Embed Size (px)
Citation preview

British Journal ofOphthalmology, 1982, 66, 600-606
Apparent monoclonal origin of lymphocytes andplasma cells infiltrating ocular adnexal amyloiddeposits: report of 2 cases
D. R. LUCAS, FIONA KNOX, AND S. DAVIES
From the Departments of Ophthalmology and Pathology of the University of Manchester
SUMMARY Two cases of primary amyloidosis involving the orbit and lid respectively are described.Immunoperoxidase staining of the associated infiltrate of lymphocytes and plasma cells showed aclear preponderance of cells carrying light chains in one case and K in the other. The predominantheavy chains were IgA and IgG respectively. It is suggested that these cases are 'burnt out' localplasmacytomas.
Although not common, amyloid infiltration of the lidand conjunctiva has been reported on manyoccasions. But similar involvement of the orbit israre.' In most cases there is no history or evidence ofany pre-existing local or systemic disease. Clinicallythe condition appears as a slowly progressive painlessswelling involving lids or orbit.The pathogenesis of the amyloid deposits remains
obscure, but a consistent pathological feature isinfiltration by lymphocytes, plasma cells, and foreignbody giant cells.2 Though these cells may represent areaction to the deposition of amyloid, there is a strongpossibility that the plasma cells may play a role in itsdeposition. This being so, the question arises whetheror not they are 'neoplastic.' The boundary betweenorbital 'pseudotumours' in which amyloid is laiddown and primary localised amyloidosis in whichcellular infiltration is absent or minimal is not clear,3and a local plasmacytoma of the conjunctiva in whichamyloid was later deposited has been reported.4
Identifying the immunoglobulins carried bylymphocytes and derived cells is of value indifferentiating pseudotumours from lymphomas inthat the former tend to have a heterogeneouspopulation while the latter often show apredominance of cells carrying a particular lightchain.57 The present paper reports on theimmunoglobulin labelling of cells associated withamyloid deposits in 2 cases in which the orbit andeyelid were respectively involved.Correspondence to Dr D. R. Lucas. Department of Pathology, NewMedical School. Oxford Road. Manchester M13 9PT.
Material and methods
CASES1. A 78-year-old man presented with a 2-yearhistory of a painless swelling in the right upper lidwhich was now causing ptosis to the extent of closingthe eye. On examination a smooth hard mass waspalpated in the right upper orbit; this protruded intothe upper lid from behind and displaced the globedownwards. Right upward movement was limited.Right optic atrophy was noted. Orbital x-ray wasnormal, and CT scan showed no extension of thetumour behind the globe.The patient had had a myocardial infarction 3 years
previously and complained of shortness of breath butwas otherwise well. Haemoglobin, white cell andplatelet counts, and plasma urea and electrolytelevels were nonnal at this time.At operation the tumour was poorly encapsulated
and extended back over the globe for some distance.The tumour was therefore removed in a piecemealmanner. At follow-up a month after operation thelesion was thought to be returning: a finn mass,measuring approximately 1 cm in length was palpableunder the orbital rim. The patient was lost to furtherfollow-up.
2. A 46-year-old woman presented withthickening of the left lower lid resulting in entropion,which was subsequently corrected. Eighteen monthslater she was readmitted with recurrence ofthickening of the left lateral canthus and tarsal platefor which a tarsal plate biopsy was performed.
600
on July 20, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.66.9.600 on 1 Septem
ber 1982. Dow
nloaded from

Apparent monoclonal origin of lymphocytes and plasma cells infiltrating ocular adnexal amyloid deposits 601
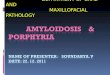
Fig. I Case 1. Amyloid inadipose tissue and walls ofsmallblood vessels and cuffing ofa smallblood vessel by lymphocytes. (PASx 145).
..v :........ .S
..........
. O £. . > A +~~~~~~~~44 4
*............. '~~~~~~~~~~~~~~~~~~~~~~~~......
e........* g e
, .......... . : : .
Subsequent investigations showed normal haemato-logical indices and bone marrow. Immunoglobulinlevels lay within the normal range and no paraproteinwas present. Light chains were not detected in theurine. Chest x-ray was normal, and no evidence ofmyeloma was seen in the dorsal spine. She was other-wise well apart from recurrent urinary frequency andfrequent ectopic beats.
METHODSThe tissue was fixed in unbuffered 10% formalin andembedded in ester wax for normal histology andparaffin wax for immunoperoxidase staining. Tissuefor electron microscopy was postfixed in bufferedglutaraldehyde (after recovery from the paraffinblock in case 2). The PAP method8 was used todemonstrate immunoglobulins. Rabbit antisera forhuman IgG, M, A, and D 150 types and K and A lightchains were obtained from Dako except anti-IgE,which was supplied by Behring. The IgG and Mantisera were diluted to 1/2000, the IgA, D, and E to1/1000, and the anti-K and X to 1/3000. Most sectionswere counterstained by the sodium sulphate-alcianblue method for amyloid.9 In case 1 sections wereexposed to the antisera both with and without priortrypsinisation.
Results
CASE 1Pathological appearances. The specimen consisted of2 pieces of firm fibrofatty tissue measuring 3-0cmX2 5 cmxl5 cm and 2-5 cmx0 5 cm and a hardtranslucent nodule 1-3 cmx0 5 cm.
Microscopically the specimen consisted pre-dominantly of structureless masses of eosinophilic
material together with some fatty tissue and striatedmuscle. The hyaline material stained with Congo redand by the PAS method. It was birefringent andshowed green dichroism after Congo red staining.Numerous foreign body giant cells were present, andthere were foci of lymphocytic infiltration.Occasional plasma cells were identified in these foci,and there was cuffing of small blood vessels bylymphocytes.The hyaline material was observed being laid down
in rings in fatty tissue and also in striated muscle fibres(Fig. 1). A small area of bone formation was present(Fig. 2).
Electron microscopy. The hyaline material showed
Fig. 2 Case 1. Boneformation between masses ofamyloid(Hand E, x54).
on July 20, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.66.9.600 on 1 Septem
ber 1982. Dow
nloaded from

D. R. Lucas, Fiona Knox, and S. Davies
Fig. 3 Case 1. Electronmicrograph showing typicalbundles ofamyloidfibrils.(x38000).
interlacing bundles of non-branching fibrils typical ofamyloid (Fig. 3).Immunoperoxidase staining. Staining of substantial
numbers of the lymphocytes and plasma cellsoccurred only with antisera for X light chains (Fig. 4)and IgA. Labelled cells were not randomly dis-tributed but tended to occur round the periphery offocal aggregates. It was therefore difficult to estimatethe number stained with any accuracy, but in someaggregates it appeared to approach 50%. Onlyoccasional cells stained with antisera for K light chains(Fig. 5), IgG, IgM, IgE, or IgD. Prior treatment withtrypsin appeared to increase the number of cellscarrying IgA but otherwise did not affect the resultssignificantly. Staining of the amyloid with or withoutprior trypsinisation was erratic. With anti-K, X, IgG,and IgM the larger masses were unstained except attheir margins. Occasional small masses engulfed ingiant cell cytoplasm were stained. Occasional giantcells also showed faint diffuse cytoplasmic stainingwith these antisera. The hyaline material was stainedby the sodium-alcian blue counterstain.
CASE 2Pathological appearances. The specimen consisted ofan irregular strip of tissue, 1 5 cmx0 5 cmx0 4 cm.
Microscopically the tissue was composed ofcircumscribed masses of almost acellular hyalinematerial which stained positively by the PAS methodand showed red-green dichroism with Congo red.Small arteries and arterioles in the vicinity alsoshowed hyaline infiltration and mural thickening. Afew foreign body giant cells were seen in relation tothe material.
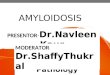
In the adjacent stroma was a mass of lymphocytes,plasma cells, and some histiocytes. Numerous Russellbodies and several small islands of hyaline materialwere present in the infiltrate (Figs. 6a,b). Noepithelium was present in the specimen.
Electron microscopy. The hyaline material had thetypical unbranched fibrillary structure of amyloid.Immunoperoxidase staining. At the periphery of
focal aggregates nearly 100% of the lymphocytes andplasma cells stained for the K chain, though islands ofunstained cells were present (Fig. 7). Somewhat
602
on July 20, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.66.9.600 on 1 Septem
ber 1982. Dow
nloaded from

Apparent monoclonal origin of lymphocytes and plasma cells infiltrating ocular adnexal amyloid deposits 603
Fig. 4 Case 1.Immunoperoxidase stainingfor Xlight chains, substantial group ofheavily stained cells. (x357).
fewer stained for IgG, and the staining was less dense(Fig. 8). Less than 1% of cells stained for the X chain(Fig. 9), while occasional cells also stained for IgAand IgM. No cells stained for IgD and IgE.The amyloid was generally unstained. Some giant
cells showed weak staining with anti-X and K sera.The hyaline material was stained by the sodium
sulphate-alcian blue counterstain.
Discussion
By 1979, 14 cases of orbital amyloidosis had beenpublished and these have been fully reviewed.'0 Sincethen a further 2 cases have appeared." 12 Computed
tomographic scanning contributed to the diagnosis ofthese cases. The ages of the 16 cases ranged from 24 to78, and 11 were females. Deposits of amyloid werenot discovered elsewhere in these cases, but in arather unusual case in a girl of 913 amyloidosisinvolved the inferior nasal meatus, the vocal cords,hard palate, and inner aspect of the nasal bridge,whence it extended into the upper and lower eyelidsto the level of the orbital rims.Amyloid (or hyaline) infiltration of the eyelid has
been described and reviewed.2 1418 The cases appearto show a similar age and sex distribution to thosearising in the orbit.
Deposits in ocular adnexal structures are very
Fig. 5 Case 1.Immunoperoxidase stainingfor Klight chains; only 2 positivelystained cells infield comparable tothat shown in Fig. 4. (x357).
*
* 0,! 4
....: S:..p
X X .. +~~~4
9t $
on July 20, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.66.9.600 on 1 Septem
ber 1982. Dow
nloaded from

D. R. Lucas, Fiona Knox, and S. Davies
(a 6bFig. 6 Case 2. (a) Heavy infiltrate oflymphocytes andplasma cells separatedfrom mass ofamyloid byfibrous band. (x 178).(b) Samefield, numerous Russell bodies mainly alongfibrous band. (x 750).
uncommon in systemic amyloidosis.'8 By contrastdeposits in the central retinal artery and vitreous bodyare more often seen in association with systemicamyloidosis than in its absence. 9The principal pathological features are similar
whatever the location of the adnexal deposits. Thereis deposition of amyloid both as large masses and in
the walls of small blood vessels and in adipose tissue.Giant cells are present in varying numbers, and acellular infiltrate composed of lymphocytes andplasma cells is usually present, though its density mayvary considerably and is sometimes minimal. 2 The 2cases described here show these general features butdiffer in minor particulars. In case 1 the giant cell
Fig. 7 Case 2.Immunoperoxidase stainingfor Klight chains, substantial group ofheavily stained cells atperiphery ofa lvmphoidfocus. (x357).
04u
on July 20, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.66.9.600 on 1 Septem
ber 1982. Dow
nloaded from

Apparent monoclonal origin of lymphocytes and plasma cells infiltrating ocular adnexal amyloid deposits 605
Fig. 8 Case 2.Immunoperoxidase stainingforIgG, substantial group ofcellsshowing positive staining mainly atperiphery oflymphoidfocus.(x357).
reaction is particularly conspicuous; the cellularinfiltration is predominantly lymphocytic and notvery dense. Bone formation is unusual, but has beendescribed previously.20 In case 2 the giant cellreaction was minimal and the cellular infiltrate denserand predominantly plasmacytic. The very numerousRussell bodies are also unusual but have been notedpreviously.2'The electron microscope findings serve to confirm
that the material has the typical fibrillary structure ofamyloid, but fixation was too poor to allow any con-clusions to be drawn as to the relationship of thefibrils to component tissue cells, which is at presentsomeWhat controversial.'2 '3The reaction of the amyloid itself and associated
giant cells to immunoperoxidase staining was tooerratic for conclusions to be drawn.The principal interest of the 2 cases is the apparent
monoclonality of the cellular infiltrate associated withthe amyloid. Thus, those cells that were labelledshowed an overwhelming preponderance reacting forX chains and IgA in case 1 and for K chains in IgG incase 2. A greater proportion of the infiltrate reactedin case 2, probably because of the higher proportionof plasma cells. No previous immunoperoxidasestudies appear to have been made on comparablecases, but in a case of orbital amyloidosis a suspensionof cells obtained was stained with fluorescein-labelledantisera and found to show 30% of the cells reactingfor IgG, 24% for K chains and4% for X chains.2' Since
Fig. 9 Case 2.Immunoperoxidase stainingfor Xlightchains; only3stainedcells infield comparable to that shown in
* ,w * - Fig. 7. (x357).
*.i
on July 20, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.66.9.600 on 1 Septem
ber 1982. Dow
nloaded from

D. R. Lucas, Fiona Knox, and S. Davies
in normal serum 65% of the immunoglobulinmolecules are of the K type and 35% X,22 it issurprising that this was not considered by the authorto indicate monoclonality.The general pathogenesis of amyloid deposition
has recently been comprehensively reviewed,2325 asalso has its deposition in relation to the eye andadnexa.226 The relative importance of immunocytesand macrophages remains controversial. Making theassumption that the lymphocytes and plasma cellsassociated with the amyloid infiltrates have a primarypathogenetic role, the apparent monoclonality of thepopulations is consistent with the view expressed byGlenner25 that they represent 'burnt out' local extra-medullary plasmacytomas. That there is no clear-cutboundary between orbital amyloidosis and pseudo-tumours3 does not rule out such a conclusion becauseplasmacytic pseudotumours are difficult to distinguishfrom true extramedullary plasmacytomas except onthe basis of the monoclonality or otherwise of theirconstituent cells.27
In view of the large local population of lympho-cytes and plasma cells in the tarsal conjunctiva it is notsurprising that the conjunctiva and lids are involvedmore frequently than the orbit. It is noteworthy thatin case 1, in which the process apparently started inthe orbit, the predominant heavy chain carried by theinfiltrating cells was IgA, which is consistent withderivation of the progenitor cell or cells from theconjunctiva.Note added in proof: Case 2 has developed a
localised thickening of the eyelid at the same site afteran interval of 2 years and 4 months. Tissue excised forcosmetic reasons and examined histologically con-tained amyloid with very few infiltrating cells.
Thanks are due to Mr 1. M. Strachan. Mr S. K. Sharma, andDr W. C. Walker for providing clinical details and to Miss K. Hughesand Mrs L. Thomas for skilled technical assistance. Professor W. L.Ford kindlv read the manuscript and made helpful comments.
References
Duke-Elder S. Amvloidosis of the orbit. System ofOphthalmology. London: Henrv Kimpton. 1974: 3 (2).
2 Knowles DM 11. Jakobiec F. Rosen M. Howard G. Ocularamvioidosis. Suirv Ophthalmol 1975; 19: 367-84.
3 Henderson JW. Orbital Tuimors. Philadelphia: Saunders, 1973.
4 Glass R, Scheie HG, Yanoff M. Conjunctival amyloidosis arisingfrom a plasmacytoma. Ann Ophthalmol 1971;3: 823-5.
5 Levv R, Warnke R, Dorfman RF, Haimovich J. The mono-clonalitv of human B-cell lymphomas. J Exp Med 1977; 145:1014-8.
6 Warnke R. Levv R. Immunopathology of follicular lymphomas.N Engl J Med 1978; 298: 481-6.
7 Knowles DM, Jakobiec F. Halper AP. Immunological character-isation of ocular adnexal lymphoid neoplasms. Am J Ophthalmol1979; 87: 603-19.
8 Burns J. Background staining and sensitivity of the unlabelledantibody-enzyme (PAP) method. Comparison with theperoxidase labelled antibody sandwich method using formalinfixed paraffin embedded material. Histochemistrv 1975; 43:291-4.
9 Lendrum AC, Slidders W, Fraser DS. A study of renal hyalineamyloidosis and diabetic fibrinous vasculosis with new stainingmethods. J Clin Pathol 1972; 25: 373-96.
10 Nehen JH. Primary localised orbital amyloidosis. ActaOphthalmol (Kbh) 1979; 57: 287-95.
11 Cohen MM. Lessell S. Amyloid tumours of the orbit. Neuro-radiology 1979;18: 157-9.
12 Finlay KR, Rootman J, Dimmick J. Optic atrophy in primaryorbital amvloidosis. Can J Ophthalmol 1980; 15: 189-92.
13 Kaiser-Kupfer MI. McAdam KPWJ, Kuwabara T. Localisedamvloidosis of the orbit and upper respiratorv tract. Am JOphthalmol 1977; 84: 721-8.
14 Ashton N. Rey A. Hvaline infiltration of the eyelid. Br JOphthalmol 1951; 35: 125-33.
15 Richlin JJ, Kuwabara T. Amyloid disease of the eyelid and con-junctiva. Arch Ophthalmol 1962; 67: 139-42.
16 Halasa AH. Amyloid disease of the eyelid and conjunctiva. ArchOphthalmol 1965; 74: 298-301.
17 Smith ME. Zimmerman L. Amyloidosis of the eyelid and con-junctiva. Arch Ophthalmol 1965; 75:42-51.
18 Brownstein MH. Elliott R. Helwig E. Ophthalmologic aspects ofamvloidosis. Am J Ophthalr,zol 1970; 69: 423-30.
19 Ferrv AP, Lieberman TW. Bilateral amvioidosis of the vitreousbodv. Arch Ophthalmol 1976; 94: 982-91.
20 Hameed S. Nath K. Bone formation in the tarsal plate associatedwith amvloidosis following trauma. Am J Ophthalmol 1960; 49:814-5.
21 Jensen OA. Bilateral amyloidosis of the orbit. Ophthalmologica1976:173: 70-8.
22 Roitt IM. Essential Immunology. Oxford: Blackwell, 1977.23 Scheinberg MA. Cathcart ES. New concepts in the pathogenesis
of primary and secondary amyloid disease. Clin Exp Immunol1978; 33: 185-90.
24 Glenner GG. Amyloid deposits and amyloidosis: the , fibrilloses.Part 1. N EnglJ Med 1980; 302:1283-92.
25 Glenner GG. Amyloid deposits and amyloidosis: the 13 fibrilloses.Part 2. N EnglJ Med 1980; 302: 1333-43.
26 Doughman DJ. Ocular amyloidosis. Sunrv Ophthalmol 1968; 13:33-42.
27 Khalil MK. Huang S. Viloria J. Duguid WP. Extramedullaryplasmacvtoma of the orbit: case report with results of immuno-cvtochemical studies. Can J Ophthalmol 1981; 16: 39-42.
606
on July 20, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.66.9.600 on 1 Septem
ber 1982. Dow
nloaded from