Embed Size (px)
Citation preview

inform | transform | outperform Proprietary & Confidential inform | transform | outperform Proprietary & Confidential
Reports on the health status of the Roma population in the EU
& data collection in the Member States
David Murray - Head of Public Health, Optimity Matrix, London, UK
Consumer Health and Food Executive Agency - European Commission
Expert Group on Social Determinant of Health & Health Inequalities: 22 October 2014 Luxembourg

inform | transform | outperform Proprietary & Confidential 2
Project scope, concept & structure
Objectives & methods
Indicator findings
Conclusions & recommendations
Presentation overview

inform | transform | outperform Proprietary & Confidential 3
• Roma health issues are widely acknowledged
• The project & report considers 2 Roma health
issues:
–Health status (Part 1)
–Health data collection (Part 2)
• Full & executive summary versions of the reports
are available http://ec.europa.eu/health/social_determinants/docs/2014_roma_health_report_en.pdf
• The presentation provides an overview of both
Scope & structure

inform | transform | outperform Proprietary & Confidential 4
Source: WHO Regional Office for Europe (2010). ”How health system can address health inequities linked to migration and ethnicity”.
Copenhagen, WHO Regional Office for Europe. (p.14)
Concept

inform | transform | outperform Proprietary & Confidential 5
Project scope, concept & structure
Objectives & methods
Indicator findings
Conclusions, recommendations & challenges
Presentation overview

inform | transform | outperform Proprietary & Confidential 6
• Study objectives: provide the most up-to-date picture about Roma health status and data collection in this area
• Methodology:
o Evidence review of literature on Roma health, covering 2008-2013 o Interviews with experts o Delphi survey with stakeholders and national contact points
• We considered study findings relating to both: – Determinants of health & health status the outcomes of the studies (7 main
indicators (all countries) & 19 granular indicators (11 countries) – Data collection mechanisms & strategies
• 31 countries analysed (EU-28 plus Iceland, Liechtenstein and Norway) on the
basis of 7 indicators. • Focus on 11 countries with large (indigenous and migrant) Roma populations:
Bulgaria, Croatia, the Czech Republic, France, Greece, Italy, Hungary, Romania, Slovakia, Spain, and the United Kingdom.
• Implemented in collaboration with:
– Centre for the Study of Democracy, European Public Health Alliance & individual national researchers
Objectives & methods

inform | transform | outperform Proprietary & Confidential 7
Methods: health indicators

inform | transform | outperform Proprietary & Confidential 8
Project scope, concept & structure
Objectives & methods
Indicator findings
Conclusions, recommendations & challenges
Presentation overview

inform | transform | outperform Proprietary & Confidential 9
• Life expectancy data is very limited on a national and regional level. Most data is
based upon estimates. The most widely cited data stems from the Council of
Europe.
• The Roma population is noticeably younger than non-Roma across Europe.
• Roma experience substantially lower (up to 20 years) life expectancy compared
to non-Roma.
• Shorter life expectancy for Roma occurs as a result of the broader environmental
conditions they experience.
• Higher rates of infant mortality are reported in some Roma populations (those
living in poor housing, with low educational levels and migrant Roma) compared
to non-Roma (Bulgaria, the Czech Republic, Hungary, Italy and Slovakia).
Mortality & life expectancy

inform | transform | outperform Proprietary & Confidential 10
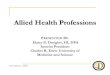
Mortality & life expectancy
Country Estimated Roma life expectancy compared
to non-Roma Austria Estimated but not quantified Belgium Estimated but not quantified Bulgaria -10 years Croatia -10 years The Czech Republic -5 to -10 years Finland Estimated but not quantified Hungary -9 years Ireland -5 to -10 years Italy -20 years The Netherlands -12 years Poland Estimated but not quantified Romania -12 years Slovakia -5 to -10 years Slovenia Estimated but not quantified
Spain -7 years The United Kingdom -2 to -10 years
Estimates of Roma life expectancy years compared to non-Roma by country

inform | transform | outperform Proprietary & Confidential 11
• Barriers to access health care services are closely linked to social exclusion
factors:
– Language and literacy barriers
– A lack of knowledge of available health care systems
– Discrimination by health care professionals
– A lack of trust in health professionals
– Physical barriers – mobility and distance
– A lack of identification and/or insurance.
• Patterns of health care utilisation among Roma differ from the general population.
– higher levels of use of acute hospital services, because of lower levels of
engagement with access to preventive primary care.
• The economic crisis is disproportionately impacting on Roma populations’ access
to health care.
Access to and use of health services and prevention programmes

inform | transform | outperform Proprietary & Confidential 12
Access to and use of health services and prevention programmes
Respondents aged 18 and above with medical insurance (%)

inform | transform | outperform Proprietary & Confidential 13
• Recent comprehensive data on infectious diseases within Roma communities is not readily available
• Data obtainable are: – often old
– small-scale research
– collected during disease outbreaks.
• Higher rates of infectious diseases or risk of infectious disease outbreaks amongst Roma (including Measles and Hepatitis A)
• Evidence relating to rates of HIV/Aids is more mixed, though some reports find faster disease progression.
• Roma have lower or much lower childhood vaccination rates (exceptions are Croatia, Hungary and Czech Republic)
Prevalence of major infectious disease & immunization uptake

inform | transform | outperform Proprietary & Confidential
Prevalence of major infectious disease & immunization uptake
Percentage of Roma measles cases compared with the general population and GDP, by region, 2010, Bulgaria

inform | transform | outperform Proprietary & Confidential 15
• Data on health lifestyles and behaviours among Roma populations are limited
• Roma people have poorer health related lifestyles.
• Healthy diet and physical activities to stay healthy are less common in the Roma population.
• Data on smoking from Austria, Croatia, the Czech Republic, Slovakia, Bulgaria, Hungary, Ireland, Portugal and Romania consistently show smoking is more common in the Roma population.
• Evidence on alcohol and illicit drug consumption amongst Roma communities reports conflicting findings.
• Limited interventions for specifically targeting the health behaviours of Roma
(exceptions include drug rehabilitation programmes in Croatia, Finland, Ireland, Latvia and Lithuania).
Healthy lifestyles & behaviours

inform | transform | outperform Proprietary & Confidential 16
• European institutions (the FRA and Eurofound) publish the most comprehensive data on environmental and other socio-economic factors.
• The housing situation of Roma worse than the housing situation of non-Roma citizens
• In Germany, Lithuania and Sweden access to social housing and standards were comparable to the general population (Germany, Lithuania, and Sweden).
• Accommodation overcrowding is most severe in Slovakia and Hungary
• Roma usually have a lower level of education than non-Roma.
• Comparatively low educational attendance (Bulgaria, Greece and Romania) and Segregation remain challenges in Estonia and Germany
• Unemployment rates of Roma are higher than those of non-Roma. Particularly in Bulgaria, Croatia, Ireland, Lithuania, and Hungary.
Environmental and socio-economic determinants of health

inform | transform | outperform Proprietary & Confidential 17
• Higher rates of chronic disease (i.e. asthma, diabetes, cardiovascular
disease, and hypertension) and the associated disability and limitations
on daily activities.
• Small scale studies highlight dramatically higher and more complex
cases of chronic disease amongst Roma across a range of European
Countries (Germany, Finland, Poland, the UK (migrant Roma), Romania,
Ireland, Italy, Spain and France).
• There is link between higher rates of chronic disease and:
- higher prevalence of risk factors (e.g. diet, exercise, stress),
- poor access to and uptake of primary care
- preventive health programmes among Roma.
Prevalence of major chronic diseases

inform | transform | outperform Proprietary & Confidential 18
• Roma women are generally in worse health and more disadvantaged than Roma men and non-Roma alike.
• Expectations to fulfil traditional gender roles:
– limited educational and employment opportunities,
– physical and social isolation and
– poor living conditions
• Maternal health risks (i.e. early and late pregnancies, large families, poor access to and low uptake of antenatal care) and poor outcomes (i.e. miscarriage and still birth) are more common in Roma women.
• Roma women are at higher risk of domestic violence and associated mental health risks.
• A Spanish study reported:
– position of Roma women had improved as a result in part due to lower birth rates, but
– they suffer from obesity, depression, metabolic diseases, and sexual health problems;
– they exercise less
– had lower uptake of breast and cervical cancer screening.
• Mediation Programmes in France is effective to engage with Roma women about health issues
Factors related to the role of women in the Roma community

inform | transform | outperform Proprietary & Confidential 19
Scope, concept & structure
Objectives & methods
Indicator findings
Conclusions, recommendations & challenges
Presentation overview

inform | transform | outperform Proprietary & Confidential 20
• In line with previous findings, the evidence currently available for the comprehensive indicators included in this project continue to demonstrate that, notwithstanding some variation between countries, Roma populations in Europe generally:
– Suffer greater exposure to wider determinants of ill health (e.g. socio-economic and environmental).
– Live less healthy lifestyles.
– Have poorer access to and lower uptake of primary care and preventive health services.
– Suffer poorer health outcomes, in terms of morbidity from both infectious and chronic diseases, and shorter life expectancy.
• Furthermore there are some indications that, as a result of the economic crisis and subsequent recessions in European countries, Roma health status and health access is deteriorating further in a number of places as a result of cutbacks.
Overall conclusions

inform | transform | outperform Proprietary & Confidential 21
• Public health interventions continue to be required across Europe to improve the
health of Roma.
• Wider determinants of health
– Access to and engagement with educational systems;
– Improvement of employment opportunities;
– Reductions in segregation and marginalisation;
– Improvements in the provision of facilities with improved living conditions.
• Healthy lifestyles and behaviour
– Provision of tailored health information materials;
– Community initiatives to improve health engagement in Roma communities.
• Disease prevention
– Improved information provision and marketing of disease prevention opportunities and services to Roma communities;
– Adequate provision of tailored disease prevention programmes and services acceptable to Roma communities and meeting their particular needs (e.g. mobility and living circumstances).
Recommendations I

inform | transform | outperform Proprietary & Confidential 22
• Improving accessibility to high-quality services that are acceptable to Roma communities – Provision of tailored health services that are acceptable to Roma communities
– Adherence to good practice standards (including discrimination) in the provision of health services to Roma by universal health care providers and professionals.
• Knowledge underpinning programmes: – Improving generation of consistent information on the health risks and outcomes
experienced by Roma communities to monitor progress, tailor action and target resources.
– Monitoring and evaluation of interventions to improve Roma health (i.e. European Structural Fund Technical Assistance).
– Translating effective interventions into best practice guidelines for policy-makers and programme mangers
– Primary research into key obstacles in improving Roma health
– Conclu the debate on the collection of data on the base of ethnicity (i.e. poverty mapping)
– Roma population should be compered with non Roma population in the same socio-economic conditions
• Investment and Funding – Investment in Roma health issues should be reviewed through systematic processes
examining the size and needs of Roma communities
Recommendations II

inform | transform | outperform Proprietary & Confidential 23
• Meaningfully characterising the diversity of Roma
communities across & within EU countries
• Political commitment – EU, national, & local
• Austerity & legitimacy of investment
• Effective community engagement
• Sensitivity to risks of alienation
• Prejudice & education of health professionals
• Data collection
• Engagement beyond the health sector (i.e. holistic
approach)
Challenges

inform | transform | outperform Proprietary & Confidential 24
For questions or comments please contact:
David Murray - Senior Associate: Head of Public Health
Laura Todaro - Consultant
Thanks!
Optimity Matrix
Kemp House, 152-160 City Road
London EC1V 2NP
+44 (0)20 7553 4800
The information, materials and opinions in this presentation (the "Information") are intended to describe the activities of Matrix knowledge only. It
should not be used for any other purpose or in any other context and Matrix accepts no responsibility for its use in either regard.
In keeping with our values of integrity and excellence, Matrix has taken reasonable professional care in the preparation of this
document. Although Matrix has made reasonable efforts, we cannot guarantee absolute accuracy or completeness of information, data and any
other sources used in producing this document.
This document has been produced on the basis of the information and explanations made available to Matrix at the time this document was
prepared. Accordingly, no representation or warranty, express or implied, is given and no responsibility or liability is accepted by or on behalf of
Matrix or by any of its employees or agents or any other person as to the accuracy, completeness or correctness of the information contained in
this document or any oral information made available and any such liability is expressly disclaimed.
To the fullest extent possibly, Matrix disclaims any liability arising out of the use or non-use of this document and its contents, including any
action or decision taken as a result of such use or non-use.
Except where permitted under the provisions of confidentiality above, this document may not be made available, reproduced, retained or stored
beyond the period of validity, or transmitted in whole or in part to any person without Matrix’s prior written permission.
All copyright and other proprietary rights in this document remain the property of Matrix (unless otherwise provided in this document) and all
rights are reserved.
If you require any clarification or further information about this document, please contact Matrix on [email protected].

inform | transform | outperform Proprietary & Confidential 25
Annex
Additional findings indicators

This paper was produced for a meeting organized by Health & Consumers DG and represents the views of its author on thesubject. These views have not been adopted or in any way approved by the Commission and should not be relied upon as a statement of the Commission's or Health & Consumers DG's views. The European Commission does not guarantee the accuracy of the dataincluded in this paper, nor does it accept responsibility for any use made thereof.