Embed Size (px)
Citation preview

Letters to the Editor
number of patients, especially in thesurgical group (n ¼ 13).
Exclusion of patients with cancerat the time of pulmonary embolism,however, is more complicated thanperforming a Kaplan-Meier survivalanalysis with fewer patients atfollow-up. There are several differenttypes of cancer, of course, and thesurvival and prognosis are influencednot only by the type of cancer (Hodg-kin lymphoma vs pancreatic cancerfor example) but also by the staging(localized vs metastatic), the overallcondition of the patient, and the pa-tient’s age. We agree with McGuireand Rubens that a patient with meta-static cancer will likely have a verypoor prognosis and probably shouldnot undergo aggressive surgery forpulmonary embolism, and this is anassessment that should be performedby the surgeon, the patient, and thefamily at the bedside. If, however,a patient has a history of cancer thathas been treated successfully withsurgery, chemotherapy, or radiationtherapy and as a result has a meaning-ful survival (>1 year), then surgeryfor pulmonary embolism should becarefully considered. In general, forpatients with known diagnosis of can-cer at the time of pulmonary embo-lism, our practice is to consult ourmedical oncology colleagues, whenpatient stability makes this feasible,to give us an assessment of the esti-mated survival. If survival is esti-mated at greater than 1 year, weconsider pulmonary embolism sur-gery and go over this with the patientand family.
Marzia Leacche, MDJohn G. Byrne, MD
Vanderbilt Heart & Vascular InstituteNashville, Tenn
Reference1. Greelish JP, Leacche M, Solenkova N, Ahmad RM,
Byrne JG. Improved long-term outcomes for type A
(central) pulmonary emboli treated surgically. J
Thorac Cardiovasc Surg. 2011;142:1423-9.
http://dx.doi.org/10.1016/j.jtcvs.2012.06.033
736 The Journal of Thoracic and C
THE PARACHUTE TECHNIQUEFOR ANTERIOR LEAFLETPROLAPSETo the Editor:The publication by Zannis and col-
leagues1 highlights the critically im-portant new surgical approach for thetreatment of anterior leaflet prolapse.Konstantinos and colleagues per-formed the parachute technique on44 consecutive patients.1 Echocardio-graphic examination was performedin all patients to measure the distancefrom the tip of each papillary muscleto the annular plane at end systole inan apical view. Constructing the para-chute according to the described dis-tance may cause the persistence ofprolapse because there must be coap-tation depth between the anterior andposterior leaflets.2 The coaptationdepth is approximately 4 mm in theanterior and posterior commissuresand approximately 8 mm betweenthe A2 and P2 scallops. Adjustingthe coaptation depth is not clear inthe article.Furthermore, the authors did not
mention the causes of the patient’s dis-ease. The artificial chordal replacementcan be used in both Barlow’s diseaseand fibroelastic deficiency.3 Nonethe-less, Barlow’s disease has distinct fea-tures. It generally has complex valvepathology and dysfunction, which ismost often multisegmental. Lesions in-clude excessively thick and billowingleaflet segments, chordal elongationand chordal rupture, calcification ofthe papillary muscles or annulus withchordae restriction, and severe annulardilatation with giant valve size.4
Patients with fibroelastic deficiencyoften present withminimal, as opposedto excess, tissue, so extensive leafletresection or complex leaflet remodel-ing procedures are rarely indicated.4
All lesions present should be correctedto store not only valve competency butalso a normal valve geometry and satis-factory line closure. Because excesstissue is the hallmark lesion of Bar-low’s disease, leaflet resection andrestoration of normal relationship of
ardiovascular Surgery c September 201
the annular dimension are usually cen-tral to the surgical strategy.4,5 Theauthors state that in the beginning oftheir experience, large anterior mitralleaflet prolapses had been addressedby triangular resection of some ofthe excess tissue before parachuteimplantation. In the perennial concernof simplification and standardizationof surgical techniques, they havecompletely abandoned anterior mitralleaflet triangular resection, and therunning suture was used to crimpexcessive tissue on the Dacron strip ofthe parachute.1 However, crimpingmay only remove the excess tissue ver-tically, not horizontally. So performingtriangular resection in the anterior leaf-let may improve the result in selectedcases.
This is an admirable study. Thereaders thank the authors for sharingtheir experience and knowledge. Theexplanation of previously describedpoints will be helpful for betterunderstanding.
Murat Tavlasoglu, MDDepartment of Cardiovascular
SurgeryDiyarbakir Military Medical Hospital
Diyarbakir, Turkey
References1. Zannis K,Mitchell-Heggs L,DiNittoV,KirschME,
NoghinM,Ghorayeb G, et al. Correction of anterior
mitral prolapse: the parachute technique. J Thorac
Cardiovasc Surg. 2012;143(4 Suppl):S24-8.
2. Carpentier A, Adams DH, Filsoufi F. Surgical anat-
omyand physiology. In:Carpentier’s Reconstructive
Valve Surgery. St Louis, MO: Saunders; 2010:31.
3. Rankin JS, Orozco RE, Rodgers TL, Alfery DD,
Glower DD. ‘‘Adjustable’’ artificial chordal re-
placement for repair of mitral valve prolapse. Ann
Thorac Surg. 2006;81:1526-8.
4. Anyanwu AC, Adams DH. Etiologic classification
of degenerative mitral valve disease: Barlow’s dis-
ease and fibroelastic deficiency. Semin Thorac Car-
diovasc Surg. 2007;19:90-6.
5. Carpentier A, Adams DH, Filsoufi F. Degenerative
valvular disease. In: Carpentier’s Reconstructive
Valve Surgery. St Louis, MO: Saunders; 2010:270-5.
http://dx.doi.org/10.1016/j.jtcvs.2012.03.085
Reply to the Editor:In this patient series,1 we report our
experience regarding the correction of
2
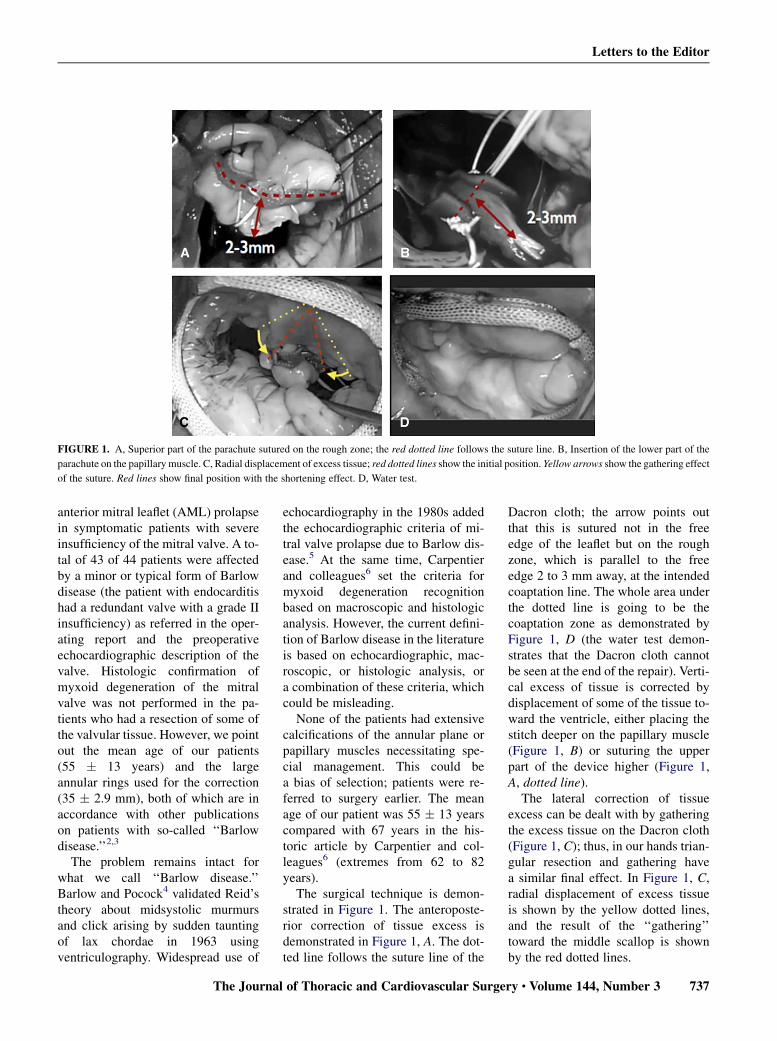
FIGURE 1. A, Superior part of the parachute sutured on the rough zone; the red dotted line follows the suture line. B, Insertion of the lower part of the
parachute on the papillary muscle. C, Radial displacement of excess tissue; red dotted lines show the initial position. Yellow arrows show the gathering effect
of the suture. Red lines show final position with the shortening effect. D, Water test.
Letters to the Editor
anterior mitral leaflet (AML) prolapsein symptomatic patients with severeinsufficiency of the mitral valve. A to-tal of 43 of 44 patients were affectedby a minor or typical form of Barlowdisease (the patient with endocarditishad a redundant valve with a grade IIinsufficiency) as referred in the oper-ating report and the preoperativeechocardiographic description of thevalve. Histologic confirmation ofmyxoid degeneration of the mitralvalve was not performed in the pa-tients who had a resection of some ofthe valvular tissue. However, we pointout the mean age of our patients(55 � 13 years) and the largeannular rings used for the correction(35 � 2.9 mm), both of which are inaccordance with other publicationson patients with so-called ‘‘Barlowdisease.’’2,3
The problem remains intact forwhat we call ‘‘Barlow disease.’’Barlow and Pocock4 validated Reid’stheory about midsystolic murmursand click arising by sudden tauntingof lax chordae in 1963 usingventriculography. Widespread use of
The Journal
echocardiography in the 1980s addedthe echocardiographic criteria of mi-tral valve prolapse due to Barlow dis-ease.5 At the same time, Carpentierand colleagues6 set the criteria formyxoid degeneration recognitionbased on macroscopic and histologicanalysis. However, the current defini-tion of Barlow disease in the literatureis based on echocardiographic, mac-roscopic, or histologic analysis, ora combination of these criteria, whichcould be misleading.
None of the patients had extensivecalcifications of the annular plane orpapillary muscles necessitating spe-cial management. This could bea bias of selection; patients were re-ferred to surgery earlier. The meanage of our patient was 55 � 13 yearscompared with 67 years in the his-toric article by Carpentier and col-leagues6 (extremes from 62 to 82years).
The surgical technique is demon-strated in Figure 1. The anteroposte-rior correction of tissue excess isdemonstrated in Figure 1, A. The dot-ted line follows the suture line of the
of Thoracic and Cardiovascular Surge
Dacron cloth; the arrow points outthat this is sutured not in the freeedge of the leaflet but on the roughzone, which is parallel to the freeedge 2 to 3 mm away, at the intendedcoaptation line. The whole area underthe dotted line is going to be thecoaptation zone as demonstrated byFigure 1, D (the water test demon-strates that the Dacron cloth cannotbe seen at the end of the repair). Verti-cal excess of tissue is corrected bydisplacement of some of the tissue to-ward the ventricle, either placing thestitch deeper on the papillary muscle(Figure 1, B) or suturing the upperpart of the device higher (Figure 1,A, dotted line).
The lateral correction of tissueexcess can be dealt with by gatheringthe excess tissue on the Dacron cloth(Figure 1, C); thus, in our hands trian-gular resection and gathering havea similar final effect. In Figure 1, C,radial displacement of excess tissueis shown by the yellow dotted lines,and the result of the ‘‘gathering’’toward the middle scallop is shownby the red dotted lines.
ry c Volume 144, Number 3 737

Letters to the Editor
Patients with AML prolapse due toBarlow disease were managed usingthe parachute technique in our study.For those patients with extreme excessof tissue, our initial strategy was trian-gular resection to eliminate some ofthe tissue and parachute for treatingthe prolapse. However, triangularresection was completely abandonedfor the most recent patients. As an al-ternative, we have started to crimpexcess tissue on the Dacron cloth,which has further simplified and accel-erated the correction ofAMLprolapse.
Konstantinos Zannis, MDLaurens Mitchell-Heggs, MDD�epartement de Pathologie
CardiaqueInstitut Mutualiste Montsouris
Paris, France
References1. Zannis K, Mitchell-Heggs L, Di Nitto V,
Kirsch ME, Noghin M, Ghorayeb G, et al. Correc-
tion of anterior mitral prolapse: the parachute
technique. J Thorac Cardiovasc Surg. 2012;
143(4 Suppl):S24-8.
2. Adams DH, Rosenhek R, Falk V. Degenerative mi-
tral valve regurgitation: best practice revolution.
Eur Heart J. 2010;31:1958-66.
3. Adams DH, Anyanwu AC, Rahmanian PB,
Abascal V, Salzberg SP, Filsoufi F. Large annulo-
plasty rings facilitate mitral valve repair in
Barlow’s disease. Ann Thorac Surg. 2006;82:
2096-101.
4. Barlow JB, Pocock WA. The significance of late
systolic murmurs and mid-late systolic clicks. Md
State Med J. 1963;12:76-7.
5. Barlow JB, Pocock WA. Billowing, floppy, pro-
lapsed or flail mitral valves? Am J Cardiol. 1985;
55:501-2.
6. Carpentier A, Chauvaud S, Fabiani JN, Deloche A,
Relland J, Lessana A, et al. Reconstructive surgery
of mitral valve incompetence: ten-year appraisal.
J Thorac Cardiovasc Surg. 1980;79:338-48.
http://dx.doi.org/10.1016/j.jtcvs.2012.05.039
THE EFFECT OF INNOMINATECANNULATION ON CEREBRALPERFUSIONTo the Editor:
We congratulate Shi and col-leagues1 on their study, ‘‘Repair ofStanford Type A Aortic DissectionWith Ascending Aorta and HemiarchReplacement Combined With Stent-Graft Elephant Trunk Technique by
738 The Journal of Thoracic and C
Using Innominate Cannulation.’’ Inthis study, the flow in the innominateartery during total body perfusionwas toward the arcus aorta. Duringcerebral perfusion, the flow rate was8 to 10 mL/(kg $ min). Transient neu-rologic deficit occurred in 10 patients,which indicates that this situation isnot a focal event but is related to perfu-sion defect. Urbanski and associates2
pointed out that pressure monitoringis mandatory and explained the com-plications arising from low perfusion.During total body perfusion, the direc-tion of flow is toward the arcus aorta,which causes Venturi effect in thecerebral bed and affects the cerebralperfusion. We conclude that this tech-niquemay cause neurologic complica-tions. We think if pressure monitoringwere to be instituted, this problemcould be predicted.
Sahin Bozok, MDa
Mert Kestelli, MDb
Hakan Karamustafa, MDa
Sedat Ozan Karakisi, MDa
aDepartment of CardiovascularSurgery
Rize University Faculty of MedicineRize, Turkey
bDepartment of CardiovascularSurgery
_Izmir Ataturk Training and ResearchHospital
_Izmir, Turkey
References1. Shi E, Gu T, Yu L, Xiu Z, Zhang Z, Wang C, et al.
Repair of Stanford type A aortic dissection with
ascending aorta and hemiarch replacement com-
bined with stent-graft elephant trunk technique by
using innominate cannulation. J Thorac Cardiovasc
Surg. 2011;142:1458-63.
2. Urbanski PP, Lenos A, Zacher M, Diegeler A. Uni-
lateral cerebral perfusion: right versus left. Eur
J Cardiothorac Surg. 2010;37:1332-6.
http://dx.doi.org/10.1016/j.jtcvs.2012.03.086
Reply to the Editor:We thank Bozok and colleagues for
their insightful comments on thetechnique of innominate artery cannu-lation during surgical repair of
ardiovascular Surgery c September 201
Stanford type A aortic dissection, asdescribed in our recently publishedarticle.1
Cannulation of the innominate arterydirectly2 or with a side graft3 has beenshown to be a simple and effective al-ternative in aortic arch surgery. In ourseries, 10 patients showed transientneurologic dysfunction, and in mostcases this was simple confusion lastingless than 48 hours. No permanent neu-rologic dysfunction occurred. Tran-sient neurologic dysfunction such asconfusion is a frequent complicationafter cardiac surgery, especially amongaged patients. We do not think that ourresults for brain protection are bad.During total body perfusion, the braincan be perfused through the left carotidartery as well as the right carotid artery.Therefore innominate artery cannula-tion is safe during surgical repair ofStanford A aortic dissection. We alsoagree, however, that pressure monitor-ing makes cerebral perfusion moreaccurate.
Enyi Shi, MD, PhDTianxiang Gu, MD, PhD
Department of Cardiac SurgeryFirst Affiliated Hospital
China Medical UniversityShenyang, China
References1. Shi E, Gu T, Yu L, Xiu Z, Zhang Z, Wang C, et al.
Repair of Stanford type A aortic dissection with as-
cending aorta and hemiarch replacement combined
with stent-graft elephant trunk technique by using
innominate cannulation. J Thorac Cardiovasc
Surg. 2011;142:1458-63.
2. Ji S, Yang J, Ye X, Wang X. Brain protection by
using innominate artery cannulation during aor-
tic arch surgery. Ann Thorac Surg. 2008;86:
1030-2.
3. Huang FJ, WuQ, Ren CW, Lai YQ, Yang S, Rui QJ,
et al. Cannulation of the innominate artery with
a side graft in arch surgery. Ann Thorac Surg.
2010;89:800-3.
http://dx.doi.org/10.1016/j.jtcvs.2012.05.062
ALCOHOL AND ADHESIONSTo the Editor:
The recent article by Lassaletta andcolleagues1 fascinated me, just as did
2





























