Embed Size (px)
Citation preview
Vol. 34 No. 1S July 2007 Journal of Pain and Symptom Management S49
Special Article
Report of the Clinical ProtocolCommittee: Developmentof Randomized Trials for MalignantBowel ObstructionThomas Anthony, MD, Todd Baron, MD, Sebastiano Mercadante, MD,Sylvan Green, MD, Dennis Chi, MD, John Cunningham, MD, FACP, FACG,Anne Herbst, MD, Elizabeth Smart, and Robert S. Krouse, MD, FACSDepartment of Surgery (T.A.), University of Texas, Southwestern Medical Center, and Veterans Affairs
North Texas Health Care System (T.A.), Dallas, Texas; Gastroenterology and Hepatology Department
(T.B.), Mayo Clinic-Rochester, Rochester, Minnesota; Oncology Department (S.M.), La Maddalena
Cancer Center, Palermo, Italy; Department of Biometry (S.G.), Arizona Cancer Center, University of
Arizona, Tucson, Arizona; Department of Surgery (D.C.), Memorial Sloan-Kettering Cancer Center,
New York, New York; Division of Gastroenterology (J.C.) and Department of Surgery (A.H., R.S.K.),
University of Arizona College of Medicine, Tucson, Arizona; National Coalition for Cancer
Survivorship (E.S.), Silver Spring, Maryland; and Southern Arizona Veterans Affairs Health Care
System (R.S.K.), Tucson, Arizona, USA
AbstractMalignant bowel obstruction (MBO) is a commonly encountered palliative care problem.There have been very few comparative trials in this area, and consequently there is verylittle clinical evidence upon which therapy can be rationally based. The purpose of thispaper is to highlight the discussion and decision-making process that was undertaken bythe Clinical Protocol Subcommittee during the development of a proposed clinical trial ofbest medical care versus surgical or endoscopic treatment for MBO. The development ofthe proposed clinical trials followed an orderly process. The first step taken wasa discussion of a specific definition for MBO. Once agreed upon, this definition helpedidentify inclusion and exclusion criteria for the proposed trial. This was followed by anextensive literature review, which helped define both surgical and endoscopic approachesto MBO as well as what constituted best medical care. An extensive discussion wasthen undertaken concerning the best outcome measure of success for medical, surgical,and endoscopic interventions. All of the above steps culminated in two proposedprotocols, one for MBO of the small intestine distal to the ligament of Treitz anda second for colonic obstructions. The small intestinal trial is designed to comparesurgical intervention versus best medical care, whereas the colonic trial seeks to comparesurgery with endoscopically-placed intraluminal stents coupled with best medical
Address reprint requests to: Thomas Anthony, MD, VANorth Texas Health Care System, 5323 Harry HinesBlvd., Dallas, TX 75390-9155, USA. E-mail:[email protected]
� 2007 U.S. Cancer Pain Relief CommitteePublished by Elsevier Inc. All rights reserved.
Accepted for publication: April 18, 2007.
0885-3924/07/$esee front matterdoi:10.1016/j.jpainsymman.2007.04.011

S50 Vol. 34 No. 1S July 2007Anthony et al.
care. J Pain Symptom Manage 2007;34:S49eS59. � 2007 U.S. Cancer PainRelief Committee. Published by Elsevier Inc. All rights reserved.
Key WordsMalignancy, bowel obstruction, clinical trial
IntroductionMalignant bowel obstruction (MBO) is
a common palliative care problem for whichthere is no defined algorithm of care. A majorgoal of the International Conference on MBOwas to develop the framework for clinical trialsthat would help address some of the questionssurrounding this clinical dilemma, includingthe efficacy of operative and nonoperativeforms of palliation. The two trials proposedby the Clinical Protocol Committee are basedon location of the intestinal obstruction. Thefirst trial intends to include patients with smallbowel obstructions distal to the ligament ofTreitz (LT) as well as multisite colonic block-ages. These patients will be randomized to un-dergo either operative decompression or bestmedical management. The second trial will in-clude patients with solitary obstructions of thecolon and rectum, and patients will be ran-domized to undergo either surgical decom-pression or endoscopic stent placement. Thefollowing article describes the backgroundfor, and clinical issues relevant to, these pro-posed trials for treatment of MBO. The com-mittee has addressed many of the majorissues and come to reasonable consensus, in-cluding an algorithm for a future trial. Thispaper hopes to clarify the thought processesand decision making for the conclusionsdrawn related to these palliative care trials.
Definition of Malignant BowelObstruction and Developmentof Inclusion and Exclusion Criteria
One of the more difficult tasks facing the In-ternational Conference on MBO and the Clin-ical Protocol Committee was deciding how todefine MBO for a clinical trial, and secondarilyspecifying inclusion and exclusion criteria. Pa-tients with underlying malignancy who are ad-ditionally suffering from signs and symptoms
of bowel obstruction represent a difficult diag-nostic and therapeutic challenge. In distinc-tion to nonmalignant bowel obstruction,there are multiple complicating factors thatare unique to the individuals with underlyingmalignancy. These additional factors may beentirely or partially responsible for the clinicalpicture of MBO. Altered motility from tumorinfiltration of the celiac and myenteric plexus,anticholinergic medication, opioids, and elec-trolyte imbalances due to malignancy (e.g., hy-percalcemia, hypokalemia) can all contributeto a bowel obstruction-like pattern for patientswith advanced cancer. These factors need to beconsidered when assessing a patient for thepossibility of MBO.
The committee felt that the first step towarddeveloping a clinical trial was to specify the cri-teria that would be used to define patients forinclusion in the studies. In fact, variability ininclusion criteria and definitions is one ofthe major problems in the MBO literature,and one reason why there is such wide varia-tion in findings. The committee’s definitioncriteria for MBO are outlined in Table 1. First,the patient must have clear clinical criteria ofa bowel obstruction. This is based on history,physical examination, and radiological criteria.In addition, the committee felt it was impor-tant that each patient have a computed tomog-raphy (CT) scan of the abdomen to clearlydocument findings related to obstruction (di-lated proximal bowel, a transition point, de-compressed distal bowel, etc.) as well as eitherindirect or direct evidence of cancer-relatedfindings, such as carcinomatosis, evidence
Table 1Definition of Malignant Bowel Obstruction
1. Clinical evidence of a bowel obstruction (via history/physical/radiographic examination).
2. Bowel obstruction beyond the LT.3. Intra-abdominal primary cancer with incurable disease.4. Non-intra-abdominal primary cancer with clear
intraperitoneal disease.

Vol. 34 No. 1S July 2007 S51Randomized Trial Development for MBO
of metastatic disease, or ascites. Second, be-cause the location of an MBO can determinethe treatment options, the committee felt itnecessary to concentrate on specific parts ofthe intestine. Obstructions proximal to theLT are commonly treated endoscopically, ei-ther with dilatation, stenting, ablation, ora combination of techniques. The committeefelt that there was little controversy concern-ing the endoscopic approach as the primarytreatment modality for obstructions in theselocations. There was general agreement thattreatment decisions became less clear forthe obstructions beyond the LT. Therefore,obstructions beyond the LT became the focusof the proposed clinical trials. Third, priordocumentation of an intraperitoneal cancer(e.g., colorectal, ovarian, or gastric cancer,carcinoid, etc.) and incurable disease wouldbe required for inclusion in the study. Fourth,for the rare, but known patient with a primarynonintraperitoneal cancer (e.g., lung orbreast cancer) and a bowel obstruction, therewould have to be clear evidence, either viaa previous procedure or radiological studies,of intraperitoneal metastases.
Bowel obstruction is occasionally the firstpresentation of a patient with intra-abdominalmalignancy. Retrospective and autopsy serieshave suggested that intestinal obstruction oc-curs in 5%e51% of ovarian cancer patientsand in 10%e28% of gastrointestinal cancers.1
Obstruction is also thought to be more com-mon among late-stage tumors. Despite theassociation with late-stage disease, many indi-viduals presenting with obstruction can becured, as can individuals with obstructionsdue to limited local recurrence of disease.Because individuals who present either withprimary obstructing cancers or with limited lo-cal recurrence can potentially be treated forcure, it was deemed inappropriate for these pa-tients to be included in a trial that includedpossible randomization to a noncurativetreatment.
For patients with MBO in the context ofprior history of cancer treatment, the questionfrequently arises whether or not the patienthas a recurrence of their cancer as the etiologyfor the obstruction. Bowel obstruction frommalignancy often occurs as a slowly progressiveprocess, with gradual worsening of symptomsover an extended period of time. Only very
infrequently is emergency surgery required.2
It is widely recognized that not all patientswith a prior history, or even current evidence,of intra-abdominal malignancy, who presentwith bowel obstruction, will have a malignantetiology for this obstruction. Adhesions fromprior surgery, radiation enteritis, chronicischemia, inflammatory bowel disease, and var-ious infections are some examples of potentialnonmalignant sources of mechanical obstruc-tion. In these situations, the likelihood thatan obstruction is due to a recurrence of malig-nancy is related to a number of factors, includ-ing the original stage of the malignancy, timeelapsed since surgery, and the presence ofother signs or symptoms of recurrent/meta-static disease. None of these historical factorsare, however, sufficient to differentiate MBOfrom nonmalignant etiologies. Studies have es-timated that benign causes of bowel obstruc-tion will be present in 3%e48% of patientswho present with obstruction after abdominalsurgery for cancer.3e5 The clinical presenta-tion of patients with nonmalignant obstructionand MBO is often indistinguishable. In the ma-jority of patients, physical examination does notprovide help in differentiating benign from ma-lignant obstruction. It is frequently difficult toidentify the source of an obstruction even withradiologic evaluations. Plain films can offer con-firmatory evidence of bowel obstruction, butrarely provide enough information to definethe source of bowel obstruction. CT and mag-netic resonance imaging (MRI) have beenused to help evaluate both the location andthe likely etiology of bowel obstruction.
Both CT and MRI are very good with respectto differentiation of partial and completebowel obstruction.6,7 These studies have, how-ever, been much less accurate in defining theetiology of the obstruction. With improvingtechnology, there have been more encourag-ing preliminary reports concerning theaccuracy of radiological differentiation ofbenign and malignant obstruction. Low andcolleagues, for example, recently reported sen-sitivity, specificity, and accuracy of approxi-mately 90% in identifying the etiology of theobstruction using gadolinium-enhanced MRIand criteria that included the presence of anobstructing mass, focal mural thickening, orevidence of disseminated abdominal tumor.8
At this point, however, neither CT nor MRI

S52 Vol. 34 No. 1S July 2007Anthony et al.
possesses a sufficient specificity to reliably dif-ferentiate benign from malignant causes of ob-struction. Therefore, despite improvements inimaging technologies, intraoperative patho-logic findings remain the gold standard for eti-ologic diagnosis.
Given that preoperative definition of the eti-ology of an obstruction in the setting of priorintra-abdominal cancer is often impossible,requiring defining the underlying etiology ofthe obstruction prior to patient enrollment isimpractical. However, since this trial focuseson patients with advanced incurable cancer,the etiology of the obstruction becomes a lessimportant consideration. Indeed, it is reason-able to treat patients with nonmalignant ob-structions nonoperatively because there isevidence that this is unlikely to cause complica-tions.9,10 Randomization of patients will alsoprovide some assurance of equal representa-tion of both nonmalignant and malignant ob-structions in each of the proposed treatmentarms. On the basis of this reasoning, a consen-sus was obtained that clear documentation ofan obstruction due to tumor was not necessaryfor patient inclusion.
Proposed inclusion and exclusion criteriafor a study are outlined in Table 2. Overall,these criteria reflect the desire to be as specificas possible to clearly identify patients for inclu-sion without making criteria so stringent as tohamper accrual to the trial.
Rationale for Treatment Algorithmsfor MBO
Many treatments have been used in an at-tempt to palliate MBO that is distal to theLT. These treatments can be broadly classifiedas surgical, endoluminal, and medical. Thereis, at this time, no standard approach tochoosing treatment for many presentationsof MBO. The primary goal in performingthe proposed clinical trials is to specificallyassess two potential therapeutic options fortreatment of MBO.
Upon presentation to the hospital, the nor-mal treatment course for a patient with a his-tory of advanced cancer and signs andsymptoms consistent with a bowel obstructionis to undergo intravenous (IV) hydration, beallowed nothing by mouth, and to undergo
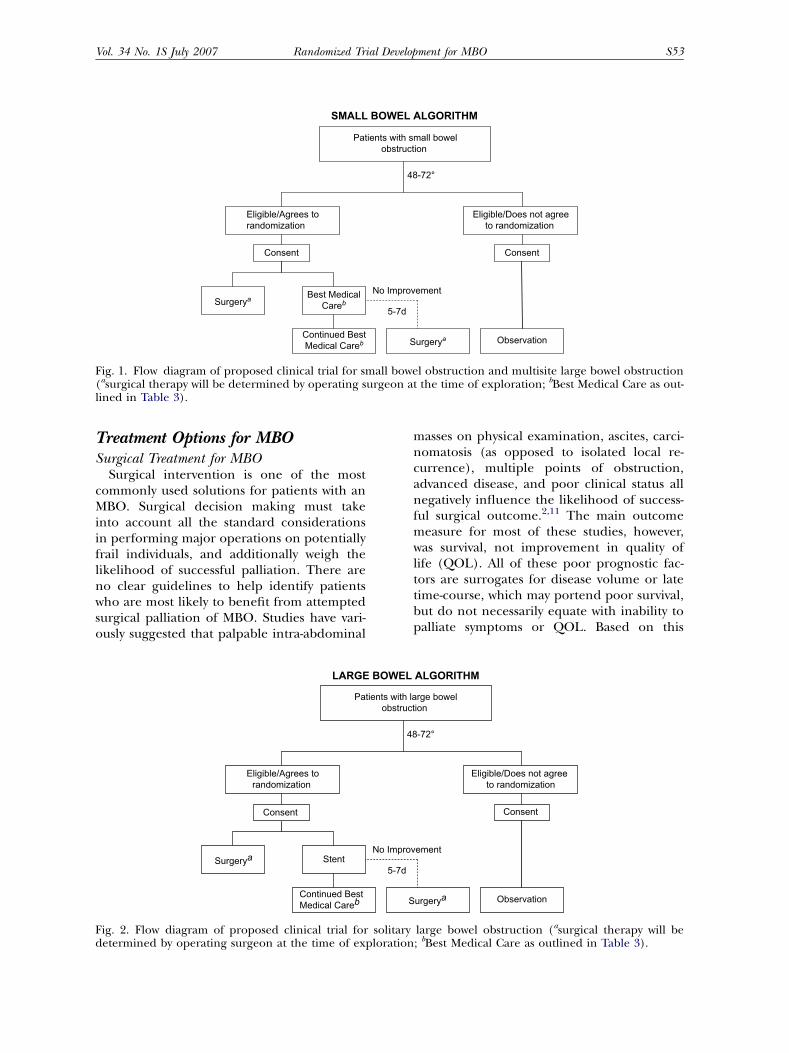
nasogastric tube decompression. A portion ofpatients will improve to the point of allowingresumption of oral intake with these standardinterventions. Although there are no dataregarding the percentage of patients likely toimprove with simple supportive measures, thecommittee believes that a much greater per-centage will actually require further treatment.Accordingly, the committee has proposed thatafter 48 hours of supportive treatment andwith a lack of symptom resolution, consentingpatients would undergo randomization. Thiswould give physicians time to ensure thatproper pre-study testing had been accom-plished, to participate in discussions with pa-tients and families concerning treatment andother end-of-life issues, and to obtain agree-ment concerning appropriateness of inclusionof the patient in the study by both the surgicaland gastroenterological teams. Patients wouldbe randomized to undergo surgical decom-pression versus either endoscopic stenting orbest medical care depending on the locationof their obstruction. Specifically, obstructionof the small bowel and multisite colon wouldbe randomized to either surgical interventionor best medical care. Patients with solitaryobstructions distal to the cecum would be can-didates for randomization between surgical de-compression and endoluminal stenting (seeFigs. 1 and 2).
Table 2Additional Study Inclusion
and Exclusion Criteria
Inclusion criteria1. Compatible with definition of MBO.2. Admission to hospital.3. Patients must be candidates for an intra-abdominal
procedure and the attendant anesthetic techniquerequired.
4. Proxy identified and involved in consent process.5. Age $18 years old.6. Performance status (Karnofsky >60% one week
prior to admission).
Exclusion criteria1. Patients in whom treatment for cure is still possible.2. Patients with obstruction requiring emergency
surgery, including sepsis, signs of perforation, or‘‘acute’’ abdomen on examination.
3. Patients who are incapable of tolerating a surgicalprocedure based on clinical status due to cancerstatus or other underlying medical problems.
4. Actively dying based on defined criteria.5. Bowel obstruction that resolves with supportive
measures within 48 hours of admission.6. Inability to obtain informed consent.
Vol. 34 No. 1S July 2007 S53Randomized Trial Development for MBO
SMALL BOWEL ALGORITHM
Patients with small bowelobstruction
Surgerya
Eligible/Does not agreeto randomization
48-72°
Consent
No Improvement
Eligible/Agrees torandomization
Continued BestMedical Careb ObservationSurgerya
Consent
Best MedicalCareb 5-7d
Fig. 1. Flow diagram of proposed clinical trial for small bowel obstruction and multisite large bowel obstruction(asurgical therapy will be determined by operating surgeon at the time of exploration; bBest Medical Care as out-lined in Table 3).
Treatment Options for MBOSurgical Treatment for MBO
Surgical intervention is one of the mostcommonly used solutions for patients with anMBO. Surgical decision making must takeinto account all the standard considerationsin performing major operations on potentiallyfrail individuals, and additionally weigh thelikelihood of successful palliation. There areno clear guidelines to help identify patientswho are most likely to benefit from attemptedsurgical palliation of MBO. Studies have vari-ously suggested that palpable intra-abdominal
masses on physical examination, ascites, carci-nomatosis (as opposed to isolated local re-currence), multiple points of obstruction,advanced disease, and poor clinical status allnegatively influence the likelihood of success-ful surgical outcome.2,11 The main outcomemeasure for most of these studies, however,was survival, not improvement in quality oflife (QOL). All of these poor prognostic fac-tors are surrogates for disease volume or latetime-course, which may portend poor survival,but do not necessarily equate with inability topalliate symptoms or QOL. Based on this
Patients with large bowelobstruction
Surgerya
Eligible/Does not agree to randomization
48-72°
LARGE BOWEL ALGORITHM
Consent
No Improvement
Eligible/Agrees torandomization
Continued BestMedical Careb ObservationSurgerya
Consent
Stent5-7d
Fig. 2. Flow diagram of proposed clinical trial for solitary large bowel obstruction (asurgical therapy will bedetermined by operating surgeon at the time of exploration; bBest Medical Care as outlined in Table 3).

S54 Vol. 34 No. 1S July 2007Anthony et al.
limited clinical information, our group feltthat exclusion of any of these subgroups wasunwarranted.
When dealing with MBO, the type of opera-tion performed is in large measure dictated bythe intraoperative findings. Aggressive resec-tion of the tumor to relieve the obstruction isusually unwarranted. The simplest surgicaltechnique to restore intestinal continuity is of-ten the best strategy. This may include creationof stomas, intestinal bypass, resection of shortsegment of bowel, or a combination of thesetechniques. With increasing laparoscopic ex-pertise, it is also possible that many of thesepatients could be treated with a minimallyinvasive approach. Minimization of operatingtime and maximization of palliation often arecompeting issues, and the highest levels of sur-gical judgment need to be used to ensure thedesired outcome. A surgical arm to a clinicaltrial of treatment for MBO will not be able tostandardize surgery to a single option, at leastat this time. Given the wide range of individualpatient characteristics and the myriad surgicaloptions, the committee felt it best not to rec-ommend any standardized approach to surgi-cal intervention.
Small case series have suggested that the useof percutaneous decompressive procedures(either gastrostomy or jejunostomy) per-formed by interventional radiologists or endo-scopists may be of benefit to patients withMBO.12,13 Although there was some dissensionamong committee members, it was felt thatthese types of procedures differed substantiallywhen compared with traditional surgical pro-cedures in terms of anesthetic requirement,morbidity, patient acceptance, and outcome.Therefore, these procedures, for the purposeof the trial, will not be considered optionssolely for the surgical arm of the trial, butcan be used as an adjunctive treatment on ei-ther arm of this trial.
There are a number of possible negative out-comes for patients undergoing attempted sur-gical correction of MBO, including potentialmorbidity, mortality, and failure to achieve pal-liation. The rates of surgical morbidity andmortality have been extremely variable. Mor-bidity rates from 0% to 90% and 30-day mortal-ity rates from 0% to 41% have been reportedin recent series.2,14,15 These rates suggest thatimperfect surgical selection criteria are being
applied to patients with MBO. Therefore, a sec-ondary goal of the proposed study will be todevelop criteria that will help better select pa-tients for surgical intervention. Additionally,not all patients who are taken to the operatingroom for palliation of MBO will achieve thisgoal. Studies have suggested that between32% and 80% of patients taken to the operat-ing room will be successfully palliated.16,17
These studies are, however, hampered by theirretrospective nature and the lack of uniformcriteria for judging success. Endpoints thathave been used include survival, tolerance oforal intake at discharge, overall QOL, abilityto return home, and absence of recurrent ob-struction.11 Even when these endpoints aremet, a significant percentage of these individ-uals develop reobstruction (10%e50%),although the time to reobstruction remainspoorly characterized.18,19 The permanence ofpalliation should, therefore, be considered asan additional endpoint for a trial of palliation.
A recent Cochrane systematic review focus-ing on the role of surgery to treat MBO con-cluded that the role of surgery remainscontroversial.1 After evaluation of the availableliterature, the committee concurred with thisassessment. Although the literature suggeststhat symptoms can be controlled in many indi-viduals, the quality of this literature does notallow for assessment of selection bias or accu-rate assessment of potential negative outcomes,including morbidity, mortality, and rates ofreobstruction.
Best Medical Care for MBOUp until 1985, surprisingly little information
was available in support of nonoperative ap-proaches to MBO. In that year, Baines and col-leagues reported on the effectiveness of severalnonoperative measures in palliating patientswith MBO.20 Since that time, a number of stud-ies have reported on a variety of additionalnonoperative (largely pharmacologic) mea-sures to treat MBO. Currently, palliative carepractitioners use a combination of medica-tions, usually including analgesics, antiemetics,and antisecretory agents. Best medical care forthis study would entail choices from each ofthese medication groups (Table 3). In addi-tion, treatments can include insertion of a per-cutaneous endoscopic gastrostomy tube (PEG)

Vol. 34 No. 1S July 2007 S55Randomized Trial Development for MBO
or total parenteral nutrition (TPN) at the dis-cretion of the research teams.
Analgesic Agents. Pain is a prominent com-plaint in patients with MBO. Pain may be char-acterized as either continuous or colicky innature. There are very limited data that per-tain to pain control in patients with MBO. An-ecdotal evidence suggests that for continuouspain, opioids such as continuous IV morphineinfusions are required.2 Due to the depressiveeffect on bowel motility, these agents may alsorelieve colicky pain. However, if colicky painpersists after opioid infusion, many experts ad-vocate the addition of an anticholinergicagent, such as hyoscine butylbromide (HB).21
This agent is more useful than hyoscine hydro-bromide because it does not cross the blood-brain barrier and is, therefore, less sedating.One prospective, randomized trial has re-ported that both scopolamine butylbromideand octreotide (the longer-acting somatostatinanalogue) had favorable effects on colicky andcontinuous pain in the setting of MBO.22
Antiemetic Agents. Two of the most debilitatingsymptoms for patients with MBO are nauseaand vomiting. A recent systematic review ofthe effectiveness of antiemetic therapy in thesetting of obstructed cancer patients foundvery variable rates of successful antiemetictherapy.23 Specifically, much higher rates of re-sponse were reported in uncontrolled trials(75%e93%) compared with randomized con-trolled trials (response rates 23%e36% fornausea and 18%e52% for vomiting). Empirictherapy was as effective as therapy based onthe patient’s clinical picture. The evidence in
Table 3Best Medical Care
AntisecretorySomatostatin analoguesa
AnticholinergicsCorticosteroids
AntiemeticsHaloperidolProchlorperazine
Pain medicationsMorphineMethadone
PEG/TPN per team decision
aMandatory for Best Medical Care arm.
favor of the use of many commonly usedagents, such as haloperidol, prochlorperazine,cyclizine, and olanzepine, was characterized asweak to nonexistent. There was some evidenceto support the use of metoclopramide (com-pared with placebo), levosulpride (a dopa-mine antagonist) versus metoclopramide, andserotonin antagonists compared with tradi-tional antiemetics. The overall evidence in sup-port of antiemetics was surprisingly weak.23
Steroids are often used in patients withMBO and are widely thought to have anti-emetic properties. They appeared to be some-what effective in resolution of obstruction, butthere are no data concerning their effective-ness as antiemetics. Resolution of bowel ob-struction with corticosteroids has been thesubject of a Cochrane review. This review con-cluded that when only randomized trials wereconsidered, there was a nonsignificant trendfor the resolution of obstruction when cortico-steroids were used (dexamethasone 6e16 mg/day given intravenously).24
Antisecretory Agents. The antisecretory agentthat has shown the most promise in the treat-ment of MBO is octreotide. Many of the nega-tive consequences of bowel obstruction can belinked to gut hormones such as vasoactiveintestinal polypeptide (VIP). Increased secre-tion of VIP during episodes of obstructionhas been linked to increased bowel hyperemia,edema, luminal secretion, and nonproductiveperistaltic activity.25,26 Octreotide is effectiveat suppressing VIP, along with several otherstimulatory gut hormones. Octreotide can beadministered subcutaneously or intravenouslyusing either continuous or intermittent dosingschedules. In the bowel, octreotide decreasesthe secretion of water, sodium, and chloride.Octreotide also improves electrolyte and waterabsorption, suppresses stimulatory gut andpancreatic secretions, decreases bowel peristal-tic activity, and reduces splanchnic blood flow.The general inhibitory effect of octreotidemay, therefore, help break the cycle of secre-tion, distension, and bowel hyperactivity thatcomplicates bowel obstruction.27 A limitednumber of studies of the effectiveness of oc-treotide in the treatment of MBO have beenperformed. Successful utilization of octreotidewas reported in three cases series.28e30 Al-though differing doses were reported in each

S56 Vol. 34 No. 1S July 2007Anthony et al.
study, octreotide had a positive effect on symp-toms. Vomiting was alleviated (usually withinone hour), and nasogastric tubes were eitherremoved or volumes aspirated were dramati-cally reduced. Importantly, almost no side ef-fects were reported.
Based on the successes reported in thesecase series, larger prospective trials were un-dertaken. Three prospective studies havebeen reported to date.22,31,32 The results ofthese studies verified the encouraging resultsnoted in the original case series. Specifically,vomiting was controlled in 39/51 (76%) pa-tients; if a nasogastric tube was used prior to in-stituting octreotide therapy, these tubes weremost often removable or aspirated volumes sig-nificantly reduced. In a prospective, random-ized, follow-up study comparing 0.3 mg/daydosing of octreotide with 60 mg/day of scopol-amine butylbromide in 17 patients (seven in-patients and 10 home care patients) withinoperable MBO, both treatments were suc-cessful in diminishing pain and allowing naso-gastric tube removal. The volume of secretionon Treatment Days 2 and 3 was significantlylower in the patients treated with octreotide.22
A second prospective randomized trial in 18patients with inoperable obstruction com-pared a 0.3 mg/day dose of octreotide to60 mg/day HB. This study found that octreo-tide was more effective at controlling gastroin-testinal symptoms: patients treated withoctreotide had fewer episodes of emesis anddecreased intensity of nausea compared withHB-treated patients.31 A final larger random-ized, controlled, double-blind trial of 68 pa-tients, assigned patients to receive eitherchlorpromazine (15e25 mg/day) plus HB(60e80 mg/day) or octreotide (0.6e0.8 mg/day). Nausea, vomiting, anorexia, and fatiguewere all noted to be better for patients receiv-ing octreotide.32
Based on the preliminary information pre-sented above, the Clinical Protocol Committeefelt that octreotide is a potential alternative tosurgery in patients with MBO. Although thedose and duration of treatment varied amongstudies, the expert opinion was for a dose of0.2 mg three times a day. It was felt that itwas reasonable to expect a significant responseby Day 5. It should be noted that a patient whodevelops signs and symptoms requiring opera-tion or in whom there is no symptomatic
improvement within 5e7 days on best medicalcare could cross over to the surgical interven-tion arm (see Fig. 1).
Endoluminal Stenting of Colonic Lesionsfor Palliation of MBO
For obstructions located distal to the cecum,surgical treatment will be compared with endo-luminal stenting. Experience with the use ofexpandable stents to palliate obstruction is ac-cumulating. Expandable stents can be placedas proximal as the cecum and as distal as therectum, as long as there is a margin of about2 cm from the anus. In addition to the pallia-tion of primary colon cancers, colorectal stentscan be used to treat extrinsically compressingprocesses such as pelvic cancers, regional me-tastases, and lymphadenopathy. Contraindica-tions to colorectal stent placement includeknown or suspected colonic ischemia or perfo-ration, multiple sites of obstruction, and stan-dard endoscopy contraindications. Thepresence of any of these factors will precludepatient entry into the trial.
Comprehensive Reviews of Colonic Stenting. Theefficacy and safety of colorectal stents havebeen systematically reviewed. Clinical successin the palliative stent patients was achieved in302/336 (90%). Complications included per-foration, migration, reobstruction, bleeding,and pain. Interventional mortality rate was1% (3/598). Stent migration was observed in10% of patients (54/551) and was managedwith stent removal or replacement or opera-tion. Reobstruction resulted from tumor in-growth (62%; 32/52), fecal impaction (25%;13/52), and migration (13%; 7/52) and wasmore common among palliative patients.Bleeding occurred in 5% (27/525). In mostcases, bleeding resolved spontaneously within24 hours.33
A pooled analysis by Sebastian et al. evalu-ated self-expanding metal stents for themanagement of patients with malignant colo-rectal obstructions.34 In palliative patients(n¼ 791), clinical success was defined as co-lonic decompression within 48 hours withoutneed for additional intervention. The techni-cal success rate in palliative patients was 93%.Cumulative technical and clinical success ratesfor palliated patients were 93% and 91%, re-spectively.34 Most cases of reobstruction can

Vol. 34 No. 1S July 2007 S57Randomized Trial Development for MBO
be treated endoscopically. Based on the en-couraging rate of palliation and the low rateof complications, it was felt that this wouldbe an appropriate treatment option to com-pare with surgical intervention for patientswith colonic obstructions.
Role of an Observational ArmThere are many publications related to
MBO, but there is little known about the natu-ral history for these patients. Although there isclear equipoise related to the major treatmentsfor many patients with MBO, making an RCTimportant, it also would be beneficial to in-clude an observational arm to such a study.There are many patients who may not be eligi-ble for this study but who could still provideimportant information. This may include pa-tients who are ineligible due to poor overallstatus, those patients wishing no further treat-ment, or those patients with a strong prefer-ence for a particular treatment option (i.e.,those not wishing to be randomized). Thecommittee felt that following these patientscould yield useful information. Informationconcerning treatment variability, treatment-re-lated morbidity, survival, and QOL could stillbe obtained albeit in an uncontrolled manner.This cohort database would be reflective ofcurrent standard practice and provide an addi-tional comparison group for the treatmentsunder study.
Statistical ConsiderationsThe statistical approaches for this study are
based on multiple considerations. More impor-tantly, an adequate primary outcome measuremust be devised to clearly delineate benefit orequality from the two treatment arms. As deter-mined during the conference, a composite mea-sure of QOL outcomes that can be clearlydocumented should be used as the primary out-come measure. This would be the number of‘‘good days,’’ defined as days out of the hospitalwithout a nasogastric tube or hydration. Thiswould mean that the patients are likely able totake in enough by mouth without needing addi-tional IV supplementation, as well as were notliving with problems related to nausea and vom-iting. The number of patients necessary for such
a study would also depend on the meaningfuldifference in ‘‘good days.’’ The median survivalof patients with MBO is approximately 10 weeks,and therefore, it was determined that a reason-able difference would be two weeks. If one canconsider such a limited life span, the confer-ence participants reasoned that two weeks of im-proved or alleviated symptoms represent animportant difference in outcome. The null hy-pothesis would be that the two treatment groupsare equivalent (difference in number of gooddays is zero). Available data from MemorialSloan-Kettering Cancer Center show a meannumber of good days (in 10 weeks) of 33 andstandard deviation of 25. To have 90% powerto detect a mean difference between treatmentgroups of 10 good days would require 133 pa-tients per group, based on a t-test at the two-sided 0.05 significance level. This correspondsto an effect size of 0.4. All patients who are ran-domized would be included in the analysis us-ing an intention-to-treat approach. Note thatfor detecting a difference of 14 days or greater(with 90% power), the required sample sizewould be approximately 70 patients per group.
SummaryMBO is a common problem that is faced by
clinicians, patients, and families. Preliminaryevidence suggests that there are various ap-proaches to the malady, especially dependingon the location of obstruction. No comparativetrials have been performed to date that haveassessed the potential role of these therapeuticapproaches in an unselected population of pa-tients with MBO. This paper outlines proposedclinical trials designed to compare differentapproaches for care of patients facing thisproblem.
As with the vast majority of issues in pallia-tive care, there is scant clinical evidence toguide therapy for these challenging patients.Current therapy is based on empiric decisionmaking, resulting in highly variable applica-tions and outcomes. Progress will only bepossible through the conduct of carefully con-trolled, prospective, randomized trials that arecarefully analyzed and reported. A trial com-paring therapies for MBO will help to defineeffective therapy, identify selection criteria,

S58 Vol. 34 No. 1S July 2007Anthony et al.
and serve as a model for future studies in pal-liative care.
References1. Feuer DJ, Broadley KE. Surgery for the resolu-
tion of symptoms in malignant bowel obstructionin advanced gynaecological and gastrointestinalcancer. [Cochrane Review]. In: The Cochrane Li-brary, Vol. 4. Chichester, UK: John Wiley & Sons,Ltd., 2004.
2. Ripamonti C, Bruera E. Palliative managementof malignant bowel obstruction. Int J Gynecol Can-cer 2002;12:135e143.
3. Ketcham AS, Hoye RC, Pilch YH, Morton DL.Delayed intestinal obstruction following treatmentfor cancer. Cancer 1970;25(2):406e410.
4. Osteen RT, Guyton S, Steele G Jr, Wilson RE.Malignant intestinal obstruction. Surgery 1980;87(6):611e615.
5. Legendre H, Vahhuyse F, Caroli-Bose FX,Pector JC. Survival and quality of life after palliativesurgery for neoplastic gastrointestinal obstruction.Eur J Surg Oncol 2001;27:364e367.
6. Maglinte DD, Heitkamp DE, Howard TJ,Kelvin FM, Lappas JC. Current concepts in imagingof small bowel obstruction. Radiol Clin North Am2003;41(2):263e283.
7. Delabrousse E, Destrumelle N, Brunelle S, et al.CT of small bowel obstruction in adults. AbdomImaging 2003;28(2):257e266.
8. Low RN, Chen SC, Barone R. Distinguishing be-nign from malignant bowel obstruction in patientswith malignancy: findings at MR imaging. Radiology2003;228(1):157e165.
9. Bastounis E, Hadjinikolaou L, Ioannou N, et al.Somatostatin as adjuvant therapy in the manage-ment of obstructive ileus. Hepatogastroenterology1989;36:538e539.
10. Mercadante S, Avola G, Maddaloni S, et al. Oc-treotide prevents the pathological laterations ofbowel obstruction in cancer patients. Support CareCancer 1996;4:393e394.
11. Krouse RS. Surgical management of malignantbowel obstruction. Surg Oncol Clin N Am 2004;13:479e490.
12. Cannizzaro R, Bortoluzzi F, Valentini M, et al.Percutaneous endoscopic gastrostomy as a decom-pressive technique in bowel obstruction due to ab-dominal carcinomatosis. Endoscopy 1995;27(4):317e320.
13. Cunningham MJ, Bromberg C, Kredentser DC,Collins MB, Malfetano JH. Percutaneous gastro-stomy for decompression in patients with advancedgynecologic malignancies. Gynecol Oncol 1995;59(2):273e276.
14. Higashi H, Shida H, Ban K, et al. Factors affect-ing successful palliative surgery for malignant bowelobstruction due to peritoneal dissemination fromcolorectal cancer. Jpn J Clin Onc 2003;33(7):357e359.
15. Yazdi GP, Miedema BW, Humphrey LJ. Highmortality after abdominal operation in patientswith large-volume malignant ascites. J Surg Oncol1996;62(2):93e96.
16. Turnbull AD, Guerra J, Starnes HF. Results ofsurgery for obstructing carcinomatosis of gastroin-testinal, pancreatic, or biliary origin. J Clin Oncol1989;7(3):381e386.
17. Lund B, Hansen M, Lundvall F, et al. Intestinalobstruction in patients with advanced carcinoma ofthe ovaries treated with combination chemotherapy.Surg Gynecol Obstet 1989;169(3):213e218.
18. Solomon HJ, Atkinson KH, Coppleson JV, et al.Complications in the management of ovarian can-cer. Aust N Z J Obstet Gynaecol 1983;23(2):65e68.
19. Phillip J, Do T, Hacker N, Grant P, Lickiss N.Outcomes in patients with GIT obstructiond62 ep-isodes in 33 patients in a 12 month period. [ab-stract]. Int J Gynecol Cancer 1997;7(Supp 2):86.
20. Baines M, Oliver DJ, Carter RL. Medical man-agement of intestinal obstruction in patients withadvanced malignant disease. Lancet 1985;2(8462):990e993.
21. Ripamonti C, Twycross R, Baines M, et al. Clin-ical-practice recommendations for the managementof bowel obstruction in patients with end-stage can-cer. Working Group of the European Assiciation forPalliative Care. Support Care Cancer 2001;9(4):223e233.
22. Ripamonti C, Mercadente S, Groff L, et al. Roleof octreotide, scopolamine butylbromide and hydra-tion in symptom control of patients with inoperablebowel obstruction and nasogastric tubes: a prospec-tive randomized trial. J Pain Symptom Manage2000;19:23e34.
23. Glare P, Pereira G, Kristjanson LJ, Stockler M,Tattersall M. Systematic review of the efficacy of an-tiemetics in the treatment of nausea in patients withfar-advanced cancer. Support Care Cancer 2004;12(6):432e440.
24. Feuer DJ, Broadley KE. Corticosteroids for theresolution of malignant bowel obstruction in ad-vanced gynaecological and gastrointestinal cancer.[Cochrane Review]. In: The Cochrane Library,Vol. 4. Chichester, UK: John Wiley & Sons, Ltd.,2004.
25. Basson MD, Fielding LP, Bilchik AJ, et al. Doesvasoactive intestinal polypeptide mediate the patho-physiology of bowel obstruction? Am J Surg 1989;157(1):109e115.
26. Neville R, Fielding LP, Cambria RP, Modlin I.Vascular responsiveness in obstructed gut. Dis Co-lon Rectum 1991;34(3):229e235.

Vol. 34 No. 1S July 2007 S59Randomized Trial Development for MBO
27. Ripamonte C. How to use octreotide for malig-nant bowel obstruction. J Support Oncol 2004;2(4):1e8.
28. Mercadante S, Maddaloni S. Octreotide in themanagement of inoperable gastrointestinal obstruc-tion in terminal cancer patients. J Pain SymptomManage 1992;7(8):496e498.
29. Khoo D, Riley J, Waxman J. Control of emesis inbowel obstruction in terminally ill patients. Lancet1992;339(8789):375e376.
30. Steadman K, Franks A. A woman with malignantbowel obstruction who did not want to die withtubes. Lancet 1996;347(9006):944.
31. Mercadante S, Ripamonti C, Casuccio A,Zecca E, Groff L. Comparison of octreotide and hy-oscine butylbromide in controlling gastrointestinal
symptoms due to malignant inoperable bowel ob-struction. Support Care Cancer 2000;8:188e191.
32. Mystakidou K, Tsilika E, Kalaidopoulou O, et al.Comparison of octreotide administration vs. conser-vative treatment in the management of inoperablebowel obstruction in patients with far advanced can-cer: a randomized, double-blind, controlled clinicaltrial. Anticancer Res 2002;22(2B):1187e1192.
33. Khot UP, Lang AW, Murali K, Parker MC. Sys-tematic review of the efficacy and safety of colorectalstents. Br J Surg 2002;89:1096e1102.
34. Sebastian S, Johnston S, Geoghegan T,Torreggiani W, Buckley M. Pooled analysis of the ef-ficacy and safety of self-expanding metal stenting inmalignant colorectal obstruction. Am J Gastroenter-ol 2004;99:2051e2057.