Embed Size (px)
Citation preview

Research ArticleGenetic Algorithm in Data Mining of Colorectal Images
Shou-Ming Chen 1 and Jun-Hui Zhang 2
1Department of Radiology, The Affiliated Hospital of Panzhihua University, Panzhihua, Sichuan 617000, China2Department of Medical Imaging, Baoji People’s Hospital, Baoji, Shaanxi 721000, China
Correspondence should be addressed to Jun-Hui Zhang; [email protected]
Received 29 August 2021; Accepted 25 September 2021; Published 15 October 2021
Academic Editor: Osamah Ibrahim Khalaf
Copyright © 2021 Shou-Ming Chen and Jun-Hui Zhang. This is an open access article distributed under the Creative CommonsAttribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work isproperly cited.
There is currently no effective analytical method in colorectal image analysis, which leads to certain errors in colorectal imageanalysis. In order to improve the accuracy of colorectal imaging detection, this study used a genetic algorithm as the datamining algorithm and combined it with image processing technology to perform image analysis. At the same time, combinedwith the actual requirements of image detection, the gray theory model is used as the basic theory of image processing, and theimage detection prediction model is constructed to predict the data. In addition, in order to study the effectiveness of thealgorithm, the experiment is carried out to analyze the validity of the data of the study, and the predicted value is comparedwith the actual value. The research shows that the proposed algorithm has certain accuracy and can provide theoreticalreference for subsequent related research.
1. Introduction
Colorectal cancer is one of the most common malignanttumors in the digestive tract. The 2012 Global Cancer Reportof the WHO/IARC (World Health Organization Interna-tional Center for Cancer Research) shows that colorectalcancer is the third most common malignant tumor in theworld and ranks fourth in the cause of malignant tumordeath and accounts for about 10% of all cancers. In the sameyear, there will be an estimated 1.36 million new cases ofcolorectal cancer, and about 694,000 patients died of the dis-ease [1]. Although the incidence of colorectal cancer isdeclining in some developed countries [1], theWorld CancerReport [2] and China’s epidemiological studies [3] show thatwith the aging of China’s population, environmental pollu-tion, and changes in living habits, the incidence of colorectalcancer in China is on the rise and there is a trend of rejuve-nation. Based on this need, effective monitoring methods areused to improve the effect of colorectal imaging analysis.
Rectal cancer patients account for about 60% of all colo-rectal cancers in China. With the continuous improvementof surgical methods, the emergence of new treatmentmethods, and the constant regulation of clinical treatment
programs, the recurrence rate of rectal cancer is significantlyreduced [4]. However, due to the large base of rectal cancerpatients, it is still necessary to further reduce the patient’srecurrence rate, improve the prognosis, and improve thesurvival rate. Accurate preoperative staging of rectal canceris the main basis for guiding the clinical selection of the besttreatment plan (including whether preoperative radiother-apy and chemotherapy, the way of surgery, and the degreeof radical cure) and evaluating the prognosis [5]. Inaccuratepreoperative staging, whether it is insufficient staging orexcessive staging, will have a significant impact on the prog-nosis of patients.
The American Cancer Association (AJCC) revised thelatest TNM staging for rectal cancer in 2010 [6] (determin-ing the T stage according to the depth of intestinal wall infil-tration of the primary tumor, the number and distributionof lymph node metastasis to determine the N stage, andwhether there is a distant metastasis to determine the Mstage), which provides a reliable theoretical basis for preop-erative staging of rectal cancer. However, accurate preopera-tive staging of rectal cancer is still a hot and difficult point inclinical and imaging studies. At present, preoperative T andM staging of rectal cancer can be accurately judged by CT,
HindawiComputational and Mathematical Methods in MedicineVolume 2021, Article ID 3854518, 8 pageshttps://doi.org/10.1155/2021/3854518

intrarectal ultrasound, MRI, PET, etc. However, there aremany reasons for causing lymphadenopathy around therectum. Therefore, routine examination based on morpho-logical changes is difficult to make accurate judgments onwhether it is benign and malignant, and the accurateevaluation of regional lymph node properties is the biggestchallenge for preoperative staging of rectal cancer [7].Therefore, it is of great significance to study and explorethe methods and techniques for accurately determining thenature of rectal cancer regional lymph nodes before surgeryto guide the clinical diagnosis and treatment of rectal cancer.There are limited methods of preoperative examination forrectal cancer. Rectal examination is simple and easy and isthe most important method for the diagnosis of rectal can-cer. It is also the primary examination and diagnosis stepfor rectal cancer. Therefore, 40%-80% of rectal cancer canbe touched during digital rectal examination [8].
Digital rectal examination can provide a preliminaryunderstanding of rectal cancer and its surroundings. How-ever, most of the lymph node metastases of rectal cancerhave been in the advanced stage of the disease, and it isimpossible to examine rectal cancer with a higher position.Therefore, the clinical examination has limited value in eval-uating the regional lymph nodes of rectal cancer. The resultsof the study of Hardy et al. [9] show that the accuracy oflymph node metastasis by experienced doctors is only 67%.At the same time, the use of digital rectal examination resultsis not reliable, and it has a great correlation with the experi-ence of the examiner, so it is not used to evaluate regionallymph nodes of rectal cancer. Colonoscopy has been widelyused in clinical practice and is the most effective method forthe diagnosis of rectal cancer. Moreover, it can directlyobserve the situation in the intestinal lumen. At the sametime, tumor tissue can be taken for pathological examinationand partial lesion removal (small lesions, polyps, etc.), whichplays an important role in the early diagnosis, treatment,and prevention of rectal cancer. However, colonoscopy notonly has many contraindications but also has many short-comings, such as the risk of perforation and bleeding, theinaccurate positioning of the tumor, and the inability toobserve the extraluminal infiltration and regional lymphnode metastasis of the tumor, so it cannot be used for theevaluation of regional lymph node staging of rectal cancer.
At present, imaging examination is the main method forevaluating rectal cancer before surgery. The traditional X-rayexamination (barium enema, gastroenterology enema con-trast) is to display the contour of the digestive tract by intro-ducing the contrast agent into the digestive tract, indirectlyobserve the anatomy and function of the digestive tract,which can identify the location, gross pathological type,and extent of the tumor, and understand and eliminate mul-tiple primary lesions of colorectal cancer. Moreover, its priceis low, and the operation is simple and easy, so it has greatclinical value for the diagnosis of rectal cancer. However, itcannot make an objective evaluation of the size of rectalcancer, the degree of extraluminal infiltration, and the sur-rounding tissue structure. Therefore, an X-ray examinationis used as a supplement or replacement only in the case ofunsatisfactory colonoscopy or colonoscopy and not as a
basis for the diagnosis of rectal cancer. When judging thebenign and malignant lymph nodes in rectal cancer, otherimaging methods are based on morphological changes suchas the lymph node size, morphology, margin, and density/-signal/echo, such as conventional abdominal pelvic CT, pel-vic MRI/intrarectal MRI, and intrarectal ultrasound (ERUS).However, there are many causes of lymph node enlargementaround the rectum, and even small lymph nodes may havemetastasis [10]. Therefore, morphological changes alonecan easily lead to false negatives and false positives, andthe accuracy is not high, which has great limitations onguiding the accurate staging of rectal cancer. In addition,the accuracy of the lymph node size of rectal cancer basedon the lymph node size reported in the literature is 55%-71% [11]. With the continuous development of medicalimaging, new inspection equipment and technology haveemerged, and functional imaging technology has attractedwidespread attention from clinical and imaging workers.Currently, common functional tests include CT perfusionimaging, MRI perfusion imaging, magnetic resonancediffusion-weighted imaging (DWI), superparamagnetic ironoxide- (USPIO-) enhanced MRI, magnetic resonance spec-troscopy (MRS), single photon emission computed tomog-raphy (SPECT), positron emission tomography (PET), andPET/CT. These can not only provide morphological infor-mation of the lesion but also reveal the functional metabo-lism of tissues and organs at the cellular and molecularlevels [12].
According to the above analysis, at present, there is noeffective analysis method in colorectal image analysis, whichleads to certain errors in colorectal image analysis, andsome interference factors directly affect the diagnosisresults. Based on this, based on the genetic algorithm, thisstudy explores the mining methods that can obtain effectiveinformation from the influence of colorectal cancer andpromote the further improvement of the diagnosis of colo-rectal cancer.
2. Research Method
2.1. GMð1, 1Þ Model. In the early 1980s, Professor DengJulong proposed the theory of gray systems. The theory isbased on a small-sample, poor-information, and uncertaintysystem that contains both known information and unknownor unascertained information. The algorithm mainly extractsvaluable information from the production and developmentof some known information and realizes the correct descrip-tion and effective monitoring of the system’s operatingbehavior and evolution law. Moreover, it finds the law ofthe data from the chaotic, finite, discrete data and thenestablishes the corresponding gray model for prediction.GMð1, 1Þ is an important part of the gray system theory,and it is also the most widely used prediction model. More-over, its core idea is to determine the best fit curve of a pointgroup generated by the accumulation of the originalsequence of the system [13].
Assuming that Xð0Þ = ðxð0Þð1Þ, xð0Þð2Þ,⋯,xð0ÞðnÞÞ, Xð1Þ =ðxð1Þð1Þ, xð1Þð2Þ,⋯,xð1ÞðnÞÞ exists,
2 Computational and Mathematical Methods in Medicine

X 0ð Þ kð Þ + ax 1ð Þ kð Þ = b, ð1Þ
is called the original form of the GMð1, 1Þ model.In equation (1), Xð0ÞðkÞ is the determined output and b is
the equivalent input obtained by calculation.Assuming that Xð0Þ and Xð1Þ are as defined above, then
Zð1Þ = ðzð1Þð2Þ, xð1Þð3Þ,⋯,xð1ÞðnÞÞ. Among them, zð1ÞðkÞ = ð1/2Þðxð1ÞðkÞ + xð1Þðk − 1ÞÞ. We call that
x 0ð Þ kð Þ + az 1ð Þ kð Þ = b, ð2Þ
is the basic form of the GMð1, 1Þ model.The meaning of the symbol GMð1, 1Þ is the gray model
of an order (Order) and a variable (Variable). In the GMð1, 1Þ model, the time response sequence of xð0ÞðkÞ + azð1ÞðkÞ= b is [14]
x∧ 1ð Þ k + 1ð Þ = x 0ð Þ 1ð Þ − ba
� �e−ak + b
a, k = 1, 2,⋯, n: ð3Þ
In the GMð1, 1Þ model, the restored value of xð0ÞðkÞ+ azð1ÞðkÞ = b is
x∧ 0ð Þ k + 1ð Þ = x∧ 1ð Þ k + 1ð Þ − x∧ 1ð Þ kð Þ, k = 1, 2,⋯, n: ð4Þ
It can be seen from equation (3) that the essence ofthe GMð1, 1Þ model is to adopt an exponential fitting sim-ilar to Neak for the original data except for the first point.The parameter −a in the model is the development coeffi-cient, and b is the gray action [15].
There are many models based on the gray system theory.So far, the most common application in the gray predictionmodel is the GMð1, 1Þ model, which is also an importantpart of the gray system theory. For decades, many scholarshave conducted a special study on the GMð1, 1Þ model,which enriches the gray system theory while improving themodeling mechanism and improving the prediction accu-racy of the model. Although good results have been achievedin the study of gray prediction models, there are still somemechanistic problems in the gray prediction model that havenot been fundamentally solved [16].
In equation (3), there is a boundary value xð0Þð1Þ, but inthe process of solving the development coefficient −a andthe gray action amount b, it is independent of the value ofthe boundary value xð0Þð1Þ. Therefore, the value of theboundary value xð0Þð1Þ should not be less than the index cor-rection effect of the prediction result. The GMð1, 1Þ modelprediction result is a fitting curve that does not pass the ð1, xð0Þð1ÞÞ point in the sense of least squares. However, theGMð1, 1Þ model-defined fit curve must pass the ð1, xð0Þð1ÞÞpoint, which is supported by no theoretical basis [17].
The GMð1, 1Þ model follows the least squares method toestimate the development coefficient −a and the gray actionb. That is, a and b satisfy
mina,b
〠n
i=1x∧ 0ð Þ ið Þ − x 0ð Þ ið Þh i2
: ð5Þ
In the prediction of the amount of image inspection, wepay more attention to the minimum relative error of the pre-diction results, that is,
mina,b
1n〠n
i=1
x∧ 0ð Þ ið Þ − x 0ð Þ ið Þ�� ��x 0ð Þ ið Þ�� �� %
" #: ð6Þ
Therefore, a and b obtained according to the leastsquares method are not the best results.
2.2. Optimization of the Image Inspection QuantityPrediction Model GMð1, 1Þ. According to the above analysisof the GMð1, 1Þ model, firstly, we can add a correction valueε to the boundary value of the optimized GMð1, 1Þ model.That is, the time response sequence of xð1Þð1Þ = xð0Þð1Þ + εin the GMð1, 1Þ model is set to [18]
x∧ 0ð Þ kð Þ = 1 − eað Þ x 0ð Þ 1ð Þ + ε −ba
� �e−a k−1ð Þ: ð7Þ
Secondly, the range of a, b, and ε is estimated accordingto the GMð1, 1Þ model, and the objective equation of equa-tion (8) is constructed, and the quantum genetic algorithm(QGA) is used to solve the parameters.
f a, b, εð Þ =mina,b,ε
1n〠n
i=1
x∧ 0ð Þ ið Þ − x 0ð Þ ið Þ�� ��x 0ð Þ ið Þ�� �� %
" #,
amin ≤ a ≤ amax,bmin ≤ b ≤ bmax,εmin ≤ ε ≤ εmax:
ð8Þ
Quantum genetic algorithm (QGA) is a product of thecombination of quantum computing properties and geneticalgorithms and is a probabilistic evolutionary algorithm pro-posed by K.H. Han in 2000. The quantum genetic algorithmintroduces the quantum state vector expression into thegenetic coding and uses the quantum logic gate to realize theevolution of the chromosome so that the quantum geneticalgorithm has a richer population than the traditional geneticalgorithm and achieves better convergence than the traditionalgenetic algorithm. In addition, quantum genetic algorithmsare based on the representation of quantum state vectors.Moreover, it uses qubits to encode chromosomes so that onechromosome can express the superposition of multiple statesand use quantum logic gates to realize chromosome variationand intersection, thus achieving the optimal solution of thetarget [19].
Quantum genetic algorithms use qubits to encode chro-mosomes, and it encodes the following.
3Computational and Mathematical Methods in Medicine

Assumingα
β
" #is a qubit,
α1 α2 ⋯ αn
β1 β2 ⋯ βn
" #is a
qubit and jαij2 + jβij2 = 1, i = 1, 2,⋯, n. Then, equation (9)is the j-th individual Xj′ of the t-th generation.
Xj′=αt1 αt2 ⋯ αtn
βt1 βt
2 ⋯ βtn
" # j = 1, 2, 3,⋯,Nð Þ: ð9Þ
The quantum genetic algorithm uses a quantum revolv-ing gate to perform the mutation operation, and its encodingmethod is as shown in
αi′
βi′
" #=
cos Δθið Þ − sin Δθið Þsin Δθið Þ cos Δθið Þ
" #×
αi
βi
" #: ð10Þ
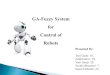
Therefore, the algorithm flow of optimization of theimage inspection quantity prediction model GMð1, 1Þ is asfollows (Figures 1):
(1) The GMð1, 1Þ model is built, and the range of a, b,and ε is estimated
(2) The objective equation f ða, b, εÞ is constructed(3) The population Qðt0Þ is initialized. Moreover, it is
assumed that the total population is n, and n isbinary coded to generate chromosomes encodedin qubits
(4) A measurement is performed on each individual inthe initial population Qðt0Þ to obtain a correspond-ing binary solution set Pðt0Þ
(5) The fitness of each determined solution is evaluatedby the fitness function
(6) Optimal individuals and corresponding fitness arerecorded
(7) It is judged whether the calculation process can beended, and if the end condition is satisfied, it isexited; otherwise, the calculation is continued
(8) Each individual in the population QðtÞ is subjectedto a measurement to obtain a corresponding binarysolution set
(9) The quantum revolving gate UðtÞ is used to per-form update and mutation operations on individ-uals to obtain new populations Qðt + 1Þ
(10) Optimal individuals and corresponding fitness arerecorded
(11) The number of iterations t is incremented by 1, andthe algorithm returns to step (5)
(12) a, b, and ε are substituted into the time responsesequence of the modelGMð1, 1Þ
(13) The restored value is solved
3. Results
The participants include 50 patients with colorectal adeno-carcinoma who underwent colorectal adenocarcinomaresection and underwent abdominal pelvic perfusion scanbefore surgery and were confirmed pathologically as acolorectal adenocarcinoma from January 2018 to Decem-ber 2018.
The standard constraints are as follows. (1) During CTexamination and before surgery, the patient did not haveany antitumor treatment. (2) The patient had no history ofallergy to iodine contrast agents and signed informed con-sent. (3) The patient has no serious heart, lung, liver, kidney,and other diseases. (4) The patient is in good general condi-tion and can cooperate with the entire examination process.(5) The patient has no contraindications for antispasmodicdrugs (such as prostatic hypertrophy and glaucoma). (6)The patient does not currently have hyperthyroidism. (7)The patient had not had gastrointestinal angiography within1 week before CT examination and did not take metal-containing drugs. (8) The postoperative pathological dataof the patient was recorded in complete detail.
All patients required a less slag diet within 2 days priorto the exam, and the patient required fasting the nightbefore the exam. The body mass was measured to determinethe amount of contrast injection. 30-90 minutes before theexamination, the patient orally administered 1500ml 2.5%mannitol until the contrast agent reached the rectum,thereby allowing the gastrointestinal tract to fully expand.15 minutes before the scan, the patient’s buttock musclewas injected with 10mg of anisodamine hydrochloride toremove body surface metal objects. Moreover, patients needto have repeated breath-holding training. For patients whocannot adhere to it, we need to keep the patient breathingcalmly. Conventionally, the abdominal band is added toreduce abdominal movements and to ensure that the patientis at rest during the scan. In addition, the examination pro-cess is informed to the patient, and the patient is informedthat a normal reaction such as pain and transient feveroccurs when the contrast agent is injected. At the same time,it is necessary to obtain the cooperation of the patient toavoid the patient’s respiratory movement due to suddendiscomfort.
1
MEAN AGO
+
–
Ash action b White output
a
Figure 1: GMð1, 1Þ control chart.
4 Computational and Mathematical Methods in Medicine

According to the CT scan image, the tumor position isdetermined, and the largest level of the lesion is selected.Moreover, with this layer as the center, 8 layers are selectedas the target level, and the suspected enlarged lymph nodesin the fat space around the lesion are included as much aspossible. Thereafter, 300mg of I/100ml of iohexol wasinjected through the median vein of the elbow at a rate of4.0ml/s. When injecting contrast agents, close patientresponse is required. Once there is an adverse reaction, weneed to stop the injection and scan immediately. After thecontrast agent was injected, 20ml of physiological salinewas injected at the same rate. The film scanning methodwas used for the same layer dynamic enhanced scanning,and the 8 s sweep was delayed, and the continuous acquisi-tion was 40 s, and 320 perfusion images were obtained.Moreover, the Z-axis coverage is 4 cm, the layer thicknessis 5mm, the average scanning interval is 1.0 s, and the scan-ning parameter is 120 kV, 40mA.
The acquired perfusion data is transferred to the GEAdvantage Workstation 4.3 for viewing images. Whetherthe lesion is located in the observed scan plane is correct,and whether the lesion position is too large is judged toselect the eligible case. The body tumor perfusion softwarein the preinstalled Perfusion 3.0 software package was thenapplied for data processing. Thereafter, the threshold rangeis set to -200 to 120 HU to remove images of tissues suchas bone, fat, and air. The first target plane without anyenhancement is selected as the basal plane, the plane of themost obvious phase is selected for lesion enhancement, andthe abdominal aorta, external iliac artery, or femoral arteryis selected as the input artery. After that, the Region OfInterest (ROI) is manually depicted. The ROI is selected atthe largest level of the tumor and avoids the edge of thetumor, the markedly enhanced blood vessels, and thenecrotic cystic changes and calcifications within the mass,avoiding the effects of partial volume effects. After that, thesolid part of the tumor is selected, and the area containsthe entire tumor as much as possible (Figures 2 and 3).The perfusion software can automatically analyze the time-density curve (TDC) of the target artery and lesion ROI,the CT perfusion pseudocolor map of this level, and a seriesof perfusion parameter values such as blood flow (BF), bloodvolume (BV), mean transit time (MTT), and surface perme-ability (PS).
Image processing is performed on the above image, andon the basis of this, Figures 2 and 3 can be, respectively,shown in the form shown in Figures 4 and 5.
Figure 4 is used for data mining through the algorithm ofthis study, and the following information is obtained. Thepatient is male and has rectal cancer. Surgical pathologyconfirmed that it was a moderately differentiated adenocar-cinoma, invading the whole layer; the two margins werenot involved in cancer, and no cancer metastasis was foundin the lymph nodes of each group, and the rectal wall under-went eccentric thickening.
Figure 5 is used for data mining through the algorithm ofthis study, and the following information is obtained. Thepatient is male and has sigmoid colon cancer. Surgicalpathology confirmed that it is a highly differentiated adeno-
carcinoma that invades the muscular layer. Moreover, therewas no cancer involvement in the two margins and the anas-tomosis ring, and no cancer metastasis was found in thelymph nodes of each group, and eccentric thickeningoccurred locally in the sigmoid colon.
In order to further study the role of the genetic algorithmmodel in colorectal image data mining, this study takes therole of ADC as an example for analysis.
Figure 2: Tumor scan mark image.
Artery
Figure 3: Image of tumor ROI.
Figure 4: Image of tumor scan marks after image processing.
5Computational and Mathematical Methods in Medicine

In this experiment, the number of lymph nodes includedin the metastatic group was 19, and the number of metastaticnodules included was 13. Moreover, the maximum shortdiameter of the metastatic lymph nodes ranged from6.20mm to 17.60mm, 9 cases were round and elliptical,and 10 cases were lobulated and not smooth. The T2WIfat suppression is a high signal, and the short diameter ofthe metastatic nodules is 2.10mm~7.80mm, which is roundor oval, and the boundary is smooth. FST2WI fat suppres-sion is a high signal, and malignant lymph nodes and meta-static nodules are high signals on DWI. The measured ADCvalues of malignant lymph nodes were 0:80 ± 0:18 × 10−3 mm2/s, and the metastatic nodule ADC values were 0:78 ±0:25 × 10−3 mm2/s, and p = 0:80 > 0:05, so the differencewas not statistically significant. The comparison betweenthe two groups is shown in Table 1.
The collected test image results are shown in Figure 6.Image processing is performed on the above image, and
the result is shown in Figure 7.
4. Analysis and Discussion
Local lymph node metastasis (paraspinal lymph nodes,mesangial lymph nodes) is the most common metastaticpathway for colorectal adenocarcinoma. Therefore, CT per-fusion examination of colorectal adenocarcinoma can addi-tionally provide hemodynamic status of regional lymphnodes of colorectal adenocarcinoma in the scan range andindirectly evaluate its angiogenesis. However, there are fewreports on the evaluation of regional lymph nodes in colo-rectal adenocarcinoma by CT perfusion imaging. Compared
with tumors, the size of lymph nodes is smaller, and it ismore susceptible to intestinal peristalsis, respiratory move-ment, and partial volume effect. Therefore, this study onlyselected the largest metastatic lymph node in patients withlymph node metastasis as the “target” lymph node. A totalof 19 patients with lymph node metastasis were confirmedby postoperative pathology in this group of data. Amongthem, 1 case of metastatic lymph nodes was not includedin the perfusion scan range, 1 case of lesion position shiftin the scan plane due to intestinal peristalsis was too large,and 1 patient’s perfusion parameters could not be calculated,so the patient was not included in the study. Moreover, the
1a 1b
1c 1d
Figure 7: Detection image of colorectal cancer after imageprocessing. The (a–d) obtained by the algorithm of this study are,respectively, expressed as follows. (a) The sigmoid wall isthickened, about 10-13mm thick, the intestinal wall is intact, andthe T1WI is low. (b) T2WI fat suppression is a high signal. (c)DWI is a high signal, and the intestinal wall is intact. (d) ADCdiagram shows a low signal.
1a 1b
1c 1d
Figure 6: Detection image of colorectal cancer.Table 1: Comparison of ADC values between malignant lymphnodes and metastatic nodules.
Group Number ADC values (×10-3mm2/s)
Malignant lymph nodes 19 0:80 ± 0:18Metastatic nodules 13 0:78 ± 0:25p = 0:80
Artery
Figure 5: Image of cancer ROI after image processing.
6 Computational and Mathematical Methods in Medicine

data standard deviation of this group is large. At present,some scholars use CT perfusion imaging technology to eval-uate the nature of lymph node lesions in the neck, axilla,inguinal region, mediastinum, etc., but the results are verydifferent. Therefore, CT perfusion can provide informationon blood perfusion of lymph nodes, but the value of evaluat-ing lymph node properties remains to be further studied.
In this study, a genetic algorithm is used as the basicalgorithm of data mining, and the detection result has cer-tain superiority compared with the traditional detectionalgorithm. The predictive performance of image inspectionis superior for several reasons. First, the GSVR model ofimage inspection fully utilizes the preprocessing of data inthe gray model, reduces the randomness of the data,increases the regularity of the data, and is more consistentwith the nonlinear mapping characteristics of the supportvector machine. These make the support vector machineconverge more quickly. Second, if the parameters are notproperly selected, the support vector machine will be over-fitting or underfitting. In this study, the detection functioncan determine the appropriate parameters to predict theamount of image examination. Furthermore, the GSVRmodel minimizes structural risk without minimizing train-ing errors and better solves problems such as small samples,nonlinearity, overfitting, dimensionality disasters, and localminima. Therefore, its generalization and promotion abilityare excellent.
The genetic algorithm has obvious advantages in thediagnosis and prognosis of colorectal cancer compared withthe traditional imaging examination. With the developmentof new technologies, genetic algorithms are playing anincreasingly important role, but they also have certain limi-tations. Different histological subtypes in colorectal cancerpatients also have certain differences in radioactive uptake.Moreover, colorectal cancer containing mucus componentsmay be false negative, and the degree of mucus concentra-tion in tumors is related to the mucus content in tumorcells. The lesser the mucus component, the lesser theamount of mucus ingested, and there is even no significantradioactive concentration. In the diagnosis of postoperativerecurrence of colorectal cancer patients, the increase ofradioactive intake may be caused by postoperative anasto-motic stomatitis, intestinal polyps, intestinal physiologicuptake, and other benign lesions, causing false positives. Inaddition, in terms of lung metastasis, increased radiationintake may be affected by benign lesions such as tuberculo-sis and inflammation, causing false positives. Firstly, themetastasis of rectal cancer is slightly different from themetastasis of other parts of the colon. The special venousreturn system in the lower part of the rectum can cause sol-itary lung metastasis without liver metastasis, which is diffi-cult to distinguish from single lung nodules. With theapplication of genomics in the prognosis assessment of colo-rectal cancer patients, how to label more specific probes atthe molecular level will be an opportunity and challengefor the development of nuclear medicine. Secondly, in theupsurge of tumor heterogeneity research, the genetic algo-rithm plays an important role as a good means of tumorheterogeneity research.
5. Conclusion
Based on the genetic algorithm, this study explores the min-ing methods that can obtain effective information from theinfluence of colorectal cancer and promote the furtherimprovement of the diagnosis of colorectal cancer. Thequantum genetic algorithm is based on the representationof quantum state vectors. It uses qubits to encode chromo-somes, allows one chromosome to express multiple states,and uses quantum logic gates to achieve chromosome varia-tion and intersection, thus achieving the optimal solution ofthe target. At the same time, in this study, according to theCT scan image, the tumor position was determined in theimage processing, and the largest level of the lesion wasselected. Moreover, with this layer as the center, 8 layersare selected as the target level, and the suspected enlargedlymph nodes in the fat space around the lesion are includedas much as possible. In addition, this paper designs a controlexperiment for analysis. The research results show that thegenetic algorithm is used as the basic algorithm of data min-ing. The detection results have certain advantages over thetraditional detection algorithms and can be graduallyapplied to the clinical detection of colorectal effects.
Data Availability
The data used to support the findings of this study have notbeen made available because we did not obtain permissionfor data sharing from the data provider.
Conflicts of Interest
The authors have no competing interests.
References
[1] Y. Liu, U. Aickelin, J. Feyereisl, and L. G. Durrant, “Waveletfeature extraction and genetic algorithm for biomarker detec-tion in colorectal cancer data,” Knowledge-Based Systems,vol. 37, pp. 502–514, 2013.
[2] H. Bozcuk, U. Bilge, E. Koyuncu, and H. Gulkesen, “An appli-cation of a genetic algorithm in conjunction with other datamining methods for estimating outcome after hospitalizationin cancer patients,” Medical Science Monitor InternationalMedical Journal of Experimental & Clinical Research, vol. 10,no. 6, pp. CR246–CR251, 2004.
[3] K. X. Lai, B. T. Phung, and T. R. Blackburn, “Descriptive datamining of partial discharge using decision tree with geneticalgorithm,” Australian Journal of Electrical and ElectronicsEngineering, vol. 6, no. 3, pp. 249–259, 2009.
[4] Z. Detorakis and G. Tambouratzis, “Applying a sectionedgenetic algorithm to word segmentation,” Pattern Analysisand Applications, vol. 13, no. 1, pp. 93–104, 2010.
[5] D. M. Liou and W. P. Chang, “Applying data mining for theanalysis of breast cancer data,” in Data Mining in ClinicalMedicine, Methods in Molecular Biology, Springer, 2014.
[6] R. J. Mstafa and K. M. Elleithy, “A video steganography algo-rithm based on Kanade-Lucas-Tomasi tracking algorithmand error correcting codes,” Multimedia Tools and Applica-tions, vol. 75, no. 17, pp. 10311–10333, 2016.
7Computational and Mathematical Methods in Medicine

[7] M. Sakamoto, T. Nakajima, and T. Alexandrova, “Enhancingvalues through virtuality for intelligent artifacts that influencehuman attitude and behavior,”Multimedia Tools and Applica-tions, vol. 74, no. 24, pp. 11537–11568, 2015.
[8] T. Zarraonandia, P. Diaz, I. Aedo, and M. R. Ruiz, “Designingeducational games through a conceptual model based on rulesand scenarios,” Multimedia Tools & Applications, vol. 74,no. 13, pp. 4535–4559, 2015.
[9] S. Hardy, T. Dutz, J. Wiemeyer, S. Göbel, and R. Steinmetz,“Framework for personalized and adaptive game-based train-ing programs in health sport,” Multimedia Tools and Applica-tions, vol. 74, no. 14, pp. 5289–5311, 2015.
[10] H. Tu, N. Kumar, J. Kim, and J. Seo, “A strongly securepairing-free certificateless authenticated key agreement proto-col suitable for smart media and mobile environments,” Mul-timedia Tools and Applications, vol. 74, no. 16, pp. 6365–6377, 2015.
[11] A. H. Elbaz, “Hybrid intelligent system-based rough set andensemble classifier for breast cancer diagnosis,” Neural Com-puting & Applications, vol. 26, no. 2, pp. 437–446, 2015.
[12] V. Chang, “An overview, examples and impacts offered byemerging services and analytics in cloud computing,” NeuralComputing & Applications, vol. 29, no. 5, pp. 1243–1256, 2018.
[13] M. Khan, T. Shah, and S. I. Batool, “Construction of S-boxbased on chaotic Boolean functions and its application inimage encryption,” Neural Computing & Applications,vol. 27, no. 3, pp. 677–685, 2016.
[14] D. Bacciu, “Unsupervised feature selection for sensor time-series in pervasive computing applications,” Neural Comput-ing & Applications, vol. 27, no. 5, pp. 1077–1091, 2016.
[15] S. Yu and S. Deng, “Adaptive vehicle extraction in real-timetraffic video monitoring based on the fusion of multi-objective particle swarm optimization algorithm,” EURASIPJournal on Image and Video Processing, vol. 2018, no. 1, ArticleID 145, 2018.
[16] Y. Guo, X. Zong, M. Qi, Y. Zhang, and H. Wang, “Feasibilitystudy on color evaluation of jadeite based on GemDialoguecolor chip images,” EURASIP Journal on Image and Video Pro-cessing, vol. 2018, no. 1, Article ID 95, 2018.
[17] K. M. Lin, J. R. Lin, M. J. Chen, C. H. Yeh, and C. A. Lee, “Fastinter-prediction algorithm based on motion vector informa-tion for high efficiency video coding,” EURASIP Journal onImage and Video Processing, vol. 2018, no. 1, Article ID 99,2018.
[18] A. Ivanavičius, H. Simonavičius, J. Gelšvartas et al., “Real-timeCUDA-based stereo matching using Cyclops2 algorithm,”EURASIP Journal on Image and Video Processing, vol. 2018,no. 1, Article ID 12, 2018.
[19] F. Chen, P. Wen, Z. Peng, G. Jiang, M. Yu, and H. Chen, “Hier-archical complexity control algorithm for HEVC based oncoding unit depth decision,” EURASIP Journal on Image andVideo Processing, vol. 2018, no. 1, Article ID 96, 2018.
8 Computational and Mathematical Methods in Medicine