormalise
dmom
ents(N
mkg)
measuredatthen
ondo
minantsho
uldera
tthe
fived
ifferentslopesa
swellasresultsof
theA
NOVA
and
postho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Normalisedmoments(Nmkg)
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Mean
0140(0056)
0226(0067)
0248(0081)
0233(0083)
0242(015
1)0027
0288
lt0001
0003
0433
0966
Peak
(maxim
um)
0292(010
9)0512(015
2)0546(016
7)0559(012
8)0733(0302)lt0001
0588
lt0001
000
40867
0049
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashaddu
ction(+)abdu
ction(minus)
Mean
minus0016(0023)minus006
0(0050)minus0069(0046
)minus0090(0043)minus0103(0036)lt0001
0623
lt0001
0414
0147
0366
Peak
(minim
um)minus0088(0041)minus0257(010
5)minus0278(010
4)minus0369(013
7)minus0494(013
3)lt0001
0797
lt0001
0149
0002
0002
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Mean
0097(0036)
0189(0050)
0222(0064
)0252(0065)
0344(010
1)lt0001
0726
lt0001
000
40191
0010
Peak
(maxim
um)
0196(0078)
0415(014
4)0456(012
9)0530(014
8)0780(018
4)lt0001
0801
lt0001
0001
0103
0001
BioMed Research International 11
00
02
04
06
08
10
Ant
erio
r delt
oid
(a)
00
02
04
06
08
10
(b)
00
02
04
06
08
10
(c)
00
02
04
06
08
10
12
Poste
rior d
eltoi
d
(d)
00
02
04
06
08
10
12
(e)
00
02
04
06
08
10
12
(f)
00
02
04
06
08
10
Clav
icul
ar h
ead
of p
ecto
ralis
maj
or
(g)
00
02
04
06
08
10
(h)
00
02
04
06
08
10
(i)
00
02
04
06
08
10
12
14
16
0 20 40 60 80 100
Ster
nal h
ead
of p
ecto
ralis
maj
or
Normalised time (100)Mean MUR pattern (1)
0∘
27∘
36∘
48∘
71∘
(j)
00
02
04
06
08
10
12
14
16
Mean MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(k)
00
02
04
06
08
10
12
14
16
Peak MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(l)
Figure 3 Group averaged time-normalized mean profile (solid line) and standard deviation (dotted line) (a d g and j) as well as group-average (SD) mean (b e h and k) and peak (c f i and l) muscle utilization ratio (MUR) during the push phase for the five slopes tested atself-selected natural speed
12 BioMed Research International
Table6Group
average(
1SD)meanmuscle
utilisatio
nratio
(MUR)peakMUR(1)and
indicatoro
fmuscle
work(IMW)v
aluesfor
each
muscle
assessed
atthen
ondo
minantsho
uldera
tfived
ifferentslope
angles
aswellasresultsof
theA
NOVA
andpo
stho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Anteriord
eltoid
Anteriord
eltoid
MeanMUR(1)
007
(004)
021
(009)
023
(012
)026
(010
)034
(013
)lt0001
0831
lt0001
0002
lt0001
0001
Peak
MUR(1)
014
(008)
044
(023)
048
(026)
054
(026)
068
(028)lt0001
0836
lt0001
0002
lt0001
lt0001
IMW
718(398)
2070(943)
2348(1237)
2606(1043)
3448(1304)lt0001
0829
lt0001
0003
lt0001
0002
Poste
riord
eltoid
Poste
riord
eltoid
MeanMUR(1)
008
(007)
020
(014
)024
(024)
023
(010
)027
(006)lt0001
0907
lt0001
0144
lt0001
lt0001
Peak
MUR(1)
020
(014
)052
(031
)062
(051)
060
(019
)077
(019
)lt0001
0894
lt0001
0027
0001
0005
IMW
795(692)
2036(1384)
2443(2381)
2335
(1047)
2734(648)lt0001
0906
lt0001
0143
lt0001
lt0001
Clavicular
fiberso
fpectoralis
major
Clavicular
fiberso
fpectoralis
major
MeanMUR(1)
007
(004)
018
(010
)020
(010
)027
(014
)035
(018
)lt0001
0754
lt0001
0003
lt0001
0005
Peak
MUR(1)
014
(009)
038
(022)
042
(023)
057
(031
)071
(029)lt0001
0814
lt0001
000
9lt0001
0001
IMW
700(426)
1837
(977)
2041(1046)
2704(14
32)
3528(175
7)lt0001
0752
lt0001
0003
lt0001
0005
Sternalfi
bersof
pectoralismajor
Sternalfi
bersof
pectoralismajor
MeanMUR(1)
012
(008)
030
(015
)032
(013
)037
(015
)053
(024)lt0001
0781
lt0001
0005
0001
000
6Peak
MUR(1)
021
(015
)054
(023)
059
(023)
071
(026)
101(042)lt0001
0829
lt0001
0003
lt0001
0002
IMW
1194(753)
3023(14
77)
3227(1323)
3753
(1511)
5280(2406)lt0001
0780
lt0001
0005
0001
000
6
BioMed Research International 13
0
10
20
30
40
50
60
70
80
Ant
erio
r delt
oid
Poste
rior d
eltoi
d
Clav
icul
ar h
ead
ofpe
ctor
alis
maj
or
Ster
nal h
ead
of
pect
oral
is m
ajor
IMW
0∘
27∘
36∘
48∘
71∘
Figure 4 Group averaged (SD) mean indicator of muscle work(IMW) during the push phase for the five slopes tested at self-selected natural speed
At the shoulder the maximum shoulder flexion move-ment amplitude significantly increased as the slope becamesteeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments It is possible that increasedmaximumshoulder flexionwas needed to accommodate for the increased forward trunkflexion and to apply most of the force tangentially on thehandrim to preserve mechanical efficiencyThe fact that onlythe duration of the recovery period drastically decreasedas the slope became steeper can also explain in part therelatively stable shoulder flexion-extension excursion (iesimilar push phase durations across slopes) This finding isconsistent to some extent with the work of Yang et al [3]who found comparable values of movement-related adap-tation at the shoulder when comparing level overgroundand uphill (ie 3∘ slope) MWC propulsions However theshoulder flexion-extension excursion significantly increasedon average by 937∘ and the shoulder extension remainedsimilar in their study contrary to the results of the presentstudy These discrepancies may be attributed to the fact thatparticipants used test wheelchairs that were not anchoredto a safety system when propelling up a 3∘ slope at 09mson a motorized treadmill the level surface propulsion (0∘slope) was performed overground and the shoulder kine-matic calculation differed from the work by Yang et al [3]Nevertheless all these results confirmed kinematic adapta-tions at the shoulder as the slope progressed Lastly theincreased forward trunk flexion coupled with an increasedshoulder flexion that modifies the orientation of the forcegenerated at the shoulder may increase posterior shoulderjoint forces and explain the elevated muscular demand at theposterior deltoid occurring towards the end of the push phase[22]
42 Shoulder Joint Mechanical and Muscular Effort Adap-tations The shoulder joint moments adaptations partiallysupport the hypothesis that their outcome measures wouldgradually and significantly increase with each slope incre-ment while the speed remained constant For two out of thethree shoulder net joint moments investigated most of themean and peak values for the shoulder flexor and internalrotator moments progressively increased as the slope becamesteeper aside from some outcomemeasures during the 27∘ to36∘ or the 36∘ to 48∘ slope increment The relative musculardemand adaptations and muscular work computed for allmuscles investigated fully support this hypothesis since theiroutcomemeasures gradually and significantly increased witheach slope increment while the speed remained constantHence once the results of these two approaches are com-bined it is clear that the shoulder mechanical and musculareffort increases are key contributors to the adaptation processassociated with the steeper slopes Moreover these resultsare in line with the perceived UL efforts expressed by theparticipants and may explain in part The decreasing successrate with a steeper slope as shoulder strength generatingcapability most likely becomes a determinant for propellingon steeper slopes
43 Implications for Clinical Practice With the use of a slopeor of a combination of slopes when a MWC user propelshimselfherself on a motorized treadmill therapists may beable to offer task-specific high-intensity short duration inter-val training programs to increase UL strength particularlyat the shoulders Cautiousness is advised with this practicesince the risk exposure (ie increased shoulder mechanicaland muscular demands) will progressively and significantlyincrease as the slope becomes steeper and will vary accordingto the strength-generating capability of each MWC user Inaddition since the risk exposure could trigger the develop-ment or exacerbation of secondary impairments at the ULparticularly at the shoulders such a program should alsobe accompanied by proper warm-up and cool-down periodsas well as by antagonist muscle strengthening to preventmuscle strength imbalance Alternatively therapists may alsooffer task-specific cardiorespiratory fitness training programswhen a MWC user propels on a motorized treadmill withno slope or minimal slope (lt27∘) with minimal demandsduring a prolonged period of time (ie cardiorespiratoryfitness training)
44 Limits of the Study The present study included a rela-tively small sample size (119899 = 18) of experienced MWC userswho have completed their rehabilitation process which maylimit the strength of the evidence and potential to generalizethe results with new MWCs respectively The fact that theparticipants used their personal wheelchairs during the studywarrants consideration as optimal wheelchair positioningand configuration parameters most likely differs across par-ticipants and impacts the outcome measures of interest inthe present study and the risk of the MWC tilting or fallingbackwards when propelling up a slope The use of the instru-mented wheels which slightly increase the width and weight
14 BioMed Research International
of the wheelchair along with rolling resistance may havemodified participantsrsquo propulsion technique (eg increasedshoulder abduction) and fatigue level (eg increased ULeffort) in comparison to propelling with their own wheelsThe self-selected natural treadmill speed determined for eachparticipant maintained across all slopes tested in an effort toisolate the effect of speed also requires consideration sinceMWCusers tend to reduce their speedwhen propelling uphillin daily life particularly on steep slopes [2] Finally thekinematic and kinetic and electromyographic variables solelyfocused on the trunk and nondominant shoulder prevent afull understanding of UL adaptations (ie elbow and wristnot studied) during motorized treadmill MWC propulsionacross different slopes
5 Conclusion
This study confirms that MWC users with a SCI increaseforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increase during simulated uphillMWC propulsion on a motorized treadmill Few similaritieswere found between the 27∘ to 36∘ and the 36∘ to 48∘ slopeincrements for shoulder flexion and adduction momentsFuture studies incorporating interactions with various slopesand velocities could strengthen the results of the presentstudy and provide additional evidence-based knowledge onwheelchair propulsion on a motorized treadmill
Abbreviations
AIS American Spinal Injury AssociationImpairment Scale
EMG ElectromyographyER External rotationLED Light-emitting diodeIMW Indicator of muscle workIR Internal rotationJCS Joint coordinate systemMUR Muscle utilization ratioMVC Maximum voluntary contractionMWC Manual wheelchairUL Upper limbWUSPI Wheelchair Userrsquos Shoulder Pain
Index
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors would like to thank Michel Goyette (Eng)Daniel Marineau (Technician) Youssef El Khamlichi(Research Associate) and Philippe Gourdou (ResearchAssociate) for their contributions to this project DanyGagnon holds a Junior 1 Research Career Award from
the Fonds de la recherche du Quebec-Sante (FRQ-S)Annie-Claude Babineau and Guillaume Desroches aresupported by a summer internship and a post-doctoralfellowship from the Canadian Institutes of Health Researchrespectively DanyGagnon andRachid Aissaoui aremembersof the Multidisciplinary SensoriMotor RehabilitationResearch Team (httpwwwerrsmca) supported bythe CIHR and the Quebec-Ontario Spinal Cord InjuryMobility (SCI-MOB) Research Group funded by theQuebec Rehabilitation Research Network (REPARhttpwwwreparca) and the Ontario NeuroTraumaFoundation (ONF httpwwwonforg) The project wasfunded in part by the Fonds de la recherche du Quebec-Sante(FRQS) The equipment and material required for theresearch completed at the Pathokinesiology Laboratory wasfinanced by the Canada Foundation for Innovation (CFI)
References
[1] B Mason J Lenton C Leicht and V Goosey-Tolfrey ldquoAphysiological and biomechanical comparison of over-groundtreadmill and ergometer wheelchair propulsionrdquo Journal ofSports Sciences vol 32 no 1 pp 78ndash91 2014
[2] W M Richter R Rodriguez K R Woods and P W AxelsonldquoStroke pattern and handrim biomechanics for level and uphillwheelchair propulsion at self-selected speedsrdquo Archives of Phys-ical Medicine and Rehabilitation vol 88 no 1 pp 81ndash87 2007
[3] Y-S Yang A M Koontz S-J Yeh and J-J Chang ldquoEffectof backrest height on wheelchair propulsion biomechanics forlevel and uphill conditionsrdquo Archives of Physical Medicine andRehabilitation vol 93 no 4 pp 654ndash659 2012
[4] D H Gagnon A-C Babineau A Champagne G Desrochesand R Aissaoui ldquoPushrim biomechanical changes with pro-gressive increases in slope during motorized treadmill manualwheelchair propulsion in individuals with spinal cord injuryrdquoJournal of Rehabilitation Research amp Development vol 51 no 5pp 789ndash802 2014
[5] J W Chow T A Millikan L G Carlton W-S Chae Y-T Lim and M I Morse ldquoKinematic and electromyographicanalysis of wheelchair propulsion on ramps of different slopesfor young men with Paraplegiardquo Archives of Physical Medicineand Rehabilitation vol 90 no 2 pp 271ndash278 2009
[6] S van Drongelen L H van Der Woude T W Janssen E LAngenot E K Chadwick and D H Veeger ldquoMechanical loadon the upper extremity during wheelchair activitiesrdquo Archivesof Physical Medicine and Rehabilitation vol 86 no 6 pp 1214ndash1220 2005
[7] H Arabi R Aissaoui J Rousseau D Bourbonnais and JDansereau ldquoEvaluation of minimal mechanical effort duringthe ramp access of manual wheelchairrdquo Ergonomia vol 26 no3 pp 253ndash259 2004
[8] K Kulig S S Rao S J Mulroy et al ldquoShoulder joint kineticsduring the push phase of wheelchair propulsionrdquo ClinicalOrthopaedics and Related Research no 354 pp 132ndash143 1998
[9] L J Chapman and J P Chapman ldquoThe measurement ofhandednessrdquoBrain andCognition vol 6 no 2 pp 175ndash183 1987
[10] Gouvernement du Quebec Regie du Batiment du Quebec(RBQ) Construction Code Building Act Chapter 1 Architec-tural and Transportation Barriers Compliance Board 2013
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 5
the anthropometric characteristics as well as the UL kine-matics and the pushrim kinetics with respect to the labcoordinate system Shoulder net joint moments were thenexpressed in the same coordinate system used to expressshoulder joint kinematics and normalized against the bodymass of each participant In fact moderate to high associ-ations were found between body mass and mean and peakshoulder net joint moments when propelling with no slope(119903 = 0554 and 0577) and with slopes of varying degrees(119903 = 0713 to 0809) The peak and mean shoulder net jointmoments in the sagittal frontal and transverse plane werethe main outcome measures
27 Shoulder Muscular Demand The electromyographicactivity of the anterior and posterior portions of the del-toid along with the clavicular and sternal heads of thepectoralis major was recorded at the nondominant upperextremity at a sampling frequency of 1200Hz using a portabletelemetric system (NORAXON USA Inc Scottsdale Ari-zona Telemyo 900) Skin preparation and the placementof the surface electrodes (BlueSensor M AMBU BallerupDanmark) (AgAgCl sensor ndash132mm2 active surface area)were made in accordance with SENIAM recommendations(refer to httpwwwseniamorg) Following baseline noiseremoval all EMG signals recorded were visually inspectedbefore being filtered with a 4th order zero-lag Butterworthbandpass filter with low and high cut-off frequencies set at30 and 500Hz respectively Thereafter EMG patterns werefull-wave rectified and filtered with a 6Hz low-pass filterto generate EMG linear envelopes for each muscle studiedThe muscular utilization ratio (MUR ()) was calculatedfor each muscle studied by normalizing the amplitude ofthe EMG signals recorded during the experimental tasksagainst the peak EMG signal recorded over a 05 secondperiod during one of the two static maximum voluntarycontractions (MVC) Muscle-specific manual resistance wasapplied by a trained physiotherapist to generate the MVCswhile participants remained seated in their own wheelchairMeanwhile another research associate manually providedadditional trunk and wheelchair stability to participants Foreach muscle studied the peak and mean MURs as well as anindicator of muscle work (IMW) were calculated using theintegral of the MUR data were the main outcome measuresAll EMG signal processing was performed digitally using acustom-developed MATLAB algorithm
28 Statistical Analyses Descriptive statistics (mean plusmn SD)were calculated for the demographic and clinical character-istics of all participants as well as for the kinematic kineticand muscular demand outcome measures For these lastoutcome measures 10 propulsion cycles were averaged pertrial resulting in a total of 20 propulsion cycles for eachslope tested The kinematic kinetic and muscular demanddata recorded during the push phase of each cycle analyzedwere also time-normalized over 100 (ie 100 data points)to generate a profile for each participant and a mean groupprofile Shapiro-Wilk tests confirmed that the kinematickinetic and electromyographic outcome measures for all
slopes tested were normally distributed and justified the useof parametric statistical tests One-way repeated-measureanalyses of variance (ANOVA) with one within-subjectsfactor (slopes of 0∘ 27∘ 36∘ 48∘ and 71∘) using a generallinear model was used to determine the effect of the slopeson the kinematic and kinetic and electromyographic outcomemeasures and an eta-squared value was used to confirmif the proportion of the total variability attributable to theslope factor (ie effect size) was small (gt002) moderate(gt013) or large (gt026) Whenever an ANOVA revealedsignificant differences (main effect 119875 lt 005) after the resultof the Mauchlyrsquos test of sphericity of the covariance matrixwas taken into consideration Studentrsquos 119905-tests for pairedsamples were computed (post hoc tests) with a Bonferronicorrection setting the significance level at 119875 le 00125(119875 le 0054 pairwise comparisons) as a result of thefour possible slope increments (ie 0∘ to 27∘ 27∘ to 36∘36∘ to 48∘ and 48∘ to 71∘) All statistical analyses wereperformed with SPSS Statistics 170 software for WindowsNote that the kinematic and electromyographic data wereonly collected and computed at the nondominant UL sincequasi-symmetrical ULmovement strategies and efforts wereassumed in order to safely propel on a linear trajectory onthe motorized treadmill [21] and since the nondominant ULstrength generating capability is generally weaker than theone at the dominant UL possibly resulting in higher relativedemand at the nondominant UL during the performance ofa symmetrical functional task
3 Results
31 Completion Rate At a mean natural and constant self-selected propulsion speed of 117 plusmn 018ms [min = 091msmax = 165ms] all participants (completion rate = 100)were able to propel themselves on the 0∘ slope and up the27∘ slope (Table 2)The completion rate reached 889 (119873 =1618 participants) 778 (119873 = 1418 participants) and556 (119873 = 1018 participants) for the 36∘ 48∘ and 71∘slopes respectively (Table 2)
32 Temporal Parameters Table 3 summarizes the meanduration of the push and recovery phases and the totalduration of a propulsion cycle in seconds for the differenttreadmill slopes The average durations of the push phasewere similar for all tested slopes (ANOVA 119875 = 0267)whereas the average duration of the recovery phase declinedas the slope became steeper (post hoc tests 119875 le 0043) Thetotal duration significantly decreased as the slope becamesteeper (post hoc tests 119875 le 0001) except during the 27∘ to36∘ slope increment that remained similar
33 Trunk and Shoulder Kinematics The trunk and shouldermovement patterns are illustrated in Figures 2(a) 2(b) 2(c)and 2(d) whereas the minimum maximum and excur-sion of the trunk and shoulder movement amplitudes aresummarized in Table 4 The slopes of the treadmill signifi-cantly influenced most minimum maximum and excursiontrunk and shoulder movement amplitudes At the trunk all
6 BioMed Research International
Table 2 Description of self-selected comfortable propulsion speed experimental tasks completed and rate of perceived exertion
Participants Self-selected speed (ms) Slopes Rate of perceived exertion (10)0∘ 27∘ 36∘ 48∘ 71∘ 0∘ 27∘ 36∘ 48∘ 71∘
1 111 09 74 55 81 952 165 01 22 03 03 mdash3 105 13 13 39 44 714 118 08 17 37 48 785 120 17 48 25 59 796 091 30 63 77 mdash mdash7 148 09 97 mdash mdash mdash8 116 0 03 09 mdash mdash9 104 18 38 33 42 mdash10 127 0 0 0 0 011 139 10 15 33 27 3212 099 11 41 40 75 mdash13 106 42 88 mdash mdash mdash14 125 12 52 67 64 8515 103 00 06 19 36 mdash16 107 07 34 46 66 9217 106 07 62 26 65 8918 111 29 46 61 66 73Mean 117 119899 = 18 119899 = 18 119899 = 16 119899 = 14 119899 = 10 12 39 35 47 68SD 018 11 29 22 25 30
Table 3 Group average (SD) mean temporal parameter measured of the push phase measured at the nondominant handrim at the fivedifferent slopes tested
Slopes0∘ 27∘ 36∘ 48∘ 71∘
Temporal parameters (s)Push phase 048 plusmn 008 048 plusmn 008 049 plusmn 008 048 plusmn 007 048 plusmn 006Recovery phase 059 plusmn 022 027 plusmn 010 026 plusmn 009 022 plusmn 008 018 plusmn 005Total (cycle) 107 plusmn 023 075 plusmn 016 075 plusmn 014 070 plusmn 013 066 plusmn 010
minimum maximum and excursion movement amplitudessignificantly increased as the slope became steeper except forminimum and maximum values during the 27∘ to 36∘ slopeincrement that remained similar The greatest maximumforward trunk flexion (609∘) which was accompanied by thegreatest forward trunk excursion (224∘) was reached duringthe 71∘ slope At the shoulder the maximum shoulder flexionmovement amplitude significantly increased as the slopebecame steeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments The minimum maximum and excursion shoulderabduction movement amplitudes remained comparable asthe slope became steeper The minimum maximum andexcursion shoulder internal rotation movement amplitudesalso remained comparable as the slope became steeper with
the exception of the minimum and excursion values whichsignificantly increased during the 0∘ to 27∘ slope increment
34 Shoulder Kinetics The net shoulder flexion abductionand internal rotation moment patterns are illustrated inFigures 2(e) 2(f) and 2(g) while their mean and maximumvalues are summarized in Table 5 The greatest maximumshoulder moments were found during flexion across allslopes except for the 71∘ slope when the internal rotationgenerated the greatest moment All mean and maximumshouldermoments were significantly influenced by the slopesof the treadmill The mean and maximum flexion momentssignificantly improved as the slope increased except for the36∘ to 48∘ and 48∘ to 71∘ slope increments The meanadduction moments only significantly improved as the slopeincreased between 0∘ and 27∘ whereas the peak mean valueonly significantly improved as the slope increased between
BioMed Research International 7
0
10
20
30
40
50
60
70
80
Trun
k fle
xion
(+)
exte
nsio
n (minus
)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(a)
60
40
20
0
minus20
minus40
minus60
Shou
lder
flex
ion
(+)
exte
nsio
n (minus
)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(b)
0
10
20
30
40
50
60
Shou
lder
abdu
ctio
n (+
) ad
duct
ion
(minus)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(c)
0
10
20
30
40
50
60
70
0 20 40 60 80 100
Normalized time (100)Angle (∘)
Shou
lder
IR (+
) ER
(minus)
(d)
12
08
04
00
minus04
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder flexion (+) extension (minus)
(e)
04
02
00
minus02
minus04
minus06
minus08
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder abduction (+) adduction (minus)
(f)
Figure 2 Continued
8 BioMed Research International
10
08
06
04
02
00
minus02
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder IR (+) ER (minus)
(g)
Figure 2 Group averaged time-normalized profile (solid line) and standard deviation (dotted line) of the shoulder and trunk kinematics (ab c and d) and weight-normalised shoulder moments (e f and g) during the push phase for the five slopes tested at self-selected naturalspeed
the 0∘ to 27∘ 36∘ to 48∘ and 48∘ to 71∘ slope incrementsThemean and maximum internal rotation moments significantlyincreased as the slope became steeper except for the 36∘ to48∘ slope increment
35 Shoulder Muscular Demand The MUR patterns of themuscles studied are illustrated in Figure 3 while their meanand maximum values are summarized in Table 6 The meanIMWs of the muscles studied are summarized in Table 6 andillustrated in Figure 4 For allmuscles studied theirmean andmaximum MURs as well as their indicator of muscle workvalue significantly increased as the slope became steeperexcept for the posterior deltoid that remained comparablebetween the 27∘ to 36∘ slope increment
4 Discussion
This study quantified trunk and nondominant shoulderkinematic changes along with nondominant shoulder jointmoments and electromyographic changes during MWCpropulsion on a motorized treadmill set at a self-selectednatural speed on five different slopes (ie 0∘ 27∘ 36∘ 48∘and 71∘) Overall the MWC users with a SCI increasedforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increased during simulated uphillMWC propulsion on a motorized treadmill
41 Trunk and Shoulder Movement-Related Adaptations Themovement-related adaptations occurring at the trunk andshoulder partially support the hypothesis that their outcome
measures would gradually and significantly increase witheach slope increment while the speed remained constantAt the trunk the maximum forward trunk flexion and thetotal trunk excursion increased significantly as the slopebecame steeper except for the 27∘ to 36∘ slope incrementChow et al [5] obtained somewhat comparable resultsin terms of trunk kinematics although no difference wasrevealed when comparing 4∘ and 8∘ slopes This may beexplained by the fact that participants propelled at self-selected speeds that decreased progressively in their protocolas the slope increased Nonetheless the increased maximumforward trunk flexion coupled with the increased forwardtrunk excursion may allow MWC users to move their centreof mass further and faster anteriorly and to maintain itsprojection in front of the rear wheel axle in order toprevent backward tilt and falls as the slope increases Thismay also explain why maximum forward trunk flexion andforward trunk excursion became greater as the gravitationaleffects became harder to overcome with steeper slopes Thedecreasing success rate with a steeper slope may be explainedin part by the fact that some participants were classified asbeing overweight (body mass index gt 25) or class I obese(body mass index = 300ndash349) with associated abdominalobesity that limited their ability to increase forward trunkflexion to accommodate for the steeper slopes In fact 556of participants who were unable to propel up the 71∘ slopewere overweight (119873 = 3) or obese (119873 = 2) whereasonly 30 of participants who were able to propel up the 71∘slope were overweight (119873 = 2) or obese (119873 = 1) Henceabdominal circumference may deserve additional attentionwhen investigating wheelchair propulsion technique or man-ual wheelchair skills such as uphill propulsion
BioMed Research International 9
Table4Group
average(SD)totalexcursio
n(∘ )
and
maxim
umandminim
um(∘ )
kinematicvalues
measuredatthetrun
kandno
ndom
inantsho
uldera
tthe
fivedifferent
slopestestedas
wellasthe
results
oftheA
NOVA
andpo
stho
ccom
paris
ontest
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Jointangle(∘
)
Trun
kmdashflexion
(+)extension(minus)
Trun
kmdashflexion
(+)extension(minus)
Excursion
588
(212
)1267(340)
1456(277)
1761
(396)
2237
(600)lt0001
0907
lt0001
000
6lt0001
0003
Maxim
um1927(623)
3592(845)
3945(831
)4579(853
)6093(113
0)lt0001
0889
lt0001
0031
0002
0005
Minim
um1339
(614
)2326(775)
2490(805)
2818
(771)
3857(859)lt0001
0910
lt0001
0028
lt0001
lt0001
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Excursion
5567(920)
5817
(1092)
5963(901)
6019
(698)
6499(895)
0019
0296
0072
0183
0473
0217
Maxim
um1131
(934)
1800(820)
1935
(762)
2259(730)
3088(745)lt0001
0849
lt0001
0001
0054
lt0001
Minim
umminus44
36(935
)minus40
17(936)minus40
27(915
)minus3760(834)minus3410
(1036)lt0001
0651
lt0001
000
6lt0001
lt0001
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Excursion
935(343)
1227(716)
1348(661)
1488(756)
1965(118
8)0012
0337
0010
0363
0158
0047
Maxim
um3325(800)
3481(1065)
3540(1026)
3488(1057)
4060(1543)
0083
mdashmdash
mdashmdash
mdashMinim
um2390(627)
2253
(726)
2192(666)
2000(545)
2094(570)
0038
mdashmdash
mdashmdash
mdashShou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Excursion
2486(820)
3055(1024)
3335(883)
3452
(944)
4328(113
4)lt0001
0623
000
4004
00765
0013
Maxim
um3157(1682)
3789(1846
)40
15(19
17)
4302(1223)
4969(871)lt0001
0665
lt0001
0029
0855
0033
Minim
um671
(1357)
734(1510)
680
(1694)
850
(918
)641
(770)
0152
mdashmdash
mdashmdash
mdash
10 BioMed Research International
Table5Group
average(
SD)m
eanandpeak
weight-n
ormalise
dmom
ents(N
mkg)
measuredatthen
ondo
minantsho
uldera
tthe
fived
ifferentslopesa
swellasresultsof
theA
NOVA
and
postho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Normalisedmoments(Nmkg)
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Mean
0140(0056)
0226(0067)
0248(0081)
0233(0083)
0242(015
1)0027
0288
lt0001
0003
0433
0966
Peak
(maxim
um)
0292(010
9)0512(015
2)0546(016
7)0559(012
8)0733(0302)lt0001
0588
lt0001
000
40867
0049
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashaddu
ction(+)abdu
ction(minus)
Mean
minus0016(0023)minus006
0(0050)minus0069(0046
)minus0090(0043)minus0103(0036)lt0001
0623
lt0001
0414
0147
0366
Peak
(minim
um)minus0088(0041)minus0257(010
5)minus0278(010
4)minus0369(013
7)minus0494(013
3)lt0001
0797
lt0001
0149
0002
0002
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Mean
0097(0036)
0189(0050)
0222(0064
)0252(0065)
0344(010
1)lt0001
0726
lt0001
000
40191
0010
Peak
(maxim
um)
0196(0078)
0415(014
4)0456(012
9)0530(014
8)0780(018
4)lt0001
0801
lt0001
0001
0103
0001
BioMed Research International 11
00
02
04
06
08
10
Ant
erio
r delt
oid
(a)
00
02
04
06
08
10
(b)
00
02
04
06
08
10
(c)
00
02
04
06
08
10
12
Poste
rior d
eltoi
d
(d)
00
02
04
06
08
10
12
(e)
00
02
04
06
08
10
12
(f)
00
02
04
06
08
10
Clav
icul
ar h
ead
of p
ecto
ralis
maj
or
(g)
00
02
04
06
08
10
(h)
00
02
04
06
08
10
(i)
00
02
04
06
08
10
12
14
16
0 20 40 60 80 100
Ster
nal h
ead
of p
ecto
ralis
maj
or
Normalised time (100)Mean MUR pattern (1)
0∘
27∘
36∘
48∘
71∘
(j)
00
02
04
06
08
10
12
14
16
Mean MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(k)
00
02
04
06
08
10
12
14
16
Peak MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(l)
Figure 3 Group averaged time-normalized mean profile (solid line) and standard deviation (dotted line) (a d g and j) as well as group-average (SD) mean (b e h and k) and peak (c f i and l) muscle utilization ratio (MUR) during the push phase for the five slopes tested atself-selected natural speed
12 BioMed Research International
Table6Group
average(
1SD)meanmuscle
utilisatio
nratio
(MUR)peakMUR(1)and
indicatoro
fmuscle
work(IMW)v
aluesfor
each
muscle
assessed
atthen
ondo
minantsho
uldera
tfived
ifferentslope
angles
aswellasresultsof
theA
NOVA
andpo
stho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Anteriord
eltoid
Anteriord
eltoid
MeanMUR(1)
007
(004)
021
(009)
023
(012
)026
(010
)034
(013
)lt0001
0831
lt0001
0002
lt0001
0001
Peak
MUR(1)
014
(008)
044
(023)
048
(026)
054
(026)
068
(028)lt0001
0836
lt0001
0002
lt0001
lt0001
IMW
718(398)
2070(943)
2348(1237)
2606(1043)
3448(1304)lt0001
0829
lt0001
0003
lt0001
0002
Poste
riord
eltoid
Poste
riord
eltoid
MeanMUR(1)
008
(007)
020
(014
)024
(024)
023
(010
)027
(006)lt0001
0907
lt0001
0144
lt0001
lt0001
Peak
MUR(1)
020
(014
)052
(031
)062
(051)
060
(019
)077
(019
)lt0001
0894
lt0001
0027
0001
0005
IMW
795(692)
2036(1384)
2443(2381)
2335
(1047)
2734(648)lt0001
0906
lt0001
0143
lt0001
lt0001
Clavicular
fiberso
fpectoralis
major
Clavicular
fiberso
fpectoralis
major
MeanMUR(1)
007
(004)
018
(010
)020
(010
)027
(014
)035
(018
)lt0001
0754
lt0001
0003
lt0001
0005
Peak
MUR(1)
014
(009)
038
(022)
042
(023)
057
(031
)071
(029)lt0001
0814
lt0001
000
9lt0001
0001
IMW
700(426)
1837
(977)
2041(1046)
2704(14
32)
3528(175
7)lt0001
0752
lt0001
0003
lt0001
0005
Sternalfi
bersof
pectoralismajor
Sternalfi
bersof
pectoralismajor
MeanMUR(1)
012
(008)
030
(015
)032
(013
)037
(015
)053
(024)lt0001
0781
lt0001
0005
0001
000
6Peak
MUR(1)
021
(015
)054
(023)
059
(023)
071
(026)
101(042)lt0001
0829
lt0001
0003
lt0001
0002
IMW
1194(753)
3023(14
77)
3227(1323)
3753
(1511)
5280(2406)lt0001
0780
lt0001
0005
0001
000
6
BioMed Research International 13
0
10
20
30
40
50
60
70
80
Ant
erio
r delt
oid
Poste
rior d
eltoi
d
Clav
icul
ar h
ead
ofpe
ctor
alis
maj
or
Ster
nal h
ead
of
pect
oral
is m
ajor
IMW
0∘
27∘
36∘
48∘
71∘
Figure 4 Group averaged (SD) mean indicator of muscle work(IMW) during the push phase for the five slopes tested at self-selected natural speed
At the shoulder the maximum shoulder flexion move-ment amplitude significantly increased as the slope becamesteeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments It is possible that increasedmaximumshoulder flexionwas needed to accommodate for the increased forward trunkflexion and to apply most of the force tangentially on thehandrim to preserve mechanical efficiencyThe fact that onlythe duration of the recovery period drastically decreasedas the slope became steeper can also explain in part therelatively stable shoulder flexion-extension excursion (iesimilar push phase durations across slopes) This finding isconsistent to some extent with the work of Yang et al [3]who found comparable values of movement-related adap-tation at the shoulder when comparing level overgroundand uphill (ie 3∘ slope) MWC propulsions However theshoulder flexion-extension excursion significantly increasedon average by 937∘ and the shoulder extension remainedsimilar in their study contrary to the results of the presentstudy These discrepancies may be attributed to the fact thatparticipants used test wheelchairs that were not anchoredto a safety system when propelling up a 3∘ slope at 09mson a motorized treadmill the level surface propulsion (0∘slope) was performed overground and the shoulder kine-matic calculation differed from the work by Yang et al [3]Nevertheless all these results confirmed kinematic adapta-tions at the shoulder as the slope progressed Lastly theincreased forward trunk flexion coupled with an increasedshoulder flexion that modifies the orientation of the forcegenerated at the shoulder may increase posterior shoulderjoint forces and explain the elevated muscular demand at theposterior deltoid occurring towards the end of the push phase[22]
42 Shoulder Joint Mechanical and Muscular Effort Adap-tations The shoulder joint moments adaptations partiallysupport the hypothesis that their outcome measures wouldgradually and significantly increase with each slope incre-ment while the speed remained constant For two out of thethree shoulder net joint moments investigated most of themean and peak values for the shoulder flexor and internalrotator moments progressively increased as the slope becamesteeper aside from some outcomemeasures during the 27∘ to36∘ or the 36∘ to 48∘ slope increment The relative musculardemand adaptations and muscular work computed for allmuscles investigated fully support this hypothesis since theiroutcomemeasures gradually and significantly increased witheach slope increment while the speed remained constantHence once the results of these two approaches are com-bined it is clear that the shoulder mechanical and musculareffort increases are key contributors to the adaptation processassociated with the steeper slopes Moreover these resultsare in line with the perceived UL efforts expressed by theparticipants and may explain in part The decreasing successrate with a steeper slope as shoulder strength generatingcapability most likely becomes a determinant for propellingon steeper slopes
43 Implications for Clinical Practice With the use of a slopeor of a combination of slopes when a MWC user propelshimselfherself on a motorized treadmill therapists may beable to offer task-specific high-intensity short duration inter-val training programs to increase UL strength particularlyat the shoulders Cautiousness is advised with this practicesince the risk exposure (ie increased shoulder mechanicaland muscular demands) will progressively and significantlyincrease as the slope becomes steeper and will vary accordingto the strength-generating capability of each MWC user Inaddition since the risk exposure could trigger the develop-ment or exacerbation of secondary impairments at the ULparticularly at the shoulders such a program should alsobe accompanied by proper warm-up and cool-down periodsas well as by antagonist muscle strengthening to preventmuscle strength imbalance Alternatively therapists may alsooffer task-specific cardiorespiratory fitness training programswhen a MWC user propels on a motorized treadmill withno slope or minimal slope (lt27∘) with minimal demandsduring a prolonged period of time (ie cardiorespiratoryfitness training)
44 Limits of the Study The present study included a rela-tively small sample size (119899 = 18) of experienced MWC userswho have completed their rehabilitation process which maylimit the strength of the evidence and potential to generalizethe results with new MWCs respectively The fact that theparticipants used their personal wheelchairs during the studywarrants consideration as optimal wheelchair positioningand configuration parameters most likely differs across par-ticipants and impacts the outcome measures of interest inthe present study and the risk of the MWC tilting or fallingbackwards when propelling up a slope The use of the instru-mented wheels which slightly increase the width and weight
14 BioMed Research International
of the wheelchair along with rolling resistance may havemodified participantsrsquo propulsion technique (eg increasedshoulder abduction) and fatigue level (eg increased ULeffort) in comparison to propelling with their own wheelsThe self-selected natural treadmill speed determined for eachparticipant maintained across all slopes tested in an effort toisolate the effect of speed also requires consideration sinceMWCusers tend to reduce their speedwhen propelling uphillin daily life particularly on steep slopes [2] Finally thekinematic and kinetic and electromyographic variables solelyfocused on the trunk and nondominant shoulder prevent afull understanding of UL adaptations (ie elbow and wristnot studied) during motorized treadmill MWC propulsionacross different slopes
5 Conclusion
This study confirms that MWC users with a SCI increaseforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increase during simulated uphillMWC propulsion on a motorized treadmill Few similaritieswere found between the 27∘ to 36∘ and the 36∘ to 48∘ slopeincrements for shoulder flexion and adduction momentsFuture studies incorporating interactions with various slopesand velocities could strengthen the results of the presentstudy and provide additional evidence-based knowledge onwheelchair propulsion on a motorized treadmill
Abbreviations
AIS American Spinal Injury AssociationImpairment Scale
EMG ElectromyographyER External rotationLED Light-emitting diodeIMW Indicator of muscle workIR Internal rotationJCS Joint coordinate systemMUR Muscle utilization ratioMVC Maximum voluntary contractionMWC Manual wheelchairUL Upper limbWUSPI Wheelchair Userrsquos Shoulder Pain
Index
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors would like to thank Michel Goyette (Eng)Daniel Marineau (Technician) Youssef El Khamlichi(Research Associate) and Philippe Gourdou (ResearchAssociate) for their contributions to this project DanyGagnon holds a Junior 1 Research Career Award from
the Fonds de la recherche du Quebec-Sante (FRQ-S)Annie-Claude Babineau and Guillaume Desroches aresupported by a summer internship and a post-doctoralfellowship from the Canadian Institutes of Health Researchrespectively DanyGagnon andRachid Aissaoui aremembersof the Multidisciplinary SensoriMotor RehabilitationResearch Team (httpwwwerrsmca) supported bythe CIHR and the Quebec-Ontario Spinal Cord InjuryMobility (SCI-MOB) Research Group funded by theQuebec Rehabilitation Research Network (REPARhttpwwwreparca) and the Ontario NeuroTraumaFoundation (ONF httpwwwonforg) The project wasfunded in part by the Fonds de la recherche du Quebec-Sante(FRQS) The equipment and material required for theresearch completed at the Pathokinesiology Laboratory wasfinanced by the Canada Foundation for Innovation (CFI)
References
[1] B Mason J Lenton C Leicht and V Goosey-Tolfrey ldquoAphysiological and biomechanical comparison of over-groundtreadmill and ergometer wheelchair propulsionrdquo Journal ofSports Sciences vol 32 no 1 pp 78ndash91 2014
[2] W M Richter R Rodriguez K R Woods and P W AxelsonldquoStroke pattern and handrim biomechanics for level and uphillwheelchair propulsion at self-selected speedsrdquo Archives of Phys-ical Medicine and Rehabilitation vol 88 no 1 pp 81ndash87 2007
[3] Y-S Yang A M Koontz S-J Yeh and J-J Chang ldquoEffectof backrest height on wheelchair propulsion biomechanics forlevel and uphill conditionsrdquo Archives of Physical Medicine andRehabilitation vol 93 no 4 pp 654ndash659 2012
[4] D H Gagnon A-C Babineau A Champagne G Desrochesand R Aissaoui ldquoPushrim biomechanical changes with pro-gressive increases in slope during motorized treadmill manualwheelchair propulsion in individuals with spinal cord injuryrdquoJournal of Rehabilitation Research amp Development vol 51 no 5pp 789ndash802 2014
[5] J W Chow T A Millikan L G Carlton W-S Chae Y-T Lim and M I Morse ldquoKinematic and electromyographicanalysis of wheelchair propulsion on ramps of different slopesfor young men with Paraplegiardquo Archives of Physical Medicineand Rehabilitation vol 90 no 2 pp 271ndash278 2009
[6] S van Drongelen L H van Der Woude T W Janssen E LAngenot E K Chadwick and D H Veeger ldquoMechanical loadon the upper extremity during wheelchair activitiesrdquo Archivesof Physical Medicine and Rehabilitation vol 86 no 6 pp 1214ndash1220 2005
[7] H Arabi R Aissaoui J Rousseau D Bourbonnais and JDansereau ldquoEvaluation of minimal mechanical effort duringthe ramp access of manual wheelchairrdquo Ergonomia vol 26 no3 pp 253ndash259 2004
[8] K Kulig S S Rao S J Mulroy et al ldquoShoulder joint kineticsduring the push phase of wheelchair propulsionrdquo ClinicalOrthopaedics and Related Research no 354 pp 132ndash143 1998
[9] L J Chapman and J P Chapman ldquoThe measurement ofhandednessrdquoBrain andCognition vol 6 no 2 pp 175ndash183 1987
[10] Gouvernement du Quebec Regie du Batiment du Quebec(RBQ) Construction Code Building Act Chapter 1 Architec-tural and Transportation Barriers Compliance Board 2013
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
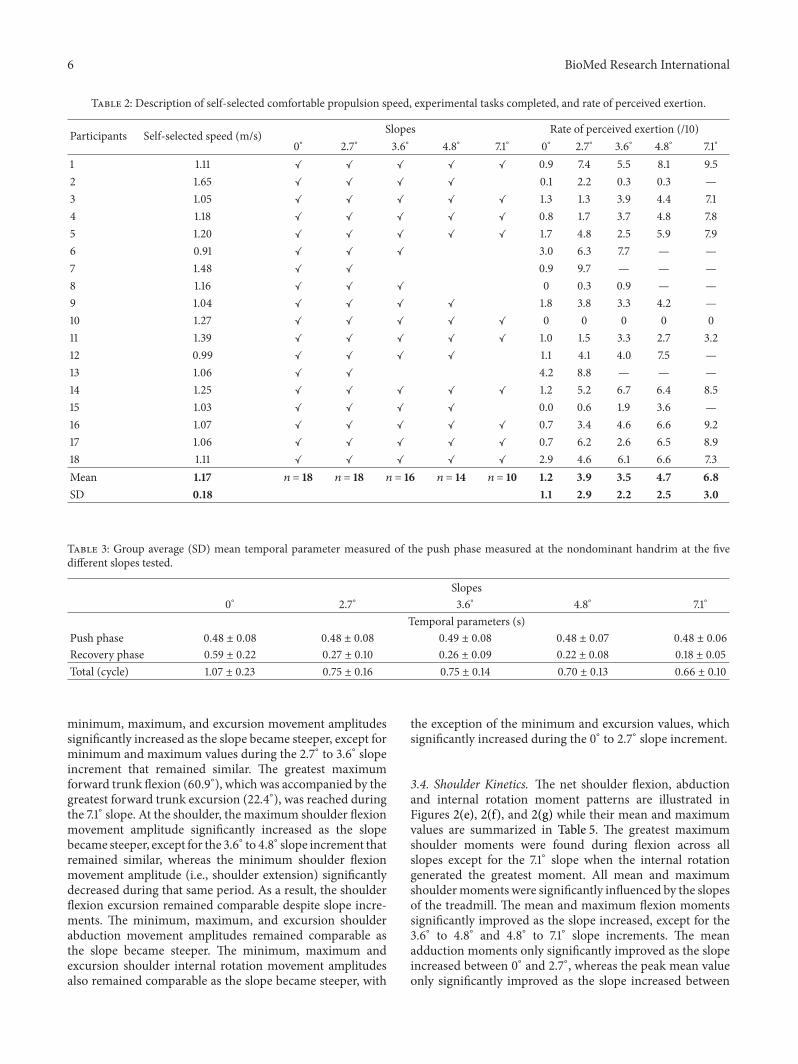
6 BioMed Research International
Table 2 Description of self-selected comfortable propulsion speed experimental tasks completed and rate of perceived exertion
Participants Self-selected speed (ms) Slopes Rate of perceived exertion (10)0∘ 27∘ 36∘ 48∘ 71∘ 0∘ 27∘ 36∘ 48∘ 71∘
1 111 09 74 55 81 952 165 01 22 03 03 mdash3 105 13 13 39 44 714 118 08 17 37 48 785 120 17 48 25 59 796 091 30 63 77 mdash mdash7 148 09 97 mdash mdash mdash8 116 0 03 09 mdash mdash9 104 18 38 33 42 mdash10 127 0 0 0 0 011 139 10 15 33 27 3212 099 11 41 40 75 mdash13 106 42 88 mdash mdash mdash14 125 12 52 67 64 8515 103 00 06 19 36 mdash16 107 07 34 46 66 9217 106 07 62 26 65 8918 111 29 46 61 66 73Mean 117 119899 = 18 119899 = 18 119899 = 16 119899 = 14 119899 = 10 12 39 35 47 68SD 018 11 29 22 25 30
Table 3 Group average (SD) mean temporal parameter measured of the push phase measured at the nondominant handrim at the fivedifferent slopes tested
Slopes0∘ 27∘ 36∘ 48∘ 71∘
Temporal parameters (s)Push phase 048 plusmn 008 048 plusmn 008 049 plusmn 008 048 plusmn 007 048 plusmn 006Recovery phase 059 plusmn 022 027 plusmn 010 026 plusmn 009 022 plusmn 008 018 plusmn 005Total (cycle) 107 plusmn 023 075 plusmn 016 075 plusmn 014 070 plusmn 013 066 plusmn 010
minimum maximum and excursion movement amplitudessignificantly increased as the slope became steeper except forminimum and maximum values during the 27∘ to 36∘ slopeincrement that remained similar The greatest maximumforward trunk flexion (609∘) which was accompanied by thegreatest forward trunk excursion (224∘) was reached duringthe 71∘ slope At the shoulder the maximum shoulder flexionmovement amplitude significantly increased as the slopebecame steeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments The minimum maximum and excursion shoulderabduction movement amplitudes remained comparable asthe slope became steeper The minimum maximum andexcursion shoulder internal rotation movement amplitudesalso remained comparable as the slope became steeper with
the exception of the minimum and excursion values whichsignificantly increased during the 0∘ to 27∘ slope increment
34 Shoulder Kinetics The net shoulder flexion abductionand internal rotation moment patterns are illustrated inFigures 2(e) 2(f) and 2(g) while their mean and maximumvalues are summarized in Table 5 The greatest maximumshoulder moments were found during flexion across allslopes except for the 71∘ slope when the internal rotationgenerated the greatest moment All mean and maximumshouldermoments were significantly influenced by the slopesof the treadmill The mean and maximum flexion momentssignificantly improved as the slope increased except for the36∘ to 48∘ and 48∘ to 71∘ slope increments The meanadduction moments only significantly improved as the slopeincreased between 0∘ and 27∘ whereas the peak mean valueonly significantly improved as the slope increased between
BioMed Research International 7
0
10
20
30
40
50
60
70
80
Trun
k fle
xion
(+)
exte
nsio
n (minus
)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(a)
60
40
20
0
minus20
minus40
minus60
Shou
lder
flex
ion
(+)
exte
nsio
n (minus
)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(b)
0
10
20
30
40
50
60
Shou
lder
abdu
ctio
n (+
) ad
duct
ion
(minus)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(c)
0
10
20
30
40
50
60
70
0 20 40 60 80 100
Normalized time (100)Angle (∘)
Shou
lder
IR (+
) ER
(minus)
(d)
12
08
04
00
minus04
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder flexion (+) extension (minus)
(e)
04
02
00
minus02
minus04
minus06
minus08
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder abduction (+) adduction (minus)
(f)
Figure 2 Continued
8 BioMed Research International
10
08
06
04
02
00
minus02
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder IR (+) ER (minus)
(g)
Figure 2 Group averaged time-normalized profile (solid line) and standard deviation (dotted line) of the shoulder and trunk kinematics (ab c and d) and weight-normalised shoulder moments (e f and g) during the push phase for the five slopes tested at self-selected naturalspeed
the 0∘ to 27∘ 36∘ to 48∘ and 48∘ to 71∘ slope incrementsThemean and maximum internal rotation moments significantlyincreased as the slope became steeper except for the 36∘ to48∘ slope increment
35 Shoulder Muscular Demand The MUR patterns of themuscles studied are illustrated in Figure 3 while their meanand maximum values are summarized in Table 6 The meanIMWs of the muscles studied are summarized in Table 6 andillustrated in Figure 4 For allmuscles studied theirmean andmaximum MURs as well as their indicator of muscle workvalue significantly increased as the slope became steeperexcept for the posterior deltoid that remained comparablebetween the 27∘ to 36∘ slope increment
4 Discussion
This study quantified trunk and nondominant shoulderkinematic changes along with nondominant shoulder jointmoments and electromyographic changes during MWCpropulsion on a motorized treadmill set at a self-selectednatural speed on five different slopes (ie 0∘ 27∘ 36∘ 48∘and 71∘) Overall the MWC users with a SCI increasedforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increased during simulated uphillMWC propulsion on a motorized treadmill
41 Trunk and Shoulder Movement-Related Adaptations Themovement-related adaptations occurring at the trunk andshoulder partially support the hypothesis that their outcome
measures would gradually and significantly increase witheach slope increment while the speed remained constantAt the trunk the maximum forward trunk flexion and thetotal trunk excursion increased significantly as the slopebecame steeper except for the 27∘ to 36∘ slope incrementChow et al [5] obtained somewhat comparable resultsin terms of trunk kinematics although no difference wasrevealed when comparing 4∘ and 8∘ slopes This may beexplained by the fact that participants propelled at self-selected speeds that decreased progressively in their protocolas the slope increased Nonetheless the increased maximumforward trunk flexion coupled with the increased forwardtrunk excursion may allow MWC users to move their centreof mass further and faster anteriorly and to maintain itsprojection in front of the rear wheel axle in order toprevent backward tilt and falls as the slope increases Thismay also explain why maximum forward trunk flexion andforward trunk excursion became greater as the gravitationaleffects became harder to overcome with steeper slopes Thedecreasing success rate with a steeper slope may be explainedin part by the fact that some participants were classified asbeing overweight (body mass index gt 25) or class I obese(body mass index = 300ndash349) with associated abdominalobesity that limited their ability to increase forward trunkflexion to accommodate for the steeper slopes In fact 556of participants who were unable to propel up the 71∘ slopewere overweight (119873 = 3) or obese (119873 = 2) whereasonly 30 of participants who were able to propel up the 71∘slope were overweight (119873 = 2) or obese (119873 = 1) Henceabdominal circumference may deserve additional attentionwhen investigating wheelchair propulsion technique or man-ual wheelchair skills such as uphill propulsion
BioMed Research International 9
Table4Group
average(SD)totalexcursio
n(∘ )
and
maxim
umandminim
um(∘ )
kinematicvalues
measuredatthetrun
kandno
ndom
inantsho
uldera
tthe
fivedifferent
slopestestedas
wellasthe
results
oftheA
NOVA
andpo
stho
ccom
paris
ontest
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Jointangle(∘
)
Trun
kmdashflexion
(+)extension(minus)
Trun
kmdashflexion
(+)extension(minus)
Excursion
588
(212
)1267(340)
1456(277)
1761
(396)
2237
(600)lt0001
0907
lt0001
000
6lt0001
0003
Maxim
um1927(623)
3592(845)
3945(831
)4579(853
)6093(113
0)lt0001
0889
lt0001
0031
0002
0005
Minim
um1339
(614
)2326(775)
2490(805)
2818
(771)
3857(859)lt0001
0910
lt0001
0028
lt0001
lt0001
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Excursion
5567(920)
5817
(1092)
5963(901)
6019
(698)
6499(895)
0019
0296
0072
0183
0473
0217
Maxim
um1131
(934)
1800(820)
1935
(762)
2259(730)
3088(745)lt0001
0849
lt0001
0001
0054
lt0001
Minim
umminus44
36(935
)minus40
17(936)minus40
27(915
)minus3760(834)minus3410
(1036)lt0001
0651
lt0001
000
6lt0001
lt0001
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Excursion
935(343)
1227(716)
1348(661)
1488(756)
1965(118
8)0012
0337
0010
0363
0158
0047
Maxim
um3325(800)
3481(1065)
3540(1026)
3488(1057)
4060(1543)
0083
mdashmdash
mdashmdash
mdashMinim
um2390(627)
2253
(726)
2192(666)
2000(545)
2094(570)
0038
mdashmdash
mdashmdash
mdashShou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Excursion
2486(820)
3055(1024)
3335(883)
3452
(944)
4328(113
4)lt0001
0623
000
4004
00765
0013
Maxim
um3157(1682)
3789(1846
)40
15(19
17)
4302(1223)
4969(871)lt0001
0665
lt0001
0029
0855
0033
Minim
um671
(1357)
734(1510)
680
(1694)
850
(918
)641
(770)
0152
mdashmdash
mdashmdash
mdash
10 BioMed Research International
Table5Group
average(
SD)m
eanandpeak
weight-n
ormalise
dmom
ents(N
mkg)
measuredatthen
ondo
minantsho
uldera
tthe
fived
ifferentslopesa
swellasresultsof
theA
NOVA
and
postho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Normalisedmoments(Nmkg)
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Mean
0140(0056)
0226(0067)
0248(0081)
0233(0083)
0242(015
1)0027
0288
lt0001
0003
0433
0966
Peak
(maxim
um)
0292(010
9)0512(015
2)0546(016
7)0559(012
8)0733(0302)lt0001
0588
lt0001
000
40867
0049
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashaddu
ction(+)abdu
ction(minus)
Mean
minus0016(0023)minus006
0(0050)minus0069(0046
)minus0090(0043)minus0103(0036)lt0001
0623
lt0001
0414
0147
0366
Peak
(minim
um)minus0088(0041)minus0257(010
5)minus0278(010
4)minus0369(013
7)minus0494(013
3)lt0001
0797
lt0001
0149
0002
0002
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Mean
0097(0036)
0189(0050)
0222(0064
)0252(0065)
0344(010
1)lt0001
0726
lt0001
000
40191
0010
Peak
(maxim
um)
0196(0078)
0415(014
4)0456(012
9)0530(014
8)0780(018
4)lt0001
0801
lt0001
0001
0103
0001
BioMed Research International 11
00
02
04
06
08
10
Ant
erio
r delt
oid
(a)
00
02
04
06
08
10
(b)
00
02
04
06
08
10
(c)
00
02
04
06
08
10
12
Poste
rior d
eltoi
d
(d)
00
02
04
06
08
10
12
(e)
00
02
04
06
08
10
12
(f)
00
02
04
06
08
10
Clav
icul
ar h
ead
of p
ecto
ralis
maj
or
(g)
00
02
04
06
08
10
(h)
00
02
04
06
08
10
(i)
00
02
04
06
08
10
12
14
16
0 20 40 60 80 100
Ster
nal h
ead
of p
ecto
ralis
maj
or
Normalised time (100)Mean MUR pattern (1)
0∘
27∘
36∘
48∘
71∘
(j)
00
02
04
06
08
10
12
14
16
Mean MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(k)
00
02
04
06
08
10
12
14
16
Peak MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(l)
Figure 3 Group averaged time-normalized mean profile (solid line) and standard deviation (dotted line) (a d g and j) as well as group-average (SD) mean (b e h and k) and peak (c f i and l) muscle utilization ratio (MUR) during the push phase for the five slopes tested atself-selected natural speed
12 BioMed Research International
Table6Group
average(
1SD)meanmuscle
utilisatio
nratio
(MUR)peakMUR(1)and
indicatoro
fmuscle
work(IMW)v
aluesfor
each
muscle
assessed
atthen
ondo
minantsho
uldera
tfived
ifferentslope
angles
aswellasresultsof
theA
NOVA
andpo
stho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Anteriord
eltoid
Anteriord
eltoid
MeanMUR(1)
007
(004)
021
(009)
023
(012
)026
(010
)034
(013
)lt0001
0831
lt0001
0002
lt0001
0001
Peak
MUR(1)
014
(008)
044
(023)
048
(026)
054
(026)
068
(028)lt0001
0836
lt0001
0002
lt0001
lt0001
IMW
718(398)
2070(943)
2348(1237)
2606(1043)
3448(1304)lt0001
0829
lt0001
0003
lt0001
0002
Poste
riord
eltoid
Poste
riord
eltoid
MeanMUR(1)
008
(007)
020
(014
)024
(024)
023
(010
)027
(006)lt0001
0907
lt0001
0144
lt0001
lt0001
Peak
MUR(1)
020
(014
)052
(031
)062
(051)
060
(019
)077
(019
)lt0001
0894
lt0001
0027
0001
0005
IMW
795(692)
2036(1384)
2443(2381)
2335
(1047)
2734(648)lt0001
0906
lt0001
0143
lt0001
lt0001
Clavicular
fiberso
fpectoralis
major
Clavicular
fiberso
fpectoralis
major
MeanMUR(1)
007
(004)
018
(010
)020
(010
)027
(014
)035
(018
)lt0001
0754
lt0001
0003
lt0001
0005
Peak
MUR(1)
014
(009)
038
(022)
042
(023)
057
(031
)071
(029)lt0001
0814
lt0001
000
9lt0001
0001
IMW
700(426)
1837
(977)
2041(1046)
2704(14
32)
3528(175
7)lt0001
0752
lt0001
0003
lt0001
0005
Sternalfi
bersof
pectoralismajor
Sternalfi
bersof
pectoralismajor
MeanMUR(1)
012
(008)
030
(015
)032
(013
)037
(015
)053
(024)lt0001
0781
lt0001
0005
0001
000
6Peak
MUR(1)
021
(015
)054
(023)
059
(023)
071
(026)
101(042)lt0001
0829
lt0001
0003
lt0001
0002
IMW
1194(753)
3023(14
77)
3227(1323)
3753
(1511)
5280(2406)lt0001
0780
lt0001
0005
0001
000
6
BioMed Research International 13
0
10
20
30
40
50
60
70
80
Ant
erio
r delt
oid
Poste
rior d
eltoi
d
Clav
icul
ar h
ead
ofpe
ctor
alis
maj
or
Ster
nal h
ead
of
pect
oral
is m
ajor
IMW
0∘
27∘
36∘
48∘
71∘
Figure 4 Group averaged (SD) mean indicator of muscle work(IMW) during the push phase for the five slopes tested at self-selected natural speed
At the shoulder the maximum shoulder flexion move-ment amplitude significantly increased as the slope becamesteeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments It is possible that increasedmaximumshoulder flexionwas needed to accommodate for the increased forward trunkflexion and to apply most of the force tangentially on thehandrim to preserve mechanical efficiencyThe fact that onlythe duration of the recovery period drastically decreasedas the slope became steeper can also explain in part therelatively stable shoulder flexion-extension excursion (iesimilar push phase durations across slopes) This finding isconsistent to some extent with the work of Yang et al [3]who found comparable values of movement-related adap-tation at the shoulder when comparing level overgroundand uphill (ie 3∘ slope) MWC propulsions However theshoulder flexion-extension excursion significantly increasedon average by 937∘ and the shoulder extension remainedsimilar in their study contrary to the results of the presentstudy These discrepancies may be attributed to the fact thatparticipants used test wheelchairs that were not anchoredto a safety system when propelling up a 3∘ slope at 09mson a motorized treadmill the level surface propulsion (0∘slope) was performed overground and the shoulder kine-matic calculation differed from the work by Yang et al [3]Nevertheless all these results confirmed kinematic adapta-tions at the shoulder as the slope progressed Lastly theincreased forward trunk flexion coupled with an increasedshoulder flexion that modifies the orientation of the forcegenerated at the shoulder may increase posterior shoulderjoint forces and explain the elevated muscular demand at theposterior deltoid occurring towards the end of the push phase[22]
42 Shoulder Joint Mechanical and Muscular Effort Adap-tations The shoulder joint moments adaptations partiallysupport the hypothesis that their outcome measures wouldgradually and significantly increase with each slope incre-ment while the speed remained constant For two out of thethree shoulder net joint moments investigated most of themean and peak values for the shoulder flexor and internalrotator moments progressively increased as the slope becamesteeper aside from some outcomemeasures during the 27∘ to36∘ or the 36∘ to 48∘ slope increment The relative musculardemand adaptations and muscular work computed for allmuscles investigated fully support this hypothesis since theiroutcomemeasures gradually and significantly increased witheach slope increment while the speed remained constantHence once the results of these two approaches are com-bined it is clear that the shoulder mechanical and musculareffort increases are key contributors to the adaptation processassociated with the steeper slopes Moreover these resultsare in line with the perceived UL efforts expressed by theparticipants and may explain in part The decreasing successrate with a steeper slope as shoulder strength generatingcapability most likely becomes a determinant for propellingon steeper slopes
43 Implications for Clinical Practice With the use of a slopeor of a combination of slopes when a MWC user propelshimselfherself on a motorized treadmill therapists may beable to offer task-specific high-intensity short duration inter-val training programs to increase UL strength particularlyat the shoulders Cautiousness is advised with this practicesince the risk exposure (ie increased shoulder mechanicaland muscular demands) will progressively and significantlyincrease as the slope becomes steeper and will vary accordingto the strength-generating capability of each MWC user Inaddition since the risk exposure could trigger the develop-ment or exacerbation of secondary impairments at the ULparticularly at the shoulders such a program should alsobe accompanied by proper warm-up and cool-down periodsas well as by antagonist muscle strengthening to preventmuscle strength imbalance Alternatively therapists may alsooffer task-specific cardiorespiratory fitness training programswhen a MWC user propels on a motorized treadmill withno slope or minimal slope (lt27∘) with minimal demandsduring a prolonged period of time (ie cardiorespiratoryfitness training)
44 Limits of the Study The present study included a rela-tively small sample size (119899 = 18) of experienced MWC userswho have completed their rehabilitation process which maylimit the strength of the evidence and potential to generalizethe results with new MWCs respectively The fact that theparticipants used their personal wheelchairs during the studywarrants consideration as optimal wheelchair positioningand configuration parameters most likely differs across par-ticipants and impacts the outcome measures of interest inthe present study and the risk of the MWC tilting or fallingbackwards when propelling up a slope The use of the instru-mented wheels which slightly increase the width and weight
14 BioMed Research International
of the wheelchair along with rolling resistance may havemodified participantsrsquo propulsion technique (eg increasedshoulder abduction) and fatigue level (eg increased ULeffort) in comparison to propelling with their own wheelsThe self-selected natural treadmill speed determined for eachparticipant maintained across all slopes tested in an effort toisolate the effect of speed also requires consideration sinceMWCusers tend to reduce their speedwhen propelling uphillin daily life particularly on steep slopes [2] Finally thekinematic and kinetic and electromyographic variables solelyfocused on the trunk and nondominant shoulder prevent afull understanding of UL adaptations (ie elbow and wristnot studied) during motorized treadmill MWC propulsionacross different slopes
5 Conclusion
This study confirms that MWC users with a SCI increaseforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increase during simulated uphillMWC propulsion on a motorized treadmill Few similaritieswere found between the 27∘ to 36∘ and the 36∘ to 48∘ slopeincrements for shoulder flexion and adduction momentsFuture studies incorporating interactions with various slopesand velocities could strengthen the results of the presentstudy and provide additional evidence-based knowledge onwheelchair propulsion on a motorized treadmill
Abbreviations
AIS American Spinal Injury AssociationImpairment Scale
EMG ElectromyographyER External rotationLED Light-emitting diodeIMW Indicator of muscle workIR Internal rotationJCS Joint coordinate systemMUR Muscle utilization ratioMVC Maximum voluntary contractionMWC Manual wheelchairUL Upper limbWUSPI Wheelchair Userrsquos Shoulder Pain
Index
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors would like to thank Michel Goyette (Eng)Daniel Marineau (Technician) Youssef El Khamlichi(Research Associate) and Philippe Gourdou (ResearchAssociate) for their contributions to this project DanyGagnon holds a Junior 1 Research Career Award from
the Fonds de la recherche du Quebec-Sante (FRQ-S)Annie-Claude Babineau and Guillaume Desroches aresupported by a summer internship and a post-doctoralfellowship from the Canadian Institutes of Health Researchrespectively DanyGagnon andRachid Aissaoui aremembersof the Multidisciplinary SensoriMotor RehabilitationResearch Team (httpwwwerrsmca) supported bythe CIHR and the Quebec-Ontario Spinal Cord InjuryMobility (SCI-MOB) Research Group funded by theQuebec Rehabilitation Research Network (REPARhttpwwwreparca) and the Ontario NeuroTraumaFoundation (ONF httpwwwonforg) The project wasfunded in part by the Fonds de la recherche du Quebec-Sante(FRQS) The equipment and material required for theresearch completed at the Pathokinesiology Laboratory wasfinanced by the Canada Foundation for Innovation (CFI)
References
[1] B Mason J Lenton C Leicht and V Goosey-Tolfrey ldquoAphysiological and biomechanical comparison of over-groundtreadmill and ergometer wheelchair propulsionrdquo Journal ofSports Sciences vol 32 no 1 pp 78ndash91 2014
[2] W M Richter R Rodriguez K R Woods and P W AxelsonldquoStroke pattern and handrim biomechanics for level and uphillwheelchair propulsion at self-selected speedsrdquo Archives of Phys-ical Medicine and Rehabilitation vol 88 no 1 pp 81ndash87 2007
[3] Y-S Yang A M Koontz S-J Yeh and J-J Chang ldquoEffectof backrest height on wheelchair propulsion biomechanics forlevel and uphill conditionsrdquo Archives of Physical Medicine andRehabilitation vol 93 no 4 pp 654ndash659 2012
[4] D H Gagnon A-C Babineau A Champagne G Desrochesand R Aissaoui ldquoPushrim biomechanical changes with pro-gressive increases in slope during motorized treadmill manualwheelchair propulsion in individuals with spinal cord injuryrdquoJournal of Rehabilitation Research amp Development vol 51 no 5pp 789ndash802 2014
[5] J W Chow T A Millikan L G Carlton W-S Chae Y-T Lim and M I Morse ldquoKinematic and electromyographicanalysis of wheelchair propulsion on ramps of different slopesfor young men with Paraplegiardquo Archives of Physical Medicineand Rehabilitation vol 90 no 2 pp 271ndash278 2009
[6] S van Drongelen L H van Der Woude T W Janssen E LAngenot E K Chadwick and D H Veeger ldquoMechanical loadon the upper extremity during wheelchair activitiesrdquo Archivesof Physical Medicine and Rehabilitation vol 86 no 6 pp 1214ndash1220 2005
[7] H Arabi R Aissaoui J Rousseau D Bourbonnais and JDansereau ldquoEvaluation of minimal mechanical effort duringthe ramp access of manual wheelchairrdquo Ergonomia vol 26 no3 pp 253ndash259 2004
[8] K Kulig S S Rao S J Mulroy et al ldquoShoulder joint kineticsduring the push phase of wheelchair propulsionrdquo ClinicalOrthopaedics and Related Research no 354 pp 132ndash143 1998
[9] L J Chapman and J P Chapman ldquoThe measurement ofhandednessrdquoBrain andCognition vol 6 no 2 pp 175ndash183 1987
[10] Gouvernement du Quebec Regie du Batiment du Quebec(RBQ) Construction Code Building Act Chapter 1 Architec-tural and Transportation Barriers Compliance Board 2013
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
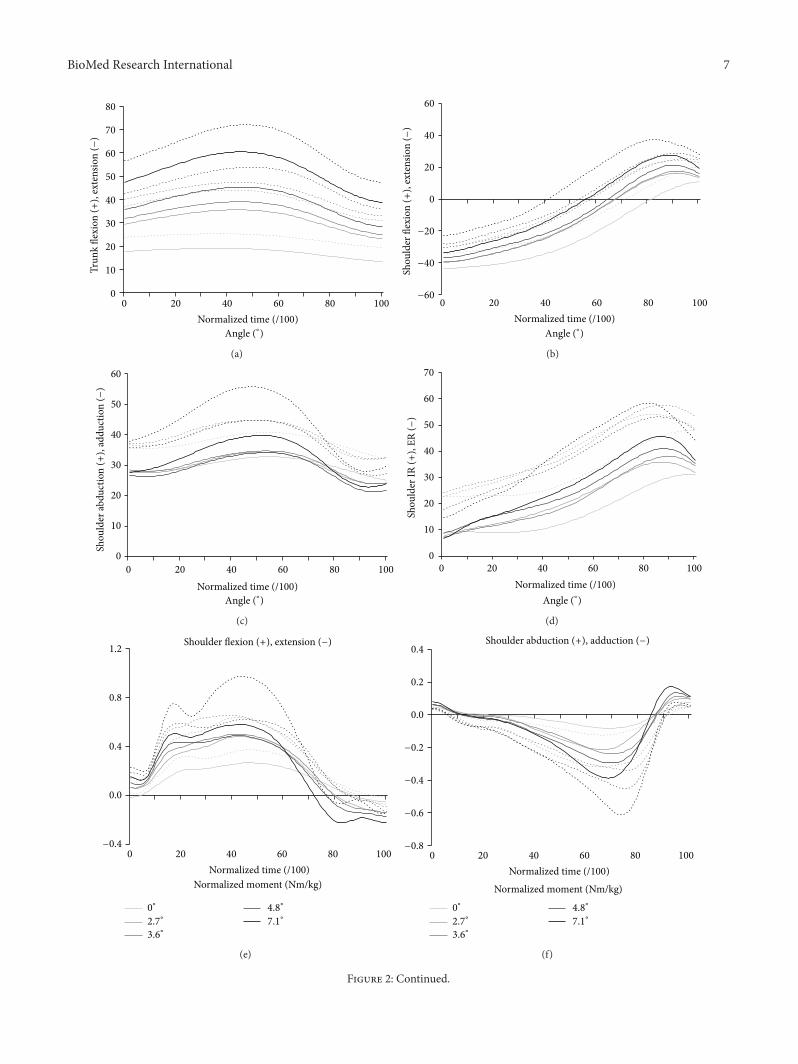
BioMed Research International 7
0
10
20
30
40
50
60
70
80
Trun
k fle
xion
(+)
exte
nsio
n (minus
)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(a)
60
40
20
0
minus20
minus40
minus60
Shou
lder
flex
ion
(+)
exte
nsio
n (minus
)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(b)
0
10
20
30
40
50
60
Shou
lder
abdu
ctio
n (+
) ad
duct
ion
(minus)
0 20 40 60 80 100
Normalized time (100)Angle (∘)
(c)
0
10
20
30
40
50
60
70
0 20 40 60 80 100
Normalized time (100)Angle (∘)
Shou
lder
IR (+
) ER
(minus)
(d)
12
08
04
00
minus04
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder flexion (+) extension (minus)
(e)
04
02
00
minus02
minus04
minus06
minus08
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder abduction (+) adduction (minus)
(f)
Figure 2 Continued
8 BioMed Research International
10
08
06
04
02
00
minus02
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder IR (+) ER (minus)
(g)
Figure 2 Group averaged time-normalized profile (solid line) and standard deviation (dotted line) of the shoulder and trunk kinematics (ab c and d) and weight-normalised shoulder moments (e f and g) during the push phase for the five slopes tested at self-selected naturalspeed
the 0∘ to 27∘ 36∘ to 48∘ and 48∘ to 71∘ slope incrementsThemean and maximum internal rotation moments significantlyincreased as the slope became steeper except for the 36∘ to48∘ slope increment
35 Shoulder Muscular Demand The MUR patterns of themuscles studied are illustrated in Figure 3 while their meanand maximum values are summarized in Table 6 The meanIMWs of the muscles studied are summarized in Table 6 andillustrated in Figure 4 For allmuscles studied theirmean andmaximum MURs as well as their indicator of muscle workvalue significantly increased as the slope became steeperexcept for the posterior deltoid that remained comparablebetween the 27∘ to 36∘ slope increment
4 Discussion
This study quantified trunk and nondominant shoulderkinematic changes along with nondominant shoulder jointmoments and electromyographic changes during MWCpropulsion on a motorized treadmill set at a self-selectednatural speed on five different slopes (ie 0∘ 27∘ 36∘ 48∘and 71∘) Overall the MWC users with a SCI increasedforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increased during simulated uphillMWC propulsion on a motorized treadmill
41 Trunk and Shoulder Movement-Related Adaptations Themovement-related adaptations occurring at the trunk andshoulder partially support the hypothesis that their outcome
measures would gradually and significantly increase witheach slope increment while the speed remained constantAt the trunk the maximum forward trunk flexion and thetotal trunk excursion increased significantly as the slopebecame steeper except for the 27∘ to 36∘ slope incrementChow et al [5] obtained somewhat comparable resultsin terms of trunk kinematics although no difference wasrevealed when comparing 4∘ and 8∘ slopes This may beexplained by the fact that participants propelled at self-selected speeds that decreased progressively in their protocolas the slope increased Nonetheless the increased maximumforward trunk flexion coupled with the increased forwardtrunk excursion may allow MWC users to move their centreof mass further and faster anteriorly and to maintain itsprojection in front of the rear wheel axle in order toprevent backward tilt and falls as the slope increases Thismay also explain why maximum forward trunk flexion andforward trunk excursion became greater as the gravitationaleffects became harder to overcome with steeper slopes Thedecreasing success rate with a steeper slope may be explainedin part by the fact that some participants were classified asbeing overweight (body mass index gt 25) or class I obese(body mass index = 300ndash349) with associated abdominalobesity that limited their ability to increase forward trunkflexion to accommodate for the steeper slopes In fact 556of participants who were unable to propel up the 71∘ slopewere overweight (119873 = 3) or obese (119873 = 2) whereasonly 30 of participants who were able to propel up the 71∘slope were overweight (119873 = 2) or obese (119873 = 1) Henceabdominal circumference may deserve additional attentionwhen investigating wheelchair propulsion technique or man-ual wheelchair skills such as uphill propulsion
BioMed Research International 9
Table4Group
average(SD)totalexcursio
n(∘ )
and
maxim
umandminim
um(∘ )
kinematicvalues
measuredatthetrun
kandno
ndom
inantsho
uldera
tthe
fivedifferent
slopestestedas
wellasthe
results
oftheA
NOVA
andpo
stho
ccom
paris
ontest
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Jointangle(∘
)
Trun
kmdashflexion
(+)extension(minus)
Trun
kmdashflexion
(+)extension(minus)
Excursion
588
(212
)1267(340)
1456(277)
1761
(396)
2237
(600)lt0001
0907
lt0001
000
6lt0001
0003
Maxim
um1927(623)
3592(845)
3945(831
)4579(853
)6093(113
0)lt0001
0889
lt0001
0031
0002
0005
Minim
um1339
(614
)2326(775)
2490(805)
2818
(771)
3857(859)lt0001
0910
lt0001
0028
lt0001
lt0001
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Excursion
5567(920)
5817
(1092)
5963(901)
6019
(698)
6499(895)
0019
0296
0072
0183
0473
0217
Maxim
um1131
(934)
1800(820)
1935
(762)
2259(730)
3088(745)lt0001
0849
lt0001
0001
0054
lt0001
Minim
umminus44
36(935
)minus40
17(936)minus40
27(915
)minus3760(834)minus3410
(1036)lt0001
0651
lt0001
000
6lt0001
lt0001
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Excursion
935(343)
1227(716)
1348(661)
1488(756)
1965(118
8)0012
0337
0010
0363
0158
0047
Maxim
um3325(800)
3481(1065)
3540(1026)
3488(1057)
4060(1543)
0083
mdashmdash
mdashmdash
mdashMinim
um2390(627)
2253
(726)
2192(666)
2000(545)
2094(570)
0038
mdashmdash
mdashmdash
mdashShou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Excursion
2486(820)
3055(1024)
3335(883)
3452
(944)
4328(113
4)lt0001
0623
000
4004
00765
0013
Maxim
um3157(1682)
3789(1846
)40
15(19
17)
4302(1223)
4969(871)lt0001
0665
lt0001
0029
0855
0033
Minim
um671
(1357)
734(1510)
680
(1694)
850
(918
)641
(770)
0152
mdashmdash
mdashmdash
mdash
10 BioMed Research International
Table5Group
average(
SD)m
eanandpeak
weight-n
ormalise
dmom
ents(N
mkg)
measuredatthen
ondo
minantsho
uldera
tthe
fived
ifferentslopesa
swellasresultsof
theA
NOVA
and
postho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Normalisedmoments(Nmkg)
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Mean
0140(0056)
0226(0067)
0248(0081)
0233(0083)
0242(015
1)0027
0288
lt0001
0003
0433
0966
Peak
(maxim
um)
0292(010
9)0512(015
2)0546(016
7)0559(012
8)0733(0302)lt0001
0588
lt0001
000
40867
0049
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashaddu
ction(+)abdu
ction(minus)
Mean
minus0016(0023)minus006
0(0050)minus0069(0046
)minus0090(0043)minus0103(0036)lt0001
0623
lt0001
0414
0147
0366
Peak
(minim
um)minus0088(0041)minus0257(010
5)minus0278(010
4)minus0369(013
7)minus0494(013
3)lt0001
0797
lt0001
0149
0002
0002
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Mean
0097(0036)
0189(0050)
0222(0064
)0252(0065)
0344(010
1)lt0001
0726
lt0001
000
40191
0010
Peak
(maxim
um)
0196(0078)
0415(014
4)0456(012
9)0530(014
8)0780(018
4)lt0001
0801
lt0001
0001
0103
0001
BioMed Research International 11
00
02
04
06
08
10
Ant
erio
r delt
oid
(a)
00
02
04
06
08
10
(b)
00
02
04
06
08
10
(c)
00
02
04
06
08
10
12
Poste
rior d
eltoi
d
(d)
00
02
04
06
08
10
12
(e)
00
02
04
06
08
10
12
(f)
00
02
04
06
08
10
Clav
icul
ar h
ead
of p
ecto
ralis
maj
or
(g)
00
02
04
06
08
10
(h)
00
02
04
06
08
10
(i)
00
02
04
06
08
10
12
14
16
0 20 40 60 80 100
Ster
nal h
ead
of p
ecto
ralis
maj
or
Normalised time (100)Mean MUR pattern (1)
0∘
27∘
36∘
48∘
71∘
(j)
00
02
04
06
08
10
12
14
16
Mean MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(k)
00
02
04
06
08
10
12
14
16
Peak MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(l)
Figure 3 Group averaged time-normalized mean profile (solid line) and standard deviation (dotted line) (a d g and j) as well as group-average (SD) mean (b e h and k) and peak (c f i and l) muscle utilization ratio (MUR) during the push phase for the five slopes tested atself-selected natural speed
12 BioMed Research International
Table6Group
average(
1SD)meanmuscle
utilisatio
nratio
(MUR)peakMUR(1)and
indicatoro
fmuscle
work(IMW)v
aluesfor
each
muscle
assessed
atthen
ondo
minantsho
uldera
tfived
ifferentslope
angles
aswellasresultsof
theA
NOVA
andpo
stho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Anteriord
eltoid
Anteriord
eltoid
MeanMUR(1)
007
(004)
021
(009)
023
(012
)026
(010
)034
(013
)lt0001
0831
lt0001
0002
lt0001
0001
Peak
MUR(1)
014
(008)
044
(023)
048
(026)
054
(026)
068
(028)lt0001
0836
lt0001
0002
lt0001
lt0001
IMW
718(398)
2070(943)
2348(1237)
2606(1043)
3448(1304)lt0001
0829
lt0001
0003
lt0001
0002
Poste
riord
eltoid
Poste
riord
eltoid
MeanMUR(1)
008
(007)
020
(014
)024
(024)
023
(010
)027
(006)lt0001
0907
lt0001
0144
lt0001
lt0001
Peak
MUR(1)
020
(014
)052
(031
)062
(051)
060
(019
)077
(019
)lt0001
0894
lt0001
0027
0001
0005
IMW
795(692)
2036(1384)
2443(2381)
2335
(1047)
2734(648)lt0001
0906
lt0001
0143
lt0001
lt0001
Clavicular
fiberso
fpectoralis
major
Clavicular
fiberso
fpectoralis
major
MeanMUR(1)
007
(004)
018
(010
)020
(010
)027
(014
)035
(018
)lt0001
0754
lt0001
0003
lt0001
0005
Peak
MUR(1)
014
(009)
038
(022)
042
(023)
057
(031
)071
(029)lt0001
0814
lt0001
000
9lt0001
0001
IMW
700(426)
1837
(977)
2041(1046)
2704(14
32)
3528(175
7)lt0001
0752
lt0001
0003
lt0001
0005
Sternalfi
bersof
pectoralismajor
Sternalfi
bersof
pectoralismajor
MeanMUR(1)
012
(008)
030
(015
)032
(013
)037
(015
)053
(024)lt0001
0781
lt0001
0005
0001
000
6Peak
MUR(1)
021
(015
)054
(023)
059
(023)
071
(026)
101(042)lt0001
0829
lt0001
0003
lt0001
0002
IMW
1194(753)
3023(14
77)
3227(1323)
3753
(1511)
5280(2406)lt0001
0780
lt0001
0005
0001
000
6
BioMed Research International 13
0
10
20
30
40
50
60
70
80
Ant
erio
r delt
oid
Poste
rior d
eltoi
d
Clav
icul
ar h
ead
ofpe
ctor
alis
maj
or
Ster
nal h
ead
of
pect
oral
is m
ajor
IMW
0∘
27∘
36∘
48∘
71∘
Figure 4 Group averaged (SD) mean indicator of muscle work(IMW) during the push phase for the five slopes tested at self-selected natural speed
At the shoulder the maximum shoulder flexion move-ment amplitude significantly increased as the slope becamesteeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments It is possible that increasedmaximumshoulder flexionwas needed to accommodate for the increased forward trunkflexion and to apply most of the force tangentially on thehandrim to preserve mechanical efficiencyThe fact that onlythe duration of the recovery period drastically decreasedas the slope became steeper can also explain in part therelatively stable shoulder flexion-extension excursion (iesimilar push phase durations across slopes) This finding isconsistent to some extent with the work of Yang et al [3]who found comparable values of movement-related adap-tation at the shoulder when comparing level overgroundand uphill (ie 3∘ slope) MWC propulsions However theshoulder flexion-extension excursion significantly increasedon average by 937∘ and the shoulder extension remainedsimilar in their study contrary to the results of the presentstudy These discrepancies may be attributed to the fact thatparticipants used test wheelchairs that were not anchoredto a safety system when propelling up a 3∘ slope at 09mson a motorized treadmill the level surface propulsion (0∘slope) was performed overground and the shoulder kine-matic calculation differed from the work by Yang et al [3]Nevertheless all these results confirmed kinematic adapta-tions at the shoulder as the slope progressed Lastly theincreased forward trunk flexion coupled with an increasedshoulder flexion that modifies the orientation of the forcegenerated at the shoulder may increase posterior shoulderjoint forces and explain the elevated muscular demand at theposterior deltoid occurring towards the end of the push phase[22]
42 Shoulder Joint Mechanical and Muscular Effort Adap-tations The shoulder joint moments adaptations partiallysupport the hypothesis that their outcome measures wouldgradually and significantly increase with each slope incre-ment while the speed remained constant For two out of thethree shoulder net joint moments investigated most of themean and peak values for the shoulder flexor and internalrotator moments progressively increased as the slope becamesteeper aside from some outcomemeasures during the 27∘ to36∘ or the 36∘ to 48∘ slope increment The relative musculardemand adaptations and muscular work computed for allmuscles investigated fully support this hypothesis since theiroutcomemeasures gradually and significantly increased witheach slope increment while the speed remained constantHence once the results of these two approaches are com-bined it is clear that the shoulder mechanical and musculareffort increases are key contributors to the adaptation processassociated with the steeper slopes Moreover these resultsare in line with the perceived UL efforts expressed by theparticipants and may explain in part The decreasing successrate with a steeper slope as shoulder strength generatingcapability most likely becomes a determinant for propellingon steeper slopes
43 Implications for Clinical Practice With the use of a slopeor of a combination of slopes when a MWC user propelshimselfherself on a motorized treadmill therapists may beable to offer task-specific high-intensity short duration inter-val training programs to increase UL strength particularlyat the shoulders Cautiousness is advised with this practicesince the risk exposure (ie increased shoulder mechanicaland muscular demands) will progressively and significantlyincrease as the slope becomes steeper and will vary accordingto the strength-generating capability of each MWC user Inaddition since the risk exposure could trigger the develop-ment or exacerbation of secondary impairments at the ULparticularly at the shoulders such a program should alsobe accompanied by proper warm-up and cool-down periodsas well as by antagonist muscle strengthening to preventmuscle strength imbalance Alternatively therapists may alsooffer task-specific cardiorespiratory fitness training programswhen a MWC user propels on a motorized treadmill withno slope or minimal slope (lt27∘) with minimal demandsduring a prolonged period of time (ie cardiorespiratoryfitness training)
44 Limits of the Study The present study included a rela-tively small sample size (119899 = 18) of experienced MWC userswho have completed their rehabilitation process which maylimit the strength of the evidence and potential to generalizethe results with new MWCs respectively The fact that theparticipants used their personal wheelchairs during the studywarrants consideration as optimal wheelchair positioningand configuration parameters most likely differs across par-ticipants and impacts the outcome measures of interest inthe present study and the risk of the MWC tilting or fallingbackwards when propelling up a slope The use of the instru-mented wheels which slightly increase the width and weight
14 BioMed Research International
of the wheelchair along with rolling resistance may havemodified participantsrsquo propulsion technique (eg increasedshoulder abduction) and fatigue level (eg increased ULeffort) in comparison to propelling with their own wheelsThe self-selected natural treadmill speed determined for eachparticipant maintained across all slopes tested in an effort toisolate the effect of speed also requires consideration sinceMWCusers tend to reduce their speedwhen propelling uphillin daily life particularly on steep slopes [2] Finally thekinematic and kinetic and electromyographic variables solelyfocused on the trunk and nondominant shoulder prevent afull understanding of UL adaptations (ie elbow and wristnot studied) during motorized treadmill MWC propulsionacross different slopes
5 Conclusion
This study confirms that MWC users with a SCI increaseforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increase during simulated uphillMWC propulsion on a motorized treadmill Few similaritieswere found between the 27∘ to 36∘ and the 36∘ to 48∘ slopeincrements for shoulder flexion and adduction momentsFuture studies incorporating interactions with various slopesand velocities could strengthen the results of the presentstudy and provide additional evidence-based knowledge onwheelchair propulsion on a motorized treadmill
Abbreviations
AIS American Spinal Injury AssociationImpairment Scale
EMG ElectromyographyER External rotationLED Light-emitting diodeIMW Indicator of muscle workIR Internal rotationJCS Joint coordinate systemMUR Muscle utilization ratioMVC Maximum voluntary contractionMWC Manual wheelchairUL Upper limbWUSPI Wheelchair Userrsquos Shoulder Pain
Index
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors would like to thank Michel Goyette (Eng)Daniel Marineau (Technician) Youssef El Khamlichi(Research Associate) and Philippe Gourdou (ResearchAssociate) for their contributions to this project DanyGagnon holds a Junior 1 Research Career Award from
the Fonds de la recherche du Quebec-Sante (FRQ-S)Annie-Claude Babineau and Guillaume Desroches aresupported by a summer internship and a post-doctoralfellowship from the Canadian Institutes of Health Researchrespectively DanyGagnon andRachid Aissaoui aremembersof the Multidisciplinary SensoriMotor RehabilitationResearch Team (httpwwwerrsmca) supported bythe CIHR and the Quebec-Ontario Spinal Cord InjuryMobility (SCI-MOB) Research Group funded by theQuebec Rehabilitation Research Network (REPARhttpwwwreparca) and the Ontario NeuroTraumaFoundation (ONF httpwwwonforg) The project wasfunded in part by the Fonds de la recherche du Quebec-Sante(FRQS) The equipment and material required for theresearch completed at the Pathokinesiology Laboratory wasfinanced by the Canada Foundation for Innovation (CFI)
References
[1] B Mason J Lenton C Leicht and V Goosey-Tolfrey ldquoAphysiological and biomechanical comparison of over-groundtreadmill and ergometer wheelchair propulsionrdquo Journal ofSports Sciences vol 32 no 1 pp 78ndash91 2014
[2] W M Richter R Rodriguez K R Woods and P W AxelsonldquoStroke pattern and handrim biomechanics for level and uphillwheelchair propulsion at self-selected speedsrdquo Archives of Phys-ical Medicine and Rehabilitation vol 88 no 1 pp 81ndash87 2007
[3] Y-S Yang A M Koontz S-J Yeh and J-J Chang ldquoEffectof backrest height on wheelchair propulsion biomechanics forlevel and uphill conditionsrdquo Archives of Physical Medicine andRehabilitation vol 93 no 4 pp 654ndash659 2012
[4] D H Gagnon A-C Babineau A Champagne G Desrochesand R Aissaoui ldquoPushrim biomechanical changes with pro-gressive increases in slope during motorized treadmill manualwheelchair propulsion in individuals with spinal cord injuryrdquoJournal of Rehabilitation Research amp Development vol 51 no 5pp 789ndash802 2014
[5] J W Chow T A Millikan L G Carlton W-S Chae Y-T Lim and M I Morse ldquoKinematic and electromyographicanalysis of wheelchair propulsion on ramps of different slopesfor young men with Paraplegiardquo Archives of Physical Medicineand Rehabilitation vol 90 no 2 pp 271ndash278 2009
[6] S van Drongelen L H van Der Woude T W Janssen E LAngenot E K Chadwick and D H Veeger ldquoMechanical loadon the upper extremity during wheelchair activitiesrdquo Archivesof Physical Medicine and Rehabilitation vol 86 no 6 pp 1214ndash1220 2005
[7] H Arabi R Aissaoui J Rousseau D Bourbonnais and JDansereau ldquoEvaluation of minimal mechanical effort duringthe ramp access of manual wheelchairrdquo Ergonomia vol 26 no3 pp 253ndash259 2004
[8] K Kulig S S Rao S J Mulroy et al ldquoShoulder joint kineticsduring the push phase of wheelchair propulsionrdquo ClinicalOrthopaedics and Related Research no 354 pp 132ndash143 1998
[9] L J Chapman and J P Chapman ldquoThe measurement ofhandednessrdquoBrain andCognition vol 6 no 2 pp 175ndash183 1987
[10] Gouvernement du Quebec Regie du Batiment du Quebec(RBQ) Construction Code Building Act Chapter 1 Architec-tural and Transportation Barriers Compliance Board 2013
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 BioMed Research International
10
08
06
04
02
00
minus02
0 20 40 60 80 100
Normalized time (100)Normalized moment (Nmkg)
0∘
36∘
48∘
27∘
71∘
Shoulder IR (+) ER (minus)
(g)
Figure 2 Group averaged time-normalized profile (solid line) and standard deviation (dotted line) of the shoulder and trunk kinematics (ab c and d) and weight-normalised shoulder moments (e f and g) during the push phase for the five slopes tested at self-selected naturalspeed
the 0∘ to 27∘ 36∘ to 48∘ and 48∘ to 71∘ slope incrementsThemean and maximum internal rotation moments significantlyincreased as the slope became steeper except for the 36∘ to48∘ slope increment
35 Shoulder Muscular Demand The MUR patterns of themuscles studied are illustrated in Figure 3 while their meanand maximum values are summarized in Table 6 The meanIMWs of the muscles studied are summarized in Table 6 andillustrated in Figure 4 For allmuscles studied theirmean andmaximum MURs as well as their indicator of muscle workvalue significantly increased as the slope became steeperexcept for the posterior deltoid that remained comparablebetween the 27∘ to 36∘ slope increment
4 Discussion
This study quantified trunk and nondominant shoulderkinematic changes along with nondominant shoulder jointmoments and electromyographic changes during MWCpropulsion on a motorized treadmill set at a self-selectednatural speed on five different slopes (ie 0∘ 27∘ 36∘ 48∘and 71∘) Overall the MWC users with a SCI increasedforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increased during simulated uphillMWC propulsion on a motorized treadmill
41 Trunk and Shoulder Movement-Related Adaptations Themovement-related adaptations occurring at the trunk andshoulder partially support the hypothesis that their outcome
measures would gradually and significantly increase witheach slope increment while the speed remained constantAt the trunk the maximum forward trunk flexion and thetotal trunk excursion increased significantly as the slopebecame steeper except for the 27∘ to 36∘ slope incrementChow et al [5] obtained somewhat comparable resultsin terms of trunk kinematics although no difference wasrevealed when comparing 4∘ and 8∘ slopes This may beexplained by the fact that participants propelled at self-selected speeds that decreased progressively in their protocolas the slope increased Nonetheless the increased maximumforward trunk flexion coupled with the increased forwardtrunk excursion may allow MWC users to move their centreof mass further and faster anteriorly and to maintain itsprojection in front of the rear wheel axle in order toprevent backward tilt and falls as the slope increases Thismay also explain why maximum forward trunk flexion andforward trunk excursion became greater as the gravitationaleffects became harder to overcome with steeper slopes Thedecreasing success rate with a steeper slope may be explainedin part by the fact that some participants were classified asbeing overweight (body mass index gt 25) or class I obese(body mass index = 300ndash349) with associated abdominalobesity that limited their ability to increase forward trunkflexion to accommodate for the steeper slopes In fact 556of participants who were unable to propel up the 71∘ slopewere overweight (119873 = 3) or obese (119873 = 2) whereasonly 30 of participants who were able to propel up the 71∘slope were overweight (119873 = 2) or obese (119873 = 1) Henceabdominal circumference may deserve additional attentionwhen investigating wheelchair propulsion technique or man-ual wheelchair skills such as uphill propulsion
BioMed Research International 9
Table4Group
average(SD)totalexcursio
n(∘ )
and
maxim
umandminim
um(∘ )
kinematicvalues
measuredatthetrun
kandno
ndom
inantsho
uldera
tthe
fivedifferent
slopestestedas
wellasthe
results
oftheA
NOVA
andpo
stho
ccom
paris
ontest
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Jointangle(∘
)
Trun
kmdashflexion
(+)extension(minus)
Trun
kmdashflexion
(+)extension(minus)
Excursion
588
(212
)1267(340)
1456(277)
1761
(396)
2237
(600)lt0001
0907
lt0001
000
6lt0001
0003
Maxim
um1927(623)
3592(845)
3945(831
)4579(853
)6093(113
0)lt0001
0889
lt0001
0031
0002
0005
Minim
um1339
(614
)2326(775)
2490(805)
2818
(771)
3857(859)lt0001
0910
lt0001
0028
lt0001
lt0001
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Excursion
5567(920)
5817
(1092)
5963(901)
6019
(698)
6499(895)
0019
0296
0072
0183
0473
0217
Maxim
um1131
(934)
1800(820)
1935
(762)
2259(730)
3088(745)lt0001
0849
lt0001
0001
0054
lt0001
Minim
umminus44
36(935
)minus40
17(936)minus40
27(915
)minus3760(834)minus3410
(1036)lt0001
0651
lt0001
000
6lt0001
lt0001
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Excursion
935(343)
1227(716)
1348(661)
1488(756)
1965(118
8)0012
0337
0010
0363
0158
0047
Maxim
um3325(800)
3481(1065)
3540(1026)
3488(1057)
4060(1543)
0083
mdashmdash
mdashmdash
mdashMinim
um2390(627)
2253
(726)
2192(666)
2000(545)
2094(570)
0038
mdashmdash
mdashmdash
mdashShou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Excursion
2486(820)
3055(1024)
3335(883)
3452
(944)
4328(113
4)lt0001
0623
000
4004
00765
0013
Maxim
um3157(1682)
3789(1846
)40
15(19
17)
4302(1223)
4969(871)lt0001
0665
lt0001
0029
0855
0033
Minim
um671
(1357)
734(1510)
680
(1694)
850
(918
)641
(770)
0152
mdashmdash
mdashmdash
mdash
10 BioMed Research International
Table5Group
average(
SD)m
eanandpeak
weight-n
ormalise
dmom
ents(N
mkg)
measuredatthen
ondo
minantsho
uldera
tthe
fived
ifferentslopesa
swellasresultsof
theA
NOVA
and
postho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Normalisedmoments(Nmkg)
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Mean
0140(0056)
0226(0067)
0248(0081)
0233(0083)
0242(015
1)0027
0288
lt0001
0003
0433
0966
Peak
(maxim
um)
0292(010
9)0512(015
2)0546(016
7)0559(012
8)0733(0302)lt0001
0588
lt0001
000
40867
0049
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashaddu
ction(+)abdu
ction(minus)
Mean
minus0016(0023)minus006
0(0050)minus0069(0046
)minus0090(0043)minus0103(0036)lt0001
0623
lt0001
0414
0147
0366
Peak
(minim
um)minus0088(0041)minus0257(010
5)minus0278(010
4)minus0369(013
7)minus0494(013
3)lt0001
0797
lt0001
0149
0002
0002
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Mean
0097(0036)
0189(0050)
0222(0064
)0252(0065)
0344(010
1)lt0001
0726
lt0001
000
40191
0010
Peak
(maxim
um)
0196(0078)
0415(014
4)0456(012
9)0530(014
8)0780(018
4)lt0001
0801
lt0001
0001
0103
0001
BioMed Research International 11
00
02
04
06
08
10
Ant
erio
r delt
oid
(a)
00
02
04
06
08
10
(b)
00
02
04
06
08
10
(c)
00
02
04
06
08
10
12
Poste
rior d
eltoi
d
(d)
00
02
04
06
08
10
12
(e)
00
02
04
06
08
10
12
(f)
00
02
04
06
08
10
Clav
icul
ar h
ead
of p
ecto
ralis
maj
or
(g)
00
02
04
06
08
10
(h)
00
02
04
06
08
10
(i)
00
02
04
06
08
10
12
14
16
0 20 40 60 80 100
Ster
nal h
ead
of p
ecto
ralis
maj
or
Normalised time (100)Mean MUR pattern (1)
0∘
27∘
36∘
48∘
71∘
(j)
00
02
04
06
08
10
12
14
16
Mean MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(k)
00
02
04
06
08
10
12
14
16
Peak MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(l)
Figure 3 Group averaged time-normalized mean profile (solid line) and standard deviation (dotted line) (a d g and j) as well as group-average (SD) mean (b e h and k) and peak (c f i and l) muscle utilization ratio (MUR) during the push phase for the five slopes tested atself-selected natural speed
12 BioMed Research International
Table6Group
average(
1SD)meanmuscle
utilisatio
nratio
(MUR)peakMUR(1)and
indicatoro
fmuscle
work(IMW)v
aluesfor
each
muscle
assessed
atthen
ondo
minantsho
uldera
tfived
ifferentslope
angles
aswellasresultsof
theA
NOVA
andpo
stho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Anteriord
eltoid
Anteriord
eltoid
MeanMUR(1)
007
(004)
021
(009)
023
(012
)026
(010
)034
(013
)lt0001
0831
lt0001
0002
lt0001
0001
Peak
MUR(1)
014
(008)
044
(023)
048
(026)
054
(026)
068
(028)lt0001
0836
lt0001
0002
lt0001
lt0001
IMW
718(398)
2070(943)
2348(1237)
2606(1043)
3448(1304)lt0001
0829
lt0001
0003
lt0001
0002
Poste
riord
eltoid
Poste
riord
eltoid
MeanMUR(1)
008
(007)
020
(014
)024
(024)
023
(010
)027
(006)lt0001
0907
lt0001
0144
lt0001
lt0001
Peak
MUR(1)
020
(014
)052
(031
)062
(051)
060
(019
)077
(019
)lt0001
0894
lt0001
0027
0001
0005
IMW
795(692)
2036(1384)
2443(2381)
2335
(1047)
2734(648)lt0001
0906
lt0001
0143
lt0001
lt0001
Clavicular
fiberso
fpectoralis
major
Clavicular
fiberso
fpectoralis
major
MeanMUR(1)
007
(004)
018
(010
)020
(010
)027
(014
)035
(018
)lt0001
0754
lt0001
0003
lt0001
0005
Peak
MUR(1)
014
(009)
038
(022)
042
(023)
057
(031
)071
(029)lt0001
0814
lt0001
000
9lt0001
0001
IMW
700(426)
1837
(977)
2041(1046)
2704(14
32)
3528(175
7)lt0001
0752
lt0001
0003
lt0001
0005
Sternalfi
bersof
pectoralismajor
Sternalfi
bersof
pectoralismajor
MeanMUR(1)
012
(008)
030
(015
)032
(013
)037
(015
)053
(024)lt0001
0781
lt0001
0005
0001
000
6Peak
MUR(1)
021
(015
)054
(023)
059
(023)
071
(026)
101(042)lt0001
0829
lt0001
0003
lt0001
0002
IMW
1194(753)
3023(14
77)
3227(1323)
3753
(1511)
5280(2406)lt0001
0780
lt0001
0005
0001
000
6
BioMed Research International 13
0
10
20
30
40
50
60
70
80
Ant
erio
r delt
oid
Poste
rior d
eltoi
d
Clav
icul
ar h
ead
ofpe
ctor
alis
maj
or
Ster
nal h
ead
of
pect
oral
is m
ajor
IMW
0∘
27∘
36∘
48∘
71∘
Figure 4 Group averaged (SD) mean indicator of muscle work(IMW) during the push phase for the five slopes tested at self-selected natural speed
At the shoulder the maximum shoulder flexion move-ment amplitude significantly increased as the slope becamesteeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments It is possible that increasedmaximumshoulder flexionwas needed to accommodate for the increased forward trunkflexion and to apply most of the force tangentially on thehandrim to preserve mechanical efficiencyThe fact that onlythe duration of the recovery period drastically decreasedas the slope became steeper can also explain in part therelatively stable shoulder flexion-extension excursion (iesimilar push phase durations across slopes) This finding isconsistent to some extent with the work of Yang et al [3]who found comparable values of movement-related adap-tation at the shoulder when comparing level overgroundand uphill (ie 3∘ slope) MWC propulsions However theshoulder flexion-extension excursion significantly increasedon average by 937∘ and the shoulder extension remainedsimilar in their study contrary to the results of the presentstudy These discrepancies may be attributed to the fact thatparticipants used test wheelchairs that were not anchoredto a safety system when propelling up a 3∘ slope at 09mson a motorized treadmill the level surface propulsion (0∘slope) was performed overground and the shoulder kine-matic calculation differed from the work by Yang et al [3]Nevertheless all these results confirmed kinematic adapta-tions at the shoulder as the slope progressed Lastly theincreased forward trunk flexion coupled with an increasedshoulder flexion that modifies the orientation of the forcegenerated at the shoulder may increase posterior shoulderjoint forces and explain the elevated muscular demand at theposterior deltoid occurring towards the end of the push phase[22]
42 Shoulder Joint Mechanical and Muscular Effort Adap-tations The shoulder joint moments adaptations partiallysupport the hypothesis that their outcome measures wouldgradually and significantly increase with each slope incre-ment while the speed remained constant For two out of thethree shoulder net joint moments investigated most of themean and peak values for the shoulder flexor and internalrotator moments progressively increased as the slope becamesteeper aside from some outcomemeasures during the 27∘ to36∘ or the 36∘ to 48∘ slope increment The relative musculardemand adaptations and muscular work computed for allmuscles investigated fully support this hypothesis since theiroutcomemeasures gradually and significantly increased witheach slope increment while the speed remained constantHence once the results of these two approaches are com-bined it is clear that the shoulder mechanical and musculareffort increases are key contributors to the adaptation processassociated with the steeper slopes Moreover these resultsare in line with the perceived UL efforts expressed by theparticipants and may explain in part The decreasing successrate with a steeper slope as shoulder strength generatingcapability most likely becomes a determinant for propellingon steeper slopes
43 Implications for Clinical Practice With the use of a slopeor of a combination of slopes when a MWC user propelshimselfherself on a motorized treadmill therapists may beable to offer task-specific high-intensity short duration inter-val training programs to increase UL strength particularlyat the shoulders Cautiousness is advised with this practicesince the risk exposure (ie increased shoulder mechanicaland muscular demands) will progressively and significantlyincrease as the slope becomes steeper and will vary accordingto the strength-generating capability of each MWC user Inaddition since the risk exposure could trigger the develop-ment or exacerbation of secondary impairments at the ULparticularly at the shoulders such a program should alsobe accompanied by proper warm-up and cool-down periodsas well as by antagonist muscle strengthening to preventmuscle strength imbalance Alternatively therapists may alsooffer task-specific cardiorespiratory fitness training programswhen a MWC user propels on a motorized treadmill withno slope or minimal slope (lt27∘) with minimal demandsduring a prolonged period of time (ie cardiorespiratoryfitness training)
44 Limits of the Study The present study included a rela-tively small sample size (119899 = 18) of experienced MWC userswho have completed their rehabilitation process which maylimit the strength of the evidence and potential to generalizethe results with new MWCs respectively The fact that theparticipants used their personal wheelchairs during the studywarrants consideration as optimal wheelchair positioningand configuration parameters most likely differs across par-ticipants and impacts the outcome measures of interest inthe present study and the risk of the MWC tilting or fallingbackwards when propelling up a slope The use of the instru-mented wheels which slightly increase the width and weight
14 BioMed Research International
of the wheelchair along with rolling resistance may havemodified participantsrsquo propulsion technique (eg increasedshoulder abduction) and fatigue level (eg increased ULeffort) in comparison to propelling with their own wheelsThe self-selected natural treadmill speed determined for eachparticipant maintained across all slopes tested in an effort toisolate the effect of speed also requires consideration sinceMWCusers tend to reduce their speedwhen propelling uphillin daily life particularly on steep slopes [2] Finally thekinematic and kinetic and electromyographic variables solelyfocused on the trunk and nondominant shoulder prevent afull understanding of UL adaptations (ie elbow and wristnot studied) during motorized treadmill MWC propulsionacross different slopes
5 Conclusion
This study confirms that MWC users with a SCI increaseforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increase during simulated uphillMWC propulsion on a motorized treadmill Few similaritieswere found between the 27∘ to 36∘ and the 36∘ to 48∘ slopeincrements for shoulder flexion and adduction momentsFuture studies incorporating interactions with various slopesand velocities could strengthen the results of the presentstudy and provide additional evidence-based knowledge onwheelchair propulsion on a motorized treadmill
Abbreviations
AIS American Spinal Injury AssociationImpairment Scale
EMG ElectromyographyER External rotationLED Light-emitting diodeIMW Indicator of muscle workIR Internal rotationJCS Joint coordinate systemMUR Muscle utilization ratioMVC Maximum voluntary contractionMWC Manual wheelchairUL Upper limbWUSPI Wheelchair Userrsquos Shoulder Pain
Index
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors would like to thank Michel Goyette (Eng)Daniel Marineau (Technician) Youssef El Khamlichi(Research Associate) and Philippe Gourdou (ResearchAssociate) for their contributions to this project DanyGagnon holds a Junior 1 Research Career Award from
the Fonds de la recherche du Quebec-Sante (FRQ-S)Annie-Claude Babineau and Guillaume Desroches aresupported by a summer internship and a post-doctoralfellowship from the Canadian Institutes of Health Researchrespectively DanyGagnon andRachid Aissaoui aremembersof the Multidisciplinary SensoriMotor RehabilitationResearch Team (httpwwwerrsmca) supported bythe CIHR and the Quebec-Ontario Spinal Cord InjuryMobility (SCI-MOB) Research Group funded by theQuebec Rehabilitation Research Network (REPARhttpwwwreparca) and the Ontario NeuroTraumaFoundation (ONF httpwwwonforg) The project wasfunded in part by the Fonds de la recherche du Quebec-Sante(FRQS) The equipment and material required for theresearch completed at the Pathokinesiology Laboratory wasfinanced by the Canada Foundation for Innovation (CFI)
References
[1] B Mason J Lenton C Leicht and V Goosey-Tolfrey ldquoAphysiological and biomechanical comparison of over-groundtreadmill and ergometer wheelchair propulsionrdquo Journal ofSports Sciences vol 32 no 1 pp 78ndash91 2014
[2] W M Richter R Rodriguez K R Woods and P W AxelsonldquoStroke pattern and handrim biomechanics for level and uphillwheelchair propulsion at self-selected speedsrdquo Archives of Phys-ical Medicine and Rehabilitation vol 88 no 1 pp 81ndash87 2007
[3] Y-S Yang A M Koontz S-J Yeh and J-J Chang ldquoEffectof backrest height on wheelchair propulsion biomechanics forlevel and uphill conditionsrdquo Archives of Physical Medicine andRehabilitation vol 93 no 4 pp 654ndash659 2012
[4] D H Gagnon A-C Babineau A Champagne G Desrochesand R Aissaoui ldquoPushrim biomechanical changes with pro-gressive increases in slope during motorized treadmill manualwheelchair propulsion in individuals with spinal cord injuryrdquoJournal of Rehabilitation Research amp Development vol 51 no 5pp 789ndash802 2014
[5] J W Chow T A Millikan L G Carlton W-S Chae Y-T Lim and M I Morse ldquoKinematic and electromyographicanalysis of wheelchair propulsion on ramps of different slopesfor young men with Paraplegiardquo Archives of Physical Medicineand Rehabilitation vol 90 no 2 pp 271ndash278 2009
[6] S van Drongelen L H van Der Woude T W Janssen E LAngenot E K Chadwick and D H Veeger ldquoMechanical loadon the upper extremity during wheelchair activitiesrdquo Archivesof Physical Medicine and Rehabilitation vol 86 no 6 pp 1214ndash1220 2005
[7] H Arabi R Aissaoui J Rousseau D Bourbonnais and JDansereau ldquoEvaluation of minimal mechanical effort duringthe ramp access of manual wheelchairrdquo Ergonomia vol 26 no3 pp 253ndash259 2004
[8] K Kulig S S Rao S J Mulroy et al ldquoShoulder joint kineticsduring the push phase of wheelchair propulsionrdquo ClinicalOrthopaedics and Related Research no 354 pp 132ndash143 1998
[9] L J Chapman and J P Chapman ldquoThe measurement ofhandednessrdquoBrain andCognition vol 6 no 2 pp 175ndash183 1987
[10] Gouvernement du Quebec Regie du Batiment du Quebec(RBQ) Construction Code Building Act Chapter 1 Architec-tural and Transportation Barriers Compliance Board 2013
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
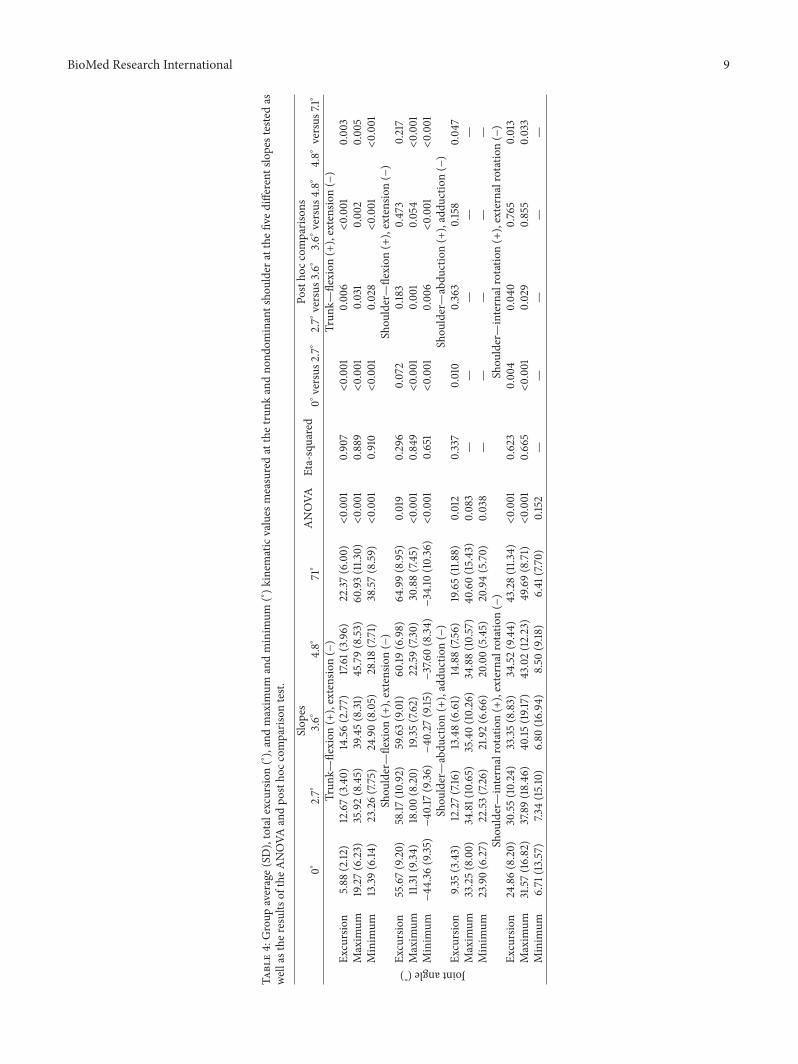
BioMed Research International 9
Table4Group
average(SD)totalexcursio
n(∘ )
and
maxim
umandminim
um(∘ )
kinematicvalues
measuredatthetrun
kandno
ndom
inantsho
uldera
tthe
fivedifferent
slopestestedas
wellasthe
results
oftheA
NOVA
andpo
stho
ccom
paris
ontest
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Jointangle(∘
)
Trun
kmdashflexion
(+)extension(minus)
Trun
kmdashflexion
(+)extension(minus)
Excursion
588
(212
)1267(340)
1456(277)
1761
(396)
2237
(600)lt0001
0907
lt0001
000
6lt0001
0003
Maxim
um1927(623)
3592(845)
3945(831
)4579(853
)6093(113
0)lt0001
0889
lt0001
0031
0002
0005
Minim
um1339
(614
)2326(775)
2490(805)
2818
(771)
3857(859)lt0001
0910
lt0001
0028
lt0001
lt0001
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Excursion
5567(920)
5817
(1092)
5963(901)
6019
(698)
6499(895)
0019
0296
0072
0183
0473
0217
Maxim
um1131
(934)
1800(820)
1935
(762)
2259(730)
3088(745)lt0001
0849
lt0001
0001
0054
lt0001
Minim
umminus44
36(935
)minus40
17(936)minus40
27(915
)minus3760(834)minus3410
(1036)lt0001
0651
lt0001
000
6lt0001
lt0001
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Excursion
935(343)
1227(716)
1348(661)
1488(756)
1965(118
8)0012
0337
0010
0363
0158
0047
Maxim
um3325(800)
3481(1065)
3540(1026)
3488(1057)
4060(1543)
0083
mdashmdash
mdashmdash
mdashMinim
um2390(627)
2253
(726)
2192(666)
2000(545)
2094(570)
0038
mdashmdash
mdashmdash
mdashShou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Excursion
2486(820)
3055(1024)
3335(883)
3452
(944)
4328(113
4)lt0001
0623
000
4004
00765
0013
Maxim
um3157(1682)
3789(1846
)40
15(19
17)
4302(1223)
4969(871)lt0001
0665
lt0001
0029
0855
0033
Minim
um671
(1357)
734(1510)
680
(1694)
850
(918
)641
(770)
0152
mdashmdash
mdashmdash
mdash
10 BioMed Research International
Table5Group
average(
SD)m
eanandpeak
weight-n
ormalise
dmom
ents(N
mkg)
measuredatthen
ondo
minantsho
uldera
tthe
fived
ifferentslopesa
swellasresultsof
theA
NOVA
and
postho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Normalisedmoments(Nmkg)
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Mean
0140(0056)
0226(0067)
0248(0081)
0233(0083)
0242(015
1)0027
0288
lt0001
0003
0433
0966
Peak
(maxim
um)
0292(010
9)0512(015
2)0546(016
7)0559(012
8)0733(0302)lt0001
0588
lt0001
000
40867
0049
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashaddu
ction(+)abdu
ction(minus)
Mean
minus0016(0023)minus006
0(0050)minus0069(0046
)minus0090(0043)minus0103(0036)lt0001
0623
lt0001
0414
0147
0366
Peak
(minim
um)minus0088(0041)minus0257(010
5)minus0278(010
4)minus0369(013
7)minus0494(013
3)lt0001
0797
lt0001
0149
0002
0002
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Mean
0097(0036)
0189(0050)
0222(0064
)0252(0065)
0344(010
1)lt0001
0726
lt0001
000
40191
0010
Peak
(maxim
um)
0196(0078)
0415(014
4)0456(012
9)0530(014
8)0780(018
4)lt0001
0801
lt0001
0001
0103
0001
BioMed Research International 11
00
02
04
06
08
10
Ant
erio
r delt
oid
(a)
00
02
04
06
08
10
(b)
00
02
04
06
08
10
(c)
00
02
04
06
08
10
12
Poste
rior d
eltoi
d
(d)
00
02
04
06
08
10
12
(e)
00
02
04
06
08
10
12
(f)
00
02
04
06
08
10
Clav
icul
ar h
ead
of p
ecto
ralis
maj
or
(g)
00
02
04
06
08
10
(h)
00
02
04
06
08
10
(i)
00
02
04
06
08
10
12
14
16
0 20 40 60 80 100
Ster
nal h
ead
of p
ecto
ralis
maj
or
Normalised time (100)Mean MUR pattern (1)
0∘
27∘
36∘
48∘
71∘
(j)
00
02
04
06
08
10
12
14
16
Mean MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(k)
00
02
04
06
08
10
12
14
16
Peak MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(l)
Figure 3 Group averaged time-normalized mean profile (solid line) and standard deviation (dotted line) (a d g and j) as well as group-average (SD) mean (b e h and k) and peak (c f i and l) muscle utilization ratio (MUR) during the push phase for the five slopes tested atself-selected natural speed
12 BioMed Research International
Table6Group
average(
1SD)meanmuscle
utilisatio
nratio
(MUR)peakMUR(1)and
indicatoro
fmuscle
work(IMW)v
aluesfor
each
muscle
assessed
atthen
ondo
minantsho
uldera
tfived
ifferentslope
angles
aswellasresultsof
theA
NOVA
andpo
stho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Anteriord
eltoid
Anteriord
eltoid
MeanMUR(1)
007
(004)
021
(009)
023
(012
)026
(010
)034
(013
)lt0001
0831
lt0001
0002
lt0001
0001
Peak
MUR(1)
014
(008)
044
(023)
048
(026)
054
(026)
068
(028)lt0001
0836
lt0001
0002
lt0001
lt0001
IMW
718(398)
2070(943)
2348(1237)
2606(1043)
3448(1304)lt0001
0829
lt0001
0003
lt0001
0002
Poste
riord
eltoid
Poste
riord
eltoid
MeanMUR(1)
008
(007)
020
(014
)024
(024)
023
(010
)027
(006)lt0001
0907
lt0001
0144
lt0001
lt0001
Peak
MUR(1)
020
(014
)052
(031
)062
(051)
060
(019
)077
(019
)lt0001
0894
lt0001
0027
0001
0005
IMW
795(692)
2036(1384)
2443(2381)
2335
(1047)
2734(648)lt0001
0906
lt0001
0143
lt0001
lt0001
Clavicular
fiberso
fpectoralis
major
Clavicular
fiberso
fpectoralis
major
MeanMUR(1)
007
(004)
018
(010
)020
(010
)027
(014
)035
(018
)lt0001
0754
lt0001
0003
lt0001
0005
Peak
MUR(1)
014
(009)
038
(022)
042
(023)
057
(031
)071
(029)lt0001
0814
lt0001
000
9lt0001
0001
IMW
700(426)
1837
(977)
2041(1046)
2704(14
32)
3528(175
7)lt0001
0752
lt0001
0003
lt0001
0005
Sternalfi
bersof
pectoralismajor
Sternalfi
bersof
pectoralismajor
MeanMUR(1)
012
(008)
030
(015
)032
(013
)037
(015
)053
(024)lt0001
0781
lt0001
0005
0001
000
6Peak
MUR(1)
021
(015
)054
(023)
059
(023)
071
(026)
101(042)lt0001
0829
lt0001
0003
lt0001
0002
IMW
1194(753)
3023(14
77)
3227(1323)
3753
(1511)
5280(2406)lt0001
0780
lt0001
0005
0001
000
6
BioMed Research International 13
0
10
20
30
40
50
60
70
80
Ant
erio
r delt
oid
Poste
rior d
eltoi
d
Clav
icul
ar h
ead
ofpe
ctor
alis
maj
or
Ster
nal h
ead
of
pect
oral
is m
ajor
IMW
0∘
27∘
36∘
48∘
71∘
Figure 4 Group averaged (SD) mean indicator of muscle work(IMW) during the push phase for the five slopes tested at self-selected natural speed
At the shoulder the maximum shoulder flexion move-ment amplitude significantly increased as the slope becamesteeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments It is possible that increasedmaximumshoulder flexionwas needed to accommodate for the increased forward trunkflexion and to apply most of the force tangentially on thehandrim to preserve mechanical efficiencyThe fact that onlythe duration of the recovery period drastically decreasedas the slope became steeper can also explain in part therelatively stable shoulder flexion-extension excursion (iesimilar push phase durations across slopes) This finding isconsistent to some extent with the work of Yang et al [3]who found comparable values of movement-related adap-tation at the shoulder when comparing level overgroundand uphill (ie 3∘ slope) MWC propulsions However theshoulder flexion-extension excursion significantly increasedon average by 937∘ and the shoulder extension remainedsimilar in their study contrary to the results of the presentstudy These discrepancies may be attributed to the fact thatparticipants used test wheelchairs that were not anchoredto a safety system when propelling up a 3∘ slope at 09mson a motorized treadmill the level surface propulsion (0∘slope) was performed overground and the shoulder kine-matic calculation differed from the work by Yang et al [3]Nevertheless all these results confirmed kinematic adapta-tions at the shoulder as the slope progressed Lastly theincreased forward trunk flexion coupled with an increasedshoulder flexion that modifies the orientation of the forcegenerated at the shoulder may increase posterior shoulderjoint forces and explain the elevated muscular demand at theposterior deltoid occurring towards the end of the push phase[22]
42 Shoulder Joint Mechanical and Muscular Effort Adap-tations The shoulder joint moments adaptations partiallysupport the hypothesis that their outcome measures wouldgradually and significantly increase with each slope incre-ment while the speed remained constant For two out of thethree shoulder net joint moments investigated most of themean and peak values for the shoulder flexor and internalrotator moments progressively increased as the slope becamesteeper aside from some outcomemeasures during the 27∘ to36∘ or the 36∘ to 48∘ slope increment The relative musculardemand adaptations and muscular work computed for allmuscles investigated fully support this hypothesis since theiroutcomemeasures gradually and significantly increased witheach slope increment while the speed remained constantHence once the results of these two approaches are com-bined it is clear that the shoulder mechanical and musculareffort increases are key contributors to the adaptation processassociated with the steeper slopes Moreover these resultsare in line with the perceived UL efforts expressed by theparticipants and may explain in part The decreasing successrate with a steeper slope as shoulder strength generatingcapability most likely becomes a determinant for propellingon steeper slopes
43 Implications for Clinical Practice With the use of a slopeor of a combination of slopes when a MWC user propelshimselfherself on a motorized treadmill therapists may beable to offer task-specific high-intensity short duration inter-val training programs to increase UL strength particularlyat the shoulders Cautiousness is advised with this practicesince the risk exposure (ie increased shoulder mechanicaland muscular demands) will progressively and significantlyincrease as the slope becomes steeper and will vary accordingto the strength-generating capability of each MWC user Inaddition since the risk exposure could trigger the develop-ment or exacerbation of secondary impairments at the ULparticularly at the shoulders such a program should alsobe accompanied by proper warm-up and cool-down periodsas well as by antagonist muscle strengthening to preventmuscle strength imbalance Alternatively therapists may alsooffer task-specific cardiorespiratory fitness training programswhen a MWC user propels on a motorized treadmill withno slope or minimal slope (lt27∘) with minimal demandsduring a prolonged period of time (ie cardiorespiratoryfitness training)
44 Limits of the Study The present study included a rela-tively small sample size (119899 = 18) of experienced MWC userswho have completed their rehabilitation process which maylimit the strength of the evidence and potential to generalizethe results with new MWCs respectively The fact that theparticipants used their personal wheelchairs during the studywarrants consideration as optimal wheelchair positioningand configuration parameters most likely differs across par-ticipants and impacts the outcome measures of interest inthe present study and the risk of the MWC tilting or fallingbackwards when propelling up a slope The use of the instru-mented wheels which slightly increase the width and weight
14 BioMed Research International
of the wheelchair along with rolling resistance may havemodified participantsrsquo propulsion technique (eg increasedshoulder abduction) and fatigue level (eg increased ULeffort) in comparison to propelling with their own wheelsThe self-selected natural treadmill speed determined for eachparticipant maintained across all slopes tested in an effort toisolate the effect of speed also requires consideration sinceMWCusers tend to reduce their speedwhen propelling uphillin daily life particularly on steep slopes [2] Finally thekinematic and kinetic and electromyographic variables solelyfocused on the trunk and nondominant shoulder prevent afull understanding of UL adaptations (ie elbow and wristnot studied) during motorized treadmill MWC propulsionacross different slopes
5 Conclusion
This study confirms that MWC users with a SCI increaseforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increase during simulated uphillMWC propulsion on a motorized treadmill Few similaritieswere found between the 27∘ to 36∘ and the 36∘ to 48∘ slopeincrements for shoulder flexion and adduction momentsFuture studies incorporating interactions with various slopesand velocities could strengthen the results of the presentstudy and provide additional evidence-based knowledge onwheelchair propulsion on a motorized treadmill
Abbreviations
AIS American Spinal Injury AssociationImpairment Scale
EMG ElectromyographyER External rotationLED Light-emitting diodeIMW Indicator of muscle workIR Internal rotationJCS Joint coordinate systemMUR Muscle utilization ratioMVC Maximum voluntary contractionMWC Manual wheelchairUL Upper limbWUSPI Wheelchair Userrsquos Shoulder Pain
Index
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors would like to thank Michel Goyette (Eng)Daniel Marineau (Technician) Youssef El Khamlichi(Research Associate) and Philippe Gourdou (ResearchAssociate) for their contributions to this project DanyGagnon holds a Junior 1 Research Career Award from
the Fonds de la recherche du Quebec-Sante (FRQ-S)Annie-Claude Babineau and Guillaume Desroches aresupported by a summer internship and a post-doctoralfellowship from the Canadian Institutes of Health Researchrespectively DanyGagnon andRachid Aissaoui aremembersof the Multidisciplinary SensoriMotor RehabilitationResearch Team (httpwwwerrsmca) supported bythe CIHR and the Quebec-Ontario Spinal Cord InjuryMobility (SCI-MOB) Research Group funded by theQuebec Rehabilitation Research Network (REPARhttpwwwreparca) and the Ontario NeuroTraumaFoundation (ONF httpwwwonforg) The project wasfunded in part by the Fonds de la recherche du Quebec-Sante(FRQS) The equipment and material required for theresearch completed at the Pathokinesiology Laboratory wasfinanced by the Canada Foundation for Innovation (CFI)
References
[1] B Mason J Lenton C Leicht and V Goosey-Tolfrey ldquoAphysiological and biomechanical comparison of over-groundtreadmill and ergometer wheelchair propulsionrdquo Journal ofSports Sciences vol 32 no 1 pp 78ndash91 2014
[2] W M Richter R Rodriguez K R Woods and P W AxelsonldquoStroke pattern and handrim biomechanics for level and uphillwheelchair propulsion at self-selected speedsrdquo Archives of Phys-ical Medicine and Rehabilitation vol 88 no 1 pp 81ndash87 2007
[3] Y-S Yang A M Koontz S-J Yeh and J-J Chang ldquoEffectof backrest height on wheelchair propulsion biomechanics forlevel and uphill conditionsrdquo Archives of Physical Medicine andRehabilitation vol 93 no 4 pp 654ndash659 2012
[4] D H Gagnon A-C Babineau A Champagne G Desrochesand R Aissaoui ldquoPushrim biomechanical changes with pro-gressive increases in slope during motorized treadmill manualwheelchair propulsion in individuals with spinal cord injuryrdquoJournal of Rehabilitation Research amp Development vol 51 no 5pp 789ndash802 2014
[5] J W Chow T A Millikan L G Carlton W-S Chae Y-T Lim and M I Morse ldquoKinematic and electromyographicanalysis of wheelchair propulsion on ramps of different slopesfor young men with Paraplegiardquo Archives of Physical Medicineand Rehabilitation vol 90 no 2 pp 271ndash278 2009
[6] S van Drongelen L H van Der Woude T W Janssen E LAngenot E K Chadwick and D H Veeger ldquoMechanical loadon the upper extremity during wheelchair activitiesrdquo Archivesof Physical Medicine and Rehabilitation vol 86 no 6 pp 1214ndash1220 2005
[7] H Arabi R Aissaoui J Rousseau D Bourbonnais and JDansereau ldquoEvaluation of minimal mechanical effort duringthe ramp access of manual wheelchairrdquo Ergonomia vol 26 no3 pp 253ndash259 2004
[8] K Kulig S S Rao S J Mulroy et al ldquoShoulder joint kineticsduring the push phase of wheelchair propulsionrdquo ClinicalOrthopaedics and Related Research no 354 pp 132ndash143 1998
[9] L J Chapman and J P Chapman ldquoThe measurement ofhandednessrdquoBrain andCognition vol 6 no 2 pp 175ndash183 1987
[10] Gouvernement du Quebec Regie du Batiment du Quebec(RBQ) Construction Code Building Act Chapter 1 Architec-tural and Transportation Barriers Compliance Board 2013
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

10 BioMed Research International
Table5Group
average(
SD)m
eanandpeak
weight-n
ormalise
dmom
ents(N
mkg)
measuredatthen
ondo
minantsho
uldera
tthe
fived
ifferentslopesa
swellasresultsof
theA
NOVA
and
postho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Normalisedmoments(Nmkg)
Shou
ldermdashflexion
(+)extension(minus)
Shou
ldermdashflexion
(+)extension(minus)
Mean
0140(0056)
0226(0067)
0248(0081)
0233(0083)
0242(015
1)0027
0288
lt0001
0003
0433
0966
Peak
(maxim
um)
0292(010
9)0512(015
2)0546(016
7)0559(012
8)0733(0302)lt0001
0588
lt0001
000
40867
0049
Shou
ldermdashabdu
ction(+)addu
ction(minus)
Shou
ldermdashaddu
ction(+)abdu
ction(minus)
Mean
minus0016(0023)minus006
0(0050)minus0069(0046
)minus0090(0043)minus0103(0036)lt0001
0623
lt0001
0414
0147
0366
Peak
(minim
um)minus0088(0041)minus0257(010
5)minus0278(010
4)minus0369(013
7)minus0494(013
3)lt0001
0797
lt0001
0149
0002
0002
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Shou
ldermdashinternalrotatio
n(+)externalrotatio
n(minus)
Mean
0097(0036)
0189(0050)
0222(0064
)0252(0065)
0344(010
1)lt0001
0726
lt0001
000
40191
0010
Peak
(maxim
um)
0196(0078)
0415(014
4)0456(012
9)0530(014
8)0780(018
4)lt0001
0801
lt0001
0001
0103
0001
BioMed Research International 11
00
02
04
06
08
10
Ant
erio
r delt
oid
(a)
00
02
04
06
08
10
(b)
00
02
04
06
08
10
(c)
00
02
04
06
08
10
12
Poste
rior d
eltoi
d
(d)
00
02
04
06
08
10
12
(e)
00
02
04
06
08
10
12
(f)
00
02
04
06
08
10
Clav
icul
ar h
ead
of p
ecto
ralis
maj
or
(g)
00
02
04
06
08
10
(h)
00
02
04
06
08
10
(i)
00
02
04
06
08
10
12
14
16
0 20 40 60 80 100
Ster
nal h
ead
of p
ecto
ralis
maj
or
Normalised time (100)Mean MUR pattern (1)
0∘
27∘
36∘
48∘
71∘
(j)
00
02
04
06
08
10
12
14
16
Mean MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(k)
00
02
04
06
08
10
12
14
16
Peak MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(l)
Figure 3 Group averaged time-normalized mean profile (solid line) and standard deviation (dotted line) (a d g and j) as well as group-average (SD) mean (b e h and k) and peak (c f i and l) muscle utilization ratio (MUR) during the push phase for the five slopes tested atself-selected natural speed
12 BioMed Research International
Table6Group
average(
1SD)meanmuscle
utilisatio
nratio
(MUR)peakMUR(1)and
indicatoro
fmuscle
work(IMW)v
aluesfor
each
muscle
assessed
atthen
ondo
minantsho
uldera
tfived
ifferentslope
angles
aswellasresultsof
theA
NOVA
andpo
stho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Anteriord
eltoid
Anteriord
eltoid
MeanMUR(1)
007
(004)
021
(009)
023
(012
)026
(010
)034
(013
)lt0001
0831
lt0001
0002
lt0001
0001
Peak
MUR(1)
014
(008)
044
(023)
048
(026)
054
(026)
068
(028)lt0001
0836
lt0001
0002
lt0001
lt0001
IMW
718(398)
2070(943)
2348(1237)
2606(1043)
3448(1304)lt0001
0829
lt0001
0003
lt0001
0002
Poste
riord
eltoid
Poste
riord
eltoid
MeanMUR(1)
008
(007)
020
(014
)024
(024)
023
(010
)027
(006)lt0001
0907
lt0001
0144
lt0001
lt0001
Peak
MUR(1)
020
(014
)052
(031
)062
(051)
060
(019
)077
(019
)lt0001
0894
lt0001
0027
0001
0005
IMW
795(692)
2036(1384)
2443(2381)
2335
(1047)
2734(648)lt0001
0906
lt0001
0143
lt0001
lt0001
Clavicular
fiberso
fpectoralis
major
Clavicular
fiberso
fpectoralis
major
MeanMUR(1)
007
(004)
018
(010
)020
(010
)027
(014
)035
(018
)lt0001
0754
lt0001
0003
lt0001
0005
Peak
MUR(1)
014
(009)
038
(022)
042
(023)
057
(031
)071
(029)lt0001
0814
lt0001
000
9lt0001
0001
IMW
700(426)
1837
(977)
2041(1046)
2704(14
32)
3528(175
7)lt0001
0752
lt0001
0003
lt0001
0005
Sternalfi
bersof
pectoralismajor
Sternalfi
bersof
pectoralismajor
MeanMUR(1)
012
(008)
030
(015
)032
(013
)037
(015
)053
(024)lt0001
0781
lt0001
0005
0001
000
6Peak
MUR(1)
021
(015
)054
(023)
059
(023)
071
(026)
101(042)lt0001
0829
lt0001
0003
lt0001
0002
IMW
1194(753)
3023(14
77)
3227(1323)
3753
(1511)
5280(2406)lt0001
0780
lt0001
0005
0001
000
6
BioMed Research International 13
0
10
20
30
40
50
60
70
80
Ant
erio
r delt
oid
Poste
rior d
eltoi
d
Clav
icul
ar h
ead
ofpe
ctor
alis
maj
or
Ster
nal h
ead
of
pect
oral
is m
ajor
IMW
0∘
27∘
36∘
48∘
71∘
Figure 4 Group averaged (SD) mean indicator of muscle work(IMW) during the push phase for the five slopes tested at self-selected natural speed
At the shoulder the maximum shoulder flexion move-ment amplitude significantly increased as the slope becamesteeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments It is possible that increasedmaximumshoulder flexionwas needed to accommodate for the increased forward trunkflexion and to apply most of the force tangentially on thehandrim to preserve mechanical efficiencyThe fact that onlythe duration of the recovery period drastically decreasedas the slope became steeper can also explain in part therelatively stable shoulder flexion-extension excursion (iesimilar push phase durations across slopes) This finding isconsistent to some extent with the work of Yang et al [3]who found comparable values of movement-related adap-tation at the shoulder when comparing level overgroundand uphill (ie 3∘ slope) MWC propulsions However theshoulder flexion-extension excursion significantly increasedon average by 937∘ and the shoulder extension remainedsimilar in their study contrary to the results of the presentstudy These discrepancies may be attributed to the fact thatparticipants used test wheelchairs that were not anchoredto a safety system when propelling up a 3∘ slope at 09mson a motorized treadmill the level surface propulsion (0∘slope) was performed overground and the shoulder kine-matic calculation differed from the work by Yang et al [3]Nevertheless all these results confirmed kinematic adapta-tions at the shoulder as the slope progressed Lastly theincreased forward trunk flexion coupled with an increasedshoulder flexion that modifies the orientation of the forcegenerated at the shoulder may increase posterior shoulderjoint forces and explain the elevated muscular demand at theposterior deltoid occurring towards the end of the push phase[22]
42 Shoulder Joint Mechanical and Muscular Effort Adap-tations The shoulder joint moments adaptations partiallysupport the hypothesis that their outcome measures wouldgradually and significantly increase with each slope incre-ment while the speed remained constant For two out of thethree shoulder net joint moments investigated most of themean and peak values for the shoulder flexor and internalrotator moments progressively increased as the slope becamesteeper aside from some outcomemeasures during the 27∘ to36∘ or the 36∘ to 48∘ slope increment The relative musculardemand adaptations and muscular work computed for allmuscles investigated fully support this hypothesis since theiroutcomemeasures gradually and significantly increased witheach slope increment while the speed remained constantHence once the results of these two approaches are com-bined it is clear that the shoulder mechanical and musculareffort increases are key contributors to the adaptation processassociated with the steeper slopes Moreover these resultsare in line with the perceived UL efforts expressed by theparticipants and may explain in part The decreasing successrate with a steeper slope as shoulder strength generatingcapability most likely becomes a determinant for propellingon steeper slopes
43 Implications for Clinical Practice With the use of a slopeor of a combination of slopes when a MWC user propelshimselfherself on a motorized treadmill therapists may beable to offer task-specific high-intensity short duration inter-val training programs to increase UL strength particularlyat the shoulders Cautiousness is advised with this practicesince the risk exposure (ie increased shoulder mechanicaland muscular demands) will progressively and significantlyincrease as the slope becomes steeper and will vary accordingto the strength-generating capability of each MWC user Inaddition since the risk exposure could trigger the develop-ment or exacerbation of secondary impairments at the ULparticularly at the shoulders such a program should alsobe accompanied by proper warm-up and cool-down periodsas well as by antagonist muscle strengthening to preventmuscle strength imbalance Alternatively therapists may alsooffer task-specific cardiorespiratory fitness training programswhen a MWC user propels on a motorized treadmill withno slope or minimal slope (lt27∘) with minimal demandsduring a prolonged period of time (ie cardiorespiratoryfitness training)
44 Limits of the Study The present study included a rela-tively small sample size (119899 = 18) of experienced MWC userswho have completed their rehabilitation process which maylimit the strength of the evidence and potential to generalizethe results with new MWCs respectively The fact that theparticipants used their personal wheelchairs during the studywarrants consideration as optimal wheelchair positioningand configuration parameters most likely differs across par-ticipants and impacts the outcome measures of interest inthe present study and the risk of the MWC tilting or fallingbackwards when propelling up a slope The use of the instru-mented wheels which slightly increase the width and weight
14 BioMed Research International
of the wheelchair along with rolling resistance may havemodified participantsrsquo propulsion technique (eg increasedshoulder abduction) and fatigue level (eg increased ULeffort) in comparison to propelling with their own wheelsThe self-selected natural treadmill speed determined for eachparticipant maintained across all slopes tested in an effort toisolate the effect of speed also requires consideration sinceMWCusers tend to reduce their speedwhen propelling uphillin daily life particularly on steep slopes [2] Finally thekinematic and kinetic and electromyographic variables solelyfocused on the trunk and nondominant shoulder prevent afull understanding of UL adaptations (ie elbow and wristnot studied) during motorized treadmill MWC propulsionacross different slopes
5 Conclusion
This study confirms that MWC users with a SCI increaseforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increase during simulated uphillMWC propulsion on a motorized treadmill Few similaritieswere found between the 27∘ to 36∘ and the 36∘ to 48∘ slopeincrements for shoulder flexion and adduction momentsFuture studies incorporating interactions with various slopesand velocities could strengthen the results of the presentstudy and provide additional evidence-based knowledge onwheelchair propulsion on a motorized treadmill
Abbreviations
AIS American Spinal Injury AssociationImpairment Scale
EMG ElectromyographyER External rotationLED Light-emitting diodeIMW Indicator of muscle workIR Internal rotationJCS Joint coordinate systemMUR Muscle utilization ratioMVC Maximum voluntary contractionMWC Manual wheelchairUL Upper limbWUSPI Wheelchair Userrsquos Shoulder Pain
Index
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors would like to thank Michel Goyette (Eng)Daniel Marineau (Technician) Youssef El Khamlichi(Research Associate) and Philippe Gourdou (ResearchAssociate) for their contributions to this project DanyGagnon holds a Junior 1 Research Career Award from
the Fonds de la recherche du Quebec-Sante (FRQ-S)Annie-Claude Babineau and Guillaume Desroches aresupported by a summer internship and a post-doctoralfellowship from the Canadian Institutes of Health Researchrespectively DanyGagnon andRachid Aissaoui aremembersof the Multidisciplinary SensoriMotor RehabilitationResearch Team (httpwwwerrsmca) supported bythe CIHR and the Quebec-Ontario Spinal Cord InjuryMobility (SCI-MOB) Research Group funded by theQuebec Rehabilitation Research Network (REPARhttpwwwreparca) and the Ontario NeuroTraumaFoundation (ONF httpwwwonforg) The project wasfunded in part by the Fonds de la recherche du Quebec-Sante(FRQS) The equipment and material required for theresearch completed at the Pathokinesiology Laboratory wasfinanced by the Canada Foundation for Innovation (CFI)
References
[1] B Mason J Lenton C Leicht and V Goosey-Tolfrey ldquoAphysiological and biomechanical comparison of over-groundtreadmill and ergometer wheelchair propulsionrdquo Journal ofSports Sciences vol 32 no 1 pp 78ndash91 2014
[2] W M Richter R Rodriguez K R Woods and P W AxelsonldquoStroke pattern and handrim biomechanics for level and uphillwheelchair propulsion at self-selected speedsrdquo Archives of Phys-ical Medicine and Rehabilitation vol 88 no 1 pp 81ndash87 2007
[3] Y-S Yang A M Koontz S-J Yeh and J-J Chang ldquoEffectof backrest height on wheelchair propulsion biomechanics forlevel and uphill conditionsrdquo Archives of Physical Medicine andRehabilitation vol 93 no 4 pp 654ndash659 2012
[4] D H Gagnon A-C Babineau A Champagne G Desrochesand R Aissaoui ldquoPushrim biomechanical changes with pro-gressive increases in slope during motorized treadmill manualwheelchair propulsion in individuals with spinal cord injuryrdquoJournal of Rehabilitation Research amp Development vol 51 no 5pp 789ndash802 2014
[5] J W Chow T A Millikan L G Carlton W-S Chae Y-T Lim and M I Morse ldquoKinematic and electromyographicanalysis of wheelchair propulsion on ramps of different slopesfor young men with Paraplegiardquo Archives of Physical Medicineand Rehabilitation vol 90 no 2 pp 271ndash278 2009
[6] S van Drongelen L H van Der Woude T W Janssen E LAngenot E K Chadwick and D H Veeger ldquoMechanical loadon the upper extremity during wheelchair activitiesrdquo Archivesof Physical Medicine and Rehabilitation vol 86 no 6 pp 1214ndash1220 2005
[7] H Arabi R Aissaoui J Rousseau D Bourbonnais and JDansereau ldquoEvaluation of minimal mechanical effort duringthe ramp access of manual wheelchairrdquo Ergonomia vol 26 no3 pp 253ndash259 2004
[8] K Kulig S S Rao S J Mulroy et al ldquoShoulder joint kineticsduring the push phase of wheelchair propulsionrdquo ClinicalOrthopaedics and Related Research no 354 pp 132ndash143 1998
[9] L J Chapman and J P Chapman ldquoThe measurement ofhandednessrdquoBrain andCognition vol 6 no 2 pp 175ndash183 1987
[10] Gouvernement du Quebec Regie du Batiment du Quebec(RBQ) Construction Code Building Act Chapter 1 Architec-tural and Transportation Barriers Compliance Board 2013
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 11
00
02
04
06
08
10
Ant
erio
r delt
oid
(a)
00
02
04
06
08
10
(b)
00
02
04
06
08
10
(c)
00
02
04
06
08
10
12
Poste
rior d
eltoi
d
(d)
00
02
04
06
08
10
12
(e)
00
02
04
06
08
10
12
(f)
00
02
04
06
08
10
Clav
icul
ar h
ead
of p
ecto
ralis
maj
or
(g)
00
02
04
06
08
10
(h)
00
02
04
06
08
10
(i)
00
02
04
06
08
10
12
14
16
0 20 40 60 80 100
Ster
nal h
ead
of p
ecto
ralis
maj
or
Normalised time (100)Mean MUR pattern (1)
0∘
27∘
36∘
48∘
71∘
(j)
00
02
04
06
08
10
12
14
16
Mean MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(k)
00
02
04
06
08
10
12
14
16
Peak MUR (1)0∘27
∘36
∘48
∘71
∘
0∘
27∘
36∘
48∘
71∘
(l)
Figure 3 Group averaged time-normalized mean profile (solid line) and standard deviation (dotted line) (a d g and j) as well as group-average (SD) mean (b e h and k) and peak (c f i and l) muscle utilization ratio (MUR) during the push phase for the five slopes tested atself-selected natural speed
12 BioMed Research International
Table6Group
average(
1SD)meanmuscle
utilisatio
nratio
(MUR)peakMUR(1)and
indicatoro
fmuscle
work(IMW)v
aluesfor
each
muscle
assessed
atthen
ondo
minantsho
uldera
tfived
ifferentslope
angles
aswellasresultsof
theA
NOVA
andpo
stho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Anteriord
eltoid
Anteriord
eltoid
MeanMUR(1)
007
(004)
021
(009)
023
(012
)026
(010
)034
(013
)lt0001
0831
lt0001
0002
lt0001
0001
Peak
MUR(1)
014
(008)
044
(023)
048
(026)
054
(026)
068
(028)lt0001
0836
lt0001
0002
lt0001
lt0001
IMW
718(398)
2070(943)
2348(1237)
2606(1043)
3448(1304)lt0001
0829
lt0001
0003
lt0001
0002
Poste
riord
eltoid
Poste
riord
eltoid
MeanMUR(1)
008
(007)
020
(014
)024
(024)
023
(010
)027
(006)lt0001
0907
lt0001
0144
lt0001
lt0001
Peak
MUR(1)
020
(014
)052
(031
)062
(051)
060
(019
)077
(019
)lt0001
0894
lt0001
0027
0001
0005
IMW
795(692)
2036(1384)
2443(2381)
2335
(1047)
2734(648)lt0001
0906
lt0001
0143
lt0001
lt0001
Clavicular
fiberso
fpectoralis
major
Clavicular
fiberso
fpectoralis
major
MeanMUR(1)
007
(004)
018
(010
)020
(010
)027
(014
)035
(018
)lt0001
0754
lt0001
0003
lt0001
0005
Peak
MUR(1)
014
(009)
038
(022)
042
(023)
057
(031
)071
(029)lt0001
0814
lt0001
000
9lt0001
0001
IMW
700(426)
1837
(977)
2041(1046)
2704(14
32)
3528(175
7)lt0001
0752
lt0001
0003
lt0001
0005
Sternalfi
bersof
pectoralismajor
Sternalfi
bersof
pectoralismajor
MeanMUR(1)
012
(008)
030
(015
)032
(013
)037
(015
)053
(024)lt0001
0781
lt0001
0005
0001
000
6Peak
MUR(1)
021
(015
)054
(023)
059
(023)
071
(026)
101(042)lt0001
0829
lt0001
0003
lt0001
0002
IMW
1194(753)
3023(14
77)
3227(1323)
3753
(1511)
5280(2406)lt0001
0780
lt0001
0005
0001
000
6
BioMed Research International 13
0
10
20
30
40
50
60
70
80
Ant
erio
r delt
oid
Poste
rior d
eltoi
d
Clav
icul
ar h
ead
ofpe
ctor
alis
maj
or
Ster
nal h
ead
of
pect
oral
is m
ajor
IMW
0∘
27∘
36∘
48∘
71∘
Figure 4 Group averaged (SD) mean indicator of muscle work(IMW) during the push phase for the five slopes tested at self-selected natural speed
At the shoulder the maximum shoulder flexion move-ment amplitude significantly increased as the slope becamesteeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments It is possible that increasedmaximumshoulder flexionwas needed to accommodate for the increased forward trunkflexion and to apply most of the force tangentially on thehandrim to preserve mechanical efficiencyThe fact that onlythe duration of the recovery period drastically decreasedas the slope became steeper can also explain in part therelatively stable shoulder flexion-extension excursion (iesimilar push phase durations across slopes) This finding isconsistent to some extent with the work of Yang et al [3]who found comparable values of movement-related adap-tation at the shoulder when comparing level overgroundand uphill (ie 3∘ slope) MWC propulsions However theshoulder flexion-extension excursion significantly increasedon average by 937∘ and the shoulder extension remainedsimilar in their study contrary to the results of the presentstudy These discrepancies may be attributed to the fact thatparticipants used test wheelchairs that were not anchoredto a safety system when propelling up a 3∘ slope at 09mson a motorized treadmill the level surface propulsion (0∘slope) was performed overground and the shoulder kine-matic calculation differed from the work by Yang et al [3]Nevertheless all these results confirmed kinematic adapta-tions at the shoulder as the slope progressed Lastly theincreased forward trunk flexion coupled with an increasedshoulder flexion that modifies the orientation of the forcegenerated at the shoulder may increase posterior shoulderjoint forces and explain the elevated muscular demand at theposterior deltoid occurring towards the end of the push phase[22]
42 Shoulder Joint Mechanical and Muscular Effort Adap-tations The shoulder joint moments adaptations partiallysupport the hypothesis that their outcome measures wouldgradually and significantly increase with each slope incre-ment while the speed remained constant For two out of thethree shoulder net joint moments investigated most of themean and peak values for the shoulder flexor and internalrotator moments progressively increased as the slope becamesteeper aside from some outcomemeasures during the 27∘ to36∘ or the 36∘ to 48∘ slope increment The relative musculardemand adaptations and muscular work computed for allmuscles investigated fully support this hypothesis since theiroutcomemeasures gradually and significantly increased witheach slope increment while the speed remained constantHence once the results of these two approaches are com-bined it is clear that the shoulder mechanical and musculareffort increases are key contributors to the adaptation processassociated with the steeper slopes Moreover these resultsare in line with the perceived UL efforts expressed by theparticipants and may explain in part The decreasing successrate with a steeper slope as shoulder strength generatingcapability most likely becomes a determinant for propellingon steeper slopes
43 Implications for Clinical Practice With the use of a slopeor of a combination of slopes when a MWC user propelshimselfherself on a motorized treadmill therapists may beable to offer task-specific high-intensity short duration inter-val training programs to increase UL strength particularlyat the shoulders Cautiousness is advised with this practicesince the risk exposure (ie increased shoulder mechanicaland muscular demands) will progressively and significantlyincrease as the slope becomes steeper and will vary accordingto the strength-generating capability of each MWC user Inaddition since the risk exposure could trigger the develop-ment or exacerbation of secondary impairments at the ULparticularly at the shoulders such a program should alsobe accompanied by proper warm-up and cool-down periodsas well as by antagonist muscle strengthening to preventmuscle strength imbalance Alternatively therapists may alsooffer task-specific cardiorespiratory fitness training programswhen a MWC user propels on a motorized treadmill withno slope or minimal slope (lt27∘) with minimal demandsduring a prolonged period of time (ie cardiorespiratoryfitness training)
44 Limits of the Study The present study included a rela-tively small sample size (119899 = 18) of experienced MWC userswho have completed their rehabilitation process which maylimit the strength of the evidence and potential to generalizethe results with new MWCs respectively The fact that theparticipants used their personal wheelchairs during the studywarrants consideration as optimal wheelchair positioningand configuration parameters most likely differs across par-ticipants and impacts the outcome measures of interest inthe present study and the risk of the MWC tilting or fallingbackwards when propelling up a slope The use of the instru-mented wheels which slightly increase the width and weight
14 BioMed Research International
of the wheelchair along with rolling resistance may havemodified participantsrsquo propulsion technique (eg increasedshoulder abduction) and fatigue level (eg increased ULeffort) in comparison to propelling with their own wheelsThe self-selected natural treadmill speed determined for eachparticipant maintained across all slopes tested in an effort toisolate the effect of speed also requires consideration sinceMWCusers tend to reduce their speedwhen propelling uphillin daily life particularly on steep slopes [2] Finally thekinematic and kinetic and electromyographic variables solelyfocused on the trunk and nondominant shoulder prevent afull understanding of UL adaptations (ie elbow and wristnot studied) during motorized treadmill MWC propulsionacross different slopes
5 Conclusion
This study confirms that MWC users with a SCI increaseforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increase during simulated uphillMWC propulsion on a motorized treadmill Few similaritieswere found between the 27∘ to 36∘ and the 36∘ to 48∘ slopeincrements for shoulder flexion and adduction momentsFuture studies incorporating interactions with various slopesand velocities could strengthen the results of the presentstudy and provide additional evidence-based knowledge onwheelchair propulsion on a motorized treadmill
Abbreviations
AIS American Spinal Injury AssociationImpairment Scale
EMG ElectromyographyER External rotationLED Light-emitting diodeIMW Indicator of muscle workIR Internal rotationJCS Joint coordinate systemMUR Muscle utilization ratioMVC Maximum voluntary contractionMWC Manual wheelchairUL Upper limbWUSPI Wheelchair Userrsquos Shoulder Pain
Index
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors would like to thank Michel Goyette (Eng)Daniel Marineau (Technician) Youssef El Khamlichi(Research Associate) and Philippe Gourdou (ResearchAssociate) for their contributions to this project DanyGagnon holds a Junior 1 Research Career Award from
the Fonds de la recherche du Quebec-Sante (FRQ-S)Annie-Claude Babineau and Guillaume Desroches aresupported by a summer internship and a post-doctoralfellowship from the Canadian Institutes of Health Researchrespectively DanyGagnon andRachid Aissaoui aremembersof the Multidisciplinary SensoriMotor RehabilitationResearch Team (httpwwwerrsmca) supported bythe CIHR and the Quebec-Ontario Spinal Cord InjuryMobility (SCI-MOB) Research Group funded by theQuebec Rehabilitation Research Network (REPARhttpwwwreparca) and the Ontario NeuroTraumaFoundation (ONF httpwwwonforg) The project wasfunded in part by the Fonds de la recherche du Quebec-Sante(FRQS) The equipment and material required for theresearch completed at the Pathokinesiology Laboratory wasfinanced by the Canada Foundation for Innovation (CFI)
References
[1] B Mason J Lenton C Leicht and V Goosey-Tolfrey ldquoAphysiological and biomechanical comparison of over-groundtreadmill and ergometer wheelchair propulsionrdquo Journal ofSports Sciences vol 32 no 1 pp 78ndash91 2014
[2] W M Richter R Rodriguez K R Woods and P W AxelsonldquoStroke pattern and handrim biomechanics for level and uphillwheelchair propulsion at self-selected speedsrdquo Archives of Phys-ical Medicine and Rehabilitation vol 88 no 1 pp 81ndash87 2007
[3] Y-S Yang A M Koontz S-J Yeh and J-J Chang ldquoEffectof backrest height on wheelchair propulsion biomechanics forlevel and uphill conditionsrdquo Archives of Physical Medicine andRehabilitation vol 93 no 4 pp 654ndash659 2012
[4] D H Gagnon A-C Babineau A Champagne G Desrochesand R Aissaoui ldquoPushrim biomechanical changes with pro-gressive increases in slope during motorized treadmill manualwheelchair propulsion in individuals with spinal cord injuryrdquoJournal of Rehabilitation Research amp Development vol 51 no 5pp 789ndash802 2014
[5] J W Chow T A Millikan L G Carlton W-S Chae Y-T Lim and M I Morse ldquoKinematic and electromyographicanalysis of wheelchair propulsion on ramps of different slopesfor young men with Paraplegiardquo Archives of Physical Medicineand Rehabilitation vol 90 no 2 pp 271ndash278 2009
[6] S van Drongelen L H van Der Woude T W Janssen E LAngenot E K Chadwick and D H Veeger ldquoMechanical loadon the upper extremity during wheelchair activitiesrdquo Archivesof Physical Medicine and Rehabilitation vol 86 no 6 pp 1214ndash1220 2005
[7] H Arabi R Aissaoui J Rousseau D Bourbonnais and JDansereau ldquoEvaluation of minimal mechanical effort duringthe ramp access of manual wheelchairrdquo Ergonomia vol 26 no3 pp 253ndash259 2004
[8] K Kulig S S Rao S J Mulroy et al ldquoShoulder joint kineticsduring the push phase of wheelchair propulsionrdquo ClinicalOrthopaedics and Related Research no 354 pp 132ndash143 1998
[9] L J Chapman and J P Chapman ldquoThe measurement ofhandednessrdquoBrain andCognition vol 6 no 2 pp 175ndash183 1987
[10] Gouvernement du Quebec Regie du Batiment du Quebec(RBQ) Construction Code Building Act Chapter 1 Architec-tural and Transportation Barriers Compliance Board 2013
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

12 BioMed Research International
Table6Group
average(
1SD)meanmuscle
utilisatio
nratio
(MUR)peakMUR(1)and
indicatoro
fmuscle
work(IMW)v
aluesfor
each
muscle
assessed
atthen
ondo
minantsho
uldera
tfived
ifferentslope
angles
aswellasresultsof
theA
NOVA
andpo
stho
ccom
paris
ontests
Slop
esANOVA
Eta-squared
Postho
ccom
paris
ons
0∘27∘
36∘
48∘
71∘
0∘versus
27∘
27∘
versus
36∘
36∘
versus
48∘
48∘
versus
71∘
Anteriord
eltoid
Anteriord
eltoid
MeanMUR(1)
007
(004)
021
(009)
023
(012
)026
(010
)034
(013
)lt0001
0831
lt0001
0002
lt0001
0001
Peak
MUR(1)
014
(008)
044
(023)
048
(026)
054
(026)
068
(028)lt0001
0836
lt0001
0002
lt0001
lt0001
IMW
718(398)
2070(943)
2348(1237)
2606(1043)
3448(1304)lt0001
0829
lt0001
0003
lt0001
0002
Poste
riord
eltoid
Poste
riord
eltoid
MeanMUR(1)
008
(007)
020
(014
)024
(024)
023
(010
)027
(006)lt0001
0907
lt0001
0144
lt0001
lt0001
Peak
MUR(1)
020
(014
)052
(031
)062
(051)
060
(019
)077
(019
)lt0001
0894
lt0001
0027
0001
0005
IMW
795(692)
2036(1384)
2443(2381)
2335
(1047)
2734(648)lt0001
0906
lt0001
0143
lt0001
lt0001
Clavicular
fiberso
fpectoralis
major
Clavicular
fiberso
fpectoralis
major
MeanMUR(1)
007
(004)
018
(010
)020
(010
)027
(014
)035
(018
)lt0001
0754
lt0001
0003
lt0001
0005
Peak
MUR(1)
014
(009)
038
(022)
042
(023)
057
(031
)071
(029)lt0001
0814
lt0001
000
9lt0001
0001
IMW
700(426)
1837
(977)
2041(1046)
2704(14
32)
3528(175
7)lt0001
0752
lt0001
0003
lt0001
0005
Sternalfi
bersof
pectoralismajor
Sternalfi
bersof
pectoralismajor
MeanMUR(1)
012
(008)
030
(015
)032
(013
)037
(015
)053
(024)lt0001
0781
lt0001
0005
0001
000
6Peak
MUR(1)
021
(015
)054
(023)
059
(023)
071
(026)
101(042)lt0001
0829
lt0001
0003
lt0001
0002
IMW
1194(753)
3023(14
77)
3227(1323)
3753
(1511)
5280(2406)lt0001
0780
lt0001
0005
0001
000
6
BioMed Research International 13
0
10
20
30
40
50
60
70
80
Ant
erio
r delt
oid
Poste
rior d
eltoi
d
Clav
icul
ar h
ead
ofpe
ctor
alis
maj
or
Ster
nal h
ead
of
pect
oral
is m
ajor
IMW
0∘
27∘
36∘
48∘
71∘
Figure 4 Group averaged (SD) mean indicator of muscle work(IMW) during the push phase for the five slopes tested at self-selected natural speed
At the shoulder the maximum shoulder flexion move-ment amplitude significantly increased as the slope becamesteeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments It is possible that increasedmaximumshoulder flexionwas needed to accommodate for the increased forward trunkflexion and to apply most of the force tangentially on thehandrim to preserve mechanical efficiencyThe fact that onlythe duration of the recovery period drastically decreasedas the slope became steeper can also explain in part therelatively stable shoulder flexion-extension excursion (iesimilar push phase durations across slopes) This finding isconsistent to some extent with the work of Yang et al [3]who found comparable values of movement-related adap-tation at the shoulder when comparing level overgroundand uphill (ie 3∘ slope) MWC propulsions However theshoulder flexion-extension excursion significantly increasedon average by 937∘ and the shoulder extension remainedsimilar in their study contrary to the results of the presentstudy These discrepancies may be attributed to the fact thatparticipants used test wheelchairs that were not anchoredto a safety system when propelling up a 3∘ slope at 09mson a motorized treadmill the level surface propulsion (0∘slope) was performed overground and the shoulder kine-matic calculation differed from the work by Yang et al [3]Nevertheless all these results confirmed kinematic adapta-tions at the shoulder as the slope progressed Lastly theincreased forward trunk flexion coupled with an increasedshoulder flexion that modifies the orientation of the forcegenerated at the shoulder may increase posterior shoulderjoint forces and explain the elevated muscular demand at theposterior deltoid occurring towards the end of the push phase[22]
42 Shoulder Joint Mechanical and Muscular Effort Adap-tations The shoulder joint moments adaptations partiallysupport the hypothesis that their outcome measures wouldgradually and significantly increase with each slope incre-ment while the speed remained constant For two out of thethree shoulder net joint moments investigated most of themean and peak values for the shoulder flexor and internalrotator moments progressively increased as the slope becamesteeper aside from some outcomemeasures during the 27∘ to36∘ or the 36∘ to 48∘ slope increment The relative musculardemand adaptations and muscular work computed for allmuscles investigated fully support this hypothesis since theiroutcomemeasures gradually and significantly increased witheach slope increment while the speed remained constantHence once the results of these two approaches are com-bined it is clear that the shoulder mechanical and musculareffort increases are key contributors to the adaptation processassociated with the steeper slopes Moreover these resultsare in line with the perceived UL efforts expressed by theparticipants and may explain in part The decreasing successrate with a steeper slope as shoulder strength generatingcapability most likely becomes a determinant for propellingon steeper slopes
43 Implications for Clinical Practice With the use of a slopeor of a combination of slopes when a MWC user propelshimselfherself on a motorized treadmill therapists may beable to offer task-specific high-intensity short duration inter-val training programs to increase UL strength particularlyat the shoulders Cautiousness is advised with this practicesince the risk exposure (ie increased shoulder mechanicaland muscular demands) will progressively and significantlyincrease as the slope becomes steeper and will vary accordingto the strength-generating capability of each MWC user Inaddition since the risk exposure could trigger the develop-ment or exacerbation of secondary impairments at the ULparticularly at the shoulders such a program should alsobe accompanied by proper warm-up and cool-down periodsas well as by antagonist muscle strengthening to preventmuscle strength imbalance Alternatively therapists may alsooffer task-specific cardiorespiratory fitness training programswhen a MWC user propels on a motorized treadmill withno slope or minimal slope (lt27∘) with minimal demandsduring a prolonged period of time (ie cardiorespiratoryfitness training)
44 Limits of the Study The present study included a rela-tively small sample size (119899 = 18) of experienced MWC userswho have completed their rehabilitation process which maylimit the strength of the evidence and potential to generalizethe results with new MWCs respectively The fact that theparticipants used their personal wheelchairs during the studywarrants consideration as optimal wheelchair positioningand configuration parameters most likely differs across par-ticipants and impacts the outcome measures of interest inthe present study and the risk of the MWC tilting or fallingbackwards when propelling up a slope The use of the instru-mented wheels which slightly increase the width and weight
14 BioMed Research International
of the wheelchair along with rolling resistance may havemodified participantsrsquo propulsion technique (eg increasedshoulder abduction) and fatigue level (eg increased ULeffort) in comparison to propelling with their own wheelsThe self-selected natural treadmill speed determined for eachparticipant maintained across all slopes tested in an effort toisolate the effect of speed also requires consideration sinceMWCusers tend to reduce their speedwhen propelling uphillin daily life particularly on steep slopes [2] Finally thekinematic and kinetic and electromyographic variables solelyfocused on the trunk and nondominant shoulder prevent afull understanding of UL adaptations (ie elbow and wristnot studied) during motorized treadmill MWC propulsionacross different slopes
5 Conclusion
This study confirms that MWC users with a SCI increaseforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increase during simulated uphillMWC propulsion on a motorized treadmill Few similaritieswere found between the 27∘ to 36∘ and the 36∘ to 48∘ slopeincrements for shoulder flexion and adduction momentsFuture studies incorporating interactions with various slopesand velocities could strengthen the results of the presentstudy and provide additional evidence-based knowledge onwheelchair propulsion on a motorized treadmill
Abbreviations
AIS American Spinal Injury AssociationImpairment Scale
EMG ElectromyographyER External rotationLED Light-emitting diodeIMW Indicator of muscle workIR Internal rotationJCS Joint coordinate systemMUR Muscle utilization ratioMVC Maximum voluntary contractionMWC Manual wheelchairUL Upper limbWUSPI Wheelchair Userrsquos Shoulder Pain
Index
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors would like to thank Michel Goyette (Eng)Daniel Marineau (Technician) Youssef El Khamlichi(Research Associate) and Philippe Gourdou (ResearchAssociate) for their contributions to this project DanyGagnon holds a Junior 1 Research Career Award from
the Fonds de la recherche du Quebec-Sante (FRQ-S)Annie-Claude Babineau and Guillaume Desroches aresupported by a summer internship and a post-doctoralfellowship from the Canadian Institutes of Health Researchrespectively DanyGagnon andRachid Aissaoui aremembersof the Multidisciplinary SensoriMotor RehabilitationResearch Team (httpwwwerrsmca) supported bythe CIHR and the Quebec-Ontario Spinal Cord InjuryMobility (SCI-MOB) Research Group funded by theQuebec Rehabilitation Research Network (REPARhttpwwwreparca) and the Ontario NeuroTraumaFoundation (ONF httpwwwonforg) The project wasfunded in part by the Fonds de la recherche du Quebec-Sante(FRQS) The equipment and material required for theresearch completed at the Pathokinesiology Laboratory wasfinanced by the Canada Foundation for Innovation (CFI)
References
[1] B Mason J Lenton C Leicht and V Goosey-Tolfrey ldquoAphysiological and biomechanical comparison of over-groundtreadmill and ergometer wheelchair propulsionrdquo Journal ofSports Sciences vol 32 no 1 pp 78ndash91 2014
[2] W M Richter R Rodriguez K R Woods and P W AxelsonldquoStroke pattern and handrim biomechanics for level and uphillwheelchair propulsion at self-selected speedsrdquo Archives of Phys-ical Medicine and Rehabilitation vol 88 no 1 pp 81ndash87 2007
[3] Y-S Yang A M Koontz S-J Yeh and J-J Chang ldquoEffectof backrest height on wheelchair propulsion biomechanics forlevel and uphill conditionsrdquo Archives of Physical Medicine andRehabilitation vol 93 no 4 pp 654ndash659 2012
[4] D H Gagnon A-C Babineau A Champagne G Desrochesand R Aissaoui ldquoPushrim biomechanical changes with pro-gressive increases in slope during motorized treadmill manualwheelchair propulsion in individuals with spinal cord injuryrdquoJournal of Rehabilitation Research amp Development vol 51 no 5pp 789ndash802 2014
[5] J W Chow T A Millikan L G Carlton W-S Chae Y-T Lim and M I Morse ldquoKinematic and electromyographicanalysis of wheelchair propulsion on ramps of different slopesfor young men with Paraplegiardquo Archives of Physical Medicineand Rehabilitation vol 90 no 2 pp 271ndash278 2009
[6] S van Drongelen L H van Der Woude T W Janssen E LAngenot E K Chadwick and D H Veeger ldquoMechanical loadon the upper extremity during wheelchair activitiesrdquo Archivesof Physical Medicine and Rehabilitation vol 86 no 6 pp 1214ndash1220 2005
[7] H Arabi R Aissaoui J Rousseau D Bourbonnais and JDansereau ldquoEvaluation of minimal mechanical effort duringthe ramp access of manual wheelchairrdquo Ergonomia vol 26 no3 pp 253ndash259 2004
[8] K Kulig S S Rao S J Mulroy et al ldquoShoulder joint kineticsduring the push phase of wheelchair propulsionrdquo ClinicalOrthopaedics and Related Research no 354 pp 132ndash143 1998
[9] L J Chapman and J P Chapman ldquoThe measurement ofhandednessrdquoBrain andCognition vol 6 no 2 pp 175ndash183 1987
[10] Gouvernement du Quebec Regie du Batiment du Quebec(RBQ) Construction Code Building Act Chapter 1 Architec-tural and Transportation Barriers Compliance Board 2013
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 13
0
10
20
30
40
50
60
70
80
Ant
erio
r delt
oid
Poste
rior d
eltoi
d
Clav
icul
ar h
ead
ofpe
ctor
alis
maj
or
Ster
nal h
ead
of
pect
oral
is m
ajor
IMW
0∘
27∘
36∘
48∘
71∘
Figure 4 Group averaged (SD) mean indicator of muscle work(IMW) during the push phase for the five slopes tested at self-selected natural speed
At the shoulder the maximum shoulder flexion move-ment amplitude significantly increased as the slope becamesteeper except for the 36∘ to 48∘ slope increment thatremained similar whereas the minimum shoulder flexionmovement amplitude (ie shoulder extension) significantlydecreased during that same period As a result the shoulderflexion excursion remained comparable despite slope incre-ments It is possible that increasedmaximumshoulder flexionwas needed to accommodate for the increased forward trunkflexion and to apply most of the force tangentially on thehandrim to preserve mechanical efficiencyThe fact that onlythe duration of the recovery period drastically decreasedas the slope became steeper can also explain in part therelatively stable shoulder flexion-extension excursion (iesimilar push phase durations across slopes) This finding isconsistent to some extent with the work of Yang et al [3]who found comparable values of movement-related adap-tation at the shoulder when comparing level overgroundand uphill (ie 3∘ slope) MWC propulsions However theshoulder flexion-extension excursion significantly increasedon average by 937∘ and the shoulder extension remainedsimilar in their study contrary to the results of the presentstudy These discrepancies may be attributed to the fact thatparticipants used test wheelchairs that were not anchoredto a safety system when propelling up a 3∘ slope at 09mson a motorized treadmill the level surface propulsion (0∘slope) was performed overground and the shoulder kine-matic calculation differed from the work by Yang et al [3]Nevertheless all these results confirmed kinematic adapta-tions at the shoulder as the slope progressed Lastly theincreased forward trunk flexion coupled with an increasedshoulder flexion that modifies the orientation of the forcegenerated at the shoulder may increase posterior shoulderjoint forces and explain the elevated muscular demand at theposterior deltoid occurring towards the end of the push phase[22]
42 Shoulder Joint Mechanical and Muscular Effort Adap-tations The shoulder joint moments adaptations partiallysupport the hypothesis that their outcome measures wouldgradually and significantly increase with each slope incre-ment while the speed remained constant For two out of thethree shoulder net joint moments investigated most of themean and peak values for the shoulder flexor and internalrotator moments progressively increased as the slope becamesteeper aside from some outcomemeasures during the 27∘ to36∘ or the 36∘ to 48∘ slope increment The relative musculardemand adaptations and muscular work computed for allmuscles investigated fully support this hypothesis since theiroutcomemeasures gradually and significantly increased witheach slope increment while the speed remained constantHence once the results of these two approaches are com-bined it is clear that the shoulder mechanical and musculareffort increases are key contributors to the adaptation processassociated with the steeper slopes Moreover these resultsare in line with the perceived UL efforts expressed by theparticipants and may explain in part The decreasing successrate with a steeper slope as shoulder strength generatingcapability most likely becomes a determinant for propellingon steeper slopes
43 Implications for Clinical Practice With the use of a slopeor of a combination of slopes when a MWC user propelshimselfherself on a motorized treadmill therapists may beable to offer task-specific high-intensity short duration inter-val training programs to increase UL strength particularlyat the shoulders Cautiousness is advised with this practicesince the risk exposure (ie increased shoulder mechanicaland muscular demands) will progressively and significantlyincrease as the slope becomes steeper and will vary accordingto the strength-generating capability of each MWC user Inaddition since the risk exposure could trigger the develop-ment or exacerbation of secondary impairments at the ULparticularly at the shoulders such a program should alsobe accompanied by proper warm-up and cool-down periodsas well as by antagonist muscle strengthening to preventmuscle strength imbalance Alternatively therapists may alsooffer task-specific cardiorespiratory fitness training programswhen a MWC user propels on a motorized treadmill withno slope or minimal slope (lt27∘) with minimal demandsduring a prolonged period of time (ie cardiorespiratoryfitness training)
44 Limits of the Study The present study included a rela-tively small sample size (119899 = 18) of experienced MWC userswho have completed their rehabilitation process which maylimit the strength of the evidence and potential to generalizethe results with new MWCs respectively The fact that theparticipants used their personal wheelchairs during the studywarrants consideration as optimal wheelchair positioningand configuration parameters most likely differs across par-ticipants and impacts the outcome measures of interest inthe present study and the risk of the MWC tilting or fallingbackwards when propelling up a slope The use of the instru-mented wheels which slightly increase the width and weight
14 BioMed Research International
of the wheelchair along with rolling resistance may havemodified participantsrsquo propulsion technique (eg increasedshoulder abduction) and fatigue level (eg increased ULeffort) in comparison to propelling with their own wheelsThe self-selected natural treadmill speed determined for eachparticipant maintained across all slopes tested in an effort toisolate the effect of speed also requires consideration sinceMWCusers tend to reduce their speedwhen propelling uphillin daily life particularly on steep slopes [2] Finally thekinematic and kinetic and electromyographic variables solelyfocused on the trunk and nondominant shoulder prevent afull understanding of UL adaptations (ie elbow and wristnot studied) during motorized treadmill MWC propulsionacross different slopes
5 Conclusion
This study confirms that MWC users with a SCI increaseforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increase during simulated uphillMWC propulsion on a motorized treadmill Few similaritieswere found between the 27∘ to 36∘ and the 36∘ to 48∘ slopeincrements for shoulder flexion and adduction momentsFuture studies incorporating interactions with various slopesand velocities could strengthen the results of the presentstudy and provide additional evidence-based knowledge onwheelchair propulsion on a motorized treadmill
Abbreviations
AIS American Spinal Injury AssociationImpairment Scale
EMG ElectromyographyER External rotationLED Light-emitting diodeIMW Indicator of muscle workIR Internal rotationJCS Joint coordinate systemMUR Muscle utilization ratioMVC Maximum voluntary contractionMWC Manual wheelchairUL Upper limbWUSPI Wheelchair Userrsquos Shoulder Pain
Index
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors would like to thank Michel Goyette (Eng)Daniel Marineau (Technician) Youssef El Khamlichi(Research Associate) and Philippe Gourdou (ResearchAssociate) for their contributions to this project DanyGagnon holds a Junior 1 Research Career Award from
the Fonds de la recherche du Quebec-Sante (FRQ-S)Annie-Claude Babineau and Guillaume Desroches aresupported by a summer internship and a post-doctoralfellowship from the Canadian Institutes of Health Researchrespectively DanyGagnon andRachid Aissaoui aremembersof the Multidisciplinary SensoriMotor RehabilitationResearch Team (httpwwwerrsmca) supported bythe CIHR and the Quebec-Ontario Spinal Cord InjuryMobility (SCI-MOB) Research Group funded by theQuebec Rehabilitation Research Network (REPARhttpwwwreparca) and the Ontario NeuroTraumaFoundation (ONF httpwwwonforg) The project wasfunded in part by the Fonds de la recherche du Quebec-Sante(FRQS) The equipment and material required for theresearch completed at the Pathokinesiology Laboratory wasfinanced by the Canada Foundation for Innovation (CFI)
References
[1] B Mason J Lenton C Leicht and V Goosey-Tolfrey ldquoAphysiological and biomechanical comparison of over-groundtreadmill and ergometer wheelchair propulsionrdquo Journal ofSports Sciences vol 32 no 1 pp 78ndash91 2014
[2] W M Richter R Rodriguez K R Woods and P W AxelsonldquoStroke pattern and handrim biomechanics for level and uphillwheelchair propulsion at self-selected speedsrdquo Archives of Phys-ical Medicine and Rehabilitation vol 88 no 1 pp 81ndash87 2007
[3] Y-S Yang A M Koontz S-J Yeh and J-J Chang ldquoEffectof backrest height on wheelchair propulsion biomechanics forlevel and uphill conditionsrdquo Archives of Physical Medicine andRehabilitation vol 93 no 4 pp 654ndash659 2012
[4] D H Gagnon A-C Babineau A Champagne G Desrochesand R Aissaoui ldquoPushrim biomechanical changes with pro-gressive increases in slope during motorized treadmill manualwheelchair propulsion in individuals with spinal cord injuryrdquoJournal of Rehabilitation Research amp Development vol 51 no 5pp 789ndash802 2014
[5] J W Chow T A Millikan L G Carlton W-S Chae Y-T Lim and M I Morse ldquoKinematic and electromyographicanalysis of wheelchair propulsion on ramps of different slopesfor young men with Paraplegiardquo Archives of Physical Medicineand Rehabilitation vol 90 no 2 pp 271ndash278 2009
[6] S van Drongelen L H van Der Woude T W Janssen E LAngenot E K Chadwick and D H Veeger ldquoMechanical loadon the upper extremity during wheelchair activitiesrdquo Archivesof Physical Medicine and Rehabilitation vol 86 no 6 pp 1214ndash1220 2005
[7] H Arabi R Aissaoui J Rousseau D Bourbonnais and JDansereau ldquoEvaluation of minimal mechanical effort duringthe ramp access of manual wheelchairrdquo Ergonomia vol 26 no3 pp 253ndash259 2004
[8] K Kulig S S Rao S J Mulroy et al ldquoShoulder joint kineticsduring the push phase of wheelchair propulsionrdquo ClinicalOrthopaedics and Related Research no 354 pp 132ndash143 1998
[9] L J Chapman and J P Chapman ldquoThe measurement ofhandednessrdquoBrain andCognition vol 6 no 2 pp 175ndash183 1987
[10] Gouvernement du Quebec Regie du Batiment du Quebec(RBQ) Construction Code Building Act Chapter 1 Architec-tural and Transportation Barriers Compliance Board 2013
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

14 BioMed Research International
of the wheelchair along with rolling resistance may havemodified participantsrsquo propulsion technique (eg increasedshoulder abduction) and fatigue level (eg increased ULeffort) in comparison to propelling with their own wheelsThe self-selected natural treadmill speed determined for eachparticipant maintained across all slopes tested in an effort toisolate the effect of speed also requires consideration sinceMWCusers tend to reduce their speedwhen propelling uphillin daily life particularly on steep slopes [2] Finally thekinematic and kinetic and electromyographic variables solelyfocused on the trunk and nondominant shoulder prevent afull understanding of UL adaptations (ie elbow and wristnot studied) during motorized treadmill MWC propulsionacross different slopes
5 Conclusion
This study confirms that MWC users with a SCI increaseforward trunk flexion and peak shoulder flexion while alsoincreasing shouldermechanical andmuscular efforts to adaptto slopes that progressively increase during simulated uphillMWC propulsion on a motorized treadmill Few similaritieswere found between the 27∘ to 36∘ and the 36∘ to 48∘ slopeincrements for shoulder flexion and adduction momentsFuture studies incorporating interactions with various slopesand velocities could strengthen the results of the presentstudy and provide additional evidence-based knowledge onwheelchair propulsion on a motorized treadmill
Abbreviations
AIS American Spinal Injury AssociationImpairment Scale
EMG ElectromyographyER External rotationLED Light-emitting diodeIMW Indicator of muscle workIR Internal rotationJCS Joint coordinate systemMUR Muscle utilization ratioMVC Maximum voluntary contractionMWC Manual wheelchairUL Upper limbWUSPI Wheelchair Userrsquos Shoulder Pain
Index
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors would like to thank Michel Goyette (Eng)Daniel Marineau (Technician) Youssef El Khamlichi(Research Associate) and Philippe Gourdou (ResearchAssociate) for their contributions to this project DanyGagnon holds a Junior 1 Research Career Award from
the Fonds de la recherche du Quebec-Sante (FRQ-S)Annie-Claude Babineau and Guillaume Desroches aresupported by a summer internship and a post-doctoralfellowship from the Canadian Institutes of Health Researchrespectively DanyGagnon andRachid Aissaoui aremembersof the Multidisciplinary SensoriMotor RehabilitationResearch Team (httpwwwerrsmca) supported bythe CIHR and the Quebec-Ontario Spinal Cord InjuryMobility (SCI-MOB) Research Group funded by theQuebec Rehabilitation Research Network (REPARhttpwwwreparca) and the Ontario NeuroTraumaFoundation (ONF httpwwwonforg) The project wasfunded in part by the Fonds de la recherche du Quebec-Sante(FRQS) The equipment and material required for theresearch completed at the Pathokinesiology Laboratory wasfinanced by the Canada Foundation for Innovation (CFI)
References
[1] B Mason J Lenton C Leicht and V Goosey-Tolfrey ldquoAphysiological and biomechanical comparison of over-groundtreadmill and ergometer wheelchair propulsionrdquo Journal ofSports Sciences vol 32 no 1 pp 78ndash91 2014
[2] W M Richter R Rodriguez K R Woods and P W AxelsonldquoStroke pattern and handrim biomechanics for level and uphillwheelchair propulsion at self-selected speedsrdquo Archives of Phys-ical Medicine and Rehabilitation vol 88 no 1 pp 81ndash87 2007
[3] Y-S Yang A M Koontz S-J Yeh and J-J Chang ldquoEffectof backrest height on wheelchair propulsion biomechanics forlevel and uphill conditionsrdquo Archives of Physical Medicine andRehabilitation vol 93 no 4 pp 654ndash659 2012
[4] D H Gagnon A-C Babineau A Champagne G Desrochesand R Aissaoui ldquoPushrim biomechanical changes with pro-gressive increases in slope during motorized treadmill manualwheelchair propulsion in individuals with spinal cord injuryrdquoJournal of Rehabilitation Research amp Development vol 51 no 5pp 789ndash802 2014
[5] J W Chow T A Millikan L G Carlton W-S Chae Y-T Lim and M I Morse ldquoKinematic and electromyographicanalysis of wheelchair propulsion on ramps of different slopesfor young men with Paraplegiardquo Archives of Physical Medicineand Rehabilitation vol 90 no 2 pp 271ndash278 2009
[6] S van Drongelen L H van Der Woude T W Janssen E LAngenot E K Chadwick and D H Veeger ldquoMechanical loadon the upper extremity during wheelchair activitiesrdquo Archivesof Physical Medicine and Rehabilitation vol 86 no 6 pp 1214ndash1220 2005
[7] H Arabi R Aissaoui J Rousseau D Bourbonnais and JDansereau ldquoEvaluation of minimal mechanical effort duringthe ramp access of manual wheelchairrdquo Ergonomia vol 26 no3 pp 253ndash259 2004
[8] K Kulig S S Rao S J Mulroy et al ldquoShoulder joint kineticsduring the push phase of wheelchair propulsionrdquo ClinicalOrthopaedics and Related Research no 354 pp 132ndash143 1998
[9] L J Chapman and J P Chapman ldquoThe measurement ofhandednessrdquoBrain andCognition vol 6 no 2 pp 175ndash183 1987
[10] Gouvernement du Quebec Regie du Batiment du Quebec(RBQ) Construction Code Building Act Chapter 1 Architec-tural and Transportation Barriers Compliance Board 2013
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
BioMed Research International 15
[11] K A Curtis K E Roach E B Applegate et al ldquoDevelopmentof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 5 pp 290ndash293 1995
[12] K A Curtis K E Roach T Amar et al ldquoReliability and validityof the Wheelchair Userrsquos Shoulder Pain Index (WUSPI)rdquoParaplegia vol 33 no 10 pp 595ndash601 1995
[13] S C Kirshblum S P Burns F Biering-Sorensen et al ldquoInter-national standards for neurological classification of spinal cordinjury (revised 2011)rdquo Journal of Spinal Cord Medicine vol 34no 6 pp 535ndash546 2011
[14] M Lalumiere D H Gagnon J Hassan G Desroches R Zoryand D Pradon ldquoAscending curbs of progressively higher heightincreases forward trunk flexion along with upper extremitymechanical andmuscular demands in manual wheelchair userswith a spinal cord injuryrdquo Journal of Electromyography andKinesiology vol 23 no 6 pp 1434ndash1445 2013
[15] M Stokdijk J Nagels and P M Rozing ldquoThe glenohumeraljoint rotation centre in vivordquo Journal of Biomechanics vol 33no 12 pp 1629ndash1636 2000
[16] H E J Veeger ldquoThe position of the rotation center of theglenohumeral jointrdquo Journal of Biomechanics vol 33 no 12 pp1711ndash1715 2000
[17] G Wu F C T van der Helm H E J Veeger et al ldquoISBrecommendation on definitions of joint coordinate systems ofvarious joints for the reporting of human joint motion Part IIshoulder elbow wrist and handrdquo Journal of Biomechanics vol38 no 5 pp 981ndash992 2005
[18] M Senk and L Cheze ldquoRotation sequence as an importantfactor in shoulder kinematicsrdquoClinical Biomechanics vol 21 no1 pp S3ndashS8 2006
[19] R A Cooper ldquoSmartWheel from concept to clinical practicerdquoProsthetics and Orthotics International vol 33 no 3 pp 198ndash209 2009
[20] R Dumas R Aissaoui and J A de Guise ldquoA 3D genericinverse dynamicmethod usingwrench notation and quaternionalgebrardquo Computer Methods in Biomechanics and BiomedicalEngineering vol 7 no 3 pp 159ndash166 2004
[21] W J Hurd M M Morrow K R Kaufman and K-N AnldquoBiomechanic evaluation of upper-extremity symmetry duringmanual wheelchair propulsion over varied terrainrdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 10 pp 1996ndash2002 2008
[22] S J Mulroy J K Gronley C J Newsam and J Perry ldquoElec-tromyographic activity of shoulder muscles during wheelchairpropulsion by paraplegic personsrdquoArchives of PhysicalMedicineand Rehabilitation vol 77 no 2 pp 187ndash193 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom










![Motion Capture BIOMECHANICS. T – trunk, El – elbow, SH – shoulder, Fl – flexion EX extention MUSCLE GROUP X [Nm]WojtekLuciaLi-TingSamuelAndrew FL T M](https://img.dokumen.tips/doc/110x75/56649cbf5503460f949854eb/motion-capture-biomechanics-t-trunk-el-elbow-sh-shoulder-fl.jpg)


















