Embed Size (px)
Citation preview

Reproductive, Maternal, Newborn and Child Health in India
Page 1 of 18
Report of Workshop on
“Reproductive, Maternal,
Newborn and Child Health
in India”
Date: 13th September 2014
Organized by:
Rapporteur:
Dr. Mugdha Potnis‐Lele,
Scientific Advisor and Program Manager – SIIP
Email: [email protected]
http://www.venturecenter.co.in/campaigns/mch/events.php

Reproductive, Maternal, Newborn and Child Health in India
Page 2 of 18
A workshop on “Reproductive, Maternal, Newborn and Child Health in India” was
organized by Bioincubator at Venture Center (Bioincubator at Venture Center is
supported by BIRAC, Government of India) on Saturday, 13th September 2014.
This report contains:
Key Lessons from the workshop 3
Detailed record of the workshop 7
Appendix 1: Workshop outline 15
Appendix 2: Photos 18

Reproductive, Maternal, Newborn and Child Health in India
Page 3 of 18
Key Lessons from the workshop
1. Need for diagnostic innovations
• Quick diagnosis of Post‐partum hemorrhage, Eclampsia and Pre‐eclampsia (hypertension with
proteinuria at more than 20 weeks) with fits and obstructed labour leading to uterine rupture,
anaemia, Malaria, Cardiac disease and Hepatitis infections in pregnancy: especially non‐A, non‐B
types
• Detecting fetal / maternal health risks
• Correct estimation of timing of birth and mode of delivery
• Restoring blood volume to bring down hemorrhage related deaths
• Managing critically ill women (Near miss cases) by providing EmOC
• Recognising and managing complications
• Making technology (essential diagnostics, equipment, facilities ) available
• Detecting fetal growth restriction
• Predicting preterm birth
• New lab testing techniques
• New ways of detecting complications
• Upgrading research technologies into usable products.
• Treating children with these diseases with appropriate treatment by improvement in care
seeking and appropriate and timely referrals, case management at the community and health
facility, adequate supply of ORS, zinc, antibiotics, and oxygen, continuation in feeding /
breastfeeding during illness episodes.
• Point‐of‐care interventions for monitoring hemoglobin, preferably non‐invasive method,
measurement of blood loss during delivery minimization of blood loss, eclampsia drills or
obstetric drills, training for giving ampoules in eclampsia cases, simple gadgets for monitoring
fetal movement
• Point‐of‐care diagnostics for Hepatitis B and HIV at the home setting
Reproductive, Maternal, Newborn and Child Health in India
Page 4 of 18
• Diagnosis of vaginal discharge during pregnancy
• Development of multivalent (hexa/heptavalent) vaccines to compress the immunization
schedule
• Development of easily available diagnostics for infectious diseases like pneumonia
2. Need for nutritional interventions
• Nutritional interventions: Improving nutrition : Prevention of anaemia, Low Birth Weight babies
• Development of innovative teaching modules to improve nutritional awareness
• Methods to establish linkages and networks with public health systems and NGOs working at
the community level for sustainability of nutrition intervention activities
• Simple gadget to measure length/height of infant (as it has impact on SAM/MAM
categorization)
• Gadget to measure weight of infant/child, especially where floor is not straight
• Nutritionally better and tasty medical nutrition therapy products (eg: nutribars/nutritional chips
or wafers etc)
• Locally produced food products
• Simplification in measurement of height, weight, mid‐upper arm circumference (MUAC) which
give correct categorization of malnutrition status
3. Increasing awareness about health services
• Protecting children by establishing good health practices from birth like exclusive breastfeeding
for 6 months from birth, adequate complementary feeding after 6 months, vitamin A
supplementation.
• Preventing children from infectious diseases by adequate vaccinations, simple hand‐washing
techniques, safe drinking water and sanitation, reducing household air pollution, HIV
prevention.
4. Improving access to health services
• Post‐partum sepsis: due to aseptic precautions and anaemia
• Unsafe abortion: mainly due to teenage pregnancy problems
• Institutionalized deliveries attended by Skilled/trained birth attendants
• Improving access to Institutional health services

Reproductive, Maternal, Newborn and Child Health in India
Page 5 of 18
• Availability of affordable and accessible Emergency Obstetric Care (EmOC)
• Availability of Family Planning and safe abortion services
• Reaching out to every pregnant woman: Rural/urban gap; Poverty, ignorance, misconceptions‐
health seeking behavior
• Delivering essential care through pregnancy‐delivery‐postdelivery period
• Deliverying every pregnant woman by SBA in an institution
5. Improving communications by technological innovations
• Communication : Use of SMS, mobile calls
• Mobile apps
• Development of good surveillance systems including AEFI detection and reporting systems
• Surveillance systems
• Mobile apps which act as reminders about immunization schedules
• Electronic devices to maintain immunization records
• Involvement of IT industry to build robust surveillance systems.
6. Need for social change
• Female literacy and Women Empowerment
• Developing educated and aware political will
• Effective information education and communication activities
• Support to indigenous vaccine industry in form of resources (manpower, financial etc)
• Involvement of self‐help groups to provide need based services to women
• Regulations to make immunization compulsory. Eg: at entry at school level immunization record
is mandatory document
7. Establishing legal and regulatory networks
• Regulatory and ethical issues should be addressed
• Integrative approach in designing interventions where medical and non‐medical personnel are
working together in a medical setup.

Reproductive, Maternal, Newborn and Child Health in India
Page 6 of 18
8. Need for training to health professionals
• Training to primary health care workers for diagnosis of diseases like cervical cancers
• For improving training to health personnel, development of “near to real life” Mannequins for
use in skill labs
• Education modules for generating awareness and building confidence about vaccines. Wrong
propaganda about vaccines should be discouraged
• Generating awareness regarding rampant use of antibiotics
• Exposure of innovators to primary health care situations to understand the actual needs.

Reproductive, Maternal, Newborn and Child Health in India
Page 7 of 18
Detailed record of the workshop
A workshop on “Reproductive, Maternal, Newborn and Child Health in India” was organized by
Bioincubator at Venture Center (Bioincubator at Venture Center is supported by BIRAC, Government of
India) on Saturday, 13th September 2014.
The audience was well represented by participants from the academia, NGOs, technocrats,
entrepreneurs and medical professionals. The workshop began with a brief welcome by Dr. Premnath
introducing the various activities of Venture Center. A brief summary of the earlier workshop conducted
in September 2013 was given by Pradnya Aradhye. Report is shared at:
http://www.venturecenter.co.in/campaigns/mch/
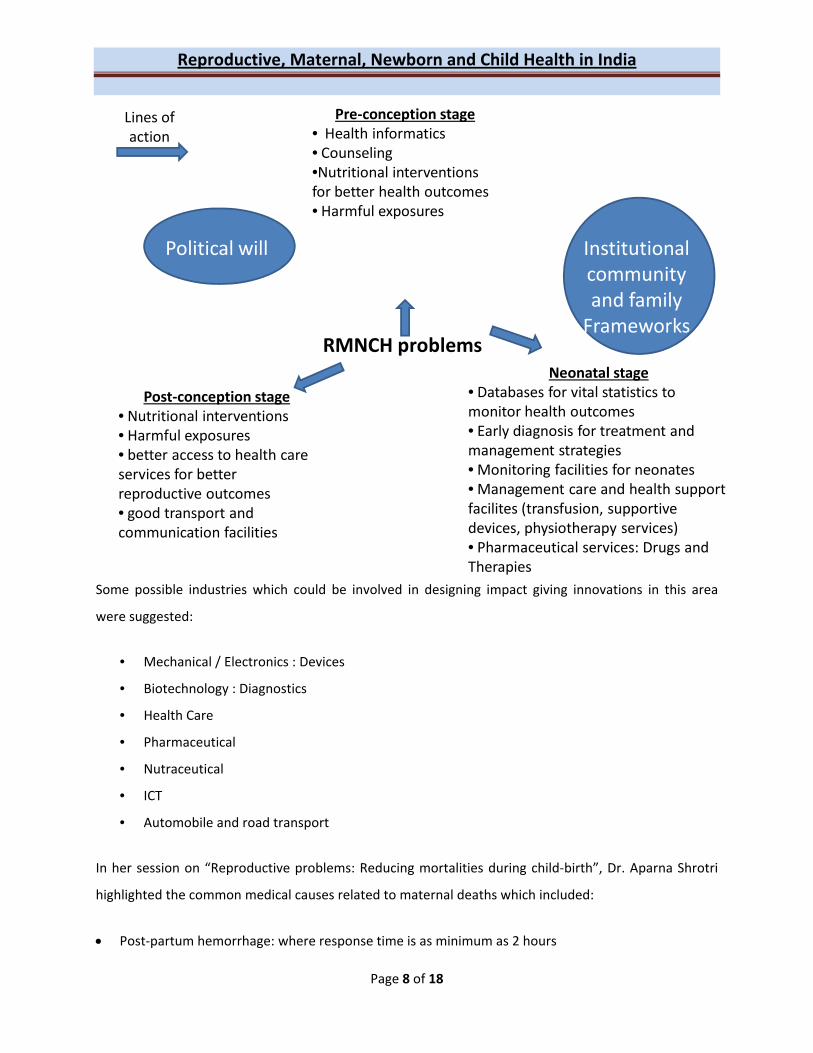
Setting the stage for the workshop was done by Mugdha Lele, where in addition to summarizing the
various problems in the areas of reproductive, maternal, newborn and child health in India, specific lines
of action were suggested as summarized below:
Reproductive, Maternal, Newborn and Child Health in India
Page 8 of 18
RMNCH problems
Pre‐conception stage• Health informatics• Counseling•Nutritional interventions for better health outcomes • Harmful exposures
Post‐conception stage• Nutritional interventions• Harmful exposures• better access to health care services for better reproductive outcomes• good transport and communication facilities
Neonatal stage• Databases for vital statistics to monitor health outcomes• Early diagnosis for treatment and management strategies• Monitoring facilities for neonates• Management care and health support facilites (transfusion, supportive devices, physiotherapy services)• Pharmaceutical services: Drugs and Therapies
Lines of action
Political will Institutional community and family Frameworks
Some possible industries which could be involved in designing impact giving innovations in this area
were suggested:
• Mechanical / Electronics : Devices
• Biotechnology : Diagnostics
• Health Care
• Pharmaceutical
• Nutraceutical
• ICT
• Automobile and road transport
In her session on “Reproductive problems: Reducing mortalities during child‐birth”, Dr. Aparna Shrotri
highlighted the common medical causes related to maternal deaths which included:
• Post‐partum hemorrhage: where response time is as minimum as 2 hours
Reproductive, Maternal, Newborn and Child Health in India
Page 9 of 18
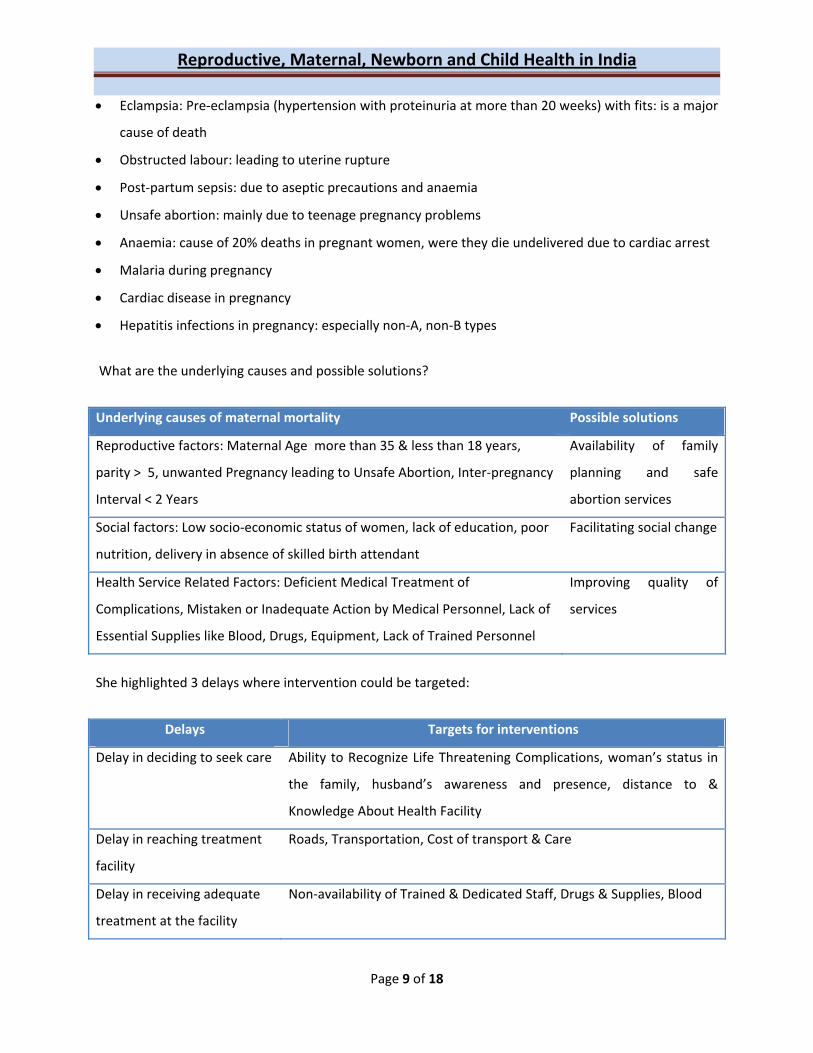
• Eclampsia: Pre‐eclampsia (hypertension with proteinuria at more than 20 weeks) with fits: is a major
cause of death
• Obstructed labour: leading to uterine rupture
• Post‐partum sepsis: due to aseptic precautions and anaemia
• Unsafe abortion: mainly due to teenage pregnancy problems
• Anaemia: cause of 20% deaths in pregnant women, were they die undelivered due to cardiac arrest
• Malaria during pregnancy
• Cardiac disease in pregnancy
• Hepatitis infections in pregnancy: especially non‐A, non‐B types
What are the underlying causes and possible solutions?
Underlying causes of maternal mortality Possible solutions
Reproductive factors: Maternal Age more than 35 & less than 18 years,
parity > 5, unwanted Pregnancy leading to Unsafe Abortion, Inter‐pregnancy
Interval < 2 Years
Availability of family
planning and safe
abortion services
Social factors: Low socio‐economic status of women, lack of education, poor
nutrition, delivery in absence of skilled birth attendant
Facilitating social change
Health Service Related Factors: Deficient Medical Treatment of
Complications, Mistaken or Inadequate Action by Medical Personnel, Lack of
Essential Supplies like Blood, Drugs, Equipment, Lack of Trained Personnel
Improving quality of
services
She highlighted 3 delays where intervention could be targeted:
Delays Targets for interventions
Delay in deciding to seek care Ability to Recognize Life Threatening Complications, woman’s status in
the family, husband’s awareness and presence, distance to &
Knowledge About Health Facility
Delay in reaching treatment
facility
Roads, Transportation, Cost of transport & Care
Delay in receiving adequate
treatment at the facility
Non‐availability of Trained & Dedicated Staff, Drugs & Supplies, Blood

Reproductive, Maternal, Newborn and Child Health in India
Page 10 of 18
Some examples which have worked focused on:
• Institutionalized deliveries attended by Skilled/trained birth attendants
• Improving access to Institutional health services
• Availability of affordable and accessible Emergency Obstetric Care (EmOC)
• Availability of Family Planning and safe abortion services
• Female literacy and Women Empowerment
Some suggested interventions were:
• Diagnostic innovations: like anaemia detection & correction.
• Nutritional interventions: Improving nutrition : Prevention of anaemia, Low Birth Weight babies
• Detecting fetal / maternal health risks
• Correct estimation of timing of birth and mode of delivery
• Restoring blood volume to bring down hemorrhage related deaths
• Managing critically ill women (Near miss cases) by providing EmOC
Some challenges:
• Reaching out to every pregnant woman: Rural/urban gap; Poverty, ignorance, misconceptions‐
health seeking behavior
• Delivering essential care through pregnancy‐delivery‐postdelivery period
• Deliverying every pregnant woman by SBA in an institution
• Recognising and managing complications
• Making technology (essential diagnostics, equipment, facilities ) & trained manpower available
Some innovations required were:
• Detection of severe anaemia
• Detecting high blood pressure
• Detecting fetal growth restriction
• Predicting preterm birth
• Communication : Use of SMS, mobile calls

Reproductive, Maternal, Newborn and Child Health in India
Page 11 of 18
• Mobile apps
• New lab testing techniques
• New ways of detecting complications
Some life‐saving technologies are available in research settings, but the same are not practically usable.
Hence, innovations should be targeted to upgrade such technologies into usable products.
The talk by Dr. Anuja Jayaraman focused on, “Models for improving nutritional security in community
through technological interventions”. She presented the model of the Aahar program of SNEHA, an
organization working in the Dharavi slums of Mumbai to improve the nutritional status of children under
3 years of age, to bring down wasting (severe acute malnutrition‐SAM and moderate acute malnutrition‐
MAM). This project is using technology in the form smart phones to collect information, to calculate
malnutrition based on these data and plan interventions accordingly. Using technology has resulted in
easy scalability and replicability of this model, data visualization is instant/real time and easy, immediate
feedback can be given to the field workers by the supervisors. Intervention is in the form of Medical
Nutrition Therapy (MNT), which is a formulation prepared for the SAM and MAM children to restore
them to normalcy.
In her talk on nutritional interventions in adolescent girls, Angeline Jeyakumar highlighted that an
integrated approach need to be taken at the community level. Interventions need to be targeted at the
individual level (adolescent girls), organizational level (NGOs) and schools. Some teaching modules using
the play‐way method were developed for these interventions. Also there is a need to establish linkages
and networks with public health systems and the NGOs working at the community level for
sustainability of these nutrition intervention activities.
On the problems related to Vaccines and Immunization, Dr. Prasad Kulkarni highlighted the problems
related to immunization coverage in the Indian scenario which include:
• Huge population growth rates
• Poor access
• Huge inter‐state variations in coverage
• Large geographical diversity
• Political instability
• Cultural diversity and barriers

Reproductive, Maternal, Newborn and Child Health in India
Page 12 of 18
• Migrant population
• Lack of awareness and motivation on part of recipients and health care providers
• Adverse events following immunization (AEFI): eg: Pentavalent vaccine related deaths
• Weak surveillance system to track burden of vaccine preventable diseases
• Inadequate health services (poorly trained and inadequate staff, poor supply for vaccines etc)
• Falsification of data and over‐reporting of rates
• Emergency applications of vaccination over‐emphasized rather than preventable. Eg: H1N1
vaccine
Key challenges in this field are:
• Price point pressure
• Temperature sensitive supply chain
• No regulatory guidelines developed in India
• Lag period for availability of vaccines in developed and developing countries
• Lack of access to technologies in India
Some solutions:
• Developing educated and aware political will
• Effective information education and communication activities
• Development of good surveillance systems including AEFI detection and reporting systems
• Regulatory and ethical issues should be addressed
• Support to indigenous vaccine industry in form of resources (manpower, financial etc)
Dr. Agharkhedkar highlighted the rampant use of antibiotics in the treatment of infectious diseases like
pneumonia as a major problem. Also more research needs to be done on the different pathogens
causing pneumonia and the ways they are transmitted. Advocacy should also be done for the strategy of
“protect, prevent and treat” for reducing the morbidity and mortality due to pneumonia and diarrhea.
This includes:
Reproductive, Maternal, Newborn and Child Health in India
Page 13 of 18
• Protecting children by establishing good health practices from birth like exclusive breastfeeding
for 6 months from birth, adequate complementary feeding after 6 months, vitamin A
supplementation.
• Preventing children infectious diseases by adequate vaccinations, simple hand‐washing
techniques, safe drinking water and sanitation, reducing household air pollution, HIV
prevention.
• Treating children with these diseases with appropriate treatment by improvement in care
seeking and appropriate and timely referrals, case management at the community and health
facility, adequate supply of ORS, zinc, antibiotics, and oxygen, continuation in feeding /
breastfeeding during illness episodes.
Panel discussion was carried with the participation of all speakers and moderated by Dr. Premnath. The
discussion on priorities of intervention had the following suggestions:
Maternal interventions:
• Point‐of‐care interventions for monitoring hemoglobin, preferably non‐invasive method
• measurement of blood loss during delivery
• minimization of blood loss
• eclampsia drills or obstetric drills
• training for giving ampoules in eclampsia cases
• simple gadgets for monitoring fetal movement
• Point‐of‐care diagnostics for Hepatitis B and HIV at the home setting
• Diagnosis of vaginal discharge during pregnancy
• Training to primary health care workers for diagnosis of diseases like cervical cancers
• Involvement of self‐help groups to provide need based services to wormen
• For improving training to health personnel, development of “near to real life” Mannequins for
use in skill labs.
Nutritional interventions:
• Simple gadget to measure length/height of infant (as it has impact on SAM/MAM
categorization)
• Gadget to measure weight of infant/child, especially where floor is not straight

Reproductive, Maternal, Newborn and Child Health in India
Page 14 of 18
• Nutritionally better and tasty medical nutrition therapy products (eg: nutribars/nutritional chips
or wafers etc)
• Locally produced food products
• Simplification in measurement of height, weight, mid‐upper arm circumference (MUAC) which
give correct categorization of malnutrition status
Vaccination/immunization related interventions:
• Surveillance systems
• Education modules for generating awareness and building confidence about vaccines. Wrong
propaganda about vaccines should be discouraged
• Mobile apps which act as reminders about immunization schedules
• Development of multivalent (hexa/heptavalent) vaccines to compress the immunization
schedule
• Regulations to make immunization compulsory. Eg: at entry at school level immunization record
is mandatory document
• Electronic devices to maintain immunization records
Interventions in the field of respiratory illnesses:
• Generating awareness regarding rampant use of antibiotics
• Development of easily available diagnostics for infectious diseases like pneumonia
Other suggestions:
• Integrative approach in designing interventions where medical and non‐medical personnel are
working together in a medical setup.
• Exposure of innovators to primary health care situations to understand the actual needs.
• Involvement of IT industry to build robust surveillance systems.
The event concluded by a Skype call with Sonia Gandhi the Program Manager for the SPARSH scheme
from BIRAC‐DBT. A call for proposals has been given for “Reproductive, Maternal, Newborn and Child
Health”. Also details regarding the Social Innovations Immersion Program under the SPARSH scheme
were shared. Further details are available on the BIRAC website.

Reproductive, Maternal, Newborn and Child Health in India
Page 15 of 18
Appendix 1
Workshop Outline
Time Session title Faculty
0930‐945 Registration
0945‐1000 Welcome to Venture Center BioIncubator. Introduction to the
workshop.
Pradnya Aradhye
1000‐1015 Quick update of MCH 2013 event: Action taken and results Pradnya Aradhye
1015‐1030 Overview of disease burden for:
• Reproductive and maternal problems
• Newborn and Child health problems
Setting the stage with an overview of key issues
Pradnya Aradhye
Mugdha Lele
1030‐1100 Reproductive problems: Reducing mortalities during child‐birth Aparna Shrotri
1100‐1115 Networking tea
1115‐1145 Models for improving nutritional security in community through
technological interventions
Anuja Jayaraman
1145‐1215 Nutritional interventions for adolescent girls: impact on reproductive,
maternal, newborn and child health
Angeline Jeyakumar
1215‐1300 Vaccines and immunization: Problems in the Indian scenario Prasad Kulkarni
1300‐1400 Lunch Break
1400‐1500 Panel discussion
• Identification and stream lining of certain key issues related to
Reproductive, Maternal, New born and Child health: Defining
problems and areas where technology interventions are needed,
exploring user‐friendly solutions for using in the community set
Moderator: Premnath V
Panelists: Sharad
Agarkhedkar, Aparna
Reproductive, Maternal, Newborn and Child Health in India
Page 16 of 18
up. Where will technology intervention work within a reasonable
time frame and cost? Ideas for compilation and for the workshop
white paper.
Shrotri, Anjeline Jeykumar,
Anuja Jayaraman, Prasad
Kulkarni
Rapporteur: Mugdha Lele
1500‐1530 Diagnostic limitations for the common respiratory illnesses Sharad Agarkhedkar
1530‐1600 An overview of emerging funding opportunities: SPARSH from BIRAC
focused on Reproductive, Maternal, Newborn and Child Health
(Deadline: 30 Sept 2014)
Pradnya Aradhye
1600‐1630 Q&A for SPARSH funding scheme: (over SKYPE) BIRAC: Sonia Gandhi
1630‐1645 Insights by 2013 SPARSH grantees
1645‐1700 Closing comments and closure of the event and Tea
Speakers and Panelists (in alphabetical order of last names)
SHARAD AGARKHEDKAR
Sharad Agarkhedkar is MD in Pediatrics and currently Professor and Head of Department of Pediatrics at Padmashree Dr. D. Y. Patil Medical College, Hospital & Research Centre. He has few national and international publications to his credit and is involved in mentoring post-graduate students in research and academic activities.
PRADNYA ARADHYE
Pradnya Aradhye is currently Associate, Bioincubator, Venture Center. She has done her M.Tech in Biological Sciences and Bioengineering from IIT Kanpur. Currently she is handling all BioIncubator activites at Venture Center. She is responsible for creating a pipeline of potential and signing-up incubates for the Bioincubator. Contribute to building scientific support systems and resources for VC incubates including specific expertise. Discussions with scientists to understand their competencies.
SONIA GANDHI
Sonia Gandhi is currently assisting the Investment group of BIRAC, New Delhi as Project Manager and is responsible for proper functioning of the grants management system, ensuring compliance to regulations, evaluation and management of projects as per guidelines. Previous to this she worked with BIRAP as Program Manager for Healthcare with responsibility of Techno-commercial guidance and support for projects in identified areas of Healthcare Industry. Prior to this, she was in Quality Management Systems of Reliance Life Sciences and is involved in ensuring the compliance of various processes of the product development to applicable regulatory guidelines. She is double Masters in Biotechnology and Quality Management and also a Certified Quality Management Professional from Birla Institute of Technology and Science and Reliance Institute of Life Sciences. She also visited the EMA, MHRA, HTA and NICE offices at UK to understand the regulatory scenario impacting Medical Devices, Clinical Trials, Vaccines and Stem Cells development.

Reproductive, Maternal, Newborn and Child Health in India
Page 17 of 18
ANJELINE JEYAKUMAR
Anjeline Jeyakumar has done her M.Sc. In Nutrition and Dietetics and M.Phil in Foods and Nutrition. Her doctoral work focuses on Iron deficiency among adolescent girls. She has been the coordinator of the Masters' programme in dietetics at the School of Health Sciences, University of Pune. She is also coordinating the UGC funded e-pathshala project for Public health nutrition. She is a visiting faculty at SNDT Women’s University.
ANUJA JAYARAMAN
Dr Anuja completed a PhD in Agricultural, Environmental and Regional Economics and Demography from the Pennsylvania State University, USA and has over 10 years of rich and varied international experience in the field of development. She has expertise in monitoring and evaluation of health programs. Her research focuses on areas of non - income dimensions of well - being including health (maternal and child health, HIV / AIDS), housing and education in the context of South Asia and Africa.
PRASAD KULKARNI
Prasad Kulkarni is MD in Clinical Pharmacology and is currently Medical Director at Serum Institute of India Ltd., Pune. He has been involved in many clinical trials on vaccines like BCG, Measles, Rubella, Hepatitis B, Hib, H1N1, Influenza to name a few and various therapeutic products. He has several national and International publications to his credit. He has also been an advisor to WHO. He is a visiting faculty at various research and academic institutes in the country and has been a part of Institutional Ethics Committees. He is also associated with some journals in the capacity of editorial board member and referee.
MUGDHA LELE
Dr Mugdha Lele is a Scientific Advisor at Venture Center, NCL Innovation Park, Pune. She was previously an Assistant Professor in Dept of Genetics, Immunology and Biochemistry at Maharashtra University of Health Sciences. Her research work is related to epidemiological profiling and development of molecular diagnostics for Genetic disorders. She has a few national and international publications to her credit.
APARNA SHROTRI
Aparna Shrotri has been a Professor at Dept of Obstetrics & Gynecology, B. J. Medical College, Pune. She is currently visiting faculty at Maharashtra University of Health Sciences. She is Member and Chairperson of Institutional Ethics committees of various medical and research institutions. She has several national and international publications to her credit. She is also master trainer for training programs in reproductive health for Govt of Maharashtra.
PREMNATH VENUGOPALAN
Dr. V. Premnath Founding Director – Venture Center and Head, NCL Innovations.He holds a B.Tech. from the Indian Institute of Technology - Bombay and a Ph.D. from the Massachusetts Institute of Technology, USA. He has also been a Chevening Technology Enterprise Fellow with the Centre for Scientific Enterprises, London Business School and Cambridge University, UK. He brings with him considerable experience in technology development and commercialization, working with start-up companies (in Cambridge-UK and India) and engaging with large corporations on research and consulting projects as project leader.

Reproductive, Maternal, Newborn and Child Health in India
Page 18 of 18
Appendix 2:
Photos
*****