Embed Size (px)
Citation preview

Research ArticleDetection of Doppler Microembolic SignalsUsing High Order Statistics
Maroun Geryes12 Sebastien Meacutenigot1 Walid Hassan3 Ali Mcheick2
Jamal Charara2 and Jean-Marc Girault1
1Universite Francois Rabelais de Tours UMR Imagerie et Cerveau Inserm U930 Tours France2Department of Physics and Electronics Faculty of Sciences I Lebanese University Beirut Lebanon3Clarivate Analytics Dubai UAE
Correspondence should be addressed to Jean-Marc Girault jean-marcgiraultuniv-toursfr
Received 5 September 2016 Accepted 17 November 2016
Academic Editor Po-Hsiang Tsui
Copyright copy 2016 Maroun Geryes et alThis is an open access article distributed under the Creative CommonsAttribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Robust detection of the smallest circulating cerebral microemboli is an efficient way of preventing strokes which is second causeof mortality worldwide Transcranial Doppler ultrasound is widely considered the most convenient system for the detection ofmicroemboli Themost common standard detection is achieved through the Doppler energy signal and depends on an empiricallyset constant threshold On the other hand in the past few years higher order statistics have been an extensive field of research asthey represent descriptive statistics that can be used to detect signal outliers In this study we propose new types of microembolicdetectors based on the windowed calculation of the third moment skewness and fourth moment kurtosis of the energy signalDuring energy embolus-free periods the distribution of the energy is not altered and the skewness and kurtosis signals do notexhibit any peak values In the presence of emboli the energy distribution is distorted and the skewness and kurtosis signals exhibitpeaks corresponding to the latter emboli Applied on real signals the detection of microemboli through the skewness and kurtosissignals outperformed the detection through standard methods The sensitivities and specificities reached 78 and 91 and 80and 90 for the skewness and kurtosis detectors respectively
1 Introduction
Sudden intensity increases in the Transcranial Doppler(TCD) signal are majorly interpreted as signatures resultingfrom cerebral emboliThe passage of cerebral emboli throughblood vessels feeding the brain could result in blockage ofthese vessels and consequently lead to stroke the secondcause of mortality worldwide Embolic strokes constitute upto 14 of all strokes [1] Therefore embolic strokes representa major death threat and thus the early detection of thesmallest microemboli is an important issue for which robustsolutionsmust be foundThis early detectionwould be a basisfor early stroke diagnosis and thus avoiding its occurrenceNowadays TCD is considered the most effective embolicstroke diagnosis system
Although the characteristics and physical nature ofembolic signals in the TCD signal have been well definedthe task of detecting embolic and particularly smallmicroem-bolic signals still poses a tough challenge The gold standard
method of detecting the passage of emboli is the audibledetection of the sudden ldquochirprdquo or ldquomoanrdquo produced byemboli as well as the visual detection of the time-frequencyrepresentation (spectrogram) generated on the TCD screenAmain limitation of the gold standard is the inability to audi-bly detect microembolic signals located at the systolic phasedue to temporal and frequency masking effects in audio files
The standard signal processing method of detectingembolic signals is based on calculating the energy fromthe spectrogram and applying constant thresholds to pickup the emboli which according to Rayleigh theory [2]backscatter ultrasound energy higher than that backscatteredby the surrounding blood The major limitations in standardtechniques reside in the inability of detecting small microem-bolic signals having lower intensities than the surroundingbackground blood mainly at the systolic peak
As a purpose to detect the smallest microemboli manyresearch works have been carried out We list some of the
Hindawi Publishing CorporationComputational and Mathematical Methods in MedicineVolume 2016 Article ID 3243290 8 pageshttpdxdoiorg10115520163243290
2 Computational and Mathematical Methods in Medicine
most punctual methods Frequency filtering methods wereintroduced in [3 4]The study reported high detection sensi-tivity and specificity rates Subsequently an online automatedembolic signal detection algorithm based on frequency fil-tering was developed in [5 6] The latter system showedhigh performances in terms of sensitivity and specificity forparticular cases (postcarotid endarterectomy) However inother conditions (atrial fibrillation) the systemrsquos sensitivityand specificity severely decreasedMoreover the systemrsquos per-formance in the detection of low energymicroembolic signalswas arguably less efficient with much lower sensitivity andspecificity Methods based on detection of sudden changeswere introduced in [7] Nonparametric detection methodsmainly the Fourier Wigner-Ville and wavelet approacheswere compared to parametric autoregressive methods Thenew parametric methods were proven to be highly perfor-mant and efficient in the detection of small microemboliHowever the methods were tested on synthetic simulatedDoppler signals and never on a set of real signals Anotherhighly productive wavelet-based system was established in[8] The system achieved a high combination of sensitivityand specificity However the systemrsquos rates decreased in thecase of low energymicroembolic signals A remarkable offlinedetection was proposed in [9] The system had excellentperformance for emboli having high intensities relative tobackground blood clutter However it is to be noticed thatthe study did not take into consideration the detection ofweak embolic signalsThe authors in [10] introduced anotherhighly achieving detection procedure based on the discretewavelet transform (DWT) DWT allowed major increases inspecificity and sensitivity Nonetheless a major deficiencyof the DWT implementation was the reduced frequencyresolution at low frequency scales in which embolic signalsare mostly found In [11] the authors proposed embolicdetection using the adaptive wavelet packet basis and neu-rofuzzy classification The adaptive wavelet packet basis wasused to make a sparse representation of Doppler ultrasoundblood flow signals The method produced highly accurateand robust performances However when compared to othermethods only the sensitivity was taken into account and thecorrelated specificity was not calculatedThe study submittedin [12] requested the use of Fractional Fourier Transformrather than the short time Fourier transform the standardmethod of detection in TCD systemsThe results showed thatdiscriminating parameters based on the Fractional FourierTransform help easier analysis and detection of embolicsignals Despite its simplicity and acceptable results thismethodwas not proven reliably decent for the detection of thesmallest microemboliThemethod proposed in [13] achievedvery high sensitivity and specificity but large detection errorsoccurred due to small gaseous emboli exhibiting smallreflected signals
In most articles previously introduced the main limi-tation lies in the fact that the information on which thedetection takes place is time-varyingwhile the threshold usedis constant To match between the time-varying informationand the threshold two solutions can be proposed The first isproposing a time-varying threshold as in [14 15] thatmatchesthe time-varying trend of the decision information Second
is proposing a constant threshold that matches the decisioninformation for which the time-varying trend is removed
In this work the methods we proposed of matchingbetween a constant threshold and an energy free of itstime-varying trend are based on the use of high orderstatistic (HOS) of windowed Doppler energy signal Wetend to prove the skewness and kurtosis as two solid meansto detect microembolic signals when asymptomatic caroidartery patients are monitored with a Holter TCD
2 The Offline Microembolic Detection Unit
As previously mentioned our objective is to perceive amicroemboli detector more sensitive and robust regardingmost standard detectors
In this study the typical offline signal processing unit isdecomposed into 3 units
(i) Unit A allocated for loading the wave file 10-secondsignal segmentation short time Fourier transform(STFT) calculation and instantaneous energy calcu-lation from the STFT
(ii) Unit B allocated for standard energy detection on theenergy signal obtained in Unit A
(iii) Unit C allocated for the new energy detection tech-niques based on skewness and kurtosis calculation ofthe energy signal obtained in Unit A
21 Unit A Doppler Signal Extraction STFT and Instan-taneous Energy Calculation The different systems that wewant to test depicted in Figure 1 share a common structureFrom the SD card plugged out from the Holter system andplugged into the personal computer the Doppler signal ispicked up and put in memory From this Doppler digitalsignal the short time Fourier transform is calculated firstto display the spectrogram and second to estimate instanta-neously the Doppler energy Calculations of the STFT andthe instantaneous energy are carried out repetitively on 10-second segments extracted from the Doppler signal
Most commercial TCD ultrasound systems are based onthe short time Fourier transform The short time Fouriertransform is an adapted form of the Fourier transform thatanalyzes only a small segment of the signal at a time atechnique called windowing of the signal or also WindowedFourier Transform (WFT) Short time Fourier transform isused when the Doppler signal within the analyzing windowis stationary In reality transforming data into the frequencydomain results in loss of time information By applying theFourier transform of a signal it is impossible to identifywhen a particular event takes place The STFT was thusproposed to correct this deficiency The STFT maps a signalinto a two-dimensional function of time and frequency Thisrepresentation is known as the spectrogram
The STFT frequency estimator with a sliding window canbe formally written as follows
119878 (119905 119891) = 1003816100381610038161003816100381610038161003816int 119909 (120591) 119908lowast (119905 minus 120591) expminus11989521205871198911199051198891205911003816100381610038161003816100381610038161003816
2
(1)
Computational and Mathematical Methods in Medicine 3
SD card memory
Instantaneous energy estimator
Standard energydetector
Automaticcounter 1
New energy detector
Automaticcounter 3
Constant empiricalthreshold estimation
Number of embolicdetections Output 1
Output 2
Input
Automaticcounter 2
Skewnesscalculation
Kurtosiscalculation
Number of embolicdetections
Output 3
Data-basedthreshold estimation
Number of embolicdetections
Data-basedthreshold estimation
Unit A
Unit BUnit C
STFT (10ms)
Extraction of a digital sequence (10 s)
Figure 1 A typical embolus detection system including standard detection and our new detection procedure Unit A includes extracting 10 sdigital Doppler signal sequences from the SD card extracted from the Holter system calculating the short time Fourier transform and lastlycalculating the instantaneous energy from STFT estimators Unit B represents the detection achieved using standard methods while Unit Crepresents the new detection procedure we have developed based on skewness and kurtosis calculation
where 119909(119905) is the analyzed Doppler signal 119908(119905) is a slidingwindow and lowast stands for complex conjugation
When using the STFT to process embolic signals itis of great importance that the STFT parameters are opti-mized The three processing parameters are the window sizethe window type and the overlap ratio Despite the factthat setting the parameters significantly affects the embolusdetection system based on STFT calculations little work onthe effect of the different parameters has been reported Afundamental work was reported in [16] The authors evalu-ated the effect of varying the three parameters on embolicsignal temporal and frequency resolutions time of embolicsignal onset and the power of the embolus at the frequencywith maximum power relative to the average power of thebackground intensity Based on [16] and after a preliminarystage of experimental optimization of the STFT parametersthe STFT in this study is performed using a 146-millisecondHamming window with an overlap of 65
The instantaneous energy at a fixed time 119905 can be obtainedfrom STFT frequency estimators in (1) by
119890 (119905) = int 119878 (119905 119891) 119889119891 (2)
Note that the energy returned by a microembolus wouldbe greater than that returned by billions of red blood cells(RBCs) since a microembolus is often larger than RBCsHence the backscattered energy would function as a solid
indicator from which the presence of embolic and microem-bolic signatures could be detected This justifies why mostdetectors are chosen to be mainly based on energy criteria
22 Unit B Standard Microembolic Detection The standarddetection methods to which we compare the new proposedmethods are based on a direct detection of the embolicsignatures in the energy signal An empirical thresholdis commonly used This constant threshold can be fixedempirically by the trained user for the entire examination Itis patient- operator- and device-dependent This thresholdis set above the maximal background energy of the Dopplersignal when no embolus is present [17] that is the systolicpeak The microembolic standard detection based on aconstant threshold is represented in Figure 2(a)
The main limitation of using such method resides incomparing the energy which is time-varying to a constantthreshold To match between the time-varying trend of theenergy and the threshold two solutions can be proposedeither a time-varying threshold as in [14 15 18] that matchesthe time-varying trend of the decision information or aconstant threshold that matches the energy while removingthe time-varying trend
23 Unit C Skewness and Kurtosis Based Microembolic Detec-tion As previously mentioned it is a threshold-orienteddetection As shown in Figure 2 weak embolic events are
4 Computational and Mathematical Methods in Medicine
120583 HITS 120583 HITS 120583 HITS
1 2 3 4 5 6 7 8 9 100Time (s)
002040608
1
Dop
pler
ener
gy
(a)
07
120583 HITS120583 HITS120583 HITS
t1 t2 t31 2 3 4 5 6 7 8 9 100Time (s)
0123456
Skew
ness
(b)
32
120583 HITS 120583 HITS 120583 HITS
t1 t2 t31 2 3 4 5 6 7 8 9 100Time (s)
0
5
10
15
Kurt
osis
(c)
Figure 2 (a)TheDoppler energy signal An empirical threshold is applied to obtain themicroembolic standard detection (b) Skewness signalcalculated from the windowed energy signal A data-based threshold is applied to complete the microembolic detection The mean value ofthe skewness signal is 07 (c) Kurtosis signal calculated from the windowed energy signal A data-based threshold is applied to complete themicroembolic detection The mean value of the kurtosis signal is 32 Moreover we choose in (b) and (c) three time positions 1199051 = 072 sduring which an embolus is present and 1199052 = 47 s and 1199053 = 88 s when no embolus is present We detect in the case of absence of embolus119878(1199052) asymp 119878(1199053) asymp 07 and119870(1199052) asymp 119870(1199053) asymp 32 while in the presence of embolus we detect 119878(1199051) = 28 = 119878(1199053) asymp 07 and119870(1199051) = 11 = 119870(1199053) asymp 32
impossible to detect with a constant threshold One wayto overcome this issue is to remove the time-varying trendin the instantaneous Doppler energy To prove that highorder statistics such as the skewness and the kurtosis aresuitable candidates to overcome this limitation consider aDoppler signal free of microembolic events and assume thatthe statistical distribution remains unchanged whatever thetime position is even if the mean 120583119894(119905) and the variance1205901198942(119905) vary with time Suppose there exists two Gaussianrandom variables 119883(1199052) = 119873(1205831(1199052) 1205901(1199052)) and 119883(1199053) =119873(1205832(1199053) 1205902(1199053)) It can be shown for the skewness 119878 that119878(1199052) = 119878(119883(1199052)) = 119878(119883(1199053)) = 0 and for the kurtosis 119870that 119870(1199052) = 119870(119883(1199052)) = 119870(119883(1199053)) = 3 In this example theskewness and the kurtosis are stationary since 119878(119905) = 0 and119870(119905) = 3 for all 119905 This outcome can be verified whatever thedistribution form while it remains unchanged over all timevalues The only change occurs in the value of the skewnessand the kurtosis but not in their stationarity Consequentlywhen a microembolic event occurs at a time position 1199051 thedistribution changes The direct consequence is 119878(1199051) = 119878(1199052)and119870(1199051) = 119870(1199052)
Therefore we can propose a new detector based oncalculating the skewness and kurtosis from the energy signalThe calculations are performed using a sliding window 119892(119905)where the optimal window length and overlap ratio are setduring a training phase (see Results section)
The skewness is the third-order standardized momentWhen calculated instantaneously (by the sliding window) onthe energy it is given by the following equation
119878 (119905) = 119864 [119890 (119905) minus 120583119890 (119905)]3
120590119890 (119905)3 (3)
The kurtosis is the fourth-order standardized momentWhen calculated instantaneously on the energy it is given bythe following equation
119870 (119905) = 119864 [119890 (119905) minus 120583119890 (119905)]4
120590119890 (119905)4 (4)
where 120583119890(119905) and 120590119890(119905) are the instantaneous mean and stan-dard deviation of the energy while 119864[] denotes the expectedvalue
Computational and Mathematical Methods in Medicine 5
(a) (b)
Figure 3 (a) Robot probe and (b) Holter Transcranial Doppler System (TCD-X Atys Medical Soucieu en Jarrest France)
The microembolic detection based on the skewness andkurtosis signals is represented in Figures 2(b) and 2(c)
In order to complete the detection on the skewnessand kurtosis signals a threshold has to be set in order topick up the peak signals We decided to establish a data-based threshold for the skewness and kurtosis signals fromtheir respective means 120583119904 and 120583119896 and respective standarddeviations 120590119904 and 120590119896 This threshold is defined as 120582119904 =120583119904 + 119898120590119904 for skewness and 120582119896 = 120583119896 + 119898120590119896 for kurtosiswhere 119898 is a parameter whose value is adjusted using anoptimization training phase in a manner that increases thesystemrsquos sensitivity and specificity (refer to Results section)The thresholds are represented in Figures 2(b) and 2(c)
3 The Holter System and the Protocol
TCD is a noninvasive nonionizing inexpensive portableand safe technique which renders it as a convenient toolfor the detection of cerebral microemboli Long time probepositioning and the short effective examination durationare the main limitations of traditional TCD systems TheTranscranial Holter (TCD-X Atys Medical Soucieu en Jar-rest France) shown in Figure 3 allows prolonged patientmonitoring (higher than 5 hours) with the patient no longerattached to a TCD and does not need to be laying on a bedbut rather can be monitored under naturalistic conditionsTheHolter is equipped with a robotized automatic probe thathelps find the best TCD signal and tracks it automaticallyduring the whole recording
A database obtained from the Centre HospitalierRegional Universitaire (CHRU) de Lille (2 Avenue OscarLambret 59000 Lille France) is used Informed consent for
Holter monitoring was obtained from all monitored patientsThe recordings were acquired from the middle cerebralartery of the patients The ultrasonic wave frequency was15MHz the pulse repetition frequency (PRF) was 64 kHzand the ultrasound power was 50mWcm2
After the clinical examination an analogous conversion isperformed on theDoppler digital signal and then theDopplersignal is sent to a loudspeaker From the audible Dopplersignal and from the spectrogram displayed on a screen wedetect and count manually the number of microembolicevents in order to constitute our gold standard of detectionThe gold standard is subject to interagreement betweenthree experts of our laboratory Then the positions in timeof audibly and visually agreed-on microembolic events arenoted This gold standard is used to assess the results ofthe different detectors used and validate their performancesAlthough the gold standard detections obtained from expertsand nonexperts might be the same as stated in [19] theexperience of the latter experts was useful to distinguishbetween microembolic signals and artifact signals discussednext We should also point out that listening to the audiofiles is made at the normal playing speed and another time athalf the normal speed which allows us to detect microembolipreviously inaudible due to the well-known temporal andfrequency masking effects in audio files
4 Results
The different detectors are tested through algorithms wedeveloped using the numerical calculation software Matlab(Mathworks Natick MA USA) Our database is composedof 18 recorded signals divided into two categories The first
6 Computational and Mathematical Methods in Medicine
Table 1 Training phase results of the optimal thresholds that best maximize the sensitivity and specificity for the standard energy detectorand skewness and kurtosis based detectors
Optimal threshold that maximizes the sensitivity and specificity Sensitivity () Specificity ()Standard energy detector 5 dB 67 58Skewness detector 120582119904 = 120583119904 + 4120590119904 76 91Kurtosis detector 120582119896 = 120583119896 + 5120590119896 77 91
Table 2 Results (sensitivity and specificity) for the standard energy detector and the new detectors based on skewness and kurtosiscalculations of the Doppler energy signal
Detector type True positive False positive Sensitivity () Specificity ()Gold standard detections = 136Standard detection 88 58 65 60Skewness detection 106 10 78 91Kurtosis detection 109 12 80 90
is the training phase (8 signals) dedicated to determining thebest settings of the detectors used The second is the testingphase (10 signals) dedicated to assessing the performances ofthe detectors used under the optimal settings determined inthe training phase
Two parameters are used to evaluate the detectors
(i) Sensitivity (or Detection Rate) calculated as the num-ber of true positive detectionsthe number of goldstandard detections True positive detection refers tothe detection of an embolus recorded in the goldstandard
(ii) Specificity calculated as 1 minus False Alarm Rate (FAR)the latter being the number of false positive detec-tionsthe total number of detections False positivedetection refers to the detection of an embolus notrecorded in the gold standard or in other words anembolus which has not crossed the sample volume
41 Training Phase Results Since the threshold applied on theenergy signal to achieve the standard detection is empiricallyset through the choice of the user different microembolicdetections could be obtained To overcome this we initializea training phase to preset the best empirical threshold tobe used in the testing phase 3 to 9 dB values are usedTable 1 shows the empirical threshold that best maximizes thesensitivity and specificity
Moreover since the skewness and kurtosis calculationsare performed using a sliding window 119892(119905) on the energysignal an experimental test on the training phase signals isinitialized to determine the optimal length of thewindow119892(119905)and the optimal overlap ratio The optimal temporal windowlength is 73milliseconds and the optimal overlap used is 95Also using these settings we test in the training phase the bestdata-based threshold 120582119904 = 120583119904 + 119898120590119904 and 120582119896 = 120583119896 + 119898120590119896 forthe skewness and kurtosis signals respectively Values of 119898ranging between 3 and 7 are tested Table 1 shows the data-based threshold for the skewness and kurtosis signals thatbest maximizes the sensitivity and specificity
42 Testing Phase Results Table 2 represents the testingphase results for the three different energy detectors Forthe standard energy detector with empirical threshold thesensitivity is 65 and the specificity is 60 For the energydetector based on skewness calculation the sensitivity is 78and the specificity is 91 For the energy detector based onkurtosis calculation the sensitivity is 80 and the specificityis 90
The results presented show that the new detectors areable to significantly increase the specificity compared tostandard detection (more than 30) Moreover the sensi-tivity achieved by the new detectors is increased by 13for the skewness detector and 15 for the kurtosis detectorcompared to that achieved by standard detectors Theseresults assert the accuracy and superiority of the detectionbased on skewness and kurtosis calculation of the Dopplerenergy signal over the standard detection applied directly onthe Doppler energy signal
5 Discussion
The results obtained were clear The methods based on HOSoverpassed by far the standard method based on the second-order statistics The reason explaining such superiority liesin the HOS sensitivity in modifying the distribution formKnowing that the occurrence of a microembolus superim-posed on the Doppler energy signal imposes changes in thedistribution of this signal we propose to use the skewnessand kurtosis as new tools for microembolus detectionDuring embolus-free periods the Doppler energy signalsrsquodistribution is fixed and its skewness and kurtosis are neveraltered They do not show any variations However in thepresence of a microembolus superimposed on the energysignal the skewness and kurtosis signals are altered andthe embolus is attributed with a peak whose peakednesslevel is higher than all the other points of the signal Thisdetection can outperform standard methods After beingtested on a set of real signals the skewness and kurtosis baseddetection offered significant improvements including very
Computational and Mathematical Methods in Medicine 7
high specificity reaching up to 91 and 90 respectivelycompared to 60 achieved by the standard method Inaddition the sensitivity is increased from 65 for standardmethods to 78 and 80 for skewness and kurtosis baseddetectors respectively
Consequently we can affirm that skewness and kurtosiscan offer a robust and more reliable detection than standarddetection methods and thus can be considered as newtechniques for enhancing microembolic detection systems
In view of the fact that we have proposed 2 detectorsone based on skewness detection and the other on kurtosisdetection it is convenient to give note that the two detectorsperform very similarly and yield very close results The onlydifference that could be observed is that the kurtosis signaldisplays small fluctuations around the embolic peak detectedwhile the skewness signal fluctuatesmore strongly around theembolic peaks This provides the kurtosis detection with asmall advantage in terms of the detection thresholdwhich canbe more easily and robustly set
6 Conclusion
In this research study we propose two detectors based onthe calculation of the skewness and kurtosis of the Dopplerenergy signal as a tool for an enhanced cerebral microem-bolus detection Compared to the standard detector wherethe detection is performed directly on the energy signal theskewness and kurtosis based detectors allow increasing ofboth the sensitivity and the specificity
This study emphasizes that standard microembolicenergy detectors with empirical threshold still pose seriousdifficulties for the robust detection of microemboli It alsoshows that detectors incorporating detection based on skew-ness and kurtosis calculation from the energy allow a muchadvanced detection of microemboli precursors of cominglarge emboli with strong stroke risksThus using these simpleand straightforward detectors would be an additional facilityboosting the efforts to reduce the occurrence of strokes
The upcoming step would be attempting to increase theoverall performance of the techniques particularly in termsof sensitivity and validating the developed algorithms on alarger database Moreover we are on course of includingin the whole detection system automatic artifact rejectiontechniques rather than using manual techniques
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This research was financially supported by the DoctoralSchool of Sciences and Technology Lebanese UniversityLebanon the National Council for Scientific Research CNRSLebanon and the French Institute of Health and MedicalResearch INSERM France The authors would like to sin-cerely thankMarilys Almar and Benoit Guibert for theHolter
TCD equipmentThey also acknowledge Corinne Gautier forthe Holter Doppler recordings
References
[1] B Murtagh and R W Smalling ldquoCardioembolic strokerdquo Cur-rent Atherosclerosis Reports vol 8 no 4 pp 310ndash316 2006
[2] P M Morse and K U Ingard Theoretical Acoustics PrincetonUniversity Press Princeton NJ USA 1968
[3] H Markus M Cullinane and G Reid ldquoImproved automateddetection of embolic signals using a novel frequency filteringapproachrdquo Stroke vol 30 no 8 pp 1610ndash1615 1999
[4] H S Markus and G Reid ldquoFrequency filtering improvesultrasonic embolic signal detectionrdquo Ultrasound in Medicine ampBiology vol 25 no 5 pp 857ndash860 1999
[5] M Cullinane G Reid R Dittrich et al ldquoEvaluation of newonline automated embolic signal detection algorithm includingcomparison with panel of international expertsrdquo Stroke vol 31no 6 pp 1335ndash1341 2000
[6] M Cullinane Z Kaposzta S Reihill andH S Markus ldquoOnlineautomated detection of cerebral embolic signals from a varietyof embolic sourcesrdquo Ultrasound in Medicine amp Biology vol 28no 10 pp 1271ndash1277 2002
[7] J-M Girault D Kouame A Ouahabi and F Patat ldquoMicro-emboli detection an ultrasound doppler signal processingviewpointrdquo IEEE Transactions on Biomedical Engineering vol47 no 11 pp 1431ndash1439 2000
[8] S Marvasti D Gillies F Marvasti and H S Markus ldquoOnlineautomated detection of cerebral embolic signals using awavelet-based systemrdquo Ultrasound in Medicine amp Biology vol30 no 5 pp 647ndash653 2004
[9] L Fan D H Evans and A R Naylor ldquoAutomated embolusidentification using a rule-based expert systemrdquo Ultrasound inMedicine amp Biology vol 27 no 8 pp 1065ndash1077 2001
[10] N Aydin F Marvasti and H S Markus ldquoEmbolic Dopplerultrasound signal detection using discrete wavelet transformrdquoIEEE Transactions on Information Technology in Biomedicinevol 8 no 2 pp 182ndash190 2004
[11] Y Chen and Y Wang ldquoDoppler embolic signal detection usingthe adaptive wavelet packet basis and neurofuzzy classificationrdquoPattern Recognition Letters vol 29 no 10 pp 1589ndash1595 2008
[12] M Gencer G Bilgin and N Aydin ldquoEmbolic Doppler ultra-sound signal detection via fractional Fourier transformrdquo inProceedings of the 2013 35th Annual International Conference ofthe IEEE Engineering in Medicine and Biology Society (EMBCrsquo13) pp 3050ndash3053 Osaka Japan July 2013
[13] C Lueang-On C Tantibundhit and S MuengtaweepongsaldquoProcessing time improvement for automatic embolic signaldetection using fuzzy c-meanrdquo in Proceedings of the 10thInternational Conference on Electrical EngineeringElectronicsComputer Telecommunications and Information Technology(ECTI-CON rsquo13) pp 1ndash5 IEEE Krabi Thailand May 2013
[14] J-M Girault and Z Zhao ldquoSynchronous detector as a newparadigm for automaticmicroembolus detectionrdquo InternationalJournal of Biomedical Engineering and Technology vol 14 no 1pp 60ndash70 2014
[15] S Menigot L Dreibine N Meziati and J-M Girault ldquoAuto-matic detection of microemboli by means of a synchronouslinear prediction techniquerdquo in Proceedings of the IEEE Inter-national Ultrasonics Symposium (IUS rsquo09) pp 2371ndash2374 IEEERome Italy September 2009
8 Computational and Mathematical Methods in Medicine
[16] N Aydin and H S Markus ldquoOptimization of processingparameters for the analysis and detection of embolic signalsrdquoEuropean Journal of Ultrasound vol 12 no 1 pp 69ndash79 2000
[17] E B Ringelstein DW Droste V L Babikian et al ldquoConsensuson microembolus detection by TCDrdquo Stroke vol 29 no 3 pp725ndash729 1998
[18] J-M Girault ldquoCerebral microembolism synchronous detectionwith wavelet packetsrdquo in Signal and Image MultiresolutionAnalysis chapter 4 pp 245ndash287 John Wiley amp Sons 2013
[19] E Chung L Fan C Degg and D H Evans ldquoDetectionof Doppler embolic signals psychoacoustic considerationsrdquoUltrasound in Medicine amp Biology vol 31 no 9 pp 1177ndash11842005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Computational and Mathematical Methods in Medicine
most punctual methods Frequency filtering methods wereintroduced in [3 4]The study reported high detection sensi-tivity and specificity rates Subsequently an online automatedembolic signal detection algorithm based on frequency fil-tering was developed in [5 6] The latter system showedhigh performances in terms of sensitivity and specificity forparticular cases (postcarotid endarterectomy) However inother conditions (atrial fibrillation) the systemrsquos sensitivityand specificity severely decreasedMoreover the systemrsquos per-formance in the detection of low energymicroembolic signalswas arguably less efficient with much lower sensitivity andspecificity Methods based on detection of sudden changeswere introduced in [7] Nonparametric detection methodsmainly the Fourier Wigner-Ville and wavelet approacheswere compared to parametric autoregressive methods Thenew parametric methods were proven to be highly perfor-mant and efficient in the detection of small microemboliHowever the methods were tested on synthetic simulatedDoppler signals and never on a set of real signals Anotherhighly productive wavelet-based system was established in[8] The system achieved a high combination of sensitivityand specificity However the systemrsquos rates decreased in thecase of low energymicroembolic signals A remarkable offlinedetection was proposed in [9] The system had excellentperformance for emboli having high intensities relative tobackground blood clutter However it is to be noticed thatthe study did not take into consideration the detection ofweak embolic signalsThe authors in [10] introduced anotherhighly achieving detection procedure based on the discretewavelet transform (DWT) DWT allowed major increases inspecificity and sensitivity Nonetheless a major deficiencyof the DWT implementation was the reduced frequencyresolution at low frequency scales in which embolic signalsare mostly found In [11] the authors proposed embolicdetection using the adaptive wavelet packet basis and neu-rofuzzy classification The adaptive wavelet packet basis wasused to make a sparse representation of Doppler ultrasoundblood flow signals The method produced highly accurateand robust performances However when compared to othermethods only the sensitivity was taken into account and thecorrelated specificity was not calculatedThe study submittedin [12] requested the use of Fractional Fourier Transformrather than the short time Fourier transform the standardmethod of detection in TCD systemsThe results showed thatdiscriminating parameters based on the Fractional FourierTransform help easier analysis and detection of embolicsignals Despite its simplicity and acceptable results thismethodwas not proven reliably decent for the detection of thesmallest microemboliThemethod proposed in [13] achievedvery high sensitivity and specificity but large detection errorsoccurred due to small gaseous emboli exhibiting smallreflected signals
In most articles previously introduced the main limi-tation lies in the fact that the information on which thedetection takes place is time-varyingwhile the threshold usedis constant To match between the time-varying informationand the threshold two solutions can be proposed The first isproposing a time-varying threshold as in [14 15] thatmatchesthe time-varying trend of the decision information Second
is proposing a constant threshold that matches the decisioninformation for which the time-varying trend is removed
In this work the methods we proposed of matchingbetween a constant threshold and an energy free of itstime-varying trend are based on the use of high orderstatistic (HOS) of windowed Doppler energy signal Wetend to prove the skewness and kurtosis as two solid meansto detect microembolic signals when asymptomatic caroidartery patients are monitored with a Holter TCD
2 The Offline Microembolic Detection Unit
As previously mentioned our objective is to perceive amicroemboli detector more sensitive and robust regardingmost standard detectors
In this study the typical offline signal processing unit isdecomposed into 3 units
(i) Unit A allocated for loading the wave file 10-secondsignal segmentation short time Fourier transform(STFT) calculation and instantaneous energy calcu-lation from the STFT
(ii) Unit B allocated for standard energy detection on theenergy signal obtained in Unit A
(iii) Unit C allocated for the new energy detection tech-niques based on skewness and kurtosis calculation ofthe energy signal obtained in Unit A
21 Unit A Doppler Signal Extraction STFT and Instan-taneous Energy Calculation The different systems that wewant to test depicted in Figure 1 share a common structureFrom the SD card plugged out from the Holter system andplugged into the personal computer the Doppler signal ispicked up and put in memory From this Doppler digitalsignal the short time Fourier transform is calculated firstto display the spectrogram and second to estimate instanta-neously the Doppler energy Calculations of the STFT andthe instantaneous energy are carried out repetitively on 10-second segments extracted from the Doppler signal
Most commercial TCD ultrasound systems are based onthe short time Fourier transform The short time Fouriertransform is an adapted form of the Fourier transform thatanalyzes only a small segment of the signal at a time atechnique called windowing of the signal or also WindowedFourier Transform (WFT) Short time Fourier transform isused when the Doppler signal within the analyzing windowis stationary In reality transforming data into the frequencydomain results in loss of time information By applying theFourier transform of a signal it is impossible to identifywhen a particular event takes place The STFT was thusproposed to correct this deficiency The STFT maps a signalinto a two-dimensional function of time and frequency Thisrepresentation is known as the spectrogram
The STFT frequency estimator with a sliding window canbe formally written as follows
119878 (119905 119891) = 1003816100381610038161003816100381610038161003816int 119909 (120591) 119908lowast (119905 minus 120591) expminus11989521205871198911199051198891205911003816100381610038161003816100381610038161003816
2
(1)
Computational and Mathematical Methods in Medicine 3
SD card memory
Instantaneous energy estimator
Standard energydetector
Automaticcounter 1
New energy detector
Automaticcounter 3
Constant empiricalthreshold estimation
Number of embolicdetections Output 1
Output 2
Input
Automaticcounter 2
Skewnesscalculation
Kurtosiscalculation
Number of embolicdetections
Output 3
Data-basedthreshold estimation
Number of embolicdetections
Data-basedthreshold estimation
Unit A
Unit BUnit C
STFT (10ms)
Extraction of a digital sequence (10 s)
Figure 1 A typical embolus detection system including standard detection and our new detection procedure Unit A includes extracting 10 sdigital Doppler signal sequences from the SD card extracted from the Holter system calculating the short time Fourier transform and lastlycalculating the instantaneous energy from STFT estimators Unit B represents the detection achieved using standard methods while Unit Crepresents the new detection procedure we have developed based on skewness and kurtosis calculation
where 119909(119905) is the analyzed Doppler signal 119908(119905) is a slidingwindow and lowast stands for complex conjugation
When using the STFT to process embolic signals itis of great importance that the STFT parameters are opti-mized The three processing parameters are the window sizethe window type and the overlap ratio Despite the factthat setting the parameters significantly affects the embolusdetection system based on STFT calculations little work onthe effect of the different parameters has been reported Afundamental work was reported in [16] The authors evalu-ated the effect of varying the three parameters on embolicsignal temporal and frequency resolutions time of embolicsignal onset and the power of the embolus at the frequencywith maximum power relative to the average power of thebackground intensity Based on [16] and after a preliminarystage of experimental optimization of the STFT parametersthe STFT in this study is performed using a 146-millisecondHamming window with an overlap of 65
The instantaneous energy at a fixed time 119905 can be obtainedfrom STFT frequency estimators in (1) by
119890 (119905) = int 119878 (119905 119891) 119889119891 (2)
Note that the energy returned by a microembolus wouldbe greater than that returned by billions of red blood cells(RBCs) since a microembolus is often larger than RBCsHence the backscattered energy would function as a solid
indicator from which the presence of embolic and microem-bolic signatures could be detected This justifies why mostdetectors are chosen to be mainly based on energy criteria
22 Unit B Standard Microembolic Detection The standarddetection methods to which we compare the new proposedmethods are based on a direct detection of the embolicsignatures in the energy signal An empirical thresholdis commonly used This constant threshold can be fixedempirically by the trained user for the entire examination Itis patient- operator- and device-dependent This thresholdis set above the maximal background energy of the Dopplersignal when no embolus is present [17] that is the systolicpeak The microembolic standard detection based on aconstant threshold is represented in Figure 2(a)
The main limitation of using such method resides incomparing the energy which is time-varying to a constantthreshold To match between the time-varying trend of theenergy and the threshold two solutions can be proposedeither a time-varying threshold as in [14 15 18] that matchesthe time-varying trend of the decision information or aconstant threshold that matches the energy while removingthe time-varying trend
23 Unit C Skewness and Kurtosis Based Microembolic Detec-tion As previously mentioned it is a threshold-orienteddetection As shown in Figure 2 weak embolic events are
4 Computational and Mathematical Methods in Medicine
120583 HITS 120583 HITS 120583 HITS
1 2 3 4 5 6 7 8 9 100Time (s)
002040608
1
Dop
pler
ener
gy
(a)
07
120583 HITS120583 HITS120583 HITS
t1 t2 t31 2 3 4 5 6 7 8 9 100Time (s)
0123456
Skew
ness
(b)
32
120583 HITS 120583 HITS 120583 HITS
t1 t2 t31 2 3 4 5 6 7 8 9 100Time (s)
0
5
10
15
Kurt
osis
(c)
Figure 2 (a)TheDoppler energy signal An empirical threshold is applied to obtain themicroembolic standard detection (b) Skewness signalcalculated from the windowed energy signal A data-based threshold is applied to complete the microembolic detection The mean value ofthe skewness signal is 07 (c) Kurtosis signal calculated from the windowed energy signal A data-based threshold is applied to complete themicroembolic detection The mean value of the kurtosis signal is 32 Moreover we choose in (b) and (c) three time positions 1199051 = 072 sduring which an embolus is present and 1199052 = 47 s and 1199053 = 88 s when no embolus is present We detect in the case of absence of embolus119878(1199052) asymp 119878(1199053) asymp 07 and119870(1199052) asymp 119870(1199053) asymp 32 while in the presence of embolus we detect 119878(1199051) = 28 = 119878(1199053) asymp 07 and119870(1199051) = 11 = 119870(1199053) asymp 32
impossible to detect with a constant threshold One wayto overcome this issue is to remove the time-varying trendin the instantaneous Doppler energy To prove that highorder statistics such as the skewness and the kurtosis aresuitable candidates to overcome this limitation consider aDoppler signal free of microembolic events and assume thatthe statistical distribution remains unchanged whatever thetime position is even if the mean 120583119894(119905) and the variance1205901198942(119905) vary with time Suppose there exists two Gaussianrandom variables 119883(1199052) = 119873(1205831(1199052) 1205901(1199052)) and 119883(1199053) =119873(1205832(1199053) 1205902(1199053)) It can be shown for the skewness 119878 that119878(1199052) = 119878(119883(1199052)) = 119878(119883(1199053)) = 0 and for the kurtosis 119870that 119870(1199052) = 119870(119883(1199052)) = 119870(119883(1199053)) = 3 In this example theskewness and the kurtosis are stationary since 119878(119905) = 0 and119870(119905) = 3 for all 119905 This outcome can be verified whatever thedistribution form while it remains unchanged over all timevalues The only change occurs in the value of the skewnessand the kurtosis but not in their stationarity Consequentlywhen a microembolic event occurs at a time position 1199051 thedistribution changes The direct consequence is 119878(1199051) = 119878(1199052)and119870(1199051) = 119870(1199052)
Therefore we can propose a new detector based oncalculating the skewness and kurtosis from the energy signalThe calculations are performed using a sliding window 119892(119905)where the optimal window length and overlap ratio are setduring a training phase (see Results section)
The skewness is the third-order standardized momentWhen calculated instantaneously (by the sliding window) onthe energy it is given by the following equation
119878 (119905) = 119864 [119890 (119905) minus 120583119890 (119905)]3
120590119890 (119905)3 (3)
The kurtosis is the fourth-order standardized momentWhen calculated instantaneously on the energy it is given bythe following equation
119870 (119905) = 119864 [119890 (119905) minus 120583119890 (119905)]4
120590119890 (119905)4 (4)
where 120583119890(119905) and 120590119890(119905) are the instantaneous mean and stan-dard deviation of the energy while 119864[] denotes the expectedvalue
Computational and Mathematical Methods in Medicine 5
(a) (b)
Figure 3 (a) Robot probe and (b) Holter Transcranial Doppler System (TCD-X Atys Medical Soucieu en Jarrest France)
The microembolic detection based on the skewness andkurtosis signals is represented in Figures 2(b) and 2(c)
In order to complete the detection on the skewnessand kurtosis signals a threshold has to be set in order topick up the peak signals We decided to establish a data-based threshold for the skewness and kurtosis signals fromtheir respective means 120583119904 and 120583119896 and respective standarddeviations 120590119904 and 120590119896 This threshold is defined as 120582119904 =120583119904 + 119898120590119904 for skewness and 120582119896 = 120583119896 + 119898120590119896 for kurtosiswhere 119898 is a parameter whose value is adjusted using anoptimization training phase in a manner that increases thesystemrsquos sensitivity and specificity (refer to Results section)The thresholds are represented in Figures 2(b) and 2(c)
3 The Holter System and the Protocol
TCD is a noninvasive nonionizing inexpensive portableand safe technique which renders it as a convenient toolfor the detection of cerebral microemboli Long time probepositioning and the short effective examination durationare the main limitations of traditional TCD systems TheTranscranial Holter (TCD-X Atys Medical Soucieu en Jar-rest France) shown in Figure 3 allows prolonged patientmonitoring (higher than 5 hours) with the patient no longerattached to a TCD and does not need to be laying on a bedbut rather can be monitored under naturalistic conditionsTheHolter is equipped with a robotized automatic probe thathelps find the best TCD signal and tracks it automaticallyduring the whole recording
A database obtained from the Centre HospitalierRegional Universitaire (CHRU) de Lille (2 Avenue OscarLambret 59000 Lille France) is used Informed consent for
Holter monitoring was obtained from all monitored patientsThe recordings were acquired from the middle cerebralartery of the patients The ultrasonic wave frequency was15MHz the pulse repetition frequency (PRF) was 64 kHzand the ultrasound power was 50mWcm2
After the clinical examination an analogous conversion isperformed on theDoppler digital signal and then theDopplersignal is sent to a loudspeaker From the audible Dopplersignal and from the spectrogram displayed on a screen wedetect and count manually the number of microembolicevents in order to constitute our gold standard of detectionThe gold standard is subject to interagreement betweenthree experts of our laboratory Then the positions in timeof audibly and visually agreed-on microembolic events arenoted This gold standard is used to assess the results ofthe different detectors used and validate their performancesAlthough the gold standard detections obtained from expertsand nonexperts might be the same as stated in [19] theexperience of the latter experts was useful to distinguishbetween microembolic signals and artifact signals discussednext We should also point out that listening to the audiofiles is made at the normal playing speed and another time athalf the normal speed which allows us to detect microembolipreviously inaudible due to the well-known temporal andfrequency masking effects in audio files
4 Results
The different detectors are tested through algorithms wedeveloped using the numerical calculation software Matlab(Mathworks Natick MA USA) Our database is composedof 18 recorded signals divided into two categories The first
6 Computational and Mathematical Methods in Medicine
Table 1 Training phase results of the optimal thresholds that best maximize the sensitivity and specificity for the standard energy detectorand skewness and kurtosis based detectors
Optimal threshold that maximizes the sensitivity and specificity Sensitivity () Specificity ()Standard energy detector 5 dB 67 58Skewness detector 120582119904 = 120583119904 + 4120590119904 76 91Kurtosis detector 120582119896 = 120583119896 + 5120590119896 77 91
Table 2 Results (sensitivity and specificity) for the standard energy detector and the new detectors based on skewness and kurtosiscalculations of the Doppler energy signal
Detector type True positive False positive Sensitivity () Specificity ()Gold standard detections = 136Standard detection 88 58 65 60Skewness detection 106 10 78 91Kurtosis detection 109 12 80 90
is the training phase (8 signals) dedicated to determining thebest settings of the detectors used The second is the testingphase (10 signals) dedicated to assessing the performances ofthe detectors used under the optimal settings determined inthe training phase
Two parameters are used to evaluate the detectors
(i) Sensitivity (or Detection Rate) calculated as the num-ber of true positive detectionsthe number of goldstandard detections True positive detection refers tothe detection of an embolus recorded in the goldstandard
(ii) Specificity calculated as 1 minus False Alarm Rate (FAR)the latter being the number of false positive detec-tionsthe total number of detections False positivedetection refers to the detection of an embolus notrecorded in the gold standard or in other words anembolus which has not crossed the sample volume
41 Training Phase Results Since the threshold applied on theenergy signal to achieve the standard detection is empiricallyset through the choice of the user different microembolicdetections could be obtained To overcome this we initializea training phase to preset the best empirical threshold tobe used in the testing phase 3 to 9 dB values are usedTable 1 shows the empirical threshold that best maximizes thesensitivity and specificity
Moreover since the skewness and kurtosis calculationsare performed using a sliding window 119892(119905) on the energysignal an experimental test on the training phase signals isinitialized to determine the optimal length of thewindow119892(119905)and the optimal overlap ratio The optimal temporal windowlength is 73milliseconds and the optimal overlap used is 95Also using these settings we test in the training phase the bestdata-based threshold 120582119904 = 120583119904 + 119898120590119904 and 120582119896 = 120583119896 + 119898120590119896 forthe skewness and kurtosis signals respectively Values of 119898ranging between 3 and 7 are tested Table 1 shows the data-based threshold for the skewness and kurtosis signals thatbest maximizes the sensitivity and specificity
42 Testing Phase Results Table 2 represents the testingphase results for the three different energy detectors Forthe standard energy detector with empirical threshold thesensitivity is 65 and the specificity is 60 For the energydetector based on skewness calculation the sensitivity is 78and the specificity is 91 For the energy detector based onkurtosis calculation the sensitivity is 80 and the specificityis 90
The results presented show that the new detectors areable to significantly increase the specificity compared tostandard detection (more than 30) Moreover the sensi-tivity achieved by the new detectors is increased by 13for the skewness detector and 15 for the kurtosis detectorcompared to that achieved by standard detectors Theseresults assert the accuracy and superiority of the detectionbased on skewness and kurtosis calculation of the Dopplerenergy signal over the standard detection applied directly onthe Doppler energy signal
5 Discussion
The results obtained were clear The methods based on HOSoverpassed by far the standard method based on the second-order statistics The reason explaining such superiority liesin the HOS sensitivity in modifying the distribution formKnowing that the occurrence of a microembolus superim-posed on the Doppler energy signal imposes changes in thedistribution of this signal we propose to use the skewnessand kurtosis as new tools for microembolus detectionDuring embolus-free periods the Doppler energy signalsrsquodistribution is fixed and its skewness and kurtosis are neveraltered They do not show any variations However in thepresence of a microembolus superimposed on the energysignal the skewness and kurtosis signals are altered andthe embolus is attributed with a peak whose peakednesslevel is higher than all the other points of the signal Thisdetection can outperform standard methods After beingtested on a set of real signals the skewness and kurtosis baseddetection offered significant improvements including very
Computational and Mathematical Methods in Medicine 7
high specificity reaching up to 91 and 90 respectivelycompared to 60 achieved by the standard method Inaddition the sensitivity is increased from 65 for standardmethods to 78 and 80 for skewness and kurtosis baseddetectors respectively
Consequently we can affirm that skewness and kurtosiscan offer a robust and more reliable detection than standarddetection methods and thus can be considered as newtechniques for enhancing microembolic detection systems
In view of the fact that we have proposed 2 detectorsone based on skewness detection and the other on kurtosisdetection it is convenient to give note that the two detectorsperform very similarly and yield very close results The onlydifference that could be observed is that the kurtosis signaldisplays small fluctuations around the embolic peak detectedwhile the skewness signal fluctuatesmore strongly around theembolic peaks This provides the kurtosis detection with asmall advantage in terms of the detection thresholdwhich canbe more easily and robustly set
6 Conclusion
In this research study we propose two detectors based onthe calculation of the skewness and kurtosis of the Dopplerenergy signal as a tool for an enhanced cerebral microem-bolus detection Compared to the standard detector wherethe detection is performed directly on the energy signal theskewness and kurtosis based detectors allow increasing ofboth the sensitivity and the specificity
This study emphasizes that standard microembolicenergy detectors with empirical threshold still pose seriousdifficulties for the robust detection of microemboli It alsoshows that detectors incorporating detection based on skew-ness and kurtosis calculation from the energy allow a muchadvanced detection of microemboli precursors of cominglarge emboli with strong stroke risksThus using these simpleand straightforward detectors would be an additional facilityboosting the efforts to reduce the occurrence of strokes
The upcoming step would be attempting to increase theoverall performance of the techniques particularly in termsof sensitivity and validating the developed algorithms on alarger database Moreover we are on course of includingin the whole detection system automatic artifact rejectiontechniques rather than using manual techniques
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This research was financially supported by the DoctoralSchool of Sciences and Technology Lebanese UniversityLebanon the National Council for Scientific Research CNRSLebanon and the French Institute of Health and MedicalResearch INSERM France The authors would like to sin-cerely thankMarilys Almar and Benoit Guibert for theHolter
TCD equipmentThey also acknowledge Corinne Gautier forthe Holter Doppler recordings
References
[1] B Murtagh and R W Smalling ldquoCardioembolic strokerdquo Cur-rent Atherosclerosis Reports vol 8 no 4 pp 310ndash316 2006
[2] P M Morse and K U Ingard Theoretical Acoustics PrincetonUniversity Press Princeton NJ USA 1968
[3] H Markus M Cullinane and G Reid ldquoImproved automateddetection of embolic signals using a novel frequency filteringapproachrdquo Stroke vol 30 no 8 pp 1610ndash1615 1999
[4] H S Markus and G Reid ldquoFrequency filtering improvesultrasonic embolic signal detectionrdquo Ultrasound in Medicine ampBiology vol 25 no 5 pp 857ndash860 1999
[5] M Cullinane G Reid R Dittrich et al ldquoEvaluation of newonline automated embolic signal detection algorithm includingcomparison with panel of international expertsrdquo Stroke vol 31no 6 pp 1335ndash1341 2000
[6] M Cullinane Z Kaposzta S Reihill andH S Markus ldquoOnlineautomated detection of cerebral embolic signals from a varietyof embolic sourcesrdquo Ultrasound in Medicine amp Biology vol 28no 10 pp 1271ndash1277 2002
[7] J-M Girault D Kouame A Ouahabi and F Patat ldquoMicro-emboli detection an ultrasound doppler signal processingviewpointrdquo IEEE Transactions on Biomedical Engineering vol47 no 11 pp 1431ndash1439 2000
[8] S Marvasti D Gillies F Marvasti and H S Markus ldquoOnlineautomated detection of cerebral embolic signals using awavelet-based systemrdquo Ultrasound in Medicine amp Biology vol30 no 5 pp 647ndash653 2004
[9] L Fan D H Evans and A R Naylor ldquoAutomated embolusidentification using a rule-based expert systemrdquo Ultrasound inMedicine amp Biology vol 27 no 8 pp 1065ndash1077 2001
[10] N Aydin F Marvasti and H S Markus ldquoEmbolic Dopplerultrasound signal detection using discrete wavelet transformrdquoIEEE Transactions on Information Technology in Biomedicinevol 8 no 2 pp 182ndash190 2004
[11] Y Chen and Y Wang ldquoDoppler embolic signal detection usingthe adaptive wavelet packet basis and neurofuzzy classificationrdquoPattern Recognition Letters vol 29 no 10 pp 1589ndash1595 2008
[12] M Gencer G Bilgin and N Aydin ldquoEmbolic Doppler ultra-sound signal detection via fractional Fourier transformrdquo inProceedings of the 2013 35th Annual International Conference ofthe IEEE Engineering in Medicine and Biology Society (EMBCrsquo13) pp 3050ndash3053 Osaka Japan July 2013
[13] C Lueang-On C Tantibundhit and S MuengtaweepongsaldquoProcessing time improvement for automatic embolic signaldetection using fuzzy c-meanrdquo in Proceedings of the 10thInternational Conference on Electrical EngineeringElectronicsComputer Telecommunications and Information Technology(ECTI-CON rsquo13) pp 1ndash5 IEEE Krabi Thailand May 2013
[14] J-M Girault and Z Zhao ldquoSynchronous detector as a newparadigm for automaticmicroembolus detectionrdquo InternationalJournal of Biomedical Engineering and Technology vol 14 no 1pp 60ndash70 2014
[15] S Menigot L Dreibine N Meziati and J-M Girault ldquoAuto-matic detection of microemboli by means of a synchronouslinear prediction techniquerdquo in Proceedings of the IEEE Inter-national Ultrasonics Symposium (IUS rsquo09) pp 2371ndash2374 IEEERome Italy September 2009
8 Computational and Mathematical Methods in Medicine
[16] N Aydin and H S Markus ldquoOptimization of processingparameters for the analysis and detection of embolic signalsrdquoEuropean Journal of Ultrasound vol 12 no 1 pp 69ndash79 2000
[17] E B Ringelstein DW Droste V L Babikian et al ldquoConsensuson microembolus detection by TCDrdquo Stroke vol 29 no 3 pp725ndash729 1998
[18] J-M Girault ldquoCerebral microembolism synchronous detectionwith wavelet packetsrdquo in Signal and Image MultiresolutionAnalysis chapter 4 pp 245ndash287 John Wiley amp Sons 2013
[19] E Chung L Fan C Degg and D H Evans ldquoDetectionof Doppler embolic signals psychoacoustic considerationsrdquoUltrasound in Medicine amp Biology vol 31 no 9 pp 1177ndash11842005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Computational and Mathematical Methods in Medicine 3
SD card memory
Instantaneous energy estimator
Standard energydetector
Automaticcounter 1
New energy detector
Automaticcounter 3
Constant empiricalthreshold estimation
Number of embolicdetections Output 1
Output 2
Input
Automaticcounter 2
Skewnesscalculation
Kurtosiscalculation
Number of embolicdetections
Output 3
Data-basedthreshold estimation
Number of embolicdetections
Data-basedthreshold estimation
Unit A
Unit BUnit C
STFT (10ms)
Extraction of a digital sequence (10 s)
Figure 1 A typical embolus detection system including standard detection and our new detection procedure Unit A includes extracting 10 sdigital Doppler signal sequences from the SD card extracted from the Holter system calculating the short time Fourier transform and lastlycalculating the instantaneous energy from STFT estimators Unit B represents the detection achieved using standard methods while Unit Crepresents the new detection procedure we have developed based on skewness and kurtosis calculation
where 119909(119905) is the analyzed Doppler signal 119908(119905) is a slidingwindow and lowast stands for complex conjugation
When using the STFT to process embolic signals itis of great importance that the STFT parameters are opti-mized The three processing parameters are the window sizethe window type and the overlap ratio Despite the factthat setting the parameters significantly affects the embolusdetection system based on STFT calculations little work onthe effect of the different parameters has been reported Afundamental work was reported in [16] The authors evalu-ated the effect of varying the three parameters on embolicsignal temporal and frequency resolutions time of embolicsignal onset and the power of the embolus at the frequencywith maximum power relative to the average power of thebackground intensity Based on [16] and after a preliminarystage of experimental optimization of the STFT parametersthe STFT in this study is performed using a 146-millisecondHamming window with an overlap of 65
The instantaneous energy at a fixed time 119905 can be obtainedfrom STFT frequency estimators in (1) by
119890 (119905) = int 119878 (119905 119891) 119889119891 (2)
Note that the energy returned by a microembolus wouldbe greater than that returned by billions of red blood cells(RBCs) since a microembolus is often larger than RBCsHence the backscattered energy would function as a solid
indicator from which the presence of embolic and microem-bolic signatures could be detected This justifies why mostdetectors are chosen to be mainly based on energy criteria
22 Unit B Standard Microembolic Detection The standarddetection methods to which we compare the new proposedmethods are based on a direct detection of the embolicsignatures in the energy signal An empirical thresholdis commonly used This constant threshold can be fixedempirically by the trained user for the entire examination Itis patient- operator- and device-dependent This thresholdis set above the maximal background energy of the Dopplersignal when no embolus is present [17] that is the systolicpeak The microembolic standard detection based on aconstant threshold is represented in Figure 2(a)
The main limitation of using such method resides incomparing the energy which is time-varying to a constantthreshold To match between the time-varying trend of theenergy and the threshold two solutions can be proposedeither a time-varying threshold as in [14 15 18] that matchesthe time-varying trend of the decision information or aconstant threshold that matches the energy while removingthe time-varying trend
23 Unit C Skewness and Kurtosis Based Microembolic Detec-tion As previously mentioned it is a threshold-orienteddetection As shown in Figure 2 weak embolic events are
4 Computational and Mathematical Methods in Medicine
120583 HITS 120583 HITS 120583 HITS
1 2 3 4 5 6 7 8 9 100Time (s)
002040608
1
Dop
pler
ener
gy
(a)
07
120583 HITS120583 HITS120583 HITS
t1 t2 t31 2 3 4 5 6 7 8 9 100Time (s)
0123456
Skew
ness
(b)
32
120583 HITS 120583 HITS 120583 HITS
t1 t2 t31 2 3 4 5 6 7 8 9 100Time (s)
0
5
10
15
Kurt
osis
(c)
Figure 2 (a)TheDoppler energy signal An empirical threshold is applied to obtain themicroembolic standard detection (b) Skewness signalcalculated from the windowed energy signal A data-based threshold is applied to complete the microembolic detection The mean value ofthe skewness signal is 07 (c) Kurtosis signal calculated from the windowed energy signal A data-based threshold is applied to complete themicroembolic detection The mean value of the kurtosis signal is 32 Moreover we choose in (b) and (c) three time positions 1199051 = 072 sduring which an embolus is present and 1199052 = 47 s and 1199053 = 88 s when no embolus is present We detect in the case of absence of embolus119878(1199052) asymp 119878(1199053) asymp 07 and119870(1199052) asymp 119870(1199053) asymp 32 while in the presence of embolus we detect 119878(1199051) = 28 = 119878(1199053) asymp 07 and119870(1199051) = 11 = 119870(1199053) asymp 32
impossible to detect with a constant threshold One wayto overcome this issue is to remove the time-varying trendin the instantaneous Doppler energy To prove that highorder statistics such as the skewness and the kurtosis aresuitable candidates to overcome this limitation consider aDoppler signal free of microembolic events and assume thatthe statistical distribution remains unchanged whatever thetime position is even if the mean 120583119894(119905) and the variance1205901198942(119905) vary with time Suppose there exists two Gaussianrandom variables 119883(1199052) = 119873(1205831(1199052) 1205901(1199052)) and 119883(1199053) =119873(1205832(1199053) 1205902(1199053)) It can be shown for the skewness 119878 that119878(1199052) = 119878(119883(1199052)) = 119878(119883(1199053)) = 0 and for the kurtosis 119870that 119870(1199052) = 119870(119883(1199052)) = 119870(119883(1199053)) = 3 In this example theskewness and the kurtosis are stationary since 119878(119905) = 0 and119870(119905) = 3 for all 119905 This outcome can be verified whatever thedistribution form while it remains unchanged over all timevalues The only change occurs in the value of the skewnessand the kurtosis but not in their stationarity Consequentlywhen a microembolic event occurs at a time position 1199051 thedistribution changes The direct consequence is 119878(1199051) = 119878(1199052)and119870(1199051) = 119870(1199052)
Therefore we can propose a new detector based oncalculating the skewness and kurtosis from the energy signalThe calculations are performed using a sliding window 119892(119905)where the optimal window length and overlap ratio are setduring a training phase (see Results section)
The skewness is the third-order standardized momentWhen calculated instantaneously (by the sliding window) onthe energy it is given by the following equation
119878 (119905) = 119864 [119890 (119905) minus 120583119890 (119905)]3
120590119890 (119905)3 (3)
The kurtosis is the fourth-order standardized momentWhen calculated instantaneously on the energy it is given bythe following equation
119870 (119905) = 119864 [119890 (119905) minus 120583119890 (119905)]4
120590119890 (119905)4 (4)
where 120583119890(119905) and 120590119890(119905) are the instantaneous mean and stan-dard deviation of the energy while 119864[] denotes the expectedvalue
Computational and Mathematical Methods in Medicine 5
(a) (b)
Figure 3 (a) Robot probe and (b) Holter Transcranial Doppler System (TCD-X Atys Medical Soucieu en Jarrest France)
The microembolic detection based on the skewness andkurtosis signals is represented in Figures 2(b) and 2(c)
In order to complete the detection on the skewnessand kurtosis signals a threshold has to be set in order topick up the peak signals We decided to establish a data-based threshold for the skewness and kurtosis signals fromtheir respective means 120583119904 and 120583119896 and respective standarddeviations 120590119904 and 120590119896 This threshold is defined as 120582119904 =120583119904 + 119898120590119904 for skewness and 120582119896 = 120583119896 + 119898120590119896 for kurtosiswhere 119898 is a parameter whose value is adjusted using anoptimization training phase in a manner that increases thesystemrsquos sensitivity and specificity (refer to Results section)The thresholds are represented in Figures 2(b) and 2(c)
3 The Holter System and the Protocol
TCD is a noninvasive nonionizing inexpensive portableand safe technique which renders it as a convenient toolfor the detection of cerebral microemboli Long time probepositioning and the short effective examination durationare the main limitations of traditional TCD systems TheTranscranial Holter (TCD-X Atys Medical Soucieu en Jar-rest France) shown in Figure 3 allows prolonged patientmonitoring (higher than 5 hours) with the patient no longerattached to a TCD and does not need to be laying on a bedbut rather can be monitored under naturalistic conditionsTheHolter is equipped with a robotized automatic probe thathelps find the best TCD signal and tracks it automaticallyduring the whole recording
A database obtained from the Centre HospitalierRegional Universitaire (CHRU) de Lille (2 Avenue OscarLambret 59000 Lille France) is used Informed consent for
Holter monitoring was obtained from all monitored patientsThe recordings were acquired from the middle cerebralartery of the patients The ultrasonic wave frequency was15MHz the pulse repetition frequency (PRF) was 64 kHzand the ultrasound power was 50mWcm2
After the clinical examination an analogous conversion isperformed on theDoppler digital signal and then theDopplersignal is sent to a loudspeaker From the audible Dopplersignal and from the spectrogram displayed on a screen wedetect and count manually the number of microembolicevents in order to constitute our gold standard of detectionThe gold standard is subject to interagreement betweenthree experts of our laboratory Then the positions in timeof audibly and visually agreed-on microembolic events arenoted This gold standard is used to assess the results ofthe different detectors used and validate their performancesAlthough the gold standard detections obtained from expertsand nonexperts might be the same as stated in [19] theexperience of the latter experts was useful to distinguishbetween microembolic signals and artifact signals discussednext We should also point out that listening to the audiofiles is made at the normal playing speed and another time athalf the normal speed which allows us to detect microembolipreviously inaudible due to the well-known temporal andfrequency masking effects in audio files
4 Results
The different detectors are tested through algorithms wedeveloped using the numerical calculation software Matlab(Mathworks Natick MA USA) Our database is composedof 18 recorded signals divided into two categories The first
6 Computational and Mathematical Methods in Medicine
Table 1 Training phase results of the optimal thresholds that best maximize the sensitivity and specificity for the standard energy detectorand skewness and kurtosis based detectors
Optimal threshold that maximizes the sensitivity and specificity Sensitivity () Specificity ()Standard energy detector 5 dB 67 58Skewness detector 120582119904 = 120583119904 + 4120590119904 76 91Kurtosis detector 120582119896 = 120583119896 + 5120590119896 77 91
Table 2 Results (sensitivity and specificity) for the standard energy detector and the new detectors based on skewness and kurtosiscalculations of the Doppler energy signal
Detector type True positive False positive Sensitivity () Specificity ()Gold standard detections = 136Standard detection 88 58 65 60Skewness detection 106 10 78 91Kurtosis detection 109 12 80 90
is the training phase (8 signals) dedicated to determining thebest settings of the detectors used The second is the testingphase (10 signals) dedicated to assessing the performances ofthe detectors used under the optimal settings determined inthe training phase
Two parameters are used to evaluate the detectors
(i) Sensitivity (or Detection Rate) calculated as the num-ber of true positive detectionsthe number of goldstandard detections True positive detection refers tothe detection of an embolus recorded in the goldstandard
(ii) Specificity calculated as 1 minus False Alarm Rate (FAR)the latter being the number of false positive detec-tionsthe total number of detections False positivedetection refers to the detection of an embolus notrecorded in the gold standard or in other words anembolus which has not crossed the sample volume
41 Training Phase Results Since the threshold applied on theenergy signal to achieve the standard detection is empiricallyset through the choice of the user different microembolicdetections could be obtained To overcome this we initializea training phase to preset the best empirical threshold tobe used in the testing phase 3 to 9 dB values are usedTable 1 shows the empirical threshold that best maximizes thesensitivity and specificity
Moreover since the skewness and kurtosis calculationsare performed using a sliding window 119892(119905) on the energysignal an experimental test on the training phase signals isinitialized to determine the optimal length of thewindow119892(119905)and the optimal overlap ratio The optimal temporal windowlength is 73milliseconds and the optimal overlap used is 95Also using these settings we test in the training phase the bestdata-based threshold 120582119904 = 120583119904 + 119898120590119904 and 120582119896 = 120583119896 + 119898120590119896 forthe skewness and kurtosis signals respectively Values of 119898ranging between 3 and 7 are tested Table 1 shows the data-based threshold for the skewness and kurtosis signals thatbest maximizes the sensitivity and specificity
42 Testing Phase Results Table 2 represents the testingphase results for the three different energy detectors Forthe standard energy detector with empirical threshold thesensitivity is 65 and the specificity is 60 For the energydetector based on skewness calculation the sensitivity is 78and the specificity is 91 For the energy detector based onkurtosis calculation the sensitivity is 80 and the specificityis 90
The results presented show that the new detectors areable to significantly increase the specificity compared tostandard detection (more than 30) Moreover the sensi-tivity achieved by the new detectors is increased by 13for the skewness detector and 15 for the kurtosis detectorcompared to that achieved by standard detectors Theseresults assert the accuracy and superiority of the detectionbased on skewness and kurtosis calculation of the Dopplerenergy signal over the standard detection applied directly onthe Doppler energy signal
5 Discussion
The results obtained were clear The methods based on HOSoverpassed by far the standard method based on the second-order statistics The reason explaining such superiority liesin the HOS sensitivity in modifying the distribution formKnowing that the occurrence of a microembolus superim-posed on the Doppler energy signal imposes changes in thedistribution of this signal we propose to use the skewnessand kurtosis as new tools for microembolus detectionDuring embolus-free periods the Doppler energy signalsrsquodistribution is fixed and its skewness and kurtosis are neveraltered They do not show any variations However in thepresence of a microembolus superimposed on the energysignal the skewness and kurtosis signals are altered andthe embolus is attributed with a peak whose peakednesslevel is higher than all the other points of the signal Thisdetection can outperform standard methods After beingtested on a set of real signals the skewness and kurtosis baseddetection offered significant improvements including very
Computational and Mathematical Methods in Medicine 7
high specificity reaching up to 91 and 90 respectivelycompared to 60 achieved by the standard method Inaddition the sensitivity is increased from 65 for standardmethods to 78 and 80 for skewness and kurtosis baseddetectors respectively
Consequently we can affirm that skewness and kurtosiscan offer a robust and more reliable detection than standarddetection methods and thus can be considered as newtechniques for enhancing microembolic detection systems
In view of the fact that we have proposed 2 detectorsone based on skewness detection and the other on kurtosisdetection it is convenient to give note that the two detectorsperform very similarly and yield very close results The onlydifference that could be observed is that the kurtosis signaldisplays small fluctuations around the embolic peak detectedwhile the skewness signal fluctuatesmore strongly around theembolic peaks This provides the kurtosis detection with asmall advantage in terms of the detection thresholdwhich canbe more easily and robustly set
6 Conclusion
In this research study we propose two detectors based onthe calculation of the skewness and kurtosis of the Dopplerenergy signal as a tool for an enhanced cerebral microem-bolus detection Compared to the standard detector wherethe detection is performed directly on the energy signal theskewness and kurtosis based detectors allow increasing ofboth the sensitivity and the specificity
This study emphasizes that standard microembolicenergy detectors with empirical threshold still pose seriousdifficulties for the robust detection of microemboli It alsoshows that detectors incorporating detection based on skew-ness and kurtosis calculation from the energy allow a muchadvanced detection of microemboli precursors of cominglarge emboli with strong stroke risksThus using these simpleand straightforward detectors would be an additional facilityboosting the efforts to reduce the occurrence of strokes
The upcoming step would be attempting to increase theoverall performance of the techniques particularly in termsof sensitivity and validating the developed algorithms on alarger database Moreover we are on course of includingin the whole detection system automatic artifact rejectiontechniques rather than using manual techniques
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This research was financially supported by the DoctoralSchool of Sciences and Technology Lebanese UniversityLebanon the National Council for Scientific Research CNRSLebanon and the French Institute of Health and MedicalResearch INSERM France The authors would like to sin-cerely thankMarilys Almar and Benoit Guibert for theHolter
TCD equipmentThey also acknowledge Corinne Gautier forthe Holter Doppler recordings
References
[1] B Murtagh and R W Smalling ldquoCardioembolic strokerdquo Cur-rent Atherosclerosis Reports vol 8 no 4 pp 310ndash316 2006
[2] P M Morse and K U Ingard Theoretical Acoustics PrincetonUniversity Press Princeton NJ USA 1968
[3] H Markus M Cullinane and G Reid ldquoImproved automateddetection of embolic signals using a novel frequency filteringapproachrdquo Stroke vol 30 no 8 pp 1610ndash1615 1999
[4] H S Markus and G Reid ldquoFrequency filtering improvesultrasonic embolic signal detectionrdquo Ultrasound in Medicine ampBiology vol 25 no 5 pp 857ndash860 1999
[5] M Cullinane G Reid R Dittrich et al ldquoEvaluation of newonline automated embolic signal detection algorithm includingcomparison with panel of international expertsrdquo Stroke vol 31no 6 pp 1335ndash1341 2000
[6] M Cullinane Z Kaposzta S Reihill andH S Markus ldquoOnlineautomated detection of cerebral embolic signals from a varietyof embolic sourcesrdquo Ultrasound in Medicine amp Biology vol 28no 10 pp 1271ndash1277 2002
[7] J-M Girault D Kouame A Ouahabi and F Patat ldquoMicro-emboli detection an ultrasound doppler signal processingviewpointrdquo IEEE Transactions on Biomedical Engineering vol47 no 11 pp 1431ndash1439 2000
[8] S Marvasti D Gillies F Marvasti and H S Markus ldquoOnlineautomated detection of cerebral embolic signals using awavelet-based systemrdquo Ultrasound in Medicine amp Biology vol30 no 5 pp 647ndash653 2004
[9] L Fan D H Evans and A R Naylor ldquoAutomated embolusidentification using a rule-based expert systemrdquo Ultrasound inMedicine amp Biology vol 27 no 8 pp 1065ndash1077 2001
[10] N Aydin F Marvasti and H S Markus ldquoEmbolic Dopplerultrasound signal detection using discrete wavelet transformrdquoIEEE Transactions on Information Technology in Biomedicinevol 8 no 2 pp 182ndash190 2004
[11] Y Chen and Y Wang ldquoDoppler embolic signal detection usingthe adaptive wavelet packet basis and neurofuzzy classificationrdquoPattern Recognition Letters vol 29 no 10 pp 1589ndash1595 2008
[12] M Gencer G Bilgin and N Aydin ldquoEmbolic Doppler ultra-sound signal detection via fractional Fourier transformrdquo inProceedings of the 2013 35th Annual International Conference ofthe IEEE Engineering in Medicine and Biology Society (EMBCrsquo13) pp 3050ndash3053 Osaka Japan July 2013
[13] C Lueang-On C Tantibundhit and S MuengtaweepongsaldquoProcessing time improvement for automatic embolic signaldetection using fuzzy c-meanrdquo in Proceedings of the 10thInternational Conference on Electrical EngineeringElectronicsComputer Telecommunications and Information Technology(ECTI-CON rsquo13) pp 1ndash5 IEEE Krabi Thailand May 2013
[14] J-M Girault and Z Zhao ldquoSynchronous detector as a newparadigm for automaticmicroembolus detectionrdquo InternationalJournal of Biomedical Engineering and Technology vol 14 no 1pp 60ndash70 2014
[15] S Menigot L Dreibine N Meziati and J-M Girault ldquoAuto-matic detection of microemboli by means of a synchronouslinear prediction techniquerdquo in Proceedings of the IEEE Inter-national Ultrasonics Symposium (IUS rsquo09) pp 2371ndash2374 IEEERome Italy September 2009
8 Computational and Mathematical Methods in Medicine
[16] N Aydin and H S Markus ldquoOptimization of processingparameters for the analysis and detection of embolic signalsrdquoEuropean Journal of Ultrasound vol 12 no 1 pp 69ndash79 2000
[17] E B Ringelstein DW Droste V L Babikian et al ldquoConsensuson microembolus detection by TCDrdquo Stroke vol 29 no 3 pp725ndash729 1998
[18] J-M Girault ldquoCerebral microembolism synchronous detectionwith wavelet packetsrdquo in Signal and Image MultiresolutionAnalysis chapter 4 pp 245ndash287 John Wiley amp Sons 2013
[19] E Chung L Fan C Degg and D H Evans ldquoDetectionof Doppler embolic signals psychoacoustic considerationsrdquoUltrasound in Medicine amp Biology vol 31 no 9 pp 1177ndash11842005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Computational and Mathematical Methods in Medicine
120583 HITS 120583 HITS 120583 HITS
1 2 3 4 5 6 7 8 9 100Time (s)
002040608
1
Dop
pler
ener
gy
(a)
07
120583 HITS120583 HITS120583 HITS
t1 t2 t31 2 3 4 5 6 7 8 9 100Time (s)
0123456
Skew
ness
(b)
32
120583 HITS 120583 HITS 120583 HITS
t1 t2 t31 2 3 4 5 6 7 8 9 100Time (s)
0
5
10
15
Kurt
osis
(c)
Figure 2 (a)TheDoppler energy signal An empirical threshold is applied to obtain themicroembolic standard detection (b) Skewness signalcalculated from the windowed energy signal A data-based threshold is applied to complete the microembolic detection The mean value ofthe skewness signal is 07 (c) Kurtosis signal calculated from the windowed energy signal A data-based threshold is applied to complete themicroembolic detection The mean value of the kurtosis signal is 32 Moreover we choose in (b) and (c) three time positions 1199051 = 072 sduring which an embolus is present and 1199052 = 47 s and 1199053 = 88 s when no embolus is present We detect in the case of absence of embolus119878(1199052) asymp 119878(1199053) asymp 07 and119870(1199052) asymp 119870(1199053) asymp 32 while in the presence of embolus we detect 119878(1199051) = 28 = 119878(1199053) asymp 07 and119870(1199051) = 11 = 119870(1199053) asymp 32
impossible to detect with a constant threshold One wayto overcome this issue is to remove the time-varying trendin the instantaneous Doppler energy To prove that highorder statistics such as the skewness and the kurtosis aresuitable candidates to overcome this limitation consider aDoppler signal free of microembolic events and assume thatthe statistical distribution remains unchanged whatever thetime position is even if the mean 120583119894(119905) and the variance1205901198942(119905) vary with time Suppose there exists two Gaussianrandom variables 119883(1199052) = 119873(1205831(1199052) 1205901(1199052)) and 119883(1199053) =119873(1205832(1199053) 1205902(1199053)) It can be shown for the skewness 119878 that119878(1199052) = 119878(119883(1199052)) = 119878(119883(1199053)) = 0 and for the kurtosis 119870that 119870(1199052) = 119870(119883(1199052)) = 119870(119883(1199053)) = 3 In this example theskewness and the kurtosis are stationary since 119878(119905) = 0 and119870(119905) = 3 for all 119905 This outcome can be verified whatever thedistribution form while it remains unchanged over all timevalues The only change occurs in the value of the skewnessand the kurtosis but not in their stationarity Consequentlywhen a microembolic event occurs at a time position 1199051 thedistribution changes The direct consequence is 119878(1199051) = 119878(1199052)and119870(1199051) = 119870(1199052)
Therefore we can propose a new detector based oncalculating the skewness and kurtosis from the energy signalThe calculations are performed using a sliding window 119892(119905)where the optimal window length and overlap ratio are setduring a training phase (see Results section)
The skewness is the third-order standardized momentWhen calculated instantaneously (by the sliding window) onthe energy it is given by the following equation
119878 (119905) = 119864 [119890 (119905) minus 120583119890 (119905)]3
120590119890 (119905)3 (3)
The kurtosis is the fourth-order standardized momentWhen calculated instantaneously on the energy it is given bythe following equation
119870 (119905) = 119864 [119890 (119905) minus 120583119890 (119905)]4
120590119890 (119905)4 (4)
where 120583119890(119905) and 120590119890(119905) are the instantaneous mean and stan-dard deviation of the energy while 119864[] denotes the expectedvalue
Computational and Mathematical Methods in Medicine 5
(a) (b)
Figure 3 (a) Robot probe and (b) Holter Transcranial Doppler System (TCD-X Atys Medical Soucieu en Jarrest France)
The microembolic detection based on the skewness andkurtosis signals is represented in Figures 2(b) and 2(c)
In order to complete the detection on the skewnessand kurtosis signals a threshold has to be set in order topick up the peak signals We decided to establish a data-based threshold for the skewness and kurtosis signals fromtheir respective means 120583119904 and 120583119896 and respective standarddeviations 120590119904 and 120590119896 This threshold is defined as 120582119904 =120583119904 + 119898120590119904 for skewness and 120582119896 = 120583119896 + 119898120590119896 for kurtosiswhere 119898 is a parameter whose value is adjusted using anoptimization training phase in a manner that increases thesystemrsquos sensitivity and specificity (refer to Results section)The thresholds are represented in Figures 2(b) and 2(c)
3 The Holter System and the Protocol
TCD is a noninvasive nonionizing inexpensive portableand safe technique which renders it as a convenient toolfor the detection of cerebral microemboli Long time probepositioning and the short effective examination durationare the main limitations of traditional TCD systems TheTranscranial Holter (TCD-X Atys Medical Soucieu en Jar-rest France) shown in Figure 3 allows prolonged patientmonitoring (higher than 5 hours) with the patient no longerattached to a TCD and does not need to be laying on a bedbut rather can be monitored under naturalistic conditionsTheHolter is equipped with a robotized automatic probe thathelps find the best TCD signal and tracks it automaticallyduring the whole recording
A database obtained from the Centre HospitalierRegional Universitaire (CHRU) de Lille (2 Avenue OscarLambret 59000 Lille France) is used Informed consent for
Holter monitoring was obtained from all monitored patientsThe recordings were acquired from the middle cerebralartery of the patients The ultrasonic wave frequency was15MHz the pulse repetition frequency (PRF) was 64 kHzand the ultrasound power was 50mWcm2
After the clinical examination an analogous conversion isperformed on theDoppler digital signal and then theDopplersignal is sent to a loudspeaker From the audible Dopplersignal and from the spectrogram displayed on a screen wedetect and count manually the number of microembolicevents in order to constitute our gold standard of detectionThe gold standard is subject to interagreement betweenthree experts of our laboratory Then the positions in timeof audibly and visually agreed-on microembolic events arenoted This gold standard is used to assess the results ofthe different detectors used and validate their performancesAlthough the gold standard detections obtained from expertsand nonexperts might be the same as stated in [19] theexperience of the latter experts was useful to distinguishbetween microembolic signals and artifact signals discussednext We should also point out that listening to the audiofiles is made at the normal playing speed and another time athalf the normal speed which allows us to detect microembolipreviously inaudible due to the well-known temporal andfrequency masking effects in audio files
4 Results
The different detectors are tested through algorithms wedeveloped using the numerical calculation software Matlab(Mathworks Natick MA USA) Our database is composedof 18 recorded signals divided into two categories The first
6 Computational and Mathematical Methods in Medicine
Table 1 Training phase results of the optimal thresholds that best maximize the sensitivity and specificity for the standard energy detectorand skewness and kurtosis based detectors
Optimal threshold that maximizes the sensitivity and specificity Sensitivity () Specificity ()Standard energy detector 5 dB 67 58Skewness detector 120582119904 = 120583119904 + 4120590119904 76 91Kurtosis detector 120582119896 = 120583119896 + 5120590119896 77 91
Table 2 Results (sensitivity and specificity) for the standard energy detector and the new detectors based on skewness and kurtosiscalculations of the Doppler energy signal
Detector type True positive False positive Sensitivity () Specificity ()Gold standard detections = 136Standard detection 88 58 65 60Skewness detection 106 10 78 91Kurtosis detection 109 12 80 90
is the training phase (8 signals) dedicated to determining thebest settings of the detectors used The second is the testingphase (10 signals) dedicated to assessing the performances ofthe detectors used under the optimal settings determined inthe training phase
Two parameters are used to evaluate the detectors
(i) Sensitivity (or Detection Rate) calculated as the num-ber of true positive detectionsthe number of goldstandard detections True positive detection refers tothe detection of an embolus recorded in the goldstandard
(ii) Specificity calculated as 1 minus False Alarm Rate (FAR)the latter being the number of false positive detec-tionsthe total number of detections False positivedetection refers to the detection of an embolus notrecorded in the gold standard or in other words anembolus which has not crossed the sample volume
41 Training Phase Results Since the threshold applied on theenergy signal to achieve the standard detection is empiricallyset through the choice of the user different microembolicdetections could be obtained To overcome this we initializea training phase to preset the best empirical threshold tobe used in the testing phase 3 to 9 dB values are usedTable 1 shows the empirical threshold that best maximizes thesensitivity and specificity
Moreover since the skewness and kurtosis calculationsare performed using a sliding window 119892(119905) on the energysignal an experimental test on the training phase signals isinitialized to determine the optimal length of thewindow119892(119905)and the optimal overlap ratio The optimal temporal windowlength is 73milliseconds and the optimal overlap used is 95Also using these settings we test in the training phase the bestdata-based threshold 120582119904 = 120583119904 + 119898120590119904 and 120582119896 = 120583119896 + 119898120590119896 forthe skewness and kurtosis signals respectively Values of 119898ranging between 3 and 7 are tested Table 1 shows the data-based threshold for the skewness and kurtosis signals thatbest maximizes the sensitivity and specificity
42 Testing Phase Results Table 2 represents the testingphase results for the three different energy detectors Forthe standard energy detector with empirical threshold thesensitivity is 65 and the specificity is 60 For the energydetector based on skewness calculation the sensitivity is 78and the specificity is 91 For the energy detector based onkurtosis calculation the sensitivity is 80 and the specificityis 90
The results presented show that the new detectors areable to significantly increase the specificity compared tostandard detection (more than 30) Moreover the sensi-tivity achieved by the new detectors is increased by 13for the skewness detector and 15 for the kurtosis detectorcompared to that achieved by standard detectors Theseresults assert the accuracy and superiority of the detectionbased on skewness and kurtosis calculation of the Dopplerenergy signal over the standard detection applied directly onthe Doppler energy signal
5 Discussion
The results obtained were clear The methods based on HOSoverpassed by far the standard method based on the second-order statistics The reason explaining such superiority liesin the HOS sensitivity in modifying the distribution formKnowing that the occurrence of a microembolus superim-posed on the Doppler energy signal imposes changes in thedistribution of this signal we propose to use the skewnessand kurtosis as new tools for microembolus detectionDuring embolus-free periods the Doppler energy signalsrsquodistribution is fixed and its skewness and kurtosis are neveraltered They do not show any variations However in thepresence of a microembolus superimposed on the energysignal the skewness and kurtosis signals are altered andthe embolus is attributed with a peak whose peakednesslevel is higher than all the other points of the signal Thisdetection can outperform standard methods After beingtested on a set of real signals the skewness and kurtosis baseddetection offered significant improvements including very
Computational and Mathematical Methods in Medicine 7
high specificity reaching up to 91 and 90 respectivelycompared to 60 achieved by the standard method Inaddition the sensitivity is increased from 65 for standardmethods to 78 and 80 for skewness and kurtosis baseddetectors respectively
Consequently we can affirm that skewness and kurtosiscan offer a robust and more reliable detection than standarddetection methods and thus can be considered as newtechniques for enhancing microembolic detection systems
In view of the fact that we have proposed 2 detectorsone based on skewness detection and the other on kurtosisdetection it is convenient to give note that the two detectorsperform very similarly and yield very close results The onlydifference that could be observed is that the kurtosis signaldisplays small fluctuations around the embolic peak detectedwhile the skewness signal fluctuatesmore strongly around theembolic peaks This provides the kurtosis detection with asmall advantage in terms of the detection thresholdwhich canbe more easily and robustly set
6 Conclusion
In this research study we propose two detectors based onthe calculation of the skewness and kurtosis of the Dopplerenergy signal as a tool for an enhanced cerebral microem-bolus detection Compared to the standard detector wherethe detection is performed directly on the energy signal theskewness and kurtosis based detectors allow increasing ofboth the sensitivity and the specificity
This study emphasizes that standard microembolicenergy detectors with empirical threshold still pose seriousdifficulties for the robust detection of microemboli It alsoshows that detectors incorporating detection based on skew-ness and kurtosis calculation from the energy allow a muchadvanced detection of microemboli precursors of cominglarge emboli with strong stroke risksThus using these simpleand straightforward detectors would be an additional facilityboosting the efforts to reduce the occurrence of strokes
The upcoming step would be attempting to increase theoverall performance of the techniques particularly in termsof sensitivity and validating the developed algorithms on alarger database Moreover we are on course of includingin the whole detection system automatic artifact rejectiontechniques rather than using manual techniques
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This research was financially supported by the DoctoralSchool of Sciences and Technology Lebanese UniversityLebanon the National Council for Scientific Research CNRSLebanon and the French Institute of Health and MedicalResearch INSERM France The authors would like to sin-cerely thankMarilys Almar and Benoit Guibert for theHolter
TCD equipmentThey also acknowledge Corinne Gautier forthe Holter Doppler recordings
References
[1] B Murtagh and R W Smalling ldquoCardioembolic strokerdquo Cur-rent Atherosclerosis Reports vol 8 no 4 pp 310ndash316 2006
[2] P M Morse and K U Ingard Theoretical Acoustics PrincetonUniversity Press Princeton NJ USA 1968
[3] H Markus M Cullinane and G Reid ldquoImproved automateddetection of embolic signals using a novel frequency filteringapproachrdquo Stroke vol 30 no 8 pp 1610ndash1615 1999
[4] H S Markus and G Reid ldquoFrequency filtering improvesultrasonic embolic signal detectionrdquo Ultrasound in Medicine ampBiology vol 25 no 5 pp 857ndash860 1999
[5] M Cullinane G Reid R Dittrich et al ldquoEvaluation of newonline automated embolic signal detection algorithm includingcomparison with panel of international expertsrdquo Stroke vol 31no 6 pp 1335ndash1341 2000
[6] M Cullinane Z Kaposzta S Reihill andH S Markus ldquoOnlineautomated detection of cerebral embolic signals from a varietyof embolic sourcesrdquo Ultrasound in Medicine amp Biology vol 28no 10 pp 1271ndash1277 2002
[7] J-M Girault D Kouame A Ouahabi and F Patat ldquoMicro-emboli detection an ultrasound doppler signal processingviewpointrdquo IEEE Transactions on Biomedical Engineering vol47 no 11 pp 1431ndash1439 2000
[8] S Marvasti D Gillies F Marvasti and H S Markus ldquoOnlineautomated detection of cerebral embolic signals using awavelet-based systemrdquo Ultrasound in Medicine amp Biology vol30 no 5 pp 647ndash653 2004
[9] L Fan D H Evans and A R Naylor ldquoAutomated embolusidentification using a rule-based expert systemrdquo Ultrasound inMedicine amp Biology vol 27 no 8 pp 1065ndash1077 2001
[10] N Aydin F Marvasti and H S Markus ldquoEmbolic Dopplerultrasound signal detection using discrete wavelet transformrdquoIEEE Transactions on Information Technology in Biomedicinevol 8 no 2 pp 182ndash190 2004
[11] Y Chen and Y Wang ldquoDoppler embolic signal detection usingthe adaptive wavelet packet basis and neurofuzzy classificationrdquoPattern Recognition Letters vol 29 no 10 pp 1589ndash1595 2008
[12] M Gencer G Bilgin and N Aydin ldquoEmbolic Doppler ultra-sound signal detection via fractional Fourier transformrdquo inProceedings of the 2013 35th Annual International Conference ofthe IEEE Engineering in Medicine and Biology Society (EMBCrsquo13) pp 3050ndash3053 Osaka Japan July 2013
[13] C Lueang-On C Tantibundhit and S MuengtaweepongsaldquoProcessing time improvement for automatic embolic signaldetection using fuzzy c-meanrdquo in Proceedings of the 10thInternational Conference on Electrical EngineeringElectronicsComputer Telecommunications and Information Technology(ECTI-CON rsquo13) pp 1ndash5 IEEE Krabi Thailand May 2013
[14] J-M Girault and Z Zhao ldquoSynchronous detector as a newparadigm for automaticmicroembolus detectionrdquo InternationalJournal of Biomedical Engineering and Technology vol 14 no 1pp 60ndash70 2014
[15] S Menigot L Dreibine N Meziati and J-M Girault ldquoAuto-matic detection of microemboli by means of a synchronouslinear prediction techniquerdquo in Proceedings of the IEEE Inter-national Ultrasonics Symposium (IUS rsquo09) pp 2371ndash2374 IEEERome Italy September 2009
8 Computational and Mathematical Methods in Medicine
[16] N Aydin and H S Markus ldquoOptimization of processingparameters for the analysis and detection of embolic signalsrdquoEuropean Journal of Ultrasound vol 12 no 1 pp 69ndash79 2000
[17] E B Ringelstein DW Droste V L Babikian et al ldquoConsensuson microembolus detection by TCDrdquo Stroke vol 29 no 3 pp725ndash729 1998
[18] J-M Girault ldquoCerebral microembolism synchronous detectionwith wavelet packetsrdquo in Signal and Image MultiresolutionAnalysis chapter 4 pp 245ndash287 John Wiley amp Sons 2013
[19] E Chung L Fan C Degg and D H Evans ldquoDetectionof Doppler embolic signals psychoacoustic considerationsrdquoUltrasound in Medicine amp Biology vol 31 no 9 pp 1177ndash11842005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Computational and Mathematical Methods in Medicine 5
(a) (b)
Figure 3 (a) Robot probe and (b) Holter Transcranial Doppler System (TCD-X Atys Medical Soucieu en Jarrest France)
The microembolic detection based on the skewness andkurtosis signals is represented in Figures 2(b) and 2(c)
In order to complete the detection on the skewnessand kurtosis signals a threshold has to be set in order topick up the peak signals We decided to establish a data-based threshold for the skewness and kurtosis signals fromtheir respective means 120583119904 and 120583119896 and respective standarddeviations 120590119904 and 120590119896 This threshold is defined as 120582119904 =120583119904 + 119898120590119904 for skewness and 120582119896 = 120583119896 + 119898120590119896 for kurtosiswhere 119898 is a parameter whose value is adjusted using anoptimization training phase in a manner that increases thesystemrsquos sensitivity and specificity (refer to Results section)The thresholds are represented in Figures 2(b) and 2(c)
3 The Holter System and the Protocol
TCD is a noninvasive nonionizing inexpensive portableand safe technique which renders it as a convenient toolfor the detection of cerebral microemboli Long time probepositioning and the short effective examination durationare the main limitations of traditional TCD systems TheTranscranial Holter (TCD-X Atys Medical Soucieu en Jar-rest France) shown in Figure 3 allows prolonged patientmonitoring (higher than 5 hours) with the patient no longerattached to a TCD and does not need to be laying on a bedbut rather can be monitored under naturalistic conditionsTheHolter is equipped with a robotized automatic probe thathelps find the best TCD signal and tracks it automaticallyduring the whole recording
A database obtained from the Centre HospitalierRegional Universitaire (CHRU) de Lille (2 Avenue OscarLambret 59000 Lille France) is used Informed consent for
Holter monitoring was obtained from all monitored patientsThe recordings were acquired from the middle cerebralartery of the patients The ultrasonic wave frequency was15MHz the pulse repetition frequency (PRF) was 64 kHzand the ultrasound power was 50mWcm2
After the clinical examination an analogous conversion isperformed on theDoppler digital signal and then theDopplersignal is sent to a loudspeaker From the audible Dopplersignal and from the spectrogram displayed on a screen wedetect and count manually the number of microembolicevents in order to constitute our gold standard of detectionThe gold standard is subject to interagreement betweenthree experts of our laboratory Then the positions in timeof audibly and visually agreed-on microembolic events arenoted This gold standard is used to assess the results ofthe different detectors used and validate their performancesAlthough the gold standard detections obtained from expertsand nonexperts might be the same as stated in [19] theexperience of the latter experts was useful to distinguishbetween microembolic signals and artifact signals discussednext We should also point out that listening to the audiofiles is made at the normal playing speed and another time athalf the normal speed which allows us to detect microembolipreviously inaudible due to the well-known temporal andfrequency masking effects in audio files
4 Results
The different detectors are tested through algorithms wedeveloped using the numerical calculation software Matlab(Mathworks Natick MA USA) Our database is composedof 18 recorded signals divided into two categories The first
6 Computational and Mathematical Methods in Medicine
Table 1 Training phase results of the optimal thresholds that best maximize the sensitivity and specificity for the standard energy detectorand skewness and kurtosis based detectors
Optimal threshold that maximizes the sensitivity and specificity Sensitivity () Specificity ()Standard energy detector 5 dB 67 58Skewness detector 120582119904 = 120583119904 + 4120590119904 76 91Kurtosis detector 120582119896 = 120583119896 + 5120590119896 77 91
Table 2 Results (sensitivity and specificity) for the standard energy detector and the new detectors based on skewness and kurtosiscalculations of the Doppler energy signal
Detector type True positive False positive Sensitivity () Specificity ()Gold standard detections = 136Standard detection 88 58 65 60Skewness detection 106 10 78 91Kurtosis detection 109 12 80 90
is the training phase (8 signals) dedicated to determining thebest settings of the detectors used The second is the testingphase (10 signals) dedicated to assessing the performances ofthe detectors used under the optimal settings determined inthe training phase
Two parameters are used to evaluate the detectors
(i) Sensitivity (or Detection Rate) calculated as the num-ber of true positive detectionsthe number of goldstandard detections True positive detection refers tothe detection of an embolus recorded in the goldstandard
(ii) Specificity calculated as 1 minus False Alarm Rate (FAR)the latter being the number of false positive detec-tionsthe total number of detections False positivedetection refers to the detection of an embolus notrecorded in the gold standard or in other words anembolus which has not crossed the sample volume
41 Training Phase Results Since the threshold applied on theenergy signal to achieve the standard detection is empiricallyset through the choice of the user different microembolicdetections could be obtained To overcome this we initializea training phase to preset the best empirical threshold tobe used in the testing phase 3 to 9 dB values are usedTable 1 shows the empirical threshold that best maximizes thesensitivity and specificity
Moreover since the skewness and kurtosis calculationsare performed using a sliding window 119892(119905) on the energysignal an experimental test on the training phase signals isinitialized to determine the optimal length of thewindow119892(119905)and the optimal overlap ratio The optimal temporal windowlength is 73milliseconds and the optimal overlap used is 95Also using these settings we test in the training phase the bestdata-based threshold 120582119904 = 120583119904 + 119898120590119904 and 120582119896 = 120583119896 + 119898120590119896 forthe skewness and kurtosis signals respectively Values of 119898ranging between 3 and 7 are tested Table 1 shows the data-based threshold for the skewness and kurtosis signals thatbest maximizes the sensitivity and specificity
42 Testing Phase Results Table 2 represents the testingphase results for the three different energy detectors Forthe standard energy detector with empirical threshold thesensitivity is 65 and the specificity is 60 For the energydetector based on skewness calculation the sensitivity is 78and the specificity is 91 For the energy detector based onkurtosis calculation the sensitivity is 80 and the specificityis 90
The results presented show that the new detectors areable to significantly increase the specificity compared tostandard detection (more than 30) Moreover the sensi-tivity achieved by the new detectors is increased by 13for the skewness detector and 15 for the kurtosis detectorcompared to that achieved by standard detectors Theseresults assert the accuracy and superiority of the detectionbased on skewness and kurtosis calculation of the Dopplerenergy signal over the standard detection applied directly onthe Doppler energy signal
5 Discussion
The results obtained were clear The methods based on HOSoverpassed by far the standard method based on the second-order statistics The reason explaining such superiority liesin the HOS sensitivity in modifying the distribution formKnowing that the occurrence of a microembolus superim-posed on the Doppler energy signal imposes changes in thedistribution of this signal we propose to use the skewnessand kurtosis as new tools for microembolus detectionDuring embolus-free periods the Doppler energy signalsrsquodistribution is fixed and its skewness and kurtosis are neveraltered They do not show any variations However in thepresence of a microembolus superimposed on the energysignal the skewness and kurtosis signals are altered andthe embolus is attributed with a peak whose peakednesslevel is higher than all the other points of the signal Thisdetection can outperform standard methods After beingtested on a set of real signals the skewness and kurtosis baseddetection offered significant improvements including very
Computational and Mathematical Methods in Medicine 7
high specificity reaching up to 91 and 90 respectivelycompared to 60 achieved by the standard method Inaddition the sensitivity is increased from 65 for standardmethods to 78 and 80 for skewness and kurtosis baseddetectors respectively
Consequently we can affirm that skewness and kurtosiscan offer a robust and more reliable detection than standarddetection methods and thus can be considered as newtechniques for enhancing microembolic detection systems
In view of the fact that we have proposed 2 detectorsone based on skewness detection and the other on kurtosisdetection it is convenient to give note that the two detectorsperform very similarly and yield very close results The onlydifference that could be observed is that the kurtosis signaldisplays small fluctuations around the embolic peak detectedwhile the skewness signal fluctuatesmore strongly around theembolic peaks This provides the kurtosis detection with asmall advantage in terms of the detection thresholdwhich canbe more easily and robustly set
6 Conclusion
In this research study we propose two detectors based onthe calculation of the skewness and kurtosis of the Dopplerenergy signal as a tool for an enhanced cerebral microem-bolus detection Compared to the standard detector wherethe detection is performed directly on the energy signal theskewness and kurtosis based detectors allow increasing ofboth the sensitivity and the specificity
This study emphasizes that standard microembolicenergy detectors with empirical threshold still pose seriousdifficulties for the robust detection of microemboli It alsoshows that detectors incorporating detection based on skew-ness and kurtosis calculation from the energy allow a muchadvanced detection of microemboli precursors of cominglarge emboli with strong stroke risksThus using these simpleand straightforward detectors would be an additional facilityboosting the efforts to reduce the occurrence of strokes
The upcoming step would be attempting to increase theoverall performance of the techniques particularly in termsof sensitivity and validating the developed algorithms on alarger database Moreover we are on course of includingin the whole detection system automatic artifact rejectiontechniques rather than using manual techniques
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This research was financially supported by the DoctoralSchool of Sciences and Technology Lebanese UniversityLebanon the National Council for Scientific Research CNRSLebanon and the French Institute of Health and MedicalResearch INSERM France The authors would like to sin-cerely thankMarilys Almar and Benoit Guibert for theHolter
TCD equipmentThey also acknowledge Corinne Gautier forthe Holter Doppler recordings
References
[1] B Murtagh and R W Smalling ldquoCardioembolic strokerdquo Cur-rent Atherosclerosis Reports vol 8 no 4 pp 310ndash316 2006
[2] P M Morse and K U Ingard Theoretical Acoustics PrincetonUniversity Press Princeton NJ USA 1968
[3] H Markus M Cullinane and G Reid ldquoImproved automateddetection of embolic signals using a novel frequency filteringapproachrdquo Stroke vol 30 no 8 pp 1610ndash1615 1999
[4] H S Markus and G Reid ldquoFrequency filtering improvesultrasonic embolic signal detectionrdquo Ultrasound in Medicine ampBiology vol 25 no 5 pp 857ndash860 1999
[5] M Cullinane G Reid R Dittrich et al ldquoEvaluation of newonline automated embolic signal detection algorithm includingcomparison with panel of international expertsrdquo Stroke vol 31no 6 pp 1335ndash1341 2000
[6] M Cullinane Z Kaposzta S Reihill andH S Markus ldquoOnlineautomated detection of cerebral embolic signals from a varietyof embolic sourcesrdquo Ultrasound in Medicine amp Biology vol 28no 10 pp 1271ndash1277 2002
[7] J-M Girault D Kouame A Ouahabi and F Patat ldquoMicro-emboli detection an ultrasound doppler signal processingviewpointrdquo IEEE Transactions on Biomedical Engineering vol47 no 11 pp 1431ndash1439 2000
[8] S Marvasti D Gillies F Marvasti and H S Markus ldquoOnlineautomated detection of cerebral embolic signals using awavelet-based systemrdquo Ultrasound in Medicine amp Biology vol30 no 5 pp 647ndash653 2004
[9] L Fan D H Evans and A R Naylor ldquoAutomated embolusidentification using a rule-based expert systemrdquo Ultrasound inMedicine amp Biology vol 27 no 8 pp 1065ndash1077 2001
[10] N Aydin F Marvasti and H S Markus ldquoEmbolic Dopplerultrasound signal detection using discrete wavelet transformrdquoIEEE Transactions on Information Technology in Biomedicinevol 8 no 2 pp 182ndash190 2004
[11] Y Chen and Y Wang ldquoDoppler embolic signal detection usingthe adaptive wavelet packet basis and neurofuzzy classificationrdquoPattern Recognition Letters vol 29 no 10 pp 1589ndash1595 2008
[12] M Gencer G Bilgin and N Aydin ldquoEmbolic Doppler ultra-sound signal detection via fractional Fourier transformrdquo inProceedings of the 2013 35th Annual International Conference ofthe IEEE Engineering in Medicine and Biology Society (EMBCrsquo13) pp 3050ndash3053 Osaka Japan July 2013
[13] C Lueang-On C Tantibundhit and S MuengtaweepongsaldquoProcessing time improvement for automatic embolic signaldetection using fuzzy c-meanrdquo in Proceedings of the 10thInternational Conference on Electrical EngineeringElectronicsComputer Telecommunications and Information Technology(ECTI-CON rsquo13) pp 1ndash5 IEEE Krabi Thailand May 2013
[14] J-M Girault and Z Zhao ldquoSynchronous detector as a newparadigm for automaticmicroembolus detectionrdquo InternationalJournal of Biomedical Engineering and Technology vol 14 no 1pp 60ndash70 2014
[15] S Menigot L Dreibine N Meziati and J-M Girault ldquoAuto-matic detection of microemboli by means of a synchronouslinear prediction techniquerdquo in Proceedings of the IEEE Inter-national Ultrasonics Symposium (IUS rsquo09) pp 2371ndash2374 IEEERome Italy September 2009
8 Computational and Mathematical Methods in Medicine
[16] N Aydin and H S Markus ldquoOptimization of processingparameters for the analysis and detection of embolic signalsrdquoEuropean Journal of Ultrasound vol 12 no 1 pp 69ndash79 2000
[17] E B Ringelstein DW Droste V L Babikian et al ldquoConsensuson microembolus detection by TCDrdquo Stroke vol 29 no 3 pp725ndash729 1998
[18] J-M Girault ldquoCerebral microembolism synchronous detectionwith wavelet packetsrdquo in Signal and Image MultiresolutionAnalysis chapter 4 pp 245ndash287 John Wiley amp Sons 2013
[19] E Chung L Fan C Degg and D H Evans ldquoDetectionof Doppler embolic signals psychoacoustic considerationsrdquoUltrasound in Medicine amp Biology vol 31 no 9 pp 1177ndash11842005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
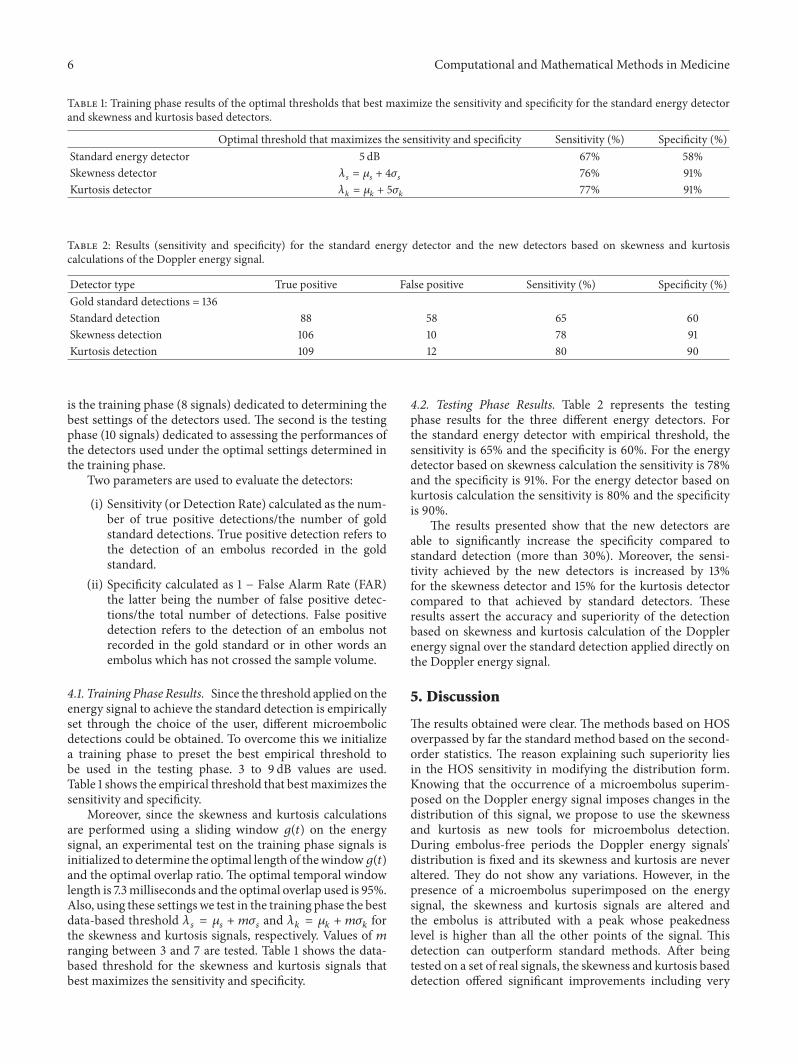
6 Computational and Mathematical Methods in Medicine
Table 1 Training phase results of the optimal thresholds that best maximize the sensitivity and specificity for the standard energy detectorand skewness and kurtosis based detectors
Optimal threshold that maximizes the sensitivity and specificity Sensitivity () Specificity ()Standard energy detector 5 dB 67 58Skewness detector 120582119904 = 120583119904 + 4120590119904 76 91Kurtosis detector 120582119896 = 120583119896 + 5120590119896 77 91
Table 2 Results (sensitivity and specificity) for the standard energy detector and the new detectors based on skewness and kurtosiscalculations of the Doppler energy signal
Detector type True positive False positive Sensitivity () Specificity ()Gold standard detections = 136Standard detection 88 58 65 60Skewness detection 106 10 78 91Kurtosis detection 109 12 80 90
is the training phase (8 signals) dedicated to determining thebest settings of the detectors used The second is the testingphase (10 signals) dedicated to assessing the performances ofthe detectors used under the optimal settings determined inthe training phase
Two parameters are used to evaluate the detectors
(i) Sensitivity (or Detection Rate) calculated as the num-ber of true positive detectionsthe number of goldstandard detections True positive detection refers tothe detection of an embolus recorded in the goldstandard
(ii) Specificity calculated as 1 minus False Alarm Rate (FAR)the latter being the number of false positive detec-tionsthe total number of detections False positivedetection refers to the detection of an embolus notrecorded in the gold standard or in other words anembolus which has not crossed the sample volume
41 Training Phase Results Since the threshold applied on theenergy signal to achieve the standard detection is empiricallyset through the choice of the user different microembolicdetections could be obtained To overcome this we initializea training phase to preset the best empirical threshold tobe used in the testing phase 3 to 9 dB values are usedTable 1 shows the empirical threshold that best maximizes thesensitivity and specificity
Moreover since the skewness and kurtosis calculationsare performed using a sliding window 119892(119905) on the energysignal an experimental test on the training phase signals isinitialized to determine the optimal length of thewindow119892(119905)and the optimal overlap ratio The optimal temporal windowlength is 73milliseconds and the optimal overlap used is 95Also using these settings we test in the training phase the bestdata-based threshold 120582119904 = 120583119904 + 119898120590119904 and 120582119896 = 120583119896 + 119898120590119896 forthe skewness and kurtosis signals respectively Values of 119898ranging between 3 and 7 are tested Table 1 shows the data-based threshold for the skewness and kurtosis signals thatbest maximizes the sensitivity and specificity
42 Testing Phase Results Table 2 represents the testingphase results for the three different energy detectors Forthe standard energy detector with empirical threshold thesensitivity is 65 and the specificity is 60 For the energydetector based on skewness calculation the sensitivity is 78and the specificity is 91 For the energy detector based onkurtosis calculation the sensitivity is 80 and the specificityis 90
The results presented show that the new detectors areable to significantly increase the specificity compared tostandard detection (more than 30) Moreover the sensi-tivity achieved by the new detectors is increased by 13for the skewness detector and 15 for the kurtosis detectorcompared to that achieved by standard detectors Theseresults assert the accuracy and superiority of the detectionbased on skewness and kurtosis calculation of the Dopplerenergy signal over the standard detection applied directly onthe Doppler energy signal
5 Discussion
The results obtained were clear The methods based on HOSoverpassed by far the standard method based on the second-order statistics The reason explaining such superiority liesin the HOS sensitivity in modifying the distribution formKnowing that the occurrence of a microembolus superim-posed on the Doppler energy signal imposes changes in thedistribution of this signal we propose to use the skewnessand kurtosis as new tools for microembolus detectionDuring embolus-free periods the Doppler energy signalsrsquodistribution is fixed and its skewness and kurtosis are neveraltered They do not show any variations However in thepresence of a microembolus superimposed on the energysignal the skewness and kurtosis signals are altered andthe embolus is attributed with a peak whose peakednesslevel is higher than all the other points of the signal Thisdetection can outperform standard methods After beingtested on a set of real signals the skewness and kurtosis baseddetection offered significant improvements including very
Computational and Mathematical Methods in Medicine 7
high specificity reaching up to 91 and 90 respectivelycompared to 60 achieved by the standard method Inaddition the sensitivity is increased from 65 for standardmethods to 78 and 80 for skewness and kurtosis baseddetectors respectively
Consequently we can affirm that skewness and kurtosiscan offer a robust and more reliable detection than standarddetection methods and thus can be considered as newtechniques for enhancing microembolic detection systems
In view of the fact that we have proposed 2 detectorsone based on skewness detection and the other on kurtosisdetection it is convenient to give note that the two detectorsperform very similarly and yield very close results The onlydifference that could be observed is that the kurtosis signaldisplays small fluctuations around the embolic peak detectedwhile the skewness signal fluctuatesmore strongly around theembolic peaks This provides the kurtosis detection with asmall advantage in terms of the detection thresholdwhich canbe more easily and robustly set
6 Conclusion
In this research study we propose two detectors based onthe calculation of the skewness and kurtosis of the Dopplerenergy signal as a tool for an enhanced cerebral microem-bolus detection Compared to the standard detector wherethe detection is performed directly on the energy signal theskewness and kurtosis based detectors allow increasing ofboth the sensitivity and the specificity
This study emphasizes that standard microembolicenergy detectors with empirical threshold still pose seriousdifficulties for the robust detection of microemboli It alsoshows that detectors incorporating detection based on skew-ness and kurtosis calculation from the energy allow a muchadvanced detection of microemboli precursors of cominglarge emboli with strong stroke risksThus using these simpleand straightforward detectors would be an additional facilityboosting the efforts to reduce the occurrence of strokes
The upcoming step would be attempting to increase theoverall performance of the techniques particularly in termsof sensitivity and validating the developed algorithms on alarger database Moreover we are on course of includingin the whole detection system automatic artifact rejectiontechniques rather than using manual techniques
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This research was financially supported by the DoctoralSchool of Sciences and Technology Lebanese UniversityLebanon the National Council for Scientific Research CNRSLebanon and the French Institute of Health and MedicalResearch INSERM France The authors would like to sin-cerely thankMarilys Almar and Benoit Guibert for theHolter
TCD equipmentThey also acknowledge Corinne Gautier forthe Holter Doppler recordings
References
[1] B Murtagh and R W Smalling ldquoCardioembolic strokerdquo Cur-rent Atherosclerosis Reports vol 8 no 4 pp 310ndash316 2006
[2] P M Morse and K U Ingard Theoretical Acoustics PrincetonUniversity Press Princeton NJ USA 1968
[3] H Markus M Cullinane and G Reid ldquoImproved automateddetection of embolic signals using a novel frequency filteringapproachrdquo Stroke vol 30 no 8 pp 1610ndash1615 1999
[4] H S Markus and G Reid ldquoFrequency filtering improvesultrasonic embolic signal detectionrdquo Ultrasound in Medicine ampBiology vol 25 no 5 pp 857ndash860 1999
[5] M Cullinane G Reid R Dittrich et al ldquoEvaluation of newonline automated embolic signal detection algorithm includingcomparison with panel of international expertsrdquo Stroke vol 31no 6 pp 1335ndash1341 2000
[6] M Cullinane Z Kaposzta S Reihill andH S Markus ldquoOnlineautomated detection of cerebral embolic signals from a varietyof embolic sourcesrdquo Ultrasound in Medicine amp Biology vol 28no 10 pp 1271ndash1277 2002
[7] J-M Girault D Kouame A Ouahabi and F Patat ldquoMicro-emboli detection an ultrasound doppler signal processingviewpointrdquo IEEE Transactions on Biomedical Engineering vol47 no 11 pp 1431ndash1439 2000
[8] S Marvasti D Gillies F Marvasti and H S Markus ldquoOnlineautomated detection of cerebral embolic signals using awavelet-based systemrdquo Ultrasound in Medicine amp Biology vol30 no 5 pp 647ndash653 2004
[9] L Fan D H Evans and A R Naylor ldquoAutomated embolusidentification using a rule-based expert systemrdquo Ultrasound inMedicine amp Biology vol 27 no 8 pp 1065ndash1077 2001
[10] N Aydin F Marvasti and H S Markus ldquoEmbolic Dopplerultrasound signal detection using discrete wavelet transformrdquoIEEE Transactions on Information Technology in Biomedicinevol 8 no 2 pp 182ndash190 2004
[11] Y Chen and Y Wang ldquoDoppler embolic signal detection usingthe adaptive wavelet packet basis and neurofuzzy classificationrdquoPattern Recognition Letters vol 29 no 10 pp 1589ndash1595 2008
[12] M Gencer G Bilgin and N Aydin ldquoEmbolic Doppler ultra-sound signal detection via fractional Fourier transformrdquo inProceedings of the 2013 35th Annual International Conference ofthe IEEE Engineering in Medicine and Biology Society (EMBCrsquo13) pp 3050ndash3053 Osaka Japan July 2013
[13] C Lueang-On C Tantibundhit and S MuengtaweepongsaldquoProcessing time improvement for automatic embolic signaldetection using fuzzy c-meanrdquo in Proceedings of the 10thInternational Conference on Electrical EngineeringElectronicsComputer Telecommunications and Information Technology(ECTI-CON rsquo13) pp 1ndash5 IEEE Krabi Thailand May 2013
[14] J-M Girault and Z Zhao ldquoSynchronous detector as a newparadigm for automaticmicroembolus detectionrdquo InternationalJournal of Biomedical Engineering and Technology vol 14 no 1pp 60ndash70 2014
[15] S Menigot L Dreibine N Meziati and J-M Girault ldquoAuto-matic detection of microemboli by means of a synchronouslinear prediction techniquerdquo in Proceedings of the IEEE Inter-national Ultrasonics Symposium (IUS rsquo09) pp 2371ndash2374 IEEERome Italy September 2009
8 Computational and Mathematical Methods in Medicine
[16] N Aydin and H S Markus ldquoOptimization of processingparameters for the analysis and detection of embolic signalsrdquoEuropean Journal of Ultrasound vol 12 no 1 pp 69ndash79 2000
[17] E B Ringelstein DW Droste V L Babikian et al ldquoConsensuson microembolus detection by TCDrdquo Stroke vol 29 no 3 pp725ndash729 1998
[18] J-M Girault ldquoCerebral microembolism synchronous detectionwith wavelet packetsrdquo in Signal and Image MultiresolutionAnalysis chapter 4 pp 245ndash287 John Wiley amp Sons 2013
[19] E Chung L Fan C Degg and D H Evans ldquoDetectionof Doppler embolic signals psychoacoustic considerationsrdquoUltrasound in Medicine amp Biology vol 31 no 9 pp 1177ndash11842005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Computational and Mathematical Methods in Medicine 7
high specificity reaching up to 91 and 90 respectivelycompared to 60 achieved by the standard method Inaddition the sensitivity is increased from 65 for standardmethods to 78 and 80 for skewness and kurtosis baseddetectors respectively
Consequently we can affirm that skewness and kurtosiscan offer a robust and more reliable detection than standarddetection methods and thus can be considered as newtechniques for enhancing microembolic detection systems
In view of the fact that we have proposed 2 detectorsone based on skewness detection and the other on kurtosisdetection it is convenient to give note that the two detectorsperform very similarly and yield very close results The onlydifference that could be observed is that the kurtosis signaldisplays small fluctuations around the embolic peak detectedwhile the skewness signal fluctuatesmore strongly around theembolic peaks This provides the kurtosis detection with asmall advantage in terms of the detection thresholdwhich canbe more easily and robustly set
6 Conclusion
In this research study we propose two detectors based onthe calculation of the skewness and kurtosis of the Dopplerenergy signal as a tool for an enhanced cerebral microem-bolus detection Compared to the standard detector wherethe detection is performed directly on the energy signal theskewness and kurtosis based detectors allow increasing ofboth the sensitivity and the specificity
This study emphasizes that standard microembolicenergy detectors with empirical threshold still pose seriousdifficulties for the robust detection of microemboli It alsoshows that detectors incorporating detection based on skew-ness and kurtosis calculation from the energy allow a muchadvanced detection of microemboli precursors of cominglarge emboli with strong stroke risksThus using these simpleand straightforward detectors would be an additional facilityboosting the efforts to reduce the occurrence of strokes
The upcoming step would be attempting to increase theoverall performance of the techniques particularly in termsof sensitivity and validating the developed algorithms on alarger database Moreover we are on course of includingin the whole detection system automatic artifact rejectiontechniques rather than using manual techniques
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This research was financially supported by the DoctoralSchool of Sciences and Technology Lebanese UniversityLebanon the National Council for Scientific Research CNRSLebanon and the French Institute of Health and MedicalResearch INSERM France The authors would like to sin-cerely thankMarilys Almar and Benoit Guibert for theHolter
TCD equipmentThey also acknowledge Corinne Gautier forthe Holter Doppler recordings
References
[1] B Murtagh and R W Smalling ldquoCardioembolic strokerdquo Cur-rent Atherosclerosis Reports vol 8 no 4 pp 310ndash316 2006
[2] P M Morse and K U Ingard Theoretical Acoustics PrincetonUniversity Press Princeton NJ USA 1968
[3] H Markus M Cullinane and G Reid ldquoImproved automateddetection of embolic signals using a novel frequency filteringapproachrdquo Stroke vol 30 no 8 pp 1610ndash1615 1999
[4] H S Markus and G Reid ldquoFrequency filtering improvesultrasonic embolic signal detectionrdquo Ultrasound in Medicine ampBiology vol 25 no 5 pp 857ndash860 1999
[5] M Cullinane G Reid R Dittrich et al ldquoEvaluation of newonline automated embolic signal detection algorithm includingcomparison with panel of international expertsrdquo Stroke vol 31no 6 pp 1335ndash1341 2000
[6] M Cullinane Z Kaposzta S Reihill andH S Markus ldquoOnlineautomated detection of cerebral embolic signals from a varietyof embolic sourcesrdquo Ultrasound in Medicine amp Biology vol 28no 10 pp 1271ndash1277 2002
[7] J-M Girault D Kouame A Ouahabi and F Patat ldquoMicro-emboli detection an ultrasound doppler signal processingviewpointrdquo IEEE Transactions on Biomedical Engineering vol47 no 11 pp 1431ndash1439 2000
[8] S Marvasti D Gillies F Marvasti and H S Markus ldquoOnlineautomated detection of cerebral embolic signals using awavelet-based systemrdquo Ultrasound in Medicine amp Biology vol30 no 5 pp 647ndash653 2004
[9] L Fan D H Evans and A R Naylor ldquoAutomated embolusidentification using a rule-based expert systemrdquo Ultrasound inMedicine amp Biology vol 27 no 8 pp 1065ndash1077 2001
[10] N Aydin F Marvasti and H S Markus ldquoEmbolic Dopplerultrasound signal detection using discrete wavelet transformrdquoIEEE Transactions on Information Technology in Biomedicinevol 8 no 2 pp 182ndash190 2004
[11] Y Chen and Y Wang ldquoDoppler embolic signal detection usingthe adaptive wavelet packet basis and neurofuzzy classificationrdquoPattern Recognition Letters vol 29 no 10 pp 1589ndash1595 2008
[12] M Gencer G Bilgin and N Aydin ldquoEmbolic Doppler ultra-sound signal detection via fractional Fourier transformrdquo inProceedings of the 2013 35th Annual International Conference ofthe IEEE Engineering in Medicine and Biology Society (EMBCrsquo13) pp 3050ndash3053 Osaka Japan July 2013
[13] C Lueang-On C Tantibundhit and S MuengtaweepongsaldquoProcessing time improvement for automatic embolic signaldetection using fuzzy c-meanrdquo in Proceedings of the 10thInternational Conference on Electrical EngineeringElectronicsComputer Telecommunications and Information Technology(ECTI-CON rsquo13) pp 1ndash5 IEEE Krabi Thailand May 2013
[14] J-M Girault and Z Zhao ldquoSynchronous detector as a newparadigm for automaticmicroembolus detectionrdquo InternationalJournal of Biomedical Engineering and Technology vol 14 no 1pp 60ndash70 2014
[15] S Menigot L Dreibine N Meziati and J-M Girault ldquoAuto-matic detection of microemboli by means of a synchronouslinear prediction techniquerdquo in Proceedings of the IEEE Inter-national Ultrasonics Symposium (IUS rsquo09) pp 2371ndash2374 IEEERome Italy September 2009
8 Computational and Mathematical Methods in Medicine
[16] N Aydin and H S Markus ldquoOptimization of processingparameters for the analysis and detection of embolic signalsrdquoEuropean Journal of Ultrasound vol 12 no 1 pp 69ndash79 2000
[17] E B Ringelstein DW Droste V L Babikian et al ldquoConsensuson microembolus detection by TCDrdquo Stroke vol 29 no 3 pp725ndash729 1998
[18] J-M Girault ldquoCerebral microembolism synchronous detectionwith wavelet packetsrdquo in Signal and Image MultiresolutionAnalysis chapter 4 pp 245ndash287 John Wiley amp Sons 2013
[19] E Chung L Fan C Degg and D H Evans ldquoDetectionof Doppler embolic signals psychoacoustic considerationsrdquoUltrasound in Medicine amp Biology vol 31 no 9 pp 1177ndash11842005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 Computational and Mathematical Methods in Medicine
[16] N Aydin and H S Markus ldquoOptimization of processingparameters for the analysis and detection of embolic signalsrdquoEuropean Journal of Ultrasound vol 12 no 1 pp 69ndash79 2000
[17] E B Ringelstein DW Droste V L Babikian et al ldquoConsensuson microembolus detection by TCDrdquo Stroke vol 29 no 3 pp725ndash729 1998
[18] J-M Girault ldquoCerebral microembolism synchronous detectionwith wavelet packetsrdquo in Signal and Image MultiresolutionAnalysis chapter 4 pp 245ndash287 John Wiley amp Sons 2013
[19] E Chung L Fan C Degg and D H Evans ldquoDetectionof Doppler embolic signals psychoacoustic considerationsrdquoUltrasound in Medicine amp Biology vol 31 no 9 pp 1177ndash11842005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom









![MinimalisticApproachtoCoreferenceResolutionin LithuanianMedicalRecordsdownloads.hindawi.com/journals/cmmm/2019/9079840.pdf · 2019. 7. 30. · RU-sys2[49] Rulebased 0.71 0.58 0.64](https://img.dokumen.tips/doc/110x75/60a096cd713ea42a5125ccd7/minimalisticapproachtocoreferenceresolutionin-lithuanianmed-2019-7-30-ru-sys249.jpg)



















