Embed Size (px)
Citation preview

H[te
agogn
C
Trm
R
[6] Cho YK, Kim JK, Kim WT, Chung JW. Hepatic resection versus radiofrequencyablation for very early stage hepatocellular carcinoma: a Markov modelanalysis. Hepatology 2010;51:1284–1290.
[7] Feng K, Yan J, Li X, Xia F, Ma K, Wang S, et al. A randomized controlled trial ofradiofrequency ablation and surgical resection in the treatment of smallhepatocellular carcinoma. J Hepatol 2012;57:794–802.
[8] Lindner U, Trachtenberg J, Lawrentschuk N. Focal therapy in prostate cancer:modalities, findings and future considerations. Nat Rev Urol2010;7:562–567.
[9] Livraghi T, Meloni F, Di Stasi M, Rolle E, Solbiati L, Tinelli C, et al. Sustainedcomplete response and complications rates after radiofrequency ablation ofvery early hepatocellular carcinoma in cirrhosis: is resection still thetreatment of choice? Hepatology 2008;47:82–89.
[10] Francica G, Saviano A, De Sio I, De Matthaeis N, Brunello F, Cantamessa A,
L
6
If one considers the high rate of effectiveness in destroyingCC lesions up to 3 cm with low morbidity and no mortality
9,10], then RFA is the ideal technique to eradicate a smallumoral focus (early HCC), minimizing the risk associated withxpectant management.
Thanks to the large experience in local ablation of liver cancerccumulated over the last three decades, all among hepatologists,astroenterologists, and radiologists involved in the managementf patients with HCC, seem to be far ahead along the way urolo-ists are tempting to pursue. We think that a step backward isot warranted at this time.
etters to the Editor
onflict of interest
he authors declared that they do not have anything to discloseegarding funding or conflict of interest with respect to this
anuscript.
eferences
[1] Midorikawa Y, Takayama T, Shimada K, Nakayama H, Higaki T, Moriguchi M,et al. Marginal survival benefit in the treatment of early hepatocellularcarcinoma. J Hepatol 2013;58:306–311.
[2] Heidenreich A, Bellmunt J, Bolla M, Joniau S, Mason M, Matveev V, et al. EAUguidelines on prostate cancer. Part 1: screening, diagnosis, and treatment ofclinically localised disease. Eur Urol 2011;59:61–71.
[3] Dall’Era MA, Albertsen PC, Bangma C, Carroll PR, Carter HB, Cooperberg MR,et al. Active surveillance for prostate cancer: a systematic review of theliterature. Eur Urol 2012;62:976–983.
[4] Llovet JM, Vilana R, Bru C, Bianchi L, Salmeron JM, Boix L, et al. Increased riskof tumor seeding after percutaneous radiofrequency ablation for singlehepatocellular carcinoma. Hepatology 2001;33:1124–1129.
[5] Livraghi T, Lazzaroni S, Meloni F, Solbiati L. Risk of tumour seeding afterpercutaneous radiofrequency ablation for hepatocellular carcinoma. Br JSurg 2005;92:856–858.
et al. Long-term effectiveness of radiofrequency ablation for solitary smallhepatocellular carcinoma: a retrospective analysis of 363 patients. Dig LiverDis 2013;45:336–341.
Giampiero Francica⇑Interventional Ultrasound Unit, Pinetagrande Hospital,
Castelvolturno (CE), Italy⇑Corresponding author.E-mail address: [email protected]
Ilario de SioDepartment of Internal Medicine and Gastroenterology,
Second University of Naples, Naples, Italy
Maurizio PompiliDepartment of Internal Medicine,
Catholic University of The Sacred Heart, Rome, Italy
Tito LivraghiInterventional Radiology Department, Istituto Clinico Humanitas,
Rozzano (MI), Italy
Reply to: ‘‘ ‘‘Wait and see’’ policy for early hepatocellular carcinoma’’
To the Editor:Is early hepatocellular carcinoma (HCC) really a life-threateningdisease?
We would like to thank Dr. Francica for his interest in ourrecently published article on the marginal survival benefit of sur-gery for early HCC [1]. Although our data did not refer to thetreatment for early HCC by radiofrequency ablation (RFA), wehad expected their proposal that early HCC patients are good can-didates for RFA because of its low complication rate and high cur-ability. Yet, we believe that their point of view is absolutely notobjective owing to the reasons described below.
First, the cirrhotic liver harboring early HCC is in quite ahighly carcinogenic state, and despite complete removal of earlyHCCs, most of the patients have second primary HCCs, whichreally need to be cured, as shown in Fig. 3B of our article [1]. Inaddition to the long lead-time required for early HCC to becomeovert HCC, it is not too late if early HCCs are resected or ablatedby RFA at the stage of ‘real’ HCC. Thus, early HCC is not a targetlesion for treatment, but a signaling lesion for a second primaryHCC.
Next, it cannot be determined whether early HCC (small hyp-ovascular tumors) treated by RFA are actually HCC or not because
needle biopsy is not usually performed in patients who receiveRFA, as reported by Livraghi et al. [2], in their study, needle biopsywas performed only in 18.3% of patients. This fact suggests thatgood outcomes by RFA might be overestimated because of treat-ment for precursor lesions of HCC. Actually, an apparently lowneoplastic-seeding rate by RFA in high-volume centers asdescribed above can be achieved by avoiding needle biopsy. Wetherefore do not assume that good outcomes of RFA necessarilylead to lower morbidity.
Finally, whether RFA for small HCCs is as effective as liverresection also remains controversial because of the small num-bers of patients enrolled in randomized controlled trials. Onerandomized controlled trial performed by Feng et al. [3] sug-gested that the outcomes of liver resection and RFA are not sig-nificantly different in patients with small HCCs. However, theirstudy group comprised only 168 patients. They concluded thatthe result of percutaneous RFA depended on tumor location,and recommended open or laparoscopic ‘surgery’. It is thereforedifficult to standardize the use of RFA for the treatment of earlyHCC. In addition, a Markov model analysis performed by Choet al. [4] revealed that overall survival after RFA was identicalto that after liver resection, provided that RFA was followed
36 Journal of Hepatology 2013 vol. 59 j 631–640
by liver resection in patients with initial local failure. On theother hand, another randomized controlled trial in larger num-bers of patients reported that liver resection was significantlymore advantageous [5]. Thus, it cannot be simply concludedthat liver resection and RFA are of similar effectiveness forthe treatment of small HCC. To answer the question whetherliver resection is superior to RFA or not, a nationwide random-ized controlled trial involving 600 patients is now ongoing inJapan [6].
We should estimate treatment outcomes for early HCC fromthe stand point of biological characteristics, which differ fromthose of other types of cancers, including prostate cancer. Ourexperience with patients with treated and untreated early HCCsuggests that early HCC pathologically definable as cancer mightclinically be a precancerous lesion. Therefore, the good outcomesobtained by RFA for small HCCs that may include early HCC arelikely to be overestimated by lead-time bias.
Taken together, we advocate that early HCC is not a life-threatening disease and, therefore, both liver resection and RFAare unnecessary treatments for early HCC that cannot be justified,regardless of minimal invasiveness or lower morbidity.
Conflict of interest
The authors declared that they do not have anything to discloseregarding funding or conflict of interest with respect to thismanuscript.
References
[1] Midorikawa Y, Takayama T, Shimada K, Nakayama H, Higaki T, Moriguchi M,et al. Marginal survival benefit in the treatment of early hepatocellularcarcinoma. J Hepatol 2013;58:306–311.
[2] Livraghi T, Lazzaroni S, Meloni F, Solbiati L. Risk of tumour seeding afterpercutaneous radiofrequency ablation for hepatocellular carcinoma. Br J Surg2005;92:856–858.
[3] Feng K, Yan J, Li X, Xia F, Ma K, Wang S, et al. A randomized controlled trial ofradiofrequency ablation and surgical resection in the treatment of smallhepatocellular carcinoma. J Hepatol 2012;57:794–802.
[4] Cho YK, Kim JK, Kim WT, Chung JW. Hepatic resection versus radiofrequencyablation for very early stage hepatocellular carcinoma: a Markov modelanalysis. Hepatology 2010;51:1284–1290.
[5] Huang J, Yan L, Cheng Z, Wu H, Du L, Wang J, et al. A randomized trialcomparing radiofrequency ablation and surgical resection for HCC conform-ing to the Milan criteria. Ann Surg 2010;252:903–912.
[6] Hasegawa K, Kokudo N, Shiina S, Tateishi R, Makuuchi M. Surgery versusradiofrequency ablation for small hepatocellular carcinoma: start of arandomized controlled trial (SURF trial). Hepatol Res 2010;40:851–852.
Yutaka MidorikawaTadatoshi Takayama⇑
Department of Digestive Surgery,Nihon University School of Medicine,
30-1 Oyaguchikami-machi, Itabashi-ku,Tokyo 173-8610, Japan⇑Corresponding author.
E-mail address: [email protected]
Tuberculous sepsis during antiviral HCV triple therapy
To the Editor:Drug users are a high-risk group for contracting infectious dis-eases like tuberculosis (TB), HIV, hepatitis B (HBV), and hepatitisC (HCV). The prevalence of latent tuberculosis infection in drugusers varies from 10% to 59%, and the prevalence of chronicHCV infection in drug users ranges from 25% to 75% [1].
The standard of care for chronic HCV consists of pegylatedinterferon (PegIFN), ribavirin, and boceprevir or telaprevir ingenotype (GT) 1 patients [2]. These drugs have complex immuno-modulatory and antiproliferative effects, which can lead to alter-ations in the cytokine cascade [3,4].
A 33-year-old white male former drug user and prison inmatewas willing to undergo antiviral treatment for HCV after jailrelease. He participated in an opioid maintenance program andhad PCR-proven, treatment-naive, chronic hepatitis C infection,genotype 1a, IL28B polymorphism CT. HBV and HIV co-infectionswere excluded before starting therapy. Active pulmonary TBinfection was ruled out by a normal chest radiograph.
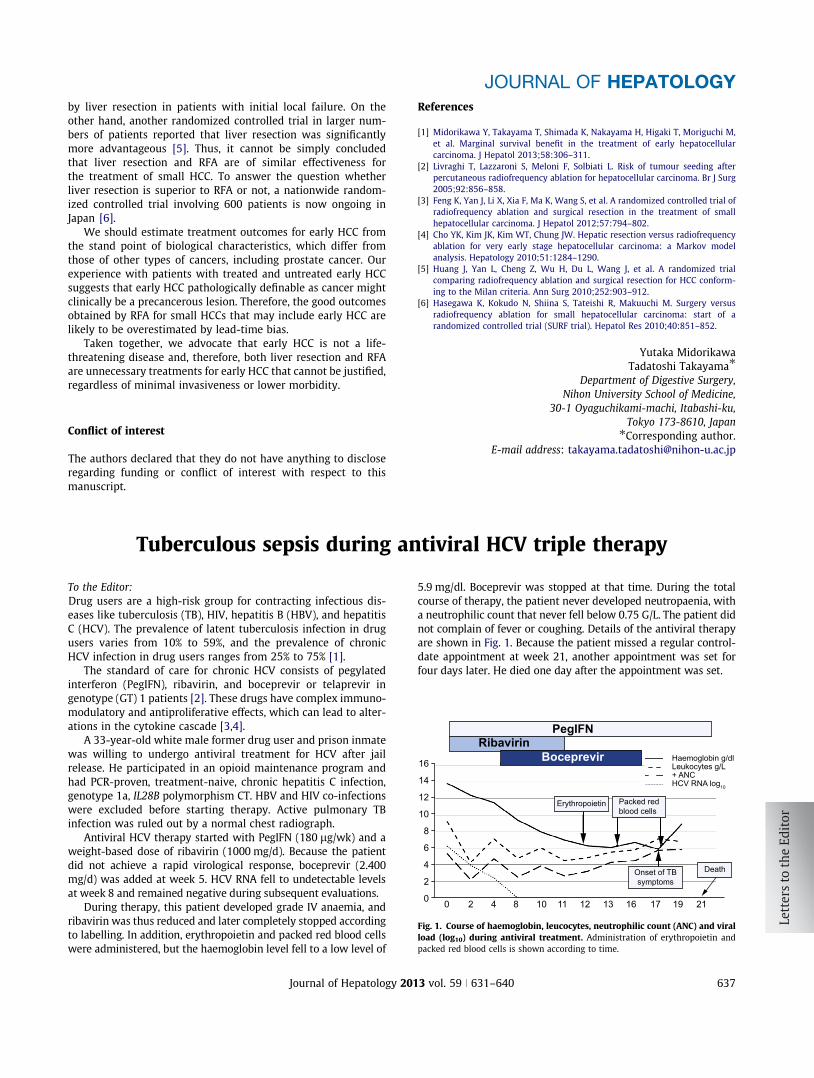
Antiviral HCV therapy started with PegIFN (180 lg/wk) and aweight-based dose of ribavirin (1000 mg/d). Because the patientdid not achieve a rapid virological response, boceprevir (2.400mg/d) was added at week 5. HCV RNA fell to undetectable levelsat week 8 and remained negative during subsequent evaluations.
During therapy, this patient developed grade IV anaemia, andribavirin was thus reduced and later completely stopped accordingto labelling. In addition, erythropoietin and packed red blood cellswere administered, but the haemoglobin level fell to a low level of
5.9 mg/dl. Boceprevir was stopped at that time. During the totalcourse of therapy, the patient never developed neutropaenia, witha neutrophilic count that never fell below 0.75 G/L. The patient didnot complain of fever or coughing. Details of the antiviral therapyare shown in Fig. 1. Because the patient missed a regular control-date appointment at week 21, another appointment was set forfour days later. He died one day after the appointment was set.
PegIFNRibavirin
Boceprevir
Erythropoietin
16
14
12
10
10 11 12 13 16 17 19 21
8
8
6
4
4
2
20 0
Onset of TBsymptoms
Death
Packed redblood cells
Haemoglobin g/dlLeukocytes g/L+ ANCHCV RNA log10
Fig. 1. Course of haemoglobin, leucocytes, neutrophilic count (ANC) and viralload (log10) during antiviral treatment. Administration of erythropoietin andpacked red blood cells is shown according to time.
JOURNAL OF HEPATOLOGY
Journal of Hepatology 2013 vol. 59 j 631–640 637


























